THE EMPLOYER’S ROLE IN MEDICARE Henry de Vos Lawrie, Jr. Kathryn J. Greenlief McGuire Woods Battle USAA & Boothe LLP

THE EMPLOYER’S ROLE IN MEDICARE Henry de Vos Lawrie, Jr.Kathryn J. Greenlief McGuire Woods BattleUSAA & Boothe LLP.
Dec 29, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THE EMPLOYER’S ROLE IN MEDICARE
Henry de Vos Lawrie, Jr. Kathryn J. Greenlief McGuire Woods Battle USAA & Boothe LLP

2
TRADITIONAL MEDICARE
Defined Benefit Fee-For-Service Out-of-Pocket
– Part A (Hospital) $768 (1-60)
– Part B (Medical) $100 Deductible 20% Co-Pay
3
TRADITIONAL MEDICARE (continued)
Major Coverage Exclusions– Prescription Drugs– Routine Physician Exams– Long Term Care– Dental and Dentures– Hearing Aids– Routine Eye Care
Per Capital Out-of-Pocket est. $2,454
4
TRADITIONAL EMPLOYER WRAP PLAN
Coordinates With Parts A and B– Co-insurance and Out-of-Pockets– Additional Benefits (Prescription)– Medicare Primary
Retiree Contribution FAS 106 Liability No Coordination With Medicare HMOs
5
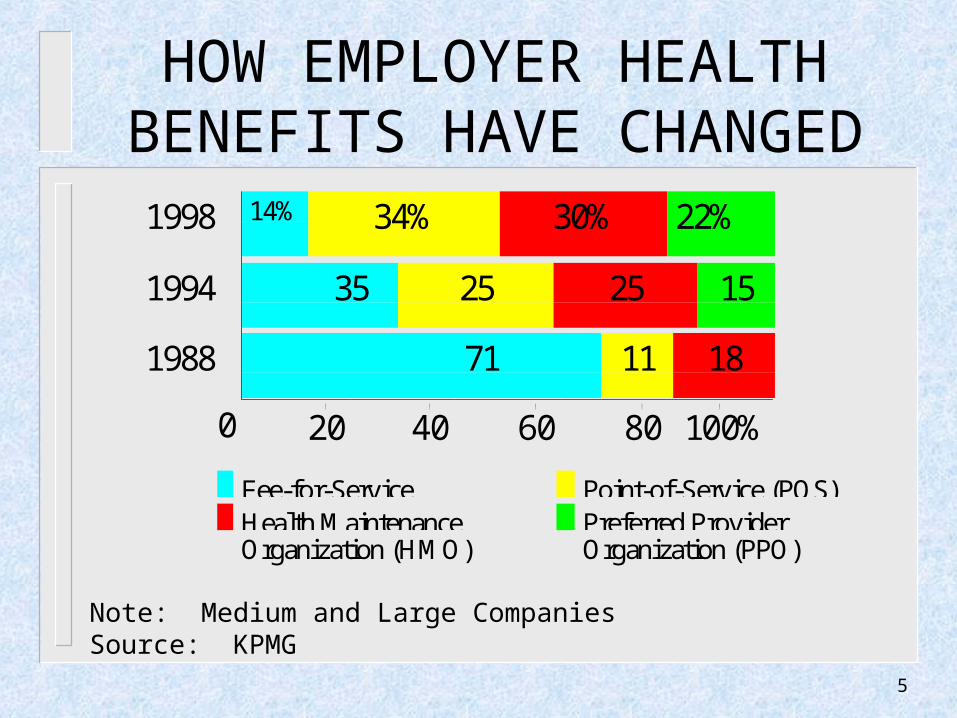
HOW EMPLOYER HEALTH BENEFITS HAVE CHANGED
1998 14% 34% 30% 22%
1994 35 25 25 15
1988 71 11 18
0 2'0 4'0 6'0 8'0 10'0%
Fee-for-Service Point-of-Service (POS)Health Maintenance Preferred ProviderOrganization (HMO) Organization (PPO)
Note: Medium and Large CompaniesSource: KPMG

6
BALANCED BUDGET ACT OF 1997
Fewer Dollars for Providers More Managed Care Effective 1999 Introduces Medicare Part C

7
MEDICARE + CHOICE(Part C of Medicare)
More Coordinated Care Plans (HMO, PPO, PSO or POS)
Private Fee-for-Service Plan MSA Plan Parts A & B Remain Alternatives

8
MEDICARE RISK HMOs
Introduced in 1985 Enrollment Quadrupled to 14% Since 12/93 Current Primary Vehicle Under Medicare +
Choice
9
HOW MEDICARE RISK HMOs WORK
Contract With Health Care Financing Administration (HCFA)
HMO Assumes Full Risk For Medicare Parts A & B Coverage
HCFA Pays Capitated Rate to HMO Under Medicare + Choice Rules, HCFA
Pays Greater of:– Blend of Local/National Rates– Floor Amount ($367/month)– Minimum Annual Increase (2%)
10
HOW MEDICARE RISK HMOs WORK (continued)
Normal HMO Coordinated Care Features– Defined Geographic Area– Gatekeeper– Network Limitations– Possibly POS Option

11
ADVANTAGES OF MEDICARE RISK HMOs
Lower Cost or Higher Benefit Level at Same Cost
More Predictable, Budgetable Expense
12
THE CURRENT HMO MARKET
Reduced or No Out-of-Pockets Some Zero Premium Plans Offer Additional Benefits Pricing Too Good to Be True?

13
VARIATIONS IN SAVINGS
Vendor Network Effectiveness Plan Location Enrollment Employer/Employee Contributions for
Existing Medicare Coverage

14
FAS 106 RELIEF
Estimate of Total Liability Driven By Current and Anticipated Expense Impact of Migration to Medicare Managed
Care

15
CHOICES FOR THE EMPLOYER
Whether to Embrace or Merely Tolerate Medicare + Choice
Strategy for Encouraging Migration Extent of Plan Redesign
16
INITIAL EMPLOYER ISSUES
Coverage Availability in Employer’s Area Benefit and Price Differences Among
Available Options Quality of Service Due Diligence Determine Likelihood of Acceptability of
Managed Care to Current and Future Retiree Population

17
DESIGN ISSUES
Medicare + Choice as Alternative or Mandate
Single or Multiple Coordinated Care Options Supply Benefit Enhancement to Encourage
Migration to Managed Care Limitations on Transfers Among Alternative
Choices

18
DESIGN ISSUES(continued)
Define the Employer’s Subsidy Develop Communications and Enrollment
Strategies
19
ILLUSTRATION OF DEFINED CONTRIBUTION PLAN
Account Balance Feature– $2,500 Annual Credits Beginning Age 40– Ten Year Limit– Interest Credited
Access to Funds– Termination After Age 55/15 Years Services– Forfeiture Upon Early Separation

20
ILLUSTRATION OF DEFINED CONTRIBUTION PLAN
(continued)
Use of Funds– Premiums For Range of Plans– Retiree Elects Annual Allocation Amount– Individual Contributions Permitted– Eligible Dependents– Premiums Only; No Cash
21
ILLUSTRATION OF DEFINED CONTRIBUTION PLAN
(continued) Advantages of Program
– Coordinates Well With Medicare + Choice– High Employee Visibility– Rewards for Service, Not Age– Employee Flexibility– FAS 106 Relief
Related Documents










![PARTIES: LAWRIE, Delia Phoebe LAWLER, John TITLE … · lawrie v lawler [2015] ntsc 19 . parties: lawrie, delia phoebe . v . lawler, john . title of court: supreme court of the northern](https://static.cupdf.com/doc/110x72/5ad464727f8b9a1a028bce85/parties-lawrie-delia-phoebe-lawler-john-title-v-lawler-2015-ntsc-19-parties.jpg)
