THE FAMILIES AND DEMOCRACY AND CITIZEN HEALTH CARE PROJECT William J. Doherty, Tai J. Mendenhall, and Jerica M. Berge University of Minnesota This article describes and updates the work of the Families and Democracy and Citizen Health Care Project, which engages with community concerns in order to effect change on many system levels. The project draws on family therapy’s tradition of interest in larger social issues and adds democratic public theory and community organizing strate- gies. Since 1999 we have developed 14 citizen initiatives with a wide range of groups on a diverse set of problem areas. We describe the overall project and several of its initiatives, we address research and evaluation issues, and we outline opportunities for marriage and family therapists to learn how to do this work in their own communities. ORIGINS OF THE PROJECT Family therapy began as a movement—not just as another way to do clinical practice. Pio- neers like Gregory Bateson and Virginia Satir were interested in larger social issues and wanted to make a difference beyond conventional mental health practice. They saw systems theory as something bigger than family dynamics alone. But this broader vision became difficult to sus- tain as the field matured, professionalized, and fought for its place in reimbursement systems. This article describes the origins and latest work of the Families and Democracy and Citizen Health Care Project, which engages with community concerns in order to effect change on many system levels. Since 1999 we have developed 14 citizen initiatives with a wide range of groups on a diverse set of problem areas, and have begun to train family therapists and other professionals in a new form of community organizing. As mentioned, pioneers as different as Bateson (1972), Bowen (1976), Auerswald (1968), Satir (1972), and Minuchin, Montalvo, Guerney, Rosman, and Schumer (1967) sought to understand and influence the larger social worlds that families live in. Subsequent innovators extended this vision through the lenses of feminism, race, global politics, and narrative therapy (Boyd-Franklin, 1989; Gould & DeMuth, 1994; Hardy, 2001; Hare-Mustin, 1978; Madigan & Epston, 1995; Walters, Carter, Papp, & Silverstein, 1988; White & Epston, 1990). More recent developments include the work of Almeida, Vecchio, and Parker (2008) on social justice and family therapy; Rojano’s (2004) model of Community Family Therapy to engage urban, low-income families; and Landau’s (2007) Linking Human Systems Community Resilience Model, which specializes in work with communities that have undergone rapid transition or traumatic loss. In addition to building on these pioneers in family therapy, our work draws on democratic public theory and community organizing strategies. Our exposure to these fields began in the William J. Doherty, PhD, Professor and Director of the Citizen Professional Center, Department of Family Social Science, University of Minnesota; Tai J. Mendenhall, PhD, Assistant Professor, Department of Family Medicine and Community Health, University of Minnesota; Jerica M. Berge, PhD, Assistant Professor, Department of Family Medicine and Community Health, University of Minnesota. Address correspondence to William J. Doherty, University of Minnesota, Department of Family Social Science, 290 McNeal Hall, St. Paul, Minnesota 55108; E-mail: [email protected] Journal of Marital and Family Therapy doi: 10.1111/j.1752-0606.2009.00142.x October 2010, Vol. 36, No. 4, 389–402 October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 389

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
THE FAMILIES AND DEMOCRACY AND CITIZENHEALTH CARE PROJECT
William J. Doherty, Tai J. Mendenhall, and Jerica M. BergeUniversity of Minnesota
This article describes and updates the work of the Families and Democracy and CitizenHealth Care Project, which engages with community concerns in order to effect changeon many system levels. The project draws on family therapy’s tradition of interest inlarger social issues and adds democratic public theory and community organizing strate-gies. Since 1999 we have developed 14 citizen initiatives with a wide range of groups on adiverse set of problem areas. We describe the overall project and several of its initiatives,we address research and evaluation issues, and we outline opportunities for marriage andfamily therapists to learn how to do this work in their own communities.
ORIGINS OF THE PROJECT
Family therapy began as a movement—not just as another way to do clinical practice. Pio-neers like Gregory Bateson and Virginia Satir were interested in larger social issues and wantedto make a difference beyond conventional mental health practice. They saw systems theory assomething bigger than family dynamics alone. But this broader vision became difficult to sus-tain as the field matured, professionalized, and fought for its place in reimbursement systems.This article describes the origins and latest work of the Families and Democracy and CitizenHealth Care Project, which engages with community concerns in order to effect change onmany system levels. Since 1999 we have developed 14 citizen initiatives with a wide range ofgroups on a diverse set of problem areas, and have begun to train family therapists and otherprofessionals in a new form of community organizing.
As mentioned, pioneers as different as Bateson (1972), Bowen (1976), Auerswald (1968),Satir (1972), and Minuchin, Montalvo, Guerney, Rosman, and Schumer (1967) sought tounderstand and influence the larger social worlds that families live in. Subsequent innovatorsextended this vision through the lenses of feminism, race, global politics, and narrative therapy(Boyd-Franklin, 1989; Gould & DeMuth, 1994; Hardy, 2001; Hare-Mustin, 1978; Madigan &Epston, 1995; Walters, Carter, Papp, & Silverstein, 1988; White & Epston, 1990). More recentdevelopments include the work of Almeida, Vecchio, and Parker (2008) on social justiceand family therapy; Rojano’s (2004) model of Community Family Therapy to engage urban,low-income families; and Landau’s (2007) Linking Human Systems Community ResilienceModel, which specializes in work with communities that have undergone rapid transition ortraumatic loss.
In addition to building on these pioneers in family therapy, our work draws on democraticpublic theory and community organizing strategies. Our exposure to these fields began in the
William J. Doherty, PhD, Professor and Director of the Citizen Professional Center, Department of Family
Social Science, University of Minnesota; Tai J. Mendenhall, PhD, Assistant Professor, Department of Family
Medicine and Community Health, University of Minnesota; Jerica M. Berge, PhD, Assistant Professor,
Department of Family Medicine and Community Health, University of Minnesota.
Address correspondence to William J. Doherty, University of Minnesota, Department of Family Social
Science, 290 McNeal Hall, St. Paul, Minnesota 55108; E-mail: [email protected]
Journal of Marital and Family Therapydoi: 10.1111/j.1752-0606.2009.00142.xOctober 2010, Vol. 36, No. 4, 389–402
October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 389

mid-1990s and was informed by the Public Work Model, developed by Harry Boyte, NancyKari, Nancy Shelton, and their colleagues at the Center for Democracy and Citizenship at theUniversity of Minnesota (Boyte, 2005, 2007; Boyte & Kari, 1996; Boyte, Kari, Lewis, Skelton,& O’Donoghue, 2000). The following description of the Public Work Model is adapted fromDoherty and Carroll (2002):
Harry Boyte, a political theorist who was schooled in the civil rights struggles of the 1960sand the Saul Alinsky tradition of community organizing, moved from a radical-left politicalphilosophy in the 1970s to what he called a ‘‘new populism’’ in the 1980s and 1990s. The PublicWork Model brings together strands of American Pragmatism (e.g., John Dewey, 1997), publicrealm theorists such as Hannah Arendt (1958) and Jurgen Habermas (1979), and related philo-sophical and theological traditions dealing with humans as ‘‘homo faber’’ (constructing theworld). The model has three principal orientating ideas:
1. Human beings as producers or cocreators of the world. Public work is defined as sus-tained, visible, and serious effort by a diverse mix of ordinary people that createsthings of lasting civic or public significance. In contrast, the provider ⁄ consumerdynamic of American culture renders people passive recipients of services (from profes-sionals, the state, and the market) rather than cocreators of important work.
2. The importance of public life. Without denying the importance of the intimate sphereof family and friends, the model emphasizes the role of a public life to a full humanlife. Private life cannot be cut off from the public life in the ‘‘commons,’’ and the priv-atization of contemporary life leads to the unhealthy dominance of the market and thestate over human affairs.
3. Democratic, relational power. Ordinary people working together can influence, through‘‘civic muscle,’’ the world of institutions, professions, and the marketplace. ‘‘Democ-racy’’ in this sense is not just about voting and volunteering as a private citizen; it isabout joining with other citizens to build a robust public world. Although not timidabout conflict, the model stresses the development of relationships of mutual interestand collaborative energy to work on public solutions, in contrast to the traditionalpolitics of protest.
The Public Work Model sensitized us to civic and citizenship arenas of health care that extendbeyond the traditional clinical setting. We moved away from the language of ‘‘intervention’’ tothat of ‘‘citizen work’’; we think of ourselves as citizen professionals developing initiatives withother citizens and especially with families as citizens. We also became sensitized to the limitationsof conventional interdisciplinary, collaborative models of clinical care because the culture ofhealth care emphasizes provider ⁄ consumer relationships. In particular, collaborative, wraparoundservices and larger systems interventions generally do not move past the provider ⁄ consumerhierarchy, and the emphasis remains on care provided for one patient or family at a time.Similarly, we grew wary of advocacy approaches to social change in which the expert professionalattempts to obtain resources on behalf of passive communities. Engaging families and citizens ascocreators of health care and cultural change, we concluded, would mean developing new ways ofworking. That is where the community organizing tradition became appealing.
Modern community organizing originated with Saul Alinsky (1946) and those whofollowed him in the Industrial Areas Foundation (IAF) and subsequent groups. Contemporarycommunity organizing, however, has moved past Alinsky’s politics of protest and insteademphasizes the renewal of local democracy, the reorganization of relationships between powerand politics, and the restructuring of the physical and civic infrastructures of communities(Warren, 2001). From the IAF we learned the importance of listening to individuals and fami-lies to determine what is of most importance to them, to work closely with them around under-standing a problem before generating action solutions, and to continually identify and developnew leaders in health care settings and communities. Unlike most community organizingapproaches, which have been mistrustful of professionals (often for good reason), ours
390 JOURNAL OF MARITAL AND FAMILY THERAPY October 2010

maintains a role for professionals as partners and, at the outset, catalytic leaders. Of course, weare not alone in working toward more collaborative approaches to professional ⁄ communitypartnerships. For example, the Healthy Communities 2010 initiative has stimulated innovationsacross the United States (http://www.healthypeople.gov/Publications/HealthyCommunities2001/default.htm). There is a rich tradition of community-oriented primary care in medicine (Harper,Baker, & Reif, 2001), and important social justice efforts in counseling psychology (Aldarondo,2007).
OVERVIEW OF THE MODEL
We refer to the overall framework as the Families and Democracy Model. As applied tohealth care, we call it Citizen Health Care. As described elsewhere (Doherty & Carroll, 2002,2007; Doherty & Mendenhall, 2006), the model includes six guiding principles and seven corestrategies for implementing citizen action initiatives. It stresses the importance of civic engage-ment to strengthen family life, emphasizes the need to transcend traditional provider ⁄ consumermodels of health care and professional service delivery, and offers a vision of families and pro-fessionals together creating public initiatives. Here are the main principles:
1. The greatest untapped resource for strengthening families and improving health care isthe knowledge, wisdom, and lived experience of individuals, families, and communitieswho are facing difficult challenges in their everyday lives.
2. People must be engaged as coproducers of health care and community change, not justas patients or consumers of services.
3. Professionals can play a catalytic role in fostering citizen initiatives when they developtheir public skills as citizen professionals in groups with flattened hierarchies.
4. If you begin with an established program, you will not end up with an initiative that is‘‘owned and operated’’ by citizens. But a citizen initiative might create or adopt a pro-gram as one of its activities.
5. Local communities must retrieve their own historical, cultural, and religious traditionsof health and healing, and bring these into dialogue with contemporary health careand other community systems.
6. Citizen initiatives should have a bold vision (a BHAG—a big, hairy, audacious goal)while working pragmatically on focused, specific projects.
We implement these principles through democratic, small-group strategies that lead to col-lective action. We are vigilant about the ever-present risk of lapsing back into a traditional pro-gram and professional service models, and we avoid the typical ‘‘volunteer’’ approach thatinvolves people as helpers but not as productive citizens. Here are the core implementationstrategies:
1. Employ democratic planning and decision making at every step.2. Emphasize mutual teaching and learning among families.3. Create ways to fold new learnings back into the community.4. Continually identify and develop new leaders.5. Use professional expertise selectively—‘‘on tap,’’ not ‘‘on top.’’6. Generate public visibility through media and community events.7. Forge a sense of larger purpose beyond helping immediate participants.
Recently, we have developed a less academic way to articulate these principles and strate-gies, as we found the original versions challenging for communities where many members donot speak English as their first language and where citizen action group members do not havehigh levels of education. Table 1 contains this version of the core principles, which has becomeour preferred way to describe the model to all community groups. Table 2 contains moredetails about the implementation strategies.
October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 391
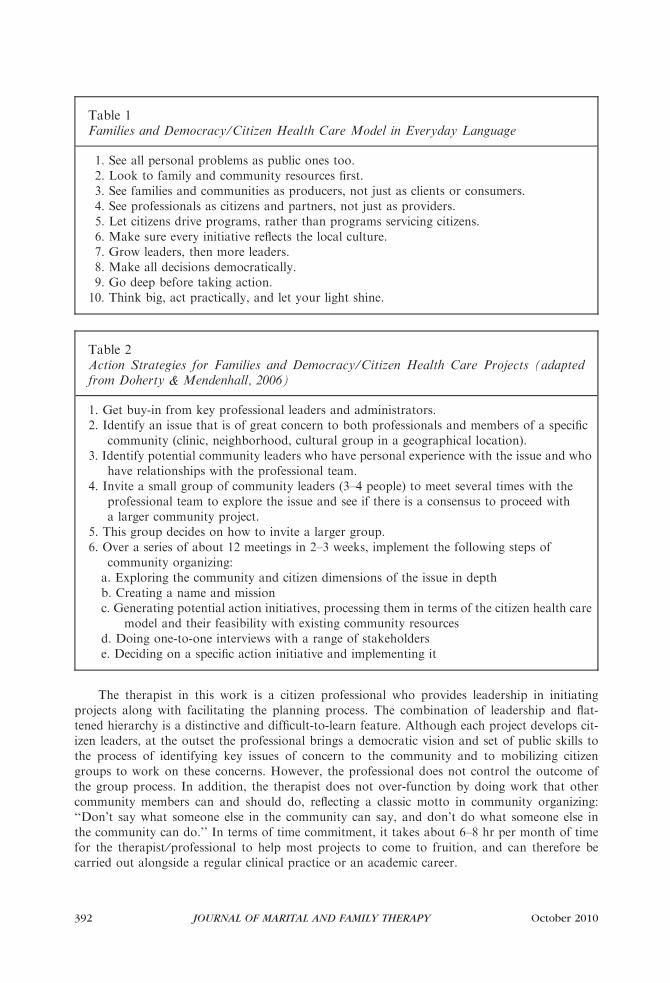
The therapist in this work is a citizen professional who provides leadership in initiatingprojects along with facilitating the planning process. The combination of leadership and flat-tened hierarchy is a distinctive and difficult-to-learn feature. Although each project develops cit-izen leaders, at the outset the professional brings a democratic vision and set of public skills tothe process of identifying key issues of concern to the community and to mobilizing citizengroups to work on these concerns. However, the professional does not control the outcome ofthe group process. In addition, the therapist does not over-function by doing work that othercommunity members can and should do, reflecting a classic motto in community organizing:‘‘Don’t say what someone else in the community can say, and don’t do what someone else inthe community can do.’’ In terms of time commitment, it takes about 6–8 hr per month of timefor the therapist ⁄professional to help most projects to come to fruition, and can therefore becarried out alongside a regular clinical practice or an academic career.
Table 1Families and Democracy ⁄Citizen Health Care Model in Everyday Language
1. See all personal problems as public ones too.2. Look to family and community resources first.3. See families and communities as producers, not just as clients or consumers.4. See professionals as citizens and partners, not just as providers.5. Let citizens drive programs, rather than programs servicing citizens.6. Make sure every initiative reflects the local culture.7. Grow leaders, then more leaders.8. Make all decisions democratically.9. Go deep before taking action.
10. Think big, act practically, and let your light shine.
Table 2Action Strategies for Families and Democracy ⁄Citizen Health Care Projects (adaptedfrom Doherty & Mendenhall, 2006)
1. Get buy-in from key professional leaders and administrators.2. Identify an issue that is of great concern to both professionals and members of a specific
community (clinic, neighborhood, cultural group in a geographical location).3. Identify potential community leaders who have personal experience with the issue and who
have relationships with the professional team.4. Invite a small group of community leaders (3–4 people) to meet several times with the
professional team to explore the issue and see if there is a consensus to proceed witha larger community project.
5. This group decides on how to invite a larger group.6. Over a series of about 12 meetings in 2–3 weeks, implement the following steps of
community organizing:a. Exploring the community and citizen dimensions of the issue in depthb. Creating a name and missionc. Generating potential action initiatives, processing them in terms of the citizen health care
model and their feasibility with existing community resourcesd. Doing one-to-one interviews with a range of stakeholderse. Deciding on a specific action initiative and implementing it
392 JOURNAL OF MARITAL AND FAMILY THERAPY October 2010
Although all helping professionals can learn to do Families and Democracy work, we havefound that family therapists have something distinctive to offer from our clinical training.Systems thinking is obviously the main advantage, along with experience working in groupsand not just one-to-one. We know how to connect with multiple people who often begin withdifferent needs and agendas. We have skills in forging a common purpose across diverging pur-poses. We know how to create processes where everyone has a voice and where powerful indi-viduals do not dominate the dialogue. We know how to ask key questions of a group of peopleand let the interaction flow to surprising places that we could not have anticipated in advance.We know how to be central to the process when necessary to keep it productive, and how tobe peripheral when we are getting in the way. In other words, there is continuity between theknowledge and skill sets of marriage and family therapists and this work of the citizen profes-sional.
THE PROJECTS
A key point in implementing projects is the delineation of the community to be involved ina project. Here the model reflects the influence of the community organizing tradition and itsemphasis on mobilizing relatively small communities where a group of citizen organizers canpotentially know many of the stakeholders, or at least have access to them. Our approach isnot as suitable for entire metro areas where few ordinary citizens would be networked broadly.We have found that a clinic population often serves as a good community boundary for CitizenHealth Care initiatives—and within that clinic community, a subcommunity of people dealingwith the same health issues, such as diabetes or depression. In a new project, we might startwith a clinic and then engage a larger local community, but even then we will work with a sub-community of people facing a common challenge (Berge, Mendenhall & Doherty, in press).Other projects outside of health care systems that we have initiated have involved a culturalcommunity in a midsized town, and parents in urban neighborhoods. The point here is thatthe project begins when there is an issue of great concern to everyday citizens in an identifi-able community—and is an issue that the therapist or other professionals care deeply aboutas well.
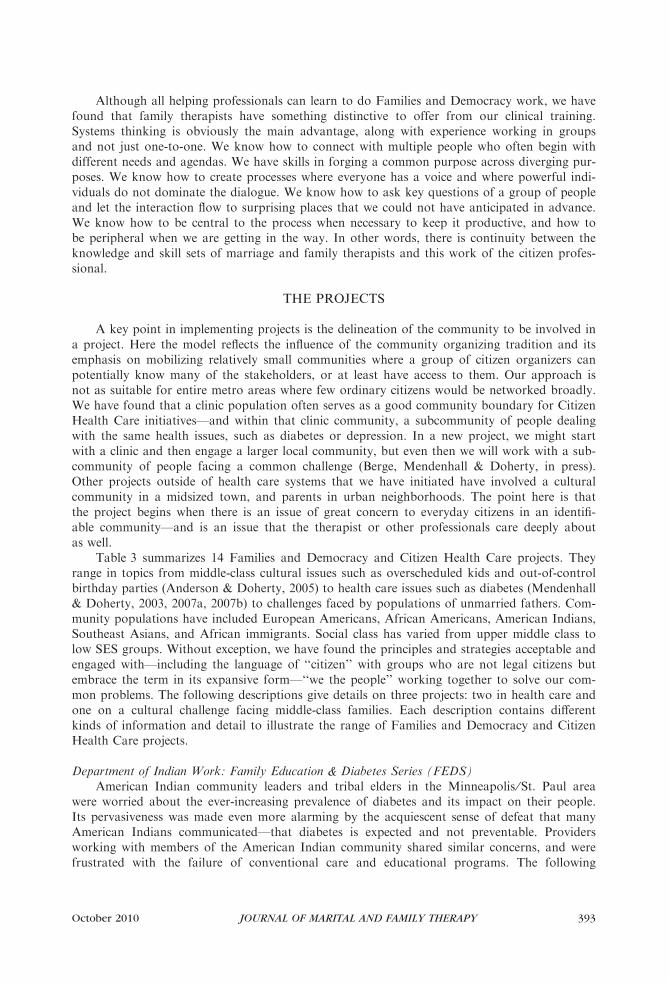
Table 3 summarizes 14 Families and Democracy and Citizen Health Care projects. Theyrange in topics from middle-class cultural issues such as overscheduled kids and out-of-controlbirthday parties (Anderson & Doherty, 2005) to health care issues such as diabetes (Mendenhall& Doherty, 2003, 2007a, 2007b) to challenges faced by populations of unmarried fathers. Com-munity populations have included European Americans, African Americans, American Indians,Southeast Asians, and African immigrants. Social class has varied from upper middle class tolow SES groups. Without exception, we have found the principles and strategies acceptable andengaged with—including the language of ‘‘citizen’’ with groups who are not legal citizens butembrace the term in its expansive form—‘‘we the people’’ working together to solve our com-mon problems. The following descriptions give details on three projects: two in health care andone on a cultural challenge facing middle-class families. Each description contains differentkinds of information and detail to illustrate the range of Families and Democracy and CitizenHealth Care projects.
Department of Indian Work: Family Education & Diabetes Series (FEDS)American Indian community leaders and tribal elders in the Minneapolis ⁄St. Paul area
were worried about the ever-increasing prevalence of diabetes and its impact on their people.Its pervasiveness was made even more alarming by the acquiescent sense of defeat that manyAmerican Indians communicated—that diabetes is expected and not preventable. Providersworking with members of the American Indian community shared similar concerns, and werefrustrated with the failure of conventional care and educational programs. The following
October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 393

Table 3Citizen Health Care ⁄Families in Democracy Projects
Students Against Nicotine and Tobacco Addiction (SANTA). This initiative, started in2006 and funded by ClearWay-Minnesota, engages local providers in partnership withstudents, teachers, and administrators in the HHH St. Paul Job Corps community toaddress on-campus smoking (and the concomitant reduction of students’ stressors andthe adoption of healthier lifestyles). Its mission is to improve the health and well-beingof students at Job Corps through smoking cessation, education, stress reduction, and support.
Family Education & Diabetes Series (FEDS). This health promotion initiative wascreated through the collaborative efforts of providers affiliated with the University ofMinnesota and local leaders in the St. Paul ⁄Minneapolis American Indiancommunity. Begun in 2001 and funded through a variety of internal and external grantmonies, it works to engage low-income, urban-dwelling American Indians and theirfamilies in an active forum of education, fellowship, and support. Its mission is toimprove the health and well-being of American Indian people through diabeteseducation, fellowship, and support in manners that embrace their heritage, values, and culture.
Hmong Women United Against Depression (HWUAD). This initiative, begun in 2005,engages local providers and representatives of the St. Paul Hmong community in acollaborative partnership oriented to investigating, understanding, and improving thelives of patients and refugees who are struggling with a variety of life stressors related todepression, chronic physical health problems, and psychosocial difficulties associatedwith relocation. Its mission is to tap the wisdom and resources of the St. Paul Hmongcommunity to empower, support, encourage, and offer hope to Hmong women and theirfamilies who live with depression.
A Neighbor Giving Encouragement, Love & Support (ANGELS). This initiative,started in 2002, encompasses providers working in partnership with teens who havediabetes and their parents to connect with families who are struggling with diabetes toothers who have lived experiences with the disease. Its mission is to empower andsupport adolescents and their families as they traverse the crisis of diagnosis and adjustwell in early phases of diabetes management. These efforts begin at the time ofdiagnosis—generally in the context(s) of emergency hospitalization—and continueacross a variety of patient ⁄ family combinations (adolescents with adolescents, parentswith parents, families with families) on and off hospital grounds.
Sisters Together Overachieving in Raising Kids (STORKS). This initiative targets at-riskurban single pregnant teens in North Minneapolis. Its mission is to promote healthychild development in children with teenage mothers and to provide community supportfor young single mothers. It began in 2004 and ended in 2006.
Parenting Partnerships. First begun in 2007, this initiative targets urban parents ofteenagers in North Minneapolis. Its mission is to promote healthy behaviors in at-riskteenagers. This initiative uses multifamily mentoring with parent ⁄ teenager groupswithin the community to address violence and high-risk behaviors in youth.
Family Formation Project. This initiative encompasses at-risk urban unmarried coupleswith children in Minneapolis and St. Paul being mentored by experienced marriedcouples and forming their own leadership group. Its mission is to promote stable familyformation and healthy marriage in urban couples who desire this for themselves. Theinitiative, which began in 2004, has received both federal and state funding. See http://fsos.che.umn.edu/projects/mnffp.html.
394 JOURNAL OF MARITAL AND FAMILY THERAPY October 2010

description of the process of initiating a Citizen Health Care project on this area is adaptedand updated from Mendenhall and Doherty (2005) and Doherty and Mendenhall (2006):
Tai Mendenhall and leaders in the St. Paul Department of Indian Work (Nan LittleWalker,Betty GreenCrow, Sheila WhiteEagle, and Steve BrownBear) approached this challenge with acommunity-based participatory research approach, using Citizen Health Care as a guide. Con-siderable effort was spent in designing a partnership with providers that was very different fromconventional top-down models of care. American Indian community members succeeded in
Table 3(Continued)
Putting Family First. Parents in Wayzata, a suburb of Minneapolis, began organizing thisinitiative around the problem of overscheduled kids in 1999. Their mission is: ‘‘PuttingFamily First works to raise awareness about the crucial connections between parentsand children, and helps families find balance in their lives.’’ See http://www.PuttingFamilyFirst.org.
Balance4Success. This initiative (started in 2005) involves parents in Apple Valley andnearby suburbs of Minneapolis ⁄St. Paul organizing with a mission to liberate their kidsfrom out-of-control sports schedules and to change the culture of hypercompetitivechildhood by replacing busyness with balance.
Community Engaged Parent Education. This initiative, begun in 2004 and supported bythe McKnight and Bremer Foundations, engages parent educators in developing citizenawareness and civic action in parents across Minnesota. Its mission is to encouragecitizen deliberation on public issues relating to children’s well-being. Evaluation findingsindicate that parent educators can learn the skills and that parents respond by engaging inpublic dialogue and civic action. See http://fsos.che.umn.edu/projects/cepe.html andDoherty, Jacob and Cutting (in press).
Birthdays Without Pressure. This initiative, started in 2006, involves parents in St. Paul,Minnesota, organizing against out-of-control birthday parties. Its mission is to raiseawareness of the problem of out-of-control birthday parties, to offer alternatives, and tolaunch a local and national conversation about the problem. See http://www.BirthdaysWithoutPressure.org.
Intervention Approaches to Reduce Tobacco Use Among Southeast Asian Communities.This initiative partners four Southeast Asian communities in Minneapolis ⁄St. Paul—Hmong, Cambodian, Laotian, and Vietnamese—in a mission to design and carry out pilotprojects on tobacco use that call upon the culture resources of Southeast Asiancommunities. Funded by the Minnesota Partnership for Action Against Tobacco, thiswork was first launched in 2006.
Family Health, Child Success. This CBPR initiative involves parents and professionalsorganizing to promote child well-being among sub-Sahara African immigrant families inHennepin County, Minnesota. Started in 2007, its mission during its first stage ofdevelopment is to design and pilot a project that accesses the resources of thecommunity to meet challenges facing African families and children.
Citizen Father Project. A group of mostly African American, low-income single fathers hasdeveloped an initiative to make a difference in the lives of children, fathers, and mothersin the community by fostering healthy, active fathering, challenging false images ofmanhood, and rebuilding family and community values. The men are deliveringcommunity presentations to fathers, including incarcerated fathers, and to mothers,youth, and professional groups.
October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 395
sensitizing clinical researchers regarding the process, pace, and importance of building trustwithin American Indian circles. As the team engaged in a series of meetings, discussions, andAmerican Indian community events, this trust evolved. Researchers learned about AmericanIndian culture, the diversity of cultures ⁄ tribes within this larger frame (e.g., Dakota, Ojibwe,Hocak), belief systems, and manners—all because they were allowed into the American Indiancommunity itself. In turn, community members gained more insight regarding how Westernmedicine is oriented, and thereby gained insight into providers’ habitudes and perspectives incare delivery.
The St. Paul Area Council of Churches’ Department of Indian Work’s (DIW) Family Edu-cation & Diabetes Series was designed and implemented as a supplement to standard care formembers of the American Indian community touched by diabetes. Patients, their families(spouses, parents, children), and providers (physicians, nurses, dieticians, mental health person-nel) come together every other week for an evening of fellowship, education, and support. Gen-erally, 6–7 providers, 4–5 tribal elders, and 30–35 community members attend. Meetings beginwith members checking and recording each other’s blood sugars, weight, body mass index, andconducting foot checks. Participants cook meals together that are consistent with AmericanIndian culture and traditions, and a great deal of discussion is put forth regarding the meal’singredients, portion sizes, and relevance to diabetes. Educational sequences follow (which aredesigned according to participants’ interests and wants), and take place in talking circles and avariety of lively activities (e.g., traditional and modern music, chair dancing and aerobics,impromptu theater ⁄ role-plays). Instructional topics are similarly diverse (e.g., basic diabeteseducation, obesity, foot care, stress management, exercise, family relationships, retinopathy,dental care, and resources to facilitate access to medical services and supplies). FEDS eveningsconclude with devoted time for informal sharing and support. These biweekly series are sched-uled to last for three hours, but most participants arrive early and stay late.
Clinical and lay participants in FEDS worked collaboratively throughout every stage ofthe initiative’s development—from early efforts in relationship-building and establishing mutualrespect and trust, to brainstorming the program’s design, educational foci and formats, publicvisibility, implementation, and ongoing modifications. The DIW and its clinical collaboratorsare now working to extend their efforts to create new programs in areas of the AmericanIndian community that are not readily reached by state- or reservation-sponsored care systems(e.g., inner-city, low-income American Indians).
Discontent Among Middle-Class Parents: The Case of Overscheduled KidsFor many middle-class children, childhood is becoming a rat race of hyperscheduling, over-
busyness, and loss of family time (Anderson & Doherty, 2005). The following description ofthe process of initiating a Families and Democracy project on this area is adapted and updatedfrom Anderson and Doherty (2005):
Bill Doherty was invited to give a keynote talk to a large conference for parents in Wayzata,Minnesota, on the topic of family time and family rituals. In his presentation, Doherty raisedthe problem of the loss of family time to outside activities for children, and the importance oftaking back family life from overscheduled family hyperactivity and the consumer culture ofchildhood. Parents responded enthusiastically to the message, but seemed at a loss about howto turn back the tide of overbusyness. Several school and community officials reflected inprivate that their organizations unintentionally contribute to this problem by offering more andmore activities for children and youth, without alerting parents to the inevitable toll on familytime that these activities take.
Later, Doherty was invited to return the next spring to give a similar talk as part of alecture series on parenting. He declined, saying that he only gives the same talk once in acommunity, but that if Wayzata wanted to organize to take action on the problem, he wouldreturn to help with that process. In subsequent discussions with Barbara Carlson, the local
396 JOURNAL OF MARITAL AND FAMILY THERAPY October 2010

leader who made the invitation, Doherty suggested an approach to civic engagement based onthe Public Work Model.
Doherty then gave a presentation and facilitated a town meeting for which Barbara Carl-son and her colleagues had extensively advertised and recruited parents and community leadersto attend. About 300 parents attended, and afterwards more than 80 people went to a smallerroom for the town meeting. Consensus emerged that the problem of declining family time wasa community problem, not just an individual family problem. At the end of the town meeting,parents and community leaders signed up for a leadership and planning group to provide lead-ership for a grassroots movement to make family life a higher priority in their community.Putting Family First was the name given to this community initiative; the organization is nowindependent and ongoing (http://www.PuttingFamilyFirst.org). This was the launching of thefirst community project in the country on the problem of overscheduled kids and underconnectedfamilies.
Over the next year the leadership group set about developing a mission, a desired future,and a vision of what the community could be if both individual families and communityinstitutions put family first. The leadership group took the important step of conductingstakeholder interviews throughout the community in order to understand how members of thecommunity saw the problem, what resources or solutions they had for tackling the problem,and whether or not they would be interested in joining future initiatives.
During the following spring, Putting Family First held a public ‘‘launch event’’ toannounce the initiative and to generate media attention. Community action initiatives werepresented and attendees were invited to participate in putting the new initiatives on the ground,with the previous leadership team splitting up and serving as leaders to the new initiatives.There were several initiatives that developed from this process: a Putting Family First Seal ofApproval, which would be given to organizations and businesses whose policies and practicessupport balancing outside activities with family time; a Consumer Guide, which providedparents with a detailed analysis of the time and financial demands of local children’s activitiessuch as sports and music programs that helped parents to make informed choices about whatto enroll their children in; a faith community partnership; an online Internet discussion groupfor parents; a book titled Putting Family First: Successful Strategies for Reclaiming Family Lifein a Hurry-Up World (Doherty & Carlson, 2002); and a focused approach to generating intensemedia attention around the subject of family time and about the initiative both locally andnationally.
Putting Family First stimulated a national conversation about a problem that had beennamed by a grassroots group of parents. It coined the term ‘‘overscheduled kids’’ and put itinto the American lexicon. And it inspired at least a dozen other community initiatives locallyand nationally, including family dinner initiatives (e.g., Eat.Talk.Connect in Minnesota); annualFamily Nights during which all community activities are cancelled so that families can betogether as families (e.g., Ready.Set.Relax in Ridgewood, New Jersey, USA); and a parent-ledboycott of Sunday youth sports in Carver County, Minnesota (BalanceforSuccess.org).
STORKS: Sisters Together Overachieving in Raising KidsJerica Berge was approached by several nurses within her family medicine clinic in an
inner-city neighborhood regarding their frustration with trying to help young teenage mothersin the clinic community with parenting. Commonly at medical visits the nurses would notice inthe young mothers self-doubt, naı̈ve parenting skills, permissiveness, and a lack of motivationto provide for their family. These observations caused the nurses to worry about the fate of thenext generation of children. Several of the nurses themselves had been single mothers andshared stories about how they were able to overcome the difficulties of raising their children ontheir own through community support. One nurse described a time-dollars community of sorts(For every hour you spend doing something for someone in your community, you earn one
October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 397

‘‘time dollar.’’ Then you have a time dollar to spend on having someone do something for you;http://www.timebanks.org). For instance, when this nurse was a young single mother trying toincrease her potential to provide for her family, she traded off child care with a neighbor in orderto go to school to get her nursing degree while she offered her skills in hair braiding to the neigh-bor and her children in exchange. The nurses in the clinic wanted to create a similar communityfor the teenage mothers in the clinic. This primarily African American community identified theneed of taking more responsibility as a community in raising the next generation as an issue,based on their cultural philosophy of ‘‘it takes a community to raise a village.’’
Berge met with the nurses and other providers (staff physicians, medical residents, andmental health staff) and identified this issue as a community pressure point and something theywanted to commit to doing something about. Over the course of four monthly meetings thegroup worked to identify community clinic members who could add their lived expertise to thisinitiative. Providers nominated several teenage mothers who were effectively parenting theirchildren—and who appeared to maintain solid self-esteem and progress in working towardimproving their ability to provide for their family—and asked them to join the group asmentors for other young teenage mothers who were struggling. The professionals and teenagementors worked together collaboratively throughout the process of creating this initiative. Theteenage mentors, nurses (who were both mentors and providers), physicians, and mental healthstaff met monthly for over 6 months to (a) explore the community and citizen dimensionsregarding single parenting and raising the next generation, (b) create a name and mission, (c)conduct one-to-one interviews with a range of stakeholders, and (d) decide on specific actioninitiatives and implementation strategies.
During regular medical visits, other teenage mothers from the clinic who were strugglingwith mothering were invited to become involved with the STORKS initiative. The mentoringteenage mothers would then contact the potential new members to initiate a connection andmentoring relationship. There were three main components of this initiative: (a) regular phonecalls, one-on-one visits, or emails between the mentoring teenage mothers and struggling moth-ers for support and coaching, (b) a time-dollars element in which all members of the STORKSinitiative participated in exchanging goods, skills, and talents with each other, and (c) biweeklymeetings with the struggling teenage mothers to discuss parenting skills. The mentoring teenagemothers took part in the meetings by co-teaching parenting skills with Berge and organizingthe time-dollars component of the initiative.
The STORKS initiative began a conversation within a community feeling hopeless andoverwhelmed about the fate of the next generation, and went on to tap the expertise of thosewho had lived experience and wisdom in overcoming these perceived barriers. Citizen partner-ing between professionals and clinic community members resulted in action strategies thataddressed a local problem that was central to this clinic community.
RESEARCH AND EVALUATION
During the first 5 years of this work, we focused on learning how to engage with communi-ties and put the model on the ground. Table 4 summarizes a number of these core informallearnings. In recent years we have developed more formal methods for evaluating Families andDemocracy and Citizen Health Care projects, and are implementing these evaluations acrossindividual, family, and community levels (Berge et al., in press). These efforts include bothqualitative evaluations of projects’ evolution and process (e.g., Mendenhall and Doherty,2007b) and quantitative assessments of outcomes directly associated with dependent variablesof interest unique to a particular project. For example, outcome evaluation of the FEDS pro-gram is focusing on physiological (e.g., A1c, BMI, weight, blood pressure), knowledge (e.g.,regarding diabetes, community resources), and disease management behaviors (e.g., blood glu-cose monitoring, exercise, diet). In our Hmong Women United Against Depression project (see
398 JOURNAL OF MARITAL AND FAMILY THERAPY October 2010

Table 3), data are being collected regarding participants’ depressive symptoms and severity,family members’ relief, and public visibility of depression as a safe topic to discuss. In the Stu-dents Against Nicotine and Tobacco Addiction (SANTA) project (see Table 3), we are collect-ing a broad range of data related to students’ smoking behaviors, readiness to change, andstress. In every case, evaluation tools are discussed and agreed upon by the whole group of citi-zen professionals and other citizens from the community.
In addition to projects that focus on specific local communities, we think of Putting FamilyFirst and its offspring as ‘‘cultural organizing’’ initiatives that harness the power of a localgroup of parents to name and challenge a problem in the larger mainstream American culture,and to gain media attention to launch local and national conversations. A recent example is theBirthdays Without Pressure Project, through which a group of parents in St. Paul, Minnesota,named the problem of out-of-control kids’ birthday parties; examined its sources in a super-sizing culture and its consequences for children, parents, and the community; developed anengaging website (http://www.BirthdaysWithoutPressure.org); and attracted widespread mediaattention nationally and internationally. For the Birthdays Without Pressure initiative, wedeveloped a way to measure media visibility and web presence as an outcome measure ofimpact on the broader cultural conversation. In the overscheduled kids project and the birthdayproject, there was enormous national and international media attention and web recognition ofthe work of the citizen groups. A subsequent citizen parent group is now planning an initiativeto address the oversexualization of young girls in today’s culture.
OPPORTUNITIES FOR MARRIAGE AND FAMILY THERAPISTS
A crucial issue at the beginning of our community engagement work was whether we couldteach this model to others or whether it represented only the local connections, vision, andskills of its originators. We now know that it is learnable because we have mentored
Table 4The Citizen Health Care Project: Key Lessons Learned (Doherty & Mendenhall, 2006)
1. This work is about identity transformation as a citizen professional, not just aboutlearning a new set of skills.
2. It is about identifying and developing leaders in the community more than about aspecific issue or action.
3. It is about sustained initiatives, not one-time events.4. Citizen initiatives are often slow and messy during the gestation period.5. You need a champion with influence in the institution.6. Until grounded in an institution’s culture and practices, these initiatives are quite
vulnerable to shifts in the organizational context.7. A professional who is putting too much time into a project is overfunctioning and
not using the model. We have found the average time commitment to be on the orderof 6–8 hr per month, but over a number of years.
8. External funding at the outset can be a trap because of timelines and deliverables,but funding can be useful for capacity building to learn the model, and for expandingthe scope of citizen projects once they are developed.
9. The pull of the traditional provider ⁄ consumer model is very strong on all sides;democratic decision making requires eternal vigilance.
10. You cannot learn this approach without mentoring, and it takes 2 years to getgood at it.
October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 399
10 professionals beyond the founding team. In September 2008, we created a Citizen Profes-sional Center at the University of Minnesota for training professionals and students in demo-cratic community engagement and for conducting community-based participatory research thatadvances knowledge and solves local problems. This center is sponsored by the College of Edu-cation and Human Development and the College of Medicine, with the main stakeholders beingthe Department of Family Social Science and the Department of Family Medicine and Com-munity Health. We are focusing initially on building a critical mass of trained citizen profes-sionals in our local region, and then branching out to national and international participants.
Public process skills require time to learn and mature. Learning to do Families andDemocracy and Citizen Health Care work well takes up to 2 years of learning the model andhaving supervised experience on a specific project. It cannot simply be taught in a weekendworkshop format. To implement the training, we anticipate offering a formal certificate basedon course work and supervised field work in the participant’s home community.
What sort of therapist might be most suitable for this kind of training experience? We envi-sion three MFT audiences for Families and Democracy ⁄Citizen Health Care training:
1. Therapists. This includes therapists at any career stage who have a passionate interestin this kind of work. Therapists in two particular career stages might especially beinterested. Students and new therapists might want to add this skill set to their reper-toire. Retiring therapists might want to give back to their communities in a differentway than providing pro bono therapy. Therapists who need to maximize income fromevery hour of professional work might not be suitable. Groups of therapists in clinicswith an outreach mission would be ideal for engaging previous clients and other com-munity members in citizen work to promote psychological and family well-being.
2. Training programs. Clinical programs inside and outside of academia might be inter-ested in faculty development in order to incorporate citizen health care training intotheir programs. On-campus clinics can serve as venues for inviting citizens to share inthe mission of the clinic.
3. Researchers. Those interested in citizen projects using community-based participatoryresearch might want to be trained in the practice and research methods involved in thiskind of work. There are increasing funding opportunities across federal and local levelsfor research that engages communities as active participants.
Our model does not require that professionals be connected to any specific kind of commu-nity (such as low-income, distressed communities) or have expertise in any specific issue (suchas trauma or diabetes). This is a generic citizen development ⁄ community organizing approachthat requires just three elements to instigate: (a) a challenge that a community of individualsand families cares deeply about, (b) a citizen professional who has a relationship of trust withthis community and who also cares deeply about the challenge, and (c) the challenge lends itselfto local action that accesses the current resources of the community, as opposed to requiringpublic policy or institutional change for headway to be made. For example, the Citizen FatherProject has engaged low-income African American fathers in pursuing their goal of revivinga culture of active, involved fathering through outreach to fathers, mothers, and youth inthe community; the group made a conscious strategic decision to not base its success onpolicy makers changing their minds about opening more legal options to nonresidential singlefathers.
The first criterion requires a ‘‘pressure point’’ affecting the well-being of people and theirfamilies in settings such as a geographical community, a school or school district, a clinic orgroup of clinics, or a faith community. The second criterion emphasizes that the therapist hasalready established the trust of enough people in this community to be able to start the publicconversation. The third criterion reflects the difference between the Families and Democ-racy ⁄Citizen Health Care approach and the advocacy approach wherein the professional triesto mobilize people to influence powerful public or private groups to change their practices or
400 JOURNAL OF MARITAL AND FAMILY THERAPY October 2010

provide more resources (Doherty & Carroll, 2002). Our model focuses on coproduction ratherthan protest and petition (Doherty, 2008).
This work also does not require that the therapist have expert knowledge of the prob-lem area being addressed, at least at the outset, because his or her expertise is primarily inbringing the democratic model to address the problem and in facilitating the process. Weknew less about diabetes than anyone else in the room when we began our citizen diabeteswork, but soon learned enough. We knew little about the experiences of Liberian immi-grants and other sub-Sahara African groups, but could catalyze a community initiative thataccesses the knowledge, wisdom, and experience of Africans and non-Africans who workwith the community.
A downside of this work is that it rarely involves paid positions in the early stages,although funding has come at some point for seven of the 13 projects. For instance, our FamilyEducation Diabetes Series with the American Indian population and our Hmong Women Uni-ted Against Depression projects are now funded through both internal and external grants. Onthe other hand, citizen professional work does not require an extensive time commitment; asmentioned before, it can be done in about 6–8 hr per month over an extended period of time.Many professionals already contribute this amount of time to community service work or topro bono therapy; they could shift their time to citizen professional work.
Finally, we have learned that community engagement must meet the needs of the profes-sional as well as communities. If this kind of public practice outside the office fits within theirvalues and vision, professionals experience an expanded sense of professional contribution andenjoy a much closer relationship to their local community. They take on a new identity—thatof a citizen professional—and feel part of something larger: a movement toward democraticrenewal. As a woman from Ghana said in a meeting, ‘‘Back in Africa we knew about pseudo-democracy; what I am seeing here is real empowered democracy.’’ Her citizen group is tacklingthe challenge of the ongoing impact of war and trauma on children and families in the Africanimmigrant community of northwest Hennepin County, Minnesota. Led by Paul Orieny, anAfrican marriage and family therapy doctoral student who is being mentored by one of theauthors, the group aims to break the silence about the enduring impact of war and trauma thatis fragmenting their community and weakening the heart of its people.
If our current health care and human service systems are to be redesigned in the UnitedStates, it will take more than new clinical strategies for the consulting room, fairer reimburse-ment systems, or even universal health care reform (as important as these changes would be).Quality and cost challenges will continue to overwhelm our care systems if we rely on the twotraditional models—frontline professionals delivering services to people who are not empoweredto take responsibility for their own health and that of their communities, and public health pro-fessionals providing education to passive individuals and communities. The driving mission ofthe Families and Democracy and Citizen Health Care Project is to create a democratic modelof health care and human services that unleashes the capacity of ordinary citizens as producersof health and social change for themselves and their communities. Thoroughly consistent withthe new political leadership in Washington, DC, this mission requires the development of a newkind of professional—the citizen professional. With our legacy of valuing social change and ourunderstanding of how complex systems work, family therapists are ideally suited for this workand this mission.
REFERENCES
Aldarondo, E. (Ed.). (2007). Advancing social justice through clinical practice. Mahway, NJ: Lawrence Erlbaum.
Alinsky, S. D. (1946). Reveille for radicals. New York: Random House.
Almeida, R. V., Vecchio, K. D.-D., & Parker, L. (2008). Transformative family therapy: Just families in a just
society I. Boston: Pearson.
October 2010 JOURNAL OF MARITAL AND FAMILY THERAPY 401

Anderson, J., & Doherty, W. (2005). Democratic community initiatives: The case of overscheduled children.
Family Relations, 54, 654–665.
Arendt, H. (1958). The human condition. Chicago: University of Chicago Press.
Auerswald, E. (1968). Interdisciplinary versus ecological approach. Family Process, 7, 202–215.
Bateson, G. (1972). Steps to an ecology of mind. New York: Ballantine Books.
Bowen, M. (1976). Theory in the practice of psychotherapy. In P. J. Guerin, Jr. (Ed.), Family therapy: Theory
and practice (pp. 42–90). New York: Garner Press.
Boyd-Franklin, N. (1989). Black families in therapy. New York: Guilford Press.
Boyte, H. (2005). Everyday politics. Philadelphia: University of Pennsylvania Press.
Boyte, H. (2008). The citizen solution. St. Paul, MN: Minnesota Historical Society.
Boyte, H., & Kari, N. (1996). Building America: The democratic promise of public work. Philadelphia: Temple
University Press.
Boyte, H., Kari, N., Lewis, J., Skelton, N., & O’Donoghue, J. (2000). Creating the commonwealth: Public politics
and the philosophy of public work. Dayton, OH: Kettering.
Dewey, J. (1997). Democracy and education. New York: Free Press.
Doherty, W. J., & Carroll, J. S. (2002). The families and democracy model. Family Process, 41, 579–589.
Doherty, W. J. (2008). Beyond the consulting room: Therapists as catalysts for social change. Psychotherapy Net-
worker, November ⁄December, 28–35.
Doherty, W. J., & Carlson, B. Z. (2002). Putting family first: Successful strategies for reclaiming family life in a
hurry-up world. New York: Henry Holt.
Doherty, W. J., & Carroll, J. S. (2007). Families and therapists as citizens: The Families and Democracy Project.
In E. Aldarondo (Ed.), Advancing social justice through clinical practice (pp. 225–244). Mahwah, NJ: Law-
rence Erlbaum.
Doherty, W., & Mendenhall, T. (2006). Citizen health care: A model for engaging patients, families, and commu-
nities as co-producers of health. Families, Systems & Health, 24, 251–263.
Gould, B. B., & DeMuth, D. H. (Eds.). (1994). The global family therapist: Integrating the personal, professional,
and political. Boston: Allyn and Bacon.
Habermas, J. (1979). Knowledge and human interest. Boston: Beacon Press.
Hardy, J. (2001). Healing the world in fifty-minute intervals: A response to Family Therapy Saves the Planet.
Journal of Marital and Family Therapy, 27, 19–22.
Hare-Mustin, R. (1978). A feminist approach to family therapy. Family Process, 17, 181–194.
Harper, P. G., Baker, N. T., & Reif, C. J. (2001). Implementing community oriented primary care in an urban
family practice residency. Family Medicine, 32, 683–690.
Landau, J. (2007). Enhancing resilience: Families and communities as agents for change. Family Process, 46, 351–365.
Madigan, S., & Epston, D. (1995). From ‘‘Spy-chiatric Gaze’’ to communities of concern: From professional
monologue to dialogue. In S. Friedman (Ed.), The reflecting team in action: Innovations in clinical practice
(pp. 257–276). New York: Guilford Press.
Mendenhall, T. J., & Doherty, W. J. (2003). Partners in diabetes: A collaborative, democratic initiative in
primary care. Families, Systems & Health, 21, 329–335.
Mendenhall, T. J., & Doherty, W. J. (2005). Action research methods in family therapy. In F. Piercy & D. Spren-
kle (Eds.), Research methods in family therapy (2nd ed., pp. 100–118). New York: Guilford Press.
Mendenhall, T., & Doherty, W. (2007a). The ANGELS (A Neighbor Giving Encouragement, Love and Support):
A collaborative project for teens with diabetes. In D. Linville & K. Hertlein (Eds.), The therapist’s notebook
for family healthcare (pp. 91–101). New York: Hayworth Press.
Mendenhall, T., & Doherty, W. (2007b). Partners in diabetes: A community-based participatory research project
in a family practice context. Action Research 5, 378–406.
Minuchin, S., Montalvo, B., Guerney, B., Rosman, B., & Schumer, S. (1967). Families of the slums. New York:
Basic Books.
Rojano, R. (2004). The practice of community family therapy. Family Process, 43(1), 59–77.
Satir, V. (1972). Peoplemaking. Palo Alto, CA: Science and Behavior Books.
Walters, M., Carter, B., Papp, P., & Silverstein, O. (1988). The invisible web: Gender patterns in family relation-
ships. Family Relations, 41, 256–263.
Warren, M. R. (2001). Dry bones rattling: Community building to revitalize American democracy. Princeton, NJ:
Princeton University Press.
White, M., & Epston, D. (1990). Narrative means to therapeutic ends. New York: Norton.
402 JOURNAL OF MARITAL AND FAMILY THERAPY October 2010
Related Documents











