COPYRIGHT AND CITATION CONSIDERATIONS FOR THIS THESIS/ DISSERTATION o Attribution — You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use. o NonCommercial — You may not use the material for commercial purposes. o ShareAlike — If you remix, transform, or build upon the material, you must distribute your contributions under the same license as the original. How to cite this thesis Surname, Initial(s). (2012). Title of the thesis or dissertation (Doctoral Thesis / Master’s Dissertation). Johannesburg: University of Johannesburg. Available from: http://hdl.handle.net/102000/0002 (Accessed: 22 August 2017).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
COPYRIGHT AND CITATION CONSIDERATIONS FOR THIS THESIS/ DISSERTATION
o Attribution — You must give appropriate credit, provide a link to the license, and indicate ifchanges were made. You may do so in any reasonable manner, but not in any way thatsuggests the licensor endorses you or your use.
o NonCommercial — You may not use the material for commercial purposes.
o ShareAlike — If you remix, transform, or build upon the material, you must distribute yourcontributions under the same license as the original.
How to cite this thesis
Surname, Initial(s). (2012). Title of the thesis or dissertation (Doctoral Thesis / Master’s Dissertation). Johannesburg: University of Johannesburg. Available from: http://hdl.handle.net/102000/0002 (Accessed: 22 August 2017).
The Effects of Ischaemic Compression versus Therapeutic Massage with a Percussive Device in Treating Hamstring
Myofascial Pain Dysfunction
A research dissertation presented to the Faculty of Health Sciences, University of
Johannesburg, as a partial fulfilment for the Master’s Degree in Technology,
Chiropractic by
Charlizé Jonker
Student Number: 201300673
Supervisor: ______________________ Date: __________________
Dr C. Yelverton

ii
DECLARATION
I, Charlizé Jonker, do hereby declare that this dissertation is my own unaided work,
except where otherwise indicated in text. This dissertation is being submitted in
partial fulfilment for the degree of Master of Technology, in the programme of
Chiropractic, at the University of Johannesburg. It has not been submitted before for
any degree or examination in any other tertiary institute.
_________________
Charlizé Jonker
On this _______ day of _______________ 2019
iv
DEDICATION
I wish to dedicate this dissertation to everyone that believed in me, supported me
and loved me during the course of this degree.
To my parents: thank you for giving me the opportunity to follow my dream and for
your endless love and support. If not for you, I would have been a lesser version of
myself. Thank you for always striving to give me the best, even when you weren’t
able to. You have been the motivation I have needed to succeed. I am truly blessed
to have you as my parents. Brian Tracy once said: “If you raise your children to feel
that they can accomplish any goal or task they decide upon, you will have succeeded
as a parent and you will have given your children the greatest of all blessing.”
To my grandfather, who has been my biggest fan since the day I was born: thank
you for always being in my corner, whether it was on the side of the sports field or
supporting me during this degree. I am truly blessed and grateful to have you in my
life and to share this great achievement with you.
To my brother: thank you for always listening to my never-ending stories about my
studies and for being there in difficult times. Best of luck with your journey ahead.
To my friend Colette: thank you for the amazing journey together. I am truly blessed
to have met a lifelong friend during this course, who shares the same hopes and
dreams. It has been a long journey with lots of memories that I will treasure for life.
Thank you for the early mornings, the numerous cups of coffee and the endless
chats when we were supposed to be studying. I will forever be grateful.
v
ACKNOWLEDGEMENTS
I would like to thank my supervisor, Dr Chris Yelverton, for your advice and
knowledge in helping me complete this study. I will always be grateful for all your
hard work, guidance and patience.
I would also like to thank Dr Glen Paton for being my mentor over the last two years
and reigniting my passion for the profession. Thank you for all the exciting
conversations and for sharing your knowledge and expertise.
vi
ABSTRACT
Purpose:
Soft tissue mechanotherapy can have an effect and be of benefit to muscle tissue,
because of the mechanosensitivity of the muscle, by shortening the recovering time
after exercise, improving muscle strength after the application of device-assisted soft
tissue manipulation, offsetting the effects of aging and facilitating the healing
process. The effect of device-assisted soft tissue manipulation on myofascial trigger
points and its effects on clinical outcomes needs to be further investigated, which
this study aims to do.
Design:
Thirty participants between the ages of 18 and 50 years old presenting with active
hamstring myofascial trigger points were included in this study. The participants were
randomly divided into two groups of 15 participants each (group A and group B).
Group A received ischemic compression and group B received therapeutic massage
with a percussive device on the active trigger point in the hamstring muscle. Each
participant was treated six times over a period of three weeks.
Measurements:
All measurements were collected at the first and fourth consultations prior to
treatment and on the seven consultation, where no treatment was performed. The
subjective measurements included the Numerical Pain Rating Scale. Objective
measurements included pressure algometric readings of pressure pain threshold of
the hamstring muscle trigger points, and hamstring extensibility was recorded using
a baseline goniometer.

vii
Results and Conclusion:
The outcome of this study suggests that patients with hamstring trigger point pain
can be treated effectively with each approach, as active trigger points respond well
to both ischemic compression and therapeutic massage with a percussive device.
Both groups showed a reduction in self-reported pain, an increase in pain pressure
threshold and an increase in hamstring extensibility over active hamstring trigger
points.
viii
DECLARATION ii
AFFIDAVIT iii
DEDICATION iv
ACKNOWLEDGMENTS v
ABSTRACT vi
CHAPTER ONE: INTRODUCTION
1.1 Problem Statement 1
1.2 Aim of the Study 2
1.3 Possible Outcomes of the Study 3
CHAPTER TWO: LITERATURE REVIEW
2.1 Introduction 4
2.2 Skeletal Muscle 4
2.2.1 Structure 4
2.2.2 Functional unit 5
2.2.3 Physiology of muscle contraction 6
2.3 Mechanoreceptors Specialised to Receive Tactile Information 8
2.3.1 Meissner’s corpuscles 8
2.3.2 Pacinian corpuscles 8
2.3.3 Markel’s disks and Ruffini’s corpuscles 9
2.4 The Hamstring Muscle Group 10
2.4.1 The anatomy of the hamstring muscle group 10
2.4.2 Innervation of the hamstring muscle group 10
2.4.3 Function of the hamstring muscle group 11
2.5 Myofascial Trigger Points 12
2.5.1 Introduction 12
ix
2.5.2 Myofascial trigger point criteria 12
2.5.3 Myofascial trigger point classifications 13
2.5.4 Pathophysiology of a myofascial trigger point 13
2.5.5 Hamstring trigger point location 15
2.5.6 Predisposing factors of hamstring trigger point development 16
2.5.7 Management of myofascial trigger points 17
CHAPTER THREE: METHODOLOGY
3.1 Introduction 21
3.2 Study Design 21
3.2.1 Participant recruitment 21
3.2.2 Sample selection and size 21
3.2.3 Inclusion criteria 22
3.2.4 Exclusion criteria 22
3.2.5 Random group allocation 23
3.3 Treatment Approach 23
3.3.1 First visit 23
3.3.2 Follow-up visits 24
3.4 Hamstring Trigger Point Examination 25
3.5 Intervention 26
3.5.1 Ischaemic compression 27
3.5.2 Percussive massage device 27
3.6 Subjective Measurements 28
3.6.1 Numerical Pain Rating Scale 28
3.7 Objective Measurements 28
3.7.1 Pressure algometer 28
3.7.2 Baseline goniometer 30
3.8 Data Analysis 31
3.9 Ethical Considerations 32
x
CHAPTER FOUR: RESULTS
4.1 Introduction 34
4.1.1 Normality testing 35
4.1.2 Descriptive and clinical analysis 35
4.1.3 Intragroup analysis 35
4.1.4 Intergroup analysis 35
4.2 Demographic Data Analysis 36
4.3 Subjective Data Analysis 36
4.3.1 Intragroup analysis of the Numerical Pain Rating Scale 36
4.3.2 Intergroup analysis of the Numerical Pain Rating Scale 40
4.4 Objective Data Analysis 41
4.4.1 Intragroup analysis of pressure algometer 41
4.4.2 Intergroup analysis of the pressure algometer 45
4.4.3 Intragroup analysis of the baseline goniometer 46
4.4.4 Intergroup analysis of the baseline goniometer 50
CHAPTER FIVE: DISCUSSION
5.1 Introduction 52
5.2 Demographic Data 52
5.2.1 Age and gender distribution 52
5.3 Subjective Data 52
5.3.1 Intragroup analysis of the Numerical Pain Rating Scale 52
5.3.2 Intergroup analysis of the Numerical Pain Rating Scale 54
5.3.3 Subjective data discussion 54
5.4 Objective Data 56
5.4.1 Intragroup analysis of the pressure algometer 56
5.4.2 Intergroup analysis of the pressure algometer 57
5.4.3 Discussion of pressure algometer results 57
xi
5.4.4 Intragroup analysis of the baseline goniometer 58
5.4.5 Intergroup analysis of the baseline goniometer 59
5.4.6 Discussion of the baseline goniometer results 60
CHAPTER SIX: CONCLUSION AND RECOMMENDATIONS
6.1 Conclusion 62
6.2 Recommendations 63
REFERNCES 64
xii
APPENDIX A: ADVERTISEMENT 75
APPENDIX B: INFORMATION FORM 76
APPENDIX C: CONSENT FORM 80
APPENDIX D: CASE HISTORY 81
APPENDIX E: PHYSICAL EXAMINATION 85
APPENDIX F: LUMBAR SPINE REGIONAL 90
APENDIX G: NUMRICAL PAIN RATING SCALE 93
APPENDIX H: HAMSTRING TRIGGER POINT EXAMINATION 94
APPENDIX I: ALGOMETER AND GONIOMETER READINGS 95
APPENDIX J: LETTER OF REQUEST 96
APPENDIX K: ETHICS CLERANCE LETTER 97
APPENDIX L: HIGHER DEGREES LETTER 98
APPENDIX M: SIMILARITY LETTER 99
APPENDIX N: EDITOR’S LETTER 100

xiii
LIST OF FIGURES
Figure 2.1 Organisation of Skeletal Muscle 5
Figure 2.2 Functional Unit of a Muscle 6
Figure 2.3 Hamstring Muscle Anatomy and Innervation 11
Figure 2.4 Hamstring Muscle Trigger Point Location 16
Figure 3.1 Patient Position for Semimembranosus and Semitendinosus 26
Figure 3.2 Thumper Maxi Pro 27
Figure 3.3 Pressure Algometer 29
Figure 3.4 Baseline Goniometer 31
Figure 4.1 Bar Graph Representing the NPRS Values of Each Visit for
Both Groups 40
Figure 4.2 Changes in the Mean Pain Threshold of the Pressure Algometer
for Group A and Group B 45
Figure 4.3 Changes in the Mean Readings of Baseline Goniometer 50
xiv
LIST OF TABLES
Table 4.1 Demographic Data within the Sample of 30 Participants 36
Table 4.2 Friedman Test Changes in NPRS Values of Group A 37
Table 4.3 Wilcoxon Signed-Rank Test for Group A 38
Table 4.4 Friedman Test Changes in NPRS Values of Group B 38
Table 4.5 Wilcoxon Signed-Rank Test for Group B 39
Table 4.6 Group A Column Statistics of the Pressure Algometer 41
Table 4.7 Group A Friedman Test for Changes in Pressure Algometer Mean
Values 42
Table 4.8 Group A Wilcoxon Signed-Rank Test for Changes over Time
(Pressure Algometer) 42
Table 4.9 Group B Column Statistics of the Pressure Algometer 43
Table 4.10 Group B Friedman Test for Changes in Pressure Algometer
Mean Values 43
Table 4.11 Group B Wilcoxon Signed-Rank Test for Changes over Time
(Pressure Algometer) 44
Table 4.12 Mann-Whitney U Test for Pressure Algometer Mean Values 45
Table 4.13 Group A Column Statistics of the Baseline Goniometer 46
Table 4.14 Group A Friedman Test for Changes in Baseline
Goniometer Mean Values 47
Table 4.15 Group A Wilcoxon Signed-Rank Test for Changes over Time
(Baseline Goniometer) 47
Table 4.16 Group B Column Statistics of the Baseline Goniometer 48
Table 4.17 Group B Friedman Test for Changes in Baseline
Goniometer Mean Values 48
Table 4.18 Group B Wilcoxon Signed-Rank Test for Changes over Time
(Baseline Goniometer) 49
Table 4.19 Mann-Whitney U Test for Comparison of Baseline
Goniometer Mean Values 51
1
CHAPTER ONE: INTRODUCTION
1.1 PROBLEM STATEMENT
Device-assisted soft tissue manipulation is regarded as a type of
mechanotherapy, which has a significant effect in the prevention of disease,
promotion of health and physical rehabilitation (Field, 2016). Device-assisted soft
tissue manipulation, e.g. therapeutic massage, is regarded as a manual therapy
used commonly by clinicians worldwide to treat musculoskeletal pain disorders
(Karels, Polling and Bierma-Zeinstra, 2006). Mechanotherapy applies a non-
invasive mechanical stimulus to the body surface, influencing molecules, cells
and tissue structures by means of mechanotransduction, which ultimately leads
to improved clinical outcomes and muscle function (Khan and Scott, 2009; Huang,
Holfeld, Schaden, Orgill and Ogawa, 2013).
Soft tissue mechanotherapy can have an effect and be of benefit to muscle tissue
because of the mechanosensitivity of the tissue, shortening the recovery time
after exercise, improving muscle strength after the application of device-assisted
soft tissue manipulation, offsetting the effects of aging and facilitating the healing
process (Brooks et al., 2005). Nevertheless, the effects of device-assisted soft
tissue manipulation on myofascial trigger points and its effects on clinical
outcomes need to be further investigated (Loghmani and Whitted, 2016).
Indeed, the human body consists of 50% skeletal muscle, one of the largest
organs in the human body, and any of these muscles can develop a dysfunction
or pain known as myofascial pain syndrome (Ching, 2007). According to Harden,
Bruehl, Gass, Niemiec and Barbick (2002), myofascial pain is one of the leading
diagnoses of pain sufferers by pain management physicians and general
practitioners.
Myofascial pain is defined as pain that derives from myofascial trigger points in
the skeletal muscle, which are small, very sensitive areas in the skeletal muscle.
2
These areas are hypersensitive, palpable, taut bands of muscle that produce pain
on touch. The patient’s symptoms and can cause localised or referred pain
(Travell and Simons, 1999; Bron and Dommerholt, 2012). Myofascial pain has a
high occurrence among individuals with regional pain complaints. It has been
found that the prevalence varied from 21% to 30% of general medical clinic
patients to as high as 85% to 93% of patients presenting to pain management
centers (Kaergaard and Andersen, 2002).
A latent myofascial trigger point is defined as a trigger point that is tender locally
on touch and may be associated with limited range of motion and muscle stiffness
but is not associated with spontaneous complaints of pain. An active myofascial
trigger point is thus associated with a clinical pain complaint. Muscles with
myofascial trigger points each have their own characteristic pain pattern, helping
the physician to identify which muscle may contain the responsible myofascial
trigger point (Borg-Stein and Simons, 2002).
There are a wide variety of therapies available for the treatment of myofascial
trigger points but there is little consensus as to the best treatment protocol
(Vernon and Schneider, 2008). Myofascial trigger points are routinely identified
and treated by clinicians in various health care disciplines by a non-invasive
method called ischemic compression. De Las Peñas, Alonso-Banco, Fernandez-
Carnero and Miangolarra-Page (2006) have proven ischemic compression to be
a safe and effective non-invasive procedure, known to successfully reduce the
tenderness caused by myofascial trigger points.
1.2 AIM OF THE STUDY
The aim of this study was to compare the efficacy of ischemic compression with
that of therapeutic massage with a percussive device in the treatment of active
hamstring myofascial trigger points in order to determine which of the two
treatment protocols is superior.
3
1.3 POSSIBLE OUTCOMES OF THIS STUDY
The possible outcome of the study would determine which of the two treatment
protocols, i.e. ischemic compression or device-assisted soft tissue massage, is
superior in the treatment of hamstring myofascial pain syndrome. The outcome
of the study could also provide additional understanding and knowledge of
myofascial pain dysfunction and the efficacy of treatment methods used by
chiropractors, physiotherapists and other health care practitioners.
4
CHAPTER TWO: LITERATURE REVIEW
2.1 INTRODUCTION
This chapter serves to give detail on relevant previously published literature and
research to provide background literature for this specific study. Emphasis is placed
on the relevant anatomic structures, such as skeletal muscle structure, specifically
of the hamstring muscles, the development of myofascial trigger points, and
ischemic compression and percussive massage devices used as treatment to this
condition.
2.2 SKELETAL MUSCLE
2.2.1 Structure
Skeletal muscle consists predominantly of muscle cells that are specialised for
contraction in order to produce skeletal movement, maintain body posture and
maintain body temperature (Martini, Nath and Bartholomew, 2018). As
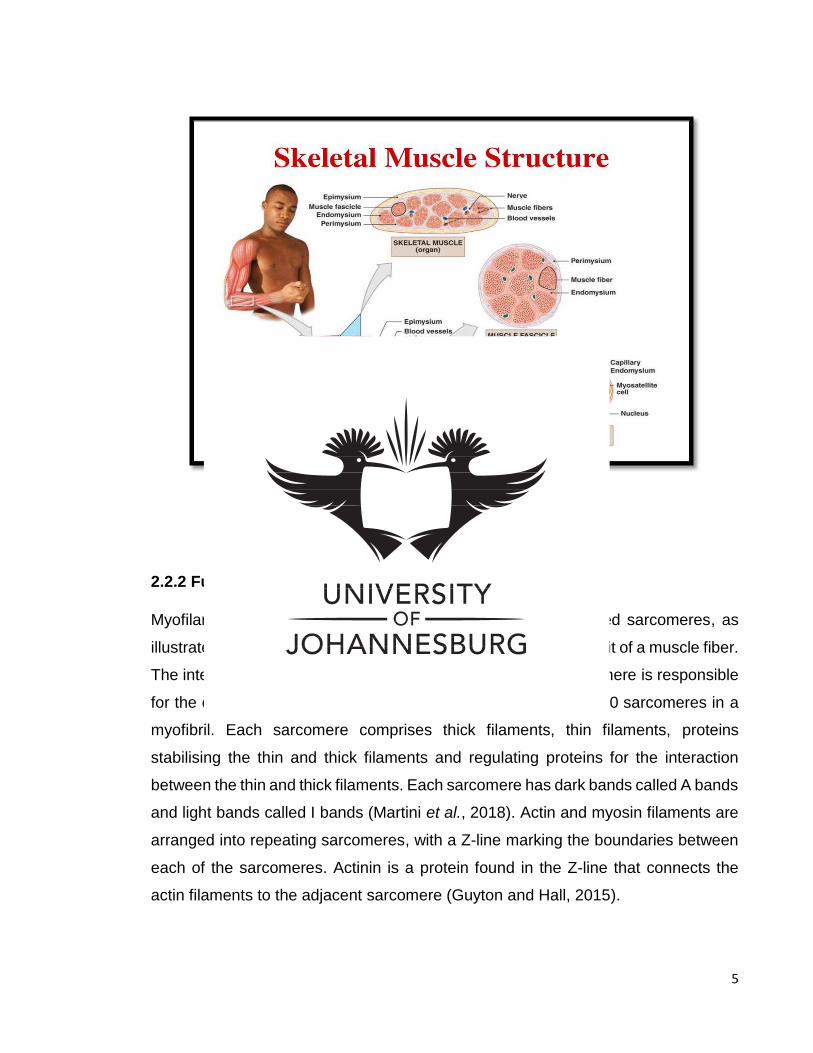
demonstrated in figure 2.1, each muscle has three connective tissue layers: the
epimysium, perimysium and an endomysium. The epimysium covers the entire
muscle and consists of a dense layer of collagen fibers. The epimysium separates
the muscle from the surrounding structures. The perimysium divides the skeletal
muscle into different compartments. These compartments contain muscle fiber
bundles called fascicles. There are blood vessels and nerves within the perimysium
to supply the muscle fibers within the muscle fascicles (Martini et al., 2018).
A delicate connective tissue endomysium found within the fascicle surrounds each
individual skeletal muscle cell, called a muscle fiber. Every muscle fiber contains a
number of myofilaments that are composed of actin and myosin filaments, which
have the ability to shorten and allow for a contraction (Martini et al., 2018).
5
Figure 2.1 Organisation of Skeletal Muscle
(Martini et al., 2018)
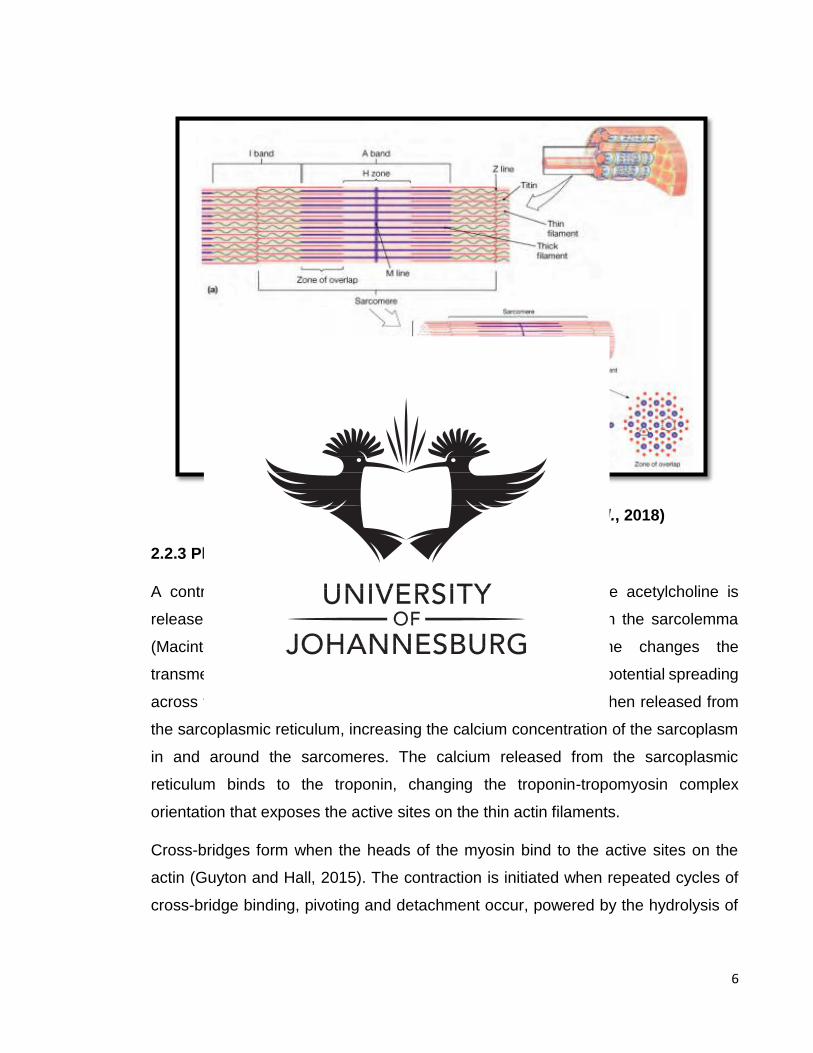
2.2.2 Functional unit
Myofilaments are organised into repeating functional units called sarcomeres, as
illustrated in figure 2.2. Sarcomeres are the smallest functional unit of a muscle fiber.
The interaction between the thin and thick filaments of the sarcomere is responsible
for the contraction of the muscle. There are approximately 10 000 sarcomeres in a
myofibril. Each sarcomere comprises thick filaments, thin filaments, proteins
stabilising the thin and thick filaments and regulating proteins for the interaction
between the thin and thick filaments. Each sarcomere has dark bands called A bands
and light bands called I bands (Martini et al., 2018). Actin and myosin filaments are
arranged into repeating sarcomeres, with a Z-line marking the boundaries between
each of the sarcomeres. Actinin is a protein found in the Z-line that connects the
actin filaments to the adjacent sarcomere (Guyton and Hall, 2015).
6
Figure 2.2 Functional Unit of a Muscle (Martini et al., 2018)
2.2.3 Physiology of a Muscle Contraction
A contraction is initiated at the neuromuscular junction, where acetylcholine is
released from the synaptic terminal binding to the receptors on the sarcolemma
(Macintosh, Gardiner and McComas, 2006). Acetylcholine changes the
transmembrane potential of the muscle fiber, leading to an action potential spreading
across the entire surface of the muscle fiber. Stored calcium is then released from
the sarcoplasmic reticulum, increasing the calcium concentration of the sarcoplasm
in and around the sarcomeres. The calcium released from the sarcoplasmic
reticulum binds to the troponin, changing the troponin-tropomyosin complex
orientation that exposes the active sites on the thin actin filaments.
Cross-bridges form when the heads of the myosin bind to the active sites on the
actin (Guyton and Hall, 2015). The contraction is initiated when repeated cycles of
cross-bridge binding, pivoting and detachment occur, powered by the hydrolysis of
7
adenosine triphosphate (ATP). This event allow for the filaments to slide and for
shortening of the muscle fibers (Martini et al., 2018).
The muscle contraction cycle is reliant on energy in the form of ATP, which transfers
energy from one location to another. In muscle, this energy is used to shorten the
sarcomeres, sliding the myofilaments and restoring the calcium to the sarcoplasmic
reticulum after the muscle contraction is completed. Most of the cells in the body
generate ATP through aerobic metabolism in the mitochondria and glycolysis in the
cytoplasm (which is anaerobic) (Martini et al., 2018).
ATP demands are low in a resting skeletal muscle. Enough oxygen is available for
the mitochondria to meet the demand, and they produce extra ATP. During moderate
activity levels, the ATP demand of muscle cells increases. The demand is met by
the mitochondria as the rate of ATP production and oxygen consumption rises. The
muscle fibers require all the ATP and no extra ATP is produced. The skeletal muscle
depends primarily on aerobic metabolism to generate ATP (Martini et al., 2018).
The ATP and oxygen demands are enormous during strenuous exercise, where the
ATP production by the mitochondria is at its maximum. However, the rate of the
oxygen diffusion into the muscle fiber cannot reach the ATP demand; the
mitochondria can only produce about one third of the needed ATP. The remainder
is generated by glycolysis. This process occurs when glucose is broken down to
glycogen into pyruvate. The surplus pyruvate accumulates in the sarcoplasm and is
converted into lactic acid, changing the intercellular pH (Martini et al., 2018).
Skeletal muscle optimal function depends on four factors: substantial intracellular
energy reserves, good blood circulation, normal blood-oxygen and normal pH in the
muscle fibers (Martini et al., 2018). Disruption to these factors will impair skeletal
muscle bioenergetics, leading to muscle dysfunction (Preedy and Peters, 2002).
8
2.3 MECHANORECEPTORS SPECIALISED TO RECEIVE TACTILE INFORMATION
Mechanotherapy applies a non-invasive mechanical stimulus to the body surface,
influencing molecules, cells and tissue structures by means of
mechanotransduction, which ultimately leads to improved clinical outcomes and
muscle function (Khan and Scott, 2009; Huang et al., 2013). There are four major
types of mechanoreceptors: Meissner’s corpuscles, Pacinian corpuscles, Markel’s
disk and Ruffini’s corpuscles. These mechanoreceptors are specialised to provide
information to the central nervous system about touch, pressure, vibration and
cutaneous tension. They are referred to as low-threshold or high-sensitivity
mechanoreceptors. They can produce an action potential with a weak mechanical
stimulation to the skin. Large myelinated type Aβ axons innervate the low-threshold
mechanoreceptors, ensuring rapid central transmission of tactile information (Ebara,
Furuta and Kumamoto, 2017)
2.3.1 Meissner’s corpuscles
Meissner’s corpuscles are found between the dermal papillae just below the
epidermis of the fingers, palms and soles. The elongated receptors are formed by a
connective tissue capsule that comprises several lamellae of Schwann cells. The
capsule centre contains one or more afferent nerve fibers, which generate rapid
action potentials with minimal skin depression. Meissner’s corpuscles allow for
transduction of low-frequency vibration (30-50 HZ) (Ebara et al., 2017).
2.3.2 Pacinian corpuscles
Pacinian corpuscles are large encapsulated endings located in the subcutaneous
tissue. These mechanoreceptors differ from the Meissner’s corpuscles in their
morphology, distribution and response to threshold. The Pacinian corpuscle has an
9
onion-like capsule in which the inner core of the membrane lamellae is separated
from the outer lamella by a fluid-filled space. There are one or more rapidly adapting
afferent axons located in the centre of the structure. The capsule acts as a filter,
allowing only transient disturbances at high frequencies (250-350Hz) to activate the
nerve endings. The Pacinian corpuscles adapt more rapidly than Meissner’s
corpuscles and have a lower response threshold. This feature suggests that
Pacinian corpuscles are involved in the discrimination of fine surface textures or
other moving stimuli that produce high-frequency vibration of the skin. Pacinian
corpuscles provide information primarily about dynamic qualities of mechanical
stimuli (Ebara et al., 2017)
2.3.3 Merkel’s disks and Ruffini’s corpuscles
Merkel’s disks and Ruffini’s corpuscles are slow-adapting mechanoreceptors.
Merkel’s disks are located in the epidermis, where they are aligned with papillae that
lie beneath the dermal ridges. The slow-adapting nerve fiber associated with each
Merkel’s disk enlarges into a saucer-shaped ending that is closely applied to another
specialised cell containing vesicles that apparently release peptides that modulate
the nerve terminal. Merkel’s disks play a major role in the static discrimination of
shapes, edges and rough textures (Ebara et al., 2017).
Ruffini’s corpuscles are structurally similar to other mechanoreceptors, but are not
well understood. They have elongated, spindle-shaped capsules and are located
deep in the skin, as well as in ligaments and tendons. Ruffini’s corpuscles are
sensitive to cutaneous stretching produced by digital or limb movement. They
primarily respond to internally generated stimuli (Ebara et al., 2017).
10
2.4 THE HAMSTRING MUSCLE GROUP
2.4.1 The anatomy of the hamstring muscle group
The hamstring muscle group consists of the biceps femoris, semitendinosus and
semimembranosus. Some literature considers the adductor magnus muscle to be a
hamstring muscle as a result of its vertical line of pull (Koulouris and Connell, 2005).
The biceps femoris makes up the lateral component of the thigh and has two heads,
namely a long head originating from the medial facet of the ischial tuberosity and a
short head originating from the lateral linea aspera, lateral supracondylar line and
intermuscular septum. The short head of biceps femoris only crosses a single joint,
the knee. The distal tendon of biceps femoris muscle inserts onto the head of the
fibula (Moore, Dalley and Agur, 2017).
The medial component of the posterior thigh is made up of the semitendinosus
muscle (proximal part) and the semimembranosus muscle (distal part) (Koulouris
and Connell, 2005). The semitendinosus muscle overlies the semimembranosus
muscle. The semitendinosus and semimembranosus originate from the ischial
tuberosity. The semitendinosus inserts on the medial surface of the superior part of
the tibia as part of the pes anserinus. The semimembranosus inserts on the posterior
part of the medial tibial condyle (Moore et al., 2017).
2.4.2 Innervation of the hamstring muscle group
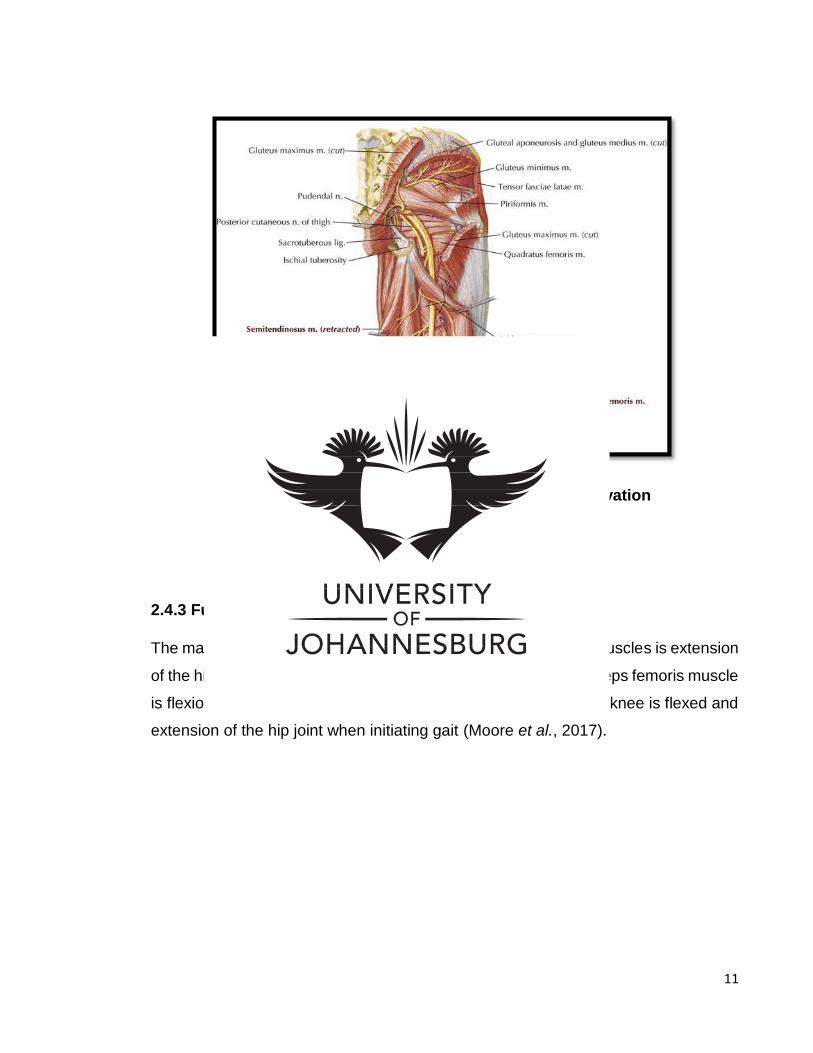
Figure 2.3 demonstrates the innervation of the hamstring muscle group. The long
head of biceps femoris muscle and the semitendinosus and semimembranosus
muscles are innervated by the tibial division of the sciatic nerve, which is derived
from nerve roots L5, S1 and S2. The short head of biceps femoris muscle is
innervated by the common fibular nerve of the sciatic nerve, derived from the L5, S1
and S2 nerve roots (Moore et al., 2017).
11
Figure 2.3 Hamstring Muscle Anatomy and Innervation
(Netter, 2018)
2.4.3 Function of the hamstring muscle group
The main action of the semitendinosus and semimembranosus muscles is extension
of the hip joint and flexion of the knee joint. The main action of biceps femoris muscle
is flexion of the knee joint and lateral rotation of the leg when the knee is flexed and
extension of the hip joint when initiating gait (Moore et al., 2017).
12
2.5 MYOFASCIAL TRIGGER POINTS
2.5.1 Introduction
The most commonly used description of trigger point is that by Travell and Simons
(1999). Travell and Simons (1999) define a trigger point as the presence of
tenderness at a nodule in a palpable taut band of muscle.
Trigger points can develop in skeletal muscle or its fascia, tendons, joint capsule,
ligaments and in the skin (Simmonds, Miller and Gemmell, 2010). Myofascial trigger
points cause pain on digital pressure and may give rise to distinguishing patterns of
referred pain, tenderness, restricted range of motion and autonomic nervous system
symptoms (Rickards, 2006). The muscle exhibits a muscle fasciculation, or the
whole body moves as a response to the digital compression. Trigger points may
cause muscle dysfunction, which may result in weakness, muscle imbalance and
impaired motor activation pattern (Lucas, Polus and Rich, 2003).
2.5.2 Myofascial trigger point criteria
The criteria for the presence of an active myofascial trigger point involve the
combined presence of the following (De Las Peñas, Campo, Carnero and
Miangolarra-Page, 2005):
A taut palpable band in skeletal muscle
A hypersensitive spot in the taut band
Patient recognition of the pain as ‘familiar’
Pain when stretching the tissue
Limited range of motion
Local twitch response
Referred pain
Muscle weakness without muscle atrophy
13
According to Tough, White, Richards and Campbell (2007), the four most commonly
applied diagnostic criteria of a myofascial trigger point are:
o Tender spot in a taught band of the skeletal muscle
o Patient pain recognition
o Predicted pain referral pattern
o Local twitch response
2.5.3 Myofascial trigger point classifications
A myofascial trigger point is classified as either latent or active. Active trigger points
usually cause symptoms that occur spontaneously at rest. Latent trigger points only
elicit pain when manually or actively stimulated, and are therefore considered
asymptomatic (Shah and Gilliams, 2008).
Raj and Paradise (2004) define three other classifications of a trigger point, i.e.
primary, secondary and satellite. A trigger point that develops independently of any
other trigger point is classified as a primary trigger point. It usually develops due to
overuse, either acute or chronic. Secondary trigger points usually develop in a
muscle as a result of compensational overload on a muscle that contains a primary
trigger point. Secondary trigger points may also develop after a primary trigger point
is removed. Satellite trigger points can develop because of their location within the
area of the primary trigger point referral area of pain (Raj and Paradise, 2004).
2.5.4 Pathophysiology of a myofascial trigger point
If a muscle is exposed to trauma, overuse, mechanical overload, postural faults or
psychological stress, it may lead to the development of myofascial trigger points
(Huguenin, 2004). The pathophysiology of a myofascial trigger point is still
debatable, although there is evidence that indicates a disruption of the
neuromuscular endplate (Fryer and Hodgson, 2005).
14
There are various hypotheses regarding trigger point development. The most
important, according to Mense and Simons (2000) and Kostopoulos and Rizopoulos
(2001), are as follows:
Muscle spindle hypothesis: states that the abnormal muscle spindle produces
an abnormal electrophysiological signal in the proximity of the trigger point.
Neuropathic hypothesis: states that the nerve supplying the specific muscle
involved in a neuropathic process results in trigger point hypersensitivity.
Fibrotic scar tissue hypothesis: states that damaged muscle tissue that heals
in the form of scar tissue forms a trigger point in that specific area.
Poor posture due to overwork and muscle fatigue: results in tension and
stiffness leading to the development of trigger points.
The energy crisis hypothesis is also a widely accepted hypothesis according to
Mense and Simons (2000) and Kostopoulos and Rizopoulos (2001). According to
this hypothesis, the sarcoplasmic reticulum functions to store and release calcium to
stimulate the activity of the contractile elements, shortening the sarcomere. Trauma,
overuse, mechanical overload, postural faults or psychological stress initiate(s) the
excessive release of acetylcholine, producing the local energy crisis, which accounts
for myofascial trigger point characteristics (Simons, 2004). The sarcomere contracts
continuously, causing ischemia and hypoxia with an increased energy demand.
The combination of loss of energy supply and increased demand in energy creates
the energy crisis. The result of the energy crisis is the release of sensitising, noxious
substances responsible for the pain associated with myofascial trigger points
(Kostopoulos and Rizopoulos, 2001; Mense and Simons 2000; Simons, 2004).
Kostopoulos and Rizopoulos (2001) further state that these processes lead to an
excess amount of calcium in the production of a normal amount of ATP, resulting in
the initiation of myofibrils and a sustained contraction. The sustained contraction
15
leads to a decrease of blood flow to the area, which is associated with
vasoconstriction due to the autonomic nervous system. Changes in the muscle may
cause muscle dysfunction, which results in weakness, muscle imbalance, an
impaired motor activation pattern and pain (Lucas et al., 2003).
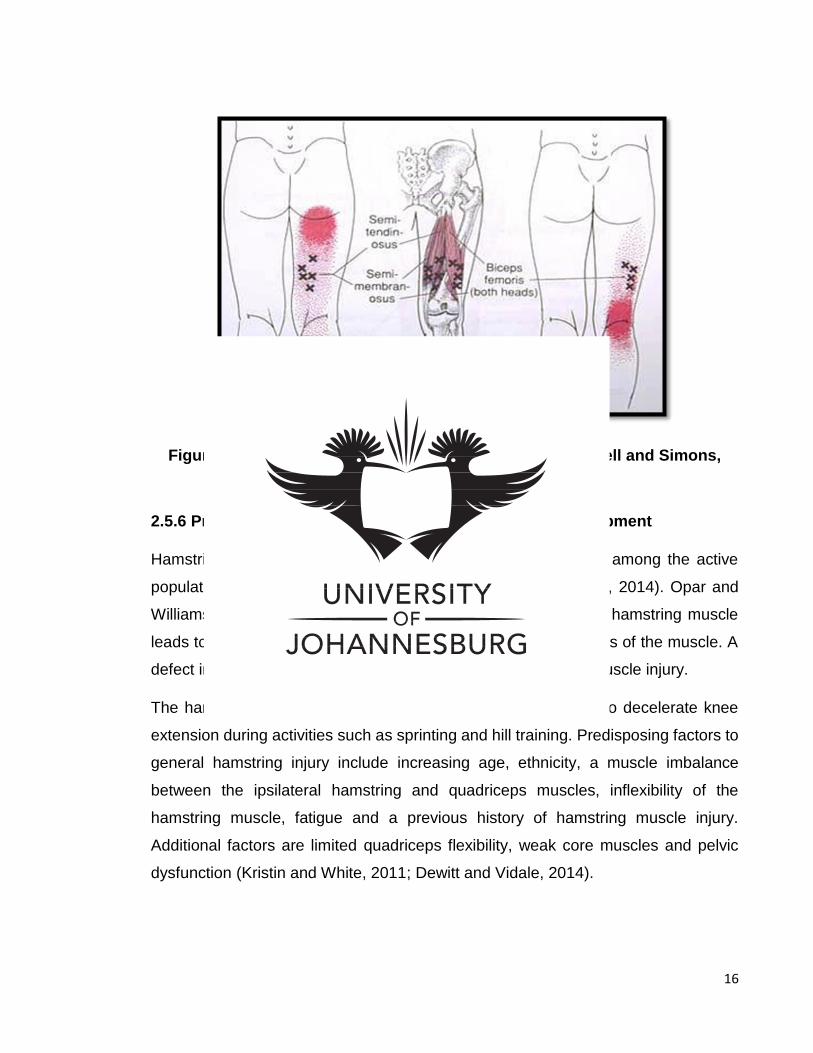
2.5.5 Hamstring trigger point location
The semimembranosus and semitendinosus muscle trigger points are located on the
distal medial aspect of the posterior thigh. Pincer palpation can be used to grasp the
distal hamstring mass to pull the mass away from the femur to palpate the taut bands
within the muscle. The myofascial trigger points are clustered around the distal
medial posterior thigh, as demonstrated in figure 2.4. The myofascial trigger points
of biceps femoris are located on the posterior-lateral aspect of the posterior thigh
and are usually clustered in this area (Travell and Simons, 1999).
The referral pattern for semimembranosus and semitendinosus is pain generally
upwards to the lower gluteal region and inferiorly over the upper medial calf. The
biceps femoris pain referral pattern is upwards to the lower gluteal region and
inferiorly over the lower upper lateral popliteal fossa and calf. The hamstring muscle
group referral patterns are demonstrated in figure 2.4 (Hunter and Speed, 2007).
16
Figure 2.4 Hamstring Muscle Trigger Point Location (Travell and Simons, 1999)
2.5.6 Predisposing factors of hamstring trigger point development
Hamstring strain injuries are one of the most common injuries among the active
population, and have high rates of re-injury (DeWitt and Vidale, 2014). Opar and
Williams (2012) showed that lengthening and shortening of the hamstring muscle
leads to trigger point formation, which can contribute to weakness of the muscle. A
defect in hamstring muscle strength then leads to a hamstring muscle injury.
The hamstrings are predisposed to injury as they are working to decelerate knee
extension during activities such as sprinting and hill training. Predisposing factors to
general hamstring injury include increasing age, ethnicity, a muscle imbalance
between the ipsilateral hamstring and quadriceps muscles, inflexibility of the
hamstring muscle, fatigue and a previous history of hamstring muscle injury.
Additional factors are limited quadriceps flexibility, weak core muscles and pelvic
dysfunction (Kristin and White, 2011; Dewitt and Vidale, 2014).

17
2.5.7 Management of myofascial trigger points
Therapy for the treatment of myofascial trigger points can be classified as either
invasive or non-invasive treatment, both of which are focused on the relief of pain
(Huguenin, 2004). Invasive techniques include dry needling, corticosteroid use, local
anesthesia and botulism toxin A injections. Non-invasive techniques includes
vapocoolant spray, muscle stretch techniques, chiropractic manipulation therapy,
transcutaneous electrical stimulation (TENS), ultrasound, laser therapy, instrument-
assistant techniques and pressure-release therapies (Lavelle, Lavelle and Smith,
2007). The main goal of the treatment protocols is inactivation of myofascial trigger
points, restoring normal muscle length and eliminating and/or correcting the factors
that created the myofascial trigger points (Saxena, Chansoria, Tomar and Kumar
2015).
Ischemic compression
Ischemic compression is a non-invasive treatment. It is a sustained, firm, strong
digital pressure applied to the myofascial trigger point with the purpose of reducing
the tenderness of the trigger point (Travell and Simons, 1999).
Ischemic compression can be applied as a direct pressure to the trigger point or by
a pincer grip. This sustained digital pressure is delivered for a period of second to a
minute with the goal of reducing the tension in the taut band of the muscle (Arnau-
Masanet, Barrios-Pitarque, Bosch-Morell, Montanez-Aguilera, Pecos-Martin and
Valtuena-Gimeno, 2010). The sustain pressure applied to the muscle temporarily
occludes blood flow to the area, so release results in a reactive hyperemia. The rapid
increase in blood flow functions to flush out the inflammatory exudate metabolites
from the trigger point formed in the muscle (Fritz and Grosenbach, 2009).
A continuous pressure to the trigger point is applied until the tension in the muscle
is relieved, which implies inactivation of the myofascial trigger point (Raj and
Paradise, 2004). It is important to follow ischemic compression with stretching of the
18
muscle to re-establish an optimal length-tension relationship (Fritz and Grosenbach,
2009). Ischemic compression induces some trauma to the involved muscle tissue,
which might cause minor bruising. Bruising is reduced during treatment, however,
as pressure is applied for short periods at a time (Hains, 2002).
Ischemic compression was one of the earliest modalities recommended for the
treatment of pain related to myofascial trigger points, pioneered by Nimmon and
Travell in the early 1960s (Travell and Simons, 1999). Moderately strong evidence
supports ischemic compression as one of the most common techniques used among
chiropractors for pain relief related to myofascial trigger points (Vernon and
Schneider, 2008). Authors have also found ischemic compression to be effective for
pain relief and disabilities caused by myofascial trigger points in various types of
pathologies such as cervical spine (Cagnie, Dewitte, Coppieters, Van Oosterwijck,
Cools and Danneels, 2013) and shoulder pain (Hains, Descarreaux, and Hains,
2010).
De Las Peñas et al (2006) conducted a pilot study on the effects of ischemic
compression and that of cross friction on tenderness in subjects with active and
latent myofascial trigger points. They found a significant increase in pain threshold
of the participants that received ischemic compression as well as the participants
that received cross friction treatment, with no difference between the two treatment
protocols. Both these treatment protocols are considered to be effective in the
treatment of myofascial trigger points, with the authors encouraging further research
to study the effects of different manual therapies.
In another relevant study, Gemmell, Miller and Nordstrom (2008) examined 45
subjects with non-specific neck pain related to trapezius myofascial pain syndrome.
The aim of the study was to compare the effects of ischemic compression and sham
ultrasound on non-specific neck pain in these subjects. It was confirmed by the
results that ischemic compression is superior to sham ultrasound, and the subjects
that received ischemic compression were five times more likely to improve compared
to those who received sham ultrasound.
19
Finally, Menakam and Kalaichandran (2015) investigated the efficacy of ischemic
compression combined with stretching regimes. Ischemic compression followed by
passive stretching was found to be affective in the relief of pain and a significant
increase in the pain pressure threshold over the myofascial trigger points.
Percussive massage device
The application of electro-mechanical and device-assisted soft tissue mobilisation
has a unique action of steady, comfortable pulsed acupressure that delivers a
thorough and effective massage. The vibration frequency penetrates large parts of
the body without having to dig deep as one does with hand massage. The action of
these devices was originally designed to mimic the action of massage therapist’s
hands gliding over the tissue (Thumper Massager, 2019). These therapeutic devices
are used worldwide in sport medicine, physical therapy and rehabilitation owing to
the beneficial effects they have on neuromuscular systems (Karacan, Cidem,
Yilmaz, Sebik, Cakar and Türker, 2016).
Most of the devices used for soft tissue manipulation operate with an ordinary 120-
volt household current at a frequency of 50-60 Hz with a speed impact of 1200-2100
rate per minute (20-35 pulses) (Comeaux, 2011). Device-assisted soft tissue
manipulation requires little to no energy as the therapeutic friction is produced by the
motor and device applicator. The therapeutic effect is achieved in a much shorter
time than manual therapy because these devices achieve a much higher degree of
friction than that of the human hand, allowing the therapist to cover a greater surface
area (Comeaux, 2011).
Deep tissue work can be challenging for massage therapists, chiropractors,
physiotherapists and physical therapists, especially in high-volume clinical
environments where routinely they engage in using hands for repetitive soft tissue
manipulation techniques. In such cases, the use of the device-assisted soft tissue
manipulation tool can significantly reduce strain and load on the therapist’s body
20
(Green and Goggins, 2006). However, there is little research on the effect of these
devices on myofascial pain syndrome and the clinical outcomes (Best, Crawford,
Haas, Charles and Zhao, 2014).
So far, Comeaux (2011) has reviewed several of these devices, such as the
percussion vibrator, vibrational platform and deep tissue oscillation. He describes
the possible mechanisms of effect on the fascial and neuromuscular systems,
emphasising the physiological phenomenon of the tonic vibratory reflex.
Schillinger, Koenig, Haefele, Vogt and Heinrich (2006) then demonstrated that
participants that received soft tissue manipulation had a more rapid decrease in
muscle enzymes indicative of muscle damage after a strenuous exercise test
compared to a control group. The application of soft tissue manipulation was found
to reduce the recovery period after exercise and increase muscle strength
(Schillinger et al., 2006).
Furthermore, Bakhtiary, Fatemi, Khalili and Ghorbani (2011) investigated the
application of device-assisted soft tissue manipulation on hamstring extensibility and
reported a general increase in range of motion and flexibility of the hamstring muscle.
21
CHAPTER THREE: METHODOLOGY
3.1 INTRODUCTION
This chapter serves to explain how the study was conducted.
3.2 STUDY DESIGN
This study was a comparative, quasi-experimental study that made use of
convenience sampling and random group allocation.
3.2.1 Participant recruitment
Individuals of any gender between the ages of 18-50 years who suffered with
posterior thigh pain were considered. Participants were recruited by word of mouth
and by means of advertisements (Appendix A) placed in and around the University
of Johannesburg’s Doornfontein campus and the Chiropractic Day Clinic.
3.2.2 Sample selection and size
The study was explained to each of the participants, who were required to read the
information form (Appendix B) and sign the consent form (Appendix C) specific to
this study. Each participant underwent a screening process to determine whether
s/he was eligible for this study, taking into consideration the inclusion and exclusion
criteria. Participants had to present with active hamstring myofascial trigger points.
Participants were excluded and included from this study based on the following:
22
3.2.3 Inclusion criteria
To be included into the study, the participants needed to comply with the following
criteria:
Be either male or female
Be between the ages of 18-50 years old with active hamstring myofascial trigger
points of the hamstring muscle.
According to Tough et al., (2007) the four most commonly applied diagnostic criteria
of a myofascial trigger point are:
o Tender spot in a taught band of the skeletal muscle
o Patient pain recognition
o Predicted pain referral pattern
o Local twitch response
3.2.4 Exclusion criteria
Participants were excluded from the study if they:
Used non-steroidal anti-inflammatory drugs, analgesic drugs or muscle relaxants
for the duration of the study (Fleckenstein, Zaps, Rüger, Lehmeyer, Freiburg,
Lang and Irnich, 2010).
Showed any contra-indications to massage and ischemic compression, as listed
by Batavia (2004) and Perle, Schneider and Seaman (1999):
o Acute trauma: open wounds, muscle ruptures, tendon ruptures,
contusions, burns broken bone
o Periostitis and bursitis
o Rheumatoid arthritis and gout
o Myositis ossificans
o Infection: bacterial, viral and fungal
o Bleeding disorders, artificial blood vessels and thrombosis
23
o Tumors
o Application over neurovascular bundles
o Patients taking anti-coagulant medication or long-term steroids
3.2.5 Random group allocation
A sample group of 30 participants were divided into one of two groups that consisted
of 15 participants each. The allocation of the participants was determined by asking
the participants to draw a piece of paper on which was written either a letter “A” or
“B” out of a hat. The hat contained 15 pieces of paper labeled “A” and 15 pieces of
paper labeled “B”, which represented group A and group B respectively. As such,
the letter drawn by each participant from the hat represented the group to which s/he
was allocated.
Participants in group A received ischemic compression directly applied to the active
hamstring myofascial trigger point. Participants in group B received a percussive
massage with a device over the entirety of the hamstring muscle containing active
myofascial trigger points.
3.3 TREATMENT APPROACH
3.1.3 First visit
The initial visit for both groups involved the following:
The researcher conducted a case history (Appendix D), a full physical
examination (Appendix E), and a lumbar spine examination (Appendix F).
Thereafter, a Subjective Objective Assessment Plan (SOAP) form was
completed.
Each participant completed subjective measurements in the form of a Numerical
Pain Rating Scale (NPRS) (Appendix G) under the supervision of the researcher.
24
A hamstring trigger point examination (Appendix H) that consisted of digital
palpation was done by the researcher in order to locate an active hamstring
trigger point in either the left or right muscle.
Objective measurements were taken using a hand-held pressure algometer. The
tip of the pressure algometer was applied to determine the amount of pressure
that caused the participants’ first point of pain, known as pain threshold. The
readings were recorded for all participants on the first, fourth and seventh visits
(Appendix I). The hamstring flexibility of each participant was measured with a
baseline goniometer on the first, fourth and seventh visits.
Thereafter, participants received treatment:
o Group A: Ischemic compression was applied to the most active hamstring
myofascial trigger point found during examination for 60 seconds.
o Group B: therapeutic massage was applied by the researcher with a
percussive device over the entirety of the hamstring muscle containing the
most active myofascial trigger point for 60 seconds.
3.3.2 Follow-up visits
Subjective indications of pain (using the NPRS) were provided by each participant
at the first, fourth and seventh visits prior to treatment, under the supervision of the
researcher. A baseline goniometer was used to measure the popliteal angle, which
determined the hamstring flexibility at the first, fourth and seventh visits. Pressure
algometry of the same trigger point found during the first visit was again undertaken
at the fourth and seventh visits to determine the changes in pain threshold and the
pain tolerance of all participants.
At each visit, participants were reassessed and a SOAP note was completed to
update the current display of pain and symptoms of each participant.
Participants were treated over a three-week period, where they attended seven
visits. At the first six, they received treatment and measurements were taken, while
25
at the seventh visit, only measurements were taken. Group A and group B received
two treatments over a three-week period to ensure tissue recovery (Travell and
Simons, 1999; Puri, Flatow and Soslowsky, 2015)
Participants in group A received ischemic compression applied to the most
active hamstring myofascial trigger point found during examination for 60
seconds.
Participants in group B received therapeutic massage applied by the
researcher with a percussive device over the entirety of the hamstring muscle
containing the most active trigger point for 60 seconds.
3.4 HAMSTRING TRIGGER POINT EXAMINATION
Each participant had to undergo a hamstring trigger point examination (Appendix H)
on the initial visit. There were a number of trigger points located in the hamstring
muscle group.
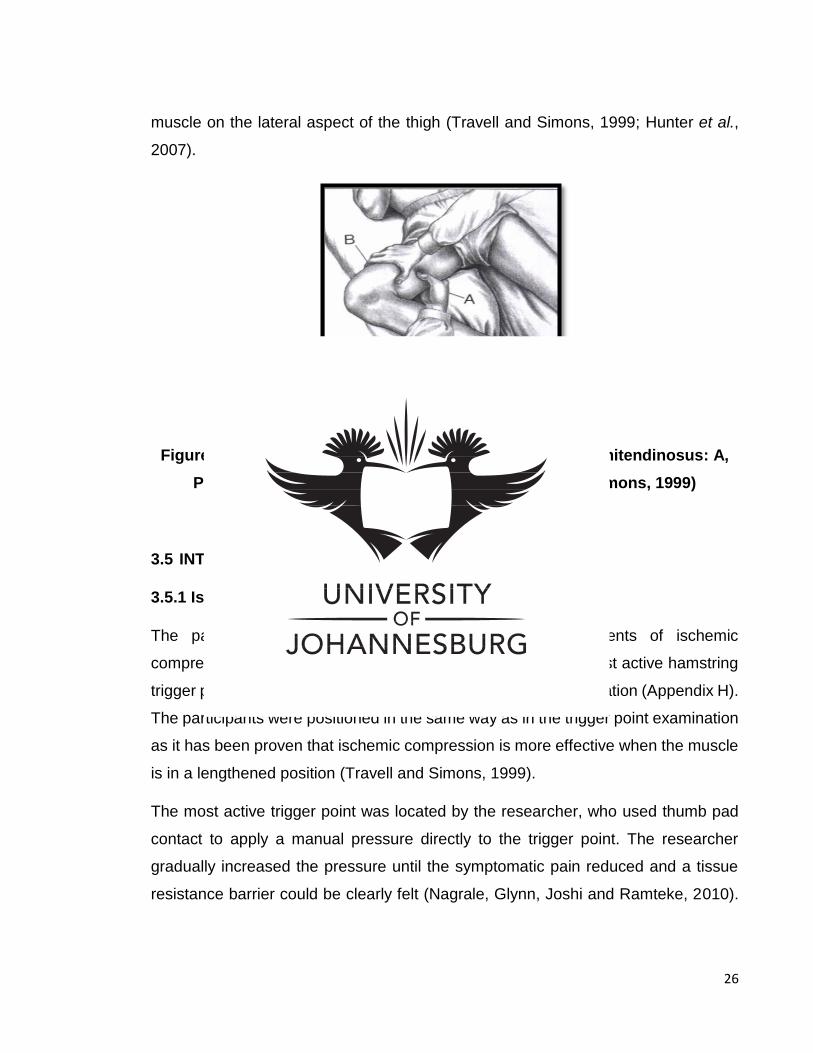
The semimembranosus and the semitendinosus trigger points were approached
from the medial aspect of the thigh (Travell and Simons, 1999; Hunter and Speed,
2007). The participant was in a supine position as demonstrated in figure 3.1, with
the involved thigh abducted, the knee flexed to change the tension in the muscle and
the lower limb supported with a pillow.
For the pincer palpation, the researcher used the thumb and index fingers to grasp
the distal medial hamstring mass 8-12 cm superior to the posterior knee fold. The
pinched muscle mass was pulled away from the femur to ensure that all of the
semitendinosus and semimembranosus musculature was included for palpation.
The researcher then rolled the muscle mass between the digital contacts to examine
for a taut band and a tender spot (Travell and Simons, 1999; Hunter et al., 2007).
The biceps femoris trigger points were examined from the posterior aspect of the
thigh in a lateral recumbent position on the opposite side with the knee slightly bent.
The researcher used flat palpation to identify the trigger points in the biceps femoris
26
muscle on the lateral aspect of the thigh (Travell and Simons, 1999; Hunter et al.,
2007).
Figure 3.1. Patient Position for Semimembranosus and Semitendinosus: A, Pincer Grip Palpation; B, Flat Palpation (Travell and Simons, 1999)
3.5 INTERVENTION
3.5.1 Ischemic compression
The participants from group A each received six treatments of ischemic
compression. Ischemic compression was only applied to the most active hamstring
trigger point identified through the hamstring trigger point examination (Appendix H).
The participants were positioned in the same way as in the trigger point examination
as it has been proven that ischemic compression is more effective when the muscle
is in a lengthened position (Travell and Simons, 1999).
The most active trigger point was located by the researcher, who used thumb pad
contact to apply a manual pressure directly to the trigger point. The researcher
gradually increased the pressure until the symptomatic pain reduced and a tissue
resistance barrier could be clearly felt (Nagrale, Glynn, Joshi and Ramteke, 2010).
27
The digital pressure was sustained for 60 seconds only, with no stroking, rubbing or
stripping movements (De Las Peñas et al., 2006).
3.5.2 Percussive massage device
Participants from group B received six treatments of therapeutic massage with a
percussive device. Percussive massage with a device was applied over the entirety
of the hamstring muscle on the side containing the most active trigger point identified
through the hamstring trigger point examination (Appendix H).
The device-assisted soft tissue manipulation technique was performed by the
researcher with a percussive massaging device. In this research, the Thumper Maxi
Pro demonstrated in figure 3.2 was used. The Thumper Maxi Pro device operates
with ordinary 230-240-volt household current at a frequency of 50-60 Hz with a
speed impact of 1200-2100 rate per minute (20-35 pulses per second) (Thumper
Massager, 2019).
Figure 3.2 Thumper Maxi Pro (Thumper Massager, 2019)
Participants were asked to expose the hamstring muscle by putting on shorts, after
which they were shown the device and informed of the procedure. Participants were
positioned in a prone position with their hips and knees extended. The Thumper Maxi
28
Pro was wiped clean with a dampened cloth before every intervention and plugged
in. No oil or liniment were used as instructed by the Thumper Maxi Pro operator’s
manual. The percussive massaging device was switched on and applied over the
entirety of the hamstring muscle on the side containing the most active trigger points
for 60 seconds. The device was kept stationary during the treatment.
3.6 SUBJECTIVE MEASUREMENTS
3.6.1 Numerical Pain Rating Scale
The NPRS (Appendix G) is a horizontal line that is divided into equal parts of ten. A
vertical line marks each equal part and is assigned a number from 0 to 10. Zero
indicated ‘no pain’ and 10 indicated the ‘worst possible pain’, while 4-5 indicated
moderate pain. A study conducted by Young, Cleland, Michener and Brown (2010)
have proved the NPRS to be viable and reliable. It is one of the most frequently used
tool for the subjective measurement of pain (Ferreira-Valente, Pais-Ribeiro and
Jensen, 2011).
In this study, the NPRS (Appendix G) was used to monitor the pain intensity from
the hamstring myofascial trigger point as perceived by the participants throughout
the trial period. The NPRS was completed by all participants with regards to their
hamstring trigger point pain. Participants read and filled out a NPRS on the first,
fourth and seventh visits.
3.7 OBJECTIVE MEASUREMENTS
3.7.1 Pressure algometer
The pressure algometer seen in figure 3.3 is a device used to measure pain pressure
threshold. Algometer testing is based on the minimum amount of pressure that
initiates pain and is a good indication of an individual’s pain sensitivity. The hand-
29
held device consists of a spring operator force gauge that is attached to a rounded
1cm rubber tip. The pressure algometer is calibrated in kg/cm² and allows the
recording of measurements and for the device to be reset between measurements
(Harrison and Siskin, 2013). A study by Kinser, Sands, and Stone (2009)
demonstrated the reliability of the pressure algometer when the application force
was compared and correlated with that of the force plate.
Figure 3.3 Pressure Algometer (Fischer, 1986).
The measurements with the pressure algometer were done on the active hamstring
trigger point found during the hamstring trigger point examination on all participants.
Algometer measurements took place on the initial, fourth and seventh visits. The
hand-held device was placed perpendicular on the body surface over the trigger
point. A gradual increasing downwards pressure was applied onto the trigger point
and the researcher instructed the participant to inform when the first point of pain or
discomfort was felt. At that time, the researcher then stopped applying the pressure
and recorded the reading (Kinser et al., 2009).
30
3.7.2 Baseline goniometer
A goniometer is used to measure the total amount motion at a specific joint during
both active and passive range of motion. For this study, a universal goniometer was
used. This goniometer consisted of a stationary arm that was held on a fixed part of
the body and a moving arm that was moved with the moving joint to measure the
respective value. It has been found that manual goniometers can be used with
confidence for clinical assessments (Nussbaumer, Leunig, Glatthorn, Stauffacher
Gerber and Maffiuletti, 2010).
The baseline goniometer was used to record measurements of hamstring
extensibility during passive knee extension. Muscle extensibility is defined as ability
of a muscle to extend to a set endpoint, which is usually measured by the relevant
joint angle (Weppler and Magnusson, 2010). The passive knee extension test has
excellent inter rater as well as test-retest reliability (Gnat, Kuszewski, Koczar and
Dziewońska, 2010).
For the passive knee extension test, the participant was asked to lie in a supine
position. The researcher lifted the leg with the most active trigger points so that the
hip and knee were flexed to 90 degrees. The researcher ensured that the opposite
lower limb remained extended on the bed throughout the test. From this position, the
hip flexion was maintained at 90 degrees while the knee was passively extended
until firm resistance to motion was felt. During the procedure, a plastic standard 360-
degree goniometer with two arms demonstrated in figure 3.4 was used to measure
the popliteal angle to determine the hamstring extensibility (Bakhtiary et al., 2011).
31
Figure 3.4 Baseline Goniometer (Prohealthsys, 2019)
3.8 DATA ANALYSIS
Objective and subjective data were collected by the researcher and analysed by a
consultant from STATKON (located on the University of Johannesburg Kingsway
Campus). The analyst used normality tests, descriptive data and clinical statistics to
summarise, organise and interpret the data gathered from the entire sample of 30
participants. The Shapiro-Wilk test was used to check normality of the variables.
Intra-group analysis consisted of one-way repeated measures ANOVA and the
Friedman test when the data was distributed non-parametrically. This test
determined the possibility of any statistically significant changes pre and post
treatment over the three-week trial period and when (i.e. between which visits) those
changes occurred. Inter-group analysis was done by the use of the independent t-
test (for data distributed parametrically) and the Mann-Whitney U test (for data
distributed non-parametrically) in order to check statistically significant differences
between the two groups.
32
3.9 ETHICAL CONSIDERATIONS
All participants that took part in this study were requested to read the information
form (Appendix B) and sign the consent form (Appendix C) specific to this study. The
information form outlined the details of the researcher, purpose of the study and
benefits of participating in the study, as well as participant assessment and treatment
procedure.
Any risks, benefits and discomforts related to the treatment involved were explained
and the participants’ safety were ensured at all times (prevention of harm). The
information and consent forms stipulated that the participant’s privacy was protected
by ensuring their anonymity (no names/personal information were taken) and
standard doctor-patient confidentiality was ensured for the duration of the study. The
participant was provided with a research number and a research file that was kept
safe within the chiropractic clinic to ensure confidentiality. After the study, all the
information was converted to data and could not be traced back to the participant.
Participants were informed that their participation was on a voluntary basis only and
that they were free to withdraw at any stage during the study without penalty. Results
of the study will be made available to participants on request.
Risk regarding with ischemic compression therapy and percussive massage therapy
with a device is minimal. Some participants experienced slight discomfort and pain
during ischemic compression and percussive massage, which is normal. Some
participants reported itching with the percussive massage device. The pain,
discomfort and itching never exceeded the participant’s pain tolerance. Post-
treatment stiffness, pain and red temporary discoloration of the skin were expected,
as these are normal responses.
Professor Christopher Stein (Chairperson of the Faculty of Health Sciences
Research Ethics Committee at the University of Johannesburg) was asked for
permission to use students on the campus as participants in this study, which was
granted. The treatment took place on the University of Johannesburg Doornfontein
campus after the necessary Higher Degrees Committee clearance letter (Appendix
33
K) and Ethics Committee clearance letter (Appendix L) were obtained. Participants
were referred to appropriate health care professionals when necessary.
A similarity report for this study has been obtained through the Turnitin programme
of the University of Johannesburg (Appendix M). This dissertation has been edited
by a qualified language practitioner (Appendix N).

34
CHAPTER FOUR: RESULTS
4.1 INTRODUCTION
The results presented in this chapter were obtained during the clinical study. The
sample group consisted of 30 participants, 15 of whom received ischemic
compression (group A) and 15 of whom received therapeutic massage with a
percussive device (group B).
All the subjective and objective data captured were analysed and tabulated in order
to capture any clinically or statistically significant improvements that occurred in each
of the individual treatment groups as well as to determine any significant differences
between the two treatment groups.
The analyses of this study were based on three readings that were recorded at the
initial visit, visit four and visit seven and included:
Demographical data analysis of age and gender
Subjective data analysis
o NPRS
Objective data analysis
o pressure algometer
o baseline goniometer
The probability value (p-value) for all the test was set at 0.05, representing the level
of significance. Therefore, only a p-value that that was ≤ 0.05 was statistically
significant.
The method used for the clinical analysis of the data with regards to the percentage
increase or decrease of the mean values over a treatment period was as follows:
Percentage increase of the mean value over a treatment period:
𝑃𝑒𝑟𝑐𝑒𝑛𝑡𝑎𝑔𝑒 𝑖𝑛𝑐𝑟𝑒𝑎𝑠𝑒 =New Amount−Original Amount
Original Amount 𝑥 100
35
Percentage decrease of mean value over treatment period:
𝑃𝑒𝑟𝑐𝑒𝑛𝑡𝑎𝑔𝑒 𝑑𝑒𝑐𝑟𝑒𝑎𝑠𝑒 =Original Amount−New Amount
Original Amount 𝑥 100
4.1.1 Normality testing
The Shapiro-Wilk test was used to establish the normality, and is used for sample
sizes of ≤ 50 participants. The statistics found were not normally distributed, due to
the small sample size and independent sample groups, therefore non-parametric
testing was applied for inter-and intragroup analysis.
4.1.2 Descriptive and clinical analysis
The descriptive and clinical statistics were used to summarise and describe the data
collected.
4.1.3 Intragroup analysis
The Friedman test, a non-parametric test, was used for the intragroup analysis. It
was used to determine if there was a significant difference in any of the two individual
groups as well as the total sample over a time period. To determine when these
differences occurred, i.e. between which visits, the non-parametric Wilcoxon signed-
rank test was done to establish any statistical significance.
4.1.4 Intergroup analysis
The intergroup analysis was done using the Mann-Whitney U test, a non-parametric
test used to establish the mean equivalence. The test compares the mean rank
values of the two individual groups, to determine whether one group is superior to
the other.
36
4.2 DEMOGRAPHIC DATA ANALYSIS
The sample group of this study consisted of 15 males and 15 females. Group A
consisted of 15 participants; seven females and eight males. Group B consisted of
15 participants; eight females and seven males. The mean age, demonstrated in
table 4.1, was 24.93 years for group A and 25.2 years for group B, making the total
sample group mean age 25.07 years.
Table 4.1 Demographic Data within the Sample of 30 Participants
Data Group A Group B Combined Total
Age Distribution (Years)
23-30 21-32 21-32
Mean age (Years)
24.93 25.2 25.07
Gender distribution
3.6 Female
8 Male 3.7 Female
7 Male 15 Female
15 Male
4.3 SUBJECTIVE DATA ANALYSIS
The subjective data for this study were obtained using the NPRS.
4.3.1 Intragroup analysis of the Numerical Pain Rating Scale
The NPRS was used to capture the participants’ perceived pain intensity on a scale
of 0 to 10. The Friedman test was used to compare that results from each individual
group over time. To detect exactly where any differences occurred over the time
within each individual group, the Wilcoxon signed-rank test was used. The test was
37
able to detect the differences between the first and fourth visits, fourth and seventh
visits as well as the first and seventh visits.
4.3.1.1 Numerical Pain Rating Scale statistics for group A
Group A had a mean value of 5.80 at the first consultation, 3.93 at fourth consultation
and at 1.47 at the seventh. Based on the mean NPRS values obtained for group A,
a percentage was calculated in order to determine whether there was an overall
improvement or a lack thereof. Group A showed a 74.66% change.
Table 4.2 Friedman Test Changes in NPRS Values of Group A
Group A: Friedman Test
Visit Mean Rank P-Value
Visit 1 2.97 0.000 Visit 4 2.03
Visit 7 1.00
As table 4.2 demonstrates, group A had a mean rank value of 2.97 at visit 1, 2.03 at
visit 4 and 1.00 at visit 7. The Friedman test for group A showed a p-value of 0.000, which was statistically significant (p≤0.05).
To detect exactly where any differences occurred over the time within group A, the
Wilcoxon signed-rank test was used. The test was able to detect the differences
between the first and fourth visits, the fourth and seventh visits, and the first and
seventh visits.
38
Table 4.3 Wilcoxon Signed-Rank Test for Group A
Group A: Wilcoxon Signed-Rank Test
Visit P-Value
Visit 1 – Visit 4 0.001
Visit 4 – Visit 7 0.001
Visit 1 – Visit 7 0.001
The NPRS values for group A demonstrated in table 4.3 show a statistically
significant improvement for the intervals between the first and fourth visits (p=0.001),
between the fourth and seventh visits (p=0.001), and between the first and seventh
visits (p=0.001). Therefore, the change in scores from group A showed a significant
difference (p≤0.05) that occurred over the time intervals.
4.3.1.2 Numerical Pain Rating Scale Statistics for group B
Group B had a mean value of 5.87 at the first consultation, 3.93 at the fourth
consultation and 1.40 at the seventh consultation.
Based on the mean NPRS values obtained for group B, a percentage was calculated
in order to determine whether there was an overall improvement or a lack thereof.
Group B showed a 76.15% change.
Table 4.4 Friedman Test Changes in NPRS Values of Group B
Group B: Friedman Test
Visit Mean Rank P-Value
Visit 1 2.97 0.000 Visit 4 2.00
Visit 7 1.03
39
To detect exactly where any differences occurred over the time within group B, the
Wilcoxon signed-rank test was used. The test was able to detect the differences
between the first and fourth visits, the fourth and seventh visits, and the first and
seventh visits.
Table 4.5 Wilcoxon Signed-Rank Test for Group B
Group B: Wilcoxon Signed-Rank Test
Visit P-Value
Visit 1 – Visit 4 0.001
Visit 4 – Visit 7 0.001
Visit 1 – Visit 7 0.001
The NPRS values for group B demonstrated in table 4.5 show a statistically
significant improvement for the intervals between the first and fourth visits (p=0.001),
the fourth and seventh visits (p=0.001) and the first and seventh visits (p=0.001).
Therefore, group B showed a significant improvement (p≤0.05), which occurred over
all time intervals.
40
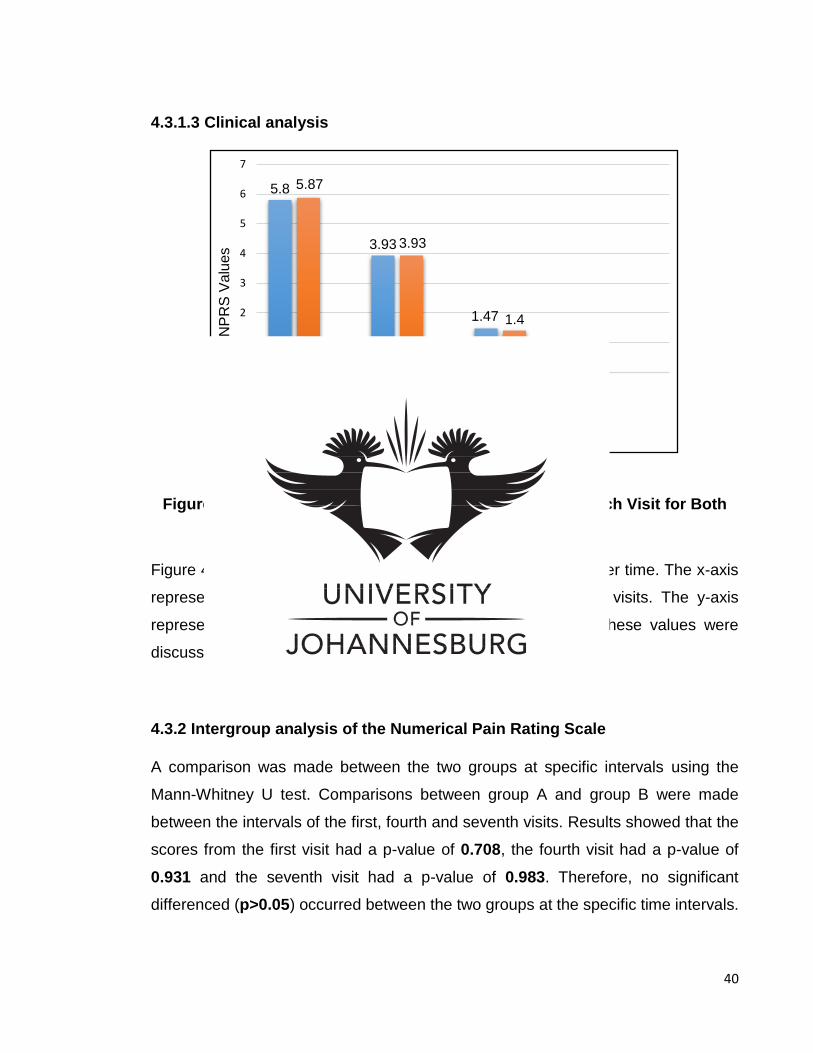
4.3.1.3 Clinical analysis
Figure 4.1 Bar Graph Representing the NPRS Values of Each Visit for Both Groups
Figure 4.1 compares the NPRS mean values for both groups over time. The x-axis
represents the NPRS results at the first, fourth and seventh visits. The y-axis
represents the improvement seen on the scale of 0 to 10. These values were
discussed
4.3.2 Intergroup analysis of the Numerical Pain Rating Scale
A comparison was made between the two groups at specific intervals using the
Mann-Whitney U test. Comparisons between group A and group B were made
between the intervals of the first, fourth and seventh visits. Results showed that the
scores from the first visit had a p-value of 0.708, the fourth visit had a p-value of
0.931 and the seventh visit had a p-value of 0.983. Therefore, no significant
differenced (p>0.05) occurred between the two groups at the specific time intervals.
5.8
3.93
1.47
5.87
3.93
1.4
0
1
2
3
4
5
6
7
Visit 1 Visit 4 Visit 7
NPR
S Va
lues
Visits
Group A Group B
41
4.4 OBJECTIVE DATA ANALYSIS
Objective data for this study was obtained using the pressure algometer and
baseline goniometer.
4.4.1. Intragroup analysis of pressure algometer
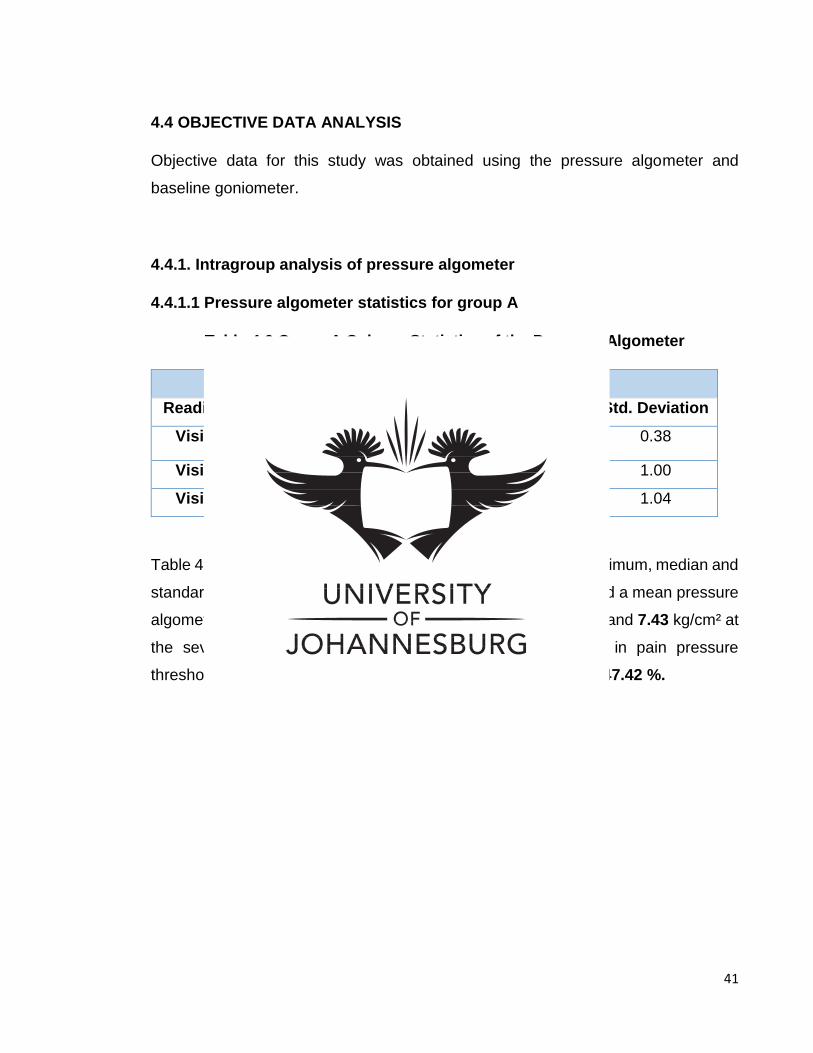
4.4.1.1 Pressure algometer statistics for group A
Table 4.6 Group A Column Statistics of the Pressure Algometer
Group A: Pressure Algometer kg/cm²
Readings Mean Maximum Minimum Median Std. Deviation
Visit 1 5.04 6.0 4.5 5.0 0.38
Visit 4 6.21 8.5 4.0 6.0 1.00
Visit 7 7.43 9.0 5.5 7.3 1.04
Table 4.6 illustrates the pressure algometer mean, maximum, minimum, median and
standard deviation values of group A. Group A at the first visit had a mean pressure
algometer reading of 5.04 kg/cm², 6.21 kg/cm² at the fourth visit, and 7.43 kg/cm² at
the seventh visit. Therefore, the mean percentage increase in pain pressure
threshold measured by the pressure algometer for group A was 47.42 %.
42
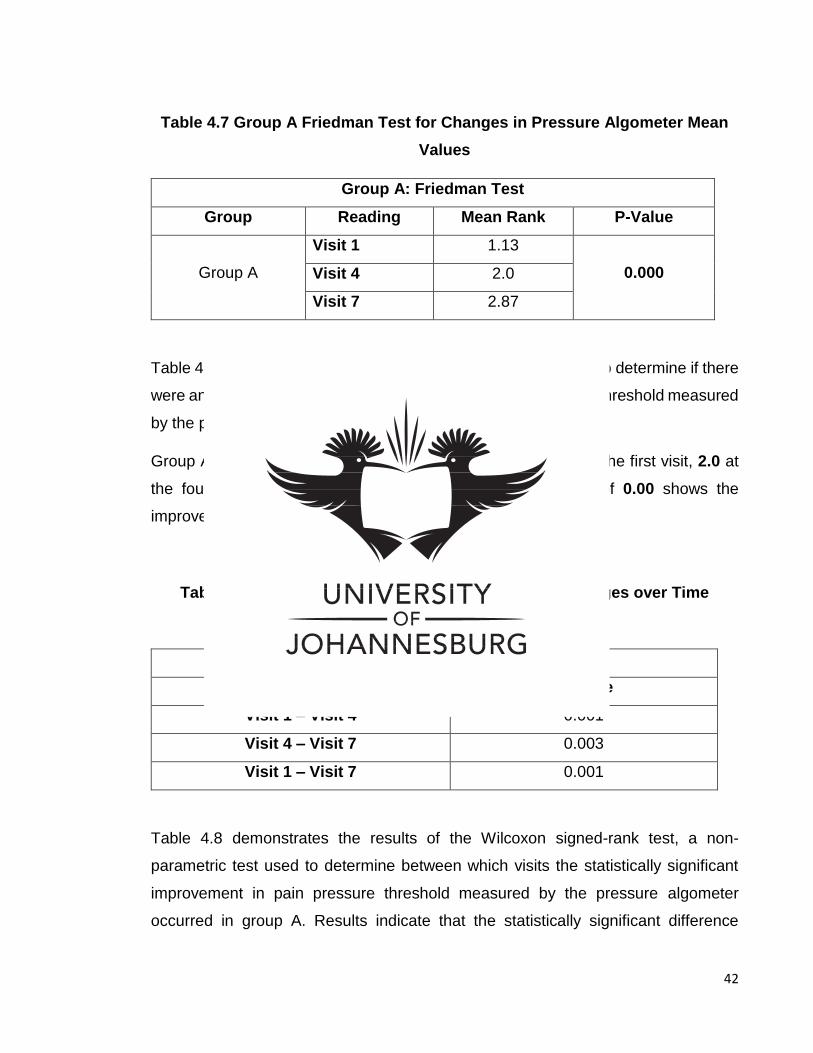
Table 4.7 Group A Friedman Test for Changes in Pressure Algometer Mean Values
Group A: Friedman Test
Group Reading Mean Rank P-Value
Group A
Visit 1 1.13 0.000 Visit 4 2.0
Visit 7 2.87
Table 4.7 demonstrates the non-parametric Friedman test used to determine if there
were any changes of any statistical significance in pain pressure threshold measured
by the pressure algometer within group A over the trial period.
Group A had a mean rank pressure algometer value of 1.13 at the first visit, 2.0 at
the fourth visit, and 2.87 at the seventh visit. The p-value of 0.00 shows the
improvement was statistically significant (p≤0.05).
Table 4.8 Group A Wilcoxon Signed-Rank Test for Changes over Time (Pressure Algometer)
Group A: Wilcoxon Signed-Rank Test
Visits P-Value
Visit 1 – Visit 4 0.001
Visit 4 – Visit 7 0.003
Visit 1 – Visit 7 0.001
Table 4.8 demonstrates the results of the Wilcoxon signed-rank test, a non-
parametric test used to determine between which visits the statistically significant
improvement in pain pressure threshold measured by the pressure algometer
occurred in group A. Results indicate that the statistically significant difference
43
(p≤0.05) was found between visit 1 and visit 4 (p=0.001), between visit 4 and visit 7
(p=0.003), and between visit 1 and visit 7 (p=0.001).
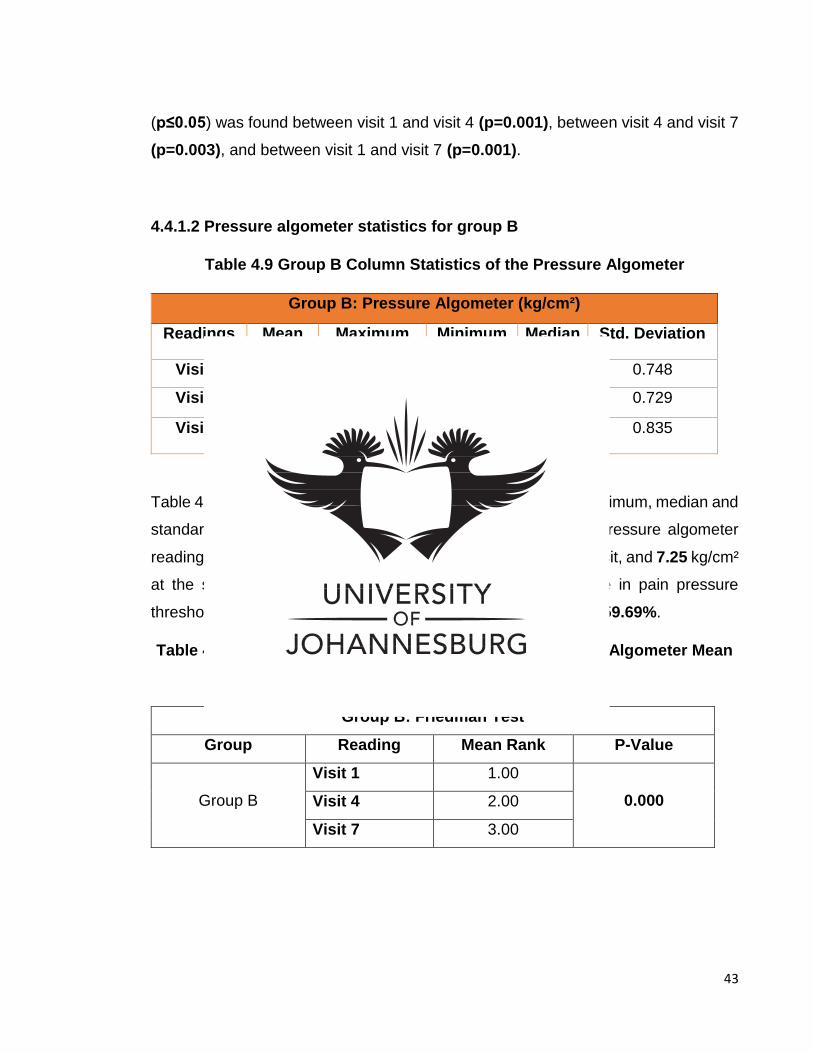
4.4.1.2 Pressure algometer statistics for group B
Table 4.9 Group B Column Statistics of the Pressure Algometer
Group B: Pressure Algometer (kg/cm²)
Readings Mean Maximum Minimum Median Std. Deviation
Visit 1 4.54 5.7 3.2 4.7 0.748
Visit 4 5.99 7.3 4.7 6.0 0.729
Visit 7 7.25 8.5 5.7 7.0 0.835
Table 4.9 illustrates the pressure algometer mean, maximum, minimum, median and
standard deviation values of Group B. Group B had a mean pressure algometer
reading of 4.54 kg/cm² at the first visit, 5.99 kg/cm² at the fourth visit, and 7.25 kg/cm²
at the seventh visit. Therefore, the mean percentage increase in pain pressure
threshold measured by the pressure algometer for group B was 59.69%.
Table 4.10 Group B Friedman Test for Changes in Pressure Algometer Mean Values
Group B: Friedman Test
Group Reading Mean Rank P-Value
Group B
Visit 1 1.00 0.000 Visit 4 2.00
Visit 7 3.00
44
Table 4.10 demonstrates the results of the non-parametric Friedman test, which was
used to determine if there were changes of any statistical significant in pain pressure
threshold measured by the pressure algometer within group B over the trial period.
Group B had a mean rank pressure algometer value of 1.0 at the first visit, 2.0 at the
fourth visit, and 3.0 at the seventh visit. The p-value of 0.00 ≤ shows that the
improvement was statistically significant (p≤0.05).
Table 4.11 Group B Wilcoxon Signed-Rank Test for Changes over Time (Pressure Algometer)
Group B: Wilcoxon Signed-Rank Test
Visits P-Value
Visit 1 – Visit 4 0.001
Visit 4 – Visit 7 0.001
Visit 1 – Visit 7 0.001
Table 4.11 demonstrates the results from the Wilcoxon signed-rank test, a non-
parametric test, used to determine between which visits the statistically significant
improvement in pain pressure threshold measured by the pressure algometer
occurred in group B.
The statistically significant difference (p≤0.05) was found between the visit first and
fourth visits (p=0.001), between the fourth and seventh visits (p=0.001), and
between the first and seventh visits (p=0.001).
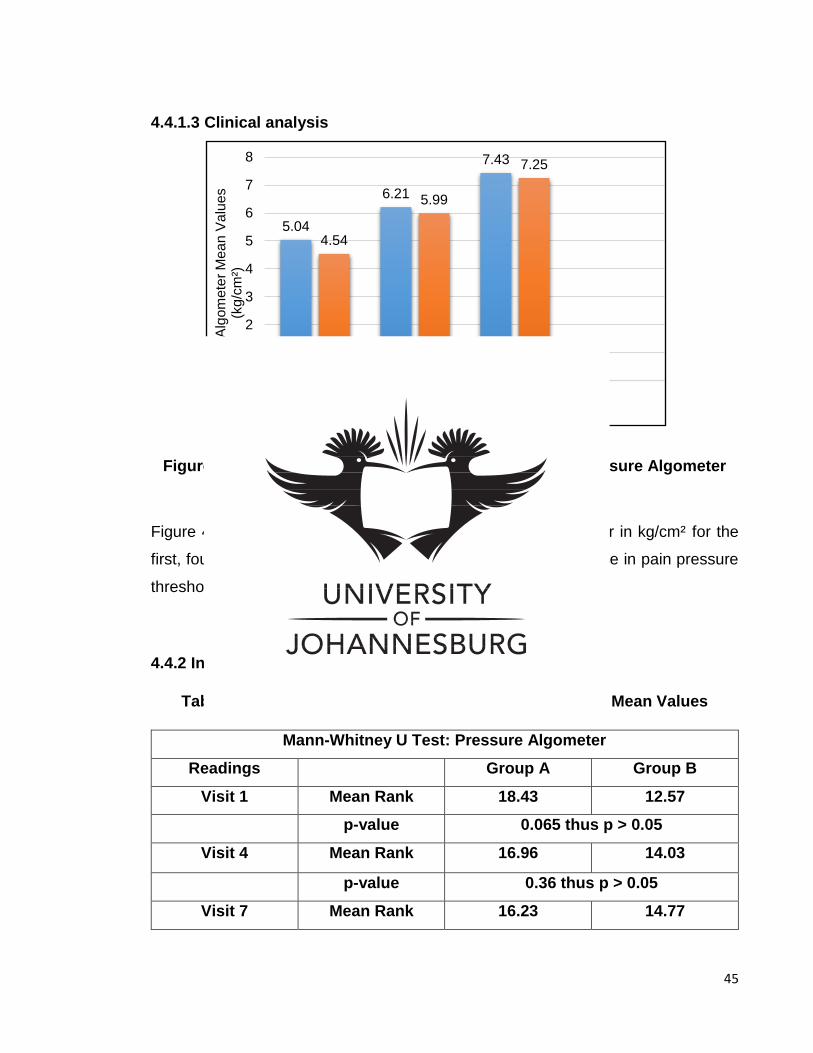
45
4.4.1.3 Clinical analysis
Figure 4.2 Changes in the Mean Pain Threshold of the Pressure Algometer for Group A and Group B
Figure 4.2 illustrates the mean values of the pressure algometer in kg/cm² for the
first, fourth, and the seventh visits. It indicates an overall increase in pain pressure
threshold.
4.4.2 Intergroup analysis of the pressure algometer
Table 4.12 Mann-Whitney U Test for Pressure Algometer Mean Values
Mann-Whitney U Test: Pressure Algometer
Readings Group A Group B
Visit 1 Mean Rank 18.43 12.57
p-value 0.065 thus p > 0.05
Visit 4 Mean Rank 16.96 14.03
p-value 0.36 thus p > 0.05
Visit 7 Mean Rank 16.23 14.77
5.04
6.21
7.43
4.54
5.99
7.25
0
1
2
3
4
5
6
7
8
Visit 1 Visit 4 Visit 7Pre
ssur
e A
lgom
eter
Mea
n V
alue
s (k
g/cm
²)
Group A Group B
46
p-value 0.65 thus > 0.05
Table 4.12 demonstrates the results from the non-parametric Mann-Whitney U test
that was used to compare mean rank pressure algometer values of the two groups.
The test determined whether the difference between the groups was purely by
chance or if it was statistically significant and revealing of the more superior
treatment.
The baseline reading of the p-value at visit 1 was 0.065, therefore the groups started
off comparable. The p-value remained greater at visit 4 (0.36) and at visit 7 (0.65). These results indicate no statistically significant difference (p>0.05) in the mean
pressure algometer readings between group A and group B.
4.4.3 Intragroup analysis of the baseline goniometer
4.4.3.1 Baseline goniometer statistics of group A
Table 4.13 Group A Column Statistics of the Baseline Goniometer
Group A: Baseline Goniometer (Degrees)
Readings Mean Maximum Minimum Median Std. Deviation
Visit 1 29.47 50 15 30 8.236
Visit 4 22.53 37 5 20 9.702
Visit 7 17.20 30 3 20 9.049
Table 4.13 illustrates the baseline goniometer mean, maximum, minimum, median
and standard deviation values of group A. The popliteal angle was measured from
90 degrees to 0 degrees. A decrease in degrees indicates an increase in hamstring
flexibility. Group A had a mean baseline goniometer reading of 29.47° at the first
visit, 22.53° at the fourth visit and 17.20° at the seventh visit. The mean percentage
47
change in hamstring extensibility measured by the baseline goniometer for group A
was 71.34 %.
Table 4.14 Group A Friedman Test for Changes in Baseline Goniometer Mean Values
Group A: Friedman Test
Group Reading Mean Rank P-Value
Group A
Visit 1 2.60 0.001 Visit 4 2.07
Visit 7 1.33
Table 4.14 demonstrates the results of the non-parametric Friedman test used to
determine if there were changes of any statistical significant in hamstring extensibility
measured by the baseline goniometer within group A over the trial period.
Group A had a mean rank baseline goniometer value of 2.60 at the first visit, 2.07 at
the fourth visit and 1.33 at the seventh visit. The p-value of 0.001 shows that the
improvement was statistically significant (p≤0.05).
Table 4.15 Group A Wilcoxon Signed-Rank Test for Changes over Time (Baseline Goniometer)
Group A: Wilcoxon Signed-Rank Test
Visits P-Value
Visit 1-Visit 4 0.017
Visit 4- Visit 7 0.029
Visit 1-Visit 7 0.002
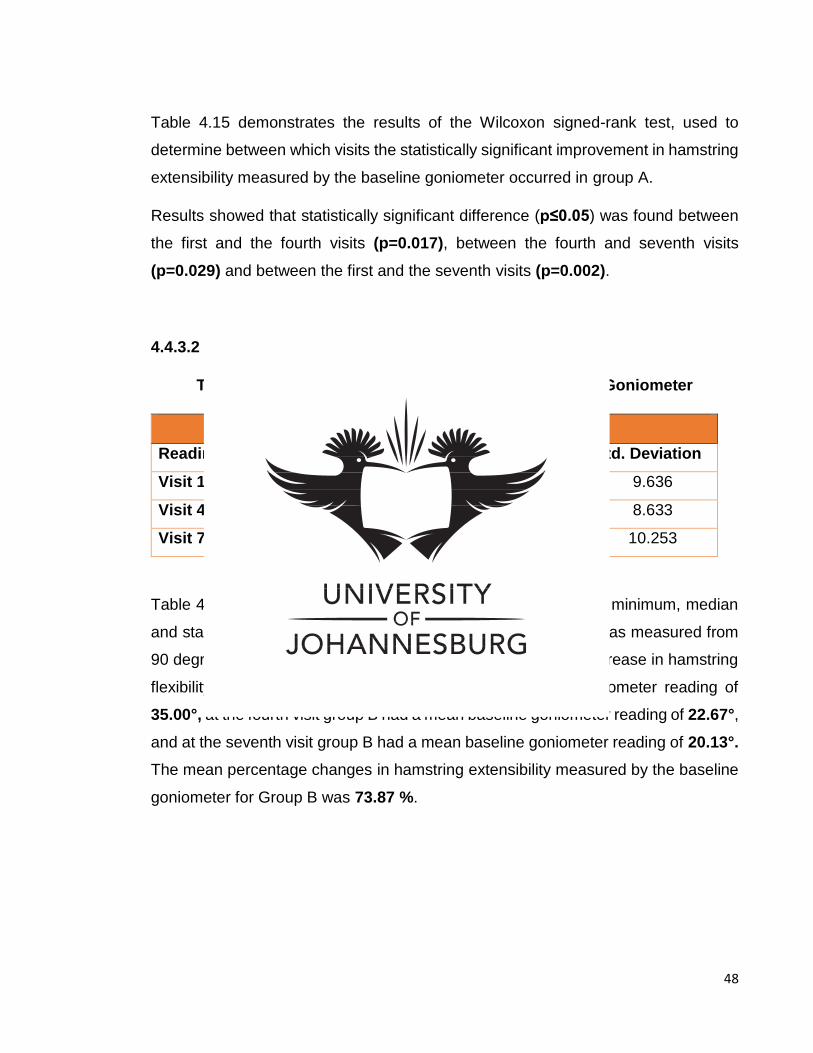
48
Table 4.15 demonstrates the results of the Wilcoxon signed-rank test, used to
determine between which visits the statistically significant improvement in hamstring
extensibility measured by the baseline goniometer occurred in group A.
Results showed that statistically significant difference (p≤0.05) was found between
the first and the fourth visits (p=0.017), between the fourth and seventh visits
(p=0.029) and between the first and the seventh visits (p=0.002).
4.4.3.2 Baseline goniometer statistics of group B
Table 4.16 Group B Column Statistics of the Baseline Goniometer
Group B: Baseline Goniometer
Readings Mean Maximum Minimum Median Std. Deviation
Visit 1 35 55 20 35 9.636
Visit 4 22.67 35 5 25 8.633
Visit 7 20.13 40 5 19 10.253
Table 4.16 illustrates the baseline goniometer mean, maximum, minimum, median
and standard deviation values of Group B. The popliteal angle was measured from
90 degrees to 0 degrees. A decrease in degrees indicates an increase in hamstring
flexibility. At the first visit Group B had a mean baseline goniometer reading of
35.00°, at the fourth visit group B had a mean baseline goniometer reading of 22.67°, and at the seventh visit group B had a mean baseline goniometer reading of 20.13°. The mean percentage changes in hamstring extensibility measured by the baseline
goniometer for Group B was 73.87 %.
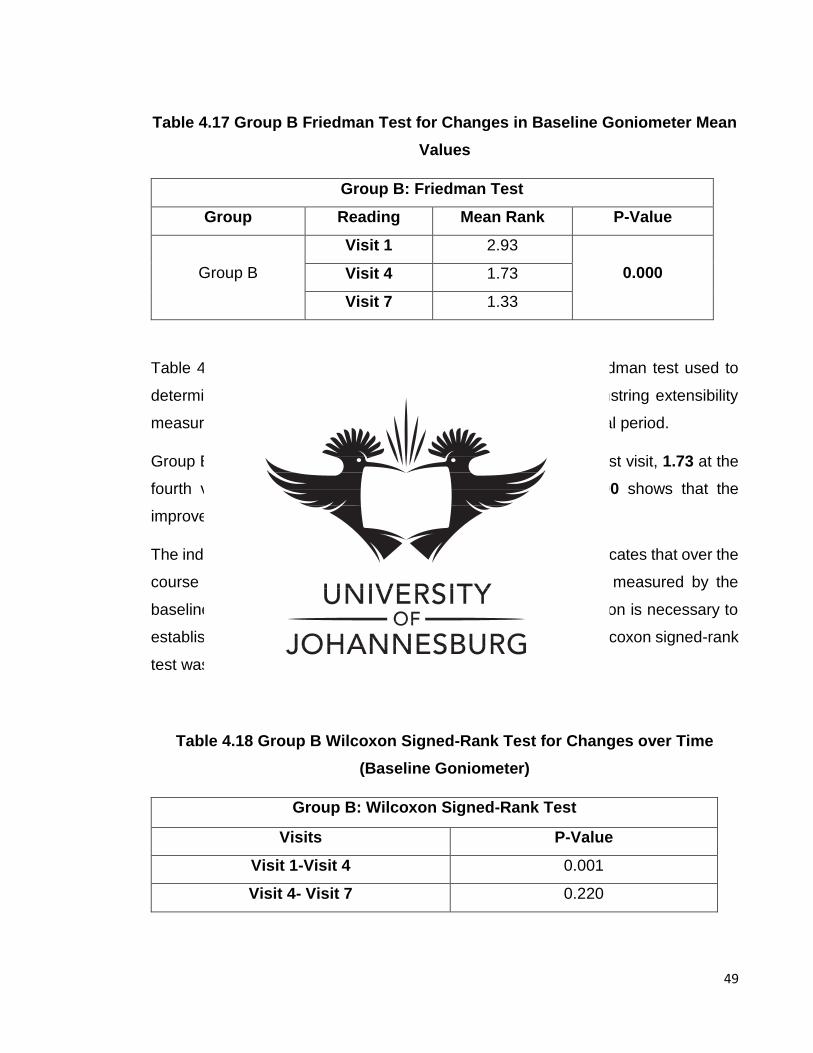
49
Table 4.17 Group B Friedman Test for Changes in Baseline Goniometer Mean Values
Group B: Friedman Test
Group Reading Mean Rank P-Value
Group B
Visit 1 2.93 0.000 Visit 4 1.73
Visit 7 1.33
Table 4.17 demonstrates the results of the non-parametric Friedman test used to
determine if there were changes of statistical significant in hamstring extensibility
measured by the baseline goniometer within group B over the trial period.
Group B had a mean baseline goniometer value of 2.93 at the first visit, 1.73 at the
fourth visit and 1.33 at the seventh visit. The p-value of 0.00 shows that the
improvement was statistically significant (p≤0.05).
The individual groups displayed a p-value of 0.00 ≤ 0.05. This indicates that over the
course of the trial, the improvement in hamstring extensibility measured by the
baseline goniometer was statistically significant. Further evaluation is necessary to
establish between which visits the improvement occurred. The Wilcoxon signed-rank
test was used to evaluate where the improvement occur.
Table 4.18 Group B Wilcoxon Signed-Rank Test for Changes over Time (Baseline Goniometer)
Group B: Wilcoxon Signed-Rank Test
Visits P-Value
Visit 1-Visit 4 0.001
Visit 4- Visit 7 0.220
50
Visit 1-Visit 7 0.001
Table 4.18 demonstrates the results of the Wilcoxon signed-rank test, a non-
parametric test used to determine between which visits the statistically significant
improvement in hamstring extensibility measured by the baseline goniometer
occurred in group B.
The statistically significant difference (p≤0.05) was found between the first and fourth
visits (p=0.001), and between the first and seventh visits (p=0.001). There was no
statistically difference (p>0.05) between visit four and visit seven (p=0.220).
4.4.3.2 Clinical analysis
Figure 4.3 Changes in the Mean Readings of Baseline Goniometer
Figure 4.3 illustrates the mean values of the baseline goniometer of both groups of
the first, fourth, and the seventh visits. It indicates an overall increase in hamstring
extensibility.
29.47
22.53
17.2
35
22.6720.13
0
5
10
15
20
25
30
35
40
Visit 1 Visit 4 Visit 7
Bas
elin
e G
onio
met
er (D
egre
es)
Group A Group B
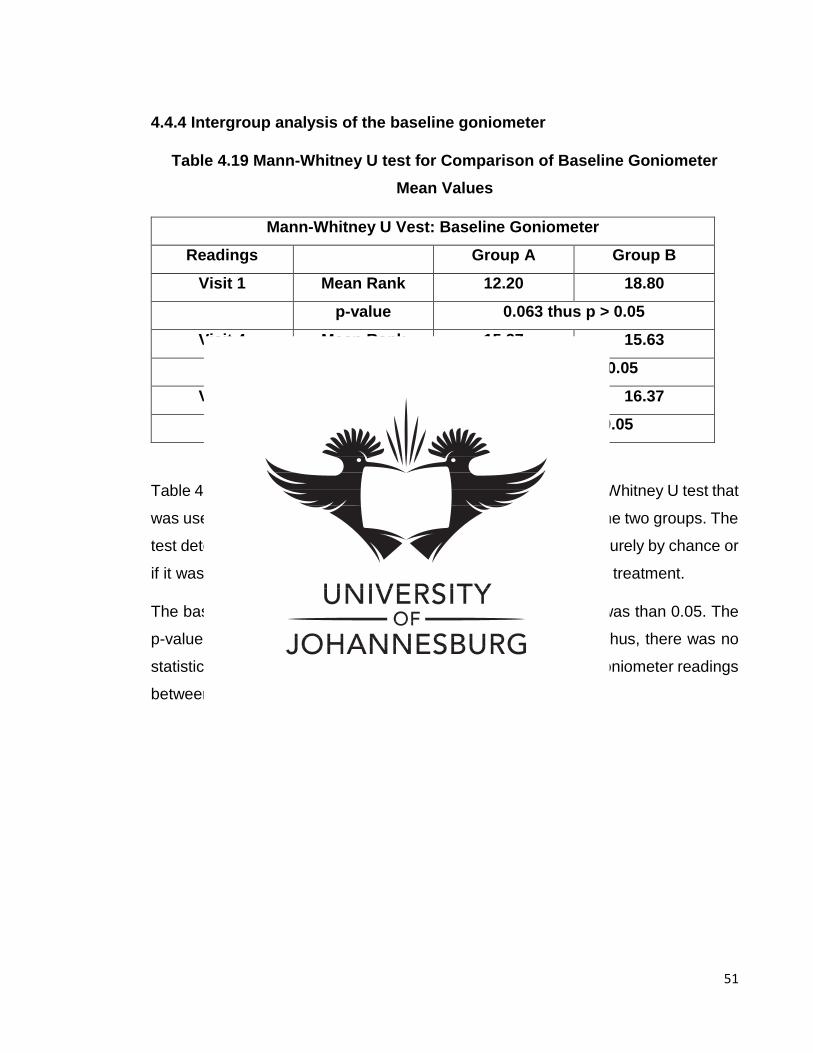
51
4.4.4 Intergroup analysis of the baseline goniometer
Table 4.19 Mann-Whitney U test for Comparison of Baseline Goniometer Mean Values
Mann-Whitney U Vest: Baseline Goniometer
Readings Group A Group B
Visit 1 Mean Rank 12.20 18.80
p-value 0.063 thus p > 0.05
Visit 4 Mean Rank 15.37 15.63
P-value 0.93 thus p >0.05
Visit 7 Mean Rank 14.37 16.37
p-value 0.59 thus > 0.05
Table 4.19 demonstrates the results of the non-parametric Mann-Whitney U test that
was used to compare mean rank baseline goniometer values of the two groups. The
test determined whether the difference between the groups was purely by chance or
if it was statistically significant and revealing of the more superior treatment.
The baseline reading of the p-value at visit 1 (p=0.063) greater was than 0.05. The
p-value remained greater at visit 4 (0.93) and at visit 7 (0.59). Thus, there was no
statistically significant difference (p>0.05) in the mean baseline goniometer readings
between group A and group B.
52
CHAPTER FIVE: DISCUSSION
5.1 INTRODUCTION
The results presented in chapter four will be discussed in this chapter, particularity
those results that were of statistical significance. These findings will be compared
with the findings of previous research as discussed in the literature review presented
in chapter two, together with additional relevant research.
5.2 DEMOGRAPHIC DATA
5.2.1 Age and gender analysis
Participants between the ages of 18 and 50 years were used for this study. As
illustrated in table 4.1, the sample group was composed of 15 male and 15 female
participants, with a mean age of 25.07 years of age. The minimum age was 21 and
the maximum age was 32 years.
According to Vecchiet (2002), persons under the age of 50 years are the most likely
to have active myofascial trigger points, owing to the fact that persons of this age
group are the most active, therefore their muscles are more likely to be overused,
and have resulting micro-trauma.
5.3 SUBJECTIVE DATA
5.3.1 Intragroup analysis of the Numerical Pain Rating Scale
The results indicated that the ischemic compression group and the percussive
massage device group both demonstrated a statistically significant improvement
with regards to the NPRS values that were obtained over time. These statistically
significant changes were consistent throughout the treatment period.
53
5.3.1.1 Numerical Pain Rating Scale statistics for the ischemic compression group
The results from the Wilcoxon signed-rank test, demonstrated in table 4.3, indicated
that the ischemic compression group had a statistically significant improvement
(p≤0.05) over time from the first to the seventh treatment (p=0.001). Ischemic
compression on an active hamstring trigger point proved to have a statistically
significant improvement from the first visit to the fourth visit regarding pain perception
(p=0.001), as well as from the fourth visit to the seventh visit (p=0.001). The clinical
analysis also demonstrated that the ischemic compression group had a positive
affect over time, with decreasing pain perception of 74.66% when comparing the
measurements taken at the beginning of the trial to those taken at the end.
5.3.1.2 Numerical Pain Rating Scale statistics for the percussive massage device group
The results of the Wilcoxon signed-rank test, demonstrated in table 4.5, indicated
that the percussive massage device group had a statistically significant improvement
(p≤0.05) over time when comparing the results taken at the first visit to those from
the seventh (p=0.001). The test revealed that therapeutic massage with a percussive
device on an active hamstring trigger point proved to have a statistically significant
improvement regarding pain perception when comparing the results from the first
visit to those from the fourth visit (p=0.001), and the fourth visit to the seventh visit
(p=0.001). Clinical interpretation also showed that the percussive massage group
had a positive affect over time, with a decreasing pain perception of 76.15% from
the beginning of the trial to the end.
54
5.3.2 Intergroup analysis of the Numerical Pain Rating Scale
A comparison was made between the two groups at specific intervals using the
Mann-Whitney U test. Comparisons between the ischemic compression group and
the percussive massage group were made between the intervals of the first, fourth
and seventh visits. The first measurement had a p-value of 0.708, the fourth
measurement had a p-value of 0.931 and the seventh measurement had a p-value
of 0.983. Therefore, no significant differences (p>0.05) occurred between the two
groups at the specific time intervals with regards to pain perception.
5.3.3 Subjective data discussion
The results were conclusive in that there was a definite improvement in the extent of
the subjective pain perception experienced by both groups. When considering the
NPRS, the results indicate that both groups improved between the first and the
seventh visits. The ischemic compression group showed a more favorable
improvement than the percussive massage device group.
5.3.3.1 The effect of ischemic compression on pain perception
Ischemic compression is a non-invasive treatment method that causes temporary
decrease in blood within the myofascial trigger point in order to ultimately increase
the blood flow. The increase in blood to the myofascial trigger point flushes out the
waste product and the inflammatory exudate molecules from the myofascial trigger
point (Fritz and Grosenbach, 2009). This phenomenon then leads to an increase in
the local oxygen supply to the myofascial trigger point, allowing the affected tissue
to initiate the healing process (Arnau-Masanet et al., 2010).
Ischemic compression creates a mechanical disruption of the actin-myosin myofibril
cross links that are locked within the trigger point (Mense and Simons, 2000; Perle
et al., 1999). This disruption causes a decrease in sensory afferent input of noxious
55
stimuli to the brain via the pain gate theory (Mense et al., 2000). The pain relief
associated with ischemic compression is also linked with alternating spinal reflex
mechanisms that cause a decrease in muscle spasm (Ingbur, Kostopoulos, Larkin
and Nelson, 2008).
Behrangrad and Kamali (2017) similarly demonstrated a statistically significant
improvement (p ≤ 0.05) using the NPRS in a comparative study between ischemic
compression and lumbar pelvic manipulation as trigger point therapy for
patellofemoral pain syndrome in young adults. Ischemic compression showed to be
superior to lumbopelvic manipulation therapy in both the short and the long term with
regards to effectiveness for the treatment of patellofemoral pain syndrome.
Hou, Tsai, Cheng, Chung, and Hong (2002) investigated the immediate effect of
physical therapeutic modalities on myofascial pain in the upper trapezius muscle and
found that ischemic compression provided an immediate relieve in pain perception
and decreased the sensitivity of the myofascial trigger point.
5.3.3.2 The effect of therapeutic massage with a percussive device on pain perception
One of the reported benefits of device-assisted soft tissue manipulation is an
analgesic effect, which is a temporarily reduction or elimination of pain perceived.
Device-assisted soft tissue manipulation provides a noxious stimulation for pain
modulation, leading to an analgesic response. The pain gate theory asserts that the
pain signals are then inhibited, which could be a possible explanation for the
analgesic effect. Consequently, reduced pain lead to muscle relaxation, which allows
for normalised neuromuscular movement and improvement of the function of the soft
tissue. Soft tissue mechanotherapy is effective in treating pain, leading to muscle
relaxation (Weerapong, Hume and Kolt, 2005).
According to Frey, Evans, Knudtson, Nus, Scholl and Sluka (2008), device-assisted
soft tissue manipulation causes friction between the tissues that disrupt the tissue
56
and causes fibroblastic proliferation to the soft tissue, which results in tissue
regeneration and recovery. Scar tissue is broken down, which reinitiates the healing
process. This process begins with the increase of blood flow to the tissue, bringing
healing substances phagocytosed by white blood cells to the micro-injury site (area
of tissue disruption caused by the treatment). The repair process of the tissue leads
to less painful tissue.
5.4 OBJECTIVE DATA
5.4.1 Intragroup analysis of the pressure algometer
The results from the pressure algometer statistical analysis showed that both the
ischemic compression group and the percussive massage device group had
significant differences in the pressure algometer readings over time.
5.4.1.1 Pressure algometer statistics for the ischemic compression group
The results using the Wilcoxon signed-rank test, demonstrated in table 4.8, indicated
that the ischemic compression group had a statistically significant improvement
(p≤0.05) over time when comparing the results from the first to the seventh treatment
(p=0.001). Ischemic compression on an active hamstring trigger point proved to
have a statistically significant improvement with regards to pressure pain threshold
between the first visit and the fourth visit, (p=0.001), and between the fourth and the
seventh visit (p=0.003). The clinical interpretation also proved that ischemic
compression had a positive affect over time, with the group showing an increased
pressure pain threshold of 47.42% from the beginning of the trial to the end.
57
5.4.1.2 Pressure algometer statistics for the percussive massage device group
The results from the Wilcoxon signed-rank test, demonstrated in table 4.8, indicated
that the percussive massage device group had a statistically significant improvement
(p≤0.05) over time from the first visit to the seventh (p=0.001). The test revealed that
therapeutic massage with a percussive device on an active hamstring trigger point
proved to have a statistically significant improvement with regards to pressure pain
threshold between the first visit and the fourth visit (p=0.001), and the fourth visit and
the seventh visit (p=0.001). The clinical interpretation also proved that the
percussive massage device had a positive affect over time, with the group showing
and increased pressure pain threshold of 59.69% from the beginning of the trial to
the end.
5.4.2 Intergroup analysis of the pressure algometer
A comparison was made between the two groups at specific intervals using the
Mann-Whitney U test. Comparisons were made between the ischemic compression
group and the percussive massage group at the intervals of the first, fourth and
seventh visits. The first measurement had a p-value of 0.065, the fourth
measurement a p-value of 0.360 and the seventh a p-value of 0.650. Therefore, no
significant differences (p>0.05) occurred between the two groups at the specific time
intervals with regards to pressure pain threshold.
5.4.3 Discussion of pressure algometer results
5.4.3.1 The effect of ischemic compression on pain threshold
Dearing and Hamilton (2008) established that ischemic compression was a more
effective technique than the muscle energy technique in decreasing pressure pain
threshold in trigger points in asymptomatic patients. The effect of ischemic
compression therapy in increasing the pressure pain threshold may be attributed to

58
the reactive hyperemia caused by the temporarily occlusion of blood supply (Hou et
al., 2002). This reaction helps in flushing the muscle of inflammatory exudates and
pain metabolites, breaking down scar tissue and reducing muscle tone. Applying
direct ischemic compression diminishes the sensitivity of nodules (Travell and
Simons, 1999) and may restore the length of sarcomeres in the myofascial trigger
point (Simons, 2002). These changes may result in normal resting length of muscles.
5.4.3.2 The effect of a percussive massage device on pain threshold
According to Costantino, Galuppo, and Romiti (2017), vibration and percussion
devices have an effect in the pain gate theory by affecting the afferent discharge
from fast-adapting mechanoreceptors and muscle spindles, therefore decreasing the
pressure pain threshold.
It is thought that when vibration or percussion devices are applied directly on the
skin, the large afferent nerve fibers are activated and the small afferent nerve fibers
are inhibited. This process allows signals to be sent to the spinal cord from the large
fibers and not the small fibers, which normally transmit signals of pain, therefore
reducing the pain perceived as well as the pressure pain threshold (Magee,
Zachazewski and Quillen, 2007).
5.4.4 Intragroup analysis of the baseline goniometer
5.4.4.1 Baseline goniometer statistics for the ischemic compression group
The results of the Wilcoxon signed-rank test, demonstrated in table 4.15, indicated
that the ischemic compression group had a statistically significant improvement
(p≤0.05) over time when comparing the results from the first treatment to those of
the seventh treatment (p=0.002). The test revealed that ischemic compression on
an active hamstring trigger point proved to have a statistically significant
improvement with regards to pressure pain threshold between the first visit and the
59
fourth visit, (p=0.017), and the fourth visit and the seventh visit (p=0.029). The
clinical interpretation also proved that ischemic compression had a positive affect
over time, with this group showing an increased hamstring extensibility of 71.34 %
from the beginning of the trial to the end.
5.4.4.2 Baseline goniometer statistics for the percussive massage device group
The results of the Wilcoxon signed-rank test, demonstrated in table 4.18, indicated
that the percussive massage device group had a statistically significant improvement
(p≤0.05) over time when comparing results of the first visit to those of the seventh
(p=0.001). The test revealed that therapeutic massage with a percussive device on
an active hamstring trigger point proved to have a statistically significant
improvement with regards to pressure pain threshold between the first visit and the
fourth visit (p=0.001).There was no statistically difference between (p>0.05) the
fourth and the seventh visits (p=0.220). The clinical interpretation also proved that
percussive massaging had a positive affect over time, with this group showing an
increased hamstring extensibility of 73.87 % from the beginning of the trial to the
end.
5.4.5 Intergroup analysis of the baseline goniometer
A comparison was made between the two groups at specific intervals using the
Mann-Whitney U test. Comparisons between the ischemic compression group and
the percussive massage group were made between the intervals of the first, fourth
and seventh visits. The first measurement had a p-value of 0.063, the fourth
measurement had a p-value of 0.930 and the seventh measurement had a p-value
of 0.590. Therefore, no significant differences (p>0.05) occurred between the two
groups at the specific time intervals with regards hamstring extensibility.

60
5.4.6 Discussion of the baseline goniometer results
5.4.6.1 The effect of ischemic compression on hamstring extensibility
Desai and Jeswani (2018) compared the effectiveness of myofascial release and
ischemic compression on acute trapezitis in young adults between the ages of 18
and 30. The results show that both the techniques were effective in reducing pain
and neck disability and increasing cervical lateral flexion in the tested subjects.
Aguilera, Martin, Masanet, Botella, Soler and Morell (2009) compared the immediate
effects of ischemic compression and ultrasound for the treatment of latent myofascial
trigger points in the trapezius muscle. The results revealed an immediate decrease
in electrical activity of the trapezius muscle and a decrease of myofascial trigger
point sensitivity after both types of treatment, while improvement in the active
cervical range of motion was only noted in the ischemic compression group only.
As mentioned in section 5.4.3.1, ischemic compression therapy increases the
pressure pain threshold due to reactive hyperemia caused by the temporarily
constriction of blood supply (Hou et al., 2002), which then flushes the muscle of
inflammatory exudates and pain metabolites, breaks down scar tissue and reduces
muscle tone. These processes then reduce the of sensitivity of the myofascial trigger
point (Travell and Simons, 1999) and restore the length of sarcomeres in the
myofascial trigger point (Simons, 2002). These changes may result in normal resting
length of muscles, therefore increasing the flexibility of the muscle.
5.4.6.2 The effect of a therapeutic massage with a percussive device on hamstring extensibility
Issurin (2005) suggests that percussive massage devices may enhance excitatory
inflow from the muscle spindles to the alpha motor neuron pools and control the
recruitment thresholds and firing rates of motor units. They also decrease the
inhibitory impact of the Golgi tendon organs, providing more flexibility.
61
Furthermore, Bakhtiary et al. (2011) report a general increase in range of motion and
flexibility of the hamstring muscle in their investigation of the application of device-
assisted soft tissue manipulation on hamstring extensibility.
Finally, percussive massage devices create mechanical pressure on the muscle
tissue in order to decrease adhesions in the tissue. Mobilising and elongating
shortened or adhered connective tissue may increase muscle-tendon compliance.
Improved muscle compliance results in a less stiff muscle-tendon unit. These effects
help to restore muscle flexibility and restoring range of motion (Imtiyaz, Veqar,
Shareef (2014).
62
CHAPTER SIX: CONCLUSION AND RECOMMENDATIONS
6.1 CONCLUSION
The aim of this study was to compare the efficacy of ischemic compression with that
of therapeutic massage with a percussive device in the treatment of active hamstring
trigger point pain. The outcome of this study suggested that patients with hamstring
trigger point pain were treated effectively with either, as active trigger points respond
well to both ischemic compression and therapeutic massage with a percussive
device. Both groups showed a reduction in self-reported pain, an increase in pain
pressure threshold and an increase in hamstring extensibility over active hamstring
trigger points.
The results of this study showed that the clinical difference was statistically
insignificant (p<0.05). In conclusion, no treatment intervention was superior to the
other in treating active hamstring trigger points. Statistical results indicate that both
treatment interventions are effective in reducing hamstring pain and increasing the
hamstring extensibility.
This study thus indicated that both ischemic compression and therapeutic massage
with a percussive device were used to treat hamstring trigger point pain effectively
provided that no contraindications were present. In the case of patient being
contraindicated to one treatment intervention, the other is a suitable alternative.
The clinical importance of this study provides the chiropractic profession with two
different treatment interventions to effectively treat patients with hamstring
myofascial trigger point pain. Numerous studies have been done to determine the
effect of chiropractic manipulative therapy on myofascial trigger points, as it is the
profession’s primary treatment intervention. Ischemic compression and therapeutic
massage with a device, however, could serve as an effective post manipulative or
alternative treatment interventions to spinal manipulation. The device-assisted soft
tissue manipulation could also help prevent or reduce fatigue and injuries in manual
therapists.
63
6.2 RECOMMENDATIONS
The following recommendations should be taken into consideration for further
research regarding the treatment of active hamstring myofascial trigger points:
A larger sample size should be used to offer generalisability.
The long-term effects of both treatment interventions can be investigated by
increasing the treatment period or adding a one month follow-up after the
completion of the six treatments.
The effect of a combination of ischemic compression and therapeutic
massage with a percussive massage should be examined in the treatment of
active hamstring myofascial trigger points.
A research study should be done with two sample groups, one receiving a
sacroiliac chiropractic manipulation and ischemic compression, with the other
receiving chiropractic sacroiliac manipulation and therapeutic massage with
a percussive device. Doing so could provide a comparison of chiropractic
manipulation interventions.
An additional objective measurement could be added to assess range of
motion or muscle strength. Doing so could provide more information on the
different physiological effects of the two treatment interventions.
64
REFERENCES Arnau-Masanet, R., Barrios-Pitarque, C., Bosch-Morell, F., Montanez-Aguilera, F.J.,
Pecos-Martin, D. and Valtuena-Gimeno, N., (2010). Changes in a patient with neck
pain after application of ischemic compression as a trigger point therapy. Journal of
Back and Musculoskeletal Rehabilitation, 23(2):101-104.
Aguilera, F.J, Martín, D.P., Masanet, R.A., Botella, A.C., Soler, L.B. and Morell, F.B.,
(2009). Immediate effect of ultrasound and ischemic compression techniques for the
treatment of trapezius latent myofascial trigger points in healthy subjects: a
randomized controlled study. Journal of Manipulative and Physiological
Therapeutics, 32(7): 515-520
Bakhtiary, A. H., Fatemi, E., Khalili, M.A. and Ghorbani, R., (2011). Localized
application of vibration improves passive knee extension in women with apparent
reduced hamstring extensibility: a randomised trial. Journal of Physiotherapy, 57(3):
165-171.
Batavia, M., (2004). Contraindications for therapeutic massage: do sources agree?
Journal of Bodywork and Movement Therapies, 8(1): 48-57.
Behrangrad, S. and Kamali, F., (2017). Comparison of ischemic compression and
lumbopelvic manipulation as trigger point therapy for patellofemoral pain syndrome
in young adults: A double-blind randomized clinical trial. Journal of Body and
Movement Therapies, 21(3): 554-564.
Borg-Stein, J. and Simons, D.G., (2002). Focused review – myofascial pain.
Archives of Physical Medicine and Rehabilitation, 83(3): 40-49.
65
Best, T.M., Crawford, S.K., Haas, C., Charles, L. and Zhao, Y., (2014). Transverse
forces in skeletal muscle with massage-like loading in a rabbit model. BMC
Complementary Alternative Medicine, 14: 393.
Brooks, C.P, Woodruff, L.D., Wright, L.L. and Donatelli, R., (2005). The immediate
effects of manual massage on power-grip performance after maximal exercise in
healthy adults. The Journal of Alternative and Complementary Medicine, 11(6):
1093-1101.
Bron, C. and Dommerholt, J.D., (2012). Etiology of myofascial trigger points. Current
Pain and Headaches Reports, 16(5): 439-444.
Cagnie, B., Dewitte, V., Coppieters, I., Van Oosterwijck, J., Cools, A. and Danneels,
L., (2013). Effect of ischemic compression on trigger points in the neck and shoulder
muscles in office workers: a cohort study. Journal of Manipulative and Physiological
Therapeutics, 36(8): 482-489.
Ching, E.Y., (2007). Myofascial pain – an overview. Annals of Academy of Medicine
Singapore, 36(1): 43-48.
Comeaux, Z., (2011). Dynamic fascial release and the role of mechanical/vibrational
assist devices in manual therapies. Journal of Bodywork and Movement Therapies,
15: 35-41.
Costantino, C., Galuppo, L. and Romiti, D., (2017). Short-term effect of local muscle
vibration treatment versus sham therapy on upper limb in chronic post-stroke
patients: a randomized controlled trial. European Journal of Physical and
Rehabilitation Medicine, 53(1): 32-40.
66
De Las Peñas, C.F., Campo, M.S., Carnero, J.F. and Miangolarra-Page, J.C.,
(2005). Manual therapies in myofascial trigger point treatment: a systemic review.
Journal of Bodywork and Movement Therapies, 9: 27-34.
De Las Peñas, C. F., Alonso-Blanco, P.T., Fernandez-Carnero, C. and Miangolarra-
Page, J.C., (2006). The immediate effect of ischemic compression technique and
transverse friction massage on tenderness of active and latent myofascial trigger
points. Journal of Bodywork and Movement Therapies, 10(1): 3-9.
DeWitt, J. and Vidale, T., (2014). Recurrent hamstring injury: consideration following
operative and non-operative management. The International Journal of Sport
Physical Therapy, 9(6): 798-812.
Dearing, J. and Hamilton, F., (2008). An examination of pressure-pain thresholds
(PPT’s) at myofascial trigger points (MTrP’s), following muscle energy technique or
ischaemic compression treatment. Manual Therapy, 13:87-88.
Desai, S. and Jeswani, K., (2018). To compare the effect of myofascial release and
ischemic compression on pain, cervical lateral flexion and function in acute trapezitis
in young adults. International Journal of Applied research, 4(3): 448-454.
Ebara, S., Furuta, T. and Kumamoto, K. (2017). Vibrissal mechanoreceptors –
Scholarpedia [ONLINE]. Available at:
http://www.scholarpedia.org/article/Vibrissal_mechanoreceptors. [Accessed 05 February
2019.]
Ferreira-Valentea, M.A., Pais-Ribeiroa, J.L. and Jensen, M.P., (2011). Validity of four
pain intensity rating scales. The Journal of the International Association for the Study
of Pain, 152(10): 2399-2404.
67
Field, T., (2016). Massage therapy research review. Complementary Therapies in
Clinical Practice, 20(4): 19-31.
Fischer, A.A., (1986). Pressure threshold meter: its use for quantification of tender
points. Archives of Physical Medicine and Rehabilitation, 67(11): 836-838.
Fleckenstein, J., Zaps, D., Rüger, J.L., Lehmeyer, L., Freiberg, F., Lang, P.M. and
Irnich, D., (2010). Discrepancy between prevalence and perceived effectiveness of
treatment methods in myofascial pain syndrome: results of a cross-sectional,
nationwide survey. BMC Musculoskeletal Disorders, 11: 32.
Frey, L.A., Evans, S., Knudtson, J., Nus, S., Scholl, K. and Sluka, K.A., (2008).
Massage reduces pain perception and hyperalgesia in experimental muscle pain: a
randomized, controlled trial. The Journal of Pain, 19(8): 714-721.
Fritz, S. and Grosenbach, M.J., (2009). Mosby’s Essential Sciences for Therapeutic
Massage: Anatomy, Physiology, Biomechanics, and Pathology, 3rd Edition, St. Louis:
Mosby Elsevier
Fryer, G. and Hodgson, L., (2005). The effect of manual pressure release on
myofascial trigger points in the upper trapezius muscle. Journal of Bodywork and
Movement Therapies, 9(4): 248-255.
Gemmell, H., Miller, P. and Nordstrom, H., (2008). Immediate effect of ischemic
compression and trigger point pressure release on neck pain and upper trapezius
trigger points; a randomised controlled trial. Clinical Chiropractic, 11: 30-36.
Gnat, R., Kuszewski, M., Koczar, R. and Dziewońska, A., (2010). Reliability of the
passive knee flexion and extension tests in healthy subjects. Journal of Manipulative
and Physiological Therapeutics, 33(9): 659-665.
68
Green, L. and Goggins, R.W., (2006). Musculoskeletal Symptoms and Injuries
among Experienced Massage and Bodywork Professionals. Foundations of
Massage, 3rd Edition. Philadelphia: 48-58.
Guyton, A.C. and Hall, J.E., (2015). Textbook of Medical Physiology, 13th Edition,
Philadelphia: Saunders: 71, 73-74, 78, 859-860.
Hains, G., (2002). Chiropractic management of shoulder pain and dysfunction of
myofascial origin using ischemic compression technique. The Journal of the
Canadian Chiropractic Association, 46(3): 192-200.
Hains, G., Descarreaux, M. and Hains, F., (2010). Chronic shoulder pain of
myofascial origin: a randomized clinical trial using ischemic compression therapy.
Journal of Manipulative and Physiological Therapeutics, 33(5): 362-369.
Harden, R.N., Bruehl, S.P., Gass, S., Niemiec, C. and Barbick, B., (2002). Signs and
symptoms of the myofascial pain syndrome: a national survey of pain management
providers. The Clinical Journal of Pain, 16(1): 64-72.
Harrison, D.D. and Sisken, L.A., (2013). Best Practices and Practice Guidelines.
Virginia: International Chiropractic Association: 76-78.
Hou, C.R., Tsai, L.C., Cheng, K.F., Chung, K.C. and Hong, C.Z., (2002). Immediate
effects of various physical therapeutic modalities on cervical myofascial pain and
trigger-point sensitivity. Archives of Physical Medicine and Rehabilitation, 83(10):
1406-1414.
Huang, C., Holfeld, J., Schaden, W., Orgill, D. and Ogawa, R., (2013)
Mechanotherapy: revisiting physical therapy and recruiting mechanobiology for a
new era in medicine. Trends in Molecular Medicine, 19(9): 555-564.
69
Huguenin, L.K., (2004). Myofascial trigger points: the current evidence. Physical
Therapy in Sport, 5: 2-12.
Hunter, D.G. and Speed, C.A., (2007). The assessment and management of chronic
hamstring/posterior thigh pain. Best Practice and Research Clinical Rheumatology,
21(2): 261-277.
Ingbur, R.S., Kostopoulos, P., Larkin, R.W. and Nelson, A.J., (2008). Reduction of
spontaneous electrical activity and pain perception of trigger point in the upper
trapezius muscle through trigger point compression and passive stretching. Journal
of Musculoskeletal Pain, 16(4): 266-278.
Imtiyaz. S, Veqar, Z. and Shareef, M.Y., (2014). To compere the effect of vibration
therapy and massage in prevention of delayed onset muscle soreness (DOMS).
Journal of Clinical and Diagnostic Research, 8(1): 133-136.
Issurin, V.B., (2005). Vibration and their application in sport; a review. The Journal
of Sports Medicine and Physical Fitness, 45(3): 324-336.
Kaergaard, A. and Andersen, J.H., (2002). Musculoskeletal disorder of the neck and
shoulders in female sewing machine operators: prevalence, incidence and
prognosis. Occupational and Environmental Medicine, 57(8): 528-534.
Karacan, I., Cidem, M., Yilmaz, G., Sebik, O., Cakar, H. I. and Türker, K.S., (2016).
Tendon reflex is suppressed during whole-body vibration. Journal of
Electromyography and Kinesiology, 30: 191-195.
Karels, C.H., Polling, W. and Bierma-Zeinstra, S.M.A., (2006). Treatment of arm,
neck and/or shoulder complaints in physical therapy practice. Spine, 31(17): 584-
589.
70
Khan, K.M. and Scott, A., (2009). Mechanotherapy: how physical therapists’
prescription of exercise promotes tissue repair. British Journal of Sport Medicine,
43(4): 247-252.
Kinser, A.M., Sands, W.A. and Stone M.H., (2009). Reliability and validity of a
pressure algometer. Journal of Strength and Conditional Research, 23(1): 312-314.
Kostopoulos, D. and Rizopoulos, K., (2001). The Manual of Trigger Point and
Myofascial Therapy. Slack Incorporated: 20, 21, 22, 63, and 64.
Koulouris, G. and Connell, D., (2005). Hamstring muscle complex; an image review.
RadioGraphics, 25(3): 571-586.
Kristin, E. and White, D.C., (2011). High hamstring tendinopathy in three female long
distance runners. Journal of Chiropractic Medicine, 10(2): 93-99.
Lavelle, E.D., Lavelle, W. and Smith, H.S., (2007). Myofascial trigger points.
Anesthesiology Clinics, 25(4): 841-851.
Loghmani, M.T. and Whitted, M., (2016). Soft tissue manipulation: a powerful form
of mechanotherapy. Journal of Physiotherapy & Physical Rehabilitation, 1(4): 122-
127.
Lucas, K.R., Polus, B. and Rich, P.A., (2003). Latent myofascial trigger points: their
effects on muscle activation and movement efficiency. Journal of Bodywork and
Movement Therapies, 8(3): 160-166.
Macintosh, B.R., Gardiner, P.F. and McComas, A.J., (2006). Skeletal Muscle Form
and Function, 2nd Edition. United States: Human Kinetics: 22.
71
Magee, D.J., Zachazewski, J.E. and Quillen, W.S., (2007). Scientific Foundations
and Principles of Practice in Musculoskeletal Rehabilitation. St Louis: Saunders
Elsevier: 217-231
Martini, F.H., Nath, J.L. and Bartholomew, E.F. (2018). Fundamentals of Anatomy
and Physiology, 11th Edition. San Francisco: Benjamin Cummings: 280-305.
Menakam, P.T. and Kalaichandran, M.O.T., (2015). Effect of ischemic compression
followed by stretching on myofascial trigger points. International Journal of Scientific
Research Publications, 5(1).
Mense, S. and Simons, D.G., (2000). Muscle Pain: Understanding Its Nature,
Diagnosis, and Treatment. Baltimore: Williams and Wilkins: 2-38.
Moore, K.L., Dalley, A.F. and Agur, A.M.R, (2017). Clinical Orientated Anatomy, 8th
Edition. London, New York: Lippincott Williams and Wilkens: 81,759.
Nagrale, A.V., Glynn, P., Joshi, A. and Ramteke, G., (2010). The efficacy of an
integrated neuromuscular inhabitation technique on upper trapezius trigger points in
subjects with non- specific neck pain: a randomized controlled trial. Journal of
Manual and Manipulative Therapy, 18(1): 37-43.
Netter, F.H., (2018). Atlas of Human Anatomy, seventh Edition, Philadelphia, PA:
Saunders/ Elsevier: Plate 482-485.
Nussbaumer, S., Leunig, M., Glatthorn, J., Stauffacher, S., Gerber, H. and Maffiuletti,
N.A., (2010). Validity and test-retest reliability of manual goniometers for measuring
passive hip range of motion in femoroacetabular impingement patients. BMC
Musculoskeletal Disorders, 11: 194.
72
Opar, D.A. and Williams, M.D., (2012). Hamstring strain injuries: factors that lead to
injury and reinjury. Sportmed, 42(3): 209-226.
Perle, S. M., Schneider, M.J. and Seaman, D.R., (1999). Chiropractic management
of peripheral neuropathy: pathophysiology, assessment and treatment. Topics in
Clinical Chiropractic, 6(4): 6-19.
Preedy, V. and Peters, T., (2002). Skeletal Muscle: Pathology, Diagnosis and
Management of Disease. London: Get Media Management (GMM): 3-4.
Prohealthsys, (2019). Pain Scale Goniometer - Prohealthsys [ONLINE]. Available
at: https://prohealthsys.com/shop/clinical-tools/pain-scale-goniometer/. [Accessed 09
February 2019.]
Puri, N.A., Flatow, E.L. and Soslowsky, L.J., (2015). Tendon basic sciences:
development, repair, regeneration, and healing. Journal of Orthopaedic Research,
33(6): 780-784.
Raj, P.P., and Paradise, L.A., (2004). Myofascial pain syndrome and its treatment in
lower back pain. Seminars in Pain Medicine, 4(2): 167-174.
Rickards, L.D., (2006). The effectiveness of non-invasive treatments for active
myofascial trigger point pain: a systemic review of the literature. International Journal
of Osteopathic Medicine, 9(4): 120-136.
Saxena, A., Chansoria, M., Tomar, G. and Kumar, A., (2015). Myofascial pain
syndrome: an overview. Journal of Pain and Palliative Care Pharmacotherapy, 29(1):
16-21.

73
Schillinger, A., Koenig, D., Haefele, C., Vogt, S. and Heinrich, L., (2006). Effect of
manual lymph drainage on the course of serum levels of muscle enzymes after
treadmill exercise. American Journal of Physical Medicine and Rehabilitation, 85(6):
516-520.
Shah, J.P. and Gilliams, E.A., (2008). Uncovering the biochemical milieu of
myofascial trigger points using in vivo microdialysis: an application of muscle pain
concepts to myofascial pain syndrome. Journal of Bodywork and Movement
Therapies, 12(4): 371-384.
Simmonds, N., Miller, P. and Gemmell, H., (2010). A theoretical framework for role
of fascia in manual therapy. Journal of Bodywork and Movement Therapies, 16(1):
83-93.
Simons, D.G., (2002). Understanding effective treatments of myofascial trigger
points. Journal of Bodywork and Movement Therapies, 6(2): 81-88.
Simons, D.G., (2004). Review of enigmatic MTrPs as a common cause of enigmatic
musculoskeletal pain and dysfunction. Journal of Electromyography and
Kinesiology, 14(1): 95-107.
Thumper Massager, (2019). Maxi Pro – Thumper® Massagers - Chiropractic
Massager [ONLINE]. Available at: https://www.thumpermassager.com/massagers/maxi-
pro/. [Accessed 09 February 2019.]
Tough, E.A., White, A.R., Richards, S. and Campbell, J., (2007). Variability of criteria
used to diagnose myofascial trigger point pain syndrome: evidence from a review of
literature. The Clinic Journal of Pain, 23(3): 278-286.
74
Travell, J.G. and Simons, D.G., (1999). Myofascial Pain and Dysfunction: The
Trigger Point Manual. Lippincott Williams and Wilkins: Baltimore. Vol.1: 623-635.
Vecchiet, L., (2002). Muscle pain and aging. Journal of Musculoskeletal Pain, 10(1):
5-22.
Vernon, H. and Schneider, M., (2008). Chiropractic management of myofascial
trigger points and myofascial pain syndrome: a systemic review of the literature.
Journal of Manipulative and Physiological Therapeutics, 32(1): 14-24.
Weerapong, P., Hume, P.A. and Kolt, G.S., (2005). The mechanisms of massage
and effects on performance, muscle recovery and injury prevention. Sports
Medicine, 35(3): 235-256.
Weppler, C.H. and Magnusson, S.P., (2010). Increasing muscle extensibility: a
matter of increasing length or modifying sensation. Physical Therapy, 90(3): 438-
439.
Young, I.A., Cleland, J.A., Michener, L.A. and Brown, C., (2010). Reliability,
construct validity, and responsiveness of the neck disability index, patient-specific
functional scale, and numeric pain rating scale in patients with cervical radiculopathy.
American Journal of Physical Medicine and Rehabilitation, 89(10): 831-839.
75
APPENDIX A: ADVERTISEMENT
Research study Are you between the ages of 18-50? Do you suffer from hamstring pain?
Are you currently not receiving any treatment for your pain?
You may be eligible to participate in my research study, which aims to compare the effects of ischemic compression with therapeutic massage with a percussive
device in treating hamstring pain.
The research will be conducted at the Chiropractic Clinic at the University of Johannesburg Doornfontein Campus.
If you are interested in taking part, please contact: Charlize Jonker
[email protected] 0784707514
Ethics clearance number: REC-241112-035
76
APPENDIX B: INFORMATION LETTER
DEPARTMENT OF CHIROPRACTIC
RESEARCH STUDY INFORMATION LETTER
Good Day,
My name is Charlize Jonker. I WOULD LIKE TO INVITE YOU TO PARTICIPATE in a research study, on ‘The effect of ischemic compression versus therapeutic massage with a percussive device in treating hamstring myofascial pain dysfunction.’
Before you decide on whether to participate, I would like to explain to you why the research is being done and what it will involve for you. I will go through the information letter with you and answer any questions you have. This should take about 10 to 20 minutes. The study is part of a research project being completed as a requirement for a Master’s Degree in Chiropractic through the University of Johannesburg.
THE PURPOSE OF THIS STUDY is to compare the effects of ischemic compression versus therapeutic massage with a percussive device in treating active myofascial hamstring trigger points.
Below, I have compiled a set of questions and answers that I believe will assist you in understanding the relevant details of participation in this research study. Please read through these. If you have any further questions I will be happy to answer them for you.
DO I HAVE TO TAKE PART? No, you don’t have to. It is up to you to decide to participate in the study. I will describe the study and go through this information sheet. If you agree to take part, I will then ask you to sign a consent form.
77
WHAT EXACTLY WILL I BE EXPECTED TO DO IF I AGREE TO PARTICIPATE? You must be between ages of 18-50, with localised pain that is concentrated in the hamstring region. You will not be included in to the study if you have any of the following: trauma or surgeries to the region, tumors or infection, or a rupture of any of the hamstring muscle. If you qualify to participate in this study, you would not be able to participate in any other research studies during this time nor take any medications that may influence the outcomes of this study. Not all medications may be a problem, so please be open with me regarding any medication or supplements you are using. Also, please be open with me regarding your health history, since you may otherwise harm yourself by participating in this study.
You will be allocated to one of two groups consisting of 15 participants. You will then be assigned to your group by drawing a number from a hat. The hat will contain 30 pieces of paper labelled A or B (representing the group numbers). The number you draw is the group you will be allocated to. Group A will only receive treatment in the form of ischemic compression on hamstring myofascial trigger points, meaning the researcher will apply localised pressure on the hamstring muscle trigger point. Group B will receive a therapeutic massage with a device that vibrates on the hamstring muscle.
A case history, physical examination and a lower back examination will be performed. A series of tests will be gathered for data collection. The first test is a Numerical Pain Rating Scale. You will be asked to rate your pain on a scale of 0 to 10, i.e. from no pain and to the worse pain you have ever experienced. Thereafter the researcher will locate a trigger point that reproduces the pain on the hamstring region. The researcher will the preform a test with a pressure algometer to record your pain threshold. Thereafter you will be positioned on your back with your knee and your hip bend to 90 degrees. The researcher will use a baseline goniometer to measure the popliteal angle, e.g. you will try to straighten your leg as far as possible and the researcher will measure the angel of your knee.
Thereafter you will be treated for the duration of 60 seconds. You will be treated over a three-week period, twice per week, and the seventh visit will be for data collection only.
WHAT WILL HAPPEN IF I WANT TO WITHDRAW FROM THE STUDY? If you decide to participate, you are free to withdraw your consent at any time without giving a reason and without any consequences. If you wish to withdraw your consent, you must please inform me as soon as possible.
IF I CHOOSE TO PARTICIPATE, WILL THERE BE ANY EXPENSES FOR ME, OR PAYMENT DUE TO ME? You will not be paid to participate in this study and you will not bear any expenses either.
78
RISKS INVOLVED IN PARTICIPATION: Ischemic compression and therapeutic massage with a vibrating device are not harmful to the participant. The massage device may cause some itching or a warm sensation due to the increasing blood flow to the area. You might also have slight discomfort over the trigger point, which is completely normal. With the ischemic compression group, you might have a slight discomfort when the pressure is applied on the point of pain. You might a small bruise but the chances of bruising are minimal.
BENEFITS INVOLVED IN PARTICIPATION: Therapeutic massage with a vibrating device is aimed at decreasing muscle spasm and pain, increasing the blood flow to the area, which will stimulate healing and improve the function of the muscle. During ischemic compression the researcher will apply pressure to the myofascial trigger point causing hypoxia (decrease of blood flow) to the trigger point. The pressure will be released after 60 seconds, causing an influx of blood to stimulate healing.
WILL MY PARTICIPATION IN THIS STUDY BE KEPT CONFIDENTIAL? Yes. Names on the data sheet will be removed once analysis starts. All data and back-ups thereof will be kept in password-protected folders and/or locked away as applicable. Only I or my research supervisor will be authorised to use and/or disclose your anonymised information in connection with this research study. Any other person wishing to work with you anonymised information as part of the research process (e.g. an independent data coder) will be required to sign a confidentiality agreement before being allowed to do so.
OR
WILL MY TAKING PART IN THIS STUDY BE ANONYMOUS? Yes. Anonymous means that your personal details will not be recorded anywhere by me. As a result, it will not be possible for me or anyone else to identify your responses once these have been submitted.
WHAT WILL HAPPEN TO THE RESULTS OF THE RESEARCH STUDY? The results will be written into a research report that will be assessed. In some cases, results may also be published in a scientific journal. In either case, you will not be identifiable in any documents, reports or publications. You will be given access to the study results if you would like to see them, by contacting me.
WHO IS ORGANISING AND FUNDING THE STUDY? The study is being organised by me, under the guidance of my research supervisor at the Department of Chiropractic in the University of Johannesburg. All funding for the study will be provided by the supervisor-linked bursary.
WHO HAS REVIEWED AND APPROVED THIS STUDY? Before this study was allowed to start, it was reviewed in order to protect your interests. This review was
79
done first by the Department of Chiropractic, and then by the Faculty of Health Sciences Research Ethics Committee at the University of Johannesburg. In both cases, the study was approved.
WHAT IF THERE IS A PROBLEM? If you have any concerns or complaints about this research study, its procedures or risks and benefits, you should ask me. You should contact me at any time if you feel you have any concerns about being a part of this study. My contact details are:
Charlizé Jonker 078 470 7514 [email protected]
You may also contact my research supervisor:
Dr Chris Yelverton [email protected]
If you feel that any questions or complaints regarding your participation in this study have not been dealt with adequately, you may contact the Chairperson of the Faculty of Health Sciences Research Ethics Committee at the University of Johannesburg:
Prof. Christopher Stein Tel: 011 559-6564 Email: [email protected] FURTHER INFORMATION AND CONTACT DETAILS: Should you wish to have more specific information about this research project information, or have any questions, concerns or complaints about this research study, its procedures, risks and benefits, you should communicate with me using any of the contact details given above.
Researcher:
_______________________
Charlizé Jonker
80
APPENDIX C: CONSENT FORM
DEPARTMENT OF CHIROPRACTIC
RESEARCH CONSENT FORM
The effects of ischemic compression versus therapeutic massage with a percussive device in treating hamstring myofascial pain dysfunction
Please initial each box below:
I confirm that I have read and understand the information letter dated 19/07/2016 for the above study. I have had the opportunity to consider the information and ask questions, and have had these answered satisfactorily.
I understand that my participation is voluntary and that I am free to withdraw from this study at any time without giving any reason and without any consequences to me.
I agree to take part in the above study.
_______________________ _________________________ ________________
Name of Participant Signature of Participant Date
_______________________ _________________________ ________________
Name of Researcher Signature of Researcher Date
81
APPENDIX D: CASE HISTORY
82
83
84
85
APPENDIX E: PHYSICAL EXAMINATION
86
87
88

89
90
APPENDIX F: LUMBAR SPINE REGIONAL
91
92
93
APPENDIX G: NUMERICAL PAIN RATING SCALE Visit 1: Patient Instructions
Please indicate the intensity of current, best, and worst pain levels over the past 24
hours on a Scale of 0 (no pain) to 10 (worst pain imaginable) |______|______|______|______|______|______|______|______|______|______|
0 1 2 3 4 5 6 7 8 9 10
No pain Mild Pain Moderate Pain Worst
Visit 4: Patient Instructions
Please indicate the intensity of current, best, and worst pain levels over the past 24
hours on a Scale of 0 (no pain) to 10 (worst pain imaginable) |______|______|______|______|______|______|______|______|______|______|
0 1 2 3 4 5 6 7 8 9 10
No pain Mild Pain Moderate Pain Worst
Visit 7 Patient Instructions
Please indicate the intensity of current, best, and worst pain levels over the past 24
hours on a Scale of 0 (no pain) to 10 (worst pain imaginable) |______|______|______|______|______|______|______|______|______|______|
0 1 2 3 4 5 6 7 8 9 10
No pain Mild Pain Moderate Pain Worst
94
APPENDIX H: HAMSTRING TRIGGER POINT EXAMINATION
File Number:
Date:
L R
Spot Tenderness: Yes / No
Referred Pain: Yes / No
Where:

95
APPENDIX I: PRESSURE ALGOMETER AND GONIOMETER READINGS
Research file number:
Hamstring muscle trigger point:
Readings Date Algometer (kg/cm²)
Goniometer Degrees
Visit 1
Visit 4
Visit 7
96
APPENDIX J: LETTER OF REQUEST
To the division for institutional planning, evaluation and monitoring management, I would like to ask permission to perform my research on the University of Johannesburg Doornfontein Campus. The research will take place at the Chiropractic Clinic with possible involvement of students studying on this campus. The study is titled ‘The effect of ischemic compression versus therapeutic massage with a percussive device on hamstring myofascial pain dysfunction.’ Thirty participants will be involved in twice-a-week consultation for three weeks.
This study has been approved by the University of Johannesburg’s Ethics
Committee. Ethics clearance number: REC-241112-035 Kind Regards Charlize Jonker Master’s Student 078 470 7514
97
APPENDIX K: ETHICS CLEARANCE LETTER
98
APPENDIX L : HIGHER DEGREES LETTER

99
APPENDIX M: SIMILARITY REPORT
100
APPENDIX N: EDITOR’S LETTER
22/02/2019
To whom it may concern,
This letter serves to confirm that the attached dissertation, “The effects of ischemic
compression versus therapeutic massage with a percussive device in treating hamstring
myofascial pain dysfunction”, has been edited by a qualified language practitioner. For
further verification, I may be contacted by email: [email protected] or by phone:
0616150292.
Kind regards,
Kelly-Anne Gilbertson
BA (Hons, Cum laude), MA (Cum laude), PhD
Related Documents











