1 Unit 6 ©2014 Barkley & Associates Unit 6 ©2014 Barkley & Associates Advanced Pharmacology: Endocrine Pharmacology Part I Thomas W. Barkley, Jr., PhD, ACNP‐BC, FAANP President, Barkley & Associates www.NPCourses.com and Professor of Nursing Director of Nurse Practitioner Programs California State University, Los Angeles Robert Fellin, Pharm.D., BCPS Lecturer, Barkley & Associates Clinical Pharmacist Cedars‐Sinai Medical Center Los Angeles, CA Unit 6 ©2014 Barkley & Associates Unit 6 ©2014 Barkley & Associates The Endocrine System • Comprised of various glands that secrete hormones (chemical messengers released in response to a change in the body’s internal homeostasis)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Advanced Pharmacology:Endocrine Pharmacology Part I
Thomas W. Barkley, Jr., PhD, ACNP‐BC, FAANPPresident, Barkley & Associates
www.NPCourses.comand
Professor of NursingDirector of Nurse Practitioner Programs
California State University, Los Angeles
Robert Fellin, Pharm.D., BCPSLecturer, Barkley & Associates
Clinical Pharmacist Cedars‐Sinai Medical Center
Los Angeles, CA
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
The Endocrine System• Comprised of various glands
that secrete hormones (chemical messengers released in response to a change in the body’s internal homeostasis)

2
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Hypothalamus and Pituitary: Physiology Review
• Hypothalamus: secretes releasing hormones pituitary
• Releasing hormones trigger the pituitary to know which hormones are to be released
• Hypothalamus secretes thyrotropin-releasing hormone (TRH) pituitary secrete TSH thyroid hormones
• Pituitary
• Anterior (adenohypophysis): consists of glandular tissue and secretes ACTH, TSH, growth hormone, prolactin, FSH and LH
• Posterior (neurohypophysis): contains nervous tissue rather than glandular, and neurons in the posterior pituitary store ADH and oxytocin (released in response from nerve stimulation in the hypothalamus)
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Hypothalamic & Pituitary Hormones
Pharmacology for Nurses: A Pathophysiologic Approach (4th Edition)
3
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
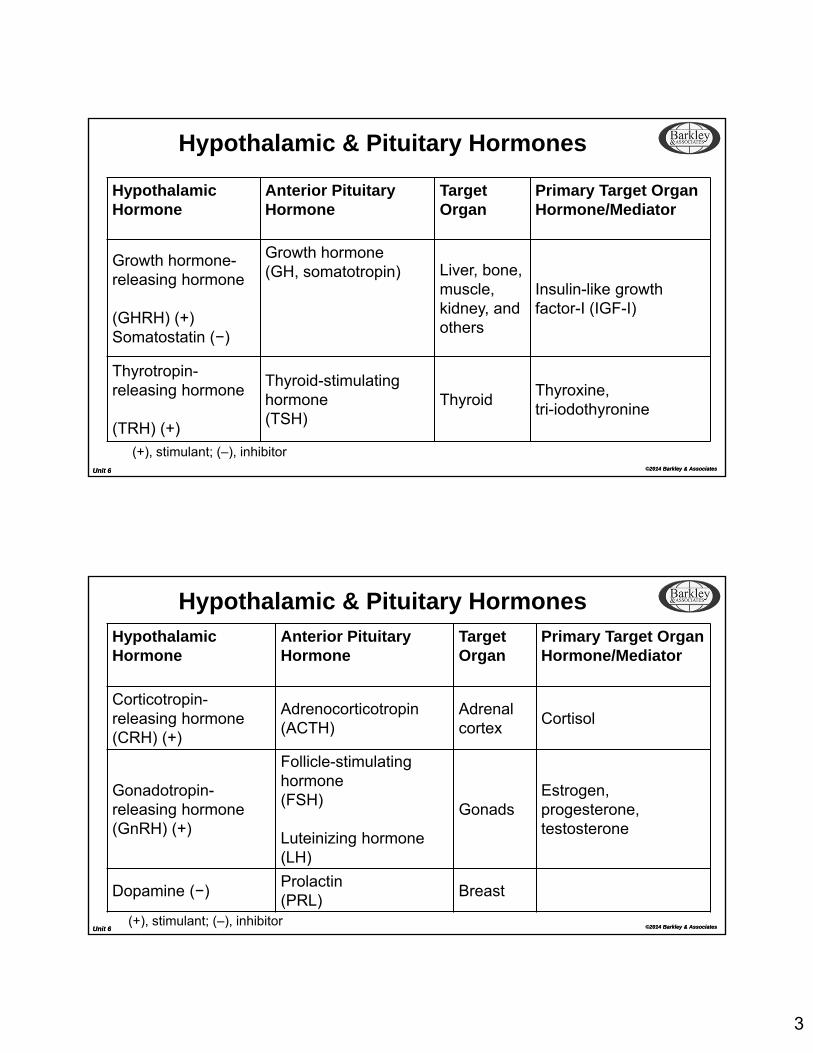
Hypothalamic & Pituitary Hormones
Hypothalamic Hormone
Anterior Pituitary Hormone
Target Organ
Primary Target Organ Hormone/Mediator
Growth hormone-releasing hormone
(GHRH) (+)Somatostatin (−)
Growth hormone(GH, somatotropin) Liver, bone,
muscle, kidney, and others
Insulin-like growth factor-I (IGF-I)
Thyrotropin-releasing hormone
(TRH) (+)
Thyroid-stimulating hormone(TSH)
ThyroidThyroxine,tri-iodothyronine
(+), stimulant; (–), inhibitor
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Hypothalamic & Pituitary HormonesHypothalamic Hormone
Anterior Pituitary Hormone
Target Organ
Primary Target Organ Hormone/Mediator
Corticotropin-releasing hormone (CRH) (+)
Adrenocorticotropin(ACTH)
Adrenal cortex
Cortisol
Gonadotropin-releasing hormone (GnRH) (+)
Follicle-stimulating hormone(FSH)
Luteinizing hormone(LH)
GonadsEstrogen, progesterone, testosterone
Dopamine (−)Prolactin(PRL)
Breast
(+), stimulant; (–), inhibitor

4
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Clinical Uses of Hypothalamic Hormones
Hypothalamic Hormone Clinical UsesGrowth hormone-releasing hormone(GHRH)
Used rarely as a diagnostic test for GH and GHRH sufficiency
Thyrotropin-releasing hormone(TRH, protirelin)
May be used to diagnose TRH or TSH deficiencies
Corticotropin-releasing hormone(CRH)
Used rarely to distinguish Cushing's disease from ectopic ACTH secretion
Gonadotropin-releasing hormone(GnRH)
May be used in pulses to treat infertility caused by GnRH deficiency
Dopamine Dopamine agonists (bromocriptine, cabergoline) used for treatment of hyperprolactinemia
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Anterior Pituitary AgentsGROWTH HORMONE (GH)somatropinMOA: Recombinant form of human GH; acts through GH
receptors to increase production of IGF-I
Effects: Restores normal growth and metabolic GH effects in GH-deficient individuals Increases final adult height in some children with short stature not due to GH deficiency
Clinical Applications:
Replacement in GH deficiency Increased final adult height in children with certain conditions associated with short statureWasting in HIV infectionShort bowel syndrome

5
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Anterior Pituitary AgentsSOMATOSTATIN ANALOGSoctreotide, lanreotide
MOA: Agonist at somatostatin receptors
Effects: Inhibits production of GH and, to a lesser extent, of TSH, glucagon, insulin and gastrin
Clinical Applications:
Acromegaly and several other hormone-secreting tumors Octreotide: Acute control of bleeding from esophageal varicesLanreotide: similar to octreotide; available as a long-acting formulation for acromegaly
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Anterior Pituitary AgentsIGF-I AGONISTmecaserminMOA: Recombinant form of IGF-I that stimulates IGF-I receptors
Effects: Improves growth and metabolic IGF-I effects in individuals with IGF-I deficiency due to severe GH resistance
Clinical Applications: Replacement in IGF-I deficiency that is not responsive to exogenous GH
GH RECEPTOR ANTAGONISTpegvisomantMOA: Blocks GH receptorsEffects: Ameliorates effects of excess GH production
Clinical Applications: Acromegaly

6
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Anterior Pituitary AgentsHormone Diagnostic Use
Thyroid-stimulating hormone(TSH; thyrotropin)
In patients who have been treated surgically for thyroid carcinoma, to test for recurrence by assessing TSH-stimulated whole-body 131I scans and serum thyroglobulin determinations
Adrenocorticotropin(ACTH, Cosyntropin)
In patients suspected of adrenal insufficiency, either central (CRH/ACTH deficiency) or peripheral (cortisol deficiency), in particular in suspected cases of congenital adrenal hyperplasia
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Posterior Pituitary AgentsOXYTOCINMOA: Activates oxytocin receptorsEffects: Increased uterine contractionsClinical Applications:
Induction and augmentation of laborControl of uterine hemorrhage after delivery
OXYTOCIN RECEPTOR ANTAGONISTAtosibanMOA: Blocks oxytocin receptorsEffects: Decreased uterine contractionsClinical Applications:
Tocolysis for preterm labor

7
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Posterior Pituitary AgentsVASOPRESSIN RECEPTOR AGONISTSdesmopressin, vasopressinMOA: relatively selective vasopressin V2 receptor agonistEffects: Acts in the kidney collecting duct cells to decrease the excretion
of water; acts on extrarenal V2 receptors to increase factor VIII and von Willebrand factor
Clinical Applications:
Pituitary diabetes insipidus; pediatric primary nocturnalEnuresis; Hemophilia A and von Willebrand disease
VASOPRESSIN RECEPTOR ANTAGONISTconivaptan, tolvaptanMOA: Antagonist of vasopressin V1a and V2 receptors
Effects: Increase in water excretion, decrease in urine osmolality, increased serum sodium concentration
Clinical Applications:
Reduced renal excretion of water in conditions associated with increased vasopressin; hyponatremia in hospitalized patients
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Thyroid Physiology• Thyroid gland secretes hormones to
normalize growth and development, body temperature and energy levels
• Follicular cells in the gland secrete thyroid hormone, which actually consists of two different hormones:
• thyroxine (T4)
• tri-iodothyronine (T3)
• Parafollicular cells secrete calcitonin, a hormone that is involved with calcium homeostasis
Ph
arm
aco
log
y for N
urse
s: A P
ath
op
hysio
log
icA
pp
roa
ch (4
th E
ditio
n)
8
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
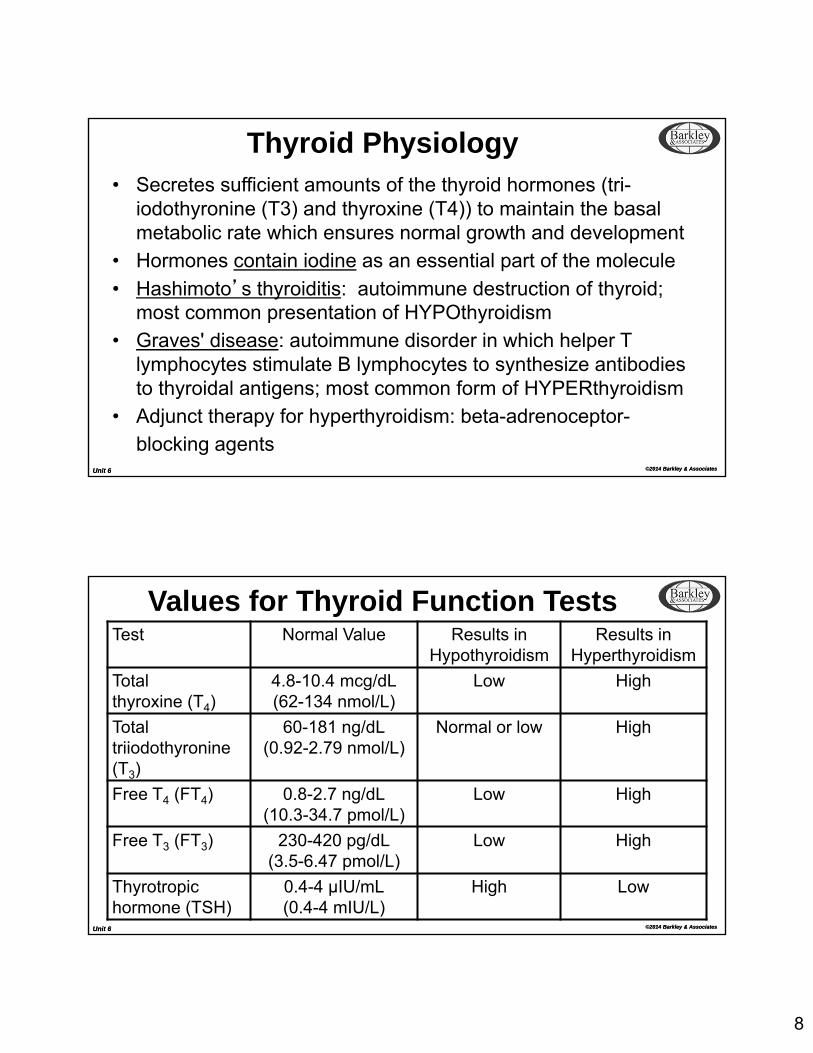
Thyroid Physiology• Secretes sufficient amounts of the thyroid hormones (tri-
iodothyronine (T3) and thyroxine (T4)) to maintain the basal metabolic rate which ensures normal growth and development
• Hormones contain iodine as an essential part of the molecule
• Hashimoto’s thyroiditis: autoimmune destruction of thyroid; most common presentation of HYPOthyroidism
• Graves' disease: autoimmune disorder in which helper T lymphocytes stimulate B lymphocytes to synthesize antibodies to thyroidal antigens; most common form of HYPERthyroidism
• Adjunct therapy for hyperthyroidism: beta-adrenoceptor-
blocking agents
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Values for Thyroid Function TestsTest Normal Value Results in
HypothyroidismResults in
Hyperthyroidism
Totalthyroxine (T4)
4.8-10.4 mcg/dL(62-134 nmol/L)
Low High
Totaltriiodothyronine(T3)
60-181 ng/dL(0.92-2.79 nmol/L)
Normal or low High
Free T4 (FT4) 0.8-2.7 ng/dL(10.3-34.7 pmol/L)
Low High
Free T3 (FT3) 230-420 pg/dL(3.5-6.47 pmol/L)
Low High
Thyrotropic hormone (TSH)
0.4-4 μIU/mL(0.4-4 mIU/L)
High Low

9
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Thyroid Agentslevothyroxine (T4) (Levothroid, Synthroid), liothyronine (T3) (Cytomel, Triostat), liotrix (Thyrolar),thyroid (Armour Thyroid, Thyroid USP)MOA: Activation of nuclear receptors results in gene
expression with RNA formation and protein synthesis
Indication: Hypothyroidism
Comments: Maximum effect seen after 6–8 weeks of therapyToxicity: symptoms of thyroid excess
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Anti-Thyroid AgentsTHIOAMIDES:methimazole (Tapazole), propylthiouracil (PTU)
MOA: Inhibit thyroid peroxidase reactions block iodine organification inhibit peripheral deiodination of T4 and T3 (primarily PTU)
Indication: Hyperthyroidism
Comments: OralDelayed onset of actionMethimazole duration of action: 24 hoursPTU duration of action: 6–8 hours

10
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Anti-Thyroid AgentsIODIDES: Lugol's solution, potassium iodide
MOA: Inhibit organification and hormone release reduce the size and vascularity of the gland
Indication: Preparation for surgical thyroidectomy
Comments: Oral; acute onset within 2–7 days
RADIOACTIVE IODINE131I (RAI)
MOA: Radiation destruction of thyroid parenchyma
Indication: Hyperthyroidism
Comments: Oral; half-life 5 days; onset of 6–12 weeks, maximum effect in 3–6 months; patients should be euthyroid or on beta-blockers before RAI; avoid in pregnancy/nursing mothers
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Adrenal Glands: Physiology ReviewSecrete 3 essential classes of steroids:1. Gonadocorticoids:
Androgens > estrogens (less than testes or ovaries)2. Mineralocorticoids:
Aldosterone accounts for 95% Primary function is to regulate plasma volume (promote Na reabsorption and K
excretion by the renal tubules) Decreased plasma volume kidneys secrete renin production of angiotensin II aldosterone secretion promotes Na and water retention
Hyperaldosteronism: excessive aldosterone secretion usually a result of adrenal tumors, characterized by HTN and hypokalemia
3. Glucocorticoids: More than 30 glucocorticoids are secreted Cortisol (hydrocortisone) secreted in highest amount Influence the function of most cells in the body
11
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Glucocorticoids• Wide range of physiologic effects, including regulation of intermediary
metabolism, cardiovascular function as well as growth and immunity
• Hydrocortisone (cortisol): most important pharmacologically; prepares the body for long-term stress
• Glucocorticoids & mineralocorticoids also called corticosteroids or adrenocortical hormones
• Glucocorticoid & corticosteroid often used interchangeably, however “corticosteroid” implies both glucocorticoid and mineralocorticoid activity
• Corticosteroids: primarily used as replacement therapy for adrenal insufficiency (lack of corticosteroid) and reduce inflammation & immune response
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
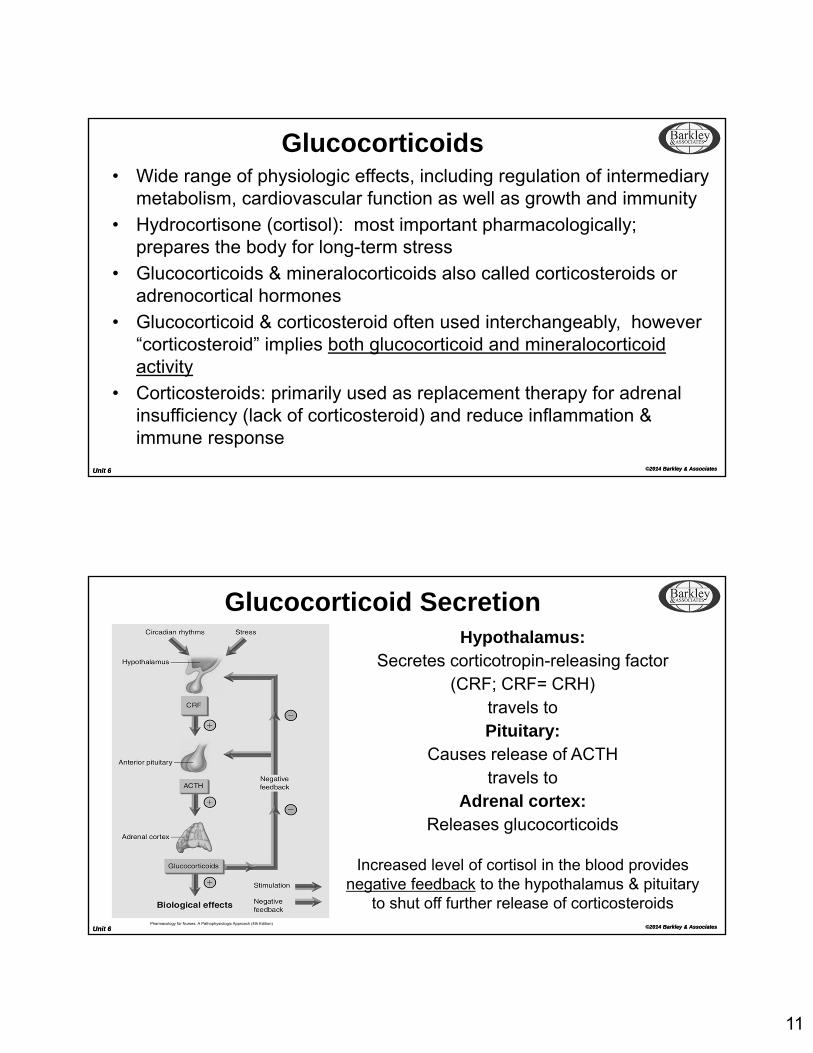
Glucocorticoid SecretionHypothalamus:
Secretes corticotropin-releasing factor(CRF; CRF= CRH)
travels toPituitary:
Causes release of ACTHtravels to
Adrenal cortex:Releases glucocorticoids
Increased level of cortisol in the blood provides negative feedback to the hypothalamus & pituitary
to shut off further release of corticosteroidsPharmacology for Nurses: A Pathophysiologic Approach (4th Edition)

12
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Effects of GlucocorticoidsPhysiologic Effects Permissive effects: without glucocorticoids many normal
functions become deficient: response of vascular and bronchial smooth muscle to catecholamines is diminished in the absence of cortisol and restored by physiologic amountsEffects are dose-related: become magnified when large amounts are administered
Metabolic Effects Influence carbohydrate, protein and fat metabolism; stimulategluconeogenesis
Catabolic and Anti-anabolic Effects
Involved in lymphoid and connective tissue, muscle, peripheral fat, bone and skin
Anti-Inflammatory & Immunosuppressive Effects
Reduce inflammation through suppression of inflammatory cytokines; inhibit macrophage function; reduce prostaglandin synthesis
Other Effects Influence the nervous system; produce behavioraldisturbances, suppress pituitary release of ACTH, GH, TSH
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Select Indications for GlucocorticoidsIndication CommentsAdrenocortical Insufficiency Acute: Initiate treatment immediately
hydrocortisone (usually large doses initially) supplementation with mineralcorticoid (fludrocortisone) is delayed until hydrocortisone is reduced to 50 mg/day
Chronic(Addison's Disease):
Hydrocortisone supplemented with a mineralocorticoid (fludrocortisone)

13
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Select Indications for Glucocorticoids
Indication Comments
Use of Glucocorticoids for Diagnostic PurposesDexamethasonesuppression test
Diagnosis of Cushing's syndrome
Cosyntropin stimulation test
Diagnose or exclude primary and secondary adrenal insufficiency; Measurement of cortisol in serum for evaluation of adrenal dysfunctionCosyntropin 250 mcg IV x1 then check cortisol level at 30 minutes and 60 minutes
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Select Indications for GlucocorticoidsIndication Comments
Hyperaldosteronism
Primary: usually results from excessive production of aldosterone by an adrenal adenoma
Secondary: spironolactone, an aldosterone receptor-blocking agent can be used
MiscellaneousCorticosteroids and stimulation of lung maturation in the fetus
When delivery is anticipated before 34 weeks of gestation, intramuscular betamethasone 12 mg, followed by an additional dose of 12 mg 18-24 hours later, is commonly used
14
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Select Indications for Glucocorticoids Nonadrenal Disorders
Allergies (seasonal rhinitis) Chronic inflammatory bowel disease Asthma and COPD Edematous states caused by hepatic, neurological and renal
disorders Neoplastic disease Post-transplant surgery Rheumatic diseases Shock Skin disorders (rashes, contact dermatitis, etc.)
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Glucocorticoids Many drug-drug interactions
• Hyperglycemic effects may reduce effectiveness of the anti-diabetic agents
• Combining with NSAIDs increase risk for PUD
• Administering with non-potassium-sparing diuretics hypokalemia and hypocalcemia
Glucocorticoid prescribing strategies:
• Use lowest possible dose to achieve therapeutic effect
• Administer every other day to limit adrenal atrophy
• Acute conditions: large amounts for a few days, then gradually decrease the dose until discontinued
• Use inhalation, topical or intra-arterial routes to reduce the possibility of systemic effects
Long-term administration Cushing’s syndrome
15
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
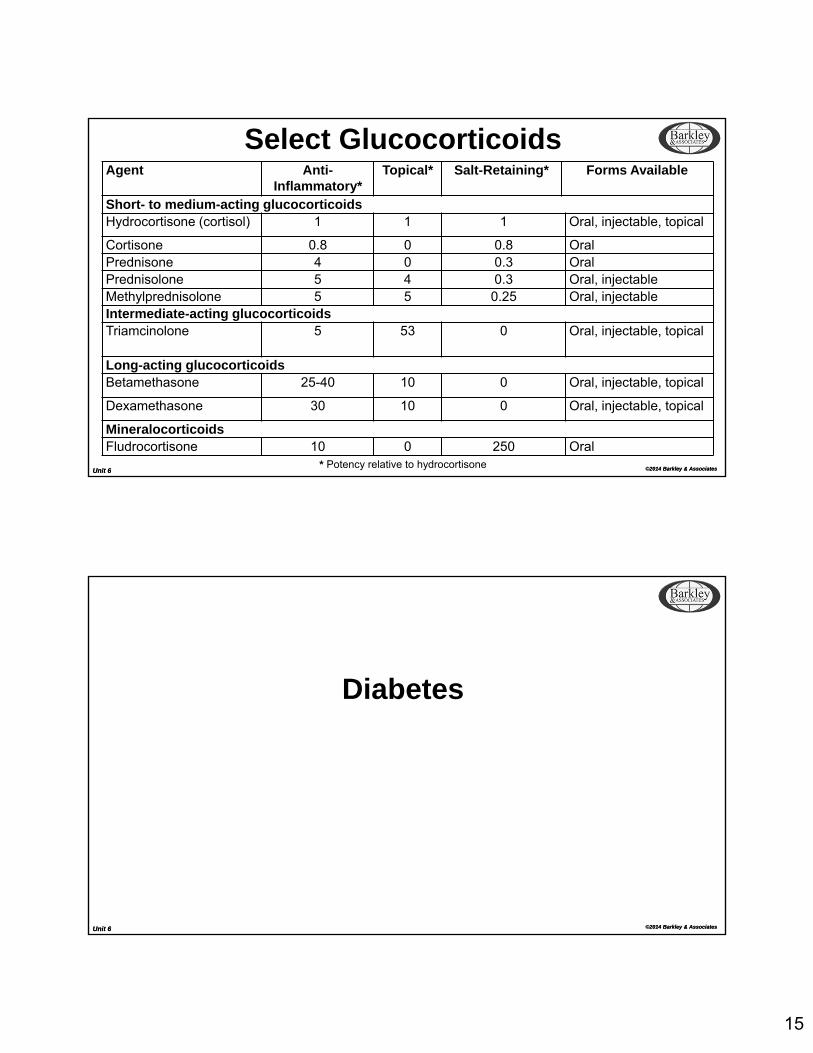
Select GlucocorticoidsAgent Anti-
Inflammatory*Topical* Salt-Retaining* Forms Available
Short- to medium-acting glucocorticoidsHydrocortisone (cortisol) 1 1 1 Oral, injectable, topical
Cortisone 0.8 0 0.8 OralPrednisone 4 0 0.3 OralPrednisolone 5 4 0.3 Oral, injectableMethylprednisolone 5 5 0.25 Oral, injectableIntermediate-acting glucocorticoidsTriamcinolone 5 53 0 Oral, injectable, topical
Long-acting glucocorticoidsBetamethasone 25-40 10 0 Oral, injectable, topical
Dexamethasone 30 10 0 Oral, injectable, topical
MineralocorticoidsFludrocortisone 10 0 250 Oral
* Potency relative to hydrocortisone
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Diabetes

16
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Common Early MorningHyperglycemia Problems
Dawn Phenomenon: results when tissue becomes desensitized to insulin nocturnally – blood glucose becomes progressively elevated throughout the night
Tx: Add or increase the bedtime dose of insulin
Somogyi Effect: nocturnal hypoglycemia develops, stimulating a surge of counter regulatory hormones which raises blood sugar
Tx: Reduce or omit bedtime dose of insulin
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
BiguanidesIndications: DOC; first line therapy for Type 2 DMAgents: metformin (Glucophage)MOA: decreases hepatic gluconeogenesis, improves insulin
sensitivity, increases glucose utilization by muscle
Adverse
Effects:
nausea, vomiting, diarrhea, decreased appetite, lactic acidosis
Comments: Liver disease: avoid metformin
Contraindicated: renal dysfunction (serum creatinine >1.5 mg/dL (males) or 1.4 mg/dL (females)); monitor serum creatinine
Promotes weight loss
Special instructions for patients who require contrast

17
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Insulin SecretagoguesIndications: Monotherapy or combination therapy for Type 2 DMAgents: nateglinide (Starlix), repaglinide (Prandin)MOA: stimulates insulin release from pancreasAdverse
Effects:
hypoglycemia, diarrhea, arthralgia, headache, sinusitis, upper respiratory infection
Comments: Liver disease: use with caution
May require dose adjustment for renal dysfunction
Several drug-drug interactions
Rapid onset (given with meals)
Short duration of action (requires TID dosing)
Nonsulfonylureas (Glinides)
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Insulin SecretagoguesIndications: Monotherapy or combination therapy for Type 2 DMAgents: chlorpropamide (Diabinese), tolazamide (Tolinase),
tolbutamide (Tol-Tab), glyburide (Diabeta, Micronase), glipizide (Glucotrol), glimepiride (Amaryl)
MOA: stimulates insulin release from pancreas, enhances beta cell sensitivity to glucose
AdverseEffects:
hypoglycemia, nausea, bloating, weight gain, photosensitivity, disulfiram reaction (chlorpropamide)
Comments: Use with caution in liver dysfunctionDose adjustment required for renal dysfunction Several drug-drug interactionsOver time response to therapy may diminishSulfonylureas

18
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
ThiazolidinedionesIndications: Monotherapy or combination therapy for Type 2 DM
Agents: pioglitazone (Actos), rosiglitazone (Avandia)
MOA: increases receptor sensitivity to insulin, decreases both insulin resistance and hepatic gluconeogenesis
AdverseEffects:
hepatotoxicity, weight gain, peripheral edema, rash, macular edema, heart failure exacerbation, increased risk of MI (rosiglitazone)
Comments: Use with caution (if at all) in liver dysfunctionBaseline LFT’s then periodically thereafterSeveral drug-drug interactionsContraindicated in NYHA class III or IVMay increase risk of osteoporosisMay increase risk of bladder cancer (pioglitazone)REMS program (rosiglitazone)
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Alpha-glucosidase InhibitorsIndications: Adjunct therapy only for Type 2 DMAgents: acarbose (Precose), miglitol (Glyset)MOA: reduces rate and extent of CHO digestion and
absorptionAdverseEffects:
flatulence, diarrhea, abdominal pain, decrease absorption of iron (anemia)
Comments: Do not use in renal dysfunction (creatinine > 2.0)Baseline LFT’s then periodically thereafter (acarbose)May influence the absorption of other drugsContraindicated in malabsorption, IBD or intestinal obstructionGlucose (dextrose) is recommended for treating hypoglycemia as sucrose metabolism is inhibited

19
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Glucagon-Like Peptide-1 AgonistsIndications: Monotherapy (exenatide) or combination therapy for Type 2
DM; generally considered as adjunctAgents: exenatide (Byetta), liraglutide (Victoza)MOA: increase insulin release in the presence of elevated glucose
concentrations, decrease glucagon secretion in a glucose-dependent manner and delay gastric emptying
AdverseEffects:
nausea, vomiting, diarrhea, headache, hypoglycemia, pancreatitis, teratogenic, injection site reactions, renal failure, thyroid tumors
Comments: Several drug-drug interactionsContraindicated in severe renal dysfunction (both), h/o pancreatitis (both) or h/o thyroid cancer (liraglutide)Does NOT replace insulinREMS program
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Dipeptidyl Peptidase-4 InhibitorsIndications: Monotherapy or combination therapy for Type 2 DM;
generally considered as adjunct therapyAgents: sitagliptin (Januvia), saxagliptin (Onglyza), linagliptin
(Tradjenta)MOA: Inhibit the degradation of GIP and GLP-1Adverse
Effects:
increased risk of infection, headache, hypoglycemia, pancreatitis, hypersensitivity reactions, peripheral edema (saxagliptin)
Comments: Several drug-drug interactions (saxagliptin)
Contraindicated in ESRD (sitagliptin, saxagliptin)
Dose adjustment in renal impairment (sitagliptin, saxagliptin)

20
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associateshttp://casesblog.blogspot.com/2006/11/dpp-4-inhibitors-for-treatment-of.html
GLP-1 and DPP-4 MOA:
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Amylin Receptor AgonistsIndications: Adjunct therapy for Type 1 and Type 2 DM
Agents: pramlintide (Symlin)MOA: Inhibit the degradation of GIP and GLP-1AdverseEffects:
abdominal pain, loss of appetite, nausea, vomiting,hypoglycemia, dizziness, headache, cough, fatigue
Comments: Contraindicated in patients with hypoglycemic unawareness or gastroparesisBlack box warning for individuals while drivingSevere hypoglycemia with concurrent insulin or oral hypoglycemic agentWhen initiating pramlintide: reduce dose of any secretagogues; reduce insulin dose by at least 50%

21
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Sodium Glucose Cotransporter 2 (SGLT2) InhibitorIndications: Type 2 DM; place in therapy currently unclear
Agents: canagliflozin (Invokana)MOA: increases the excretion of urinary glucose
AdverseEffects:
polyuria, UTI, genital mycotic infections, hypovolemia, hyperkalemia, pancreatitis, renal impairment
Comments: Adjust dose in renal impairmentAvoid use in severe liver impairmentCan cause severe hypoglycemiaSafety/effectiveness not established in patients younger than 18 yearsLong-term safety issues (cardiovascular, cancer risk)Role not addressed in recent ADA guidelinesMore clinical trials will better establish their role
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Insulin PreparationsInsulin Preparation Onset of Action
(hours)Peak Action
(hours)Duration of Action
(hours)
Rapid-Acting:
Insulin Lispro (Humalog)
5-15 minutes 30-90 minutes < 5Insulin Aspart (NovoLog)
Insulin Glulisine (Apidra)
Short-Acting:
Regular insulin (Humulin R)
0.5-1 2-4 5-7

22
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Insulin PreparationsInsulin Preparation
Onset of Action(hours)
Peak Action(hours)
Duration of Action(hours)
Intermediate-Acting:
NPH 2-4 4-12 12-18
Long-Acting:
Insulin glargine (Lantus)
1.5 No pronounced
peak
20-24
Insulin detemir (Levemir)
0.8-2 Relatively flat
5.7-23.2
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Insulin PreparationsPremixed Insulin Brand Name
NPH/regular (70%/30%) Humulin 70/30Novolin 70/30
Insulin aspart protamine suspension/insulin aspart (70%/30%)
NovoLog Mix 70/30
Insulin lispro protamine suspension/insulin lispro (75%/25%)
Humalog Mix 75/25
Insulin lispro protamine suspension/insulin lispro (50%/50%)
Humalog Mix 50/50
23
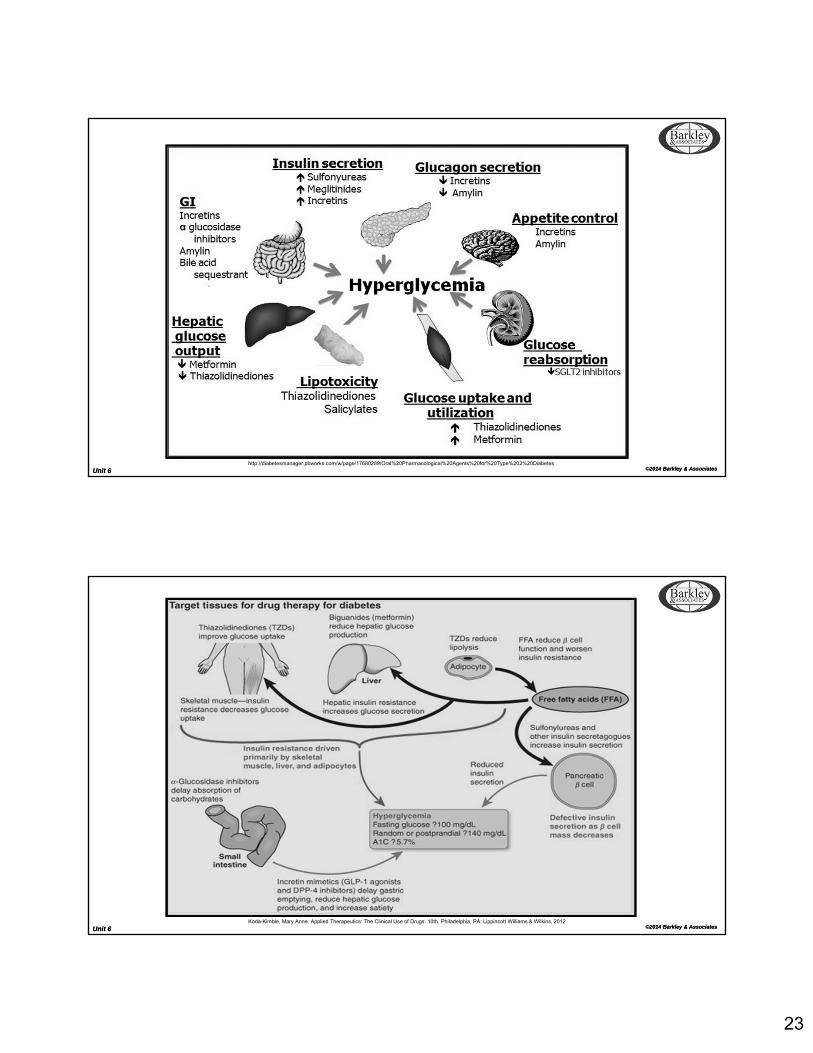
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associateshttp://diabetesmanager.pbworks.com/w/page/17680289/Oral%20Pharmacological%20Agents%20for%20Type%202%20Diabetes
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & AssociatesKoda-Kimble, Mary Anne. Applied Therapeutics: The Clinical Use of Drugs. 10th. Philadelphia, PA: Lippincott Williams & Wilkins, 2012

24
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
Inzucchi SE, Bergenstal RM, Buse JB, et al.; American Diabetes Association (ADA); European Association for the Study of Diabetes (EASD). Management of hyperglycemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012;35:1364–1379
Unit 6 ©2014 Barkley & AssociatesUnit 6 ©2014 Barkley & Associates
The End
Related Documents











