The comparison of pre- and post-treatment 99m Tc HMPAO brain SPECT images in patients with obsessive-compulsive disorder Filiz Karada˘ g a , Nalan Kalkan O˘ guzhano˘ glu a,n , Do˘ gang ¨ un Y ¨ uksel b , Suna Kırac - b , C - i˘ gdem Cura a , Osman O ¨ zdel a , Figen Ates -ci a a Pamukkale University, Medical Faculty, Department of Psychiatry, Denizli 20100, Turkey b Pamukkale University, Medical Faculty, Department of Nuclear Medicine, Denizli 20100, Turkey article info Article history: Received 7 February 2011 Received in revised form 20 June 2012 Accepted 11 July 2012 Keywords: Obsessive-compulsive disorder SSRI Risperidone HMPAO-SPECT abstract The objective of the present study was to compare brain activation in patients with obsessive-compulsive disorder (OCD) who received pharmacotherapy (selective serotonin reuptake inhibitor (SSRI) or a SSRI– risperidone combination) with that in healthy controls using 99m Tc-hexamethyl propyleneamine oxime (HMPAO) brain single photon emission tomography (SPECT). Twelve OCD patients achieving clinical response (seven SSRI responders, five patients responded to SSRI plus risperidone) underwent post- treatment SPECT scan. The baseline regional cerebral blood flow (rCBF) was significantly reduced in a large part of the cerebral cortex and the left cingulate gyrus in OCD patients compared with controls. After a 50% reduction of the OCD symptoms, bilaterally increased rCBF in the thalamus showed a significant effect of time in both of the patient groups. In the remitted state, although rCBF in the cingulate gyrus did not differ in SSRI responders compared with controls, patients who responded to the combination of SSRI þ risperidone showed significant hypoperfusion in the left anterior cingulate gyrus. SSRI responders had normalized rCBF in the frontal region relative to the control group. Consequently, based on our results, we attribute the observed thalamic rCBF alteration to SSRI treatment. Our results also suggested that brain perfusion changes associated with clinical remission may differ across patient subgroups. & 2012 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Functional brain imaging studies have consistently shown a dysfunction of cortico-thalamo-striatal circuits in the pathophy- siology of obsessive-compulsive disorder (Saxena and Rauch, 2000). Findings have suggested functional abnormalities in the orbitofrontal cortex (OFC), thalamus, caudate nucleus and cingu- late gyrus of patients with obsessive-compulsive disorder (OCD) (Friedlander and Desrocher, 2006). These findings seem to be state- dependent, as successful treatment with a serotonin reuptake inhibitor (SRI) or behavioral therapy decreases the cerebral meta- bolism in these regions (Benkelfat et al., 1990; Swedo et al., 1992; Baxter et al., 1992; Perani et al., 1995; Rubin et al., 1995; Schwartz et al., 1996; Saxena et al., 1999, 2002). Although selective serotonin reuptake inhibitors (SSRIs) are the treatment of choice in OCD patients, as many as 40–60% of patients may not respond or may have only a partial response to these medications (Bloch et al., 2006; Pallanti and Quercioli, 2006). In such cases, the addition of a low dose atypical anti- psychotic, such as risperidone or olanzapine, to ongoing SSRI treatment has been shown to be effective (McDougle et al., 2000; Bystritsky et al., 2004). Only one-third of treatment-refractory OCD patients show a meaningful treatment response to anti- psychotic augmentation (Bloch et al., 2006). These differences suggest that OCD is a highly heterogeneous condition, and it is possible that there are biological differences among subgroups of OCD as defined by pharmacological response or symptom clusters (Gilbert et al., 2008; van den Heuvel et al., 2009; Sumitani et al., 2007; Buchsbaum et al., 2006). Two recent brain-imaging studies have suggested the presence of psychopharmacological subtypes within OCD. Sumitani et al. (2007) reported that OCD patients who responded to augmentation of SSRI treatment with an atypical antipsychotic (risperidone) had distinct biological abnormalities in the anterior cingulate. Buchsbaum et al. (2006) found that a successful treatment with an SSRI plus risperidone was associated with low relative metabolic rates in the striatum and high relative metabolic rates in the anterior cingulate gyrus in OCD patients who were nonrespondent to serotonin reuptake inhibitors. In order to understand the underlying pathophysiology and to investigate trait characteristics rather than state-dependent altera- tions, the comparison of brain activity between remitted OCD patients and healthy controls may be more valuable than only Contents lists available at SciVerse ScienceDirect journal homepage: www.elsevier.com/locate/psychresns Psychiatry Research: Neuroimaging 0925-4927/$ - see front matter & 2012 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.pscychresns.2012.07.005 n Correspondence to: Pamukkale University, Medical Faculty, Department of Psychiatry, Doktorlar Cad. No: 42/613, Denizli 20100, Turkey. Tel.: þ90 542 6309600; fax: þ90 258 2410040. E-mail addresses: [email protected], [email protected] (N. Kalkan O˘ guzhano˘ glu). Psychiatry Research: Neuroimaging 213 (2013) 169–177

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Psychiatry Research: Neuroimaging 213 (2013) 169–177
Contents lists available at SciVerse ScienceDirect
Psychiatry Research: Neuroimaging
0925-49
http://d
n Corr
Psychia
Tel.: þ9
E-m
noguzh
journal homepage: www.elsevier.com/locate/psychresns
The comparison of pre- and post-treatment 99mTc HMPAO brainSPECT images in patients with obsessive-compulsive disorder
Filiz Karadag a, Nalan Kalkan Oguzhanoglu a,n, Dogangun Yuksel b, Suna Kırac- b,C- igdem Cura a, Osman Ozdel a, Figen Ates-ci a
a Pamukkale University, Medical Faculty, Department of Psychiatry, Denizli 20100, Turkeyb Pamukkale University, Medical Faculty, Department of Nuclear Medicine, Denizli 20100, Turkey
a r t i c l e i n f o
Article history:
Received 7 February 2011
Received in revised form
20 June 2012
Accepted 11 July 2012
Keywords:
Obsessive-compulsive disorder
SSRI
Risperidone
HMPAO-SPECT
27/$ - see front matter & 2012 Elsevier Irelan
x.doi.org/10.1016/j.pscychresns.2012.07.005
espondence to: Pamukkale University, Med
try, Doktorlar Cad. No: 42/613, Denizli 20100
0 542 6309600; fax: þ90 258 2410040.
ail addresses: [email protected],
[email protected] (N. Kalkan Oguzhanoglu).
a b s t r a c t
The objective of the present study was to compare brain activation in patients with obsessive-compulsive
disorder (OCD) who received pharmacotherapy (selective serotonin reuptake inhibitor (SSRI) or a SSRI–
risperidone combination) with that in healthy controls using 99mTc-hexamethyl propyleneamine oxime
(HMPAO) brain single photon emission tomography (SPECT). Twelve OCD patients achieving clinical
response (seven SSRI responders, five patients responded to SSRI plus risperidone) underwent post-
treatment SPECT scan. The baseline regional cerebral blood flow (rCBF) was significantly reduced in a
large part of the cerebral cortex and the left cingulate gyrus in OCD patients compared with controls.
After a 50% reduction of the OCD symptoms, bilaterally increased rCBF in the thalamus showed a
significant effect of time in both of the patient groups. In the remitted state, although rCBF in the
cingulate gyrus did not differ in SSRI responders compared with controls, patients who responded to the
combination of SSRIþ risperidone showed significant hypoperfusion in the left anterior cingulate gyrus.
SSRI responders had normalized rCBF in the frontal region relative to the control group. Consequently,
based on our results, we attribute the observed thalamic rCBF alteration to SSRI treatment. Our results
also suggested that brain perfusion changes associated with clinical remission may differ across patient
subgroups.
& 2012 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Functional brain imaging studies have consistently shown adysfunction of cortico-thalamo-striatal circuits in the pathophy-siology of obsessive-compulsive disorder (Saxena and Rauch,2000). Findings have suggested functional abnormalities in theorbitofrontal cortex (OFC), thalamus, caudate nucleus and cingu-late gyrus of patients with obsessive-compulsive disorder (OCD)(Friedlander and Desrocher, 2006). These findings seem to be state-dependent, as successful treatment with a serotonin reuptakeinhibitor (SRI) or behavioral therapy decreases the cerebral meta-bolism in these regions (Benkelfat et al., 1990; Swedo et al., 1992;Baxter et al., 1992; Perani et al., 1995; Rubin et al., 1995; Schwartzet al., 1996; Saxena et al., 1999, 2002).
Although selective serotonin reuptake inhibitors (SSRIs) arethe treatment of choice in OCD patients, as many as 40–60% ofpatients may not respond or may have only a partial responseto these medications (Bloch et al., 2006; Pallanti and Quercioli,
d Ltd. All rights reserved.
ical Faculty, Department of
, Turkey.
2006). In such cases, the addition of a low dose atypical anti-psychotic, such as risperidone or olanzapine, to ongoing SSRItreatment has been shown to be effective (McDougle et al., 2000;Bystritsky et al., 2004). Only one-third of treatment-refractoryOCD patients show a meaningful treatment response to anti-psychotic augmentation (Bloch et al., 2006). These differencessuggest that OCD is a highly heterogeneous condition, and it ispossible that there are biological differences among subgroups ofOCD as defined by pharmacological response or symptom clusters(Gilbert et al., 2008; van den Heuvel et al., 2009; Sumitani et al.,2007; Buchsbaum et al., 2006). Two recent brain-imaging studieshave suggested the presence of psychopharmacological subtypeswithin OCD. Sumitani et al. (2007) reported that OCD patients whoresponded to augmentation of SSRI treatment with an atypicalantipsychotic (risperidone) had distinct biological abnormalities inthe anterior cingulate. Buchsbaum et al. (2006) found that asuccessful treatment with an SSRI plus risperidone was associatedwith low relative metabolic rates in the striatum and high relativemetabolic rates in the anterior cingulate gyrus in OCD patients whowere nonrespondent to serotonin reuptake inhibitors.
In order to understand the underlying pathophysiology and toinvestigate trait characteristics rather than state-dependent altera-tions, the comparison of brain activity between remitted OCDpatients and healthy controls may be more valuable than only
F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177170
comparing the pre- and post-treatment differences. We were able tocarry out a limited number of neuroimaging studies comparingremitted OCD patient with health individuals. Two of them havebeen reported by Nabeyama et al. (2008) and Lazaro et al. (2009).
The objective of the present study was to compare the brainactivity in OCD patients who responded to an SSRI trial and an SSRIplus an atypical antipsychotic drug (risperidone), using 99mTc-hexa-methyl propyleneamine oxime (HMPAO) brain SPECT (single photonemission computed tomography) imaging. According to our firsthypothesis consistent with the pathophysiological models of OCD,at the beginning OCD, patients would initially be expected to showabnormal brain perfusion in frontostriatal circuits as compared withthe healthy subjects as well as in other central and posterior brainregions in which abnormalities are reported less frequently. Secondly,OCD patients who respond to different pharmacotherapeutic regi-mens would be expected to show differential brain perfusion changesin the particular brain regions under treatment. And finally, besidesthe pre- and post-treatment changes, we also planned to comparebrain perfusion in two remitted patient groups with that in healthysubjects to examine whether brain perfusion in remitted patientsnormalized after positive treatment response.
2. Methods
2.1. Participants
Participants comprised 23 OCD patients and 10 healthy controls. All partici-
pants gave written informed consent to take part in the study after the procedures
were explained and all recommendations of the local ethical committee were met.
OCD patients were consecutively recruited from psychiatric outpatient clinics, and
control subjects were chosen among hospital staff. OCD and comorbid diagnoses
were established using the Structured Clinical Interview for DSM-IV (SCID-I) (First
et al., 1997; Ozkurkc- ugil et al., 1999). The patients had been drug-free for at least 2
weeks before the study; the patients included in the study had either never been
treated for OCD or had needed to be switched over from an ongoing SSRI therapy
to other medications due to intolerable side effects or ineffectiveness.
Patients completed the Yale-Brown Obsessive Compulsive Scale (Y-BOCS)
(Goodman et al., 1989) and Hamilton Depression Rating Scale (HDRS-17)
(Hamilton, 1960). Exclusion criteria for the patients were as follows: current
medical illness, lifetime history of alcohol or substance abuse or dependence,
history of head injury, epilepsy or any other neurological disease, or exposure to
any medication known to have a significant effect upon the central nervous
system in the 2 weeks preceding the study. Comorbid depression or any other
psychiatric diagnoses, e.g., panic disorder or generalized anxiety disorder, were
also considered as exclusion criteria for OCD patients. Exclusion criteria for the
control subjects were lifetime history of head injury or any DSM-IV Axis I
diagnosis, current medical problems, and current or prior neurological disease.
All subjects were right-handed.
2.2. 99mTc-HMPAO SPECT study
The participants rested in a supine position with closed eyes in a silent and
darkened room for approximately 20 min before radiopharmaceutical
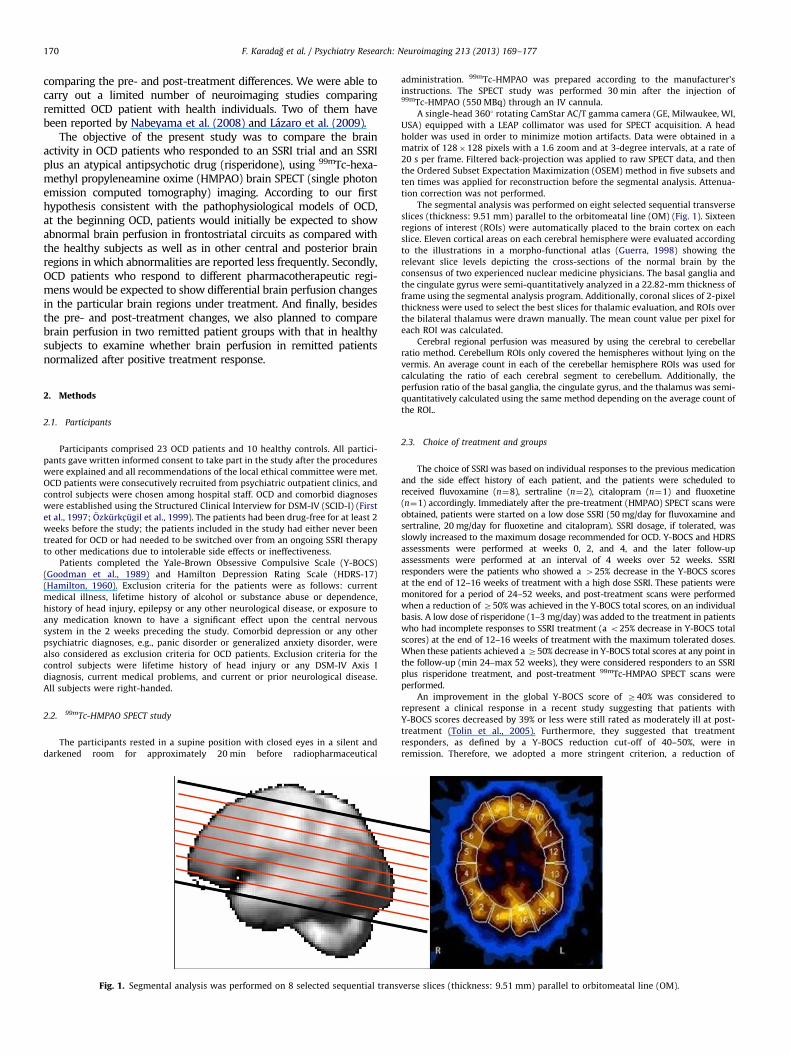
Fig. 1. Segmental analysis was performed on 8 selected sequential trans
administration. 99mTc-HMPAO was prepared according to the manufacturer’s
instructions. The SPECT study was performed 30 min after the injection of99mTc-HMPAO (550 MBq) through an IV cannula.
A single-head 3601 rotating CamStar AC/T gamma camera (GE, Milwaukee, WI,
USA) equipped with a LEAP collimator was used for SPECT acquisition. A head
holder was used in order to minimize motion artifacts. Data were obtained in a
matrix of 128�128 pixels with a 1.6 zoom and at 3-degree intervals, at a rate of
20 s per frame. Filtered back-projection was applied to raw SPECT data, and then
the Ordered Subset Expectation Maximization (OSEM) method in five subsets and
ten times was applied for reconstruction before the segmental analysis. Attenua-
tion correction was not performed.
The segmental analysis was performed on eight selected sequential transverse
slices (thickness: 9.51 mm) parallel to the orbitomeatal line (OM) (Fig. 1). Sixteen
regions of interest (ROIs) were automatically placed to the brain cortex on each
slice. Eleven cortical areas on each cerebral hemisphere were evaluated according
to the illustrations in a morpho-functional atlas (Guerra, 1998) showing the
relevant slice levels depicting the cross-sections of the normal brain by the
consensus of two experienced nuclear medicine physicians. The basal ganglia and
the cingulate gyrus were semi-quantitatively analyzed in a 22.82-mm thickness of
frame using the segmental analysis program. Additionally, coronal slices of 2-pixel
thickness were used to select the best slices for thalamic evaluation, and ROIs over
the bilateral thalamus were drawn manually. The mean count value per pixel for
each ROI was calculated.
Cerebral regional perfusion was measured by using the cerebral to cerebellar
ratio method. Cerebellum ROIs only covered the hemispheres without lying on the
vermis. An average count in each of the cerebellar hemisphere ROIs was used for
calculating the ratio of each cerebral segment to cerebellum. Additionally, the
perfusion ratio of the basal ganglia, the cingulate gyrus, and the thalamus was semi-
quantitatively calculated using the same method depending on the average count of
the ROI..
2.3. Choice of treatment and groups
The choice of SSRI was based on individual responses to the previous medication
and the side effect history of each patient, and the patients were scheduled to
received fluvoxamine (n¼8), sertraline (n¼2), citalopram (n¼1) and fluoxetine
(n¼1) accordingly. Immediately after the pre-treatment (HMPAO) SPECT scans were
obtained, patients were started on a low dose SSRI (50 mg/day for fluvoxamine and
sertraline, 20 mg/day for fluoxetine and citalopram). SSRI dosage, if tolerated, was
slowly increased to the maximum dosage recommended for OCD. Y-BOCS and HDRS
assessments were performed at weeks 0, 2, and 4, and the later follow-up
assessments were performed at an interval of 4 weeks over 52 weeks. SSRI
responders were the patients who showed a 425% decrease in the Y-BOCS scores
at the end of 12–16 weeks of treatment with a high dose SSRI. These patients were
monitored for a period of 24–52 weeks, and post-treatment scans were performed
when a reduction of Z50% was achieved in the Y-BOCS total scores, on an individual
basis. A low dose of risperidone (1–3 mg/day) was added to the treatment in patients
who had incomplete responses to SSRI treatment (a o25% decrease in Y-BOCS total
scores) at the end of 12–16 weeks of treatment with the maximum tolerated doses.
When these patients achieved a Z50% decrease in Y-BOCS total scores at any point in
the follow-up (min 24–max 52 weeks), they were considered responders to an SSRI
plus risperidone treatment, and post-treatment 99mTc-HMPAO SPECT scans were
performed.
An improvement in the global Y-BOCS score of Z40% was considered to
represent a clinical response in a recent study suggesting that patients with
Y-BOCS scores decreased by 39% or less were still rated as moderately ill at post-
treatment (Tolin et al., 2005). Furthermore, they suggested that treatment
responders, as defined by a Y-BOCS reduction cut-off of 40–50%, were in
remission. Therefore, we adopted a more stringent criterion, a reduction of
verse slices (thickness: 9.51 mm) parallel to orbitomeatal line (OM).
F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177 171
Z50% in the Y-BOCS total scores, for the clinical outcome of pharmacotherapy
than most of the previous studies.
Of the 23 patients, three patients were lost to follow-up during weeks 4 and 8;
four patients dropped out in follow-up visits because of lack of response to
treatment, and four patients did not give their consent for a post-treatment SPECT
scan despite clinical improvement. Finally, 12 OCD patients who achieved a
clinical response (seven patients responded to SSRI treatment and five patients
responded to SSRI plus risperidone) underwent post-treatment SPECT scans. The
results of this study were based on the data of those 12 patients (four men, eight
women) who completed the study.
2.4. Statistical analysis
Statistical analysis was performed using SPSS 15.0 version for Windows. Data
are presented as number or mean7standard deviation (mean7S.D.), where
appropriate. The differences between patients and control groups were examined
using the Chi Square test for categorical variables (i.e. gender). Continuous variables
(age, years of education, rCBF values) were compared using the Mann–Whitney U
test (where two groups are compared; patients vs. controls) and the Kruskal–Wallis
analysis of variance (where three groups are compared, OCD treatment groups vs.
controls). When there is a significant difference between groups in terms of any
variable on the Kruskal–Wallis analysis of variance, post-hoc comparison was
performed using the Mann–Whitney U test with the Bonferroni correction (sig-
nificance level considered as p¼0.050/3o0.016). The pre- and post-treatment rCBF
values of the OCD groups were analyzed using repeated measures of analysis of
variance (ANOVA) and undertaken time (pre–post-treatment) as the within-
subjects factor, and treatment groups (SSRI and SSRIþrisperidone group) as the
between-subject factor. The correlations between regional cerebral perfusion and
clinical rating scores were investigated by the partial correlation analysis for
controlling age and scan intervals.
3. Results
3.1. Clinical and sociodemographic characteristics
OCD patients who completed the study and the control groupwere not significantly different with respect to sociodemographiccharacteristics (Table 1). In addition, no significant difference wasobserved between the OCD patients who completed the study andthe drop-outs with respect to age (p¼0.443), gender (p¼0.467) andillness duration (p¼0.134). Clinical and demographic features of theSSRI and the SSRI plus risperidone groups are also summarized inTable 1. The SSRI plus risperidone group was younger than the SSRI
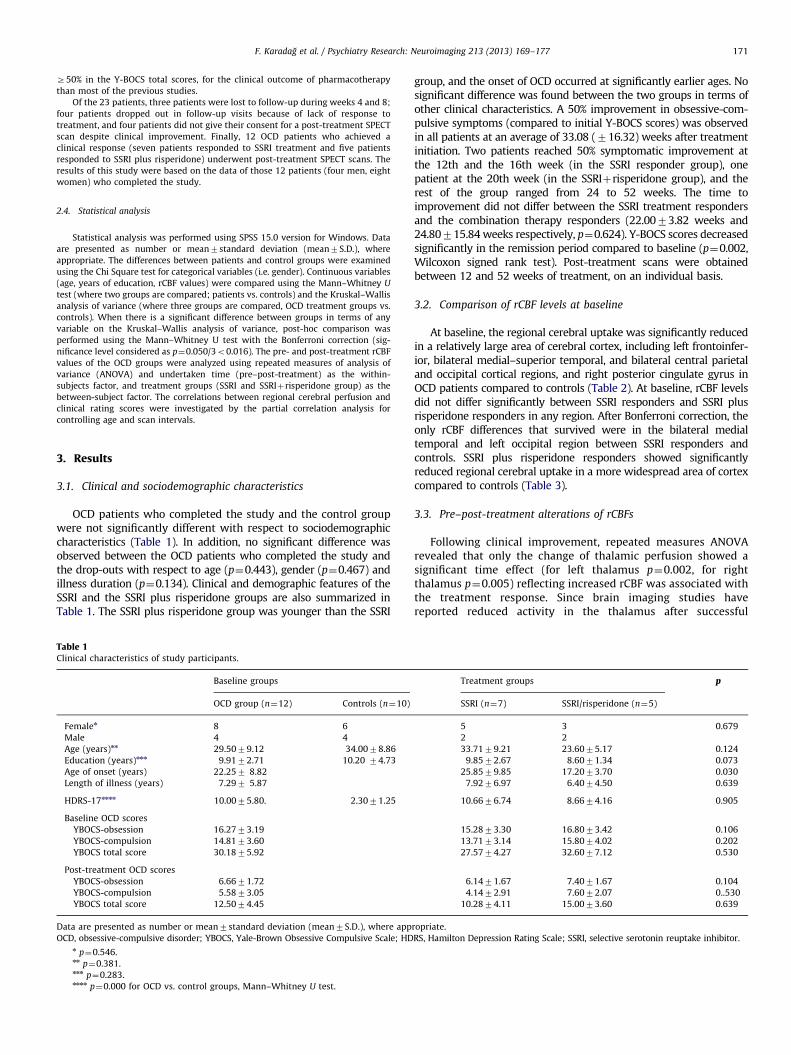
Table 1Clinical characteristics of study participants.
Baseline groups
OCD group (n¼12) Controls (n¼10)
Femalen 8 6
Male 4 4
Age (years)nn 29.5079.12 34.0078.86
Education (years)nnn 9.9172.71 10.20 74.73
Age of onset (years) 22.257 8.82
Length of illness (years) 7.297 5.87
HDRS-17nnnn 10.0075.80. 2.3071.25
Baseline OCD scores
YBOCS-obsession 16.2773.19
YBOCS-compulsion 14.8173.60
YBOCS total score 30.1875.92
Post-treatment OCD scores
YBOCS-obsession 6.6671.72
YBOCS-compulsion 5.5873.05
YBOCS total score 12.5074.45
Data are presented as number or mean7standard deviation (mean7S.D.), where app
OCD, obsessive-compulsive disorder; YBOCS, Yale-Brown Obsessive Compulsive Scale; HDn p¼0.546.nn p¼0.381.nnn p¼0.283.nnnn p¼0.000 for OCD vs. control groups, Mann–Whitney U test.
group, and the onset of OCD occurred at significantly earlier ages. Nosignificant difference was found between the two groups in terms ofother clinical characteristics. A 50% improvement in obsessive-com-pulsive symptoms (compared to initial Y-BOCS scores) was observedin all patients at an average of 33.08 (716.32) weeks after treatmentinitiation. Two patients reached 50% symptomatic improvement atthe 12th and the 16th week (in the SSRI responder group), onepatient at the 20th week (in the SSRIþrisperidone group), and therest of the group ranged from 24 to 52 weeks. The time toimprovement did not differ between the SSRI treatment respondersand the combination therapy responders (22.0073.82 weeks and24.80715.84 weeks respectively, p¼0.624). Y-BOCS scores decreasedsignificantly in the remission period compared to baseline (p¼0.002,Wilcoxon signed rank test). Post-treatment scans were obtainedbetween 12 and 52 weeks of treatment, on an individual basis.
3.2. Comparison of rCBF levels at baseline
At baseline, the regional cerebral uptake was significantly reducedin a relatively large area of cerebral cortex, including left frontoinfer-ior, bilateral medial–superior temporal, and bilateral central parietaland occipital cortical regions, and right posterior cingulate gyrus inOCD patients compared to controls (Table 2). At baseline, rCBF levelsdid not differ significantly between SSRI responders and SSRI plusrisperidone responders in any region. After Bonferroni correction, theonly rCBF differences that survived were in the bilateral medialtemporal and left occipital region between SSRI responders andcontrols. SSRI plus risperidone responders showed significantlyreduced regional cerebral uptake in a more widespread area of cortexcompared to controls (Table 3).
3.3. Pre–post-treatment alterations of rCBFs
Following clinical improvement, repeated measures ANOVArevealed that only the change of thalamic perfusion showed asignificant time effect (for left thalamus p¼0.002, for rightthalamus p¼0.005) reflecting increased rCBF was associated withthe treatment response. Since brain imaging studies havereported reduced activity in the thalamus after successful
Treatment groups p
SSRI (n¼7) SSRI/risperidone (n¼5)
5 3 0.679
2 2
33.7179.21 23.6075.17 0.124
9.8572.67 8.6071.34 0.073
25.8579.85 17.2073.70 0.030
7.9276.97 6.4074.50 0.639
10.6676.74 8.6674.16 0.905
15.2873.30 16.8073.42 0.106
13.7173.14 15.8074.02 0.202
27.5774.27 32.6077.12 0.530
6.1471.67 7.4071.67 0.104
4.1472.91 7.6072.07 0..530
10.2874.11 15.0073.60 0.639
ropriate.
RS, Hamilton Depression Rating Scale; SSRI, selective serotonin reuptake inhibitor.
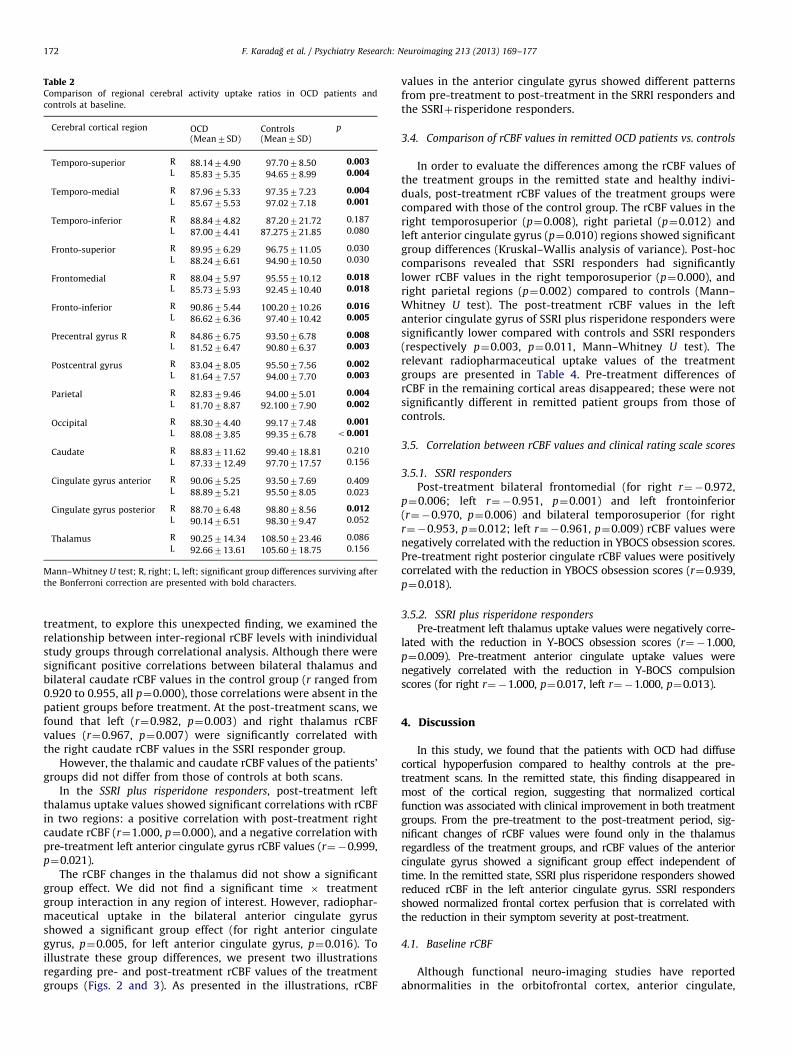
Table 2Comparison of regional cerebral activity uptake ratios in OCD patients and
controls at baseline.
Cerebral cortical region OCD Controls p
(Mean7SD) (Mean7SD)
Temporo-superior R 88.1474.90 97.7078.50 0.003L 85.8375.35 94.6578.99 0.004
Temporo-medial R 87.9675.33 97.3577.23 0.004L 85.6775.53 97.0277.18 0.001
Temporo-inferior R 88.8474.82 87.20721.72 0.187
L 87.0074.41 87.275721.85 0.080
Fronto-superior R 89.9576.29 96.75711.05 0.030
L 88.2476.61 94.90710.50 0.030
Frontomedial R 88.0475.97 95.55710.12 0.018L 85.7375.93 92.45710.40 0.018
Fronto-inferior R 90.8675.44 100.20710.26 0.016L 86.6276.36 97.40710.42 0.005
Precentral gyrus R R 84.8676.75 93.5076.78 0.008L 81.5276.47 90.8076.37 0.003
Postcentral gyrus R 83.0478.05 95.5077.56 0.002L 81.6477.57 94.0077.70 0.003
Parietal R 82.8379.46 94.0075.01 0.004L 81.7078.87 92.10077.90 0.002
Occipital R 88.3074.40 99.1777.48 0.001L 88.0873.85 99.3576.78 o0.001
Caudate R 88.83711.62 99.40718.81 0.210
L 87.33712.49 97.70717.57 0.156
Cingulate gyrus anterior R 90.0675.25 93.5077.69 0.409L 88.8975.21 95.5078.05 0.023
Cingulate gyrus posterior R 88.7076.48 98.8078.56 0.012L 90.1476.51 98.3079.47 0.052
Thalamus R 90.25714.34 108.50723.46 0.086
L 92.66713.61 105.60718.75 0.156
Mann–Whitney U test; R, right; L, left; significant group differences surviving after
the Bonferroni correction are presented with bold characters.
F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177172
treatment, to explore this unexpected finding, we examined therelationship between inter-regional rCBF levels with inindividualstudy groups through correlational analysis. Although there weresignificant positive correlations between bilateral thalamus andbilateral caudate rCBF values in the control group (r ranged from0.920 to 0.955, all p¼0.000), those correlations were absent in thepatient groups before treatment. At the post-treatment scans, wefound that left (r¼0.982, p¼0.003) and right thalamus rCBFvalues (r¼0.967, p¼0.007) were significantly correlated withthe right caudate rCBF values in the SSRI responder group.
However, the thalamic and caudate rCBF values of the patients’groups did not differ from those of controls at both scans.
In the SSRI plus risperidone responders, post-treatment leftthalamus uptake values showed significant correlations with rCBFin two regions: a positive correlation with post-treatment rightcaudate rCBF (r¼1.000, p¼0.000), and a negative correlation withpre-treatment left anterior cingulate gyrus rCBF values (r¼�0.999,p¼0.021).
The rCBF changes in the thalamus did not show a significantgroup effect. We did not find a significant time � treatmentgroup interaction in any region of interest. However, radiophar-maceutical uptake in the bilateral anterior cingulate gyrusshowed a significant group effect (for right anterior cingulategyrus, p¼0.005, for left anterior cingulate gyrus, p¼0.016). Toillustrate these group differences, we present two illustrationsregarding pre- and post-treatment rCBF values of the treatmentgroups (Figs. 2 and 3). As presented in the illustrations, rCBF
values in the anterior cingulate gyrus showed different patternsfrom pre-treatment to post-treatment in the SRRI responders andthe SSRIþrisperidone responders.
3.4. Comparison of rCBF values in remitted OCD patients vs. controls
In order to evaluate the differences among the rCBF values ofthe treatment groups in the remitted state and healthy indivi-duals, post-treatment rCBF values of the treatment groups werecompared with those of the control group. The rCBF values in theright temporosuperior (p¼0.008), right parietal (p¼0.012) andleft anterior cingulate gyrus (p¼0.010) regions showed significantgroup differences (Kruskal–Wallis analysis of variance). Post-hoccomparisons revealed that SSRI responders had significantlylower rCBF values in the right temporosuperior (p¼0.000), andright parietal regions (p¼0.002) compared to controls (Mann–Whitney U test). The post-treatment rCBF values in the leftanterior cingulate gyrus of SSRI plus risperidone responders weresignificantly lower compared with controls and SSRI responders(respectively p¼0.003, p¼0.011, Mann–Whitney U test). Therelevant radiopharmaceutical uptake values of the treatmentgroups are presented in Table 4. Pre-treatment differences ofrCBF in the remaining cortical areas disappeared; these were notsignificantly different in remitted patient groups from those ofcontrols.
3.5. Correlation between rCBF values and clinical rating scale scores
3.5.1. SSRI responders
Post-treatment bilateral frontomedial (for right r¼�0.972,p¼0.006; left r¼�0.951, p¼0.001) and left frontoinferior(r¼�0.970, p¼0.006) and bilateral temporosuperior (for rightr¼�0.953, p¼0.012; left r¼�0.961, p¼0.009) rCBF values werenegatively correlated with the reduction in YBOCS obsession scores.Pre-treatment right posterior cingulate rCBF values were positivelycorrelated with the reduction in YBOCS obsession scores (r¼0.939,p¼0.018).
3.5.2. SSRI plus risperidone responders
Pre-treatment left thalamus uptake values were negatively corre-lated with the reduction in Y-BOCS obsession scores (r¼�1.000,p¼0.009). Pre-treatment anterior cingulate uptake values werenegatively correlated with the reduction in Y-BOCS compulsionscores (for right r¼�1.000, p¼0.017, left r¼�1.000, p¼0.013).
4. Discussion
In this study, we found that the patients with OCD had diffusecortical hypoperfusion compared to healthy controls at the pre-treatment scans. In the remitted state, this finding disappeared inmost of the cortical region, suggesting that normalized corticalfunction was associated with clinical improvement in both treatmentgroups. From the pre-treatment to the post-treatment period, sig-nificant changes of rCBF values were found only in the thalamusregardless of the treatment groups, and rCBF values of the anteriorcingulate gyrus showed a significant group effect independent oftime. In the remitted state, SSRI plus risperidone responders showedreduced rCBF in the left anterior cingulate gyrus. SSRI respondersshowed normalized frontal cortex perfusion that is correlated withthe reduction in their symptom severity at post-treatment.
4.1. Baseline rCBF
Although functional neuro-imaging studies have reportedabnormalities in the orbitofrontal cortex, anterior cingulate,
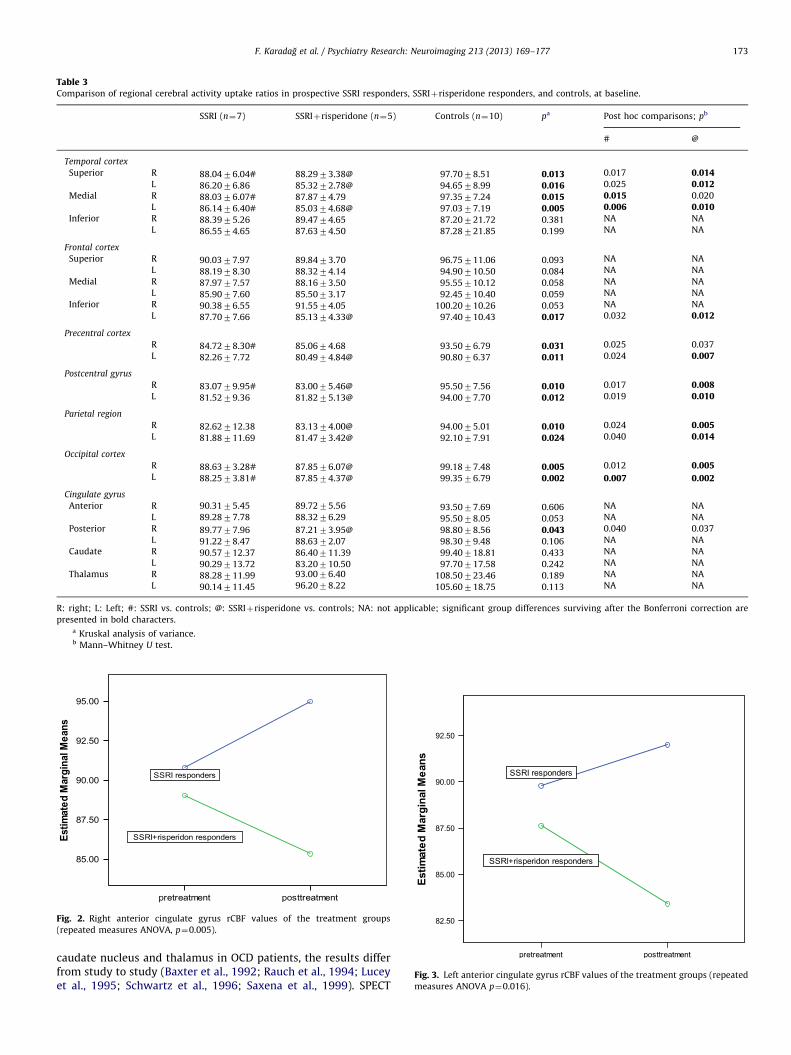
Table 3Comparison of regional cerebral activity uptake ratios in prospective SSRI responders, SSRIþrisperidone responders, and controls, at baseline.
SSRI (n¼7) SSRIþrisperidone (n¼5) Controls (n¼10) pa Post hoc comparisons; pb
# @
Temporal cortex
Superior R 88.0476.04# 88.2973.38@ 97.7078.51 0.013 0.017 0.014L 86.2076.86 85.3272.78@ 94.6578.99 0.016 0.025 0.012
Medial R 88.0376.07# 87.8774.79 97.3577.24 0.015 0.015 0.020
L 86.1476.40# 85.0374.68@ 97.0377.19 0.005 0.006 0.010Inferior R 88.3975.26 89.4774.65 87.20721.72 0.381 NA NA
L 86.5574.65 87.6374.50 87.28721.85 0.199 NA NA
Frontal cortex
Superior R 90.0377.97 89.8473.70 96.75711.06 0.093 NA NA
L 88.1978.30 88.3274.14 94.90710.50 0.084 NA NA
Medial R 87.9777.57 88.1673.50 95.55710.12 0.058 NA NA
L 85.9077.60 85.5073.17 92.45710.40 0.059 NA NA
Inferior R 90.3876.55 91.5574.05 100.20710.26 0.053 NA NA
L 87.7077.66 85.1374.33@ 97.40710.43 0.017 0.032 0.012
Precentral cortex
R 84.7278.30# 85.0674.68 93.5076.79 0.031 0.025 0.037
L 82.2677.72 80.4974.84@ 90.8076.37 0.011 0.024 0.007
Postcentral gyrus
R 83.0779.95# 83.0075.46@ 95.5077.56 0.010 0.017 0.008L 81.5279.36 81.8275.13@ 94.0077.70 0.012 0.019 0.010
Parietal region
R 82.62712.38 83.1374.00@ 94.0075.01 0.010 0.024 0.005L 81.88711.69 81.4773.42@ 92.1077.91 0.024 0.040 0.014
Occipital cortex
R 88.6373.28# 87.8576.07@ 99.1877.48 0.005 0.012 0.005L 88.2573.81# 87.8574.37@ 99.3576.79 0.002 0.007 0.002
Cingulate gyrus
Anterior R 90.3175.45 89.7275.56 93.5077.69 0.606 NA NA
L 89.2877.78 88.3276.29 95.5078.05 0.053 NA NA
Posterior R 89.7777.96 87.2173.95@ 98.8078.56 0.043 0.040 0.037
L 91.2278.47 88.6372.07 98.3079.48 0.106 NA NA
Caudate R 90.57712.37 86.40711.39 99.40718.81 0.433 NA NA
L 90.29713.72 83.20710.50 97.70717.58 0.242 NA NA
Thalamus R 88.28711.99 93.0076.40 108.50723.46 0.189 NA NA
L 90.14711.45 96.2078.22 105.60718.75 0.113 NA NA
R: right; L: Left; #: SSRI vs. controls; @: SSRIþrisperidone vs. controls; NA: not applicable; significant group differences surviving after the Bonferroni correction are
presented in bold characters.a Kruskal analysis of variance.b Mann–Whitney U test.
Fig. 2. Right anterior cingulate gyrus rCBF values of the treatment groups
(repeated measures ANOVA, p¼0.005).
Fig. 3. Left anterior cingulate gyrus rCBF values of the treatment groups (repeated
measures ANOVA p¼0.016).
F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177 173
caudate nucleus and thalamus in OCD patients, the results differfrom study to study (Baxter et al., 1992; Rauch et al., 1994; Luceyet al., 1995; Schwartz et al., 1996; Saxena et al., 1999). SPECT
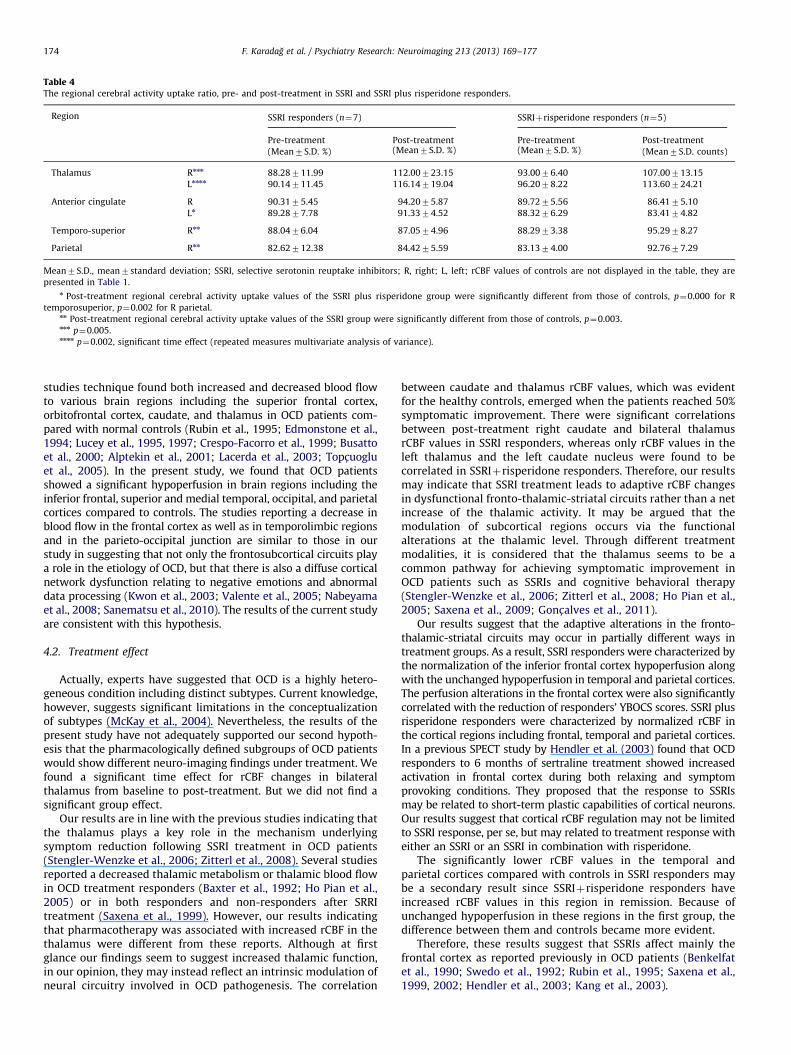
Table 4The regional cerebral activity uptake ratio, pre- and post-treatment in SSRI and SSRI plus risperidone responders.
Region SSRI responders (n¼7) SSRIþrisperidone responders (n¼5)
Pre-treatment Post-treatment Pre-treatment Post-treatment
(Mean7S.D. %) (Mean7S.D. %) (Mean7S.D. %) (Mean7S.D. counts)
Thalamus Rnnn 88.28711.99 112.00723.15 93.0076.40 107.00713.15
Lnnnn 90.14711.45 116.14719.04 96.2078.22 113.60724.21
Anterior cingulate R 90.3175.45 94.2075.87 89.7275.56 86.4175.10
Ln 89.2877.78 91.3374.52 88.3276.29 83.4174.82
Temporo-superior Rnn 88.0476.04 87.0574.96 88.2973.38 95.2978.27
Parietal Rnn 82.62712.38 84.4275.59 83.1374.00 92.7677.29
Mean7S.D., mean7standard deviation; SSRI, selective serotonin reuptake inhibitors; R, right; L, left; rCBF values of controls are not displayed in the table, they are
presented in Table 1.n Post-treatment regional cerebral activity uptake values of the SSRI plus risperidone group were significantly different from those of controls, p¼0.000 for R
temporosuperior, p¼0.002 for R parietal.nn Post-treatment regional cerebral activity uptake values of the SSRI group were significantly different from those of controls, p¼0.003.nnn p¼0.005.nnnn p¼0.002, significant time effect (repeated measures multivariate analysis of variance).
F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177174
studies technique found both increased and decreased blood flowto various brain regions including the superior frontal cortex,orbitofrontal cortex, caudate, and thalamus in OCD patients com-pared with normal controls (Rubin et al., 1995; Edmonstone et al.,1994; Lucey et al., 1995, 1997; Crespo-Facorro et al., 1999; Busattoet al., 2000; Alptekin et al., 2001; Lacerda et al., 2003; Topc-uogluet al., 2005). In the present study, we found that OCD patientsshowed a significant hypoperfusion in brain regions including theinferior frontal, superior and medial temporal, occipital, and parietalcortices compared to controls. The studies reporting a decrease inblood flow in the frontal cortex as well as in temporolimbic regionsand in the parieto-occipital junction are similar to those in ourstudy in suggesting that not only the frontosubcortical circuits playa role in the etiology of OCD, but that there is also a diffuse corticalnetwork dysfunction relating to negative emotions and abnormaldata processing (Kwon et al., 2003; Valente et al., 2005; Nabeyamaet al., 2008; Sanematsu et al., 2010). The results of the current studyare consistent with this hypothesis.
4.2. Treatment effect
Actually, experts have suggested that OCD is a highly hetero-geneous condition including distinct subtypes. Current knowledge,however, suggests significant limitations in the conceptualizationof subtypes (McKay et al., 2004). Nevertheless, the results of thepresent study have not adequately supported our second hypoth-esis that the pharmacologically defined subgroups of OCD patientswould show different neuro-imaging findings under treatment. Wefound a significant time effect for rCBF changes in bilateralthalamus from baseline to post-treatment. But we did not find asignificant group effect.
Our results are in line with the previous studies indicating thatthe thalamus plays a key role in the mechanism underlyingsymptom reduction following SSRI treatment in OCD patients(Stengler-Wenzke et al., 2006; Zitterl et al., 2008). Several studiesreported a decreased thalamic metabolism or thalamic blood flowin OCD treatment responders (Baxter et al., 1992; Ho Pian et al.,2005) or in both responders and non-responders after SRRItreatment (Saxena et al., 1999). However, our results indicatingthat pharmacotherapy was associated with increased rCBF in thethalamus were different from these reports. Although at firstglance our findings seem to suggest increased thalamic function,in our opinion, they may instead reflect an intrinsic modulation ofneural circuitry involved in OCD pathogenesis. The correlation
between caudate and thalamus rCBF values, which was evidentfor the healthy controls, emerged when the patients reached 50%symptomatic improvement. There were significant correlationsbetween post-treatment right caudate and bilateral thalamusrCBF values in SSRI responders, whereas only rCBF values in theleft thalamus and the left caudate nucleus were found to becorrelated in SSRIþrisperidone responders. Therefore, our resultsmay indicate that SSRI treatment leads to adaptive rCBF changesin dysfunctional fronto-thalamic-striatal circuits rather than a netincrease of the thalamic activity. It may be argued that themodulation of subcortical regions occurs via the functionalalterations at the thalamic level. Through different treatmentmodalities, it is considered that the thalamus seems to be acommon pathway for achieving symptomatic improvement inOCD patients such as SSRIs and cognitive behavioral therapy(Stengler-Wenzke et al., 2006; Zitterl et al., 2008; Ho Pian et al.,2005; Saxena et al., 2009; Gonc-alves et al., 2011).
Our results suggest that the adaptive alterations in the fronto-thalamic-striatal circuits may occur in partially different ways intreatment groups. As a result, SSRI responders were characterized bythe normalization of the inferior frontal cortex hypoperfusion alongwith the unchanged hypoperfusion in temporal and parietal cortices.The perfusion alterations in the frontal cortex were also significantlycorrelated with the reduction of responders’ YBOCS scores. SSRI plusrisperidone responders were characterized by normalized rCBF inthe cortical regions including frontal, temporal and parietal cortices.In a previous SPECT study by Hendler et al. (2003) found that OCDresponders to 6 months of sertraline treatment showed increasedactivation in frontal cortex during both relaxing and symptomprovoking conditions. They proposed that the response to SSRIsmay be related to short-term plastic capabilities of cortical neurons.Our results suggest that cortical rCBF regulation may not be limitedto SSRI response, per se, but may related to treatment response witheither an SSRI or an SSRI in combination with risperidone.
The significantly lower rCBF values in the temporal andparietal cortices compared with controls in SSRI responders maybe a secondary result since SSRIþrisperidone responders haveincreased rCBF values in this region in remission. Because ofunchanged hypoperfusion in these regions in the first group, thedifference between them and controls became more evident.
Therefore, these results suggest that SSRIs affect mainly thefrontal cortex as reported previously in OCD patients (Benkelfatet al., 1990; Swedo et al., 1992; Rubin et al., 1995; Saxena et al.,1999, 2002; Hendler et al., 2003; Kang et al., 2003).

F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177 175
The correlations between rCBF values in the thalamus and thecaudate under treatment showed some differences between thetreatment groups. These correlations came closer to those of healthyindividuals by virtue of the involvement of the bilateral thalamusand the right caudate.
The interpretation of these findings is not easy, since the rCBFvalues in these regions in OCD patients did not differ from those inhealthy individuals during either the pre-treatment or the post-treatment period. We also did not find any study reporting inter-regional rCBF correlations in OCD patients. However, abnormalactivity in the right caudate in OCD patients and its reversal withSSRI treatment has been reported in OCD patients (Apostolova et al.,2010; Hansen et al., 2002; Baxter et al., 1992). In the SSRI plusrisperidone responder group, findings were quite different from thosein the other groups due to the correlations of rCBF between right thecaudate and the left thalamus. SSRI plus risperidone responders maybe a subgroup representing a reduced capability for establishingneuronal connectivity compared to SSRI responders. A similar ideawas suggested by Hendler et al. (2003). They argued that SSRInonresponsive OCD patients may lack the capability for short-termcortical plasticity by SSRI due to mainly subcortical deficits. Consis-tent with this, an abnormal activity has been reported due to theabnormal neuronal metabolism in the right basal ganglia andthalamus associated with the lack of response to SSRI treatmentin OCD patients (Mohamed et al., 2007). Thus these patients mayrequire a more complex modulation of fronto-thalamic-striatalcircuits to achieve clinical improvement. Risperidone augmenta-tion may be mediated by increasing rCBF in several corticalregions as reported in patients with psychotic disorders (Breweret al., 2007; Narumoto et al., 2006). However, this interpretationshould be considered cautiously. It is also possible this increasein cortical activity is due to the effects of medication indepen-dently of clinical improvement. We cannot provide any con-clusive result since our sample lacked nonresponder patientsreceiving risperidone.
As a conclusion, one might argue that fronto-thalamic-striatalcircuits became reorganized through rCBF alteration in the thalamusunder different pharmacological treatment conditions. In this respectour findings have suggested the dysfunction of fronto-thalamic-striatal circuits or reduced functional connectivity in fronto-subcorticalcircuitry and their improvement with effective treatment in OCDpatients as in the previous studies (Graybiel and Rauch, 2000;Nabeyama et al., 2006; Jang et al., 2010; Hendler et al., 2003).However, functional connectivity studies have often used PET orfunctional magnetic resonance imaging. Therefore, it is open to debatewhether treatment-associated inter-regional rCBF correlations reflectfunctional connectivity. In our opinion, considering the presence ofinter-regional rCBF correlations in healthy controls and their emer-gence in the remitted state (not baseline) in OCD patients, it may bepossible.
We also found that rCBF values of the anterior cingulate gyrusshowed a significant group effect independent of time in repeatedmeasures of the ANOVA. Regonal CBF in the left anterior cingulategyrus showed a tendency to decrease in the SSRIþrisperidoneresponders at the baseline (p¼0.053) compared to the controls.That difference reached a significant level at post-treatmentcompared with healthy controls and SSRI responders. In contrast,there were no differences between SSRI responders and controlsregarding rCBF values in this region at the pre- and post-treat-ment scans. This may explain the group effect in the ANOVA.There are two brain imaging studies on OCD patients whorespond to the adjunctive use of risperidone or atypical antipsy-chotics, although they are quite different from the current studyregarding the brain imaging technique used, study design, andpatient characteristics (Sumitani et al., 2007; Buchsbaum et al.,2006). In one of the studies, brain imaging was performed after
treatment (Buchsbaum et al., 2006). However, these studies seemto agree that baseline metabolic abnormality in the anteriorcingulate may predict unresponsiveness to SSRI. The same suchtrend was observed in our study. In a placebo-controlled PETstudy by Buchsbaum et al. (2006) it was found that effectiverisperidone treatment was associated with significant increases inrelative metabolic rate in the striatum, cingulate gyrus, andorbitofrontal cortex in SSRI-refractory patients. However, thestudy did not include SRRI-responsive patients. They performedbaseline evaluations under SSRI treatment that reflected a lack ofresponsivity to SSRIs. We did not perform a SPECT scan in non-response status for the SSRI plus risperidone group. In addition,one of their patient groups was still symptomatic at the post-treatment period. In the present study both of the patient groupswere remitted at the end point. Therefore, it does not seempossible to directly compare our findings with those of this study.Our results indicate that along with the normalization of rCBF incerebral cortex, there is a limited connection between thalamusand basal ganglia and, there is reduced activity of cingulate gyrusas well as an inverse relationship between pre-treatment anteriorcingulate gyrus perfusion and the reduction of obsessive compul-sive symptoms in SSRIþrisperidone responders; these findingscan be explained in two ways: first, the responders to SSRI plusrisperidone may need a different neuromodulation involvementof the cingulate cortex within the frontostriatal circuit than wasrequired by the responders to SSRI alone. The beneficial effect ofneurosurgical interventions such as capsulotomy, subcaudatetractotomy, limbic leucotomy and anterior cingulotomy targetingthe connections between the thalamus and the subgenual andpregenual cingulate in treatment-refractory OCD patients sup-ports this opinion (Greenberg et al., 2010). The dopaminergicblockade effect of risperidone could have mediated such amodulation in the current study. Secondly, this treatment effectdata might be related to the effect of risperidone itself. Unfortu-nately, we cannot clarify this subject due to the lack of a SPECTscan in the response status in these patients. Nevertheless theexact nature of the modulator role of the anterior cingulate inclinical response is still unclear in SSRI-unresponsive OCDpatients. A larger sample of OCD patients with an unmedicatedbaseline, a single SSRI scan and the augmentation scan (and/or arisperidone first, SSRI augmentation arm) is really needed to fullyexplore this issue.
This treatment effect data might seem to contradict severalreports on reduced activation in prefrontal cortex and thalamusfollowing effective pharmacological or behavioral treatment inOCD (see review by Saxena and Rauch, 2000). However, thediscrepancy between studies might be related to the differencesamong post-treatment scan intervals and clinical improvementcriteria. In our study, post-treatment SPECT scans were performedafter a relatively longer period (for the majority of our patientsranging 20–52 weeks), compared to many previous studies (ran-ging 12–14 weeks). Longer or shorter duration of treatment maylead to different patterns of changes in regional cerebral blood flow(Saxena et al., 2009; Hendler et al., 2003; Han et al., 2011). Hendleret al. (2003) after prolonged SSRI treatment (6 months) in theirpatients have reported increased cortical activation associated withtreatment response in OCD, although many others have reportedthe opposite. Increased anterior cingulate activity has beenreported after successful brief intensive cognitive-behavioral ther-apy (CBT, 4 weeks) contrary to the standard CBT procedure (Saxenaet al., 2009). These suggest that acute and chronic effects oftreatment modalities may lead to different adaptive changes inthe fronto-thalamostriatal circuit. Our patients may be consideredas a sample being exposed to pharmacotherapy in a longer periodrepresenting remission status rather than treatment response. Wedefined treatment response as a decrease of 50% or more in the

F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177176
YBOCS scores, which is proposed as clinical remission criteria(Tolin et al., 2005). In most of the previous studies, treatmentresponse has been defined as a decrease of 25–35% in YBOCSscores.
5. Conclusion
We found a significant time effect for rCBF increase in bilateralthalamus from baseline to clinical remission in both the treat-ment groups. In remitted status, SSRI plus risperidone respondersshowed reduced rCBF in the left anterior cingulate gyrus whereasSSRI responders showed normalized perfusion in the inferiorfrontal cortex compared to the healthy controls. The hypoperfu-sion in the right superior temporal and parietal regions did notchange after treatment. These all have suggested that brainperfusion changes associated with clinical remission may differacross patient subgroups compared to the healthy individuals. Toour knowledge, there is no study investigating the brain imagingfindings associated with clinical remission in OCD patients. Indepressed patients, increases in prefrontal cortex and decreases insubgenual cingulate are critical for illness remission (Mayberg,2003). Despite a small sample size, the current study may beconsidered as a preliminary result on this issue regarding OCDpatients.
5.1. Limitations
Our study has some limitations. First, the sample size was smalland the applied thresholds were not fully corrected for multiplecomparisons. Thus our results may be difficult to generalizebecause of the limited statistical power and small sample size,further underscoring the need for replication. The low spatialresolution (9.51 mm) in the SPECT imaging and ROI-based analysisare among other important limitations of the present study. For theassessment of rCBF, voxel-based mapping methods are desirable,due to the fact that they are superior to the ROI-based methods. Butat the time of the study, we had the program package for evaluationof brain rCBF in a single-headed camera as the processor unit. Wedid not have voxel-based brain mapping program, and to maintainproject standards according to the ROI-based brain analysismethod, we have used the same camera and the method for allthe patients and controls. Another study also benefited from thesame method (Culha et al., 2008). There are also studies using ROI-based analysis methods (Buchsbaum et al., 1982; Alptekin et al.,2001).
Additionally, we failed to examine the treatment-refractorypatients due to the large drop-out rate. A study design requiring alonger follow-up period may have a negative effect on patients’compliance to the study protocol.
On the other hand, the evaluation of pre- and post-treatmentchanges in OCD patients who achieved remission and the com-parison of their results with healthy controls are the mainadvantages of the present study.
Acknowledgments
This study was supported by the Committee of ScientificResearch Project of Pamukkale University, School of Medicine(Project acceptance no. 07.11.2002/01).
References
Alptekin, K., Degirmenci, B., Kivircik, B., Durak, H., Yemez, B., Derebek, E., Tunca, Z.,2001. Tc-99m HMPAO brain perfusion SPECT in drug-free obsessive-
compulsive patients without depression. Psychiatry Research: Neuroimaging107, 51–56.
Apostolova, I., Block, S., Buchert, R., Osen, B., Conradi, M., Tabrizian, S., Gensichen,S., Schroder-Hartwig, K., Fricke, S., Rufer, M., Weiss, A., Hand, I., Clausen, M.,Obrocki, J., 2010. Effects of behavioral therapy or pharmacotherapy on brainglucose metabolism in subjects with obsessive-compulsive disorder asassessed by brain FDG PET. Psychiatry Research: Neuroimaging 184, 105–116.
Baxter, L.R., Schwartz, J.M., Bergman, K.S., Szuba, M.P., Guze, B.H., Mazziotta, J.C.,Alazraki, A., Selin, C.E., Ferng, H.K., Munford, P., 1992. Caudate glucosemetabolic rate changes with both drug and behavior therapy for obsessive-compulsive disorder. Archives of General Psychiatry 49, 681–689.
Benkelfat, C., Nordahl, T.E., Semple, W.E., King, A.C., Murphy, D.L., Cohen, R.M.,1990. Local cerebral glucose metabolic rates in obsessive-compulsive disorder.Patients treated with clomipramine. Archives of General Psychiatry 47, 840–848.
Bloch, M.H., Landeros-Weisenberger, A., Kelmendi, B., Coric, V., Bracken, M.B.,Leckman, J.F., 2006. A systematic review: antipsychotic augmentation withtreatment refractory obsessive-compulsive disorder. Molecular Psychiatry 11,622–632.
Brewer, W.J., Yucel, M., Harrison, B.J., McGorry, P.D., Olver, J., Egan, G.F., Velakoulis,D., Pantelis, C., 2007. Increased prefrontal cerebral blood flow in first-episodeschizophrenia following treatment: longitudinal positron emission tomogra-phy study. Australian New Zealand Journal of Psychiatry 41, 129–135.
Buchsbaum, M.S., Ingvar, D.H., Kessler, R., Waters, R.N., Cappelletti, J., van Kam-men, D.P., King, A.C., Johnson, J.L., Manning, R.G., Flynn, R.W., Mann, L.S.,Bunney Jr, W.E., Sokoloff, L., 1982. Cerebral glucography with positrontomography. Use in normal subjects and in patients with schizophrenia.Archives of General Psychiatry 39, 251–259.
Buchsbaum, M.S., Hollander, E., Pallanti, S., Baldini Rossi, N, Platholi, J., Newmark,R., Bloom, R., Sood, E., 2006. Positron emission tomography imaging ofrisperidone augmentation in serotonin reuptake inhibitor-refractory patients.Neuropsychobiology 53, 157–168.
Busatto, G.F., Zamignani, D.R., Buchpiguel, C.A., Garrido, G.E.J., Glabus, M.F., Rocha,E.T., Maia, A.F., Rosario-Campos, M.C., Campi Castro, C., Furuie, S.S., Gutierrez,M.A., McGuire, P.K., Miguel, E.C., 2000. A voxel-based investigation of regionalcerebral blood flow abnormalities in obsessive–compulsive disorder usingsingle photon emission computed tomography (SPECT). Psychiatry Research:Neuroimaging 99, 15–27.
Bystritsky, A., Ackerman, D.L., Rosen, R.M., Vapnik, T., Gorbis, E., Maidment, K.M.,Saxena, S., 2004. Augmentation of serotonin reuptake inhibitors in refractoryobsessive-compulsive disorder using adjunctive olanzapine: a placebo-con-trolled trial. Journal of Clinical Psychiatry 65, 565–568.
Crespo-Facorro, B., Cabranes, J.A., Lopez-Ibor Alcocer, M.I., Paya, B., FernandezPerez, C., Encinas, M., Ayuso Mateos, J.L., Lopez-Ibor, J.J., 1999. Regionalcerebral blood flow in obsessive-compulsive patients with and without achronic tic disorder. A SPECT study. European Archives of Psychiatry ClinicalNeuroscience 249, 156–161.
Culha, A.F., Osman, O., Dogangun, Y., Filiz, K., Suna, K., Kalkan, O.N., Gulfizar, V.,Beyza, A., 2008. Changes in regional cerebral blood flow demonstrated by99mTc-HMPAO SPECT in euthymic bipolar patients. European Archives ofPsychiatry Clinical Neuroscience 258, 144–151.
Edmonstone, Y., Austin, M.P., Prentice, N., Dougall, N., Freeman, C.P., Ebmeier, K.P.,Goodwin, G.M., 1994. Uptake of 99mTc-exametazime shown by single photonemission computerized tomography in obsessive-compulsive disorder com-pared with major depression and normal controls. Acta Psychiatrica Scandi-navica 90, 298–303.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1997. Structured ClinicalInterview for DSM-IV Clinical Version (SCID-I/CD). American Psychiatric Press,Washington, DC.
Friedlander, L., Desrocher, M., 2006. Neuroimaging studies of obsessive-compul-sive disorder in adults and children. Clinical Psychology Review 26, 32–49.
Gilbert, A.R., Mataix-Cols, D., Almeida, J.R., Lawrence, N., Nutche, J., Diwadkar, V.,Keshavan, M.S., Phillips, M.L., 2008. Brain structure and symptom dimensionrelationships in obsessive-compulsive disorder: a voxel-based morphometrystudy. Journal of Affective Disorders 109, 117–126.
Gonc-alves, O.F., Carvalho, S., Leite, J., Pocinho, F., Relvas, J., Fregni, F., 2011.Obsessive compulsive disorder as a functional interhemispheric imbalanceat the thalamic level. Medical Hypotheses 77, 445–447.
Goodman, W.K., Price, L.H., Rasmussen, S.A., Mazure, C., Fleischmann, R.L., Hill, C.L.,Heninger, G.R., Charney, D.S., 1989. The Yale-Brown Obsessive CompulsiveScale. I. Development, use, and reliability. Archives of General Psychiatry 46,1006–1011.
Graybiel, A.M., Rauch, S.L., 2000. Toward a neurobiology of obsessive compulsivedisorder. Neuron 28, 343–347.
Greenberg, B.D., Rauch, S.L., Haber, S.N., 2010. Invasive circuitry-based neuro-therapeutics: stereotactic ablation and deep brain stimulation for OCD.Neuropsychopharmacology 35, 317–336.
Guerra, UP (Ed.), 1998. Brain SPECT: A Normal Brain Morphofunctional Atlas.Gruppoimmagine, Roma.
Hamilton, M., 1960. A rating scale for depression. Journal of Neurology, Neurosurgery,and Psychiatry 23, 56–62.
Han, J.Y., Kang, D.H., Gu, B.M., Jung, W.H., Choi, J.S., Choi, C.H., Jang, J.H., Kwon, J.S.,2011. Altered brain activation in ventral frontal-striatal regions following a16-week pharmacotherapy in unmedicated obsessive-compulsive disorder.Journal of Korean Medical Science 26, 665–674.
Hansen, E.S., Hasselbalch, S., Law, I., Bolwig, T.G., 2002. The caudate nucleus inobsessive-compulsive disorder. Reduced metabolism following treatment

F. Karadag et al. / Psychiatry Research: Neuroimaging 213 (2013) 169–177 177
with paroxetine: a PET study. International Journal Neuropsychopharmacol-ogy 5, 1–10.
Hendler, T., Goshen, E., Tzila Zwas, S., Sasson, Y., Gal, G., Zohar, J., 2003. Brainreactivity to specific symptom provocation indicates prospective therapeuticoutcome in OCD. Psychiatry Research: Neuroimaging 124, 87–103.
Ho Pian, K.L., van Megen, H.J., Ramsey, N.F., Mandl, R., van Rijk, P.P., Wynne, H.J.,Westenberg, H.G., 2005. Decreased thalamic blood flow in obsessive compul-sive disorder patients responding to fluvoxamine. Psychiatry Research: Neu-roimaging 138, 89–97.
Jang, J.H., Kim, J.H., Jung, W.H., Choi, J.S., Jung, M.H., Lee, J.M., Choi, C.H., Kang, D.H.,Kwon, J.S., 2010. Functional connectivity in fronto-subcortical circuitry duringthe resting state in obsessive-compulsive disorder. Neuroscience Letters 474,158–162.
Kang, D,H., Kwon, J.S., Kim, J.J., Youn, T., Park, H.J., Kim, M.S., Lee, D.S., Lee, M.C.,2003. Brain glucose metabolic changes associated with neuropsychologicalimprovements after 4 months of treatment in patients with obsessive-compulsive disorder. Acta Psychiatrica Scandinavica 107, 291–297.
Kwon, J.S., Kim, J.J., Lee, D.W., Lee, J.S., Lee, D.S., Kim, M.S., Lyoo, I.K., Cho, M.J.,Lee, M.C., 2003. Neural correlates of clinical symptoms and cognitive dysfunc-tions in obsessive-compulsive disorder. Psychiatry Research: Neuroimaging122, 37–47.
Lacerda, A.L., Dalgalarrondo, P., Caetano, D., Camargo, E.E., Etchebehere, E.C.,Soares, J.C., 2003. Elevated thalamic and prefrontal regional cerebral bloodflow in obsessive-compulsive disorder: a SPECT study. Psychiatry Research:Neuroimaging 123, 125–134.
Lazaro, L., Bargallo, N., Castro-Fornieles, J., Falcon, C., Andres, S., Calvo, R., Junque, C.,2009. Brain changes in children and adolescents with obsessive-compulsivedisorder before and after treatment: a voxel-based morphometric MRI study.Psychiatry Research: Neuroimaging 172, 140–146.
Lucey, J.V., Costa, D.C., Blanes, T., Busatto, G.F., Pilowsky, L.S., Takei, N., Marks, I.M.,Ell, P.J., Kerwin, R.W., 1995. Regional cerebral blood flow in obsessive-compulsive disordered patients at rest. Differential correlates with obsessive-compulsive and anxious-avoidant dimensions. British Journal of Psychiatry 167,629–634.
Lucey, J.V., Costa, D.C., Adshead, G., Deahl, M., Busatto, G., Gacinovic, S., Travis, M.,Pilowsky, L., Ell, P.J., Marks, I.M., Kerwin, R.W., 1997. Brain blood flow inanxiety disorders. OCD, panic disorder with agoraphobia, and post-traumaticstress disorder on 99mTcHMPAO single photon emission tomography (SPET).The British Journal of Psychiatry 171, 346–350.
McDougle, C.J., Epperson, C.N., Pelton, G.H., Wasylink, S., Price, L.H., 2000.A double-blind, placebo-controlled study of risperidone addition in serotoninreuptake inhibitor-refractory obsessive-compulsive disorder. Archives ofGeneral Psychiatry 57, 794–801.
McKay, D., Abramowitz, J.S., Calamari, J.E., Kyrios, M., Radomsky, A., Sookman, D.,Taylor, S., Wilhelm, S., 2004. A critical evaluation of obsessive–compulsivedisorder subtypes: symptoms versus mechanisms. Clinical Psychology Review24, 283–313.
Mayberg, H.S., 2003. Modulating dysfunctional limbic-cortical circuits in depres-sion: towards development of brain-based algorithms for diagnosis andoptimised treatment. British Medical Bulletin 65, 193–207.
Mohamed, M.A., Smith, M.A., Schlund, M.W., Nestadt, G., Barker, P.B., Hoehn-Saric, R.,2007. Proton magnetic resonance spectroscopy in obsessive-compulsive disorder:a pilot investigation comparing treatment responders and non-responders.Psychiatry Research: Neuroimaging 156, 175–179.
Nabeyama, M., Nakagawa., A., Yoshiura, T., Nakao, T., Nakatani, E., Togao, O.,Yoshizato, C., Yoshioka, K., Tomita, M., Kanba, S., 2008. Functional MRI study ofbrain activation alterations in patients with obsessive-compulsive disorderafter symptom improvement. Psychiatry Research: Neuroimaging 163,236–247.
Narumoto, J., Ueda, H., Tsuchida, H., Yamashita, T., Kitabayashi, Y., Fukui, K., 2006.Regional cerebral blood flow changes in a patient with delusional parasitosisbefore and after successful treatment with risperidone: a case report. Pro-gressive Neuropsychopharmacology & Biological Psychiatry 30, 737–740.
Ozkurkc- ugil, A., Aydemir, O., Yıldız., M., Esen Danacı., A., Koroglu., E., 1999. DSM-IVEksen I bozuklukları ic- in yapılandırılmıs- klinik gorus-menin Turkc-eye uyarlan-ması ve guvenilirlik c-alıs-ması. _Ilac- ve Tedavi Dergisi 12, 233–236.
Pallanti, S., Quercioli, L., 2006. Treatment-refractory obsessive-compulsive dis-order: methodological issues, operational definitions and therapeutic lines.Progress in Neuropsychopharmacol Biological Psychiatry 30, 400–412.
Perani, D., Colombo, C., Bressi, S., Bonfanti, A., Grassi, F., Scarone, S., Bellodi, L.,Smeraldi, E., Fazio, F., 1995. [F-18] FDG PET study in obsessive-compulsivedisorder—a clinical/metabolic clinical/metabolic correlation study after treat-ment. British Journal of Psychiatry 166, 244–250.
Rauch, S.L., Jenike, M.A., Alpert, N.M., Baer, L., Breiter, H.C., Savage, C.R., Fischman, A.J.,1994. Regional cerebral blood flow measured during symptom provocation inobsessive-compulsive disorder using oxygen 15-labeled carbon dioxide andpositron emission tomography. Archives of General Psychiatry 51, 62–70.
Rubin, R.T., Ananth, J., Villanueva-Meyer, J., Trajmar, P.G., Mena, I., 1995. Regionalxenon-133 cerebral blood flow and cerebral Tc-99m-HMPAO uptake inpatients with obsessive-compulsive disorder before and during treatment.Biological Psychiatry 38, 429–437.
Sanematsu, H., Nakao, T., Yoshiura, T., Nabeyama, M., Togao, O., Tomita, M.,Masuda, Y., Nakatani, E., Nakagawa, A., Kanba, S., 2010. Predictors of treatmentresponse to fluvoxamine in obsessive-compulsive disorder: an fMRI study.Journal of Psychiatry Research 44, 193–200.
Saxena, S., Brody, A.L., Maidment, K.M., Dunkin, J.J., Colgan, M., Alborzian, S.,Phelps, M.E., Baxter Jr., L.R., 1999. Localized orbitofrontal and subcorticalmetabolic changes and predictors of response to paroxetine treatment inobsessive-compulsive disorder. Neuropsychopharmacology 21, 683–693.
Saxena, S., Rauch, S.L., 2000. Functional neuroimaging and the neuroanatomy ofobsessive-compulsive disorder. Psychiatric Clinics of North America 23,563–586.
Saxena, S., Brody, A.L., Ho, M.L., Alborzian, S., Maidment, K.M., Zohrabi, N., Ho, M.K.,Huang, S., Wu, H., Baxter Jr., L.R., 2002. Differential cerebral metabolic changeswith paroxetine treatment of obsessive-compulsive disorder vs. major depres-sion. Archives of General Psychiatry 59, 250–261.
Saxena, S., Gorbis, E., O’Neill, J., Baker, S.K., Mandelkern, M.A., Maidment, K.M.,Chang, S., Salamon, N., Brody, A.L., Schwartz, J.M., London, E.D., 2009.Rapid effects of brief intensive cognitive-behavioral therapy on brainglucose metabolism in obsessive-compulsive disorder. Molecular Psychiatry14, 197–205.
Schwartz, J.M., Stoessel, P.W., Baxter, L.R., Martin, K.M., Phelps, M.E., 1996.Systematic changes in cerebral glucose metabolic rate after successful beha-vior modification treatment of obsessive- compulsive disorder. Archives ofGeneral Psychiatry 53, 109–113.
Sumitani, S., Harada, M., Kubo, H., Ohmori, T., 2007. Proton magnetic resonancespectroscopy reveals an abnormality in the anterior cingulate of a subgroup ofobsessive-compulsive disorder patients. Psychiatry Research: Neuroimaging154, 85–92.
Stengler-Wenzke, K., Muller, U., Barthel, H., Angermeyer, M.C., Sabri, O., Hesse, S.,2006. Serotonin transporter imaging with [123I]beta-CIT SPECT before andafter one year of citalopram treatment of obsessive-compulsive disorder.Neuropsychobiology 53, 40–45.
Swedo, S.E., Pietrini, P., Leonard, H.L., Schapiro, M.B., Rettew, D.C., Goldberger, E.L.,Rapoport, S.I., Rapoport, J.L., Grady, C.L., 1992. Cerebral glucose metabolismin childhood-onset obsessive-compulsive disorder. Revisualization duringpharmacotherapy. Archives of General Psychiatry 49, 690–694.
Tolin, D.F., Abramowitz, J.S., Diefenbach, G.J., 2005. Defining response in clinicaltrials for obsessive–compulsive disorder: a signal detection analysis of theYale-Brown Obsessive Compulsive Scale. Journal of Clinical Psychiatry 66,1549–1557.
Topc-uoglu, V., Comert, B., Karabekiroglu, A., Dede, F., Erdil, T.Y., Turoglu, H.T., 2005.Right basal ganglion hypoperfusion in obsessive compulsive disorder patientsdemonstrated by Tc-99m-HMPAO brain perfusion SPECT: a controlled study.International Journal of Neuroscience 115, 1643–1655.
Valente, A.A., Miguel, E.C., Castro, C.C., Amaro, E., Duran, F.L., Buchpiguel, C.A.,Chitnis, X., McGuire, P.K., Busatto, G.F., 2005. Regional gray matter abnorm-alities in obsessive-compulsive disorder: a voxel-based morphometry study.Biological Psychiatry 58, 479–487.
van den Heuvel, O.A., Remijnse, P.L., Mataix-Cols, D., Vrenken, H., Groenewegen, H.J.,Uylings, H.B., van Balkom, A.J., Veltman, D.J., 2009. The major symptomdimensions of obsessive-compulsive disorder are mediated by partially distinctneural systems. Brain 132, 853–868.
Zitterl, W., Aigner, M., Stompe, T., Zitterl-Eglseer, K., Gutierrez-Lobos, K., Wenzel, T.,Zettinig, G., Hornik, K., Pirker, W., Thau, K., 2008. Changes in thalamus-hypothalamus serotonin transporter avsailability during clomipramineadministration in patients with obsessive-compulsive disorder. Neuropsycho-pharmacology 33, 3126–3134.
Related Documents











