C 2008, the Authors Journal compilation C 2008, Blackwell Publishing, Inc. DOI: 10.1111/j.1540-8175.2007.00579.x The Effect of Isolated Left Bundle Branch Block on the Myocardial Velocities and Myocardial Performance Index Mehmet Akif Duzenli, M.D., Kurtulus Ozdemir, M.D., Ahmet Soylu, M.D., Nazif Aygul, M.D., Mehmet Yazici, M.D., and Mehmet Tokac, M.D. Department of Cardiology, Faculty of Medicine, Selcuk University, Konya, Turkey Objectives: This study was planned in order to investigate the effect of left bundle branch block (LBBB) on myocardial velocities obtained by tissue Doppler echocardiography (TDE) and myocardial per- formance index (MPI). Methods: Subjects with LBBB (n = 61) and age-matched healthy subjects (n = 60) were enrolled in the study. Left ventricular (LV) ejection fraction (EF), mitral inflow veloci- ties (E-wave and A-wave), isovolumetric contraction and relaxation time (ICT and IRT), ejection time (ET), and flow propagation velocity (Vp) were measured by conventional echocardiography. Systolic velocity (Sm), early and late diastolic velocities (Em and Am) and time intervals were measured by TDE. MPI was calculated by the formula (ICT + IRT)/ET. Results: LVEF and mitral E/A ratio were similar in both groups. Vp was lower in the LBBB group than in the control group, whereas the E/Em and the E/Vp ratio was higher. LV Sm and Em/Am ratio were lower in LBBB group. Right ventricular Sm and Em/Am ratio were similar in both groups. LV mean and RV MPI were significantly increased in LBBB group. Conclusion: These findings obtained by TDE show that iso- lated LBBB impairs the ventricular functions. Both of the LV and RV dysfunctions shown by the new parameters may contribute to increased morbidity and mortality in cases with isolated LBBB. (ECHOCARDIOGRAPHY, Volume 25, March 2008) left bundle branch block, tissue Doppler echocardiography, myocardial performance index, myocardial velocity, cardiac function Left bundle branch block (LBBB) is an elec- trical conduction disturbance found both in healthy individuals 1–3 and in patients with structural heart diseases. 4,5 Cardiovascular mortality is known to be increased in patients with LBBB and structural heart diseases. 6–8 Moreover, epidemiologic studies have demon- strated that cardiovascular diseases and mor- tality risk are increased in apparently healthy individuals with isolated LBBB. 1,3 Left bundle branch block delays mechanical activation of the left ventricle, leading to inter- ventricular asynchrony and causes impairment of the left ventricular (LV) systolic and diastolic functions. Data exist as to how this impairment affects conventional echocardiography param- eters. Tissue Doppler echocardiography (TDE) Address for correspondence and reprint requests: Mehmet Akif Duzenli, Havzan mah.Beyzade evleri 21 blok da:12, 42080 Meram/Konya/Turkey. Fax: +90 332 323 2641; E- mail: [email protected] is a recent technique that allows better assess- ment of regional and global LV functions by the quantification of myocardial velocities. On the other hand, the myocardial performance index (MPI), which provides information about com- bined systolic and diastolic functions, is cur- rently being investigated from the point of view of its relation to heart diseases. Myocardial ve- locities and MPI have been demonstrated to be determining parameters in both the diagnosis and prognosis of various cardiac diseases. 9–14 The effects of isolated LBBB on myocardial ve- locities and ventricular MPI have not been ade- quately evaluated. Therefore, demonstration of the effect of LBBB on these parameters provid- ing the opportunity of further detailed assess- ment of ventricular function compared to con- ventional electrocardiographic parameters may shed light on the negative effects of LBBB on prognosis. This study has been planned in order to investigate the effects of isolated LBBB on 256 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 25, No. 3, 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

C© 2008, the AuthorsJournal compilation C© 2008, Blackwell Publishing, Inc.DOI: 10.1111/j.1540-8175.2007.00579.x
The Effect of Isolated Left Bundle Branch Blockon the Myocardial Velocities and MyocardialPerformance IndexMehmet Akif Duzenli, M.D., Kurtulus Ozdemir, M.D., Ahmet Soylu, M.D., Nazif Aygul, M.D.,Mehmet Yazici, M.D., and Mehmet Tokac, M.D.
Department of Cardiology, Faculty of Medicine, Selcuk University, Konya, Turkey
Objectives: This study was planned in order to investigate the effect of left bundle branch block (LBBB)on myocardial velocities obtained by tissue Doppler echocardiography (TDE) and myocardial per-formance index (MPI). Methods: Subjects with LBBB (n = 61) and age-matched healthy subjects(n = 60) were enrolled in the study. Left ventricular (LV) ejection fraction (EF), mitral inflow veloci-ties (E-wave and A-wave), isovolumetric contraction and relaxation time (ICT and IRT), ejection time(ET), and flow propagation velocity (Vp) were measured by conventional echocardiography. Systolicvelocity (Sm), early and late diastolic velocities (Em and Am) and time intervals were measured byTDE. MPI was calculated by the formula (ICT + IRT)/ET. Results: LVEF and mitral E/A ratiowere similar in both groups. Vp was lower in the LBBB group than in the control group, whereasthe E/Em and the E/Vp ratio was higher. LV Sm and Em/Am ratio were lower in LBBB group.Right ventricular Sm and Em/Am ratio were similar in both groups. LV mean and RV MPI weresignificantly increased in LBBB group. Conclusion: These findings obtained by TDE show that iso-lated LBBB impairs the ventricular functions. Both of the LV and RV dysfunctions shown by thenew parameters may contribute to increased morbidity and mortality in cases with isolated LBBB.(ECHOCARDIOGRAPHY, Volume 25, March 2008)
left bundle branch block, tissue Doppler echocardiography, myocardial performance index,myocardial velocity, cardiac function
Left bundle branch block (LBBB) is an elec-trical conduction disturbance found both inhealthy individuals1–3 and in patients withstructural heart diseases.4,5 Cardiovascularmortality is known to be increased in patientswith LBBB and structural heart diseases.6–8
Moreover, epidemiologic studies have demon-strated that cardiovascular diseases and mor-tality risk are increased in apparently healthyindividuals with isolated LBBB.1,3
Left bundle branch block delays mechanicalactivation of the left ventricle, leading to inter-ventricular asynchrony and causes impairmentof the left ventricular (LV) systolic and diastolicfunctions. Data exist as to how this impairmentaffects conventional echocardiography param-eters. Tissue Doppler echocardiography (TDE)
Address for correspondence and reprint requests: MehmetAkif Duzenli, Havzan mah.Beyzade evleri 21 blok da:12,42080 Meram/Konya/Turkey. Fax: +90 332 323 2641; E-mail: [email protected]
is a recent technique that allows better assess-ment of regional and global LV functions by thequantification of myocardial velocities. On theother hand, the myocardial performance index(MPI), which provides information about com-bined systolic and diastolic functions, is cur-rently being investigated from the point of viewof its relation to heart diseases. Myocardial ve-locities and MPI have been demonstrated to bedetermining parameters in both the diagnosisand prognosis of various cardiac diseases.9–14
The effects of isolated LBBB on myocardial ve-locities and ventricular MPI have not been ade-quately evaluated. Therefore, demonstration ofthe effect of LBBB on these parameters provid-ing the opportunity of further detailed assess-ment of ventricular function compared to con-ventional electrocardiographic parameters mayshed light on the negative effects of LBBB onprognosis.
This study has been planned in order toinvestigate the effects of isolated LBBB on
256 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 25, No. 3, 2008

ISOLATED LEFT BUNDLE BRANCH BLOCK AND CARDIAC FUNCTIONS
myocardial velocities and the ventricular MPI,which together provide more quantitative dataon regional and global ventricular functionsthan conventional echocardiography parame-ters.
Material and Methods
Patient Population
The subject cases were selected from the pa-tients who were referred to coronary angiog-raphy due to atypical complaints between theyears 1998 and 2006 and whose angiographyresults were normal. LBBB was defined ac-cording to standard electrocardiography crite-ria, as QRS duration greater than 120 ms, ab-sence of initial septal Q-waves and presence ofwide-notched R-waves on derivations V5 andV6, presence of mono phasic QS on derivationsV1 and V2, and absence of the secondary R.Sixty-one individuals with LBBB and 60 pa-tients with sinus rhythm were matched by age,sex, heart rate, hypertension, and body massindex. Patients with <55% ejection fraction,abnormal wall motion on the echocardiogra-phy (apart from the septum in LBBB group),>55 mm LV end-diastolic diameter, >40 mmLV end-systolic diameter, previous myocardialinfarction, cardiomyopathy, moderate or severevalvular diseases or congenital heart diseases,Hb <12 mg/dl, thyroid diseases, and those withliver and renal failure were excluded from thestudy.
Echocardiographic Evaluation
All echocardiographic examinations wereperformed after 20–30 minutes of rest, withthe patient in the partial left decubitus posi-tion, and in quiet respiration using the ATL5000 echocardiography machine with a 2–4 MHz transducer and with simultaneous elec-trocardiography recording. Echocardiographicparameters were measured according to theAmerican Society of Echocardiography criteria,as summarized elsewhere by Pearlman et al.15
Average of measurements obtained from fiveconsecutive beats were taken for all parame-ters.
The M-mode echocardiographic study of theleft ventricle was performed under a two-dimensional (2D) control. Left ventricular end-diastolic diameter, end-systolic diameter, andthe thickness of intraventricular septum andposterior wall at end-diastole were measured,
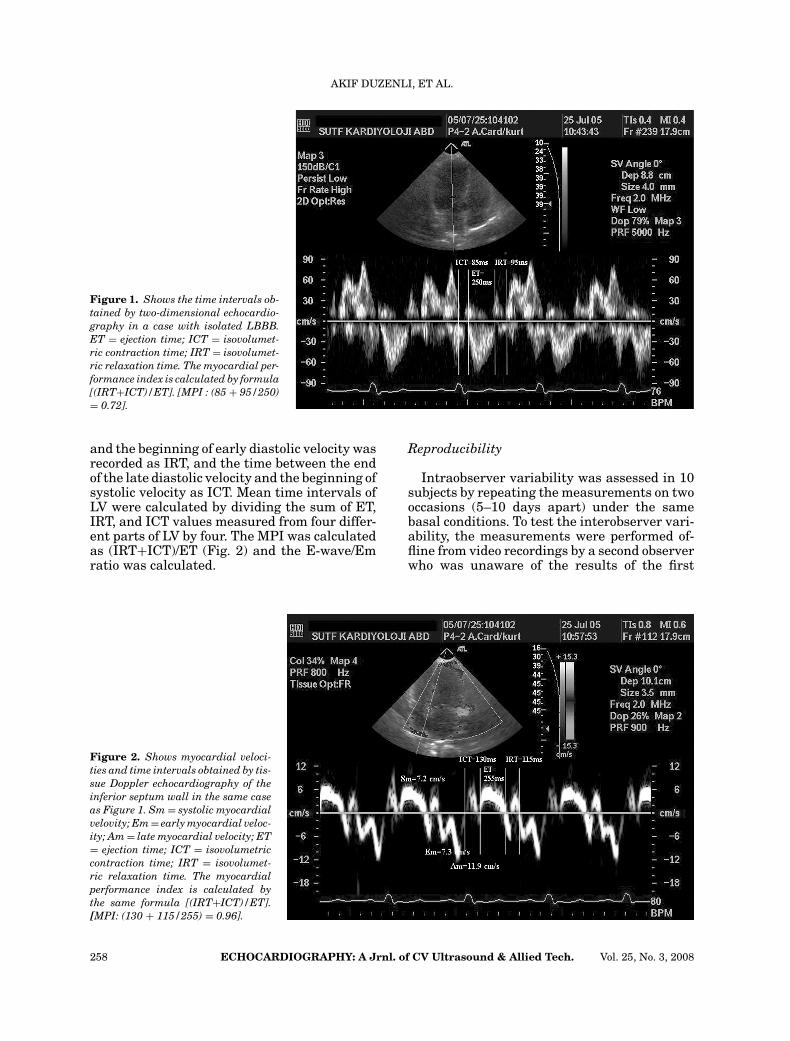
and ejection fraction was calculated by usingthe Teichholz method.16 Mitral inflow velocitieswere recorded at a sweep speed of 100 mm/sfrom the apical four-chamber view, by placingthe pulsed-wave Doppler sample volume at thetips of mitral leaflets. Rapid filling peak flowvelocity (E-wave) and the peak atrial filling ve-locity (A-wave) were measured, and E/A ratiowas calculated. Diastolic period (DP) was mea-sured at intervals between the beginning of theE-wave and the end of the A-wave. Ejection time(ET) was measured as the interval between thebeginning and the end of the ejection period byrecording blood flow velocity of LV outflow tract.Then the LV outflow tract and the mitral bloodflow velocities were recorded simultaneously inapical five-chamber view. The time between theend of ET and the beginning of mitral inflowvelocity was recorded as isovolumetric relax-ation time (IRT), and the time between the endof the mitral A-wave and the beginning of ETwas recorded as isovolumetric contraction time(ICT). The MPI was calculated by the followingformula: (IRT+ICT)/ET (Fig. 1).
Subsequently, from the apical four-chamberview, the color M-mode flow propagation ve-locity (Vp; centimeters per second) was mea-sured as the slope of the first aliasing veloc-ity during early filling, according to Garcia’smethod.17 The mitral E-wave/Vp ratio was cal-culated as an additional index of the LV fillingpressure.
Pulsed-wave TDE was performed by activat-ing the TDE function in the same echocardio-graphic system. The filter settings were keptlow (50 Hz), and gains were adjusted at the min-imal optimal level to minimize noise and elim-inate the signals produced by the transmitralflow. A sample volume of 3.5-mm was used. Inthe apical four-chamber view the TDE cursorwas placed at the septal and lateral side of themitral annulus and right ventricular (RV) freewall side of the tricuspid annulus in such a waythat the annulus moved along the sample vol-ume line. In the apical two-chamber view, theTDE cursor was placed at the anterior and in-ferior side of the mitral annulus in the samemanner. A Doppler velocity range of −20 to20 cm/s was selected for this study. Systolicmyocardial velocity (Sm), early myocardial ve-locity (Em), and late myocardial velocity (Am)were measured at each segment, and Em/Amratio was calculated for each. The systolic ve-locity duration was measured as ET, whereasthe time between the end of the systolic velocity
Vol. 25, No. 3, 2008 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 257
AKIF DUZENLI, ET AL.
Figure 1. Shows the time intervals ob-tained by two-dimensional echocardio-graphy in a case with isolated LBBB.ET = ejection time; ICT = isovolumet-ric contraction time; IRT = isovolumet-ric relaxation time. The myocardial per-formance index is calculated by formula[(IRT+ICT)/ET]. [MPI : (85 + 95/250)= 0.72].
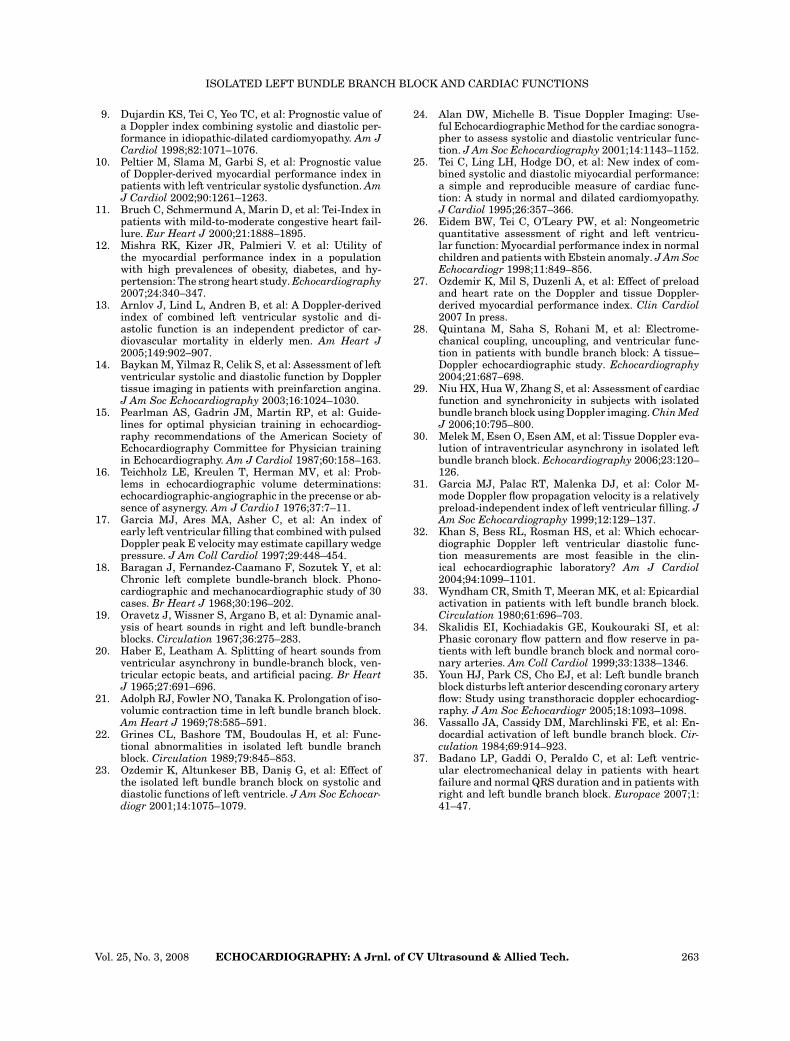
and the beginning of early diastolic velocity wasrecorded as IRT, and the time between the endof the late diastolic velocity and the beginning ofsystolic velocity as ICT. Mean time intervals ofLV were calculated by dividing the sum of ET,IRT, and ICT values measured from four differ-ent parts of LV by four. The MPI was calculatedas (IRT+ICT)/ET (Fig. 2) and the E-wave/Emratio was calculated.
Figure 2. Shows myocardial veloci-ties and time intervals obtained by tis-sue Doppler echocardiography of theinferior septum wall in the same caseas Figure 1. Sm = systolic myocardialvelovity; Em = early myocardial veloc-ity; Am = late myocardial velocity; ET= ejection time; ICT = isovolumetriccontraction time; IRT = isovolumet-ric relaxation time. The myocardialperformance index is calculated bythe same formula [(IRT+ICT)/ET].[MPI: (130 + 115/255) = 0.96].
Reproducibility
Intraobserver variability was assessed in 10subjects by repeating the measurements on twooccasions (5–10 days apart) under the samebasal conditions. To test the interobserver vari-ability, the measurements were performed of-fline from video recordings by a second observerwho was unaware of the results of the first
258 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 25, No. 3, 2008

ISOLATED LEFT BUNDLE BRANCH BLOCK AND CARDIAC FUNCTIONS
examination. Variability was calculated as themean percentage error, derived as the differ-ence between the two sets of measurements, di-vided by the mean observations.
Statistics
All statistics were calculated by the SPSSsoftware 11.0 for Windows (SPSS. Inc., Chicago,IL, USA). Descriptive data were expressed asa mean value ± SD. Comparisons between thegroups of parametric values were tested by stu-dent’s t test. chi-square test was used for thecomparison of nonparametric values. A valueof P < 0.05 was considered significant.
Results
Age, body mass index, heart rate, and bloodpressure were similar in both groups (Table I).
M-Mode and Mitral Flow PW DopplerParameters
Left ventricular EF, LV interventricular sep-tum and posterior wall thickness, aortic and leftatrial diameter, and LV end-diastolic diameterwere found to be similar in both groups. On theother hand, LV end-systolic diameter was foundto be higher in the LBBB group in comparisonto the control group (Table II). The mitral E-and A-wave velocities were found to be simi-lar in both groups. Although the mitral E/A ra-tio of the LBBB group was lower in relation tothe control group, this difference was statisti-cally insignificant. While the LV ICT and IRTwere longer in LBBB group than in the controlgroup (P < 0.01, P < 0.05, respectively), the DP
TABLE I
Demographic and Clinical Characteristics of Subjects in
LBBB and Groups
LBBB Control P-value
Age (year) 55 ± 13 56 ± 12 NS
Heart rate (beats/min) 75 ± 12 72 ± 11 NS
Sex (Male/Female) 30/31 31/28 NS
Body-mass index (kg/m2) 27 ± 5.6 27 ± 4.6 NS
Systolic blood pressure 130 ± 16 132 ± 15 NS
(mmHg)
Diastolic blood pressure 80 ± 11 79 ± 12 NS
(mmHg)
Hypertension 7 7 NS
Diabetes mellitus 3 3 NS
NS = not significant.
TABLE II
Two-Dimensional M-mode Echocardiography Parameters
in LBBB and Control Groups
LBBB Control P-value
End-diastolic diameter 4.8 ± 0.5 4.6 ± 0.4 NS
(mm)
End-systolic diameter 3.1 ± 0.4 2.9 ± 0.3 = 0.01
(mm)
Interventricular septum 9.1 ± 1.5 8.9 ± 1.3 NS
(mm)
Posterior wall (mm) 8.7 ± 1.3 8.4 ± 1.3 NS
LV Ejection fraction (%) 63 ± 6 64 ± 9 NS
Left atrial diameter (cm) 3.6 ± 0.4 3.5 ± 0.4 NS
Aortic diameter (cm) 2.8 ± 0.4 2.7 ± 0.4 NS
NS = not significant.
and ET were shorter (P < 0.05, P < 0.01, re-spectively). The LV MPI was found to be signifi-cantly high in the LBBB group (P < 0.001). TheVp was lower in the LBBB group than in thecontrol group (P < 0.01), whereas the E/Vp andE/Em ratios were higher (P < 0.005 for each)(Table III).
TDE Parameters
LV inferior septum, lateral and inferior walls,and LV mean Sm values were found to be lowerin the LBBB group than those in the control
TABLE III
Doppler Indexes of Left Ventricular Filling and Time
Intervals Obtained by Conventional Echocardigraphy in
LBBB and Control Groups
LBBB Control P-value
E-wave (m/s) 0.65 ± 0.20 0.65 ± 0.15 NS
A-wave (m/s) 0.79 ± 0.19 0.73 ± 0.18 NS
E/A 0.86 ± 0.30 0.94 ± 0.30 NS
Vp (ms) 0.44 ± 0.12 0.65 ± 0.25 <0.01
E/Vp 1.74 ± 0.24 1.10 ± 0.40 <0.005
DP (ms) 377 ± 98 422 ± 114 <0.05
IRT (ms) 105 ± 47 88 ± 26 <0.05
ICT (ms) 79 ± 38 40 ± 27 <0.01
ET (ms) 273 ± 32 286 ± 22 <0.01
MPI (%) 68 ± 17 45 ± 10 <0.001
E/Em 7.9 ± 3.2 6.5 ± 1.7 <0.005
A-wave = peak atrial velocity; DP = diastolic period;E-wave = peak early diastolic velocity; EDT = E-wavedeceleration time; ET = ejection time; ICT = isovolumetriccontraction time; IRT = isovolumetric relaxation time;MPI = myocardial performance index; NS = not significant,Vp = flow propagation velocity.
Vol. 25, No. 3, 2008 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 259

AKIF DUZENLI, ET AL.
TABLE IV
Tissue Doppler Echocardiography Parameters in LBBB
and Control Groups
LBBB Control P-value
Anterior
Sm (cm/s) 9.7 ± 2.2 10.2 ± 2.0 NS
Em (cm/s) 9.7 ± 3.2 10.9 ± 2.8 <0.05
Am (cm/s) 12.6 ± 2.7 12.6 ± 3.1 NS
Em/Am 0.80 ± 0.32 0.90 ± 0.29 NS
Inferior
Sm (cm/s) 8.3 ± 1.9 9.4 ± 1.4 <0.001
Em (cm/s) 7.5 ± 2.6 9.9 ± 2.3 <0.001
Am (cm/s) 12.0 ± 2.6 12.3 ± 2.3 NS
Em/Am 0.64 ± 0.24 0.84 ± 0.24 <0.001
Lateral
Sm (cm/s) 9.5 ± 1.9 10.5 ± 2.0 <0.01
Em (cm/s) 9.9 ± 2.8 11.2 ± 2.6 <0.01
Am (cm/s) 12.6 ± 2.6 11.8 ± 2.7 NS
Em/Am 0.83 ± 0.35 1.02 ± 0.44 = 0.01
Inferior septum
Sm (cm/s) 7.9 ± 1.7 8.9 ± 1.7 = 0.01
Em (cm/s) 7.2 ± 2.2 8.8 ± 2.5 <0.001
Am (cm/s) 11.1 ± 2.2 11.1 ± 2.2 NS
Em/Am 0.67 ± 0.23 0.81 ± 0.26 = 0.02
LV mean
Sm (cm/s) 8.8 ± 1.4 9.8 ± 1.4 = 0.01
Em (cm/s) 8.6 ± 2.3 10.2 ± 2.1 <0.01
Am (cm/s) 12.1 ± 2.0 11.9 ± 1.8 NS
Em/Am 0.73 ± 0.23 0.88 ± 0.25 = 0.01
RV
Sm (cm/s) 15.2 ± 3.1 14.9 ± 2.5 NS
Em (cm/s) 12.6 ± 3.4 0 12.5 ± 2.4 NS
Am (cm/s) 17.7 ± 4.6 16.7 ± 3.2 NS
Em/Am 0.75 ± 0.28 0.77 ± 0.22 NS
Am = late myocardial velocity; Em = early myocardialvelocity; LV = left ventricular; NS = not significant; RV =right ventricular; Sm = systolic myocardial velocity.
group. However, LV anterior Sm value wassimilar in both groups. LV regional and globalEm values were found to be significantly lowerin the LBBB group than in the control group.On the other hand, LV regional and global Amvalues were similar in both groups. No differ-ence was established between both groups con-cerning the RV Sm, Em, and Am. The Em/Amratio of LV inferior septum, lateral, and inferiorwalls and LV mean Em/Am values were foundto be lower in the LBBB group than those of thecontrol group. However, the Em/Am ratio of LVanterior wall and RV Em/Am ratio were similarin both groups (Table IV).
LV regional and mean ICT and IRT werefound to be significantly longer in the LBBBgroup than those in the control group. The ET
TABLE V
Time Intervals and Myocardial Performance Index
Obtained by Doppler Tissue Echocardiography in LBBB
and Control Groups
LBBB Control P-value
Anterior
ICT (ms) 103 ± 28 73 ± 25 <0.001
IRT (ms) 109 ± 28 81 ± 18 <0.001
ET (ms) 275 ± 28 283 ± 24 NS
MPI (%) 78 ± 20 59 ± 34 <0.001
Inferior
ICT (ms) 117 ± 28 66 ± 16 <0.001
IRT (ms) 121 ± 33 81 ± 19 <0.001
ET (ms) 256 ± 29 285 ± 29 <0.001
MPI (%) 95 ± 24 52 ± 11 <0.001
Lateral
ICT (ms) 108 ± 30 76 ± 27 <0.001
IRT (ms) 103 ± 29 76 ± 19 <0.001
ET (ms) 273 ± 33 279 ± 25 NS
MPI (%) 79 ± 22 55 ± 14 <0.001
Inferior septum
ICT (ms) 108 ± 26 68 ± 16 <0.001
IRT (ms) 123 ± 30 89 ± 18 <0.001
ET (ms) 256 ± 28 281 ± 22 <0.001
MPI (%) 92 ± 20 56 ± 10 <0.001
LV mean
ICT (ms) 109 ± 23 70 ± 18 <0.001
IRT (ms) 114 ± 26 86 ± 26 <0.001
ET (ms) 265 ± 26 281 ± 22 = 0.001
MPI (%) 85 ± 18 55 ± 13 <0.001
RV
ICT (ms) 77 ± 27 60 ± 14 <0.001
IRT (ms) 78 ± 34 72 ± 27 NS
ET (ms) 276 ± 35 285 ± 29 NS
MPI (%) 57 ± 22 48 ± 13 <0.005
ET = ejection time; ICT = Isovolumetric contractiontime; IRT = isovolumetric relaxation time; LV = leftventricular; MPI = myocardial performance index; NS =not significant; RV = right ventricular.
of LV inferior and inferior septum walls andLV mean ET were shorter in the LBBB groupthan in the control group. However, LV ante-rior and lateral wall ET values were similar inboth groups. RV ICT was found to be longer inthe LBBB group than that in the control group,whereas the IRT and ET values were similar.The LV regional and global MPI and the RVMPI values were higher in the LBBB group(Table V).
In the isolated LBBB group, the meanQRS duration was 141 ± 12.1 msec and itwas weakly-moderately correlated with E/Em,E/Vp, TDE-MPI, LV mean Sm, and LV meanEm/Am. (r = 0.40, P < 0.05; r = 0.36, P < 0.05;
260 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 25, No. 3, 2008

ISOLATED LEFT BUNDLE BRANCH BLOCK AND CARDIAC FUNCTIONS
r = 0.42, P < 0.01; r = −0.34, P < 0.05; r =−0.48, P = 0.01; respectively).
Reproducibility
Intraobserver and interobserver variabilityfor myocardial velocities (Sm, Em, and Am)ranged from 2.7% to 6.1%. Intraobserver vari-ability for conventional MPI was 3.7% ± 2.6%while interobserver variability was 3.9% ±2.9%. Intraobserver variability for MPI by TDEwas 3.6% ± 1.9% while interobserver variabil-ity was 4.9% ± 3.1%.
Discussion
In this study, it was demonstrated that globaland regional Sm and Em/Am ratio, except forthose of the anterior wall, of LV were signifi-cantly lower in cases with isolated LBBB thanthose in the control group. However, isolatedLBBB did not affect RV myocardial velocities.In addition, LV and RV MPI were higher incases with isolated LBBB.
In patients with LBBB, the systolic and dias-tolic functions, together with ventricular hemo-dynamics, were evaluated by the use of differ-ent techniques in previous studies including asmall number of patients.18–23 Myocardial ve-locities and MPI are new noninvasive param-eters that provide more quantitative informa-tion about systolic and diastolic functions thanthe standard parameters. While myocardial ve-locities are obtained by TDE, ventricular MPIare calculated by 2D Doppler echocardiographyor TDE. These parameters are not affected byventricular geometric shape and are relativelyindependent of the heart rate and blood pres-sure.24–26 Also it has been demonstrated thatespecially the MPI obtained by TDE does notdepend on preload27and that these parametershave diagnostic and prognostic reliability invarious cardiac diseases; therefore, they havebeen currently used in clinical cardiology.9–14
Up to date, there have been three studies inwhich ventricular functions were evaluated inpatients with LBBB by using TDE parameters.Quintana et al.28 demonstrated that the LV re-gional and mean Sm and LV mean Em/Am val-ues were lower in subjects with LBBB (n = 20)than in the control group (n = 20) and in sub-jects with right bundle branch block (n = 20). Inthis study, LV EF was lower in cases with LBBB(46% ± 8%) than what it was in those with theright bundle branch block (59% ± 6%) and in thecontrol groups (54% ± 4%). In another study,29
the Sm value obtained from the septal and lat-eral walls in 10 patients with LBBB was foundto be lower than the control group. In this study,it was reported that LV EF was similar in bothgroups. Contrary to these two studies, in a re-cent study,30 it was reported that in patientswith LBBB who demonstrated a lower LV EFthan did the control group, the Sm values ob-tained from the basal and mid segments of theanterior septum and of the posterior and lateralwalls of LV were similar to those in the controlgroup. In conclusion, there were inconsistentfindings concerning the effect of LBBB on my-ocardial velocities. These contradictory findingsmay be explained by the fact that those studieson LBBB did not include homogenous patientpopulation. We firstly evaluated the ventricularsystolic and diastolic functions by using the my-ocardial velocities and the MPI obtained fromthe annuli of the four LV walls and from thetricuspid lateral annulus in homogenous LBBBgroup including cases with LV EF ≥55% andwith normal coronary angiogram. The myocar-dial longitudinal functions of lateral wall of RVand of the anterior, inferior, inferior septum,and lateral walls of LV were evaluated sincethe myocardial velocities obtained by TDE atannulus are known to reflect the functions ofthe region adjacent to the annulus. The findingsobtained from this study show that global LVfunction decreases in cases with isolated LBBB.An increased MPI of LV, which was reportedto give information about systolic and diastolicfunctions, seems to support this idea. Also, theincreased MPI of RV may indicate RV dysfunc-tion. In addition, the changes in Vp, E/Vp, andE/Em account for the impairment of LV diastolicfunction: As previously demonstrated in a vari-ety of diseases,31,32 the decrease in Vp and theincrease in E/Em and E/Vp ratios establishedin this study can be accepted as indicators ofa disturbance of LV diastolic function in sub-jects with isolated LBBB. These changes werealso weakly-moderately correlated with QRSduration.
The disturbance of systolic and diastolic func-tions observed in cases with LBBB can be ex-plained by two mechanisms: One of these mech-anisms is the disturbance of depolarization andrepolarization associated with conduction delaywhich causes longer ICT and IRT and shorterET and diastolic duration of LV. Normally, RVand LV contraction is simultaneous. In LBBB,RV contraction occurs before that of the leftventricle.33 This may result in hemodynamicchanges throughout the cardiac cycle in both
Vol. 25, No. 3, 2008 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 261

AKIF DUZENLI, ET AL.
pressure and volume between the ventricles. Intime, the global and regional functions of theventricles may be impaired by these hemody-namic changes. The other mechanism may bethat the impairment of early diastolic blood flowin the left descending coronary artery in LBBBcan cause abnormal cardiac functions.34,35
In this study, when the regional myocardialvelocity and MPI values obtained from TDIwere evaluated together, it was demonstratedthat LBBB impaired especially the functionsof the inferior and inferior septal walls of LV.Interestingly, systolic and diastolic functions ofthe anterior wall were found to be affected byLBBB to a lesser extent than the other wallswere. The Em/Am ratio of the anterior wall, asin Sm value, is similar in cases with isolatedLBBB to that of the control group. These find-ings can be accounted for by the intraventric-ular asynchronization that LBBB leads to. Inan electrophysiological study36 in which the se-quence of LV activation was evaluated in LBBB,it was demonstrated that the sequence of LV ac-tivation was heterogeneous and was generallyfound to be anteroinferior orientation. Similarto this previous study, our study also demon-strated regional differences in systolic anddiastolic time intervals, and the delay in me-chanical activation was more in the inferior, in-ferior septum, and lateral walls; however, it wasless in the anterior wall. On the other hand, atthe lateral and anterior walls, ET was found tobe similar to that in the control group. In re-cent study on TDE,37 it was shown in parallelto our study that the anterior wall was activatedbefore the inferior, inferior septum, and lateralwalls. When evaluated together with those find-ings, the results of our study demonstrate thatisolated LBBB causes regional differences andthat these differences are probably associatedwith the sequence of activation.
In a large group of subjects with isolatedLBBB showed that patients with isolated LBBBhad an increased risk of dying from cardiacdisease and suggested that this might be dueto LV systolic and diastolic dysfunction.3 Inour study, although cardiac functions in sub-ject with isolated LBBB determined by con-ventional echocardiographic parameters werenormal, we discovered that myocardial velocityand MPI, which were shown to provide reliableand quantitative information about prognosisin cardiac diseases, were negatively affected.We consider that these new findings may ac-count for the poor prognosis of cases with iso-lated LBBB.
Limitations
Evaluation of systolic functions in patientswith LBBB by the 2D and M-mode echocar-diography is difficult because of abnormal sep-tal movement. Thus, LV EF calculated by bothSimpson’s and Teichold methods has some lim-itations. In this study, we calculated EF by Te-ichold method. We considered the limitationsof Teichold method to be unimportant becausethere was no wall motion abnormality (exceptfor the anterior wall of those patients withLBBB) in our patients—after all, the main aimof this study was not to evaluate the EF.
In conclusion, subjects with LBBB that wereshown to have normal systolic and diastolic LVfunction by conventional echo-Doppler methodswere found to have impaired LV systolic and di-astolic functions according to MPI and the my-ocardial velocities obtained from TDE, whichare relatively new parameters. Also, our resultsindicated that LV dysfunction had regional dif-ferences as a result of intraventricular asyn-chronization in isolated LBBB. In addition, itwas demonstrated that the increase in RV MPImight show the RV ventricular dysfunction inspite of normal Sm. These findings may con-tribute to increased morbidity and mortality incases with isolated LBBB.
References
1. Hardarson T, Arnoson A, Eliasson GJ, et al: Left bun-dle branch block: prevalence, incidence, follow-up andoutcome. Eur Heart J 1978;8:1075–1079.
2. Kreger BE, Anderson KM, Kannel WB: Prevalence ofintraventricular block in the general population: TheFramingham Study. Am Heart J 1989;117:903–910.
3. Fahy GJ, Pinski SL, Miller DP, et al: Natural his-tory of isolated bundle branch block. Am J Cardiol1996;77:1185–1190.
4. Herbert WH. Left bundle branch block and coronaryartery disease. J Electrocardiol 1975;8:317–24.
5. Freedman RA, Alderman EL, Sheffield LT, et al: Bun-dle branch block in patients with chronic coronaryartery disease: Angiographic correlates and prognos-tic significance. J Am Coll Cardiol 1987;10:73–80.
6. Schneider JF, Thomas HE Jr., Sorlie P, et al: Compar-ative features of newly acquired left and right bundlebranch block in the general population: The Framing-ham study. Am J Cardiol 1981;4:931–940.
7. Baldasseroni S, Opasich C, Gorini M, et al: Leftbundle-branch block is associated with increased 1-year sudden and total mortality rate in 5517 outpa-tients with congestive heart failure: a report from theItalian network on congestive heart failure. Am HeartJ 2002;143:398–405.
8. Iuliano S, Fisher SG, Karasik PE, et al: Department ofveterans affairs survival trial of antiarrhythmic ther-apy in congestive heart failure: QRS duration and mor-tality in patients with congestive heart failure. AmHeart J 2002;143:1085–1091.
262 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 25, No. 3, 2008
ISOLATED LEFT BUNDLE BRANCH BLOCK AND CARDIAC FUNCTIONS
9. Dujardin KS, Tei C, Yeo TC, et al: Prognostic value ofa Doppler index combining systolic and diastolic per-formance in idiopathic-dilated cardiomyopathy. Am JCardiol 1998;82:1071–1076.
10. Peltier M, Slama M, Garbi S, et al: Prognostic valueof Doppler-derived myocardial performance index inpatients with left ventricular systolic dysfunction. AmJ Cardiol 2002;90:1261–1263.
11. Bruch C, Schmermund A, Marin D, et al: Tei-Index inpatients with mild-to-moderate congestive heart fail-lure. Eur Heart J 2000;21:1888–1895.
12. Mishra RK, Kizer JR, Palmieri V. et al: Utility ofthe myocardial performance index in a populationwith high prevalences of obesity, diabetes, and hy-pertension: The strong heart study. Echocardiography2007;24:340–347.
13. Arnlov J, Lind L, Andren B, et al: A Doppler-derivedindex of combined left ventricular systolic and di-astolic function is an independent predictor of car-diovascular mortality in elderly men. Am Heart J2005;149:902–907.
14. Baykan M, Yilmaz R, Celik S, et al: Assessment of leftventricular systolic and diastolic function by Dopplertissue imaging in patients with preinfarction angina.J Am Soc Echocardiography 2003;16:1024–1030.
15. Pearlman AS, Gadrin JM, Martin RP, et al: Guide-lines for optimal physician training in echocardiog-raphy recommendations of the American Society ofEchocardiography Committee for Physician trainingin Echocardiography. Am J Cardiol 1987;60:158–163.
16. Teichholz LE, Kreulen T, Herman MV, et al: Prob-lems in echocardiographic volume determinations:echocardiographic-angiographic in the precense or ab-sence of asynergy. Am J Cardio1 1976;37:7–11.
17. Garcia MJ, Ares MA, Asher C, et al: An index ofearly left ventricular filling that combined with pulsedDoppler peak E velocity may estimate capillary wedgepressure. J Am Coll Cardiol 1997;29:448–454.
18. Baragan J, Fernandez-Caamano F, Sozutek Y, et al:Chronic left complete bundle-branch block. Phono-cardiographic and mechanocardiographic study of 30cases. Br Heart J 1968;30:196–202.
19. Oravetz J, Wissner S, Argano B, et al: Dynamic anal-ysis of heart sounds in right and left bundle-branchblocks. Circulation 1967;36:275–283.
20. Haber E, Leatham A. Splitting of heart sounds fromventricular asynchrony in bundle-branch block, ven-tricular ectopic beats, and artificial pacing. Br HeartJ 1965;27:691–696.
21. Adolph RJ, Fowler NO, Tanaka K. Prolongation of iso-volumic contraction time in left bundle branch block.Am Heart J 1969;78:585–591.
22. Grines CL, Bashore TM, Boudoulas H, et al: Func-tional abnormalities in isolated left bundle branchblock. Circulation 1989;79:845–853.
23. Ozdemir K, Altunkeser BB, Danis G, et al: Effect ofthe isolated left bundle branch block on systolic anddiastolic functions of left ventricle. J Am Soc Echocar-diogr 2001;14:1075–1079.
24. Alan DW, Michelle B. Tisue Doppler Imaging: Use-ful Echocardiographic Method for the cardiac sonogra-pher to assess systolic and diastolic ventricular func-tion. J Am Soc Echocardiography 2001;14:1143–1152.
25. Tei C, Ling LH, Hodge DO, et al: New index of com-bined systolic and diastolic miyocardial performance:a simple and reproducible measure of cardiac func-tion: A study in normal and dilated cardiomyopathy.J Cardiol 1995;26:357–366.
26. Eidem BW, Tei C, O’Leary PW, et al: Nongeometricquantitative assessment of right and left ventricu-lar function: Myocardial performance index in normalchildren and patients with Ebstein anomaly. J Am SocEchocardiogr 1998;11:849–856.
27. Ozdemir K, Mil S, Duzenli A, et al: Effect of preloadand heart rate on the Doppler and tissue Doppler-derived myocardial performance index. Clin Cardiol2007 In press.
28. Quintana M, Saha S, Rohani M, et al: Electrome-chanical coupling, uncoupling, and ventricular func-tion in patients with bundle branch block: A tissue–Doppler echocardiographic study. Echocardiography2004;21:687–698.
29. Niu HX, Hua W, Zhang S, et al: Assessment of cardiacfunction and synchronicity in subjects with isolatedbundle branch block using Doppler imaging. Chin MedJ 2006;10:795–800.
30. Melek M, Esen O, Esen AM, et al: Tissue Doppler eva-lution of intraventricular asynchrony in isolated leftbundle branch block. Echocardiography 2006;23:120–126.
31. Garcia MJ, Palac RT, Malenka DJ, et al: Color M-mode Doppler flow propagation velocity is a relativelypreload-independent index of left ventricular filling. JAm Soc Echocardiography 1999;12:129–137.
32. Khan S, Bess RL, Rosman HS, et al: Which echocar-diographic Doppler left ventricular diastolic func-tion measurements are most feasible in the clin-ical echocardiographic laboratory? Am J Cardiol2004;94:1099–1101.
33. Wyndham CR, Smith T, Meeran MK, et al: Epicardialactivation in patients with left bundle branch block.Circulation 1980;61:696–703.
34. Skalidis EI, Kochiadakis GE, Koukouraki SI, et al:Phasic coronary flow pattern and flow reserve in pa-tients with left bundle branch block and normal coro-nary arteries. Am Coll Cardiol 1999;33:1338–1346.
35. Youn HJ, Park CS, Cho EJ, et al: Left bundle branchblock disturbs left anterior descending coronary arteryflow: Study using transthoracic doppler echocardiog-raphy. J Am Soc Echocardiogr 2005;18:1093–1098.
36. Vassallo JA, Cassidy DM, Marchlinski FE, et al: En-docardial activation of left bundle branch block. Cir-culation 1984;69:914–923.
37. Badano LP, Gaddi O, Peraldo C, et al: Left ventric-ular electromechanical delay in patients with heartfailure and normal QRS duration and in patients withright and left bundle branch block. Europace 2007;1:41–47.
Vol. 25, No. 3, 2008 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 263
Related Documents











