The Florida Alzheimer’s Disease Medicaid Waiver Program: An Evaluation of Alzheimer’s Beneficiaries Prior to Program Initiation David A. Chiriboga,* Marion Becker,** Lisa Brown,*** Sharon Anderson, Donna Cohen, Larry Dupree, Amber Gum, Margaret Kane, Yuri Jang, William Kearns, Glenn Mitchell II, Victor Molinari, Larry Schonfeld, Mary Ann Watson June, 2005 Louis de la Parte Florida Mental Health Institute University of South Florida Suggested citation: Chiriboga, D., Becker, M., Brown, L., Anderson, S., A., Cohen, D., Dupree, L., et al. (2005) The Florida Alzheimer’s Disease Medicaid waiver program: An evaluation of Alzheimer’s beneficiaries prior to program initiation. Tampa FL: University of South Florida, Louis de la Parte Florida Mental Health Institute. *Principal investigator; **Principal investigator on pharmacy substudy; ***Co-principal investigator Submitted to the Florida Agency for Health Care Administration under contract M0505. i

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Florida Alzheimer’s Disease Medicaid Waiver Program: An Evaluation of Alzheimer’s Beneficiaries Prior to Program Initiation
David A. Chiriboga,* Marion Becker,** Lisa Brown,*** Sharon Anderson,
Donna Cohen, Larry Dupree, Amber Gum, Margaret Kane,
Yuri Jang, William Kearns, Glenn Mitchell II, Victor Molinari,
Larry Schonfeld, Mary Ann Watson
June, 2005 Louis de la Parte Florida Mental Health
Institute University of South Florida
Suggested citation: Chiriboga, D., Becker, M., Brown, L., Anderson, S., A., Cohen, D., Dupree, L., et al. (2005) The Florida Alzheimer’s Disease Medicaid waiver program: An evaluation of Alzheimer’s beneficiaries prior to program initiation. Tampa FL: University of South Florida, Louis de la Parte Florida Mental Health Institute. *Principal investigator; **Principal investigator on pharmacy substudy; ***Co-principal investigator Submitted to the Florida Agency for Health Care Administration under contract M0505.
i

Table of Contents Executive Summary .............................................................................................................................................1Part One.................................................................................................................................................................3
Background and Literature Review...............................................................................................................3Background ..................................................................................................................................................3
Pinellas County: Gulf Coast Jewish Family Services, Inc. (GCJFS). ..............................................5Miami/Dade and Broward Counties: Miami Jewish Home and Hospital for the Aged, Inc (MJHHA). ................................................................................................................................................5Current Status of Vendor Operations .................................................................................................5Eligibility of Waiver Program Participants .........................................................................................6The Evaluation Process as Described in the Request to CMS........................................................6
Statement of the Question.........................................................................................................................7Supporting Literature..................................................................................................................................7
Prevalence of Alzheimer’s Disease by Age.........................................................................................9Nature of the Disease ............................................................................................................................9Dementia Research...............................................................................................................................10Treatment of AD and Related Dementias........................................................................................10AD and Mental Illness .........................................................................................................................11AD and Sex............................................................................................................................................11AD and Race/Ethnicity.......................................................................................................................11AD and Depressive Symptoms and Disorders................................................................................13AD and Wandering ..............................................................................................................................15AD and Lethal Violence ......................................................................................................................16
.................................................................................................................................................................Caregiving and Family Training .........................................................................................................17AD and Psychotropic Medication......................................................................................................19Dementia and Nursing Home Placement.........................................................................................20
Part Two. Research Methods and Results for Questions 1-3 .....................................................................20General Procedures .......................................................................................................................................21
Identification and Development of the Two Comparison Groups..................................................21The Aged and Disabled Comparison Group. ..................................................................................23The Mixed Group.................................................................................................................................23
Procedures ..................................................................................................................................................23Results..............................................................................................................................................................27
Socio-Demographic, Health and Utilization Differences by Group ................................................27Demographic Differences. ..................................................................................................................27Mental and Physical Health Indicators..............................................................................................30Days spent living in the community. .................................................................................................30Ethnic/racial differences in days spent in community. ..................................................................30Nursing Facility Admission.................................................................................................................32Ethnic/racial differences in Medicaid days spent in nursing facilities. ........................................33Months of Medicaid eligibility. ...........................................................................................................33
Cost Implications ......................................................................................................................................34Behavioral health. .................................................................................................................................34Non-specific health expenditures.......................................................................................................38Psychotropic and cognate medications. ............................................................................................39Non-specific and overall pharmacy expenditures. ..........................................................................39Total expenditures. ...............................................................................................................................39
The Socio-Demographic Predictors of Admission to a Nursing Facility ........................................40Discussion and Policy Implications ............................................................................................................41
Evaluation Study Limitations ..................................................................................................................44
ii

Table of Contents Part Three: Drug Issues in Care of Beneficiaries with Alzheimer’s Disease ...........................................44
Context of the Investigation of Drug Issues.............................................................................................44Need for Research.....................................................................................................................................45Specific Aims .............................................................................................................................................45
Study Questions ....................................................................................................................................45Hypotheses ............................................................................................................................................45
Methods and Data Sets .................................................................................................................................46Sample .........................................................................................................................................................46
Results..............................................................................................................................................................47Study Question 1 .......................................................................................................................................47
Demographic Characteristics..............................................................................................................48Age and Sex.......................................................................................................................................48Race/Ethnicity..................................................................................................................................48Mental Health Diagnoses................................................................................................................48Psychotropic Medication ................................................................................................................49
Study Question 2 .......................................................................................................................................54Nursing Home Admission and Time to Nursing Home Placement............................................54
Study Question 3 .......................................................................................................................................56Study Question 4 .......................................................................................................................................58
Study Limitations ...........................................................................................................................................59Discussion and Policy Implications ............................................................................................................59
References............................................................................................................................................................61Appendix A: FMHI PSRDC Catcaid Documentation.................................................................................72
Background.....................................................................................................................................................72Steps in Mental Health Catcaid Assignment .............................................................................................73Steps in Physical Health Catcaid Assignment ...........................................................................................74
List of Tables Table 1. Total Deaths From Alzheimer’s Disease, Top Six Counties in Florida......................................3 Table 2. Recipient Race/Ethnicity Codes for 10% of All Medicaid Clients ...........................................12 Table 3. Race Distribution For Medicaid Beneficiaries Over 60 Years of Age ......................................12 Table 4. Data Sets Used to Create Comparison Groups ............................................................................22 Table 5. Hierarchy Of ICD-9-CM Codes For Mental Health Diagnoses................................................24 Table 6. ICD-9-CM Codes For Mental Retardation, Alcohol Abuse And Substance Abuse...............24 Table 7. Service Category Descriptions and Corresponding Catcaid Codes...........................................25 Table 8. Dates of Study Entry, FY 2001–2002 ............................................................................................25 Table 9. Nursing Home Admission Dates, FY 2001–2002........................................................................26 Table 10. Mixed Group and ADW Group Demographics, FY 2001–2002..........................................29 Table 11. Participants’ Medicaid-Eligible Community Days, by Race......................................................32 Table 12. Participants’ Medicaid-Eligible Days in a Nursing Facility, by Race .......................................33 Table 13a. Service Costs for AD Beneficiaries Participating in the Aged/Disabled Waiver Program 35Table 13b. Service Costs for AD Beneficiaries Not Participating in the Aged/Disabled Waiver
Program ......................................................................................................................................................36 Table 13c. Service Cost Data for All Study Participants Combined.........................................................37 Table 14. Correlations of Demographic Characteristics with Nursing Facility Admission ..................40 Table 15. Hierarchy of ICD-9-CM Codes for Mental Health Diagnoses ................................................47 Table 16. Other ICD-9-CM Codes Employed for Classification..............................................................47 Table 17a. Characteristics of Elders with AD and a Cognate Drug .........................................................50
iii

List of Tables Table 17b. Characteristics of Elders With AD Not Taking a Cognate Drug..........................................51 Table 18a. Characteristics of Elders Without AD Receiving Psychotropic and Cognate Drugs.........52 Table 18b. Characteristics of Elders Without AD Receiving Cognate Drugs..........................................53 Table 19. Service Categories and Catcaid Codes...........................................................................................56 Table 20a. Medicaid Expenditures for Elders Receiving Cognate Therapy & No Psychotropics.......57 Table 20b. Medicaid Expenditures for Elders Receiving a Cognate Drug and “Newer” Psychotropic
......................................................................................................................................................................57Table 20c. Medicaid Expenditures for Elders Receiving a Cognate Drug and “Older” Psychotropic
......................................................................................................................................................................58 List of Figures Figure 1. Conditional Probability of Nursing Home Admission ..............................................................55
iv

Executive Summary Alzheimer’s disease afflicts over 4.5 million persons in the United States, and almost half a million Floridians. In response to the social, medical and fiscal challenges posed by the disease, Florida has initiated a new waiver program, the Florida Medicaid Alzheimer’s Home and Community-Based Waiver Program. The four counties that comprise the site of the waiver program are those that historically have demonstrated the highest number of deaths due to Alzheimer’s disease: Dade, Palm Beach, Broward and Pinellas. As a means of establishing the characteristics of Medicaid beneficiaries with Alzheimer’s disease during a time prior to the implementation of the new waiver program, two sets of investigations were conducted. The first looked at some general questions about the socio-demographic and health characteristics of beneficiaries with Alzheimer’s disease, their patterns of service utilization and associated costs, and variations by racial/ethnic group membership. The second investigation looked specifically at medications used by beneficiaries with Alzheimer’s disease and other dementias, and was based on a slightly different sampling approach. In the first investigation, found in Part Two of the report, the initial screen for sample eligibility was based on Florida Medicaid beneficiaries who entered fiscal year (FY) 2001–2002 with a diagnosis of Alzheimer’s disease. From an initial pool consisting of all beneficiaries with Alzheimer’s disease, those who entered the study period with no recent history of nursing home stays and who were age 60 and over were selected. Two groups were then established, based on Medicaid administrative data. The first group (n = 58) was designated as the Aged and Disabled Waiver (ADW) Group. It consisted of beneficiaries who during the study year participated for six months or more in the Aged and Disabled home and community-based waiver program; the latter was specified in the Florida submission to CMS as the appropriate comparison group for the actual Alzheimer’s disease waiver program evaluation. The second group (n = 390), designated as the Mixed Group, consisted of beneficiaries who had not participated for any length of time in the Aged and Disabled waiver program. It should be noted that beneficiaries in the two comparison groups were drawn from the entire state of Florida: there were insufficient numbers of beneficiaries with Alzheimer’s disease in the four county area of the Alzheimer’s Waiver Program to rely solely on those counties. The two study groups were generally similar in socio-demographic factors, except that the Mixed Group contained significantly more African Americans, and the ADW Group contained significantly more beneficiaries whose race/ethnicity was identified as “Other.” The proportion of individuals in the “Other” category was a rather surprising 45%, in the ADW Group. Those in the Mixed Group were also more likely to have a diagnosis of major psychotic disorder, and overall were more likely to have a mental health diagnosis than were members of the ADW Group. The two groups did not differ in the number of physical health problems, as measured by the Charlson Index, nor did they differ in the number of Medicaid-eligible days spent in the community (as opposed to a nursing facility). Given the greater likelihood of mental health problems in the Mixed Group, it is surprising that per member annual costs associated with mental health service utilization were significantly higher for the ADW Group. Also surprising is that health service expenditures were significantly higher—in both a statistical and an overall cost sense—for those in the ADW Group. This is in spite of the fact that the two groups did not demonstrate an overall difference in the number of physical problems. Since the rates of admission to nursing facilities were roughly comparable for the two groups, the question remains open as to whether or not participation in the Aged and Disabled waiver program was allowing beneficiaries to remain in the community longer, by addressing physical health problems. Participation in the ADW program may not be that helpful for beneficiaries with AD.
1

With regard to race/ethnicity, the investigation found that Hispanic beneficiaries in the Mixed Group had significantly fewer Medicaid-eligible days in the community than both Whites and Others. On the other hand, there were no significant differences by race/ethnicity in the average number of days spent in a nursing facility. The small sample sizes (and a resulting lack of statistical power) may have been the reason for the lack of significant results, however, since in terms of percentages there do seem to be impressive differences (i.e., a substantial effect size). Specifically, nearly 24% of the Hispanic beneficiaries in the combined sample were admitted to a nursing facility, compared with 13% of Whites and 7% of those in the Other category. Clearly, race and ethnicity deserve more attention, particularly from the perspective of whether the needs of Hispanic beneficiaries are being met. It also would be helpful to obtain a better understanding of the composition of the “Other” category, since this group was well-represented in both study groups. The correlations by race with admission to a facility did indicate that Hispanics in the Mixed Group were more likely to be admitted, and that those in the “Other” category were least likely. One policy-relevant finding emerged from an examination of the correlates of admission to a nursing facility. Two indicators of mental health problems, the presence of a major psychotic disorder and a history of a Baker Act exam, were significantly associated with admission to a nursing facility in the Mixed Group and in the combined sample. These correlations, coupled with the findings in both Parts Two and Three that the overall use of cognate drugs was relatively low for beneficiaries with an existing diagnosis of Alzheimer’s disease, underscore the need for medication review and appropriate use of the existing, established cognate medications. In Part Three, the focus of the investigation was the different usages of newer and older antipsychotic and antidepressants. The sample consisted of all Medicaid recipients in FY 2002–2003 who were aged 60 and over and were receiving cognate therapy, either because they had been diagnosed with Alzheimer’s disease, or because they in the “pre-clinical” stage of the disease. Results indicated that, contrary to expectations, elderly Medicaid recipients receiving cognate therapy and “newer,” more expensive psychotropic medications, not only had increased average per user per month (PUPM) Medicaid pharmacy expenditures but also increased PUPM expenditures for mental health, physical health, and inpatient mental health services. The reason why elderly beneficiaries receiving “newer” psychotropic drugs also had increased non-pharmacy expenditures is unknown. However, it is possible that elders receiving “newer” atypical antipsychotic medication were treatment-resistant patients with more severe mental illnesses who were switched from “older” medications due to previous treatment difficulties. In addition, elders receiving the more expensive psychotropic drugs had an increased number of Baker Act examinations and mental health hospitalizations. Overall, there was no evidence that provision of the more expensive drugs resulted in improved outcomes for the study population. Expenditure data also indicated that within the population of Medicaid elders receiving cognate therapy, those who were receiving psychotropic medication used more services, at greater cost to Medicaid. In conclusion, results presented in Part Three indicated that sub-groups within the community-dwelling Medicaid population of elders that we examined had disparate expenditure outcomes, disparate rates of nursing home admission and disparate time to nursing home placement. Taken together, these data suggest that any future evaluation of the cost neutrality of Florida’s Aged and Disabled Waiver Program should evaluate sub-groups within the population separately to determine the costs and benefits of future Waiver Program services provided.
2

This report is divided into three parts. Part One presents the background to the overall evaluation, literature pertaining to Alzheimer’s disease and associated problems and interventions, and a statement of the four research questions to be addressed in the report. Part Two presents the research methodology and findings related to those research questions dealing with characteristics of the Medicaid beneficiaries who were assessed, the types of services they received, and ethnic minority variations in days spent in community. Part Three presents results from a separate investigation dealing with research questions specific to pharmacy issues.
Part One
Background and Literature Review Background The Florida Medicaid Program submitted a 1915 (b)(4) home- and community-based waiver proposal, and a concurrent 1915 (c) proposal, to the federal Centers for Medicare and Medicaid Services (CMS) in November 2003. As approved by CMS, the proposal called for a Medicaid Alzheimer’s Home and Community-Based Waiver Program—one of five condition- or disease-specific waivers available in Florida. In the subsequent request for proposals generated by the Florida Agency for Health Care Administration (Agency for Health Care Administration [AHCA], 2004), the intent of the Florida Medicaid Alzheimer’s Home and Community-Based Waiver Program was expressed as being “to assist persons with Alzheimer’s disease to remain in the community and maintain their functioning as long as possible by providing supportive services to the beneficiaries and their caregivers.” A competitive process was included to select three vendors, to singly serve one of the three areas included in the waiver: Dade and Broward counties, Pinellas county, and Palm Beach county. The vendor for Dade and Broward counties was projected to enroll and maintain a caseload of 190 beneficiaries, while the remaining two vendors were projected to each enroll and maintain a caseload of 80 beneficiaries. Table 1 presents the total deaths in Florida attributable to Alzheimer’s disease (AD) from 1999 through 2003 for the six highest-ranked counties in 2003. The four counties selected for the waiver reported the highest death rates. For comparison purposes, Table 1 also includes Hillsborough and Volusia counties, which were fifth- and sixth-ranked. Combined, the four counties included in the waiver account for over a third—approximately 35.56%—of deaths attributed to AD in Florida for 2003. It is also notable that the these four counties vary widely in the percent change between 1999 and 2003 in deaths attributable to AD, suggesting that very different dynamics are at work in these counties. Similar fluctuations were found in Hillsborough and Volusia, suggesting that wide variations percentage change can be expected. Table 1. Total Deaths From Alzheimer’s Disease, Top Six Counties in Florida*
County 1999 2000 2001 2002 2003 Change, 99–03
Dade 343 371 395 438 537 56.56% Palm Beach 298 295 323 354 382 28.19% Broward 309 274 362 360 362 18.30% Pinellas 252 291 290 281 252 0.0% Hillsborough 138 125 158 183 213 54.35% Volusia 138 119 130 150 179 29.71% State Total 3,057 3,257 3,632 4,046 4,311 41.02% * Source: Florida Department of Health
3

The successful vendors were expected to:
1. Develop a network of service providers to deliver direct services to beneficiaries. The direct services were to consist of those identified by each vendor as commensurate with or equal to “best practices that are effective in meeting the needs of persons with Alzheimer’s disease (AHCA, 2004).” Authorized services included:
a. Case management b. Adult day care c. Respite care d. Wanderer alarm systems e. Wanderer identification and location programs f. Caregiver training g. Behavioral assessment and intervention h. Incontinence supplies i. Personal care assistance j. Environmental modifications k. Pharmacy review,
2. Assist with screening, assessing, and enrolling eligible beneficiaries, 3. Plan and implement a continuing array of services for beneficiaries as their condition
declines, 4. Coordinate discharge of beneficiaries from the program to appropriate settings when
necessary, 5. Document successful interventions for dissemination to other practitioners, and 6. Assist the State in evaluating processes and outcomes in order to develop successful
initiatives for further implementation The Alzheimer’s Disease Medicaid Waiver Program was targeted to a specific subset of beneficiaries with Alzheimer’s disease. For inclusion, the beneficiary had to be:
• Age 60 or older; • Medicaid eligible (up to 300% of the Supplemental Security Income level – Medicaid
Institutional Care program income standard); • Have a diagnosis of Alzheimer’s disease made or confirmed by a Memory Disorder Clinic,
neurologist or medical doctor with experience in neurology; • Have an assessment completed by the Department of Elder Affairs Long Term Care
Comprehensive Assessment Review and Evaluation Services (CARES) staff and meet nursing home level of care criteria; and
• Live with a capable caregiver in a private home or apartment. • Live in a service area covered by the waiver
A key provision of program eligibility is the presence of a caregiver. A review of the services to be provided makes it clear that the program was designed to assist caregivers in the task of maintaining their family member or friend at home, rather than in assisted living or a nursing facility. The timetables to implement all the activities and services described above were delayed due to a variety of circumstances. As of May, 2005 contracts had been signed by two of the three proposed vendors, one responsible for services in Pinellas County and the other responsible for services in Miami/Dade and Broward counties. The award process for the third service area, Palm Beach County, had been contested, and the bidding process was re-initiated; start-up for this third site is planned for FY 2005–2006. A brief description of the two approved vendors follows.
4

Pinellas County: Gulf Coast Jewish Family Services, Inc. (GCJFS). As stated in its contract proposal, the GCJFS “mission is to provide adults, children, families and elders with quality, cost-effective, community-based services to enhance their independence, economic self-sufficiency, and emotional and physical well-being” (Gulf Coast Jewish Family Services, 2004, p. 24). The agency is a 501 C (3) nonprofit corporation, has employees in 12 counties, and offices in Pinellas, Pasco, Hillsborough, Sarasota, and Broward counties. Based in Clearwater, Florida, it currently is a direct provider or services manager for several Medicaid waivers, including:
• Aged and Disabled Adults Waiver: case management for elders in Pinellas County (the Community Care for the Elderly Program)
• Aged and Disabled Adults Waiver: case management and in-home care for disabled adults in Pinellas, Pasco and Hillsborough Counties (the Community Care for Disabled Adults Program)
• Project AIDS Care Waiver: case management in Pinellas, Pasco, Hillsborough and Hernando Counties
• Assisted Living Waiver: case management for elders in Pinellas County Home and • Community-Based Services Waiver for Developmentally Disabled: support coordination in
Pinellas, Pasco, Hillsborough, Polk, Highlands and Hardee Counties. Established in the early 1980’s, GCJFS currently employs over 250 case managers and offers a broad continuum of services. It provides services to over 800 frail elders, including participants in the multi-service Florida Alzheimer’s Disease Initiative.
Miami/Dade and Broward Counties: Miami Jewish Home and Hospital for the Aged, Inc (MJHHA). MJHHA was established nearly 60 years ago. As stated in its contract proposal, its mission is “To be the premier multi-component, not-for-profit, charitable health care system in South Florida, guided by traditional Jewish values, dedicated to effectively and efficiently serving a non-sectarian population of elderly, mentally ill, disabled, and chronically ill people with a broad range of the highest quality, institutionally-based, community-based and ambulatory care services” (Miami Jewish Home and Hospital for the Aged, 2004, p. 10). MJHHA offers a diverse array of community and facility-based services, and multiple programs. A service leader in Florida, it was the first agency in the state to implement a PACE (Program of All-Inclusive Care for the Elderly) program. The MJHHA also offers several Alzheimer’s respite programs, adult day care, short term emergency case management services, operates an assisted living facility, and a number of other services directly related to those included in the Medicaid Alzheimer’s disease waiver program. It has also been the recipient of multiple federal, state, and foundation grants. From 1989 through 1994, when funding expired, it was one of only 8 national sites to participate in the Medicare Alzheimer’s Project (MAP), which in terms of services was very similar to the Alzheimer’s disease waiver program. It also has a broad and diverse network of service providers available for the waiver program.
Current Status of Vendor Operations As of May 2005, the two approved and uncontested vendors were awaiting the assignment of provider numbers, and anticipating a reasonably smooth startup. As a result of the timetable delays, the present report does not include assessments of the comparative efficacy of the Alzheimer’s disease Medicaid waiver program. Instead, it examines basic questions related to the service utilization of Medicaid-eligible individuals with Alzheimer’s disease, during the time prior to the implementation of the Alzheimer’s waiver.
5

To examine the service utilization of Medicaid-eligible individuals with Alzheimer’s disease during the time prior to the implementation of the Alzheimer’s waiver, two groups of individuals with AD were compared. One group consisted of individuals who were enrolled for six months or more in the Aged and Disabled Medicaid waiver (ADW) program. This group was designated as the comparison group in the AHCA contract with CMS. In that contract it was stipulated that in determining the comparison group to be used in the evaluation, the appropriate “comparable population is Medicaid recipients enrolled in the Aged/Disabled Adult 1915 (c) waiver that utilized the services in the ADA waiver that are being offered in this waiver (Florida Medicaid Program, 2004).” The other group identified in this report consisted of individuals with Alzheimer’s disease who were not enrolled in the ADW. The non-ADW group members could have been participants in other programs, but none had participated in ADW during the year of study or for the two prior years. To put these comparison groups in context, members of the ADW Group were all drawn from a comprehensive diversion program for individuals with disabilities. The diversion program was designed to allow “physically disabled persons aged 18+ who meet nursing facility level of care to remain living at home and in the community. Services include: adult day health care, attendant care, case management, homemaker, personal care services, and home-delivered meals” (Center for Personal Assistance Services, 2005). As such, ADW participants with Alzheimer’s disease could be expected to have received a reasonably comprehensive set of services during the fiscal year studied (FY 2001–2002).
Eligibility of Waiver Program Participants Exclusionary criteria included residence in a nursing home or intermediate care facility for persons with mental retardation, eligibility as medically needy, or participation in another 1915 (c) home and community-based waiver. Inclusionary criteria, in addition to an age of 60 and over, a diagnosis of Alzheimer’s disease, and the presence of a live-in caregiver, included two additional criteria for eligibility, as signified by the “X” in the following extract from the grant proposal submitted to the Centers for Medicaid and Medicare Services (Florida Medicaid Program, 2004, p. 4): “3. X __ SSI - Supplemental Security Income and SSI-related. “4. X __ Other - Please describe:
“Medicaid eligibility for this waiver program is specified in a 1915(c) waiver application that was submitted for approval concurrently with this waiver. Eligibility criteria specified in the 1915 (c) application include:
“Optional categorically needy (aged 60 and over) who have income at or below 88% of FPL, which is lower than 100% of FPL. “Individuals who would be eligible for Medicaid if they were in a medical institution and who need home and community-based services in order to remain in the community; a special income level equal to 300% of the SSI Federal benefit (FBR).”
The Evaluation Process as Described in the Request to CMS The present report was mandated by the AHCA contract with CMS. In that contract it was stipulated that in determining the comparison group to be used in the evaluation, the appropriate “comparable population was Medicaid recipients enrolled in the Aged/Disabled Adult 1915 (c) waiver that utilized the services in the ADA waiver that are being offered in this waiver (Florida Medicaid Program,
6
2004).” As will be seen in the methodological description in Part Two of this report, the actual number of Medicaid recipients with Alzheimer’s disease who were enrolled in the Aged and Disabled waiver during the fiscal year to be evaluated is relatively small. For this reason, and also to allow an examination of the outcomes and costs associated with Alzheimer’s disease among a broader group of Medicaid recipients, the same rules of inclusion and exclusion that applied to the new Alzheimer’s disease waiver and to the comparable population of enrollees in the Aged and Disabled waiver, were also applied to the selection of a non-waiver comparison group of Medicaid recipients with Alzheimer’s disease.
Statement of the Question The underlying question driving the investigations and analyses contained in this report is whether or not the 1915 (b)(c) Alzheimer’s Home and Community-Based Services (HCBS) waiver program is successful in providing quality services to the target population in a cost effective and budget-neutral manner, and in meeting its stated goal of allowing beneficiaries to remain at home longer than they would without the waiver program services. Due to delays in initiating the program that eliminated the possibility of comparing the Alzheimer’s disease waiver program beneficiaries to those who were not in the program, the present report deals with four basic questions that can be addressed in the absence of Alzheimer’s waiver beneficiaries. Results will provide administrators with information needed to help determine the situation generally faced by Medicaid beneficiaries in the absence of the waiver program. The four questions that guide the overall effort are as follows:
1. What are the characteristics of Medicaid beneficiaries with Alzheimer’s disease (AD) who participate in the Aged and Disabled Medicaid waiver program, as compared with AD beneficiaries of similar age who are not so enrolled?
2. What are the types and costs of services provided and are they comparable in the two groups?
3. What variations exist by racial/ethnic minority group in overall days spent in the community?
4. What role do medications play in the progression towards institutionalization?
Supporting Literature There is both good news and bad news about Florida’s Medicaid budget. The bad news is that costs have risen an average of 12.5% over the past five years. Indeed, Medicaid spending has gone from approximately $5 billion in 1994 to over $13 billion in 2003. The good news is that these increases have been largely driven by increasing numbers of people enrolled in Medicaid, and the rate of increase may actually slow in the next few years (Alker & Portelli, 2004). Contrary to what might be expected, only about 10.1% of Medicaid enrollees are aged 65 and over. However this relatively small percentage actually incurs a disproportionate share of expenses, approximately 21.2% of Florida’s Medicaid expenditures. Moreover, the elderly are the most likely to develop Alzheimer’s disease, the third most costly disease in the United States (Bartels & Colenda, 1998). Five observations emphasize the importance of the Alzheimer’s Medicaid waiver program, whose explicit goal is to effect a delay in the institutionalization of individuals with Alzheimer’s disease into long term care. First, there are approximately 420,000 elders diagnosed with Alzheimer’s disease (AD) currently living in Florida, a substantial increase from the 370,000 estimated as recently as 2001 (e.g., Office of Program Policy Analysis and Government Accountability, 2001). A significant majority,
7

approximately 70-75%, live at home, but cognitive decline is a leading predictor of institutionalization (e.g., Mehta, Yaffe, & Covinsky, 2002). Second, AD patients often live from 10 to 15 years after being diagnosed with Alzheimer’s disease or another dementia (Kawas, 1999). Most spend a significant portion of this time being cared for by informal caregivers, with up to 80% of caregiving provided by family or friends rather than by health professionals (Dwyer, Barton & Vogel, 1994). The burden of providing care can be significant, and increases as the dementia progresses. This burden often arises from diverse sources, and can be most adequately addressed by flexible arrangements for services (Borrayo, Salmon, Polivka, & Dunlop, 2002). Of particular importance, when the caregiver resides with the patient, the attitudes and perspectives of the caregiver play a critical role in services utilized (Borrayo, Salmon, Polivka, & Dunlop, 2002; Chiriboga, in press; Chiriboga, Yee & Weiler, 1992). Hence, increasing the number of months and years spent outside of an institutional setting, by improving services provided to Medicaid beneficiaries and their family caregivers, has the potential of significant cost savings. Third, the estimated prevalence of dementia in the long-term care population ranges from 50% to 70% (e.g., Kane, Ouslander & Abrass, 2004). In one study of Medicaid costs in California, 10% of all expenditures for elder beneficiaries were associated with AD and related dementias (Menzin, Lang, Friedman, Neumann & Cummings, 1999). Fourth, the overall costs to society are great. It has been estimated that total direct and indirect costs associated with AD may go as high as $88.3 billion for the country as a whole (Bloom, de Pouvourville & Straus, 2003). Estimated costs per individual case range from $1,500 to $91,000, depending on the stage of the disease, co-morbidities, and availability of informal caregivers. Fifth, nursing home costs account for approximately 17% of the Florida Medicaid Budget (Crayton, 2004), with expenditures of well over $2 billion annually. Based on 1999 figures, it has been estimated that upwards of $50,000 in Medicare and Medicaid services are used for each individual with AD (Bartels, Clark, Peacock, Dums, & Pratt, 2003). The same investigators further estimated that there could be an annual savings of approximately $38,000 for each individual with Alzheimer’s disease who remains in the community. Many issues of concern will be addressed in this report, based on evaluations by a multidisciplinary team. Central to the report are the demographics of Alzheimer’s disease, the services that are utilized, and the costs associated with these services. As the waiver program itself becomes operational, future considerations will focus on whether the packaging of services that underlie the waiver project (1) increase length of stay in the community and (2) are cost-neutral. Another concern will be to identify which beneficiary and caregiver constellations are likely to benefit most from which particular package of services. The current report, however, focuses on the characteristics of two groups of individuals with AD, those who participate in the waver program, and those who do not. AD is progressively disabling, and what is effective at one stage may be ineffective at another, later stage. The knowledge base for the management of AD is expanding rapidly, but general dissemination of this information to both professionals and the lay public lags behind. Even more problematic is the fact that the majority of health care providers know little-to-nothing about how to successfully assist ethnic minority families that have a family member with the signs and symptoms of AD. This lack of information is a health disparities issue that is made more compelling by evidence that there is a higher age-specific prevalence of the dementias in Hispanic and African American elders (e.g., Gurland et al, 1999). In addition, there is evidence that Hispanic and African Americans are significantly less knowledgeable about AD than non-Hispanic Whites, and are generally less likely to access supporting services (e.g., Ayalan & Arean, 2004). We also know that at least some Hispanic caregivers may be at greatest risk of caregiver burden and distress, and that
8

certain groups of Asian caregivers may be at a lesser risk (e.g., Aranda & Knight, 1997). As ever-enlarging cohorts of ethnic populations grow older and become at risk for AD, identifying effective treatments for ethnic minority families is urgent, especially since Florida is among the most ethnically diverse states and is likely to become even more so in the near future.
Prevalence of Alzheimer’s Disease by Age It has been estimated that from 60 to 75% of all dementias occurring in later life are of the Alzheimer’s type (Kane, et al., 2004). Due to its prevalence, and to the Medicare and Medicaid costs associated with it, AD holds major significance for agencies concerned about controlling cost escalation. Estimates of the national prevalence of AD extend to upwards of 4.5 million, with a middle-series projection of a national three-fold increase by 2050 (Brookmeyer, Gray, Kawas, 1998; Khachaturian, 1997; Hebert, Scherr, Bienias, Bennett & Evans, 2003; Henderson & Jorm, 2002). Florida is one of seven states with an estimated AD population greater than 200,000; for 2000 it has been estimated as having 360,000 persons with AD—approximately 2.3% of its population (Hebert, Scherr, Bienias, Bennett & Evans, 2004). Future projections are influenced by population dynamics. Florida has the largest proportion of elders of any state in the United States, and Florida’s expected changes in the AD population are disproportionately large when compared to most other states. For example, Hebert et al. (2004) estimate that the numbers of individuals with AD in Florida will rise to 450,000 by 2010, 510,000 in 2020, and 590,000 by 2025. Other estimations are even higher. The relatively conservative Hebert et al. (2004) estimation represents a projected 64% increase in prevalence from 2000 to 2025. During the same time period, the state is projected to go from a 2.3% AD population to 2.8%, an increase all the more important because of the rapid population growth expected for the state. These projections have direct implications for growth in the costs in Medicaid, since AD has long been recognized as a major risk factor for institutionalization (e.g., Mehta, et al., 2002; Wygaard & Albreksten, 1992).
Nature of the Disease Alzheimer’s disease is an age-related disease, and therefore the number of individuals with the disease will increase substantially as the population ages. AD has the potential to increase Medicaid expenditures by increasing the risk of nursing home placement as well as raising prescription drug and other health care costs. While AD and other dementias affect about 7 to 10% of adults over the age of 65 (Brayne, 1994; Hendrie, 1998) the estimated prevalence of AD in the long-term care population is 50-70% (Kane, et al., 2004). AD is considered to be one of the most debilitating of diseases, impairing the ability of affected individuals to live independently and reducing quality of life. As AD advances, individuals become progressively impaired in cognitive, functional and behavioral capacities and the behavioral and psychological symptoms increase the risk of nursing home placement (Cummings, Frank & Cherry, 2002; Friedman, Steinwachs, Rathouz, Burton, & Mukamel, 2005; Heyman, Peterson, Fillenbaum, & Pieper, 1997). Not much is known about the problems faced by persons with AD who are living in the community. Not only is a diagnosis difficult to make, but it has been common for persons with any form of dementia to be excluded from research on community dwelling populations. AD is the most common type of dementia, accounting for about one-half to two-thirds of all dementia cases (Hendrie, 1998). AD has an insidious onset that may begin as long as 20 years prior to a clinical diagnosis (Elias, Beiser, Wolf, Au, White, & D’Agostinio, 2000). Early symptoms of AD usually involve mild cognitive deficits such as forgetfulness, but usually also include loss of initiative, anxiety, depression, and functional and behavioral deficits. Brains of Alzheimer’s patients have been found to contain β-amyloid-based plaques and neurofibrillary tangles (Snowdon, et al., 1996) that appear to accelerate loss of functional brain tissue. Eventually, neuropathology manifests itself in a loss of
9

personal identity, difficulties performing even relatively routine tasks, and inability to live independently.
Dementia Research Recent published reviews detail the diagnostic and therapeutic issues related to AD (Gold, Giannakopoulos, & Bouras, 2001; Reisberg, Franssen, & Shah, 2000; Samuels & Davis, 2001). There are usually three characteristic stages of decline in this disease, mild, moderate, and severe, with measurable cognitive and functional decline extending over 5-8 years. The initial “pre-clinical” or mild stage of cognitive impairment usually lasts a number of years, during which time the person shows short term memory impairment accompanied with anxiety and depression. The “pre-clinical phase” of AD refers to the period of mild cognitive decline that precedes the onset of diagnosable disease (Jeliz & Winblad, 2003). As research on prognostic methods and therapeutic interventions to slow AD advances, early detection of “pre-clinical AD” will become increasingly important. During the stage of moderate cognitive impairment, the person may develop delusions, visual hallucinations and sleep disturbances. In the severe stage of AD, motor impairment and more prominent cognitive decline occur (Gauthier, et al., 2002). As the disease progresses, nursing home placement becomes common, and the loss of functional autonomy has a major affect on quality of life for both persons with AD and their caregivers (Gelinas & Auer, 2001).
Treatment of AD and Related Dementias Recent advances in pharmacotherapy offer some hope for AD, and have led to the development of cognate drugs, designed to enhance cognition and slow functional decline and deterioration. Currently, three cognate drugs are commonly used and funded under Medicaid to treat AD, including Aricept (donepezil), Reminyl (galantamine), Exelon (rivastigmine tartrate). Because these cognate drugs increase pharmacy costs, it is important to evaluate the value of administering the drugs in preventing other medical expenses such as institutionalization. Currently, the main approach to treating dementia is to enhance the functioning of cholinergic neurotransmitters by use of acetylcholinesterase inhibitors. These comprise the only class of cognate drugs approved for the treatment of dementia by the Food and Drug Administration (FDA) (Whitehouse, 2000). Cholinesterase inhibitors inhibit the breakdown of acetylcholine—an important neurotransmitter in sending messages between neurons—and thus improve the overall function of the brain. Evidence-based guidelines recommend cognate therapy as standard treatment for AD (Whitehouse, 2004). Four cognate drugs have been approved by the FDA and are funded under Medicaid. Of these, only donepezil, rivastigmine, and galantamine are in common use and well-researched (Johnsson, Lindgren & Wimo, 1999; Ritchie, Ames, Clayton, & Lai, 2004; Rosler, Anand, & Cicin-Sain, 1999; Raskind, Peskind, Wessel, & Yuan, 2000; Samuels & Davis, 2001). Although the reported effects of currently approved cognate drugs are questionable, with limited, temporary improvement or stabilization of cognitive and functional performance reported in only about half of patients (Gauthier, et al., 2004; Gelmacher, Provenzano, McRae, Mastey, & Ieni 2003; Whitehouse, 2004; Wilcock, Lilienfeld, & Gaens, 2000; Wilcock, et al., 2003), the results of some clinical trials suggest there may be important secondary effects, e.g., improved quality of life, delayed institutionalization, and decreased healthcare costs (Evans & Watson, 2000; Farlow & Schneider 1998; Farlow, Hake, Messina, Hartman, Veach, & Anand, 2001; Rosler, et al., 1999; Whitehouse, 2004; Wilcock et al., 2000, 2003). Researchers speculate that the delays in nursing home placements may be related to reductions in the rate of loss of activity of daily living skills, or to improved behavior, because these factors often influence the decision to institutionalize older adults with dementia. Unfortunately, most clinical trials have been short (of 6 months duration), and the
10

effectiveness of acetylcholinesterase inhibitors in improving cognition, functioning, or behavior is questionable, especially in older adults with more advanced disease. The findings from cognate drug clinical trials may be difficult to generalize to the entire elder population, because the participants in clinical trials are often not representative of the general population of older adults with dementia, and also likely different than Medicaid populations. Individuals participating in clinical trials tend to be better-educated, wealthier, and younger than the persons with dementia who did not enroll (Albert, et al., 1997; Schneider, Olin & Lyness, 1997). Participants also have fewer co-morbid conditions and illnesses, as well as less disruptive behavioral and psychological symptoms, than persons not involved in dementia studies (Schneider, et al., 1997). Finally, few minorities have been included in the existing clinical trials of cognate drugs. Therefore, the effect of cognate medications on community-dwelling Medicaid populations is uncertain, as is the potential for delays in the time to nursing home placement, or on healthcare costs.
AD and Mental Illness Management of mental illnesses in elderly individuals with dementia is quite challenging and expensive (Lantz, 2004; Alloul, Saurial, & Kennedy, 1998). Elderly adults with mental illness and AD utilize health services at a high rate (Bartels, Forester & Miles, 2000). There are associations between overall health status, the behavioral and psychological symptoms of dementia (BPSD), mental illness, cognitive functioning and outcomes for elders with dementia (e.g., Jorm, 2000; Van Hooren, et al., 2005). BPSD specifically refers to the spectrum of non-cognitive manifestations of dementia, that include verbal and physical aggression, agitation, psychotic symptoms including hallucinations and delusions, depression, sleep disturbance, and wandering (American Psychiatric Association [APA], 2003). Within the realm of mental illnesses, major depressive disorder (MDD) is particularly problematic for persons with AD, because it accelerates the neurodegenerative process and is independently associated with decline in cognitive functioning and information processing (Comijs, Jonker, Beekman, & Deeg, 2001). The behavioral and psychological symptoms of dementia and mental illnesses influence the outcome of AD significantly, because they impair role functioning, reduce quality of life for patients and caregivers, increase caregiver burden, and the likelihood of admission to an institution (Albert, et al., 1996; Bass, McClendon, Deimling, & Mukherjee, 1994; Cohen, et al., 1993).
AD and Sex A review of the literature describing sex differences in the incidence of neurological disease suggests that age-adjusted incidence of AD is higher in women, especially with advancing age (Hauser & Amatniek, 1998). Because AD is associated with aging, and women have a longer life expectancy than men, the prevalence of AD is higher in women. Women, indeed, account for more than two-thirds of the older adult population with this disease. Although Jorm and Jolley (1998) found no significant sex difference in a meta-analysis of 23 AD incidence studies; they reported a trend toward higher incidence among women in the oldest age groups.
AD and Race/Ethnicity Coding for minority status is problematic in the Medicaid data set through at least FY 2002–2003. The information is provided either by the client, a caregiver or significant other, or case manager. The problems arise as a result of the fact that what is referred to as the “Race” variable actually represents a linear or categorical combination of race and ethnicity, such that only one item can be endorsed. One result is that Hispanics may endorse either “White” or “Hispanic.” Systematic bias may result, since there is evidence that Cuban Americans are more likely than other Hispanic groups to endorse the “White” category. Similarly, individuals whose racial ancestry is Black but who were raised in a Hispanic culture such as that of the Dominican Republic may endorse “Hispanic” rather
11

than “Black.” The “Other” category provides another set of problems. This latter category includes people, such as those originally from the Middle East or India or Pakistan, who are not one of the designated categories. It also may include individuals who consider themselves to cross categorical lines (i.e., who self-perceive as multicultural), but may also include refusals and “don’t know” responses. With the above caveats in mind, when compared to estimated overall proportions of the population of Florida, Medicaid beneficiaries are disproportionately distributed across different racial/ethnic group. As shown in the following table, which was calculated across all age groups on the basis of a 10% random sampling of Florida Medicaid beneficiaries (500,000 beneficiaries out of 5,113,724 total; age as of July 1, 2001), African American and Hispanic American clients are over-represented, while Whites are under-represented. This distribution of course reflects in large part the economic disadvantages that are associated with minority status.
Table 2. Recipient Race/Ethnicity Codes for 10% of All Medicaid Clients
Race/Ethnicity Frequency Percent Cumulative Frequency
Cumulative Percent
1-White 180605 36.12 180606 36.12 2-African American 153346 30.67 333952 66.79
3-American Indian 239 0.05 334191 66.84
4-Asian American 2601 0.52 336792 67.36
5-Hispanic American 112181 22.44 448973 89.79
6-Others 51027 10.21 500000 100.00 For beneficiaries aged 60 and over the distributions are slightly different, due in part to differences in life expectancy and immigration factors. As shown in Table 3, the proportion of older Whites receiving Medicaid benefits has increased from 36% to over 46%, while the relative proportion of African Americans and Hispanic Americans has dropped substantially. The “Other” category represents a mixed and undecipherable bag. Clearly, there are more beneficiaries aged 60 and over who endorse the “other” category of self-identified race/ethnicity. In analyses not shown in tabular form, it was found that the percentage of persons aged 60 and over in the “Other” category rose from 21.94% at age 60 to a high of 28.53 at age 68; and from age 69 on there was a gradual decline to a low of 10.34% at age 99. The important thing to note in Table 3 is that while the proportion of Whites has increased, they still represent less than 50% of Medicaid beneficiaries. The increase in proportion of Whites is most likely due to selective immigration (including immigrants from northern states) as well as the greater life expectancy of Whites. The doubling of the proportion in the “other” category is of unknown origins; its significance will be discussed later in this report.
Table 3. Race Distribution For Medicaid Beneficiaries Over 60 Years of Age
Race Frequency Percent Cumulative Frequency Cumulative Percent
1-White 139,831 47.39 139,843 47.39
12

Table 3. Race Distribution For Medicaid Beneficiaries Over 60 Years of Age
Race Frequency Percent Cumulative Frequency Cumulative Percent
2-African American 49,546 16.79 189,389 64.18
3-American Indian 51 0.02 189,440 64.20
4-Asian American 627 0.21 190,067 64.41
5-Hispanic American 34,546 11.71 224,613 76.12
6-Others 70,456 23.88 295,069 100.00 * As of July 1, 2001
Given the generally disproportionate use of Medicaid services by different racial/ethnic groups, it is important from a cost-predictive perspective to consider ethnic minority issues associated with AD. There is some recent evidence of differential racial/ethnic vulnerabilities to Alzheimer’s disease, and a greater prevalence of AD has been reported for example among Hispanic or Latino elders by Clark, et al. (2005). In two separate studies of elder Latino and Anglo subjects diagnosed with AD, Latinos were found to be 5–7 years younger than non-Hispanic Whites when symptoms of the disease were first noticed by key informants. Among the possible reasons cited are higher rates among Hispanics of hypertension and diabetes, both of which are risk factors for AD. In general, research on the prevalence and problems associated with AD among minorities suggest that AD may be a greater problem for minorities. While these findings suggest that one effective strategy might be to design services focused on specific ethnic and racial groups, Iliffe and Manthorpe (2004) argue that the factors contributing to cross-group differences, including greater within-group than across-group variations in prevalence as well as caregiver needs, suggest against group specific interventions:
…the important issues for service providers to consider are language, religious belief and observance, cultural practices (including food and personal care practices) and social support and coping mechanisms. …[the argument of the paper is] that these issues are applicable to all individuals with dementia, independent of apparent ethnicity, and that promotion of cultural competence in service provision should not be relegated to an ethnic minority agenda. The task for health and social care providers is therefore to recognize the diversity of users and to increase access to appropriate quality mainstream person-centered services rather than to develop segregated or specialized services” (Iliffe & Manthorpe, 2004).
AD and Depressive Symptoms and Disorders Depressive symptoms are common in individuals with AD and are associated with negative outcomes and exacerbation of cognitive deficits (e.g., Bartolini, Coccia, Luzzi, Provinciali & Ceravolo, 2005; Milwain & Nagy, 2005). At any point in time, an estimated 20%-25% of AD patients meet the criteria for major depression, and an additional 27% have minor depression. Those who are depressed are likely to remain depressed or have recurrences of depression. Depressive symptoms are also independently associated with cognitive and functional impairment, agitation and other behavioral disturbances, e.g., wandering. Furthermore, the occurrence of depression in patients is associated with caregiver depression, caregiver burden, and nursing home placement. Remission of
13

depression is associated with improvements in global function and the reduction of behavioral disturbances. The high prevalence of depression in family members dealing with the stress and strain of caregiving is well documented, especially in Alzheimer families. Older spouses have the highest prevalence of depression, likely reflecting the responsibilities, values, and commitments of marital loyalties. Depression occurs in more than 60% of wives, 40% of husbands, 40% of daughters and daughter-in-laws, 25% of sons, and 25% of other relatives caring for relatives with dementia at home (Cohen, 2000). Despite frequent medical care visits, depression in family members goes unrecognized. Even when caregivers know they are having emotional problems, they are usually reluctant or unwilling to admit it and to reach out to family members or professionals for help. This is especially true for men, who also manifest depression differently than women. Caregivers who are depressed are not only less able to care for the dependent family member or their own health, they are also at an increased risk of harming their relative or themselves. The overall prevalence of severe violence, e.g., kicking, hitting, stabbing, in family members caring for relatives with dementia at home is 17% (Paveza et al., 1992). About 6% are cases where caregivers are violent towards patients, 15% are circumstances where patients are violent towards caregivers, and 4% are situations of mutually interactive violence. The presence of significant depression in the caregiver was associated with a three-fold increased risk of severe violence. However, caregiver depression, coupled with a living arrangement where the patient lived with family members other than their spouse, was associated with a nine-fold increased risk for severe violence. For these reasons, treatment of depressive symptoms and disorders are an important element of AD treatment. In addition to improving the individual’s quality of life, treatment may reduce functional impairment, caregiver burden, and institutionalization, thereby increasing the period of time spent at home and in the community. Unfortunately, little is known about the availability, accessibility, utilization, and efficacy of depression-targeted mental health services. The AD waiver program will assess service utilization variables related to psychosocial services, to determine whether these services can impact days in the community. Some variables already are planned for inclusion, such as use of antidepressant medications and contacts with the formal program staff. Caregivers and patients may access services outside the AD waiver program, however, that could impact a number of outcomes, including patient depression, caregiver burden, and days in the community. These services can take a variety of forms, including support groups, formal psychotherapy (individual, family, or group), activity groups, or educational interventions (e.g., psychoeducation, training the caregiver to manage patient’s depression or agitation). Because services delivered to caregivers can impact patient depression, it is important to assess caregiver services as well as services delivered directly to the patient. Finally, depression is associated with other psychiatric symptoms, so it will be important to ask about other potential causes for initiating mental health treatment. At present there are a number of depression-related questions about service provision to Medicare clients with AD, and their caregivers, that remain unanswered. Such questions include the efficacy of differing types and implementations of services, the impact of medications, and the impact of depressive symptoms—both for client and caregivers—on trajectories towards institutionalization. These questions would provide useful information about service use, its relation to patient depression and other psychiatric symptoms, and the impact of service use. This information could be used to guide future intervention efforts to improve quality of life for both AD patient and caregiver, as well as potentially delay institutionalization.
14

AD and Wandering Wandering behavior received comparatively little attention until about 20 years ago, and even today there is no clear definition for it (Lai & Arthur, 2003). Despite ambiguities as to what characteristics are included, it is generally recognized that wandering behavior of the Alzheimer’s client is a source of great distress to family caregivers, and can lead to disruption of the community as well (Zarit & Zarit, 1998; Mace & Rabins, 2000). Not only is it distressing, but it also occurs with some frequency among community-resident individuals with AD. Generally it is found among those with moderate to moderately severe AD and other dementias. Estimates of the prevalence of wandering behavior range from 17% to 65% for this population (e.g., Holtzer, et al., 2003; Klein, et al., 1999; McShane, et al., 1998). Of consequence to caregiving efforts is that, once present, wandering behavior tends to continue up to the point where the individual becomes unable to walk. Hence, wandering is not only a stressor but a persistent stressor. Wandering is a significant issue for the elderly across the care continuum because of the associated adverse outcomes including falls, accidents, fractures and other injuries, weight loss, fatigue, sleep disturbances, berating and abuse, getting lost, elopement, victimization, decreased functional skills, premature institutionalization, and untimely death, as well as to an increased caregiver burden (Algase, 1992, 1998, 2005; Beattie, 2005;Cancro, 1968; Fompa-Loy, 1988; Rheaume, Riley, & Volicer, 1987; Soverini, 1968; Stokes, 1986). Wanderers are at increased risk of falling (Keily, Kiel, Burrows, & Lipsitz, 1998; Marx, Cohen-Mansfield, & Werner, 1990) and have an extremely high risk for hip fractures (Snyder, et al., 1978). Wandering also contributes to earlier mortality, especially among fallers (Holtzer, et al., 2003; Kopetz, et al., 2000; McShane, et al. 1998). Studies have found that wanderers were more likely than other persons with dementia to be institutionalized (Algase, 1992; Fompa-Loy, 1988; Cumming, Jonker, Beekman, & Deeg, 1982; Kopetz, et al., 2000; Lam, Sewell, Bell, & Katona, 1989; Moak, 1990; Rockwood, Stolee, & Brahim, 1991; Rowe & Glover, 2001; Sanford, 1975; Stokes, 1986; Vieweg, et al., 1995). Elopement, a situation where the individual becomes missing at least temporarily, is probably the most hazardous outcome of wandering. In a longitudinal study, nearly half of 104 community-residing persons with dementia eloped at least once and for them the risk of institutionalization was very high (Algase, 1992). Most wanderers who eloped did so once or twice in within eight months and for those with repeated episodes (up to 52 occurrences per participant), the behavior endured for up to 28 months. Among participants who never eloped, 43% were at identifiable risk to do so. The same study found that many wanderers were restricted from walking freely within their homes by a caregiver and had a five-fold increased risk for institutionalization. For participants who got lost, the increased risk for institutionalization was greater than seven-fold, and 68% were institutionalized within the year following the first incident of getting lost. Good topographical memory had a negative predictive value (of 90%), but poor topographical memory had only a modest positive predictive value (44%). While wandering can lead to getting lost, the proportion of all getting lost episodes of persons with dementia attributable to wandering is not known, largely because studies of these phenomena often blur distinctions between wandering and getting lost. It is estimated that 60% of people with AD will wander and become lost (Alzheimer's Association, 2004). Unless discovered within 24 hours of disappearance, their outlook for survival is often poor. Of those wanderers who were found, 14% of the cases had been living alone; 80% lived in the community with a caregiver, while the small remainder lived in long-term care settings (Rowe, 2001). In a subsequent study (Teri, Larson, & Reifler, 1988) wanderers whose bodies were recovered had died of exposure (68%), drowning (23%), or accidents. Wandering represents a significant expense (Small, McDonnell, Brooks, & Papadopoulis, 2002). In an Israeli study, 30% of the annual cost of care for non-institutionalized persons with AD (equivalent
15

to $4,115 U.S.) was invested in the direct management of symptoms of dementia (Beeri, Werner, Davidson, & Noy, 2002). Because wandering is a leading cause of nursing home placement for persons with dementia (Balesteri, Grossberg, & Grossberg, 2000) it also contributes substantially to both private and Medicaid expenditures for long-term care. In 1999, combined Medicare and Medicaid costs for dementia care ranged between $30,000 and $50,000 per capita, depending upon the age of the person with dementia (Bartels, et al., 2003). For each year that one wanderer can be sustained in the community, a current average annual savings of $57,700 in nursing home expenditures was reported. Once institutionalized, wanderers are not necessarily protected from adverse outcomes. Wandering off the unit or out of the facility was the fourth-most common adverse event in one study of long-term care settings, occurring in 3 out of 100 beds per year (Gurwitz, Sanchez-Cross, Eckler, & Matulis, 1994) accounting for 10% of all lawsuits against long-term care settings, at an average expense of $100,000 per case (Foxwell, 1994). Notably, in 70% of these cases, elopements from long term care settings resulted in death (Rodriguez, 1993). For all the reasons cited above, including not only the risk of institutionalization and mortality but also the stresses associated with wandering behavior, reduction in wandering has been targeted as a way of lengthening time in the community and decreasing the costs borne by the government and/or caregivers for more expensive institutional care alternatives. At the same time, the lack of information about why and when wandering occurs poses challenges to those concerned with the development of effective interventions (Lai & Arthur, 2003).
AD and Lethal Violence The stress of caregiving can lead to abuse and sometimes violence. Lethal violence involving patients with Alzheimer’s disease and other dementias is rare, but it is an emerging public health challenge, with a long-lasting impact on family members and the communities where they occur (Cohen, 2004; in press). A small subset of dementia patients is capable of committing homicide or homicide-suicide, but a larger number are at risk of being killed by family caregivers. Cohen (2004) estimated that the prevalence for dementia-perpetrated homicide is 0.22 per 100,000 persons with dementia, and that the rate for caregiver perpetrated homicides and homicide-suicides is five times higher. Although the precise national as well as statewide prevalence is not known, these events will likely increase as the population ages and the number of persons with dementia increase. Most AD homicide perpetrators are men who kill a spouse or intimate with a firearm in the home, and 20% are homicide-suicides. The best predictor for violence is a history of previous violence, and if there is no history, clarification of the closest the person ever came to being aggressive or violent. Active paranoia and psychotic symptoms, psychotic depression, military/law enforcement/firefighter history, presence of vascular dementia, and history of catastrophic reactions are also risk factors. However, the prediction of the risk for dangerousness, as with that for suicide, is difficult. Almost all of these cases of violence associated with AD are not willful, intentional acts to injure and kill. They are usually the tragic outcomes of a combination of circumstances: the individual’s sensory, cognitive, emotional and medical status; the individual’s fearfulness and ability to communicate; a lack of awareness and preparedness of those who interact with the patient; biopsychosocial and environmental stressors; and the availability of firearms, knives, heavy objects, and other lethal means. The negative consequences of caring for relatives with dementia have been well documented, e.g., depression and other psychiatric problems, disrupted work and family life, physical exhaustion (Cohen, 2000). Newspaper surveillance studies suggest a possible increase in the occurrence of family violence involving caregivers who kill the patient and sometimes kill themselves or attempt to kill themselves (Malphurs & Cohen, 2002).
16

Caregivers who kill frequently make the headlines, but the memories of these circumstances recede, except in those families and communities affected (Cohen, 2004). For whatever reason, these tragedies have not attracted sustained public debate. Some professional organizations, such as the American Psychological Association, have raised policy concerns about the vulnerability of individuals with dementia to family violence, and several states (e.g., Arizona, Missouri, and Florida) have expanded the focus of domestic violence mortality review committees to examine homicide-suicides and elder deaths. Maryland may be the only state where the Office of the Attorney General specifically identified the importance of detecting violence and violent deaths, in a 2004 policy report on Alzheimer’s disease and other dementias. Cohen (2004; in press) has begun to develop a profile of caregiver homicide offenders. Most have been a caregiver for a long time, and the homicide or homicide-suicide usually occurs at home. Older married male caregivers kill their wives in about half the reported cases. Adult child caregivers, usually a son, commit the remaining 50%. Older men usually kill with firearms, followed by asphyxiation, poisoning, and stabbing. In contrast, adult children most frequently kill by asphyxiation, followed by firearms, beating, and neglect. About two-thirds of the adult children who killed had a history of mental illness. Naturally, most caregivers were devoted to the patient, with no evidence of abuse, neglect, violence, financial exploitation, or malice, and they were depressed and exhausted from their caregiving roles and responsibilities. One of the ongoing issues in studies of caregiver violence is that community studies are urgently needed. Violent deaths, where caregivers kill older family members with dementia or patients kill family caregivers, are likely to become a more frequent occurrence with the rapid aging of our society and the increasing numbers of persons with Alzheimer’s disease and related disorders. Data from patients and caregivers living at home are urgently needed to identify the epidemiology and clinical patterns, risk factors, characteristics of perpetrators and victims, and events leading up to the homicides/homicide-suicides in order to develop and implement effective intervention and prevention strategies.
Caregiving and Family Training The Administration on Aging (2005) estimates that approximately 3.7 million older Medicaid beneficiaries receive help from either a family caregiver or from service agencies. Of these, approximately two-thirds receive help only from family and friends. This help comes at some cost–what is commonly referred to as caregiver burden. Numerous studies attest to the stresses and burdens of providing caregiving to family and friends (e.g., Center on an Aging Society, 2005). The physical, social and financial burden of caregiving is generally recognized to be greatest for those who care for persons with Alzheimer’s disease. The reasons for the greater burden are multiple. AD affects individuals in many ways, including changes not only in cognition but also in personality and emotionality (e.g., Balsis, Carpenter, & Storandt, 2005). There are numerous studies documenting the emotional, physical, social, vocational and financial toll for family caregivers of those with dementia (Cohen, 2000; Cohen, & Eisdorfer, 2001; Ory, Hoffman, Yee, Tennestedt & Schulz, 1999; Schulz, Vistainer, & Williamson, 1990). This burden on caregivers has been shown to be predictive of institutionalization for individuals with dementia (Yaffe, et al., 2002). Pearlin, Mullan, Sample, and Skaff (1990) introduced the concepts of primary stressors (hardships directly due to caregiving) and secondary stressors (intra-psychic strains and those hassles outside of caregiving proper). This conceptualization has proven to be of heuristic value for caregiving research. Indeed, much of the caregiving research has focused either on educational interventions to reduce caregiver hardships dealing with disruptive behavior (primary stressors), and on support groups to address the psycho-social aspects of care via peer support (secondary stressors). Research outcomes have either been directed to improvements in patients and/or caregivers (Teri, 1999).
17

Robinson and Yates (1994) found that both behavior management and social skills programs helped decrease the objective burden and improved caregiver’s attitudes towards asking for help and using day care. Hepburn, Tornatore, Center, and Ostwald (2001) evaluated a community-based 14-hour training program rooted in stress and coping theory, and found that providing information, linkage, and role coaching was beneficial for family caregivers. Caregiver training programs have also been devised to address communication difficulties in AD patients. Ripich (1994) developed a program designed around specific strategies to alter communication patterns. Caregivers undergoing this program were found to have improved attitudes toward AD patients, better knowledge of AD, and greater knowledge of communication strategies to be used with AD patients. An international study found caregiver training programs decreased behavioral problems and improved caregiver self-efficacy in Taiwanese families (Huang, Shyu, Chen, Chen, & Lin, 2003). Gerdner, Hall, and Buckwalter (1996) recommend that nurses implementing caregiving training protocols be aware of the research foundation supporting the intervention strategy, and address diagnostic considerations, desired patient outcomes, patient acceptance and feasibility of the intervention, and skill set of the nurse implementing the intervention. Some studies have utilized randomized control trial methodology. Ostwald, Hepburn, Caron, Burns, and Mantel (1999) designed a 3-year randomized clinical trial that tested the effectiveness of an interdisciplinary psychoeducational family group intervention. They found that the intervention reduced caregivers’ negative reactions to difficult behaviors and reduced caregiver burden over time. Teri et al. (2003) conducted a randomized controlled trial of a behavioral management program for patients with Alzheimer’s disease (AD). They found that exercise training for patients with AD, together with teaching caregivers behavioral management strategies, was effective in improving the physical health and depression of patients with AD. Brodaty, Gresham, and Luscombe (1997) evaluated a structured, residential, 10-day training program that was enhanced by follow-ups and telephone conferences. An eight-year survival analysis indicated that patients whose caregivers received this training stayed at home and lived longer. A randomized control trial of 406 spouse-caregivers of patients with AD found that a multi-component caregiver intervention which included counseling and support changed caregiver appraisals of problem behaviors, although it did not reduce the frequency of behavior problems (Mittelman, Roth, Haley & Zarit, 2004). Brodaty, Green, and Koschera (2003) conducted a meta-analysis of 45 studies of psychosocial interventions for dementia caregivers. They concluded that caregiver interventions have significant but modest benefits on caregiver knowledge, psychological morbidity, coping skills, and social support. Caregivers are frequently satisfied with the interventions, appraise their coping skills as improved, and say they would use the training again. Successful elements of training programs are involvement of the extended family, structured individualized counseling, and flexible long term support. Unsuccessful interventions are support groups alone, single interviews, or brief modules with no long-term follow-up. Teri (1999) summarized the research on training families to provide care to those with dementia, and made recommendations to improve the quality of research. She notes that the literature has consistently shown that caregivers are able to learn specific techniques to reduce problematic behaviors. Controlled trails suggest that caregiver training programs are effective in reducing disruptive behavior or delaying institutionalization in patients with dementia, when part of an overall program of care. But she outlines a number of research issues that must be addressed for the field to continue to develop. The terms ‘training’ and ‘family’ need to be better defined. The use of valid, sensitive measures of assessment of treatment efficacy must be embedded within studies that utilize reasonable sample sizes, well-described subjects, and well-articulated training procedures. One fine start in this direction has been the REACH multi-site study, a consortium of universities that partnered with the Alzheimer Association to test the effectiveness of caregiver interventions, which
18

has yielded promising results (Belle, Zhang, Czaja, Burns, & Schulz, 2004; Burns, Nichols, Martindale-Adams, Graney, & Lummus, 2003). Teri (1999) concludes that we are now at the stage where we need to be posing much more detailed questions, where the focus is on identifying the specific strategies that work for specific situations and caregivers. In summary, it is clear that more well-controlled research on family caregiver interventions is necessary across a variety of fronts. In particular, health professionals and funding agencies would benefit from studies that analyze large data bases, generate cost/benefit analyses, and that include quantitative and qualitative information from family members as well as patients. The actual procedures of the targeted caregiver intervention need to be better-described, and the evaluation/outcome measures should be carefully chosen. In this respect the field is fortunate to have available several well-validated data collection tools. As presented and discussed in Part Four of this report, many of these tools are highly appropriate for use by the contracting providers, as a means of quantifying risk factors and predictors of institutionalization as well as assessing characteristics of caregivers that are likely to affect the outcomes of beneficiaries with AD.
AD and Psychotropic Medication The management of mental illness and /or BPSD in elders with AD is not standardized, and a variety of psychotropic medications are used (Hamid, Howard, & Silverman, 1995; Young, Klap, Shebourne, & Wells, 2001; Young, et al., 2004). Special care must be taken when prescribing psychotropic medications for elders (APA, 2003; Brauner, Muir & Sachs, 2000; Small, Rabins, & Barry, 1997). Compared to younger adults without AD, the risk-benefit ratio of psychotropic medications prescribed for elders with AD can be compromised (Flint, 1998). Older adults with AD have increased sensitivity to certain adverse effects of psychotropic medication, greater potential difficulty following medication regimens, and reduced ability to recognize and report adverse events (Brauner, Muir & Sachs, 2000). Further, age-related changes in pharmacokinetics and pharmacodynamics may result in greater propensity for drug toxicity in the elderly. Of particular concern for elders with serious mental illness (SMI) is the fact that age-related changes can result in increased sensitivity to the typical antipsychotic drugs, causing an increased incidence of movement disorders or extrapyramidal side effects such as tardive dyskinesia (TD) and postural hypotension (Catterson, Preskorn, & Martin, 1997; Jeste, et al., 1995). For many years typical antipsychotic drugs (e.g. haloperidol, prolixin) were the most common form of treatment for behavioral and psychological symptoms. While there is extensive experience and prescription of typical or “older” antipsychotic medications (particularly for older adults), these drugs are only modestly effective and have potentially serious adverse effects that limit their usefulness in elders, compared to the “newer” second-generation (and more expensive) atypical antipsychotic drugs (Schneider, et al., 1997). Health care professionals should also consider the increased risks involved when prescribing the “older” tricyclic antidepressant medications with significant anticholinergic activity for elders with AD (Kawas, 1999; Small, et al., 1997). Advances in antidepressant medication parallel the advances in antipsychotic medication. Newer, more expensive selective serotonin reuptake inhibitors (SSRIs) have been developed that result in fewer side effects and have greater efficacy than the “older” tricyclic antidepressants in the treatment of geriatric depression. Based on their opposing mechanisms of action, concomitant use of cholinesterase inhibitors (cognate drugs) and tricyclic antidepressants in elders with AD can result in pharmacological antagonism (Roe, Anderson, & Barry, 2002). Despite best practice guidelines supporting the need for and use of newer antipsychotic and antidepressant medications as the first line of treatment for elders, studies have shown that older and less expensive antipsychotic and antidepressant medications are regularly prescribed for elderly patients (APA, 2003; Gray, Lai & Larson, 2000). African American elders in particular are less likely to receive newer classes of antipsychotic and antidepressant drugs, and at least two studies suggest a worsening of these drug-treatment disparities from 1980s to the 1990s (Blazer, Hybels, Simonsick, &
19

Hanlon, 2001; Young, et al., 2001; Smothers, et al., 2005). Thus, we argue that treatment outcomes for elders with AD and BPSD needs special attention. Medicaid data and the current study offer a unique opportunity to examine psychotropic prescribing practices and associated outcomes for Florida’s elderly Medicaid recipients with AD.
Dementia and Nursing Home Placement Currently the Health Care Financing Administration is predicting that national long-term care expenditures may reach $87.2 billion by 2007 and will continue to increase well into the future (Health Care Financing Administration [HCFA], 1999). Among the greatest projected increases are nursing home, pharmacy and home health care expenditures (Taylor & Sloan, 2000). These predicted expenditures are of great concern to Medicaid, the largest purchaser of nursing home service for low-income elderly in the U.S. (Strahan, 1997). The situation in Florida is equally compelling. Given that nursing home expenditures account for approximately 17% of the $15 billion Florida Medicaid budget (Crayton, 2004), provision of cognate drugs has the potential to be cost-effective, if it increases the time cognate drug recipients spend outside of an institutional setting, decreases the rate of nursing home placement or reduces non-pharmacy healthcare costs. Studies of elders have shown that individuals with AD are at increased risk for nursing home placement (Gaugler, et al., 2000; Becker, Andel, & Rohrer, 2005; Meaney, Croke, & Kirby, 2005; Severson, Smith, & Tangalos, 1994). In addition to a diagnosis of AD, age, income, marital status, majority status and co-occurring mental illness have all been shown to be significant predictors of nursing home placement in the general population (Cohen, et al., 1993; Heyman, et al., 1997; Miller, Prohaska, & Furner, 1999; Stevens, Owen, Roth, Clay, Bartoucci, & Haley, 2004). Problem behaviors in AD patients and associated caregiver stress have also been shown to increase the risk of nursing home placement (Mittleman, Ferris, Shulman, Steinberg, & Levin, 1996). Thus, in addition to the provision of psychotropic drugs, we examine the impact of Baker Act (BA) examinations on nursing home placement in this study because we suspect individuals who require psychotropic medication and/or an involuntary psychiatric evaluation may be at an increased risk for nursing home placement.
Part Two. Research Methods and Results for Questions 1-3 The following are the three Research Questions that will be addressed in this section:
1. How do the characteristics of Medicaid beneficiaries with AD who participate in the Aged and Disabled Medicaid waiver program compare to those AD beneficiaries who are not so enrolled?
2. What are the types and costs of services provided, and are they comparable in the two
groups? 3. What variations exist among different racial/ethnic beneficiaries in the time spent in
community or in nursing homes?
In addition, there are two hypotheses and one corollary to be tested: There will be differences across the two groups in the risk of institutionalization, as
measured by days-in-community and rate of institutionalization. Race and ethnic group status will be associated with a reduced risk of institutionalization; and thus
20

There will be significant variations across racial and ethnic groups in the overall number of days spent in community.
General Procedures A number of data sets were used to answer the first set of research questions posed in this part of the report: Research Questions 1–3. These questions have been modified as a result of impediments to the overall progress of the Medicaid waiver program that is the principal focus of the evaluation. Three evaluation groups were originally proposed so that the effects of the waiver program could be truly assessed. In addition to the target group of beneficiaries who would participate in the new waiver, two comparison groups were to be constructed and evaluated. The current status of the implementation of the program, as well as the ensuing lack of data regarding participants in the Alzheimer’s disease waiver program, has permitted the development of only the two comparison groups (i.e., beneficiaries with AD who do or do not participate in the Aged and Disabled Medicaid waiver program), and therefore assessments of these two comparison groups form the focus of the present report. The target group will be established at a later date, as information becomes available. The procedures used to identify samples for the first two comparison groups described here.
Identification and Development of the Two Comparison Groups The original proposal by the state of Florida to the Centers for Medicare and Medicaid Services specifically identifies FY 2001–2002 as the base year from which to draw a comparison group of persons participating in the Florida Aged and Disabled Waiver (ADW) program. For the purposes of the present report, an additional comparison group was added, to assess people not participating in the ADW. Because the goal was to use the full twelve months of FY 2001–2002, the strategy for study eligibility required that data be drawn from the immediately-preceding fiscal year. Data sets that were obtained for that fiscal year, FY 2000–2001 (i.e., July 1, 2000 to June 30, 2001) included those maintained by the Florida Agency for Healthcare Administration on Medicaid eligibility and Medicaid fee for service claims Sources for data sets for FY 2001–2002 (July 1, 2001 to June 30, 2002) also included:
Florida Department of Children and Family Services, for data on substance abuse and mental health claims; (IDS/SAMH) for all Medicaid and general revenue funded services;
Florida Agency for Health Care Administration for data sets on Medicaid eligibility, Medicaid fee for service claims, Medicaid reimbursed pharmacy claims, and Medicaid long-term care;
Florida Mental Health Institute; and Baker Act Reporting Center, for short-term, involuntary or ‘Baker Act’ examination data.
Unique Medicaid identifiers were used to identify the sample of persons to be included in the two comparison groups. The general criterion for inclusion consisted of being age 60 or over, residence in the community, a diagnosis of Alzheimer’s disease, and participation in the Aged/Disabled Waiver program. The populations of elders identified at each stage of the comparison group identification process is described in Table 4.
21

Table 4. Data Sets Used to Create the Comparison Groups
Description of group Population
Number of subjects in Medicaid Eligibility file from FY 01–2002 who were not in AHCA-defined areas 1 or 6.
1,482,054 (unduplicated)
All data below EXCLUDE beneficiaries in AHCA Areas 1 and 6. These areas lack specific service use records
Number of subjects who were 60 and over as of July 1, 2001. 295,069 (unduplicated)
Number of subjects with a diagnosis of Alzheimer’s as indicated by a diagnosis code of ‘331.0’ in the Medicaid claims (n = 1,692) or institution files (n = 271) in FY 00–2001.
1,896 (unduplicated)
Number of subjects who were 60 and over as of July 1, 2001 AND diagnosed with Alzheimer’s as indicated by a diagnosis code of ‘331.0’ only in the Medicaid claims or institution files.
1,250 (unduplicated)
Number of subjects in a nursing home in July of 2001 50,572 (unduplicated)
Number of subjects in a nursing home: either in June of 2001 OR more than 3 months out of the last 6 months (Jan. 2001–June 2001).
53,204 (unduplicated)
Number of subjects who were in a nursing home in July of 2001 OR June of 2001 OR more than 3 months out of the last 6 months (January 2001–June 2001).
56,481 (unduplicated)
Number of subjects who: were 60 and older, had a diagnosis of Alzheimer’s and were not in a nursing home. Sample meets the study criteria for ADW and Mixed Groups.
467 (unduplicated)
Number of subjects in the Aged/Disabled Waiver program from 1999–2002. 23,327 (unduplicated)
ADW Group: Subjects who were 60 and older, had a diagnosis of Alzheimer’s disease, were not in a nursing home and participated in the Aged/Disabled waiver program.*
77 (unduplicated)
Mixed Group: Subjects who were 60 and older, had a diagnosis of Alzheimer’s diseases, were not in a nursing home and DID NOT participate in the Aged/Disabled waiver program for more than 5 months.
390 (unduplicated)
Number of subjects remaining in the Aged/Disabled waiver data file who did not meet study criteria.
23,250 (unduplicated)
* While a total of 71 such subjects participated in the Aged/Disabled Waiver program in FY 2001–2002, only 58 participated in the Aged/Disabled Waiver program for 6 months or more in FY 2001–2002. The latter are the subjects included in the ADW Group. The selection process began with data from the previous FY 2000–2001. That is, participants were initially selected from the Medicaid files from FY 2000–2001 if they had a diagnosis of Alzheimer’s disease, as indicated by an exact code of ‘331.0’ (only diagnosis codes of 331.0 are indicative of
22

Alzheimer’s Disease; codes that were similar to 331.0, such as 3310 or 331.00, were not included since it was unclear what disease state was actually being referenced). Data from files for FY 2001–2002 were then used to further select elders who met the rules for inclusion. As shown in Table 4, there were a total of 1,482,054 unduplicated Medicaid recipients for FY 2001–2002 who did not reside in Areas 1 or 6 (the latter two areas are served by HMOs that are not presently required to provide encounter information, and hence clients in these areas were omitted from the study). For inclusion, all subjects also had to be 60 years old or older as of July 1, 2001; application of this criterion resulted in there being 295,069 (19.91% of the total number) candidate beneficiaries. Based on the exclusion of all persons without Alzheimer’s disease, there were 1,896 (unduplicated) individuals who entered the July 1, 2001 evaluation period with a diagnosis of Alzheimer’s disease. The criterion that beneficiaries also not be in a nursing home in June or July of 2001 or for more than three months from January 2001 through June 2001 reduced the total to 467 individuals who met all the aforementioned criteria. These individuals were then sorted into one or the other of the two comparison groups, using the inclusionary and exclusionary rules provided in Table 4.
The Aged and Disabled Comparison Group. To select the ADW comparison group, the next step was to identify a subgroup of individuals who had participated in the Aged and Disabled Waiver (ADW) program during the evaluation year (in this case, FY 2001–2002). The ADW is a fee-for-service program for aged and disabled adults who are at risk of nursing home admission. To be eligible for the ADW, individuals must be aged 18-64 and disabled or blind, or age 65 and over. They must also be a U.S. citizen or qualified non-citizen, be a Florida resident, have a Social Security number (or apply for one), and meet nursing facility level of care criteria established by the Department of Elder Affairs. Identifiers for participants in the ADW program were obtained by month for three fiscal years (FYs 1999–2000, 2000–2001, & 2001–2002). There were 23,327 unduplicated records in the data set. Of the 467 subjects in the original data set who met study criteria, 77 participated in the ADW program at some point in the three fiscal years. Seventy-one elders were enrolled in the program in FY 2001–2002. After reviewing the number of months of eligibility for the program for the sample, the research team decided that in order to be included in the ADW group, subjects would have to have at least six months of enrollment in the ADW. This reduced the number of subjects from 71 to 58. A total of 58 people therefore comprised the sample for this group.
The Mixed Group. The second comparison group consisted of those subjects from the originally identified group of 467 eligible subjects who remained after the ADW subsample was removed. Here called the “Mixed” group, they are in fact a miscellaneous group whose only common characteristic is that they did not participate in the Aged and Disabled waiver program for three fiscal years, 2000–2002. There were 390 people in the Mixed Group. A total of 448 subjects, in both the comparison groups, were examined for this phase of the study.
Procedures Data were analyzed to generate demographic characteristics of both groups and included descriptive information such as age, gender, race, and mental health disorders. For the latter, the primary mental health diagnosis for subjects was based on a hierarchy. For the purposes of the study, the primary diagnosis for individuals with multiple mental health disorders was the most severe condition.
23
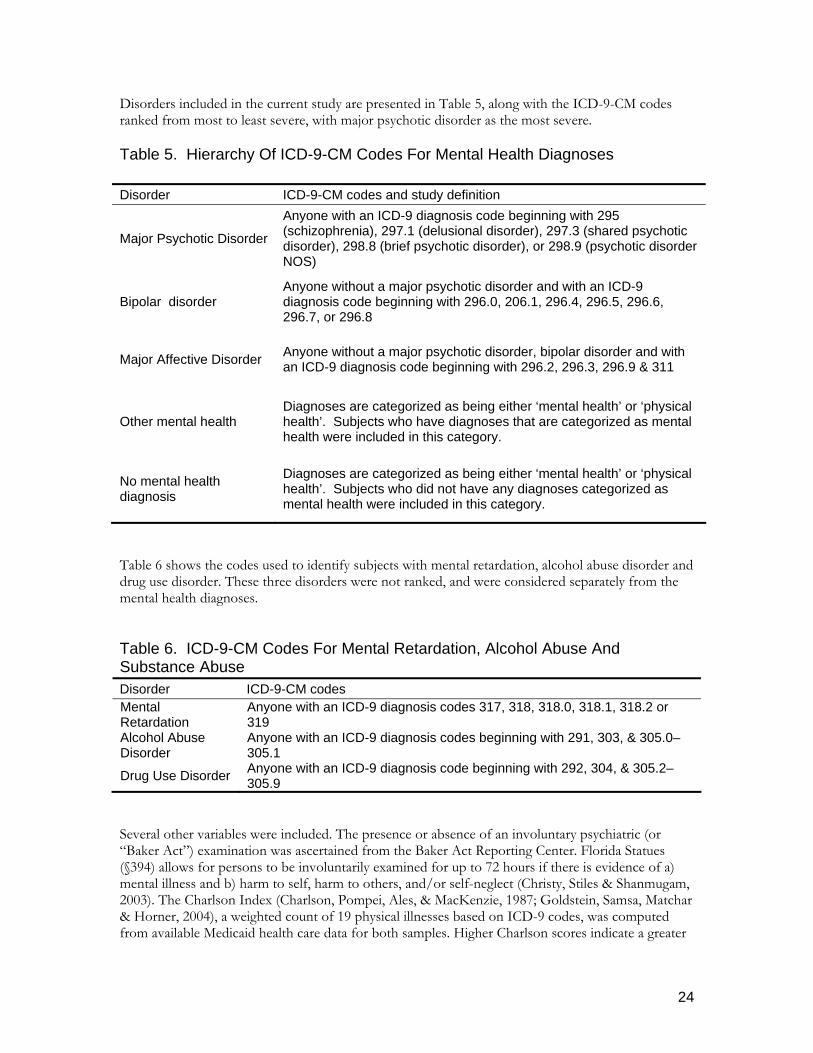
Disorders included in the current study are presented in Table 5, along with the ICD-9-CM codes ranked from most to least severe, with major psychotic disorder as the most severe. Table 5. Hierarchy Of ICD-9-CM Codes For Mental Health Diagnoses
Disorder ICD-9-CM codes and study definition
Major Psychotic Disorder
Anyone with an ICD-9 diagnosis code beginning with 295 (schizophrenia), 297.1 (delusional disorder), 297.3 (shared psychotic disorder), 298.8 (brief psychotic disorder), or 298.9 (psychotic disorder NOS)
Bipolar disorder Anyone without a major psychotic disorder and with an ICD-9 diagnosis code beginning with 296.0, 206.1, 296.4, 296.5, 296.6, 296.7, or 296.8
Major Affective Disorder Anyone without a major psychotic disorder, bipolar disorder and with an ICD-9 diagnosis code beginning with 296.2, 296.3, 296.9 & 311
Other mental health Diagnoses are categorized as being either ‘mental health’ or ‘physical health’. Subjects who have diagnoses that are categorized as mental health were included in this category.
No mental health diagnosis
Diagnoses are categorized as being either ‘mental health’ or ‘physical health’. Subjects who did not have any diagnoses categorized as mental health were included in this category.
Table 6 shows the codes used to identify subjects with mental retardation, alcohol abuse disorder and drug use disorder. These three disorders were not ranked, and were considered separately from the mental health diagnoses. Table 6. ICD-9-CM Codes For Mental Retardation, Alcohol Abuse And Substance Abuse Disorder ICD-9-CM codes Mental Retardation
Anyone with an ICD-9 diagnosis codes 317, 318, 318.0, 318.1, 318.2 or 319
Alcohol Abuse Disorder
Anyone with an ICD-9 diagnosis codes beginning with 291, 303, & 305.0–305.1
Drug Use Disorder Anyone with an ICD-9 diagnosis code beginning with 292, 304, & 305.2–305.9
Several other variables were included. The presence or absence of an involuntary psychiatric (or “Baker Act”) examination was ascertained from the Baker Act Reporting Center. Florida Statues (§394) allows for persons to be involuntarily examined for up to 72 hours if there is evidence of a) mental illness and b) harm to self, harm to others, and/or self-neglect (Christy, Stiles & Shanmugam, 2003). The Charlson Index (Charlson, Pompei, Ales, & MacKenzie, 1987; Goldstein, Samsa, Matchar & Horner, 2004), a weighted count of 19 physical illnesses based on ICD-9 codes, was computed from available Medicaid health care data for both samples. Higher Charlson scores indicate a greater
24

likelihood of one-year mortality. Nursing home admission rates, as well as mean time from study entry to nursing home admission were also reviewed. Mean time to nursing home admission was calculated by subtracting the study start date, July 1, 2001, from the date a subject was admitted to a nursing home. If a subject did not enter a nursing home, their study end date was June 30, 2002 for this portion of the evaluation. A series of statistical significance tests were run between the two groups across all of the demographic characteristics. Depending on the variable being compared (continuous vs. dichotomous), a χ2 or a t-test was used to determine whether there were any statistically significant differences between the comparison groups. Services were grouped into categories using Catcaid codes (for a complete explanation and list of Catcaid codes, see Appendix A). Cost data were computed according to the categories. Costs included all service and pharmacy expenditures that were incurred only while an individual resided in the community. Totals do not include the cost of care once an individual was admitted to a nursing home. Table 7 presents descriptions of the categories as well as the corresponding codes. Table 7. Service Category Descriptions and Corresponding Catcaid Codes
Category description Defining Catcaid codes Inpatient behavior health service use 01.00, 01.50, 03.00, 03.50
Emergency room service 04.00
Outpatient (BH) treatment 04.50, 05.00, 05.25, 05.50, 08.00, 10.00, 18.00, 20.00, 20.10, 20.20, 20.30, 20.40
Day treatment/partial hospitalization 01.20, 03.20, 12.00
Case management services 06.00, 07.00, 07.50, 13.00 Total behavioral health < 50.00 Total physical health expenditures > = 50.00 Psychotropic drug expenditures* Brand/generic name Cognate drug expenditures* Brand/generic name Other pharmacy expenditures* Brand/generic name Total pharmacy expenditures All expenditures Total expenditures All expenditures
* Brand and generic names were to select specific medications, rather than Catcaid codes The study entry date for the purposes of calculating costs was the first day of FY 01–2002 that a subject was eligible for Medicaid. In most instances, this was the July 1, 2001 (Table 8 presents the frequency distribution for study start dates). The date a subject exited the study was either the date of admission to a nursing facility or the last day of FY 2001–2002, whichever came first. Total costs for 432 persons while community-dwelling were included in the tables.
Table 8. Dates of Study Entry, FY 2001–2002* (n = 433)
Start date Frequency % 7/1/01 428 98.85 9/1/01 1 0.23 10/1/01 2 0.46
25
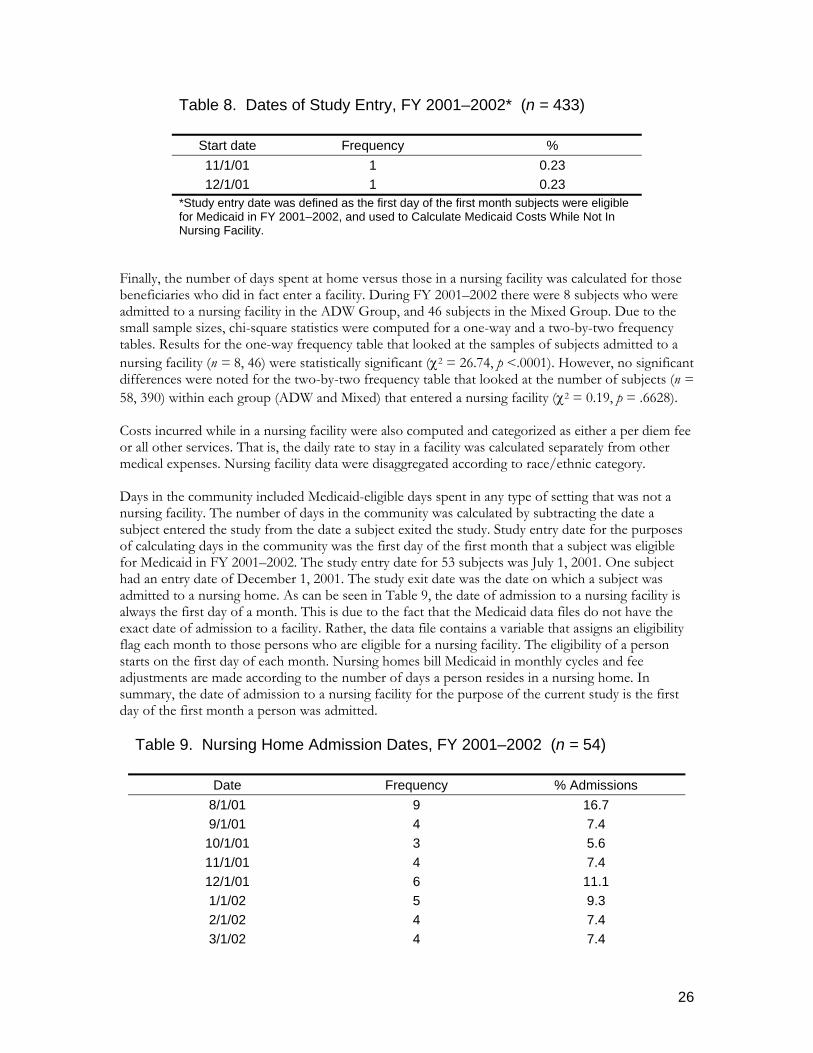
Table 8. Dates of Study Entry, FY 2001–2002* (n = 433)
Start date Frequency % 11/1/01 1 0.23 12/1/01 1 0.23
*Study entry date was defined as the first day of the first month subjects were eligible for Medicaid in FY 2001–2002, and used to Calculate Medicaid Costs While Not In Nursing Facility.
Finally, the number of days spent at home versus those in a nursing facility was calculated for those beneficiaries who did in fact enter a facility. During FY 2001–2002 there were 8 subjects who were admitted to a nursing facility in the ADW Group, and 46 subjects in the Mixed Group. Due to the small sample sizes, chi-square statistics were computed for a one-way and a two-by-two frequency tables. Results for the one-way frequency table that looked at the samples of subjects admitted to a nursing facility (n = 8, 46) were statistically significant (χ2 = 26.74, p <.0001). However, no significant differences were noted for the two-by-two frequency table that looked at the number of subjects (n = 58, 390) within each group (ADW and Mixed) that entered a nursing facility (χ2 = 0.19, p = .6628). Costs incurred while in a nursing facility were also computed and categorized as either a per diem fee or all other services. That is, the daily rate to stay in a facility was calculated separately from other medical expenses. Nursing facility data were disaggregated according to race/ethnic category. Days in the community included Medicaid-eligible days spent in any type of setting that was not a nursing facility. The number of days in the community was calculated by subtracting the date a subject entered the study from the date a subject exited the study. Study entry date for the purposes of calculating days in the community was the first day of the first month that a subject was eligible for Medicaid in FY 2001–2002. The study entry date for 53 subjects was July 1, 2001. One subject had an entry date of December 1, 2001. The study exit date was the date on which a subject was admitted to a nursing home. As can be seen in Table 9, the date of admission to a nursing facility is always the first day of a month. This is due to the fact that the Medicaid data files do not have the exact date of admission to a facility. Rather, the data file contains a variable that assigns an eligibility flag each month to those persons who are eligible for a nursing facility. The eligibility of a person starts on the first day of each month. Nursing homes bill Medicaid in monthly cycles and fee adjustments are made according to the number of days a person resides in a nursing home. In summary, the date of admission to a nursing facility for the purpose of the current study is the first day of the first month a person was admitted.
Table 9. Nursing Home Admission Dates, FY 2001–2002 (n = 54)
Date Frequency % Admissions 8/1/01 9 16.7 9/1/01 4 7.4
10/1/01 3 5.6 11/1/01 4 7.4 12/1/01 6 11.1 1/1/02 5 9.3 2/1/02 4 7.4 3/1/02 4 7.4
26

Table 9. Nursing Home Admission Dates, FY 2001–2002 (n = 54)
Date Frequency % Admissions 4/1/02 4 7.4 5/1/02 8 14.8 6/1/02 3 5.6
Used for calculating mean number of days in the community and days in a nursing home Mean number of days in a nursing home was calculated in three steps. First, the date of admission to a nursing home was subtracted from the last day of the last month that a subject had a flag for nursing home eligibility. Second, the number of days spent in a hospital or in an inpatient setting during the nursing home eligibility time frame were summed for each person. Third, the number of inpatient days spent in a hospital were subtracted from the number of days spent in a nursing home as indicated in the first step. There were 11 subjects who, during the course of their eligibility for Medicaid while in a nursing home, were briefly admitted to a general hospital for treatment. A review of the data indicated that the sample of subjects did not access any other type of inpatient or residential treatment facilities while they were eligible for a nursing home. Therefore, only general hospital stays were addressed. Any other inpatient stays would also have been subtracted from the time spent in a nursing home. The cost for nursing home care was calculated by summing all of the claims that were incurred during the time a person was in a nursing home. However, the cost of nursing home care only includes the per diem rate. Other expenses such as fees for medical services, prescription drugs, etc. were summed separately. Comparison groups three and four will replicate the criteria for comparison groups one and two, respectively. However, demographic data, service use and cost information and number of days in the community will be calculated using files from FY 2003–2004. Subjects must have a diagnosis in FY 2002–2003 in order to be included in either group three or four.
Results Socio-Demographic, Health and Utilization Differences by Group By and large the two samples were more alike than they were different.
Demographic Differences. As shown in Table 10, the two comparison groups did not differ in age, with the average age of both approximating 80. Although the non-waiver group had more men (25.13%) than the ADW group (13.79%), the difference was not statistically significant (the probability was p = .06, however, suggesting that there was a 6% chance of finding a difference of this magnitude by chance). In contrast to age and gender, significant differences were found for ethnic/racial groups. In particular, while no differences were found for non-Hispanic Whites and Hispanics, there were significantly more African Americans in the ADW Group. African Americans made up approximately 31% of the ADWs, and only about 8.5% of the Mixed. In addition, there were significantly more from the miscellaneous “Other” category for the Mixed Group. The Other category consists of persons who endorsed a mixed or multicultural category of ethnic/racial identity, who felt their ancestry was not included in the available categories, who refused to respond or did not know how to categorize themselves, or who were misclassified by intake staff. The fact that 177 persons in the Mixed Group,
27

slightly over 45%, were categorized as "Other" raises concerns, since little if anything is known about who they are, or what their needs might be.
28

Table 10. Mixed Group (n = 390) and ADW Group (n = 58) Demographics, FY 2001–2002
Characteristic
Mixed Group of Medicaid
Clients with AD, n = 390
Medicaid Aged/Disabled Waiver
Comparison Group Clients with AD, n =
58
n % n % χ2 or t
Age at study entry 60-64 28 7.18% 2 3.45% 65-69 40 10.26% 4 6.90% 70-74 33 8.46% 5 8.62% 75-79 76 19.49% 8 13.79% 80-84 92 23.59% 15 25.86% 85-89 61 15.64% 15 25.86% 90 and above 60 15.38% 9 15.52%
5.73
Mean Age (sd) 79.21 (9.2) 81.19 (8.5) 1.55 b
Sex Male 98 25.13% 8 13.79% Female 292 74.87% 50 86.21% 3.59
Race White 138 35.38% 21 36.21% 0.02
Black 33 8.46% 18 31.03% 25.50 ***
Amer. Indian 0 0% 0 0% NA Oriental 0 0% 0 0% NA Hispanic 42 10.77% 4 6.90% 0.82
Others 177 45.38% 15 25.86% 7.86 **
MH Diagnosis
Major psychotic 30 7.69% 0 0% 0.022 a, *
Bipolar disorder 4 1.03% 0 0% 1.000
a
Affective disorder 31 7.95% 2 3.45% 0.289 a
Other mental disorder 17 4.36% 0 0% 0.156 a
No MH diagnosis 308 78.87% 56 96.55% 0.003 a, **
Other Problems Mental retardation 0 0% 0 0% NA
Baker Act exam 10 2.56% 0 0% 0.374 a
Alcohol use disorder 0 0% 0 0% NA Drug use disorder 0 0% 0 0% NA
Charlson Co-morbidity Score 0.83 0.71 -0.96 b
29

Place of Residence Mean Medicaid Eligible Days in Community 323.86 (83.29) 309.72 (101.99) 1.01
b
Number% with nursing facility (NF) admission 46 11.79% 8 13.79% 0.19
Mean time to first NF Admission, in months 5.88 (3.45) 5.02 (2.72) -0.69
b
Mean number of Medicaid days in NF 138.11 (99.28) 117.13 (53.99) -0.58
b
Medicaid Eligibility
Total Months eligible 10.82 (2.79) 11.60 (1.24) 3.65 b ***
* p < .05, ** p < .01 *** p < .001 a Fisher’s exact test, because cells had small expected frequencies. b t-tests were used when the variable was continuous.
Mental and Physical Health Indicators. Table 10 also includes a number of health indicators. The only area of difference between the two groups was in mental health diagnoses. The Mixed Group was generally more likely to have a reported mental health problem than were those in the ADW Group. In terms of specific diagnoses, the Mixed Group was significantly more likely to have a diagnosis of major psychosis. While none of the ADW suffered from a major psychosis, nearly 8% of the Mixed Group had been so diagnosed. For other mental health problems, the non-waiver comparison sample had a higher frequency than the ADW sample, but the results did not reach significance. Perhaps the most dramatic mental health difference was in the proportion for whom no mental health diagnosis had been reported: approximately 97% of the ADW sample had no MH diagnosis, as compared to only 79% of the non-waiver group. For other problems, including alcohol/substance abuse and Baker Act referrals, as well as overall physical health status, the two samples were comparable. Noteworthy was that none of the clients included in either sample used services related to mental retardation, or alcohol and substance abuse. Moreover, given that all members of the ADW Group had to meet Medicaid level of care requirements for nursing home certification, one would have assumed that this group would be more disadvantaged in physical health than members of the Mixed Group.
Days spent living in the community. As shown in Table 10, on average the two groups spent a similar number of days living in the community. Note that days in community was here defined as all days not spent in a nursing facility; as a result, days in community therefore actually includes days spent in assisted living as well as inpatient hospital days. Moreover, there is an important caveat about the variable, which is that due to restrictions imposed by the nature of the data source, the count of days in community actually consists of a count of Medicaid-eligible days, not the total number of calendar days. Both groups averaged well over 300 Medicaid-eligible days in community, with the Mixed Group spending more (324) days in community than did the ADW Group (310 days). The differences, again, were not significant.
Ethnic/racial differences in days spent in community. While the analysis of overall group differences revealed that the ADW group did not differ from the Mixed group in terms of overall time to nursing homes, a question that is important to Florida is whether there were differences across racial and minority groups. As presented in Table 11, one of the unusual findings is that beneficiaries in the “Other” category generally had the greatest number of Medicaid-eligible days in the community. In other words while Medicaid eligible – a status based primarily on meeting criteria for low income – those “Other” category of minority status spent more
30

days in community. Hispanics were generally lowest in days spent in community; this result is primarily a based on Hispanics from the Mixed Group, since none of the very few Hispanic beneficiaries enrolled in the ADW waiver spent any Medicaid-eligible days outside of the community. However, in terms of a significant differences, Hispanics in the combined sample differed only from those in the “Other” category for the combined sample, and from both the Others and Whites in the Mixed Group.
31

Table 11. Participants’ Medicaid-Eligible Community Days, by Race* n Mean SD All
White 159 310.84 99.94 Black 51 296.82 107.67 Hispanic 46 270.28 117.08 Others 192 325.94 90.01
Group 1: ADW White 21 330.43 99.62 Black 18 304.61 82.71 Hispanic A 4 365.0 0.0 Others 15 326.80 68.76
Group 2: Mixed White 138 307.86 100.01 Black 33 292.58 120.11 Hispanic A, B 42 261.26 118.69 Others 177 325.86 91.75
* Community days are all days not spent in a nursing facility. A* Hispanics differ from Others, p = .05 B* Hispanics differ from Whites, p = .05
Nursing Facility Admission. Over the one year of study, small and comparable proportions of people in both groups were admitted to nursing facilities (Table 10). For the Mixed Group, 11.79% were admitted (n = 46), and 13.79% of the ADW Group (n = 8). This represents 12.05% of the combined sample. For those people who ended up being admitted to a nursing facility, the average time from beginning of the evaluation period to admission was between five and six months. To put these figures into perspective, recall that all clients in the two comparison groups were age 60 or over and had a diagnosis of AD in July, 2001, the start of the evaluation period. Further, none had been in a nursing facility within three months of July, and none had been admitted during July. These findings suggest that for any group of Medicaid beneficiaries aged 60 and over with AD, whether participating in the ADW or not, it can be expected at least 12% will be institutionalized—even if members of the group have no recent history of institutionalization. The fact that the average time to institutionalization was less than six months, for those who were in fact admitted, is of particular interest. Again, recall that at the beginning of the study year (FY 2001–2002) none of the sample, including the 54 people who were eventually admitted to nursing facilities, had a recent history of institutionalization. What factors were associated with admission will be discussed in a later section of this report. Finally, on average— including those who were admitted as well as those who were not admitted to a nursing facility—the ADW Group spent approximately 117 days in a nursing home, and those in the Mixed Group spent approximately 138 days. Due to the small sample sizes, the mean difference was not significant. It is worth pointing out, however, that the ADW Group spent somewhat fewer days in the community, but also spent somewhat fewer days in a nursing facility. The reason for this seeming non-sequitur appears to be that those in the Mixed Group, if admitted, spent more days
32

than did those in the ADW Group. This explanation is substantiated by the fact that, while the differences once again were not significant, the ADW Group members who did become institutionalized did so sooner (5.02 months) than did those in the Mixed Group (5.88 months). Further studies with a greater number of subjects might provide the statistical power needed to ascertain the magnitude of these effects.
Ethnic/racial differences in Medicaid days spent in nursing facilities. Due at least in part to the small number (only 54, or 12% of the total sample) of beneficiaries who were admitted to a nursing home during the study period, the breakdown by race did not reveal any significant differences by group or for the combined sample (Table 12). Comparing the results of Table 12 with those for days spent in the community (Table 11), it becomes clear that considerable work would be required before it would be possible to understand ethnic minority disparities in nursing home utilization. In addition to containing information on Medicaid days spent in a nursing facility, Table 12 includes information on the number and proportion of people from different ethnic/racial categories who were admitted to a facility. Looking just at the overall sample, of particular interest is the comparatively low proportion (7.3%) of persons in the “Other” category who spent time in a nursing facility. That percent stands in contrast to the 23.9% of Hispanics in the combined sample. Looking at the two groups, it is interesting that Blacks, who made up 31% of the ADW Group, were the most likely of any ethnic/racial category in that sample to be placed in a nursing facility. In the Mixed Group, Hispanics were the most likely to be institutionalized, and again, Others were least likely.
Table 12. Participants’ Medicaid-Eligible Days in a Nursing Facility, by Race Number (% of category) Mean Days (SD) All Subjects
White 21 (13.2%) 134.61 (86.06) Black 8 (15.7%) 172.00 (100.27) Hispanic 11 (23.9%) 116.64 (85.89) Others 14 (7.3%) 128.86 (110.77)
ADW Group White 2 (9.5%) 121.50 (43.13) Black 4 (22.2%) 148.25 (43.12) Hispanic 0 (0%) n/a (n/a) Others 2 (13.3%) 50.50 (13.44)
Mixed Group White 19 (13.8%) 136.00 (90.03) Black 4 (12.1%) 195.75 (141.76) Hispanic 11 (26.2%) 116.63 (85.89) Others 12 (6.8%) 141.91 (114.82)
Months of Medicaid eligibility. The last row in Table 10, above, shows total months out of FY 2001–2002 in which members of the two groups were Medicaid eligible. Averaging over eleven and a half months of eligibility, those in the ADW Group generally had about three quarters of a month more of eligibility than the Mixed
33

Group. This finding may simply reflect the fact that members of the ADW group had to meet strict criteria for inclusion in the ADW program, while members of the Mixed Group may or may not have had to meet any eligibility requirements for various programs.
Cost Implications When reviewing the following presentation, it should be kept in mind that cost calculations were based on value of the dollar during the fiscal year for which calculations were made: 2001–2002.
Behavioral health. Sixteen people were excluded from the sample included in the analysis of costs (see Table 13a-c, below) for the Mixed Group (n = 390), either because they had less than one month of eligibility for Medicaid (n = 1) or because they had no claims from the time they entered the study until the time they exited the study (n = 15), leaving 374 subjects in that group. No subject was eliminated from the ADW group. Tables 13a through 13c provide information on utilization and associated costs for a variety of services. The two samples differed significantly on some services and were similar on others. A number of apparent differences actually were not statistically significant, due both to small sample sizes and amount of within-group variance. Inpatient behavioral health services is a case in point. None of the ADW Group, but 14 (or 3.74%) of the Mixed Group, accessed inpatient behavioral health services. However a t-test of mean user differences in cost could not be calculated, due to the fact that none of the ADW Group used the service. On the other hand, if one magnified these differences to larger groups, the cost differences would definitely be meaningful. Medicaid spent a monthly average of approximately $714 on inpatient behavioral services for each of the 14 Mixed Group users of the service (per user per month, PUPM, sometimes referred to as per recipient, or PR). The average cost for the each member of the Mixed Group per month (regardless of whether they used the service or not), was $26.71 and the average cost for each member of the entire group of beneficiaries for the year was approximately $230.00 (the last column). Since the two groups are in some ways the result of an arbitrary split, we also combined the sample (Table 13c). Here the average monthly cost of inpatient behavioral health for all beneficiaries, user or not, was $23.13; the yearly per member average cost was $199.45. This relatively low cost is accounted for by the fact that only 14 users out of the entire combined sample, here with an n of 432, actually used inpatient behavioral health services.
34

Table 13a. Service Costs for AD Beneficiaries in the Aged/Disabled Waiver Program, FY 2001–2002* (n = 58) PUPM, 1 Users6 Annual
Penetration4 PMPM,2 Per-member Cost3
Behavioral Health Services
Inpatient behavior health $0 0 0% $0 $0
Total behavioral health $73.78 57*** 98.28% $72.51 $739.18 Physical Health Services
Emergency room service $0 0 0% $0 $0
Outpatient treatment $129.65 6 10.34% $13.41 $107.97 Day treatment $197.21 1 1.72% $3.40 $20.40 Case management services $56.67 57*** 98.28% $55.70 $610.80
Total physical health $1,262.39*** 58*** 100% $1,262.39 $13,071.61
Pharmacy Services Psychotropic drug expenditures $66.97** 23** 39.70% $26.56 $316.47
Cognate drug expenditures $79.03 27 46.55% $36.79 $417.10
Other pharmacy expenditures $170.45 55 94.83% $161.6
3 $1,790.63
Total pharmacy expenditures5 $237.26 55 94.83% $224.9
8 $2,524.21
Total expenditures $1,559.89*** 58*** 100% $1,559.89 $16,334.99
* Subjects were excluded from the cost table if they had less than one month of eligibility (n = 0) or if they had no
records of claims for the eligibility period (n = 0). ‘Eligibility period’ was defined as the time from the first date of eligibility for Medicaid in FY 2001–2002 until the last day of FY 2001–2002 or the date of entry into a nursing home, whichever comes first. Therefore, the table includes only those costs incurred while a subject was community-dwelling.
1 PUPM Per-user-per-month is the average cost of a service category per month, calculated by dividing the total cost for a service category for the fiscal year by the number of users per eligible month.
2 PMPM Per-member-per-month is the average cost of a service category per month for all subjects in the samples regardless of whether they used the service.
3 Per-member cost is the average cost of a service category for each subject for the year regardless of whether they used the service or were eligible.
4 Annual penetration rate is calculated by dividing the number of subjects who used a service during the fiscal year by the number of subjects in the sample.
5 Total pharmacy expenditures is calculated by computing the total of all pharmacy costs and then dividing by the number of subjects who received any pharmacy services. Therefore, the averages for the types of pharmacy expenditures will not necessarily equal the total ‘average’.
6 χ2 tests, or Fisher’s exact test, used to determine whether groups were significantly different from one another. * p< .05, **p < .01, ***p < .001
35

Table 13b. Service Costs for AD Beneficiaries Not Participating in the Aged/Disabled Waiver Program, FY 2001–2002 (n = 374)
PUPM1 Users Annual penetration PMPM Per-member
cost Behavioral Health Services
Inpatient behavior health $713.59 14 3.74% $26.71 $230.38
Total behavioral health $229.22 94 25.13% $57.61 $560.56
Physical Health Services
Emergency room service $14.52 9 2.41% $0.35 $1.31
Outpatient treatment $89.02 85 22.72% $20.23 $218.04
Day treatment $215.96 6 1.60% $3.46 $41.57 Case management services $82.71 31 8.29% $6.86 $69.26
Total physical health $774.26 358 95.72% $741.41 $6,252.62
Pharmacy Services Psychotropic drug expenditures $115.67 227 60.70% $70.21 $759.54
Cognate drug expenditures $83.44 184 49.20% $41.05 $449.67
Other pharmacy expenditures $176.22 357 95.45% $168.21 $1,796.98
Total pharmacy expenditures $290.34 360 96.26% $279.47 $3,006.19
Total expenditures $1,078.22 374 100% $1,078.22 $9,416.53 * Subjects were excluded from the cost table if they had less than one month of eligibility (n = 1) or if
they had no records of claims for the eligibility period (n = 15). ‘Eligibility period’ was defined as the time from the first date of eligibility for Medicaid in Fiscal Year 2001–2002 until the last day of FY 2001-2002 or the date of entry into a nursing home, whichever comes first. Therefore, the table includes only those costs incurred while a subject was community-dwelling.
PUPM Per-user-per-month is the average cost of a service category per month, calculated by dividing the total cost for a service category for the fiscal year by the number of users per eligible month.
PMPM Per-member-per-month is the average cost of a service category per month for all subjects in the samples regardless of whether they used the service.
36

Table 13c. Service Cost Data for All Study Participants Combined, FY 2001–2002 (N = 432)
Services PUPM Users Annual penetration PMPM cost Per-member
cost Behavioral Health Services
Inpatient behavior health $713.59 14 3.24% $23.13 $199.45
Total behavioral health $170.55 151 34.95% $59.61 $584.54
Physical Health Services
Emergency room service $14.52 9 2.08% $0.30 $1.13
Outpatient treatment $91.69 91 21.06% $19.32 $203.26
Day treatment $213.28 7 1.62% $3.46 $38.73 Case management services
$65.85 88 20.37% $13.41 $141.96
Total physical health $842.32 416 96.29% $811.12 $7,168.14
Pharmacy Services Psychotropic drug expenditures $111.19 250 57.87% $64.35 $700.05
Cognate drug expenditures $82.88 211 48.84% $40.48 $445.29
Other pharmacy expenditures $175.45 412 95.37% $167.33 $1796.13
Total pharmacy expenditures $283.30 415 96.06% $272.16 $2,941.48
Total expenditures $1,142.89 432 100.00% $1,142.89 $10,694.16 *Subjects were excluded from the cost table if they had less than one month of eligibility (n = 1) or if
they had no records of claims for the eligibility period (n = 15). ‘Eligibility period’ was defined as the time from the first date of eligibility for Medicaid in FY 2001–2002 until the last day of FY 2001–2002 or the date of entry into a nursing home, whichever comes first. Therefore, the table includes only those costs incurred while a subject was community-dwelling.
PUPM Per-user-per-month is the average cost of a service category per month, calculated by dividing the total cost for a service category for the fiscal year by the number of users per eligible month.
PMPM Per-member-per-month is the average cost of a service category per month for all subjects in the samples regardless of whether they used the service.
While the significance of inpatient behavioral health costs could not be calculated across groups, total behavioral health costs were computed and found to differ. The PUPM for the ADW Group was approximately $74, which was significantly lower than the $229.22 for the Mixed Group. Also significantly different was the number of users: surprisingly while their PUPM was lower, all but one of the ADW Group used a behavioral health service. In contrast, only 94 of the 374 members of the Mixed Group used a behavioral health service. As a result of these differences in cost and use, per member costs for the entire year were $739.18 for the ADW Group and $560.56 for the Mixed
37

Group. In other words, the total behavioral health cost of Mixed Group beneficiaries was lower than for ADW beneficiaries, a surprising finding given that the Mixed Group had a higher proportion of beneficiaries with a mental health diagnosis. Combining the two samples, the average monthly cost for all beneficiaries with AD was nearly $60, and the average yearly cost for all behavioral health care was $584.54. In considering these results, especially the overall use of behavioral health services by the ADW Group, it should again be emphasized that the Mixed Group had significantly more individuals with a major psychosis, and significantly more with a mental health diagnosis. Because of the greater prevalence of a diagnosed mental disorder, when expenditures for combined or total behavioral health services are compared it is surprising that nearly all the ADW Group made use of such services, as compared to slightly over 25% of the Mixed Group. As will be discussed in the following paragraphs, these costs are relatively low compared to other areas of service utilization.
Non-specific health expenditures. In this section will be considered several service areas that could reflect either physical or behavioral health care, or a combination of the two. The first is the emergency room service (see Tables 13a-13c). None of the ADW Group accessed ER services during the study year, as opposed to 9 (or 2.41%) in the Mixed Group. Due to the lack of ADW users, no test of statistical differences was calculated for this category of service. Even in the Mixed Group the proportion of ER users, at 2.41%, was quite low. The costs per service user, $14.52, were also quite low. Overall, for the two samples combined, the average per member cost for the entire 12 month period was $1.13. Day Treatment represents yet another area of group similarity. The day treatment category included partial hospitalization and respite services. Examples of partial hospitalization are attendance at a substance abuse program from 8 AM–5 PM each day; or some type of intense treatment from 8 AM–5 PM each day. The annual penetration rate for both groups was less than 2%, and for the combined sample it was 1.62%. The cost PUPM for the combined sample was approximately $213, and the per member average cost for the combined sample was only $38.73. This rather small expenditure is explained by the fact that a total of only 7 beneficiaries made use of day treatment services during the fiscal year being studied. On the other hand, it is notable that so few beneficiaries with a diagnosis of Alzheimer’s disease were availing themselves of services, of which respite is a major example. As may be recalled from the earlier review of services covered under the Medicaid Alzheimer’s Home and Community-based waiver program, respite services are an essential component. For outpatient treatment on the other hand, the differences were statistically significant. The outpatient treatment category included the following: physicians visits, home-based services, outpatient mental health services, counseling, therapy, occupational therapy, speech/language therapy, and physical therapy (along with some other minor categories). With nearly 23% of the non-waiver group using outpatient services, a proportion more than twice that of the ADW Group, the former group had a PUPM that was higher than the latter, but the PMPM and yearly per member costs were lower. With the two groups combined, the average yearly cost per member for outpatient services was $203.26. Most probably due to its inclusion within the ADW list of approved services, case management services utilization was close to 100% on the part of the ADW Group, as compared with only 8.29% of the Mixed group. The PUPM costs for the Mixed Group, at $82.71, were roughly equivalent to the $56.67 found for the ADW Group. These results suggest that the use of case management with beneficiaries with AD who are not participating in a waiver program deserves further attention: the low level of case management utilization is a cause of some concern.
38

As shown by the row indicating total costs for physical health services, the specific services presented in Table 13 clearly do not represent all the costs borne by Medicaid. Health care costs were substantial for both groups, with those for the ADW group being significantly higher: nearly twice that of the Mixed Group. The fact that the two groups do not differ significantly in days in community or nursing facility admission rates suggests that the differences in expenditures do not result in any net savings to Medicaid. In others words, based on the information reviewed in the present report, the greater costs associated with the ADW Group did not result in a significant delay in institutionalization.
Psychotropic and cognate medications. Paralleling the greater use of behavioral health services by the non-waiver group, the latter were significantly more likely to use psychotropic medications: nearly 61% as compared to approximately 40% of the ADW Group (Table 13a-c). Correspondingly, the Mixed Group also incurred significantly higher expenditures for psychotropic drugs. Their PUPM was $115.67, as compared to $66.97 for the AWD. The two samples combined had a PUPM of $111.19. From the perspective of the entire combined sample, including users and non-users, there was a PMPM of $64.35 and a yearly total cost of $700.05 for psychotropic drugs. Expenditures for cognate drugs were somewhat less, and also were roughly equivalent for the two groups. This is not surprising, given that both groups consisted of persons with a diagnosis of AD. Looking at the two samples combined, the cost PUPM for cognate drugs was $82.88, with a penetration rate of 48.84%. The penetration rate is surprisingly low, since one would anticipate that individuals entering the fiscal year with a diagnosis of AD would be receiving one of the several medications available for symptom relief. As the final report on the cognate sub-study of the Alzheimer’s disease waiver project makes clear (see Part 3 of this report), generally a much higher proportion of cognate drug utilization would be expected. There is, however, evidence that caregivers are unlikely to use available services unless they have contact with a social worker or have a physical disability (e.g., Brodaty, Thomson, Thompson, & Fine, 2005).
Non-specific and overall pharmacy expenditures. Expenditures for drugs that were neither psychotropic nor cognate in nature were comparable across the two studies. For the two samples combined (Table 13c), the cost PUPM was $175.45, with a penetration rate of 95.37%. The PMPM for the combined sample was $167.33, which is more than PMPM expenditures for the psychotropic and cognate drugs separately or in combination. The average yearly per member cost was $1796.13. Overall or total pharmacy expenditures were also comparable across groups, despite the non-waiver group’s significantly greater use of psychotropic drugs. Cost PUPM for the combined sample was $283.30, with over a 96% penetration rate. Generally it could be anticipated that the average Medicaid beneficiary with AD, aged 60 and over, would generate overall Medicaid pharmaceutical expenditures of about $3000 per year.
Total expenditures. The final row in Tables 13a-c present information on overall Medicaid expenditures reported for the two groups. On average, the PUPM cost for the Mixed Group was $481.67 less than that of the ADW Group. Most of the difference appears to be attributable to physical rather than mental health costs. Note that for both samples, PUPM is based on a 100% penetration rate, meaning that PUPM is the same as PMPM. For the combined sample, the PUPM was $1,142.89, a figure that may provide a better overall estimate of the average cost of providing services to Medicaid beneficiaries with AD and who were aged 60 and over during FY 2001–2002. The per member cost for the full 12 month period was $10,694.16 for the combined sample.
39

The Socio-Demographic Predictors of Admission to a Nursing Facility As a beginning step in ascertaining what is a truly complex phenomenon, the final set of analyses in this part of the report explores how well the socio-demographic variables used in addressing the prior questions were able to predict actual admission to a nursing facility. Here we will generally focus only on results for the combined sample of 448 beneficiaries, although results for the ADW sample in one instance will be noted. That one instance pertains to the association of admission with age. As shown in Table 14, younger beneficiaries in the ADW Group were less likely to be admitted, but age was irrelevant in the Mixed Group and in the combined sample. In interpreting this finding, it should be kept in mind that while AD is a disease whose incidence goes up with age, all beneficiaries included in the present evaluation had already been diagnosed with AD prior to the year of study. Hence, the association of age with admission to a facility has nothing to do with increasing disease prevalence. What it may pertain to is the fact that the ADW Group members, as part of becoming eligible for the ADW program, had to meet level of care standards that are particularly concerned with frailty and health needs. In other words, the ADW sample was in all likelihood quite frail from a medical point of view. This fact has already been referenced in this report, in the presentation of differences between the ADW and Mixed groups with respect to differences in physical health expenditures. It may also be the case that the younger AD patients in the ADW group were more active, and for this reason were more of a management problem. For the Mixed Group, but not those in the ADW, being a woman was associated with a greater likelihood of nursing home admission (Table 14). This finding would be anticipated from the literature review. Part of the reason is that the majority of elders have been married, but since men have a shorter life expectancy and tend to marry women who are younger, men are more likely as they get older to have a spouse for support. Women are more likely to become widows, thereby losing a critical supportive person. This last factor becomes important with respect to risk of institutionalization since one of the primary risk factors is lack of social supports (e.g., Kane, et al., 2004). The race/ethnicity of beneficiaries with Alzheimer’s disease does seem to make a difference. Somewhat surprisingly, Hispanics in the Mixed Group (and of course in the combined sample as well) were more likely to be admitted to a nursing facility than people in all other categories combined. Like that for sex, the correlation is relatively small and accounts for only about 2.6% of the variance in admission. However, these results are compatible with some interesting findings from other studies, where Hispanic caregivers to dementia patients were found to be significantly more depressed than other groups (e.g., Adams, et al., 2002; Aranda & Knight, 1997 ) There is also some evidence that Hispanics have higher rates of dementia than Whites, and both Hispanics and African American elders may become dependent at earlier ages (Aranda & Knight, 1997; Gurland, et al., 1999; Fitten, Ortiz & Ponton, 2001; Wallsten, 2000). On the other hand, we know that Hispanics, as well as Blacks and Asian groups, are significantly under-represented in nursing home populations.
Table 14. Correlations of Demographic Characteristics with Nursing Facility Admission
ADW Group Mixed Group Combined Sample
Age -.30* .01 -0.03 Male -.13 -.12* -0.12* White .09 -.05 -.03 Black -.16 -.00 -.04 Hispanic .11 -.16** -.12** Other ethnic group .01 .14** .13**
40

Table 14. Correlations of Demographic Characteristics with Nursing Facility Admission
ADW Group Mixed Group Combined Sample
Affective and Other Disorders .08 .04 0.04
Major psychotic disorder n/a -.13** -0.12** Bipolar disorder n/a -.04 -0.04 Baker Act exam n/a -.19*** -0.18*** No mental health diagnosis -.08 .06 0.05 Total months of Medicaid eligibility -.13 -.06 -0.07
Charlson Index score -.02 .06 0.05 *p = .05, **p = .01, ***p = .001 n/a – no beneficiaries in the category
In contrast to Hispanics, beneficiaries categorized as “Other” were significantly less likely to be admitted to a nursing facility. This finding parallels results presented earlier (see Table 12). While the variance accounted for is less than 2%, these results once again emphasize the need to clarify who is classified as “Other” in the Medicaid data for “race.” The only other potential risk factors that were associated with admission were found in the mental health category. Mental health indicators were significant risk factor for the Mixed Group, and for the combined sample (which is primarily composed of members of the Mixed Group). Both the presence of a major psychotic disorder for which treatment has been received, and being “Baker acted” were associated with a higher probability of being admitted to a nursing facility. Subanalyses were next conducted on the Baker Act data set. Results indicated that a total of only 10 beneficiaries were subjected to Baker Act proceedings. Of those 10, five were admitted to a nursing home. Of those five, two had Baker Act examinations prior to being admitted to the nursing home, one had the Baker Act examination around the time of nursing home admission, and two had the examinations after being admitted to a nursing home. The ambiguity in timing results from the fact that the date of admission to a nursing home in the Medicaid file is a 'header date' and is always the first day of the month in which a person was admitted. Therefore it is difficult to conclude from the present data set whether individuals who had a Baker Act on the 1st or 2nd day of the month they were admitted to a nursing home actually had been admitted just before or just after the examination. Interestingly, and consistent with their generally greater frequency of mental health diagnoses, all beneficiaries were from the 'mixed' group. There were no Baker Act examinations among beneficiaries in the ADW Group.
Discussion and Policy Implications Three research questions guided the analyses presented above. The first question was “What are the characteristics of Medicaid beneficiaries with Alzheimer’s disease who participate in the Aged and Disabled Medicaid waiver program, as compared with AD beneficiaries of similar age who are not so enrolled.” Our analyses indicated that in terms of age, gender distribution, and physical health co-morbidities (as measured by the Charlson Index), beneficiaries in the two groups were not significantly different. From a policy point of view this made the lack of difference in Medicaid-eligible days in community and days in nursing facility more interesting. That is because one might assume that the services received by beneficiaries in the ADW Group would have increased their chances of staying in the community.
41

Where the two groups did differ was in their racial/ethnic composition, and in mental health status. The ADW group had significantly more African American beneficiaries than did the Mixed Group. This suggests that members of this one ethnic minority were not being denied access to the Aged and Disabled waiver program. Similarly, while the Mixed Group had fewer African Americans, a surprisingly high 45% had been categorized as “Other” on the race variable. There is some evidence (Chen, 2005) that at least a third of those categorized as "Other" in the Medicaid race variable self-identify as Black. If this were the case in the present instance, both groups would have substantial numbers of Black beneficiaries. The need for more information about AD beneficiaries from diverse backgrounds can be seen by the overall ethnic minority composition of the combined sample. Only approximately 35% of the entire sample consisted of beneficiaries were identified as White; 11.4% were identified as Black, 10.3% as Hispanic, and 42.8% as Other. The bottom line is that Medicaid beneficiaries with a diagnosis of AD are more likely to be non-White than White. This finding emphasizes the need for cultural competence on the part of all providers. With regard to mental health characteristics, the results clearly indicate that beneficiaries in the ADW Group were much less likely than those in the larger, Mixed Group to have a mental health diagnosis. The reasons for this difference are unclear, since the criteria for enrollment in the ADW program do not include mental health disorders as exclusionary. Combined with the correlations indicating that mental health problems are risk factors for admission to nursing facilities, these results do suggest that attention be paid to the mental health needs of beneficiaries with AD. The second question was “What are the types and costs of services provided and are they comparable in the two groups?” Somewhat surprisingly, given the higher proportion of beneficiaries from the Mixed Group who had mental health diagnoses, mental health expenditures for the Mixed Group were significantly lower than those for the ADW Group. It is not clear just why this would be the case. Also surprising is that, although the Charlson Index indicated there was no significant difference between the two groups in terms of the presence of physical health problems, health services costs of the ADW Group were substantially and significantly higher than those of the Mixed Group. These latter differences suggest that the ADW Group was receiving more appropriate medical care, a conjecture supported by the fact that not a single emergency room admission was reported for any member of this group. On the other hand, and to iterate an earlier point, the ADW Group did not differ significantly from the Mixed Group in Medicaid days spent in the community. One explanation may be differences in overall vulnerability: enrollees in the ADW program must meet level of care standards appropriate for admission to a nursing facility. It should also be recalled that the variable assessing Medicaid-eligible days in community includes days spent as a hospital inpatient and days in assisted living. A more thorough assessment of trajectories of service utilization would require Medicare administrative files to complement the analyses, as well as surveys of users. The third question addressed in Part Two was “What variations exist by ethnic minority group in overall days in community?” Our results indicate that beneficiaries of Hispanic origin have the fewest Medicaid days in community and that those in the “Other” category spend the most days in community. The unknown, here, is that there was variation in days of Medicaid eligibility, and at present the relationship of Medicaid days spent in community to the actual number of calendar days is unknown. Interestingly, Hispanics were the most likely, in terms of percentages, to be admitted to a nursing facility, and those in the “Other” category were the least likely. These results again reaffirm the need for a better understanding of the differing pathways taken by members of ethnic minority groups as their AD progresses. In addition to research questions, there were two hypotheses. The first hypothesis was that there would be differences across the two study groups in the risk of institutionalization, as measured by
42

Medicaid-eligible days spent in community (as opposed to a nursing facility) and rate of institutionalization. The rationale for the hypothesis was the expectation that sustained participation in a waiver program for aged and/or disabled persons would provide greater benefit to AD beneficiaries than would participation or non-participation in a variety of other programs. This hypothesis was disproved. Despite the fact that all members of the ADW Group were participants in the Aged and Disabled Waiver Program for six months or longer during the study year, there was no evidence of any systematic difference in risk of institutionalization. The ADW Group’s greater costs for physical health services, when compared to the Mixed Group, does suggest that possibly the physical health needs of the ADW Group were not only higher but also were receiving appropriate attention. Again it should be pointed out that the criteria for participation in the ADW program include that the beneficiary meet the level of care requirements for long term care. In other words, it is possible that the services made available by the ADW program allowed participating beneficiaries to remain in the community longer than they might normally have been able to. One intriguing finding emerged when the correlates of admission to a nursing facility were examined. Two indicators of mental health problems, the presence of a major psychotic disorder and a Baker Act exam, were significantly associated with admission to a nursing facility in the Mixed Group and in the combined sample. These correlations, coupled with the finding (see also Part Three of this report) that overall use of cognate drugs was relatively low for beneficiaries with an existing diagnosis of Alzheimer’s disease, underscore the need for medication review and appropriate use of the existing, established cognate medications. The findings also emphasize the need for attention to the mental health of beneficiaries with Alzheimer’s disease. As a corollary to the first hypothesis, it was also anticipated that race and ethnic group status would be associated with a reduced risk of institutionalization. The rationale for this hypothesis was the disproportionately low prevalence of ethnic minority group residents in nursing facilities. This hypothesis corollary was only partially confirmed, if at all. Members of the “Other” category of the Medicaid race variable were indeed less likely to be institutionalized, and spent fewer Medicaid-eligible days in a nursing facility. However, approximately 23% of the Hispanics in the combined sample were placed in a nursing facility during the year in question. Looking at correlations of the various socio-demographic characteristics, for the combined sample, Hispanics were indicated to have a slightly—but still significant—greater chance of being admitted, and those in the “Other” category had a slightly lower chance than others of being admitted. These results suggest the need to further examine the trajectories to nursing homes followed by members of the several ethnic minority categories. The second hypothesis was that there would be significant variations across racial and ethnic groups in the overall number of Medicaid-eligible days spent in community. Here the rationale was that since Blacks and Hispanics are under-represented in nursing home populations, they should spend more days in the community. Results were equivocal. Hispanics spent the fewest Medicaid-eligible days in community, and members of the “Other” category spent the most. As a final comment, days in community represents a principal focus of the Alzheimer’s disease Medicaid waiver program, and is a corresponding focus of the evaluation team. In this report there could be no cost-effectiveness comparison of the relatively full package of services to be provided under waiver auspices. The report does however consider some general issues, and also examines racial and ethnic differences in days spent in community, with ambiguous results. For example, the generally better outcomes of the “Other” group identified by the race variable demonstrates the importance both of developing more effective codes for race and ethnicity (possibly using the U.S. Census survey tool as a starting point), but also of developing triangulation schemas in order to more
43

accurately classify all respondents on the basis of existing data. The results also emphasize the need to look more fully at the general area of race and ethnicity.
Evaluation Study Limitations A primary limitation of this evaluation has been the relatively small number of beneficiaries included, especially for the mandated ADW Group. The sample size not only restricts the depth of analysis possible, but also makes it clear that in future investigations of the efficacy of the Alzheimer’s disease waiver program, it will once again not be possible to restrict comparison group membership to beneficiaries resident in the four counties covered by the waiver. Another limitation was the lack of information concerning the characteristics of beneficiaries who were categorized as “Other” in what is called the “race” variable in the Medicaid data set. Nearly 43% of the entire sample of beneficiaries with AD fell into this miscellaneous category, with the majority (n = 177) being members of the Mixed Group of beneficiaries. “Race” in fact is a misnomer, since individuals of Hispanic origin represent an ethnic component of the “White” category, rather than a component of what is traditionally viewed as race. The U.S. Census Bureau and other collectors of large data sets have for years differentiated ethnicity from race. The Census Bureau, like many others, includes a separate question dealing with whether respondents view themselves as Hispanic or not. The Census Bureau, in its year 2000 questionnaire, also allows the individual to indicate membership in more than one specific ethnic and racial grouping, in recognition of the increasing presence of multicultural respondents. Finally, restriction of analyses to Medicaid data may have led to an under-estimation of overall beneficiary costs to Florida. This is because services paid through Florida’s general revenue funds were not included. For example, costs arising out of the Alzheimer’s Disease Initiative (ADI), Community Care for the Elderly (CCE), and Home Care for the Elderly (HCE) are not included in Medicaid data.
Part Three: Drug Issues in Care of Beneficiaries with Alzheimer’s Disease This section of the report deals specifically with the fourth research question guiding the analyses: What role do medications play in the progression towards institutionalization?
Context of the Investigation of Drug Issues This study of psychotropic prescribing practices and outcomes for elders with Alzheimer’s disease (AD) and/or cognate therapy is a sub-study of the independent AD Waiver Evaluation. The AD Waiver Evaluation will investigate whether or not the 1915 (b) home and community-based services (HCBS) waiver program is successful in providing quality services to older Medicaid recipients with AD in a cost effective and budget neutral manner, and in meeting its stated goal of allowing beneficiaries to remain at home longer than they would without AD Waiver Program services. The objective of this preliminary descriptive study of older Medicaid recipients is to support the independent AD Waiver Evaluation by gathering historical information on an important subset of the population targeted in the AD Waiver Program, namely, elders with AD, who may have mental illness or behavioral and psychological symptoms of dementia (BPSD), and who are or are not taking cognate medications. Specifically, this sub-study examines and compares demographic characteristics, psychotropic prescribing practices, Medicaid expenditures, the rate of nursing home admission, and time to nursing home placement for older Medicaid recipients with AD with or without cognate therapy. By providing information on key outcomes associated with the “newer” cognate and
44

psychotropic medications provided to older Medicaid recipients with AD, results from the current study will contribute to the independent AD Waiver evaluation and to the AD Waiver Program.
Need for Research In light of the urgent need to control Medicare and Medicaid costs, an important priority must be the determination of the costs and benefits of new and expensive medications provided to Medicaid enrollees. If cognate therapy and provision of the “newer” more expensive psychotropic medications have a positive effect on community tenure and delay nursing home placement, reduce non-pharmacy healthcare costs or decrease the need for institutionalization among Medicaid enrollees, then their benefits might well exceed their costs. Development of evidence-based guidelines and sound pharmacy policy for treating Medicaid enrollees with AD, mental illness and/or BPSD receiving standard community services, or AD Waiver Program services, will require increased knowledge of the cost-benefits of the “newer” cognate medications and psychotropic medications. The present study results will contribute to this needed knowledge, by providing information on the demographic characteristics and current Medicaid expenditures for this target population when living in the community.
Specific Aims The Primary Aim of this study was to examine psychotropic prescribing practices and associated outcomes for older Medicaid recipients with AD and BPSD.
Study Questions The following initial questions directed the current study:
1) What are the demographic and diagnostic characteristics of Medicaid beneficiaries over the age of 60 who have AD, mental illness and/ or BPSD? How do the characteristics of elders receiving “newer “vs. “older” antipsychotic and antidepressant medications compare?
2) When compared to elders receiving older psychotropic medication, do elders receiving
“newer” antipsychotic and/or antidepressant medication have a lower rate of nursing home admission, or increased time to nursing home admission?
3) Is the provision of “newer” antipsychotic and/or antidepressant medication and cognate
therapy for older Medicaid beneficiaries with AD associated with reduced non-pharmacy healthcare service use and costs? Specifically, does provision of these “newer” medication decrease emergency room (ER) visits, hospitalizations, mental health service use or use of psychotropic drugs?
4) Do elders with AD, mental illness and/or BPSD who receive “newer” antipsychotic or
antidepressant medication have fewer involuntary psychiatric or Baker Act (BA) examinations?
Hypotheses The Primary Hypothesis was that provision of “newer” antipsychotic and/or antidepressant medication will decrease healthcare service utilization and total Medicaid expenditures, the rate of nursing home placement, and the time to nursing home placement for individuals with a diagnosis of AD, mental illness and/or BPSD.
45

Specific Hypotheses: included the following: Hypothesis 1: The prevalence of diagnosed AD will increase with age. Hypothesis 2: Provision of “newer” antipsychotic and/or antidepressant medication for
persons with AD, mental illness and/or BPSD will reduce utilization of emergency services (ER), hospital services, MH services, psychotropic drugs and the associated Medicaid expenditures for these services.
Hypothesis 3: Provision of “newer” antipsychotic and/or antidepressant medication will be associated with reduced risk of nursing home admission and increased time to nursing home placement.
Hypothesis 4: There will be an inverse relationship between the provision of “newer” antipsychotic and/or antidepressant medication, and the frequency of BA examination.
Methods and Data Sets The data used in this study come from the following administrative data sets:
FY 2002–2003 Florida Medicaid data files, which include information on Medicaid eligibility and claims for medical, institutional, and pharmacy services.
The Baker Act data file, which includes information on involuntary civil commitments in Florida.
Sample The sample consisted of all Medicaid recipients in FY02–2003 who were 60 years of age or older, and were diagnosed with AD, or as being in the “pre-clinical” stage of AD and as a result receiving cognate therapy. Adults who received cognate drug therapy were identified in the pharmacy claims files as receiving one of the following prescription medications: Aricept (donepezil), Reminyl (galantamine), or Exelon (rivastigmine tartrate). Adults who were diagnosed with AD and a mental illness were identified using the ICD-9-CM codes in the Medicaid claims data as shown in Tables 15-16 below.
46

Table 15. Hierarchy of ICD-9-CM Codes for Mental Health Diagnoses
Disorder ICD-9-CM codes and study definition
Major Psychotic Disorder
Anyone with an ICD-9 diagnosis code beginning with 295 (schizophrenia), 297.1 (delusional disorder), 297.3 (shared psychotic disorder), 298.8 (brief psychotic disorder), or 298.9 (psychotic disorder NOS)
Bipolar disorder Anyone without a major psychotic disorder and with an ICD-9 diagnosis code beginning with 296.0, 206.1, 296.4, 296.5, 296.6, 296.7, or 296.8
Major Depressive Disorder
Anyone without a major psychotic disorder, bipolar disorder and with an ICD-9 diagnosis code beginning with 296.2, 296.3, 296.9 & 311
Other Mental Health Diagnoses are categorized as being either ‘mental health’ or ‘physical health’. Subjects who have diagnoses that are categorized as mental health were included in this category.
No Mental Health Diagnosis
Diagnoses are categorized as being either ‘mental health’ or ‘physical health’. Subjects who did not have any diagnoses categorized as mental health were included in this category.
Table 16. Other ICD-9-CM Codes Employed for Classification
Disorder ICD-9-CM codes Alzheimer’s Disease Anyone with an ICD-9 diagnosis code of 331.0
Mental Retardation Anyone with an ICD-9 diagnosis codes 317, 318, 318.0, 318.1, 318.2 or 319
Alcohol Abuse Disorder Anyone with an ICD-9 diagnosis codes beginning with 291, 303, & 305.0 – 305.1
Drug Use Disorder Anyone with an ICD-9 diagnosis code beginning with 292, 304, & 305.2 – 305.9
Results Study Question 1
What are the demographic and diagnostic characteristics of Medicaid beneficiaries over the age of 60 who have AD, mental illness and/or BPSD? How do the characteristics of elders receiving “newer “vs. “Older” antipsychotic and antidepressant medications compare?
To insure that study findings contained complete annual service use and expenditure information, study participants were required to have continuous Medicaid enrollment for the one year of the study. Subjects who received “newer” and “older” antipsychotic drugs were assigned to the “newer” group alone. Therefore, subjects were not counted twice within a drug class. Subjects were counted for each drug class they received. For instance, a subject taking “newer” and “older” antipsychotic drugs and an SSRI antidepressant, were counted in both the “newer” antipsychotic group and in the SSRI group. Summing across totals will not yield 629 subjects since subjects may be included in more than one drug class.
47

Demographic Characteristics The total study sample contained 12, 258 individuals over the age of 60 including 629 elders with a dementia diagnosis and cognate drug therapy, 478 elders with a dementia diagnosis and no cognate drug therapy, and 11,151 elders with cognate drug therapy and no diagnosis of AD.
Age and Sex
i
Study findings revealed that there were only slight and statistically non-significant differences in age between groups. In general, as might be expected given that AD is an age related disease, elders without a diagnosis of AD were younger than those with a diagnosis of AD. Elders who were receiving psychotropic medication and cognate therapy, but did not (yet) have a diagnosis of AD, were the youngest study participants, with a mean age of 77.5 years. Elders with a diagnosis of AD who were not receiving cognate therapy were the oldest study participants, with a mean age of 81.0 years. The data supported our hypothesis that the prevalence of AD would increase with age. Findings revealed that only 4.5 % of older Medicaid recipients with AD were 60–64 years of age and 42.5% of those with a diagnosis of AD were 75–84 years of age (Table 3a). As would be expected in an older Medicaid population, the majority of persons in each and every group were female.
Race/Ethnic ty The majority of participants in this study were non-White. Among participants with a diagnosis of AD, 58.3% with cognate therapy, and 52.1% of those without cognate therapy were non-White. Within the group of participants receiving cognate therapy without a diagnosis of AD 63.7% were non-White.
Mental Health Diagnoses It is noteworthy that in this sample, only a minority of persons receiving cognate therapy had a diagnosis of AD. Only 629 individuals or 5.3% of the 11,780 persons who were receiving cognate therapy had an AD diagnosis documented in the Medicaid administrative data. This finding suggests that the vast majority of older Medicaid recipients receiving cognate therapy for cognitive impairment are in what has been labeled the “pre-clinical” stage of AD. These patients were not formally diagnosed with AD, but are presumed to have the disease. Of the 1,107 study participants with a formal diagnosis of AD, slightly more than half (56.8%), were receiving cognate drugs. With regard to co-occurring mental illness, data show that the majority of elders with AD in this study did not receive a mental health diagnosis. Slightly more than half (65.0%) of persons with an AD diagnosis, and 78.1% of those without an AD diagnosis, had not received a mental health diagnosis. The diagnoses results found here are in keeping with prior studies of older populations, that consistently show rates of diagnosed mental illness under 30% (Antai-Otong, 2005; Bartels, et al., 2000; Brauner, Muir, & Sachs, 2000). As would be expected, the most common mental health diagnosis across all groups was major depressive disorder. Approximately 10.7% of persons with AD and 10.3% of older participants receiving a cognate drug without an AD diagnosis had this diagnosis. No Medicaid recipients in this study had a documented diagnosis in the Medicaid claims data of an alcohol or drug use disorder (Table 17a), this finding is in line with our previous research that found documentation of co-occurring substance use disorders is frequently absent in Florida Medicaid administrative data (Becker, Giard, & Ren, 2004). Due to the underreporting of these disorders in Medicaid data, it is impossible to determine the true frequency of substance use disorders in this study population.
48

With regard to physical health, the age 60+ Medicaid recipients receiving “older” psychotropic medications had the poorest physical health status, as indicated by a higher mean Charlson Index score (Table 17a). The Charlson Index uses ICD-9-CM physical health codes from the Medicaid claims files to weight the severity of 19 major physical illnesses. The Charlson Index is a prospective method for classifying co-occurring physical health conditions that have been shown to alter a person’s risk of morbidity and mortality. It has been extensively researched, and been shown to be a reliable and valid measure of physical health status for use in longitudinal studies using administrative data (Charlson, Pompei, Ales, & MacKenzie, 1987; Deyo, Cherkin & Ciol, 1991; Goldstein, et al., 2004).
Psychotropic Medication Review of the psychotropic medication prescribed for the study population indicates that, in keeping with current “Best Practice “ recommendations, the majority of older Medicaid recipients prescribed psychotropic medication were receiving “newer” antipsychotic and/or antidepressant drugs. Among the 1,107 Medicaid recipients with a diagnosis of dementia, a little more than a half (56.6% /627 persons) received antipsychotic medication. Of those Medicaid recipients with a diagnosis of AD receiving antipsychotic medication most (92.2%/578 elders) were receiving a “newer” or atypical antipsychotic. A little less than half of the AD population (44.5%/493 elders) were prescribed antidepressant medication. Among those elders with an AD diagnosis who were prescribed antidepressant medication very few (5.7%/28 elders) were receiving “older” tricyclic antidepressants. The pattern of psychotropic drug use for older Medicaid recipients talking a cognate drug without an AD diagnosis was quite similar (see Tables 17a and b). The majority (61.3%%/6,832 persons) of the 11,151 persons taking a cognate drug without an AD diagnosis were prescribed psychotropic medication. Among those older Medicaid recipients without an AD diagnosis receiving antipsychotic medication, 88.2% (3,266 persons) were receiving “newer” antipsychotic medications. Among those receiving antidepressant medication, 92.0% (4,846 persons) were receiving newer antidepressant medication (see Table 18a). This use of “newer” psychotropic medication in older Medicaid recipients is in keeping with APA “Best Practice” recommendations (APA, 1997). Among different age cohorts the older are most at risk to adverse consequences from “older” psychotropic medication. Adverse consequences of “older” antipsychotic medication such as TD can be life-threatening in the older, and the anticholinergic properties of the “older” antidepressants are particularly damaging for persons with AD. Demographic information for all Medicaid enrolled study participants that met the study inclusion criteria are presented in Tables 17a, b & 18a, b.
49

Table 17a. Characteristics of Elders with AD and Receiving a Cognate Drug
Characteristic (N = 629)
Atypical Anti-
psychotics (n= 365)
Typical Anti- psychotics
(n = 26)
Newer SSRIs
(n = 309)
Older Tricyclics (n = 12)
Total Sample
(n = 629)
n, (%) n, (%) n, (%) n, (%) n, (%) Age at study entry
60-64 16 (4.4%) 1 (3.9%) 19 (6.2%) 0 (0%) 29 (4.6%)
65-74 67 (18.4%) 4 (15.9%) 68 (22.0%) 2 (16.7%) 122 (19.4%)
75-84 149 (40.8%) 13 (50.0%) 129 (41.8%) 7 (58.3%) 267
(42.5%)
85 and older 133 (36.4%) 8 (30.8%) 93 (30.1%) 3 (25.0%) 211 (33.6)
Mean age 80.5 80.6 79.0 79.6 79.9 Sex
Male 80 (21.9%) 9 (34.6%) 68 (22.0%) 2 (16.7%) 154 (24.5%)
Female 285 (78.1%) 17 (65.4%) 241 (78.0%) 10
(83.3%) 475
(75.5%) Race
White 145 (39.7%) 6 (23.1%) 114 (36.9%) 5 (41.7%) 215
(34.2%)
Non-White 220 (60.3%) 20 (76.9%) 195 (63.1%) 7 (58.3%) 414
(65.8%) MH Diagnosis
Major psychotic 45 (12.3%) 2 (7.7%) 31 (10.0%) 2 (16.7%) 53 (8.4%) Bipolar disorder 6 (1.6%) 1 (3.9%) 7 (2.3%) 0 (0.0%) 7 (1.1%) Depressive disorder 41 (11.2%) 3 (11.5%) 52 (16.8%) 0 (0%) 67
(1.,65%) Other mental disorder 56 (15.3%) 5 (19.2%) 41 (13.3%) 3 (25.0%) 99
(15.7%)
No MH diagnosis 217 (59.5%) 15 (57.7%) 178 (57.6%) 7 (58.3%) 403
(64.1%) Other Problem
Mental retardation 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Baker Act exam 29 (8.0%) 0 (0%) 13 (4.2%) 1 (8.3%) 30 (4.8%) Alcohol use disorder 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Drug use disorder 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) Charlson Score 1.21 1.69 1.23 1.08 1.23 Nursing home admission 66 (18.1%) 2 (7.7%) 51 (16.5%) 1 (8.3%) 87
(13.8%) Mean time to nursing home (Months)
6.6 4.5 6.6 9.0 6.7
50

Table 17b. Characteristics of Elders With AD Not Taking a Cognate Drug
Descriptive Characteristic
Atypical Anti-psychotics ( n = 213)
Typical Anti-
psychotic ( n = 23)
SSRI ( n = 156)
Tricyclic Anti-depressant
( n = 16)
Total Sample
( N = 478)
n, (%) n, (%) n, (%) n, (%) n, (%) Age at study entry
60-64 12 (5.6%) 1 (4.4%) 5 (3.2%) 3 (18.8%) 20 (4.2%)
65-74 49 (23.0%) 3 (13.0%) 35 (22.4%) 4 (25.0%) 82 (17.2%)
75-84 84 (39.4%) 7 (30.4%) 67 (43.0%) 3 (18.8%) 177
(37.0%)
85 and older 68 (31.9%) 12 (52.7%) 49 (31.4%) 6 (37.5%) 199
(41.6%) Mean age 78.9 83.1 79.3 76.4 81.0
Sex
Male 58 (27.2%) 1 (4.4%) 39 (25.0%) 3 (18.8%) 103
(21.6%)
Female 155 (72.7%) 22 (95.7%) 117 (75.0%) 13 (81.3%) 375
(78.5%) Race
White 110 (51.6%) 10 (43.5%) 79 (50.6%) 9 (56.3%) 229
(47.9%)
Non-White 103 (48.4%) 13 (56.5%) 77 (49.4%) 7 (43.8%) 249
(52.1%) MH Diagnosis
Major psychotic 50 (23.5%) 1 (4.4%) 31 (19.9%) 1 (6.3%) 59 (12.3%)
Bipolar disorder 2 (0.9%) 0 (0%) 3 (1.9%) 0 (0%) 3 (0.6%) Depressive disorder 20 (9.4%) 1 (4.4%) 15
(9.6%) 2 (12.5%) 33 (6.9%)
Other mental disorder 30 (14.1%) 3 (13.0%) 24
(15.4%) 2 (12.5%) 67 (14.0%)
No MH diagnosis 111 (52.1%) 18 (78.3%) 83
(53.2%) 11 (68.8%) 316 (66.1%)
Other Problem Mental retardation 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Baker Act exam 14 (6.6%) 0 (0%) 6 (3.9%) 1 (6.3%) 15 (3.1%) Alcohol use disorder 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Drug use disorder 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Charlson Score 1.42 1.04 1.42 1.37 1.29 Nursing home admission 28 (13.2%) 3 (13.0%) 23
(14.7%) 3 (18.8%) 56 (11.7%)
Mean time to nursing home (mo.s)
5.4 7.5 5.6 3.8 5.4
51

Table 18a. Characteristics of Elders Without AD Receiving Psychotropic and Cognate Drugs
Descriptive Characteristic Atypical Anti-
Psychotic (n= 3,266)
Typical Anti-Psychotic (n = 435)
SSRI (n =
4,846)
Tricyclic Anti-depressant (N = 422)
n, (%) n, (%) n, (%) n, (%) Age at study entry
60-64 235 (7.2%) 26 (6.0%) 301 (6.2%) 15 (3.6%)
65-74 950 (29.1%) 134 (30.8%) 1,533 (31.6%) 134 (31.8%)
75-84 1,246 (38.2%) 170 (39.1%) 2,031 (41.9%) 172 (40.8%)
85 and older 835 (25.6%) 105 (24.1%) 981 (20.2%) 101 (23.9%)
Mean age 77.5 77.5 76.8 77.5 Sex
Male 851 (26.1%) 95 (21.8%) 1,059 (21.9%) 76 (18.0%)
Female 2,415 (73.9%) 340 (78.2%) 3,787 (78.2%) 346 (82.0%)
Race
White 1,270 (38.9%) 187 (43.0%) 1,720 (35.5%) 177 (41.9%)
Non-White 1,996 (61.1%) 248 (57.0%) 3,126 (64.5%) 245 (58.1%)
MH Diagnosis
Major psychotic 367 (11.4%) 22 (5.1%) 266 (5.5%) 14 (3.3%)
Bipolar disorder 87 (2.7%) 5 (1.2%) 72 (1.5%) 3 (0.7%)
Depressive disorder 550 (16.8%) 38 (8.7%) 833 (17.2%) 42 (10.0%)
Other mental disorder 291 (8.9%) 32 (7.4%) 342 (7.1%) 39 (9.2%)
No MH diagnosis 1,971 (60.4%) 338 (77.7%) 3,333 (68.8%) 324 (76.8%)
Other Problem Mental retardation 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Baker Act exam 168 (5.1%) 1 (0.2%) 108 (2.2%) 3 (0.7%)
Alcohol use disorder 1 (0%) 0 (0%) 1 (0%) 0 (0%) Drug use disorder 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Other (Charlson Score) 0.42 0.43 0.38 0.32
Nursing home admission 440 (13.5%) 47 (10.8%) 399 (8.2%) 27 (6.4%)
Mean time to nursing Home (Months) 6.8 5.6 7.0 7.2
52

Table 18b. Characteristics of Elders Without AD Receiving Cognate Drugs
Characteristic 1 Cognate
Drug (n = 4,035)
>1 Cognate Drugs
(n = 284)
Cognate Drug & Psychotropics (n = 6,832)
Total Sample
(N = 11,151)
n, (%) n, (%) n, (%) n, (%) Age at study entry
60-64 103 (2.6%) 3 (1.1%) 392 (5.7%) 498 (4.5%)
65-74 1,079 (26.7%) 68 (23.9%) 2,067 (30.3%) 3,214 (28.8%)
75-84 1,796 (44.5%) 139 (48.9%) 2,808 (41.1%) 4,743 (42.5%)
85 and older 1,057 (26.2%) 74 (26.1%) 1,565 (22.9%) 2,696 (24.2%)
Mean age 78.7 79.2 77.3 77.89 Sex
Male 1,176 (29.1%) 62 (21.8%) 1,588 (23.2%) 2,826 (25.3%)
Female 2,859 (70.9%) 222 (78.2%) 5,244 (76.8%) 8,325 (74.7%)
Race
White 1,421 (35.2%) 96 (33.8%) 2,533 (37.1%) 4,050 (36.3%)
Non-White 2,614 (64.8%) 188 (66.2%) 4,299 (62.9%) 7,101 (63.7%)
MH Diagnosis Major psychotic 25 (0.6%) 3 (1.1%) 422 (6.2%) 450 (7.0%)
Bipolar disorder 8 (0.2%) 1 (0.4%) 105 (1.5%) 114 (1.02%)
Depressive disorder 126 (3.1%) 12 (4.2%) 1,011 (14.8%) 1,149 (10.3%)
Other mental disorder 178 (4.4%) 21 (7.4%) 534 (7.8%) 733 (6.6%)
No MH diagnosis 3,698 (91.7%) 247 (87.0%) 4,760 (69.7%) 8,705 (78.1%)
Other Problem Mental retardation 0 (0%) 0 (0%) 0 (0%) 0 (0%) Baker Act exam 6 (0.2%) 1 (0.4%) 182 (2.7%) 189 (1.7%) Alcohol use disorder 1 (0.02%) 0 (0%) 1 (0.01%) 2 (0.02%)
Drug use disorder 0 (0%) 0 (0%) 0 (0%) 0 (0%) Other (Charlson Score) 0.25 0.23 0.38 0.33 Nursing home admission 182 (4.5%) 13 (4.6%) 649 (9.5%) 844 (7.6%)
Mean time to nursing home (mo.s) 6.7 7.0 6.8 6.8
53

Study Question 2 When compared to elders receiving older psychotropic medication do elders receiving
“newer” antipsychotic and/or antidepressant medication have a lower rate of nursing home admission or increased time to nursing home admission?
Nursing Home Admission and Time to Nursing Home Placement Data in Tables 17a and b show that 87 elders (13.8%) with a diagnosis of AD who were receiving cognate therapy and 56 elders (11.7%) with an AD diagnosis not receiving cognate therapy were placed in a nursing home during the study year. On average, Medicaid recipients with a diagnosis of AD who were receiving cognate medication remained in the community for 6.7 months, while those recipients with an AD diagnosis not receiving a cognate medication were (on average) admitted to a nursing home in 5.4 months. Among Medicaid recipients with a diagnosis of AD who were also receiving psychotropic medication, those receiving antipsychotic medication had the highest rate (17.4%) of nursing admission and shortest length of community tenure. This was followed by elders receiving antidepressant medication, who had an admission rate of 16.1% (see Tables 17a and 17b). These findings are consistent with existing studies that have shown mental illness and BPSD are risk factors for nursing home admission. Due to the small number of elders who were receiving “older” psychotropic medication in this study, we are unable to determine if persons taking “older” psychotropic medication were at increased risk for nursing home admission or shortened community tenure, compared to study participants taking “newer" medications. As would be expected, Medicaid recipients who did not have a formal AD diagnosis and were presumably in the “pre-clinical” or mild stage of cognitive impairment had (on average) the lowest rate of nursing home admission (7.6%) and longest stay in the community (6.8) months. These findings are consistent with our recently completed study of the costs and benefits of cognate therapy for persons with AD. Our previous five-year study of older Medicaid recipients showed that older persons with a diagnosis of AD or other dementia who received cognate therapy remained in the community an average of 483 days out of 36 months, or 100 days longer than persons with a diagnosis of AD or other dementia who were not taking a cognate drug. This group also had lower non-pharmacy healthcare costs. Thus there is some evidence that providing cognate medications to elders with a formal diagnosis of AD has the potential to reduce Medicaid expenditures and increase community tenure (Becker, et al., 2005). Previous study results showed that individuals in the dementia only group (without cognate therapy) were at greatest risk for nursing home placement during the first four months of that study’s follow-up time period. Medicaid recipients in the dementia & cognate drug group were at the greatest risk for nursing home placement between the 30th and 32nd month, and individuals in the matched comparison group (without an AD diagnosis or cognate therapy) had a relatively constant risk of nursing home placement over time (Becker et al., 2005) (Figure 1).
54

Figure 1. Conditional Probability of Nursing Home Admission
0%
1%
2%
3%
4%
5%
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Months
Perc
enta
ge
Dementia+Cognate Dementia Only Cognate Only Matched Comparison
55

Study Question 3 Is the provision of “newer” antipsychotic and/or antidepressant medication and cognate
therapy for older Medicaid beneficiaries with AD associated with reduced non-pharmacy healthcare service use and costs? Specifically, does provision of these “newer” medication decrease emergency room (ER) visits, hospitalizations, mental health service use or use of psychotropic drugs?
Table 19 provides information on the service categories and Catcaid codes used in this study. These are the same categories used in Part Two of this report.
Table 19. Service Categories and Catcaid Codes
Category Description Catcaid codes used to define service category Inpatient behavior health service use 01.00, 01.50, 03.00, 03.50
Emergency room service 04.00
Outpatient (BH) treatment 04.50, 05.00, 05.25, 05.50, 08.00, 10.00, 18.00, 20.00, 20.10, 20.20, 20.30, 20.40
Day treatment(partial hospitalization 01.20, 03.20, 12.00
Case management services 06.00, 07.00, 07.50, 13.00
Total behavioral health < 50.00 Total physical health expenditures > = 50.00
Psychotropic drug expenditures Brand(generic name (NDC Codes)
Cognate drug expenditures Brand(generic name (NDC Codes)
Other pharmacy expenditures Brand(generic name (NDC Codes)
Total pharmacy expenditures All Medicaid Expenditures
Total expenditures All Medicaid Expenditures
56

Tables 20a, b, & c present FY 2002–2003 Medicaid expenditure data for all Medicaid recipients in the study receiving cognate therapy. The results show that among elders receiving cognate medications, the least costly Medicaid recipients were those who were not also receiving psychotropic medication, and presumably not experiencing a mental illness or BPSD. Total per user per month (PUPM) Medicaid expenditures for persons receiving cognate medications for this group were $516.83, compared to $863.97 PUPM for elders with cognate therapy and “newer” psychotropic medications, and $752.37 for elders receiving less expensive “older” psychotropic medications.
Table 20a. Medicaid Expenditures for Elders Receiving Cognate Therapy & No Psychotropics (N = 4,366)
Service Type PUPM Users Annual penetration
Annual Expenditures
Inpatient mental health $120.19 22 0.50% $26,471.27 Emergency room service $6.21 11 0.25% $728.62
Outpatient treatment $26.19 306 7.01% $88,833.57 Day treatment $253.25 12 0.28% $34,614.28 Case management services $30.56 72 1.65% $25,299.77
Total mental health $45.88 348 7.97% $175,947.51 Total physical health $272.84 3,823 87.56% $11,392,871.65 Psychotropic drug expenditures NA NA NA NA
Cognate drug expenditures $62.78 4,366 100% $3,010,044.72
Other pharmacy expenditures $214.39 4,307 98.65% $10,501,203.47
Total pharmacy expenditures $274.27 4,366 100% $13,511,248.19
Total expenditures $516.83 4,366 100% $25,080,067.35 The comparatively lower Medicaid expenditures for persons receiving cognate medication and no psychotropic medication are reflective of the lower mental health service expenditures and lower pharmacy service expenditures incurred by this group.
Table 20b. Medicaid Expenditures for Elders Receiving a Cognate Drug and “Newer” Psychotropic Medication (N = 6,484)
Service Type PUPM Users Annual penetration Annual total cost
Inpatient mental health $402.40 156 2.41% $734,304.44
Emergency room service $6.40 131 2.02% $8,407.12
Outpatient treatment $47.67 1,672 25.79% $895,345.03
Day treatment $148.33 134 2.07% $230,592.54 Case management services $62.82 664 10.24% $482,630.91
Total mental health $102.97 1,990 30.69% $2,351,280.04 Total physical $413.05 6,023 92.89% $27,616,125.97
57

health Psychotropic drug expenditures 110.40 6,484 100% $8,079,187.28
Cognate drug expenditures $70.05 6,484 100% $5,103,498.96
Other pharmacy expenditures $270.26 6,435 99.24% $19,935,090.14
Total pharmacy expenditures $448.68 6,484 100% $33,117,776.38
Total expenditures $863.97 6,484 100% $63,085,182.39 Medicaid recipients age 60 and over receiving cognate therapy and “newer” psychotropic medications incurred the highest PUPM total costs ($863.97) of any group in this study. This observed higher total expenditure for the group reflected the fact that older participants receiving “newer” psychotropic medications and cognate therapy not only had higher psychotropic drug costs than Medicaid recipients receiving cognate therapy and “older” psychotropic medications ($110.40 vs. $4.79 PUPM, respectively), but they had higher mental health, physical health, and inpatient mental health service expenditures as well. Thus, our hypothesis that provision of “newer” psychotropic medication would be associated with lower non-pharmacy service costs were not supported by the findings in this study (Tables 20b and c).
Table 20c. Medicaid Expenditures for Elders Receiving a Cognate Drug and “Older” Psychotropic Medication (N = 542)
Service Type PUPM Users Annual penetration Annual total cost
Inpatient mental health $263.96 5 0.92% $15,596.62 Emergency room service $6.54 4 0.74% $313.80
Outpatient treatment $27.32 77 14.21% $20,953.57 Day treatment $323.83 1 0.19% $3,886.00 Case management services $39.80 25 4.61% $11,628.19
Total mental health $53.58 89 16.42% $52,378.18 Total physical health $426.85 497 91.70% $1,795,091.46 Psychotropic drug expenditures $4.79 542 100% $29,967.19
Cognate drug expenditures $67.13 542 100% $415,217.65
Other pharmacy expenditures $281.27 540 99.63% $1,755,033.75
Total pharmacy expenditures $352.16 542 100% $2,200,218.59
Total expenditures $752.37 542 100% $4,047,688.23
Study Question 4 Do elders with AD, mental illness and/or BPRS who receive “newer” antipsychotic and/or
antidepressant medication have fewer involuntary psychiatric or Baker Act (BA) examinations?
58

An involuntary psychiatric (BA) examination can be initiated by a mental health professional, law enforcement official or a judge. Evidence that an individual has a mental illness, and that the likelihood of harm to self, harm to others and/or self-neglect is present, is required to initiate an involuntary psychiatric examination. The findings did not support our hypothesis that there would be an inverse relationship between provision of “newer” psychotropic medication and the incidence of a BA examination. The study data show that older Medicaid recipients with a diagnosis of AD who were receiving “older” psychotropic medications had no BA examinations within the study year, but 43 older participants (7.4%) with AD who were receiving “newer” antipsychotic medication had at least one BA examination during FY 2002–2003.
Study Limitations There are a number of limitations associated with these analyses. First, the study contains no information on illness severity and relies solely on Medicaid administrative fee-for-service data and Baker Act data. Limitations inherent in the use of administrative data stem from the fact that record keeping is imperfect, data contain coding errors and may be incomplete, and lags occur in the data entry process. A limitation of the service use and expenditure data reported in this study is that it does not include out-of-pocket costs or private pay services, and hence, true mental and physical health service costs are underestimated. In this report the Medicaid expenditures and benefits of the drugs studied here are underestimated due to the fact that we did not have access to nursing home data. By analyzing all three cognate drugs and all “newer” psychotropic medications together we cannot generalize the study findings to specific individual drugs. Lastly, while this descriptive study provides useful historical demographic and expenditure data on older Medicaid recipients with a diagnosis of AD, additional studies that include a more sophisticated multivariate design that controls for relevant co-variates and includes nursing home expenditures are clearly needed. Such studies could provide important additional information on current costs and benefits of services provided for the AD Waiver Program's intended target population.
Discussion and Policy Implications Kitchener, Ng, Miller, & Harrington (2005) reviewed the cost-effectiveness of home-and community based long-term care services (HCBS), and suggested that since most states are expanding HCBS services, policy makers and researchers should focus on improving the efficiency and outcomes of those services. However, in order to improve and/or evaluate on the efficiency of Medicaid-funded HCBS to elders living in Florida, historical information is needed on the existing costs and outcomes of specific services. This preliminary descriptive study of characteristics and expenditures for Medicaid recipients with a diagnosis of AD and/or who are receiving cognate therapy showed that contrary to expectations, older Medicaid recipients receiving cognate therapy and “newer” more expensive psychotropic medications had increased average PUPM Medicaid expenditures, including the average expenditures for pharmacy, mental health, physical health, and inpatient mental health services. In addition, elders receiving the newer, more expensive psychotropic drugs had an increased number of BA examinations and mental health hospitalizations. Thus, in this descriptive study there was no evidence that provision of these more expensive drugs resulted in improved outcomes for the study population. The reasons behind the increased non-pharmacy expenditures for older participants receiving “newer” psychotropic drugs are not known and beyond the scope of this study. However, it is possible that elders receiving “newer” atypical antipsychotic medication were treatment-resistant patients with more severe mental illnesses that were switched from “older” medications due to their treatment difficulties.
59

Expenditure data also show that within the population of Medicaid elders receiving cognate therapy, those who were receiving psychotropic medication used more services, at greater cost to Medicaid. In conclusion, this study’s results indicate that sub-groups within the community-dwelling Medicaid elder population examined herein had disparate expenditure outcomes, rates of nursing home admission and time to nursing home placement. Taken together, these data suggest that any future evaluation of the cost neutrality of Florida’s AD Waiver Program must evaluate sub-groups within the population separately to determine the costs and benefits of future AD Waiver Program services provided.
60

References Adams, B., Aranda, M., Kemp, B., & Takagi, K. (2002). Ethnic and gender differences in distress among Anglo American, African American, Japanese American and Mexican American spousal caregivers of persons with dementia. Journal of Clinical Geropsychology, 8, 279–301. Administration on Aging. (2005). A Profile of Older Americans: 2004. Washington, DC: Department of Health and Human Services. Last updated May 2, 2005. Accessed June 10, 2005 at http://www.aoa.gov/prof/Statistics/profile/2004/profiles2004.asp Agency for Health Care Administration. (2004). Alzheimer’s Disease Medicaid Waiver Program. State of Florida Request for Proposal. Tallahassee, FL: Author. Albert, S.M., Castillo-Castaneda, C. D., Sano, M., Jacobs, D. M., Marder, K., Bell, K., et al. (1996). Quality of life in patients with Alzheimer’s disease as reported by patient proxies. Journal of the American Geriatrics Society, 44, 1342–1347. Albert, S. M., Sano, M., Marder, K., Jacobs, D. M., Brandt, J., Albert, M., et al. (1997) Participation in clinical trials and long-term outcomes in Alzheimer's disease. Neurology, 49, 38–43. Algase, D. (1992). Wandering: what, why & how? in K. Buckwalter (Ed.), Geriatric Mental Health Nursing: Current and Future Challenges p. 61–74. Thorofare, NJ: Slack Algase, D. (1998) Wandering. In B. Edelstein (Ed.), Comprehensive Clinical Psychology, p. 271–412. London: Pergamon Algase, D. (May, 2005). Wandering: State of the science. Presented at the conference for Evidence-based strategies for patient falls and wandering, Clearwater, Florida. Alker, J. & Portelli, L. (2004). Policy Brief.: Florida’s Medicaid budget: Why are costs going up? Winter Park, FL: Winter Park Health Foundation. Alloul K., Saurial L., & Kennedy W. (1998). Alzheimer’s disease: A review of the disease, its epidemiology and economic impact. Archives of Gerontology and Geriatrics, 27, 189–221. Alzheimer's Association. (2004). Statistics about Alzheimer's Disease. Retrieved January 1, 2005, from http://www.alz.org/AboutAD/statistics. American Psychiatric Association. (1997). Practice guidelines for the treatment of patients with Alzheimer’s disease and other dementias of late life. American Journal of Psychiatry, 154, 1–39. American Psychiatric Association. (2003). Diagnostic and Statistical Manual for Mental Disease, (4th rev. ed.). Washington DC.: Author. Antai-Otong, D. (2005). Psychotropic use in older adults. ADVANCE for Nurses, 13–17. Aranda, M. & Knight, B. (1997). The influence of ethnicity and culture on the caregiver stress and coping process: A sociocultural review and analysis. The Gerontologist, 3: 342–354. Ayalan, L. & Arean, P. A. (2004). Knowledge of Alzheimer’s disease in four ethnic groups of older adults. International Journal of Geriatric Psychiatry, 19, 51–57.
61

Balesteri, L., Grossberg, A., & Grossberg, G. ( 2000). Behavioral and psychological symptoms of dementia as a risk factor for nursing home placement. International Psychogeriatrics, 3, 363–366. Balsis, S., Carpenter, B. D., & Storandt, M. (2005). Personality change precedes clinical diagnosis of dementia of the Alzheimer’s type. Journal of Gerontology: Psychological Sciences, 60B (2), P98–P101.
Bartels, S.J. & Christopher C. Colenda, C.C. (1998). Mental Health Services for Alzheimer's Disease Current Trends in Reimbursement and Public Policy, and the Future Under Managed Care. Am J Geriatr Psychiatry, 6:S85-S100. Bartels S. J., Forester B., & Miles K. M. (2000). Mental health service use by elderly patients with bipolar disorder and unipolar major depression. American Journal of Geriatric Psychiatry 8, 160–166. Bartels, S. J., Clark, R. E., Peacock, W. J., Dums, B. A., & Pratt, S. I. (2003). Medicare and Medicaid costs for schizophrenia patients by age cohort compared with costs for depression, dementia, and medically ill patients. American Journal of Geriatric Psychiatry, 11, 648–657. Bartolini, M., Coccia, M., Luzzi, S., Provinciali, L. & Ceravolo, M. G. (2005). Motivational symptoms of depression mask preclinical Alzheimer’s disease in elderly subjects. Dementia and Geriatric Cognitive Disorders, 19, 31–36. Bass, D. M., McClendon, M. J., Deimling, G. T. & Mukherjee, S. (1994). The influence of a diagnosed mental impairment on family caregiver strain. Journal of Gerontology: Social Sciences, 49, S146–S155. Beattie, E. (2005, May). Impact of wandering on patient functional status. Paper presented at the conference for Evidence-based strategies for patient falls and wandering, Clearwater, Florida. Becker, M., Andel, R. & Rohrer, L. (2005). Cost-benefit evaluation of cognate drugs prescribed for Medicaid recipients with Alzheimer’s disease and other dementias. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, Department of Mental Health Law and Policy Becker, M., Giard, J., & Chen, R. (2004). Study of women with co-occurring disorders and lifetime histories of interpersonal trauma. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute Beeri, M. S., Werner, P., Davidson, M. & Noy, S. (2002). The cost of behavioral and psychological symptoms of dementia (BPSD) in community dwelling Alzheimer's disease patients. International Journal of Geriatric Psychiatry, 17, 403–408. Belle, S. H., Zhjang, S., Czaja, S. J., Burns, R. & Schulz, R. (2004). Use of cognitive enhancement medication in persons with Alzheimer disease have a family caregiver; results form the Resources for Enhancing Alzheimer Caregiver health (REACH) project. American Journal of Geriatric Psychiatry, 12, 250–257. Blazer, D., G., Hybels, C. F., Simonsick, E. M., & Hanlon, J. T. (2000). Marked differences in antidepressant use by race in an elderly community sample: 1986–96. American Journal of Psychiatry, 157, 1089–1094. Bloom, B. S., de Pouvourville, N. & Straus, W. L. (2003). Cost of illness of Alzheimer's disease: how useful are current estimates? The Gerontologist, 43, 158–164.
62

Borrayo, E.A., Salmon, J.R., Polivka, L., & Dunlop, B.D. (2002). Utilization across the continuum of long-term care services. Gerontologist, 42, 603-12. Brauner, D. J., Muir, J. C., & Sachs, G. A. (2000). Treating nondementia illnesses in patients with dementia. JAMA, 283, 3230–3235. Brayne, C. (1994). How common are cognitive impairment and dementia? An epidemiological viewpoint. In F. A. Huppert, C. Brayne, & D. W. O’Connor (Eds.), Dementia and normal aging (pp.167–207). New York: Cambridge University Press. Brodaty, H. Green, A., & Koschera, A. (2003). Meta-analysis of psychosocial interventions for caregivers of people with dementia. Journal of the American Geriatrics Society, 51, 657–664. Brodaty, H., Gresham, M., & Luscombe, G (1997). The Prince Henry Hospital dementia caregivers’ training programme. International Journal of Geriatric Psychiatry, 12, 183–192 Brodaty, H., Thomson. C., Thompson, C., & Fine, M. (2005). Why caregivers of people with dementia and memory loss don't use services. International Journal of Geriatric Psychiatry, 20, 537–546. Brookmeyer, R., Gray, S., & Kawas, C. (1998). Projections of Alzheimer’s disease in the United States and the public health impact of delaying disease onset. American Journal of Public Health, 88, 1337–1342. Burns, R., Nichols, L. O., Martindale-Adams, J., Graney, M. J., & Lummus, A. (2003). Primary care interventions for dementia caregivers: 2–year outcomes from the REACH study. The Gerontologist, 43, 547–555. Cancro, R. (1968). Elopements from the C. F. Menninger Memorial Hospital. Bulletin of the Menninger Clin, 32, 228–38. Catterson, M. L., Preskorn, S. H., & Martin, R. L. (1997). Pharmacodynamic and pharmacokinetic considerations in geriatric psychopharmacology. Psychiatric Clinics of North America, 20, 205–218. Center for Personal Assistance Services. (2005). Florida Medicaid 1915(c) HCBS Waivers, 2001. Retrieved May 5, 2005, from http://www.pascenter.org/state_based_stats/medicaid_waiver.php?state=florida#p10.9 Center on an Aging Society. (2005). How do family caregivers fare? Caregivers of Older Persons Data Profile, No. 3, June, 2005. Accessed on June 12, 2005 from http://ihcrp.georgetown.edu/agingsociety/pubhtml/caregiver3/caregiver3.html Charlson, M. E., Pompei, P., Ales, K. L., & MacKenzie, C. R. (1987). A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. Journal of Chronic Disorders, 40, 373–383. Chiriboga, D. A. (in press). Social Supports for the Caregiver: “How Do I Go On?” In S. M. LoboPrabhu, J. W. Lomax, and V. Molinari (Eds.), Caregiving in Dementia: A Guide for Health Care Providers and Caregivers. Baltimore: Johns Hopkins University Press.
63

Chiriboga, D. A., Yee, B. W. K., & Weiler, P. G. (1992) Stress in the Context of Caring. In L. Montada, S.-H. Filipp, and M. Lerner (Eds.), Life Crises and Experiences of Loss in Adulthood. New York: Plenum. Christy, A., Stiles, P., & Shanmugam, S. (2003). The Florida Mental Health Act (The Baker Act): 2002 Annual Report to Florida AHCA. October, 2003. Clark, C. M., DeCarli, C., Mungas, D., Chui, H. I., Higdon, R., Nunez, J, et al. (2005). Earlier onset of Alzheimer disease symptoms in Latino individuals compared with Anglo Individuals. Archives of Neurology, 62, 774–778 Cohen, D. (2000). Caregivers for persons with Alzheimer’s disease. Current Psychiatric Reports, 2, 32–39 Cohen, D. (2004). Behind the looking glass: Dementia caregivers who kill. Journal of Mental Health and Aging, 10, 147-150 Cohen, D. (in press). End of life issues for caregivers of relatives with Alzheimer’s disease. In R. Talley (Ed.), Caregiving and Alzheimer’s Disease. New York: Oxford Press. Cohen D. & Eisdorfer, C. (2001). The loss of self: A family resource for Alzheimer’s disease and related disorders (2nd ed.). New York: W.W. Norton. Cohen, C. A., Gold, D. P., Shulman, K. I., Wortley, J. T., McDonald, G., & Wargon, M. (1993). Factors determining the decision to institutionalize dementing individuals in a prospective study. The Gerontologist, 33, 714–20. Comijs, H. C., Jonker, C., Beekman, A. T., & Deeg, D. J. (2001). The association between depressive symptoms and cognitive decline in community dwelling elderly persons. International Journal of Geriatric Psychiatry, 16, 361–367. Crayton, G. (2004, July). A look at Florida's Medicaid Program. Presentation at the Medicaid Reform Symposium: The Future of Florida Medicaid, Orlando, FL. Cumming, J., Jonker, C., Beekman, A. T., & Deeg Cumming, E, Titus, J., Schmelzle, E. & MacDonald, J. (1982). The episodic nature of behavioral disturbances among residents of facilities for the aged. Canadian Journal of Public Health, 73, 319–322. Cummings, J. L., Frank, J. C., & Cherry, D. (2002). Guidelines for managing Alzheimer’s Disease, part II: treatment. American Family Physician 65, 2525–2534. Deyo, R. A., Cherkin, D. C., & Ciol, M. A. (1991). Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. Journal of Clinical Epidemiology, 45, 613–619. Dwyer, J. W., Barton, A. J., & Vogel, W. B. (1994). Area of Residence and the Risk of Institutionalization. Journal of Gerontology, 49, S75–S84. Elias, M. F., Beiser, A., Wolf, P. A., Au, R. White, R. F., & D’Agostinio, R. B. (2000). The preclinical phase of Alzheimer’s disease: A 22-year prospective study of the Framingham cohort. Archives of Neurology, 57, 808–813. Evans M., Ellis A., Watson D., et al. Sustained cognitive improvement following treatment of Alzheimer’s disease with donepezil. International Journal of Geriatric Psychiatry 15, 50–3.
64

Evans M., & Watson D., (2000). Sustained cognitive improvement following treatment of Alzheimer’s disease with donepezil. International Journal of Geriatric Psychiatry 15, 50–3. Farlow, M. R., Hake, A., Messina, J., Hartman, R., Veach, J. & Anand, R. (2001). Sustained cognitive improvement following treatment of Alzheimer’s disease to rivastigmine treatment is predicted by the rate of disease progression. Archives of Neurology 58, 417–22. Farlow, M. R. & Schneider L. S. (1998). Rivastigmine and response to treatment in different subgroups of patients with Alzheimer’s disease. Neurobiology of Aging, (suppl. 4S), 1264. Fitten, L. J., Ortiz, F. & Ponton, M. (2001). Frequency of Alzheimer’s disease and other dementias in a community-outreach sample of Hispanics. Journal of the American Geriatrics Society, 49, 1301–1308. Flint A. J. (1998). Choosing appropriate antidepressant therapy in the elderly. A risk-benefit assessment of available agents. Drugs and Aging, 13, 269–280. Florida Medicaid Program. (2004). Proposal for a Section 1915(b)(4) initial selective contracting waiver program: Medicaid Alzheimer’s home and community-based waiver program. Agency for Health Care Administration. (November 21, 2003; revised January 30, 2004). Tallahassee: Author. Fompa-Loy, J., (1988). Wandering: causes, consequences, and care. Journal of Psychosocial Nursing & Medical Health Services, 26, 8–11, 15–18. Foxwell, L. (1994). Elopement—Exposure and control. Journal of Long-term Care Administration, 21, 9–12. Friedman, S. M., Steinwachs, D. M., Rathouz, P. J., Burton, L. C., & Mukamel, D. B. (2005). Characteristics predicting nursing home admission in the program of all-inclusive care for elderly people. The Gerontologist 45, 157–166. Gaugler, J. E., Edwards, A. B., Femia, E. E., Zarit, S. H., Stephens, M. A. P., Townsend, A., et al. (2000). Predictors of institutionalization of cognitively impaired elders: Family help and the timing of placement. Journal of Gerontology: Psychological Sciences, 55B, P247–P255. Gauthier, S. (2004). Efficacy of Donepezil on maintenance of activities of daily living in patients with moderate-to-severe Alzheimer’s disease, and impact on caregiver burden. Geriatrics & Aging, 7, 34–36. Gauthier, S., Feldman, H., Hecker, J., Vellas, B., Emir, B., Subbiah, P., et al. (2002). Functional, cognitive and behavioral effects of donepezil in patients with moderate Alzheimer's disease. Current Medical Research and Opinion, 18, 347–54. Gelinas, I., & Auer, S. (2001) Functional autonomy. In S. Gauthier (Ed.), Clinical diagnosis and management of Alzheimer’s disease (pp. 213–26). London: Martin Dunitz. Gelmacher, D., Provenzano G., McRae T., Mastey V., & Ieni J. R. (2003). Donepezil is associated with delayed nursing home placement in patients with Alzheimer’s disease. JAGS, 51, 937–944. Gerdner, L. A., Hall, G. R., & Buckwalter, K. C. (1996). Caregiver training for people with Alzheimer’s based on a stress threshold model. Image: Journal of Nursing Scholar, 28, 241–246.
65

Gold, G., Giannakopoulos, P. & Bouras, C. (2001). Vascular dementia (pp. 131–143). In: P. Hof and C. Mobbs (Eds.), Functional Neurobiology of Aging. San Diego, CA: Academic Press. Goldstein, L. B., Samsa, G. P., Matchar, D. B., & Horner, R. D. (2004). Charlson Index comorbidity adjustment for ischemic stroke outcome studies. Stroke, 35, 1941–1945. Gray, S. L., Lai, K. V. & Larson, E. B. (2000). Drug-induced cognition disorders in the elderly. Drug Safety, 21, 101–122. Gulf Coast Jewish Family Services. (2004). Alzheimer’s Disease Medicaid Wavier Program: To Serve Pinellas County. Clearwater: Author. Gurland, B. J., Wilder, D. E., Lantigua, R., Stern, Y., Chen, J., Killeffer, E. H., et al. (1999). Rates of dementia in three ethnoracial groups. International Journal of Geriatric Psychiatry, 14, 481–493. Gurwitz, J., Sanchez-Cross, M., Eckler, M. & Matulis, J. (1994). The epidemiology of adverse and unexpected events in the long-term care setting. Journal of the American Geriatrics Society, 42, 33–38. Hamid, W. A., Howard, R., & Silverman, M. (1995). Needs assessment in old age psychiatry - a need for standardization. International Journal of Geriatric Psychiatry, 10, 553–554. Hauser, W. A., & Amatniek, J. C. (1998). Gender differences in diseases of the nervous system. In P. W. Kaplan (ed). Neurologic Disease in Women, (pp. 433–442). New York: Demos Medical Publishing Inc. Health Care Financing Administration. (1999). Health Care Financing Review: Medicare and Medicaid Statistical Supplement, 1999. Washington DC: Author. Hebert, L. E., Scherr, P., Bienias, J., Bennett, D. & Evans, D. (2003). Alzheimer's disease in the US population. Archives of Neurology, 60, 1119–1122. Hebert, L. E., Scherr, P., Bienias, J., Bennett, D. & Evans, D. (2004). State-specific projections through 2025 of Alzheimer’s disease prevalence. Neurology, 62, 1645.
Henderson, A. S. & Jorm, A. F. (2002). Definition and epidemiology of dementia a review. In M. Maj and N. Sartorious (Eds.), Dementia (2nd ed.). Chichester,UK: John Wiley. Hendrie, H. C. (1998). Epidemiology of dementia and Alzheimer’s disease. American Journal of Geriatric Psychiatry, 6, S3–S18. Hepburn, K. W., Tornatore, J., Center, B. & Ostwald, S. W. (2001) Dementia family caregiver training: Affecting beliefs about caregiving and caregiver outcomes. Journal of the American Geriatrics Society, 49, 450–457 Heyman, A., Peterson, B., Fillenbaum, G., & Pieper, C. (1997). Predictors of time to institutionalization of patients with Alzheimer’s disease. The CERAD experience, Part XVII. Neurology 48, 1304–1309. Holtzer, R., Tang, M. X., Devanand, D. P., Albert, S. M., Wegesin, D. J., Marder, K., et al. (2003). Psychopathological features in Alzheimer's disease: course and relationship with cognitive status. Journal of the American Geriatrics Society, 51, 953–960.
66

Huang, H., Shyu, Y. L., Chen, M., Chen, S., & Lin, L. (2003). A pilot study on a home-based caregiver training program fro improving caregiver self-efficacy and decreasing the behavioral problems of elders with dementia in Taiwan. International Journal of Geriatric Psychiatry, 18, 337–345. Iliffe, S., & Manthorpe, J. (2004). The debate on ethnicity and dementia: From category fallacy to person-centred care? Aging and Mental Health, 8, 283–92. Jeliz, V., & Winblad, B. (2003) Treatment of mild cognitive impairment: rationale, present future strategies. Acta Neurologia Scandinavia, 107 (Suppl. 179), 83–93. Jeste, D. V., Caligiuri, M. P., Paulsen, J. S., Heaton, R. K., Lacro, J. P., Harris, M. J., et al. (1995). Risk of tardive dyskinesia in older patients: A prospective longitudinal study of 266 outpatients. Archives of General Psychiatry, 52, 756–765. Johnsson, L., Lindgren, P., & Wimo, A. (1999). The cost effectiveness of donepezil therapy in Swedish patients with Alzheimer’s disease: a Markov model. Clinical Therapeutics, 21, 1230–1240. Jorm, A. F., & Jolley, D. (1998). The incidence of dementia: a meta-analysis. Neurology, 51, 728–733. Jorm, A.F. (2000). Is depression a risk factor for dementia or cognitive decline? A review. Gerontology, 46, 219–227. Kane, R. L., Ouslander, J. G., & Abrass, I. B. (2004). Essentials of Clinical Geriatrics (5th Ed). New York: McGraw-Hill. Kawas, C. H. (1999). Alzheimer's Disease. In W. R. Hazzard, J. P. Blass, W. H. Ettinger, J. B Halter, and J. G. Ouslander (Eds.), Principles of Geriatric Medicine and Gerontology, (pp. 1257–1269). New York: McGraw-Hill. Keily, D., Kiel, D., Burrows, A. & Lipsitz, L. (1998). Identifying nursing home residents at risk for falling. Journal of the American Geriatrics Society, 46, 551–555. Khachaturian Z.S. (1997). Plundered memories. Science, 37, 20–25. Kitchener, M., Ng, T., Miller, N. & Harrington, C. (2005). Medicaid home and community-based services: National program trends. Health Affairs, 24, 206–212. Klein, D. A., Steinberg, M., Galik, E., Steele, C., Sheppard, J., Warren, A., et al. (1999). Wandering behavior in community-residing persons with dementia. International Journal of Geriatric Psychiatry, 14, 272–279. Kopetz, S., Steele, C., Brandt, J., Baker, A., Kronberg, M., Galik, E., et al. (2000). Characteristics and outcomes of dementia residents in an assisted living facility. International Journal of Geriatric Psychiatry, 15, 586–593. Lai, C. K. Y. & Arthur, D. G. (2003). Integrative literature reviews and meta-analyses: Wandering behavior in people with dementia. Journal of Advanced Nursing, 44, 173–182. Lam, D., Sewell, M., Bell, G., & Katona, C. (1989). Who needs psychogeriatric continuing care? International Journal of Geriatric Psychiatry, 4, 109–114.
67

Lantz, M. S. (2004). Medications for late-stage Alzheimer’s disease: How should we use them? American Association for Geriatric Psychiatry, 12, 34–37. Mace, N. L., & Rabins, P. V. (2000). The 36-hour day: A family guide to caring for persons with Alzheimer’s disease, related dementing illnesses, and memory loss in later life. Baltimore: Johns Hopkins Press. Malphurs, J. E., & Cohen, D. (2002). A newspaper surveillance study of homicide-suicide in the United States. American Journal of Forensic Medicine and Pathology, 23, 142–148 Marx, M. S., Cohen-Mansfield, J. & Werner, P. (1990) Agitation and falls in institutionalized elderly persons. Journal of Applied Gerontology, 9, 106–17. McShane, R., Gedling, K., Keene, J., Fairborn, C., Jacoby, R., & Hope, T. (1998). Getting lost in dementia: a longitudinal study of a behavioral symptom. International Psychogeriatrics, 10, 253–260. Meaney, A. M., Croke, M., & Kirby, M. (2005). Needs assessment in dementia. International Journal of Geriatric Psychiatry, 20, 322–329. Mehta, K. M., Yaffe, K., & Covinsky, K. E. (2002). Cognitive impairment, depressive symptoms, and functional decline in older people. Journal of the American Geriatric Society 50, 1045–50. Menzin, J., Lang, K., Friedman, M., Neumann, P., & Cumming, J. L. (1999). The economic cost of Alzheimer's disease and related dementias to the California Medicaid program ("Medi-Cal") in 1995. American Journal of Geriatric Psychiatry, 7, 300–308. Miami Jewish Home and Hospital for the Aged. (2004). Alzheimer’s Disease Medicaid Waiver Program. Miami, FL: Author Miller, S. C., Prohaska, T. R., & Furner, S. E. (1999). Nursing home admission for African Americans with Alzheimer’s disease. Journal of Gerontology: Medical Sciences, 54A, M365–M369. Milwain, E. J., & Nagy, Z. (2005). Depressive symptoms increase the likelihood of cognitive impairment in elderly people with subclinical Alzheimer’s pathology. Dementia and Geriatric Cognitive Disorders, 19, 46–50. Mittelman, M. S., Ferris, S. H., Shulman, E., Steinberg, G., & Levin B. (1996). A family intervention to delay nursing home placement of patients with Alzheimer’s disease. A randomized controlled trial. JAMA, 276, 1725–1731. Mittelman, M. S., Roth, D. L., Haley, W. E., & Zarit, S. H. (2004). Effects of a caregiver intervention on negative caregiver appraisals of behavior problems in patients with Alzheimer’s disease: results of a randomized trial. Journal of Gerontology B Psychological and Social Sciences, 59, P27–P34. Moak, G. S. (1990). Characteristics of demented and nondemented geriatric admissions to a state hospital. Hospital and Community Psychiatry, 41, 799–801. Office of Program Policy Analysis and Government Accountability. (2001). OPPAGA Justification Review: Services to Elders Program Department of Elder Affairs. Report No. 01–66. Tallahassee FL: Author.
68

Ory, M. G., Hoffman, R. R. 3rd, Yee, J. L., Tennstedt, S., & Schulz, R (1999). Prevalence and impact of caregiving: a detailed comparison between dementia and nondementia caregivers. The Gerontologist, 39, 177–85. Ostwald, S., Hepburn, K. W., Caron, W., Burns, T., & Mantell, R. (1999). Reducing caregiver burden: A randomized psychoeducational intervention for caregivers of persons with dementia. The Gerontologist, 39, 299–309. Paveza, G. J. Cohen, D., Eisdorfer, C., Freels, S., Semla, T., Ashford, J. W., et al. (1992). Severe family violence and Alzheimer's disease: prevalence and risk factors. Gerontologist, 32, 493–7. Pearlin, L. I., Mullan, J. T., Semple, S. J., & Skaff, M. M. (1990). Caregiving and the stress process: an overview of concepts and their measures. The Gerontologist, 30, 583–594. Raskind, M. A., Peskind, E. R., Wessel, T., & Yuan, W. (2000). Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month Extension. Neurology 54, 2261–2268. Reisberg, B., Franssen, E., Shah, M. A., et al. (2000) Clinical diagnosis of dementia: A Review. In M. Maj and N Sartorius (Eds.), Dementia (pp 69–139). Chichester, UK: John Wiley & Sons Rheaume, Y., Riley, M. E., & Volicer, L. ( 1987) Meeting nutritional needs of Alzheimer patients who pace constantly. Journal of Nutr Elder, 7, 43–52. Ripich, D. N. (1994). Functional communication with AD patients: A caregiver training program. Alzheimer Disease and Associated Disorders, 8(suppl3), 95–109. Ritchie, C. W., Ames, D., Clayton, T., & Lai, R. (2004). Meta-analysis of randomized trials of the efficacy and safety of donepezil, galantamine, and rivastigmine for the treatment of Alzheimer disease. American Journal of Geriatric Psychiatry 12, 358–369. Robinson, K. & Yates, K. (1994). Effects of two caregiver-training programs on burden and attitude toward help. Archives of Psychiatric Nursing, 8, 312–319. Rockwood, K., Stolee, P. & Brahim, A. (1991) Outcomes of admission to a psychogeriatric service. Canadian Journal of Psychiatry, 36, 275–9. Rodriguez, J. (1993) Resident falls and elopements: cost and controls. Nursing Homes, 42, 16–17. Roe, C. M., Anderson, M. J., & Spivack, B. (2002). Use of anticholinergic medications by older adults with dementia. American Geriatrics Society, 50, 836–842. Rosler, M., Anand, R., & Cicin-Sain, A. (1999). Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: international randomized controlled trial. British Medical Journal 318, 633–640. Rowe, M. A. & Glover, J. C. (2001). Antecedents, descriptions, and consequences of wandering in cognitively-impaired adults and the safe return (SR) program. American Journal of Alzheimer's Disease & Other Dementias,16, 344–352. Samuels, S. C., & Davis, K. L. ( 2001). Pharmacological treatment of dementia. In: P. R. Hof and C. V. Mobbs (Eds.), Functional Neurobiology of Aging (pp 131–143). San Diego, CA: Academic Press
69

Sanford, J. (1975). Tolerance of debility in elderly dependants by supporters at home: its significance for hospital practice. British Medical Journal, 3(5981), 471–3. Schneider, L. S. (1990). Meta-analysis of controlled trials of neuroleptic treatment in dementia. Journal of the American Geriatric Society, 38, 553–63. Schneider, L. S., Olin, J. T., & Lyness, S. A. (1997). Eligibility of Alzheimer’s disease clinic patients for clinical trials. Journal of the American Geriatric Society, 45, 923–928. Schulz, R., Vistainer, P., & Williamson, G. M. (1990). Psychiatric and physical morbidity effects of caregiving. Journal of Gerontology, 45, P181–P191. Severson, M. A., Smith, G. E., & Tangalos, E. G., (1994). Patterns and predictors of institutionalization in community-based dementia patients. J American Geriatric Society, 42, 181–185. Small, G. W, McDonnell, D., Brooks, R. & Papadopoulis, G. (2002).The impact of symptom severity on the cost of Alzheimer's disease. Journal of the American Geriatrics Society, 50, 321–327. Small, G. W., Rabins, P. V. & Barry, P. P. (1997). Diagnosis and treatment of Alzheimer’s disease and related disorders. JAMA, 278, 1363–1371. Smothers, H. S., Rust, G., Minor, P., Fresh, E., Druss, B., Satcher, D. (2005). Disparities in antidepressant treatment in Medicaid elderly diagnosed with depression. American Geriatrics Society, 53, 456–461. Snowdon, D. A., Kemper, S. J., Mortimer, J. A., Greiner, L. H., Wikstein, D. R., & Markesbery, W. R. (1996). Linguistic ability in early life and cognitive function and Alzheimer’s disease in late life: Findings from the Nun Study. JAMA, 275, 528–532. Snyder, L., Rupprecht, P., Pyrek, J., Breckhus, S., & Moss, T, (1978). Wandering. The Gerontologist, 18, 272–280. Soverini, S.B.E, (1968) On a strange case of wandering in an arteriosclerotic demented patient. Gerontology, 16, 846–851. Stevens, A., Owen, J., Roth, D., Clay, O., Bartoucci, A., & Haley, W. (2004). Predictors of time to nursing home placement in White and African American individuals with dementia. Journal of Aging and Health, 16, 375–397. Stokes, G. (1986). Wandering, common problems with the elderly confused. Bicester, UK: Winslow Press. Strahan, G. W. (1997). Overview of nursing homes and their current residents: Data from the 1995 National Nursing Home Survey. Advance Data. (no. 280). Washington, D.C.: U.S. Department of Health and Human Services, National Center for Health Statistics, Centers for Disease Control and Prevention. Taylor, D. H., & Sloan F. A. (2000). How much do persons with Alzheimer’s disease cost Medicare? Journal American Geriatric Society 48, 639–46. Teri, L., Gibbons, L. E., McCurry, S. M., Logsdon, R. G., Buchner, D. M., Barlow, et al. (2003). Exercise plus behavior management in patients with Alzheimer disease: A randomized controlled trial. JAMA, 290, 2015–2022.
70

Teri, L., Larson, E., & Reifler, B. (1988). Behavioral disturbance in dementia of Alzheimer's type. Journal of the American Geriatrics Society, 36, 1–6. Teri. L. (1999) Training families to provide care: Effects on people with dementia. International Journal of Geriatric Psychiatry, 14, 110–119. Van Hooren, S. A., Valentijn, S. A., Bosma, H., Ponds, R. W., Van Boxtel, M. P., & Jolles, J. (2005). Relation between health status and cognitive functioning: A 6-year follow-up of the Maastricht aging study. Journal of Gerontology: Psychological Sciences, 60B, P57–P60. Vieweg, V., Blair, C., Tucker, R. & Lewis, R. (1995). Factors precluding patients' discharge to the community: a geropsychiatric hospital survey. Virginia Medical Quarterly, 122, 275–278. Wallsten, S. S. (2000). Effects of caregiving, gender, and race on the health, mutuality, and social supports of older couples. Journal of Aging and Health, 12, 90–111 Whitehouse, P. J. (2000). Harmonization of dementia drug guidelines (United States and Europe): A report on the International Working Group for the Harmonization for Dementia Drug Guidelines, Alzheimer’s Disease and Associated Disorders, 14 Suppl. 1, S119–S122. Whitehouse, P. J. (2004). The history of therapeutic trials in dementia. New York: Taylor & Francis Medical Publishers. Wilcock, G., Howe, I., Coles, H., Lilienfield, S., Truyen, L., Zhu, Y., et al., (2003). A long-term comparison of galantamine and donepezil in the treatment of Alzheimer’s disease. Drugs and Aging 20, 777–789. Wilcock, G., Lilienfeld, S., Gaens, E. (2000). Efficacy and safety of galantamine in patients with mild-to-moderate Alzheimer’s disease: multicentre randomised controlled trial. Galantamine International-1 Study Group. British Medical Journal, 32, 1–7. Wygaard, H. A., & Albreksten, G. (1992). Risk factors for admission to a nursing home: A study of elderly people receiving home nursing. Scandinavian Journal of Primary Health Care, 10, 128–33. Yaffe, K., Fox, P., Newcomer, R., Sands, L., Lindquist, K., Dane, K., & Covinsky, K. E. (2002). Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA, 287, 2090–2097. Young, A. S., Klap, R., Shebourne, C. D. & Wells, K. B. (2001). The quality of care for depressive and anxiety disorders in the United States. Archives of General Psychiatry, 58, 55–61. Young, R. C., Gyulai, L., Mulsant, B. H., Flint, A., Beyer, J. L., Shulman, K. I. et al. (2004). Pharmacotherapy of bipolar disorder in old age. American Journal of Geriatric Psychiatry, 12, 342–357. Zarit, S. H., & Zarit, J. M. (1998). Mental disorders in older adults: Fundamentals of assessment and treatment. New York: The Guilford Press.
71

Appendix A: FMHI PSRDC Catcaid Documentation
Background The PSRDC Catcaids were originally developed by the Florida Mental Health Institute Policy and Services Research Data Center in an attempt to identify and categorize mental health services provided by the Florida Agency for Health Care Administration (AHCA) through Medicaid. Prior to 2002, Catcaids were named catcodes. The decision to change the name came in response to the acquisition of Medicare claims data, and the subsequent need to identify and categorize Medicare mental health services. It was decided to rename the Medicaid catcodes, “Catcaids” and to name the new Medicare catcodes, “Catcares”. In evaluating the Medicaid claims service utilization data, the PSRDC recognized the need to create logical groupings of services in order to describe broad service delivery patterns to AHCA. The development of mental health Catcaids has been an ongoing process that began in 1996. Other Catcaids were also created to categorize services in the Managed Care Encounter data, which were not applicable to services in the Medicaid claims data. The existence of thousands of procedure codes used in claims billing necessitated the aggregation of procedure codes into large groups of services. Because procedure codes did not exist on every claim, other variables had to be employed in developing the categorization scheme. The variables that were used in the Medicaid Catcaid scheme included the following: procedure code, diagnosis code, record type, claim form, appropriations code, treatment provider type, treatment provider specialty, pay to provider type and age. The mental health Catcaids began as several large, inclusive groups that were defined as integer codes and later were split into more detailed categories that were defined as integer + decimal codes. A list of the mental health Catcaids, the label, a description of the category and the source variables used to construct the category (current as of 01/09/2002) is included in Table 1. Many services were separated into distinct categories based on where they were received, i.e. as an inpatient in a hospital, as an outpatient at a hospital, in an office/clinic or in a Community Mental Health Center. Then they were further divided into procedures performed at the different locations. In 1999, the need to develop physical health Catcaids in addition to the existing mental health Catcaids became apparent. The physical health Catcaids were developed as broad categories of services based on the groupings of procedure codes in the American Medical Association’s (AMA) Common Procedural Terminology (CPT) manual. The medical record type claims (which record data collected on the HCFA 1500 form) used the three levels of codes in the Health Care Financing Administration Common Procedure Coding System (HCPCS). Level I included CPT codes, level II included other national HCPCS codes, and Level III included codes reserved for assignment by the local authority. The institutional record type claims (which record data collected on the HCFA 1450 form, a.k.a. UB92 form) used ICD-9-CM procedure code, but this variable was not recorded on approximately 80% of the claims. Because of the incompleteness of the procedure code variable, the institutional claims were broadly categorized based on the claim form variable. A list of the physical health Catcaids, the label, a description of the category and the source variables used to construct the category (current as of 01/09/2002) is included in Table 2.
72

Steps in Mental Health Catcaid Assignment Step 1 (All Mental Health Catcaids 01.00 – 20.50) Understanding the hierarchical algorithm used to assign the Catcaids is very important for interpreting the results of categorical analyses using the Catcaids. The first step in Catcaid assignment is to select claims that are either medical or institutional record type, non-capitation claims. For the analyses performed on Medicaid claims data by the PSRDC, only these record types are examined. The pharmacy and capitation claims are not currently included in PSRDC analyses using Catcaids. Step 2 (All Mental Health Catcaids 01.00 – 20.50) The next step is to select and “bookmark” all of the mental health claims. A claim is selected as a mental health claim if any one of the following variables suggests it is a mental health service: procedure code, primary or secondary diagnosis code, appropriations code, treatment provider type, treatment provider specialty, pay to provider type and claim form. If a claim is selected as a mental health service based on any of the above variables, then it continues through the hierarchical algorithm (using if-then-else statements) to assign its mental health Catcaid. Step 3 (Catcaids 01.00 – 03.50) Next, the mental health claims (institutional and medical) are broadly categorized into substance abuse claims (X=03.), child (age < 21 years) claims (X=02.) and adult claims (X=01.), in that order. For instance, the substance abuse claims are selected, including both children and adults, and then the remaining claims are separated by age. Then, if certain coding conditions are met, the broadly categorized claims are assigned into inpatient hospital bed days (X.00), ancillary inpatient hospital services (X.05) and hospice/respite services (X.20). By this step, all inpatient and some medical record type claims have been assigned to Catcaids 01.00 through 03.50, if the claim was not yet assigned a Catcaid, it continues through the remaining Catcaid assignment algorithm. Step 4 (Catcaids 04.00 – 18.00) The remaining mental health Catcaid assignment only applies to the medical record type claims. Catcaids 04.00 through 18.00 are well-defined categories assigned to the mental health claims if specific criteria regarding their source variables are met. For a list of source variables used to assign these Catcaids, refer to Table 1. Step 5 (Catcaids 20.00 – 20.50) The final step involves collecting the remaining mental health claims into the “catch-all” categories 20.00 through 20.50. Catcaid 20.00 is assigned to claims with general mental procedures that are not categorized above. Catcaids 20.10 through 20.50 are categories that describe the claims that were selected as mental health claims by meeting some criterion other than a known, mental health procedure code. These claims most likely have a mental health diagnosis; however, they may have been selected based on any of the following variables: primary or secondary diagnosis code, appropriations code, treatment provider type, treatment provider specialty or pay to provider type.
73

Steps in Physical Health Catcaid Assignment Step 1 (All Physical Health Catcaids 51.00 – 99.99) All non-capitation, institutional and medical record type claims, which were not selected as mental health claims and subsequently assigned a mental health Catcaid, are then run through an algorithm for assigning a physical health Catcaid. The physical health Catcaids are based on claim forms and groupings of procedure codes within the AMA’s CPT manual. Step 2 (Catcaids 63.00 – 66.00) First, all physical health inpatient claims, institutional care claims, outpatient claims, and hospice claims are assigned a Catcaid based on claim form. Step 3 (Catcaids 51.00 – 62.00) Next, the medical record type claims with known procedure codes are run through the remaining physical health Catcaid algorithm. Step 4 (Catcaids 98.00 – 99.00) Next, the claims with national codes temporarily defined to a service while awaiting reassignment in the CPT manual are categorized into Catcaid 98.00. And finally, all other physical health services with unknown or missing procedure codes will be coded as 99.99. Claims that end up in this Catcaid should be examined every new project year to search for new codes that should be included in the algorithm. Notation regarding catcaids Procedure codes W9703 (Case management rendered by Non-Hrs staff for Aged/Disabled Waiver)and W9713 (Case aide services for Aged/Disabled Waiver) were originally categorized under catcaid 57.03. Catcaid 57.03 included assisted living, community and home support services. All costs incurred by catcaids greater than or equal to 50.00 were considered physical health costs. However, for the purposes of the present evaluation, these two procedure codes were moved from the overall physical health category and subsumed under case management services. In order to ensure equitable comparisons, the following catcaids were assigned to case management services for both groups: 06.00, 07.00, 07.50, 51.06, W9703 and W9713. No subjects in either group had catcaid 51.06 and the latter two catcaids only applied to the Aged/Disabled Waiver group.
74
Related Documents











