THE EFFECTS OF PREGNÀNCY AND FEMALE SEX STEROIDS ON GALLBLADDER EMPTYING BILTARY LIPID OUTPUT ÀND SMALL BOÚ{EL TRANSIT TIME by MICHAEL J. LA!{SON. . MBBS, BSC (MED) FRÀCP DEPÀRTMENT OF MEDICINE3, THE UNIVERSITY OF ÀDELAIDE THESIS SUBMITTED TO THE UNIVERSITY OF ÀDELAIDE FOR THE DEGREE OF DOCTOR OF MEDICINE I \ Ó.'¡s'¡áeJ ñ cr*Ã rtl 1-l \arf 6 .

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
THE EFFECTS OF PREGNÀNCY AND FEMALE SEX STEROIDS
ON GALLBLADDER EMPTYING BILTARY LIPID OUTPUT ÀND
SMALL BOÚ{EL TRANSIT TIME
by
MICHAEL J. LA!{SON. . MBBS, BSC (MED) FRÀCP
DEPÀRTMENT OF MEDICINE3, THE UNIVERSITY OF ÀDELAIDE
THESIS SUBMITTED TO THE UNIVERSITY OF
ÀDELAIDE FOR THE DEGREE OF DOCTOR OF MEDICINE
I
\Ó.'¡s'¡áeJ ñ cr*Ã rtl 1-l \arf 6 .
CONTENTS
PAGE
I
I
SUMMARY
STATEMENT
ACKNOVüLEDGEMENTS
CHAPTER I:
I.
I
I
A
B
C
D
E
. LITERATURE REVIE!'Ù
GaIl-stone Incidence
GaIIstone Cl-assif icat ion
Biliary LiPid Biochemistry in
Chol-esterol Gallstone Disease
The EnterohePatic Circulation
The Rol-e I qf the Gatlbladder in 24
Gal-lstone Format i'on
Female Sek Steroids and Smooth 25
Muscl-e MotilitY
Female Sex Steroids and BiIiarY 28
Lipid Secretion
Gastrointestinal- Peptides and 37
Gall-bl-adder Mot ilitY
Neuronal Determinants of 4L
ExtrahePatic BiJ-iarY MotiJ-itY
The RelationshiP of Gastric 44
Emptying to GaLl-bladder Emptying
II: CURRENT KNOWLEDGE AND UNANS!{ERED
QUESTIONS REGARDING GÀI,LBLADDER
MOTOR FUNCTION
Gall-bladder' Funct ion - Current 49
Concepts in PregnancY
I
5
6
8
9
9
L2
LB
I. F.
I G
I. H
I I
I. J
CHAPTER
II. À
II. B Unanswered Questions lìegarding
Gallbl-adder lrtrnct i-on
Thes i-s Aims
52
53II. C.
PAGE
CHAPTER III: METHODS ÀND RESULTS 55
Galtbtadder Function in the Human 57
Female: Effects of the OvulatorY :
Cycle, Pregnancy and Contraceptive
Steroids
Gallbladder and Small Intestinal 74
Regulation of Biliary Lipid Secretion
During Intraduodenal Infusion of
Standard Amino Acid and Liquid Formula
St imuli
The effeét's of Chronic Oestrogen 87
Administration on BiJ-iarY LiPid
Secretion, BiIe Acids and Gallbladder
Function in Post-Menopausal Women
Orocaecal Tlansit Tjne i¡ Pregrnancy 98
III. À.
III. B.
III. C.
III. D.
III. E
CHAPTER
. Co-ordination of Gastric and Gall-
bladder Emptying After Ingestion of
a Regular Meal
IV: DISCUSSION
PregnancY, Female Sex Steroids and
Gallbladder Function
The Effect of GaLIbl-adder Emptying
on Biliary LiPid Secretion
Onocaecal fransit Tjrre jrt kegnancy
108
lzs
L29
118
119IV.
IV.
IV.
À.
B.
c.
IV. D. Gastric and GalLbLadder Errtptying 136

PAGE
V
CHAPTER V: CLINICAL IMPLICATIONS OF ALTERED
GALLBLADDER EMPTYING AND BILIARY
LIPID SECRETION IN PREGNANCY
A. THE ROLE OF MORNING SICKNESS
(i) Clinical features of morning sickness
(ii) Diet and cholestenol gall-sbone formation
L42
THE POTENTIAL RELATIONSHIP OF DISEASES OF THE
ALIMENTARY SYSTEM TO ALTERATION IN BILIARY
LIPIDS IN PREGNANCY
L46
Mucosal protective effects of biliary cholesterol
Cholecystitis. in Pregnancy
Reflux oesophagitis and pepbic ul-cer disease
151
V-B
(i)(ii )
(iii )
CHAPTER VI: FINAL DISCUSSION
APPENDICES: A
F
BIBLIOC.RAPHY
ReaI Time Ultrasound Method for 15g
Determining GaIIbl-adder VoIume.
CharacLeristics of Infusates 161
Comparison of MeLhods for Measuring L62Gallbladder EmpLying.
Reported Studies of Biliary Bile 163
Acid Secretion in Subjects wibh
InLacL Gal-l-bladders and Subjects
SLaLus Post CholecystectomY.
I@asr:renent of Sma1t BoI/{tel TYansit L64Tiræ by the Hydrogen Breath llest
trÞasr:renent of Sen¡n tnmn Pancreatic t.nPollpeptide
'1.7r
B
L
D
E
1
SUMMARY
THE EFFECTS OF PREGNANCY AND FEMALE SEX STEROIDS ON GALLBLADDER
EMPTYING, BILIARY LIPID OUTPUT AND SMALL BOWEL TRANSIT TIME
In tlestern pqpulations gallstones occur in approximately 10 percent of men
and 20 percent of women by the age of 65. The majority of gallstones
are predominantì-y composed of chol-esterol. The mechanisms leading to
chol-esteroì- gallstone formation are poorJ-y understood, but prequisites
incl-ude supersaturation of biliary J-ipids with excess chol-esterof' the
presence of nucfeating factors and the retention of precipated choÌesterol-
crystals. The greater incidence of galÌstones in üIomen is probabì-y
reÌated to hormonal- factors.
Risk factors in blomen for gallstone formation incfude pregnancy and
the ingestlon of oral contrace.pþ1ve steroids. The increased probability
of gaÌlstones correlates with the number of pregnancies and women who take
oral contraceptive steroids or conjugated oestrogens double their risk of
deveJ-oping gal-lslones. The mechanisms by which pregnancy and oral
contraceptive steroids increase the risk of cholesterol- gallstones are
poorly understood but severaÌ mechanisms which include increased biJ-iary
chol-esteroL secretion and retention of precipitated cholesterol crystals
have been implicated. A factor contributing to bil-iary cholesterol
saturation in pregnancy may be the observed decrease in the numben of
ent,erohepatic cycles during pregnancy. Thj-s observation coul-d be caused
by slow transit of bife acids through the smal-l intestine, perhaps
secondary to pnogesterone or. other neurohormonaf effecls on small intestinal
muscle. Femal-e steroid hormones and pregnancy may also infl-uence gallstone
formation by aLtering the motility of the gallbJ-adder.
The aims of thi-s thesis wene to (a) quantitate gallbladder volumes throughout
the day in non-pregnant and pregnant subiects as well- as in subjects
taking oral contraceptive steroids or oestrogens aì-one, (b) assess the
2
infLuence of gaJ.Ibladder volume and small intesLine transiL time on
biliary 1ipid composition (c ) sfuay Iipid composition of gallbJ-adder bile
in women taking oral con$ugated oestrogens (d) assess orocaecal- transit time
in pregnancy and (e) examine the relationship between gastric emptying
and gallbladder emptying and time to nefilJ-ing'
Abdominal ultrasound was used to measure gallbladden volume throughout I
the day and night and during ingesbion of standard meals in pregnanl and
postpartum t¡tomen and oral contraCeptive users. Results b.Iere compared with
a control gnoup who were studied in bolh the follicular and lubeal phases
of the menstrual_ cycle. Increases in gal-lbladder volume in pregnancy
were correlated with serum progesterone. Evidence of al-tered gallbladder
motility in pregnancy was found.r The gallbladder of pregnancy was sluggish'
Fasting volume, the residual- volume after meals and the volume remaining
in the gallbladder throughout Lhe- day doubl-ed during pregnancy and these
changes cornelated with increases j.n serum progesterone. In contrasl'
emptying of the gallbJ-adder was not altered by the phase of the ovulaLory
cycle or by the ingestion of oral conLraceptive steroids. Gallbladder
refj-lling in the day did not occur in normal subjecLs ingesLing three
sLandard meals per daY.
The role of lhe enterohepatic circul-ation in biliary l-ipid secreLion was
studied as this may be an important mechanism by which altered motility of
the gal-Ibl-adder during pregnancy and the ingestion ofl conLraceptive steroids
predispose to cholesterol saturated bil-e and gaJ-J-stone formaLion' The raLe
ofl biliary secreLion was measured in human female volunLeers during naso-
gastnic infusion of both weak and poLent stimuli of gallbl-adder contracbility
(amino acids and fat respectively) and upper smal-l inLesLinal bile was
simul-taneousJ-y collected. Changes in Lhe enterohepatic circulaLion wene
monitored using abdominal ultrasound Lo quanitabe gal-Ibladder voLume and
breaLh hydrogen levels after adminisLration of bhe non-absorbable carbohydrate
lactulose to estimabe smal-l- intestine transiL ti.me. Serum levels of
J
pancreatic polypeptj-de were measured during each test. Continuous
i-ntraduodenal infusion of a sofution of amino acids that is known to
maximally stimulate pancreatic secretion uias less potent in stimulating
contraction of the galtbladder than intraduodenal- infusion of fat" Bil-e
was relatively more saturated with choÌesterol- when the gal-lbJ-adder
contracted at a sLower rate and the smal-I intestine transit time was slow.
The effects of Premarin (Ayerst), a mixture of conjugated oestnogens '/
prepared from the urine of pregnant maresr oh galJ-bl-adder emptying and
bil-iary ì-ipid secretion in postmenopausal vlomen were studied using
the techniques described above. No difference was found in biliary lipid
secretion or gal-J-bladder emptying on on off Premarin.
The lactulose breath test was used to measure orocaecal- transit time
throughout pregnancy and in the,pôstpartum period. The results were compared
with serum progestenone. Orocaecal transit time was deJ-ayed in late pregnancy
and returned to normaÌ postpanlum.- The pattern was similar to the pattern
of the sluggish gallbladder of pregnancy suggesting a common neurohormonaf
mechanism.
To investigate if the rate of emptylng of solids from the stomach controll-ed
the rate ofl gallbladder emptying and time to refilJ-ing, the relationship
bebween gallbladder and gastrlc emptying rates was studied in healthy
volunteers ¡ Fotlowing the ingestion of a standard radioactively l-abell-ed
meal gastric emptying was measured scintigraphical-ly while gallbladder vol-umes
i^rere morìitored sonÍgraphical-ly until gatlbladder refill-ing occurred. The rate
of gallbladder emptying in normal volunteers after a regulan meal was
dependent upon the rate of gastric emptying of the meal. Therefore' some of the
delay in gallbladder emptyin{ seen in late pregnancy could be due to deJ-ayed
gastric emptying.
The findings of this study provide valuable information on normal biliary
physiology and a plausibl-e rationabfe for pregnancy as a gallstone risk
factor by demonslrating the pnesence during gestation of prolonged periods
4
of gallbJ-adder stasis. The aetiology of this stasis is unlikeJ-y to be
related to high circulating oestrogen levels and is more likeJ-y due
to progesLerone effects.
Supporting evidence for the latter hypothesi-s comes from the observation
of the 1ack of influence of exogenous oestrogens on gallbladder and biliary
Iipid kinetics. The daLa also suggests.that conbraceptive sberoids are1
more likely to predispose to cholel-ithiasis by inducing changes in biliary
l-ipid metabolism rather than changes in galJ-bladder function.
5
STÀTE}4ENT
This thesis contains no material which
has been accepted for any other degree or
diploma in any Univers.ity and does not contain
any material previouqly published or written
by another person, except where due reference
is made to such material in the text.
DR. MICHAEL J. LAWSON,GE UNIT,
QUEEN EI ,.{A8EfH HOSPITALWOürivltLE,5011
45 0222
/
i, r-¡!N, :! +aràf
6
ACKNOVüLEDGEMENTS
The work contained in this thesis was carried out
during the tenure of a temporary research fellowship
in the Department of Medicine, the University of
Colorado, Health Sciences Centre, Denver, Colorado, USA.
I am deepJ-y indebted to Professor Fred Kern Jr. for
allowing me to work in his laboratory and for his
j-nvaluable guidance. I am extremely grateful to
Dr. Gregory Everson for direction and val-uab.Ie assistance
in study design, ultrasound techniques and anal-ytical'
methods. I am especially gratefuJ- for his consent to
use some of the results in, Chapter III which were
generated prior to my commencement as a Research fe.]-l-ow'
I al-so thank Dr. Craig Fausel for technical assistance
with some of the oestrogen experiments described in
Chapter III. I am grateful to Dr. Bob Hall- of the
Department of Maths and Computer Studies, South Austrafian
Institute of Technology for vafuable statistical- advice
and to Drs. Mal-col-m V'Ihiting and Michael Horowitz for
perusing the manuscript.
I wish to thank Mrs. Radene Showal-ter and Mrs. Carof
McKinley for expert technical assistance and preparation
of il-l-ustrations. The photographic work was carried out
by Mr. G. Hadaway to whom I am grateful,
I wish to thank l"lrs. Barbara Raymond who helped in the
enormous task of typing the manuscript and Dr. Stephen Rofe
who contributed his time in heJ-ping with the word
processing aspect for the preparation of this thesj-s.
7
Finally, I wish.to thank my Supervisors Dr. J. Toouli
and Dr. A. Kerr Çrant for heJ-pfuJ- criticisms and care-
fu1 perusal of the manuscript, which made the preparation
of this thesis both an educational and pleasurable
experience.
This thesis would not have been possible without the
staunch and unending support of my wife He1en and my
children Peter and Emily.
/
L
B
CHAPTER I: LITERATURE REVIEIV
Gallstone Incidence
Gallstone Classif ication
A
B
( i) Radiology
(ii) X-ray Diffraction of Stone Powders
( iii)Chemical AnalYsis
C. giliary Li pid Biochemistrv in Cholesterol
Gal.l-stone Disease
D. The EnterohePatic Circul-at ion
(i)
(ii)The role of
Interupt ionon Biliary
RoIe of the
the Gallbladder and Sma]-].
of the EnterohePatic CYcJ-eLipids
Intest ine
Effect
The cal-l-Úladder in Gal-l-stone Format ion
1
E
F
G
H
Fema.l-e Sex Steroids and Smooth Muscl-e MotilitY
( i ) Non Biliary Sr.nooth Muscle
(ii) Gal-lbladder and Small Intestinal Motility
Female Sex Steroids and Biliary LiPid Secretion
Gastrointest inal- Pe ptides and Gal]-bladder Motil-itY
( i ) Cholecystokinin
( ii) Pancreatic PoIYPePtide
( iii)Moti].in
I Neuronal- Determinants o f Extrahepatic Biliarv Motility
(i) Infl-uence of the parasympathetic autonomicnervous sYstem
(ii) Influence of the sympathetic nervous system
J . The Rel-at ionshi of Gastric EmPtYing to Gal-]-b1adder
Emptyinq
9
ii
LITERATT]RE RHÆE\^I
A. C,AI;I,STO{E INCIDENCE
Iltre incidence of gallstones is 1Ot irr lTren and 20? in \¡toûEn by the age of 50
to 65 (CIeIand 1953). In the USA gallstones are responsible for about
5001000 operations each year and approxirnately 81000 deaths. The direct
costs have been estimated to be rnore than two billion dollars (Kern 19751.
B. C.AI;I,STINE g.ASSIFICATTGT
C,allstones can be classified by tho following three nrethods:
(i) Radioloqy
Stones can be classified as:
(a) Radiopaque - This feature accounLs for 20% of stones and inclicates a
relative calciun content of greater than 4% by v'zeight.
(b) p.adiolucent - Accounts for tlre renaining 80t of stones indicating a
reJ-atively lower calciurn content.
(ii) X-ray Diffraction of Stone Povders
Using x-ray por,,rler diffractionr' the c4rstalline crcnstituerrts of gallstones
rernoved frcrn the gallbladder can be broadly classified as choLesterol and
calcir¡n salts (Si:tor ard lrlooley 19731. On this basis there are three nrai¡r
types of stones:
(a) clrolesterol (<5* calciunt) 608
(b) nixed stones 27?
(c) pure calcium 13ã
By this method it was found that men are just as likely as wonìen to form
pure calcir:rn stones but both calculi of cholesterol and those of
cholesterol with calcium salts.are nrcre ccrÌtncn i¡¡ r'ucnen-
(iii) Cholesterol vs Pigment
Gallstones can be classified fron direct chemical- analysi-s as chol-esterol
or pignrent (Trotman, Petrella,-Soloway et aI 1975) -
(a) Pigrnent
Understanding of the pattrogenesis of pigment stones has not progressed very
far. Tkre lack of clear understanding of their chernical corpositì-on has
retarded research progress. Although certain clinical associations are
noted below nrost pigrment stones in the Western worl-d and in the Orj-ent
occur in their absence.
(b) Cholesterol
Factors thought to be irrportant in the aetiology of cholesterol- gal-lstones
include the following:
l-. Infection
2. Bile Stasis
3. Changes in the conposition of hepatic bile
Originally it was thought'that infection of the gallbladder wall coul-d
/
!ü'ù
J
T
tII
I
allcx¿ bile salts to Þpass¡¡¡ely eþsçrþed -Leavi¡g ¡ç Lalrvgl
IncidenceMorphology
Compos it ion
clinicar features ::::i:":'::;:i:":::,steroids, conditions
11_
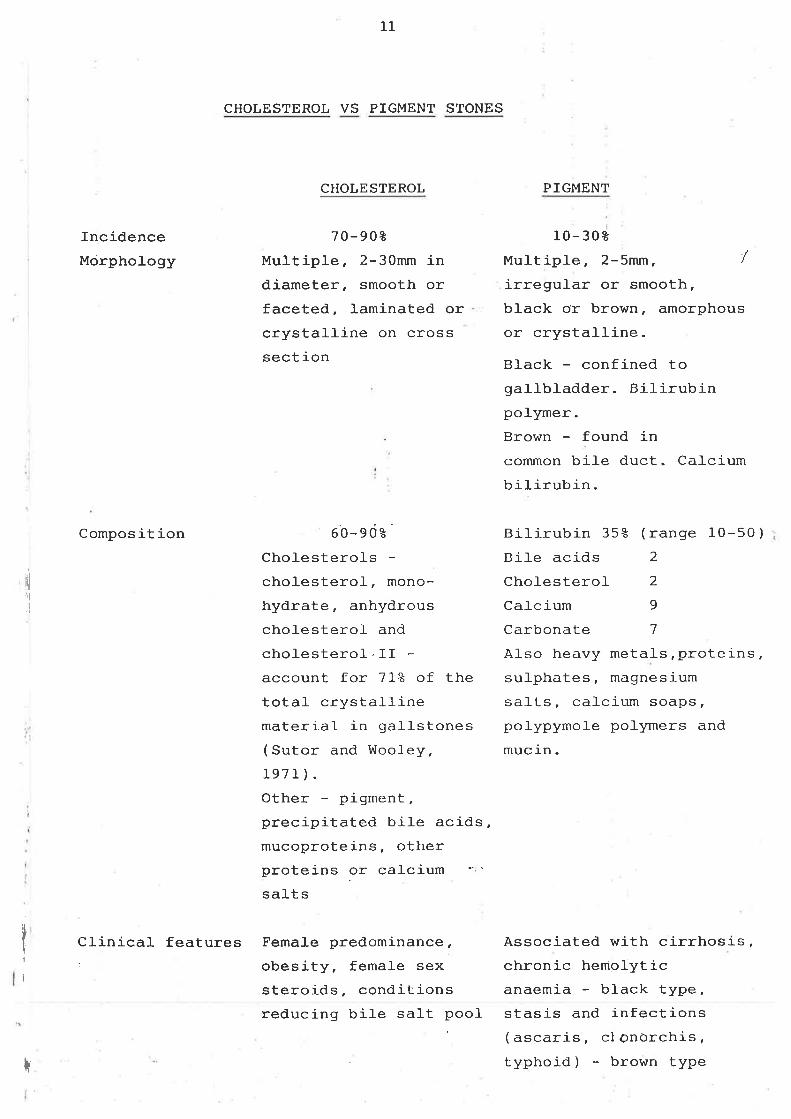
CHOLESTEROL VS PIGMENT STONES
CHOLESTEROL
70-908Multiple, 2-30mm indiameter, smooth orfaceted, laminated orcrystalline on crosssect ion
60-edåCholesterolscholesterol, mono-
hydrate, anhydrouscholesterof and
cholesterol-.IIaccount for 7IZ of thetota.l- crystallinematerial in gaÌlstones(Sutor and Wooley,1971 ).Other - pigment,precipitated biLe acids,mucoproteins, otherproteins or ca-Lcium
salt s
PIGMENT
10- 308
MultipJ-e, 2-5mrn , 1
irregular or smooth,black or brown, amorphousor crystalline.
Black - confined togallbJ-adder. Bilirubinpolymer.Brown - found inconìmon bile duct. CaLcium
bi]-irubin -
Bilirubin 35å (range 10-50)Bil-e acids 2
Chol-esterol 2
Cal-cium 9
Carbonate 7
AIso heavy metals,proteins,sul-phates, magnesium
saÌts, cal-cium soaps,pol-ypymoJ-e poJ-ymers and
mucin.
Associated with cirrhosis,chronic hemolyticanaemia - black type,
!lr¡l
I
t
reducing bile sal-t pool- stasis and infections' ( ascaris, cl onorchis,
typhoid) - brown type

T2
cholesterol in the gallbladder to nucleate and form chol-esterol- gallstones
but this no\^/ seems unlike1y. In add.ition to the rol-e of infection in
providing potential nucleating agents it is likely ttrat infection and
inflanrnation of the galì-bl-adder allow precipitation of calcium sal-ts to
initiate or accelerate gal-J-stone formation.It is noh/ generalÌy accepted
that gallstones may form without infection and biliary lipid research has
concerned itsel-f with the latter two aspects.
C BILIARY LIPID BIOCIIEIV1ISTRY IN CHOLESTM.OL GALLSTONE DISEASE
Si-nce 1968 progress has been made in r:nderstanding the pathogenesis of
cholesteroJ- gallstones but many uncertaintj-es remaj-n. The cl-arification of
the physicaf state of the lipids in bile in the nlid 60's and the
demonstration of the ìrrportance of the rel-ative nrol-ar percentage of each
lipid were key findings (A&nirandland Smafl 1968).
Gall-stones a-re fornred from organic conponents of bile.The major organic
components of bile are bj-le acids, chofesterol and phosphoJ-ipid.Bì-1e salts
are formed in the liver from chol-esterol. The rate firniting reaction in
this sequence is the 7-a1pha hydroxylation of cholesterol- (Mendefsohn,
Mendel-sohn, Staple 1965). Bile salt slmthesis may be regulated by a
negative feedback system such that bile sal-ts returning to the liver
inhibit 7-alpha hydroxylase, and the incorporation of acetate and
meval-onate into cholesterof (Shefer, Hauser, Bekersky et al- 1970). Removal
of these inhibitions may increase bile sal-t synthesis several fold. Both
cholesterol and phosphoJ-ipid are insolubl-e in water, but they are sol-uble
in bile because it is a micellar solution. Phosphofipid (l-ecithin) has a
hydrophobic and a hydrophilic portion sirnilar to bil-e acid and is present
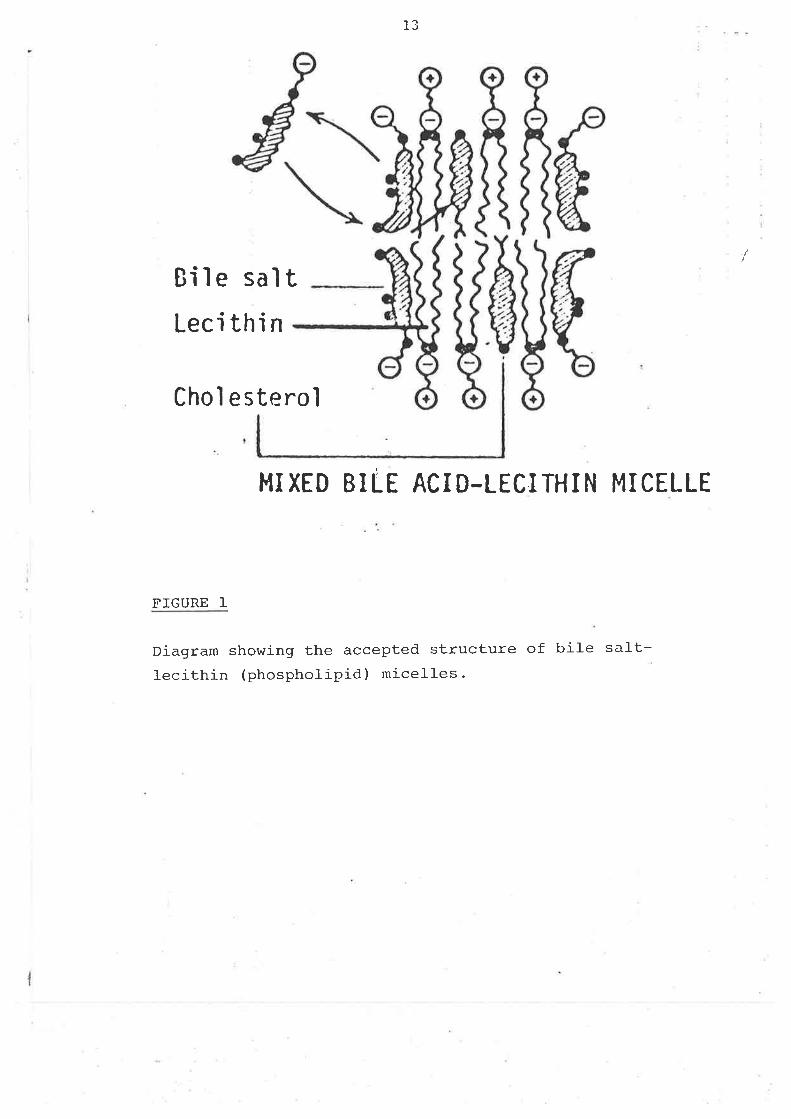
in bil-e in high concentrations (350-600nìg/100ÍLI) (Figure l-). It greatly
oçands the size of bile acid rnicelles and increases their capacity to
I
13
Biìe saltLeci thi n
Choì esterol
}.IIXED BILE ACID-LICITHIN MICELLE
FIGURE I
Diagram showing the accepted structure of bile sal-t-lecithin (phospholipid) micelles-
I
L4
sol-ubilise cholesterol-. These lipids are present normalJ-y in the rnolar
rati-os of bile sal-ts 75: phospholipid 20: cholesterol 5. I¡ühen the
cholesterol percentage is increased to greater than l-0?, either because of
increased cholesterof secretion or decreased bil-e acid secretion,
chol-esterol may precipitate in the gallbladder and initiate stone
formation. It is no\^/ recognised that cholesterol gal-lstones will form only
vrhen bile is supersaturated with cholesterol-, as it contains rnore
chol-esterol- in a single phase solution than can be solubilized in the bile
salt - phospholipid miceì-les present. ltre water insoluble chol-esterol is
maintained in solution wj-t]. bile salts, providing a sufficient
concentration of the swel-ling anphipath. Phosphoì-ipid is present to
increase the size of the rnixed rnicelles. Excess phospholipid disrupts the
micellar structure. The inter-rel-ationship of the concentrations of these
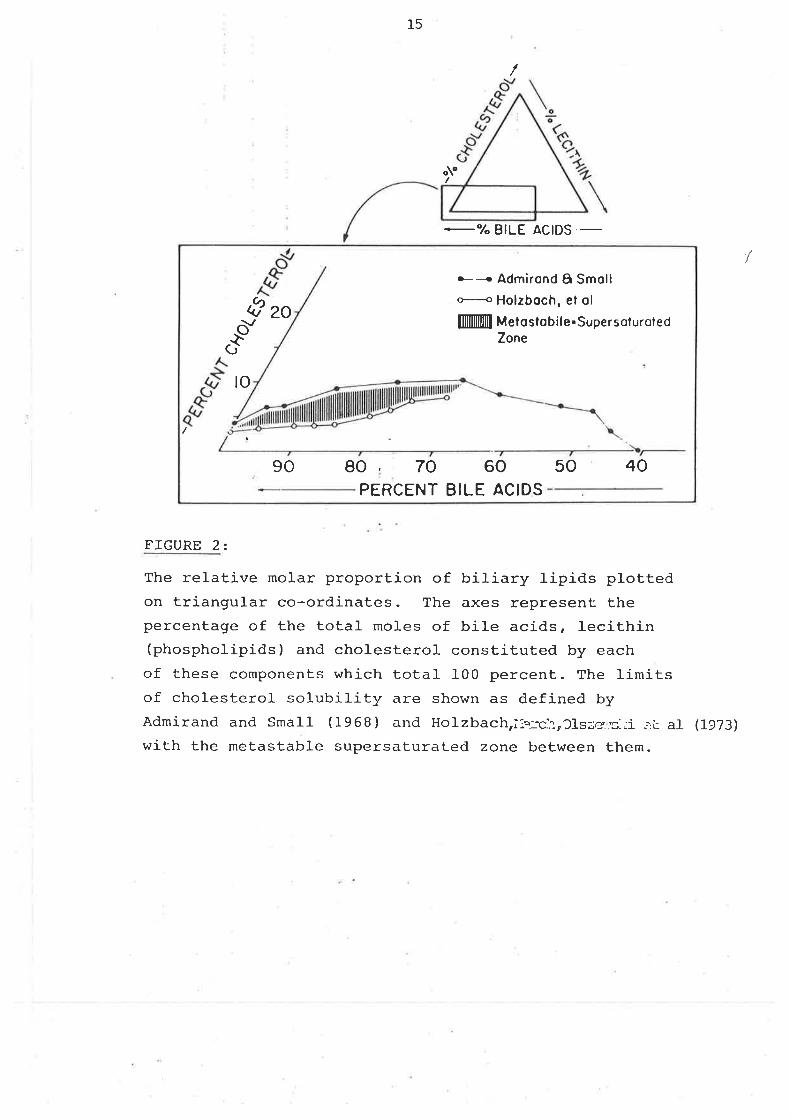
three J-ipids is nrost clearly demonstrated using the trj-angufar co-ordinates
described by A&nirand and Small- (1968). This representation assumes that
the water content is fixed at 90? by weight. A zone of concentratj-ons for
these three lipids in which a Iiquid rnicellar phase is maintained can be
demonstrated (Figure 2). Ho'o/ever, there has been considerabJ-e di-sagreement
as to the exact definition of the l-ine of supersaturation and its
significance (Metzger, Heymsfield, Gnrndy 1972),
/
15
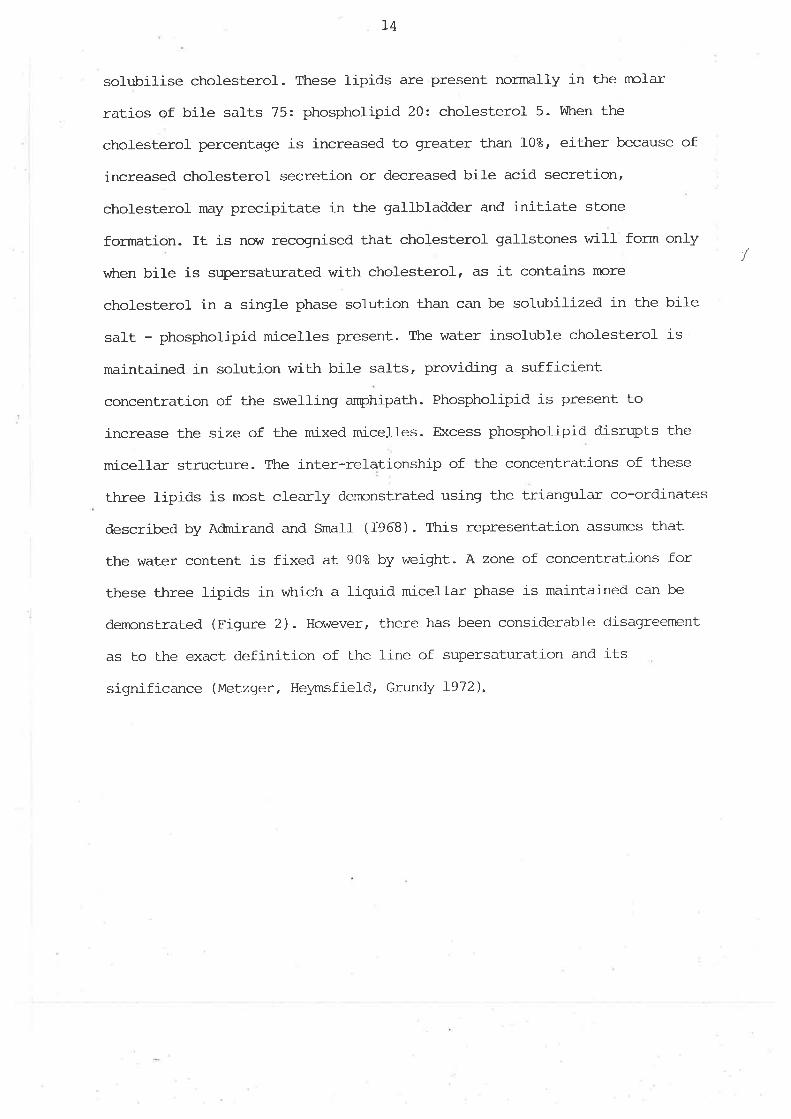
À
_O/OBILE ACID
&zoH Admirond 6 SmollH Holzboch, el ol
fllffiÏll Meloslobil e. SupersoluroledZones"
"ud
to
90 80 70 60 50 40PERCENT BILE ACIDS
FIGURE 2:
The relative molar proportion of biliary lipids plottedon triangular co-ordinates. The axes represent thepercentage of the total moles of bile acids, lecithin(phospholipids) and cholesterol constituted by eachof these components which total 100 percent. The limitsof cholesterol solubility are shown as defined byAdmirand and smarl (1968) and Horzbach,ii.:c.'.:,31sze:.s-;i :.t al (1973)
with the metastable supersaturated zone between them.
/
/
Aùnirand and Smal-I (1968) focussed attention on the liver as the site of
active bile secretion and biliary tipid production. They hlzpothesized thrat
a difference in the ability to solubilize cholesterol must exist between
human control bil-es and those from chol-esterol gallstone pati-ents and that
cholesterol insol-ubility probably represented the first step in gallstone
formation. Ttrey and subsequently others (MeLzger, Adler, Heymsfì-e1d et al,
1973) found that in patients with cholesterol gallstones, bile secreted by
the liver is supersaturated witJ^ cholesterof. In the same patients, bile
stored in the gal-Ibladder is l-00% saturated with cholesterol in micefl-ar
sol-ution and also contains cholesteroJ- crystals. They postulated tl-at
duri-ng storage in the gallbladder ,the su¡rersaturated bile was "seeded" or
nucleated by precipitated, bile pigment or other material, and that
chol-esterol- crystals precipitated frorn sofution and ini-tiated gallstone
formation.
Many investigators have found supersatr:rated or lithogenic bil-e rn
gallstone pati-ents and have identified the basis for the abnormal biliary
lipid conposition i-n several- groups of patients who a-re at high risk of
developing stones. For exanple, obese subjects secrete excessive biliary
cholesterol (Bennion and Grr.rndy 1975, Grundy, Duane, Adler et al- 1974) and
patients with il-eal resection, disease or blpass secrete reduced anrounts of
bile sal-ts (Cohen L97I). In both disorders the rel-ative molar percent
cholesterol in bil-e is increased and the incidence of gaÌIstones is high.
Vlahcevic and co-workers (Vl-ahcevic, Bell, Buhac et aI 1970¡ SweÌl, Bel-I,
Vl-ahcevic 1971) were the first to report a smalf bile salt pool size in
patients wj.th chol-esterol gallstones and to inplicate this small pool size
T7
in the pathogenesis of stones. They and others (Mok, Von Bergmann, Grundy
1977) hlpothesized that the bile salt pool size was small because of an
overly active negative feedback regulation of bile salt slmthesis. This
presumed defect in regulation, thought by sorne to be genetic, was proposed
primarily because other rnechanisms causing a small- bile salt pool size
could not be demonstrated. Specifically, the patients did not lose excess
bil-e sal-ts in the stool and they had normal hepatic slmthetic function.
A nurnber of other observations of biliary lipid conposition and bile salt
pool size cast sorne doubt u¡ron the inportance of the hypothesis just
described in the pathogenesj-s of stones.
The observations are;-
l-. Both hepatic bil-e secreted in the fasting state and bile stored
overni-ght in the gallbladder, can be supersaturated with cholesterol in
normal- subjects without gallstones (Metzger, Adler, Helzmsfield et a1
L973).The large overlap in biliaqz li-pid composition between gallstone
patients and controls suggests that supersaturated bife alone is not.
sufficlent for gallstone formation.
2. Smal-l bile salt pool sizes are also found in many subjects without
gallstones. Indeed, some investigators find no difference in mean pool size
between control and gallstone patients (Northfiel-d and Hofmann 7975).
These findings raise an inportaht question.VrThrat factors in addition to
supersaturated bile are necessarlz for gallstone formation?.
D. TTM ENTFR.OHEPATIC CIRCULATION
(i) Thre RoIe of the Gall-bl-adder and Smal-l- Intestj-ne:
The enterohepatic circulati.on (EIC) of bil-e occurs via the liver, biliary
tree, gallbladder, jejunum, il-eum and portal vein. The secretion of
cholesterol- and l-ecithin into bil-e is dependent upon bil-e acid secretion
which is in turn dependent on an intact EHC-
In heatthy individuals, il-eal bile acid absorption frsn the intestinal-
Iumen (I1¡ag and Phill-ips 1974) and hepatic bil-e acid extracton fron portal-
blood are highJ-y efficient (Reichep and Paumgartner 1980). Because bile
acid pool size is constant in the steady state and. no bile is stored in the
liver, the rate of hepatic bile acld secretion is directly proportionaL to
the frequency of enterohepatic cycling, which is largely deterrnined by the
rate of derivery of bile acid frorn the extrahepati-c bil-iar1z tree to the
terminal ileum. The delivery of bile acid to the terrninal- ileum in its ttlrn
is detennined by two mechanical pumps, the gallbladder and smalf intestine-
The gallbladder, in its reservoir capacity, determines the delivery of bile
acid to the intestinal- lumen. BiIe acid, the major conponent of biÌiar1z
secretion, is required for fat digestion and absorption thrrough the
formation of rnicelles. During fasting about 50? or nore of the bil-e acid
pooJ- is stored in the gallbladder and bite acid secretion into the
intestine is relatively Ìow (Metzger, Adler, Heysmfield et al 1973¡
Northfiel-d and Hofmann 1975¡ Mok, Von Bergrmann, Grundy 1980). During
feeding the gallbl-adder contracts and bile acid secretion into the
intestine j-ncreases in relation to the degree of gallbladder enptying,
whichrin turn, is primariJ-y a function of the content of the nreal (Rock'
Malmud, Fisher 198I; Ladas, Isaacs, Mur?hy et al- 1984). High fat rneals
ti
19
induce maxjmum galJ-bladder contraction. To integrate and optirnise the
process of digestion, gastric enptying of solids should regulate
gallbladder contraction through the release of hunroral nediators from upper
small bowel- and pancreas. Increased storage of bile acid in the
gallbladder or slowed smatl intestinal transit could slow the delivery of
bile acid to the terrninal- ileum and fower the bil-e acid secretion rate.
Biliary bite acid secretion rate is l-ower when stimufated by interrnittent
feeding (Mok, Von Bergmann, Grundy I9l9; Northfj-eld and Hofmann 1975¡
LaRusso, Szcepanik, Hofmann Ig77ì Mok, Von Bergmann, Grundy 1980; La Russo'
Hoffman, Hofmann et aI Ig75) than by continuous intraduodenal infusion
(Grundy and Metzger 19']2; Mok, Von Bergmann, Grundy I979,Yon Berg'mann'
Mott, Howard 1980, Grundy, Von Berg:mann, Grundy L979, Grundy, Duane, Adler
et aI 1914; Bennion and Gn:ndy 1975; Mabee, Meyer, Den Besten et af 19'76'
Valdivieso, Pal-ma, Nervi et aI |g':g, Mok, Von Bergmanrt, Gmndy 1978) of a
standard J-iquid formula. Because úite "ontains refatively more cholesterof
when bile acid secretion rate is ]ow, the l-ower rates of bile acid
secretion during gallbladder storage and slowed intestinal- transit coul-d be
expected to increase cholesterol saturation of bile'
The importance of the gallbladder and smal-l intestinal transit in
regulating the enterohepatic cycJ-e and pool size is suggested by several
observations: -
I. Sonre (Shaffer and small L977, Redinger L976) but not all (Adler,
MeLzger, Grundy L974¡ Shaffer,Braasch, smal-l I9l2), investigators have
noted a decrease in pool size after cholecystectomy, attributed to nearly
continuous cycling of bile acid's and riearly continuous inhibition of
hepatic bil-e acid slmthesis. These studies are difficult to interpret
because the storage firnction of the galJ-btadder before surgery was usually
not knornrn.
¿U
2. fn the dog (Parkin, Srnith, Johnston l-973) and in man (Inberg and Vuorio
1969¡ Faberberg, Grevsten, Johansson et a] 1970) truncal- vagotonqz was
fol-l-owed by increase in gallbladder vol-ume and increase in bile acid pool
size. Gallbl-adder nrctor response to standard stimuli seemed uninpaired by
vagotony but Inberg and Vuorio (1969) noted a larger residual volure in the
gallbJ-adder after a fatty meal. Stenpel and Duane (1978) more recently
found that the poor size of both primarlz bile acids' (cholic acid and
chenodeoxychol-ic acid) increased after vagoton¡z in eight male patients-
Ttrey also noted a decrease in cholesterol saturation of bile after vagotorny
and a significant inverse correlation between pool size and change in nrolar
¡rercent cholesterol. Their findings suggested that vagotonlz does not
predis¡lose to cholesterol- gallstoneq, but others have pro¡rosed that
retention and stratification of bile in the gallbladder results in certain
Iayers having a disproportj-onal percentage of cholesterol- (Thrurebon 1966¡
Nakayama and Van Der Linden 1975). Leáding to nidus formation, precipitation
of cholesterol and an increased incidence of galJ.stones.
3. In patients with coel-iac disease Low-Beer, Heaton, Heaton et aI (1971)
described enlarged gallbtadders and decreased gallbladder contractility
after a fatty meal-, with decreased bile acid turnover and increased bile
acid pool size. The changes \iùere attributed to dirninished CCI( release by
damaged smal-I intestinal mucosa and reduced stjmulation of the
gallbladder.
4. Hepner (Lg75) reduced gallbl-adder enrptying in healthy subjects by
feeding a 95å carbohydrate diet.for several days and then studied bile acid
kinetics. He found a similar increase in pool si-ze of both chol-ic acid and
chenodeoxychoric acid and a decrease in the secondarlz bite acid deo>cychoric
acid pool size. The traditional turnover rate of both prinrary bj-Ie acids
decreased slightty but significantly during the o<peri¡nental diet. The
2I
slmthesis rates v,/ere unchanged. A sjmilar diet in cholecystectornised
patients had no effect on bile acid kinetics.
5. Duane and Hanson (1978) used:indocyanine green as a marker of
gaJ-Ibladder content and rel-ated its rate of enptying after a standard meal-
to bile acid kinetics. They for:nd significant negative correlations between
rates of gallbladder enptying and pooJ- sizes of the primary bil-e acids plus
significant positive correlations between the traditional tr:rnover rate of
each bile acid and gallbladder enptying rates. Gal-l-bl-adder enptying was not
significantJ-y reJ-ated to synthesis rates of elther bile acid but slmthesis
rates did correlate positively with intestinal transit tirre measr:red by the
breath hydrogen method (Bond and Levitt 1975i Mok, Von Bergrnann, Grundy
L977). They also found an inverse Çorrelation between pool size and cycling
frequency.
6.Recent stuôies in man (Ir4ok, Von Bergmann, Gn-rndy 1980) indi-cate that
considerable amounts of bile secreted at night by pass the gallbladder
contrarlz to earlier belief. Sirnilar conclusions had been reached by
Stanley (I9lO) on the basis of his studies on the faecal excretion of bile
acids i-n obese subjects undergoing a prolonged fast and by Small et al-
(SmaII, Dowling, Redinger 1972) in their primate studies. Von Berg;mann et
al- (Von Bergmann, Mok, Grundy 1916) described the use of bili-rubin output
after stimul-ation of the gaÌlbladder to estimate ga1J-bladder storage
capacity and reported 37-86? of the bile acid pool in the gal-Ìbl-adder after
an overnight fast.
7.Small intestinal transit is an inportant deterrninant of bil-e acid cycling
frequency (Einarsson, Grundy, Hardison i-979) and thus can alter the rate of
biliary l-ipid secretion (Valdivieso, Palma, Nervi et al- L979¡ Mok, Von
Bergmann, Grundy Ig77). Faster sinalÌ intestinal transit increases bile acid
22
cycling frequency and the rate of bitiary lipid secretion. Slow small
intestinal transit woul-d slow delivery of bile acid to the terrninal ileum
and l-ower bile acid secretion rate. Because bil-e contains nx¡re cholesterol
when bile acid secretion rate is low (Northfiel-d and Hofmann 1975;
Lindblad, Lundholm, Schersten 1977¡ Wagner, Trotman, Soloway 1976, Nilsson
and Schersten 1969 i Ì(etzger, Adler, Helzmsfield et al 1973), the lower
rate of bile acid secretion during slow intestinaf transit would be
oçected to j-ncrease cholesterol saturation of bile. Small- intestinal
transit tjme is related to the type of stimulus infused j-nto the bowel
l-umen. Ruckebush and Fioranronti (1915) observed that different tlzpes of
equicaloric test neals produced d-ifferent durations of disruptions of
myoeì-ectrical- activity in the rat smal-1 intestine. Longer lasting digestive
activity was noted with oleic acidt conpared with arnino acids or glucose- De
Weaver, Eeckhout, Vantrappen et al- (l-978) showed in the dog that the
dr.ration of disruption of tJ-e sm.il-I intestine nigrati-ng myoeJ-ectric conplex
after a meal depends much more on the physicochernical conqrosition of the
food that on its volume or amount of calories. Therefore the physiochenical
composition of food may regulate smal-l- bowel motor activity and in turn
bitiary lipid secretion.
Thus an abnormality of motor function of the gal-lbladder coul-d result in a
decrease in the nunrber of enterohepatic circulations causing a decrease in
bile salt secretion rates leaving relatively greater amounts of cholesterol
in bite increasing the chance of crystat and stone formation- During
pregnancy the total bil-e acid pool is increased (Kern, Everson, De Mark et
al- 1981). pooling of bile acidd within the smalt intestine and gallbladder
coul_d contribute to an expansion of the total bile acid pooJ-.
During pregnancy, total bil-e acid pool size and gallbladder volurne are
increased (Kern, Everson, De Mark et al- 198f; Braverman, Johnson, Kern
rit
23
1980; Ylostalo, Kirkjnen, Heikkinen 1982). In addition, the size of the
bile acid pool directly correlates with the increases in gallbladder volunre
(I{ern , Everson, De },fark et al 1981 ). It is likely t}nt a hormone,
probabì-y proc;esterone, inhibits srnooth nn¡scle contraction, and irduces the
j¡rcrease in gallbtadder volume. Subsequently bile acids are sec1uestered in
the gallbladder, slowing their enterohepatic circulation, secondarily
stilrn:Iating bile acid slntlresis and æçanding the biLe acid pool to a new
steady state level. Ilov¡ever total bile acid pool size is significantly
i¡creased in the first trimester at a ti¡re '.vhen gall-bladder volume is not
significantJ-y increased. Ttl¡s in early pregnancy, the j¡crease<l bil-e acid
pool is either an effect of one or more hormonal or nretairolic changes in
bile acid synthesis or bile acid poo] sequestration is occurring in another
site. i
The rnain non-gallbladder site rvithiir tlre enterohepatic circulation where
bile acicl sequestration can occur is the s¡nall intestine. Aùrinistration of
propa.ntlreline brcrnide to healthy subjects resufts in prolonged
giastrointestinal transit tjme and expa.nsion of bile acid pool size (Duane
ancl Bond 1930). In aclclition, orocaecal transit is reversibly prolonged in
both the thiro trj-nester of pregnancy (i^Ji.ald, Van Thiel, Floechstetter et aI
19t)2) and in the luteal phase of the ovulatory cycle (i'Iald, Van
Thielriloechstetter et aI 1981 ). 'Ihus it is possj-bIe thr,at gastrointestinal
t¡ansit is proJ-onged in earty pregrìancy and therefore contributes to the
increased bile acid pool by sequestering bile acids rvithrin the intestinal
Iunen.
24
(ii)fnterruption of the Enterohepatic Cycle - Effect on Biliarlz Lipids
Thr:rebon (1962) by careful experiments on patients with occludable connìon
duct T-tubes denronstrated that interruption of the EIC for one to three
hours produced a decrease in lecithin and bil-e salt concentration. However
chol-esterol- secretion by tJ:e l-iver was unchanged causing the formatj-on of
bil-e saturated with cholesterol. Refeeding of bile collected during the
interruption returned cholesterol saturation of bile to normal. Thurebon
concl-uded that later in the storage cycle, the gallbl-adder fills with
hepatic bil-e that has changed its conposition due to natural interruption
of the EIC creati-ng favourable conditions for layer formation,
stratification and cholesterol- gallstone formation. Possibl-e causes for
this interruption courd lncl-ude dietarlz factors (e'gt predorninance of
carbohydrates) or proJ-onged periods-of fasting. Other observers have shov¡n
that interruption of the EX{C by fasting (causing sequestering of the bile
acid pool in the gallbladder) increases the chotesterol- saturation of bile
(Metzger, Ad.ì-er, Heysmfield et al- l-973¡ Mok, Von Bergmann, Grundy l97B)
E. TT{E ROLE OF TTIE GALLBI"ADDM. IN CHOLESTEROL GALLSTONE FORMATION
A stasis theory for gallstone formation was first suggested by Mecke1 von
Helmsbach (1865). The idea that inconpJ-ete gallbladder enptying contributed
to cholesterol galJ-stone formation hras supported by Montgonery (1866) and
Ord (1879). They showed that cholesterol- stones could form fron spherolJ-ths
which resulted frorn layering of liquids of different density in the
gallbladder. Steinman (faae) and Rous,McMaster and Drurlz (1924) felt
that nucl-eation or nidus formatj-on by bile pigrment spheroliths \^Ias
encouraged by gallbl-adder stasis, producing larninated gallstones. They also
suggested that inpaired gallbladder enptying allowed stratification within
I
25
the gallbladder of sol-ids of differing specific gravi-ty, thus favouring the
aggregation and subsequent additional layering of stones in a rnilieu
containing proteinaceous material or layers of bile. Poor galJ-bladder
enptyj-ng or biliary lipid rnixing could prevent the natural passage of early
rninute stones into the duodenum (Rains 1962).
In recent years however, nxcst enphasis has been on biliary lipid
conposition and there have been few studies of the gallbl-adder in rel-ation
to the pathogenesi-s of stones. Nevertheless, it is apparent that the
galtbladder must be invofved in the formation of gallstones for several
reasons:
(a) Chol-esterol- stones are rare after cholecystectorny
(b) Precipitation of chol-esterol cqystals from a suþrsaturated solution
requires time (Ho1an, HoÌzbach, Hermann et al- IgTg). BiIe retention in the
gallbJ-adder must be sufficientJ-y plolonged not only for crystal formatj-on
but for crystal agglorneration and stone formation.
(c) If gallbladder contraction is conpl-ete, lithogenic bile and cholesterol
crystals, if present, wil-I be expelJ-ed into the duodenum where they are
harml-ess. Stasis of bil-e j-n the gallbJ-adder, because of i-neffective or
inconpÌete contraction, might be the additional necessary condition for
galJ-stone formation.
F. FEMALE SÐ( STROIDS ANID SIVX]CITTI MUSCLE MOTILITY
(i) Non-Biliary Snrooth Muscle
There is good evidence that the ovarian hormones, oestrogen and
progesterone, can affect the motor activity of extra-uterine smirottr muscle.
Van v'Iagenan and Jenkins (1939) de¡n<onstrated of the
26
ureters of nronkeys in the irnnediate post partum period. Hund1ey, Diehl and
Diggs (cited Kumar 1962) showed decreased ureteric peristaltic activity in
non-pregnant wonen given progesterones. Activity increased with oestrogens.
Sjmil-ar results were found with in vivo intestinal motility studies by
Tsutsulopulos (cited by Yoshida and Mori 1969). Îøenty years l-ater Kumar
(1962) denxrnstrated that progesterone in vitro had a marked inhibitory
effect on the spontaneous contractility of ureter, large bowel and stornach.
Schatzman (1961) studied the guinea pig ileum and concluded that a decrease
in muscl-e tone occurred with the a&ninistration of progesterone or
oestradiol-. The previously conflicting resul-ts with oestrogens r,¡/ere
probably rel-ated to the high concentrations used. Yoshida and Mori (1969)
found two different level-s of oestrogen effects on in vitro intesti-nal
motility. Vrlith lower concentrations.'there \^ras an excitatory effect and with
higher concentrations an inhibitory effect. Nagler and Spiro (1961) studied
oesophageal rotility by manornetry jn_ control-s and pregrnant vvonìen.
Non-propulsive motor activity r^/as seen Íìore consistently in pregnant
subjects. This finding led the way for fi:rther investigations of the
effects of sex steroi-ds on gastrointestinal snrooth muscle ín human
subjects '
(ii) Caftbladder and Small Intestinal Motility
There is evidence that contraceptive steroids increase biliarlz cholesterol
secretj-on in wornen (Bennion, Mott, Howard l-980; Bennion, Grinzberg, Garrick
et al- 1976; Pertsernilidis,Paneveliwalla, Ahrens L974),but information on
the affect of female sex hormones and.pregnancy on gallbladder function is
scant. In separate chol-ecystographic studies Gerdes and
Boyden (1938) and Potter (l-936) suggested that inpaired gallbladder
emptying and concentrating ability occur late in pregnancy. Nil-sson and
Stat-t-in (1967 ) also used oral cholecystography to neasure gallbladder
/
zt
erptying after bol-us injection of chol-ecystokinin (CCK) in both phases of
the menstrual cycle in each of 10 subjects. They found slower enptying in
the luteal phase in eight of them. However the phase of the cycle was not
accurately documented by serum progesterone levels.
Pregrnancy and female sex steroid intake are major risk factors for
chol-esterol cholel-ithiasis (Bennion and Grr-rndy I97B¡ Kern, Erfling, Si-nx¡n
et al I97B¡ Frieùnan, KanneÌ, Da¡¡¡l¡er L966). In the pathogenic seguence of
cholesterol cholelithiasis proposed by SmaJ-J- (Small- 1980; Small 1974;
Shaffer and Smal-l- 1976) a prerequisite for cholesterol gallstone formation
is the hepatic secretion of lithoÇenic bil-e. rn addition major
physiochernical changes, incJ-udj-ng nucl-eation (Hol-an, Holzbach, Hermann et
aI 1979), crystal formation (Sefaghat and Grundy l-980; Walton 1967), and
adherance of crystal- must occur in the gallbtadder to generate cholesterol
gal-lstones. Because these changes.require tjrne, retention of lithogenic
bile in the gallbladder is necessarlz for these events to occur. If
gaÌlbladder enptying u/ere prompt and conplete, lithogenic bil-e and any
cholesterol crystals that may have formed would pass uneventfully into the
duodenum, preventing the sequence leading to gallstones. Previous studies
in pregnant women have suggested that the volume of the gallbladder is
increased and its contraction is sluggish (Braverman, Johnson, Kern l9B0;
Potter 1938; Gerdes and Boyden 1938). Gallbladder emptying in the l-uteal
phase may be impaired (Nilsson and Stattin 1967 ) but \^/olnen taking oral
contraceptive steroids seem to have normal gaìlbladder volumes and emptying
after a liquid meal (Braveïman, Johnson, Kern l-980). However enptying
during continuous intraduodenal arnino acid infusion is slower (I(ern,
Everson, De Mark et aI I9B2). Ttre latter finding inplies that gallbl-adder
contractiJ-ity rnight be irrpaired in vvorrìen tal<ing contraceptive steroids.
/
Progesterone and oestrogen l-evels increase progressively in pregnancy- rt-
¿ó
appears that progesterone rather than oestrogen causes the inhihition of
gallbladder enptying and the delay in orocaecal transit tine is noted
in the third trinester of pregnancy (Wald, Van Thiel-, Hoechstetter et al-
l9B2). Studies in experlrnental anjmals suggest that oestrogens actually
enhance srnooth nmscle activity. Ryan and Pellecchia (l-982) showed that
oestrogen pretreatnent in the in vitro mal-e gminea pig gallbladder
significantly decreased tl-e threshold acetycholine requirernents for
contraction. Progesterone had the opposite effect. Datta, Hey and Pleuvrlz
(1974) found that oestradiol- pretreatment causes a dose-dependent increase
in intestinal propul-sion when aùn-inistered to oopherectornised mice. A
rnixture of progesterone and oestradiol had no significant effect. There are
no studies in man to confirm or refute these experirnental findings of
gallbladder and intestinal smooth muscl-e excitation by oestrogen.
G. FEMALE SEX STM.OTDS AI\D BILIARY LIPID SECRETION
BiIe of \ivollten taking birttr control'p-iIls has often been shown to be
considerabJ-y nore saturated with cholesterol than that of other tn/olnen
(Benni-on, Mott, Howard l-980; Kern, Everson, De Mark et aI I9B2) - It has
been established that the higher the chol-esterol saturation anÐng patients
without gallstones, the greater the prevalence in the popuJ-ation from which
the patients were chosen (Redinqer and Small 1972). For instance the Masai
of East Africa and the Japanese have a very low cholesterol saturation and
as a consequence a low prevalence of cholesterol- gallstones, ulLrereas young
North American fndian Vùomen have a high prevalence of su¡rersaturated bil-e
(Thistl-e and shoenfie]-d, 1971-) and an exceptionally high prevalence of
gallstones(Sanpliner, Bennett, corness l-970). Tttus, the higher the
cholesterol saturation, the greater the risk of gallstones.
According to some epiderniological studies, \^/omen on birth control pitls
(Boston Collaborative Drug Surveil-lance Progranrne 1973) and postmeno-
pausal h/ontqn (Boston ColÌaborative Drug Surveillance Progranrne 1974) on
oestrogens have a risk of surgically documented gallstone disease that is
2.0 to 2.5 times tJ.at of control- groups. Hcxuever more recently the Royal
College of General Practitioners' oral contraceptive study (1982) suggested
I
29
that the use of oral contraceptì-ves confers no increased risk but simply
accelerates gal-J-bJ-adder disease onJ-y in htomen susceptible to ib. In
addition, this study suggested that the acceleration may be associated
with the dose of oestrogen in the combined oral contraceptives. These
Ìatter new observations may be due to currenl|tlow doserroestrogen
contnaceptives. I'High doserr contraceptives are prescribed onJ-y when the
l-ower dose oestnogen contraceptives prove inadequate. Many of the
physioJ-ogicaf changes in biJ-iary lipids observed with high dose oestrogen
preparations may not occur with lower doses. In addition most studies
performed in different phases of the menstrual- cycle have failed to show
significant differences in bil-iary l-ipid output and in particul-ar' the
cholesterof saturation index (Kern, Everson, De Mark et al 1981 , illiJ-l-j-ams,
Scallion, McCarthy 1980; !r/hiting,, Down, Iitlatts 1981).
A few studies have examined the effects of oestrogens on biliary i-ipids
in humans.
Oestrogens have several effects on hepatic biliary lipid metabolism whlch
resuft in the formation of lithogenic bile. These effects incl-ude the
foì-lowing: -
1 . I¡,lomen taking oraf contraceptive steroids have an increase in
cholesterol saturatlon index and the proportion of women with
supersaturated bil-e is increased (Bennion, Ginsberg, Garrick et
at 1976; Vrlhite, Howat, Schoefield 1976; Pertsemilidis, Panveli-wall-a,
Ahrens 19'14). 'l'he mechanism is probably by hepatic enhancement c¡f
choÌesterol- secretion in bife (Bennion, Mott, Howard 1980).
2. An increase in molar percénLage chol-esterol in T-bube bile from
three bromen taking Premari-n and Provera (conjugated equine oestrogens
30
Íedrox)4grogesterone acetate) al-ong with a decrease in cholicacid slmthesis
and pool size (Pertsemilidis, Panveliwalla, Ahrens 1974) -
3. Reduced bil-e acid synthesis and secretion in rats (Davis and Kern L976i
Davis and Kern 1977¡ Stranentinoli, DiPadova, Jualano et al 1981) and
hamsters (gorurorris,,Colme, Chung et aI 1977) so that bile becores
supersaturated
4. In hamsters the rate lirniting enzynìe 7-a1pha-hydro>q¿l-ase which converts
cholesterol to bile acids is reduced by ethinyl oestradiol (Bonnorris,
Co1me, Chung et al- 1977) -
5. The physical characteristics o{ the lipid conposition of the hepatic
rnicrosomal nre¡rbrane, tJle site of cholesterol conversion to bile acids is
al-tered in the rat by ethinyl oestradiol (Davis and Kern 1977) -
Suggestive evidence of an oestrogen effect coItES from the folJ-owing
obsen¡ations:-
I. Bennion, Drobny, Knowl-er et al-. (f978) found a smal-Ier total bil-e acj-d
pool and a smaller cholic acid pool in Indian and white !úofiìen cornpared with
nen. Bil-iar1z cholesterol saturation \^/as inversely correlated witl
chenodeoxycholic acid pool size.
2. Bennion, KnowJ-er, l4ott et al-. (1979) studied biliary J-ipids and bile
I
ü
tT
I
31
acid kinetics in young Pima Indian boys and girls before, during and after
puberty. Prior to puberty the bile acid pool size was the same in both
sexes. It becanre l-arger in males but not females at the tirne of puberty'
Biliary lipid saturation increased in both sexes especially females at
puberty and correl-ated positively with urinary oestrogen excretion.
3. Bennion (1977) stud'ied one young r¡/oman before and after bilateral
oophorectorny. After operation the bile acj-d pooJ- size doubl-ed without
change in distribution of bile acids and the rnol-ar percent cholesterol- in
the bile decreased.
4. fn male vol-unteers a seven day course of a 30ug oral dose of ethinyl
oestradj-ol caused a significant rise in the cholesterol- saturation index of
gallbladder bil-e (Anderson, Jamesr. McDonald et aI r9B0). However more
recently, Do,*rn, V{triting, Watts et al (1983) showed that the daily ingestion
of 30ug ethinyloestradiol alone in women had no significant effect on
Iithogenic index. The reason for this sex difference in uncl-ear' but it may
be related to the 503 fal-l in the l-evels of circulating testosterone which
al-so accontpanied the use of ethinyl- oestradiol- in men'
criticism has been directed at the anjmal- studies because of the large
doses of oestrogens required to produce biliarlz J-ipid changes. Also
physiological- changes in natural sex hormones during a normal menstrual
cycle have been shown to have l-ittle (Low-Beer, !Ùicks, Heaton et al- L977)
or no effect (Bennion, Grinzberg, Garrick et al 1981; Whiting, Down, watts
:{r\j
''r)
I
l'
$
I
l
)aJZ
I
l-981, Kern, Everson, Delvlark et aI l9B1; lrlilliams, Scaflion, l4cCarthy
re80).
hlith a variety of slmthetic oestrogen/progestin mixtures Bennion' lbtt arid
noward(I98g) shor¡red that contraceptive steroid use còuld increase both the
molar percent cholesterol in human female gatlbladder bile and hepatic
secretion of cholesterol. Kern, Everson, De l4ark et aI (l-982) showed the
same changes in healthy young $/onÊn taking a contracepti-ve steroid
cqnbination of 50ug of nestranol and lmg of norethnidrone.
Recently Do\,rm, l'ühriting, watts et aI (1983) found evidence in hea]-thy young
h¡ornen that the progestagen, norçfestrel and not the oestroçfen' ethinyÌ
oestradiol is responsible for the iricrease in bile chol-esterol saturation
which acconpanies the use of oral contraceptives. Ttrey suggested that the
overall- oestrogen to progestagen potency ratio of an oral contraceptive may
be rnore irrportant in detennining its effect on the bilia4z cholesterol
saturation index than the dose of each sex hormone'
The origin of the increased chol-esterol secreted into bile is unl<nor,n, but
there are five main possibilities:-
(i) increased dietarlz intake
(ii) enhanced absorPtion
(iii) increased slmthesi's
(iv) increased hepatic uptake of J-ipoprotein cholesterol
I
I{r
T
33
(v) decreased breakdown of cholesterol to bile acids
The first two possibilities seem unlikely. In rats the rate of cholesterol
slmthesis is greater in females than in males. (ltukherjee and Gupta 1967;
carlson, Mitchell, Goldfarb l97B). Preginancy markedJ-y stimuJ-ates hepatic
cholesterol slmthesis in the rat and the saguines fuscj-ollis nronkey
(Feingold, Wi-ley, Moser et al I9B3). Oestrogten aùninistration stirrmlates
the activity of hepatic 3-hydroxy 3-methylg1utar1zl coenzlnle A reductase'
the rate lirniting enz)nìe in cholesterol synthesi-s. However, Turley and
Dietschy QgTg) have clearly shov¡n in rats that the rate of bifiary
cholesterol secretion is independent of the rate of hepatic cholesterol
synthesj-s. Other studies in rats show that a large dose of ethinyl
oestradiot (5mg,/kg/day) increases the specific bj-nding of low density
lipoprotein (LPL) by rat liver menrbráne (Kovanen, Brown, c'oldstein 1979)
and greatly augments the uptake and catabolism of plasma LDL (chao'
Vfindler, Chen et aI 1919). Ttrose findings may be relevant to the
observation that ethinyr oestradiol (150ug'/day) increases the turnover rate
of serum cholesterol in human subjects (Nestel-, Hirsch, Couzens 1965) and
to studies suggesting that plasma ì-ipoproteins serve as the major source of
biliary cholesterol (Schwartz, Halloran, VJ-ahcevic et al I97B; Schwartz'
Berman, Vlahcevic et al- l97B). It seems possible therefore that the excess
biliary cholesterol secreted by users of contraceptive steroids could be
derived from accelerated hepatic uptake and catabolism of plaslna LDL
cholesterol, but direct study of this problem is needed.
tI
l
I
34
The relation between serum lipids and lipoproteins and biliarlz lipid and
bile acid corposition and secretion has been studied.Patients with type fV
hyperlipidaernia appear to have an increased incidence of cholesterol
gallstones (XadziolkarNil-sson, Schersten 1977), Einarsson and co-workers
have described an increase in bil-e acid slmthesis and pooJ- size, especia]-ly
cholic acid (Einarsson, Hellstrsn, KaIIner 1974) increased hepatic HI{G CoA
reductase activi-ty (Angel-in, Einarsson, Hellstron 1976) and increased
chofesterol satr:ration of bil-e. Pregnancy (Williams, Sj-mons, Turtl-e 1976)
and oral- contraceptive steroids (Odell and Mol-itch L974) are associated
with sirnilar changes in serum tipids - an increase in triglyceride
concentration, a slight variabl-e i4crease in serum cholesterol and an
increase in very low density lipoproteins. Elevated high density
lipoprotein (HDL) fevels have been associated wj-th a fower incidence of
gallstone disease (Scragg, Mclrtichäel-, Seamark 1984). The effect of
contraceptive steroids on HDL Ìevels varies with their conposition,
oestrogens causing an increase and progestagen a decrease (Bradley'
Wingerd, Petitti et al 1978). Schwartz, Berman, Vlahcevj-c et at (1978)
reported that HDL chofesterol- is the major precursor for biliarlz
cholesterol and bile acid synthesis,Ì:ut this issue cannot be regarded as
conpletely settled. Further¡¡s¡s the role of lipoprotein remnants and the
rate of metabolism of serum J-ipi-ds in biliary lipid synthesis and secretion
have not been adeguatelY studied.
The possibility of al-tered gallbtadder ftmction in response to oestrogens
has been incomptetel-y studie¿. tn addition effecls of oestrogens upon
gal1bladder storage capacity, concentrating abil-ity and contractil-ity have
not been weÌI chanacterised.
The gatlbÌadder has enormous concentrating capacity (Makhl-ouf 1979) which
has not been studied in intact man except, by choì-ecystography. Concentration
of bile is dependant upon sodium and water absorption' probabLy mediated
35
by the putative sodium pump Na+, K+ ATPase (Van Os and SJ-egers 1971).
Na+. K+ ATPase is an enzyme which suppJ-ies lhe energy for the movement
of sodium out of the hepatic cel-l- into the canalicular bife and is the
putative mediator of bile acid independant flow (Schwartz' Lindenmayer'
All_en 1975, Erlinger, Dhumeaux, Berthel-ot et al- 1970; charney, silva,
Besarab et al- 1974; Simon, Sutherland, Accatino 1977)'
Sodiurn enters gal-l-bl-adder epithel-ial- cells passivel-y across the luminaf
membranes down an electrochemical- gnadient maintained by Na+ exLrusion
across the basol-ateral- membrane by a Na+ K+ - ATP+se pump. Movement of
water is believed to be passive and- secondary to active sol-ute movement.
Cyclic Amp (c Amp) has been propoq"å t" a second messenger for the effects
ofl several mediators (fiood and Svanvik 1983). Secretin and extracts
of isl-et cell tumours bul not CCK'.or gastrin have been reported to
inhibit fl-uid absorption by the isol-ated rabbit gal-l-bladder (Leyssac'
Bukhave and Frederiksen 1974). VIP is a potent stimulant of c Amp
production by human gall-bladder cel-l-s (Dupont, Broyart, Bnoery et aI 1981)
VIp infused intravenousl-y in the cat inhibits gal-l-bladder i/later and
eJ-ectroJ-yte transport and reverses its direction to a net secretion'
Femal-e sex hormones in pharmacological doses have been reported to inhibit
gallbladder fluid absorption j-n vitro (France, Men on, Reay et at 1977)'
36
It is not known v¡trether gallbladder function is influenced by different
phases of the ovulatory cycle. Riegel, Ravdin, Morrison et a1(1935)
studied the corposition of gallbladder bile in \ÀTcrllen at term and found
changes consistent with irrpaired gallbladder concentrating fr:nction' This
effect could be due to oestrogen or progesterone. Historical reports
suggest that bil-e becones dilute in the later phases of preqnancy (Riegel'
Ravôin, !trorrison et aI 1935; Gerdes and Boyden l-938; Potter 1936) ' In the
pregnant hamster there is decreased bile racid independant bil-e ft'ow with an
associated fall in Na*K+-ATPase activity:in liver honngenates (Reyes and
Kern 1970). oestrogen a&ninistratlon qls-o decreases the bile acid
independent fraction of bile and hepatic Na+K*-ATPase activj-ty (Reichen and
Paumgartner L977) -
It is possible that the enlarged gallbladder noted in pregnancy by Kern'
Everson, De Mark et aI (r98l-) coufd be primaril-y due to reduced water
absorption without increased retention of bile acids, al-though this seems
unlikely. Ttre significance of the increased volume of the gallbl-adder in
pregnancy can be interpreted correctJ-y only with additional information
about whether bire acid mass retained in the garlbradder is arso
increased
iì
37
H. GASTROI}MESTINAL PEPTIDES A}JD GALLBLADDER. ¡4CIILITY
Gastrointestinaf peptide effects on extrahepatic bili-ary notil-ity are
multipJ-e and their integration is conplex. It has been generally accepted
that CCK is the candidate hor¡none for gallbladder contraction- (Broden
1958, Sturdevant, Stern, Resin et aI 1973).
( i ) Chol-ecystokinrn
In I92B Ivy and Oldberg used the name cholecystokinin (CCK) to describe the
active pri-nciple responsibfe for the-contraction of the gallbladder' Sone
15 years later Harper and Ra¡rer (1943) showed that intestinal extracts
stimulated secretion of pancreatic enzlnìes and named their active factor
pancreozlzrnin. subseguentJ-y, Jorpes and Mutt (1968) at the Karol-inska
Institute, Stockholm showed that these active principles (CCK and
pancreozlzrnin) were one and the same regulatory peptide capable of eliciting
both contraction of the galtbladder and secretion of pancreatic enzlzmes'Ttte
original peptide of CCK contained 33 anino acids (CCK-33) ' Subsequent'
studies demonstrated that only the octapeptide (CCK-B) located at the
carboxy-terrninus of CCK-33 was required for contraction of the gaj-lb1adder
and relaxation of the sphincter of Oddi. In addition, CCK-B was shown to be
3 to 10 times more potent than CCK-33 in stimulating contraction of the
gallbladder. ccK rel-eased frorn the small intestinal I cells may regulate
gallbtadder contraction (lrliener, Inoue, Fagan et aI tg8r) in response to
Iurninal- stimuti. Guinea pig galibladder contraction in response to CCK is a
result of a direct action on sn¡coth muscl-e cells (Yau, Makhlouf ' Edr¡¡ards et
aI l_973 ) . CCK-induced small bowel- contraction is nrediated via ner:ral
pathways (Hedner 1970). Continued release of CCK frorn upper small bowel may
be stjmulated by slow gastric enptying of solids wLrich may in turn control
3B
the rate of gallbladder contractions. During feeding the gallbladder
contracts all-owing bile acids to enter the intestine to enmlsify fat and
transport cholesterol in rnicelles. Gal-Ibladder contraction is dependent on
the content of the ¡neal- which rel-eases CCK from the jejunum and it shoul-d
therefore relate d.irectly to the rate of delivery of ingested rneals into
the upper smal-l intestine. Itrus factors controlling the rate of gastrlc
enptying could indirectly control the rate of gallbladder enptying.
Thre sphincter of oddi has the potential for altering bile partitioning
between the galtbladder and smal-l intestine. Meltzer (1917) advanced the
concept of reciprocal innervation to oçIain the simultaneous contraction
of the gallbladder and relaxation of the sphincter in res¡ronse to
intraduodenal- magnesium sulphate. 4¿civlaster and Elman (1926) also
demonstrated that sphincter resistance decreased as the gallbl-adder
contracted and that differential- pressures betwen the extra and intra
hepatic biliarlz tree and the gatlbladder could account for gallbladder
refilJ-ing (elman and McMasLer 1926). It is relevant to note from previous
studies that in addition to its direct gatlbladder effect, CCK reÌaxes the
sphincter of Oddi (Sandbl-om, Voegtlin, Ivy 1935, Hong, Magee, Crewdon
19s6).
The role of CCK in co-ordinating galJ-bladder contraction and sphincter of
Oddi rel-axation is well established (V'la1sh I97B). Guinea pig gallbladder
contraction in response to CCK is a result of a direct acl-ion on smooth
muscle cel-ls. The sphincter of Oddi in the dog (Sandbl-om, Voegtlin, fvy
1935) cat (Behar and Biancani 1978) baboon (La Morte, Gaca, VÙise et a1
l9B0) and man (V{hrite and Bourde 1970) relaxes in response to CCK, probabJ-y
by the action of nonchol-inergic, nonadrenergic inhibitory neurons (Behar
and Biancani 1980). However other studies have demcnstated that CCK
increases muscular activity in the sphincter of Oddi in o¡rosstlln a¡td rabbit-
39
species ,(Becker and Ploody I97B; Sarles, Bidart, Devaux et aI 1976; Honda,
Toouli, Dodds et aI f983).
Autonornic control- of the gallbladder plays an inportant role in
potentiation of the pressure effect of CCK and the maintenance of
gallbladder tone (Pall-in and Skoglund 1964).
(ii) Pancreatic PoJ-lpeptide
pancreatic PoÌlzpeptide (PP), a 36 arnino acid polypepti-deris found almost
exclusively in the pancreas (Lonovics, Devitt, Watson et al 19Bl). In vivo
studies j-n humans, dogs and ttre pig have demonstrated that PP
ad¡ninistration results in gaì-lbladder relaxation with increased storage of
bil-e (Lin and Chance L974; Adrian,'.l,Litchenere, Sagor et aI I9B2; Greenberg,
McCIoy, Adrian et al I97B; Greenberg, McCloy, Chadr¿ick et al 1979) -
Although the effects of PP on the biJ-iarlz tree are opposite to ccK' both
peptides rise in parallel after a meal and purified CCK is an effective
hunroral rel-easer of PP in humans (Lonovj-cs, Guzman, Devitt et al- l-980).
( iii )Motilin
Motilin, a pollzpeptide hormone of 22 anrino acid residues has been isolated
frorn the duodenum and jejunum of man and several animals (dogs, Pi9s,
baboons). It is not sjnúl-ar in structure to any mernber of either gastrin or
secretin farnifies of hornrones (Domschke l-977)-
Motilin is released during Phase III and IV activity of the interdigestive
(fasting) myoelectrical conrplex and in man is associated with bile flow
into the duodenum (Keane, Dillagno, Dozois et al- 1980). Periodic
contractions of the gall-blaclder occur in close association with the
interdigestive rnigrating contractions in the stornach and both can
,1
40
simultaneously be reproduced by exogenous aùninistration of nrotil-j-n. (Itoh
and Takahashi 19BI).Thus motilin may regulate biliarlz motility in the
period between rneals.
Pancreatic Pollzpeptide and nrotil-in have litt1e effect on in vitro
preparations of human, rabbit and dog gallbladder muscle strips (Poneranz'
Davison, Shaffer 1983, Lonovics, Devitt, Rayford et al- 1979). Ttterefore
both pp and nrotilin appear to exert their respective actions at sites
remote fron the gallbladder without directly affecting galJ-bladder muscle-
(iv) opioids
Receptors that bind opioids are found on mucosal celÌs, snooth muscle fibres
and on both the body and ternrinals.of nerve cells of the gnrt. At present
there is little data on the distribution of either cells that produce
endogenous opioids or cells that containoplcids receptors within the biliary
tree. Thus, the physiotogical rofe of opioids in reg-ulating biliary
motility is undefined.
Hrptying of the gallbladder during an infusion of CCK-B and adnrinistration
of either saline, morphine, enkephal-in or naloxone (an opioid-antagonist)
has been evaluated in man by real time ultrasonography (t{orobetz, Baker,
McCallum et al IgB2). Saline and naloxone did not alter the normal pattern
of enptying of the gal-Ibladder during intravenous infusion of CCK-8. On the
other hand, enptying during the. infusion of CCK-B was conpletely blocked by
nrorphine or enkephalin. After administration of nrorphine or enkephalin, the
gal1bJ-adder assumed a round shape and its volunre significantly increased-
Vlhen naloxone \^Ias adrninistered after morphine or enkephalin, the
gallbladder enptied rapidly. These findings suggest that the opioids
stinn:Iate the sphincter of Oddi and the pressure of the sphincter
4T
increases. As a result the resistance to the flow of bile out of the .
gallbladder and conrnon bile duct into the duodenum increases. The
gallbladder cannot enpty even though it contracts. Blockade of the opioid
effect by naloxone relaxes the sphincter and the contracting gallbJ-adder
enpties quickly.
I NET]RONAL DSTERMINATVTS OF ÐflRAHEPATIC BILIARY I\OIILITY
(i) Influence of the parasynpathetic autonornic nervous system-
Autonornic contributions to gallbJ-adder tone have been exarnined by nerve
stirrml-ation and pharmacologic methods. Tkre paras]fipathetic nervous system
is clearly involved in the maintenance of gatJ-bladder tone (Pallin and
SkogJ-und 1964) i conversely vagotomy decreases resting galJ-bladder pressure
(Liedberg 1969) Galtbladder pressirie can be elevated by intravenous
acetylcholine and pilocarpine and this effect is blocked by atropine in all-
animal species studied (Halpert and Lewis 1930; Winkelstein and Achsner
1924; Winkelstein and Aschsner 1926; Menguyr Harlenbeck, Bollman et al
r95B).
Paraslnrpathetic receptors appear to be present in the gallbJ-adder and the
paraslznrpathetic system probably interacts with hornronal stimul-i in
regul-ating gall-bladder tone.
Foesel and Sewing (1978) showed that contraction of the gallbladder caused
by a stimulation of its intrinsic paras)¡rTpathetic fibers coul-d be enhanced
42
by a sublhreshol-d concentration of CCK. This observation strongly favoured
a contibuting role of cholinergic innervation in the control of gallbladder
motor function. yau and Youther (1984) nx¡re recently performed direct
transmural fiel-d stimul-ation on guinea pig in vitro gallbladder
preparations and showed acetlychoÌj-ne-mediated contraction. The
contractions were sensitive to atropine and tetrodotoxin, indicating that
the activity of choJ-inergic neurons \^/ere responsible for the muscle
contraction.
In humans,Rock, l4almud and Fisher (1981) showed that sham feeding resulted
in enptying of 50å of galJ-bladder vo'lume. Ttre effect was abolished by
atropine. The anxcunt of bite in the, fasting galJ-bladder is doubl-ed in
humans after truncal vagotomy conpared with selective vagotomy and the
anrount of residuat bile after enptyinÇ is greater (Inberg and vuorio 1969).
Whril-e human gallstones placed in a canine galtbJ-adder usually d'issolve
pronptly one study has shov¡n that truncal vagotomy significantly retards
dissolution (Barnett and Hilburn 1966). Sequestrati-on of bil-e into a large
stagnant gal-Ibladder could result in diminished bil-e acj-d secretion and
increased cholesterol saturation of bile through interruption of the
enterohepatic circul-ation. However, studies have sho'¡¡n a decrease in
biliary chofesterol saturation when the gallbladder leaves the
enterohepatic circul-ation either by disease or surgery (Shaffer and Small
1977; Redinger 1976).
Westphal, Gleichmann and Joik (1931) .reported that electrical- stjmulation
of the vagus could increase water absorption by the dog gallbladder' TLreir
resul-ts were not consistent and nìore recently vagal stimulation in the cat
fail-ed to influence the rate of fluid transport in the gallbladder using a
peifusion technique (Bjorck, Jansson and Svanik 1983) '
43
The influence of vagotomy on the sphincter of Oddi is contnoversial. Some papers
have reported sphincter refaxation. (Dowling I97I¡ Beneventano, Rosen'
Schein 1969). In dogs results are variabl-e (Amdrup and Griffith f970)
while in the rabbit, vagotonqz does not change electrornyographic patterns
(Gerolarni and Sarles L977 ) . In the conscious dog, nretacholine has been /reported to elicit spasm of the colTrnon duct (Lin 1975)
More importantly CCK appears to inhibit phasic contractions and decrease
spincter tone by stjmulation of non-adrenergic non-cholinergic i-nhibitory
neurones (Behar and Biancani 1980) -
(ii) Infl-uence of the slznpathetic àutonomic nervous system
Slzmpathetic stj-mulation by way of the right sptancLuric nerve has been
demonstrated to cause a relaxation of the gal-lbladder and this effect is
most readi-ly seen on a gallbl-adder that is in a contracted state either
induced hormonaly or neuraly. Such adrenergic pathways are nrediated via
beta receptors (Persson Ig12). However the exact functj-onaJ- implications of
this are still unclear.
It has al-so been found that electrical stimulation of the splanchnic nerves
stimulates the rate of water absorption by the gallbladder of the cat' an
effect which can be abol-ished by alpha adrenergic receptor bl-ockade. The
precise site of action of the slznpathetic nerves on water transport by the
gallbladder is urknown. \:art from a possibte direct effect on mucosal
cells, sympathetic nerves may act on l-ocal ganglia to inhibit rel-ease of a
neurotransrnitter which inhibits water absorption. A possible transrnitter
released by locat reflexes is vas6fi&iY&.ina1 peptide (VIP).Vasoactive intestinal-
peptide is a hornrone whrich is a rnember of the secretin farnily of
44
gastrointestinal hormones. Vasoactive intestj¡rai peptide may fi:nction
physiologically to inhibit contraction of the gallbladder. In several
animals (gnrinea pig, o¡lossum, cat and rabbit), physiotogic concentrations
of VIp inhibit the contraction of the srnootlt muscl-e of the gall-bladder
induced by acetylcholine and CCK (Lonovics, Devitt, Rayford et al- 1979) - fn
add.ition, VIP has been isolated fron nerve fibres within the muscfe layers
of the gatJ-bladder of both man and cat (Sund1er, A-l-umots, Hakanson et al
re71) -
The effect of pregnancy, the nrensti'ua1 cycle or female sex steroids on the
autonorn-ic nervous system has not been studied with regard to
gastrointestinal smooth muscl-e activity. In addition no studies have
exarnined the interaction of female horrnones with cholinergic or adrenergic
receptors. Therefore it remains a.possibitity that these hormones produce
some of their effects through autonornic pathways and receptors.
J. TTIE RM,ATIONSHIPS OF GASTR.IC EMPTYING TO GALLBI"ADDM. H\4PTYING
For a thorough understanding of post prandial gallbladder enrptying it is
inrportant to exarnine the conplex regnrtatory mechanism of gastric enptying which
are poorJ-y rnderstood.
The enptying of solids and liguids frorn the human stomach is tightly
regnrlated by chenroreceptive nrechanisms that are capable of sel-ective
response to meal conponents. For exanple, these nrechanisms respond
strongly to long chain but not short chain,fatty acids (Hunt and Knox
1968), to trlptophan but not glycine (Stephens, WooJ-sen, Cooke 1975),and
more strongl-y to HCI than citric acid (Hunt and Knox 1969). The mechanisms
are not only selective but are also quantitative, regutating the quantity
of acj-d entering the duodenum, independent of its concentration (Hunt and
45
Knox 1962) and reg'ulating the number of calories enptying from the stornach
per minute despite wide variations in the cal-orie density of liquid mass
(Hunt and Stubbs 1975). Although relevant chemoreceptors have been
Iocal-i-sed in the proximal small intestine (Cooke I97l) l-itt1e is knov¿-r of
receptor nechanisms through wLrj-ch they control the flow of nutrients frorn
the stomach.
Solids and liguids entering the duodenum rnight trigger mechanisms that
inhibit propul-sive forces. For exanple, both neuronal and hornronal
nrechanisms are known to be capable of regulating the tone of the stomach
(Stephens, Woolsen, Cooke 1976). Thus, the release of intestinal hormones
or the triggering of nervous reflexes by chenroreceptors in the intestine
might slow gastric enptying by djminishing gastri-c tone and thereby
reducing gastroduodenal- pressure gçadients. The final mechanism may
operate through the vagus nerve. Phasic contraction of the antrum is known
to be inhibíted via vagal- mehanlsms by fat, trlzptophan, glucose, or acid in
the duodenum (Kel-l-y and Code l-969; Meyer and Jones 1974; Roze, Couturier,
Chariot et al- I9l7; Thomas, Crider, Morgan 1934). Such inhibition might
reduce propulsive punping by the antrum.
As a motor unit the stomach is classicaly considered as having two
fi.rnctional areas,consisting of a proximal receptacle the fundus and body,
and a distal- punp the antrum. The antrum rnixes and churns gastric contents
and propels them into the duodenum..
Antra1 contractions deterrnine the delivery rate of gastric contents
into the dudenum. Frequency, direction and velocity of antral- contractj-ons
are determined by the gastric slow waves and their superinposed spike
activity. Spike activity is required for contractions to occut (Cooke
ì1
46
19751.
i,ti>te<1 solid liqricì. nea-Is rùay sepclral-e inLo different ptrysical phases i'ùricir
r¡glz each erçty frorn the sto¡iracìr at a¡r indepenclent ra'te' |'icluii-ìs ]eave tþe
stcrnach nore rapicily tl-lall solicis (ileaciing, Toihill, ì''Iclougtrlin et al 19761'
Às tþe1z are oi¡ltiecl into Lile fluocic-¡r.u1r 'ife:' are contiiruously r-eplacecl b1t
nei.;Iy seccetecl gastric juices, liru:i c':>q:osing'tìre reiirainiix; scJ-ic'Ìs to fresir
gastric secre'tions. Liquic',s of Ìri-gh solute conterrt have sl-ot'ret: gar';tric
o-nptying rates tlnn isotonic J-ic;uicl,s (cool'-e 19751. I-io"'¡e-ver tlæ,v qterrerallT
exn¡:ty frcrit tìle sto¡ach at ra-te.s rrci:e raJ-'i-c-t tlìa:'ì fai's or solicls (l'core'
Cristiart, Ocl':,ulrì 19:--11 ).
DigestiÌrlesohc'sclr¡:t;'sllc'\'rer¡-'ro:ai:lyi;ccaus;r-:i:Ì-teatr'ri:t'o:ia-ctsasa-
sie.¿ingi a¡¿la::atUs. SuS¡x:nc-,c-ci -¡rar--tiCleS Ca-rr pass i:rrrouc,Ìr tnr: ¡1'lc-rrrus ollJ-y
i"rjrer-r ìlrey hane irea:r grounii Cior,¡¡i'ct> ¡nrLicles }ess'ijram l-¡il¡t j-n clia;;'retr:r
(i:Þyer, ohashi, .j-e.iÏi et al 1931 ). i']ariicles greater tha;-r -J'iis size are
returned io the antn¡n for furiJrer grilc]inE (ï'l'einer, Graharn' R'eeCy et al
1931 ) . i,lon-d-igestairle sol iCs ,-tå Oto,rght to remaiu in tire stor¡acli r¡-rl-il
tlre resL o¡ li-re rrreal j-s erirptie,r. ,Iiolvever, Ca:nill-eri, l-ìror'm ancl r'aiagelacla
( 1 986 ) usìr-rg non-ciígestil¡l-e laltelled bran rece¡tl)¡ shot¡ed iJrat eiçt}zì-ng o'i
tirese particles is also a function of a¡rtral p=rist:'Isis' \''iÏrile tì-ie
Ial¡eltecj Ì:ra' r..¡as selectiveJ-y retained Ì:y the s'tolr,ach rela'cive to liqriri'
it cl.icì aptlear 'co øriptir at s'iirúlar rates to oiùer solid ccrrr¡;onent:; of Lhe
nrc¡l r¿hich LncÌ l¡cc¡r grorurd j-nto sllall i'rrrticles by the antn:¡':l' In suÌ¡Ì-v¡rt
(¡f ijrese frnd.il.lgs liclt, iìeic1, 1Þylor et aI (ga2) ol'-'served si¡rilar ea¡rtyi-ug
patterns for both larger non-digesti-bte solids and' titurable liver culæs'
If gastric onptying of solicls is res¡ronsi]¡Ie for contj¡rued stj"nulati on of
galJ-biarÌ1er conbraction furen gaIIJ:I¿rdCer re-fill-ing sirould occur rvhen
gastric errptying of sol-ids is; ccxlçIete'
/
47I{ore recently King, Adam, PryCe et aI (1984) have drav¡n attention to the
function oi antral contractions and tLre role tlnt peristaltic activity of
'bhe ctistal stcxnach plays in regulating gastric an¡:tying of solids. Using
real-ti¡ne ultrasound tlrey shorved tlrat ernptyir-rg of gastric crontents tlrcugh
the pyloms terdeci to occr-rr j-n short episocles rvhen the terminal arttrum,
pylorus ancl cluodern:m ryere rela.xed. Ttre authors c.oncluded that this pa.ttern
of nrovernent v,as unlil<ely ¡o be related Lo antral ¡reristalsis or to lce
attrilcuLecl to constant in-uragastric pressure alone. Itrey also obsen¡ed
tlrat r:icst gastric ¡reristalti c cycles vüere accctilpanied by retrognade flot'¿ at
tire Pirlorus.
It is lrcssible iluri a¡i' cÌraäges in ga}IÌ:ladcler einptlrj¡c; se'en r¡iti-r increasei
enc-ìor;eucus a:rcÌ, a¡>lcvj:enolts fcnle ser: ste::oicis relt be seconCary L<-; clerrges in
ças-i::ic anptiri¡q. Ijo';.'eve:: recmt s'tudies sr-rggest tirat gastric e.i'ptying is
not al-terec- i-n eitl:r::r iire seccnC b:1res'Ler of preçrralcl' (Scirade, Pelel'anos,
1.a'¡¡1¡e et aLl 198¿¡| or tire l-utea.l pirase of the ovulatory crTcle (Ilorol.'itz,
t\Þdi.crrr, (l:atterton et al- 19Lr4).
.fi-rus in the last centurythe search for ijre aetiology of gallstones has
goire fuiJ- circl-e. Initial-J-y the'eause of gall-stone foraation vras thought to
relate to irflarLi-iLlation of Ure qallblad-der i+all and inccrnplete gallbLadc]-er
eq:t1ri¡g. I',tren i'c l¿as re¡.lisei that biliary cholesterol- satr:ration v.as
vital for stone fonr,aticn, attentiorr r.¡as directed to the liver. l'he role of
altereC gaJ-lbtaCder motiLity in the genesis of litJrog'eni-c l¡ile and.
cÍrolesterol choleliihiasis is stil-l relatively une>q,olored artcl atternpts to
descri]:e lùis as¡rect of biliary physiology rvill improve or:r unclerstanding
of the nultifac-uorial pathogenesis of cholesterol cholelitiriasis.
i',luch re¡rains to i¡e ]earned a,bout the effects of fernale se>< hornones on
biliarl¿ rnotility and the metabolism of l:iIe acids and cholesterol.
48
CHAPTER II: CURRENT KNOhILEDGE ÀND
UNANSWERED QUESTIONS REGARDING
GALLBLADDER MOTOR FUNCTION
A. Gallbladder Function Current Concepts in
Preqnancy
B. Unanswered Questions Reqardinq Gallbladder
Function
C. Thesis Aims
L
l
ì
I
49
CL]RRENIT KNOI¡ILEDGE AI{D QUESTIONS T]NA}TSV{HìED
A. GALLBI"ADDER FUNCTION - CURREITI CONCEPTS IN PREGNA}¡CY
Studies by the Gastroenterology Unit of the University of Col-orado have
already shovun that after the l3th week of pregnancy (i) the size of the
galJ-bl-adder in the fasting state is twice that of non-pregnant control-s (2)
the tjme of contraction stjmulated by a standard liquj-d meal, is longer
than in controls (3) the maxj¡num percent emptied after the meal is less and
(4) the resj-dual volume after maximum emptying is nearly three times as
great as in controls. rn early pregnancy (first 12 weeks) the only
significant alteration 1s slower emptying after the liqui-d meal. These
alterations in gallbladder function could contribute to precipitation of
cholesterol crystals and their retention in the gallbladder. F\rrther, they
could account in part for the increased bile acid pool sj-ze and for sorne of
the changes in bife acid slmttresis observed in pregnancy.
The interrel-ation of the various conqronents of the enterohepatic
circulatj-on (EIC) of bife acids is exceedingly conplex. However, to
understand chofesterol gallstone formatj-on it is apparent that knowledge of
mechanism altering bj_Ìe acid EFIC is inportant.
The storage of a J-arge proportion of bile acid pool in the gallbladder
ù:ring the night would be oçected to produce fasting hepatic bil-e that isnore lithogenic, raùtereas the storage of only a small propgrtion of the pool
would probably be associated with less lithogenic fasting hepatic bil-e. Inthe latter situation most of the bile acid pool would be nrore or less
continuously circulating thror.rgh the intestine and 1iver, causing
inhibition of bile acid synthesis and a smaller pool size, as fouhd in many
50
patients after cholecystectorny.
If a large portion of the pool is stored in the gallbladder overnight,
synthesis woufd be stjmulated and the pool size increased. On the other
hand, synthesis rate and pool size rnight be deterrnined largely by tJ:te
cornpleteness of gallbladder enptying. If the gal-J-bladder enptied completely,
a large load of bile acid eventually returning to the liver woufd be
expected to suppress synthesis, but if galtbladder errptying were inconpJ-ete
and a substantial portion of the bile acid pool was retained, fess would
return to the l-iver and synthesis would be stjmulated- Results from
Colorado have strongly suggested a central role for the gallbladder in the
,enterohepatic circulation of bile acids and bile acid kinetics and sup¡rort
the hlpothesis that altered gallbladder function in pregnancy nright play an
im¡rortant role in cholesteroJ- gallstone formation (Kern, Everson, De Mark
et a1 19Bl).
The hypothesis described assumes that bile acid absorption efficiency'from
the small intestine is the sarne du¡ing pregnancy, that intestinal transit
of bile acids is not significantly altered and that there is no effect of
pregnancy on the capacity of the liver to respond appropriately to changes
in intracellular bile acid. concentration. Alterations in the intestinal
bile acid absorption or hepatic response are not suspected,but if
experinrental resul-ts i-ndicated otherwise then direct studies would be
necessa-ry. fntestinal absorption of bile acids can be studied by ileal
perfusion, but techniques for direct studies of hepatic response to changes
in intracelluLar bil-e acid concentration in human subjects do not now
exist. Intestinal transit tìrne rnight be slowed as pregnancy progresses by a
progesterone effect or other neurohormonal alteration. It j-s als<-l
conceivable that gallbladder enptying could be inrpaired by reduced gastric
enptylng by food stjmulus to CCK release attd/or reduced production of CCK
/
5l_
by ttre intestinal mucosa. Since the gallbladder response to
intraduodenally-infused arnino acid is diminished in pregrnancy, gastric
enptying may not be an irrportant factor (Kern, Everson, De Mark et al I9B2)
At the tjrne of the present studi-es, rel-iable means for measuring CCK
were not generally available. CCK (or its octapeptide) cannot be
gj-ven to pregnant wonen for ethicaf reasons butrif necessarlz to study the
question of insufficient endogenous CCK vs irrpaired gallbladder response,
it can be given to the other groups being studied, consj-sting of normal
vùornen and those on oral contraceptive steroids
A hlzpothesis of this thesis is that the increased size of the gallbladder
after an overnight fast and after a meal in the latter two-thirds of
pregnancy has two separate causes: (a) decreased concentration of bile,
probably due to inhibition of gallbladder epithelial Na+K+ ATPase activity
resulting from high serum oestrogen concentrations and (b) decreased tone
and contractility of the gallbladder'.due to its exposure to high
concentrations of progesterone.
It is essential to know whether the-increased gallbladder volurne contains
an increased amor:nt of bile acid or whether the volu¡ne increase is due
entirely to water. Oral chol-ecystography has shown decreased concentration
of contrast material by the galJ-bladders of pregnant \^/olnen (Gerdes and
Boyden 1938). One study has suggested that oestrogens inhibit galJ-bladder
mucosal Na+K+ ATPase activity (France, Menon, Reay et aL 1-977 ), the enzlnìe
responsible for its absorption of Na* and water. The concentration of
gallbladder bile ca¡not be neasured directl-y but can be estimated from
simultaneous nìeasure¡nents of volume changes by ultrasound and bile acid
output into the duodenum. The latter can be calculated from data obtained
\,rith the noñ:ábsoibable mâiker téchnique dur-ing Çallbladder contraction.
+
I11j¡
rlql
'u¡
,i
52
Progesterone is a snrooth muscle relaxant. Both pregnancy and progesterone
aùninistration have been shov¡n to inprove gallbladder emptying in several
animal species. This feature of gallbladder physiology wiII be studied in
human subjects by nreasuring the effect of aùn-inistration of progesterone
containing componnds on gal-lbladder emptying in response to various stimul-i
and by correlating gallbladder motor activity with serum proqesterone
Ievels during pregnancy.
B. TJNANSI/ÌERED QT]ESTIONS REGARDING GALLBI,ADDM FUNCTION
fn this thesis the planned studies r¡/ere designed to answer several
questions about gallbladder function, the relation of gallbladder function
to the bile acid kinetics of the enterohepatic circulation, the nrechanism
of observed changes, and the detailed character of alterations associated
with pregnancy and female sex hornxrnes. The following questions were
exarrined: .
(f) fn pregnancy, is there more bile in the gallbladder throughout the day
than in non-pregnant controJ- subjects?
(2) Does ad¡ninistration of contraceptive steroids and oestrogen alone
affect gallbladder function in human subjects?
(3) Do increased volumes of the gallbladder influence biliarlz lipid
con-position?.
(4) Is gallbladder bile in the fastj-ng state less concentrated in
flenopausa]- women before and after taking oestrogens?
/
I
!The increased pool size of the primarlz bile acids and the decreased number
I
53
of enterohepatic cycJ-es dr:ring pregnancy couÌd be caused in part by slow
transit of bile acids through the small intestine, perhaps seconda4z to a
progesterone or other neurohormonal effect on small intestinal snx¡oth
muscle. Thus an additional question asked in thls thesis htas:-
(5) Is small intestinal transit tjme proJ-onged in pregnancy?
As the work of this thesis developed it was observed that the gallbladder
fail-ed to refill in normal subjects ingesting three meals per day. A
pro¡rosed nechanism for this observation \^/as that the sJ-ow enptying of
solids from the stomach into the upper smal-I bowel- controlled gallbJ-adder
enptying and refilllng. Therefore a further question asked \^/as:-
(6) What is tJ.e rel-ationship between the rate of gastric erçtying and
gallbladder emptying?
C TTIESIS AIMS
The aims of this thesis were designed to answer the preceding guestions and
a-re as follows:-
(I) To measure gallbladder storage and enptylngthrroughout the day and night
during ingestion of meals in four similar groups of heaì-ttty, non-obese
v/omen: (a) controls in the follicular and luteal phases of the ovulatory
cycle (b) pregnant wonen (c) post-partum h/onen (d) contraceptive steroid
users.
(2) To investigate the rol-e of the gallbÌadder and small intestine in
:*!il
I,I
tI
;
I
t
regulating the rate of biliarlz lipid secretion and biliary lipid
54
coq)osition.
(3) To deterrnine if chronic aùninistration of'the conjugated
equino-oestrogen premarin alters gallbladder fuction, biliarlz lipid
conposition and secretion in post n€nopausal women.
(4) To deterrnine if gastrointestinal t¡ansit time is prolonged in early
pregnanc)z and to neasure serj-al changes in gastrointestinal transit by
studying the same i-ndividual ttrroughout pregnancy and post-partum.
(5) To measure the ti¡e course of gall-bladder enrptying and refilling after
ingestion of a standard breakfast, to rel-ate the rate of gal-lb1adder
enptying to the rate of gastric emptying of solids, and to rel-ate
gallbladder refilling to both corpletion of gastric emptying of solids and
reduction in hunoral stimulation.
/
55
CHAPTER III: METHODS ÀND RESULTS
A. Gallbtadder Function in the Human Female:
Effect of the Ovulatorv Cvcle, Preqnancy
and Contraceptive Steroids
B
(i) Methods (a) Subjects
(b) Ànalytical Techniques
(c) Indices of Ga].]-bladder Function
(d) Analysis of Data
(ii) Results (a) Effects of the Ovulatory Cycle
(b) Effects of PregnancY
(c) Effects of Contraceptive Steroids
Gal-Ibladder and Small- Intestina]. Requlation of
Methods ( a)
(b)
Subj ect s
Gallbladder Concentration and
Emptying Af,ter IV CCK
Analytical Techniques
Biliary Lipid Secretion
Biliary Lipid Secretion During Intraduode¡gl
Infusion of Standard AminoAcid and Liquid Formula
St imul-i
(i) Methods (a) Subjects and Procedures
(b) Analytical- Techniques
(c) Analysis of Data
(ii) Results (a) Biliary Lipid Secretion
(b) Gallbladder Emptying
(c) Small Bowel Transit Time
(d) Human Serum Pancreatic Polypeptide
C. The Effects of Chronic Oestrogen Administration on
Biliarv Lipid Secretion, Bile Acids and Gallblad<ler
Function in Post-Menopausal blomen
(c)
(d)
(i)
( ii ) Results
56
(e) Bile Acids
(f) Gallbladder Volume and Emptying
with Standard Meals
(g) Analysis of Data
( a) GalJ-bladd'er EmPtYing
(b) Gallbladder Concentration
(c) Biliary Lipid Secretion
(d) Bile Acids
- Transit Time in PregnancYD. Orocaecal
(i) Methods (a)
(b)
(c)
( ii ) Results
Subj ect s
Orocaecal Transit Time
Analysis of Data
E. Co-ordination of Gastric and Gallbladder
Emptyin q After Inses tion of a Reqular Meal
( i) Methods
(ii) Results
(a)
(b)
(c)
(d)
(e)
(f)
(a)
(b)
(c)
Subj ect s
Gastric Emptying
Gatlbladder EmptYing
Gastrointestinal Transit Time
and Serum HPP
Ànalytical Techniques
Analysis of Data
Gallbladder EmPtYing
Gastric EmptYing
Serum HPP
/
57
MSTTTODS AT{D RESTILTS
A. GALLBLADDER. FUNCTION IN ITIE HT]MAN FEMALE: EFFECT OF TT]E OWI,ATORY CYCLE,
PREGNA}TCY AI{D CO}üIRACPTIVE STROIDS
( i) ¡,ETTIODS
(a) Subjects
The characteristics of subjects are shor¡¡n in Tab1e 1. There v/as no
difference in height, weight, percent ideal weight (Metropolitan Life
Insurance Conpany.statisticafsull-etin, f960) age, history of contraceptive
use, or history of pregnancy between foll-icular and l-uteal phase controls.
Although the pregnant group was heavier than the control group' the
difference \^/as consistent with hoimal-fetoplacental developnent. Conpared
with controls,.half as many pregnant \^/olnen had prior history of taking
contraceptive steroj-ds,whil. ari"å as many had had a previous pregnancy.
Wonen taking contracepti-ve steroids were slightly but not significantly
heavier than control-s. Alt of them had been taking contraceptive steroids
continuously for 0.5-6 yr (median 3 yr) and none had been pregnant-
No subjects had any known illness and none was taking any medication
(except contraceptive steroids). Al-I subjects had normal fasting serum
Ievels of aspartate amino transferase, alkaline phosphatase, and
bil-irubin.
Eleven studies were done in 9 wonen taking contraceptive steroids. Ttre
phase of the ovulatory cycle in controls was determined from nenstrual
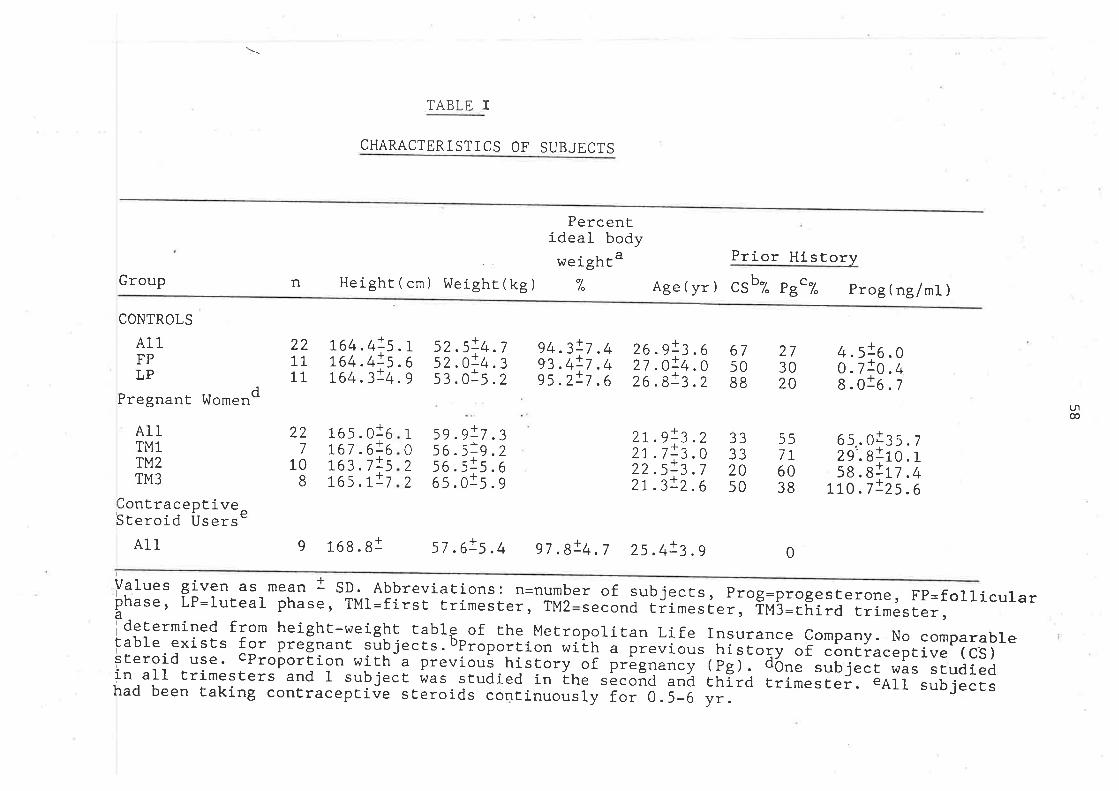
\
TABLE I
CHARACTERISTICS OF SUBJECT S
Percentideal body
, weightaHeight ( cm ) I^leighr (kg ) %
Prior HistorvPouGr n Age(yr) csb% pB"% prog(nglml)
CONTROLS
AllFPLP
Pregnant [ntorend
AllTM1Tt42TM3
Contrace pt ivee
ST eroid UsersAll
palues givenphase, LP=lutadetermined f.
lable existssteroid use.in all trimeshad been Èaki
164 .4!5 . L764.4!5 .6ß4 .3!4 . s
165 . 016rc7 .6!6Læ ,7!5ß5 . r!7
52.5!4 .752 . O!4 .353.015.2
5s.s!7 .
56.556 .565.0
94.3!7.4% .4!7 .495.2!7 .6
26.91¡. o27 .O!4.026 .8!3 .2
27 .9!Z . Z2r.7t3 .O22 .5!3 .72L.3t2 .6
22TT11
227
108
675088
33332050
(Pg).
273020
557T6038
4.st6.oo.7!0.4s.o1o.z
(-rlco
IU
22
!:9.15.r:5.
269
65..029'.858 .8
!70.7
a
-J',l*. /r110. Ia:L7.4I:25 .6
9 168.81 57.6!5.4 97.B!4.7 25.4!3.g 0
as mean t SD. Abbreviations: n=number of subjects, Prog=progesterone, FP=folliculareal phase, TMI=first trimester, TMz second trimester, TM3=third trimester,rom height-wei ght tabl f the Metropolitan Life Insurance C ompany. No comparableeo
bPtfor pregnant subjects. oportion with a previous histo y of contraceptive (cs)cPropor tion wiEh a previous history of Pregnancy One sub ject was studiedters and I subject was studied in the s econd and third tri
rd
ng contraceptive steroids continuously for 0.5-6 yr.mester. eAll subjects
59
history (ovulation \^/as considered as occr:rring 15 days before nenstruation)
and a single serum progesterone level. It was 0.15 - I.7 ng/nù in the
fol-licular phase, and 2-I7ng/ml in the luteal phase. Al-1 subjects had
regular cycles, l-l- were in the follicular and l-1 in the luteal phase of the
ovulatory cycle. The duration of pregnancy vüas deterrnined from the date of
the last normal ovulatory cyc1e. Sevän subjects were in the first
trirrester, 10 in the second, and B in the third. The contraceptive sterolds
used in this study contained Ìmg of the progestational conpound
norethindrone, and eitJrer 35, 50 or B0mg of the oestrogenic corn¡ronent,
mestranol. Studies were done on days 12 Lo 2I of pill adrninistration.
At 8.00 p.m. the evening before study, subjects ingested half a turkey
sandr¡'rich and 250 ml of whole ndl-k, and then fasted overnight. The day of
study their diet contained 2238 caI, l.5Z protein and 46? fat. They ate at
8.30 a.m., 12.00 noon, 5.00p.m. and 8.00 p.m. Breakfast consisted of one
egg, t\^¡o slices of bacon, two pieces of buttered toast, 100 ml orange
juice, 40 ml low fat nlilk, and 20O ml- of coffee or tea (610 cal, I2e",
protein, 44s" faL) A.l-J- subjects ingested the entire diet as nronitored by a
dietitian
(b) Analytical Techniques
Gallbladder size and enptying were deterrnined by real tjrne ultrasonography
(see þpendix). Ttrey were obtained during fasting at 15 min after the start
of breakfast, and eveq/ 5-10 nin for 90 min. Ttrereafter, sonographs \tere
taken hourly until rnidniqht.
Subjects ate breakfast upright, reclined at a 15-30 degree angle for the
next 90 min, but they engaged in normal physical activity the rest of the
day
60
(c) Indices of Gallbladder .t'unction
Gallbladder volumes brere calcul-ated from sonographs. Fasting volume (FV)
was lhe vol-ume befone breakflast. Residual galì-bladder volume (RV) was the
lowest volume achieved in the first 90min after breakfast' The pencent of
emptying (%E) was equal to (I-RV/FV) x 100%. The average hourly vol-ume (HV)
v¡as the average of gal-lbladder volumes mêasured every hour from 11.00 am to
midnight.
Although changes in gal-Ibladden vofume can result from bil-e entering the
gallbladder, blle leaving the gallbladder, absorption of water, and
secretion of water, onJ-y gallbladder vol-ume was measured. Emptying is defined
as bhe net decrease in volume that occurs over time. Gal-lbladder emptylng
was assumed to obey the finst-order exponential function, VL/Vo - e-(bb)'
where Vt is gallbl-adder volume at time t, Vo is initial gallbladden volume
and b is the rate constant of emptying. Since commencing this study another
group using the more easily reproducible radionuclide scanning technique
with j-ntravenous 99t.-eUlOR, has shown that gal-J-bÌadder emptying after a mixed
sotid/tiquid meal- is best describeà úy a double exponential function sinlilar
to the observations reported here (,Baxter, Grime, Critchl-ey et aI 1985)'
Rate constants of galJ-bladder emptying after breakflast were calculated from
lnllinear regression of gaIÌUf.Oa"" vofume vs time. Serum pnogesterone levels
were measured by radioimmunoassay at Endocrine Sciences (Tarzana, California).
(d) Analysis of Data
Group differences hrene evaluated by Studentrs t-test for unpaired data. The
relationship of indices of gallbladder function to other variables were
evaÌuated by J-ì-near negression analysis. Group differences in slopes of
regression lines were evaluated by F statistics using the extra sum of
squares principle (Draper and Smith 1966) -
It was intended to eval-uate each control subject in both phases of the
óvulatory cycle, each pregnant subject in each trimester o f pregnancy and
/
6
postpartum and each subject taking contraceptive steroids before and after
contraceptive use. Most subjects however decl-ined repeated studies. OnIy 2
pregnant \^¡omen were studied in more than one trinester of pregnancy, and
only 5 were studied post partum. No control was studied in both phases of
the ovulatory cycle and no contracentivl steroid user \^¡as studied before
starting this agent. Accordingly, differences in galtbladder function
induced by the ovulatory cycJ-e, pregnancy, or contraceptive steroids were
anal-ysed by conparing group mean vaÌues, a less sensitive technique to
detect differences than paired analysis.
(ii) RESTILTS
(a) Effects of the Ovul-atory Cycle
Al1 indices of gallbladder frmction \^/ere similar in the fol-licu1ar and
luteal phases of the ovulatory cycle (Table 2). Neither the day of the
ovulatory cycle nor serum progesterone level- correlated with any index of
gallbladder function in the control ?roup. Accordingly, data frorn control-
subjects were pooled for conparison in other groups.
(b) Effects of Pregnancy
Fasting, residual and average hourly volunes were increased in all
trirnesters of pregnancy (Table 2). In addition, gallbladder volume was
significantly greater in pregnant \,vornen at each hour of the day (Figure 3).
TLrus, bile retention in tfie gallbladder $/as greater in pregnancy at all
tirnes. Fasting and residual gallbladder volume (Figure 4A and 48) increased
linearly during pregnancy from the first to third trinrester. Thre l-inear
and residual gallbladder volunes corre lated directly
and significantly with week of pregnancy and serum progesterone levels
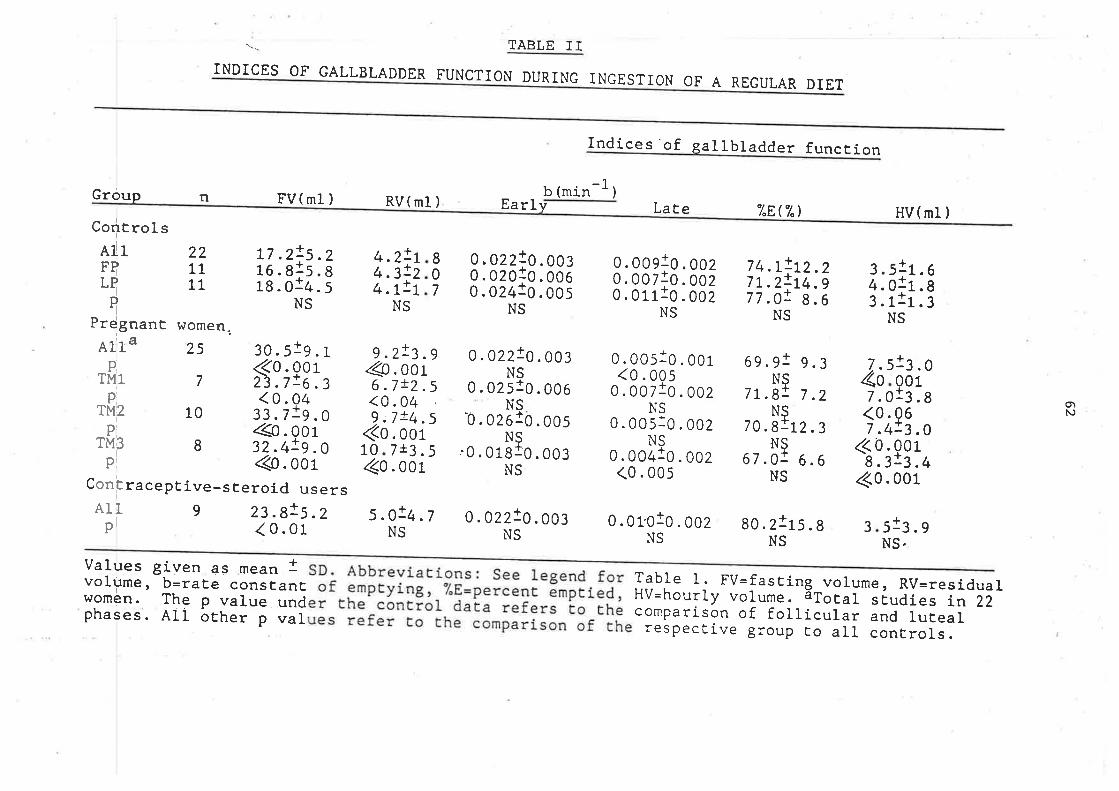
INDICES OF GALLB
FV(ml )
t7 .2!5.216.81s .818.014. 5
NS
TABLE IT
FUNCTION DURI
Earl
0.003
0.006
0 .00s
0. o2z1o. oo:NS
NG INGESÎION OF
Indices'of
-1b (min )v LaÈe
A REGULAR DIET
gal lbladder funcEion
"LE,"L)Group n
CorltrolsAlrFBLT
IPrdgnant r,romen..
LADDER
RV(ml)
4.2!4.3!4.7!
NS
21
9 .z!3.9Qs.oot6.7!2.5<0.049:7!4.5
(0. oor0 7t3.5
.0014o
5 .O!4.7NS
8 0, 02zto. oo¡0 0.02010.0067 0.02410. oo5
NS
0.00910.0020.ool!o.ooz0.01110.002
NS
HV( ml )
3.511.¿. o1r.¡ . r1r.
NS
221111
74.L!7L.2!77.0!
NS
1
9.3
7.2
6.6
L2.3
1
IIS+
NS
69 .9N
7 L.8N
70.8
1
01
S1
S+
0.005
0.022!NS
0.0251NS
0.0261NS
'0.01810.003NS
1
L2.214.98.6
683
Alla 25
7
10
8
@. oorraceptive-steroid users
9 23.8!5 .2< 0.01
I0I010+
30. 5 Ol
PTM1
PTM2
PTM3
p
onE
AltP
<0.23.7<0.
33.7
32.4
016.349.0019.0
0.005<0 .0
0.007N
N0.00/+
0.00150.002
0 .002
0.002
7.0(0.7.4
<0.8.3
<0.
7.4o
5
orN
1: .0Q01:3.gg6:3.0901-3 .4001c
<0.005
o.01.010.002NS
N67 .0
80.2115.8 3NS
st¡. g
NS,
Values given as mean Ivolume, b=raEê consEanEwomen. The p value undphases. All oÈher p val
SD. AbbreviaEions: See legend forof . emptyirg r -
"/.[=percenE ãmptied,er the conErol data refers Eo theues refer Eo the comparison of the
Table l. FV=fasÈing volume, RV=ÍêsidualHV=hourly volume. ãTotal sÉudies j,n-iZ-comparison of follicular and luEealrespective group to all conErols.
63
(Figures 5A and 58).
Average hor:rly volunes did not correlate significantJ-y witJ- either week of
pregnancy or serum progesterone levels (Fign:res 4C and 5C).
Gallbladder enrptying after breakfast is shown in Fig'ure 6. T\^/o rates of
gaÌlbladder emptying were identified. The initial rate of emptying to 50%
of fasting volune, was identical in pregnant and control subjects
(-0.022/nin and -0.022/nrin respectively; p: NS)- The second rate of
entptying in the pregnant group was one-half that of the control group
(-0.004/min vs. -0.009/min, respectiveJ-y; F(n1-2, n2-2) 8.5f4; p (0.005).
Four women \^/ere studied in the third trimester of pregnancy and again after
delivery. Fasting, residual,and hourly volunre decreased in the postpartum
period in each case (Tabl-e 3). Gallbladder vol-umes returned toward normal
as soon as 2 weeks postpartum. In al1 subjects only one rate of enptying
was observed after breakfast (Tabte 3) One subject, KLic, was studied at 18
weeks of pregnancy, 2 days postpartrìrô, and 4 weeks postpartum. At 2 days
postpartum, aII gallbladder volumes-were Iarge and enrptying was extremely
slow (Tabl-e 3). Throughout the day her gallbladder achieved only 48?
enptying. This marked degree of bile retention and slow enptying rate
approached the normal- range 4 weeks fater.
(c) effects of Contraceptive Steroids
Fasting gaì-ì-bladder volume was increased in this group, but residual and
hourly volurnes were not (Table 2). Early and late rates of gallbladder
enrptying were alnost identical to control (early =-0.022/ntn and late:
-0.0l0/nLin)., The anx¡unt of c-restrcx¡en in Lhe preparation did not correl-ate
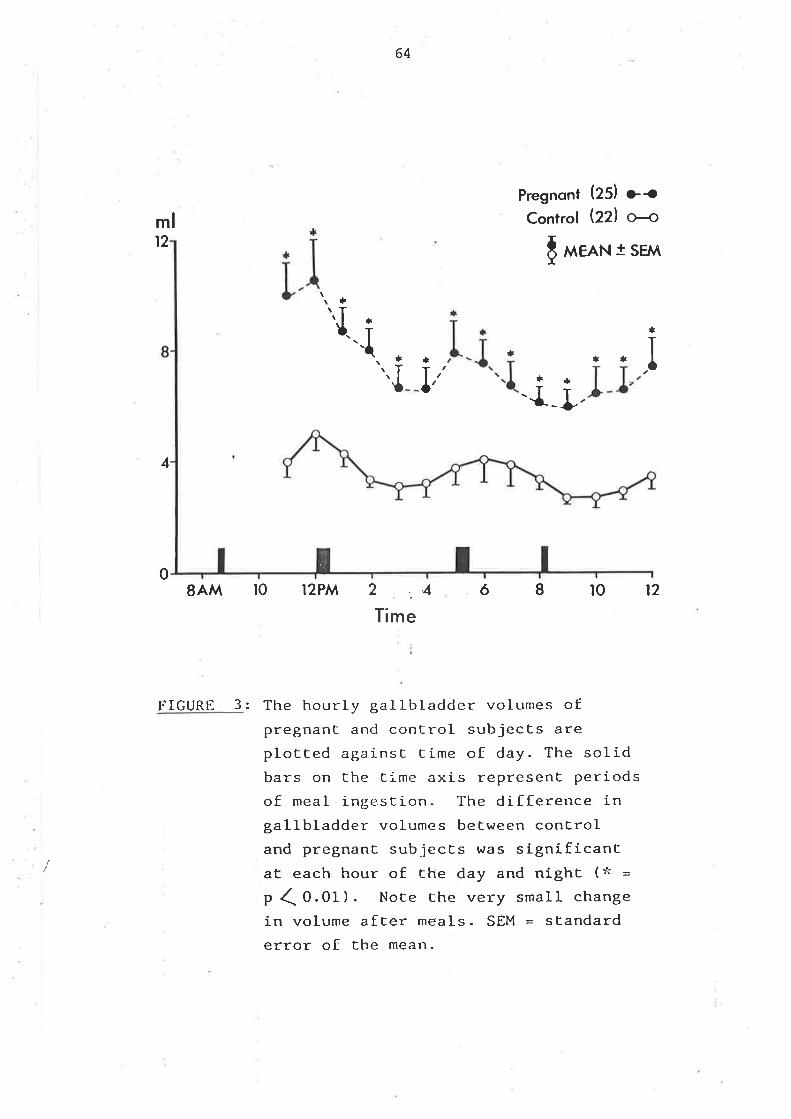
64
mlt2
4
Pregnont (ZSI r¡Gontrol þZl æ
[ ,,,rem t SEM
t.t
"rl_. i\
t
lt
f,'+
Jt¡*
t¡-J-_¡,
08AM IO I2PM
FIGURE 3:
2 ...4
Time
681012
The hourLy gallbladder volumes ofpregnant and control subjects areplotted againsE Iime of day. The solidbars on the time axis represent periodsof meal ingestion. The difference ingallbladder volumes between conCroland pregnant subjecEs hras significantaE each hour of the day and nighc (* =
p (0.0f). Note the very small change
in volume after meals. SEM = standarderror of the mean.
/
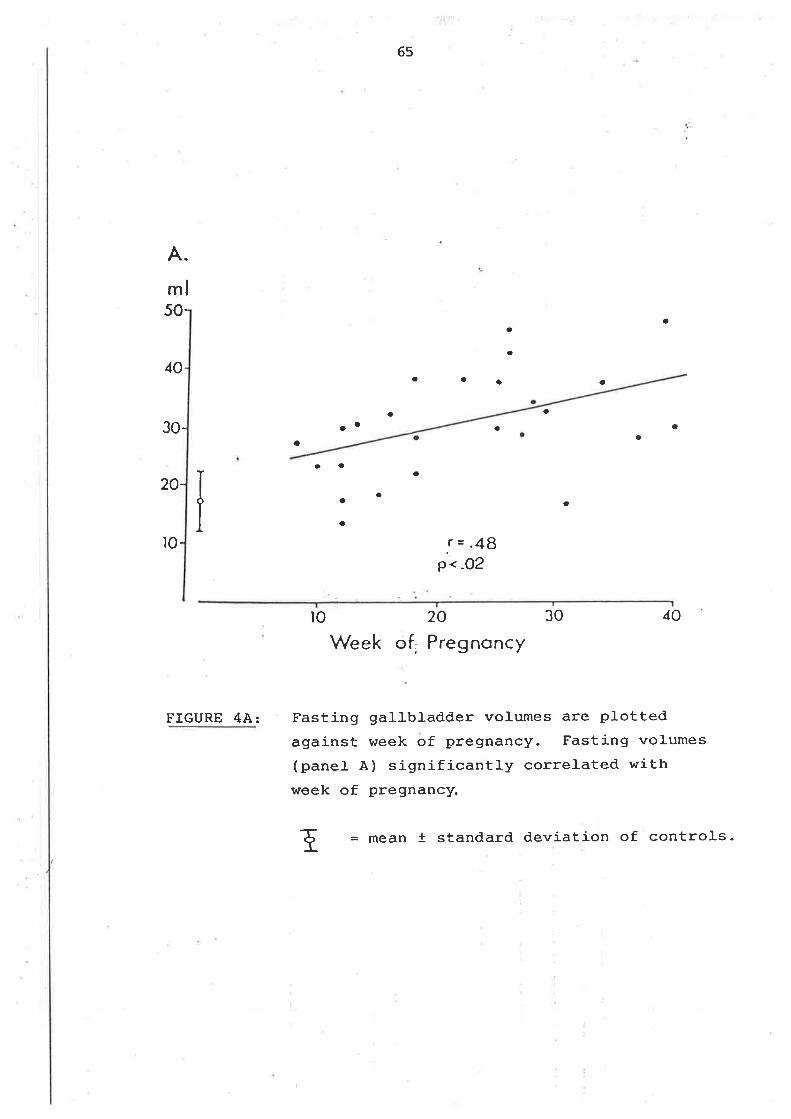
,Ì!.
65
A.
ml50-
40
30-
20-
ro-
aa
a
a
a
a a a
aaa a
aa
a
a
a
a
a
a
o
a
!=.48P..o2
FIGURE 4A:
to 20 30 40
Week of. Preg noncy
Fasting gallbladder volumes are plottedagainst week of pregnancy. Fasting volumes(panet À) significantly correlated withweek of pregnancy.
E = mean t standard deviation of controls-
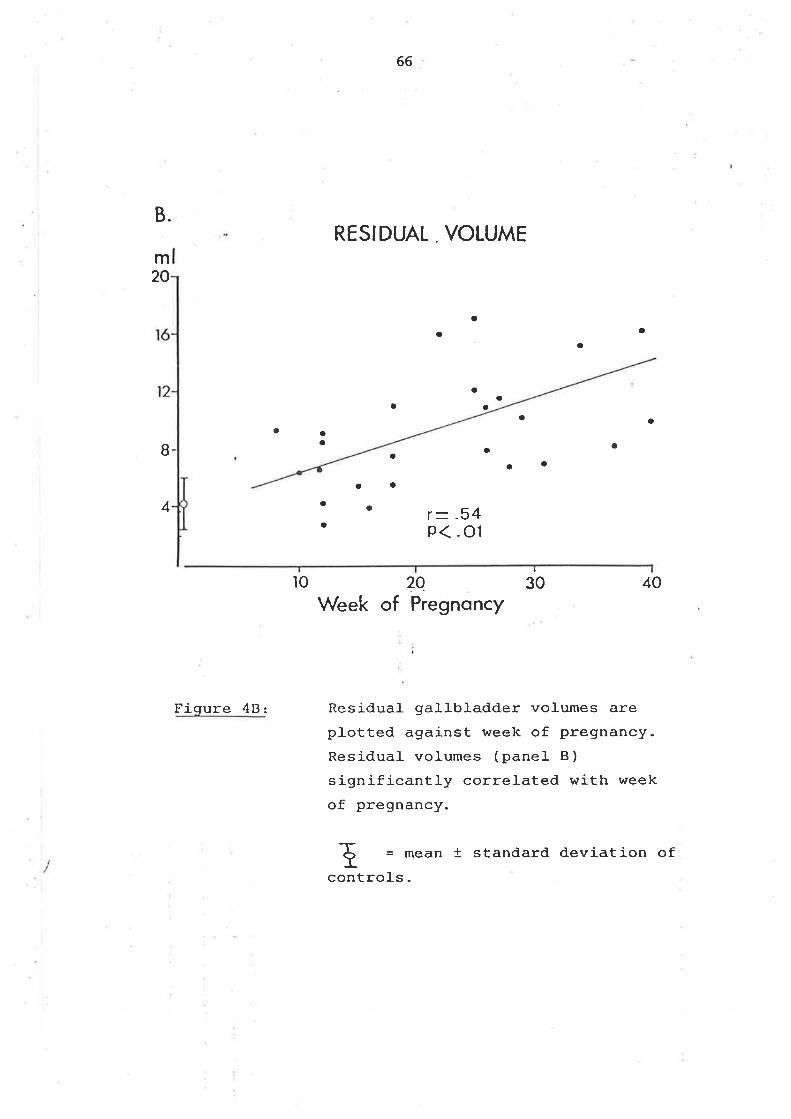
66
RESIDUAL . VOLUMEB.
m20
o
a
aaa
aa
a
ao a
a aa aaaB
I
30
aa
a
aa
a4 r- .54
p<.01
ìo ?oWeek of Pregnoncy
40
Fiqure 48: Residual gallbladder volumes areplotted against week of pregnancy.Residual volumes (pane1 B)
significantì-y correlated with week
of pregnancy.
-rt = mean + standard deviation of
controls.
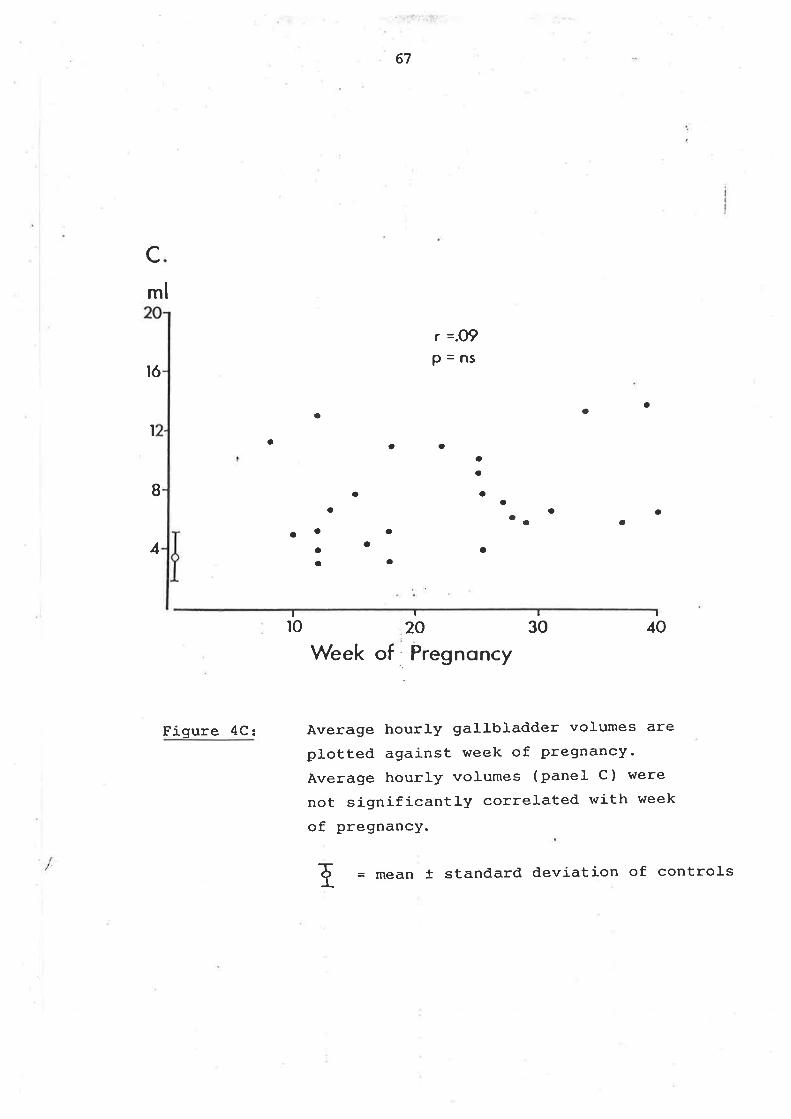
'lll.Flriþi:1
67
cml
ró
r =.o9p=ns
arta
Ia a a
I a
aa
aa
aOaaa a
o
a
a
oa
aa
a
4
I
40I
30¡
20¡
r0
Figure 4Cz
Week of Pregnoncy
Àverage hourly gallbladder volumes are
plotted against week of pregnancy.
Average hourly volumes (panel C) were
not significantly correlated with week
of pregnancy.
r = mean t standard deviation of controls
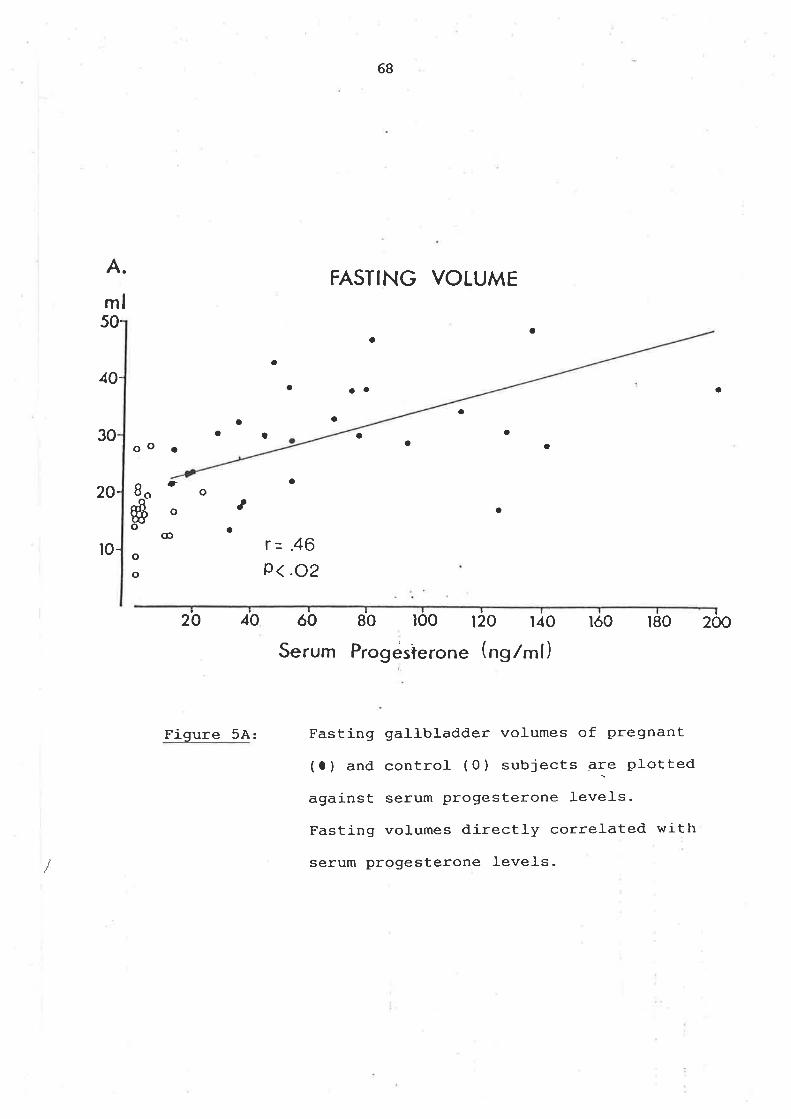
A.
ml
68
FASTING VOLUME
50-
40-
20-
r0-
oa
a
a aa a
a
aaa
aa
30 a
oo . a a
tra
aa
otj
o
@
a
oo
r=.46p<.o2
20 40 óo 80 ro0 120 t40
Serum Progésterone (ng/ml)lóo t80 200
Figure 5A: Fasting galJ-bladder volumes of pregnant
(a) and control (0) subjects E:" plotted
against serum progesterone leveJ-s.
Fasting volumes directly correlated with
serum progesterone levels-
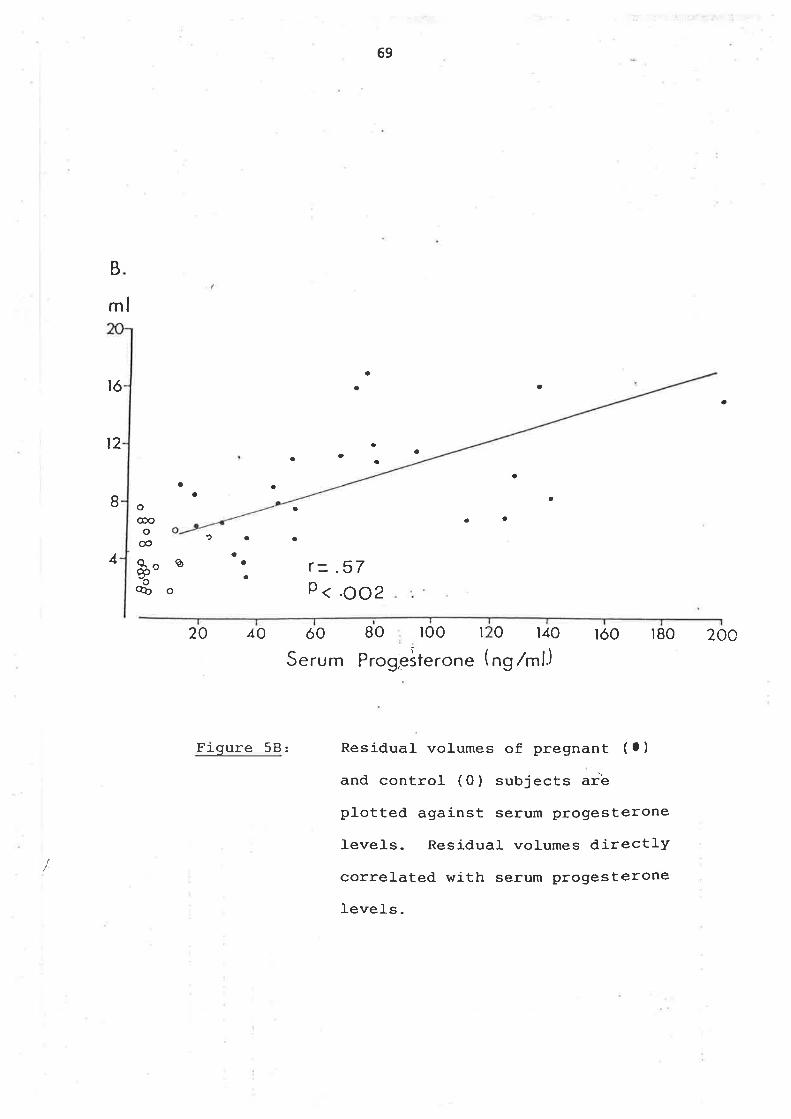
69
B
ml
tó
4
a
a a
a
ao
aa
t2
a
a8a
a
a
aa
o@oo
@
Q.^ú'o%
aa a
a
a
a
a
1
ø
o
r -_ .57P < .ooz
20 40 óo
erum
BO ì00 r 0 140 ìóo lB0 20c
Progeiterone (ng /ml.)
Residual volumes of pregnant ( O )
and control (O) subjects arê
plotted against serum progesterone
levels. Residual volumes directly
correlated with serum progesterone
IeveIs.
S
Figure 58:
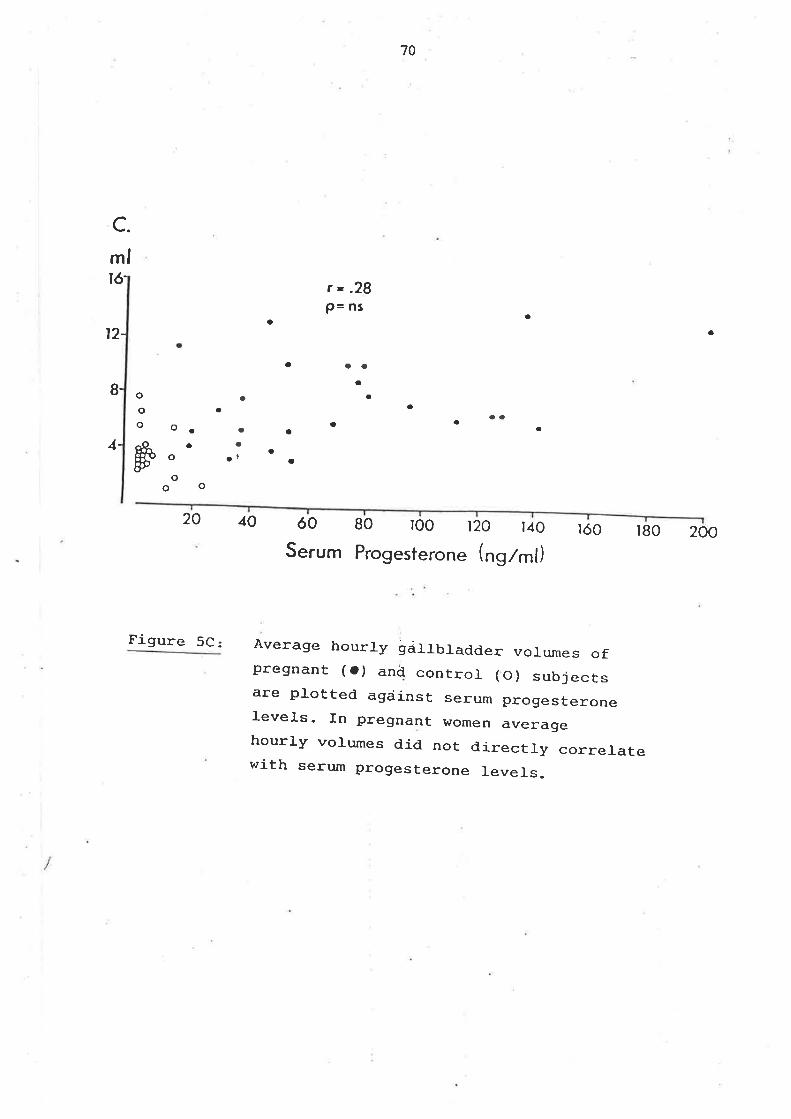
a
70
c.mlró-
a
r=.28P= ns
aaa
a
at2-
aa
a
aa
a
a
aat
a
a
aooo
8-
4-
aa
a
o.a
o
o9O
#20 40
Figure 5C:
óo
Serum
80 100 120 r40 tóo r80 200Progesterone (nglml)
Àverage hourly gáÌJ_bladder voLumes ofpregnant (o) and control (O) subjectsare plotted agáinst serum progesteroneLevels. In pregnant women averagehourly volumes did not directJ-y correlatewith serurn progesterone J.eveÌs.
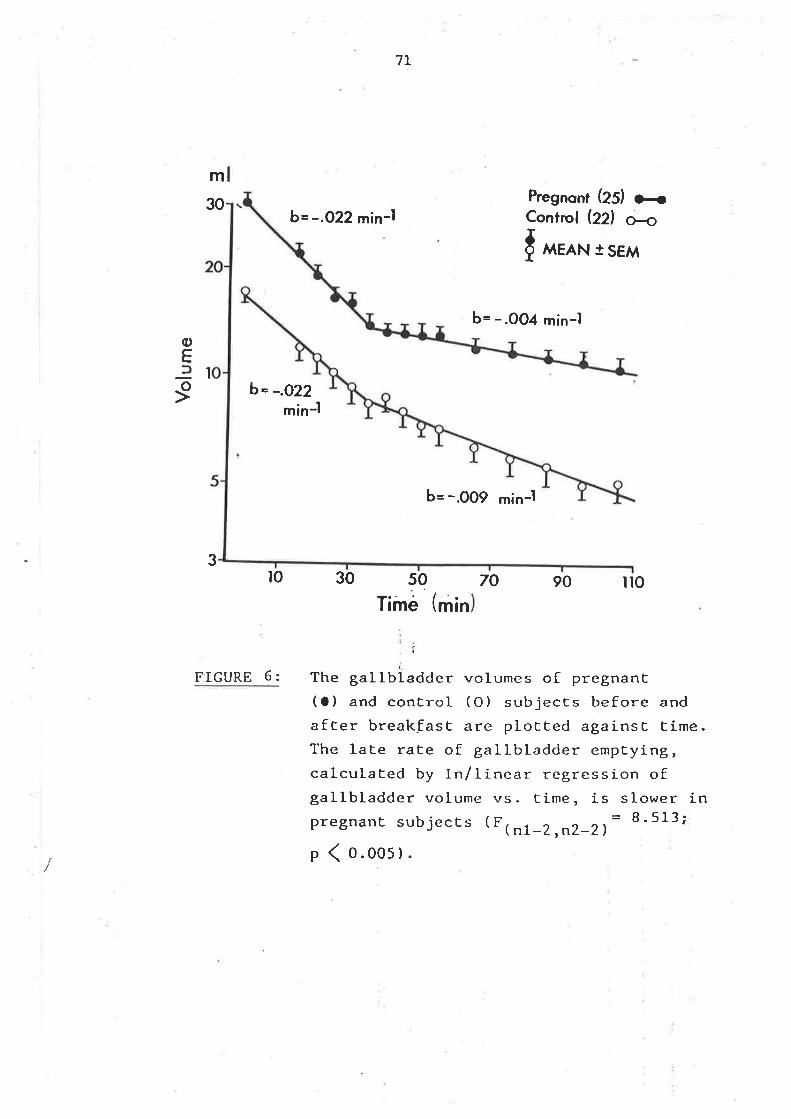
m
30b= -.O22 min-l
7I
50
Time (min
Pregnont (ZS) o<Control (22) æ{ ^^ro*
r sEM
oEtr
9-I
b= -.0O4 min-l
b= -.009 min-l
70 90 ilo
b= -.O22min-l
3to 30
FIGURE 6:
î
The gallbladder volumes of pregnanC(a) and control (O) subjects before andafCer breakEast are plotted againsC Cime.The late rate of gallbladder emptying,calculated by In/linear regression ofgallbladder volume vs. time, is slower inpregnanc sub jecEs ( F ( r,t _Z ,n2_21
B ' 513;
p ( o.oo5).
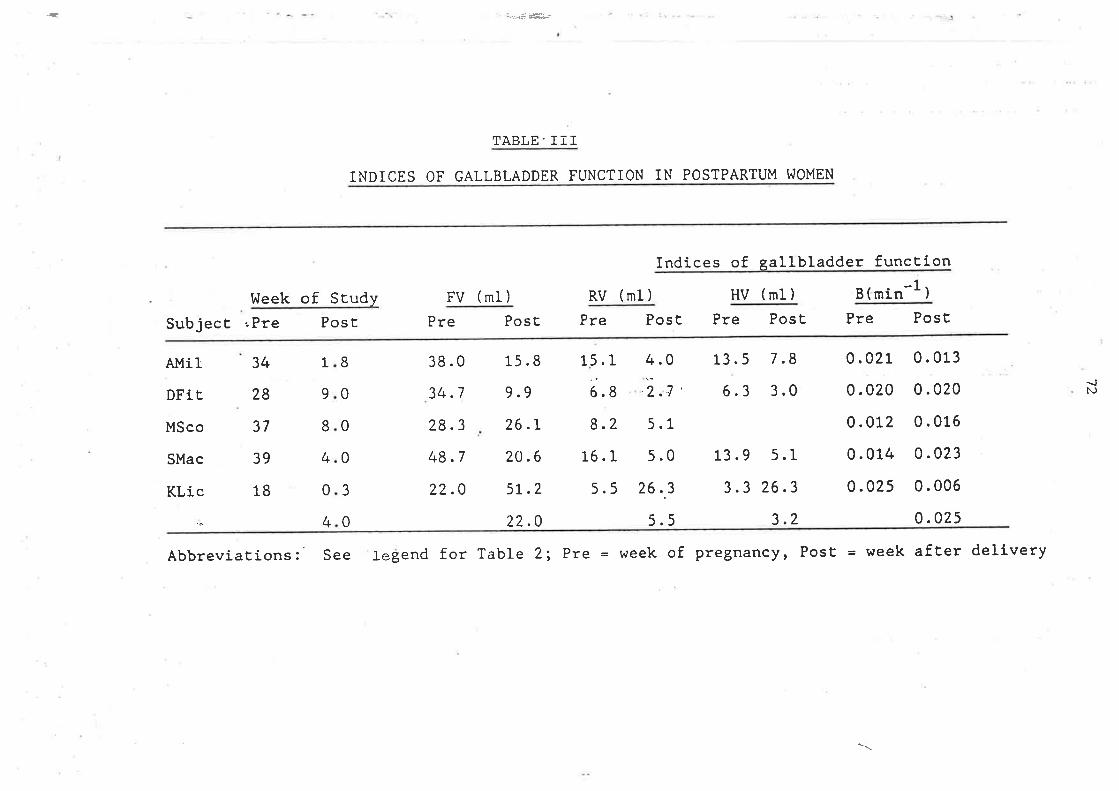
.-
38.0
34.7
28.3
48.7
22.0
15.8
9.9
26.L
20.6
5L.2
22.0
15.1
6.8
8.2
16. I5.5
13.5
6.3
7.8
3.0
0.021
0.020
0.012
0.014
0.025
0.013
0.020
0.016
0.023
0.006
0.025
2.1 '
5.1
5.0
26..3
5.5
ÎABLE' III
INDICES OF GALLBLADDER FUNCTION IN POSTPARTUM I^IOMEN
l.leek of SEudy FV (ml)
SubjecE "Pre Post Pre
Indices of. gallbladder funcEion
RV (ml) HV (ml) B(min-1
PosE Pre Post Pre PosE Pre PosE
)
AMil
DFiC
MSco
SMac
KLic
34
28
37
39
18
8
0
0
0
3
L
9
8
4
0
4
4.0{N
0
13.9 5.1
3.3 26.3
3.2
Abbreviations:' See legend for Table 2; Pre = week of pregnancy, PosE = ldêêk afEer delivery
\
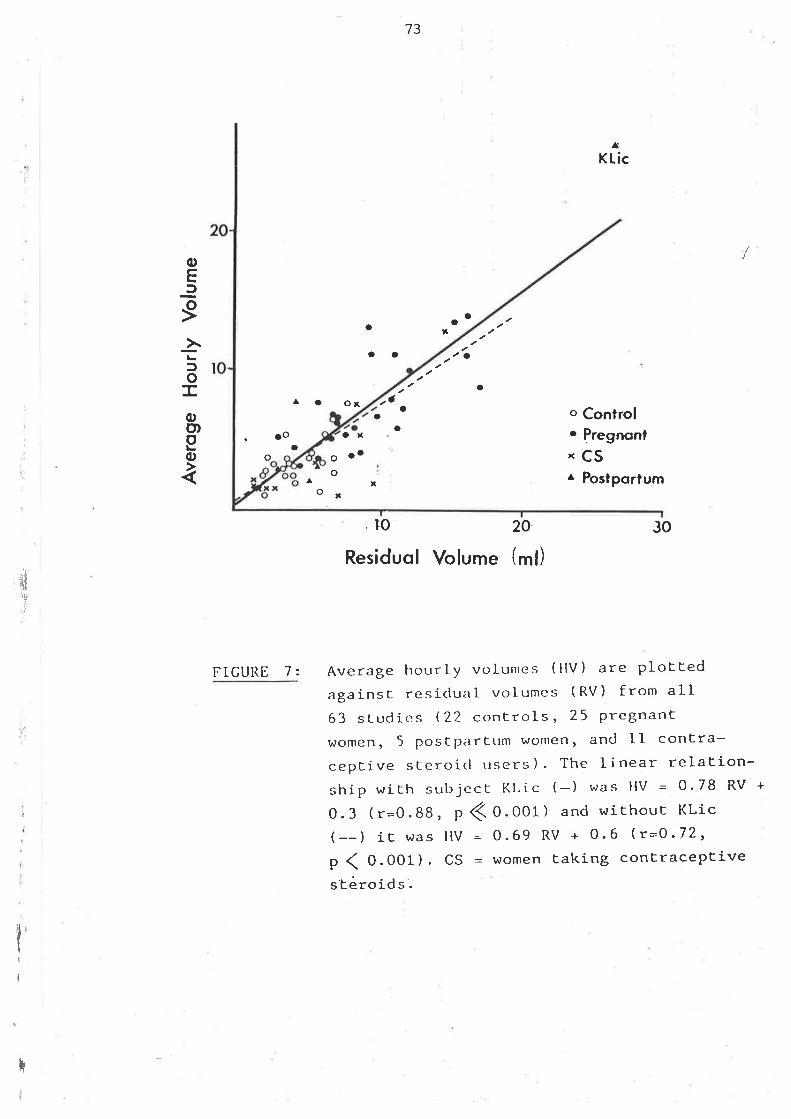
73
oo a
af
o
a
a o ox
ot
^ o
o Control. Pregnonl
'cs^ Postportum
30
AKLic
/oEf
I->loTq,o)o(,
oa
Io
ao
.Ooo
o
FIGURE I z
x
oo
T
oa
. ro 20.
Residuol Volume (ml)
¡d
"u
Average hourly vt¡Iumes ( HV ) are plottedagainsr resiclual volumes (RV) from all63 sLudics (22 controls, 25 Pregnantwomen, 5 postpartum women' and ll contra-ceptive sceroicl users) - The linear relation-ship with sul-rjccI Kl,ic (-) was HV = 0' 78 RV +
0.3 (r=0.88, p < 0-001) and without KLic(--) it eras HV 0.69 RV + 0.6 (r=O'72,
p ( 0.001). CS = rdomên taking contraceptives'Eéro id s'.
I
I
74
with any index of gal-lbladder function-
In alt 63 studies, hourly and residual volumes h/ere sirnilar (Figure 7)
Ttrus, t11e residual volure after the norning nreal- approximated the hourly
vol-ume the remainder of the daY.
B. GALLBI"ADDER. AI\D SMALL INTESTINAL REGUI,ATION OF BILIARY LIPID SECRETION
DI.]RING I}üIRADUODMüAL INFUSION OF STAT\DÀRD A}4INO ACID A}üD LIQUID FORMUI'A
ST]IqULT
(i) Methods
(a) Subjects and Procedures
Five healthy non-obese \^/ornen', aged 2I Lo 28 were each studied twice- After
they fasted overnight, a triple lumen polyvì-nyJ- tube was passed through the
nose and positioned in the duodenum by fluoroscopy with genital shielding
so that the proximal infusion orifice was adjacent to the anpulla of Vater,
12 cm from the distal- coll-ecting orj-fice. Thre third lumen was filled with
mercury frorn proximal to distal orifice and seal-ed at both ends to aid in
fluoroscopic A-ui-dance. After the tube was in position, either a rnixed am-ino
acid solution with 5mg BSPr/IOO ml as marker or li-quid fornml-a with
beta-sj-tosterol as marker was continuously infused through the proximal-
lumen (See Appendix, Tabte Ia). The amino acid sol-ution cont-ained 5?
(wt,/vo1) gJ-ucose and 4 .3% wL/vol of rnixed amino acids (Shaffer and SmaII
Lg77-). Each litre of liquid formula.contaj-ned l.32 g of powdered skinrned
milk, Bl-0 ml- of distil-]ed water, I4O ml- of polycose (Ross Laboratories,
Cofumbus, OH) and 550 ml of corn oil. The rnixture was sonicated with a
sonifier cel-] disrupter (Branson Sonic Power, Plainview NY) for 30 min just
beforc infusion. The resultant uniform emulsion was agitated every 30 min
..L
ili'tli¡
T
li
:1
*
II
I
75
throughout the study. The concentration of beta-sitosterol- in the infusate
\^/as fiìeasured in aliquots taken every hour during the period of infusion and
was constant. Liquid formul-a contains 40% of calories as fat. It has three
tj¡res nrore carbohydrate, tkrree times more calories and is slightly nore
hypertonic than the amino acid solution-
In earlier studies , ]10-20e. of subjects beca¡ne nauseated and vornited during /
infusion of the arnino acid solution, (Kern, Everson, De lt¡lark et aI l9B1).
To ensure paired data, each subject was first studied with arnino acid so
that only those completing the amino acid infusion without incident were
studied with liquid formula. TWo of seven subjects did not conplete the
anr-ino acid study because of nausea and vonr-iting. Thre interval between the
two infusions was 5-l-0h. Duodenaf'bile was continuously aspirated from the
distal orifice at a rate of O.5ml-/rnin and each 30-min sanple was treated
separately. At the bedside, du.nlicate aliquots of each sanple were
extracted with 2:l- chloroform,/nrethanol for phospholipj-d measurenent whil-e
other aliquots were refrigerated at 4 degreesC for analysis of cholesterol,
bile acid and markers. ReaI time sonographs of the gallbJ-adder were
obtained every 30 rnin by using an ADR model 2l3l- real-time scanner with a
33.5m Hz multiplexed linear array transducer, l-3.5cm length(Advanced
Diagnostic Research corp, Terçe, AZ) (See epp,endix). Bl-ood samples for
measurement of human pancreatic pollpeptide were drawn when sonographs were
obtained.
SmaII intestinal transit was nìeasured by the factulose breath test (Bond
and Levitt 1975) (See eppendix). At the 5th h of study J-Og of l-actulose in
t00m1 of water was given as a bol-us through the distal- orifice- Breath
sanples for measurement of hydrogen \^/ere collected before and every 15 rnin
for 4 h after the lactufose was given-
76
(b) Ana1ytì-cal Techniqes
Infusate and each 30 min sanple were analysed for bile acid, phospholipid,
cholesterol- and marker. Bile acid concentration was neasured
spectrofluoronretrically by the enzymatic method of Talalay (Hurlock andI
Talalay 1957), phospholipid colorirnetrically by ttre method of Bartl-ett
(Bartlett 1959) and BSP colori¡retrically (Seligson, Marino, Dodson 1957).
Cholesterol- and beta-sitosterol \¡/ere measured by gas-liquid chromatography
by using coprostanot (5-beta-chol-esterol-3-ol) as internal- standard (Kern'
Eriksson, Curstedt et al 1977). The arnino acid sol-ution contained no
cholesterol- or phospholipid. Li-quid formula contaj-ned chol-esterol (
0.lunrol,/nù) and phospholipid ( !.]unrol/mf ) The cholesterof and phospholipid
concentration of each duodenal sanpJ-e was corrected for infusate
cholesterol and phospholipid (Sée þpendix) .
Based on previous studies (Grundy and trletzger L972, Grundy, Ahrens, Salen
1968) it was assumed that negligible cholesterol- and beta-sitosterol
absorption occurred over the l-2crn perfused segment of bowel.
Gallbladder volume was measured from each gallbladder sonograph (see
append.ix). Serum human pancreatj-c polypeptide (HPP) level was deternrined
by radioinrmrnoassay (see appendix) .
Srnall- bowel- transit tirne was defíned as the time of rise in breath hydrogen
concentration fron base line' (see appendix). In each ex¡rerJrnent, this was
subjectively evaluated by eight observers blinded to the resul-ts of
galJ-bladder enptying and biliary lipid secretion. Transit tirne was
deterrnined fron the appearance of the plot of hydrogen concentration (parts
per rniJ-lion) Vs, tilrie, and re¡rorted as the nrea¡r (+/- SD) of these eight
77
estimations
(c) Analysj-s of data
Differences in gallbladder enptying, small bowel transit tjme serum levels
of human pancreatic poJ-lpeptide, mean bil-iary lj-pid secretion rates and
mean molar percent cholesterol during the two infusions were analysed by
paired t tests. Data frorn afl five subjects were included in all
statistical analyses. Biliarlz lipid secretory relationships during each
infusion were evaluated by linear and non-linear regression analysis;
linear; y:ax + b; non-l-inear; y = x/(b + ax), talhere y and x are hourì-y
lipid secretory rates and a and b are constants-
Investigators have usualÌy ignored biliary lipid oqtput during the first 4
h of study, because of its fluctuations and have calculated secretion rates
only after this period. Accordingly the results of this study were divided
into the first 4 and last 6 h.
RESULTS
(a) Biliary Iipid Secretion
With both infusions, secretion rates were fower in the l-ast 6 h than in the
first 4 h due to the high secretion rates in the first 2 h after initiating
gallbladder contraction. During both the first 4 and last 6 h of study, the
mean hourly secretion rates of bile acid, phospholipid and cholesterol
showed considerable variability but were greater during the liquid formula
than during the arnino acid infusion (Table 4) -
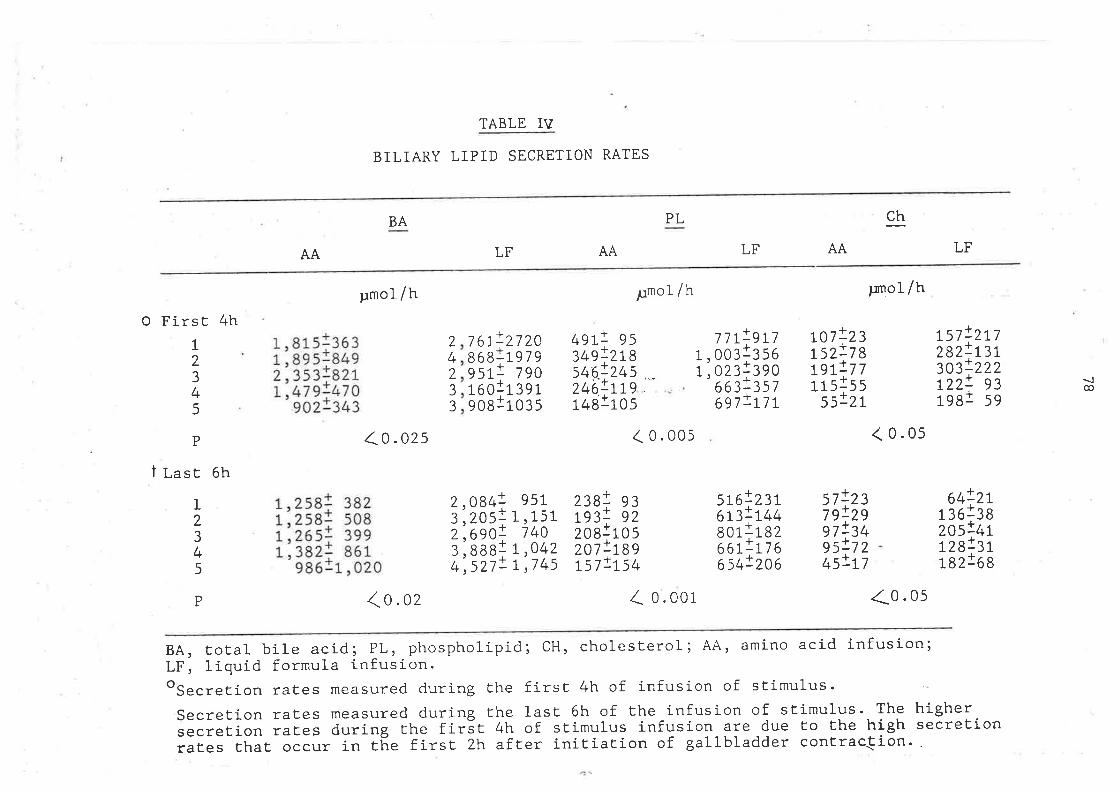
TABLE IV
BILIARY LIPID SECRETION RATES
BA
LF AA
ch
O First 4h
AA
t,81S*¡O¡1,895+8492,353+82tL,479:470
902=343
pmol /h
1o.ozs
1o.oz
7 6L!27 ZA868119799511 7gO1601139190811035
4gL! 9534s!2L8546.!245 .._
246!rL9r+alros
LF
lltlgn1. oo¡1¡sor, oz¡l¡go
6æ=357ogtlu t
576!nt6ß!L¿+4aor-1r azoatlu o654!206
PL
¡¡mol /h
( 0.00s
Z- o. oor
AA
ß7!23ßz!7 8rgtlt trrslss
sslzt
stlzstglzgw!z+r95:7 2+sltl
¡:rnof /h
< 0.0s
LF
L57282303t22198
L2345
P
j++
it
24233
zt7131222
9359
{@
t Last 6h
I2345
t,zsaI 382L,258+ 50St,zø5i 399L,382: 861
gg0rt ,020
2,0843,2052,6903,8884,527
95L1,151
71+0t,042L,745
z¡B! e3rg:1 s2zogjros207!ßsrsllts+
1tJ11
oqlzt1 36j38zos!¿rtrzaJ¡r-razlo g
P <0 .0s
BA, total bile acid; PL, phospholipid; CH, cholesterol; AA, amino acid infusion;LF, liquid formula infusion.osecretion rates measured during the firsf 4h of infusion of stimulus
Secretion rates measured during the last 6h of the infusion of stimulus. The higher.secretio' raiås during the firãt 4h of. stimulus infusion are due to the high secretionrates that occur in tñe first Zlt af.ter initiation of gallbladder contrac{ion..
t9h
The rates of bile acid and phospholipid secretion were increased more than
that of chol-esterol during liquid formul-a infusion, resulting in a lower
nrolar percent cholesterot than during the arnino acid infusion in four of
five subjects during the first 4h (p ç 0.05) and in all subjects during the
l_ast 6h (p < 0.05) (Figure B). The increments in chol-esterol secretion
coi-ncident with increments in either bile acid or phospholipid secretion
were far smaller during liquid formula infusion (Figure 9 A{). For these
reasons, biliarlz lipid secretory rel-ationships were quite different with
the two infusj-ons. More chol-esterol was secreted ¡rer nr-icrorole bile acid or
phospholipid during the arn-ino acid infusion. Ttre best fit of the conrbined
data (both arnino acid and liquid formula for chol-esterol vs. bile acid,
cholesterol vs. phospholipid or phospholipid vs bil-e acid) was the equation
for a rectangular hlperbola, y:x/, (b + ax) (TabÌe 5). However as bile acid
secretion rate increased there was considerable divergence of cholesterol
and phospholipid secretion, CH Sec-max : 298 and PL Sec : 5555 (Tab1e 5) '
As bile acj-d secretion increased t-here was little change in the ratio of
phospholipì-d to bile acid but the ratio of cholesterol to bile acid
decreased considerablY.
(b) Gallbladder HnPtYing
In each subject galJ-bladder enptying was more compl-ete with liquid formula
infusion during both the first 4 (p.<0.05) and Iast 6h (p<0.02) (Figure
l0). Gallbl-adder volumes cluring amìno acid infusion fluctuated considerably
and there were periods of apparent refilling. On the other hand, during
liquid fornml-a infusion gallb.Iadder emptying \'\ras pronrpt and more complete'
and showed li-ttl-e fluctuation (Figure tl)
In atl- studies including both amino acid and l-iquid formula infusions,
there were 23 periocls, exclurlìng tle initial hour in wh'ich gallbladder
/
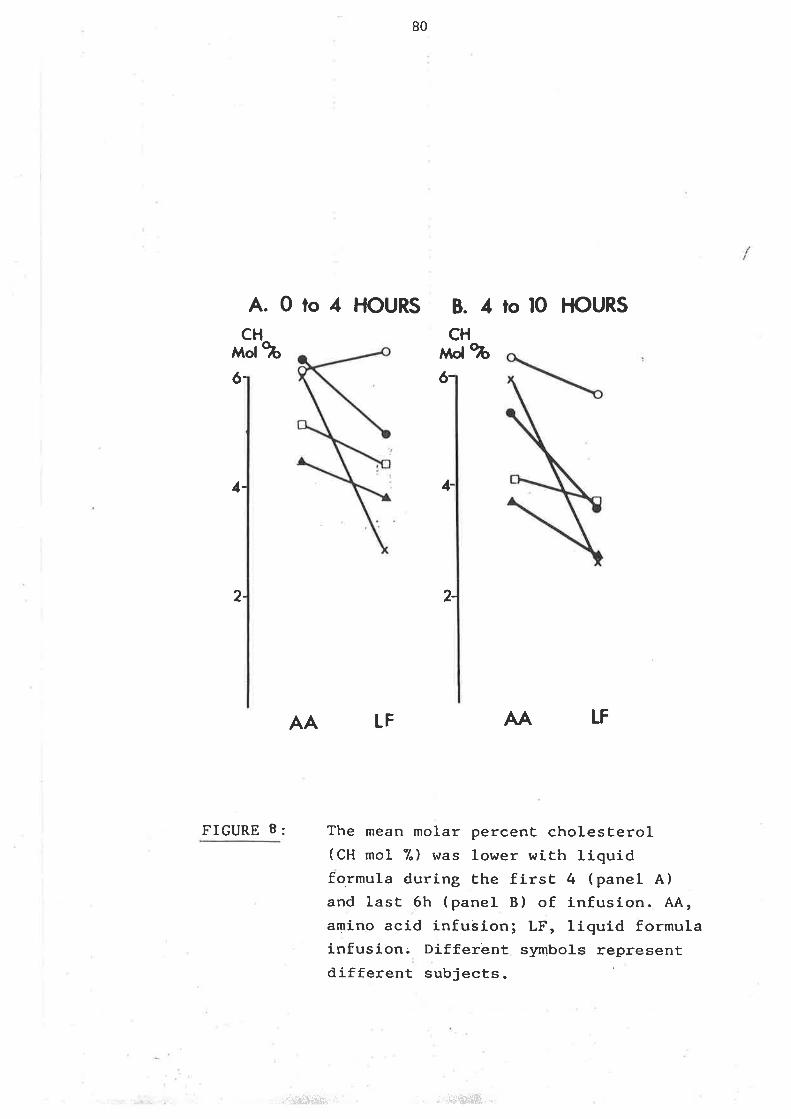
80
A. 0 to 4 HOURS B. 4 ro l0 I-IOURS
CHMd 9b
1-
2-
rrcung B:
6-
CH,$d %ó-
2-
AA LF AA I-f
The mean molar percenE cholesterol(CH mol %) hras lower with li-quidformula during Ehe firsE 4 (panel A)and last 6h (panel B) of infusion. AA,amino acid infusion; LF, liquid formulainfusion; Different slrmbols representdj-fferent subjects
1-
..,,.i$iï$!,i , . ,&?&ff[fi..
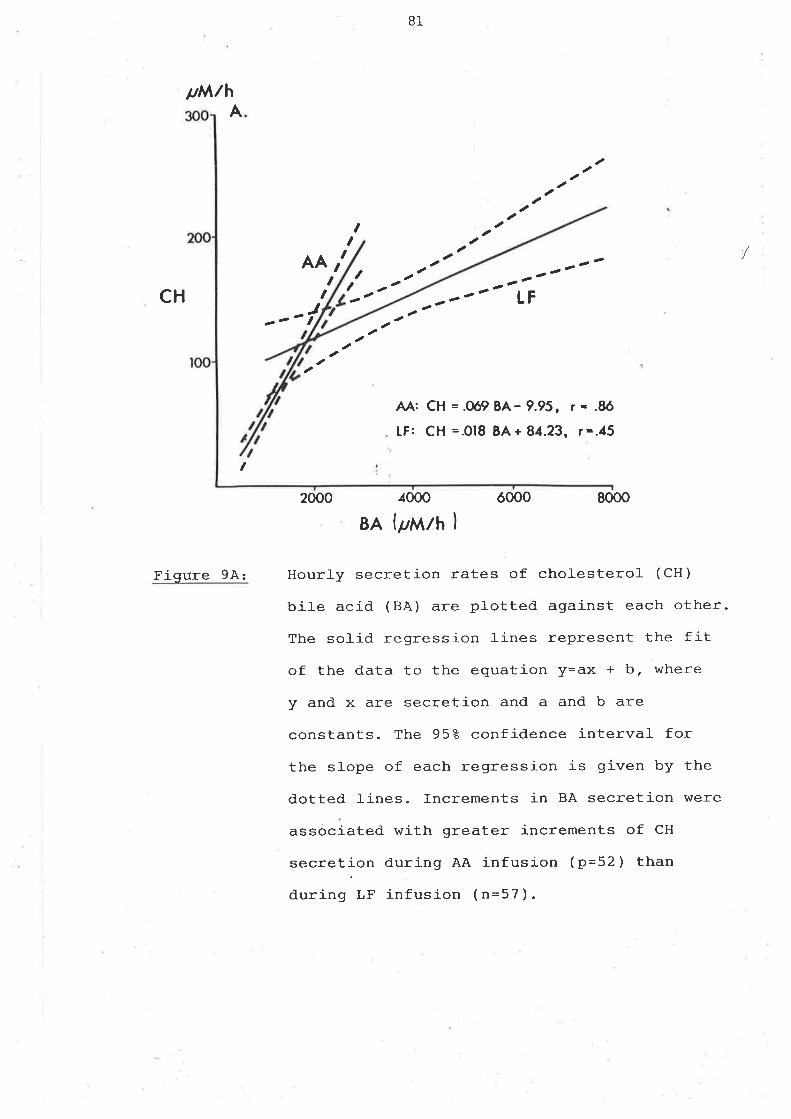
B1
pM/hA
I ,t tt
,,I ,-
,
ld: Çfl =.Oó9 BA- 9.95, r - .8ó
LF: CH =.018 BA + 84.23 , t -.15
8000
AAr---.-t2"1'
IFCH J
I
2000 4000 óooo
BA {¡¡Mlh I
Figure 9A: Hourly secretion rates of
biLe acid (BA) are plotted
The sol-id regression l-ines
of the data to the equation
y and x are secretion and a
chofesterol (CH)
against each other.
represent the fit
y=ax + b, where
and b are
constants- The 952 confidence interval for
the slope of each regression is given by the
dotted lines. Increments in BA secretion were
associated with greater increments of CH
secretion during AA infusion (p=52) than
during LF infusion (n=57).
/
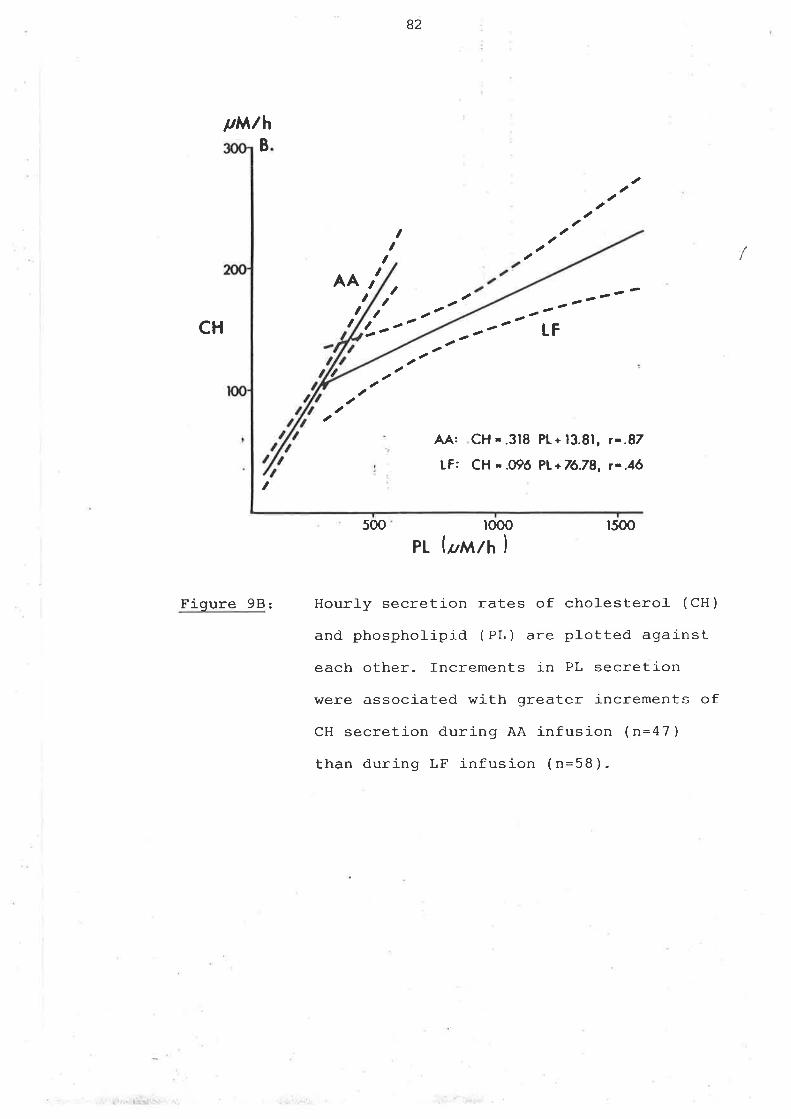
82
ttw/hB
CH
t
Figure 98:
ftI
AAt,t , t
It I, _----e
ê
tF
aa
aa
taaÀÀ:
LF:
CH -.318 PL+ 13.81, ¡-.87
CH - .09ó PL+76.78, r-.16
500 r000 r500
PL lpwth I
Hourly secretion rates of cholesterol- (CH)
and phosphoJ-ipid ( PL ) are plotted against
each other. Increments in PL secretion
were associated with greater increments of
CH secretion during AA infusion (n=47)
than during LF infusion ( n=58 ).
/
r'1 .. ti..*i j-:
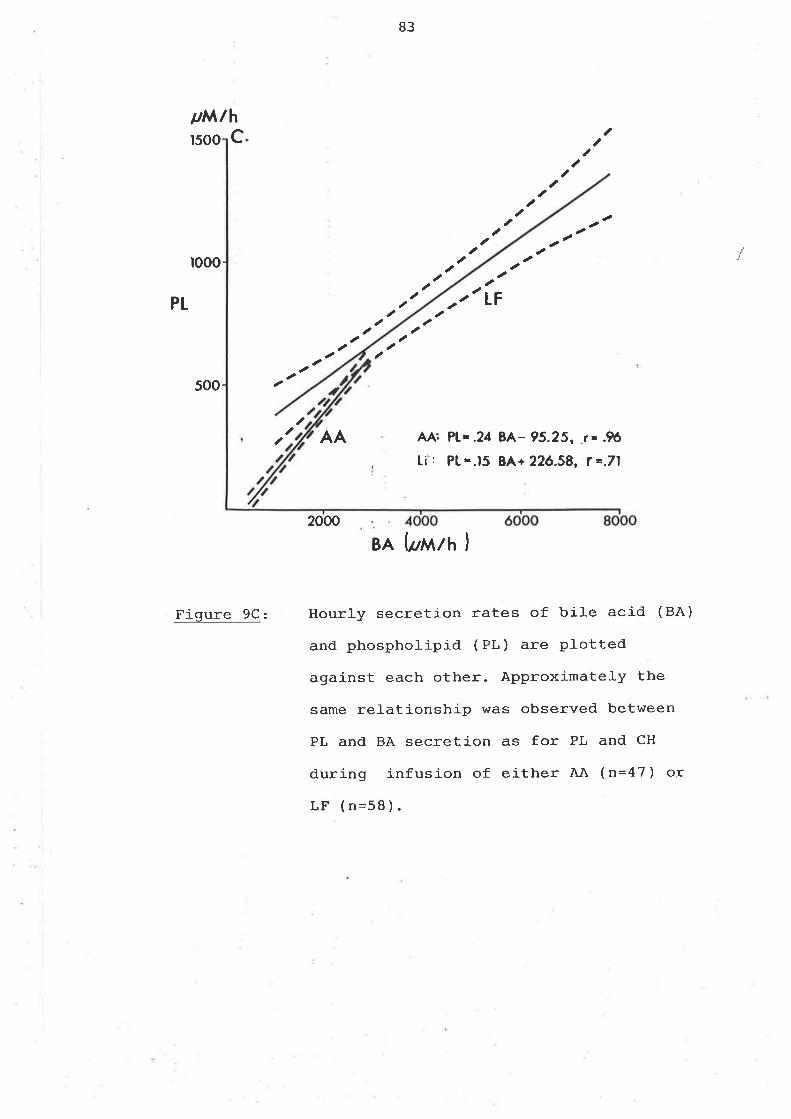
trM.lhrsoo c
rooo
B3
a
aa
aa aa aaa a tF
AA: P[- .21 gA- 95.25,,r-.fö[i-: P[-.15 BA+ 22ó.58, Í =.71
2000
BA (øMlh )
Hour1y secretion rates of bile acid (BÀ)
and phospholipid ( PL ) are Plotted
against each other. Approximately the
same relationship was observed between
PL and BÀ secretion as for PL and CH
during infusion of either AA (n=47) or
LF (n=58 ).
a
a
a
a
,aa
aaaa
aa 1
Pt aa
a
u
aaa,
soo
a
AA,a
t
Fiqure 9C:
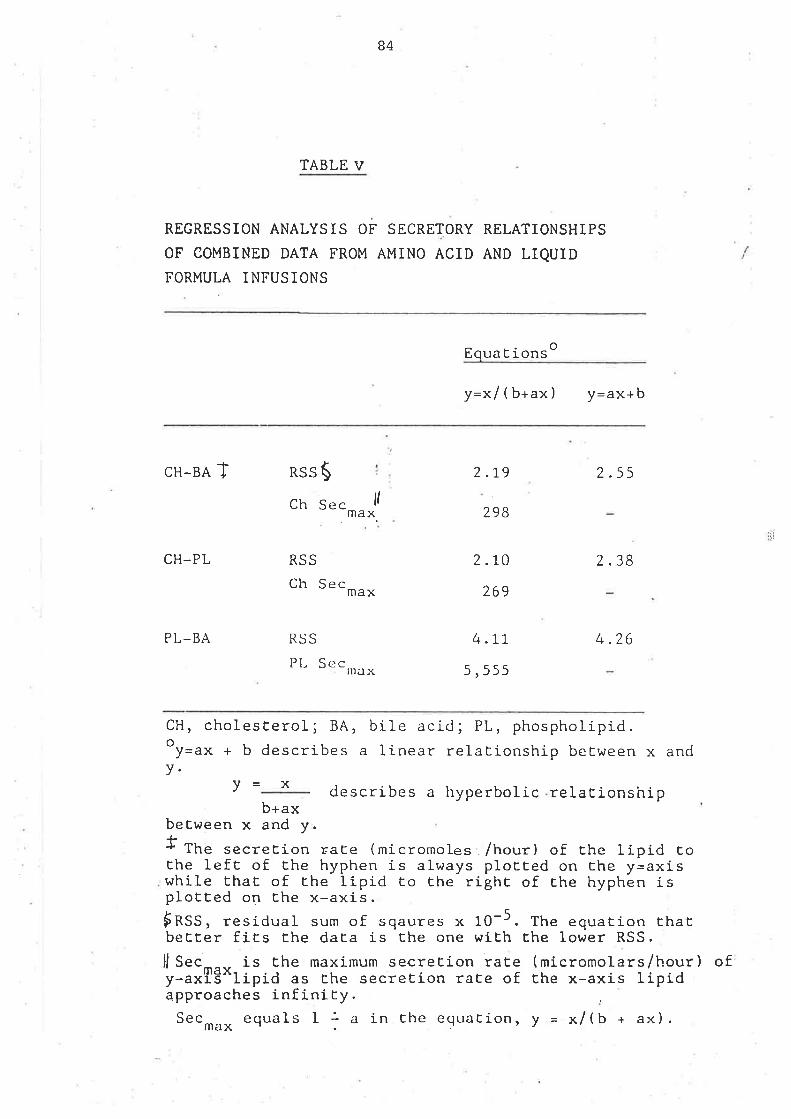
B4
TABLE V
REGRESSION ANALYSIS OF SECRETORY RELATIONSHIPS
OF COMBINED DATA FROM AMINO ACID AND LIQUIDFORMULA INFUSIONS
oLqua C rons
y=xl(b+ax) y=.**b
CH-BA T RSS$ 2.19
298
2.ro
269
4.77
5,555
2.55
2.38
4.26
CH_PL
PL-BA
ch Sec llmax
RSS
Ch Sec max
RSS
PI- Secnì¿t x
CH, cholesEerol; BA, bile acid; PL, phospholipid.oy="* + b describes a linear relationship beEween x andv.
v describes a hyperbolic relaEionshipb+ax
between x and y.f fh" secretion raEe (micromoles /hour) of Ehe Iipid toEhe left of the hyphen is always plotted on che y=axiswhile thaL of the lipid t.o Ehe righE of Ehe hyphen isploEted on Ehe x-axis.$nSS, residual sum of sqaures x 10-5. The equation EhaEbeEEer fics the daEa is the one wiEh Ehe lower RSS.
Jl Sec-^., is Ehe maximum secreEion raEe (micromolars/hour) ofy-axis'^lipid as the secreEion ra[e of Ehe x-axis lipidapproaches infinity.Sec---- equals I : a in the equation, y = x/(b + ax).max'.
x
ti
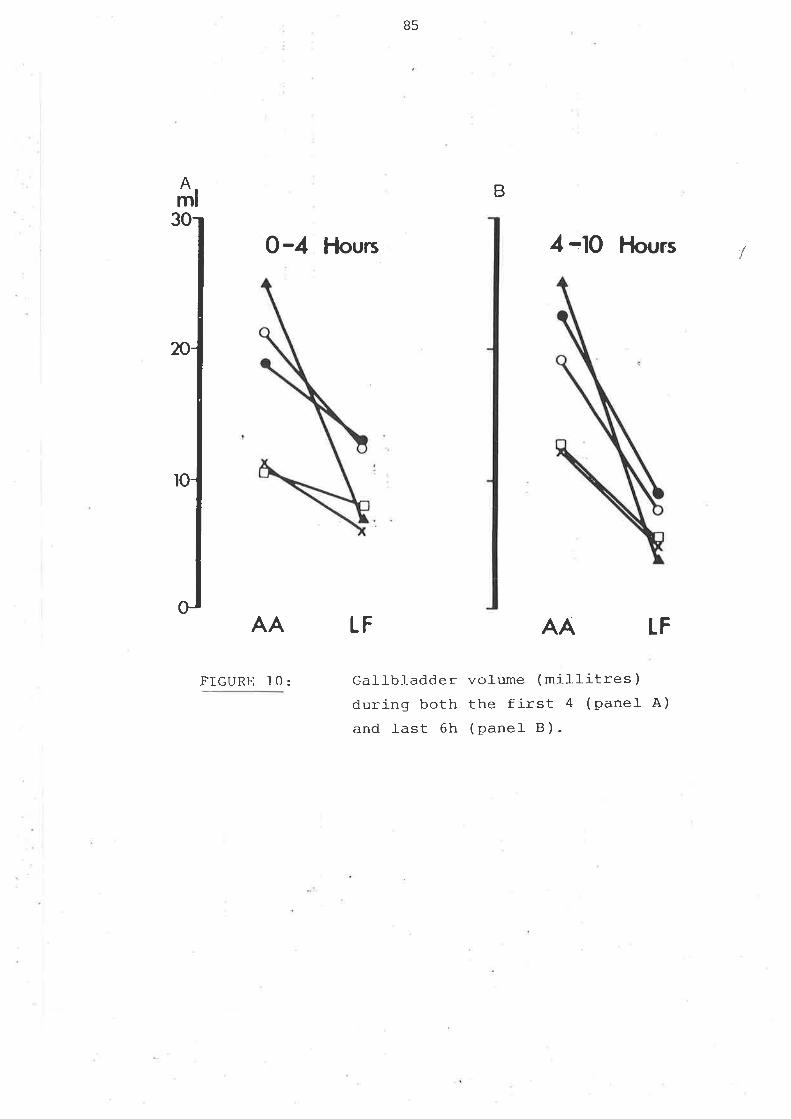
85
Aml B
O-4 Hours
AA LF
4 -lO Hours 1
LF
Gallb1adder volume (millitres)during both the first 4 (Pane]- A)
and last 6h (panel B).
AA
¡IGURE 10:
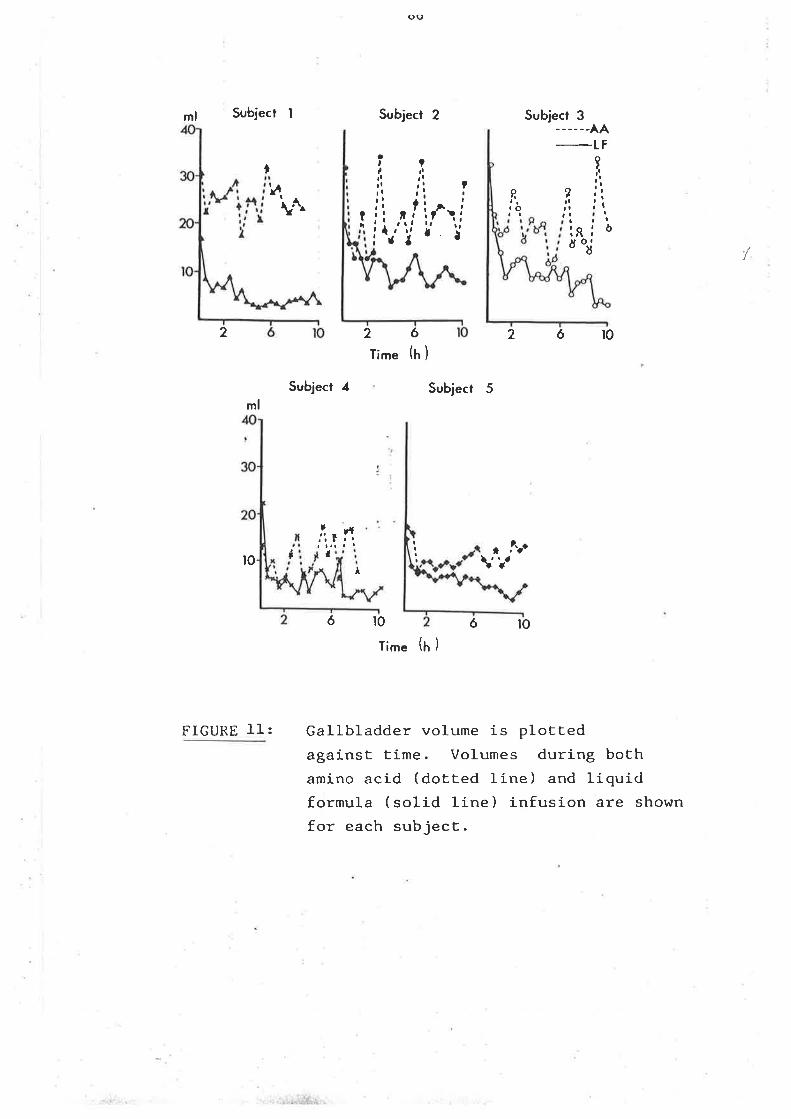
O()
ml Subject I
ml
¡0 I
FIGURE ]-I:
Subject 2
26Time (t' )
Subject 3_-__--AA
-tFt îç,r.i: j: ?¡l ¡ ! r
li ,q,lif.,ii{.,i | ¿
?¡i¡lri?
,¡,a,.
î,oI
òaa.o I
öoJ
þ\^^ ?
ai
2 2ór0
Subject 4 Subject 5
,t¡'¡
6t0 6loTime (¡ )
Gallbladder volume is plottedagainst time. Volumes during bothamino acid (dotted line) and liquidformula (solid line) infusion are shown
for each subject.
rft.'ì f I
¡I l'r't
/
-.¡:j;¡ii.r.:,
87
enptying \,\¡as 5ml or greater. During 22 of these periods there hlas a
concornitant increase in bil-e acid output.
(c) Small Bowel Transit Tinre
In four of five subjects, sma1l bowel- transit tjme was slower ù:ri-ng arnino
acid infusion (Tabl-e 6).
(d) Human Senrm Pancreatic PoJ-lzpeptide
fn four of five subjets levels of pancreatic polypeptide were two to
threefold hi-gher during both the first 4 and l-ast 6 h with liquid formula
infusion (Tabfe 7). Subject 5 had no change in pancreatic polypeptide
Ievels from basel-ine with either infusion. Nonethefess, this subject had
findings which were sjrnilar to. tþe rest of the group: increased gallbladder
enptying, faster intestinal- transit and increased bile acid secretion in
response to liquid formula. In the other subjects, the pattern of the
pancreatic polypeptide response was that of a sustained elevation from base
line with minimal fluctuations.
C. TTIE EFFECTS OF CHRONIC OESTROGH\ ADMINISTR¡IIION ON B]LIARY LIPIDS,BILE
ACIDS AI\TD GALLBIÄDDM. FUNCIION ]N POST-ME}JOPAUSAL h]OMEN
(i) Methods:
/
(a) Subjects
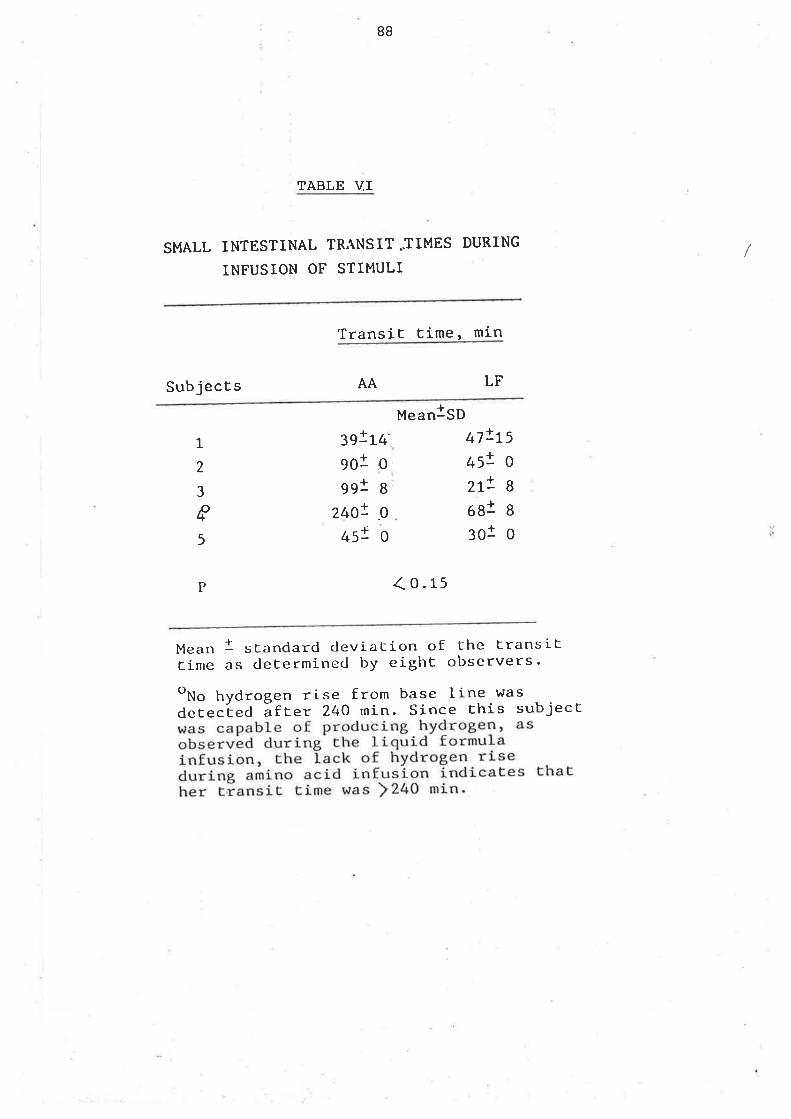
BB
TABLE VI
SMALL INTESTINAL TRANSIT JIMES DURING
INFUSION OF STIMULI
Transit time, min
Subjects AA LF
Mean!SD
1
2
3
Y!Y+9ol o991 8
240! gI45! 0
47!L545! 0
2t! 8
68J B
3ot oI5
P (o.r:
Mean l standarcl cleviation of che transittime as cle[ermined by eight observers'oNo hydtogen rise from base line was
derected ãfc". 240 min. Since this subject
1
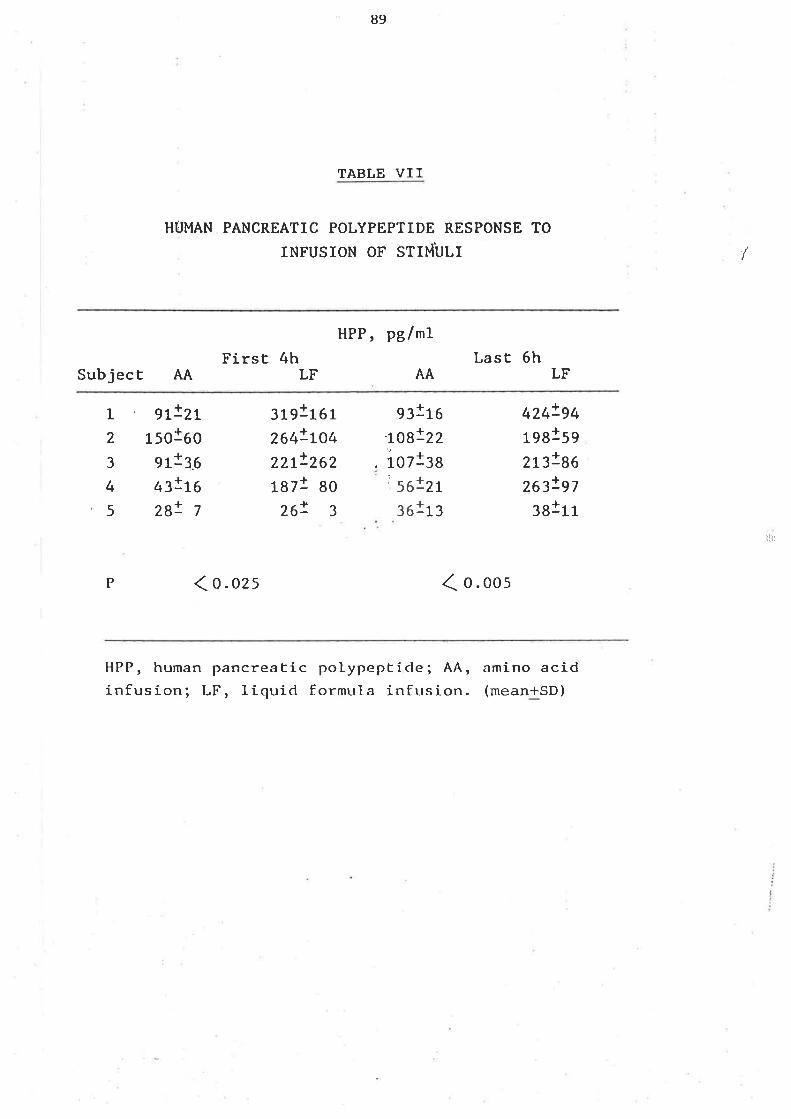
89
TABLE VII
HTJMAN PANCREATIC POLYPEPTIDE RESPONSE TO
INFUSION OF STIMULI /
HPP, pBlmlFirst 4h LasÈ 6h
SubjecE AA LF AA LF
1 g]^lzr
2 1501603191161264!LO422t!2621871 80
26! 3
g¡1ro-LO8!22
iozl:s2r13
424!94198159
2ß!86zæ!97:ajrr
3
4
5
91136
$!ßzB! 7
t 56!361
rlir
P ( o. ozs ( o. oos
HPP, human pancreatic polypepticle; AA,infusion; LF, liquid formula inft¡sion.
amino acid(mean+SD)
90
Nine post nenopausal wonten, aged 28-47 were studied off and on Premarl¡(Ayerst)
They had been taking conjugated equine oestrogens for at least 4 weeks
(nrean dose l-.39 mg dail-y) but no other drugs. To ensr:re paired data each
subject was first studied at the end of four weeks oestrogen abstínence and
again after six weeks of oestrogen intake.
(b) Gallbladder concentration and enptying after fV CCK
On day I of the study a triple l-u¡nen tube was positioned by fluoroscopy
after an overnight fast. The proximal- infusion orifice was adjacent to the
anpulla of vater, 12 cm from the distal- orifice. After the tube was
positioned, distill-ed water with the nondiffusable marker BSP (5 mgrlnù) was
infused at a rate of 3-4 mlrlnin. Duodenal bite drained continously by
gravity frorn the distat orifice: The gallbladder was stimulated to contract
by continuous fV CCK-B infusion .(.02 ug/kg/h) over 90 rnin and gallbladder
bile was aspirated for cholesterol saturation index, bile acid distribution
by GLC and cumul-atlve bil-irubin output. Sj-multaneously, the arnount of bil-e
oçelJ-ed and the rate of gallbladder errptying vüas estimated by reat time
ultrasound. Five min sanples of bile were coll-ected for 90 rnin. Aliquots
were taken frorn vortexed samples and the residual bile was retr:rned to the
duodenum.
(c) Analytical- Techniques
Each 5 rnin sanple was analysed for bilirubin by the method of Rand and Di
Pasqua (L962).
The concentration of bilirubin in gallbladder bite was determined as
follows.
by
91
The 5 rnin collections of duodenal bile are anal-ysed for bilirubin output
bili (nqlsnù ¡ = (B)Dx (M)I x R
(M)D
where (M) D= duodenal marker concentration (B) D = duodenal bil-irubin
concentration, (tq)I : infused marker concentration R= mLs markers solutions
infused over 5 min. Since gallbtadder enptying follows a first order decay
fimction,the cumulatj-ve exponential function Bt : ç(l-e-b(t-t.I,) ) describes
the output of galJ-bladder bil-irubin into the duodenum, where Þcumulative
rnilligrams of bilirubin put out at tjrne t, TL time tag in billirubin
output, C:total mitlì-grams of bilirubin enpti-ed, and b=the rate constant at
which galJ-bladder contents enter the duodenum (when galJ-bJ-adder errptying is
conplete b: the rate constant of gallbtadder enrptying). Ttre linear
parameter, C and the two non-l-inear parameters, b and TL are estjmated frorn
conputer analysis of the plot of cumul-ative bil-irubin output versus time.
Since the amount of bilirubin ejected from the gall-bladder, C and the
volume (VE) of bile ejected from the gallbl-adder can be calcul-ated one can
estimate the concentration of gallbladder bilirubin (B) GB by calculating
(B) GB = CNE
(d) Biliary Lipid Secretion
Liquid formul-a (see appendix) was infused following 90 rnin of the IV CCK-B
stimulus. The formul-a was infused over B h through the proximal port with
beta-sitosterol as a marker. Duodenal bile was continuously aspi-rated from
the distal- orifice at a rate of 0 - 5 ml-rzrnin and each 30 rnin sanple was
analysed for biliarlz lipids. (see alTerrlix) Real tinre sonograhs of the
gal-lbladder were obtained every 30 min and vol-unres nìeasured (see
/
i)
92
appendix).
On day 3 another sanple of gallbladder bile was col-lected for lithogenic
index deterrnined by the nethod of Hegardt and Dam(1971) and Ho1zbach,
Marsh, Oleszewski et al(1973).
(e) BiIe Acids
A sanple of bil-e obtained after gal-lbladder stimulation by CCK-B was added
to nethanol and 4N NaOH with 5-beta cholanic acid as an internal- standard
and hydroì-yzed. The bile acids were then extracted, methylated with
diazonrethane (Back, Sjovalì-, Sjovall 1974) or with dinrethoxlpropane (Ali
and Javitt 1970) and trimethylsilyl or acetate derivatives (Makita and
Wel-l-s 1963, Roovers, Evrard, Vanderhactlrelg68) were prepared. GIÆ was
performed on 6ft glass columns aL 220 degrees C with 18 HiEff BBP (Applied
Science Laboratories, Inc., State College, Pa. ) on IO0/L20 mesh gas chrom Q
with helium as the carrier gas at 30 ml/min (Kern, Eriksson, Curstedt et al
L971).
(f) CattUladder volume and enptying with standard rneals
On day 5 of the study gallbladder storage and ernptying throughout the day
and night \^/as measured sonographically during ingestion cf 3 standard meals
(as described previously) .
(S) anafysis of data;
Data are expressed as rean +/- SD. Differences betr,r¡een control and
treatment periods were evaluated by the Wilcoxon signed rank test.
/
93
(ii) RESULTS:
(a) Gallbladder enptying
Tabte 8 shows the neasurenents of galJ-bladder vol-ume and enptying. Ttrere
was rapid gallbladder enptying over the first 30 min of the CCK-B infusion
but no significant differences occurred between the on and off oestrogen
periods. Slower changes in galJ-bladder volume v/ere seen after a ¡nixed
solid-Iiguid meal, but there \^/ere no significant changes in enptying rates,
fasting, residual or hourly vofumes witJ: chronì-c oestrogen ingestion.
(b) callbladder concentration
There h/as no apparent effect of oestrogens on bilirubin in gallbladder biLe
(Figure. l.'2).
(c) Biliarlz J-ipid secretion
The mean lithogenic indices of gallbladder bile in the on and off oestrogen
periods were sjrnilar (FiWre 13). There \^/ere no significant effects of
oestrogen on the mean hourì-y secretj-on rate of any biliary lipid (Fig'ure
14).
(d) Bile acids \^¡ere assessed by GLC for distribution of cholic acid,
chenodeoxycholic acid and deoxycholic acid. Tkre small anrounts of secondarlz
bite acids (5 to 12å) were disregarded in calculating percentages of the
major bile acids. There \^/ere no changes in the bile acid distribution
associated with the use of oestrogens.
ü1t
J
I
r
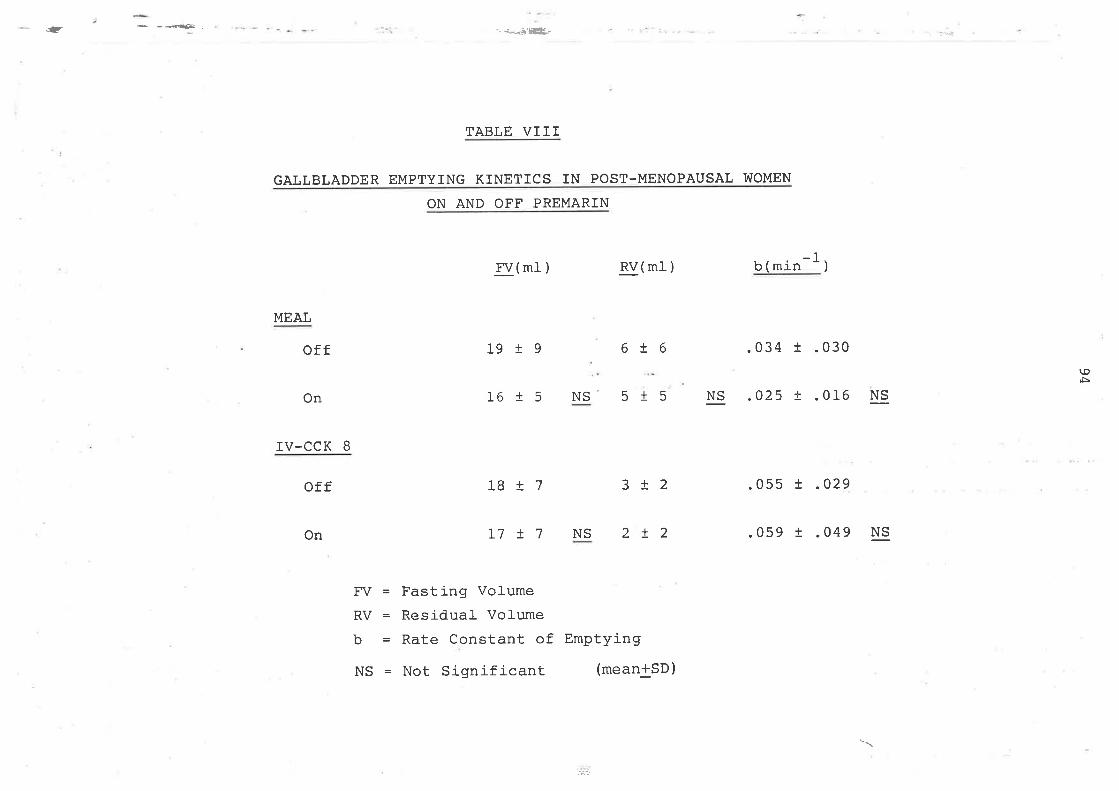
.- + _4€Ê- j*Æ'ËL-
I7!7 NS 2!2 .059 t .049 NS
GAL
MEAL
off
IV-CCK 8
off
TABLE VIII
LBLADDER EMPTYING KINETICS IN POST-MENOPAUSAL V'IOMEN
ON AND OFF PREMARIN
FV(ml- ) RV(mI )-'lb(min')
19 19 6!6 .034 t .030
16 1 5 NS' 5 t 5 NS .O25 t .016 NS
18t7 3i2 .055 ! .029
tgÈ
On
On
FV = Fasting Volume
RV = Residual Volume
b = Rate Constant of Emptying
NS = Not Significant (mean+SD)
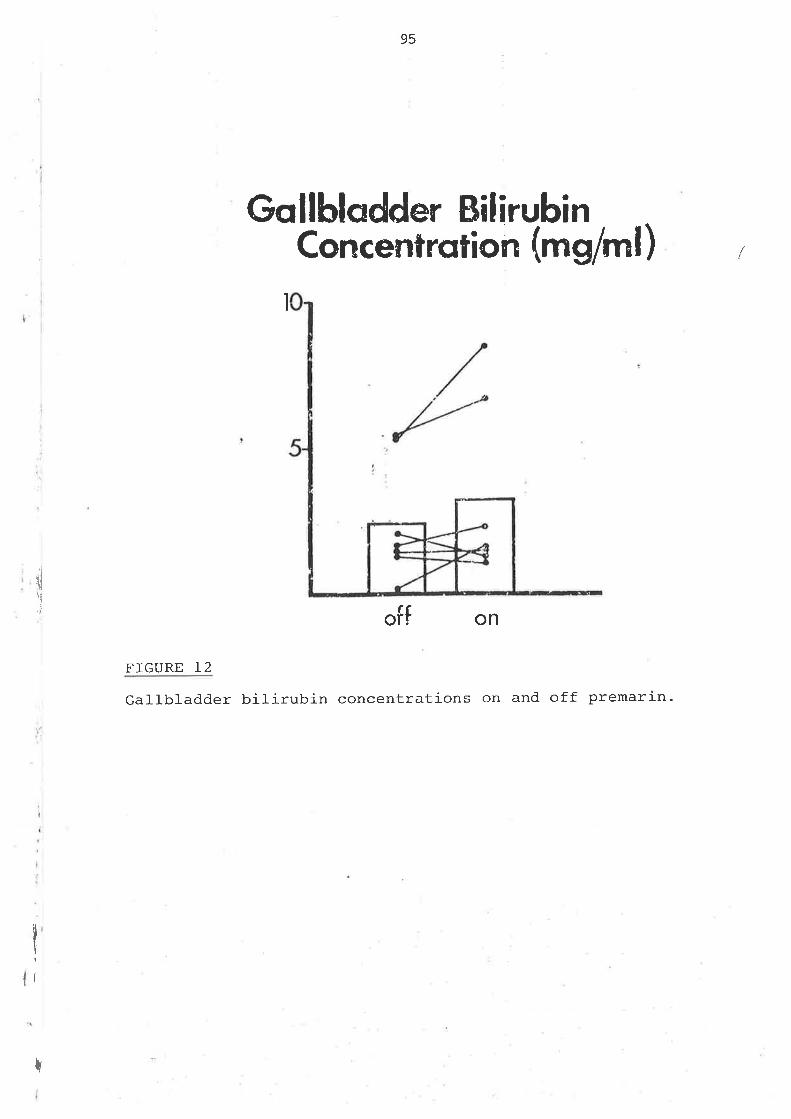
95
Gollbladder BilirubinConcentrqtion (mg/ml)
ì
i
dï.i offon
FIGURE L2
Gal-Ibladder biLirubin concentrations on and off premarin.
I
r
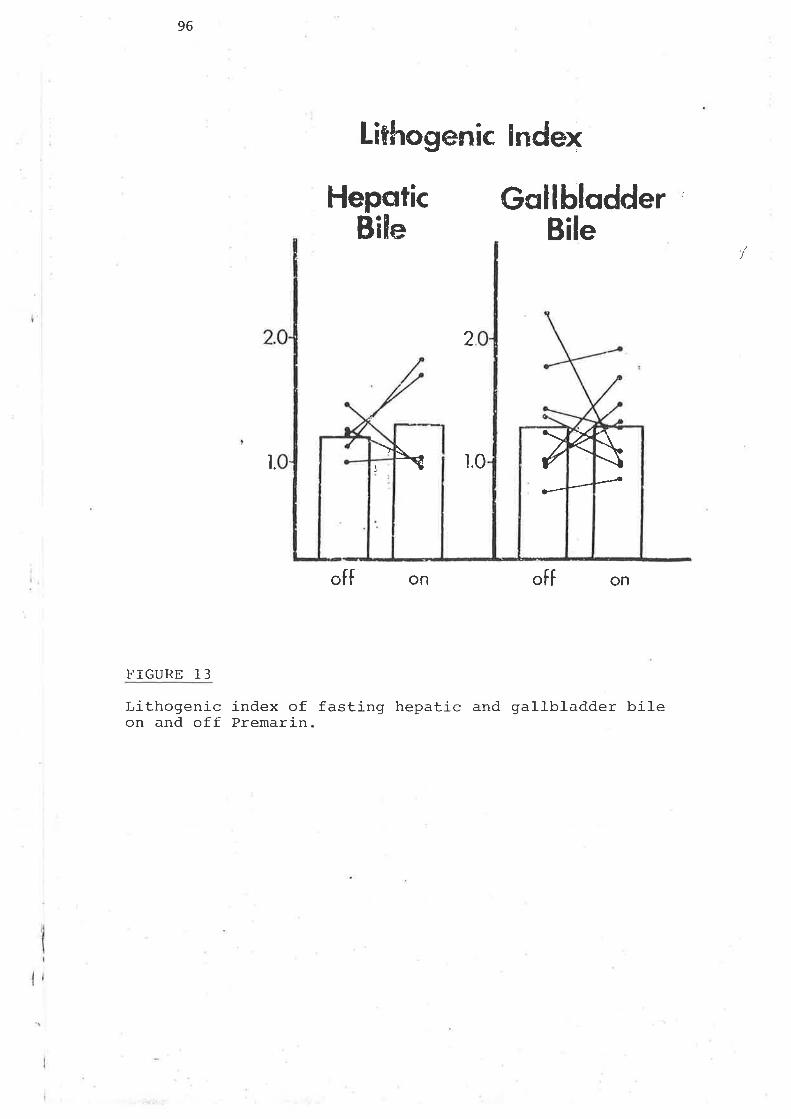
96
Lithogenic lndex
HepaticBile
Gqllblqdder :
Bile
offon
7
2
l. ì.0
off on
FIGURE 13
Lithogenic index of fasting hepatic and gallbl-adder bileon and off Premarin.
\\--â
7-
ç
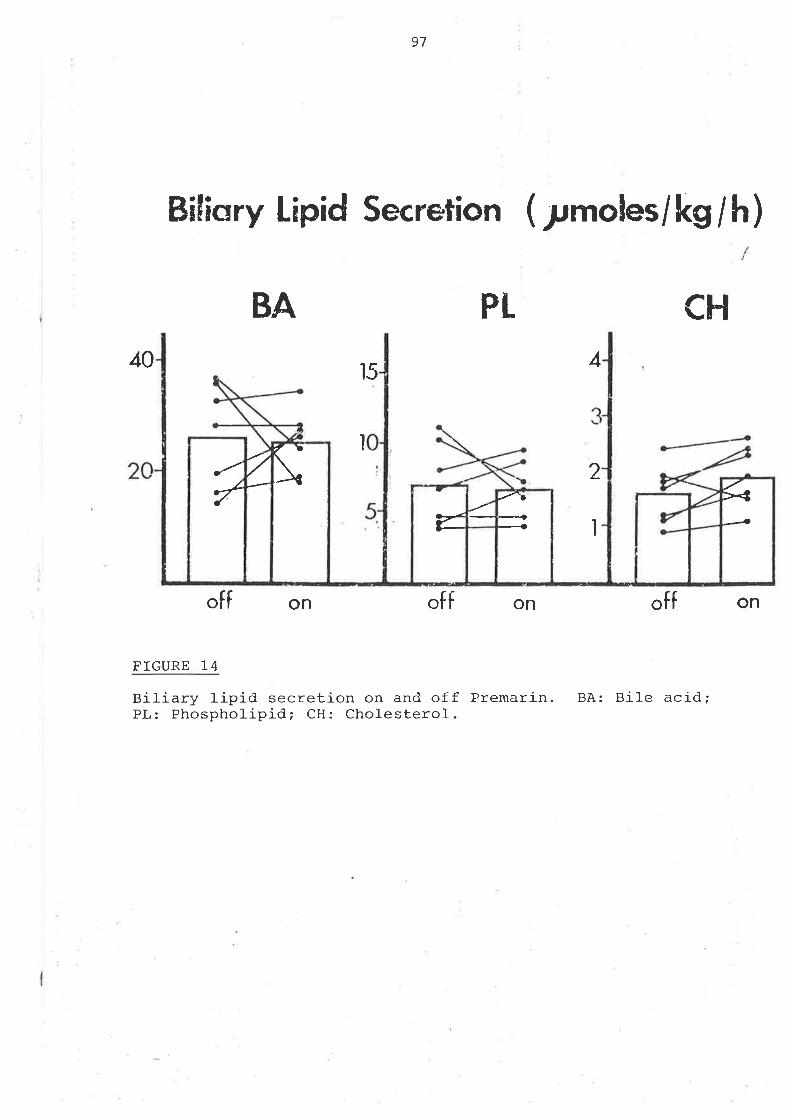
97
40
off on offon off
FIGURE 14
Biliary lipid secretion on and off Premarin. BA: Bile acid;PL: Phospholipid; CH: Chol-esterol.
Biliary Lipid Secretion ( lmoles/ Lg / h)
PL CH
I
BA
4l5
2
I
on
/\+1
a-.1ç
7<4---
ç/
9B
D. OROCAECÀL TRANSIT T]]"18 IN HUMAN PREGMI{CY
(i) r"grrioDs:
(a) Subjects
Fifty nine stuòies v¡ere perfornred (Table 9) in 27 healthy non-obese wLrite
r^roflren whose ages ranged frorn L6-34. Of B subjects initially studied in the
first trimester, 4 were subsequently stud.ied in the second trimester, 5 in
the third trimester and 5 postpartum. Of B subjects initially studied in
the second trimester 6 were studied in the third trimester and 5
postpartum. Seven of 1l- were initialJ-y studied in the third trirnester and
¡rostpartum. t .
(b) Gastrointestinal transit tinte
Thj-s was measured by the l-actulose hydrogen breath test (Bond and Levitt
1975; La Brooy, Mal-e, Beavis et al 1983; SoJ-omons, Viteri, Hanil-ton 1977)
(see Appendix).
Fasting serum progesterone level-s vùere deternined by radioirrrnunoassay at
Endocrine Sciences' Tarzana, Cal-ifornia-
(c) Anal-ysis of data
Group data were eval-uated by Student's t-test for unpaired data,and serial
studies by paired t-test.
(ii) RESULTS:
/
l4ean gastrointestinal- transit tine was 99 min in the first tri¡rester, I25
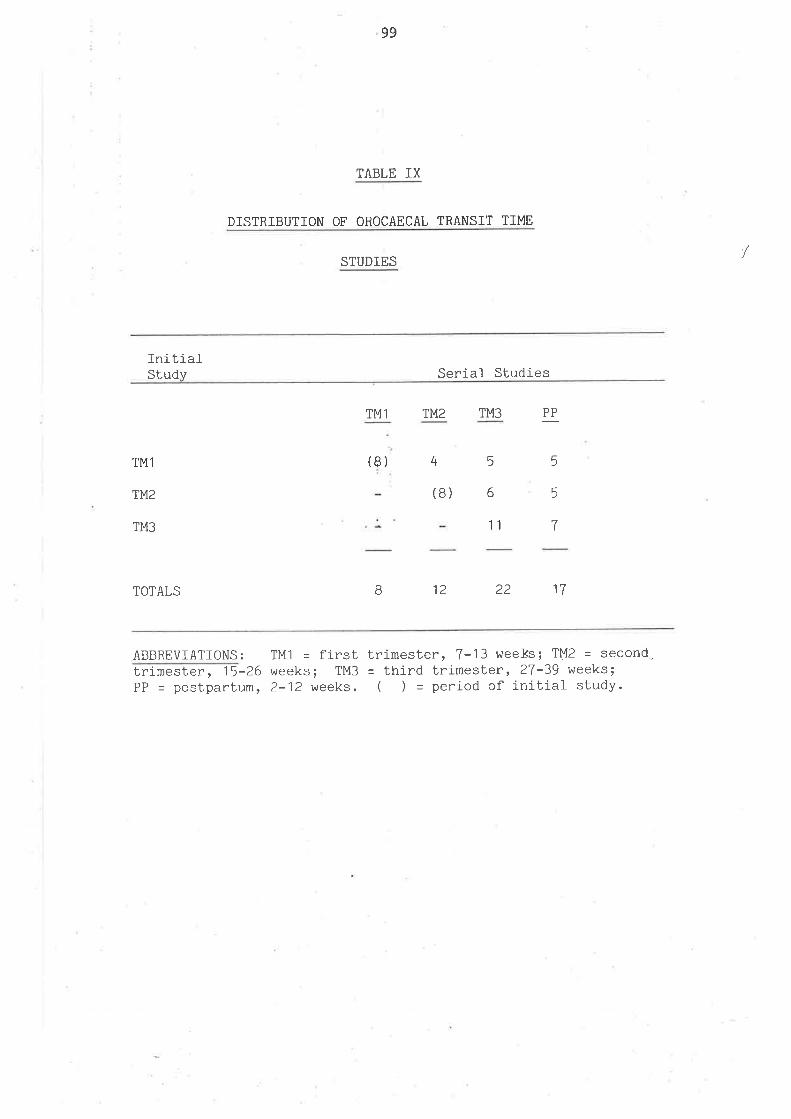
99
TABLE IX
DISTRIBUTION OF OROCAECAL TRANSIT TIME
STUDIES
Initi-alStudy Serial- Studies
TM1 TM2 TM3 PP
TMl
TM2
TM3
TOTALS
(8) 4 5
5
7
5
6(B)
B 12
11
22 17
ABBREVIATIONS: TM1 = first trimester, 7-13 weels; TMZ = second,trimester , 15-26 weeks; TM3 = third trimester, 27-39 weeks;PP = postpartum, 2-12 weeks. ( ) = period of initial study.
100
nin in the second trirnester, I37 min in tJ.e third tri¡nester and 75 rnin
postpartum (Table 10). There was considerable variation within each study
group but variation was sjrnilar between study groups, the range of the
percent coefficient of varj-ation being 39 to 44%. The sigrnificance of
differences in transit time between study groups was evaluated by both
Student's t-test for r:npaired data (S-test) and paired t-test for serial
studies (p-test), (Table l-1). Ttre results of these 2 statistical analyses
were identical. There was a sigrnificant increase in transit tinre frorn first
to second trjmester, a slight but insignificant increase frorn second to
third trinrester, and a marked decline postpartum. There \^/as no significant
difference between first tri¡nester and postpartum transit tinre. An exanple
of serial- studies of breath hydrogen curves for one subject is shcjwn in
Figmre l-5. There was a sharp sustäi-ned rise in breath hydrogen at 45
rninutes in the first trinrester, 90 rninutes in the third trimester and 30
rninutes postpartum
Serial- transit ti¡re studies of r.n/omen who were initialty studied in the
first trirrester is shov¡n in Figure 16. Transit time is expressed as the
percent of maximum transit time observed for each individual. This vafue i-s
plotted against the week of pregnancy or week postpartum- In each case, the
maximum transit time was achieved in ei-ther the second or third trimester
frorn l-5 to 40 weeks. In 4 of the 5 subjects transit time decreased
postpartum.
The relationship of transit tjJne to serum progesterone is demonstrated in
Table 12. Thre increment in transit tfune is greatest as the prq¡esterone
increases frorn I to B0 ng/fiI. There is no further incrernent in transit
time as progesterone Levels increase frorn 80 Lo 230ng/nl. However, the wide
variation of transit tjlrre within each range of serum progesterone precludes
accurate detennination of a "threshold" lcvel of progesterone, above which
l
L01
no firrtfÞr i¡¡crease i¡r transit tiÍe occurs.
hlt¡en nrouth to caecum transit tine was plotted against serun progesterone
for al-I tri¡resters and post partun, there vras no significant correlation
(figrr:re 17). Tterefore there ís only a trend for transj-t tine toj¡rcrease with serun progesterone with any significant relationship
¡nssiblï nnsl<ed by biological variation.
I
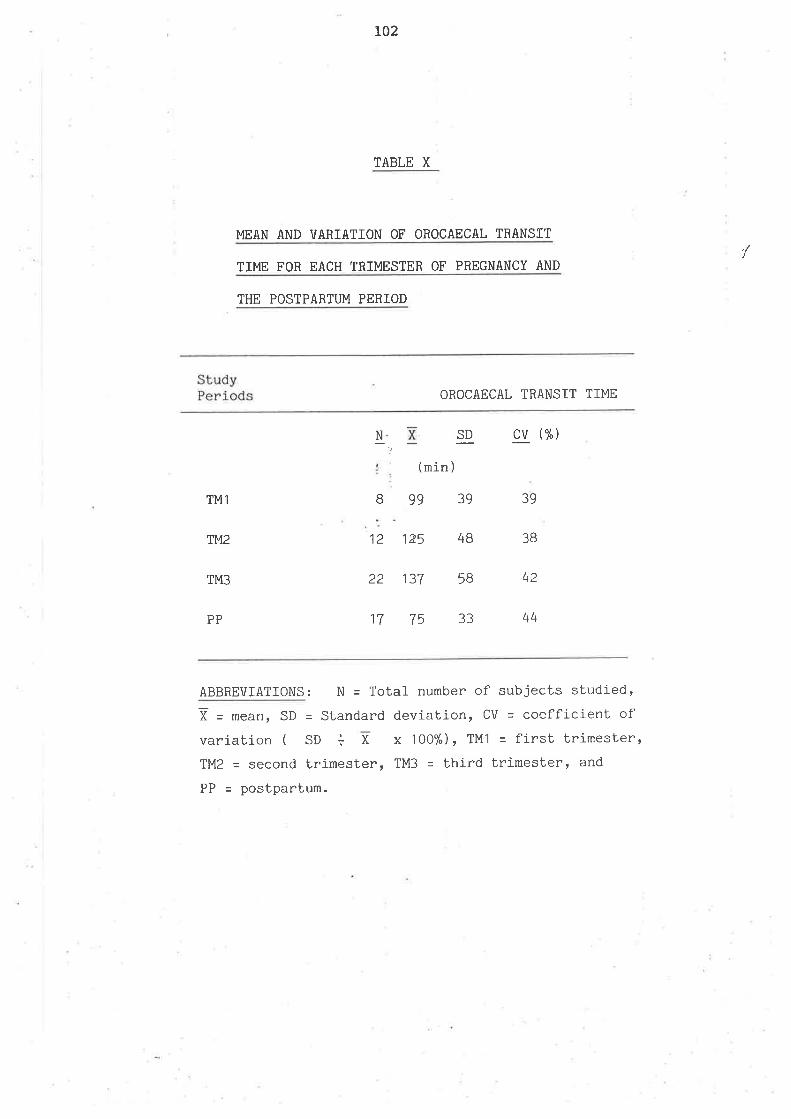
L02
TABLE X
MEAN AND VARIATION OF OROCAECAL TRANSIT
TI}48 FOR EACH TRTMESTER OF PREGNANCY AND
THE POSTPARTUM PERIOD
StudyPeriods OROCAECAL TRANSIT TI}4E
cv (%){ SD
39
4B
5B
33
TM1
TM2
TM3
8
12
22
(min )
99
125
137
75
39
3B
42
44PP 17
ABBREVIATIONS: N = Total number of subjects studied,
1 = meanr SD = Standard deviation, CV - coefficient ofvariation ( SO + X x 100%)' TM1 - first trimester'TM2 = second trimesterr TM3 = third trimester, and
PP = postpartum.
/
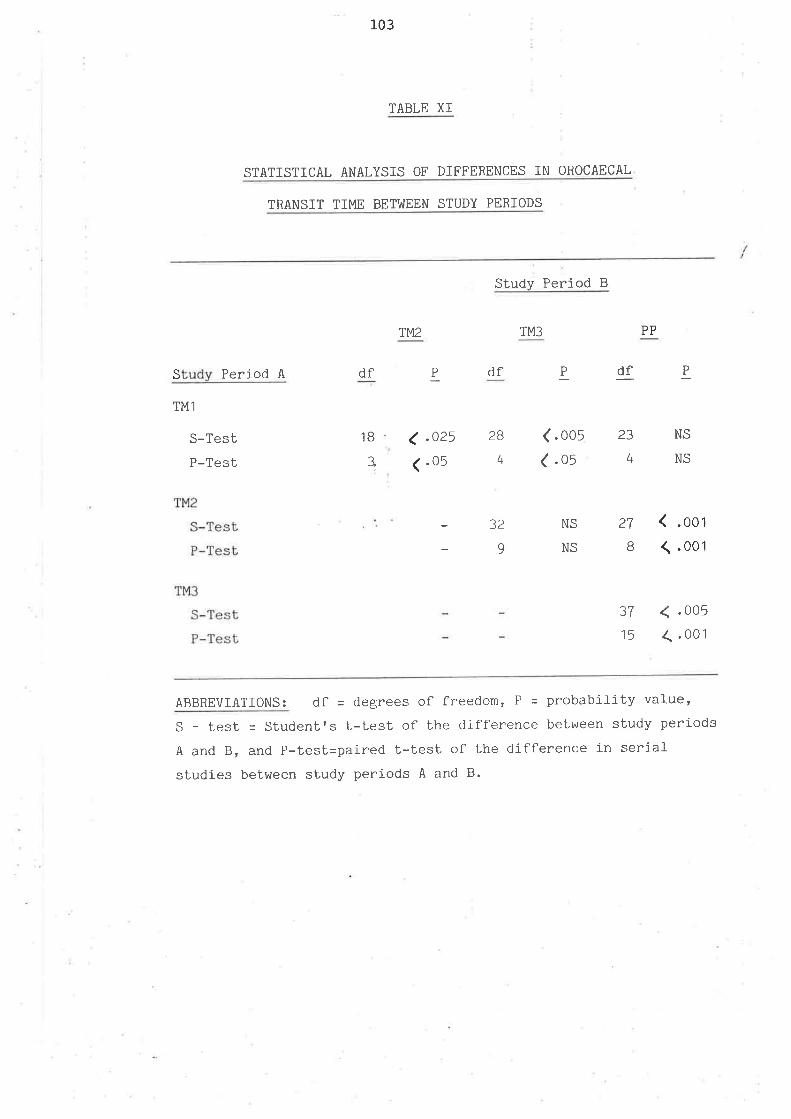
r_03
TABLE XI
STATIST]CAL ANALYSIS OF DIFFERENCES ]N OROCAECAL
TRANSIT TIME BETI,üEEN STUDY PERIODS
TM2
Study Period B
TM3
df
(.oo5( .05
32 NS
NS9
PP
23 NS
S Period A
TM1
S-Test
P-Test
TM2
S-Test
P-Test
TM3
S-Test
P-Test
df
1B .025
.05
BdfBt
1
2B
4 4NS
27
B (.001
< .005
<.001
?7
15
ABBREVIATIONS: df = degrees of flreedom, P = probabiJ-ity value,
S - test = Student's t-test of Lhe difflerence between study periods
A and B, and P-test=paired t-test of the diflference in serialstudies between study periods A and B.
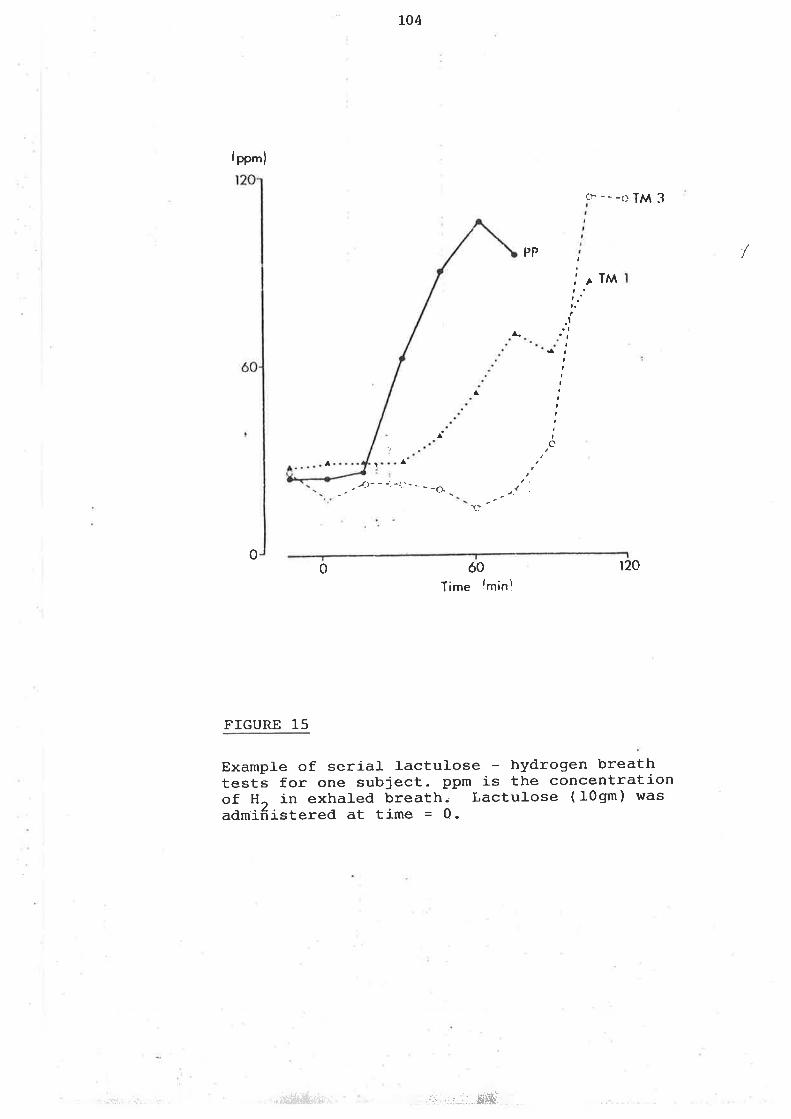
104
lpp'n)
0
cÌ- - - -r) TM3
PP /t
,
I, TM
.t
IIIIII
a
tc
^
^
^ ta
- - . r-t- - -: -i..'- .. - _cI
_
aI
'r-:
0 ó0Time lmin!
r20
FIGURE 15
Example of serial lactulose hydrogen breathtests for one subject. ppm is the concentrationof H, in exhaled breath.. Lactulose (I0gm) wasadmiñistered at time = 0.
";ç\{:1,.-r i1: .a -.1.,*ffii¡r,, ,ì;,:..:'¡i..lffi'
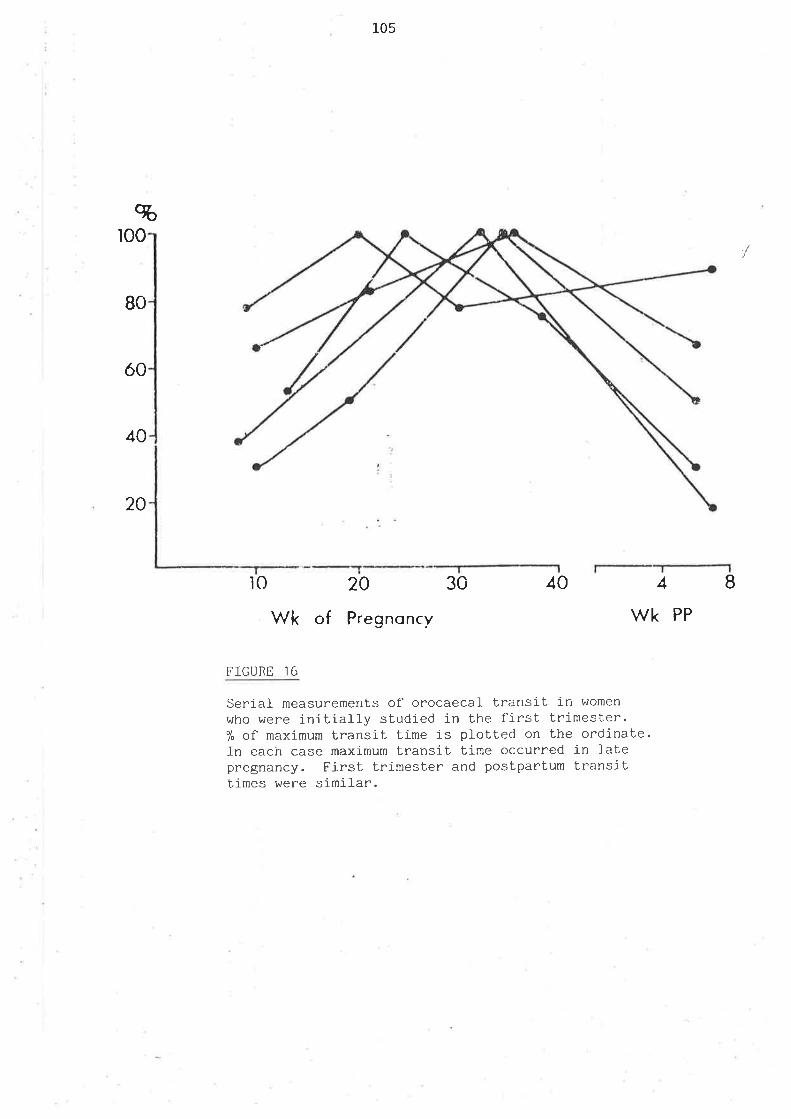
80
%ro0
óo
40
105
20 30
Wk of Pregnoncv
20
lo 40 4 8
wk
FIGURE 16
Serial measurements ol orocaecaL transit in women
who were iniLialJ-y studied in Lhe fj-rst trimester.7" of maximum transit time Ís plolted on the ordinate-In each case maximum transit time occurred in latepregnancy. First Lrimester and posLpartum transÍttimes were similar.
PP
I
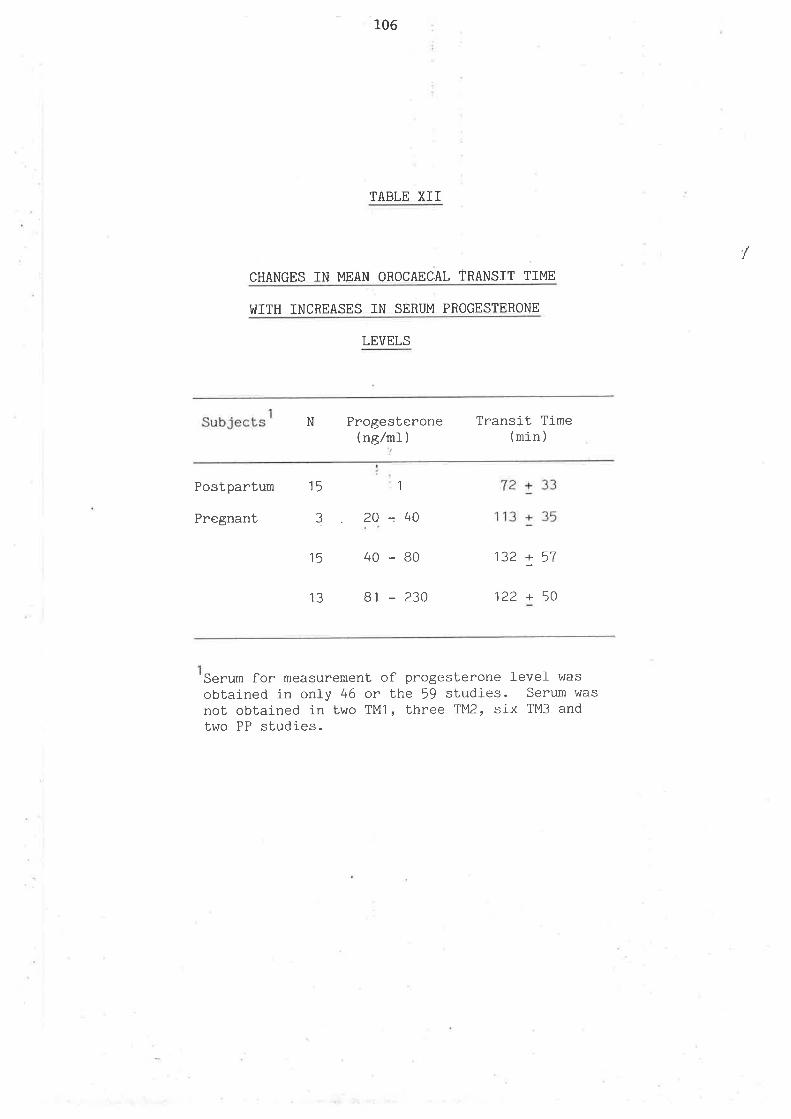
106
TABLE XII
CHANGES IN MEAN OROCAECAL ÌRANSIT TIME
I¡¡ITH INCREASES IN SERUM PROGESTERONE
LEVELS
Subjects Progesterone(nglrnl )
Transit Time(min )
N
Postpartum
Pregnant
15
3 20-40
15 40-80
13 81 - 230
72+33'113 + 35
132 + 57
122 + 50
1
Serum for measurement of progesterone level was
obtained in only 46 or the 59 sbudies. Serum was
not obtained in two TMl , three TM2, six TM3 andtwo PP studies.
/
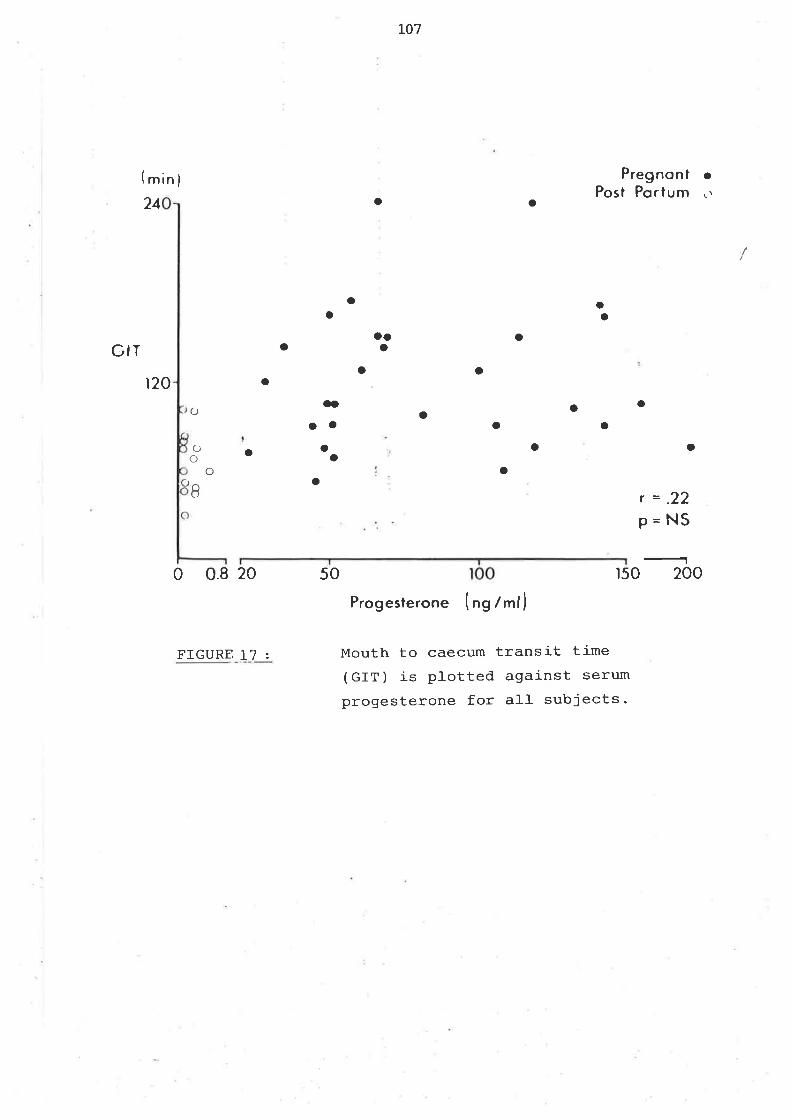
r07
GIT
lminf24
t20
o a
Pregnont .Post Porlum \ì
r=.22P=NS
oo
O
o
o
aa
OOa
O
aI
0 0.8 20 50
FIGURE L7z
Oo
oo()o
oooo
o o
a() ooaa
o o
r50 200
Progesterone (ng /ml)
Mouth to caecum transit time(GIT) is plotted against serum
progesterone for all subjects-
108
E.CO-ORDINATION OF GASTR.IC AND GALLBLADDER M4E{TYING ATIIM. INGESTTON OF A
REGT]I"AR MEAL
(i) MHIHoDS:
(a) Subjects
οel-ve healthy non-obese voJ-unteers, 6 men aged 23.8 +/- 2.9 yr (x +/- SD)
and 6 ü/onìen, aged,27-O +/- 2.5 yr were studied. Ultrasound exarnination of
the ga1-J-bladder excluded gaÌlstones in aII subjects. Since a small- amount
of radioactive material was used formeasuring gastric enptying, \^/omen rú/ere
studied only dr:ring menstruation- i
(b) Gastric enptyi-ng
After an overnight fast subjects ingested a standard breakfast of one egg
l-abelled with 200uCi of 99m Tc-sulphr.rr colloid, 2 sl-ices of bacon, 2 pieces
of toast with butter, 24omr of 22 fat (wt,/vol-) milk, and l0g of lactulose
in IOOml of water. The meaf contaj-ned 6l-0 cal- . 44e. faL, and 12? protein.
Most of the fat is associated with solid conponents of the meal and even if
partially emulsifj-ed, would enpty from the stomach with the sol-id phase
(Ji-an, Vigneron, Najea et al l-:gï2). The labelled egg $/as prepared by rnixing
rar^r egg with 2OOuCi of 99m Tc-suJ-phur colloid in an al-urninium foil tray;
the labelled egg was scrarnbl-ed in and subsequently eaten from the foil
tray. To determine binding of 99m Tc-sulphr:r coll-oid to the egg, it was
rnixed vigorously with fresh gastric juice obtained at endoscopy frorn a
separate subject. The nixture was incubated at 37 degrees C for 6 h, rnixed,
109
centrifuged., and radioactivity in the supernatant fiquid and in the solid
phase \^/as assayed. More than 95% was in the sôIid phase v¡hich is sirnilar
to the findings of I(roop, Long, Al-avi et a1(I979) -
( c )Gal1bl-adder enptYing
Subjects fasted overnight and real-time galtbladder sonographs \^/ere
obtai-ned, fasting every 5-l-0 min for the first 90 min after ingestion of
the meal (15 rnin allowed for eating), and then every 30 rnin until the
gallbladder refilled to at least 702 of its fasting volume. Gastric
scintiscans were taken at the end of ingestion of the meal and every
S-1gmin for the next 2 h. Gallbladder sonographs and gastric scintiscans
during this 2h period were obtained with the patient sitting upright'
Subjects were then moved to a bed.where they lay supine, with the head of
the bed elevated 30 degrees for the remainder of the study.
(d) Gastrointestinal Transit tiirre and serum HPP
Breath sanpJ-es for hydrogen analysis were obtained fasting and every 15 min
for 4 h after conpJ-eting the meal-. Venous blood for measurement of
pancreatic pollzpeptide level- was drawn through an indwelling venous
cathetêr fasting and every 30 rnin throughout the study'
(e) Analytical techniques
Gall-bladder volume was fiìeasured from gallbladder sonographs (see appendix);
To conpare results betwen individuals, volume rnlas expressed either as
percent of fasting volune or. as percent of volume irnnediately after meal-
ingestion. Ttre time of initiation of gal-Ibladder refiJ-ling was deterrnied
frorn inspection of each plot of volume vs tjrne-
I
110
Gastric enptying obeyed a zeto-otder functi6¡-(Headilg, Tothill, Mclouglr-lin
et al, L976\.
DPtr4txI00=kt+b
DPMo
r¡ihere DpM is disintegrations per nin, DPMo is gastric DPM at corpletion of
the nreal, DMPI is DPM at time t, k is the constant of enptying, b is the
intercept at t=o and l-00 is the conversion factor for ¡rercent. k was
calculated frorn linear regression of (DPMtÆPlaO) x 100 vs time.
The plot of breath hydrogen vs time was evaluated by two
gastroenterologists blinded to the protocol and results of the study'
Estjmates varied in only 2 cases and by only 15 rnin each.
(f) Analysis of data
Data are expressed as nìean +/- SD. bitf"rences between. ren and wornen were
evaluated by Student's t-test. Correlations of various pararneters vvere
determined by bivariate regression analysis
(ii) RESULTS:
There was no difference in gallbladder enptying, gallbJ-adder refil-Iing,
gastric enptying, or HPP response between men and \^/omen (Table 13)
AccordingJ-y, data from all- 12 studies \^/ere pooled for subsequent analysis'
The mean orocaecaf transit time of the women was twice that of the
men, 13.6 +/- 20.2 anð,37.5 +/- 22.'7 min, respectively. The transit tirnes
in these rúr'omen, who were studied early in the follicular phase of their
ovulatory cycles, are similar to those previously reported by WaJ-d et al-'
using a similar technique in healthy young l^rollten in the foll-icular phase of
the ovulatory cycle, 97 +/- 3I min (Vrlald, Van Thiel, Hoechstetter et al
19Br).
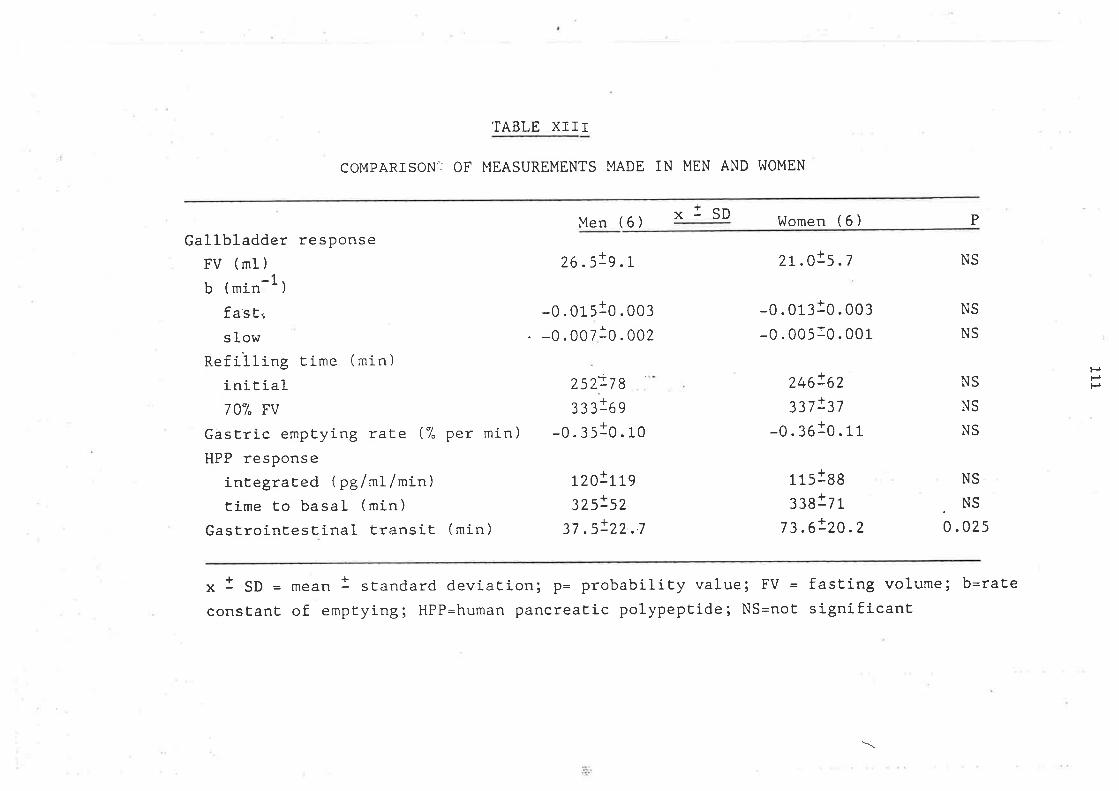
TABLE XIII
COMPARISONìJ OF MEASUREMENTS MADE IN MEN AND I^JOMEN
xlsDMen (6)
26.5!s.L
-0 . 01 slo . oo¡--0.00710.002
¿252:7 8
333169
-0.3s10.r0
LzO!Tß32s!5?
37 .5!22 ..7
l^lomen ( 6 )
-0.01¡10. oo¡
-o .0o5to. oor
246!62337!37
-o.3oto. rr
1 15188
33817 1
7 3 .6!20 .2
P
Gallbladder responseFV (mI)
_1b (min -)
fasE..
s lowRefilling time (min)
initial70% FV
Gastric emptying rate (7" per min)HPP response
integraEed ( pg/mf/min)time Eo basal (min)
GastrointesEinal transit (min)
n.o!5.7 NS
NS
NS
NS
NS
NS
NS
.NS0 .025
PPP
x I SD = *""n 1 standard deviaEion; p= probability value; FV = fasting volume; b=rate
consEant of emptyi.g; HPP=human pancreatic polypeptide; NS=noE significanE
\
LL¿
(a) Gallbladder enPtYing
Íhe ti¡ne course of gallbladder enptying and refiIling for all subjects is
shovm in Fignrre l-8. A In/J-inear pJ-ot of gallbladder volune vs tjrne from 0
to I20 min revealed two phases of enptying, an initial fast phase frorn 0 to
30 nin and a second slow phase frorn 30 to 120 rnin. TLre initial fast rate of
enptying was 0.0L5 +/- 0.003 rnin -1, wtrj-Ie the second slow rate was 0-006
+/- 0.001 rnin -I, the gal-Ibladder remained tonically contracted r:ntil
refilling began aL 249 +/- 67 rnin (l'igure l9). The time interval from
initiation of galtbÌadder refilting to achieving 70% fastì-ng vofume ranged
frorn 30 to 180 min (86-l- +/- 52.I; f +/- SD) -
(b) Gastric enptying
The zero order rate constant of gastric enptying of sol-ids after rneaf
ingestion was 0.35 +/- 0.L18 per mil and the first order rate constant of
the second slow phase of gallblader enptying was 0-006 +/- 0.001 per rnin
(Tabl-e 13, Fig,r:re 20).Substituting the mean tjme of initiation of
gatlbladder refilling (249 min) into thre eguation defining the rate of
gastric enptying, it can be seen that when gallbladder refifling begins'
only 13% of so|-ds remain in the stomach. fn addition, using the zero-order
rate constant, gastric enptying woul-d be conrplete at 286 min, I h before
the gallbl-adder refilled to 70% of original fasting volume 335 rnin'
ùrocaecaf transit tinre di-d not correlate with fast and sl-ow rates of
gaJ-lbladder enptying, rate of gastric enptying, time to initiate
gallbladder refilling or tirne of gallbladder refil-Iing to 70ø of fasting
volume
Ttre correlation between the percent of bile remaining in the galÌbladder
and percent of solids remaining in the stornach for each tirne point was
highly significant (Figure 21)-
:iií
ri!'l'¡t;¡
{
II
I
r
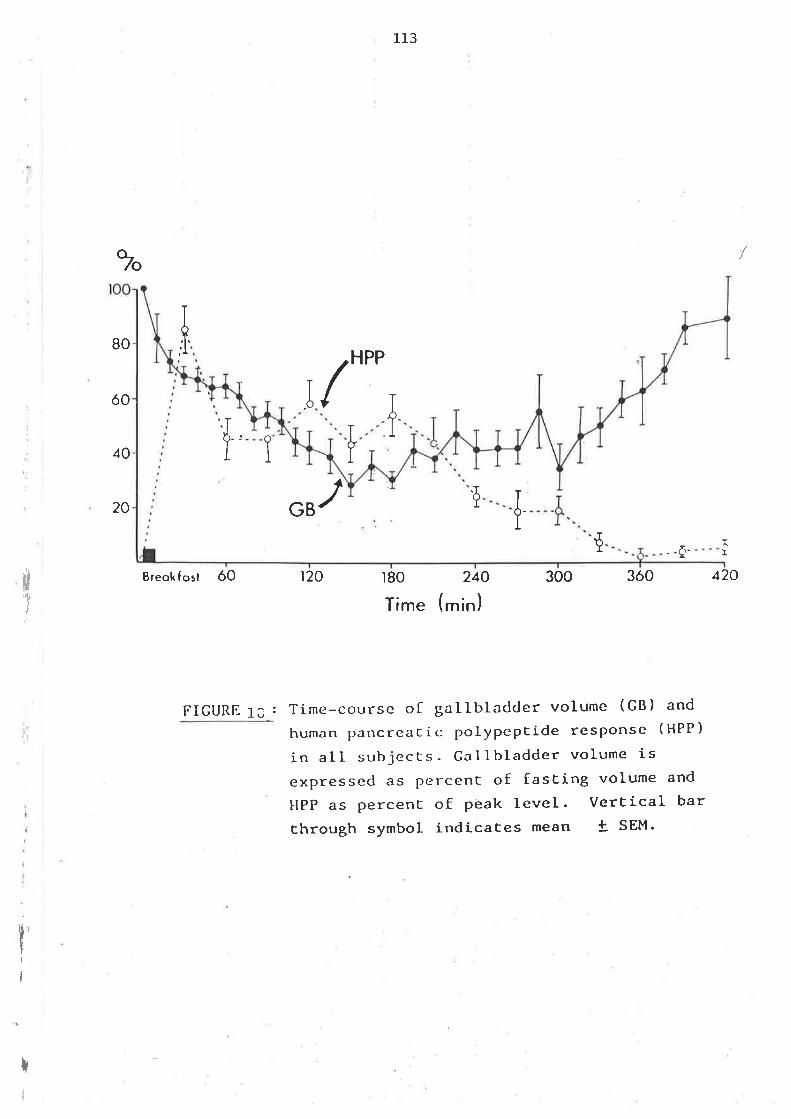
%
HPP
1_13
r80
Time (
80
ó0
40
20
,T
Breokf osl ó0
FIGURE 13 :
/
/ JI
II
ür¡t
J
I
{ iÞGB
ì20
{ I0r
min
240 300 3ó0 420
)
Time-course oI gallbladcJer volume (GB) and
human parìcreaCic polypeptide resPonse (HPP)
in all subjects. Galtbladder volume isexpressecl as percent of fasEing volume and
HPP as Percent of peak level. VerEical bar
Ehrough symbol indicaces mean ! SEM'
r
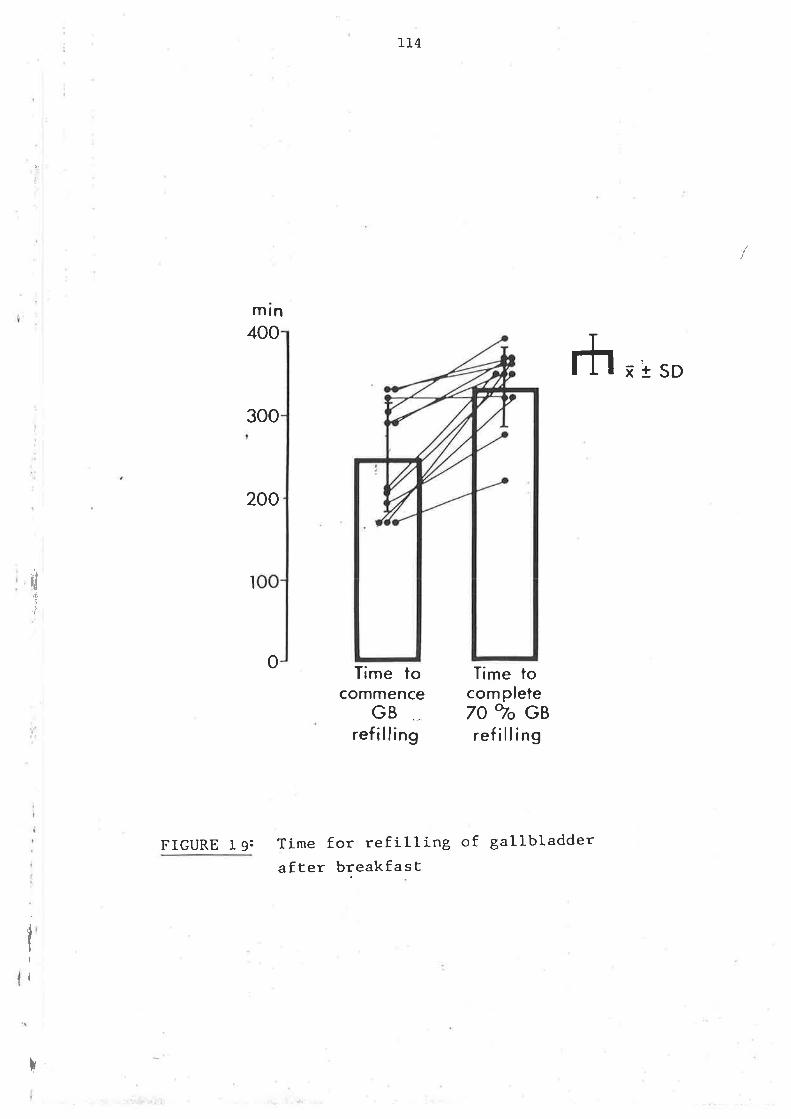
IT4
Time tocommence
GBref illing
rh xt sD
1
..I
ü't,r
mtn400
300
200
o
I
FIGURE T 9:
Time tocom pleteTO ro GBref illing
Time for refilling of gallbladderafEer breakfast
I
t
al
I
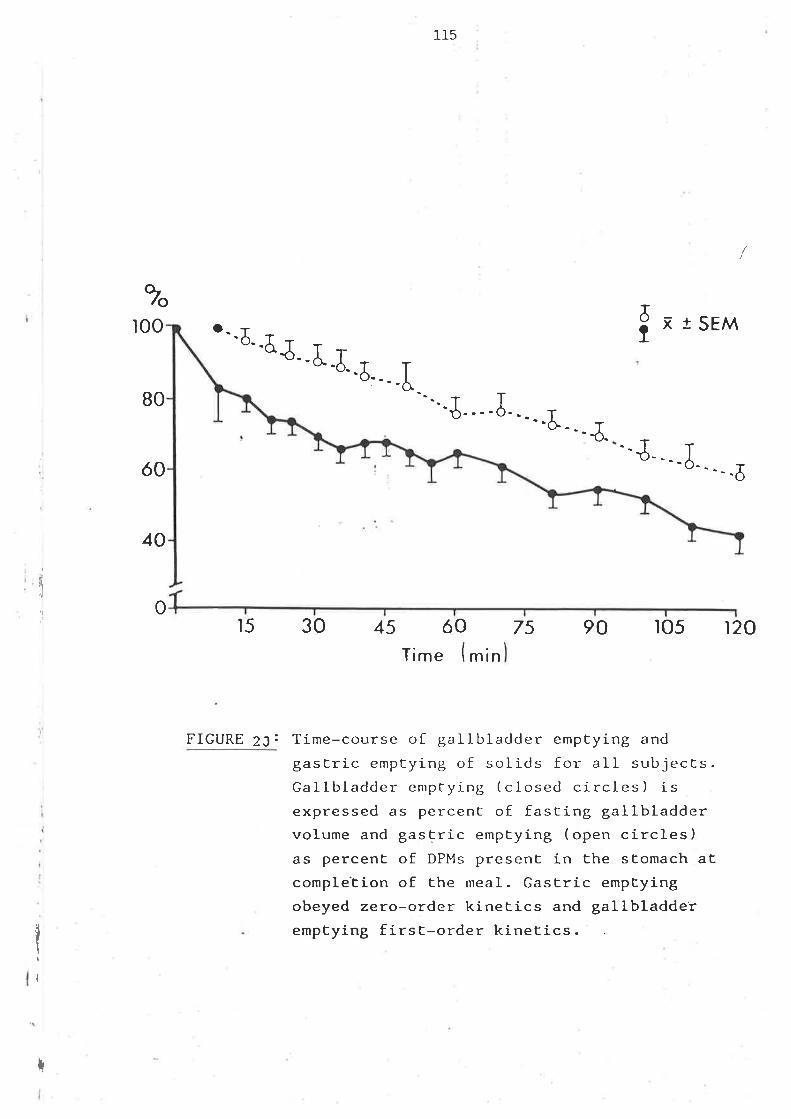
115
...T T'ö----0
%ì00
80
ó0
40
o ix t SEM'-ð_.5J..J..tr
-6....l
t.. -¿." J-...¿ -''--ð
I
q
'l 015 30 45 ó0
Time (min7s 90 lo5 t20
FIGURE 23: Time-course of gallbladder emptying and
gastric emptying of solids for alI subjects.Galll¡ladder emptying ( closed circles ) isexpressed as percenE of fasring gallbladdervolume and gastric emptying (open circles)as percent of DPMs present in the stomach atcomple'Eion of the meal. Gastric emptyingobeyed zero-order kinetics and gallbladderemptying first-order kinetics.
I
I
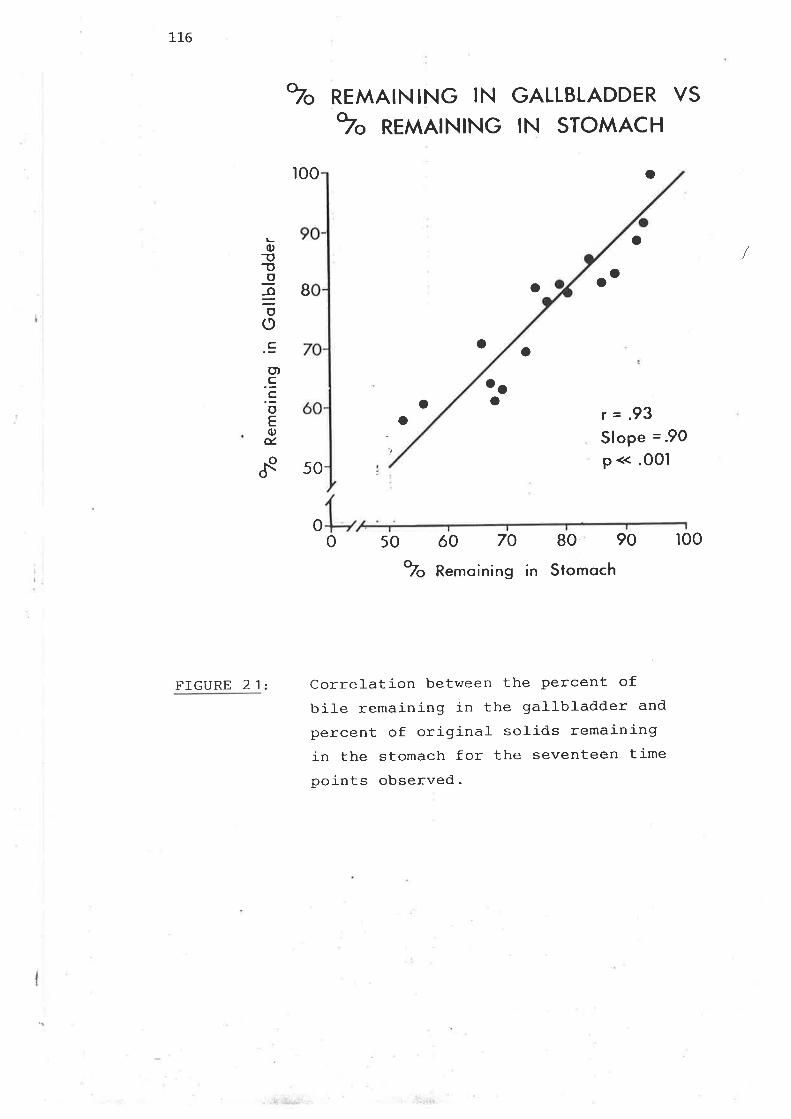
116
FIGURE 2 1 z
"" REMAIN¡NG lN
?" REMAINING
GALLBLADDER VS
IN STOMACH
roo o
o
r=.93Slope =.9O
P << .o0l
LC)
T!o
€oo
o).E.EoE0)ú.
f
1Oo
B a
o o
oo
050ó070o-/o Kemolnlng
80 90
in Stomoch
oo
o
50
or00
Correlation between the percent ofbil-e remaining in the gallbladder and
percent of original- solids remainingin the stomach for the seventeen timepoints observed.
t17
(c) Serum HPP
Plots of HPP level- and gallbladder vol-ume vs time are shown in Figiure 17.
The initial fast phase of gallbladder enptying is acconpanied by a rapid
rise and early peak in HPP response. The slow phase of gallbladder enptying
and tonic Aallbladder contraction is associated with a sustained el-evation
in HPP leve1s. Ttre return of HPP level-s to basel-ine roughly corresponds to
the time of initiation of gallbladder refilJ-ing.
The integrated HPP response did not correlate with rates of gallbJ-adder
enptying, gastic enptying, or GTT. Thre initial peak HPP l-evel- did not
correfate with the initiaf fast rate of galJ-bladder enptying. The
integrated HPP level dr.rring the slow phase of gallbladder enrptying and
tonic aallbladder contraction did not correl-ate with the average
gal-Ib1adder volume during the same- interval of tinre.
1L8,
CHAPTER IV: DISCUSSION
A. Presnancv, Female Sex Steroids and
Gallbladder Function
B
(i) Effects of the Ovulatory Cycle and
Contraceptive Steroids
(ii) Effects of Pregnancy
(iii) Effects of Chronic Oestrogen Intake
The Effect of Gallbladder Emptying on
Bitiary Lipid Secretion
Or.ocaecal - Transit Time in Pregnancy
Gastric and Gall-bladder t Ln
c
D
I
119
DISCUSSION
A. PREGNANCY, FEMAT,E SEX STEROIDS AI']D GÀLLBI,ADDER FUNCTION.
Pregnancy causes greater than normal retention of bil-e in the gallbl-adder
throughout the day and night. The retention is maximal at a ti¡ne when bil-e
is rel-atively supersaturated wj-th cholesterol-. Such changes could
contribute to the increased incidence of cholesterol cholelithiasis
associated with muJ-tiparity.
(i) nffects of the ovulatory cycle a4d contraceptive steroids
Fasting, residual- and hourl-y volume were sirnilar in t-l.e fol-l-icular and
luteal phases of the ovulatory cyc.lés. Rates of enptying after breakfast
were the same in both phases of the ovulatory cycle. Contracepti-ve steroids
increased fasting gallbladder volumes only.
Nilsson and Stattin (1967) used oral cholecystography to measure
gallbladder emptying after bolus injection of cholecystokinin in both
phases of the cycle in each of I0 subjects, and they found slower enrptying
in the l-uteal phase in B of them. However, the phase of the cycle was not
documented by serum progesterone level, as in the present study, and 5 of
these B had a l-0% decrease in enptying in the luteal phase. Nonetheless
this data indicates that the efevated progesterone levels associated with
the l-utea1 phase do not significantly alter ei-ther gallbladder vofumes or
enptying during i-ngestion of regular meals.
(ii) Effects of pregnancy
12a
Assessment of the data in the way that has been performed in this section
of the thesj-s requires further explanation. In general, the regression of
data j-s perfornred to study the rel-ationship between a predictor variabfe
and a response variabl-e. Ttre regression anal-ysis sunrnarises the refatíon
between the response and preðictor variabl-es and rneasures the correl-ation
between variables. Before regressing data it is irrportant to plot and
exarn-ine data to check for outl-iers and to define nonl-inear patterns in the
data. It is atso irrportant to look for patterns suggesting that the data
shoul-d be transformed to a different scale, such as loqarithrlic, to produce
a better fit, to tl:re data. Itre sinple linear-regression nrodel assumes that
the relationship between x and y can be sunrnarised as a straight-line
graph. However, if the data do not seem to lie on a line or if the
residual-s show a cl-ear pattern, tfre, l-i.r"ar ¡nodel- may not be consistent with
.the data. One way to deal with this problem is to attenpt to fj-t the data
to a particular crrrve, such as a troþatithnic, sinusoidal, or exponential
curve, nonlinear regression, as discussed by Bliss (1970) and Snedecor and
Cochran (1980). According to C,odfrey (1985) if part of the data seems to
lie along one line and part along another l-ine, the data can be stratified.
Using this technique, a different line is fitted to each segment of the
data, In this case it is assumed that a linear relationship hoJ-ds within
each stratum, al-though t.l.e exact relationship may not be the sanre frorn
stratum to stratum. Such a nrodel- is call-ed a piecewise linear nx¡del-. If a
sinple l-inear regression is used to study the rel-ationship between initial-
gallbladder enptying and pregncnclr there is l-ittl-e difference between
controls and pregnant subjects. However, it j-s appropriate and valid to
use a logarithrnic scale for gallbladder vol-ume and to apply a piecewise
regression. The result is that a significant difference is demonstrated
between pregnant subjects and controls in the second slower phase of
gallbladder enptying (Figure 6). Again this rel-ationship would be rnissed
if an alternative to a sirrple linear regression \^/as not used.
¡i
I2I
Fasting and residual vol-umes \^¡ere larger than control values in every
trjmester of pregnancy, and they increased J-inearJ-y dr:ring pregnancy.
For fasting volume a correlation of r = .48 (e = .016) is obtained and the
line y = 20.17 + 0.450 x is the l-ine of best fit for sinple linear
regression. Given the relative large variation between ind-ividuals, thi-s
indicates an increase in volune over the pregnancy. The guadratic
relationship does not significantly inprove the fit over the linear (R2
changes from 0-226 Lo 0.257) and the equation y:10.89 + 1.36x - 0.019x2
gives the best quadratic fit with a maxj¡num volune at 36 r,^/eeks' Ttris does
not support the hypothesis of no increase in volume in the third trimester.
An exponential growth n¡¡de1 woufd bêhave similarly-
For the residual- volume a correlatiòn of r : .54 (P : .006) is obtained and
the line y : 3 -'78 + .232 x is the line of best fit for sirrple linear
regression. Given the relatì-ve J-arge variation between individuals this
indicates an increase in volume over the pregnancy-
The quadratic relationship again does not significantly inprove the fit
over the linear (n2 changes from .290 Lo .308) and the equation y = -48 +
.55x - .0065x2 gives the best quadratic fit with a maxjmum vol-u¡ne aL 42
weeks. This does not support the hypothesis of no increase in volume in
the third trimester. An exponential growth model- woul-d behave similarly-
Vlhren the volumes in the tlree tri-mesters are conpared the means are ( 23.7 ,
33.3 and 32.1) for fasting volumes and (6.4, 9.5, 10-5) for residual
volumes. Statistically significant differences are shov¡n by one way
analysis of variance to occur at the l-evels of P : .064 (F= 3 -l.2) for
fasting vol-umes and P : 0.116 (F= 2.38) for residual volumes neither of
122
which quite reaches the connonly used value of .05 for statistical-
significance.
Hourly volumes frorn tl a.m. r:ntil rnidnight were larger than those of
control-s throughout pregnancy, without progressive change (Figure 4C). The
failure to find a progressive increase vùas due to large hourly volumes in 2
first-trinester subjects (Fignrre 4C). Because the progesterone level of
these two subjects was appropriate for the week of pregnancy, the vari-ation
in hourly volumes is probably due to individual- dj,fferences in galJ-bladder
srnooth-muscle res¡rcnse to increases in progesterone-
As fastinq, residual and hourly vol-umes return toward normal in the
postpartum period, it i-s probabJ-e thit most of the changes in gatJ-bladder
vol-ume during pregnancy are transient. !{hether vol-umes return to prepartum
val-ues in a given individual cannet be deterrnined from this study as no
subject was studied before pregnancy.
Only the last phase of galJ-bladder enptying after breakfast was sfower Ín
pregnant women. The slower late phase of enptying may be due to inpaired
gallbladder contractility or slower gastric enptying. The late rate of
gallbladder enptying correlates with gastric emptying of solids- Thus it is
possible that the sfower rate of gallbladder enptying after breakfast in
pregnant subjects i-s partì-al-ty due to slow gastric enptying of solj-ds-
An overall sunrnary of the gall-bladder enptying curves would be l-ess li-keJ-y
to contrast the differences in gallbladder enptying between controf and
pregnant subjects. The earJ-y rapid phase of gallbJ-adder enptying is a
reproducible finding as can be seen j-n Chapter III, Section E when a
different control group of volunteers \^/ere studied including males and
females. This early response is most likely vagatly innervatecl. Fisher,
1
]-23
Rock and l'la1nnrd (19861 have recentJ.y shovm in hurnan volunteers that intact
vagus nela/es and cholinergic pathvrays are required in order for the
ga1-Ibladder to respond to sh¡am feeding. T'hey found that the maxirnal
curn:Iative gallblaclcler anrptyjlg response to sham feedilg vras 44%, vrhich r,ras
not significantly different frqn the respoonse to beth,anechol and to
ingestion of a test n'¿eal of steak and potato. (holinergic blockage vrittrI
atropine eli¡¡irnteo the enptying reslænse to sham feecling and sham feeding
did not sti:rmlate gallbladder e-nptying 1n patients i.rith vagotorry.
A biphasic response has been reported for gastric erptying of digestiJcle
soticl meals v¡hen neasurernents are tal<en cluring rneal ingestion r'¡ith a 'Iag'
phase precetìing a l-j-near oiptying phr,ase (Col-Iins, Flororvitz, Cook et aI
1983 ) . Tlrerefore our earl-y phase of gallbladder enptying is unl-i]<ely to be
rel-ated to rapiC initial solid gastric ottptying.
Because tlre honnonal changes of pregr-rancy are ccxitplex (Iilo¡:¡:ert and I\rchs
1977) it is not possil:Ie to identify v¡ith certainty ttre nediator or
rediators of the alterations in galLbl¿r.dier function. It is also not
possibl-e to :--.:clucle a c-ìirect or inclirect neuronal influetlce produced iry
ÌïeEl^ranc:,,/. In aclCition neuronal chamges coul-a rnodify ani¡ honnor¡al effects
124
on motility. Nevertheless, progesterone, a knov¿r inhibitor of snxcoth
muscle contraction (Cohen l-980; Sonrlzlo and Sonqzlo l-970; Schultze and
Chri-stensen ISBO; Fj-sher, Roberts, Grabowski et al- I9lB) is a likely
candidate. The data shows a ôirect correl-ation of fasting and residual
volurne with serum progesterone concentrations. Thj-s is
consistent with, but not proof of progesterone mediation. As there was a
highly siginificant direct correlation between serum progesterone and week
of pregnancy, and the correlation of each of these variabl-es with fasting
and residual volume were identical, it cannot be concluded that
progesterone caused the effects- The changes in indices of gallbladder
function could be due to other, unnìeasured factors in pregnant women-
In sunrnarlz, the phase of the ovulätory cycle did not affect gallbladder
function, but pregnancy caused retention of bil-e in the gallbladder
throughout day and night. Prolonged contraceptive steroid use induced an
increase in fasting (overnight) but not daytime bile retention-
The results of this study indicate that in pregnant women, gallbladder bile
retention is lncreased throughout the day and night. Bil-e retention is
greatest in the second and third trimeters, a time when gal-Ìbl-adder bj-Ie is
most lithogenic (Kern, Everson, De Mark et al- 19BI). Thus, gallbladder bil-e
retention could contribute to the pathogenesj-s of cholesterol gallstones by
allowing more tinre for nucl-eation and pecipitation of cholesterol
crystal-s.
(iii) Effects of chroni-c oestrogen intake
This study has sho¡¡¡n that oestrogen is unlikely to be responsibl-e for the
increase in bile cholesterof saturation which acconpanies the use of oral
contraceptives.
t25
The results of the effects of clrronic oestrogen intak-e on cholesterol
secretion, cholesterol saturation index and gal-Ibladder concentrating
ability reporbed shov¡ no sigrnificant change v¡ith the doses used. One
possible r€¿se¡ for tkre lack of response is failure of absorption of the
conjugated oestrogens. Pre¡rnrin contains equilin sulphate (252)and as v¡ell
as other conjugated ccnrpourds, includes sulptr,ate triester of estrone túSzl
17 alpha tihydroecluihn (1 5u ) , 17 alpha d.ihydroequilenin and 1 7 beta
dihydroequilenin (15S). After oral aùninistration of Prqnarin to
postinenopausaf v¡ornen equitin sulptrate and oestrone sulphate appear in the
serum as unconjugated equilin and oestrone (Bhawrani, SarCa, ir'oolever
1981 ). T'hese findhgs indicate a-l:sorption of oral- Pre¡narin.
In the study re¡iortecl here rthe gallbladder contractil-e res¡:onse to
intravenous CCK, a núxed meal and intraduodernl ì-iquid fcxr,ula v¡zrs
unaffecbed by chrronic oestrogen aùninistration. Oestrogen pretreatmeni j-n
anj¡ral-s has previously been re¡rcrted to erùrance the in vivo contractility
of the oesophiag-us, antn-r'n ¿ncl colon (Bruce and Eehsudi 1979 ). oestrc4len
pretreai:;rent has not been shor^,'n to increase contractile responses in the il
vitro ç¡:inea pig gallbladder, but it significantly decreases the thresholcl
acetylc¡oline dose requiraments (Lffan and Pellecchia 1982l.. It is possibJ-e
tirat the gallbladder is rel-atively less sensitive than other tissues to thr
excitatory effects of oestrogen.
B. 'I]]E EIIÞ'}]CI OF GAIJ,E|T,ADDM{ Eù{HTYING CN] BT,IAIìY LIPID SECRETICN
The observatiori in pregnancy of supersaturated bile and delayed gallbtadde
onptying raised the qrestion of the role of the gallbladder j¡r controlJ-ing
biJ-iary cholesterol secretion. Secretion studies using different strength
sti¡mli we¡e desigrred to study thre effect of inconplete and alnucst ccnplet
, L26gallbladder enptying on biliary cholesterol secretion.
Il'lhen previous secretion studies are ccnrparecl it can be shov¡n tLnt bile acid
secretion rates durJlg continuous intraduodenal amino acid infusion
(Shaffer arrd Smal-I 1977¡ Kern, Everson, De l4ark et al 1981 ) are l-ess tl¡an
those neasured during c-ontinuous intraduodenal liquid formul-a infusion
(Grurüiy and lbtzger 1972; Ivlok, Von Bergmarrn, h:ndy 1979; Bennion and /Grundy 1975¡ Mabee, I"Ieyer, Den Besten et al- 1977; Valdivieso, Palma, I'Iervi
et I 1979; l{cJ<, Von Bergnrann, Gn:rrly 1978) and sjmil-ar to that measr:red
during intermittent lic-iuid formula feedings (t'iok, r/on Bergnrann, Grr-rndy
1979, Northfield and Flofnnnn 1975i La Russo, Szczeperrik, Iìofnnrrr 1977; Itok,
Von Bergnann, Grurrcìy 1980; La Russo, Hoffnnnrr, Hofinann et al 1975') and inpost cholec¡¿stectonry sr-rbjeets (Shaffer and Small 1972; I/rey, Bonorris, i,larks
et al- 1980) (see Thble 3a+ Appendi:<).
I'lhen similar groups of subjects are ccn'rpared bile acid secretion rates
ù:rhg tiquid formula infusion are Íìore th,an trvice those during a¡lino acid
j-nfusj-on. In the present stucly durilg licruid forin¡rla infusiorr the rate of
biì-iary lipid secretion r.ns higher, gallbladder onptyilg \./as pronpt and
nìore corq)Iete, and sinall in'bestinal transit \,ãs faster. It can læ
concluCed that tl're higher rate of biliary lipid secretion achievecl during
liguid formul-a in this ancl other studies is due to j-ncreased enterohepartic
q¡cling of bile acj-d causecì by more ccnplete galJ-bl-adder er,ptying and
faster snrall intestinaÌ transit. Bil-iary lipid secretion rate during amino
acid infusion is sulmaxirnal, due to inoonplete gallbladder emptyilg and
sl-ower intestinat transit.
BiJ-iary lipid ccrnposition is dependent on the ra'te of biliary bile acid
seqretion. In patients rvith bil-e fistulae the nrrl-ar percent chol-esterol- of
T¿I
bile increases as the bile acid secretion rate drops (Lindblad, Lundholm,
Schersten L977; Wagner, Trotjnan, Soloway 1916; Nilsson and Schersten 1969).
In subjects with gallbtadders, fasting sequesters part of the bil-e acid
pool- in the gallbladder, induces a lower bile acid secretion rate
(Northfiel-d and Hofmann L975¡ Mok, Von Bergmann, Grundy 1980; WLzger,
AdÌer, Heysmfield et al 1973) and increases cholesterol- saturation of bil-e
(Northfield and Hofmann L9l5; Me|zger, Adler, Helzmsfield et al L973).
When sirnilar groups of subjects from different studies are conpared' the
nolar percent cholesteroJ- during continuous liquid formula infusion (2.9
Hcward l9B0) is less than that ùring continuous arnino acid infusion
(4.3 +/- .5å Kern, Everson, De Mark et al 19Bl). In the present study a
sirnilar difference has neen sfrovå between the two infusates in the sanre
individual-. It can be concluded that the decreased molar percent
chol-esterol during liquid fornmla infusion is the result of a higher rate
of bil-e acid secretion due to nìore conplete gallbladder enptying and more
rapid smaLl intestinal- transit.
Since the rnrlar percent chol-esterol of bile varies with bile acid secretion
rate the rel-ationship of cholesterol secretion to bil-e acid secretion must
necessarily be curvilinear over the futl range of bile acid secretion
rates. However, if only a portion of the range of bile acid secretion rates
is exarnined, the relationship between bile acids or phospholipid and
chol-esterol may appear linear. !{hren the data in t}ris study fron amino acid
and liquid formula are combined the resulting relationship for bile acids
and cholesterol is curvilinear (Figu-re 9). If the data frqn each infusion
is exarnined separately then tÌ.e relationships appear linear as only a small-
portion of the range of bile salt secretion rates is being represented
(Figr:re 9). Ttris may explain d.iscrepancies shor,vn in other studies where
/
I2g
sone authors found linear relationships (Kern, Everson, De Mark et aI t9B1;
La Russo, Szczepanlk, Hofmann 1977; La Russo, Hoffinann, Hofmann et aI 1975;
Einarson, Grundy, Hardison 1979)while others showed them to be curvil-inear
(Lindblad, Lundholm, Schersten 1977; Wagner, Trotman, SoÌoway 1976) -
Gal-Lbl-adder volune fl-uctuated during infusion of both arnino acids and
Iiquid formula but large fluctuations (10-20m1) \^/ere seen only with arnino
acid infusion- Dr:ring the studlz bil-e from ttre gallbl-adder was often
e>çelled Ínto the duodenum to join the stream of hepatic bil-e. When this
occurs the measr:red secretional rate may not accurately determine the
hepatic secretion rate.
Faster small intestinal- transit increases the frequency of bile acid
recycJ-ing and increases bil-e r.iå ="".etion rates. In this study faster
intestinal transit occr:rred yith. Iiquid formula which resulted in greater
biliary lì-pid secretion rates.
Since subject 4 produced hydrogen in response to lactul-ose during liquid
formul-a infusion, the l-ack of increase in breath hydrogen during the arnino
acid infusion is most consistent with a markedly prolonged transit time.
However, there may be other explanations for the l-ack of hydrogen response.
The nasoduodenal tube may have slipped back into the stomach, the subject
may have been colonised with colonic bacteria incapable of making hydrogen
or this may represent day to day variation. Ttre first seems unlikely as
bj-Ie was continuously aspirated during the study and there was no drop in
secretion rate in the 4 hours after lactul-ose was given. The second is afso
unlikety as a dramatic change in colonic flora would have had to occr:r
within 1 week without the a&ninistration of drugs or antibiotics. The third
is extrenely unlikely as the day to day variations in transit tine neasured
r29
by this technique have been defjled and are rn:kìjmal (La Brooy, Male, Beavis
et at 1983), es¡:ecially with i¡rtraduodenal i¡rfusj-on of l-actu-lose (Bond and
Levitt, L977). Subject l, who had the biggest difference in gal-lbladder
emptying with the j¡lfusi-ons, had no change i¡r transit tilrÞ. Interestingly,
shre had a sna-l-ler increase i¡ bil-e acid secretion corgnred with thre rernaìning
subjects.
The more corplete gaJ-lbladder emptyilg and more rapid intestj¡ral transit
during liquid formul-a infusion are probably related to greater stjrrn:-l-us
for rel-ease of hr¡noral- mediators of gal-tbladder contraction and j¡rtestj¡a1
peristalsis. However it has been shov¡n that CCK can enfrìnce cholinergic
innvervation of the gal-J-bladder ( Foesel- and Sewj¡rg 7978 ) arìd therefore sqne
of the observed changes could be nediated by neurogenic ¡nthways. Pancreatic
potlpeptide reLease frcrn the pancreas paral.lels that of cholecystolcinin
and nrotilin (Floyd 1980; Keang,: DìMagno, Dozois et al- 1980), two hormones
thought to be responsibl-e for gallbJ-adder emptying and snall intesti¡al-
peristalsis. Reliable assays for the fatter two hormones were not available
but the two to threefol-d greater rise i¡l serum pancreatic pollpeptide i¡r four
of five subjects during tiquid formu-Ia i¡rfusion j¡tdicates greater hunoral.
stimul-ation.
Ttrese secretion studies h,ave shown that incornplete gallbladder emptyirg and
slower intestj¡ral- transit decrease the enterohe¡ntic cycling of bile acids
and j¡rcreases the nrolar percent cholestcrol of bile.
C. OROCAECAL TRANSIT T]]'IE IN PREGMNICY
FTqn thre secretion study reported here and from work by ottrers (Einanson,
Grundy, Hardison L979¡ Mok, Von Bergrnann, C.rundy 1977¡ Valdivieso, Pa-lrna,
¡üerr/i et aI 1919) it is apparent that snnl-I i¡ltestj¡ral tr¿rnsit tirre is an
irrçnrtant determj¡rant of the rate of cycling of biliarlr lipids and thus
,1
130
biliary lipid secretion rates.
In t.l-e first trjmester of pregnancy, an increase in bile acid pool size
without an increase in galtbladder vol-une has been previously reported
(Kern, Everson, De Mark et al IgSl). This pronpted the sequentia] study of
gastrointestinal transit in pregnancy to deterrnine if prolonged transit
ti¡ne coul-d e>çIain the expanded bil-e salt pool of the first tri¡nester of
pregnancy.
The data in this thesis has shov¡n that gastrointestinal transit is not
significantly prolonged in the first trimester of pregnancy. It is
prolonged in the second and third trimester and decreased postpartum,
approximating first trirnester valueé. Ttre postpartum fevels of progesterone
meas¡red in this study are conparabl-e to those occurring in the folÌicufar
phase of t-l-e ovulatory cycle. Likei,vise, the transit tinres of .wonen stud-ied
in the first trimester or postpartum period in this study are similar to
those observed in the folU-cutar phase of the ovulatory cycle or postpartum
by other groups usì-ng sjrnifar techniques (Wal-d, Van Thiel, Hoechstetter et
aI 1982; Wald, Van Thiel, Hoechstetter et al 19BI)
There is a threshold Ìevel of serum progesterone above which no further
prolongation of gastrointestinal transit occurs. The concordance between
studies of the relationship of smal-l intestinal transit and gallbladder
volume to progesterone levels suggests, but does not prove, that
progesterone may be the medj-ator of tJ.e alterations in motility observed in
pregnancy. Obviously, other hornrones, such as oestrogens, prolactin or
other hormones that increase during pregnancy, may correl-ate with the
observed changes j-n transit tinre and gall-bl-adder vof.ume. In addition
alterations in neuronal input rnay play a role in sore of the observed
changes.
i
131
r''bre recently Carride, Prokop, T?oncale et. aI l19B¡') studied s¡nall
intestinal transit scintigraphicalJ-y in healthy volunteers r+ith
99:r-technetir.rn-diethylenetrj-ar'rine i;en-ta acetic acid. Sublects ingeste-J the
scintigraphic solution v¡ith isosmotic Iactulose. The arrival of tfre
radionuclide label at the caecum correlated v¡eII rvitkr the rise in l¡reattt/
hydroc;en (r=.77 ) arld the transit ti.'res v¡ere sj-nil-ar for the scintigraphic
¡mtlrod (73 + 6.5 min; x +SEÞt) ancl ttre lactulose breath test (75.I + 8.3
rnin). Ino.ividr:al variations in snnl-l intestinal transit tj¡ne in Caride et
al's stucly r,rere si-gnificantly correlatecl vrith individual varia'tions in
Eastric en'çtyirrc;. Boncl and Levitt (i975) shov¡ed that indivicl-r:al varj-aticn
i:r sr¡atl intestinal t¡ansit. tùne, as fæasllrec1 by ilre l-aclulose hyclrogien
i¡reath test, coul-cÌ be siginificantly rectr-rced l:y infusing lactulose clirectÌy
into the ciuo.iem¡n via a transpylori-c tube. Ttrese findings sr-rggest that
smal-I intestinat transit tin" .r= measurecl by the factulose hrea-th test is
sic;rri-ficantly affecbed by the rate of gastric ernptying. I-Ior.rever, caution
is incicatecl before assurninq th,a'i transpl'le¡ic intul:al-ion is necessary for
acc;rate ìrêâsrrr(trrêrìt of srnall intesti:ral transit ti'ne. Di-fferences in
gastric mpLyi,rg are ual-:-kely to sicr,nificarrtlr.¡ affect the orocaecal transit
tj-rle rcsults j:-l tho first and second tri'ncs+-er of pregrnncl' aS liçti<i
elältying is not affected ity tÌre luteal phase of tÌre nrerrstruaf rycle or
preErna-ncy up to the second tri"nester (FtorowiLz, l.laddern, Clntterton <lt aI
1984i Schacie, Pe1el,:anos, I'ar-lxe et a.l 1984). Ilov¡ever as input of a rneal-
into the smal-l i:ov¡el is variable and ö,epends on the gastric anptying rate,
it is an advantage to quantitate both gastric ernptying and orooaecal
transit tjrne sinrultaneously. tÞlayed gastric ernptying is an unlik-ely car-r-se
of the prolonged gastrointestir¡al 'bra¡sit tj¡re occurring in late pregnancy
The delayecl transit ti-rne is prolxrJrly a result of prolongecl snall boi,vel
transit ti¡e due to inhibition of sma1l intestinal srx¡oth rrtuscle
LJ¿
contraction by fsriale steroid ho::aones, rost }il<-ely progesterone. Ilov¡ever ¿
neuronal effect of pregrnncy on orocaecal- transit car¡not be e-xcluC.ed.
I;r Brooy, i',la1e, Beavis et' al- (1983) have shov¡n t-hat the lactulose breath
test ca¡r be rade rTìore repraluci-ble by including a 1ic1uid. meal. They shovrer
t-nat variation in transit ti¡res betv¡een i¡dividuals v;as corrsiderable r¿ith
aII doses of lactulose ranging frorn 10 to 20gm (nean coefficient of 1
variation of 18.5 to 28.32 respectively). The addition of lactulose to aIiquid meal containi-ng carl:ohydrate, fat and, protej-n clesreased the
ooefficient of variation to 10t i-rr for-rr subjects studiecl. It is
therefore possiJole that I could have ìrnprovecl the r¡aria.bil-ity in pregnant
subjects by includjng a liquicl meal :rith the l-actulose close.
The ideal tecirnj-qrre to investiEa-ue intestinal transit shoula monitor tÌre
rrrcvenent of the liquicì or chlanous contenLs throuEh tlre lul-¡en ';¡j-thout
r-:.isturbing the phys-i-oJ-ogiôal- con-urol of gastr:ointestinal mo't-iIity. l,1ost
technic¡res used ¡e .-iuantitate transit tire to the caecuin have inadecluacies.
Tire use of barir¡'n as an ar-tificial ir,eal- to stucÌy sri'alI bolvef Lr¿r¡sit Ìras
-lÍn-i'tations ( j-n partic'uJ-ar in pr:e.;ri-nnc1' ) "encl tirc resufts cannot be
e;<'t-ra1rcJ-ateC to other rnea'ìs. Ìietncxls using non-absorJ:abl-e nüerkers l-ille
irolyethylene glyco1 (PiG) rec¡:ire Cre use of an intr¿rlr-r.ninal- Lr-rh: 'to
retrieve sarçJ-es frorn a given lccation in the intestine. this prcrìuces
stj¡:uli th,at are not '.rsually present a;rd cÂuses scme pa.tient disccxnfort.
i-Ìoi.rc:ver, the deter':rination of lrycrrogen in the i:reath after the ingestion of
Iactul-ose is non-j¡vasive. Tlre test does depencl on the presence of
bacteria in the large íntestine to riretabol-ise l-actulose. .P't l-east 5-t of
the ¡:opulation, however cannot met¿rl:rolise the sugar Ì:ecause they lacl< the
proper bacterial strains in the colon. llydrogen pro<luction rlay also be
re<luced because of lov¡ cofonic pll (Perman, l.lodlers, Olson 1981 ). It is
theoretically possibl-e tlrat a re.rluctio¡r in bicarbonate rich bile flory couli
J.JJ
Iead to a fall- in caec;tl ¡-rii i:esul'ting irl a Cecreasecl or even absent
i-ri'cit'crr* peal.., folloiving lactrilose ir:rqestion. .*ile flo.,v i¡r preçnancy' is
proì:aì:ly recuced and tiN: l:icar-l¡onate ccncen'ti'ation of bile Cecreasecl þr
cjilution. 'rlrese pertuÌ:atiol-rs .,¡ould l:eqxie nore pronounced as i)reqi),anc)'
pro:jiresses anCi r¡1ây e:ì?lain rihir scr,te ,iregrranL t¡cmen beccrne non-hyd:rogert
proclucers IaLe:: il p::egiranry.
/
I;ùrooir, ihle, B,-rvis e': al t19C3) ìravr¡ suggestecì that variations of srnall
bo..¡el- :no'i-ilitir in the fastec]. sta'te pi:oÞ.ì:J-y account for the relatively poor
rc¡-.i:oc1ucìì:ility of dre l-actul-ose breatll test j-n, or l:etrveen indiviCuals.
irio!,€vern their results ca¡¡ot be e>:t::a'.colated- to ¡:regnant r'nnen r'¡lrose
gastroi:rtest-inal- sr¡,coth n:-iscle is ',rncjer the influence of ccrlplex
neurohoi-rrcnal ciranges. Such varia.+;-i c.rr of orocaecal Lransit. tir.e in
i-,recj¡ancy has not i:een stuäreC. D:s¡rite 'lil.,ely individual varia,Ì¡ility' tlre
studies descz'iJred in tiris thes;is rr:r:e stil-'l- ai-¡le to dsnonstrate significant
seconcl ¿rnd ilirci tri-nester ilif ferences, Crre problern in interpreting breaiÌl
h)..irocjen cl,eril'ecl orocaecal Lransj-t tirr.e rneas,-rr€rireots is -th,at tire results
r-ir,, ìLo-u necessaril-r' relate tc ii-:e trinsit of focc 'Crro:Eh the sirall
ir:Lesti.ne. r-i-.,erefo::e it- i-s :i-n':or;¿lt 'to llo','r -if tl¡.e b::ea-dr Ìryiroç;eir '¡na,l'-
ccr;:clalcs,,¡iürilie tir.ic'Crat "thc ìrc¡r-ri oi: tl:e i:'.l]-i-' of the i;eal reaches the
caecll:r. if tlie ir-ltcial h;,cz'o_rel lral-. c,c-'cs ncìt correspoticl r'riLh iire heaci of
tirc r,leal r:cachj-:tg l-re cecc.r,i: i-!rc-u ¡r.:r:ireti;s i-eaìi þclrogeri excreLion r'ny ì:: a
nore precise niæ.sure of l'norri:h'to caecr:ii transit til.e. P-ead, i'iiles, Eisher
et aI (1930 ) cor{nrec'l tire ti:a;rsit t:i-i,r.e of an isotopicalty IaJ¡eIIeil ni><ecl
r,r¡al- rvj-th lrreatn hylrogen o:cretion in 14 trealtfrlz volunteers by estirratinE
raciicractiviLy over ijte caecun. 'IÌrcrc \'ras a Ìrighly siErr-ificernL correlaLion
treL',¿een tlre tj-r,c of the increase j-n r--¡rdj-oacti-vj-ty (t=.82i p < .001 ) over
tlre ca.cct-un ancl tlre tiine of ile seconc-ia-r1z incrr:ase in h1'd¡6gen olcretion
¡orocìr-rcecl Ìty ì-actulose feninn't¿r1-ion. n 9 ouL of 14 sujrjects, tìre seconcìar1z
i¡rcrease in Ìry,:ir.oçieir er:cr:etion occuri:eji al- the sanÌ.: ti¡le as the incre¿rse ill
.I-t'f
lrj
l-34
caecal radio¿rctivitlz sugt stjfì{j tj"at ¡neasüreri€nt of itre¿rth }ry-dro<;en is a
useí:ul- r,e'cl:oc-l to indicate r¡hen a rirell en"ters tlre colon. -[n 10 subjects tìte
rrEìxirr.¡r¡¡¡ coturt over tÌte caeç:un, coñ'ected for dec=y of i:ire is;oto¡-e, ¿¿j'tairreri
the level- of the initial g.astric counis suggesting tÌrat atl oi 'ijre i:'c¿rl
residue ,,./¿ìs present in the caecui¡L afLer f-assaie tlrrouEh i:he srnall
i¡rtestine, Ítere 'ivâ3 â Ìlighly sic;nifiærtt correlation (r = .66; ir < .01 )
i:et'¿een tlre tiri.e tirat the rileu{iJrrl]m concentra-tion of Ìly-clrocJen gas vIas /
excreteC in tlre lrrea-tÌr j¡r'rhese sui¡ects ¿Lno tlle tine that'clie rna::irutrt
a¡io-.ur-¡ of radicactivi-ty r.¡as recorCec-'ì- over the cêêcuÌ.ir. In 7 out of 10
stij-rjec'us, i¡ea,1i ìrydror;er-r excreLion occurreri a't ìj-re sarnei:j¡le as iÌre to'cal-
racic-.,aci:ivity l+as recortled over 'che caecl-:r,l an1 i:resur-r,tably inclj-ca'Leci tÌre
ti-irc ü.nt. aI-ì_ of LÌ:Le rneal resicÌue ira-s enierec- tfìe colotr.
:i,he close corresyrcnr,ì."n"" ùLo,=en caeca-l racioaciivity ancl ll.easurrerilent o-í
l¡reatir hyclror;err suggests Lini- tlre incr:ease in hyCiro,¡en e>''cretiot-t imy
incìicate the tine l,¡hen 'rhe heacì of the nreal- enters the caecum rvirile in at
leas'¿ 50% of the s;u:jects ¡:e;ù: hyc-ì-ræ;en excretion indicates ÌJle 1-ine ','iieir
iìie l'>t'lli of the rle¿.l entered- tl:'.e colon. If tlis is Lhe cese' Lhen-the-
ol¡ser-v¿itir:rr i-ira-t tirese t.^¡o i:i-l,es a,re closellr correl-ateti s'''r;4:orts t-'re i'ci:a
'L'raL l'iu.asu¿-rlr:nt- c¡f l-ìle increæ,:;e in Ì¡r'e¿L'tlr ili'i¡otatt exci:eti-on o;:ovide:; a-il
-ì-i'ic.Le< o-i iJie irensit ti¡,Le of -ehe ireail ¿l.s rvell as'Lire Lrull.: of t-ìre i¡cal .
iiov,cver, in viei..;, of tire reCeltt ciat¿r of i'trlagelac.;r, iìocnrtson, Srov;n et ¿rl
(198¿1) ì-his ol¡ser-.¡¿ltion is r¡-restior-rtbl.e. ri\r:cival of chyr,e j-nio tlre cofon
is infruencec:r' as :imch by tìre gastic anptizing ra'te as it is by i niestirr'ar
treursit, ¿ur¿[ can-¡ro't- be inCLivicìualise,i ]:y lieasr:ring the cu¡:nulative en'try oÍ
narker into the caecun. Isotopic neilrods for intestirnl transit ii¡ie lurve
several aclvantages over ]:re¿rtÌr hycìrcgen cstj¡rai-ions. The lactul-ose Cose
use.j for hyc-ircçj'en ìtrea'ch testing can cause dose de¡:errlent chang,es in
Earstrointestinal transit (LaBrcoy, liale, lleavis et aI 1983). 'Itre
,orocltiction of h1rlroç1err in the intestine is dependent on Lìre type of
III
¡
þ
_trtl
i
135
loacierial flora present. Tìre a:rpunt of non-absori:a:1e carbohl'olrette
iirgesteo 'úre cìay J:ej=ore tlte test i:J-us oral l:ncteri¿r can alter lrasal l-e'¿els
tÌ're follo,,+ilg iiay (P,eacr, I'iiles, Fis;her c:i al 1940, lttcritpson, O'jirien,
l..c(Þr:thiz eL aI 1979).
iligestibte fo:rj ld.¡eltecl rvi"ch a g¿urtro¿ì ernil-ting rilariier (eg 99"n Tc-egg)
ca¡u1ot -r(1easlìre transi'c tj:Lie of solicìs Lrecause the food carrier is i
hi.c'L::olyseiJ.. 'rhe <jevelopnent of 131 I la.oeltecl fibre by ifülagela<ìa'
ir..ol:ertsor-r, Bror.,m et aI (19S4) llas provic-le<i a useful- ¡rarker for stlxlil'- of
¡.ansl;ort of sr:Iic'l-s throug{rout ijle sriell ancl large l';ov;el . ':-'he use of o-r-ral
ciâi:riâ lal:elleii iLr¿'.rl<ers iras cie;äosLratecl. tint, unlil-'e -':lie sicraacil, tlle small-
L<¡1.¡etl crrr-x)s rìo't ciiscrirlina'b.e betr,¡æn iite solicl aurcì. Iir¡r'l.icl- ccrnponents of
ch¡r¡¡s. Ij: Ì:tiJr li'l¿r.rjlers are, J::gesteci- sj.u',ultaneously the lic¡rici ccrirDonent
cripties -i'¿rs;i-c:r j-rc¡i l-rre =tart¡,cri a¡rcr: arLives at- tire câe-clTrl firs't but liroür
soU-ci a:rr-j -lic-¡rrid. r.rarl.,ers ,¡awel a-Iong ìjre sr¡n-l I l¡o'"'lef at si:nilar s¡:necis -
li-hese resulis ',.¡c¡-rl-d suggest LÌrat ccntrary 1-o 'the conclusions of lìeacl-r
i,ilesrFislieretal(1980)'"Íirsi-a-r::iva-l"ofci'ryt':e'LotirecolonisnoLa
::ehaì-rle frrecr,ictojt oF tlte subse;1'.rent ti:ansit sTect::lrrr of the Ì¡ull-- oj= cÌr1zne
¿,¡ii' U,,:.:rr:fore tÌtc ìrldr<4en brea.t'lt test c¡sxlct bc u:;c'j- to i¡'nntif)'ijle
i;ans-r-'ì: 'i::ì:rx: oi -C:e 'cr-ri:ire i,c¿l} .
tle fiiniitr;s ir-r tÌris s;'c'-rd.y a-re con:;j-st.:nt i¡irir c¡'tlre¿'s'cuclies r';'Ìlicir:;Ìror"
c.:e3re:;sio¡loisitootÌrn-lsclccontractihLizÌ-ly'fcrivrÌei-torr'oncs'Tt-lgerreral'
prcçester:onc rcduceci cr¡ntractiJ-ity ',,.nile oestrcr;cn ir¿rs art o<citatori/ ei'Fect
on tÌ-le sðJrìc tissue. T'Lcse Íinitinçs suçEest uÌnt- tl-re pr:olongation of
gastroi:ttestj-nal. 't¡::ursi t cccurring j.n -l-atr: prcÐîan'ìc-v is a result cf iJre
i-r-rc:<ra¡;clì ¡;'ìrys io1,:1 j.c¿r I concentr:¿r'b-ion of prog'es-terone'
I1re a¡,¡nrent l¿tcl'- of pro:luction of lilrdt**"t in 0 of E first' I of 12
seconii, a¡ii 4 o:f 22 t\ird trinester sul-rjects l:E)z lf,f i:el-atcv-l to r¡nrlied
ÍII
i
þ
¡J1ü
136
prolongation of -transit. I:ad sarr.rples Tnen ta-l'.en for 6 or B hours, it is
pno¡ab1e that the hyclroEerr peal< lror-rld have ]reen c-,étectec. Ttre fincìirtEs that
al-l- stuclies r.¡ith laclt of trlrdro<¡en proil-uction occurreci in la-te pregnanq/
su¡4nrts tÌris j¡rterpretation. Horvever, LaB'rooy, i:iAle, Ëeavis et al (1983)
have cle¡ronstrated that lcn¡ hydrogen producers on occasions excreted no
hydrog^¡ at all in expirecl air after lactulose. This fincìi-ng indicates
that scxne subjects are occasiornl non-proclucers of hydrcr;en. rhis could /æ
iæcause tlrey krarbour onry snarl mrnÏ:ers of hydroge*n - prociucing bacteria in
the col-on, which, lvith the norrnal shifts of ba.cterial flora, beccme
depleted at tj:-¡es.
;ìlürough it is unlikel-y, Iacl< of hycrrcael proc'ì.uction nay also be cltto to
pr:egineriqy-irclucecl ch.anges in colonic ]:acteria. Breaui hyCiroEen irrccluction
is tlre net resulb of hydrog¡err proclucLion ancì. iri'Ctogsn cc,nsui:ilrtion }ry
colonic l:acteria. Since hirc-,rogen coirsulincì ¡act¿:ria. e;<ist (I-€Vitt'
Uastings, Berggrol 1974) it is possible l-jrat preqnancy indttces a ch,arrgie i-n
colonic ba-cteria favor:-rinq hl4irogen consurip'tion over hydì-roc;etl ¡:'i'cr-uction.
Ilor..rever, tlrere aïe nc oç;'eriraenLlt cleta. to ei tircr rc-fu"e ol: sl-lilÐor-t iìis
Ìriz¡rcth.esis. rf cita'r;es in colonic fl-ora cc.-rlr::ry:r iir.r:::e¡rla¡:c1i, 1ieen'tite
absence of i-re¿r{h irlzdror*. at 2/:0 ilin ryoulcl l;: CiiÍficurlt- i:c rntclri;ret.
fnis stuiV and. ¡revious stuclies of Eal-Iblaäõ.e:: ft':rction in pregnanL r'¡cxircrt
suggest bhat cira¡rges in orocaecal ü:ansit or ç;aÌ1i:IailCr:r .¡oltune c¿¡ru:ot
account for the obsen¡erf increase in bile aci.j i:col size tha.t occurs in
early pregrnncy. ir-Ìrus, t-lre increase in ]:ile acic pooJ- r.rzrlz bo relatecl to a
direct effect of fe¡nre horn¡cnes u¡nn the Ìrepai:ic syn'thesì-s of bil-e acic-ls'
D. GAS'IT{TC lll,Ð GA]:.J,EI,Ai-ìLìIIP, EI'IFTIYIÌ{G
I
Ì
The finding of cieJ-ayecì and ìlcrcrnplete gallblaclder enptying in p::egrnncy
r37
after a rnixed solid liquid nreal could have resulted frcrn impairecl gastric
ernptying of solicls resulting in cliministred'neurohn¡r¡oral stj¡auti fron the
upper jejgnum. ttrenefore it was inportant to study stornach anrl gallbladder
simultar¡eor.rsly after a si¡nilar neal. In tÌÞ pnesent studlz it tns bee¡r
shov¡n Ulat, after ingestion of a st¿ndard neaÌ containjng 40es of. calories
as fat, the sc,cond slovr phrase of galllaclder ønptying ruas related to gastric
erçtying of solids. callbladder refilling @an v¡hen 138 of solids '1
rernai¡red in tlre stcrnach. Ttris suggests that the concentration of fat and
protein that enters the intestiral h¡nen after 50 min is probably
i¡sufiicient to fully stùrn:late i¡rtesti¡al or pancreatic honnones, or botl]
and naintain gallbladder contraction. Support for this is the drop to
baseli¡e serum I-IpP levels at the tinre r^¡hen 138 of sol-ids rsnained in the
stonach. The initial rapid rate of gaì-Ibladder erptying lray represent rragal
ùne::¡ation. Èoct., tia1rTrud; Fisher (1981 ) have shor^¡n that stra'n feeCing can
resul-t in erptyilg of 50e¿.of gallbladder voh¡ne. Tn addition atropile
allov¡s the gallbladcler to acccnnrodate larger i¡fused volures (Schoetz, La
t,trrte, Vlise et aI 1981 ). Therefore contj:ruei vagal simu-l-ation could play a
r"ole i¡ ¡rnj¡tai¡ing tìre gallbladcler crcntracteC post pnandially.
Si¡rce colrnencing tl-ris study it has been shov¡n tllat gastric elçtying is
biphr,asic v¡ith an early "Iag" pLr,ase being dsnonstrated if crcunting conti¡ues
tLrroughout the nreal. This lag phase is variable rvith a me¿ux of around 20
nún (61lins, IiorortlLz, Cool< et aI 1983). As 15 min v¡as alloi'¡ed for
i¡gestion of the test nieal this lag phase was not ds¡ronstrated. The gastric
enptying studies in this thesis were ¡ærfonned r¿itlt a ¡nsterior camera to
allor,¡ abdcrnirnl- ultrasor:¡d to be performed anteriorly. Alc]<ernans, Jacrcbs,
Srout et aI ( 19S4 ) usi¡rg a similar sized nreal slror¡¡ed that in enptying
curves obtained frsn a caflera posterior to the subject, a lag phase could
not be distingrished. In tlreir studies tlre geanetric nean of bottt
anteriorly and posteriorly obtainerl cr:rves shor'¡ed tl-re laqr prhase cloarly.
138
Hcrvlever, usirig a bran fabelled meal Ba;<terrGrirer'fritchley et al (1985)
'failed to stpr,r, a lag pLrase using an anteridr canera vrhich according to the
studies of Aklcernans, Jaoobs, Srr{rt et aI (1984) shoul-d strov¡ an exaggeratecl
lag,$rase. Malagelada, P,obertson, hcovrn et aI (1984) initially shou¡ed a lag
phase in only 2 an&- of 6 tealtlry patients using labelled bnan and an
anterior camera. Later sh¡dies nþre ænsistently denr¡nstraÈed duat prases
(Calnill-eri, Borol.n, l4alagelada 1986). It dæs seern like1y that by using/
cr-rJ-y one canera an "early erçtying" phase can be arbificially introduced.
IIohever, Akl<ernans, Jaæbs, Srrr¡t et aI (1984) have shoçvn by a dual-headed
cainera teckyrigue that after gastric enqltyjxg actr.rally begins, gastric
ernptyi:lg rates neasr:red by tlre two cameras are parallel. Therefore, tlre
assessn¡ent of the slope of the post lag solid anptying pbase is not int¡al-id
usjng one caflìera brt where ¡rossible tlre gecnetric nean of gastric ernptying
should have been used. '' :
Tlrere are cbvic¡¡sJ-y several potential j¡raccuracies that rnay reduce the
sensitj-vity ancl specificity of gastric ernptying tests using radionuclides.
These pnoblems nray relate to the instn¡nents, the types of Ia-i:ellec1 solids
and tlre constitrrents of ineal-s, the arntcrny of the patients studiecl,
analysis of gastric enptying data and tlre plrysical properties of the
raclionuclides thenrselves. For exanple, an fuqrortant guestion of the stìrdy
reported lrere is vùether tlre radiqruclicle r.rixed witkr the scrarnbì-ed egg
re¡nains bound with extracellular or intracellular fat. tr'byer, l4ayer, Jehn
et aI (1986) have rec-ently shcn^n tlnt nrost of tlre jntrac-elluÌar fat ernpties
with the solicl food phase rvhereas nost of the o<tracellul-ar fat enpties as
an oil phase. Iìor,everr. both intrac.'ellular and extracellualr fat appear to
leave the stqnach at the same rate. It is also uncertain as to hov¡ rmrch of
ttre tectunetiun label is bourd to fat and hov¡ rm¡ch is bourd to pnotein and
vrùrether ttris is inportant, ín interpreting the gastric ønptying results.
139
Ttris stucþ also shows th¡at tonic aal-lbladcler crcntraction is maintained for
4 hor¡rs after the starda:rd breal<fast. This explains the " flat "
gallbladder voltrne cr.ua/e obsenzecl i¡r earlier studies vùrere regular meals
rvere eaten at 3.5 to 5.0 hourly intenzals
Unfortunately a reliable raclioj¡rnrnrnoasay for HPP but not. for CtK or /
no'tilinrvras ørly available at the tjme of performance of these studies. The
ËlPP response \,,,as biphasic, as reported. ÍIPP levels dropi:ed to Ï¡asal valt',es
at approxi-rnately the time of initiation of gallblacicler refilling a¡d dicl
not increase suÌ:secluently¡ suggesting tirat tonic gaJ-Ibladder contraction is
rrraintained by huriroral stjmulation in response to gastric erçtying of
solicls. In acldition, IIPP, scnetimes referred to as "ãnticholecystokinin!:
horrnone" (Sarles, Flage, Iau$ier et aI 19791 is not res¡nnsible for
gal-IbJ-adcier refilling after ingestion of a meal. C,alIblac1c1er refilling is
rx¡st likely a ¡:a-ssive process which occurs when ernptyìng is no longer
sti¡iulated-.
,'rrr interesting ol¡servation i,yhicìr cìeserves iurrtjrer investiga'tion, is ijre
ti.,'ofoliì slov.rer GlIr' irr inenstruating w,rr,en cont5n-reci to nten. As v¡crnen t'¡ere
rreirstn-rai-ilg at .Lire ti¡re of the stucþ it is 1:oss-ì-bì-e Lllat nenstr-ua.I
sym¡rtcrns strppressed rnotility thrrough a central ntech¿msnt.
r¡lb.Idr Van Thiel, Fioechstetter et al 1981 reported. tllat GIT in r'¡cnren is
prolongecl in the luteal phase of the ovulatory rycle presunably because of
the inqreased ]evel- of .progesterone. Iracl subjects in the luteal phase of
the ovulatory rycle been sbrdied it could be anticipated tl¡at the
difference i¡r GIT betv¡een nen and hrcren could have been even greater.
It is conch¡ded ttrat gastric ernptying of the sofid porLion of a meaL
.[
140
containing fat induces and majntains tonic gallbladder contracti-on,
probably throtrgh conti¡rued releasê of hr¡¡oral mediators, frcrn small bovrel
and pancreas. Vlhen gastric anptying is co'nplete, hr.unoral- sti¡rmlation ceases
arrd the garlbradder refilrs. Ttris gestro-biliary integration herps naintain
rnixing of bile acids with ingested fat for optirnal fat ingestion,and
absorption. AlÈered gallbladder enptying rnay be secrcndary to altered
gastric enptying. - /
.,¡
u-'rÈI
i
i
I
{t'
NII
I
t
T4T
CHAPTER V
CLINICAL IMPLICATIONS OF ALTERED GALLBLADDER EMPTYING
AND BILIARY LIPID SECRETION IN PREGNANCY
A. THE ROLE OF MONNING SICKNESS
Clinical feabures of morning sickness
Diet and cholesteroì- gallstone formatj-on
B. THE POTENTIAL RELATIONSHIP OF DISEASES OF THE
ALIMENTARY SYSTEM TO ALTERATION IN BILIARY
LIPIDS IN PREGNANCY
I{rcosal protpcti,re effeöts of bil-iary cholesterol
(i)(ii )
(i)
(ii)
(iii)
ûhoJ-ecystitis in pregnancy
Reflux -oesoþhâgitis and peptic ulcer di-sease
T
I
t
t!
,ir¡l
I i .: i-.r *$: .:.,,;, '..lli;,,..¡¡,.-.;ii ;ns#S+*N,1iffi'+ffiAng' ]
r42
g,INICãL ]]..IPLICATICb]S OF ÀLTRÐ GAI;LBT,ADDER BIVIHTYING Æ{D BILIAPJ LTPID
SECRSMCTT TN PREG'IA}']CY
A. TÍIB ROI,tr OF IqSRNING SIC]TVESS
(i) Clinical features of norni¡g sickness
Pregrnncy v¡itkr its attendant physical horrnor¡al and physiologì-c aÌterations,
significantly affects the functj-oning of the gnrt at many leve1s. It
displaces stsnach and srnall- j¡ltestine and mobilises portions of the colon
frcnl thei-r custcrnary anatcxnic l-ocations; it alters irxrtility of oesopiragus'
stcxnach, srrrall i¡rtestine, colon and biliary tree; it irnpairs appropriate
furrctionÍng of the l-ov¡er oesopf,agdt sphincter; it decreases gas'cric
acidity; it is associated rvitLr ch,anges j¡r the selecti"¡e absor¡rtion
mechanisrn of snal-l- intestine and. col-on and probably in pancreatic secretion
as l'¿el-l- and it at'tenuates tire bod-y's response to such crises as
inflanrnati on, perforation and obstruction.
Ì.Lausea, with or ivitlrout vorniting is a ccnrnon, suggestively cliagii-rostic, sel-f
Iimiting slnnpton of ezrrly pregrìa-ncy. In its nxcst j¡nocous forrn j-t is
"mornilrg sickness" oçeriencect as nausea by as Íìany as 50eu and as vcr.riting
by appr:oxiinately 30% of \¡¡Gnen during their first trimester (FainveaLlrer
1968; ScLrer 1965). Both tlrese conditions generally arise during the first
12-'14 v¡eeks of pregnanry. It i; felt furpically u¡nn arising often before
any food has béen ingestecl. It nay persist at 14 weeks in as many as 40e;,
Ìry 16 v¡eelcs in less than 20% ancl by 20 r^¡eel<s in less than 10S (Diggory arrl
Tbrnl<i¡rson 19621.
:lN!r¡
tII
¡
!
l-¡* J
In morning sicÌ<ness, no specific,gastrointestj¡ral l-esion hâs been
denxrnstrated. I..lzrry theories have been advanced. Ttre literature h,as
centred on four general areas; allergy to ¡rrtative placental or serninal
toxins (none isolated); alteration in ga.strointestinal motility (no good
correlatj-on dsnonstratecl); lrormonal ey.cesses or deficiences acting dírectly
on the gut or on the central nervous system (poor correlation beb¡¡een
hormonal titres and clinical symptcnrs: Soules 1980); and psyctroscrnatic
factors (no correlation between vcrniting and personality profil-es::Palmer
19731. Ttre changes in orocaecal transit tjrne and gallbladder ernptying occurr:ed
in late pregnancy arrd no chanEes in Eastric enpting have been denons'urated
in the first trimester. frrerefore, it is r¡niil<ely tliat rnotility
clisturbances j-nduceC. by pregnan.y *l explain tlre slzrnptcrns of nrcrning
sici,,ness.?r central cause for r,orrring:sicktress seems rrore like1y ancl the
clecreasecl inciclence of severe vcxniti:rg in recent years ha-s been linl<ed to a
npre relaxed aititucle to pregnanal;'availabil-ity of aborLion and birth
control, as v¡eII as less restrictive obstetrical attitudes and regimes
(Jacdcs and Janor'tlLz 1965).
ii ) Diet. arrd clrolester':I qallstone fomation
Several studi es lrave sÌror,¡-r a¡r i¡lcrease in chol-esterol saturation of hurnart
hepa.tic and gallbì-adder bile after an eight to 16 hour fast (t,ietzcJer I
êdler, Heymsfield et aI 1973i I'lilliarns, Þlcrse, lncnornld et aI 1977; l3Ioch,
Thorntcn, Fleaton 1980). FastinE j-s associatecl rvith the storage of a part of
the bile-acid pool j¡r the gallblaclder, a clecrease i:r the rate of biliarl¿
bile-acicl secretion, vrithout paialleJ- diminution in the biliary secretion
of chotesterol and the lrepa.tic production and secretion of su¡:ersa'turatecl
biLe. Ttris effect rnight l:e accentuated by previous bile-acicl deficiency or
Ð(cess cLrolesterol secretion or both. I'/hile high cholesterol intak'e (Lten
Besten, Connor, BeIl 1973) and ovemeight appear to play an Jmportant role
I
in galtstone fo::nation, short term, Iov¡ calorie cliets Con't appear to
effert bilian¿ cholesterol saturation (Schlierf, Schellenlcerg, Stehl et aI
1981 ).In addition, prolonged fasting, gireater tÌtan 16 hours significantl-y
decrease bile litJ:ogenicity. Ttrerefore if nornirtg sicJ<ness plays a rol-e in
gallstone formation it is unlikely to be through an effect on total
caloric intal<e alone, reducing gallbladder erptying. A lrþre likely
gallstone risk factor frcrn rrprning sickness is the effecbs of nreal tlpe and
meal frequency on gallbladder erçtying. Ttre importance of gallbladcler
ernptyilg in the fornation of gallstones v¡as dsnonstratecì by llessing,
Bories, ltunstlinger et al- (1983). They showed ttrat patients fed þr total
larenteral nutrition for 6 v¡eel<s developed biliary stasis ancl gallstones.
Vlnile it is unlikely that v.rcrnen r¡ith. n"orning sicJ<ness woul-d undergo
pu:olongecl fastìlg, meal frec¡:ency i-s 1i}<ely to l¡e recluced, Capron,
Delarnere, Eev-ve et a1 (1981 ) studiecl 115 patients with radiolucent
gal-Istones. ltre cluration of fastìng r'/a-s neasured frcrn the end of the l-ast
meal of the cr,ay until the beginning of the next neal (bre¿l<fast or lunch).
In the youngest patie-nts (20-35 years) the dr:ration of overnight fast-ing
r¡as sig'rlifj-cantly longer in bhe ¡:atients vrith gallstones tiran in aEe ani
se>< matcheci controls.
Therefore, in pregrnncy prol-ongecl o-zatn-ight fasting in the first trinester
dne to rnorning sickness coul.f contriJ¡ute to other risk factors for
gallstone formation by jrcreasing cholesterol saturation of Ì¡ile and
reducing gallbladder enptying.
/ln alterrntive e>çJ-anation for a ç;ossible role of norning sickness i-n
chol-esterol gallstone fornutj-on'may be'via a change in dietarlr prefeg nce
r,ririch might increase biliary cJ:olesterol saturation. A beneficial- effect
of v¡treat fibre, in the form of bran, on the chrolesterol satr:ration of bile
lras Leen obselvetl by rnost (Porrare, IJeaton, IÐv/-B€€r- et aI 1976¡ i".bDougall,
Yalqzmyshyn, VIaIJ<er et aI 1978¡ l^Iatts, Jablonski, Toouli 19781 but not all
/
145
\,'¡orkers (Tarpila, Ì'liettinen, Lfe-tsaranta 1978). This decrease i¡r biliary
cholesterol- saturation v¡ith dietary fibre is obsen¡ed only l^dren the bile is
initially supersaturated. Therefore lack of dietary fibre crculcl be
res¡>onsJ-ble for sqne of the bil-iary lipid changes in pregnanqy.
Orr epideniological and e4perjnrental grcurds, Heaton (1973) postulated th,at
the consurnption of refined carbohydrates (]¡etter dessibed as fj-bre
depleterl foods) favours tLre secretion of bile supersaturateC with
cholesterol and hence i¡rcreases the risk of gaLlstones. This h1n:othesis
iras rore recently been supported Ì:y the e,-,tensive epidoiriol-ogical study of
Scragg, i¡Ici,lichael anct Searnarl< (1984). ft Lns al-so been argiued tb,at the
rnture of refinecl foods, especialÌy refined sugars, is such that they
inevi'Eably inflate the intal<e of energy. Ttrornton, lfunett and Hea.ton
(19S3) sho..vecl that. a Ciet rich irr r:"iirr.o carbohydrate resulted i¡r
Eal-Ibladder bil-e i¡eing more saturatecl l+ith cholesteroi "crni-rutn
i v¡ith a diet
erxcluding refined foocls. i{ovreverr'tåe refined cliet contained nnrch l-ess
fibre. i'ierner, Enn'rett, arrd Heaton (1984) showed no effect of a si;< ',.¡eeli ac-l
libitun ãiet' supplernentecl with refined sucrose, on the clrolesterol
saLuration irrler,r of fasting gallblaCder bile or bili-arty tipid secretioir
ra-tes. 'Ihese rece¡rt results suggestei 'EhaL a refined. diet is ¡xrthø9-enic
onllr in as ir-rch as it. is ck:ficient in cii-e-uar-1' fibre. I-lo\'/ever, as tÌre Ìrigìr
sr-lcr-ose ciiet adverselir affecteC ¡:Iasnra lipicls, it is ¡lossible that in thc
long tenn, it night j¡rcrease the risl., of gallstones. Irs prergne.ncy
progiresses past tJ:e first trimester, !./crren are inore likely to se'ek high
fibre foals to counteract j.nrpendilg constipation. Flo\orever, in the first
trj¡Llester nalrsea nray mal<e pregnant r,/crTen ai¡oid tlre bloating and abdoninal
disccrnfort of unrefinecl carrbohyclrates fuhich could then leacl to an increased
risk of gallstone forrnation as a result of j:rcreased bitiary lipid
secret,ion
,1
The above results suggiest tlnt certain cliets n'ny predispose to biliarl
r46
clrolesterol saturation. The nech,a¡rism rnay be via biliary cholesterol
saturation of tbrrough jrnpaired gallbladder eaptying. Data in útapter TïI
h,as skrorvn tlnt amlno acids are less potent than a rnjxed liquricl forrm.rla j¡r
aausing gallbladder ønptlzing. Gallbladder enptyi¡g in hrrrnn strk¡ects Lr,as
also been studied after meals of differerrt ccrnposition (Rocl<, l'{alrrud,
Fisher 1981 ). Gallbladder anptying after a rnixeC. solid nreal i s decreased
significantty conpared to a lic¡rid nreal for 75 mins after neal ingestion.
By 90 nrin, tLre maxi¡ral gallbladder ernptying responses are sjmilar. The
rnxi¡nal gal-Ibladcler erptying responses to 5% ancl 50sø glucose ancl to amino
acids are similar l¡:t all are less tha-n the rnaxi¡ra1 response to a rilixed
IiqLlici rneal. Therefore, galllcladder ernptying is affecbed by the physical
ancì che¡aical ccxnposition of ingested- nreals anci arry chanEe il dietary
preference could resul-t in altered- 1and scxnetinres inccriplete gallbladd.er
enptying. Ttre subsequent biJ-iary stasis coulcl preCispose to galtstone
form¿rtion
B. THE POIIT.'rI'IAL PJ{,AIIOdS;I]P OF DISAASES OF 'IIf,I ALIÌ'[XÍ'I!]FJ SYSlE.i TO
ÀLIELÌ\TIG'] ]f{ B[.IAl']J LIPIÐS l,i PF-t-rGl?il(a-
(i) liucosal protective ei-i'ects of bi.liarl' cÌroleste.r:c¡l-
In e,-lcerirnental anin'als, bile salts have caused dari',age to tÌre sr¡all and
Iarge intestine, stcmach a'rd gal-lÌ:l-acider and in rnan they have beeu
irnplicatect in the pathogenesis o'F several gaslrointestir¡,al inflan'rnatory
states such as gasbric ulcer ancì oesophagitis.
The rn:cosa of the gallbladder, ocso¡:hagus, stcrnach and cìuodenun are
presentecl ¡,.¡irrr* the problon of a potentially injurious solution of harmful
bile salts whiclr are povJerful cletergents able l-o peneLraLe lipicl bilayers
and at high concentrations solubilise rTemlcrane phosplrolipids ultùnately
L+t
causing nrsrbrane cìamage.
As ¡.¡el,l- as represeniilg an exeetory substance, drolesterol rnay also have
an i:nportant fi:nstion in bile (together rvith plrospholipids) of preverrtìng
the darnaging effects of bile salts on the biliary and j¡ltestinal
epittrelir-un. Bile salts placecl in the canine galJ.blaCder cause haerorrhagic
drolecystitis but tkre onset of inflalmration can be delayed by addhg
cholesterol (Riegel, Pørvdil, Johnston 1931 ), F\rrther evidence for the
pnotective effect of biliary cholesierol ccrips fron a studlz on the effects
of dihyCroxy bile acids on the hr¡nan jejr:m:rn (Broor, Slota, Àn¡ipn 19e0).
It v¡as sho',.in that bile salts induced secretion of v¡ater and electrolytes
into thre intestinal h¡nen (as opposed io the norn'a1 absorption of v¡ater a-rrl
electrolytes) but tlrat this effect coul-d be bl-ocl-,ed. by adCing cholesterol
to the bile salt solutions. 'ihese observations suggest thrat biliary
cholesterol has a role in preventinb Life salt j¡rducecl nmcosal damage.
Bi1iary su¡:ersaturation by cholesterol in fasting and preçnanry may protect
the biliarl¿ ancl- j¡testinal- epihreliul frcin the toxic effects of bile
sal-ts.
(ii ) drolecl-stitis j-n pregnar-rcy
Despite the prior evidence tLr,at pre¡rnnclz preclisposes to gallstones, the
incidence of cholerystitis is Iow, around .02- .078 (Sparlcnan 1957; lIam1i:r,
Eartlett, Smith 1951 ). This does noL exceed the rate in non-pregnant r"/cmen
of the same age Troup and in faét, parity ancl age clo not influence ttre
occurence of sltmptons.
It is frosslble agaln tiut clrolesterol Ìras a protectlve actlon and desplte
significant gallbladder stasis clrolesterol crystal-s and epithelial- damage
'1
148
are not rore likely to occur. Ttrere are several pnssible oçIanations for
this apparent protective action. One possibility is th,at bile sal-ts are
bound to cLrolesterol- and plrosphotipids by liçophilic association within
miv,ed rn-icelles and are therefore less able to r<-rct r'¡ith ihe epitheliurn
along v¡hich they are bei¡g transpori:ecl. Another is th,at absorption of
cholesterol by the gallbladder an¡1 incorporation j¡¡to mernbranes, alters tlre
cellular phl¡siolog)a and norphology of the biliarlr epitheliurn.
(iii) Refh:x oesophagitis and peptj-c ul-cer disease
iYoaclly clefined, reflux oesophagitis is the constellation of slroptons
and/or cÐnsequences to the oesophaçrs i'¡hicir result frcre contact of gastri c
or intestinal contacts r,./i1jr the oespptngeal rimcosa. Reflux oesophagj-tis
leads to Lhe substernal ì:urnìreg disccxnfort of heartburn. rhis slzmptcrn has
been reported in 30-70? of pregnancies, occuring daily i¡r as nnrry as 25e;
(A'tlay, Gillison, Iiorton 1973; ltrebel , Irornes, Castell 1976'). Onset is
usually in ijre seconcl trinester aurcl frec¡uency ancl ìntensity often escalates
a-s tire pregrìarìcy proceeds, only to vanisli a-fter delivery. Ir-lI pregnanl,
v¡crûen, irres¡:ective of hea,r-ubun-r syrnç:tcxirs, tend to exhibit nrore
non-propul-sive rrotor activitl' of Lhe oesoirir.egus l¡iLh clecreasal i"rave
anplitud.e ¿urd. sl-o.,ver ireristal-Lic qrcccì (i'i.agler and Spi-ro 1951 ).
Àlthough a source of discqnfort, heartl¡urn is usually not a serious
s¡anptor. Pe¡rtic oesophageal stricture in pregnancy is rare (Swirùroe,
ûoclrrane, tíisharb 1981 ), as is L¡ae¡norrhagic oesophagitis.
Patients rvith reflux ancl regurgitation often cqrr'lent tlnt the fluid tastes
l:itter ratler tlran sour and is ye1low or green in colour due to the
Ifresënce of cluoclerlal- contents. It h¿rs been knov¡n for scle tj.lre tlraL Ì:ilt:
salts in concentrations for:nd in gastric contents will cause perreabiJ-ity
"1
r49
cha:eges in 'the oesoph,agearl nn-rcosa (Safaie-ShLrazi, DenEesten, Z:tJ<e 1975,1.
l'he lack of severe ccrnplications of reflu.x oescphagitis in pregnancy could-
be due to increased binding of bile salts as a resulb of a relative e]<cess
of biliary chol-esterol. In addition, bile salts are irore likely to be
ciilutecl out in gallJrladder bile and 1m¡:aired gallblaclder erptying rray lead
to less bile salts enterilg the duodenur¿ at any one ti¡re point.
Sìrnilarly to oesophageal disease, the ccxnpJ-icatj-ons of peptic ulcer ciiseasr:
are rare in pregnancy. In fact, peptic ulcer disease itself is distincLly
rare in pregr-rancy (Sandr,¡eissn Poclo1slry, Saì-tz:rtein l9¿¡3) vriih tìrc condifion
terx-iinç¡ to :ir'tprove slzn:ptcxi-atically in at leas't 80eà of cases as pre/jnanc)¡
Ì)rf,Ð.resses (Clark 1953). Ttp rarity of tire concli'ticn ar-rcl- its ì-r-.,r¡:rovernent
during pregnancy have been linl-,ed to crjminished. gastric aciclity a-nd 'che
irealingr effects of oestra;en. iloryever, it is ¡rossible 'ijrat the <ia,rnaging
efects of reflu,-,ed bile acicls rr-Ely l:e reduce+ì by ililution and Lhe presence
of greater ar.punts of biliary cholesterol.
I
CHAPTER VI:
150
FINAL DISCUSSION
151
FINAL D]SCUSSTON
Chapter III of this study has ' shown that biliary lipid secretion
rates are dependent on stimulation of gallbladder enptying and small
intestinal transit. Re¡rcrted differences in flrean secretion rates between
groups of subjects fron different studies or between different groups of
subjects within the same study may be due to differences in stinmlation of
gallbladder enrptying and intestinal transit. Monitoring gal-lbladder
enptying and intestinal transit during biÌiary U-pid secretion studies is
inportant for the i-nterpretation of results. fn addition in healthy
individuals gal-Ibladder enptying and small intestinal transit affect
biliarlz lipid conposition. I ,
Tn the control- group of women studied by ultrasound aftêr a rnixed nreal the
initial rate of gallbladder errptying after breakfast was approximately 40?
of that previously reported using a smal-1 volume liquid meal (Braverman,
Johnson, Kern t9B0). The tiquid meal contained 520 cal- (35% faL, I2Z
protein). Increasing the volume, fat and amount of sol-id in a meal sfows
the enptying of both liquids and solids from the stomach (Moore, ChrÍ-stian'
Coleman L9B1; Malagelada 1917, Moberg and Carlberger 1974, Kroopr Long,
A-lavi et al- 1979, Cortot, PhiJ-lips, Malagelada l-981). Thê results of
studying gastric and gallbladder emptying sjmul-taneously suggest that the
J-arge volume high fat, rnixed solid liquid meal described probably enptied
slowIy frorn the stomach, reducing the rate of release of neurohunroral
mediators of gallbladder contraction from the upper smal-l- bowel and
pancreas, and resul-ted in the slower rate of galJ-bladder enptying.
Different rates of gastric enptying of liquids and sol-ids may have caused
the two phases of gallbladder enptying observed in this study, although
. r52
vagal- i¡rren¡ation could also e>.¡plain tlre initial rapid phase and contribute
to prolongec-l galJ-bl-acid-er contraction.
ttris study has sho,l.n tiiat gatlbladder refilling C.oes not occur until 6-7
hours after breal<fast alone and that this long pe::iocl of tonic ga-Ilbladder
contraction (or IaC< of gallbtadder refilling) is related to slorv enptyirtg;
of sol-ids from the stornach.Eecause nteals i,/ere ingested at 3-5 hour /j¡tervals i:y ..^¡6r*tr in the control group the galli:laclder dic- not refill..
this al so accornts for the cl-ose agireerent of resiclual and hourly voluiircs
i.e, tire s:¡allest galJ-Ì:1ac-lder volu¡*e a-chievec'l after l-rreal:fast approxir.rated
{-he gal-lblac-ìder volume for tlie resb of tJre daiz.
'Ilrc lacli of si.gnifica:-rt gallbladder refilling before ancl after -ure noon anC
evening meal-s in atl grou.os væ.s due to tire ccrnpositi-on anc-l frequencl' of
irlgestion of tl:e rneais. t
In arf.lition to the chnnges observed in gallbladcier enptyirtg,
ga-strointestinal transit tirne is p::olonge<j- ín late pregnanc)¡- It d-ecreases
;:os-i-partu:n to the level previously re¡:orte,f for Lhe follicul-ar phase of tÌre
o..-ulai:ory ryc1e. ,9ottr oroc¿recaf transit tiirie a:,rd serurL ¡trogos-terone levels
rise ;,.roçiressively Jretrreen prog'esterorre lc.¡s1s or 0 to iìOnç;/r:rl , -1'his Cior:s
not a*<cl-uc1e, holever, the possiiril-ity Lii;ri- c'tìrer hon:ones or neuronal
clturges ¡-rod-uced ciuri:r.-J pr:egnanc)¡ rnigïtt r:cr.iiate 'anescl effccts. Tt ¿ri¡. ¿'rs
tl:¿lì: r-l-re increased bile acid pool s-ize occu'rring in earrly prcrJnallcl is not
seconclary to sequestration of bile aci Cfi ei'ïlrer .,.¡j-tirin ga1-ll:J-ai,öer or smal I
intestine. Insteacì the increaseC irile acicl ¡:coJ- is proì:erbly a clirect
r.e-t¿bolic or lrorrrtonal effect on bile acici. sintSresis.
I5J
-t-"he effects on bilia-z-y' lipid secretion anC gall-bladdler function seen cltiring
pre?i-lancy v.'ere not reprsluceil in post menoinusal r,¡cr¿en tal.-ing cirronic :
oestrogten therapy. Ilovrever, the results are appU-c.l'-:1e only to tle doses of
oestrogen usecl in this stucþ. The other studies re¡:orted here i:',tplicate
progesterone as tlre rost l-il<eJ-y honrone to be causing C,isttubance of
biliary tipici secretion and snrooth rmscle fi¡:ction jn the Eal-Ibladder ancl
gasi=ointestinal tract.
'Ihe stucr,ies descrj-T¡erf in this thesis strongllr support a Sratlrog-enetic role
for gal-Iìcl-aclder sLasis in ga.J-Ìstone fornntion.I?-ecent observations frc¡r
aninal studies supçorb this hypothesis. The prairie cioE is a relativeli'
EoorJ anirnal rnociel for studying certain as¡;ects of cholesterol gallstone
fonnation. The prairie Ccg'increases cholesterol ab,sorption r','i'ch increasecl.
ilietary clrol-esterol- intal<è and secretes this excess cholesterol- into
he-patic l¡ile lvhich is stored in tl-re gallbJ-ailder (ilc1.er and lleriÐes+-en 1977).
Hithin a fevr days cholesterol- gallstones begin to fc::rn. Freceecling stone
fo::¡retion tÌre gatlbl-aclder voh¡ne enlarges dite to stasis (I'ieyer, Ðentresten,
G\rrnell- 1978, Flutton, Sieverlr, Vennes eì: al 1982).
liphincterotcny (surgice.l rencval of the specialisei :ansculatr-ire 'Jrat
contro-ls bile flov¡ frorn the ccrnnon cuct) al'ìo',.:s j'ree drainagc of tire
gall-blarcicel: anc'I. prevents galJ-stone fonraiion, cvê-n lviren bile 'i s
su1>e.rsaturateii- rrj-th chol-esterol.
I'lcllo'øing sphincterotcnry gallblailcler voltu,res rer.lainecl significantlLy srnaller
tiran in sham operated anir:nì-s. Atropine a-h:olisìres 'Lhe p::otective effects of
sphi¡cterotcxr¡z and qal-istones ¿rre al-Ior,¡ec1 to forr,. (llubton, Sievert, Vennes
et aI 19821
Does stasis play a role i¡r cholesterol choleliLlriasis in rnan? ilessing atrd
his colleaçues (I-'iessing, Eories, I{unstlinç¡er et a1 1983) reportcd tlut
154
alrnost ìralf of 23 patients on long tenn 1:arenteral hirperalirentation in
r"'¡lrc¡¡ no gallh-.rlarclder abno:¡nalities v¡ere initially ilenonstrated devel-o,oecì
bj-J-iary "sludge" l,¡h-ich is a miz,tu::e of biliary pignr:nt a¡rcl clrolesterol
c4zstals. In al-I instances these observatiors 'rJere rLraile a rninimirnrm of
LÌrree r.¡eeks after inib.iation of total- parenteral nutrib.ion (TÐ:l). In six
of their sJ-trdge positive pa.tients tÌro subsequently developed
chpl-elithiasis, four had norrnal ultrasonography studies cìuring the initial
one to tlrree rveeks of TFN. In a-ddition, F,osl1m, Pitt, I.kr¡n et aI (1983)
reported a Ìriglrer than eçected j¡cidence of EallblaclCer C'isease incJ-r-rding
acalculou,s c?nleq¡stitj-s during the course of prolonged 1?Î'i. These stu-cli es
st-::onEly suggest a patlrogenetic rol-e for gallbladder st:rsis.
Stucies of gaì-1bl¿¡.cicì.er oiq;tying in pa.tients rriih gial-lstones give variable
::esul-ts. ilortirfir:,-d, K.u¡:f¿¡, ì'ziuCgal ei al {1980) using scinti-graphy found
a¡r incre¿isec sensitivity to intravenous CG{ in rumy çra-Ilstone patients.
(k¡nversefv rrishrer, StelzJ, Roci', et aI (1982) shcriecl a. nonnaf res¡ronse to
CfIi but a dirninislred response to an ingestedr rni:rei rieal-. They shovred titat
tlris cìj-r-ni¡iisiied respcnse v¡as lrot clue to slci.¡er gastric anptyûrg. In other
sti;Cics çalì-r;laäicr erpLyinE Ìns i:cen shorn: tc i:e cicla-'icrl (Shaffer,
ì';cC:::rcni-i, D:99;rn 1t30) or non:al (V'an ,;erEe iíenegcui;..:li, llcfl:rrnn 1973,
rlori:.irfielCi anrcì lloñirane, 1975, iloll ancl Grr:rrc4z, 1978) - Ttrese ciiscrei::urcies
c¡-i¡roi l¡c reconciled at -j-ris sta'Ee. 'lhey rlo noL a,o¡-,eau: 'to ¡:efate to tìte
ege or se>: of tÌre patien'ts stu<Lieci. I.iiret-her -these changes represent Lhe
ca,.rse or -ulre resu-l-t of ga-Ilstones has not lrcen establishecl.
Scrne clinical situations suggest that galJ-icladcler stasis alone is not a
sufficient prerequisiLe to gallbl-aclcler clisease. Coeliac sprue is
characteriseC frecluently by gallÌ:Iadder enlargorent associatexl l¡ilh
sluggish contractility (Lov¡-Ecer, Iieaton, lieaton et aI 1971 , Low-Beer,
Flarvey, Davies et aI i975). Yet no unusual suscepLibility to clrolesterol
155
cholelithiasis Ìras been reported in these coeliac sprue patients. Possibly
the reason is tlrat i-he intestiral- l-esion produces an r:ndersatr:rated bil-e.
A sj-lnilar situatio:r o<ists i'or truncal vagoto-.ny pa'-tients (Gl-anviÌIe and
D:thie 1964, In-berg anC. Vuorio 1969, I{ielsen 19641.
l-uture studies of garstrointestj¡aÌ riotility in pregrnnry lvill need to
concen'trate on relatively non-invasive techniques. l-.l:rtlrer refinernent pf
the innovative ultrasourd techn-ique of líing, Adam, Pr1rcle et aI (1g1o4l ålrf,
yield valuabl-e new da-ta on ciranges in transpyloric fluid movenent as
precj¡ancy prqjresses. T[-re scatter of cìata be'tv¡een trines-ters sho',,¡n in iJ:ri¡
'bhesis dexionstrates the need for sequentJ-al sttrdies on the sane irdiviiìual:
to detect siqrrificant chr,anges betr.¡een trj-rnesters. À reliable ultrasound
techn-i-que for measuring gastric enptying v¡ould be an iCeal rnelhod for
ron-j¡.v¿rsive sec¡rential- studi es j:r pregranci/.
Poteniial proiclenrs lvithr hydrogren breath testing irave læen outl-inecl. I\rLhe:
stuclies of transit tjnle in pregr-nnry should includle a tncuth r.,'ash to
elir,rin¿,te oral bacterial hy-drogen procl-uction. fn aCdition, a- J-iquid neal
e,s reccÈiìrirenceci 3-j1' I,e lìr:oo;r, iãl-e Bcavis et al- {1983) cor-r.l-ci iiriprove
rei;rorjllc:Lbiì-il-1'. Lecause of the tncertainty as,i io'tire reeson:ior Ìùe lacl:.
of ]-.rea.-ti:L ìri,.ci:rcr_¡oi pr:odrrctj-olr i;-l sc';,ntirirrf tri¡:s'i-e;'sr::>jects rt rr.ay Ì:e
ilÌore i):recis;e tc ccnsicìer an afienntj-ve fo:r-rl of i:::ansit 'tji'le nieastuernc:r't.
iost r¡iehio:isr of irte¿:.sursnent use ra.c],'ionucl-icles i--,,ut i-ncre: recenLly IieIIor',',
Ecrocly, tririlli¡-rs et a-l (1985) liave äescrj-l=rcl an accrrfrete neasurement oi
orccaeq¡l transit- rrsinE the appeararrce in ver-rol-ls l:Ioccl o-i tÌre sulphur
ccxir¡:onent of oral-Iy i:rqested sul¡:hasalazine. Ttris urethod may prove useiul-
in the str-rdy of 1-ransit tir-,e j:r pregrr,ant \.ictnen, buL the need for frec¡rent
btood sarnpliirg l,ioulcl be a sic¡nificant c'ìrarvback¡ Il- should also be notd
th,at tirere is a cl-ose correlation hjetweên the appearance of Ì:reath hydroger
frcrn orarl lactufose ancl the appearance of suI1:hap1-ridine in the venous
blooci after ingiestion of sulpìrasalazi¡re.
In future studies of tire effects of prr-¡rr,ancy on orocaecal r-crotility' gut
lror¡rones r,iricit change c]ur-ing pregrlanclz shoulci be crcrrelateci vlith oilserverÌ
rnotilit-y chranc¡es. T'Ìie digesl-ive ca¡rzrcily of the grut j-s increaseci cìu-ring
precrÌncy ancl lactationr. Àntral ancì plasrna levels of gastrin lrave been
slror.¡n to be el-evatct in lactat-ing rats (Lichterìberger,!Trier, 1979\ arfl,
tlrere is a significant suckÌing-rel-ated effect on scrnatostatin tevel-s ín
pigs (tlvrns- i,loberg-, Ðriksson, Blcxnquist et at 1984). Scx¡ntostatin levels
r.¡or-r.kl b: of pa.rticular i¡rte::est in pregnancy as ì:rfusion of sc¡natostati-n
lras beerr reportecì to inhibit lùe gallbladder ernl:tying resi:onse to
hl.perLonic Alucose achinistereci, orally (Johansson, I'oIIIærg, Ilfenciic et aI
1931)
In ì:he fu'i:ure it v,'ou1c1 k¡e l¡orthl'¡hil-e systor'atically studying al teration j-n
gallbtaäcer fi:nction in'other special pa.tient groups. l's in other stuäies
of the trhl'=1oto"ic and re-udrolic al-terations occurring crirrir:,g nonral
pregnancy, alteratìons in gal-lbiaclci.er ärotility iuncLion, if clernonstra.i¡l-e ir
otjrer Ìrigii risì, Eroups, i;o¿Ici l:c'_rn1i}.-eJ_1r -to be an isolated abnonu,.Ii'ty lru
one ¡nssiì:Iy aurernl.lc: t-o cire-rr,peu-uic rinnipulatj-on ar-xl ther:e.r-'ore ,.,/or'uìi
:.no'.,'i¡g al-nut.
I
I
t
L57
APPENDICES
A. Real- Time Ultrasound Method for Determining
Galtbladder Volume
B. Characteristics of Infusates
C. Compari-son of Mebhods for Measuring Gallbladder
Emptying
D. Report ed Studies of Bil-iarv Bile Acid Secretion
In Subjecls with Intact Gallb1adders and Subjects
Status Post Cholecvstectomy
E Measurement of Smatl Bowel Transit Time
by the Hydrogen Breath Test
F. l4e asurement of Serum Human Pancreatic
Polypeptide
L
I
158
REÀL TIME ULTRASOUND METHOD FOR DETERMINING GALLBLADDER
VOLUME
Sum of cyJ-inders method: This method was original-ly
used but not val-idated, in cholecystographic studies
of gallbladder vol-ume. Volume is cal-culated from
sonograms by dividing the gallbladder image into
a series of cyJ-inders of egual height (h). A transparent
grid of paral-J-e1 lines, with constant distance (h)
separating lines, is placed over the galJ-bJ-adder image.
The longitudinal axis of the gallbladder image is
positioned perpendicul-ar-,to the grid of paralJ-eJ- l-ines.
Util-ising the formu.la för volume of a cylinder, the
formul-a for gal-J-bJ-adder volume becomes:-
V n ITa.l_ l_
i= l- (r):h
2
4
where h. and d. are the respective heightl- l-
of the ith cyJ-inder, and n represents the
cylinders in the series. But since hl is
between paral-Iel lines on the grid and is
each cylinder in the series, the formul-a
vol-ume is: -
and diameter
total number of
the distance
the same for
for gallbladder
(2)V 0.78s h ,Lur'
i=rI
I¡Ihen calculating volume with this method onJ-y sonographs
of the longitudinal projection are used. Vrlhen the
gallbladder is curved, ês it often is, the longitudinal-
projection wiJ.l not pass through the central axis of
the gallbladder (Figure la). Displacement of the
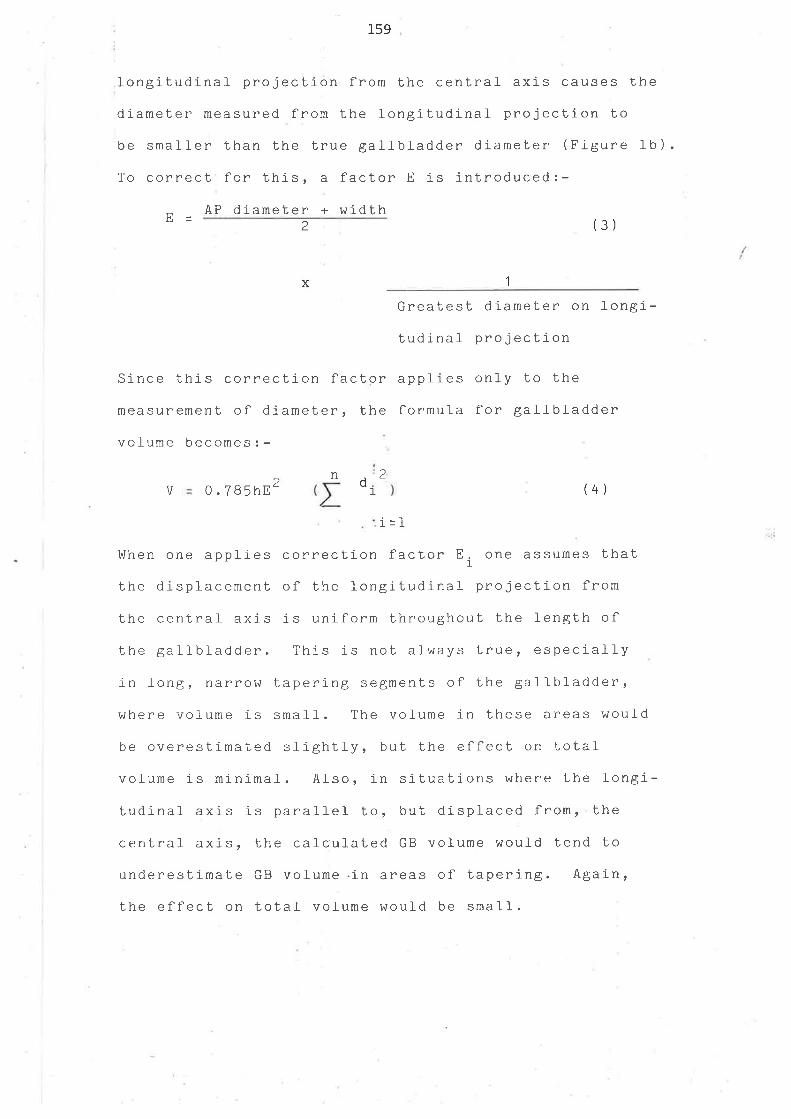
159
,longitudinal- projection from the central axis causes the
diameter measured from the longitudinal projection to
be small-er than the true galJ-bl-adder diameter (Figure 1b ) .
To correct for this, a factor E is introduced:-
tr- AP dlameter + width2 (3)
x 1
Since this correction factor
measurement of diameter, the
vofume becomes: -
Greatest diameber on longi-
tudinal projection
applies only to the
formula for gal-ì-bl-adder
V 0.7B5hE 2 d (4)
Irlhen one applies cornection factor Ei_ one assumes that
the displacement of the longitudlnal proiection from
the cenlral axis is uniform throughout the length of
the gallbladder. This is not always true, especiall-y
in Ìongr trârrohi tapering segments of the gall-bladder,
where volume is smal-l-. The volume in these areas would
n 2l_
i=l
be overestimated slightJ-y, but the effect on
volume is minimal. AJ-so, in situations ùIhere
total
the J- ongi -
thetudinal axis is paral-J-eI to, but
central axis, the caÌcul-ated GB
underestimaLe GB volume .in areas
the effect on total volume woutrd
displaced from,
volume woul-d tend
of tapering.
be small-.
to
Again,
rov
No correction factor for magnification ( as is used in
cholecystographic volume determination) is necessary
for ultrasound measurements. The measurement and
cafculation ( using a hand calculator ), of volume by the
corrected sum of cylinders method requires approximately
5 minutes for each PhotograPh-
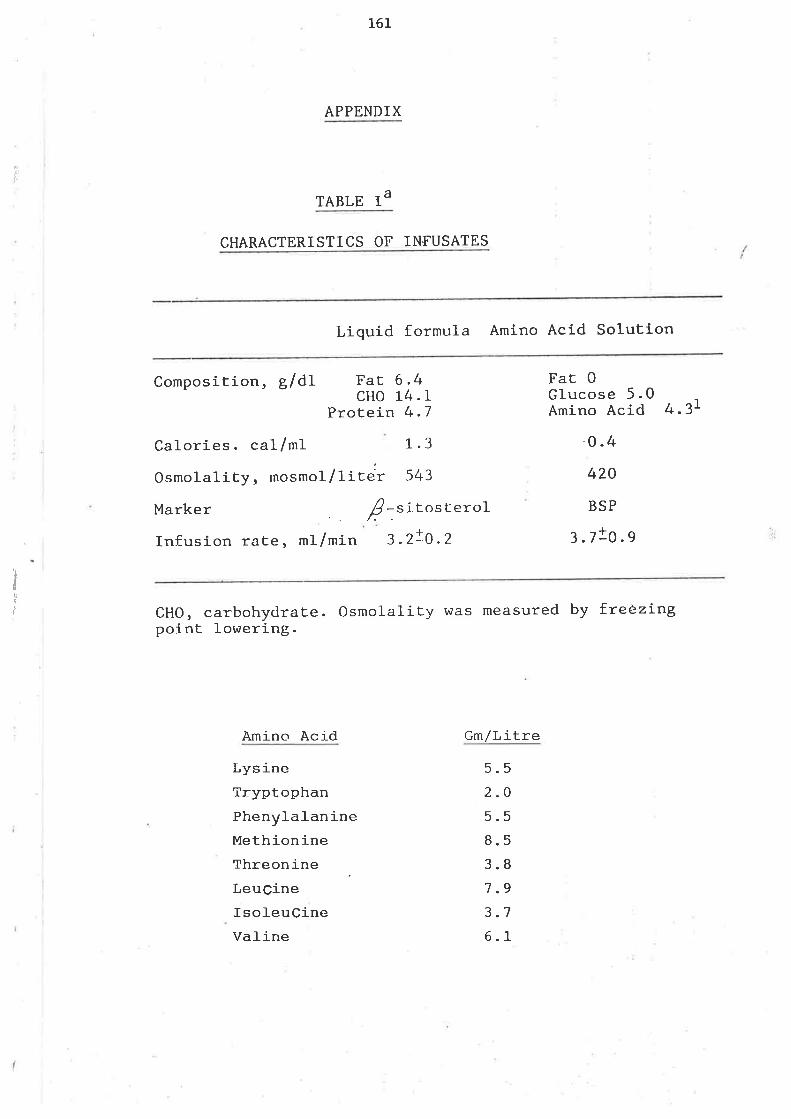
,l
161
APPENDIX
TABLE IA
CHARACTERISTICS OF INFUSATES
Liquid formula Amino Acid Solution
ItII
Composition, glðtcHo
Protein
Calories. cat/ml 1.3
Osmolality, mosmol/litelr: 543
Marker Ê .titosterolInfusion rate, ml/min 3 .2!0.2
6.414.L4.7
Fat FaE 0Glucose 5.0Amino Acid
o.4
420
BSP
3.7!o.s
4.3L
cHo, carbohydrate. osmolality was measured by fteëzí-ngpoint lowering.
Amino Acid Gm/Litre
LysineTryptophanPhenylaJ-anineMethionineThreonineLeuCineIsol-euCineVal-ine
5.52.O
5.58.53.87.93.76.1
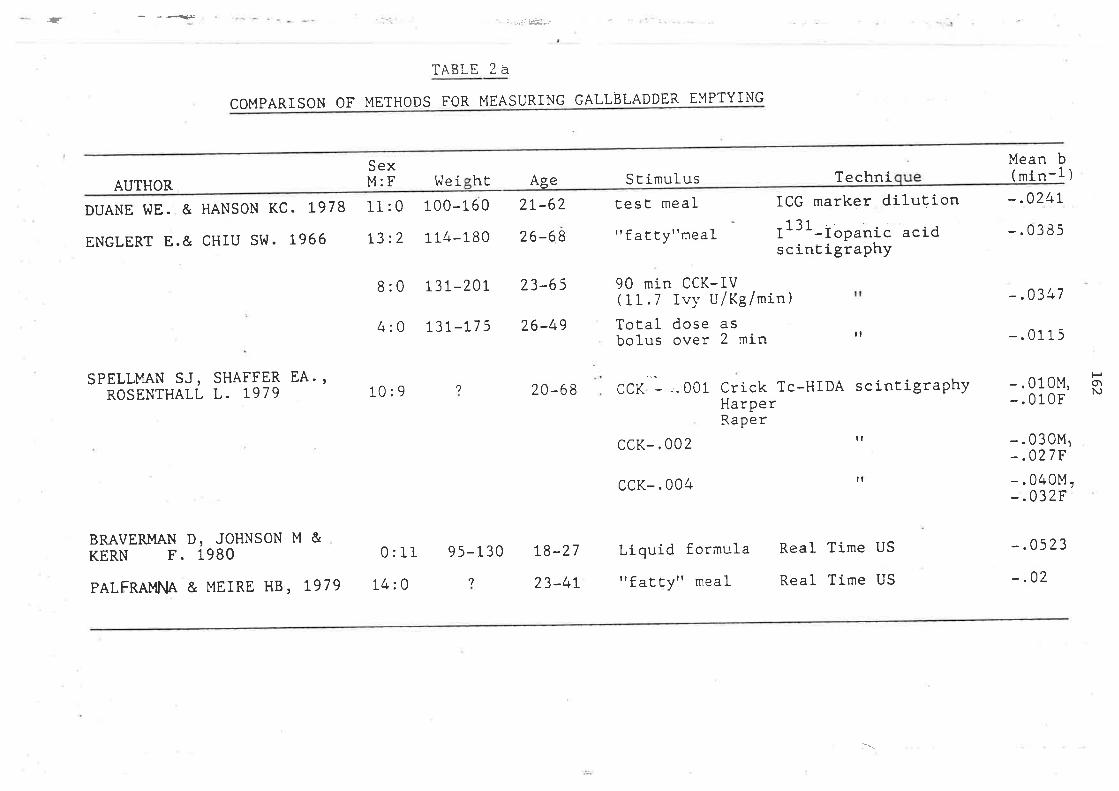
.a - ---.=<-r
COI"IPARISON OF METHODS FOR ING GALLBLADDER EYPTYING
TABLE ?A
MEASUR
AUTHOR
DUANE I^IE. & HANSON KC. L978
ENGLERT E.& CHIU Si^I. L966
SexM:F
ll:013:2
[.le i100-1 60
114-180
2L-62
26-68
hË Age S E imulustest meal
" fatty"meal
90 min CCK-IV(1r.7 Ivy u/rg/min)Total dose asbolus over 2 min
ccK-.004
Liquid formula
"fatEyl'meal
ICG marker dilutionr131-ropanic acidscintigraphy
Techni
ll
il
Real Time US
Real Time US
Mean b( min-1 )
-.02/+t
-.0385
-.0347
- . 0115
-.010M,- . 010F
-.03014ì-.027F-.040M,-.032F
-.0523
-.02
8 :0 L3L-2.0I 23-65
4:0 t3t-L7 5 26-49
10:9 20-68 CCK - ..001 Crick Tc-HIDA scinEigraphyHarPerRaPer
ccK-.002 rr
SPELLMAN SJ, SHAFFER EA.,ROSENTHALL L. 1979
BRAVERMAN D, JOHNSON M &KERN F. 1980
PALFRAMNA & MErRE HB, 1979
POrN,,1
0: II
14: 0
9 5-1 30
,|
L8-27
23-4L
'': -:l
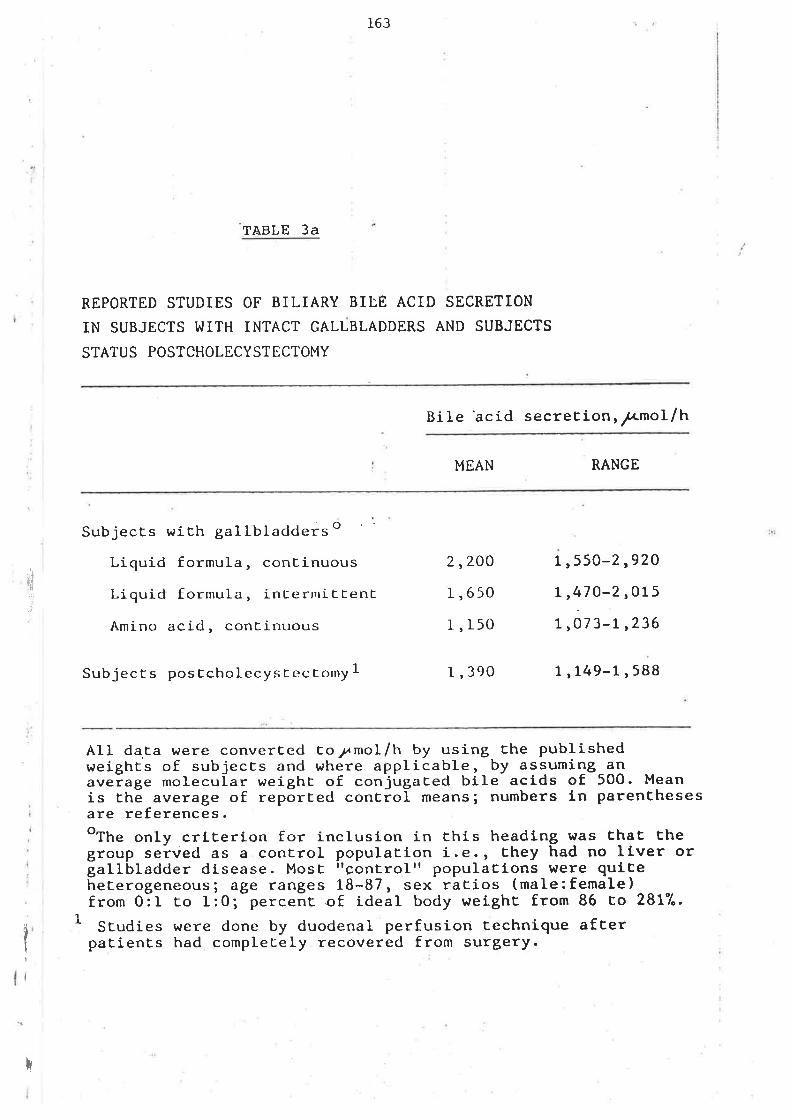
163
-TABLE 3a
REPORTED STUDIES OF BILIARY BILE ACID SECRETION
IN SUBJECTS I^IITH INTACT GALLBLADDERS AND SUBJECTS
STATUS POSTCHOLECYSTECTOMY
BiIe'acid secreElonr¡mol/h
MEAN RANGE
'tl,i,)
SubjecEs with gallbladders o
Liquid formula, continuous
Liquid formula, inl-erniEfenE
Amino acid, continuous
2,20O
r,650
l, r50
1 ,550-2 ,92O
| ,47O-2,015
1 ,07 3-L ,236
Subjects posccholecysLectomy I I ,390 7 ,149-L,588
All da.ta were converEed coTmot/h by using the publishedweighEs of subjects and where applicable, by assuming anav"i.g. molecuÍar r^reighC of conjugaCed bile- actds of 500. Meanis the average of repõrced conLiol means; numbers ln parenEhesesare references.oThe only crlEerion for inclusion in Ehis headlng was Èhal Èhegroup served as a control populatton i.e., Ehey had no llver orgallbladder disease. Most rrçontrolrr populaËLons brere qulEehererogeneous; age ranges 18-87, sex rarios (male:female)from 0:L Eo l:O;-perceñc.of ideal body weighc from 86 co 2817".
SEudies erere done by duodenal perfusion Eechnique afcerpaEienEs had complecely recovered from surgery.t
I
;
I
iÌi
I
]-64
I4easr:re¡rent of Snaf]- Bor,,¡el TTansit Tirne by the Hydroqen Breath Test
Orocaecaf transit tjrre was neasured by the lactufose hldrogen breath
test (Bond ard Levitt, 1975; Bond and Levitt 1977¡ La Brooy, Ma]-g
Beavis et al- 1983; Solcnons, Viteri, Hamil-ton 1977). Sr:bjects raere
advised to avoid excess intake of starch polysacctr,aride the day before 1
the test. After an overnight fast, subjects irgested 10 grams of factufose
i¡ 100nù of water. Breath sam¡rles for neasure¡nent of hydrogen concentration
r,,¡ere obtai¡red fasting and eveÐr 15 minutes for 4 hor:rs. Breath hydrogen
concentration was neasured with a Quj¡rtron mode.I S gas chronatograph (Quintron
Instrr:rnents Inc. lutifwaukee, Wisconsi¡r) usi¡rg argon as carrier gas at lBmI ¡:er
rni¡rutes, a molecufar sieve coJ-tmn,' and thermal- conductivity detector.
Orocaecaf transit tirre was defined as the tirre .of the first sustai¡red
rise in breath hldrogen concentrati-on frqn base.U¡re. If after 4 hours no
rise in breath hydrogen occurred, the transit tj-rne was recorded as 24O m-i¡rutes.
In each study of pregnant vvonen, transit tjrre was estirnated by 3 observers
bl-inded to the str:dy protocoJ- and design. Each subject's transit tjlrre
was reported as the nean of the 3 estjrnates. TTansit tine varied aÍìong
observers ín 242 of str:dies but j¡r each case by onJ-y 15 rnilutes. In the
secretion study fess observations were avail-abl-e and eight observers were
used. Bond and Levitt (1975) validated the H, breath test technique as
a Íþasure of srnal-I j¡ltestj¡ra-l transit by simultaneously neasuring the
appearance of non-aborbed PEG at the il-et¡n wj,th a rise i¡r breath H, Produced
frqn the intesti¡ral- bacterial- netabolism of ingested lactu-l-ose.
I4easr:renent of Serun Hunan Pancreatic Polypeptide
Sert¡n hr¡nan pancreatic pollpeptide(HPP) levef was determined by radio-
j¡rmunoassay in the taboratory of Dr. Ian TayJ-or, at tLre Centre for Ufcer
Research and Education, Veterans Adminístration Centre Vùadsworth
Hospital, Los Àngeles, California. l4ean i¡tra ard iìterassay precision
1t
I1
I
¡
i
I
I
i
I
165
h¡ere. 4å ar¡d 88 respectively. Recgvery of HPP added to serun deviated
by no npne than 178 frqn tle ocpected values otner the range of 40-340
pg/m1 senm. HÙman pancreatic pol-y¡nptide was plotted agailst tÍrÞ
and tt¡e integrated response was rneasured frqn the area urder tte HPP
curye.
CaLcu-l-ation of BiJ-ian¡ Cholesterol and Phospholipid i¡ Secretion Studies
Ite cholesterol ard phospholipid concentration of each duodenaL sanple
was corrected for jnfi¡sate cholesterol and phospholipid using the
calculation: -
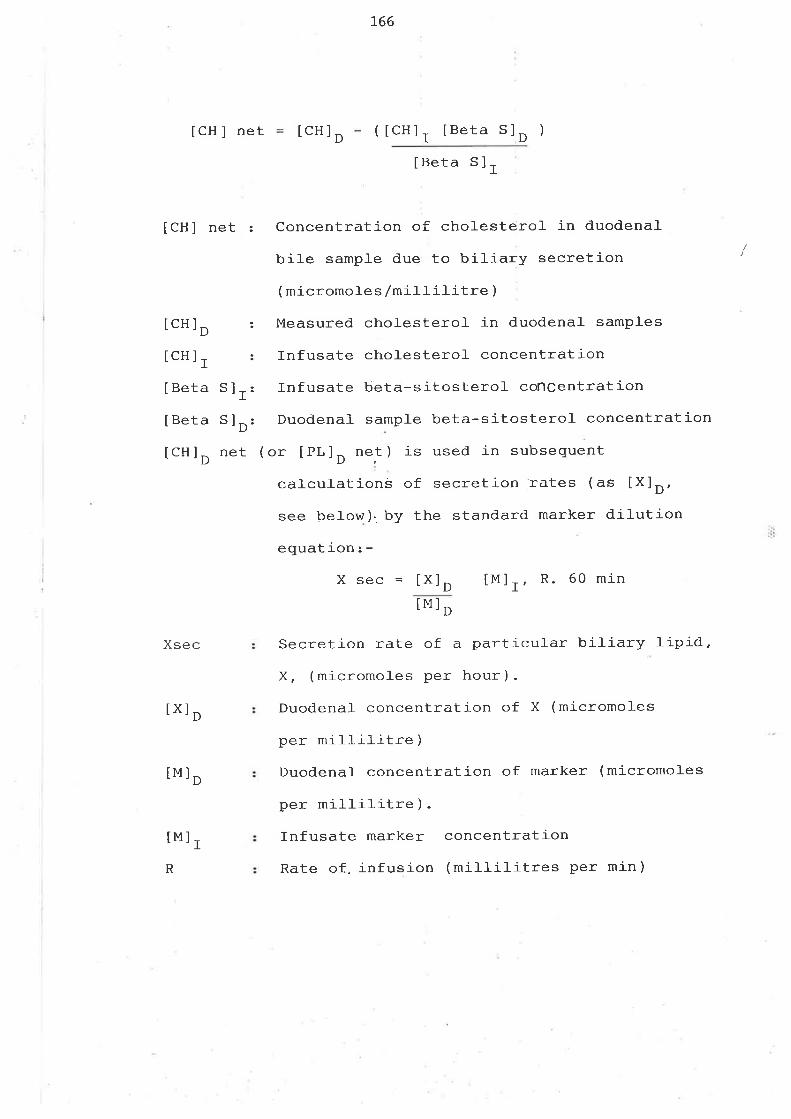
166
tCH I net tCH ] ( tCHlr IBeta 5lo )D
lCHl net
IBeta 5lr
: Concentration of cholesterof in duodenal
bile sample due to biliary secretion
( micromoles /míl-l-i]-itre )
: Measured choJ-esteroJ- in duodenal- samples
: Infusate chol-esterol concentration
: Infusate beta-sitosterol concentration
: Duodenal- sampJ-e beta-sitosterol- concentration
(or [PL]O net) is used in subsequent
calculations of secretion rates (as IX]o,
see below)' by the standard marker di.l-ution
equat ion : -
X sec = [X]¡ [M]I, R. 60 min
lMl r>
Secretion rate of a particufar biliary J-ipid,
X, (micromoles per hour).
Duodena.I concentration of X (micromoles
per millilitre )
Duodenal- concentration of marker (micromoles
per mì-IIititre ) .
Infusate marker concentration
Rate of. infusion (mil-l-il-itres per min)
lcHlo
lcHlr
I Beta
IBeta
lcHlo
sìrs1o
net
Xsec
lxlt
tMl D
tMl IR
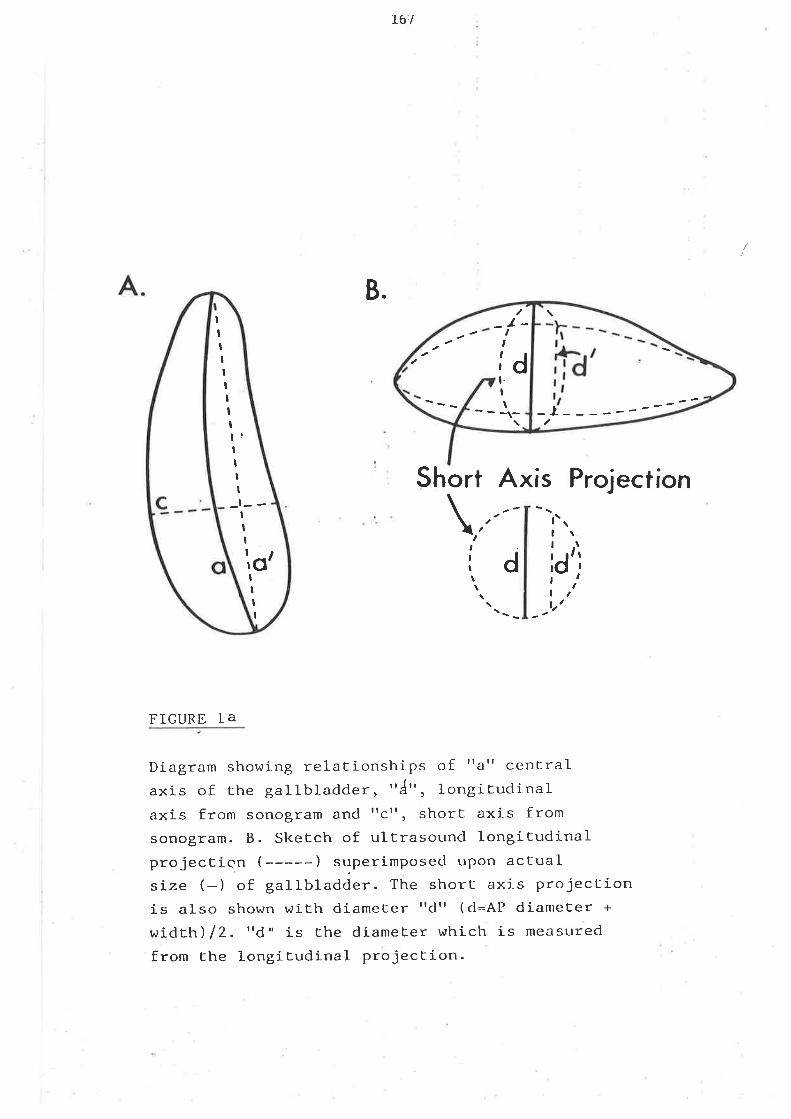
j-61
B.
Short Axis Projection
FIGURE IA
Diagram showing relationships of rtarr centralaxis of the gallbladder, 'rl'r, longiEudinalaxis from sonogram and ttct', short axis fromsonogram. B. Sketch of ultrasound longitudinalprojection (-----) superimposecl uPon actualsíze (-) of gallbladder. The short axis projectionis also shown with diameter rrdrr (d=At' diameEer +
width) /2. rrd, is the diameEer which is measured
from Ehe longitudinal projection.
\\
{z,ttd\
tltIt
f
l'aII
idII
l.t
I¡
IIIIIII
I
II
tIIrOtI
l!IItI
I
-ti -
F,
,t
ldt.It
_t-
T7I
B]BLIOGRAPHY
172
ADLm. RD, ¡4ETZGER AL, GRUNDY SM. Biliarlz lipid secretion before and after
cholecystectorny in Arnerican fndians with cholesterol gallstones.
GASTROENTER.OLæY. 1974ì 66: I2L2-I2I7 .
ADMIRAND hrH, SMALL DM. The physiochernical- basis of cholesteroÌ gallstone
formation in man. J.CLIN.IN\ÆST. 1968¡ 472 f043-1051-
AI{GELIN B, EINARSSON K, Htr-LSTRCI"I K et aI. E]-jmination of chol-esterol in
hyperlipoproteinaernia. CLIN.SCf .I'IOL.MED. 1976; 51: 393-391 -
ADRIAIJ TE, MIrcHENtrftE P, SACÐR GR. et al-. Effects of pancreatic
poJ-lzpeptide on gallbladder pressúre and hepatic bile secretion. AI\4. J.
PHYSIOL. I9B2i 2432 G204-C207.
ALI SS, JAVITf NB. Quantitatj-ve estjmations of biÌe salts in serum-
CAN.J.BIoCHm{. I970; 48z 1054-1057-
A¡4DRUP BM, GRIFFITTI CA. The effects of vagotomy upon biJ-iarlz function in
dogs. J.SURG.RES. L970; 10: 209-216.
ANDmSON A. JAMES OF. MacDONALD HS et aÌ. The effect of ethynyl oestradiol
on biliarlz lipid cornposition in young men. EUR. J. CLIN. INVEST. 1980; 10:
7l-80.
ATLAY RD, GII¿ISON EI,\I, HORT.ON AL. A fresh look at pregnancy heartburn-
J.OBSTET.GYNAECOL. BR. COMVION W. 1973; B0: 63-66-
BACK P, SJOVALL J, SJOVALL K. l4onohydroxy bile acids in plasma in
intrahepatic cholestasis of pregnancy.Identification by corputerized gas
]-73
chromatography-mass spectrometry. MED.BIOL. (Helsinki) 1974; 52t 31-38.
BARNETT V,JO, HILBURN GR. Dissol-ution of human gallstones in the dog's
gaÌl-btadder after various degnees of vagotomy. SURGERY. 1966; 60: 840-843.
BARTLETT GR. Phosphorus assay j-n column chronatography
234: 466-468
J.BIOL.CHEM. 1959;
BAXTER JN, GRIME JS, CRITCHLEY M et at. Relationship between gastric
emptying of solids and gal-lbfadder emptying in normal subjects. GUT. 1985;
26: 342-351.
BECKER JM, MOODY FG.
biliary sphincter.
Effects qfl gastrointestinaf hormones on the opossum
SURG.FORUM. l97B; 292 400-402-
BEHAR J, BIANCANI P. Effect of cholecystokinin and the octapeptide of
chol-ecystokinln on the feline sphincter of Oddi and gall-bladder: Mechanisms
of action. J.CLIN.INVEST. 1980; 66: 1231-1239.
BENEVENTANO TC, ROSEN RC, SCHEIN CJ. The physioÌogical effect of acute
vagal section on canine bili-ary dynamlcs. J.SURG.RES. 1969; 9¿ 331-336.
BENNION LJ,
acid pools.
DROBNY E, KNOhILER !'lC et al-. Sex differences in the size of bile
METABOLISM. 1978; 27: 961-969.
Risk factors for the development of cholelithiasis
1978; 2992 1161-1167, 1221-1227.
BENNION LJ. Changes in bile lipids accompanying oophorectomy in a
premenopausal woman. N. ENGL . J. MED. 1977 ; 297 z 7 O9-7 1 1 .
BENNION LJ, GRUNDY SM.
in man. N.ENGL.J.MED.
BENNION LJ, KNOI/\ILER !ìIC, MOTT DM et aI. Devel-opment of lithogenic bile
during puberty 1n Pima Indians. N.ENGI.J.MED. 1979; 300: 873-876.
174
BENNION LJ, GINZBmG RL, GARRTCK ¡'IB et al-. Effects of oraL contraceptives
on the galtbladder bile of normal \^/oilìen. N.BIG.J.MÐ. 1976;; 294: IB9-I92.
BEîJNION LJ, l4orlIt DM, HOVVARD BV. Oral- contraceptives raise the choLesterol
saturation of bile by increasing biliary cholesterol secretion. ME'IABOLISM-
I9B0; ¡ 29: IB-22.
Bm¡NION LJ, GRUNDY SM. Effects of obesity and caloric intake on biliarlz
fipid metabolism in man. J.o,IN.INVEST- 1975;¡ 562 996-l-011.
BHA\1RANI BR, SARDA IR, I/iOOLEVm. CA. Radioi¡rununoassay of plasma equi-lin and
oestrone in postmenopausaÌ vùonìen-after the aùninistration of Premarin.
J.CLIN.EIJDOCRIN.METAB. lg8l; 52,2 14I-147 - -
BJORCK S, JAIISSON R, SVANIK J. Ïnil-uence of electrical vagal stimulation
and acetyl-choline on the firnction of the feline gal-J--bladder.
SCAI{D.J.GASTROI}iTffi.OL. l9B3 ; 18: I29-I35 -
BLISS CT. Statistics in bioi-ogy: statistical nrethods for research in the
natural sciences. voLS. I,2. NEli^l YORK. McGRAW HILL. 196] , \910.
BLOCH HM, TTIOR\rrON JR, HEATìON KW. Effects of fasting on the conposition of
gallbladder bile. GUT. 1980; 21: 1087-1089-
BOND JH, LEVITT ¡4D. Investigation of small- bowel- transit time in man
utilising pulnronary hydrogen (H2) measurements. J.LAB.CLIN.MED. L975 ; 85:
546-555.
BOND ,JH, LEVITT MD. Use of breath hydrogen (H2) to guantitate smal-l bowel
transit foltowing partial gastrectonry. J.LAB.CLIN.MED. 1977; 90: 30-36'
]-75
BONORRIS C€, COYNE l,LI, CHLING A. et al. Mechanism of estrogen- induced
saturated bile in the hamster. J.LAB.CLIN.MED. 1977; 90: 963-910.
OraI contraceptives and venous tlrromboenrbolic disease, surgical-ly confirmed
gallbladder disease and breast tumours.Report from the Boston Collaborative
Dnrg Sr:rveillance Progranrne. I"ANCET. L973; i: 1399-1404.
Surgically confirmed gallbladder disease, venous thromboembolism and breast
tunours in rel-ation to ¡rostrnenopausal estrogen therapy.A Report from the
Boston Collaborative Drug Survei-llance Progranrne, Boston University Medical-
Centre. N.müG.J.MED. I974; 290:. 15-19.
BRADLEY DD, WINGERD J, PETITTI DB et al. Serum high-density-J-ipoprotein
cholesterol in \,vomen using oral'contraceptives, estrogens and progestins.
N.ÐIGL.J.MED. l-978; 2992 L7-20.
BRAVERMAN DZ, JOHNSON ¡4L, KRN F. Jr. Effects of pregnancy and
contraceptive steroids on gallbladder function. N.NG.J.MED. Ì980; 302:
262-264.
BRODEN B. Experiments with chol-ecystoki-nj-n in cholecystography.
ACTA.RADIOL. I95B; 49: 25-30.
BROOR SL. SLCIA T, AM¡4ON tlV. Cholesterol reduces the effects of dihydroxy
bile acids and fatty acids on water and solute transport in the human
jejnnum. J.CLTN.IN\¿EST. f9B0; 652 920-925.
BRUCE LA, BEHSUDI FM. Progesterone effects on three regional
gasLroint-est-inal- t-issues. LIFE SCf . 1979; 25: 729-734.
L76CAI'1IT,T.trRI M, BRChJN ML, I"IALAGEIÄDA JR. Relationship betu,een irnpaired gastric
emptyi¡g and abnornnl- gastrointestj¡al- motility. GA,STROEM. 1986¡ 91: 94-99.
CAPRON JP, DEf,,AMRE J, HRVE It4A et al. MeaI frequency and duration of
overnight fast: a role in gallstone formation? BR.MÐ.J. I98I; 283: 1435.
CARIDE VJ, PROKOP EK, TRONCALE FJ et al. Scintigraphic determination of
smafl intestine transit times: Conpárison with hydrogen breath technique.
GASTROEIüIEROLOGY - I9B4; 86: 7L4-720.
CARLSON SE, MITCHELL AD, CÐLDFARB S. Sex rel-ated differences in dil:rnal
activities and development of hepatic rnicrosonal 3-hydroxy-3-nrethyJ-glutaryl
coenzyme A reductase and chol-esteroì- Talpha hydroxylase.
BIOCHEM.BIOPTryS.ACTA. 1978; 53I: 115-119.
CFiAO YS, WINDLER EE, CHEN C'C et al. Hepatic catabolism of rat and human
lipoproteins in rats treated with J-7 alpha ethinyl oestradiol. J.
BIOL.CHEM. I979; 254: 11360-11365.
CFIARNEY AN, SILVA P, BESARAB A. et a1. Separate effects of aldosterone
DOCA and methylprednisolone o.r r".,-1 Na-K-ATPase. AM.J.PHYSfOL . 1974¡ 271:
345-350.
CFm MAT,CR, FRANCE VIvl. Effect of 17 beta oestradiol- prirning on
progesterone induced inhibition of ftuid transport by male guì-nea-pig
gall-bladder in vitro:proceedings: J.PIrySIOL. (LOND) I97B¡ ¡ 278: 30P.
CHEVREUL ME. Cited by Rains page 685
CLARK DH. Peptic ulcer in women. BR.MED.J. Ì953; L: I254-L257.
CLH"AND JB. Gal-lstones in seven thousand post-nxrrtem examinations.
177
MED.J.AUST. 1953'í 488-489 -
COHEIJ S, KAPLAN M, CÐIILfEB L et al. Liver disease and galì-stones in
regional enteritis. GASTROHVTROLOGY. L97Li 60: 237-245.
COHÐJ S. Ihe sluggish galÌbladder of.pregnancy. N.ÐüG.J.MED. I9B0; 302:
397-399.
COLLfNS PJ, HOROVVITZ M, COOK DJ et aI. Gastri-c emptying in normal subjects
- a reproducibl-e technique causi-ng a single scintillation camera and
computer system. cU'I. l-983i 24: 1117-1125.
COOKE AR. Control of gastric emptying and motility. GASTROE\IEROI¡GY 1975¡
68: 804-816.
COOkE AR. Localisation of receptors inhibiting gastric emptyi-ng in the gmt.
GASTROHVIROI,OGY. l-977 ; 722 875-880.
CORTCII A, PHILLIPS SF, MALAGEI,ADA JR. Gastrj-c ernptying of lipids after
ì-ngestion of a solid liquid meal in humans. GASTROHVTffi.OLOGY 1981; B0:
922-927
DATTA S, HEY VÀ4, PLELI\RY BJ. Effects of pregnancy and associated hormones
in nouse intestine, in vivo and in vitro. PFT.UEGERS ARCH. 1974; 3462
87-95.
DAVIS RA, KmN F.Jr. Effects of ethinyl- estradiol and phenobarbital on
bile acid synthesis and biliarlz bile acid and cholesterol excretion.
GASTROEIüTEROLOGY L976¡ 70: 1130-1135.
DAVIS RA, KRN F.Jr. Reversal by Triton I¡IR - 1339 of the effects of ethinyl
t78
estradiol (Eo) on cholesterol and bite acid (BA) rnetabou-sm in the rat
(Abstract) . GASTROEDÍTffi.OLæY L977 ¡ 722A22/L045'
DE LA SALLE. Cited bY Rains Page 685
DENBESTÐ{ L, CONNOR V{E, BELL S. The effect of dietary chofesterol on the
conrposition of human bile. SURGERY. 1973¡ 732 266-273.
DE I^IEAVER I, EECKHOUT G, VAI{TRAPPm{ G. et aI. Disruptive effect of test
meals on interdigestive motor conplex in dogs. AI{'J'PHYSIOL ' I97B; 2352
E66l-E665.
DI6RY PLC, T,OMKINSON JS. Nausea and vomiting in pregnancy: a trial of
meclozine dihydrochloride with and without pyridoxine' LANCE-I ' L962; 2:
370-372.
DOMSCHKE W. Motilin; spectrum and'mode of gastrointestinal
actions.AM.J.DIG.DIS. 1977 ¡ 22: 454-49L.
DOI/üLING BL. The effects of vagotorny and coeliac ganglionectomy on the
inrrervation of the canine gall-bladder. BR.J.SURG. L97I¡ 58: 303'
(Abstract).
DOVüI{ RHL, üJHITING I\4.I, WATIIS J et aI. Effect of synt}retj-c oestrogens and
progestagens in oral contraceptives on bile lipi-d cdrposition' GUI 1983;
242 253-249.
DRAPER NR, SI{ITH H. Íhe extra sum of squares principle in: Aflied
Regression Analysis. Ncw York. John Wil-ey and Sons- 1966; 67.
179
DUAIIE !rc, HANSON KC. RoIe of gallbladder enptying and small bowel transit
in regulation of bile pool size in man. J.LAB.CLIN.MED. 1978¡ 922 859-872.
DUAIIE Vrc, BOND JH Jr. Prolongation of intestinal transit and o<pansion of
bil-e acid pools by propanthel-ine brornide. GASÏROE$ITERCIIOGY 1980; 78:
226-230.
DUPONII C. BROYART JP, BRORY et aI. Inportance of the vasoactiive
intestinal peptide receptor in the stimulation of cyclic adenosine 3',5'-
rrcnophosphate in gallbladder epithelial cells of man. Corparison with the
gruinea pig. J.CLIN.IIIVEST. 1981i 67: 742-752.
EIMRSSON KA, HEf,,LSTROM K, KALLNER M. Bile acid kinetics in relation to
sex, serum lipids, body weights and gallbladder disease in patients with
various tlpes of hlperlipoproteinae¡nia. J.CLIN.IN\ÆST. 1974¡ 54:
1301_-131_1.
EII,IARSSON KA, GRUNDY SM, TARDISON IVGM. Enterohepatic circulation rates of
cholic acid and chenodeo>q¿cholic acid in man. GLIT. L979¡ 20: l-078-l-082.
mGLm,T Jr. E, CHIU VSw. Quantitative analysis of human biliary evacuation
with a radioisotopic technique. GASTROE$ITEROLOGY 1966; 50: 506-518.
EÍ,MAN R, ¡ltcMASTm. PD. Ttre physiologic variations in resistance to bil-e flow
to the intestine. J.EXP.MED. 1926¡ 442 15I-17I.
RLIIIGR. S, DHUMEAUX D, BHITIH,CII P et al. Effect of inhibitors of sodium
transport on bile formation in the rabbit. AI4.J.PHYSIOL. 1970; 2L9z
419-422.
EVERSON GT, BRA\ÆRMAN DZ, JOHNSON ML et al-. A critical evaluation of
180
real-tirne urtrasonography for the study of gallbJ-adder vol_une and
contraction. GASTROENTROLOGY 1980 ¡ 792 40-46.
FABR.BERG s, GREVST$¡ s, JotIANSSoN H et al. vagotomy and gallbradder
firnction. cUT. 1970; 1I: 789-793.
FAIRI¡üEATTIER DV. Nausea and vonriting in pregnancy. AM.J.OBSTET.GYNAECOL.
1968; 102: 135-175.
FEIN@LD K' WfLEY T' MOSR AII et al.De novo cholesterogenesis in pregnancy.
J.LAB.CLIN.MÐ. l9B3; l0l-z 256-263.
FfSHm. RS' ROBR.TS GS, GRABOVüSKI CJ et aI. Inhibition of lower esophageal
sphincter circular muscl-e by female sex hornones. AM.J-PHYSIOL. l97B; 234:
8243-247.
FfSHER RS, ROCK E, MALMUD LS. Gallbladder emptying response to sham feeding
1n humans. GASTR.OH\ruEROLOGY. L9B6; 90: 1854-1857.
FrsHm. RS, srm,zER F, RocK E et al. Abnormal- gal-tbladder enptying inpatients with gallstones. DIG.DTS,SCI. I9B2¡ 272 I0L9-I024.
FLOYD JC.Jr. Pancreatj-c pollpeptide. g,rN.cASTRon\TERoLoGy l9B0; 9 :
657-678.
FT,OYD JC Jr. FA^]A}IS ss, PH< s, et al. A newly recognised pancreatic
polypeptide; plasma levels in health and disease. RECHTIT PROG. HORM. RES
L977; 332 519-570.
FT-OYD JC Jr, FA^IANS SS, PEK S. Physiologic regulation of plasma l-evels of
181
PP in man. rn BL@ùI sR. ed. ctrr HORI{ONES. Edinburgh. churchirt.
Livingstone. 1979; 247-253 -
FOESEI, S, SEV'IfNG KF. Enhancement of electrically stimufated gn:inea-pig
gallbladder contraction by subthreshold. concentration of gastrointestinal
hornrcnes in vitro. EXPR.IMENTIA. I97B; 342 205-206-
FRANCE V¡4' ME ION A, REAY SR et al. TLre effect of L7 beta oestrad.iol on
fl-uid transport in the invitro guinea-pig gall-bladder:proceedings: (Lond. )
J.PHYSIOL. 1977; 266: 67p. 6Bp.
FRfEDMAI{ GD' KANNEI- VVB' DAWBER TR. The epiderniology of gallbladder disease:
observations in the Framingham study. J.cHRoN.Drs. L966; 19: 273-292.
GROLAMI A, SARLES JC. Biliarlz secretion and nrotilin. INT.REV.pHySIOL.
1977; 12: 223-256.
GRDES MM, BOIDEN EA. Ttre rate of, enrptying of the human gaì_lbladder inpregnancy. SURG.GYN. and OBSTET.. l93B; 66: 145-156.
GLANVILLE JN' DIITHIE HL. Contraction of the gallbladder before and aftertotal abdorninal vagotomy. CLIN.RADIOL. 1964; t5: 350-354.
GODFREY K. Sirç1e linear regression in nredical- research. N.ENGL.J.MED.
1985; 3L3:. 1629-1636.
GREH\BRG GR, MccL,oY RF, CHADWTCK vs et al. Effect of bovine pancreatic
polypeptide on basal- pancreatic and biliary outputs in man. DIG.DIS.SCI.
1979¡ 24: J-J--LA.
r82
GREENBRG GR, MccLoY RF; ADRTAN TE, et ar. rnhibition of pancreas and
gallbladder by pancreatic potypeptide. LANCET l97B; ii: I2BO-I282.
GRUNDY SM, DUÄÀIE I/VC, ADLR. RD et aI. Biliarlz J_ipid outputs in young \,vonìen
with cholesterol gallstones. MHIABOLISM. 1974¡ 232 67-73-
GRUNDY SM' METZGER ÄL. A physiological method for estj¡nation of hepatic
secretion of biliary lipids in man. GASTROEIIIIEROLOGY 1972; 62: I20O-L2\7 -
GRUMY sM, AHRENS EH, SALEN G. Dietarlz p-sistosterof as an internar
standard to correct for cholesterol losses in sterol bafance studies.
J.LIPID.RES- 1968; 9-- 274-387 -
HALPERT B, LEWIS JH. Exper:iments on isolated whoÌe gallbladder of the dog.
AM.J.PrrySrOL. 1930; 93: 506-520.
IIARPR. A. RAPR HS. Pancreozlznrih,'a stirnulant of the secretion of
pancreatic enzymes in the extracts of the small intesti-ne. J.PHYSIOL. 1943;
I02:115-125.
HEADTNG RC, TollHrLL P, McLOUGHLTN GP et ar. Gastric enrptying rate
measurement in man. A doubfe isotope scanning technique for simultaneous
study of J-iquid and solid components of a rneal. GASTRONTEROLOGY 1976; 7I--
45-50.
HEAT'ON KV'I. TLre epidemiorogy of garÌstones and suggested aeti-ology.
CLIN.GASTROENTffi.OL - L973; 2: 67-83.
HÐNER P. Effect of C-terrninal octapeptide of cholecystokinin on guinea pig
ileum and gallbladder in vitro. ACTA.PFIYSIOL.SCAT,]D. ITTOì 7B-. 232-235.
¿i
¡
ttd
I
I
l_83
HEGARDT FG, DAM H. The solubility of cholesterol
bile sal-ts and l-eci-thin. Z.ERNAHRUNGS!'¡ISS 1971;
in aqueous solutions of
10: 223-233.
HEPNER G¡I. Effect of decreased galtbladder stimulation on enterohepatic
cycling and kinetics of bite acids. GASTROENTEROLOGY. 1975; 68: 1574-1581.
HOLAN KR, HOLZBACH RT, HERMANN RE et ai. Nucl-eation time; a key factor in
the pathogenesis of cholesterol gallstone disease. GASTROENTEROLOGY - 1979;
77: 611-617 .
HOLT S, REID J, TAYLOR TV et aÌ. Gastric emptying of solids in man' GUT'
l9B2; 232 292-296.
HOLZBACH RT, MARSH M, OLSZEI,üSKI M et al. Cholesterol solubiÌity in bile;
evidence that supersaturated bil-e is frequent in heaLthy man.
J.CLIN.INVEST. 1973; 522 1467-1479.
HONDA R, TOOULI J, DODDS lrlJ et aI. Effect of enteric hormones on
sphincter of Oddi and gastrointestinal myoelectric activity in flasted
conscious opossums. GASTROENTEROLOGY. 1983; 84: 1-9.,¡\f"iiI
HONG SS, MAGEE DF, CREI^IDON F.
evacuation. GASTROENTER0LOGY.
Thè,physiologic negulation of gallbladder
1956; 30: 625-630.
HORO!üITZ M, MADDERN GJ, CHATTERTON BE, et al. The normal menstrual cycle
has no effect on gastric emptying. BR.J.OBSTET.GYNAECOL. 1985; 922 7ß-746.
HUNDLEY JM, DIEHL WK, DIGGS ES. Cited by Kumar page '1300.
HUNT JN, KNOX MT. The regulation of gastric emptying ofl meals containlng
citnic acid and the safts of citric acid. J. PHYSIQL. London 1962; 163:
34-45.
r
HIINT ,IN, KNOX MT. A relation between the chain length of fatby acids and
184
the slowing of gastric erçtying. J.PHYSIOL. London 1968; L94z 327-336.
ì'ILTNT ,JN, KNox Mr.
London L969¡ 20l-z
Ttre sl-owing of gastric emptying by nine acids. J.PHYSIOL.
r61-r79.
HUIIT JN, STUBBS DT. The volune and energy content of meals as deterrninants
of gastric emptying. J.PHYSIOL.(London) 1915¡ 245: 209-225.
HURLOCK G, TAIÄLAY P. Principles of the enzlzmatic measurement of steroids.
J.BIOL.CHEM. L951¡ 2272 37-52
HtfflION SVù, SIEVER'T CE,Jr. \ÆNNES JA, et a1. Inhibition of gallstone
formation by sphincterotomy in the prairie dog. Reversal by atropine.
cASTRoENTERoLocY 1982 ; 82z 1308-1313.
INBffi.G !IV, WORIO JM. Human gallbladder fr¡nction after selective gastric
and total abdomj-nal vagotomy. ACT.CHTR.SCAIJD- 1969; I35z 625-633.
INGELFINGm. F,F, EBmT RB, FINDLAND M, et al. Editors. In Controversies in
internal medicine II. W.B. Saunders, Philadelphia. 1974¡ 545-559.
ITOH Z, TAKAFaSHI I. Periodic-cóntractions of the canine gallbladder
during the interdigestive state. AM.J.PHYSIOL. 19Bl-; 240: GlB3-Cl-89.
fVY AC, OLDBERG EA. A hornone mechanism for gallbladder contraction and
evacuation. AM.J.PHYSIOL. I92B; 86: 599-61-3.
JACOBS VüH, JAIJOVVITZ HD. The digestive tract. In Rovinsky JJ, Guttmacher
ÀF(eds): Medical, Surgical and Gynaecological ConpÌications of Pregnancy,
ed. Baftimore, Willj-ams and Wilkins. 1965; Chapter 10.
JAVITT !{B. Editor. University Park Press, Balti¡rore, ¡4D. f9B0; 2L:
t03-l_50.
JIAIù R, VIGNERON N, NA^fEA Y. et aI. Gastric enptying and intragastric
clistribution of lipicls in rnarr. A new scirrtigra¡-rhic netlrcrd o-t sLutly.
DIG.DIS.SCI. L9B2; 27: 705-7ll-.
JOHANSSON C, KOLLBERG B, EFENDIC S. et al-. Effects of greater doses of
somatostatin on galtbladden empLying pancreatic enzyme output after oral-
-+!ü
1,
)
I
,J
t!
185
JORPES JE. The isol-ation and chemistry of secretl n and choJ-ecystokinin.
GASTROENTEROLOGY 1968; 552 157-164.
KADZIOLKA R, NILSSON S, SCHERSTEN T. Prevalence of hyperlipoproteinaemia
in men wibh gal-Ìstone disease. SCAND.J.GASTROENTEROL. 1977; 122 353-355.
KEANE FB, D1MAGNO EP, DOZOIS RR et al. Relationships among canì-ne
intendlgestive exocrine pancreatic and biliary flow, duodenal motor
activity, plasma pancreatic polypeptide and motilin. GASTROENTEROLOGY
1980; 7B: 310-316.
KELLOI/'I JE, BORODY TJ, PHILLIPS SF eb al. SuLfapyridine appearance in
plasma after salicylazosutfapyridine. GASTROENTEROLOGY 1986) 91: 396-400.
KELLY KA, CODE CF. Effect of transthoracic vagotomy on canine gastric
electrical activity. GASTROENTEROLOGY. 1969:' 592 51-58.
KERN F, Jr ERIKSSON H, CURSTEDT T et al-. Effect of ethinylestradiol oñ
biliary excretion of bile acids, pþosphatidylcotines and chofesterol in
the bile fistula óf the rat. .l.lipf¡ nes. 1977; 18: 623-634.
KERN F, JR. ERFLING V\i, SIMON FR et al. Effect of estrogens on the liver
GASTROENTEROLOGY 1978; 752 512-522.
KERN F, JR. Clinical aspects of bife acid metabolj-sm. RENDIC GASTROENTEROLOGY
1975; 7 z 205-212.
KERN F,Jr. EVERSON GT, DEMARK B et aI. Bì-liary lipids, bile acids, and
gallbladder function j,n the human female; effects of pregnancy and the
ovulatory cyc1e. J.CLIN.INVEST. 1981; 68: 1229-1242.
KERN F, Jr. EVERSON GT, DEMARK B et al. Biliary lipids, bile acids and
gallbì-adder function in the human female; effects of contraceptive
I
,]
TI
I
t-86
steroids. J.LAB.CLIN.MED. 1982; 992 798-805-
KEy pH, BONNORRIS GG, MARKS J!ü et al. Biliary lipid synthesis and secnetion
in. gallstone patients before and during treatment with chenodeoxycholic
acid' J'LAB'cLrN'MED' 1980;95:816-826'
KING pM, ADAM RD, PRYDE A. et al. Relalionships of human antroduodenal
motility and tnanspyloric fluid movement: non-invasive observations with
real-time ultrasound. GUT. 1984; 25¿ 1384-1391.
KLOPPERT AM, FUCHS F editors. In Endocrinology of pregnancy. 2nd edition.
1977 .Hagerstown MD, Harper and Row,
KOVANEN PT, BROhIN MS, GOLDSTEIN JL. Increased binding of low density
tipoprotein to liver membranes from rats Lreated with 17 alpha elhinyl
oestradiol. J. BIOL-CHEM. 1979, 254; 11367- 1 i373.
KRAG E, PHILLIPS SF. Actlve and passive blle acid absorption in man.
Perfusion'studies of the iLeum and jejunum. J.CLIN.INVEST. 1974; 532
1 686- 1694 .
KROOP HS, LONG !1lB, ALAVI A. et a1,. Effect of water and fat on gastric
emptying of solid meals. GASTROENTEROLOGY. 1979; 772 997-1000'
KUMAR D. fn vitro inhibitory effect of progesLerone on extrauterine human
smooth muscle. AM.J.OBST. & GYNAE. 1962; 84: 1300-1304.
La BROOy SJ, MALE PJ, BEAVIS AK et aI. Assessment of the reproducibiJ-ity
of the lactulose H2 breath as a measure of mouth to caecum transit time.
cUT. l9B3; 24¿ 893-896.
La MORTE Wt^t, GACA JM, VúISE EW et al. Choledochal sphì-ncter relaxation in
respon se to histamine 1n the prirttaLe. J. SURG. RES. l9B0 ; 28: 373-378.
La MORTE Wht, SCHOETZ DJ, Jr. BIRKETT DH et al. The role of the gallbladder
LB7
in the pathogenesis of chol-esterol gallstones. GASTROENTROLOGY. 1979¡ 772
580-592.
IÄRUSSO NF, HOFFMAN NE, HOFMANN AF et al. Effect of primarlz bile acid
ingestion on bile acid metabolism and biliarlz lipid secretion in gallstone
patients. GASTROENTROLOGY. 1975 -, 69 -. 130I-1314.
IÄRUSSO NF, SZCZEPA¡trIK PA, HOFï4ANN AF. Effect of deoxycholic acid ingestion
on bile acid metaboÌism and bì-liary J-ipid secretion j-n normal subjects.
GASTRO$TEROLæY. 1977 ; 722 I32-L40.
LADAS SD' ISAACS PET, MURPHY CM et al. Comparison of the effects of medi-um
and long chain triglyceride containing liquid meals on gal-tbtadder and
smal-I intestinal- functon in normal.man. GUT. I9B4; 252 405-41I.
LEVITT ¡4D' HASTINGS J, BRCCREN,TA. Hydrogen (H2) catabol-ism in the colon
of the rat. J.I"AB.0,IN.MED. L974¡ 84= f63-167.
LEYSSAC PP, BUKHAVE K, FREÐFRIKSÐI O. fnhibitory effect of prostagl-andins
on j-sosmotic fluid transport by rabbit gall-bladder in vi-tro and its
¡nodification by blockade of endogenous PGE biosynthesis with indonrethacin.
ACTA. PhYSIOL. SCAND. 1974¡ 92: 496-507.
LICFIEN BERGER LM, TRIER JS. Ctnnges il gastrin levels,
i¡take, and duodenal mucosal- growth during lactation.
AM.J. PHYSIOL. 1979; 237= E9B-E105
food
1BB
LfEDBRG G. Thre .effect of vagotomy on gallbladder and duodenal pressures
during rest and stimulation witl. cholecystokinin. ACTA.CHIR.SCAIJD. 1969¡
135: 695-700.
LIN TM. Actions of gastrointestnal hormones and rel-ated peptides on the
motor fr:nction of the biliary tract. GASTROEI\TEROLOGY. 1975¡ 692
r006-L022.
LfN TM, CFIANCE RE. Spectrum of gastrointestinal actions of bovine PP in
Bloom SR (ed): Gut Hormones, Edinburgh: Churchll-l Livingstone, Ì978, p
242-246 -
LIN TM, CIIÄNCE R. Bovi-ne pancreatic polypeptide (BPP) and avian pancreatic
polypeptide (APP). GASTROÐ{TEROLæY. 1974¡ 672 737-738.
LINDBLAD L, LUNDHOLIvI K, SCHRSTÐ{ T. Influence of cholic and
chenodeoxycholic acid on biliary cholesterol secretion in man.
EUR.J.g,IN.INVEST. L977 ; 7 : 383-388.
LONOVICS J, GUZMAN S, DEVITT P et aI. Rel-ease of pancreatic polypeptide in
humans by infusi-on of cholecystokj-nin. GASTROHVTROIOGY. 1980; 79:
Br7-822-
189
LONOVICS J, DEVITT P, WATSON LC et al. Pancreatic polypeptide.A review
ARCH.SURG. 1981; 1162 L256-L264.
LONOVICS J, DE:VITT P, RAYFTORD PL et al-. Actions of VIP, somatostatin and
pancreatic pollzpeptide on gal'Ibladder tension and CCK-stjmul-ated
gallbladder contraction in vj-tro. SURG.FORUM- 1979; 30: 407-409-
LOW-BEER TS, WICKS AB, HEATON Küü et al-. Fl-uctuations in serum and bile
tipid concentrations during the menstrual cycle. BR.MED-J. I9l'/; Iz
1568-1570.
LOW-BER TS, HEATON KW, HEAT'ON ST et al-. Gallbladder inertia and sluggish
enterohepatic circulation of bil-e salts in coel-iac disease. I"ANCET. L97L;
i: 99L-994.
LOIiV-BffiR TS, POMARE EW. Regulation of bile salt pool size in man. BR.MÐ.J.
\913; 2: 338-340.
LOV\]-BEER TS, IARVEY RF, DAVIES R et aI. Abnormalities of sennn
cholecystokinin and gallbladder enptying in celi-ac disease. N.ENGL.J.MED-
1915¡ 2922 96I-963.
LYNN J, I/VfLLIAIUS L, OTBRIH{ JR, et al-. Effects of estrogen upon bile.
190
Implications with nespect to gatl-stone fonmation. ANN.SURG. 1973; 178:
514-524.
MABEE TM, MEYER P, DENBESTEN L. et al. The mechanism of increased
gallstone formation in obese human suU¡ects. SURGERY. 1979; 792 460-468
MAKHLOUF GM. TransporL and motor flunctions of the gallbladder. VIEI¡IPOINTS
0N DIc.DIS. 1979; 11: No. 3.
MAKITA M, i^jELLS hlw. Quantitative analysis of fecal bile acids by gas -
Iiquid chromatography. ANAL. BIOCHEM. 1963; 5z 523-530-
MALAGELADA JR. QuantÍtation of solid liquid discrimination during digestion
of ordinary meals. GASTROENTEROLOGY. 1977; 72: 1264-1267 -
MALAGELADA JR, ROBERTSON JS, BROhIN ML et al. Intestinal transj-t of so-lid
and J-iquid compónents of a meal in health. GASTROENTEROLOGY. 1984; 87:
1255-1265.
McDOUGALL Rl'l, YAKYMYSHYN L' I/üALKER K et al-. The effect of wheat bran on
serum lipoproteins and biliary lipids. CAN.J.SURG. 1978; 212 433-435.
McMASTER PD, ELMAN R. On the expulsion of bile by the gal-lbJ-adder and a
reciprocal- relationship with the sphincten activity. J.EXP.MED. 1926; 442
1 73- 1 98.
MELTZER SJ. The disturbance of the law of contrary innervation as a
191
pathogenic factor in the diseases of the bile ducts and galÌ-bladder.
ÄI\4.J.MED.SCr. l_917; 153 z 469-477.
MnlDH,soHN D, MENIDELSOHN L, srApLE E. The catabolism in vitro ofchofesterol formation of the 7-epimeric hydroxycholesterol_s from
cholesterol in rat river. BrocHEM. BropHys.AcrA. 1965; 972 379-3gr.
MENGUY RB' HARLm{BECK GA, BOLLMAN JL et ar. rntraductal pressures and
sphincteric resistance in canj-ne pancreatic and biliary ducts after various
stimuli. SURG.cyN.OBSTET. 1958; 106: 306_320.
MESSING B, BORTES C, KUNSTT-INGER F et al. Does totaf parenteral nutritioninduce gallbladder sludge formation and lithiasis. cASTRoETÀITm.oLocy. lg83;84= 1012-1019.
METROPOLTTAII LrFE TNSURANCE coMpAIVy. Frequency of overweÍght and
underweight. Statistical Bulletin. 1960; 4I: 4.
¡'IETZGm AL, ADLER R, TIEYMSFIELD S. et aI Di-urna1 variation in biliarlz lipidcomposition. Possibl-e role in cholesterol gallstone formation.
N.ENGL.J.MÐ. I973ì 2BB: 333-336.
METZGR AL, HEYMSFIED S' GRUNDY SM. Ttre lithogenic index: a nurnerical
]-92
expression of the reÌative lithogenicity of bile. GASTROENTEROLOGY.
1972; 622 499-501.
MEYER JH, JONES RS. Canine pancreatic response to intestinally
perfused fat and products of fat di-gestion. AM.J.PHYSIOL. 1974i 226:
1 178-1187 .
MEYER PD, DENBESTEN L. A comparison of methods of bil-e saì-t pool
size measunements in the prairie dog gallstone model ( 39955 ) .
PROC.SOC.EXP.BIOL.MED. 1977 ; 1562 452-456.
MEYER PD, DENBESTEN L, GURNELL NJ. Effects of cholesterol galLstone
inductlon on gallbladder function and bile salt pooJ- size in the
prairie dog model. SURGERY. 1978; 83: 599-604.
MEYER JH, MAYER EA, JEHN D. et al-.Gástnic processing and emptying of
fat,. GASTROENTEROLOGY. 1986i 90: 1176-1187.
MEYER JH, OHASHI H, JEHN D. et al-. Size of Iiver particles emptied
from the human stomach. GASTROENTEROLOGY. 19Bi; 80: 1489-1496.
MOBERG S, CARLBERGER G. The effect on gastnic emptying of Lest meals
with various fat and osmolar concentrations. SCAND.J.GASTROENTEROL
9z 29-32.
197 4;
MOK HYI, VON BERGMANN K, GRUNDY SM. Effects of contínuous and intenmittent
feedlng on biliary lipi-d outputs in man: applicatj-on for measunements of
193
intestinal absorption of cholesterol and bile acids.J.LIPID.RES. 1979¡ 20:
389-398.
¡4OK FryI' VON Bffi,GMANN K, GRUNDY SM. Regulation of pool size of bile acids
in man. GASTROEDüTEROLæY. 1977¡ 73: 684-690.
lvOK HYI, GRUNDY SM. Gallbladder storage function in subjects with
gallstones. GASTROEIüTEROLOGY. (Abstr) I97B¡ 74: 1162.
l{OK fryI, VON BERGMANN K, GRUNDY SM. Kinetics of the enterohepatic
circulation during fasting: biliary J-ipid secretion and gallbladder
storage. GASTROEI{Tffi.OLOGY. 1980 ì 78: 1023-1033.
MOK IryI, VON Bffi.GMANN K, GRUNDY SM. Effects of interuption of enterohepatic
circulation on biliary lipid secietj-on in man. DIG.DIS.I97B; 23:
r067-I07s.
MOIüIrclvtrRY E. Cited by Rains page 686.
¡{OORE JG, CHRISTIA}J PC, COLEMAN RE. Gastric enptying of varlzing meal weight
and conposition in man. Evaluation by duaÌ liquid and solid phase isotopic
method. DIG.DIS.SCI. 1981; 26: 16-22.
L94
MUKHERJEE S, GUPTA S. Effects of gonadal hornones on cholesterol nretabol-ism
in tlre rat. J.ARTHEROSCLR..RES. 1967¡ 7: 435-452.
MUIT V, JORPES JE. Structure of porcine cholecystokinin - pancreazlzrnin.
EUR.J.BIOCHEM. l-968; 6z L56-I62.
NAII\YAI\4,\ F, VAN DER LINDEN W. Stratification of bile in the gallbladder and
gall-stone formation. SURG.cYN.OBSTET. 1975; l4l: 587-590.
NAGLFR R, SPIRO Hlt4. Heartburn in late pregna¡cy. Manometric studies of
oesophageal motor function. J.CLTN.IN\IEST. I96L; 40: 954-970.
NAMLIN E, BARTLETT MK, SI./[TTI JA.Routi-ne surgical emergencies of the abdornen
dr:rj-ng pregnancy. N.E\lcL.J.MED. 1951; 2442 l-28-13I.
NEBEI- OT, FORNES MF, CASTELL DO. ;Slzmptomatic Aastro-oesophageal reflux:
inciderice and precipitating factors. AM.J.DIG.DIS. L976; 21,: 953-956.
NESTH, PJ, HIRSCH EZ, COUZÐtrS EA. Ttre effects of chlorophenylisobutyric
acid and ethinyl estradiof on cholesterol turnover. J.CLIN.INVEST. 1965;
44: 891-895.
NEWMAII FIF, NORTFIUP JD. The autopsy incidence of gallstones. IIII.ABST.SURG.
195
1959; 109: I-l-3.
NTELSEN JR. The development of choÌel-ithiasis following vagotomy.
AM.J.DIG.DIS. 1964; 9: 506-508
NILSSON S. Gallbladder disease and sex hormones. A statistical study.
ACTA.CHIR.SCAI\D . 1966; J.32: 275-279 -
NILSSON S, SCHERSTÐ''I T. Inportance of bile acids for phosphoJ-ipid secretion
into human hepatic bile. GASTROH\IIEROLOGY. 1969; 572 525-532-
NILSSON S, STATTIN S' Gallbl-adder enptying during the normal menstrual
cycre.A chol-ecystographic study. ACTA.CLrN.scAlID. 1967; l-33 : 648-652.
NORTTIFIil,D rc, HOFMANN AF. Biliarlz lipid output during three neals and an
overnight fast. I. Relationship to,bile acid pool size and cholesterol
satnration of bile in galÌstone and control subjects. GUT. 1975; t6: l-It.
NORTIIFIÐ,D rc' KUPFR RM, MAUDGAL DP'et al. Gallb1adder sensitj-vity to
cholecystokinin in patients with gallstones. BR.MED.J. 1980; 2BO: 143-L44.
ODH-L I¡JD, Ivlol,rrcH ME. The pharmacorogy of contraceptive agents.
AIiN.REV.PHARM. 1974 ¡ 4L3-434.
]-96
ORD W. Cited by LA t"lORTE page 580.
OS CH van SLEGRS JFG. Correlation betr,r¡een (Na*-K+)-activated ATPase
activities and the rate of isotonic fluid transport of galrbladder
epittrelium- BIOCHHU.BIOPHYS.ACTA. IglI¡ 24I-. 89-96 -
PALLIN B, SKOGLUND S. Ner.¡ral and humoral- control of the
gallbladder-emptying mechanism in the cat. ACTA.PTTSfOL.SCAIJD. 1964; 60:
348-362.
PALMER RL. A psychosomatic study of vomiting of early pregnancy.
J.PSYCHOSOM.RES . 1973; I7 z 303-308.
PÄLFRAMAN A' MEIRE HB. Real tinre ultrasound. A new method for studying
gallbladder kinetj-cs. BRIT.J.RADIOL. 1979; 52: 801-803.
PARKIN GJS, SIvIIITI RB' JOHNSTON D. Gall-bladder volume and contractility
after truncal, selective (parietat ceII) and highly selective vagotomy in
man. AIiN.SURG. L973¡ I7B: 58I-586.
PERMAN JA' ¡4ODLERS S, OLSON AC. Role of pH in production of hydrogen fron
carbohydrates by colonic bacterial flora. Studies in vivo and in vitro.
L97
J.CLIN.TN\ÆST. l98l; 67: 643-650.
PERSSON CGA. Adrenoreceptors in the gallbladder. ACTA.PHARMACOL.TOXICOL-
L972; 3I: 177-185.
PRTSEMILIDIS D' PANVELfWALLA D, AHRÐ{S EH. Effects of cÌofibrate and of an
estrogen progestín combination on fasting biJ-iary lipids and cholic acid
kinetics in man. GASTROENTROIOGY. 1974¡ 662 565-573.
POMARE EW, HEATON KW, LOW-BEffi. IS et al. The effect on wheat bran upon bile
salt nretabolism and upon the lipid conposition of bile in gallstone
patients. AM.J.DIG.DTS . 1976¡ 2I; 52I-52G.
POMERANZ rs, DAVrsoN JS, stIAFFm. EA.'rn vitro effects of pancreatic
polypeptide and motilin on contractility of human gallbladder. DIG.DIS.SCf.
1983; 28: 539-544-
POTIER l4G. Observations of the gallbladder and bile during pregnancy at
term. JAMA. 1936; 106: 1070-1074.
198
RAINS AJH. Researches concerning the formation of gallstones. BR. MÐ.J.
L962¡ 2: 685-69I.
RAND RN, DIPASQUA A. A new method for the deterrnination of
bilirubin.CLIN.CHEM . 1962¡ 8z 570-578.
READ NW, MILES CA, FISHffi. D et aI. Transit of a meal through the stomach,
smafl- intestine, and colon in normal subjects and its role in the
pathogenesis of diarrhoea. GASTROEIVIR.OLOGY 1980; 79: L2l6-I282.
READ NlV, AL JAI\ABI N, BATES TE et al-. Effect of gastrointestj-nal intubation
on the passage of solid meal ttrrough the stomach and smalf intestine in
humans. GASTROÐJTEROLOGY 1983; 84: L56B-I512.
REDINGER RN. The effect of Ìoss of gallbladder function on biliarlz lipid
conposi-tion in subjects with cholestprol gallstones. GASTROÐJTffi.OLOGY 1976;
71,: 470-474.
RÐINGER RN, SMALL DM. Bil-e composition, bj-le salt metabolj-sm and
gallstones. ARCH. II\IRN.MED- L972; 130: 618-630.
REICHED{ J, PAUIGARTîJER G. Excretory function of the liver. In liver and
Biliary Tract Physj-ology. I. NIFRNATIONAL REVIEW OF PTrySIOLOGY. Chapter
3.W.B. Javitt, editor. University Park Press, Balti¡ore, M.D. 1980; 2L:
103-rs0.
REICH$J J, PAUIUIGART}IER G. Relationship between bile fl-ow and Na+ K*
adenosinetriphosphatase in liver plasma rnembranes enriched in the bite
canalictrli. J.CLIN-INVEST. l-977 ; 6O: 429-434 -
L99
REYES H, KERN F, Jr. Effect of pregnancy on bile flow and bitia4z lipids in
the hamster. GASTROENTEROLOGY 1979¡ 76: 144-150.
RIEGÐ, C' RAVDIN IS' JOHNSTON CG. Studies of gallbladder function, VI. TLre
absorption of bile sal-ts and cholesteróI from the bile free gallbladder.
AM.J.PHYSIOL. 193I-L932¡ 99 : 656-673.
RIEGEL C' RAVDIN fS, ¡4ORRISON PJ et aI. Studies of gallbladder function.
XI. The conposition of gallbladder bile i-n pregnancy. JAMA. 1935; I05:
l-343-1344.
ROCK E, MALMUD L, FISHFR. RS. Gallbladder ernptying in response to sham
feeding. GASTROENTROLOGY (Abstr) 1981; B0: 1263.
ROCK E, MALMUD L, FISHR. RS. Gallbladder enptyì-ng after meals of different
composition.CaStnoElrlERolocy (Abstr) 19Bf; B0z 1263.
ROOVRS JE, EVRARD H, VAIiDR.HAECITIE. An jnproved method for measuring human
blood bile acids, O,IN.CHIM.ACTA. ,l-968; l-9: 449-457.
ROSLYN JJ, PfTT HA, MANN LL et al. Gallbladder disease in patients on
long-term parenteral nutrition. GASTROENTEROLOGY I9B3 ; B4z l4B-154.
ROZE C, COUruRIER D, CIIARfOT J. et aI. Inhibition of gastric, electricaÌ
and nechanical activity by intraduodenal agents in pigs and the effects of
vagotonqr. DTGESTfON 1977; 15: 526-539-
ROUS P' MclvlA^STER PD, DRURY DR. Observations on some causes of gallstone
formation. r. B<perjmcntar chorcrithiasis in the absence of stones,
200
infection and gall-bl-adder influences. J.EXP.MED. 1924¡ 89: 77-96.
ROYAL COLLEGE OF GENERAL PRAOIITIONERS. Oral contraceptive study. OraI
contraceptives and gal-lbfadder diseases. LANCET L9B2¡ ii: 957-959.
RYAN JP, PET,T,ECCHIA D. Effect of ovariari hormone pretreatment on
gallbladder nxrtility in vitro. LIFE SCI. I9B2; 31: 1445-1449.
RUCKEBUSH M, FIORA¡4ONTI J. Electrical spiking activity and propulsion in
small intestine in fed and fasted rats. GASTROÐ{TEROLOGY L975; 68:
1500-t508.
SAFAfE-SHIRAZI S, DENBESTN L, ZIKE V\IL. Effect of bile salts on aonac
permeability of the esophageaÌ muscosa and their production of
eosophagitis. GASTROE\ITROLOGY 1975; 68: 728-733.
SAMPLINR RE, BH{NHIT PH, CO¡4ESS LJ. Gallbladder disease in Pjma Indians;
demonstration of high prevalence and:early onset by cholecystography.
N.ENGL.J.MED. 1970¡ 283: 1358-1364 -
SAI{DBLOM R, VOEGTLIN WL, IVY AC. Ttre effect of cholecystokinin on the
choledocho-duodenal mechanism.(Sphincter of Oddi). AM.J.PHYSIOL. 1935; 93:
175-180.
SAIIDV{EISS DJ, PODOLSKY HM, SALTZSTEIN HC. Deaths frorn perforation and
hemorrhage of gastroduodenal ulcer during pregnancy and puerperium: review
of literature and report of one case. AI"I.J.OBSTET.GYNAECOL. 1943¡ 452
131-r36.
SARLES JC, BIDART JI,l, DEVAUX It4A et al. Action of cholecystokinin and
20L
caerulein on the rabbit sphincter of Oddi. DfGESTION 1976¡ i4z 4L5-423.
SARLES H, HAGE G, LAUGfm R et aI. Present status of the
anticholecystokinin hormone. DIGESTION 1979 ¡ 19 : 733-736.
SCFIÄDE RR' PH,EKANOS Mf, TAUXE WlJ et al-. Gastric errptying dr:ring pregnancy.
GASTR.OENTR.OLOGY (Äbstr) . I9B4¡ 86: 1234.
SCHATZMAN HJ. Die wirkung eini ger steroid hornone und von hydroxydio auf
den tonus des gJ-atten darnmuskels. HELV. PHYSIOL. et PHARI4ACOL. ACTA. 196I;
19: Cl06-C110.
SCHR. E, Treatrnent for nausea of pregnancy. POSTGRÀD.MED. L965¡ 372
610-613.
SCHLIffi.F G, SCHELL${BERG B, STEFIL A et al. Biliary cholesterol saturation
and weight reduction - effects of fa.sting and Ìow calori-e diet. DIGESTION
l-981; 2Lz 44-49-
scHoETZ DJ, La t"loRTE I¡üE, wrsE w et ai. Mechanical properties of primate
gallbladder: description by a dynarnic method. AIvl.J.PtrySfOL. 1981; 24Iz
c376-381.
SCHLILTZE K, CIfiISTENSEN J. Lower sphj-ncter of the oposum esophagus in
pseudopregnancy. GASTROENTEROLæY L977 ; 73 : 1082-1085.
SCFMARTZ A' LINDENMAYffi. cE, ALLH{ JC. The sodium potassium adenosine
triphosphatase: pharmacolggic, physiological and bionrechani-cal aspects.
PHARMACOL.REV. 1975; 272 3-L34.
202
SCIII^IARTZ CC, AL¡4OND R, \ZLAHCH/IC ZR et al. Bile acid metabolism in
cirrhosis. V. Deterrnination of biliarlz lipid secretion rates in patients
with advanced cirrhosis. GASTROEIüIEROLOGY 1979¡ 772 II77-IIB2.
SCFMARTZ CC, FALLORAN IÆ, VLAHCEVIC ZR et al. Preferential- utilisation of
free cholesterol frorn high density lipoproteins for biliary chol-esterol
secretion in man. SCIBùCE. I97B¡ 200: 62-64.
SCFIWARTZ CC, BERMAN M, VI"AHCEVIC ZR et al. Multiconpartmental analysis of
chol-esterol- nretabolism in man. Characterisation of the hepatic bile acid
and biliarlz cholesterol precursor sites. J.CLfN.IN\ÆST. I97B; 6L: 4OB-423.
SCRAC,G R, IvlCtrLICFIAfl, AJ, SEAMARK RF. Oral- contraceptives, pregnancy and
endogenous oestrogens in gall stone disease. A case-control study.
BR.MED.J. I9B4¡ 2BBz I795-L799.
SCCIrII LD, LESTER R, VA]J TTIIH, DH et al. Pregnancy-reJ-ated changes j-n smal-l
intestine myoelectric activity in the rat. GASTROEXVTEROLOGY 1983; 84:
301-305.
SEDFAGHAT A, GRUNDY SM. Chol-esterol crystals and the formation of
cholesterol ga11 stones. N.ENGL.J.MED. 1980; 302: 1274-1277.
SÐ,IGSON D, MARINO J, DODSON E. Detennination of sulfobronxrpthalein in
serum. CLIN.CHEM. 1957¡ 3z 638-645.
SHAFFER EA, BRAASCH JV{, SMALL DM. BiIe conposition at and after surgery in
normal persons and patients with gall stones. Influence of cholecystectony.
N.ENGL.J.MED. 1972; 287 z L3I7-I322.
203
SHAFFR. EA. SMALL DM. Gall-stone disease: pathogenesis and managenent.
CURR.PROB.SLTRG. L976; l-3(7) z 3-72.
SHAFFR. EA' SMAI,L DIta. Biliary lipid secretion in cho]-esterol gallstone
disease. Ttre effect of cholecystectomy and obesity. J.CLIN.INVEST. L977;
59: B2B-840.
SHAFFR EA, l"lcOR¡4OND P, DUC'GAltr H. Quantitative cholescintigraphy:
assessnìent of gallbladder filling and emptying and duodenogastric refh:x.
GASTROET'ITROLOGY 1980 ; 79 : 899-906.
SfmFm. S' FIAUSER S, BEKERSKY I et al-. Biochenrical site of regulation of
bile acid biosynthesis in the rat. J.LIPTD RES. I9l0¡ 11: 404-4LI.
Sf¡4ON FB.' SLIIITIRLAND E, ACCATINO L. Stimulation of hepatic sodium and
potassium- activated adenosine triphosphate activity by phenobarbital-; its
possible role in regulation of bile flow. J-CLIN-INVEST. 1977¡ 59:
849-861.
SMALL DM. Physicochernical- studies of cholesterol gall stone formation.
GASTRONTEROLOGY 1967 ì 52 2 607-610.
SMALL DM. Management of gallstones particularly the splent variety;
advantages of a varied and individualised approach. In Controversies of
Internal Medicine II. RB Hcert, M Findland, AS Relman Editors. WB Sanders
Philadelphia. L974; 545-559.
SMALL DM. Cholesterol nucleation and growth in ga11 stone formation.
N.H{cL.J.MÐ. I9B0; 302: 1305-1306.
,l
d
204
SMALL DM' DOIVLING RH, REDINbER RN. Ttre enterohepatic circulation of bilesalts. ARCH.IIfT.MED. L972¡ 130: 552-573.
sNÐEcoR GI,v, cocHRAN IG. statisti-car methods. 7th ed. Ames, fowa: rowa
State University Press 1980.
SOLOI"IONS NW, VITffi.I FE, HAMILTON LH. þplications of a sinple
gas - chrornatograph techrnique for measuring breath hydrogen.
J.I"AB.CLIN.MED . L97l; 90: 856-862 -
SOMYLO AP' SOIVIYLO AV. Vascular snrooth muscle; pharmacology of normal- and
hlrpertensive vessels. PFTARMACOL.REV. I97O¡ 222 249-353.
souLES MR. Nausea and vorniting of pregnancy: role of human chorionic
gonadotropin and l7-hydro>qprogesterone . OBSTET. cylIAECoL . 198 0 ; 5 5 :
696-700.
SPARKMAN RS. GaÌl-stones in young \^/ornen. ANN.SuRG. 1957; r45: BL3-824.
SPELLT\4AN SJ, SHAFFER EA, ROSH\II{ALL L. Galfbladder enptying in response to
cholecystokinin. A cholescintigraphic study. cAsrRoExvTm.ol-æy L979; 77 z
11s-120.
STANLEY MM. Quantification of intestinar functj-ons during fasting:
Estimations of bile salt turnover, fecal calcium and nitrogen excretions.
METABOLISM 1970¡ 19: 865-875.
STEINMAN G. Cited by RAINS page 686.
.1
rd1i;
Í
I
t
STEMPEL JM, DUA\IE !{C. Biliarlz lipids and bile acid pool size after vagotorny
205
in man. Evidence against a predisposition to galJ-stones. GASTROEITTEROLOGY
L97B; 75: 608-611.
STEPH$JS JR. W@LSON RF, COOKE AR. Osmolyte and trlptophan receptors
controlling gastric emptying in the dog. AI4.J.PI-IYSIOL. 1976; 23I: B4B-853.
STEPHÐ'IS JR, WOOLSON R, COOKE ÄR. Effects of essential and nonessential
amino acids on gastric enptying in the dog. GASTROEIITEROLOGY 1975; 692
920-921 .
STRAMEI\IINOLf G, DI PADOVA C, JUALANO M. et al. Ethinyloestradiol--induced
inpairment of bile secretj-on j-n the rat; protective effects of
S-adenosyl-L-methionine and its implication in estrogen
metaboIism.cASTROH\TTEROLOGY 1981 ; B0 : I54-I58.
STURDEVANIT RA, STERN DH, RESIN H et al_. Effect of graded doses of
octapeptide of cholecystokinin on gallbladder size in man. GASTROBJTEROLOGY
1973; 64= 452-456- , :
SUNDLR. F',ALUI,4C|¡IS J, HAKANSON R eC aI. VIP innervation of the gallbladder.
GASTRONTEROLOGY 1977 ¡ 72: 1375-1317 -
SUI'OR DJ' !úfOLEY SE. A statistical survey of the conposition of gallstones
in eight countries. cUT I97I¡ L2z 55-64.
SUT'OR DJ' VüIOLEY SE. The nature and incidence of gallstones containing
calcium. cUT 1973¡ L z 2\5-220.
SI¡IELL L, BÐ-L cc, vr,AHCEVrc zR. Relationship of bile acid pooJ- size to
biriary lipid excretion and the formation of rithogenic bife in man.
GASIROEI\TR.OI,OGY \97L; 61 : 7],6-722.
I
t
206
SI/'IINHOE JR, COCHRANE G0, !,JISHART R, Oesophageal stricture due to reflux
oesophagitis in pregnancy: case report. BR.J.OBSTET.GYNAECOL. 1981; 88:
1249-1251.
TARPILA S, METTINEN TA, METSARANA L. Effects of bran on serum cholesterol
faecal mass, faL, bile acids and neutral stenols, and bÍliary l1pids in
patients with diverticular disease of the colon. GUT 1978; 19: 137-145.
THE CORONARY DRUG PROJECT RESEARCH GROUP. GalIbladder disease aS A SidC
effect of dnugs influencing Iipid metabolism; experience in lhe coronary
drug project. N.ENGL.J.MED. 1977; 296: 1'l85-1190.
THISTLE JL, SHOENFIELD LJ. Lithogenic bile among young fndian i4romen.
Lithogenic potential decneased with chenodeoxycholic acid. N.ENG.J.MED.
197 1 t 2B4z 177 -181 .
THISTLE JL, ECKHART KL, Jr. NENSEL RE et al. Pnevalence of gal-Ibladder
disease among Chippewa Indians. MAYO CLIN:PROC. 1971:, 46: 603-608.
THOMAS JE, CRIDER J0, MORGAN CJ. SÇudy of reffexes involving the pyloric
sphincter-and antrum and theln role in gastric evabuation. AM.J.PHYSIOL.
1934; 108: 683-700.
THOMPSON DG, O'BRIEN J, McCARTHY M et al. Oral mj-croflora afflect post
prandial exhaled breath hydrogen concentration (Abstr). GUT l9B3; 242 1978.
THORNTON JR, EMMETT PM, HEATON KIIJ. Diet and gal,Istones: effects of refined
and unrefined carbohydrate diets on bile cholesterol saturation and bile acid
metabol-ism. GUT 1983; 2: 2-6.
THUREBON E. Human hepatic bile; composition changes due to an altered
enlet'ohepatic circulation. ACTA.CLIN.SCAND.SUPPL. 1962; 303: 1-63
II
¡
207
TIEDEMANN F, GREMELIN L. cited by RAINS page 685
TRITAPERE R, D] PADOVA C,
oestrogen. N.ENG. J.MED.
ZUIN M et aI. Lithogenic bil-e afler conjugated
(letten). 1976; 295: 961-962.
TROTMAN B!ù, PETRELLA EJ, SOLOWAY'RD et al-. Evaluation of nadiographic
lucency on opaqueness of gallstones as a means of identifying cholestenol
or pigement stones. Correlation of lucency on opaqueness with calcium and
mineral. GASTROENTEROLOGY. 1975; 68: 1563-1566.
TURLEY SD, DIETSCHY JM. Regulation of biliary cholesterol output in the
rat; dissociaLion from the rate of hepatic cholesterol synLhesls, bhe size
of t,he hepatic cholesterol- ester pool and the hepatic uptake of chylomicron
cholesterol. J.LIPID.RES. 1979; 20z 923-934.
TSUTSULOPOULOS G. cited by YOLINDA and MORI page 252.
UVNAS-MOBERG K, ERIKSSON M, BLOMOUIST LE et al. Influence of suckling and
feeding on insul-in, gastrin,somatostatin and VIP fevels ln penipheraì-
venous blood of lactating sows. ACTA.PHYSIOL.SCAND. 1984; 121: 31-38.
VALDIVIESO V, PALMA R, NERVI F. et al. Secretlon of biliary Iipids in young
Chilean htomen with cholesterol gall-stones. CUT 1979; 20: 997-1000.
VAN BERGE HENEGOU!ìIEN GP, HOFMANN AF. Nocturnal galÌbladder stonage and
emptying in gallstone patients and healthy subjects. GASTROENTEROLOGy 1978;
75: 879-885.
VAN DER IIIERF SDJ, VAN BERGE HENEGOU1iIIEN GP, PALSMA DMH et aI. Gallbladder
motor function and small- intestinal- transit during lngesLlon of low doses
of ethinyl estradiol (EE) plus desogeslrel (D). GASTROENTEROLOGY (Abstr)
1984; 86: 1286.
208
VAII Tï{Im, DH' GAVALR. JS, STREMPLE J. Lower esophageal sphincter pressure
i-n wornen.using sequential oral contraceptives. GASTROH\I"IEROLOGY l-976¡ 7Lz
232-234.
VAI\ TïìItr, DH, GAVALR JS, JOSHI SN et aI. Heartburn in pregnancy.
GASTROENTROLOGY 1977 ì 722 666-668 -
VAI{ I/VAGENA}'I G, JENKINS RH. Experimental exarnination of factors causing
ureteral dilatation of pregnancy. J.LIROL. 1939¡ 422 10f0-1020.
VLAHCEVIC ZR, BET,T, CC,Jr. BUHAC I et al. Diminished bile acid pool size in
patj-ents with gal-lstones. GASTROH\IEROLOGY 1970¡ 59: 165-173.
VON BERGMAN. K, MOK HYI, GRUNDY SM. Distribution of the bife acid pool in
the fasting state in man. GASTROH\IEROLOGY 1976 ¡ ]I: A4I.
VON HH,MSBACH M. cited by I"A I4ORTE et al page 580.
WAGNER cr, TRCIMAN BVù, sor,owAY RD. Kinetic anarysis of biriary ripidsecretion in man and dog. J.CLIN.INVEST. 1976¡ 57: 473-477.
WALD A, VAN TFIIfl, DH, HOECHSTHIIER L et al. Effect of pregnancy on
gastrointestinal- transit. Dfc.DfS.SCI. I9B2; 27 z 1015-1018.
IVALD A, VAIJ.TIIIEL DH, HOECHSTHIIR L et a1. Gastrointestinal transit; the
effect of the menstrual cycJ-e. cASTRoH\].IERoLocy 19Bt; B0: ]-497-1500.
VÙALSH JH. Cholecystokinin in gastrointestinal disease, pathophysiology
209
diagnosis and management. MHY sleisenger, JS Fordtran Editors. vùB
Saunders, PhiladeJ-phia. 1978 ¡ 1,22=124.
WALTTON AG. The formation and properties of precipitates. Vol-. 23 New York.
I}üIERSCIENCE L967.
WATIS JMcK, JABLONSKI P, TOOULI J. The effect of added bran to the diet on
the saturation of bile in peopJ-e without gallstones. AM.J.SURG. 1978; 135:
32r-324 -
VüETNER K, GRAFIAI4 LS, REEDY T et al. simultaneous gastric emptying of two
solid foods. GASTROENTEROLOGY l9B1; BL: 251-266.
I/ùERNffi. D' EMMETI PM, HEATON KW. Effects of dietary sucrose on factors
inffuencing cholesterol gal-l-stone formation. cur r9B4¡ 25: 269-274.
WESTPHAL K, GLETCHMANN F, JorK AG. cited by wood and sva¡ik. 1983.
I¡IIIITE CM, HOWAT J]{I, SCHOEFfH,D PF. Lithogenic bile a study j-n wornen taking
oral contraceptives, BR.J.SURG.Ì9Bti 622 664-665.
VüIIITE Tl' BOURDE J. A new observatj-on on human intraductal pancreatic
pressure. SURG.GYN.OBSTET. 1970; I30: 275-278.
VIHITING IVLI' DOm{ RHL' WATTS J. Precisj-on and accuracy in the measurement of
t.l.e cholesterol- saturation index of duodenal bi-le. Lack of variation due to
the nenstruaÌ cycÌe. GASTROEIiTEROLOGY I9B1; B0: 533-538.
I/ùHITING lvLI' WAT'IS J. Supersaturated bile fron obese patients without
gallstones supporLs cholesterol crystal growlh but ¡rot nucleaLion
2L0
GASTROETITEROLOGY 1984i 86:' 243-248.
wrENm. r, rNouE K, FAGAN cJ et al. Rérease of cholecystokinin in man.
AIJN.SURG. 19Bl; 194: 32I-325.
VùILLIA¡4S CN, l"lORSE JWI, MacDONALD A et al. fncreased tithogenicity of bileon fasting in normaì- subjects. AM.J.DIG.DIS - I9j7; 22: IB9=194.
WILLIAMS CN' SCALLION SM, ¡4CART{Y SC. Bile acid pools, percent biliary
cholesterol saturation and serum lipids during the menstruaÌ cycle.
GASTROENTEROLOGY (Abstr). 1980; 7Bz L326.
WTLLTAMS PF, srMoNS LA, TURTLE JR. Plasma lipoproteins in pregnancy.
HORMONE RES. 1976; 7: 83-90.
WINKELSTEIN A' ACHSNER PVt. The pressure factors in the biliary duct system
of tlre dog. AI4.J.MED.SCI. Ig24r 16'8: 812-819
IVINKil,STEIN A, ACHSNR. PW.The mechani-sm of the flow of bile from the liverto the intestines:concfusions frorn previous studies. AM.J. MED.SCI. 1926¡
174: 104-11Ì.
WOOD JR, SVANVIK J. Gallbladder water and electrolyte transport and itsregulation. GUT 1983; 24-. 579-593.
WOROBETZ LJ' BAKR RJ, McCALLU¡4 JA et al. The effect of naloxone, norphine
and an enkephalin analognre on cholecystokinin octapeptide - stimuÌated
gallbJ-adder enptying. AM.J.GASTRO. 1982¡ 772 509-511.
YAU I¡¡¡4' MAKFILOUF GM' ÐVüARDS LE et al. l4ode of action of cholecystokinin
2IT
and refated peptides on gallbladder muscle. GASTROEIüTEROLOGY ]-973; 65:
45r-456 -
YAU hM, YOUEIR. ML. Modulation of gallbladder nxrtility by intrinsic
cholinergic ner:rons. AM.J.PI{YSIOL. L9B4¡ 247 : G6624666.
YLOSTALO P, KIRKINÐü P, IIEIKKINEII J et a]-. Gallbladder vol-unre and serum
bile acids in cholestasis of pregnancy. BR.J.OBSTET.& GYN. L9B2¡ 89.-
59-61.
YOSHIDA T, I4ORI T. The effects of sex steroids upon the motility of
isolated smaÌl- intestine of rabbi-ts. ACTA.OBSTET.GYNAE.JAP. L969; l-6z
252-257.
ZAHOR Z' STRNBY HN, KAGA\I A et al. Frequency of cholel-ithiasis in Prague
and Malmo. An autopsy study. SCÀND.J.GASTROENTEROL. L974¡ 9z 3-7.
Related Documents











