The current burden of pneumococcal disease in England and Wales A. Melegaro a, * , W.J. Edmunds a , R. Pebody b , E. Miller b , R. George c a Modelling and Economics Unit, Centre for Infections, 61 Colindale Avenue, Health Protection Agency, London NW9 5EQ, UK b Immunisation Department, Centre for Infections, Health Protection Agency, London NW9 5EQ, UK c Respiratory and Systemic Infection Laboratory, Centre for Infections, Health Protection Agency, London NW9 5EQ, UK Accepted 1 February 2005 Available online 17 March 2005 KEYWORDS Pneumococcus; Pnc disease; IPD; Pneumonia; Otitis media; England and Wales; AOM; CAP Summary Objective: To evaluate the potential impact of various pneumococcal conjugate vaccination strategies, it is critical to ascertain the pre-vaccination epidemiology and to have a detailed evaluation of the current burden of pneumococcal disease. Method: A variety of national data sources and GP sentinel surveillance systems were used to estimate the incidence, number of hospital admissions, deaths, and GP consultations due to pneumococcal disease in England and Wales. Clinical outcomes included pneumococcal meningitis, bacteraemia, pneumonia and otitis media. A statistical model was used to attribute GP consultation recorded as pneumonia and acute otitis media to specific aetiological causes when these were not recorded. Results: The burden of pneumococcal disease is considerable, with incidence rates of both invasive and non-invasive disease peaking in children (!5 years) and in the elderly (75C years). Around 5800 hospitalisations specifically mentioning Strepto- coccus pneumoniae are estimated to occur annually in England and Wales, almost 40 000 for lobar pneumonia and over 15 000 for otitis media. There may be an additional 70 000 GP consultations for pneumococcal related community acquire pneumonia and over 630 000 for otitis media. A significant proportion of hospitalisations and GP consultations for pneumococcal disease occur among high- risk groups, with over 80% of hospital admissions reporting more than one diagnosis. Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. Introduction Streptococcus pneumoniae is a bacterial pathogen normally residing in the nasopharynx which causes a wide range of invasive and non-invasive diseases, the most important of which are: meningitis, Journal of Infection (2006) 52, 37–48 www.elsevierhealth.com/journals/jinf 0163-4453/$30.00 Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jinf.2005.02.008 * Corresponding author. Tel.: C44 20 8327 6048. E-mail address: [email protected] (A. Melegaro).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The current burden of pneumococcal disease inEngland and Wales
A. Melegaroa,*, W.J. Edmundsa, R. Pebodyb, E. Millerb, R. Georgec
aModelling and Economics Unit, Centre for Infections, 61 Colindale Avenue, Health Protection Agency,London NW9 5EQ, UKbImmunisation Department, Centre for Infections, Health Protection Agency, London NW9 5EQ, UKcRespiratory and Systemic Infection Laboratory, Centre for Infections, Health Protection Agency, LondonNW9 5EQ, UK
Accepted 1 February 2005Available online 17 March 2005
01do
KEYWORDSPneumococcus;Pnc disease;IPD;Pneumonia;Otitis media;England and Wales;AOM;CAP
63-4453/$30.00 Q 2005 The Britishi:10.1016/j.jinf.2005.02.008
* Corresponding author. Tel.: C44 2E-mail address: alessia.melegaro@
Summary Objective: To evaluate the potential impact of various pneumococcalconjugate vaccination strategies, it is critical to ascertain the pre-vaccinationepidemiology and to have a detailed evaluation of the current burden ofpneumococcal disease.Method: A variety of national data sources and GP sentinel surveillance systemswere used to estimate the incidence, number of hospital admissions, deaths, and GPconsultations due to pneumococcal disease in England and Wales. Clinical outcomesincluded pneumococcal meningitis, bacteraemia, pneumonia and otitis media. Astatistical model was used to attribute GP consultation recorded as pneumonia andacute otitis media to specific aetiological causes when these were not recorded.Results: The burden of pneumococcal disease is considerable, with incidence ratesof both invasive and non-invasive disease peaking in children (!5 years) and in theelderly (75C years). Around 5800 hospitalisations specifically mentioning Strepto-coccus pneumoniae are estimated to occur annually in England and Wales, almost40 000 for lobar pneumonia and over 15 000 for otitis media. There may be anadditional 70 000 GP consultations for pneumococcal related community acquirepneumonia and over 630 000 for otitis media. A significant proportion ofhospitalisations and GP consultations for pneumococcal disease occur among high-risk groups, with over 80% of hospital admissions reporting more than one diagnosis.Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved.
Infection Society. Published by
0 8327 6048.hpa.org.uk (A. Melegaro).
Introduction
Streptococcus pneumoniae is a bacterial pathogennormally residing in the nasopharynx which causes awide range of invasive and non-invasive diseases,the most important of which are: meningitis,
Journal of Infection (2006) 52, 37–48
www.elsevierhealth.com/journals/jinf
Elsevier Ltd. All rights reserved.
Table 1 International classification of diseases (ICD)codes for pneumococcal related disease
Definition ICD-9 code ICD-10code
Pneumococcalmeningitis
3201 G001
A. Melegaro et al.38
septicaemia, pneumonia and otitis media. Theburden of invasive pneumococcal (Pnc) disease(IPD) is high worldwide, with reported incidencerates ranging from 23.2 per 100 000 in the U.S.A.1
(166 in !2 years of age) to around 10 per 100 000 inEuropean countries.2 In developing countries extre-mely high incidence rates of IPD have been reportedamong infants (139–224 per 100 000 in !2 years ofage)3 as well as among indigenous adult populations(190 per 100 000 in 65C years of age)4 Less seriousnon-invasive pneumococcal disease (non-IPD) rep-resents most of the pneumococcal conditions and ismuch more difficult to estimate. Microbiologicalconfirmation of S. pneumoniae infection is bothdifficult and often not performed; hence theaetiological cause remains unknown. Estimatesfrom previous studies suggest that 15–43% ofcommunity-acquired pneumonia (CAP) cases areattributable to pneumococcal infection;5 around30–35% of acute otitis media (AOM) has beenattributed to Pnc.6,7
A pneumococcal conjugate vaccine (PCV) hasbeen proved to be safe and effective against themost serious form of pneumococcal infection8–11
and also moderately effective against AOM12,13 andpneumonia.14,15 Widespread vaccination has beenintroduced in the U.S.A.16 whereas in the U.K. thevaccine is currently recommended only for childrenless than 5 years of age with specific high-riskconditions.17 Moreover, since, July 2003, a pneu-mococcal immunisation program for the healthyelderly with a 23-valent polysaccharide vaccine hasalso been introduced in England (www.dh.gov.uk)in addition to the previous policy of vaccinatinghigh-risk individuals over 2 years of age.
The aim of this work is to estimate the amount ofpneumococcal disease that is present in Englandand Wales in order to provide baseline informationfor the assessment of the potential benefits thatmay derive from vaccination.
Pneumococcalsepticaemia
0382 A403
Pneumococcalpneumonia
481 J13X
Lobar pneumonia,organism unspecified
481 J181
S. pneumoniae as thecause of the disease
410 B953
Non-suppurative otitismedia
3810–3814 H650–H659
Suppurative andunspecified otitismedia
3820–3829 H660–H669
Otitis media in diseasesclassified elsewhere
n.a. H670–H678
n.a., no equivalent ICD-9 code was available.
Methods
Data sources
Laboratory reportsThe enhanced surveillance of pneumococcal dis-ease set up jointly between the CommunicableDisease Surveillance Centre’s (CDSC) national lab-oratory reporting scheme and the Respiratory andSystemic Infection Laboratory (RSIL) at the Special-ist and Reference Microbiology Division of theHealth Protection Agency is the main data sourcefor the ascertainment of the burden of IPD in
England and Wales.18,19 The system was set up in1996 in order to improve the estimate of the burdenof IPD throughout England and Wales and to gainfurther information on serotype distribution anddisease incidence in different age groups. From thisnational surveillance system, cases of laboratoryconfirmed IPD (pneumococcal bacteraemia andmeningitis) reported from laboratories aroundEngland and Wales from January 1996 to December2000 were extracted. The extracted data includedage, sex, earliest specimen date, serogroups andserotype (when available), antimicrobial suscepti-bility information (penicillin and erythromycin),region and method of confirmation.
Hospital episode statistics (HES)Hospital episode statistics (HES—department ofhealth) (http://www.dh.gov.uk) is a computerisedhospital discharge database that covers all NationalHealth Service Hospitals in England. It containsinformation on individual episodes of illness,together with patient details (age, date of birth,postcode, sex), clinical conditions, number of daysspent in the hospital and admissions to intensivecare unit (ICU). For each record, seven diagnosticfields are available, in which the condition(s) ofeach patient are specified using the tenth revisionof the International Classification of Disease codingsystem (ICD-10). All hospital admissions thatoccurred over the period April 1995–March 2000which included an occurrence of one of thepneumococcal related ICD-10 codes (Table 1) in
Burden of pneumococcal disease 39
any of the seven diagnostic fields were extractedfrom the database and cleaned for possible dupli-cates. This included strictly IPD codes (pneumo-coccal meningitis and septicaemia), pneumococcalpneumonia code (under which both IPD and non-IPDcan be recorded) as well as non-invasive codes suchas otitis media and lobar or unspecified pneumonia.Admissions due to lobar pneumonia, organismunspecified (J181), were extracted as pneumococ-cus is considered one of the major cause of lobarpneumonia.20
GP consultationsThe weekly number of consultations to generalpractitioners for a diagnosis of either pneumo-nia/pneumonitis or AOM and population at risk wasobtained form the Royal College of GeneralPractitioners (RCGP) weekly returns system.21 Thebi-weekly number of pneumonia and AOM wascalculated for the period 1996–2000 and used asoutcome variable in a multivariate regressionanalysis (see later).
Additional information was available from themorbidity survey of general practices fourth edition(MSGP4), which is a 1-year prospective survey ofaround 500 000 patients attending GP practicesundertaken in 1991/1992.22 This database containsinformation on people attending the practices inthe survey, such as socio-economic status, detailson family composition, individual characteristics(i.e. smoking status) and the history of the patient’shealth status during the year of the survey(recorded using the ICD-9 coding system).
Data analysis
The total number of pneumococcal confirmed casesidentified by laboratory reports and HES for theperiod 1995–2000 was derived and comparisonswere made between the data sources. The seasonalpatterns were investigated from both laboratoryreports and hospitalisations data.
Multiple linear regression analysis was used,following the technique developed by Ryan andcolleagues,23 to ascertain the underlying aetiolo-gies of CAP and AOM GP consultations and toestimate the proportion attributable to S. pneumo-niae infection. The observed seasonality in agentsthat could potentially cause pneumonia and AOMwas compared to the number of consultationsreported for the two clinical outcomes over thesame time period. The bi-weekly number ofconsultations for the period 1996–2000 was usedas the dependent variable of the regression. Theindependent variables were the bi-weekly number
of national laboratory reports for the followingagents associated with CAP and AOM: S. pneumo-niae, Haemophilus influenzae, adenovirus, influ-enza A (Flu A), influenza B (Flu B), Klebsiellapneumoniae, Legionella pneumophila, Moraxellacatarrhalis. Mycoplasma pneumoniae, parain-fluenza, Pneumocistis carinii, rhinovirus, RSV,Chlamydia pneumoniae and Chlamydia psittaci.
A backward stepwise regression was performedusing STATA 6.0. This technique is based on avariable selection procedure in which all variablesare entered into the equation and then sequentiallyremoved if non-significant (P-valueO0.05). Theimportance of two-way interaction terms for theexplanation of the dependent variables was alsoinvestigated, assessing the significance (P!0.01) ofeach interaction term between the organisms in thefinal model. The validity of the model was assessed(R2) and the impact of changes in the modelspecification was investigated.
Age-specific incidence rates were calculatedfrom laboratory confirmed IPD cases (pneumo-coccal bacteraemia, meningitis and other con-ditions where pneumococcus was isolated from anormally sterile site) extracting the number ofinvasive isolates reported to the national enhancedsurveillance system for the period 1996–2000 andusing Office for National Statistics (ONS) populationestimates for the appropriate years and age groups.Similarly, hospitalisation rates were derived for anypneumococcal confirmed hospitalisations, for lobarpneumonia and for otitis media (organism unspeci-fied) using ONS population estimates for England.
The serotype distribution of IPD cases wasderived for each year from 1996 to 2000 examiningthe isolate characteristics. The proportions ofinvasive infections that were caused by the ser-otypes contained in the different formulations ofpneumococcal conjugate and polysaccharide vac-cines were estimated for different age groups.
Case-fatality rates (CFR) from 1995/1996 to1999/2000 were estimated by dividing the numberof deaths among hospitalised patients by thenumber of pneumococcal-related admissions(HES). Due to the presence of other serious co-morbidities in many patients (especially theelderly), it was not possible to ascertain withconfidence whether the patient had died becauseof the pneumococcal infection or, simply, with apneumococcal infection. For this reason we esti-mated CFR for patients reporting a pneumococcalcode in the first diagnostic code, in the first three,or in any of the seven diagnostic fields. Assumingthat the first diagnosis is more likely to report theunderlying cause of the hospitalisation, we assumedthat CFR calculated on the first diagnosis only were

A. Melegaro et al.40
more likely to be related to S. pneumoniaeinfection. From ONS, the number of pneumococcalrelated deaths (i.e. pneumococcal code as theunderlying cause of death) for the same period werealso derived and comparisons were made with HESfigures.
Average age-specific episode and consultationrates for CAP and AOM were estimated using MSGP4data and compared to the rates provided by RCGP.Moreover, from MSGP4 data, episode rates of bothCAP and AOM due to pneumococcal infection werealso derived (using the proportions estimated withthe multivariate model) for high and low-riskindividuals, stratifying the patients according towhether they had consulted their GP over the 1-year observation period for one or more of thefollowing chronic medical conditions: diabetesmellitus, chronic renal, hepatic, or pulmonarydisease, alcoholism, or neoplastic disease, chronicimmunosuppression. These represent the high-riskgroup for which the polysaccharide pneumococcalvaccine has been in the past17 and is currentlyrecommended (http://www.dh.gov.uk).
Results
The number of laboratory reports of S. pneumoniaeinfection for each year since 1990 was derived andshowed an increase in the annual figure in 1996,when the enhanced surveillance system wasimplemented (data not shown). Since, then, anannual average of around 4828 IPD cases had beenreported (range: 4692–5159). Of these, an averageof 343 (range: 314–394) were identified as cases ofpneumococcal meningitis (pneumococci isolatedfrom the CSF) whereas the remaining isolateswere obtained from bacteraemic patients withpneumococcus isolated from the blood or othersterile body sites.
A marked seasonal pattern in the presentation ofIPD with preponderance in the winter months wasobserved from both weekly laboratory reports andhospital admissions due to confirmed pneumococ-cal infection. Reported IPD cases reach a low duringAugust and peak in December and January whenreporting rates are 3–5 times higher. Fig. 1 shows acomparison between laboratory weekly reports ofIPD and hospitalisations due to all pneumococcalconfirmed infection and also admissions with adiagnosis of lobar pneumonia, organism unspeci-fied. The almost overlapping weekly patternobserved when considering all confirmed pneumo-coccus patients suggests that hospital episodes withan ICD-10 code mentioning. S. pneumoniae are an
accurate reflection of IPD incidence as reported inthe enhanced surveillance system. Moreover, asimilar seasonal pattern also characterises lobarpneumonia admissions though the numbers aremuch higher.
A multivariate regression analysis was performedto assess the proportion of GP consultations for CAPand AOM that are likely to be pneumococcal inorigin. Three models were estimated for both CAPand AOM. We found no blologically plausiblestatistically significant interaction terms. Tables 2and 3 provide estimates of the proportion of CAPand AOM attributable to each of the differentagents. The variables laboratory reports for S.pneumoniae, adenovirus, M. pneumoniae, RSV andFlu A stayed in the model for unspecified pneumoniacases (model CAP1). The adjusted R2 indicates that67% of the variation in the weekly number ofunspecified cases was explained by the model.Using this model, it was estimated that 31% ofunspecified pneumonia could be attributed to S.pneumoniae, 38% to adenovirus, 17% to M. pneu-moniae, 6% to RSV and 8% to Flu A. A slightly moreadequate fit (R2Z68%) was achieved by modelCAP2, where the variable Adenovirus was droppedfrom the model and ‘other organism’ was added toconsider all the other possible infectious and non-infectious causes of pneumonia that were notincluded in the analysis. Using CAP2, the proportionof unspecified pneumonia attributed to S. pneumo-niae was 26%, 14% to M. pneumoniae, 8% to RSV,11% to H. influenzae, 10% to Flu A and 31% to ‘otherorganism’. H. influenzae was kept in the model,though the P-value was less significant, but stillwithin the acceptable range (P-valueZ0.019). Thesensitivity of model results to the variable H.influenzae was assessed in CAP3. Using thismodel, it was estimated that the proportion ofpneumonia cases attributable to S. pneumoniaewas 29%, 12% to M. pneumoniae, 6% to RSV, 8% toFlu A and 44% to ‘other organism’. Similarly to theprevious models, the latter explained 67% for thedata variablilty. For the unspecified acute otitismedia episodes, the variables S. pneumoniae, Flu B,M. pneumoniae, RSV, rhinovirus and adenovirusstayed in the model (model AOM1), explaining 68%of the data variability. From this model, S.pneumoniae was estimated to cause 23% of AOMepisodes, 4% were due to Flu B, 12% to M.pneumoniae, 8% to RSV, 18% to rhinovirus and 36%to adenovirus. Dropping adenovirus from the modelreduced the fit to 63% and 58% when the variable‘other organism’ was, respectively, included andexcluded from the model specification. In sum-mary, from the six models just described, S.pneumoniae was estimated to cause from 26%
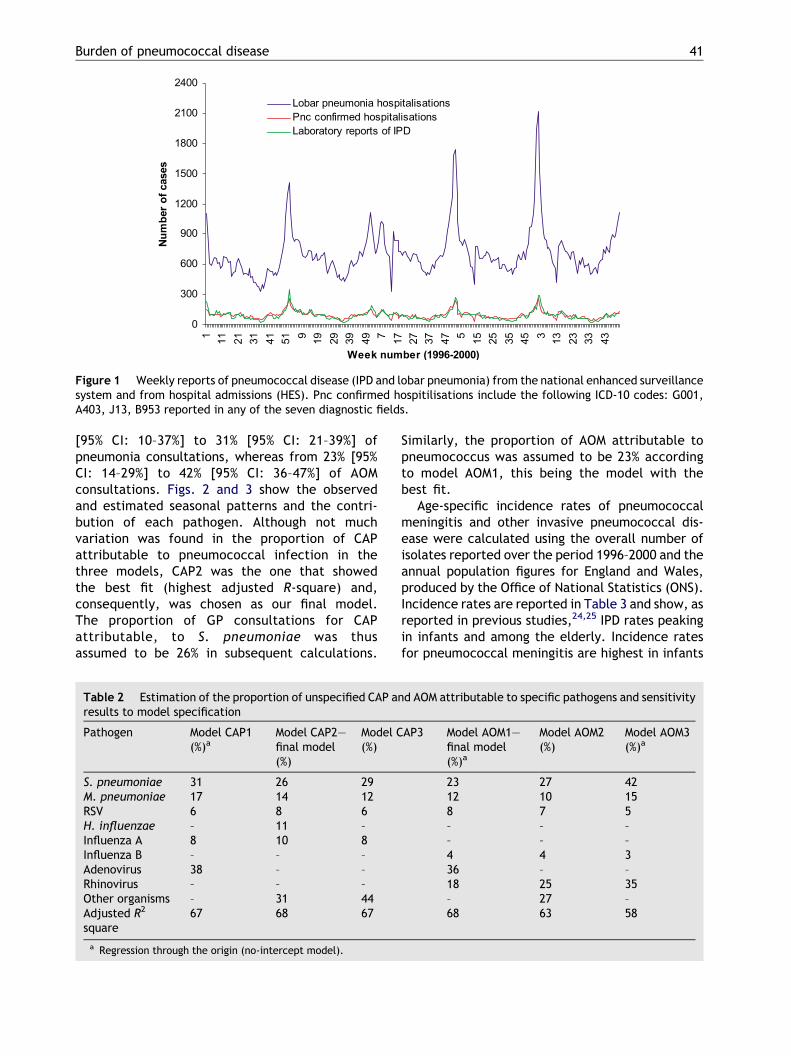
Figure 1 Weekly reports of pneumococcal disease (IPD and lobar pneumonia) from the national enhanced surveillancesystem and from hospital admissions (HES). Pnc confirmed hospitilisations include the following ICD-10 codes: G001,A403, J13, B953 reported in any of the seven diagnostic fields.
Burden of pneumococcal disease 41
[95% CI: 10–37%] to 31% [95% CI: 21–39%] ofpneumonia consultations, whereas from 23% [95%CI: 14–29%] to 42% [95% CI: 36–47%] of AOMconsultations. Figs. 2 and 3 show the observedand estimated seasonal patterns and the contri-bution of each pathogen. Although not muchvariation was found in the proportion of CAPattributable to pneumococcal infection in thethree models, CAP2 was the one that showedthe best fit (highest adjusted R-square) and,consequently, was chosen as our final model.The proportion of GP consultations for CAPattributable, to S. pneumoniae was thusassumed to be 26% in subsequent calculations.
Table 2 Estimation of the proportion of unspecified CAP aresults to model specification
Pathogen Model CAP1(%)a
Model CAP2—final model(%)
Model C(%)
S. pneumoniae 31 26 29M. pneumoniae 17 14 12RSV 6 8 6H. influenzae – 11 –Influenza A 8 10 8Influenza B – – –Adenovirus 38 – –Rhinovirus – – –Other organisms – 31 44Adjusted R2
square67 68 67
a Regression through the origin (no-intercept model).
Similarly, the proportion of AOM attributable topneumococcus was assumed to be 23% accordingto model AOM1, this being the model with thebest fit.
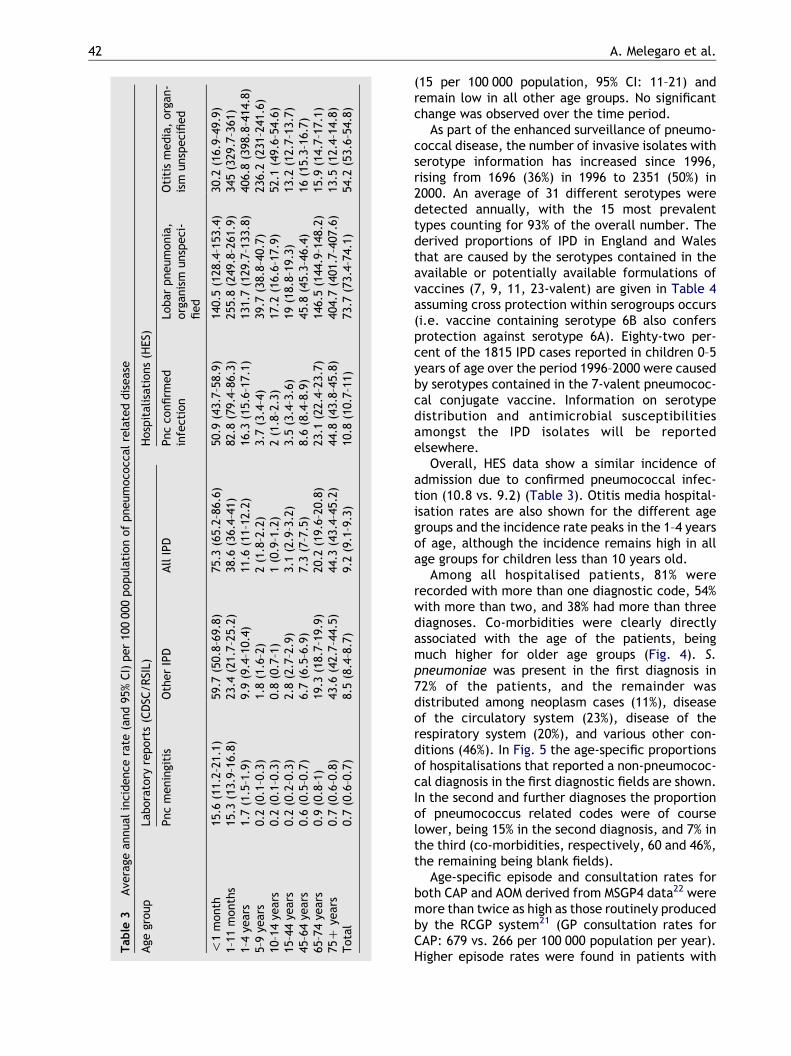
Age-specific incidence rates of pneumococcalmeningitis and other invasive pneumococcal dis-ease were calculated using the overall number ofisolates reported over the period 1996–2000 and theannual population figures for England and Wales,produced by the Office of National Statistics (ONS).Incidence rates are reported in Table 3 and show, asreported in previous studies,24,25 IPD rates peakingin infants and among the elderly. Incidence ratesfor pneumococcal meningitis are highest in infants
nd AOM attributable to specific pathogens and sensitivity
AP3 Model AOM1—final model(%)a
Model AOM2(%)
Model AOM3(%)a
23 27 4212 10 158 7 5– – –– – –4 4 336 – –18 25 35– 27 –68 63 58
Table
3Ave
rage
annual
inci
dence
rate
(and
95%
CI)
per
100
000
popula
tion
of
pneum
oco
ccal
rela
ted
dis
eas
e
Age
group
Labora
tory
report
s(C
DSC
/RSI
L)H
osp
ital
isat
ions
(HES)
Pnc
menin
giti
sO
ther
IPD
All
IPD
Pnc
confirm
ed
infe
ctio
nLo
bar
pneum
onia
,org
anis
munsp
eci
-fied
Oti
tis
media
,org
an-
ism
unsp
eci
fied
!1
month
15.6
(11.
2–21
.1)
59.7
(50.
8–69
.8)
75.3
(65.
2–86
.6)
50.9
(43.
7–58
.9)
140.
5(1
28.4
–153
.4)
30.2
(16.
9–49
.9)
1–11
month
s15
.3(1
3.9–
16.8
)23
.4(2
1.7–
25.2
)38
.6(3
6.4–
41)
82.8
(79.
4–86
.3)
255.
8(2
49.8
–261
.9)
345
(329
.7–3
61)
1–4
year
s1.
7(1
.5–1
.9)
9.9
(9.4
–10.
4)11
.6(1
1–12
.2)
16.3
(15.
6–17
.1)
131.
7(1
29.7
–133
.8)
406.
8(3
98.8
–414
.8)
5–9
year
s0.
2(0
.1–0
.3)
1.8
(1.6
–2)
2(1
.8–2
.2)
3.7
(3.4
–4)
39.7
(38.
8–40
.7)
236.
2(2
31–2
41.6
)10
–14
year
s0.
2(0
.1–0
.3)
0.8
(0.7
–1)
1(0
.9–1
.2)
2(1
.8–2
.3)
17.2
(16.
6–17
.9)
52.1
(49.
6–54
.6)
15–4
4ye
ars
0.2
(0.2
–0.3
)2.
8(2
.7–2
.9)
3.1
(2.9
–3.2
)3.
5(3
.4–3
.6)
19(1
8.8–
19.3
)13
.2(1
2.7–
13.7
)45
–64
year
s0.
6(0
.5–0
.7)
6.7
(6.5
–6.9
)7.
3(7
–7.5
)8.
6(8
.4–8
.9)
45.8
(45.
3–46
.4)
16(1
5.3–
16.7
)65
–74
year
s0.
9(0
.8–1
)19
.3(1
8.7–
19.9
)20
.2(1
9.6–
20.8
)23
.1(2
2.4–
23.7
)14
6.5
(144
.9–1
48.2
)15
.9(1
4.7–
17.1
)75
Cye
ars
0.7
(0.6
–0.8
)43
.6(4
2.7–
44.5
)44
.3(4
3.4–
45.2
)44
.8(4
3.8–
45.8
)40
4.7
(401
.7–4
07.6
)13
.5(1
2.4–
14.8
)Tota
l0.
7(0
.6–0
.7)
8.5
(8.4
–8.7
)9.
2(9
.1–9
.3)
10.8
(10.
7–11
)73
.7(7
3.4–
74.1
)54
.2(5
3.6–
54.8
)
A. Melegaro et al.42
(15 per 100 000 population, 95% CI: 11–21) andremain low in all other age groups. No significantchange was observed over the time period.
As part of the enhanced surveillance of pneumo-coccal disease, the number of invasive isolates withserotype information has increased since 1996,rising from 1696 (36%) in 1996 to 2351 (50%) in2000. An average of 31 different serotypes weredetected annually, with the 15 most prevalenttypes counting for 93% of the overall number. Thederived proportions of IPD in England and Walesthat are caused by the serotypes contained in theavailable or potentially available formulations ofvaccines (7, 9, 11, 23-valent) are given in Table 4assuming cross protection within serogroups occurs(i.e. vaccine containing serotype 6B also confersprotection against serotype 6A). Eighty-two per-cent of the 1815 IPD cases reported in children 0–5years of age over the period 1996–2000 were causedby serotypes contained in the 7-valent pneumococ-cal conjugate vaccine. Information on serotypedistribution and antimicrobial susceptibilitiesamongst the IPD isolates will be reportedelsewhere.
Overall, HES data show a similar incidence ofadmission due to confirmed pneumococcal infec-tion (10.8 vs. 9.2) (Table 3). Otitis media hospital-isation rates are also shown for the different agegroups and the incidence rate peaks in the 1–4 yearsof age, although the incidence remains high in allage groups for children less than 10 years old.
Among all hospitalised patients, 81% wererecorded with more than one diagnostic code, 54%with more than two, and 38% had more than threediagnoses. Co-morbidities were clearly directlyassociated with the age of the patients, beingmuch higher for older age groups (Fig. 4). S.pneumoniae was present in the first diagnosis in72% of the patients, and the remainder wasdistributed among neoplasm cases (11%), diseaseof the circulatory system (23%), disease of therespiratory system (20%), and various other con-ditions (46%). In Fig. 5 the age-specific proportionsof hospitalisations that reported a non-pneumococ-cal diagnosis in the first diagnostic fields are shown.In the second and further diagnoses the proportionof pneumococcus related codes were of courselower, being 15% in the second diagnosis, and 7% inthe third (co-morbidities, respectively, 60 and 46%,the remaining being blank fields).
Age-specific episode and consultation rates forboth CAP and AOM derived from MSGP4 data22 weremore than twice as high as those routinely producedby the RCGP system21 (GP consultation rates forCAP: 679 vs. 266 per 100 000 population per year).Higher episode rates were found in patients with
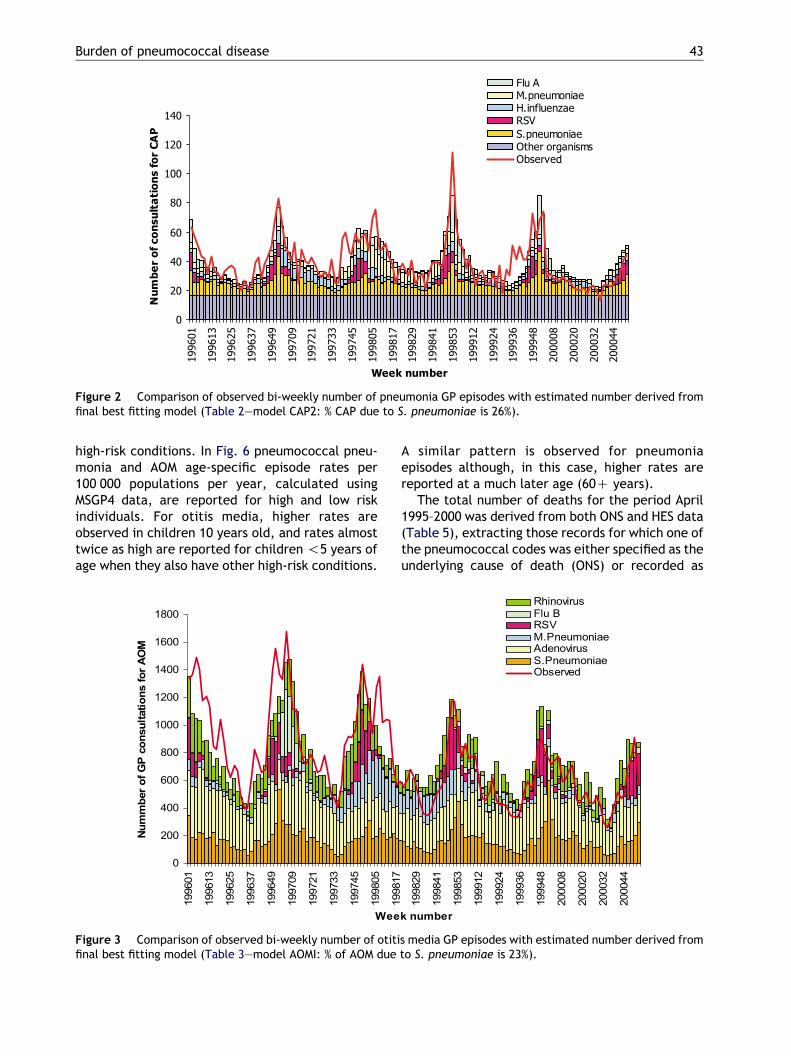
Figure 2 Comparison of observed bi-weekly number of pneumonia GP episodes with estimated number derived fromfinal best fitting model (Table 2—model CAP2: % CAP due to S. pneumoniae is 26%).
Burden of pneumococcal disease 43
high-risk conditions. In Fig. 6 pneumococcal pneu-monia and AOM age-specific episode rates per100 000 populations per year, calculated usingMSGP4 data, are reported for high and low riskindividuals. For otitis media, higher rates areobserved in children 10 years old, and rates almosttwice as high are reported for children !5 years ofage when they also have other high-risk conditions.
Figure 3 Comparison of observed bi-weekly number of otitifinal best fitting model (Table 3—model AOMI: % of AOM due
A similar pattern is observed for pneumoniaepisodes although, in this case, higher rates arereported at a much later age (60C years).
The total number of deaths for the period April1995–2000 was derived from both ONS and HES data(Table 5), extracting those records for which one ofthe pneumococcal codes was either specified as theunderlying cause of death (ONS) or recorded as
s media GP episodes with estimated number derived fromto S. pneumoniae is 23%).
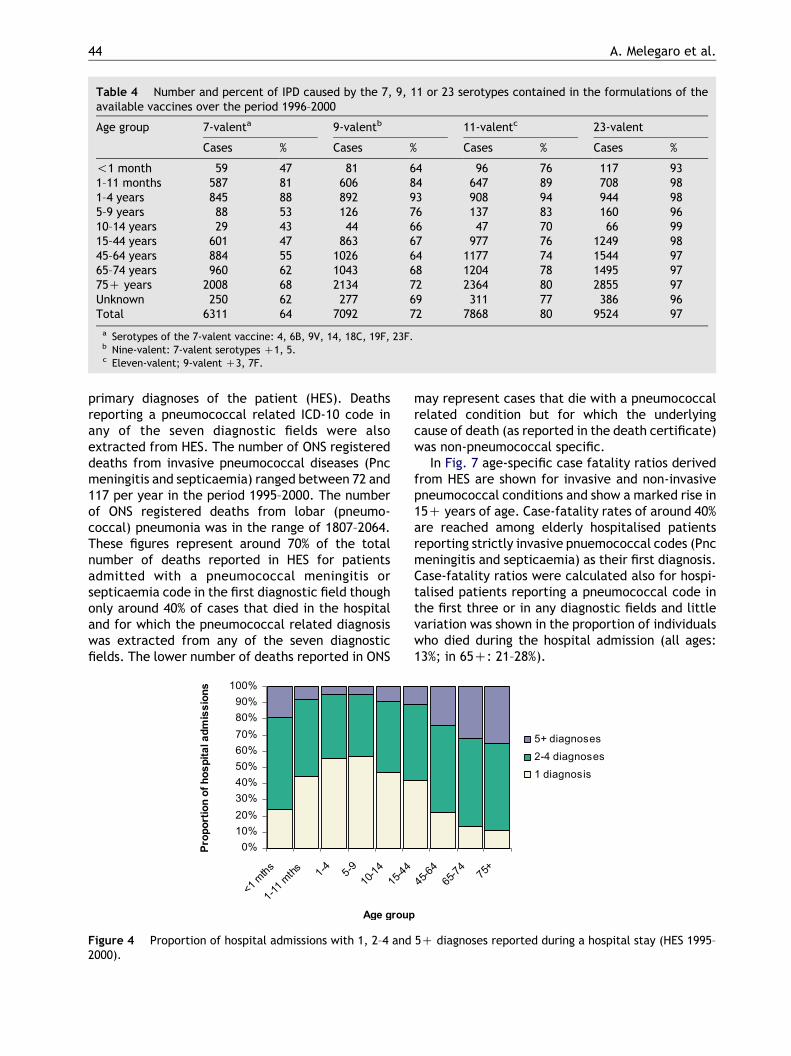
Table 4 Number and percent of IPD caused by the 7, 9, 11 or 23 serotypes contained in the formulations of theavailable vaccines over the period 1996–2000
Age group 7-valenta 9-valentb 11-valentc 23-valent
Cases % Cases % Cases % Cases %
!1 month 59 47 81 64 96 76 117 931–11 months 587 81 606 84 647 89 708 981–4 years 845 88 892 93 908 94 944 985–9 years 88 53 126 76 137 83 160 9610–14 years 29 43 44 66 47 70 66 9915–44 years 601 47 863 67 977 76 1249 9845–64 years 884 55 1026 64 1177 74 1544 9765–74 years 960 62 1043 68 1204 78 1495 9775C years 2008 68 2134 72 2364 80 2855 97Unknown 250 62 277 69 311 77 386 96Total 6311 64 7092 72 7868 80 9524 97
a Serotypes of the 7-valent vaccine: 4, 6B, 9V, 14, 18C, 19F, 23F.b Nine-valent: 7-valent serotypes C1, 5.c Eleven-valent; 9-valent C3, 7F.
A. Melegaro et al.44
primary diagnoses of the patient (HES). Deathsreporting a pneumococcal related ICD-10 code inany of the seven diagnostic fields were alsoextracted from HES. The number of ONS registereddeaths from invasive pneumococcal diseases (Pncmeningitis and septicaemia) ranged between 72 and117 per year in the period 1995–2000. The numberof ONS registered deaths from lobar (pneumo-coccal) pneumonia was in the range of 1807–2064.These figures represent around 70% of the totalnumber of deaths reported in HES for patientsadmitted with a pneumococcal meningitis orsepticaemia code in the first diagnostic field thoughonly around 40% of cases that died in the hospitaland for which the pneumococcal related diagnosiswas extracted from any of the seven diagnosticfields. The lower number of deaths reported in ONS
Figure 4 Proportion of hospital admissions with 1, 2–4 and2000).
may represent cases that die with a pneumococcalrelated condition but for which the underlyingcause of death (as reported in the death certificate)was non-pneumococcal specific.
In Fig. 7 age-specific case fatality ratios derivedfrom HES are shown for invasive and non-invasivepneumococcal conditions and show a marked rise in15C years of age. Case-fatality rates of around 40%are reached among elderly hospitalised patientsreporting strictly invasive pnuemococcal codes (Pncmeningitis and septicaemia) as their first diagnosis.Case-fatality ratios were calculated also for hospi-talised patients reporting a pneumococcal code inthe first three or in any diagnostic fields and littlevariation was shown in the proportion of individualswho died during the hospital admission (all ages:13%; in 65C: 21–28%).
5C diagnoses reported during a hospital stay (HES 1995–
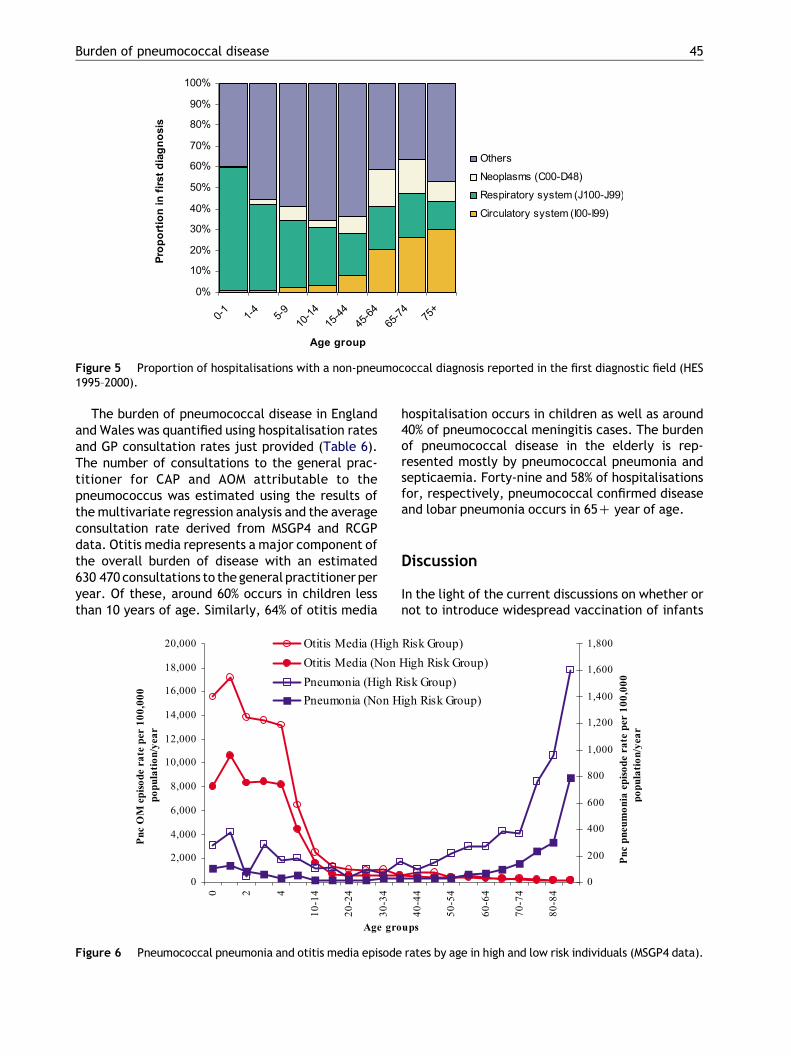
Figure 5 Proportion of hospitalisations with a non-pneumococcal diagnosis reported in the first diagnostic field (HES1995–2000).
Burden of pneumococcal disease 45
The burden of pneumococcal disease in Englandand Wales was quantified using hospitalisation ratesand GP consultation rates just provided (Table 6).The number of consultations to the general prac-titioner for CAP and AOM attributable to thepneumococcus was estimated using the results ofthe multivariate regression analysis and the averageconsultation rate derived from MSGP4 and RCGPdata. Otitis media represents a major component ofthe overall burden of disease with an estimated630 470 consultations to the general practitioner peryear. Of these, around 60% occurs in children lessthan 10 years of age. Similarly, 64% of otitis media
Figure 6 Pneumococcal pneumonia and otitis media episode
hospitalisation occurs in children as well as around40% of pneumococcal meningitis cases. The burdenof pneumococcal disease in the elderly is rep-resented mostly by pneumococcal pneumonia andsepticaemia. Forty-nine and 58% of hospitalisationsfor, respectively, pneumococcal confirmed diseaseand lobar pneumonia occurs in 65C year of age.
Discussion
In the light of the current discussions on whether ornot to introduce widespread vaccination of infants
rates by age in high and low risk individuals (MSGP4 data).
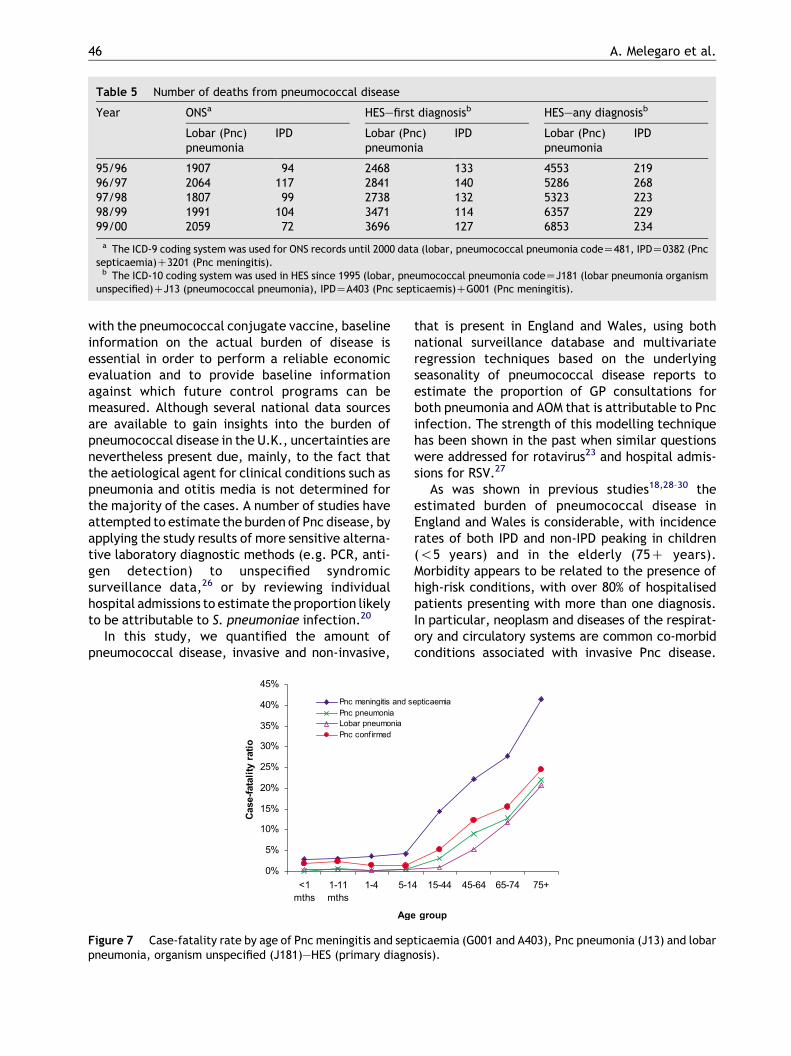
Table 5 Number of deaths from pneumococcal disease
Year ONSa HES—first diagnosisb HES—any diagnosisb
Lobar (Pnc)pneumonia
IPD Lobar (Pnc)pneumonia
IPD Lobar (Pnc)pneumonia
IPD
95/96 1907 94 2468 133 4553 21996/97 2064 117 2841 140 5286 26897/98 1807 99 2738 132 5323 22398/99 1991 104 3471 114 6357 22999/00 2059 72 3696 127 6853 234
a The ICD-9 coding system was used for ONS records until 2000 data (lobar, pneumococcal pneumonia codeZ481, IPDZ0382 (Pncsepticaemia)C3201 (Pnc meningitis).
b The ICD-10 coding system was used in HES since 1995 (lobar, pneumococcal pneumonia codeZJ181 (lobar pneumonia organismunspecified)CJ13 (pneumococcal pneumonia), IPDZA403 (Pnc septicaemis)CG001 (Pnc meningitis).
A. Melegaro et al.46
with the pneumococcal conjugate vaccine, baselineinformation on the actual burden of disease isessential in order to perform a reliable economicevaluation and to provide baseline informationagainst which future control programs can bemeasured. Although several national data sourcesare available to gain insights into the burden ofpneumococcal disease in the U.K., uncertainties arenevertheless present due, mainly, to the fact thatthe aetiological agent for clinical conditions such aspneumonia and otitis media is not determined forthe majority of the cases. A number of studies haveattempted to estimate the burden of Pnc disease, byapplying the study results of more sensitive alterna-tive laboratory diagnostic methods (e.g. PCR, anti-gen detection) to unspecified syndromicsurveillance data,26 or by reviewing individualhospital admissions to estimate the proportion likelyto be attributable to S. pneumoniae infection.20
In this study, we quantified the amount ofpneumococcal disease, invasive and non-invasive,
Figure 7 Case-fatality rate by age of Pnc meningitis and seppneumonia, organism unspecified (J181)—HES (primary diagn
that is present in England and Wales, using bothnational surveillance database and multivariateregression techniques based on the underlyingseasonality of pneumococcal disease reports toestimate the proportion of GP consultations forboth pneumonia and AOM that is attributable to Pncinfection. The strength of this modelling techniquehas been shown in the past when similar questionswere addressed for rotavirus23 and hospital admis-sions for RSV.27
As was shown in previous studies18,28–30 theestimated burden of pneumococcal disease inEngland and Wales is considerable, with incidencerates of both IPD and non-IPD peaking in children(!5 years) and in the elderly (75C years).Morbidity appears to be related to the presence ofhigh-risk conditions, with over 80% of hospitalisedpatients presenting with more than one diagnosis.In particular, neoplasm and diseases of the respirat-ory and circulatory systems are common co-morbidconditions associated with invasive Pnc disease.
ticaemia (G001 and A403), Pnc pneumonia (J13) and lobarosis).
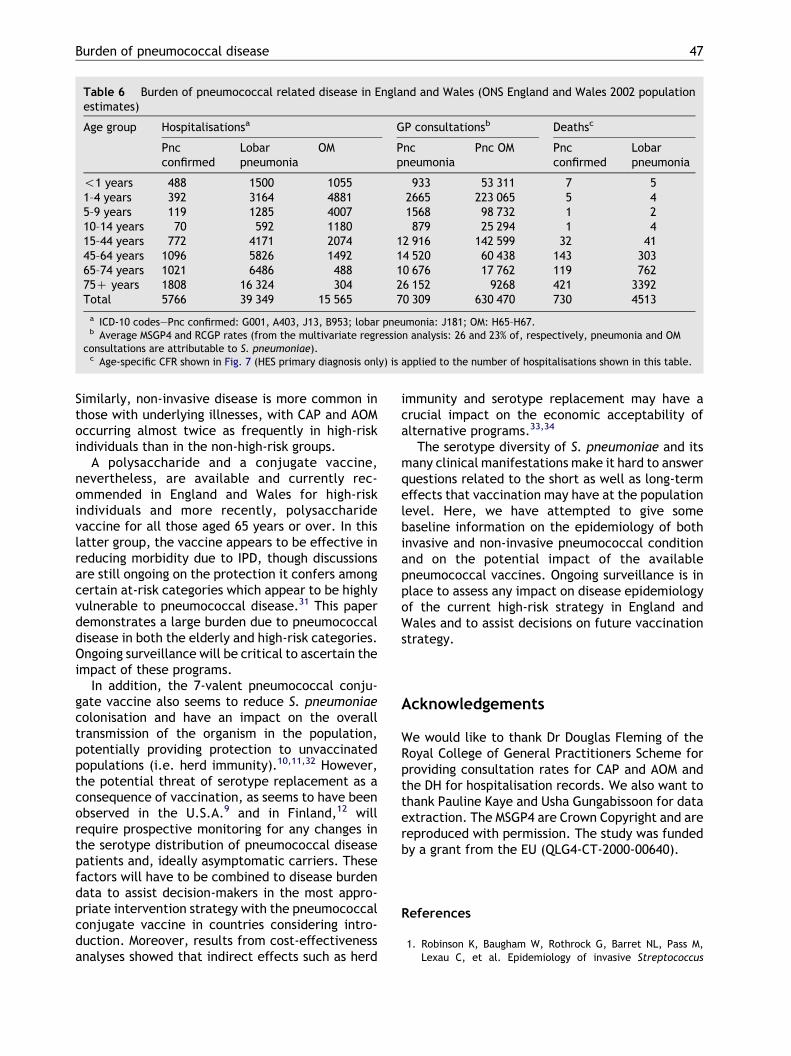
Table 6 Burden of pneumococcal related disease in England and Wales (ONS England and Wales 2002 populationestimates)
Age group Hospitalisationsa GP consultationsb Deathsc
Pncconfirmed
Lobarpneumonia
OM Pncpneumonia
Pnc OM Pncconfirmed
Lobarpneumonia
!1 years 488 1500 1055 933 53 311 7 51–4 years 392 3164 4881 2665 223 065 5 45–9 years 119 1285 4007 1568 98 732 1 210–14 years 70 592 1180 879 25 294 1 415–44 years 772 4171 2074 12 916 142 599 32 4145–64 years 1096 5826 1492 14 520 60 438 143 30365–74 years 1021 6486 488 10 676 17 762 119 76275C years 1808 16 324 304 26 152 9268 421 3392Total 5766 39 349 15 565 70 309 630 470 730 4513
a ICD-10 codes—Pnc confirmed: G001, A403, J13, B953; lobar pneumonia: J181; OM: H65–H67.b Average MSGP4 and RCGP rates (from the multivariate regression analysis: 26 and 23% of, respectively, pneumonia and OM
consultations are attributable to S. pneumoniae).c Age-specific CFR shown in Fig. 7 (HES primary diagnosis only) is applied to the number of hospitalisations shown in this table.
Burden of pneumococcal disease 47
Similarly, non-invasive disease is more common inthose with underlying illnesses, with CAP and AOMoccurring almost twice as frequently in high-riskindividuals than in the non-high-risk groups.
A polysaccharide and a conjugate vaccine,nevertheless, are available and currently rec-ommended in England and Wales for high-riskindividuals and more recently, polysaccharidevaccine for all those aged 65 years or over. In thislatter group, the vaccine appears to be effective inreducing morbidity due to IPD, though discussionsare still ongoing on the protection it confers amongcertain at-risk categories which appear to be highlyvulnerable to pneumococcal disease.31 This paperdemonstrates a large burden due to pneumococcaldisease in both the elderly and high-risk categories.Ongoing surveillance will be critical to ascertain theimpact of these programs.
In addition, the 7-valent pneumococcal conju-gate vaccine also seems to reduce S. pneumoniaecolonisation and have an impact on the overalltransmission of the organism in the population,potentially providing protection to unvaccinatedpopulations (i.e. herd immunity).10,11,32 However,the potential threat of serotype replacement as aconsequence of vaccination, as seems to have beenobserved in the U.S.A.9 and in Finland,12 willrequire prospective monitoring for any changes inthe serotype distribution of pneumococcal diseasepatients and, ideally asymptomatic carriers. Thesefactors will have to be combined to disease burdendata to assist decision-makers in the most appro-priate intervention strategy with the pneumococcalconjugate vaccine in countries considering intro-duction. Moreover, results from cost-effectivenessanalyses showed that indirect effects such as herd
immunity and serotype replacement may have acrucial impact on the economic acceptability ofalternative programs.33,34
The serotype diversity of S. pneumoniae and itsmany clinical manifestations make it hard to answerquestions related to the short as well as long-termeffects that vaccination may have at the populationlevel. Here, we have attempted to give somebaseline information on the epidemiology of bothinvasive and non-invasive pneumococcal conditionand on the potential impact of the availablepneumococcal vaccines. Ongoing surveillance is inplace to assess any impact on disease epidemiologyof the current high-risk strategy in England andWales and to assist decisions on future vaccinationstrategy.
Acknowledgements
We would like to thank Dr Douglas Fleming of theRoyal College of General Practitioners Scheme forproviding consultation rates for CAP and AOM andthe DH for hospitalisation records. We also want tothank Pauline Kaye and Usha Gungabissoon for dataextraction. The MSGP4 are Crown Copyright and arereproduced with permission. The study was fundedby a grant from the EU (QLG4-CT-2000-00640).
References
1. Robinson K, Baugham W, Rothrock G, Barret NL, Pass M,Lexau C, et al. Epidemiology of invasive Streptococcus
A. Melegaro et al.48
pneumoniae infections in the United States, 1995–1998.Opportunities for prevention in the conjugate vaccine era.JAMA 2001;285(13):1729–35.
2. Cartwright K. Pneumococcal disease in Western Europe:burden of disease, antibiotic resistance and management.Eur J Pediatr 2002;161:188–95.
3. Usen S, Adegbola R, Mulholland K, Jaffar S, Hilton S,Oparaugo A, et al. Epidemiology of invasive pneumococcaldisease in the Western Region, The Gambia. Pediatr InfectDis J 1998;17(1):23–8.
4. Watt JP, O’Brien KL, Benin AL, Whitney CG, Robinson K,Parkinson AJ, et al. Invasive pneumococcal disease amongNavajo adults, 1989–1998. Clin Infect Dis 2004;38(4):496–501.
5. Brown PD, Lerner SA. Community-acquired pneumonia.Lancet 1998;352:1295–302.
6. Pelton SI. Acute otitis media in the era of effectivepneumococcal conjugate vaccine: will new pathogensemerge? Vaccine 2001;19:S96–S9.
7. Jacobs MR, Dagan R, Appelbaum PC, Burh DJ. Prevalence ofantimicrobial-resistant pathogens in middle ear fluid: multi-national study of 917 children with acute otitis media.Antimicrob Agents Chemother 1998;42(3):589–95.
8. Black SB, Shinefield HR, Fireman B, Lewis E, Ray P,Hansen JR, et al. Efficacy, safety and immunogenicity ofheptavalent pneumococcal conjugate vaccine in children.Pediatr Infect Dis J 2000;19:187–95.
9. Kaplan SL, Mason Jr EO, Wald ER, Schutze GE, Bradley JS,Tan TQ, et al. Decrease of invasive pneumococcal infectionsin children among 8 children’s hospitals in the United Statesafter the introduction of the 7-valent pneumococcalconjugate vaccine. Pediatrics 2004;113(3):443–9.
10. Black S, Shinefield H, Baxter R, Austrian R, Bracken L,Hansen J, et al. Postlicensure surveillance for pneumococcalinvasive disease after use of heptavalent pneumococcalconjugate vaccine in Northern California Kaiser Permanente.Pediatr Infect Dis J 2004;23(6):485–9.
11. Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM,Lynfield R, et al. Decline in invasive pneumococcal diseaseafter the introduction of protein-polysaccharide conjugatevaccine. N Engl J Med 2003;348(18):1737–46.
12. Eskola J, Kilpi T, Palmu A, Jokinen J, Haapakoski J, Herva E,et al. Efficacy of a pneumococcal conjugate vaccine againstacute otitis media. N Engl J Med 2001;344(6):403–9.
13. Fireman B, Black SB, Shinefield HR, Lee J, Lewis E, Ray P.Impact of the pneumococcal conjugate vaccine on otitismedia. Pediatr Infect Dis J 2003;22(1):10–16.
14. Black SB, Shinefield HR, Ling S, Hansen J, Fireman B,Spring D, et al. Effectiveness of heptavalent pneumococcalconjugate vaccine in children younger than five years of agefor prevention of pneumonia. Pediatr Infect Dis J 2002;21(9):810–5.
15. Poehling KA, Lafleur BJ, Szilagyi PG, Edwards KM, Mitchel E,Barth R, et al. Population-based impact of pneumococcalconjugate vaccine in young children. Pediatrics 2004;114(3):755–61.
16. CDC. Prevention of pneumococcal disease: recommen-dations of the advisory committee on immunisation prac-tices (ACIP). MMWR 1997;46(RR-08):1–24.
17. [www.dh.gov.uk] Salisbury D, Begg N. Immunisation againstinfectious disease. London: HMSO; 1996.
18. Miller E, Waight P, Efstratiou A, Brisson M, Johnson A,George R. Epidemiology of invasive and other pneumococcaldisease in children in England and Wales 1996–1998. ActaPaediatr Suppl 2000;435:11–16.
19. George R, Melegaro A. Invasive pneumococcal infectionEngland and Wales, 1999. CDR Weekly 2001;11(21):6–12.
20. Djuretic T, Ryan M, Miller E, Fairley CK, Goldblatt D. Hospitaladmission in children due to pneumococcal pneumonia inEngland. J Infect 1998;37:54–8.
21. Fleming DM. Weekly returns service of the Royal College ofGeneral Practitioners. Commun Dis Public Health 1999;2(2):96–100.
22. McCormick A, Fleming D, Charlton J. Morbidity statisticsfrom general practice, Fourth National Survey 1991–1992.London: Office of Population Census and Survey (SeriesMB5:3), HMSO: 1995.
23. Ryan M, Ramsay M, Brown D, Gay N, Farrington C, Wall P.Hospital admissions attributable to rotavirus infection inEngland and Wales. J Infect Dis 1996;174(Suppl 1):S12–S18.
24. Smith M, Stuart J, Andrews N, Telfer Brunton W,Cartwright K. Invasive pneumococcal infection in Southand West England. Epidemiol Infect 1998;120:117–23.
25. Laurichesse H, Grimaud O, Waight P, Johnson AP, George R,Miller E. Pneumococcal bacteremia and meningitis inEngland and Wales, 1993 to 1995. Commun Dis Public Health1998;1:22–7.
26. McIntosh EDG, Booy R. Invasive pneumococcal disease inEngland and Wales: what is the true burden and what is thepotential for prevention using 7 valent pneumococcalconjugate vaccine? Arch Dis Child 2002;86:403–6.
27. Muller-Pebody B, Edmunds W, Zambon M, Gay N,Crowcroft N. Contribution of RSV to bronchiolitis andpneumonia-associated hospitalizations in English children,April 1995–March 1998. Epidemiol Infect 2002;129:99–106.
28. Smith MD, Stuart J, Andrews NJ, Telfer Brunton WA,Cartwright KA. Invasive pneumococcal infection in Southand West England. Epidemiol Infect 1998;120:117–23.
29. Sleeman K, Knox K, George R, Miller E, Waight P, Griffiths D,et al. Invasive pneumococcal disease in England and Wales:vaccination implications. J Infect Dis 2001;183:239–46.
30. Kyaw MH, Clarke S, Jones IG, Campbell H. Incidence ofinvasive pneumococcal disease in Scotland, 1988–99. Epide-miol Infect 2002;128:139–47.
31. Melegaro A, Edmunds WJ. The 23-valent pneumococcalpolysaccharide vaccine/Part I—efficacy of PPV in the elderly:a comparison of meta-analyses. Eur J Epidemiol 2004;19(4):353–63.
32. Givon-Lavi N, Fraser D, Dagan R. Vaccination of day-carecenter attendees reduces carriage of Streptococcus pneu-moniae among their younger siblings. Pediatr Infect Dis J2003;22(6):524–32.
33. Melegaro A, Edmunds WJ. Cost effectiveness analysis ofpneumococcal conjugate vaccination in England and Wales.Vaccine 2004;22(31–33):4203–14.
34. McIntosh ED. Cost-effectiveness studies of pneumococcalconjugate vaccines. Expert Rev Vaccines 2004;3(4):433–42.
Related Documents











