The CTN Research Utilization Committee: Putting Dissemination Research into Practice Jeffrey Selzer, MD Chair, CTN Research Utilization Committee Long Island Regional Node, CTN North Shore-Long Island Jewish Health System Albert Einstein College of Medicine

The CTN Research Utilization Committee: Putting Dissemination Research into Practice Jeffrey Selzer, MD Chair, CTN Research Utilization Committee Long.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The CTN Research Utilization Committee: Putting
Dissemination Research into Practice
Jeffrey Selzer, MD
Chair, CTN Research Utilization Committee
Long Island Regional Node, CTN
North Shore-Long Island Jewish Health System
Albert Einstein College of Medicine

A research infrastructure of 16 RRTCs & 240 CTPs across 34 States, and Puerto RicoA research infrastructure of 16 RRTCs & 240 CTPs across 34 States, and Puerto RicoA research infrastructure of 16 RRTCs & 240 CTPs across 34 States, and Puerto RicoA research infrastructure of 16 RRTCs & 240 CTPs across 34 States, and Puerto Rico
Oregon NodeOregon NodeOHSUOHSU
Washington NodeWashington NodeU. WashingtonU. Washington
Pacific NodePacific NodeUCLAUCLA
Florida NodeFlorida NodeU. MiamiU. Miami
Tri stateTri stateU. PittsburghU. PittsburghOhio Valley NodeOhio Valley Node
U. CincinnatiU. Cincinnati
South Carolina NodeSouth Carolina NodeMUSCMUSC
North Carolina NodeNorth Carolina NodeDukeDuke
California/Arizona NodeCalifornia/Arizona NodeUCSF/U. ArizonaUCSF/U. Arizona
Southwest NodeSouthwest NodeU. New MexicoU. New Mexico
Northern NE NodeNorthern NE NodeMcLean/HarvardMcLean/Harvard
California/Arizona NodeCalifornia/Arizona NodeUCSF/U. ArizonaUCSF/U. Arizona
Southwest NodeSouthwest NodeU. New MexicoU. New Mexico
Northern NE NodeNorthern NE NodeMcLean/HarvardMcLean/Harvard
New England NodeNew England NodeYaleYaleNew York NodeNew York Node
NYUNYULong Island NodeLong Island Node
NY State Psych. Inst.NY State Psych. Inst.
Delaware Valley NodeDelaware Valley NodeU. PennsylvaniaU. Pennsylvania
MidMid--Atlantic NodeAtlantic NodeJHU/MCVJHU/MCV
Texas NodeTexas NodeUT SouthwesternUT Southwestern
National Drug Abuse TreatmentNational Drug Abuse TreatmentClinical Trials NetworkClinical Trials Network

Missions of the CTN: A. Conduct studies of behavioral, pharmacological and
integrated behavioral and pharmacological treatment interventions in rigorous, multi-site clinical trials to determine effectiveness across a broad range of community based treatment settings and diversified patient populations.
B. Timely transfer of the research results to clinicians, providers, their patients and the policy makers to improve the quality of drug abuse treatment throughout the country using science as the vehicle.
CTN strategic plan includes the importance of using the CTN as an infrastructure to study best approaches to disseminating treatment innovations.
Pending, Pending, Development & Development &
ReviewReview
Pending, Pending, Development & Development &
ReviewReview
Recruitment & Recruitment & Data Data
CollectionCollection
Recruitment & Recruitment & Data Data
CollectionCollectionFollow-UpFollow-UpFollow-UpFollow-Up
Data Analysis, Data Analysis, Publication, & Publication, & DisseminationDissemination
Data Analysis, Data Analysis, Publication, & Publication, & DisseminationDissemination
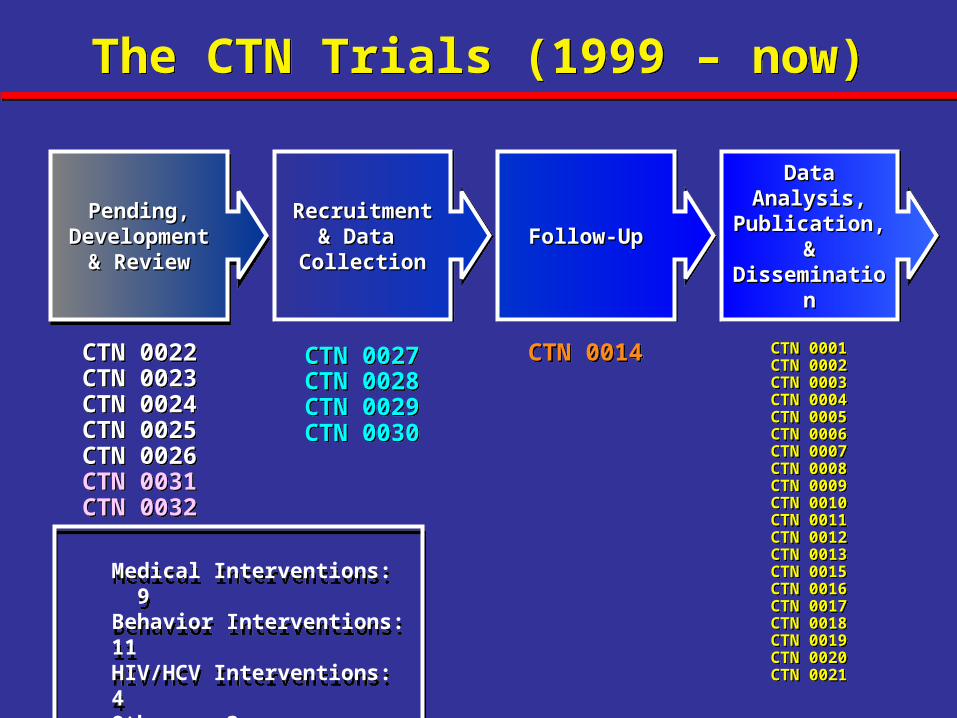
CTN 0027CTN 0028CTN 0029CTN 0030
CTN 0027CTN 0028CTN 0029CTN 0030
CTN 0014CTN 0014 CTN 0001CTN 0002CTN 0003CTN 0004CTN 0005CTN 0006CTN 0007CTN 0008CTN 0009CTN 0010CTN 0011CTN 0012CTN 0013CTN 0015CTN 0016CTN 0017CTN 0018CTN 0019CTN 0020CTN 0021
CTN 0001CTN 0002CTN 0003CTN 0004CTN 0005CTN 0006CTN 0007CTN 0008CTN 0009CTN 0010CTN 0011CTN 0012CTN 0013CTN 0015CTN 0016CTN 0017CTN 0018CTN 0019CTN 0020CTN 0021
CTN 0022CTN 0023CTN 0024CTN 0025CTN 0026CTN 0031CTN 0032
CTN 0022CTN 0023CTN 0024CTN 0025CTN 0026CTN 0031CTN 0032
The CTN Trials (1999 – now)The CTN Trials (1999 – now)
Medical Interventions: 9Behavior Interventions: 11HIV/HCV Interventions: 4Others: 3
Medical Interventions: 9Behavior Interventions: 11HIV/HCV Interventions: 4Others: 3

“I utilize the best from Freud, the best from Jung, and the best from my Uncle Marty, a very smart fellow.”

Patient Outcomes
Effective intervention practices
+Effective implementation practices
=
Good outcomes for Patients


Characteristics of an Innovation Which Is Most Easily Disseminated
(Everett Rogers, 2003):1. Confers a relative advantage compared with the current practice
2. Is compatible with other current practices
3. Is relatively simple to learn and implement
4. May be tried before making a commitment to adoption
5. Positive results are observable by the adopter
When innovations are adopted, “reinvention is inevitable.”


Widely Used Dissemination Approaches:
1. Conference presentations2. Workshops3. Distribution of printed manuals4. Performance feedback which does not occur in real-time
None of these commonly used approaches has been demonstrated to effectively promote dissemination of innovations .

Effective Strategy For Implementing a New Intervention
Three-step process– Provide opportunities to acquire basic knowledge
about intervention– Provide opportunities for practice with feedback– Provide expert coaching to improve performance
Not dissimilar from how interventions in research protocols are implemented (i.e., training with fidelity monitoring)

Conclusions reached by the RUC:
• Implementation of interventions throughout the CTN would require ongoing technical assistance (i.e., coaching)
• For implementation to occur, “maintenance was as important sales.”

Blending Initiative Initiative
• SAMHSA-NIDA Collaboration through ATTCsSAMHSA-NIDA Collaboration through ATTCs• BlendingTeam members include NIDA researchers
on a given intervention, community treatment programs with experience using the intervention, and Addiction Technology Transfer Center staff
• Blending products (Blending products (designed to promote adoptiondesigned to promote adoption): ): → Buprenorphine Awareness → Short-Term Opioid Withdrawal Using
Buprenorphine: Findings and strategies*→ SMART Treatment Planning: Utilizing the ASI→ MI Assessment: Supervisory Tools for
Enhancing Proficiency*→ Promoting Awareness of Motivational
Incentives* *Based on CTN Studies

CTN Research Utilization Workgroups:
• Motivational Interviewing
• Buprenorphine Treatment
• Motivational Incentives(Selection of interventions based on CTP
needs and by availability of Blending Products. Opportunity to “kick the tires” on the Blending Products.)

CTN Motivational Interviewing TrialCTN Motivational Interviewing Trial
• Patients (n=423) assigned to MI at intake subsequently completed more counseling sessions (mean=5.02, sd=5.15) than Standard Care patients (mean=4.03, sd=4.21) during 28 days after randomization (p<.05)
• MI patients more likely (84%) to still be enrolled at the program after one month than Standard Care patients (75%) (p<.04)
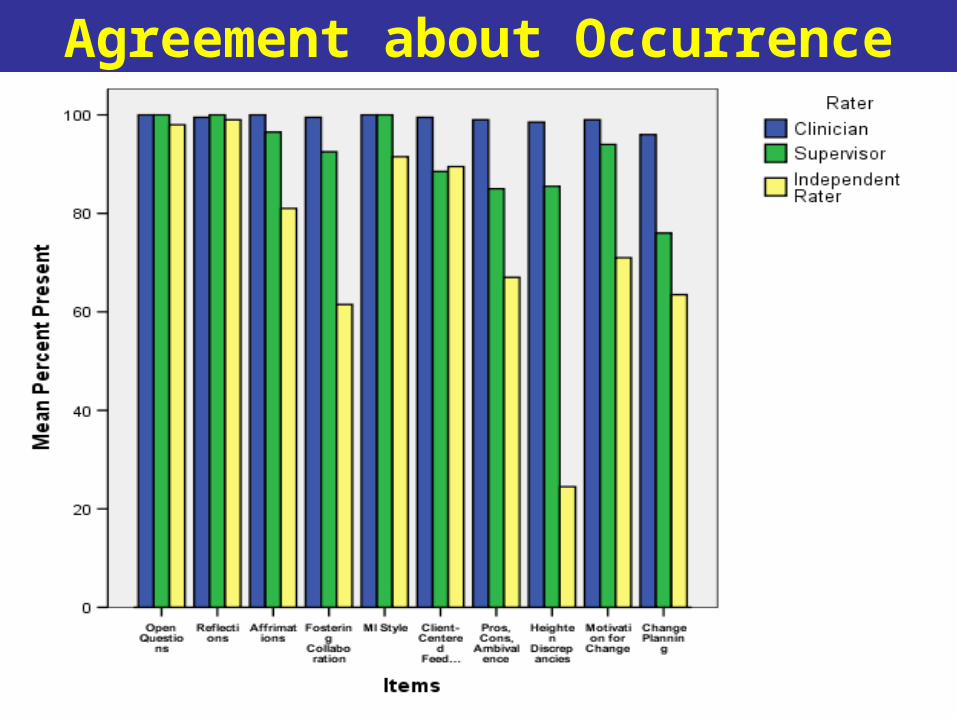
Agreement about Occurrence

M
I
A
STEP
MotivationalInterviewingAssessment:
Supervisory Tools forEnhancing Proficiency

MIA: STEP is…
– A multi-media tool kit for enhancing MI proficiency in clinicians already knowledgeable about MI (“The last thing we need is another MI training manual.” Bill Miller)
– A resource for supervisors to help them become more effective supervisors
– A supervisory model which emphasizes fidelity to the intervention and bringing actual clinical material into supervision

16 Rating ItemsMI Consistent • MI Style or Spirit
• Open-ended Questions
• Affirmations
• Reflections
• Fostering Collaboration
• Motivation to Change
• Developing Discrepancies
• Pros, Cons, and Ambivalence
• Change Planning Discussion
• Client-centered Feedback
MI Inconsistent
• Unsolicited Advice
• Emphasize Abstinence
• Direct Confrontation
• Powerlessness/Loss of Control
• Asserting Authority
• Closed-ended Questions

Motivational Interviewing Workgroup:
Bill Miller (Researcher who developed MI)
Steve Martino (Researcher in CTN MI study)
Steve Gallon (ATTC Director) Chris Farentinos (CTP Representative)
Train-the-Trainer in Use of the Blending Product
• Applicants from CTN Nodes and ATTCs had to first demonstrate MI proficiency using the MITI system.
• 51 applicants + 3 MIA: STEP trainers • 1/3 of the applicants were unable to demonstrate
MI proficiency in the first round • 26 passed from CTN/18 passed from ATTC by
the second round • Trained 42 individuals as MIA: STEP trainers

Training
• 2.5 days in Kansas City – sponsored by the ATTC National Office
• Product overview
• Step-by-step experiential walk-through of MIA: STEP
• Discussion of implementation issues

Roll-outs completed• Prince William County Community Services Board,
Virginia N = 17
• North Carolina Alcohol Drug Abuse Treatment Centers
N = 39
– Included psychiatrists, medical doctors, nurses, recreational therapists, SA counselors, social workers at three sites
• Hawaii State Providers N = 25
• ChangePoint, Oregon N = 5
• Baltimore, Maryland N = 6

Roll-outs completed
• Miami-Dade County/South Florida Provider Coalition, 240 supervisors trained
• 100 hardcopies with CDs have been distributed; NFATTC and Mid-Atlantic ATTC both have 200 copies.
• http://www.motivationalinterview.org/library/MIA-STEP.pdf is averaging 12,000 downloads per week!

Implementation Considerations
• MI training prerequisites• Individual vs. group supervision• Frequency• Setting-specific modifications• Agency support• State support• Curriculum/On-going consultations (CEUs)
• Support to train MIA: STEP

Where do we go from here?• Listserv – Mid-Atlantic ATTC?
• Ongoing technical assistance for trainers, including more practice sessions/co-ratings?
• Quarterly conference calls open to trainers and supervisors?
• Obligations of trainers and $ to support them?
• Annual training of trainers or link training to Blending Conference
• MI Proficiency standards: MITI or MIA: STEP and with what support?
• Establish point person for ATTC (Gallon?) and CTN (Martino?)
• How to monitor effectiveness of strategy?

What is missing?
99% = Investment in Intervention Research to develop solutions
1% = Investment in Implementation Research to make effective use of those solutions (Up from ¼% in 1977)
Implementation Research Underway in the CTN
• 7 Nodes• 12 Studies underway• Interventions: Motivational Interviewing; CBT;
TSF; Motivational Incentives; Process Improvement Strategies
• Implementation variables: role of fidelity measures; cultural adaptations; Web-based and interactive CD Rom-based training; factors promoting adoption after the end of CTN trials

Many thanks for your attention!
Related Documents











