The Epidemiology of Tuberculosis in Minnesota, 2012 – 2016 Minnesota Department of Health Tuberculosis Prevention and Control Program 651-201-5414 | www.health.state.mn.us/tb

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Epidemiology of Tuberculosis in Minnesota, 2012 – 2016
Minnesota Department of Health
Tuberculosis Prevention and Control Program
651-201-5414 | www.health.state.mn.us/tb
Presenter
Presentation Notes
The purpose of this slide set is to characterize the epidemiology of tuberculosis (TB) disease in Minnesota. The slides describe both demographic and clinical characteristics of TB statewide. The data in these slides pertain to confirmed cases of active TB disease reported from 2012 through 2016. In accordance with the Minnesota Communicable Disease Reporting Rule, physicians, laboratories, and other health care providers are required to report all confirmed and probable cases of TB disease among persons residing in Minnesota to the Minnesota Department of Health; such reports serve as the source of information for the data presented in these slides.

2
TB Morbidity and Mortality, MN, 2012-2016
Year No. of Cases (Rate)* No. of Deaths (%)**
2012 162 (3.0) 4 (2%)
2013 151 (2.8) 2 (1%)
2014 147 (2.7) 3 (2%)
2015 150 (2.7) 3 (2%)
2016 168 (3.0) 8 (5%)
* Cases per 100,000 population. Rates calculated using state population estimates from the U.S. Census Bureau.**Represents only deaths due to TB disease or TB drug-induced toxicity
Presenter
Presentation Notes
In 2016, 168 new cases of active TB disease among residents of Minnesota were reported to the Minnesota Department of Health, an increase of 12% from 2015, when there were 150 new cases of TB. This number corresponds to an incidence rate of 3.0 cases per 100,000 population. In comparison, 9,272 new cases of TB disease (2.9 cases per 100,000 population) were reported in the United States during 2016; the median TB incidence rate among 51 states and reporting areas nationally was 1.9 cases per 100,000 population. This slide also depicts the number of deaths attributed to TB in Minnesota between 2012 and 2016. Overall, 3% of TB cases died as a result of TB during this five-year period, ranging from 1% in 2013 to 5% in 2016. These data do not include individuals who died from causes other than TB.

3
Active TB Cases Reported, MN, 2000-2016
0
50
100
150
200
250
300
No.
of N
ew T
B Ca
ses
Mean = 185
Presenter
Presentation Notes
After case counts of TB in Minnesota dropped under 200 in 2009, they have remained fairly stable. In 2016, we saw a 12% increase compared to the previous year (168 cases compared to 150 in 2015). The mean number of new cases per year from 2000 to 2016 was 185.

4
TB Incidence Rates per 100,000 Population,U.S. and MN, 2000-2016
0
1
2
3
4
5
6
7
Case
s per
100
,000
Year of Diagnosis
United States Minnesota
Healthy People 2010 and 2020 Objective (Rate = 1.0)
Presenter
Presentation Notes
This slide depicts the incidence rate for TB in Minnesota and the United States from 2000 to 2016. The rate of TB in Minnesota is generally lower than the national rate, with the exception of 2007 and 2016. In 2016, there were 3.0 TB cases/100,000 in Minnesota, and 2.9/100,000 nationally. The rates of TB in Minnesota and nationally have not met the Healthy People 2010 and 2020 objective of 1.0 TB case per 100,000.

5
Percentage of Non U.S.-Born TB Cases, U.S. and MN, 2007-2016
0
10
20
30
40
50
60
70
80
90
100
% o
f Cas
es
Year of Diagnosis
United States Minnesota
MN Mean = 82%
U.S. Mean = 63%
Presenter
Presentation Notes
During the past decade, the percentage of non U.S.-born persons among TB cases reported in Minnesota has averaged 82%, ranging from 73% to 90%. The average non U.S.-born percentage during this time period among cases nationally was 63%. In 2016, 90% of TB cases in Minnesota were born outside the U.S., compared to 68% of TB cases reported nationally.

6
Number of Cases and Incidence of TB byLocation of Residence, MN, 2012-2016
Location of Residence
2012No. (Rate)*
2013No. (Rate)*
2014No. (Rate)*
2015No. (Rate)*
2016No. (Rate)*
Hennepin County 71 (6.1) 51 (4.3) 51 (4.3) 57 (4.7) 73 (6.0)
Ramsey County 39 (7.6) 39 (7.5) 26 (4.9) 29 (5.4) 40 (7.4)
Suburban Twin Cities Metro†
27 (2.2) 20 (1.6) 24 (2.0) 25 (2.0) 16 (1.3)
Olmsted County 3 (2.1) 10 (6.8) 16 (10.7) 12 (8.0) 11 (7.3)
Other counties 22 (1.0) 31 (1.3) 30 (1.3) 27 (1.2) 28 (1.2)
Total 162 (3.0) 151 (2.8) 147 (2.7) 150 (2.7) 168 (3.0)
* Cases per 100,000 population. Rates calculated using state population estimates from the U.S. Census Bureau.† Anoka, Carver, Dakota, Scott, and Washington counties
Presenter
Presentation Notes
This slide presents the number and rate of new TB cases reported by county of residence in Minnesota from 2012 through 2016. County-specific data are presented for Hennepin, Ramsey, and Olmsted counties, which are the three counties in Minnesota that operate public TB clinics. The slide also presents data for the five-county suburban Twin Cities metropolitan area and for Greater Minnesota, excluding Olmsted County. Among the metro area counties, the highest TB incidence rate in 2016 was reported in Ramsey County (7.4/100,000), followed by Hennepin County (6.0/100,000).

7
TB Disease Case Counts, MN, 2016
Total 168Hennepin County 73Ramsey County 40Suburban Metro 16Greater Minnesota 39
Presenter
Presentation Notes
This slide presents a map of Minnesota with counties shaded according to the number of TB cases reported in their jurisdictions during 2016. Although 20 (23%) of the state’s 87 counties reported at least one new case of TB disease in 2016, the majority of cases occurred in the Twin Cities metropolitan area. The largest number of cases occurred in Hennepin County (73, or 43%) and Ramsey County (40, or 24%). Almost a quarter (23%) of the new TB cases in 2016 were reported by Greater Minnesota counties.

8
TB Disease Case Counts, MN, 2012-2016
Total 778Hennepin County 303Ramsey County 173Suburban Metro 112Greater Minnesota 190
Presenter
Presentation Notes
This slide presents data on TB cases, by county of residence, reported in Minnesota from 2012 through 2016. Similar to the previous slide, these data emphasize that the greatest burden of TB disease occurred primarily in certain areas of the state, although the geographic distribution of cases was more widespread. Of the state’s 87 counties, 43 (49%) reported at least one case of TB disease during this five-year period. Hennepin and Ramsey counties accounted for over 61% of all new TB cases reported during this time period, while 24% of cases were reported in Greater Minnesota.

9
TB Cases by Age Group and Place of Birth,MN, 2012-2016
0
5
10
15
20
25
30
35
40
45
50
< 5 yrs 5 - 14 yrs 15 - 24 yrs 25 - 44 yrs 45 - 64 yrs >= 65 yrs
% o
f Cas
es
Age Category
U.S.-Born Non U.S.-Born
Presenter
Presentation Notes
The age distribution of TB cases reported in Minnesota differs markedly between U.S.-born and non U.S.-born patients. The largest group (43%) of non U.S.-born TB cases reported in Minnesota from 2012 to 2016 was between 25 to 44 years of age, whereas the number of U.S.-born cases was more evenly distributed, with the highest number in older age groups. These strikingly different age distributions reflect the differing risks of exposure to TB among these populations. For example, newly-arrived refugees and immigrants to Minnesota tend to be younger, and TB cases in these age groups likely were already infected with TB before arriving in the U.S. Among U.S.-born persons, adults who were born 50 or more years ago when TB was much more prevalent in Minnesota are more likely than younger U.S.-born persons to have been infected with TB. As these older U.S.-born persons age and develop other medical conditions that may weaken their immune systems, they may progress from latent TB infection to active TB disease.��The proportion of children under five years of age was much higher among U.S.-born TB cases reported in Minnesota from 2012 through 2016 than among non U.S.-born cases (15% versus <1%, respectively). Ninety percent of these young U.S.-born cases had at least one non U.S.-born parent or guardian. These second-generation children appear to experience an increased risk of TB disease that more closely resembles that of non U.S.-born persons. These children were likely exposed to TB as a result of travel to their parents’ country of origin or from family members or friends with active disease.

10
TB Cases by Sex at Birth and Place of Birth,MN, 2012-2016
0
10
20
30
40
50
60
70
Non U.S.-Born U.S.-Born Total
% o
f Cas
es
Male Female
Presenter
Presentation Notes
This slide presents data on TB cases, by sex at birth, reported in Minnesota from 2012 through 2016. More males than females were represented among TB cases reported statewide (55% to 45%), which is typical of TB cases reported in the United States. Among the U.S.-born TB cases, the difference in sex at birth was more pronounced (63% males to 37% females). Among non U.S.-born TB cases, the distribution of sex at birth was relatively more equal (54% males to 46% females). The difference in TB rates by sex at birth could be due to the unequal distribution of TB risk factors among U.S.-born cases.

11
Number of Cases and Incidence of TB by Race*/Ethnicity,MN, 2012-2016
0
5
10
15
20
25
30
35
2012 2013 2014 2015 2016
Case
s per
100
,000
**
American Indian or Alaska Native Asian or Pacific Islander African/African-AmericanWhite Hispanic/Latino All race/ethnic groups
*Race categories do not include persons of Hispanic/Latino origin**Rate per 100,000 population. Calculated using population estimates from the U.S. Census Bureau.
Presenter
Presentation Notes
This slide depicts the incidence rate of TB disease by race/ethnicity in Minnesota from 2012 through 2016. Non-white racial and ethnic populations in Minnesota are disproportionately affected by TB. In particular, the incidence rate of TB disease reported in 2016 was highest among Africans/African-Americans (25.0 cases per 100,000 population), followed by Asians or Pacific Islanders (21.1 cases per 100,000 population). In comparison, the TB case rate among non-Hispanic whites was 0.2 cases per 100,000 population. The TB incidence rates among American Indians or Alaska Natives and Hispanics/Latinos in 2016 were 1.5 and 4.2, respectively. During this five-year period, TB rates were generally highest among Africans/African-Americans and among Asians and Pacific Islanders.

12
TB Cases by Race*/Ethnicity and Place of Birth,MN, 2012-2016
Race / Ethnicity* Non U.S.-Born Cases No. (%)
U.S.-Born CasesNo. (%)
White 17 (3) 53 (40)Black 349 (54) 34 (26)Asian 230 (36) 12 (9)American Indian / Alaska Native 0 15 (11)Native Hawaiian / Pacific Islander 2 (<1) 0Multi-racial 0 1 (<1)Hispanic/Latino 49 (8) 16 (12)Total 647 (100) 131 (100)
*Race categories do not include persons of Hispanic/Latino origin
Presenter
Presentation Notes
The racial and ethnic distribution of TB cases reported in Minnesota from 2012 through 2016 differed between non U.S.-born and U.S.-born populations. Among non U.S.-born cases, the majority (54%) were black, 36% were Asian, 8% were Hispanic or Latino, 3% were white, and two cases were Native Hawaiian or Pacific Islander. Among the much smaller number of U.S.-born TB cases, the largest proportion (40%) were white, 26% were black, 12% were Hispanic or Latino, 11% were American Indian or Alaska Native, 9% were Asian, and one case was reported as multi-racial. Regardless of place of birth, non-white racial and ethnic populations were disproportionately affected by TB, comprising larger proportions among TB cases than their proportional representation in the overall state population.

Somalia44%
Ethiopia24%
US9%
Kenya7%
Liberia5%
Other 11%
13
African/African-American TB Cases by Place of Birth,MN, 2012-2016
N = 383
Presenter
Presentation Notes
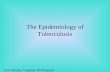
Among African or African-American TB cases in Minnesota from 2012 to 2016, 91% were born outside the U.S. The largest group of cases were persons born in Somalia (44%) and Ethiopia (24%). Among the remaining non U.S.-born persons accounting for at least 5% of all African or African-American TB cases, 7% were from Kenya and 5% were from Liberia.

Laos23%
India14%
Viet Nam14%
Philippines10%
Burma8%
Cambodia7%
Thailand5%
China5%
US5%
Other9%
14
Asian/Asian-American TB Cases by Place of Birth,MN, 2012-2016
N = 242
Presenter
Presentation Notes
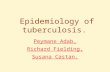
Among Asian or Asian-American TB cases reported in Minnesota from 2012 to 2016, the vast majority (95%) were born outside the U.S. The three largest groups of cases were persons born in Laos (23%), India (14%), and Viet Nam (14%). Among the remaining non U.S.-born persons accounting for at least 5% of all Asian or Asian-American cases, 10% were from the Philippines, followed by those born in Burma (8%), Cambodia (7%), Thailand (5%), and China (5%).

15
TB Cases by HIV Status and Place of Birth, MN, 2012-2016
HIV StatusNon U.S.-Born Cases
No. (%)U.S.-Born Cases
No. (%)Total
No. (%)Negative 596 (92) 120 (92) 716 (92)
Positive 32 (5) 2 (2) 34 (4)
Refused 1 (<1) 1 (<1) 2 (<1)
Not Offered 18 (3) 8 (6) 26 (3)
Total 647 (100) 131 (100) 778 (100)
Presenter
Presentation Notes
Co-infection with HIV is the most significant medical risk factor for progression from latent TB infection to active TB disease. It is estimated that individuals infected with both TB and HIV have up to a 10% annual risk of developing active TB disease, compared to a 5-10% lifetime risk for those with latent TB infection in general. For this reason, TB diagnostic and treatment guidelines recommend that patients with active TB disease receive HIV testing at the time of diagnosis, unless they already are known to be HIV-positive. This slide presents TB cases reported in Minnesota from 2012 through 2016 by HIV status and place of birth. During this time period, 96% of TB cases in Minnesota were tested for HIV. Four percent tested positive for HIV. The prevalence of HIV co-infection among non U.S.-born TB cases was greater than that of U.S.-born TB cases (5% versus 2%, respectively). Of the 28 cases not screened for HIV, the great majority (93%) were not offered the test, while only a small percentage were offered but refused testing. The proportion of TB cases who were not offered HIV testing was higher for U.S.-born than for non U.S.-born individuals (6% versus 3%), although it is recommended for all TB cases, regardless of their place of birth.

16
TB-HIV Co-infected Cases,U.S. and MN, 2007-2016
0
1
2
3
4
5
6
7
8
9
10
% C
o-in
fect
ed
Percent coinfection-U.S. Percent coinfection-MN
U.S. Mean = 8%
MN Mean = 4%
Year No. Co-infected in MN
2007 12
2008 11
2009 7
2010 6
2011 3
2012 6
2013 4
2014 4
2015 9
2016 11
Presenter
Presentation Notes
The TB-HIV co-infection rate has generally been lower in Minnesota than in the United States as a whole. However, since 2015, the Minnesota rate has been equal to or greater than the national rate. On average, 4% of all Minnesota TB cases in the past decade were co-infected with HIV. In comparison, an average of 8% of all TB cases in the U.S. since 2007 were also infected with HIV. The table presents the number of TB cases co-infected with HIV in the past 10 years in Minnesota, ranging from a low of 3 cases in 2011 to a high of 12 cases in 2007. There were 11 TB-HIV cases reported in 2016 in Minnesota.

17
HIV Testing in Persons with TB, MN, 2007-2016
*Alive at time of diagnosis
0
10
20
30
40
50
60
70
80
90
100
0
50
100
150
200
250 % of eligible TB Cases w
/ HIV resultN
o. o
f elig
ible
TB
Case
s*
No. of eligible cases* Percent of eligible cases with HIV result
National objective on HIV testing expandedto all TB patients starting in 2010
Presenter
Presentation Notes
It is critical that all TB patients with an unknown HIV status be screened, since the TB treatment regimen for individuals who are co-infected with HIV is more complex. Starting in 2010, the focus of the national objective for HIV testing of TB cases expanded from those in the 25-44 age group to all age groups. Since this change, the percentage of Minnesota TB cases with a known HIV status has consistently been high, on average over 95%. Conversely, it is also critical that HIV-infected patients be screened for latent TB infection (LTBI), as these individuals are a high priority group for LTBI treatment.

18
TB Cases by Risk Category* and Place of Birth,MN, 2012-2016
0 5 10 15 20 25 30
Incarcerated
Long-term care resident
Homeless
Healthcare worker
Substance abuse†
Other medical condition**
HIV-infected
Travel to TB endemic area
Recent TB contact
% of Cases
AllU.S.-bornNon U.S.-born
*Risk categories are not mutually exclusive**Conditions or therapies risk for progression to active TB disease, not including HIV/AIDS†Excess alcohol use and/or injection or non-injection drug use
Presenter
Presentation Notes
The distribution of risk factors for TB infection and progression to active disease differs greatly by place of birth. Note that a patient can have multiple TB risk factors. Among TB cases reported in Minnesota from 2012 and 2016, patients born in the U.S. were more likely to have been a contact to an infectious TB patient within the past 2 years, have a history of travel to a TB endemic area, have a history of substance abuse or experience homelessness within the year prior to TB diagnosis, and reside in a long-term care facility or correctional facility at the time of diagnosis. Non U.S.-born cases, on the other hand, were more likely to have worked in a healthcare setting in the year preceding their diagnosis, and also more likely to be co-infected with HIV. TB patients born in the U.S. were more likely to report having a medical risk factor for progression to active TB disease (excluding HIV/AIDS): 25% of U.S.-born TB cases compared to 20% of non U.S.-born cases. Among U.S.-born cases, the most commonly reported medical risk factor was an immunosuppressive condition (not HIV/AIDS) or therapy, accounting for 13% of these patients, followed by diabetes (12%). Among non U.S.-born patients, the most commonly reported medical condition was diabetes (12%), followed by an immunosuppressive condition (not HIV/AIDS) or therapy (6%).

19
TB Cases With Other Medical Conditions*by Type of Condition, MN, 2012-2016
Medical conditions**Cases (N=778)
No. (%)Diabetes 92 (12)
Immunosuppressive condition (not HIV/AIDS) or therapy***
59 (8)
End stage renal disease 17 (2)
Weight loss/undernutrition/malabsorption 11 (1)
Other: silicosis, hematologic disease 11 (1)
*Conditions or therapies that increase risk for progression from latent TB infection to active TB disease, not including HIV/AIDS**Patients could have > 1 medical condition***Includes TNF α antagonist therapy and post-organ transplantation
Presenter
Presentation Notes
As mentioned in the previous slide, certain medical conditions, in addition to HIV/AIDS, increase the risk that latent TB infection will progress to active TB disease. The most commonly reported condition was diabetes, accounting for 12% of all TB cases reported in Minnesota during 2012-2016. Eight percent reported having an immunosuppressive condition (not including HIV/AIDS) or were on immunosuppressive therapy at the time of the TB diagnosis. Other conditions were reported by smaller proportions of the TB cases during this time period: end stage renal disease (2%), significant weight loss or undernutrition (1%), and hematologic/reticuloendothelial disease or silicosis (1%). This slide illustrates that screening for tuberculosis (and treatment for latent TB infection, if indicated) should be routinely considered for individuals with these medical conditions.

20
Non U.S.-Born TB Cases by Region of Birth and Year of Diagnosis, MN, 2012-2016
0
10
20
30
40
50
60
70
80
90
2012 2013 2014 2015 2016
Num
ber o
f cas
es
Sub- Saharan Africa South/ Southeast Asia East Asia/ Pacific Latin America/ Caribbean Other*
* “Other” includes: Eastern Europe, North Africa/Middle East, and Western Europe
Presenter
Presentation Notes
This slide depicts the number of TB cases reported in Minnesota from 2012 through 2016 by region of birth and year of diagnosis. The trends seen in this slide are influenced by both the global incidence of TB in specific regions worldwide and also by the changing trends and demographics of immigration to Minnesota. Over the past five years, the number of TB cases reported in Minnesota has been highest among persons originating from sub-Saharan Africa, a region of the world where TB is common. Minnesota is also home to a large population of persons born in South/Southeast Asia, another TB endemic area. Patients from this region accounted for the second largest group of cases.

21
Non U.S.-Born TB Cases by Country of Birth,MN, 2012-2016
Country of Birth No. of Cases (%)
Somalia 170 (26)Ethiopia 90 (14)Laos 56 (9)India 35 (5)Viet Nam 34 (5)Mexico 29 (4)Kenya 27 (4)Other 206 (32)Total 647 (100)
Presenter
Presentation Notes
Among non U.S.-born TB cases reported in Minnesota from 2012 through 2016, the largest percentage (26%) were born in Somalia. Other countries of birth that represented at least 4% of cases included Ethiopia (14%), Laos (9%), India (5%), Viet Nam (5%), Mexico (4%), and Kenya (4%). Patients from a geographically and ethnically diverse group of 51 other countries comprised the remaining 32% of non U.S.-born TB cases reported during this period. This diversity among non U.S.-born TB cases in Minnesota poses challenges for those providing TB prevention, treatment, and control services that are appropriate for persons from such a wide array of cultural, linguistic, and socio-economic backgrounds.

22
Non U.S.-Born TB Cases byVisa Status Upon Arrival in the U.S., MN, 2012-2016
N = 647
Refugee47%
Immigrant29%
Other*19%
Unknown5%
* “Other” includes visitors, tourists, students, and those arriving on employment visas
Presenter
Presentation Notes
Persons arriving as refugees or immigrants seeking permanent residence in the United States are screened prior to immigration for conditions of public health significance, including communicable diseases such as pulmonary TB disease. (It is also recommended that all refugees be screened again within three months of their arrival in the U.S.) Forty-seven percent of the non U.S.-born TB cases reported in Minnesota from 2012 through 2016 initially arrived in the U.S. as refugees, and another 29% arrived as immigrants. Nineteen percent of non U.S.-born TB cases arrived with other non-immigrant visa classifications, including visitors, tourists, students, and those with employment visas; TB screening prior to U.S. arrival is not required for these persons. Visa status was unknown for 5% of non U.S.-born TB cases.

23
Non U.S.-Born TB Cases by Interval Between Arrival in U.S. and Diagnosis of TB, MN, 2012-2016
N = 647
< 1 year20%
1-2 years15%
3-5 years15%
6-9 years13%
10+ years36%
Unknown<1%
Presenter
Presentation Notes
Twenty percent of non U.S.-born TB cases reported in Minnesota from 2012 to 2016 had resided in the United States for less than one year when they were diagnosed with TB disease. These patients most likely acquired latent TB infection outside the U.S. and began progressing to active TB disease prior to or soon after arriving in the U.S. Although many such cases may not be preventable in the U.S., there is additional TB screening required for a number of new arrivals to promptly diagnose active disease and initiate treatment. Most of the non U.S.-born TB patients developed active disease after living in the U.S. for a number of years. Almost 50% of non U.S.-born TB cases reported in Minnesota from 2012-2016 had been in the U.S. for six years or longer prior to being diagnosed with TB disease, the majority developing active disease at least 10 years after arrival. Many of these patients reported advanced age and co-morbidities increasing the likelihood of progressing to active TB disease. These data show the importance of thorough domestic screening of recent arrivals as well as evaluation and treatment of latent TB infection among older populations with co-morbidities.

24
“TB Class” Notifications* Among Refugees/Immigrants Diagnosed with TB within One Year After Arrival to U.S., MN, 2012-2016
* Per results of pre-immigration screening performed overseas
N = 97
No TB Class32%
Class B125%
Class B28%
Unknown35%
Presenter
Presentation Notes
As mentioned in a previous slide, immigrants and refugees undergo medical evaluation, including TB screening, prior to coming to the United States. Individuals with TB-related conditions identified overseas are assigned a TB Class designation, ranging from Class A, which indicates active and potentially infectious TB disease, to Class B1, which may indicate active, non-infectious TB, to Class B2, which indicates latent TB infection. For immigrants and refugees with a TB Class condition, the U.S. Centers for Disease Control and Prevention (CDC) notifies the state public health department where the patient is expected to arrive. State and local public health professionals in Minnesota collaborate to ensure that these individuals are referred to a local health care provider for comprehensive TB evaluation and treatment, as indicated. Among new refugees and immigrants who were diagnosed with TB disease in Minnesota from 2012 to 2016 within one year after their arrival in the U.S., only 33% had a TB Class designation assigned overseas, while 32% had documented overseas screening results showing no indication of a TB Class condition. The results of the overseas medical evaluations were unknown for 35% of these non U.S.-born TB cases. These patients included persons who initially resettled in another U.S. state and whose overseas screening results were not available to the Minnesota Department of Health. These findings strongly suggest that clinicians cannot rely solely on the results of pre-immigration medical examinations performed overseas to identify TB disease among non U.S.-born persons. Clinicians should have a high index of suspicion for TB in any non U.S.-born patient from TB endemic areas who presents with signs or symptoms consistent with active TB disease.

25
TB Cases by Site of Disease, MN, 2012-2016
N = 778
Pulmonary54%Extrapulmonary
33%
Both13% Extrapulmonary
sites of disease*Cases (N=356)**
No. (%)Lymphatic 199 (56)Musculoskeletal 63 (18)Pleural 36 (10)Peritoneal 19 (5)Brain 13 (4)Genitourinary 12 (3)Other 41 (12)
* Patients may have multiple extrapulmonary sites of disease** Includes TB cases with and without concurrent pulmonary disease
Presenter
Presentation Notes
Tuberculosis disease most commonly affects the lungs, although it can affect almost any site in the body. Over half (54%) of the cases reported from 2012 to 2016 had TB disease exclusively in the lungs, and another 13% had TB in both pulmonary and extrapulmonary sites. TB was found exclusively in extrapulmonary sites in 33% of cases. In comparison, 70% of all TB cases reported nationally in 2016 were exclusively pulmonary, 20% exclusively extrapulmonary, and 10% had TB in both sites. Among extrapulmonary TB cases reported in Minnesota from 2012 through 2016, over half (56%) had lymphatic disease. Musculoskeletal (includes the bone/joint and any surrounding muscles or tissues), pleural, and peritoneal TB affected 18%, 10%, and 5% of extrapulmonary TB cases, respectively. Four percent of extrapulmonary cases had TB in the brain, and 3% had TB in the genitourinary system. Forty-one (12%) cases had other extrapulmonary sites of disease that did not fall into any of the previous categories. Note that a person can have more than one extrapulmonary site of disease.

26
TB Cases by Site of Disease and Place of Birth, MN, 2012-2016
0
10
20
30
40
50
60
70
80
90
100
Non U.S.-Born U.S.-Born All
% o
f Cas
es
Pulmonary only Extrapulmonary*
* Includes cases with or without concurrent pulmonary disease
Presenter
Presentation Notes
Extrapulmonary TB occurs more frequently among non U.S.-born persons than among U.S.-born TB cases. Consequently, due to the large proportion of TB cases in Minnesota that occur among non U.S.-born persons, extrapulmonary TB is more common in Minnesota than nationally (46% of Minnesota cases from 2012-2016 compared to only 30% of U.S. cases in 2016). Half of non U.S.-born TB cases reported in Minnesota from 2012 through 2016 had an extrapulmonary site of disease, as compared to only 26% of U.S.-born cases. This slide illustrates the need, especially in Minnesota, for clinicians to have a high index of suspicion for TB particularly for non U.S.-born patients, even when the patient does not present with a cough or abnormal chest radiograph or other common signs and symptoms of pulmonary TB.

27
TB Cases with Pulmonary Involvement by Chest Imaging* Result, MN, 2012-2016
* From initial chest x-ray or chest CT scan
N = 519
Normal< 1%
Abnormal, cavitary TB
30%
Abnormal, non-cavitary TB
68%
Abnormal, not consistent with TB
1%
Presenter
Presentation Notes
A posterior-anterior radiograph of the chest is one of the primary diagnostic tests performed to detect abnormalities suggestive of active pulmonary TB disease. In pulmonary TB, chest x-ray abnormalities often are seen in the apical and posterior upper lobes of the lungs or in the superior segments of the lower lobes. Cavitary lesions are indicative of severe or advanced disease and increase the likelihood of infectiousness in TB patients. In TB patients who are very young or who are co-infected with HIV, pulmonary TB may present with atypical, or even normal radiographic findings. Among 519 pulmonary TB cases reported in Minnesota from 2012 through 2016, the vast majority (98%) had findings from chest imaging (chest x-ray or chest CT scan) consistent with TB disease, including 156 (30%) patients with cavitary lesions. Almost 2% of pulmonary TB cases had chest imaging results that were normal or not consistent with TB disease.

28
TB Cases with Pulmonary Involvement byInitial Sputum AFB Smear Result, MN, 2012-2016
N = 519
Positive38%
Negative48%
Not done*14%
*55% of pulmonary cases without sputum smear results were under 15 years of age
Presenter
Presentation Notes
Persons with pulmonary or laryngeal TB disease may be infectious or able to transmit TB to others. Except for very unusual circumstances, extrapulmonary TB disease is not infectious. The detection of acid-fast bacilli (AFB) in smears of sputum specimens obtained from a patient with pulmonary TB disease is one indicator of the patient’s level of infectiousness. Patients with positive AFB smears from sputum are considered potentially infectious. Although transmission of TB bacteria from sputum AFB smear-negative patients has been documented, such patients are less likely than sputum AFB smear-positive patients to be infectious. Among 519 patients with pulmonary TB disease reported in Minnesota from 2012 through 2016, 38% had at least one initial sputum specimen with an AFB-positive smear result, while almost half had all initial negative AFB smears. These data suggest that close to 40% of pulmonary TB cases in Minnesota likely are infectious and have the potential to spread TB to others prior to receiving several weeks of adequate treatment for TB disease. Fourteen percent had no initial sputum smear result reported. The majority (55%) of these pulmonary patients without sputum smear results were children under the age of 15 years; this reflects the difficulty in obtaining sputum specimens for laboratory confirmation in many pediatric cases. Gastric aspirates are usually recommended for young children.

29
TB Cases by Mycobacterial Culture Result, MN, 2012-2016
N = 778
Positive for M.tbc77%
Negative for M.tbc*20%
Not done3%
*No growth or growth of other Mycobacterium species not part of M.tb complex
Presenter
Presentation Notes
Identification of Mycobacterium tuberculosis (or related species known to cause active disease, collectively called the M. tuberculosis complex) grown in culture from a clinical specimen is the “gold standard” for definitive diagnosis of TB disease, although the national surveillance case definition also allows cases to be counted on the basis of other criteria, which will be described in the next slide. Culture confirmation of TB disease is critically important for the clinical management of TB cases, because most drug susceptibility testing is performed on isolates grown in culture. Also, for pulmonary TB cases, documentation of the conversion of an initially positive culture to a negative culture is an important marker of successful response to TB treatment. Seventy-seven percent of TB cases reported in Minnesota from 2012 through 2016 were confirmed by the identification of M. tuberculosis complex from culture, while 20% had negative culture results. Initial mycobacterial culture was not performed or culture results were not reported for only 3% of cases.

30
TB Cases by Case Verification Criteria*, MN, 2012-2016
N = 778
Lab-confirmed79%
Provider diagnosis2%
Clinical case definition
19%
*Based on the public health surveillance definition for TB [CDC. (2009, June) CDC Tuberculosis Surveillance Data Training: Report of Verified Case of Tuberculosis (RVCT) Instruction Manual. Atlanta, GA: U.S. Department of Health and Human Services,CDC. (Appendix A - Tuberculosis Case Definition for Public Health Surveillance)]
Presenter
Presentation Notes
This slide shows the proportions of TB cases reported in Minnesota from 2012 through 2016 who met the various hierarchical levels of the national surveillance case definition for reportable TB disease. Almost 80% of Minnesota’s TB cases were laboratory-confirmed: counted on the basis of a culture that was positive for M. tuberculosis complex, or less commonly, a positive nucleic acid amplification test for TB, or demonstration of acid-fast bacilli when cultures could not be done. Lab tests were either negative for M. tuberculosis complex or not done in the remaining 21% of cases. Most of those patients (19% of all cases) met the clinical component of the national TB case definition: they had a positive tuberculin skin test (TST) or positive interferon gamma release assay (IGRA, or TB blood test), but no laboratory confirmation of TB. Very few (2%) cases met neither the laboratory nor the clinical case criteria and, therefore, were counted solely on the basis of a provider diagnosis.

31
TB Cases by Drug Susceptibility Patterns and Year,MN, 2012-2016
Year
Cases With Susceptibility
Results*
Any DrugResistance†
No. (%)
INH-Resistant**
No. (%)MDR-TB‡No. (%)
2012 124 23 (19) 12 (10) 1 (<1)
2013 113 24 (21) 13 (12) 0 (0)
2014 105 25 (24) 19 (18) 1 (1)
2015 115 16 (14) 9 (8) 0 (0)
2016 136 29 (21) 19 (14) 8 (6)
Total 593 117 (20) 72 (12) 10 (2)
* Culture-confirmed cases with drug susceptibility results available† Resistance to at least one first-line anti-TB drug [i.e., isoniazid (INH), rifampin (RIF), pyrazinamide (PZA), or ethambutol (EMB)]** INH-resistant cases may also be resistant to other drugs‡ Multi-drug resistant TB, defined as resistance to at least INH and rifampin
Presenter
Presentation Notes
Drug-resistant TB is a serious public health concern globally, nationally, and in Minnesota. This slide presents drug susceptibility data among culture-confirmed TB cases reported in Minnesota from 2012 through 2016. Drug susceptibility testing is performed on all culture-confirmed TB cases reported in Minnesota unless an isolate is unavailable for testing. Among culture-confirmed TB cases, 20% were resistant to at least one first-line anti-TB medication [i.e., isoniazid (INH), rifampin (RIF), pyrazinamide (PZA), or ethambutol (EMB)]. This includes 12% of cases who were resistant to at least INH and 2% who were multidrug-resistant, which is defined as resistance to at least INH and rifampin, two of the most effective TB medications. There were no cases in this time period with extensively drug-resistant TB (XDR-TB), which is a type of MDR-TB with additional resistance to any fluoroquinolone and at least one of three injectable second-line medications. In 2016, there was a substantial increase in MDR-TB in Minnesota compared to previous years; 8 of the 10 cases during this 5-year time period were reported in that year.

TB Cases by Drug Susceptibility Patterns and Place of Birth, MN, 2012–2016
Place of birth
Cases With Susceptibility
Results*
Any DrugResistance†
No. (%)
INH-Resistant**
No. (%)MDR-TB‡No. (%)
Non U.S.-Born Cases
506 106 (21) 64 (13) 9 (2)
U.S.-Born Cases 87 11 (13) 8 (9) 1 (1)Total 593 117 (20) 72 (12) 10 (2)
32
* Culture-confirmed cases with drug susceptibility results available† Resistance to at least one first-line anti-TB drug [i.e., isoniazid (INH), rifampin (RIF), pyrazinamide (PZA), or ethambutol (EMB)]** INH-resistant cases may also be resistant to other drugs‡ Multi-drug resistant TB, defined as resistance to at least INH and rifampin
Presenter
Presentation Notes
Among culture-confirmed TB cases reported in Minnesota from 2012 through 2016, non U.S.-born cases were approximately 1.6 times more likely than U.S.-born cases to be resistant to any first-line anti-TB drug and 1.4 times more likely than U.S.-born cases to be resistant to isoniazid (INH), in particular. The rates of multidrug-resistant TB, or MDR-TB, were also higher among those born outside the U.S. compared to U.S.-born cases.

33
TB Cases by Method of Case Identification, MN, 2012-2016
Method of Identification No. of Cases (%)
TB symptoms 629 (81)
TB contact investigations 35 (4)
Overseas TB Class follow-up 27 (3)
Other targeted testing 24 (3)
Domestic refugee health exam 23 (3)
Incidental chest X-ray or lab result 20 (3)
Other* 20 (3)
Total 778 (100)
* “Other” includes: other immigration exam (1%) and employment screening including health care worker screening (2%)
Presenter
Presentation Notes
While the vast majority (81%) of TB cases reported in Minnesota from 2012 through 2016 were identified as a result of patients presenting at clinics or hospitals with symptoms of TB disease, a number of cases were identified from TB screening or other active case finding methods. Four percent of TB cases were found as a result of contact investigations conducted by local health departments surrounding individuals with infectious TB. Three percent were identified through the domestic health assessment recommended for all refugees within three months of their arrival in the U.S., and another 3% were identified during follow-up evaluations of newly-arrived immigrants and refugees designated as having a TB Class condition during an overseas examination. Other immigration exams (such as change of status exams) accounted for 1% of TB cases. Three percent of cases were identified through other targeted testing, including TB screening of international students in colleges or overseas adoptees. Screening for employment purposes identified another 2% of cases. The remaining 3% of TB cases reported during this time period were identified as a result of laboratory or radiologic tests performed for reasons other than suspected TB disease.

34
TB Cases by Mode of Treatment Administration, MN, 2012-2016
Year Started treatment At least some DOT* Completely self-administered2012 160 99% 1%2013 150 99% <1%2014 146 98% 2%2015 146 99% <1%2016 167 98% 2%Total 769 99% 1%
* DOT = Directly Observed Therapy
Type of Provider Started treatment At least some DOT* Completely self-administeredPublic 452 99% <1%Private only 317 97% 3%
Presenter
Presentation Notes
The last three slides present data on the treatment and clinical management of TB cases in Minnesota. This slide presents the mode by which TB treatment was administered for TB cases reported in Minnesota from 2012 through 2016. On average, over 99% of cases received at least some portion of their TB medication through Directly Observed Therapy (DOT). DOT, which involves having a health care provider or trained outreach worker observe a TB patient taking each dose of TB medications, is the recommended standard of care for the treatment of TB disease. During this five-year period, at most only 2% of TB cases reported each year self-administered their entire course of TB treatment. The widespread use of DOT in Minnesota is facilitated by the work of the local and tribal public health nurses in each county who are primarily responsible for administering DOT for TB cases in their jurisdictions. Local and tribal public health departments throughout Minnesota provide DOT at no cost, regardless of whether the patient is being treated by a private or public provider. This slide illustrates that, among TB cases reported in Minnesota from 2012 through 2016, the use of DOT was more common among patients who received treatment for TB disease at public health clinics than among patients who received TB treatment exclusively from private clinicians. Treatment for 3% of TB cases managed by private providers was exclusively self-administered, whereas only one TB case (accounting for <1%) treated at public TB clinics received self-administered therapy exclusively.

35
Treatment Completion and Length of Therapy Among TB Cases,MN, 2011-2015
Year Started Treatment*
CompletedWithin 12 mos.**
No. (%)
CompletedOverall**No. (%)
2011 101 96 (95) 97 (96)2012 133 127 (96) 130 (98)2013 125 118 (94) 123 (98)2014 122 113 (93) 120 (98)2015 125 119 (95) 122 (98)Total 606 573 (95) 592 (98)
* Patients for whom < 12 months of therapy is indicated. This excludes: patients with rifampin resistance, meningeal TB, TB inbone or skeletal system, TB in CNS, children 14 years of age or younger with disseminated TB, patients who died or moved out of US within 366 days of starting treatment.** Treatment completion data as of 3/12/2018
Presenter
Presentation Notes
This slide presents the outcome of treatment for the TB cases reported in Minnesota from 2011 to 2015 for whom 12 months or less of treatment was indicated. (2015 is the most recent annual cohort of patients for whom data on treatment outcome is complete.) This slide excludes patients with rifampin-resistant or meningeal TB, TB in the bone or central nervous system, and pediatric patients with disseminated TB, all of whom require a longer course of treatment. It also excludes patients who died or moved outside of the U.S. within one year of starting treatment. While most uncomplicated cases of TB disease are eligible for 6-9 months of treatment, the Centers for Disease Control and Prevention (CDC) has established an objective of 95% of TB cases completing adequate therapy within 12 months by 2020, which allows a margin of error for the often unavoidable obstacles that can prolong therapy. These data indicate that the great majority (95%) of eligible TB cases reported in Minnesota from 2011 to 2015 successfully completed an adequate course of treatment within one year, meeting the CDC objective for 2020. When looking at whether these eligible cases have ever completed a full course of TB treatment, regardless of duration, the proportion increases to 98%.

36
TB Cases by Type(s) of Provider*, MN, 2012-2016
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012 2013 2014 2015 2016
% o
f Cas
es
Public health Both public and private/other Private/other
* Some patients are managed by multiple providers throughout disease course
Presenter
Presentation Notes
The three public TB clinics in Minnesota that manage patients with active TB disease are located in Hennepin, Ramsey and Olmsted counties. From 2012 to 2016, an average of 58% of all TB patients were followed by at least one of these public clinics at some point in their disease course, while 42% were followed solely by private clinics or hospitals, or, less commonly, by Veteran Administration hospitals, correctional facility medical staff, or Indian Health Service. In 2016, the percentages were 59% and 41%, respectively.
Related Documents