Dr Alex Simms Consultant Cardiologist @LTHT Specialist interest in Heart Failure, Devices, Inherited Cardiovascular Conditions and Pregnancy & heart disease The Failing Heart

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dr Alex SimmsConsultant Cardiologist @LTHT
Specialist interest in Heart Failure, Devices, Inherited Cardiovascular Conditions and Pregnancy & heart disease
The Failing Heart
Outline
• Definition
• Why important
• What you need to know
What is heart failure?
A clinical syndrome with typical symptoms/signs caused by structural and/or functional cardiac abnormality,
resulting in a reduced cardiac output or elevated intracardiac pressures at rest/stress
ESC HF guidelines. EHJ 2016; 37:2129
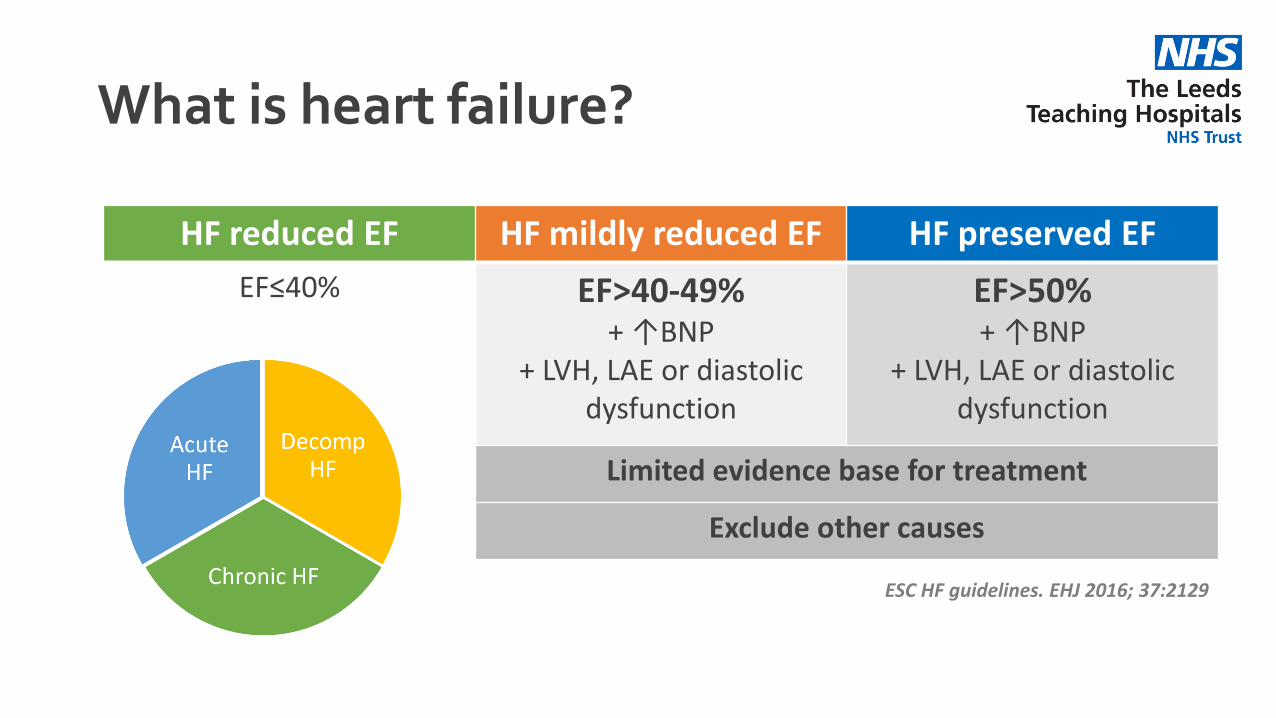
What is heart failure?
HF reduced EF HF mildly reduced EF HF preserved EF
EF≤40% EF>40-49%+ ↑BNP
+ LVH, LAE or diastolic dysfunction
EF>50%+ ↑BNP
+ LVH, LAE or diastolic dysfunction
Limited evidence base for treatment
Exclude other causes
ESC HF guidelines. EHJ 2016; 37:2129
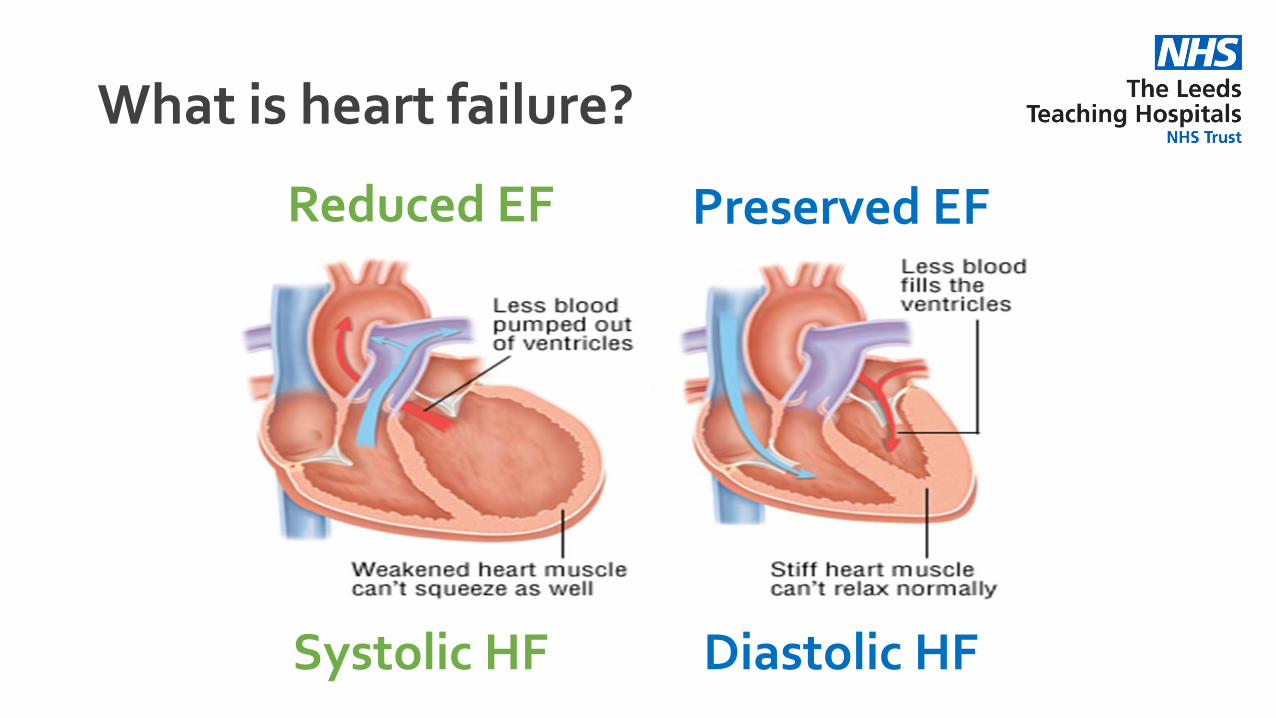
What is heart failure?
Reduced EF Preserved EF
Diastolic HFSystolic HF
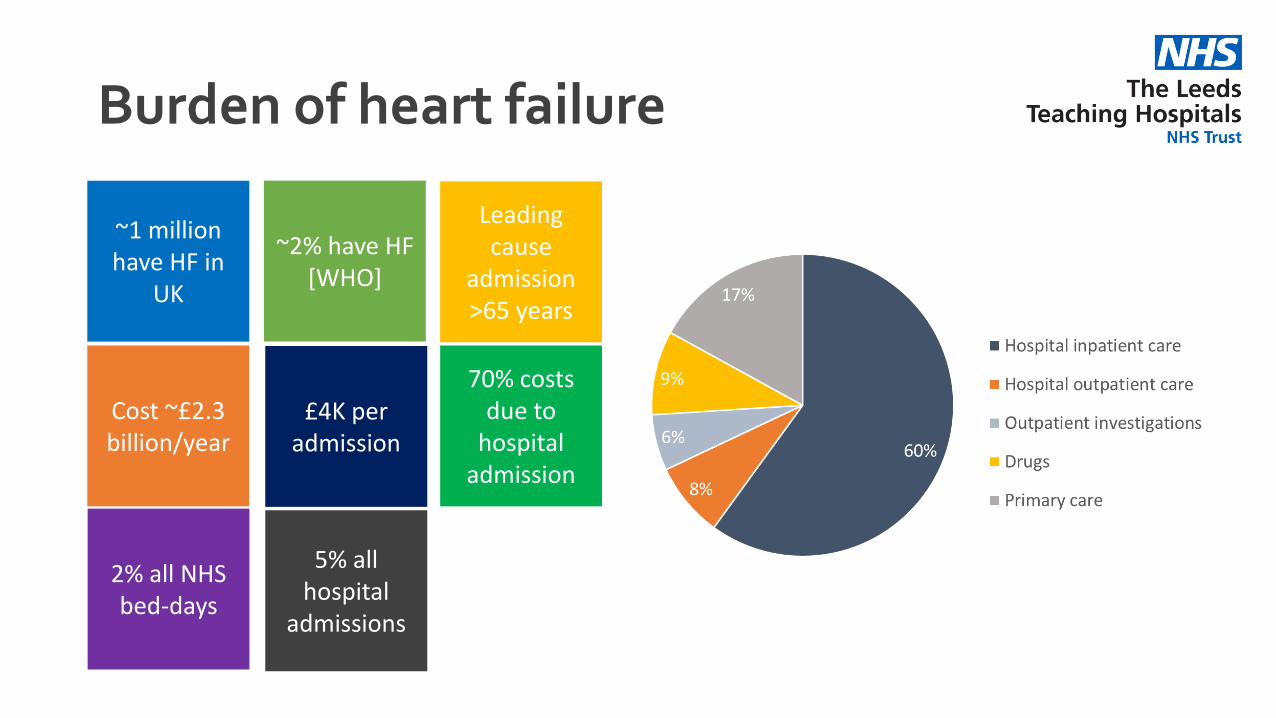
Burden of heart failure
~1 million have HF in
UK
Cost ~£2.3 billion/year
Leading cause
admission >65 years
5% all hospital
admissions
£4K per admission
~2% have HF [WHO]
2% all NHS bed-days
70% costs due to
hospital admission
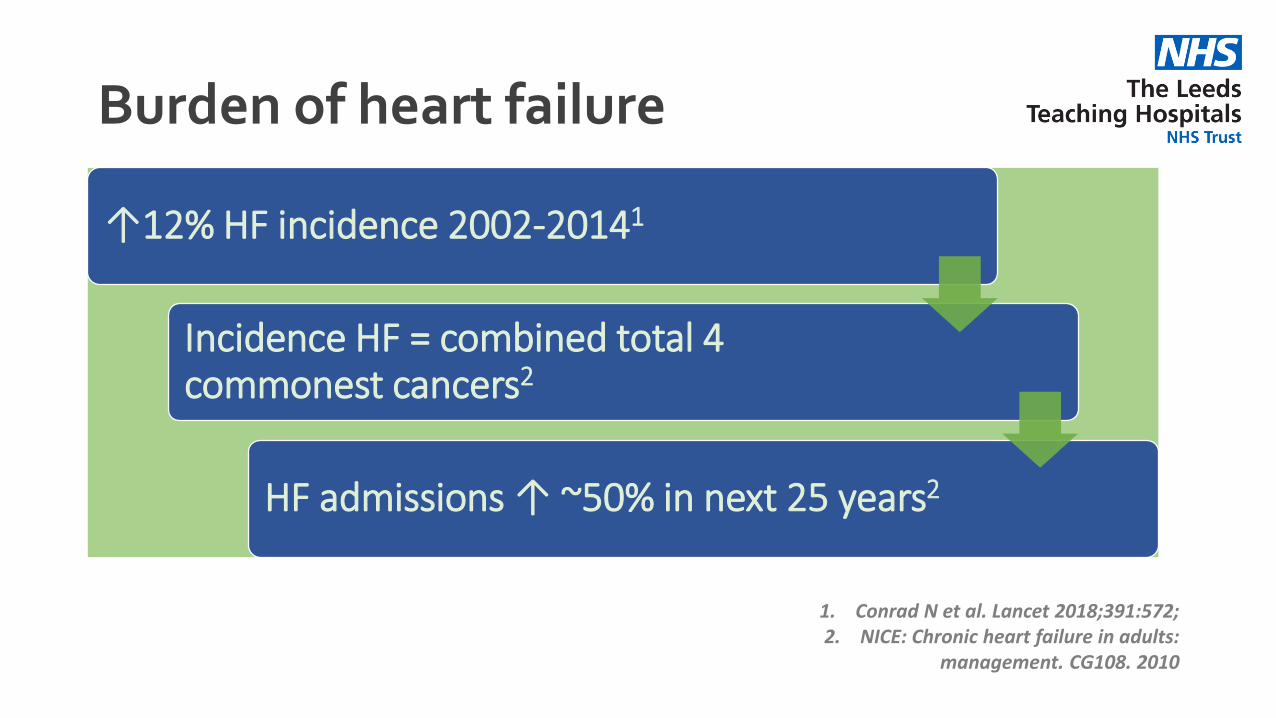
Burden of heart failure
1. Conrad N et al. Lancet 2018;391:572;2. NICE: Chronic heart failure in adults:
management. CG108. 2010
↑12% HF incidence 2002-20141
Incidence HF = combined total 4 commonest cancers2
HF admissions ↑ ~50% in next 25 years2
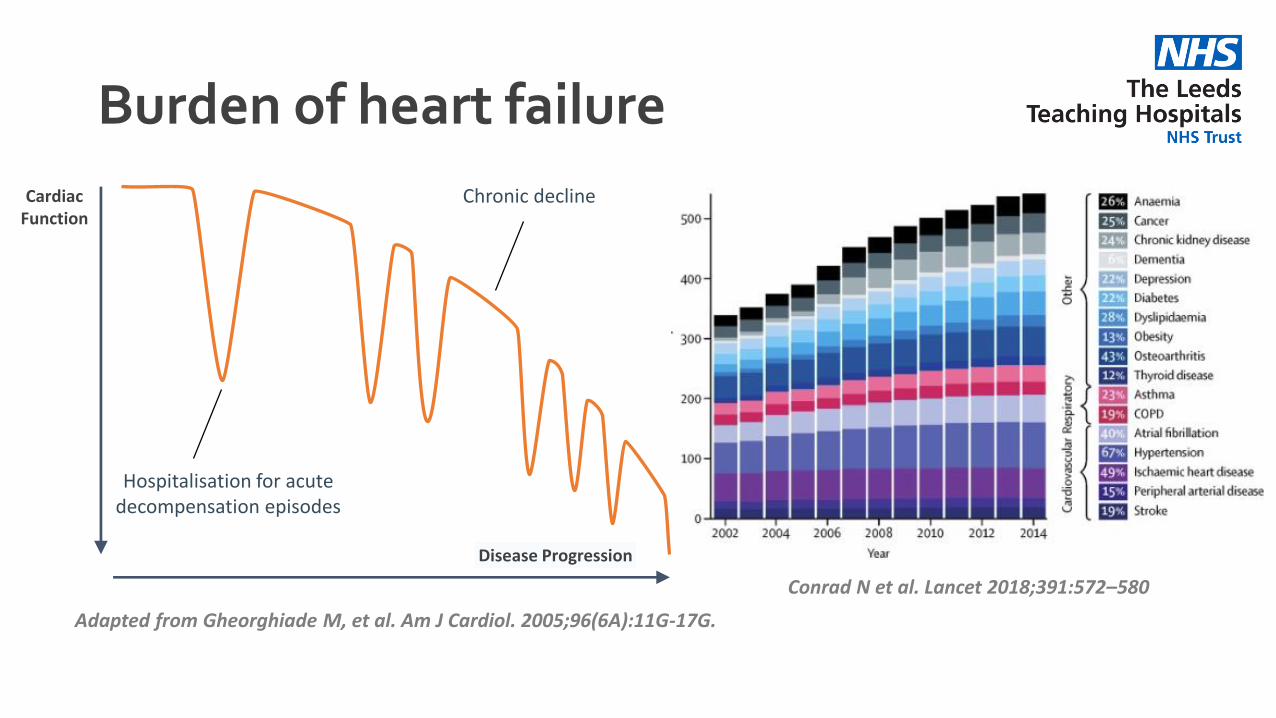
Burden of heart failure
Adapted from Gheorghiade M, et al. Am J Cardiol. 2005;96(6A):11G-17G.
Disease Progression
Cardiac Function
Chronic decline
Hospitalisation for acutedecompensation episodes
Conrad N et al. Lancet 2018;391:572–580
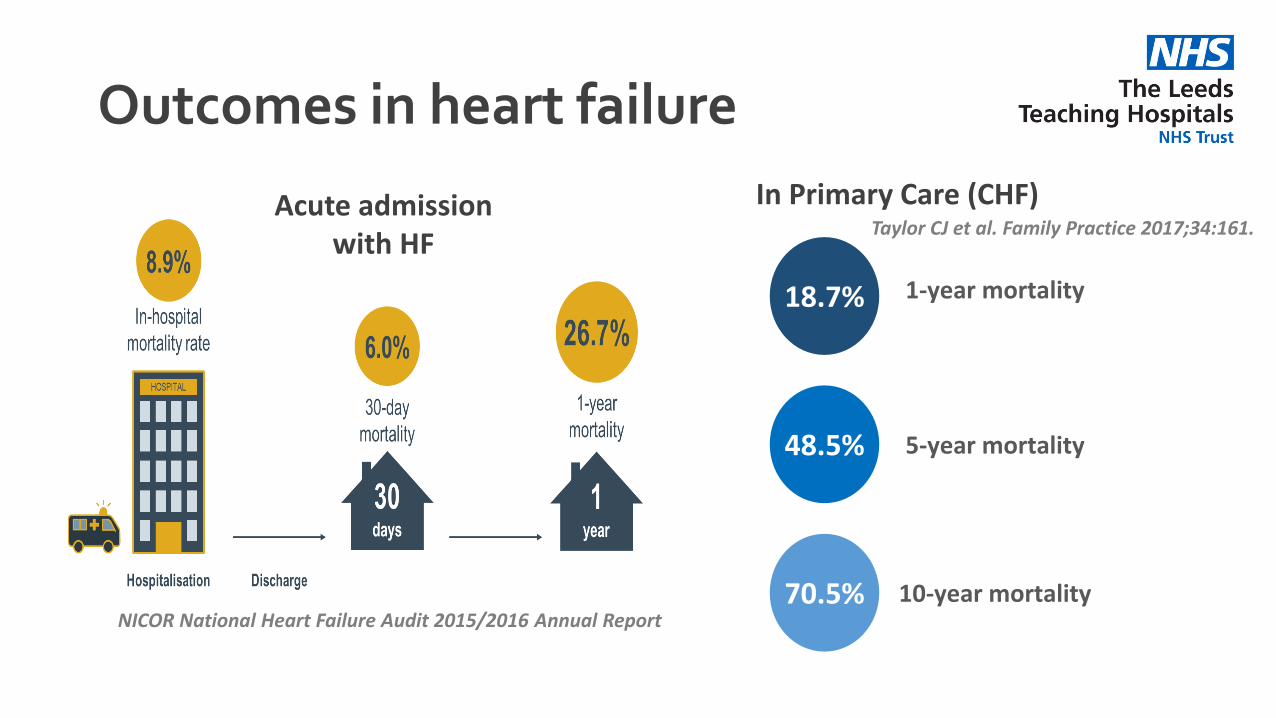
Outcomes in heart failure
Acute admission with HF
NICOR National Heart Failure Audit 2015/2016 Annual Report
18.7% 1-year mortality
70.5%
48.5%
10-year mortality
5-year mortality
In Primary Care (CHF)Taylor CJ et al. Family Practice 2017;34:161.
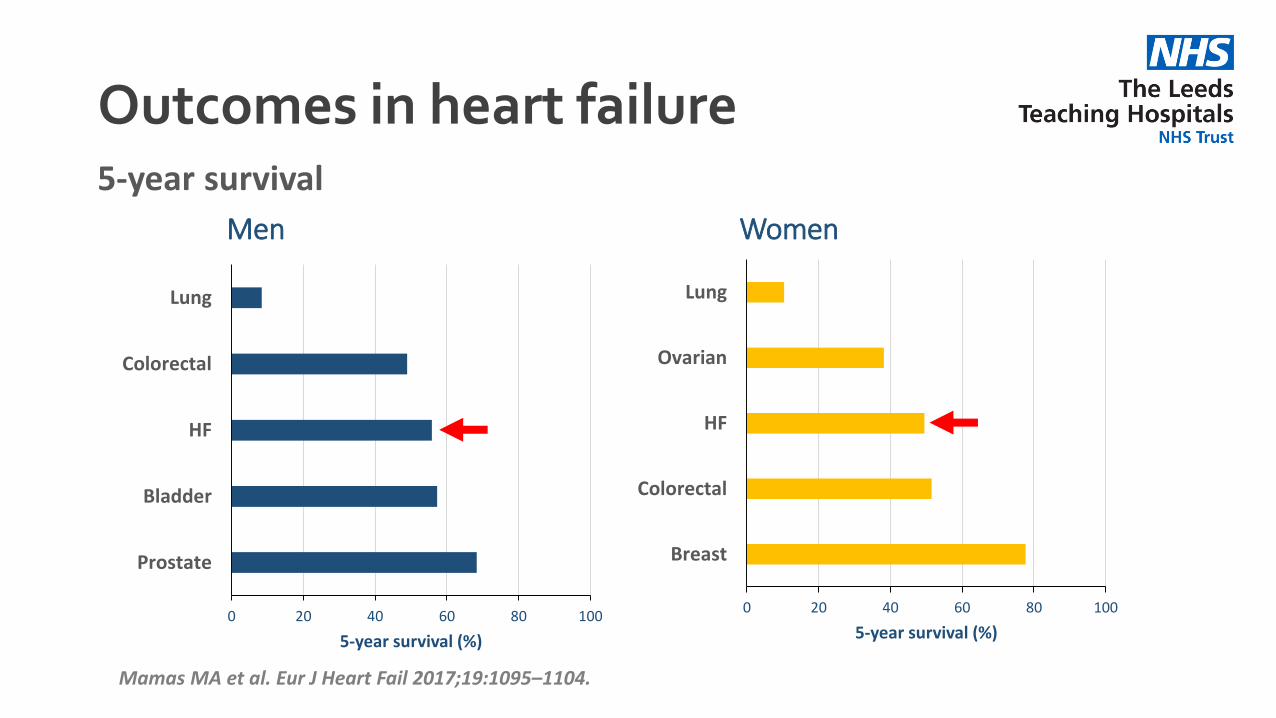
Outcomes in heart failure
0 20 40 60 80 100
Prostate
Bladder
HF
Colorectal
Lung
5-year survival (%)
Men
0 20 40 60 80 100
Breast
Colorectal
HF
Ovarian
Lung
5-year survival (%)
Women
Mamas MA et al. Eur J Heart Fail 2017;19:1095–1104.
5-year survival
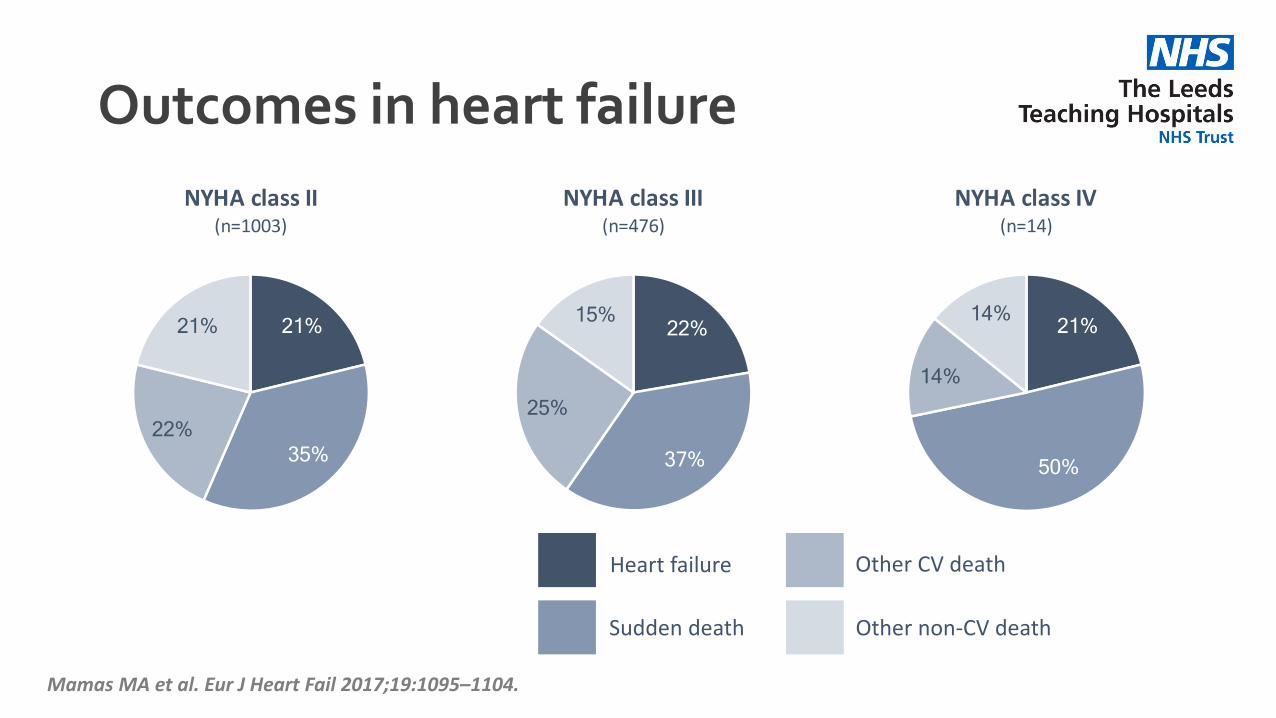
Outcomes in heart failure
Mamas MA et al. Eur J Heart Fail 2017;19:1095–1104.
Heart failure
Sudden death
Other CV death
Other non-CV death
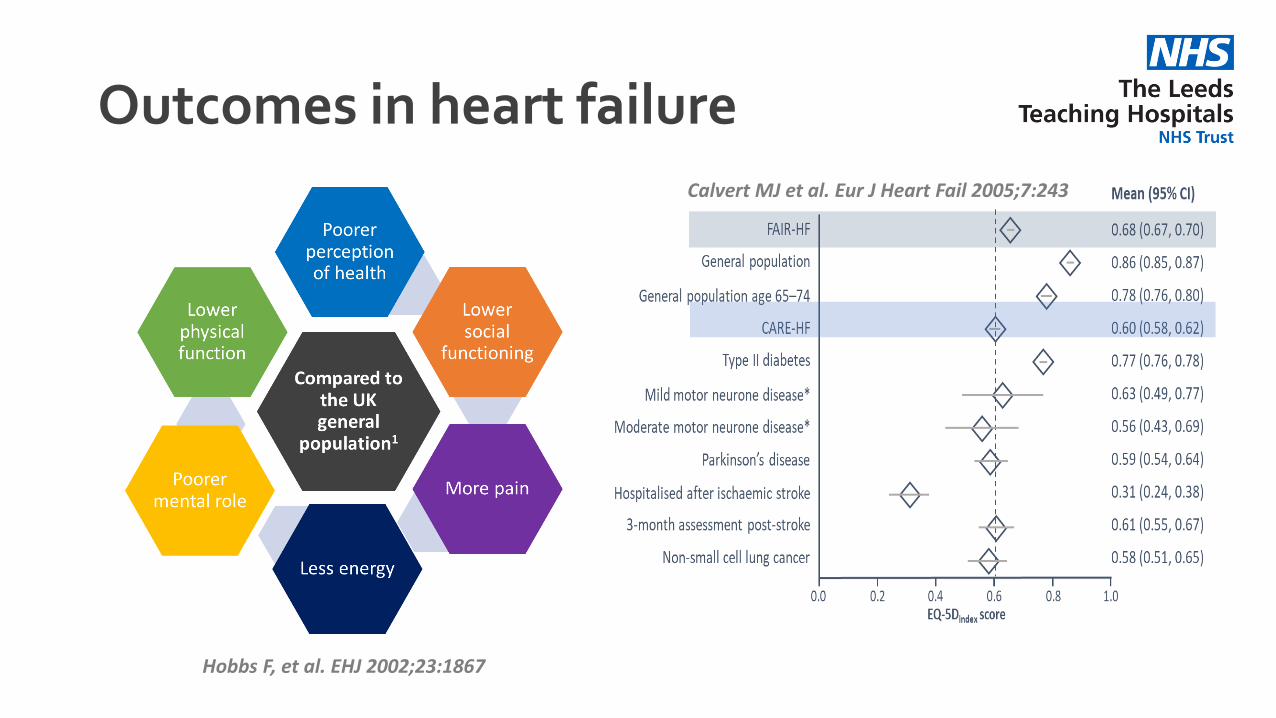
Outcomes in heart failure
Hobbs F, et al. EHJ 2002;23:1867
Calvert MJ et al. Eur J Heart Fail 2005;7:243
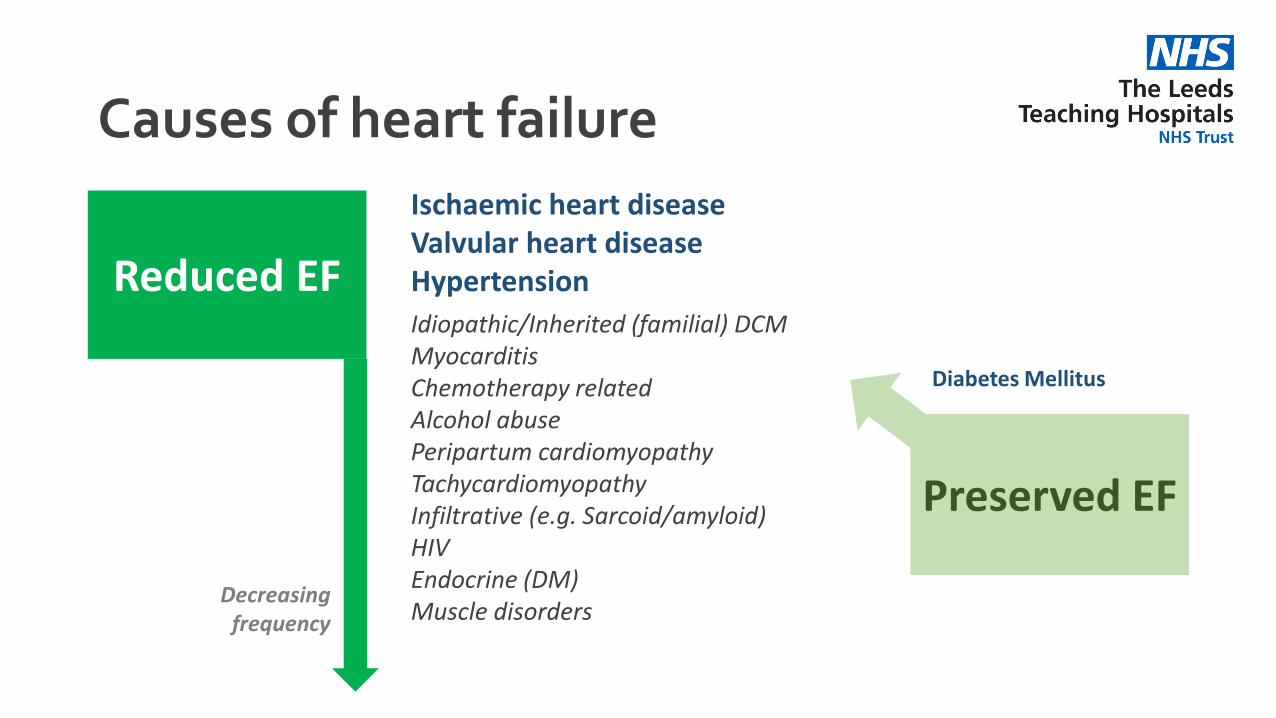
Causes of heart failure
Ischaemic heart diseaseValvular heart diseaseHypertension
Idiopathic/Inherited (familial) DCMMyocarditisChemotherapy relatedAlcohol abusePeripartum cardiomyopathyTachycardiomyopathyInfiltrative (e.g. Sarcoid/amyloid)HIVEndocrine (DM)Muscle disorders
Reduced EF
Decreasing frequency
Preserved EF
Diabetes Mellitus
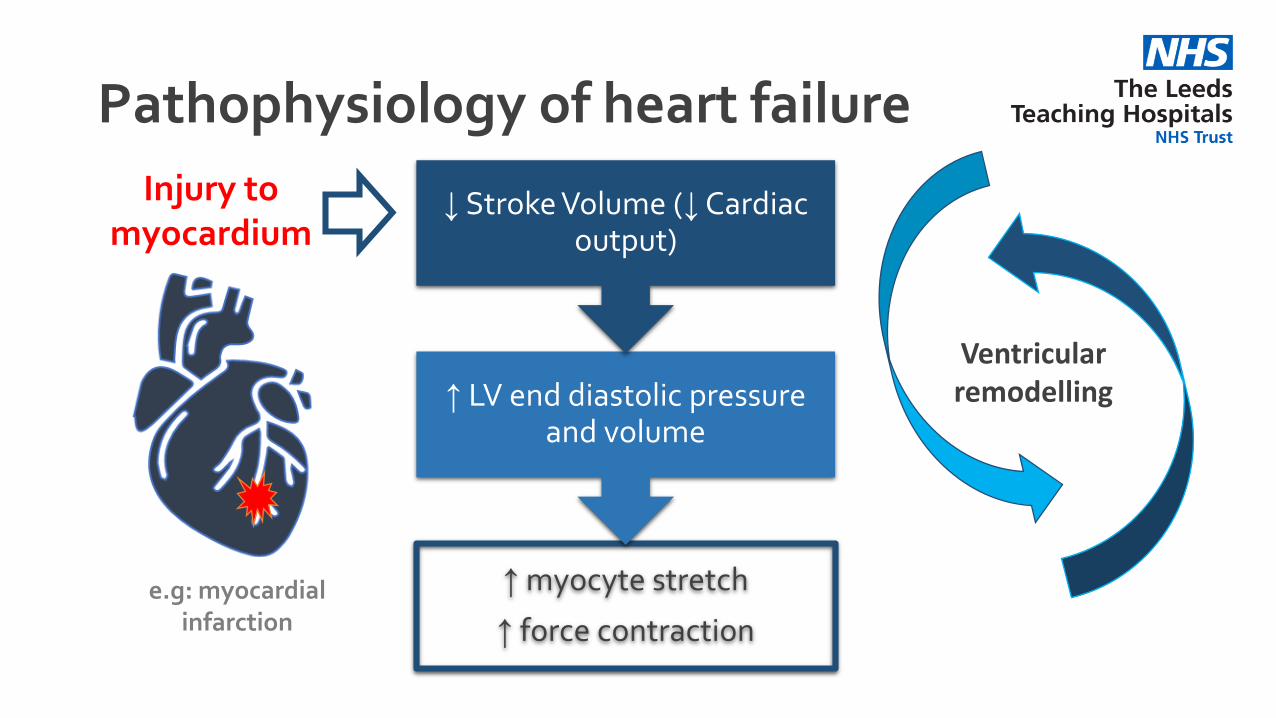
Pathophysiology of heart failure
Injury to myocardium
e.g: myocardial infarction
↑ myocyte stretch
↑ force contraction
↑ LV end diastolic pressure and volume
↓ Stroke Volume (↓Cardiac output)
Ventricular remodelling
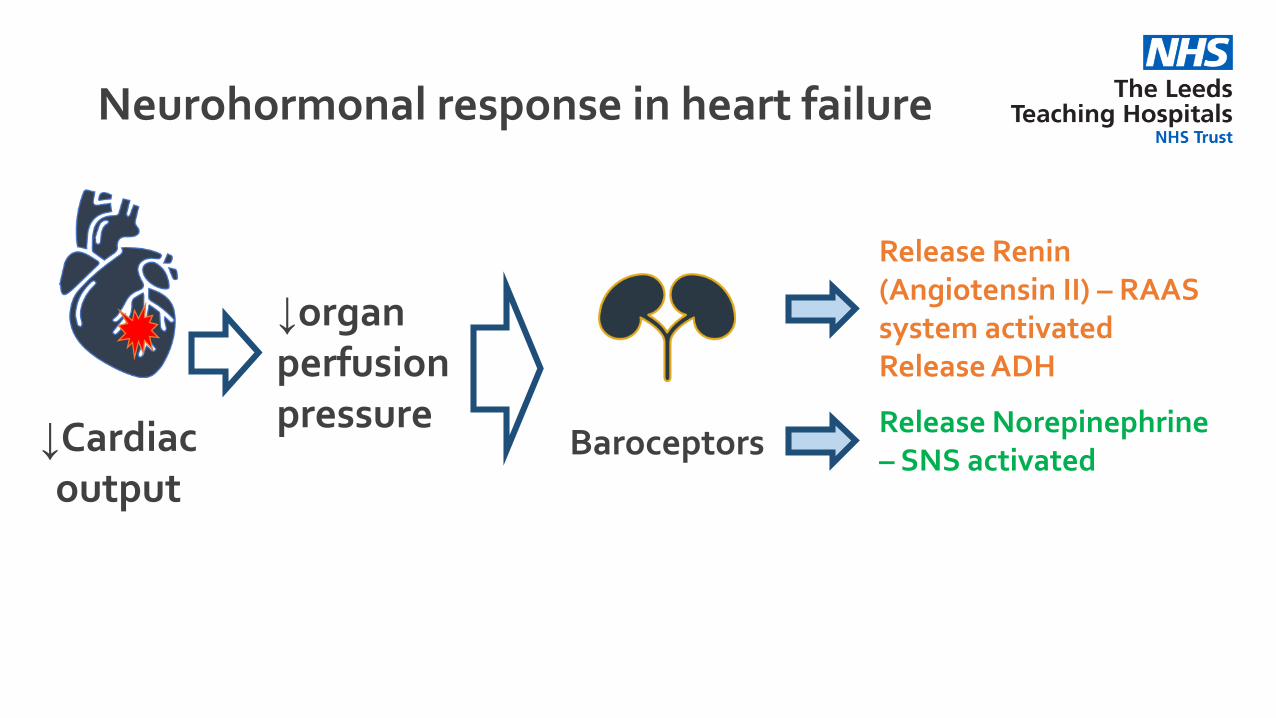
Neurohormonal response in heart failure
↓Cardiac output
↓organ perfusion pressure
Baroceptors
Release Renin (Angiotensin II) – RAAS system activatedRelease ADH
Release Norepinephrine – SNS activated
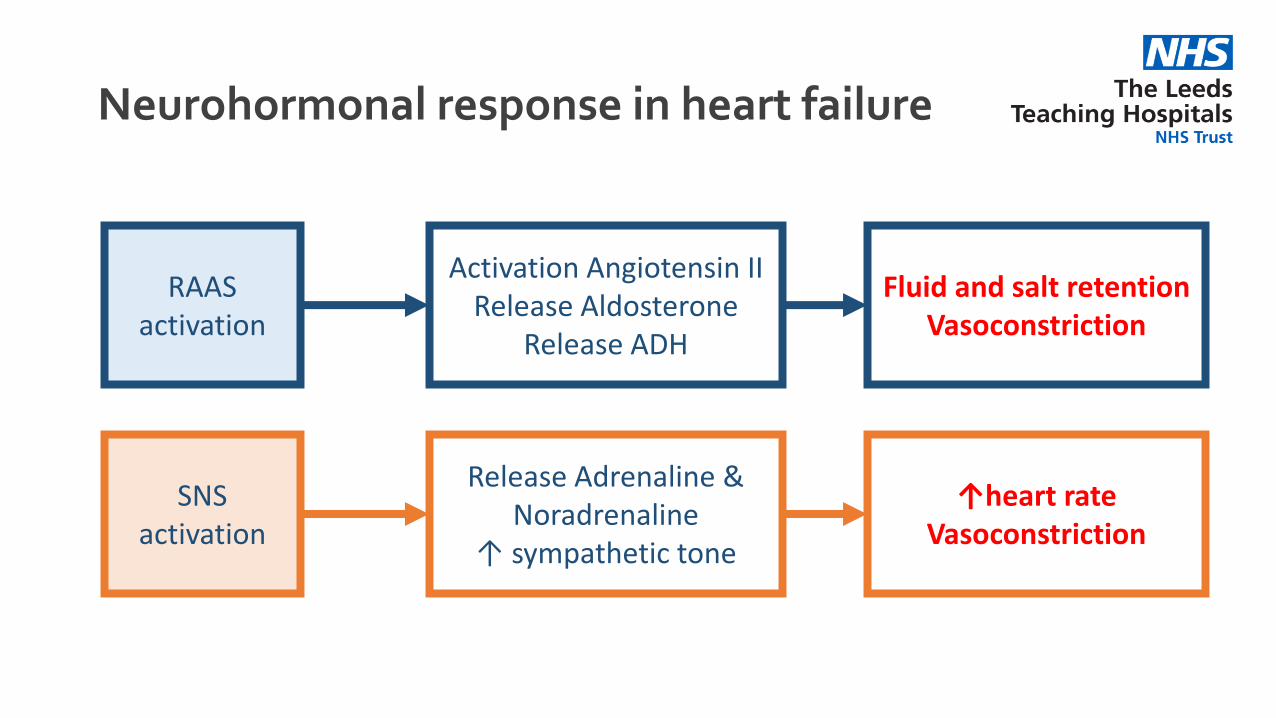
Neurohormonal response in heart failure
RAAS activation
Activation Angiotensin IIRelease Aldosterone
Release ADH
Fluid and salt retentionVasoconstriction
SNS activation
Release Adrenaline & Noradrenaline
↑ sympathetic tone
↑heart rateVasoconstriction
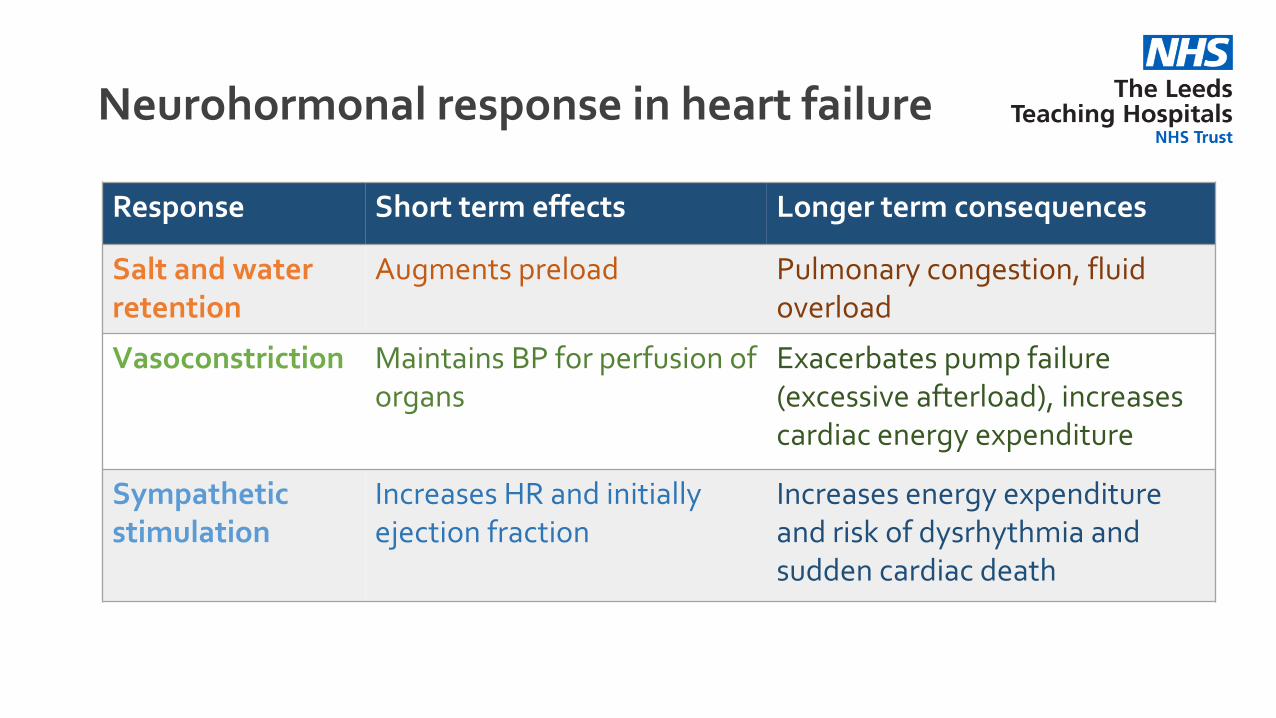
Neurohormonal response in heart failure
Response Short term effects Longer term consequences
Salt and water retention
Augments preload Pulmonary congestion, fluid overload
Vasoconstriction Maintains BP for perfusion of organs
Exacerbates pump failure (excessive afterload), increases cardiac energy expenditure
Sympathetic stimulation
Increases HR and initially ejection fraction
Increases energy expenditureand risk of dysrhythmia and sudden cardiac death
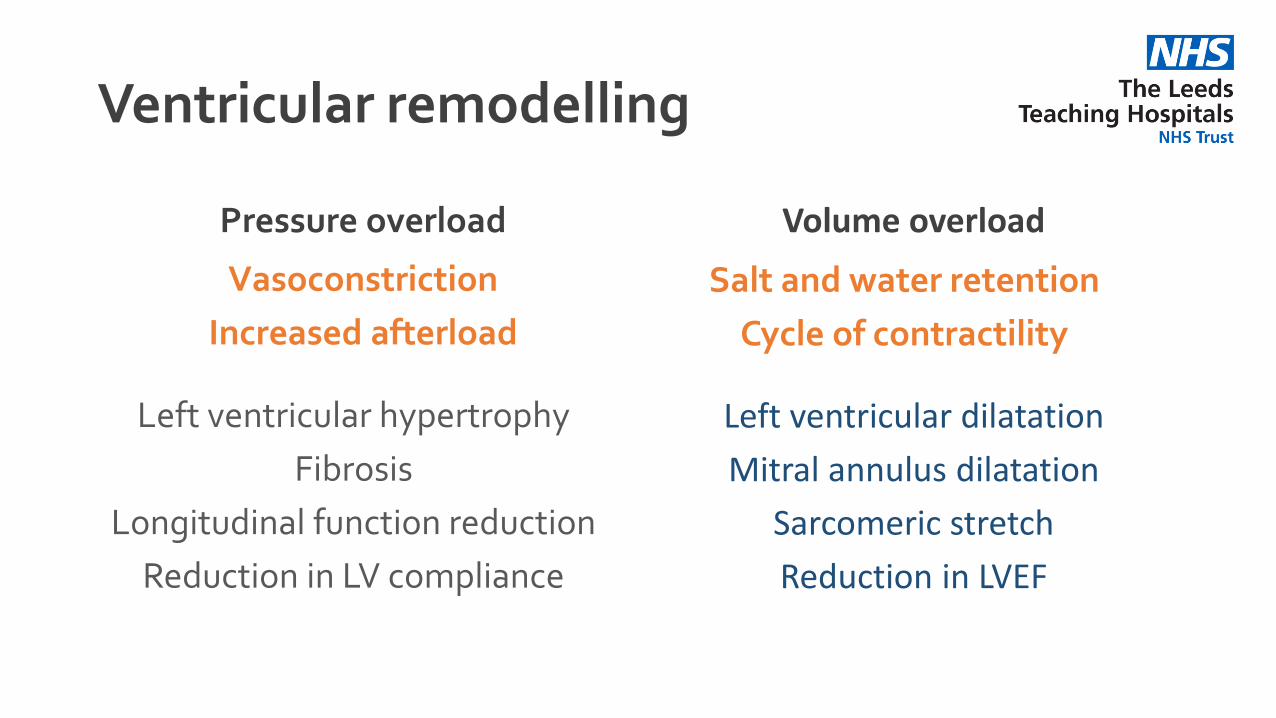
Pressure overload
Left ventricular hypertrophy
Fibrosis
Longitudinal function reduction
Reduction in LV compliance
Volume overload
Left ventricular dilatation
Mitral annulus dilatation
Sarcomeric stretch
Reduction in LVEF
Ventricular remodelling
Vasoconstriction
Increased afterload
Salt and water retention
Cycle of contractility
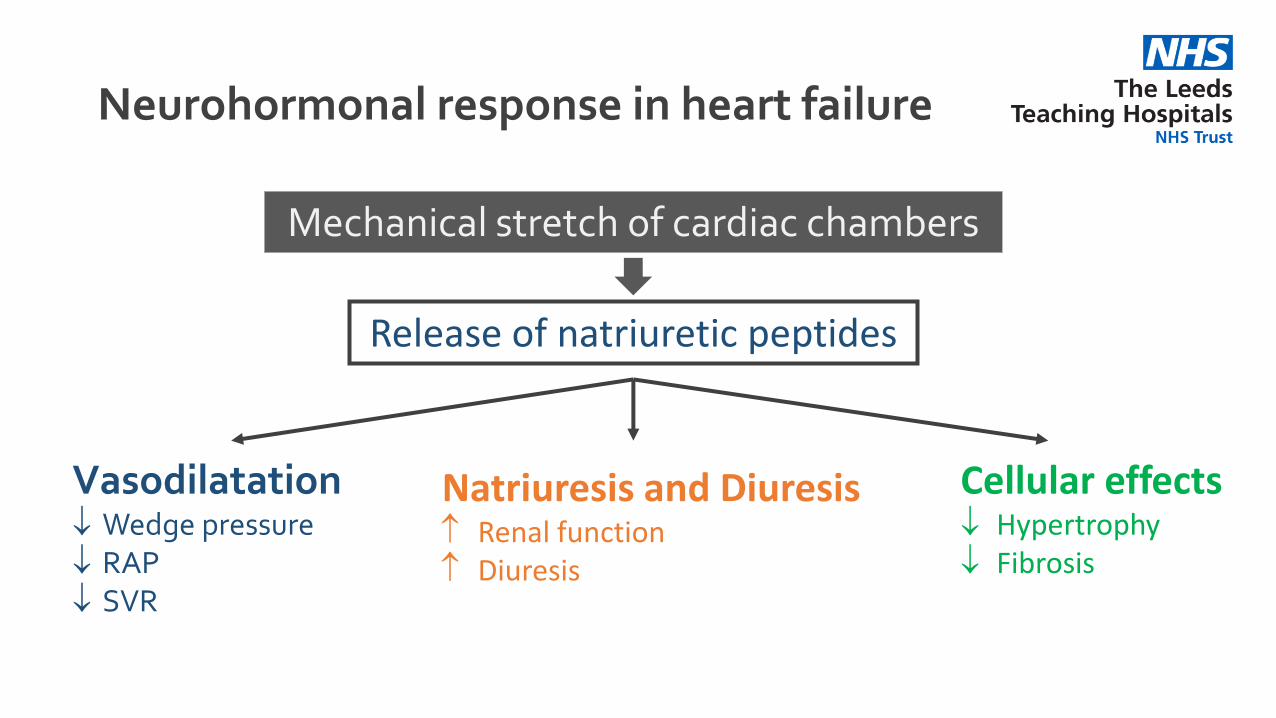
Neurohormonal response in heart failure
Mechanical stretch of cardiac chambers
Release of natriuretic peptides
Vasodilatation Wedge pressure RAP SVR
Natriuresis and Diuresis Renal function Diuresis
Cellular effects Hypertrophy Fibrosis
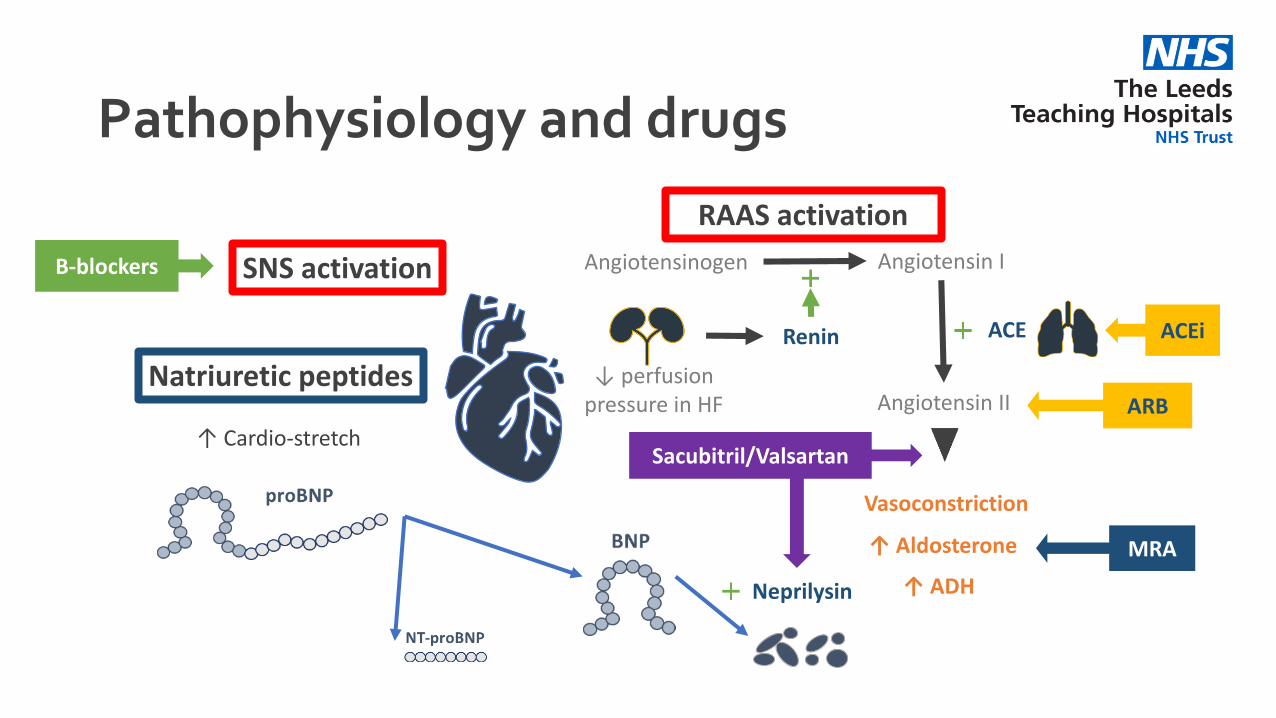
Pathophysiology and drugs
↓ perfusion pressure in HF
Renin
Angiotensinogen Angiotensin I
Angiotensin II
ACE
Vasoconstriction
↑ Aldosterone
↑ ADH
RAAS activation
SNS activation
Natriuretic peptides
↑ Cardio-stretch
Neprilysin
Β-blockers
ACEi
ARB
MRA
Sacubitril/Valsartan
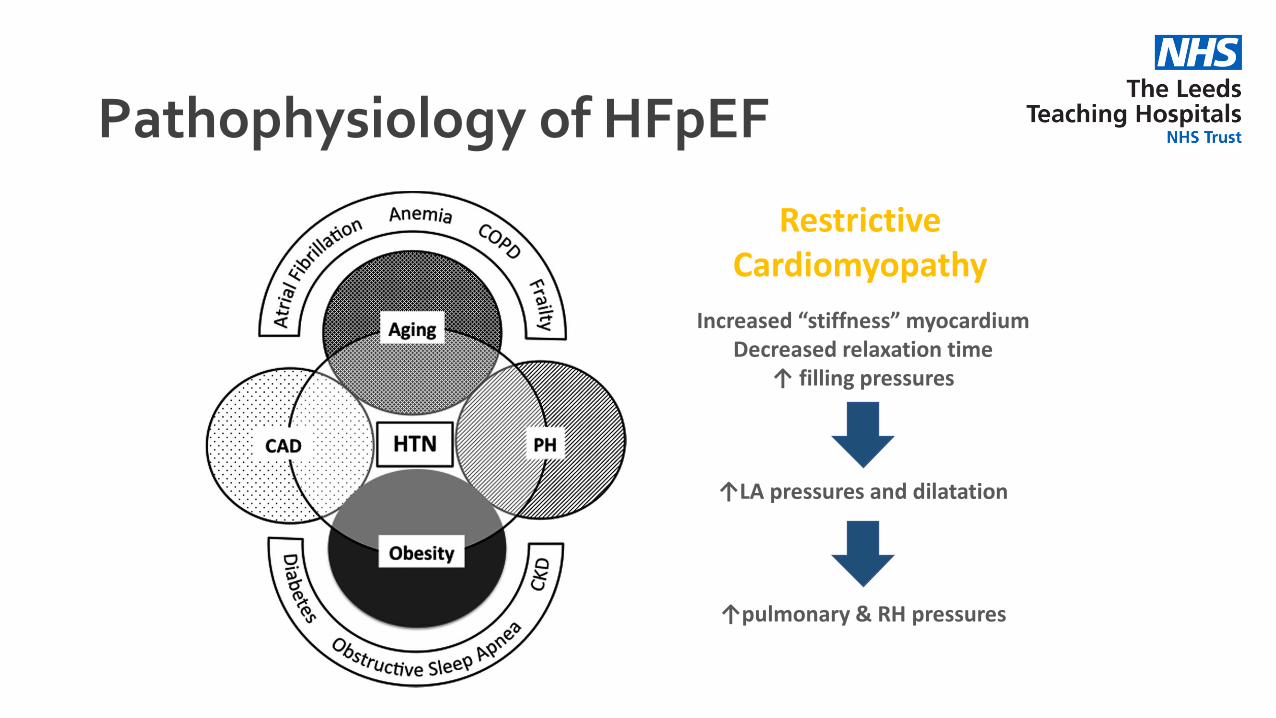
Pathophysiology of HFpEF
Increased “stiffness” myocardiumDecreased relaxation time
↑ filling pressures
↑LA pressures and dilatation
↑pulmonary & RH pressures
Restrictive Cardiomyopathy
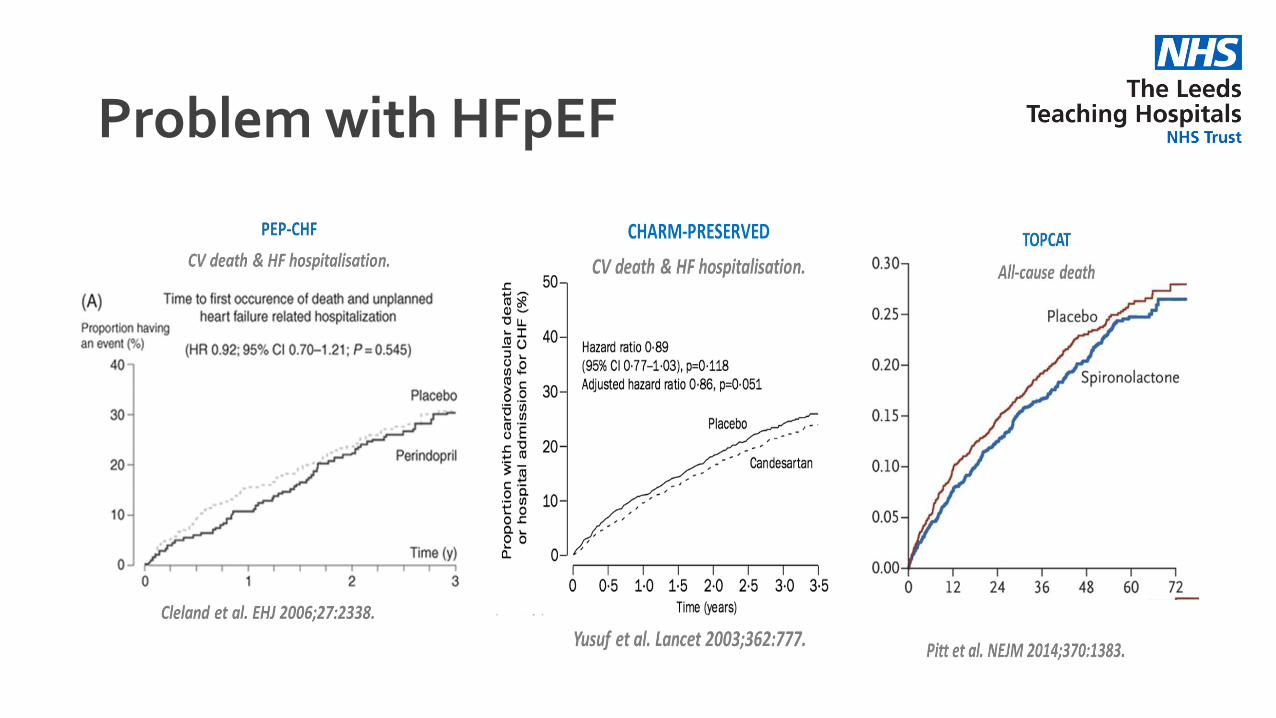
Problem with HFpEF

The Medical Registrar
What you need to know about HF
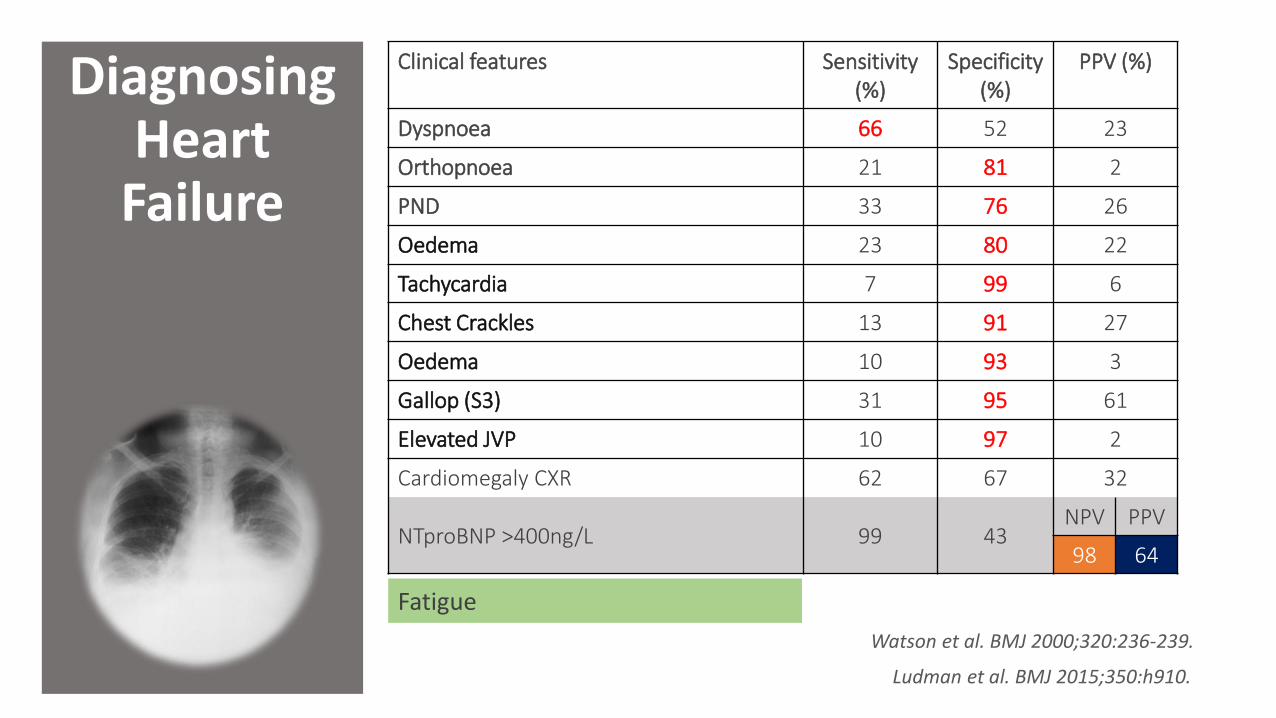
Diagnosing Heart
Failure
Clinical features Sensitivity (%)
Specificity (%)
PPV (%)
Dyspnoea 66 52 23
Orthopnoea 21 81 2
PND 33 76 26
Oedema 23 80 22
Tachycardia 7 99 6
Chest Crackles 13 91 27
Oedema 10 93 3
Gallop (S3) 31 95 61
Elevated JVP 10 97 2
Cardiomegaly CXR 62 67 32
NTproBNP >400ng/L 99 43NPV PPV
98 64
Watson et al. BMJ 2000;320:236-239.
Ludman et al. BMJ 2015;350:h910.
Fatigue
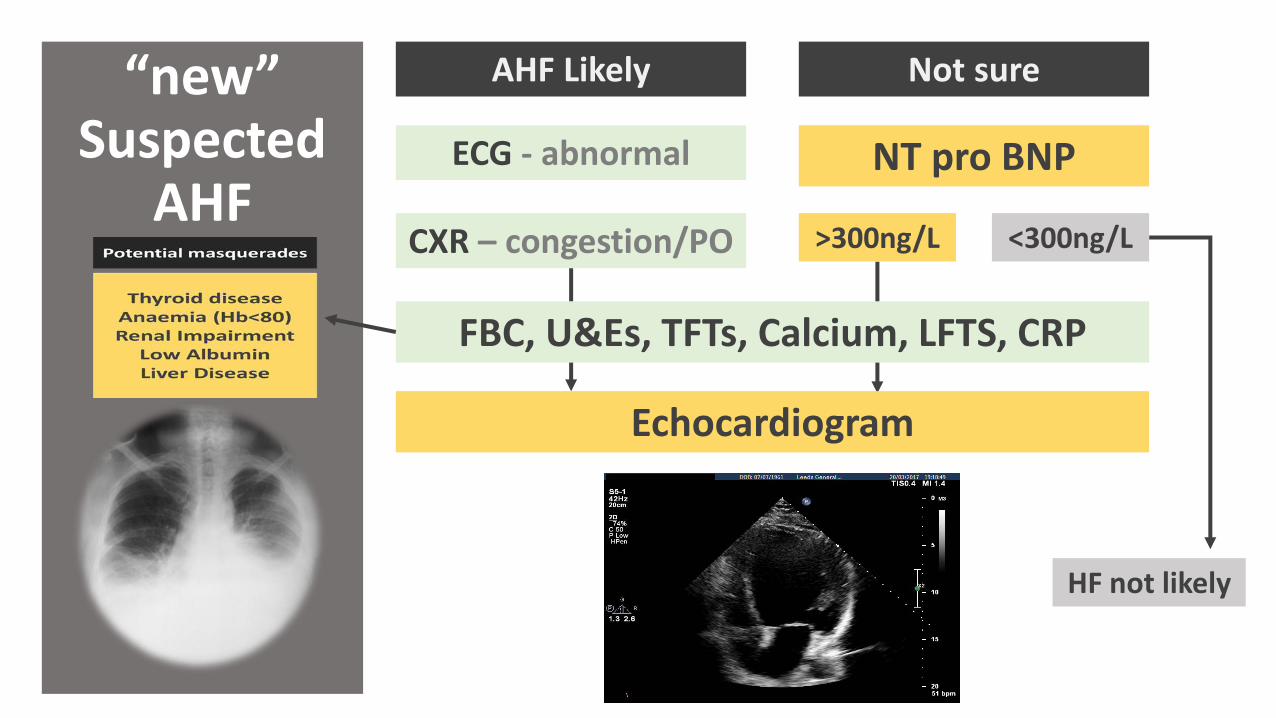
“new” Suspected
AHFECG - abnormal
CXR – congestion/PO
NT pro BNP
FBC, U&Es, TFTs, Calcium, LFTS, CRP
Echocardiogram
AHF Likely Not sure
<300ng/L>300ng/L
HF not likely
Suspected “new” AHF
NICE Quality Standards for AHF 2015
1. Adults PC new suspected acute heart failure have a single measurement of NT pro BNP.
2. Adults suspected acute heart failure and NT pro BNP have ECHO <48 hours of admission.
3. Adults with AHF have input <24 hours of admission from a dedicated specialist heart failure team.
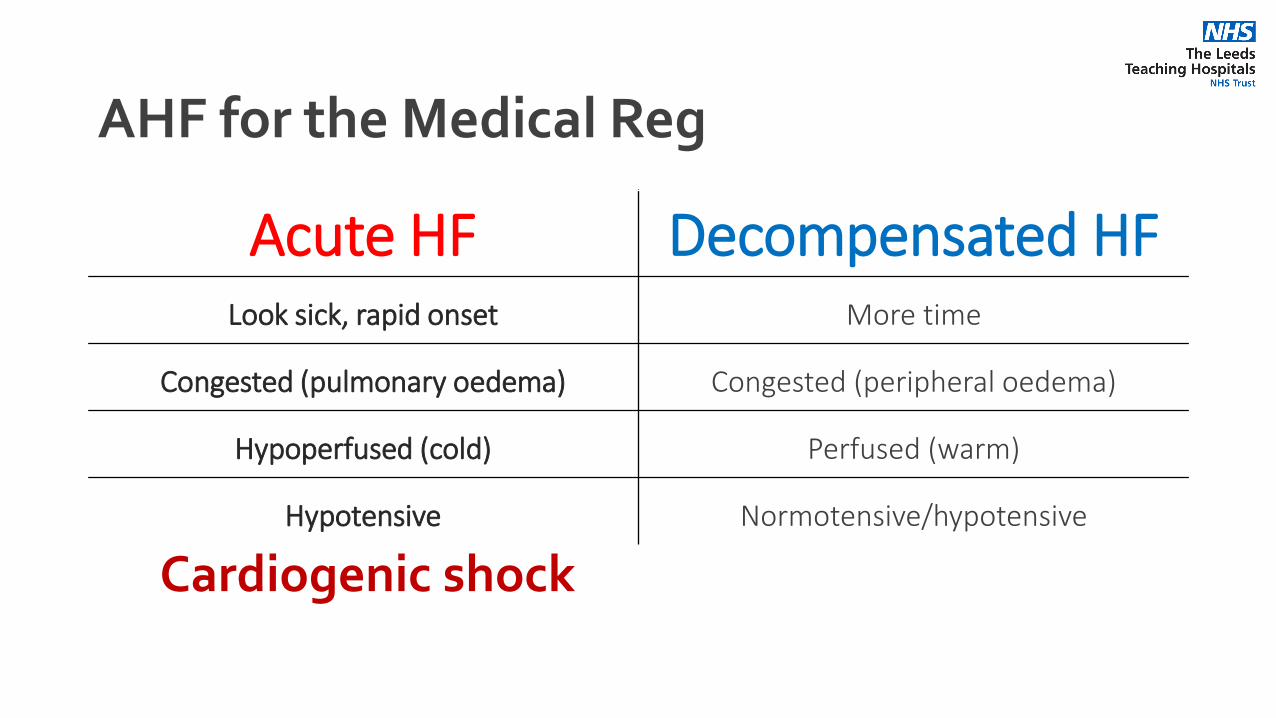
AHF for the Medical Reg
Acute HF Decompensated HFLook sick, rapid onset More time
Congested (pulmonary oedema) Congested (peripheral oedema)
Hypoperfused (cold) Perfused (warm)
Hypotensive Normotensive/hypotensive
Cardiogenic shock
Managing Cardiogenic shock

Buying time to recover
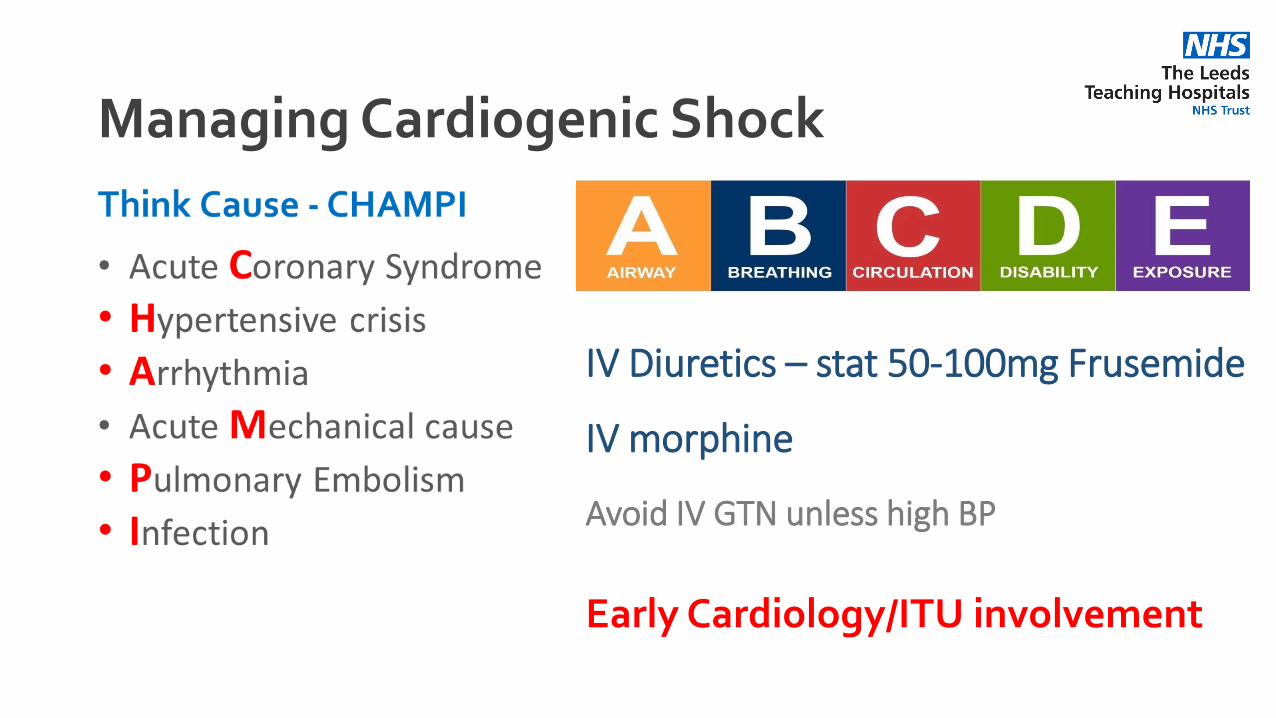
Managing Cardiogenic Shock
IV Diuretics – stat 50-100mg Frusemide
IV morphine
Avoid IV GTN unless high BP
Early Cardiology/ITU involvement
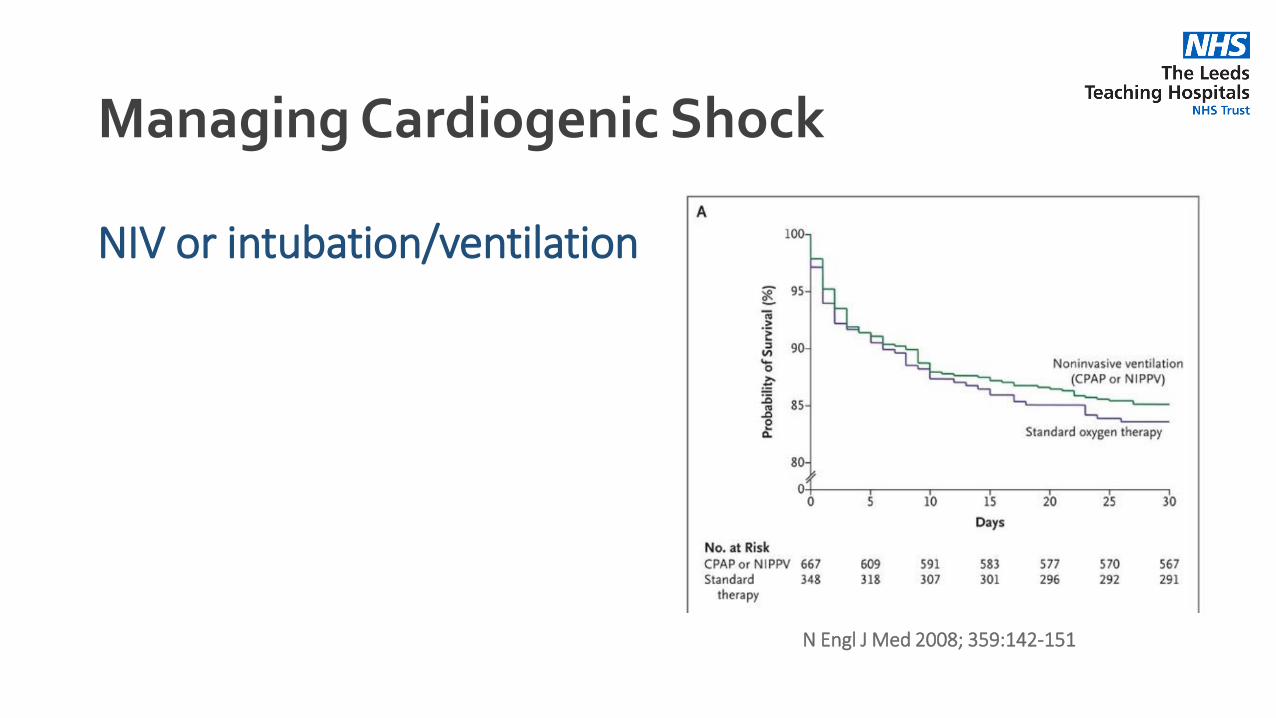
Managing Cardiogenic Shock
NIV or intubation/ventilation
N Engl J Med 2008; 359:142-151
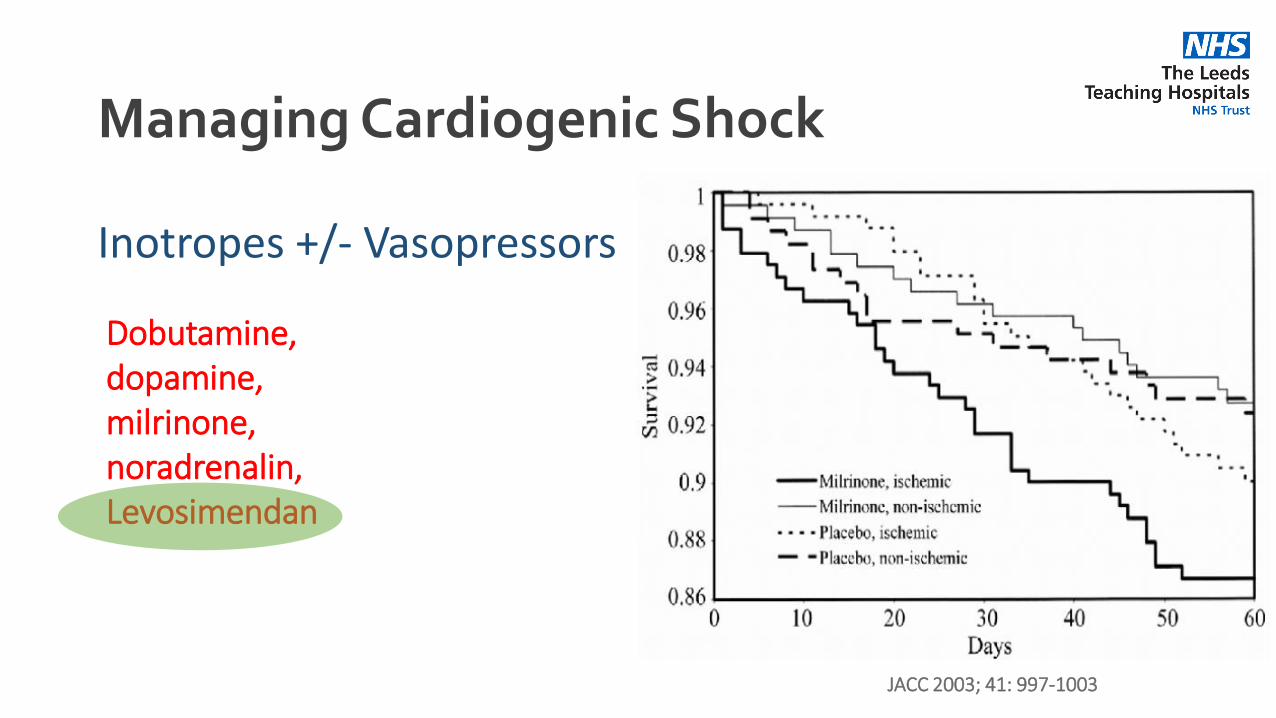
Managing Cardiogenic Shock
Inotropes +/- Vasopressors
Dobutamine, dopamine, milrinone, noradrenalin, Levosimendan
JACC 2003; 41: 997-1003
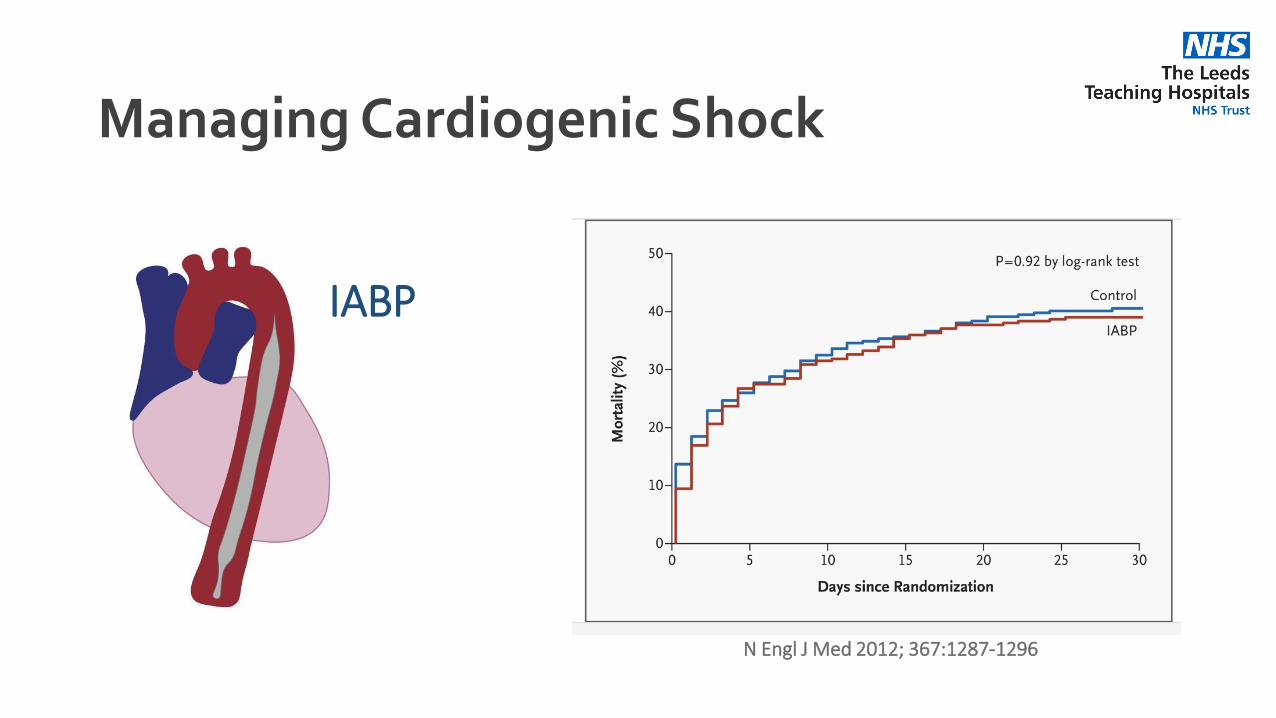
Managing Cardiogenic Shock
IABP
N Engl J Med 2012; 367:1287-1296
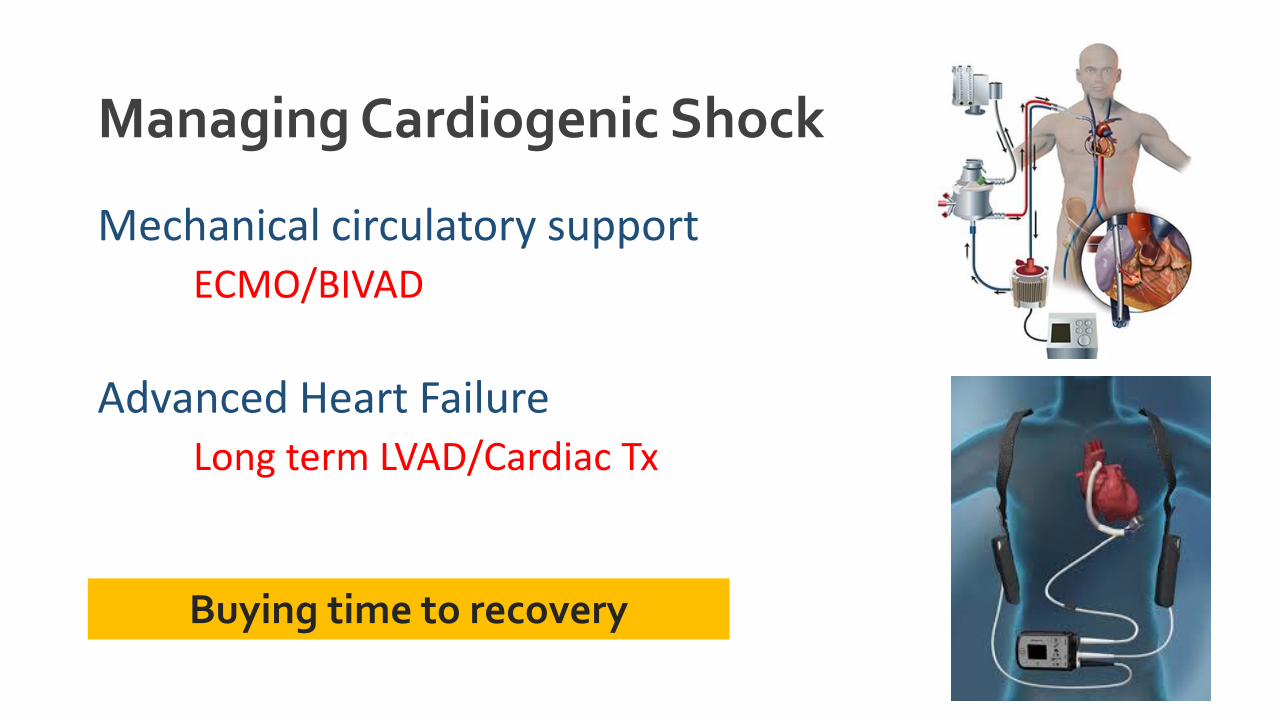
Managing Cardiogenic Shock
Mechanical circulatory supportECMO/BIVAD
Advanced Heart FailureLong term LVAD/Cardiac Tx
Buying time to recovery
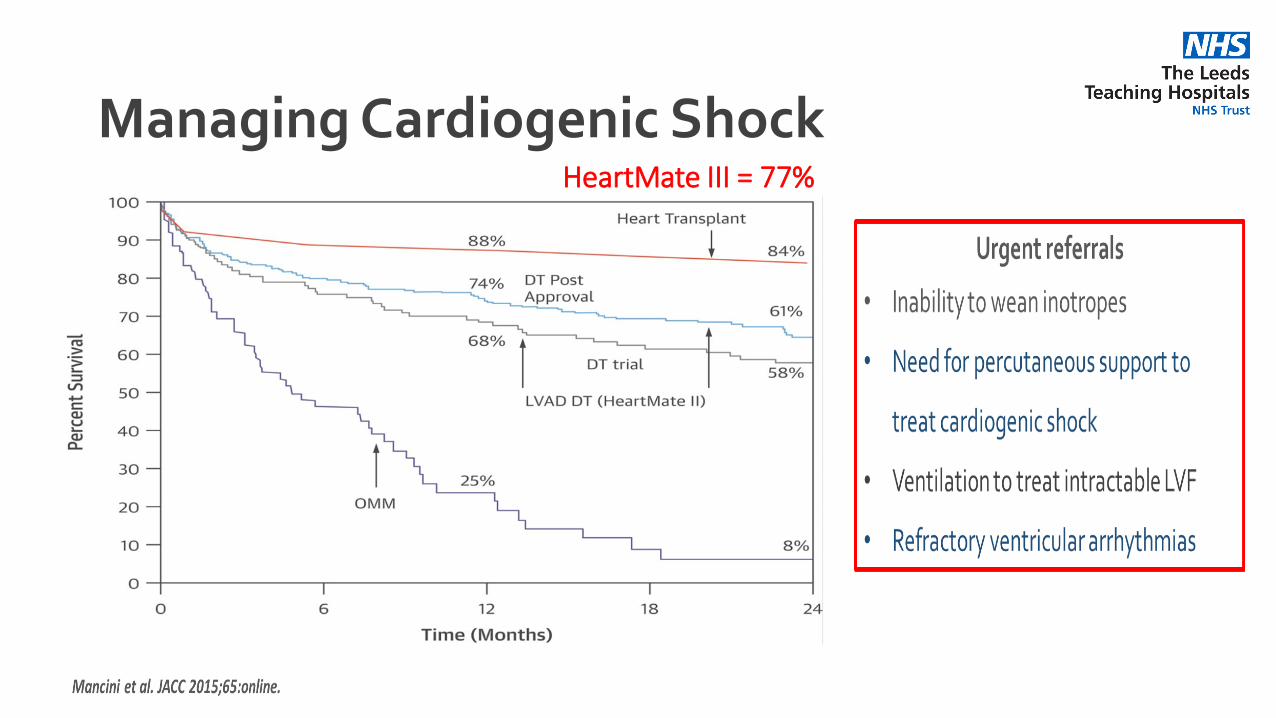
Managing Cardiogenic ShockHeartMate III = 77%

Managing Decompensated HF
Most patients ~90%

Treatment Goals
1. Improve symptoms and QoL2. Avoid hospitalisations and decompensations3. Improve prognosis/outcomes
Managing Decompensated HF
Decongest (diuretics)
Optimise treatments
Appropriate care
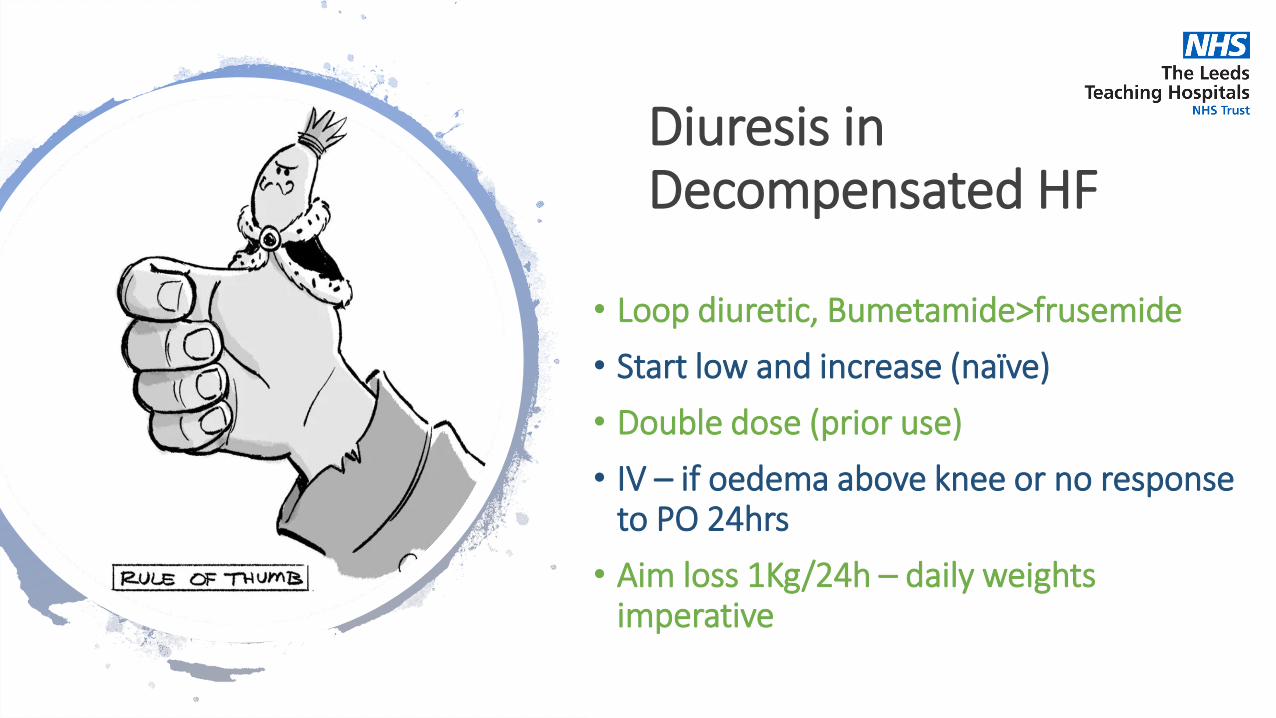
Diuresis in Decompensated HF
• Loop diuretic, Bumetamide>frusemide
• Start low and increase (naïve)
• Double dose (prior use)
• IV – if oedema above knee or no response to PO 24hrs
• Aim loss 1Kg/24h – daily weights imperative
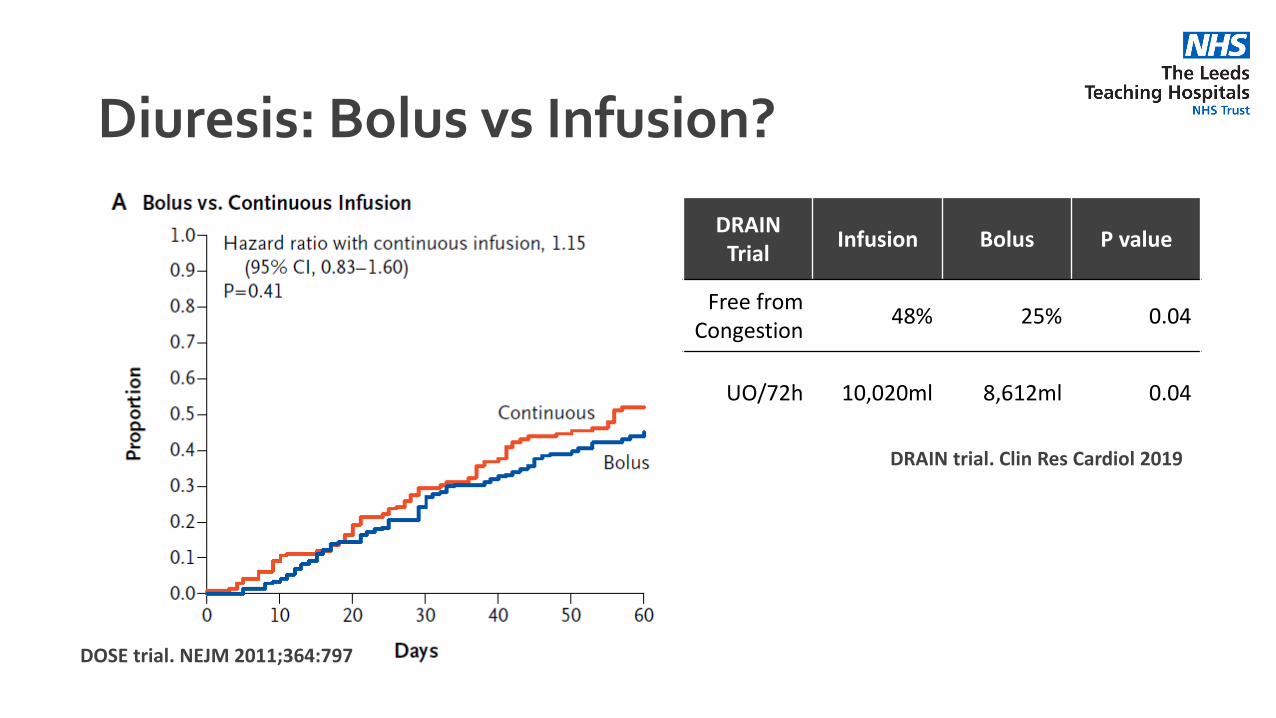
Diuresis: Bolus vs Infusion?
DOSE trial. NEJM 2011;364:797
DRAIN Trial
Infusion Bolus P value
Free from Congestion
48% 25% 0.04
UO/72h 10,020ml 8,612ml 0.04
DRAIN trial. Clin Res Cardiol 2019
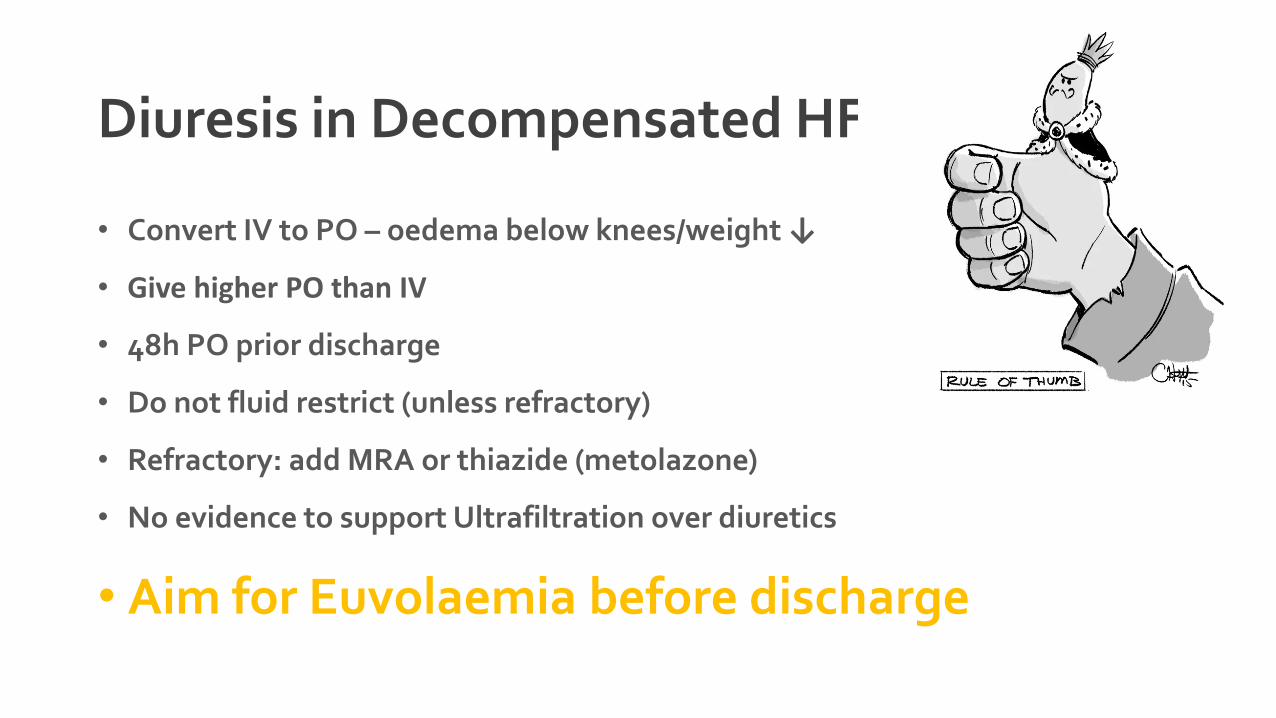
Diuresis in Decompensated HF
• Convert IV to PO – oedema below knees/weight ↓
• Give higher PO than IV
• 48h PO prior discharge
• Do not fluid restrict (unless refractory)
• Refractory: add MRA or thiazide (metolazone)
• No evidence to support Ultrafiltration over diuretics
• Aim for Euvolaemia before discharge
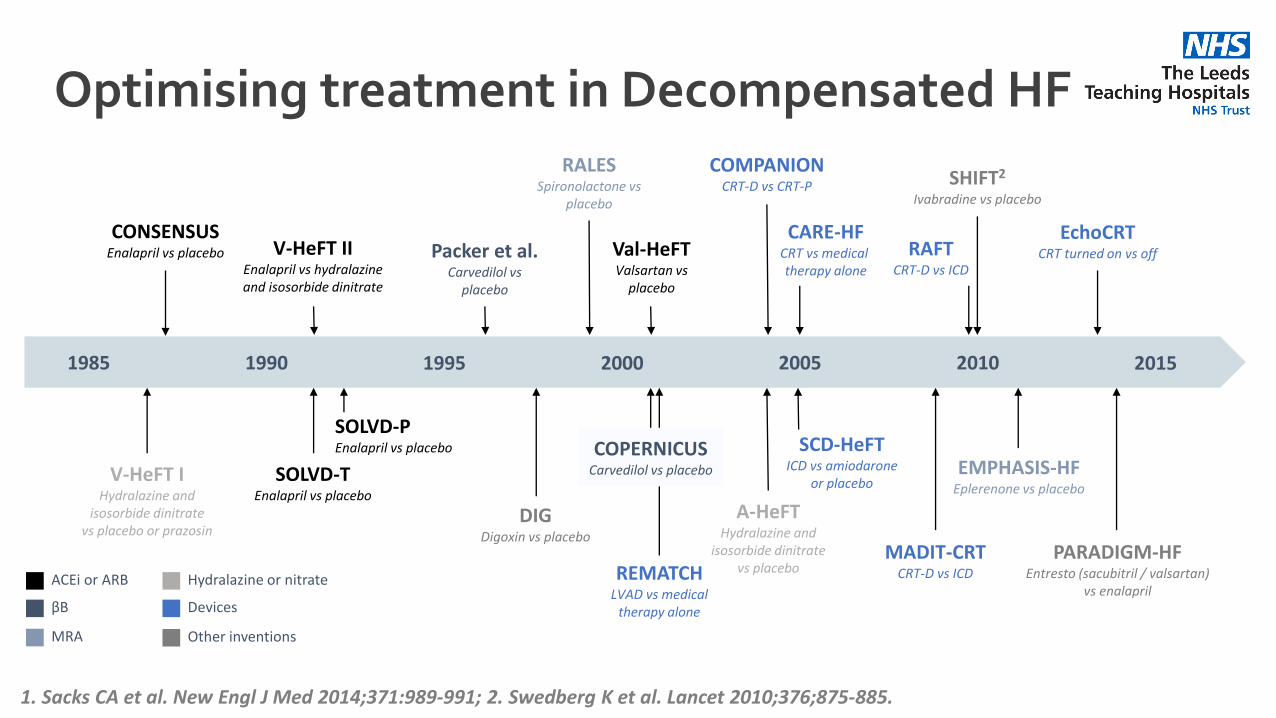
1985 1990 1995 2000 2005 2010 2015
V-HeFT IHydralazine and
isosorbide dinitratevs placebo or prazosin
CONSENSUSEnalapril vs placebo V-HeFT II
Enalapril vs hydralazineand isosorbide dinitrate
SOLVD-TEnalapril vs placebo
SOLVD-PEnalapril vs placebo
Packer et al.Carvedilol vs
placebo
DIGDigoxin vs placebo
RALESSpironolactone vs
placebo
Val-HeFTValsartan vs
placebo
REMATCHLVAD vs medical
therapy alone
COPERNICUSCarvedilol vs placebo
COMPANIONCRT-D vs CRT-P
A-HeFTHydralazine and
isosorbide dinitratevs placebo
CARE-HFCRT vs medical therapy alone
SCD-HeFTICD vs amiodarone
or placebo
SHIFT2
Ivabradine vs placebo
MADIT-CRTCRT-D vs ICD
PARADIGM-HFEntresto (sacubitril / valsartan)
vs enalapril
EMPHASIS-HFEplerenone vs placebo
RAFTCRT-D vs ICD
EchoCRTCRT turned on vs off
ACEi or ARB Hydralazine or nitrate
βB
MRA
Devices
Other inventions
1. Sacks CA et al. New Engl J Med 2014;371:989-991; 2. Swedberg K et al. Lancet 2010;376;875-885.
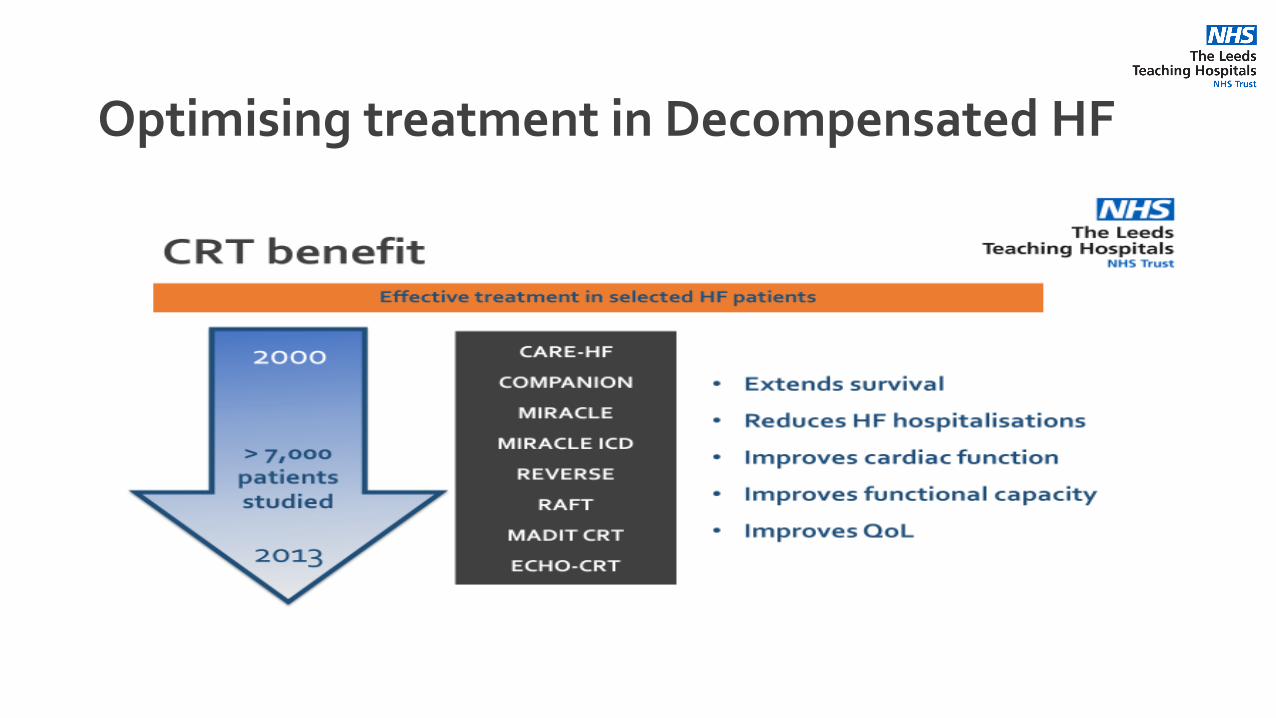
Optimising treatment in Decompensated HF
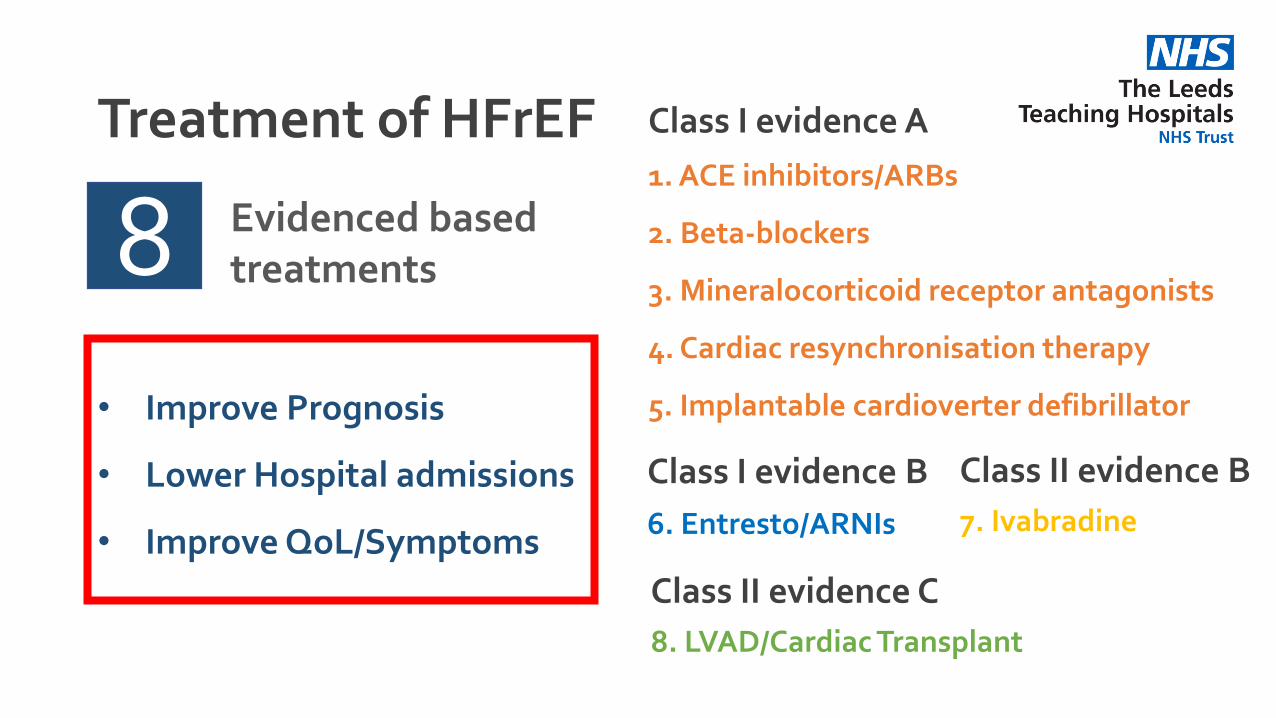
Treatment of HFrEF
81. ACE inhibitors/ARBs
2. Beta-blockers
3. Mineralocorticoid receptor antagonists
4. Cardiac resynchronisation therapy
5. Implantable cardioverter defibrillator
Class I evidence A
Class I evidence B
6. Entresto/ARNIs
Class II evidence B
7. Ivabradine
Class II evidence C
8. LVAD/Cardiac Transplant
Evidenced based treatments
• Improve Prognosis
• Lower Hospital admissions
• Improve QoL/Symptoms
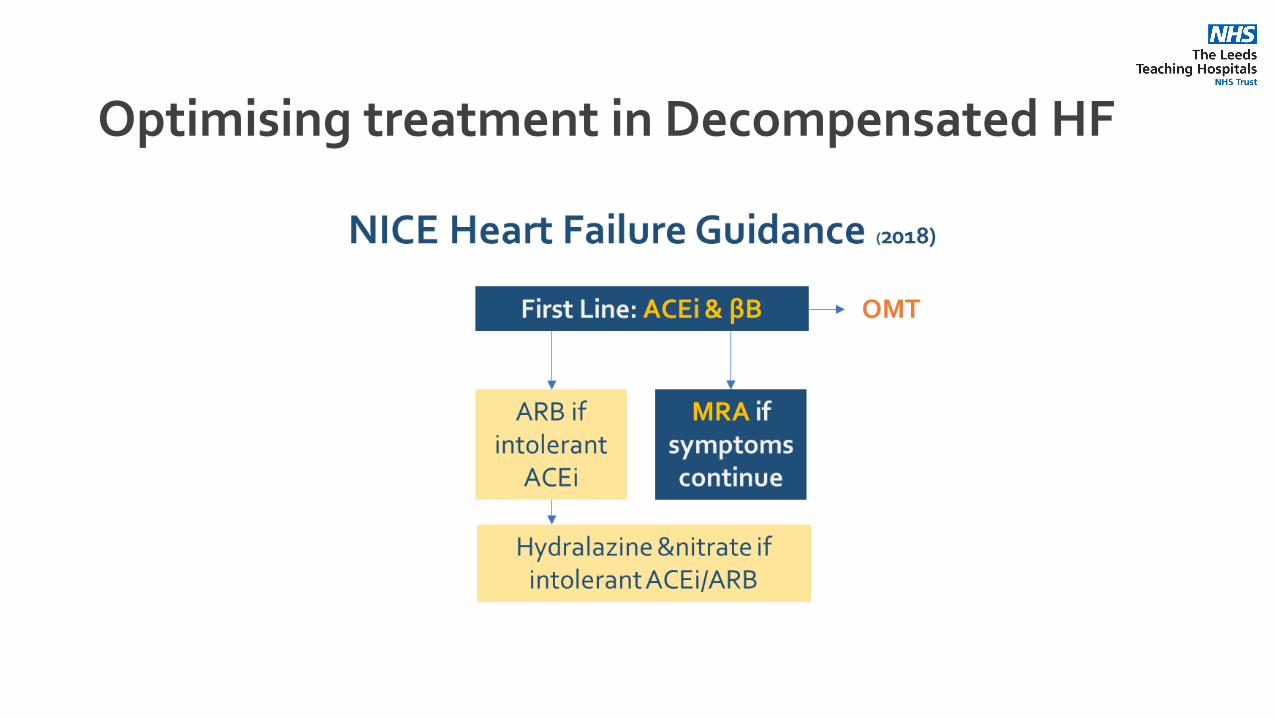
Optimising treatment in Decompensated HF
Optimising treatment in Decompensated HF
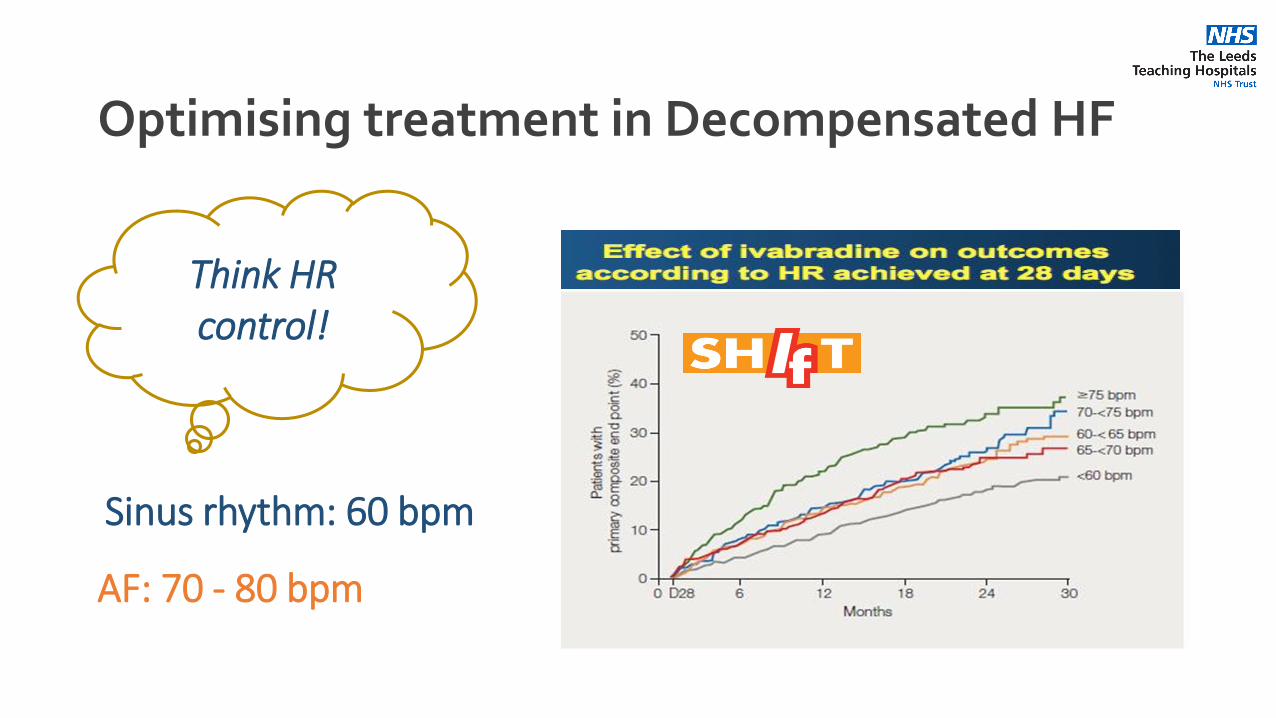
Think HR control!
Sinus rhythm: 60 bpm
AF: 70 - 80 bpm
Optimising treatment in Decompensated HF
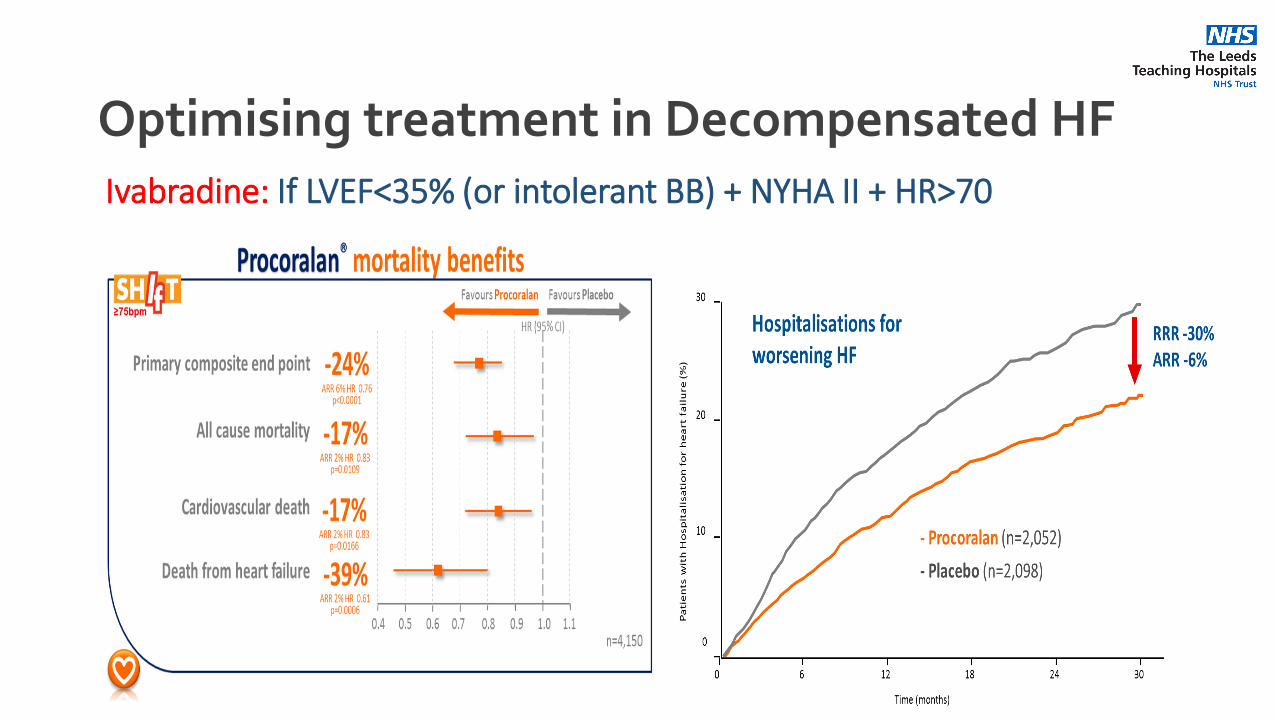
Ivabradine: If LVEF<35% (or intolerant BB) + NYHA II + HR>70
Optimising treatment in Decompensated HF
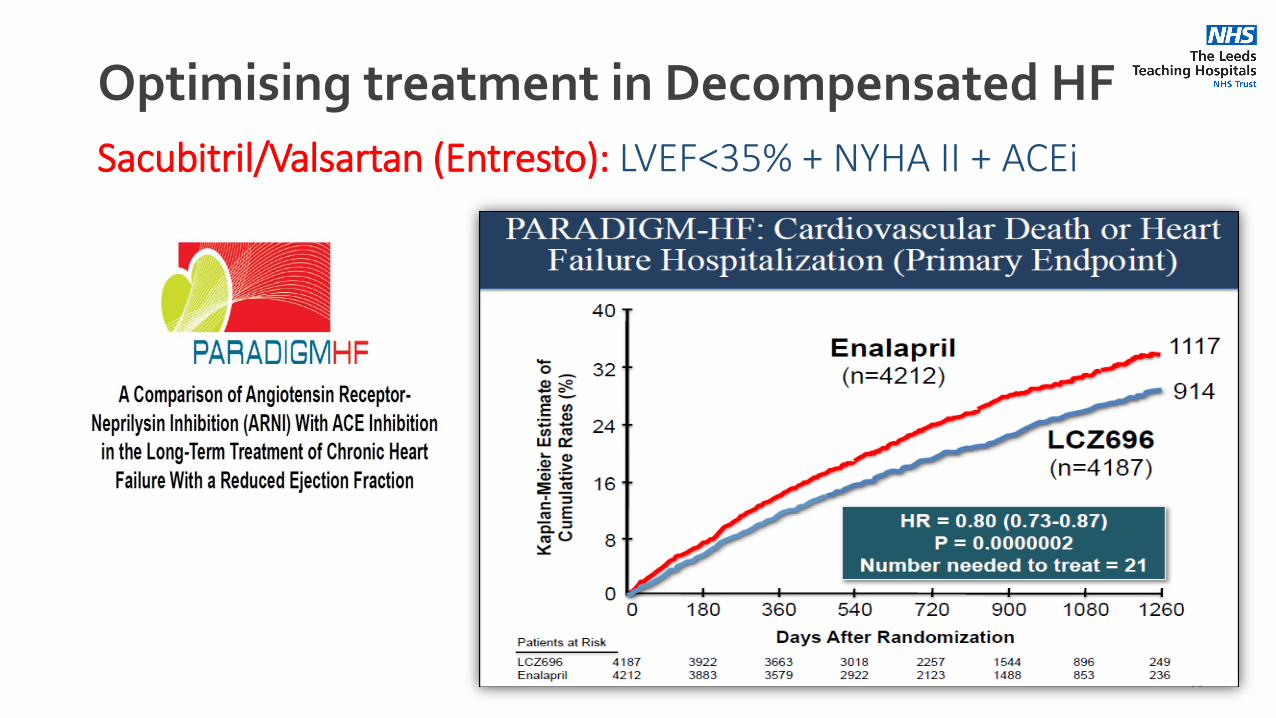
Sacubitril/Valsartan (Entresto): LVEF<35% + NYHA II + ACEi
Optimising treatment in Decompensated HF
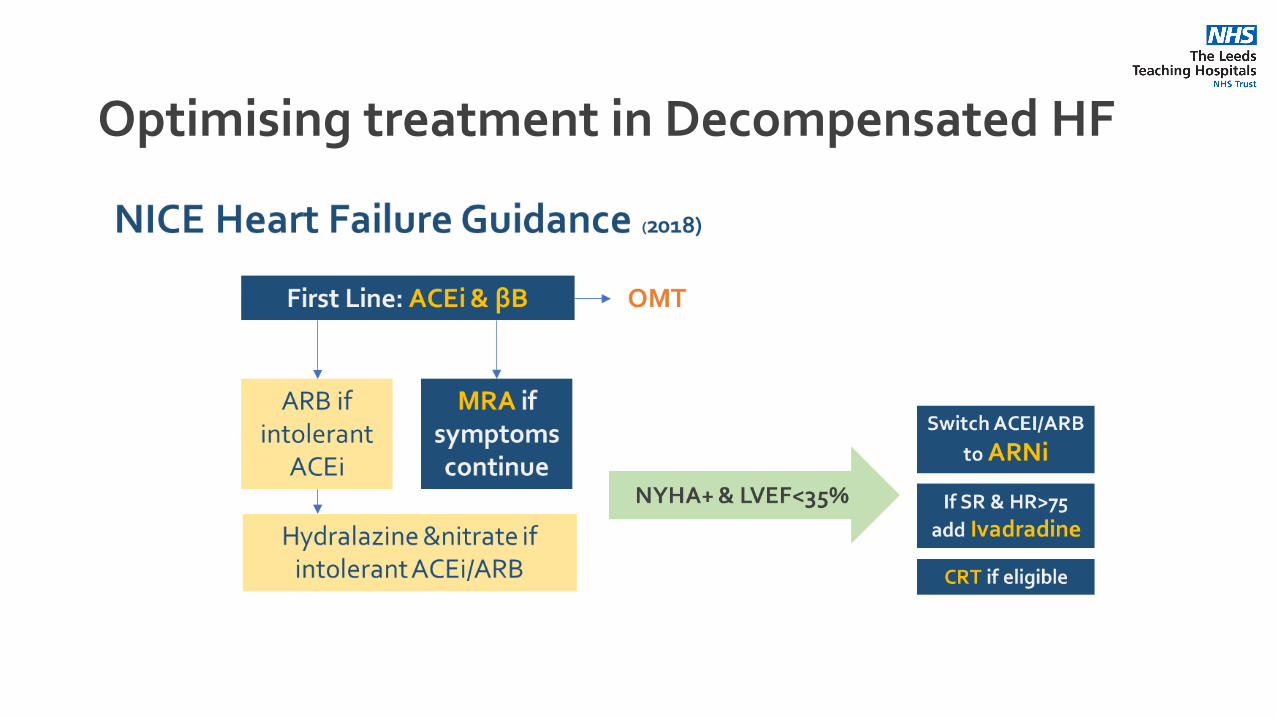
Optimising treatment in Decompensated HF
Optimising treatment in Decompensated HF
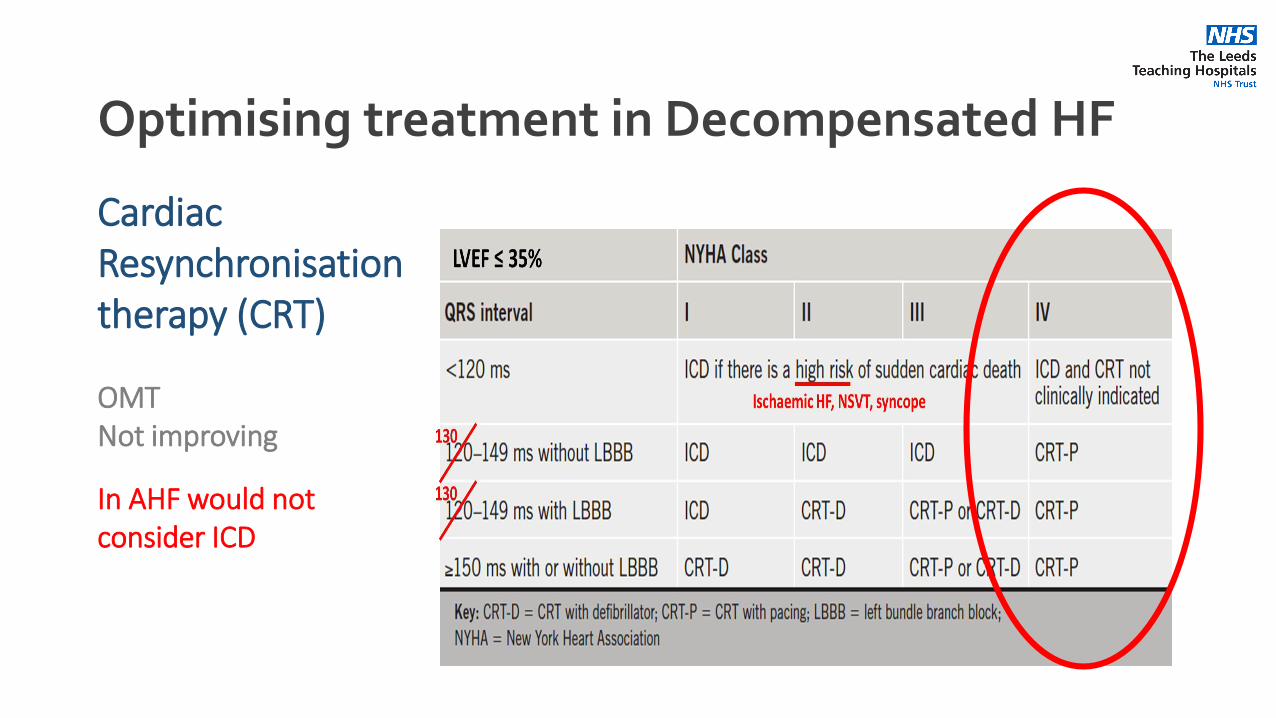
Cardiac Resynchronisation therapy (CRT)
OMTNot improving
In AHF would not consider ICD
Optimising treatment in Decompensated HF
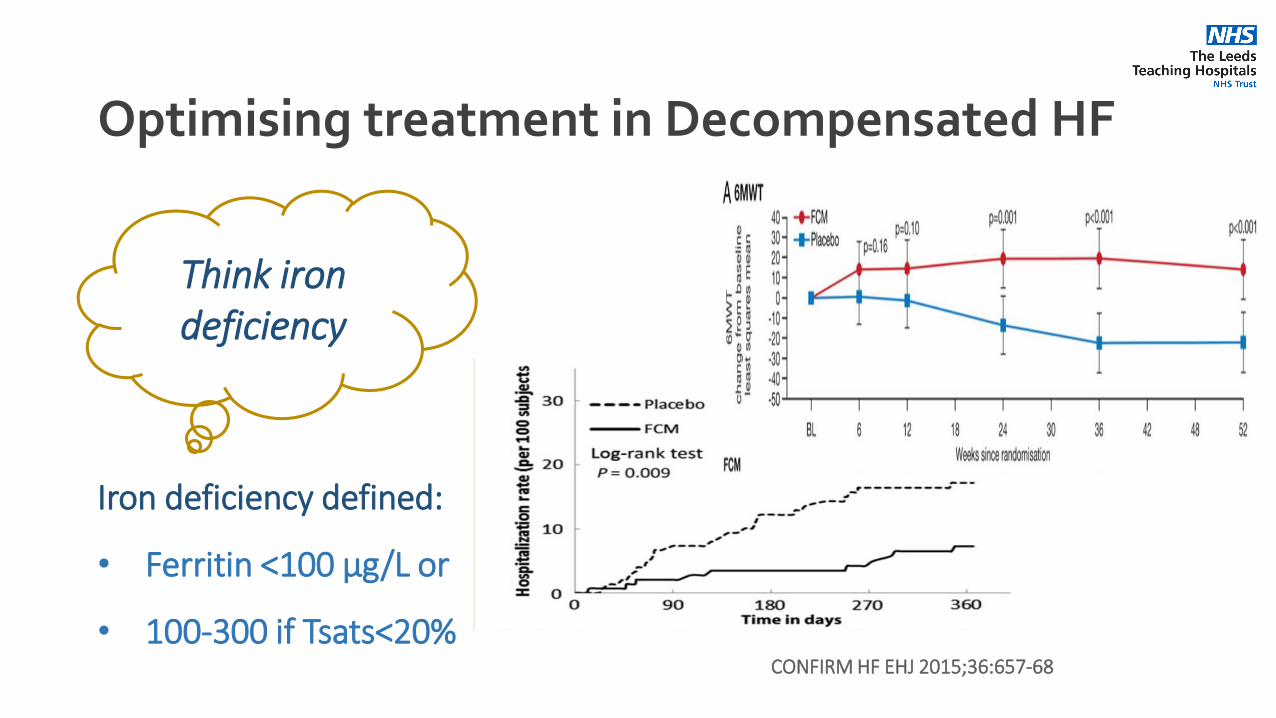
Think iron deficiency
Iron deficiency defined:
• Ferritin <100 μg/L or
• 100-300 if Tsats<20%CONFIRM HF EHJ 2015;36:657-68
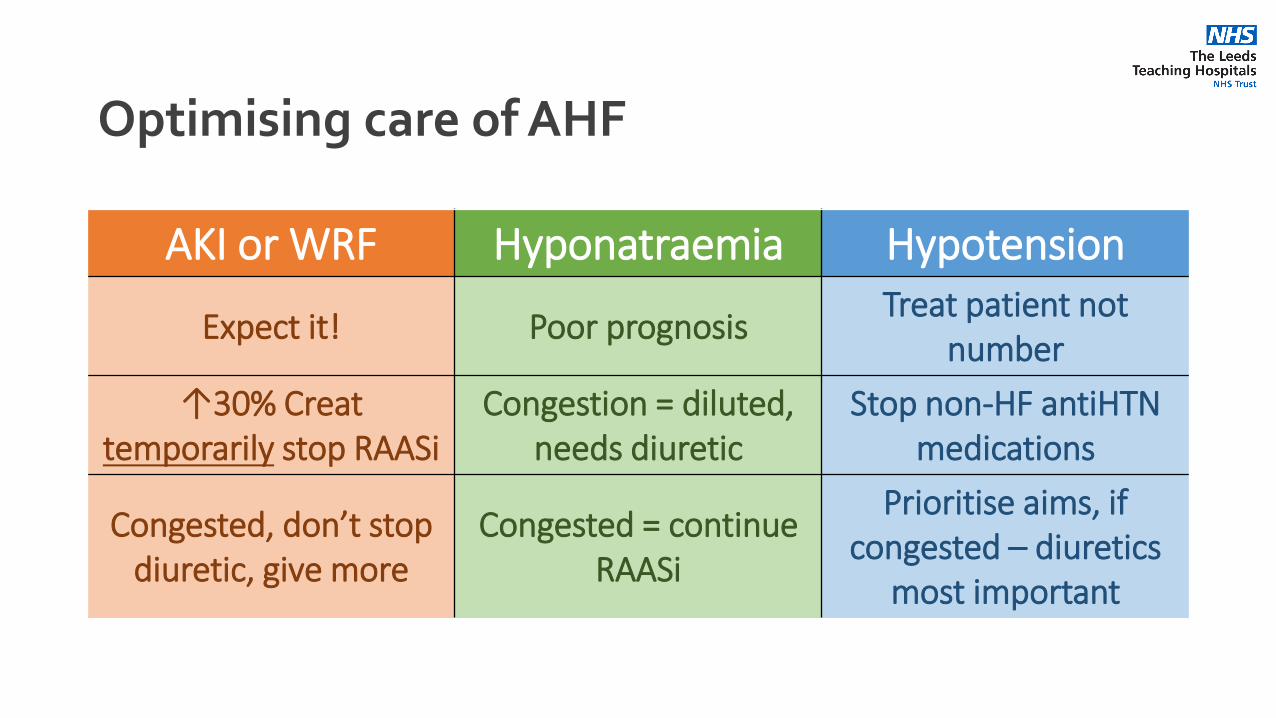
Optimising care of AHF
AKI or WRF Hyponatraemia Hypotension
Expect it! Poor prognosisTreat patient not
number
↑30% Creattemporarily stop RAASi
Congestion = diluted, needs diuretic
Stop non-HF antiHTNmedications
Congested, don’t stop diuretic, give more
Congested = continue RAASi
Prioritise aims, if congested – diuretics
most important
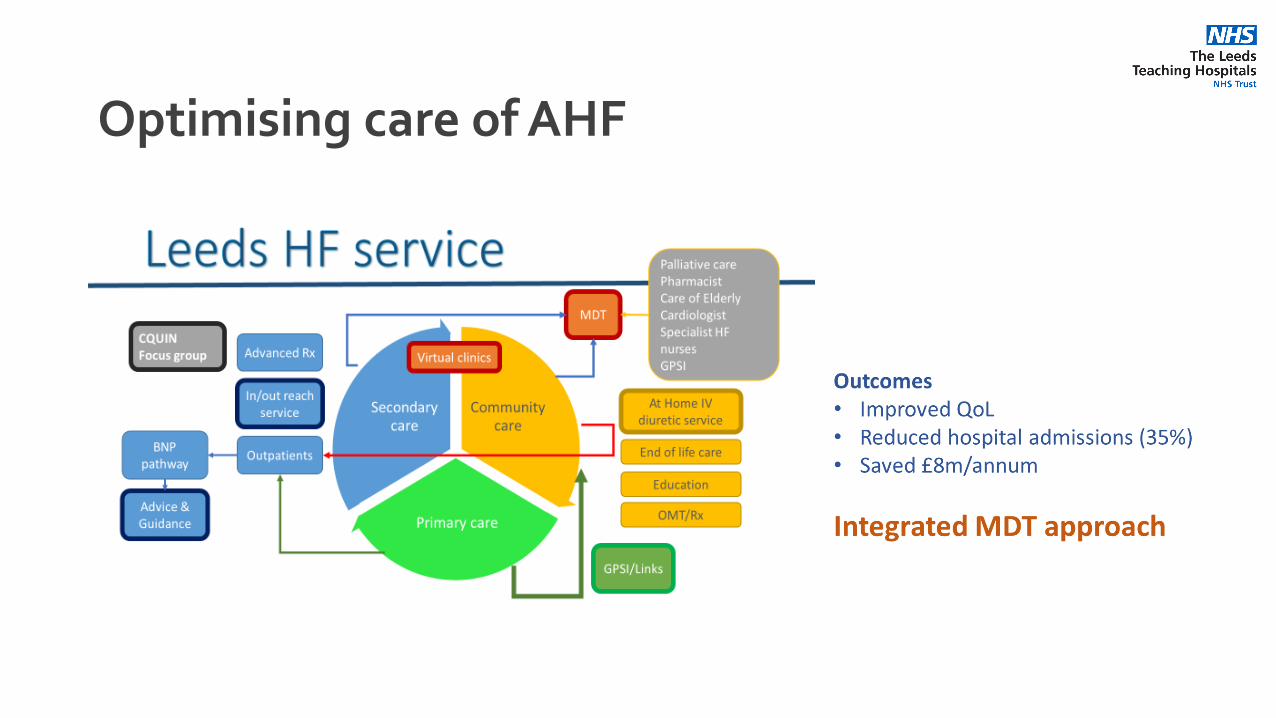
Optimising care of AHF
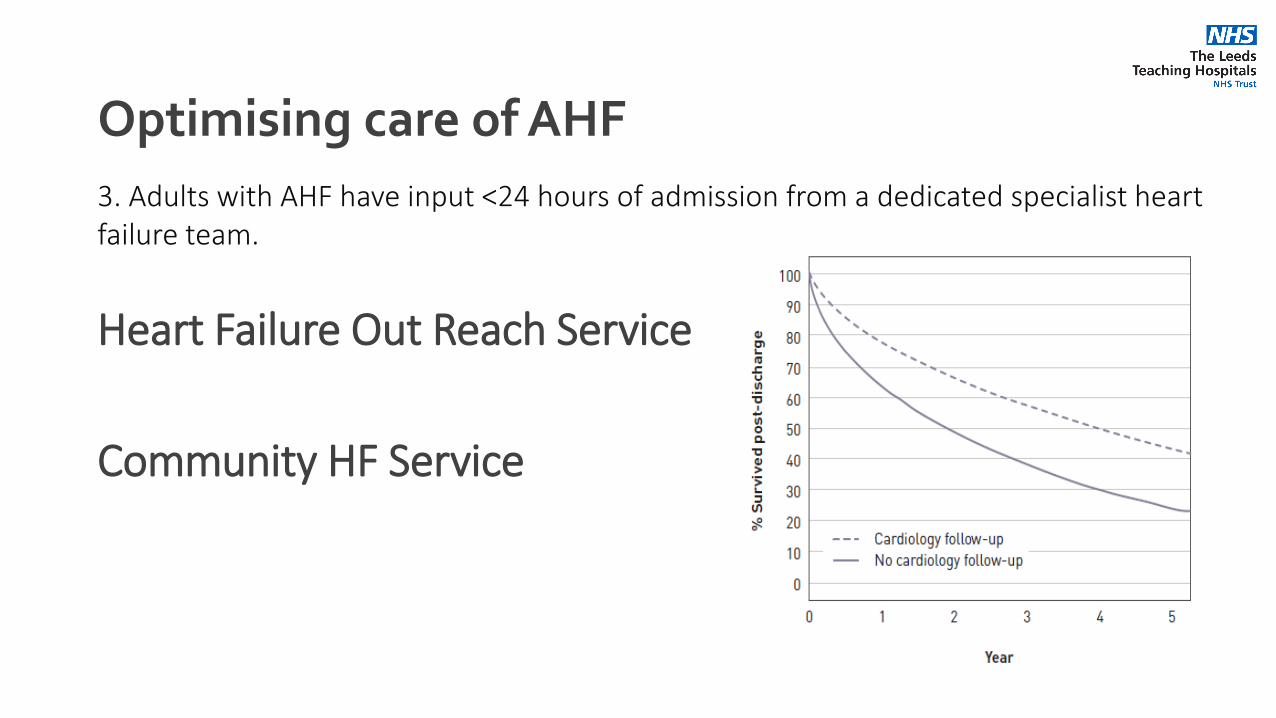
3. Adults with AHF have input <24 hours of admission from a dedicated specialist heart failure team.
Heart Failure Out Reach Service
Community HF Service
Optimising care of AHF
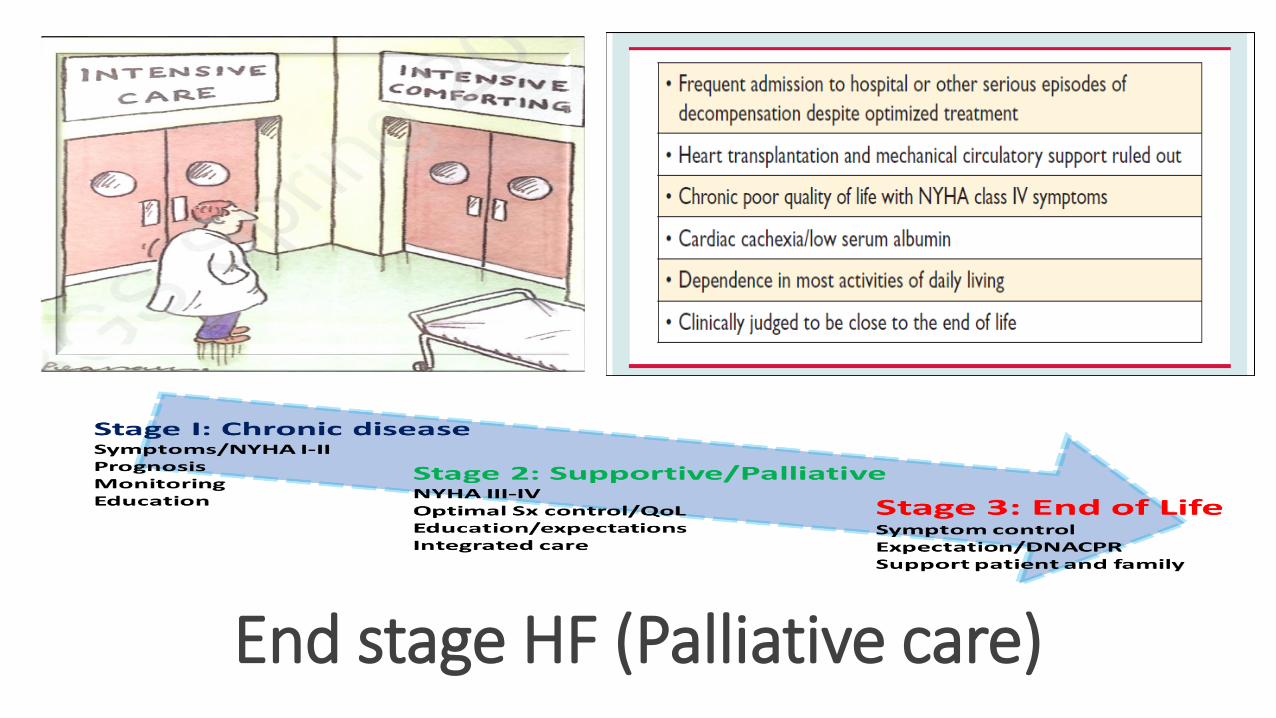
End stage HF (Palliative care)
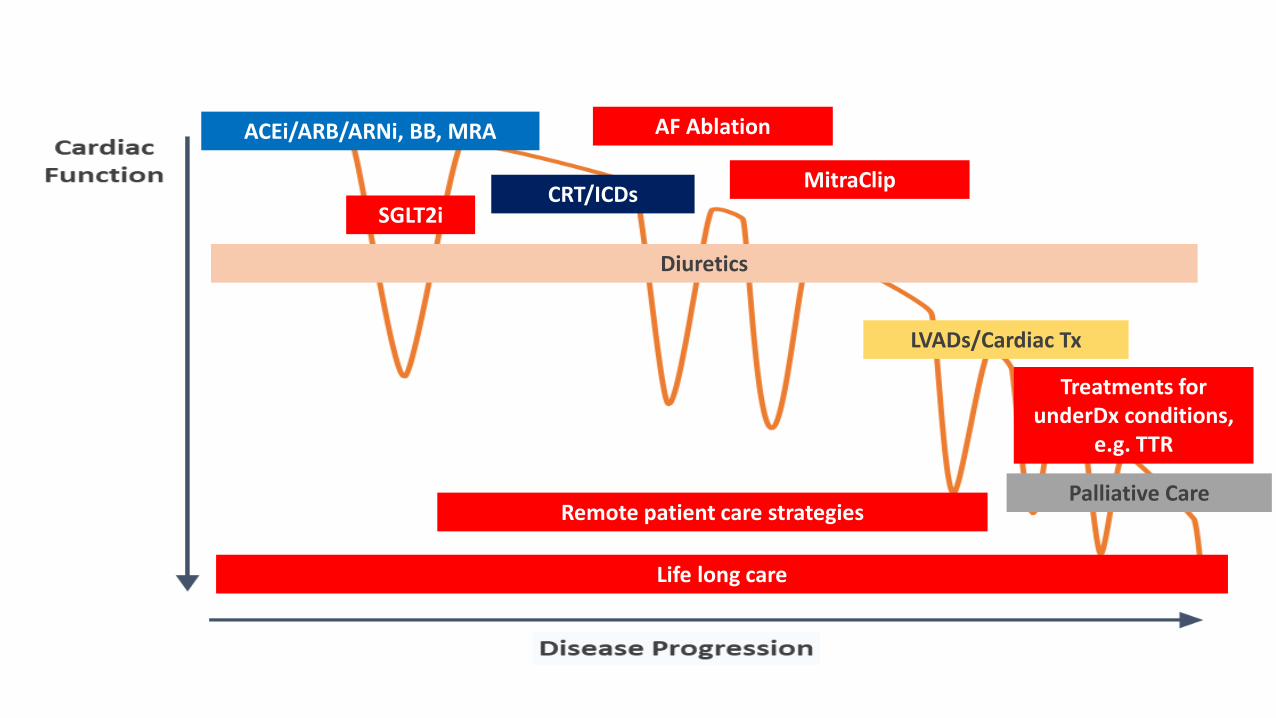
ACEi/ARB/ARNi, BB, MRA
CRT/ICDs
Diuretics
LVADs/Cardiac Tx
SGLT2i
AF Ablation
MitraClip
Palliative Care
Treatments for underDx conditions,
e.g. TTR
Remote patient care strategies
Life long care
Outline
• Definition
• Why important
• What you need to know
Thankyou
Related Documents











