The Comatose The Comatose Patient Patient Hans House, MD, FACEP Hans House, MD, FACEP Professor Professor Department of Emergency Department of Emergency Medicine Medicine University of Iowa University of Iowa

The Comatose Patient Hans House, MD, FACEP Professor Department of Emergency Medicine University of Iowa.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Comatose The Comatose PatientPatientHans House, MD, FACEPHans House, MD, FACEP
ProfessorProfessor
Department of Emergency MedicineDepartment of Emergency Medicine
University of IowaUniversity of Iowa

ObjectiveObjective
Outline the general approach to the Outline the general approach to the patient with stupor or coma, including the patient with stupor or coma, including the use of clinical, laboratory, and imaging use of clinical, laboratory, and imaging investigationsinvestigations
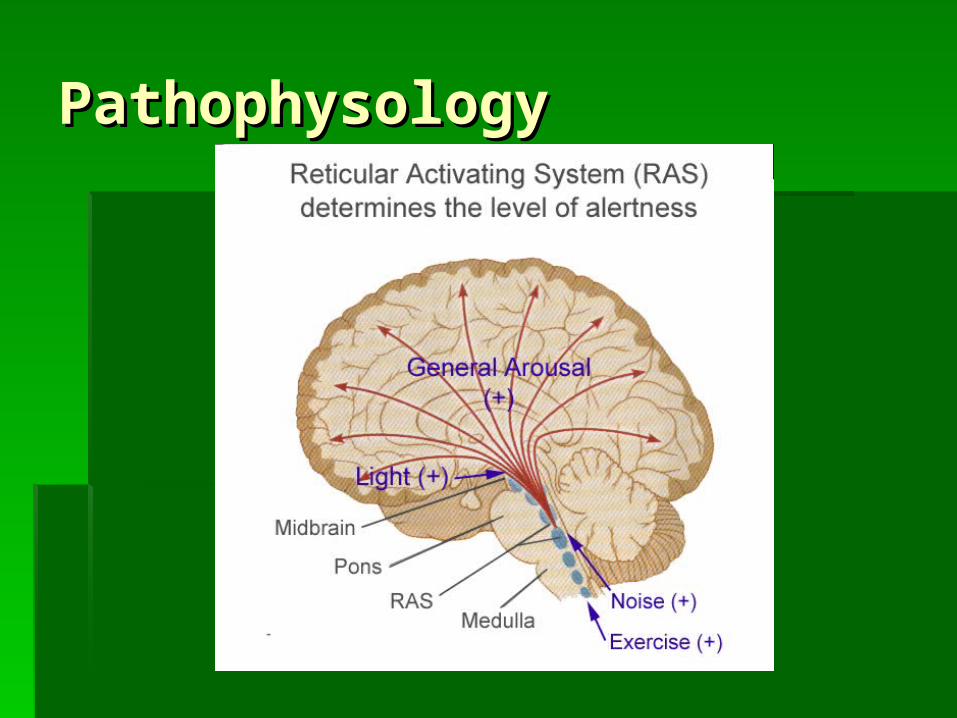
PathophysologyPathophysology

Initial ManagementInitial Management
A: Airway control if neededA: Airway control if needed B: Assist ventilations, 100% OB: Assist ventilations, 100% O22
C: Volume if hypotensiveC: Volume if hypotensive D: DextroseD: Dextrose
Consider: glucose, thiamine, nalaxoneConsider: glucose, thiamine, nalaxone
Differential DiagnosisDifferential Diagnosis
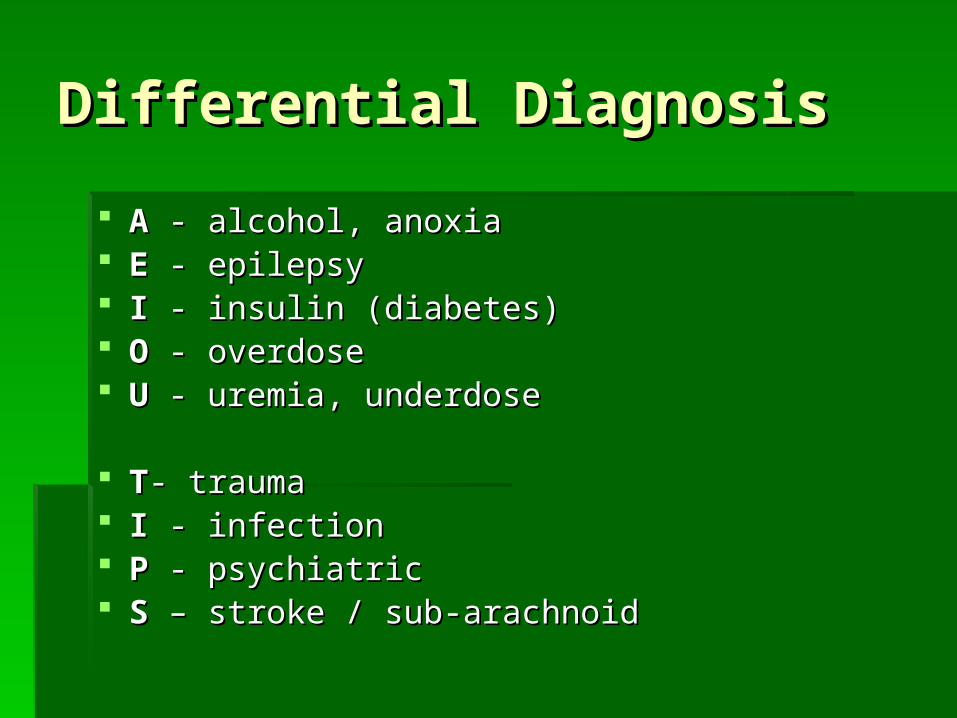
AA - alcohol, anoxia - alcohol, anoxia EE - epilepsy - epilepsy II - insulin (diabetes) - insulin (diabetes) OO - overdose - overdose U U - uremia, underdose- uremia, underdose TT- trauma- trauma II - infection - infection PP - psychiatric - psychiatric SS – stroke / sub-arachnoid – stroke / sub-arachnoid

Differential DiagnosisDifferential Diagnosis
Most common ED diagnosis:Most common ED diagnosis: TraumaTrauma CVACVA IntoxicationsIntoxications MetabolicMetabolic Post- ictal statePost- ictal state Post- cardiopulmonary arrestPost- cardiopulmonary arrest

Differential DiagnosisDifferential Diagnosis1) Cerebral Anemia
2) Mechanical injury
3) Convulsive attacks
4) CVA
5) Poisons, endogenous and exogenous
6) Infection
Young GS. Can Med Assoc J. 1934; 31(4): 381–385.

General Approach: General Approach: HistoryHistory
““Further history limited to Further history limited to patientpatient’’s medical conditions medical condition””

General Approach: General Approach: HistoryHistory
Ask family, EMS, chart:Ask family, EMS, chart: Time course of onsetTime course of onset Duration of symptomsDuration of symptoms Focal signsFocal signs Past Medical HistoryPast Medical History MedicationsMedications Alcohol or drug useAlcohol or drug use

General Approach: PhysicalGeneral Approach: Physical
PE normal in 85% of all patientsPE normal in 85% of all patients Vital signs are vital!Vital signs are vital! Elevated or lowered temp may be helpfulElevated or lowered temp may be helpful Need a core temp!Need a core temp! Ventilatory patterns not helpfulVentilatory patterns not helpful

General Approach: PhysicalGeneral Approach: Physical
After nervous, skin is After nervous, skin is the most useful system the most useful system to examineto examine
TraumaTrauma InfectionInfection ToxidromesToxidromes JaundiceJaundice Seizure traumaSeizure trauma RhinnorrheaRhinnorrhea

General Approach: PhysicalGeneral Approach: Physical
Nervous SystemNervous System Assess and document level of arousalAssess and document level of arousal Useful for prognosis, not diagnosisUseful for prognosis, not diagnosis Use GCSUse GCS ““Less than eight, in-tu-bate!Less than eight, in-tu-bate!””
General Approach: PhysicalGeneral Approach: Physical
Assessing level of arousalAssessing level of arousal Shouting, sternal rub, pinching trapezius, Shouting, sternal rub, pinching trapezius,
nailbed pressurenailbed pressure Supraorbital pressure? Smelling Salts?Supraorbital pressure? Smelling Salts?
General Approach: PhysicalGeneral Approach: Physical
Motor functionMotor function Unable to do routine oppositional forceUnable to do routine oppositional force Use reflexesUse reflexes Look for asymmertyLook for asymmerty

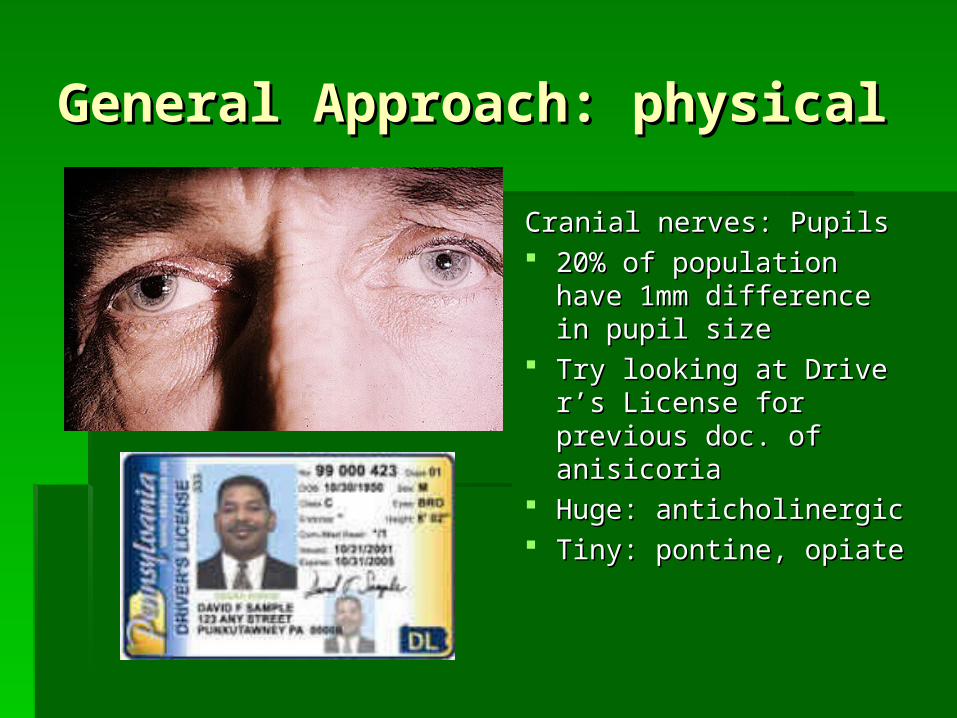
General Approach: physicalGeneral Approach: physical
Cranial nerves: PupilsCranial nerves: Pupils Supertentorial mass/ hemorrhage or Supertentorial mass/ hemorrhage or
primary brainstem lesionprimary brainstem lesion Disruption of 3Disruption of 3rdrd CN or brainstem nuclei CN or brainstem nuclei Transtentorial herniation:Transtentorial herniation:
First dilation/ loss of light reflexFirst dilation/ loss of light reflex Later, midrange (4-5mm) and fixedLater, midrange (4-5mm) and fixed May be mimicked in severe sedative O/DMay be mimicked in severe sedative O/D
General Approach: physicalGeneral Approach: physical
Cranial nerves: PupilsCranial nerves: Pupils 20% of population have 20% of population have
1mm difference in pupil 1mm difference in pupil sizesize
Try looking at DriverTry looking at Driver’’s s License for previous doc. License for previous doc. of anisicoriaof anisicoria
Huge: anticholinergicHuge: anticholinergic Tiny: pontine, opiateTiny: pontine, opiate

General Approach: PhysicalGeneral Approach: Physical
Cranial Nerves: eye movementsCranial Nerves: eye movements Large cerebral mass lesions cause Large cerebral mass lesions cause
deviation toward side of lesiondeviation toward side of lesion Seizure focus (irritable inflammation or Seizure focus (irritable inflammation or
blood) causes deviation away from lesionblood) causes deviation away from lesion Vestibuloocular reflexesVestibuloocular reflexes
Oculocephalic (dollOculocephalic (doll’’s eyes)s eyes) Oculovestibular (caloric testing)Oculovestibular (caloric testing)

General Approach: PhysicalGeneral Approach: Physical
Oculocephalic ReflexOculocephalic Reflex Normal is for the eyes to turn Normal is for the eyes to turn
opposite to head movement to opposite to head movement to keep focused on a fixed pointkeep focused on a fixed point
Do not perform in trauma patient!Do not perform in trauma patient! Positive DollPositive Doll’’s Eyes?s Eyes?

General ApproachGeneral Approach
Oculovestibular ReflexOculovestibular Reflex Torso inclined 30Torso inclined 30ºº 50ml cold water into ear50ml cold water into ear COWS:COWS:
Cold water causes nystagmus toward contralateral Cold water causes nystagmus toward contralateral earear
Warm water causes nystagmus to ipsilateralWarm water causes nystagmus to ipsilateral Conscious patients may vomitConscious patients may vomit Test both sides: may be asymmetrical Test both sides: may be asymmetrical

General Approach: PhysicalGeneral Approach: Physical
Cranial Nerves: Corneal reflexesCranial Nerves: Corneal reflexes Indicative of depth of metabolic comaIndicative of depth of metabolic coma Absent 24 hours after trauma / cardiac Absent 24 hours after trauma / cardiac
arrest indicates poor prognosisarrest indicates poor prognosis May be diminished in conscious elderly, May be diminished in conscious elderly,
diabetic, or optho patients due to loss of diabetic, or optho patients due to loss of sensation of corneasensation of cornea
ToxidromesToxidromes
Pinpoint pupils, decreased respiratory Pinpoint pupils, decreased respiratory effort and rate, hypothermia, AC scarseffort and rate, hypothermia, AC scars
Widely dilated pupils, moderate Widely dilated pupils, moderate tachycardia (120tachycardia (120’’s), flushed skin, dry skins), flushed skin, dry skin
Hyperthermia, tachycardia, tremor, Hyperthermia, tachycardia, tremor, myoclonus, rigiditymyoclonus, rigidity
Miosis, salivation, lacrimation, urination, Miosis, salivation, lacrimation, urination, defecation, emesis, bradycardiadefecation, emesis, bradycardia
ToxidromesToxidromes
Pinpoint pupils, decreased respiratory Pinpoint pupils, decreased respiratory effort and rate, hypothermia, AC scarseffort and rate, hypothermia, AC scars
Widely dilated pupils, moderate tachycardia (120Widely dilated pupils, moderate tachycardia (120’’s), flushed skin, s), flushed skin, dry skindry skin
Hyperthermia, tachycardia, tremor, myoclonus, rigidityHyperthermia, tachycardia, tremor, myoclonus, rigidity Miosis, salivation, lacrimation, urination, defecation, emesis, Miosis, salivation, lacrimation, urination, defecation, emesis,
bradycardiabradycardia

ToxidromesToxidromes
Pinpoint pupils, decreased respiratory effort and rate, Pinpoint pupils, decreased respiratory effort and rate, hypothermia, AC scarshypothermia, AC scars
Widely dilated pupils, moderate Widely dilated pupils, moderate tachycardia (120tachycardia (120’’s), flushed skin, dry skins), flushed skin, dry skin
Hyperthermia, tachycardia, tremor, myoclonus, rigidityHyperthermia, tachycardia, tremor, myoclonus, rigidity Miosis, salivation, lacrimation, urination, defecation, emesis, Miosis, salivation, lacrimation, urination, defecation, emesis,
bradycardiabradycardia

ToxidromesToxidromes
Pinpoint pupils, decreased respiratory effort and rate, Pinpoint pupils, decreased respiratory effort and rate, hypothermia, AC scarshypothermia, AC scars
Widely dilated pupils, moderate tachycardia (120Widely dilated pupils, moderate tachycardia (120’’s), flushed skin, s), flushed skin, dry skindry skin
Hyperthermia, tachycardia, tremor, Hyperthermia, tachycardia, tremor, myoclonus, rigiditymyoclonus, rigidity
Miosis, salivation, lacrimation, urination, defecation, emesis, Miosis, salivation, lacrimation, urination, defecation, emesis, bradycardiabradycardia

ToxidromesToxidromes
Pinpoint pupils, decreased respiratory effort and rate, Pinpoint pupils, decreased respiratory effort and rate, hypothermia, AC scarshypothermia, AC scars
Widely dilated pupils, moderate tachycardia (120Widely dilated pupils, moderate tachycardia (120’’s), flushed skin, s), flushed skin, dry skindry skin
Hyperthermia, tachycardia, tremor, myoclonus, rigidityHyperthermia, tachycardia, tremor, myoclonus, rigidity
Miosis, salivation, lacrimation, urination, Miosis, salivation, lacrimation, urination, defecation, emesis, bradycardiadefecation, emesis, bradycardia

Laboratory TestingLaboratory Testing
Serum labsSerum labs Radiography (Head CT)Radiography (Head CT) Lumbar PunctureLumbar Puncture EEGEEG

Laboratory Testing: Laboratory Testing: SerumSerum
Accu-check is part of the ABCDAccu-check is part of the ABCD’’s!s! Electrolytes essential to r/o metabolicElectrolytes essential to r/o metabolic
Na, BUN/Cr, anion gapNa, BUN/Cr, anion gap
ConsiderConsider UA, urine and blood culturesUA, urine and blood cultures TSHTSH CarboxyhemoglobinCarboxyhemoglobin Drug Screen and EtOH levelDrug Screen and EtOH level
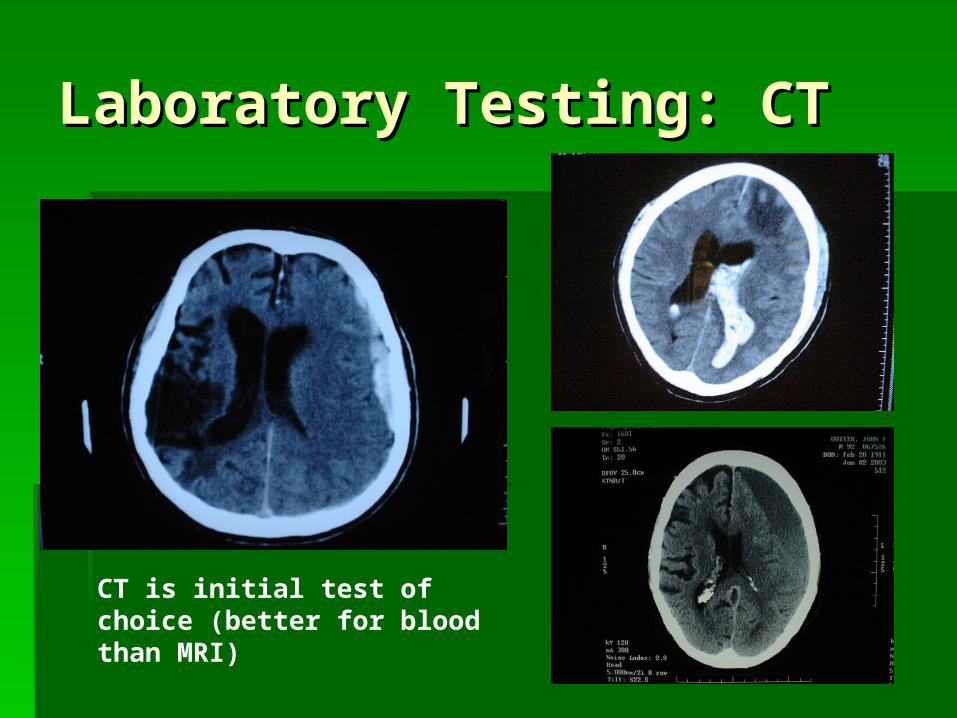
Laboratory Testing: CTLaboratory Testing: CT
CT is initial test of choice (better for blood than MRI)

Laboratory Testing: LPLaboratory Testing: LP
Head CT before LP recommended for Head CT before LP recommended for possible mass lesionspossible mass lesions
DO NOT DELAY ANTIBIOTICS/ DO NOT DELAY ANTIBIOTICS/ STEROIDS! (you have the blood STEROIDS! (you have the blood cultures . . .)cultures . . .)
LP after CT if SAH suspectedLP after CT if SAH suspected
Laboratory Testing: EEGLaboratory Testing: EEG
Indications:Indications: Status epilepticus (SE) with paralysisStatus epilepticus (SE) with paralysis Suspected non-convulsive SE (NCSE)Suspected non-convulsive SE (NCSE) Aid in diagnosis of unknown caseAid in diagnosis of unknown case
8 of 236 patients without overt seziure 8 of 236 patients without overt seziure activity in coma had NCSEactivity in coma had NCSE
Pattern may indicate cause of coma Pattern may indicate cause of coma (metabolic, structural, seizure, anoxic)(metabolic, structural, seizure, anoxic)

Case #1Case #1
78 yo male BIB RA from SNF for fever 78 yo male BIB RA from SNF for fever and altered mental statusand altered mental status
Temp 40Temp 40º, HR 110, BP 95/60, R 20º, HR 110, BP 95/60, R 20 PE: dry mucous membranes, poor tugorPE: dry mucous membranes, poor tugor Minimally responsive, groans when neck Minimally responsive, groans when neck
flexed, hot to touchflexed, hot to touch UA normalUA normal

Case #1Case #1
Blood CxBlood Cx Dexamethasone Dexamethasone
10mg q 6hrs10mg q 6hrs Vancomycin and Vancomycin and
CeftriaxoneCeftriaxone Head CTHead CT LPLP

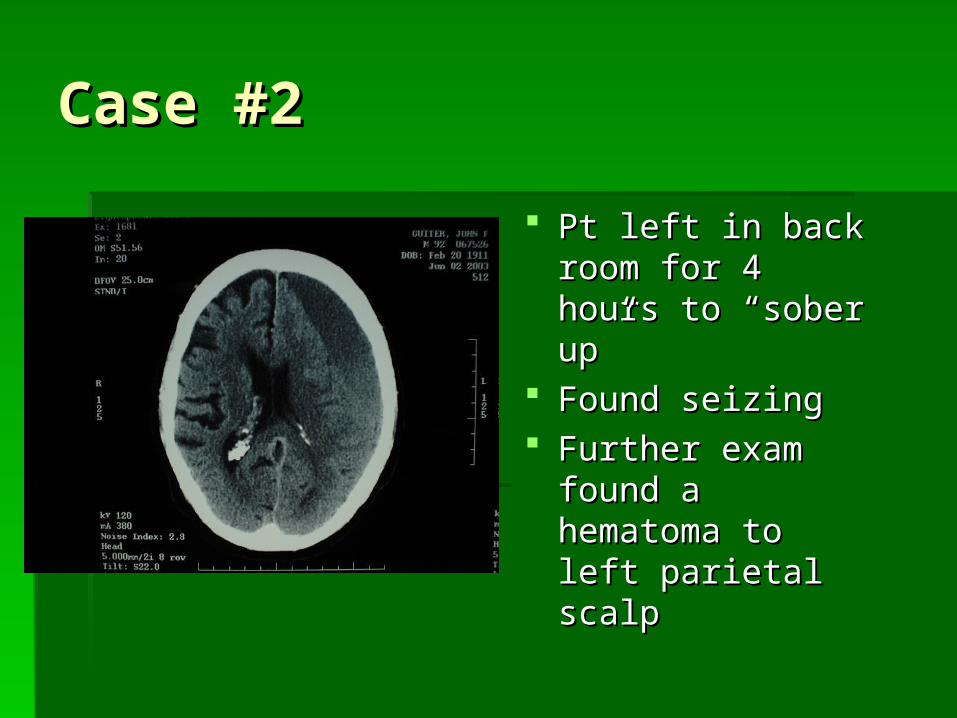
Case #2Case #2
42 yo male of 42 yo male of ““no fixed abodeno fixed abode”” BIB police BIB police after found down in streetafter found down in street
Pt is Pt is ““well known to servicewell known to service”” Vitals normal except mild hypothermiaVitals normal except mild hypothermia GCS 9 (withdraws and moans to pain)GCS 9 (withdraws and moans to pain) Odor of EtOH on breathOdor of EtOH on breath
Case #2Case #2
Pt left in back Pt left in back room for 4 hours to room for 4 hours to ““sober upsober up””
Found seizingFound seizing Further exam Further exam
found a hematoma found a hematoma to left parietal to left parietal scalpscalp

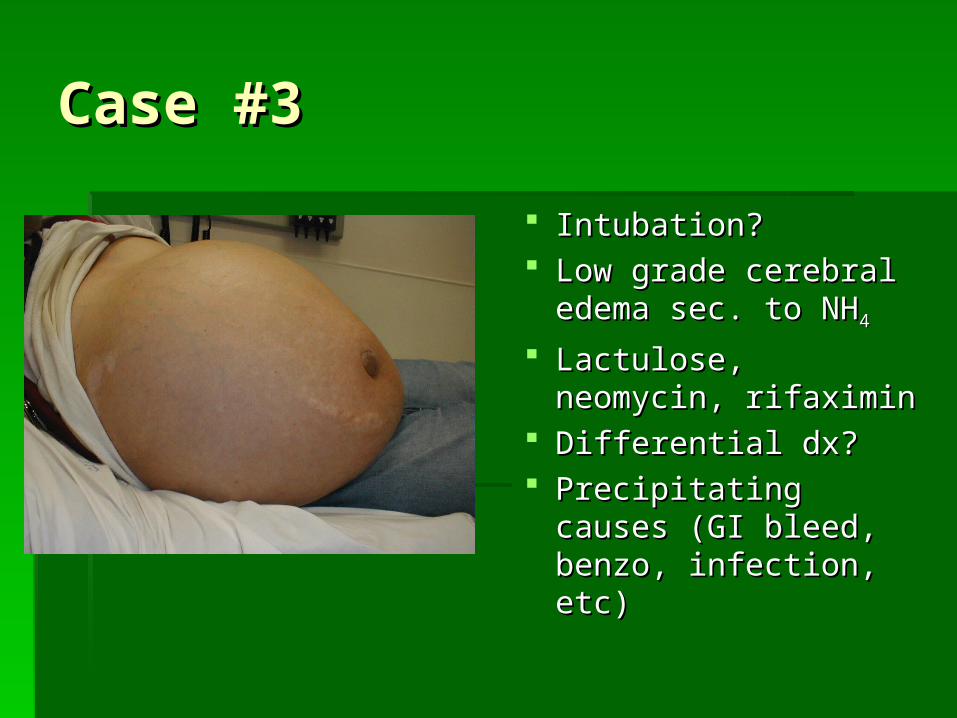
Case #3Case #3
46 yo male alcoholic BIB family for 46 yo male alcoholic BIB family for decreased consciousnessdecreased consciousness
He moans in response to stimulation, He moans in response to stimulation, withdraws from pain, eye remain shutwithdraws from pain, eye remain shut
Skin is jaundiced, sclera ictericSkin is jaundiced, sclera icteric Foul breath (fetor hepaticus)Foul breath (fetor hepaticus) Abdomen: swollen, caput medusae Abdomen: swollen, caput medusae
Case #3Case #3
Intubation?Intubation? Low grade cerebral Low grade cerebral
edema sec. to NHedema sec. to NH44
Lactulose, neomycin, Lactulose, neomycin, rifaximinrifaximin
Differential dx? Differential dx? Precipitating causes Precipitating causes
(GI bleed, benzo, (GI bleed, benzo, infection, etc)infection, etc)

Case #4Case #4
22 yo male BIB police for odd behavior22 yo male BIB police for odd behavior He was found in the street yellingHe was found in the street yelling Agitated, combative, anxiousAgitated, combative, anxious BP 184/97, HR 140, R 22, T38BP 184/97, HR 140, R 22, T38 Eyes open to pain, moves all 4Eyes open to pain, moves all 4’’s, s,
incomprehensible soundsincomprehensible sounds Eyes have rotatory nystagmusEyes have rotatory nystagmus

Case #4Case #4
Used PCPUsed PCP Essentially adrenergic Essentially adrenergic
toxidrometoxidrome HallucinogenHallucinogen Causes all forms of Causes all forms of
nystagmusnystagmus
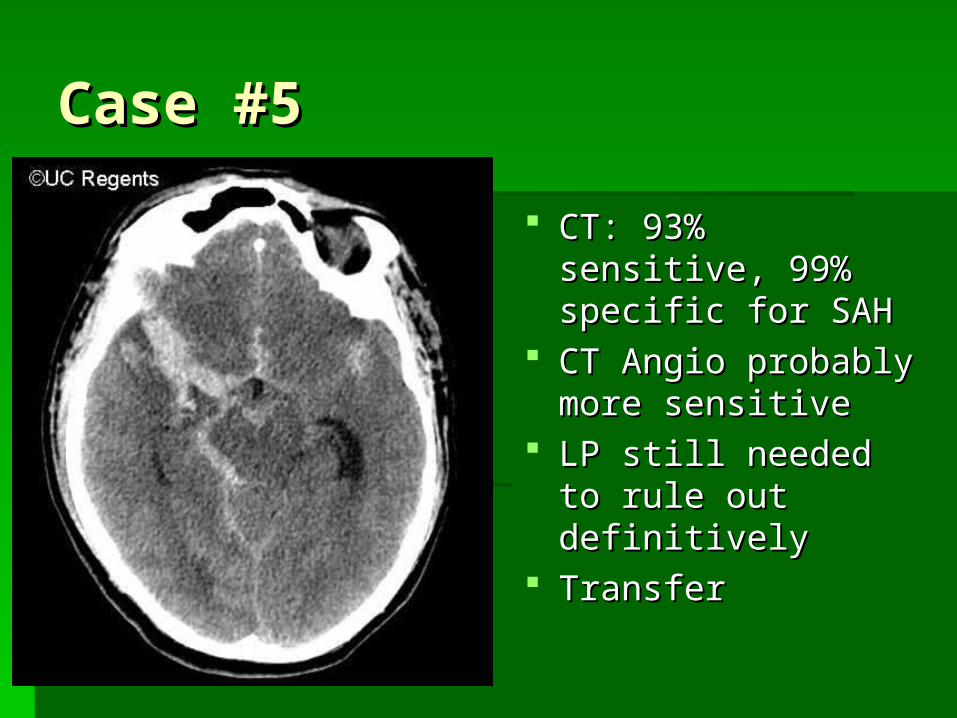
Case #5Case #5
39 yo female found down by husband39 yo female found down by husband Had complained of a headache earlierHad complained of a headache earlier PMH: HtnPMH: Htn FHx: polycystic kidney diseaseFHx: polycystic kidney disease BP 150/90, HR 65, T37BP 150/90, HR 65, T37 Eyes closed, withdraws to pain, no verbalEyes closed, withdraws to pain, no verbal
Case #5Case #5
CT: 93% sensitive, CT: 93% sensitive, 99% specific for SAH99% specific for SAH
CT Angio probably CT Angio probably more sensitivemore sensitive
LP still needed to LP still needed to rule out definitivelyrule out definitively
TransferTransfer
Case #6Case #6
27 yo female BIB family for odd behavior27 yo female BIB family for odd behavior Previous history of bipolar d/oPrevious history of bipolar d/o Now not responsiveNow not responsive No signs of trauma or intoxicationNo signs of trauma or intoxication Exam normal except for intermittent Exam normal except for intermittent
nystagmus and eye deviationnystagmus and eye deviation All labs, including head CT and drug All labs, including head CT and drug
screen WNLscreen WNL
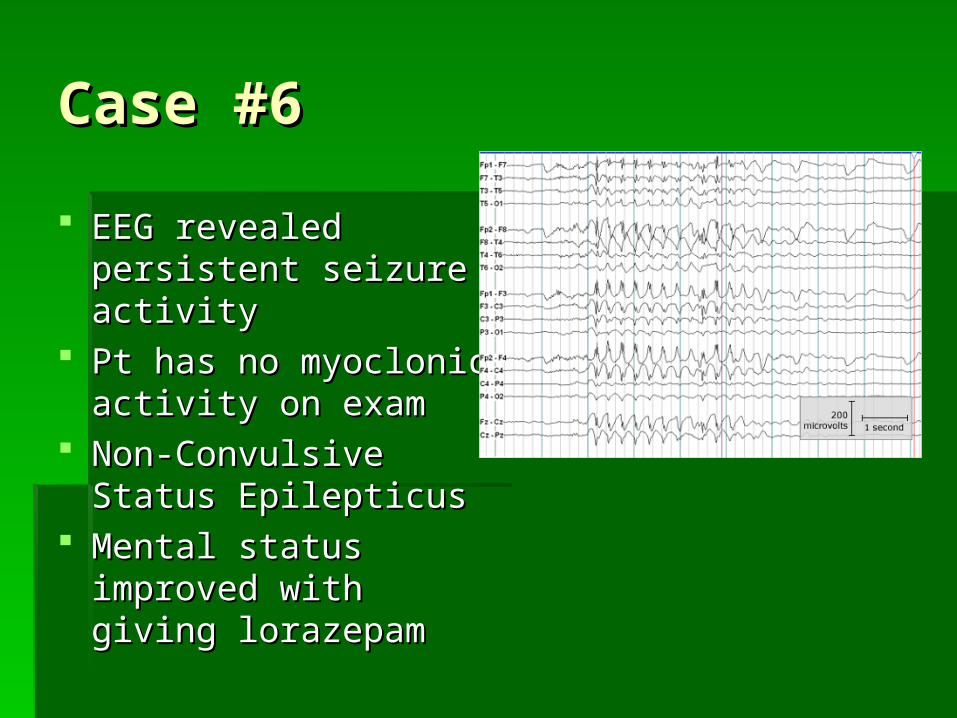
Case #6Case #6
EEG revealed EEG revealed persistent seizure persistent seizure activityactivity
Pt has no myoclonic Pt has no myoclonic activity on examactivity on exam
Non-Convulsive Status Non-Convulsive Status EpilepticusEpilepticus
Mental status improved Mental status improved with giving lorazepamwith giving lorazepam

ConclusionsConclusions
ABC-D (D is for Dextrose)ABC-D (D is for Dextrose) If elevated or low Temp would change If elevated or low Temp would change
your management, get a core tempyour management, get a core temp Less than 8, in-tu-bate!Less than 8, in-tu-bate! For meningitis: IV, then blood cultures, For meningitis: IV, then blood cultures,
then steroids, then Abx, then CT, then LPthen steroids, then Abx, then CT, then LP Beware of occult trauma in the intoxicatedBeware of occult trauma in the intoxicated

Any Questions?Any Questions?
Related Documents









![The COMATOSE ATP-Binding Cassette Transporter Is · The COMATOSE ATP-Binding Cassette Transporter Is Required for Full Fertility in Arabidopsis1[W][OA] Steven Footitt2, Daniela Dietrich,](https://static.cupdf.com/doc/110x72/5e3fcb8fadfcd6003a2272db/the-comatose-atp-binding-cassette-transporter-is-the-comatose-atp-binding-cassette.jpg)

