European Journal of Radiology 70 (2009) 549–554 The evaluation of breast tissues removed during reductive mammaplasty with dual energy X-ray absorptiometry Antonino De Lorenzo a , Gianpiero Gravante a,b,∗ , Roberto Sorge c , Fabio Nicoli d , Riccardo Caruso d , Antonino Araco d , Michele Servidio a , Augusto Orlandi e , Valerio Cervelli d a Division of Human Nutrition, University of Tor Vergata in Rome, Italy b Department of Surgery, Whipps Cross University Hospital, London, United Kingdom c Laboratory of Biometry, University of Tor Vergata in Rome, Italy d Department of Plastic Surgery, University of Tor Vergata in Rome, Italy e Department of Biopathology, Anatomic Pathology Institute, University of Tor Vergata in Rome, Italy Received 27 October 2007; received in revised form 2 February 2008; accepted 4 February 2008 Abstract Purpose: We conducted a case-control study in which patients were evaluated with dual energy X-ray absorptiometry (DEXA) before and after breast reduction surgery, and results were correlated with the histological examination. Our goal was to confirm the DEXA as a precise technique for the measurement of breast composition, in order to propose it for the preoperative evaluation of plastic surgery patients. Materials and methods: We prospectively recruited all women that underwent reduction mammaplasty and excluded patients with contraindications to the operation or those that previously underwent bariatric surgery to reduce their weight. Patients were evaluated with DEXA 1 week before and after surgery. Results: From February to October 2006 we recruited 25 patients. The statistical analysis found a significant reduction of weight, BMI, regional fat free mass and fat mass after the operation. The comparison between DEXA and the histological analysis produced a correlation r = 0.989 (r 2 = 0.978), with a predictivity of 98% and a percentage of error 8.3% (95% confidence intervals −252.6, 273.7; 95% limits of agreements of Bland and Altman −436.0, 457.1). Similar results were obtained with the analysis of fat. Conclusions: Our study demonstrated that conventional segmental DEXA is a very precise technique to measure the amount of tissue removed in breast reductions and could open future application in the preoperative assessment of patients undergoing such operations. © 2008 Elsevier Ireland Ltd. All rights reserved. Keywords: Mammary reduction; Body composition; Fat and lean mass; DEXA 1. Introduction The evaluation of breast composition is an important factor in plastic surgery. In breast reductions it is useful to (1) preoperatively know the correct amount of tissue resected during surgery, to avoid alterations of shapes and vol- umes [1–5] and (2) to define the quality of tissue removed (gland or fat), to avoid the inability to lactate [6]. Sev- eral methods are available for this purpose. Plicometry and bioelectrical impedance analysis (BIA) are cheap but inac- curate techniques, on the contrary computerized tomography ∗ Corresponding author at: Division of Human Nutrition, University of Tor Vergata, via Montpellier 1 in Rome, Italy. Tel.: +39 0672596423; fax: +39 0672596415. E-mail address: [email protected] (G. Gravante). (CT) and magnetic resonance imaging (MRI) give more accuracy but with increased costs. The dual energy X-ray absorptiometry (DEXA) combines both advantages and is actually the reference standard for whole-body composition measuring, due to its low radiation dose and high precision [7]. In order to analyse the correct amount of tissue resected dur- ing breast reductions, and define the quality of breast tissues removed, we conducted a prospective study in which patients were evaluated with DEXA, before and after surgery, and results were correlated with the qualitative and quantitative analysis obtained from the histological examination of the specimen removed. Our goal was to confirm the DEXA as a specific and precise technique for the measurement of breast composition, in order to propose it for the preoperative evaluation of patients undergoing breast surgery. 0720-048X/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2008.02.002

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A
PbfMtaRf(BCb©
K
1
ftru(ebc
Vf
0d
European Journal of Radiology 70 (2009) 549–554
The evaluation of breast tissues removed during reductivemammaplasty with dual energy X-ray absorptiometry
Antonino De Lorenzo a, Gianpiero Gravante a,b,∗, Roberto Sorge c, Fabio Nicoli d,Riccardo Caruso d, Antonino Araco d, Michele Servidio a, Augusto Orlandi e, Valerio Cervelli d
a Division of Human Nutrition, University of Tor Vergata in Rome, Italyb Department of Surgery, Whipps Cross University Hospital, London, United Kingdom
c Laboratory of Biometry, University of Tor Vergata in Rome, Italyd Department of Plastic Surgery, University of Tor Vergata in Rome, Italy
e Department of Biopathology, Anatomic Pathology Institute, University of Tor Vergata in Rome, Italy
Received 27 October 2007; received in revised form 2 February 2008; accepted 4 February 2008
bstract
urpose: We conducted a case-control study in which patients were evaluated with dual energy X-ray absorptiometry (DEXA) before and afterreast reduction surgery, and results were correlated with the histological examination. Our goal was to confirm the DEXA as a precise techniqueor the measurement of breast composition, in order to propose it for the preoperative evaluation of plastic surgery patients.
aterials and methods: We prospectively recruited all women that underwent reduction mammaplasty and excluded patients with contraindicationso the operation or those that previously underwent bariatric surgery to reduce their weight. Patients were evaluated with DEXA 1 week beforend after surgery.esults: From February to October 2006 we recruited 25 patients. The statistical analysis found a significant reduction of weight, BMI, regional
at free mass and fat mass after the operation. The comparison between DEXA and the histological analysis produced a correlation r = 0.9892
r = 0.978), with a predictivity of 98% and a percentage of error 8.3% (95% confidence intervals −252.6, 273.7; 95% limits of agreements ofland and Altman −436.0, 457.1). Similar results were obtained with the analysis of fat.onclusions: Our study demonstrated that conventional segmental DEXA is a very precise technique to measure the amount of tissue removed inreast reductions and could open future application in the preoperative assessment of patients undergoing such operations.2008 Elsevier Ireland Ltd. All rights reserved.
(aaam[
i
eywords: Mammary reduction; Body composition; Fat and lean mass; DEXA
. Introduction
The evaluation of breast composition is an importantactor in plastic surgery. In breast reductions it is usefulo (1) preoperatively know the correct amount of tissueesected during surgery, to avoid alterations of shapes and vol-mes [1–5] and (2) to define the quality of tissue removedgland or fat), to avoid the inability to lactate [6]. Sev-
ral methods are available for this purpose. Plicometry andioelectrical impedance analysis (BIA) are cheap but inac-urate techniques, on the contrary computerized tomography∗ Corresponding author at: Division of Human Nutrition, University of Torergata, via Montpellier 1 in Rome, Italy. Tel.: +39 0672596423;
ax: +39 0672596415.E-mail address: [email protected] (G. Gravante).
rwworpiu
720-048X/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2008.02.002
CT) and magnetic resonance imaging (MRI) give moreccuracy but with increased costs. The dual energy X-raybsorptiometry (DEXA) combines both advantages and isctually the reference standard for whole-body compositioneasuring, due to its low radiation dose and high precision
7].In order to analyse the correct amount of tissue resected dur-
ng breast reductions, and define the quality of breast tissuesemoved, we conducted a prospective study in which patientsere evaluated with DEXA, before and after surgery, and resultsere correlated with the qualitative and quantitative analysisbtained from the histological examination of the specimen
emoved. Our goal was to confirm the DEXA as a specific andrecise technique for the measurement of breast composition,n order to propose it for the preoperative evaluation of patientsndergoing breast surgery.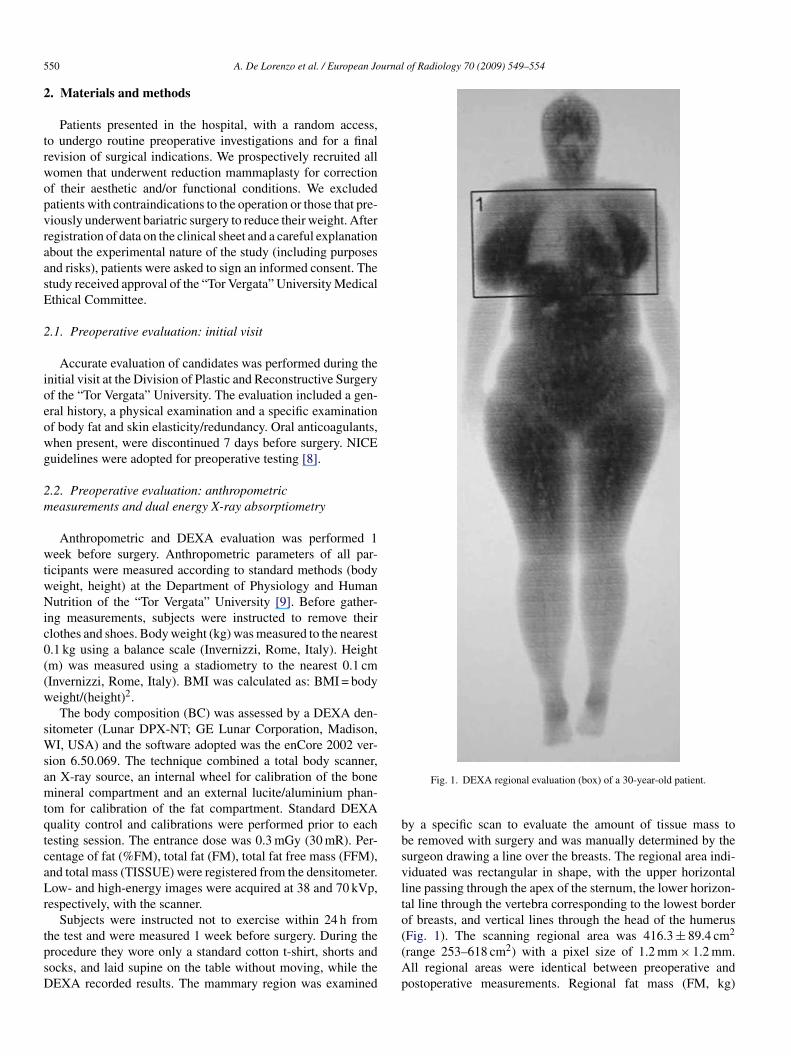
5 urnal of Radiology 70 (2009) 549–554
2
trwopvraasE
2
ioeowg
2m
wtwNic0((w
sWsamtqtcaLr
tpsD
bbsvlto
50 A. De Lorenzo et al. / European Jo
. Materials and methods
Patients presented in the hospital, with a random access,o undergo routine preoperative investigations and for a finalevision of surgical indications. We prospectively recruited allomen that underwent reduction mammaplasty for correctionf their aesthetic and/or functional conditions. We excludedatients with contraindications to the operation or those that pre-iously underwent bariatric surgery to reduce their weight. Afteregistration of data on the clinical sheet and a careful explanationbout the experimental nature of the study (including purposesnd risks), patients were asked to sign an informed consent. Thetudy received approval of the “Tor Vergata” University Medicalthical Committee.
.1. Preoperative evaluation: initial visit
Accurate evaluation of candidates was performed during thenitial visit at the Division of Plastic and Reconstructive Surgeryf the “Tor Vergata” University. The evaluation included a gen-ral history, a physical examination and a specific examinationf body fat and skin elasticity/redundancy. Oral anticoagulants,hen present, were discontinued 7 days before surgery. NICEuidelines were adopted for preoperative testing [8].
.2. Preoperative evaluation: anthropometriceasurements and dual energy X-ray absorptiometry
Anthropometric and DEXA evaluation was performed 1eek before surgery. Anthropometric parameters of all par-
icipants were measured according to standard methods (bodyeight, height) at the Department of Physiology and Humanutrition of the “Tor Vergata” University [9]. Before gather-
ng measurements, subjects were instructed to remove theirlothes and shoes. Body weight (kg) was measured to the nearest.1 kg using a balance scale (Invernizzi, Rome, Italy). Heightm) was measured using a stadiometry to the nearest 0.1 cmInvernizzi, Rome, Italy). BMI was calculated as: BMI = bodyeight/(height)2.The body composition (BC) was assessed by a DEXA den-
itometer (Lunar DPX-NT; GE Lunar Corporation, Madison,I, USA) and the software adopted was the enCore 2002 ver-
ion 6.50.069. The technique combined a total body scanner,n X-ray source, an internal wheel for calibration of the boneineral compartment and an external lucite/aluminium phan-
om for calibration of the fat compartment. Standard DEXAuality control and calibrations were performed prior to eachesting session. The entrance dose was 0.3 mGy (30 mR). Per-entage of fat (%FM), total fat (FM), total fat free mass (FFM),nd total mass (TISSUE) were registered from the densitometer.ow- and high-energy images were acquired at 38 and 70 kVp,
espectively, with the scanner.Subjects were instructed not to exercise within 24 h from
he test and were measured 1 week before surgery. During therocedure they wore only a standard cotton t-shirt, shorts andocks, and laid supine on the table without moving, while theEXA recorded results. The mammary region was examined
((Ap
Fig. 1. DEXA regional evaluation (box) of a 30-year-old patient.
y a specific scan to evaluate the amount of tissue mass toe removed with surgery and was manually determined by theurgeon drawing a line over the breasts. The regional area indi-iduated was rectangular in shape, with the upper horizontaline passing through the apex of the sternum, the lower horizon-al line through the vertebra corresponding to the lowest borderf breasts, and vertical lines through the head of the humerusFig. 1). The scanning regional area was 416.3 ± 89.4 cm2
range 253–618 cm2) with a pixel size of 1.2 mm × 1.2 mm.ll regional areas were identical between preoperative andostoperative measurements. Regional fat mass (FM, kg)

urnal of Radiology 70 (2009) 549–554 551
ar
2
tVtemii
tosoartdwh
2
omaAt1ts
2
pott
astpai
2
fW
Table 1Demographic and anthropometric characteristics
Age (years) Height (cm) Weight (kg) BMI (kg/m2)
PreoperativeMean ± S.D. 44.8 ± 8.8 160.5 ± 6.6 78.5 ± 7.1 30.5 ± 2.5Median 45 158.5 80.4 30.6Min.; max. 29; 61 152; 178 67.1; 93.0 26.2; 34.2
PostoperativeMean ± S.D. 76.9 ± 6.7 29.9 ± 2.2Median 78.0 29.7
p
taNQSe
TPaac
3
DTpaFwa
analysis demonstrated that the FM removed corresponded toapproximately 46% of the total tissues resected while the FFM to54%. The histological analysis evidenced that the more frequentpathology was the fibrocystic mastopathy, present in almost
Table 2Preoperative/postoperative results obtained with DEXA for regional and breasttissues
TISSUE regional (g) FFM regional (g) FM regional (g)
PreoperativeMean ± S.D. 16149.9 ± 1801.0 9095.9 ± 826.7 7054.0 ± 1170.6Median 16007 8899.0 7218.0Min.; max. 13200; 19843 7745; 10705 5140; 9384
PostoperativeMean ± S.D. 14589.0 ± 1079.7 8319.8 ± 728.2 6269.1 ± 1060.2
A. De Lorenzo et al. / European Jo
nd regional fat free mass (FFM, kg) were measured andecorded.
.3. Perioperative care and surgical technique
Every operation was performed by the same surgeon (VC) athe Division of Plastic and Reconstructive Surgery of the “Torergata” University. All patients underwent standard preven-
ive measures of deep vein thrombosis (heparin 4000 U/day andlastic stockings during the day of surgery and until completeobilization) and infection prophylaxis (one dose of cefurox-
me 750 mg i.v.10–30 min before surgery–erythromycin 1 g i.v.f specific allergies were referred).
All mammary reductions were conducted under general anes-hesia and according to the Planas technique [10], an evolutionf the original Pitanguy [11]. The amount of fat removed aturgery was weighted with a standard weighing machine. Post-peratively, no additional doses of antibiotics were administerednd only Tramadol was usually given as analgesic at the patient’sequest. Early mobilisation was solicited 3–6 h from the opera-ion and elastic bands were maintained for the day of surgery anduring the first postoperative day, until complete mobilizationas obtained. Patients without complications were dischargedome 48 h after the operation.
.4. Histological and histomorphometric analysis
For histological evaluation and histomorphometric analysisf the extent of adipose tissue and non-adipose components inammary tissues, serial 4 �-thick sections were deparaffined
nd stained with Hematoxylin-Eosin and Masson’s Trichrome.dipose tissue was scored by measuring the percentage of fat
issue without fibrotic changes at 250× magnifications in at least0 randomly selected fields for each case; the number of fieldso obtain a significant difference was calculated according totereological formulae [12].
.5. Postoperative follow-up
Patients underwent standard surgical follow-up visits,lanned at the 7th, 14th and 30th postoperative day. All post-perative DEXA measures were performed after 2 weeks fromhe operation to allow the inflammation process, created withhe surgical manipulation, disappear.
Primary endpoints of the study were to assess the feasibilitynd precision of DEXA in estimating the amount of total tis-ue removed during surgery. Secondary goals were to evaluatehe quality of tissue removed in terms of FFM and FM. Com-arisons between preoperative and postoperative breast regionsnd compositions calculated with DEXA were correlated withntraoperative and histologic evaluations of tissues removed.
.6. Statistical analysis
All data analysis and calculation of sample size were per-ormed using the Statistical Package for the Social Sciences
indows version 13.0 (SPSS, Chicago, Illinois, USA). Descrip-
p
A
Min.; max. 66.8; 90.8 26.0; 33.5
0.0001 0.0001
ive statistics for quantitative continuous variables were the meannd standard deviation after confirmation of normal distribution.ormality assumptions were demonstrated with histograms,–Q plots, Skewness and Kurtosis, Kolmogorov/Smirnov andhapiro Wilk testings. Descriptive statistics for qualitative cat-gorical variables was performed with frequencies.
Differences between the two study groups (T0: preoperative,1: postoperative) were tested using the 1-tailed Student’s t-test.earson’s correlation index was used to evaluate relationshipsmong variables. Bland–Altman method was used for limits ofgreements 95% and estimated terrors [13]. All p values wereonsidered significant if inferior to 0.05.
. Results
From February to October 2006 we recruited 25 patients.emographic and anthropometric characteristics are reported inable 1. Operations lasted 190 ± 50 min and no particular com-lications occurred intra- and postoperatively. The statisticalnalysis found a significant reduction of weight, BMI, regionalFM and FM after the operation. The overall weight and BMIas reduced by 2% with surgery, while tissue of breasts, FFM
nd FM by 18% (Tables 1 and 2).The preoperative and postoperative comparison of DEXA
Median 14657.4 8404,0 6476,0Min.; max. 12792; 16545 6173; 9839 4653; 8356
0.0001 0.0001 0.0001
ll data were examined with the Student’s t-test.

552 A. De Lorenzo et al. / European Journal
Table 3Results obtained with the histologic analysis
Histologic analysis N % of cases
Fibrocystic mastopathy 18 71.4Adipose involution 5 19.0Lipomatosis 4 14.3Fibroadenoma 4 14.3Ductal hyperplasia 2 9.5Adenosis 2 9.5Papilloma 1 4.8AD
ad4s5tm(8acsca12
4
rbpIsdotear[r[
itrsbwt
TC
MMM
FA
pocrine metaplasia 1 4.8uctal ectasia 1 4.8
ll patients (Table 3). The histomorphometric examination alsoemonstrated that the removed adipose tissue corresponded to3.0 ± 4.0% of the total tissues resected while the fibrotic tis-ue and the mammary epithelial structures corresponded to7 ± 3.8%. The qualitative and quantitative comparison betweenhe pre- and postoperative DEXA measurements vs. the histo-
orphometric analysis (Table 4) showed a correlation r = 0.989r2 = 0.978), with a predictivity of 98% and a percentage of error.3% (95% confidence intervals −252.6, 273.7; 95% limits ofgreements of Bland and Altman −436.0, 457.1) (Fig. 2). Theomparison between the pre- and postoperative FM DEXA mea-urements vs. fat histomorphometric analysis (Table 4) showed a
2
orrelation r = 0.993 (r = 0.986), with a predictivity of 99% andpercentage of error 8.1% (95% confidence intervals −101.6,26.9; 95% limits of agreements of Bland and Altman −181.2,06.5) (Fig. 3).dmtw
able 4orrelation between the DEXA analysis of tissues and the histomorphometric exami
DEXA evaluation
Tissue (g) FFM (g) FM (g) % FM
ean ± S.D. 1560.9 ± 840.3 842.5 ± 408.2 718.3 ± 439.0 43.0 ±edian 1537.6 750.0 671.0 43.6in.; max. 305; 3298 199; 1596 106; 1702 39.0; 4
a Histological FM and FFM derived from the percentage of fat and total tissue rem
ig. 2. Upper panel, scatter plot of tissue measured with DEXA and analysed with hiltman plot with 95% confidence intervals (black lines) and limits of agreements (re
of Radiology 70 (2009) 549–554
. Discussions
Breast reduction is a reconstructive operation performed toeduce the size and improve the cosmetic aspect of the breasty redistributing the volume among the four quadrants and re-ositioning the nipple-areola complex to the mammary folds.t is one of the most common operations performed in plasticurgery, used to correct functional and aesthetic deformities pro-uced by gigantomastias. Breasts final sizes and shapes dependn the correct interpretation of patients desires and the surgicalechnique adopted, but a scarce preoperative knowledge of skinlasticity, tissue vascularization and composition (fat vs. gland)lso influence outcomes [2–6,14]. For this reason, the operationequires a great amount of judgment and clinical experience4]. However, still up to 20% of patients are not satisfied withesults obtained mainly due to errors in shape, size and symmetry2–6,14].
Plastic surgeons reduce the breast size according to technicalssues, their experience and the patient’s wishes, and no objec-ive method currently exists to address the correct amount to beemoved. The common practice is to remove 200–250 g of tis-ue for every breast cup size to be reduced. Problems arise whenreasts are composed mainly by fat and not gland: the amount ofeight removed in the former reduces the breast volume more
han the same quantity in the latter, due to the different tissue
ensities between fat and glands. To solve this matter, a com-on practice is to remove during surgery amounts smaller thenhose planned before the operation, and temporarily close breastsith clips to check the symmetry and size obtained. This is a
nation
Histological evaluation
Tissue (g) FFM (g)a Fat (g)a % Fat
4.1 1550.4 ± 805.5 862.9 ± 430.4 687.5 ± 379.8 43.0 ± 4.01500.0 801.5 675.0 43.0
0.6 450; 3250 272; 1713 178; 1537 38.5; 40.0
oved.
stology. Identity line (red) and regression line (black). Lower panel, Bland andd lines) of differences between histologic values and DEXA measurements.

A. De Lorenzo et al. / European Journal of Radiology 70 (2009) 549–554 553
F d wita ents
uibfad
obmt[blttibbdi
Dbdacoeticlvaaet
to
5
togetta
R
[
ig. 3. Upper panel, scatter plot of fat measured with DEXA (FM) and analysend Altman plot with 95% confidence intervals (black lines) and limits of agreem
seful method, but delicate and time-consuming. Furthermore,n cases of breast asymmetries, where different amounts need toe removed from each breast, this method can be misleading. Inact, even if both breasts may look similar during surgery, thesymmetry can recur months later if the tissue composition isifferent among them.
More definitive criteria are required to evaluate the quantityf tissue to be resected. Initially, the body surface area (BSA) andody mass index (BMI) were analysed [15–18], but radiologicethods, such as magnetic resonance imaging (MRI), computed
omography (CT) and DEXA, soon proved to be more accurate19]. MRI showed a 0.63 correlation with mammography forreasts containing more than 45% of fat and 0.34 for those withess [20]. CT provides a precise measure of tissues composi-ion (<1% error) with an excellent accuracy (<1%), howeverhe whole-organ radiation dose limits its usefulness as a screen-ng tool [21]. DEXA has several advantages for the measure ofreast compositions: it is actually the gold standard for whole-ody measurements of composition, due to its low radiationose and high precision [7], and does not require a subjectiventerpretation of results.
Shepherd and colleagues found an 83% correlation betweenEXA and mammography for the evaluation of cadavericreasts density and of 52% for healthy female volunteers,emonstrating that breast composition could be precisely evalu-ted with DEXA densitometers [22,23]. In our series, a highorrelation (r = 0.989) was present between pre- and post-perative DEXA measurements and results of the histologicxamination. Furthermore, FM corresponded to 46% of theotal tissues removed and FFM to 54% (mostly gland, assum-ng that the skin’s contribution was not important). Even in thisase, a similar correlation (r = 0.993) was found with the histo-ogic examination. A more objective estimation of tissues (fats. gland) present in each patient is a new information avail-
ble that could furnish the surgeon the possibility to decide themount of each component to be removed. The percentage ofrror between histological analysis vs. DEXA was 8.3% for totalissue and 8.1% for fat, corresponding to approximately 473 g of[
[
h histology. Identity line (red) and regression line (black). Lower panel, Bland(red lines) of differences between histologic values and DEXA measurements.
otal tissues and 198 g of fat for an average hyperthophic breastf 5701 g.
. Conclusions
In conclusion, our case-control study shows that segmen-al DEXA is a technique that furnishes a precise estimationf the breast composition. This data, combined with the sur-eon’s clinical judgment, could help him in the preoperativevaluation of patients undergoing reduction mammaplasty. Fur-hermore, given its high precision, DEXA could also suggesthe exact location of tissues to be resected in patients withsymmetries.
eferences
[1] Godwin Y, Wood SH, O’Neill TJ. A comparison of the patient and surgeonopinion on the long-term aesthetic outcome of reduction mammaplasty. BrJ Plast Surg 1998;51:444–9.
[2] Serletti JM, Reading G, Caldwell E, et al. Long-term patient satisfactionfollowing reduction mammoplasty. Ann Plast Surg 1992;28:363–5.
[3] Hughes LA, Mahoney JL. Patient satisfaction with reductionmammaplasty: an early survey. Aesthetic Plast Surg 1993;17:345–9.
[4] Davis GM, Ringler SL, Short K, et al. Reduction mammaplasty: long-term efficacy, morbidity, and patient satisfaction. Plast Reconstr Surg1995;96:1106–10.
[5] McMahan JD, Wolfe JA, Cromer BA, et al. Lasting success in teenagereduction mammaplasty. Ann Plast Surg 1995;35:227–31.
[6] Pers M, Nielsen IM, Gerner N. Results following reduction mammaplastyas evaluated by the patients. Ann Plast Surg 1986;17:449–55.
[7] Laskey MA. Dual-energy X-ray absorptiometry and body composition.Nutrition 1996;12:45–51.
[8] Mayor S. NICE guidance clarifies when to do preoperative tests in electivesurgery. BMJ 2003;326:1418.
[9] Lohman TG, Roche AF, Martorell R. Anthropometric standardization ref-erence manual. Champaing, IL: Human Kinetics; 1998.
10] Planas J, Mosely LH. Improving breast shape and symmetry in reduction
mammaplasty. Ann Plast Surg 1980;4:297–303.11] Pitanguy I, Mammaplasty. Study of 245 consecutive cases and presentationof a personal technique. Rev Bras Cir 1961;42:201–20.
12] Weibel ER. Stereological methods. Practical methods for biological mor-phometry, vol. 1. London, San Francisco: Academic Press; 1979.

5 urnal
[
[
[
[
[
[
[
[
[
54 A. De Lorenzo et al. / European Jo
13] Bland JM, Altman DG. Statistical methods for assessing agreementbetween two methods of clinical measurement. Lancet 1986;i:307–10.
14] Strombeck JO. Macromastia in women and its surgical treatment. Acta ChirScand 1964;341:1–128.
15] Schnur PL, Hoehn JG, Ilstrup DM, et al. Reduction mammaplasty: cosmeticor reconstructive procedure? Ann Plast Surg 1991;27:232–7.
16] Schnur PL. Reduction mammaplasty—the schnur sliding scale revisited.Ann Plast Surg 1999;42:107–8.
17] Miller AP, Zacher JB, Berggren RB, et al. Breast reduction for symptomaticmacromastia: can objective predictors for operative success be identified?Plast Reconstr Surg 1995;95:77–83.
18] Kompatscher P, von Planta A, Seifert B, et al. A body mass index relatedscale for reconstructive breast reduction. Eur J Plast Surg 2003;26:202–6.
[
[
of Radiology 70 (2009) 549–554
19] Sutcliffe JF. A review of in vivo experimental methods to determine thecomposition of the human body. Phys Med Biol 1996;41:791–833.
20] Lee NA, Rusinek H, Weinreb J, et al. Fatty and fibroglandular tissuevolumes in the breasts of women 20–83 years old: comparison of X-ray mammography and computer-assisted MR imaging. Am J Roentgenol1997;168(2):501–6.
21] Ellis KJ. Human body composition: in vivo methods. Physiol Rev2000;80:649–80.
22] Shepherd JA, Kerlikowske KM, Smith-Bindman R, et al. Measurementof breast density with dual X-ray absorptiometry: feasibility. Radiology2002;223(2):554–7.
23] Shepherd JA, Herve L, Landau J, et al. Clinical comparison of a novel breastDXA technique to mammographic density. Med Phys 2006;33:1490–8.
Related Documents











