The Changing Role of Radioiodine in the Management of Differentiated Thyroid Cancer James C, Reynolds and Jacob Robbins This article discusses several aspects of the evaluation and management of differentiated thyroid carcinoma that are changing or may change in the near future. Although conventional treatment of this disease is highly effective, some modification may improve the welfare of patients and the overall results. Because the symptoms of hypothyroidism are vexing, there has been great interest in using recombinant human thyroid-stimulating hormone (rhTSH) to prepare pa- tients for iodine 131 imaging, rhTSH has been about as effective as thyroid hormone withdrawal for diagnos- tic imaging so that approval for this use is expected. Another topic of interest is the administration of 1311 therapy to patients whose serum thyroglobulin levels are abnormal but whose diagnostic 1311 scans are negative. Because the 1311 scans after therapy are often abnormal in these patients and a reduction of serum thyroglobulin can occur, this approach seems effec- tive. The long-term impact of this therapy on recur- rence and survival, however, is unknown. A third issue that is currently under review is the amount of 1311 that should be used for diagnostic scanning. Although past opinion favored larger doses, "stunning" of thyroid remnant and tumor can occur with diagnostic 1311 imaging. Substituting iodine 123 is an alternative for postthyroidectomy scanning, but when administered as 300 uCi it is less accurate than 1311for recurrent disease or distant metastases. Related to these issues, two other topics are reviewed: the use of other radiopharmaceuticals for imaging patients with thy- roid cancer, and 1311 dosimetry. This is a US government work. There are no restric- tions on its use. T HE TERM "differentiated thyroid cancer" is used here in its customary sense to designate neoplasia arising in the thyroid follicular cells as opposed to the parafollicular cells that are the source of medullary thyroid cancer. It also desig- nates those follicle cell cancers that are capable of functioning like normal cells. Only the thyroid follicular cells are able to accumulate and retain iodine, providing the basis for the unique role of radioiodine in managing their tumors. Since the introduction of iodine 131 in the middle of this century, there has developed what we might call a classical approach to the use of this isotope in detecting and treating thyroid cancer. After surgical excision of the tumor, together with most of the normal thyroid gland when the lesion's diameter is greater than 1 or 1.5 cm, whole body scanning with 131I is used to detect any functioning thyroid tissue in the thyroid bed, which may be residual normal or From the Nuclear Medicine Department, Warren G. Magnu- son Clinical Center; and the Genetics and Biochemistry Branch, NIDDK, National Institutes of Health, Bethesda, MD. The information and opinions in this article are entirely the responsibility of the authors and not the US Federal Govern- ment. Address reprint requests to James C. Reynolds, MD, Nuclear Medicine Department, CC, NIH, Building 10, Room 1C-401, 9000 Rockville Pike, Bethesda, MD 20892. This is a government work. There are no restrictions on its use. 0001-2998/97/2702-000550.00/0 malignant tissue, or in the regional lymph nodes, and in distant sites, usually in lung or bone. Before receiving the tracer dose of 131I, the patient is allowed to become hypothyroid so as to increase pituitary thyroid-stimulating hormone (TSH) secre- tion and thus stimulate thyroid cells to function maximally. Detection of 1311uptake is followed by a larger, therapeutic dose of 131I. If the uptake is confined to the thyroid bed, a relatively low ablation dose is administered. If there is uptake outside the thyroid bed, a larger dose is given, its size dependent on whether the metastases are regional or distant. Thyroid hormone is then administered to restore euthyroidism and suppress TSH. At intervals of 4 to 6 months or longer, depending on the stage of the disease and its treatment, the hormone replacement is interrupted to repeat 1311 whole body scanning and to administer any indicated therapy. This classical approach is, of course, not without variation as well as controversies in its application. Experience has led to the classification of thyroid cancers into those with low or high risk of recur- rence and mortality, and this is used in designing the intensity of the follow-up as well as the therapy. It is not the purpose of this article to discuss these matters, about which much has been written. 1,2 Instead, we focus on several aspects that are of current interest and are changing, or may change, the way 1311 is used in the management of differen- tiated thyroid cancer. 152 Seminars in Nuclear Medicine, Vol XXVII, No 2 (April), 1997: pp 152-164

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Changing Role of Radioiodine in the Management of Differentiated Thyroid Cancer
James C, Reynolds and Jacob Robbins
This article discusses several aspects of the evaluation and management of differentiated thyroid carcinoma that are changing or may change in the near future. Although conventional treatment of this disease is highly effective, some modification may improve the welfare of patients and the overall results. Because the symptoms of hypothyroidism are vexing, there has been great interest in using recombinant human thyroid-st imulating hormone (rhTSH) to prepare pa- t ients for iodine 131 imaging, rhTSH has been about as effective as thyroid hormone withdrawal for diagnos- tic imaging so that approval for this use is expected. Another topic of interest is the administration of 1311 therapy to patients whose serum thyroglobulin levels are abnormal but whose diagnostic 1311 scans are negative. Because the 1311 scans after therapy are often abnormal in these patients and a reduction of serum
thyroglobulin can occur, this approach seems effec- tive. The long-term impact of this therapy on recur- rence and survival, however, is unknown. A third issue that is currently under review is the amount of 1311 that should be used for diagnostic scanning. Although past opinion favored larger doses, "stunning" of thyroid remnant and tumor can occur with diagnostic 1311 imaging. Substituting iodine 123 is an alternative for postthyroidectomy scanning, but when administered as 300 uCi it is less accurate than 1311 for recurrent disease or distant metastases. Related to these issues, two other topics are reviewed: the use of other radiopharmaceuticals for imaging patients wi th thy- roid cancer, and 1311 dosimetry. This is a US g o v e r n m e n t work. There are no restric- t ions o n i ts use.
T HE TERM "differentiated thyroid cancer" is used here in its customary sense to designate
neoplasia arising in the thyroid follicular cells as opposed to the parafollicular cells that are the source of medullary thyroid cancer. It also desig- nates those follicle cell cancers that are capable of functioning like normal cells. Only the thyroid follicular cells are able to accumulate and retain iodine, providing the basis for the unique role of radioiodine in managing their tumors. Since the introduction of iodine 131 in the middle of this century, there has developed what we might call a classical approach to the use of this isotope in detecting and treating thyroid cancer. After surgical excision of the tumor, together with most of the normal thyroid gland when the lesion's diameter is greater than 1 or 1.5 cm, whole body scanning with 131I is used to detect any functioning thyroid tissue in the thyroid bed, which may be residual normal or
From the Nuclear Medicine Department, Warren G. Magnu- son Clinical Center; and the Genetics and Biochemistry Branch, NIDDK, National Institutes o f Health, Bethesda, MD.
The information and opinions in this article are entirely the responsibility of the authors and not the US Federal Govern- ment.
Address reprint requests to James C. Reynolds, MD, Nuclear Medicine Department, CC, NIH, Building 10, Room 1C-401, 9000 Rockville Pike, Bethesda, MD 20892.
This is a government work. There are no restrictions on its use.
0001-2998/97/2702-000550.00/0
malignant tissue, or in the regional lymph nodes, and in distant sites, usually in lung or bone. Before receiving the tracer dose of 131I, the patient is allowed to become hypothyroid so as to increase pituitary thyroid-stimulating hormone (TSH) secre- tion and thus stimulate thyroid cells to function maximally.
Detection of 1311 uptake is followed by a larger, therapeutic dose of 131I. If the uptake is confined to the thyroid bed, a relatively low ablation dose is administered. If there is uptake outside the thyroid bed, a larger dose is given, its size dependent on whether the metastases are regional or distant. Thyroid hormone is then administered to restore euthyroidism and suppress TSH. At intervals of 4 to 6 months or longer, depending on the stage of the disease and its treatment, the hormone replacement is interrupted to repeat 1311 whole body scanning and to administer any indicated therapy.
This classical approach is, of course, not without variation as well as controversies in its application. Experience has led to the classification of thyroid cancers into those with low or high risk of recur- rence and mortality, and this is used in designing the intensity of the follow-up as well as the therapy. It is not the purpose of this article to discuss these matters, about which much has been written. 1,2 Instead, we focus on several aspects that are of current interest and are changing, or may change, the way 1311 is used in the management of differen- tiated thyroid cancer.
152 Seminars in Nuclear Medicine, Vol XXVII, No 2 (April), 1997: pp 152-164
RADIOIODINE MANAGEMENT OF THYROID CANCER 153
STIMULATION OF FUNCTION WITH rhTSH
In the past, partially purified bovine TSH was used to stimulate 131I uptake in thyroid cancer. Because it was not as effective as endogenous TSH, and was often accompanied by allergic reactions, it was used only when the patient was unable to tolerate a hypothyroid state or when the patient's pituitary was incapable of mounting a TSH re- sponse. Bovine TSH is no longer commercially available but the imminent introduction of rhTSH into clinical use is expected to change dramatically this state of affairs.
TSH is a glycoprotein and, therefore, cannot be manufactured by recombinant methodology in bac- teria; however, the production of bioactive rhTSH on a laboratory scale in Chinese hamster ovary (CHO) cells by transfection with or- and [3-TSH subunit DNA was recently accomplished. 3"5 After scaling up to an industrial level (Thyrogen, Gen- zyme) 6 and demonstrating efficacy in monkeys, 7 a human phase IBI trial was completed and approved by the Food and Drug Administration. 8 This has been followed by a phase III trial that is still ongoing and FDA approval is awaited.
rhTSH has a higher sialic acid content than native pituitary TSH. 9 This decreases its in vitro potency but increases its in vivo potency owing to slower clearance from the circulation. Studies s were carded out in human patients with differenti- ated thyroid carcinoma in whom the effect of rhTSH was compared with that of endogenous TSH after thyroid hormone withdrawal. The phase IBI trial s established the safety of intramuscularly injected rhTSH, which had only minimal side effects especially when compared with the very troublesome symptoms of hypothyroidism. It also gave preliminary dosing information, which is under continuing investigation in the phase III trial (P.W. Ladensen et al, manuscript in preparation). The results thus far indicate that rhTSH can stimu- late 131l uptake in residual normal or neoplastic thyroid tissue, giving whole body scans that are strictly equivalent to those after thyroid hormone withdrawal in about 85% of patients and providing comparable diagnostic information in almost all patients. They also show that rhTSH injection is followed by an increase in serum thyroglobulin in almost all patients capable of responding to thyroid hormone withdrawal.
The preliminary results indicate that further
refinement of the size and timing of the rhTSH injections, and the timing of the tests that follow, will soon provide an easier and better tolerated method for detecting residual or recurrent thyroid cancer than that currently available. As experience with this agent advances we will learn whether, or how often, it is necessary to repeat a negative rhTSH test with a hormone withdrawal test. Presum- ably, this would pertain mainly to patients with high-risk cancer in whom more aggressive fol- low-up and treatment are indicated. We will also gather needed information on cost-benefit aspects of the procedure.
Another matter that will need to be addressed is the optimal way to prepare a patient for 131I therapy. Whereas, the use of rhTSH for diagnosis only requires the detection of functioning thyroid tissue, its use in 1311 therapy is more complex. This must take into account the uptake and retention of 131I in the tumor giving the desired radiation, and reten- tion in the remainder of the body giving unwanted radiation. One important difference between rhTSH and the current method of stimulating uptake is that rhTSH does not affect renal function whereas the decreased glomerular filtration that accompanies hypothyroidism leads to a delay in excretion of 13tI iodide. Although this increases whole body radiation, it also results in increased ~3~I accumula- tion in functioning thyroid tissue. How this affects the therapy decision is discussed below. It requires quantitative assessment of the anticipated radiation to tumor and to other organs, especially to bone marrow, in relation to the ~31I dose that is adminis- tered.
SERUM THYROGLOBULIN AS AN INDICATOR FOR THE PRESENCE AND THE TREATABILITY
OF RESIDUAL OR RECURRENT THYROID CANCER
Serum thyroglobulin (Tg) is an ideal tumor marker for differentiated thyroid cancer because its only source in the body is thyroid tissue. After the normal thyroid gland has been totally removed or destroyed, any Tg that can be detected signifies the presence of tumor. The absence of measurable Tg, on the other hand, does not mean that tumor is absent because it may be nonfunctional or may produce too little Tg. Although technical problems exist, including the inability to obtain an accurate estimate when blood contains anti-Tg antibodies) ~
154 REYNOLDS AND ROBBINS
measurement of serum Tg is now a mainstay in the management of thyroid cancer. The aspect that has come under consideration in recent years is whether it is reasonable to use the presence of Tg in serum as an indicator for 131I therapy when the whole body 1311 diagnostic scan is negative.
It is well known that increasing the amount of administered 131I will increase the likelihood of detecting a lesion. For example, a whole body scan performed after a therapy dose of 1311 will often detect functioning tissue not seen in the diagnostic study. 11,12 Not infrequently, distant metastases are revealed. 13,14 However, practical considerations and the problem that the tracer itself may alter the tumor's function without destroying it (the "stun- ning" effect) have tempered the movement to larger and larger diagnostic scanning dosages. But if the lesion is not visible in the diagnostic scan, the remaining question is whether there will be enough activity present with 131I therapy to achieve a significant effect. For lesions whose size can be determined by some other means, such as radiogra- phy, magnetic resonance imaging, ultrasound, or clinical examination, this question can be an- swered. Often, however, the lesions are not visible by any method so that follow-up observations are needed in patients treated when the diagnostic scan is negative.
Limited information on short-term follow-up is presently available. An example is the report of Pineda et al,15 on a 5-year follow-up of 131I therapy in 17 thyroid cancer patients with serum Tg levels above 5 ng/mL and negative diagnostic 131I SCanS. In 16 patients, the posttherapy 131I scans were positive for cervical and/or distant metastases. After one or more treatments the serum Tg level decreased in 14 patients with values in 8 patients becoming less than 5 ng/mL. Eight lesions in 8 patients became negative in subsequent post- therapy 1311 scans. Thus, the results show clearly that therapy in such patients can be followed by a decrease in the serum Tg level and a disappear- ance of detectable uptake when scanning is done after a very large 131I dose. 15 In a recent case re- port, Rudavsky and Freeman describe successful 1311 treatment of a patient with extensive bony metastases from papillary thyroid carcinoma. 16 De, spite an earlier negative diagnostic 131I scan, the patient's symptoms abated with therapy, his bony lesions began to heal, and his thyroglobulin dimin- ished from 7,800 ng/mL to 1,900 ng/mL, 16 Thus,
treatment given in this manner can have a signifi- cant effect on both tumor and patient symptoms. Obviously, long-term observations, preferably in a randomized treatment study, are needed to show whether this therapeutic effect will actually im- prove prognosis and disease-free survival.
In the meantime, practical guidelines are needed, and the following ideas and suggestions are of- fered:
At what Tg level should therapy be considered? With the current problems in obtaining an accurate assay, absolute criteria cannot be given (see below). Therefore, it is crucial, that each therapist develop information in his or her own department. As in all treatment of thyroid cancer patients, the spectrum of risk of the disease must be considered. It is clear that Tg levels as low as 8 ng/mL can indicate the presence of potentially "treatable disease, and this might be used to guide therapy in high risk patients. A higher Tg level might be more reasonable in low-risk patients, in whom the potential risks from 1311 therapy must be balanced against the risk from the tumor.
Because a tracer dose of 131I can have a "stun- ning" effect, is it sensible to omit the low dose survey or diagnostic scan entirely when the Tg level indicates the need for treatment? Once again, this might be a reasonable approach in a high-risk patient. On the other hand, the diagnostic study may reveal unknown distant metastases that would require that a larger therapy dose be given. Thus, the initial treatment probably should be preceded by a diagnostic scan, whereas subsequent treat- ments might omit the tracer study unless 1311 dosimetry is needed to determine the maximal safe dosage for the patient.
It is understood that if functioning tumor is not detected on the posttherapy scan, the treatment likely had no value. This negative outcome would be easier to justify in an older patient, in a high-risk patient, or in a patient at the end of a series of treatments in whom previous posttherapy scans had been positive.
A few additional comments about the measure- ment of serum Tg are needed. First, the results obtained from different Tg assays may vary by more than 50% because of the antibodies (antisera) and standards used. I~ This means that a series of measurements on a patient must be performed with the same assay to provide a reliable picture of the clinical course. Second, although the assays are

RADIOIODINE MANAGEMENT OF THYROID CANCER 155
specific, the Tg values may not distinguish between remnant and malignancy. Ideally, patients in whom all thyroid tissue is removed or destroyed should have undetectable levels of serum Tg, but measur- able values are frequently found after ablation therapy. 10,17 An empirically determined level of Tg is then used to identify those patients who might benefit from 1311 therapy. As an example, patients in our clinic who have negative diagnostic 131I scans are not treated with 131I unless the serum Tg is -> 10 ng/mL in our current assay. However, some pa- tients with residual cancer will have values below 10 ng/mL and will not be recognized using this cut off. In the report by Sherman et al, posttherapy 131I scans showed previously unknown distant metastases in 5 patients with serum Tg levels of less than 10 ng/mL, is Third, anti-Tg antibodies may falsely elevate Tg measurements; 15% to 30% of thyroid cancer patients have circulating antibod- ies that interfere in Tg assays. I~ Although methods are available to estimate "total" (bound plus free) Tg, a conservative view is that Tg levels measured in the presence of anti-Tg antibodies may be invalid or at least "should be interpreted with caution. ' 'u Certainly, when anti-Tg antibodies are present, 131I therapy should not be based solely on the Tg level. There are a number of ways to detect anti-Tg antibodies. Older assays, such as the hem- agglutination method, are insensitive and should not be relied on to rule out the presence of these antibodies. 10
1311 STUNNING OF THE THYROID
Stunning of thyroid tissue can be defined as the reduction of iodine uptake occurring in a thyroid remnant or thyroid cancer metastasis following an administration of 131I. Stunning follows both diag- nostic and therapeutic doses and is caused by absorbed radiation from 1311. Stunning was first described by Rawson et al, who reported that "non-cancericidal doses of 1311 markedly decreased the ability of thyroid carcinomas to concentrate the isotope for some time. ''~9 Since then, thyroidolo- gists have been aware that 131I therapy of thyroid cancer may cause a reduction of 131I concentrating function but this has been attributed to reduction in tumor size or the selection of less functioning cells. Furthermore, although it is known that the ab- sorbed radiation dosage during 1311 therapy is only about 80% of that found during a low dosage diagnostic 131I study, this has been attributed to
breakdown of tumor with release of organified 1311.20 In the last 10 years, it has become apparent that stunning also occurs following diagnostic scanning with 1311, and the concern is that this effect may limit 131I therapy.
In 1986, Jeevanram et al reported that radioio- dine uptake during 1311 therapy of thyroid cancer was lower than the uptake measured with a 4 to 5 mCi 1311 scanning dose administered 1 week ear- lier. 21 They evaluated the effect of 0.1 to 5 mCi of 131I in 52 patients whose postthyroidectomy thyroid radioiodine uptake (RAIU) was above 5%. The percent thyroidal RAIU during therapy was found to be significantly depressed when the absorbed radiation during initial scanning exceeded 1,750 rad. Overall, reduced uptake was found in 56% of the patients. In seven patients, RAIU was also depressed following a second 3.5 to 4.5 mCi dose of 1311 suggesting that lower uptake during the second study was not simply a response to the 250 mCi of radioiodine therapy. Similar studies per- formed in hyperthyroid patients who received 25 uCi for diagnostic scanning showed no reduction in RAIU during 131I therapy with 2.9 to 5.8 mCi. In the thyroid cancer patients, the degree of reduction of RAIU was not related to the time between the initial scanning procedure and therapy. However, this interval was longer than 40 days in only four patients. 2~
Park et al studied 26 postthyroidectomy thyroid cancer patients who received 3 to l0 mCi of 13JI for diagnostic scanning. 22 They visually compared the thyroidal activity in the diagnostic scan and in the post-therapy scan. In 20 patients (77%) the thyroi- dal uptake in the therapy scans was less than that in the diagnostic study. Stunning occurred in 40% of the patients who received 3 mCi, 67% of those who received 5 mCi and 89% of those who received 10 mCi of 13q. In the entire group, 15 of 24 patients with cervical lesions (62%) were stunned by the scanning dosage but only 1 of 11 distant metastases (9%) was found to have reduced activity during therapy. In one patient, there was no visible thyroid uptake 7 months after a scanning dose of 10 mCi. The effect on uptake occurred with both papillary and follicular tumors. 22
How can stunning be prevented? One method is to use a low dose of 131I for diagnostic scanning. In a preliminary report, Kim et al evaluated the effect of the 131I scanning dose on the success of remnant ablation. 23 When initial scanning was performed

156 REYNOLDS AND ROBBINS
with 10 mCi of 131I, only 37.5% of the patients could be ablated with 100 mCi of 1311.24 However, 100% of the patients who received a 1 mCi scanning dose were successfully treated, z3 Another approach is to scan with iodine 123, which gives a significantly lower absorbed radiation dose than ]311.22 Park et al found in 14 postthyroidectomy patients that 1231 scanning caused no thyroid "stun- ning. ''24 Furthermore, the accuracy of postthyroid- ectomy 1231 scans (300 laCi with imaging at twenty- four hours) was similar to that of 1311 (3 to 10 mCi with imaging at 72 hours), 89.5% versus 92.9%, respectively. 24 However, in a number of patients previously ablated with 1311, the 3 to 10 mCi 131I scans showed functioning tissue whereas the 300 laCi 1231 scans had been negative a few days earlier. In these "radioablation follow-up patients," the accuracy of 123I scanning was 69.4% compared with 92.5% for 1311.24 In this study, although there appeared to be differences in the success of ablation therapy following 123I compared to 1311 diagnostic scanning, the differences were not significant. 24
THE USE OF RADIOPHARMACEUTICALS OTHER THAN 1311
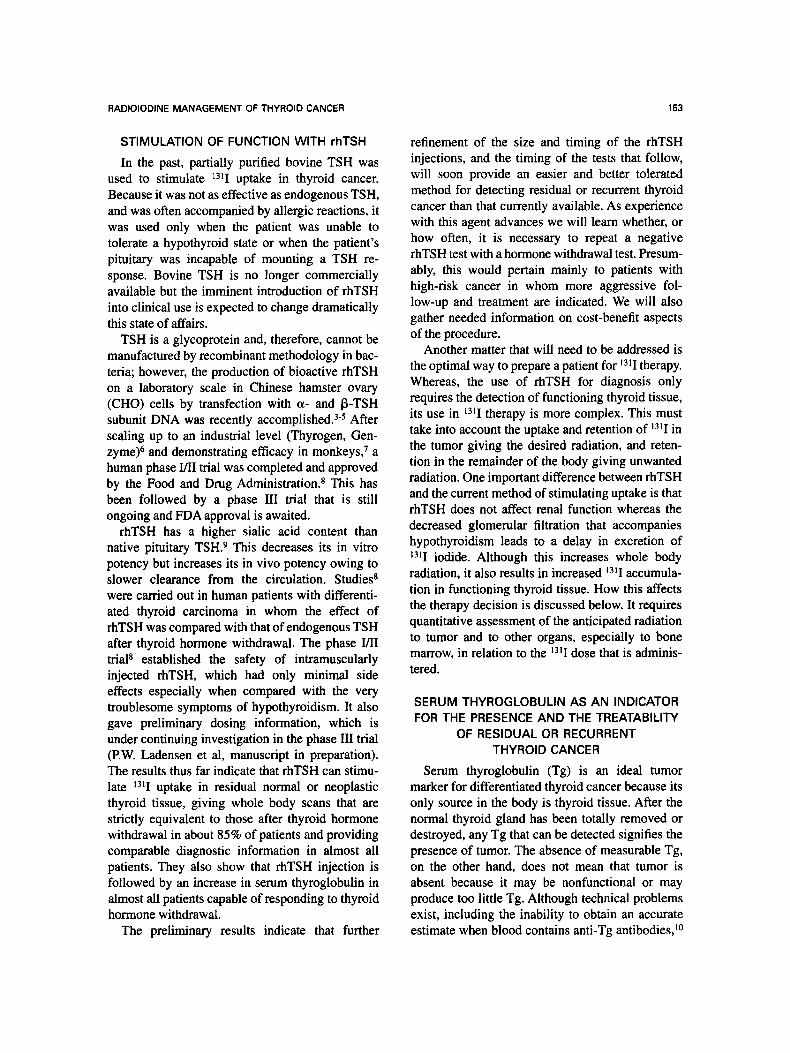
Can other radiopharmaceuticals be substituted for a31I (or 123I) in the follow-up evaluation of patients with thyroid cancer? Several alternative radiopharmaceuticals have been used including thallium 201 chloride, technetium 99m sestamibi, fluorine 18 fluorodeoxyglucose, and indium 111 pentetreotide. Tables 1 to 4 summarize a number of studies in which these pharmaceuticals were com-
pared with 1311.25-45 Because there was variability in the results of these studies, we have combined the data in an attempt to obtain an overall picture of sensitivity, specificity, and accuracy. 46 For each article, we determined the number of patients who had positive or negative scans and the number who had active thyroid cancer (ie, positive 131I images, radiographs, biopsy, or serum Tg assay evidence of disease). In general, the reports made it easy to categorize the data but in some instances judgment was needed to interpret the findings. As well as we could tell, all the patients we summarized had surgically proven differentiated thyroid cancer. Pa- tients with other forms of thyroid cancer were excluded from our analysis even if they were included in the reports. We assumed, unless stated otherwise by the authors, that 1311 was totally specific for thyroid cancer and any finding with 13]I was a true-positive. Findings with the com- pared radiopharmaceutical were considered true- positive if 131I imaging also was positive or the investigators confirmed the lesion by some other method. Any finding with the alternative radiophar- maceutical that was not confirmed was considered a false- positive. When both 13[1 and the alternative radiopharmaceutical were negative, the findings were considered a false-negative if the patient was shown to have active thyroid cancer by some other method: Tg, x-ray, biopsy, and so on. Although a few case reports are included in the tables, the final calculations used only those articles that described a series of patients.
Tables 1 to 3 show that 1311 imaging had a
Table 1. Comparison of 1311 and Z01TI Imaging of Residual or Recurrent Thyroid Carcinoma as Described in Eight Reports
No. Author
1311 + 1311 + 1311 _ lsll _ Thyroid Cancer True Positive Sensitivity Specificity Accuracy Comparison N 2~ + 2~ =~ + =~ ThCa+ ThCa- 1311 2OLTI 1311 2OLTI 2OlTIFP 2~ 1311 2~
1 Tonami (1980) Patients 28 3 0 10 15 12 16 2 Varma (1982) Lesions 40 4 11 2 23 16 24
3 Nemec (1984) Patients 15 0 0 6 9 8 7 4 Hoefnagel (1986) Patients 301 24 3 36 238 68 233
5 Brendel (1988) Lesions 51 17 26 6 2 51 0
6 Charkes (1990) Patients 49 10 2 2 6 20 29 7 Ramana (1991) Patients 51 17 4 19 11 41 10
8 Dadparvar (1993) Scans 53 9 12 9 23 25 28
Total 1 1 thru 8 588 84 58 90 327 241 347 Total 2 1, 2, 3, 4, 7, 8 488 57 30 82 319 170 318
Total 3 1, 2, 3, 7, 8 187 33 27 46 81 102 85
3 11 0.25 0.92 2 0.88 0.68 0.89
15 5 0.94 0.31 1 0.96 0.98 0.70 0 6 0.00 0.75 0 1.00 0.47 0.87
27 52 0.40 0,76 8 0,97 0.86 0,92 43 23 0.84 0.45 na na 0.84 0.45
12 17 0.63 0,85 0 1.00 0.84 0.94
21 33 0.51 0.80 3 0.70 0.61 0.76 20 14 0.80 0,56 4 0.86 0,91 0.72
141 161 0.59 0.67 18 0.86 0.83 0.83
86 121 0.51 0.71 18 0.94 0.83 0.86 59 69 0.58 0,68 10 0.88 0.77 0.77
Data from references 25-32. Abbreviations: No., series number; N, number; +, positive study; - , negative study; ThCA+, active disease; ThCa- , no evidence of
disease; FP, false positive. Total 1, includes data from all 8 reports; Total 2, includes data from 6 reports with imaging results in patients with and without active
thyroid cancer; Total 3, same as Total 2 except Hoefnagel study is omitted.

RADIOIODINE MANAGEMENT OF THYROID CANCER 157
Table 2. Comparison of 1311 and ~r~Tc Sestamibi Imaging of Residual or Recurrent Thyroid Carcinoma as Described in Five Reports
No. Author
1Sll + 1311 + lZll _ 1~11 _ Thyroid Cancer True Positive Sensitivity Specificity Accuracy
Comparison N MIBI + MIBI- MIBI + MIBI- ThCs+ ThCa- 1311 MIBI 1311 MIBI MIBIFP MIBI 13~1 MIBI
1 Yen (1994) Patients 37 4 0 14 19 22 15 4 18 0.18 0.82 0 1.00 0.51 0.89
2 Dadparvar (1995) Scans-post 1311 29 9 na 4 na 11 18 6 4 0.55 0.36 2 0.89 0.83 0.69
2a Dadparvar(1995) Scans-Pre1311 16 11 na 6 na 11 5 11 3 1.00 0.27 3 0.40 1.00 0.31
3 Russo (1996) Patients 73 10 3 6 54 23 50 13 15 0.57 0.65 1 0.98 0.86 0.88 4 Mayer (1996) Patients 70 19 8 18 25 56 14 27 37 0.48 0.66 0 1.00 0.59 0.73
5 Nemec(1996) Scans-Neck 212 na na 112 20 105 107 na 85 na 0.81 27 0.75 na 0.78
5a Nemec(1996) Scans-Lung 212 na na 27 185 19 193 na 18 na 0.95 9 0.95 na 0.95 5b Nemec(1996) Scans-Bone 212 na na 20 192 17 195 na 17 na 1.00 3 0.98 na 0.99
Total 1 ,2 ,3 ,4 ,5 421 42 11 154 118 217 204 50 159 0.71 0.73 30 0.85 0.60 0.79
Data from references 33-37.
Abbreviations: No., series number; N, number of subjects; ThCa+, active thyroid cancer; ThCa- , false positive.
Total includes data only from lines No. 1, 2, 3, 4, 5.
no evidence of thyroid cancer; FP,
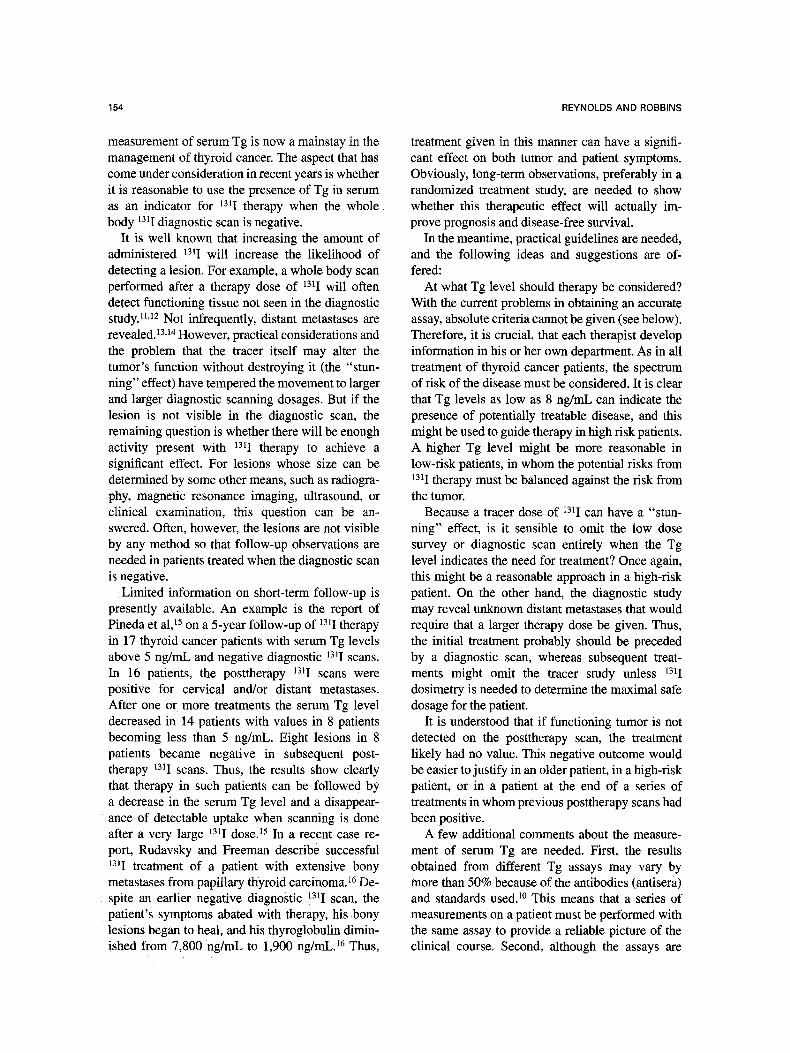
relatively low sensitivity (0.58, 0.50, 0.36, 0.71). This was probably attributable in part to the type of patients studied and to previous radioiodine therapy. The report of Nemec et al on 2~ imaging included only 131I negative patients. 27 The study by Yen et al of 99roTe sestamibi evaluated patients with Hurthle cell carcinoma which often does not concen- trate 1311.33 However, these reports contained only a small portion of the entire group that we reviewed. In a review of seven studies, Maxon and Smith found that only "about three fourths of recurrences and metastases from well differentiated [thyroid] adenocarcinoma are capable of concentrating 131I."47 Therefore, an 13q sensitivity of 100% should not be expected in patients being evaluated for recurrent or residual disease. In this light, the sensitivity of the other imaging modalities compares favorably with t3tI (0.68 for 2~ 0.73 for sestamibi, and 0.83 for FDG). Furthermore, the discordant scan results (ie, ~3tI positive with alternate radiopharmaceutical negative, or 131l negative with alternate positive), show that in many instances the alternate radiophar- maceutical alone gave more positives than did 131l alone (eg, 131I alone gave 27 whereas 2~ alone gave 46) (Table 1). The specificities of 2~ and 99mTc sestamibi imaging were 88% and 85%, respectively. The specificity of 18-FDG imaging was 95.8%. It should be remembered, however, that these studies included only patients with thyroid cancer, so that the calculated specificity does not carry over to patients with other type of neoplasms. Table 4 shows data from the only report in which a series of patients were studied with H qn pentetreotide. This study included only patients with active disease.
To better define the role of these procedures, we
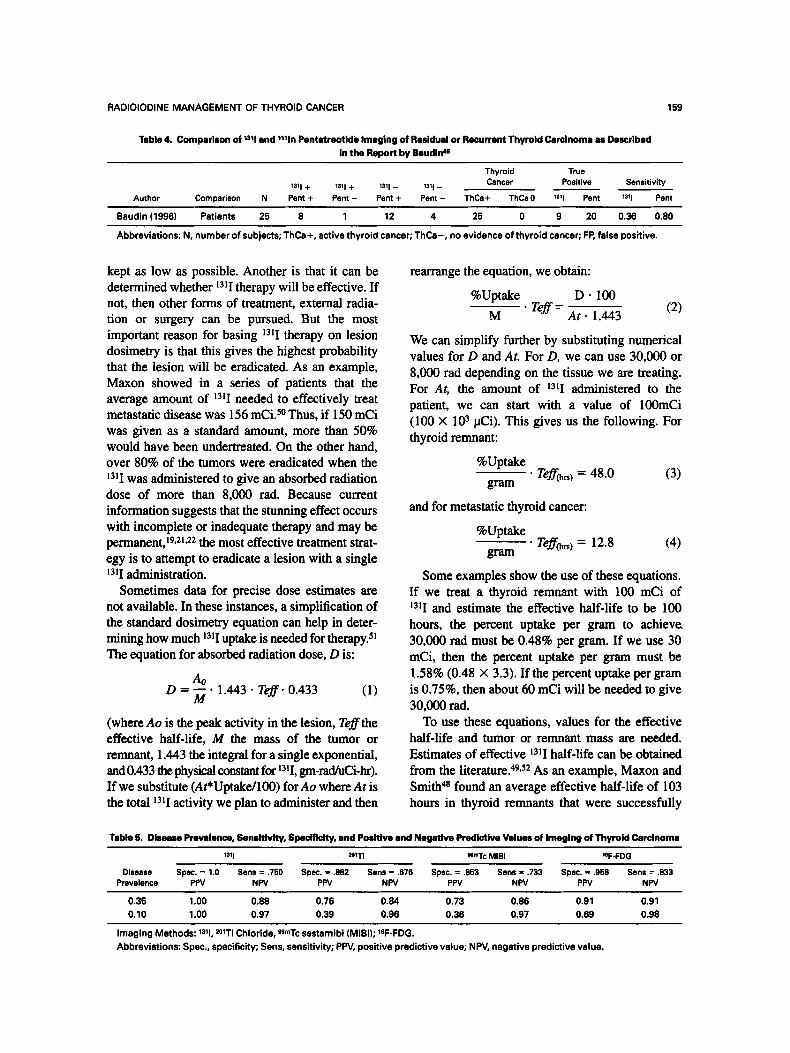
calculated their positive and negative predictive values for two different clinical situations? 6 We used data collated by Maxon and Smith 47 for disease prevalence realizing that the values for recurrence were probably an overestimate for any single point in time. At the time of initial therapy, about 35% of patients with papillary thyroid carci- noma have cervical node metastases. 48 Recurrent node metastases occur in about 10% of the pa- tients, as Sensitivity and specificity data were taken from Tables 1 to 3. For 131I, we used a sensitivity of 0.75.
Positive and negative predictive values are shown in Table 5. Because the four tests had similar sensitivity, their negative predictive values were also similar (Table 5) indicating that they were equally effective in ruling out disease. On the other hand, relatively small reductions in specificity of the radiopharmaceuticals reduced their positive predictive values and usefulness in identifying disease especially when the prevalence was <- 10%, as it might be for recurrent nodal disease. In this case, both 2~ and 99mTc sestamibi imaging had low positive predictive values making these agents less useful for screening for recurrent disease. Specificity, not sensitivity, seems to be the main issue for these radiopharmaceuticals. On the other hand, despite only modest sensitivity, 1311 (or 1231) is very useful for screening because of its almost perfect specificity.
How should 2~ and 99mTc sestamibi imaging be used to evaluate recurrent thyroid cancer? First, any findings should be interpreted in the light of other information such as serum Tg, histopathol- ogy, or posttherapy 131I scans. Second, the impact of lower specificity can be lessened by using these
158 REYNOLDS AND ROBBINS
O Q a,.
._= -=
(a r
E O g=
, - .o
o
.= ==
m ca
a,,
i M=
"O r
"6 .=_.
r e
t~
=.
I , , '
i; (.9
O
O
�9 i ~ ~ O ~ I~ r~ (~ ~t~ I
I Im O O O O O t o o3 ~
+
I,-
I t,.9
_r~ O O O O ~" LO r '~t 7n u - ~ r
+
N u-
I
+ ~
u .
+ + ~
g
d
~ = = = - = = g
5 ~ t'N tO ~1" I.O t.O I~ Z
.>
Q .
k.
e -
"O
> .
== "o
o I"
f-
8 e -
8 "to .w
o .>
+-
I-- ~g
t ;
.Q
E
,=
v ,_
�9 Z
O
pharmaceuticals in patients who likely have re- sidual, persistent or recurrent thyroid cancer. These would be high risk patients or those who continue to have evidence of disease. The reasonably high specificity of 18-FDG suggests that it may be useful in follow-up evaluations.
The alternative modalities may be useful for patients with elevated Tg levels, and negative diagnostic taxi scans, to identify tumors that can be surgically removed or to identify distant metastases that require m o r e 131I. However, several groups have shown that posttherapy 13~I scans are often positive, making proceeding directly to therapy reasonable. 12,15 Since disease location, prognosis, and the amount of lalI that is used for therapy are all related, imaging with these agents at the time of initial treatment or when new disease occurs may give a clearer understanding of what needs to be done. As an example, single-photon emission com- puted tomography (SPECT) 2mT1 images may show micronodular pulmonary metastases .when diagnostic 131I s c a n s are negative, z~
COMMENTS ON 1311 DOSIMETRY, HYPOTHYROIDISM AND WHOLE BODY 1311
KINETICS, AND THE USE OF LITHIUM IN THE MANAGEMENT OF RESIDUAL
THYROID CARCINOMA
13sI Dosimetry
At present most thyroid cancer patients are treated with standard fixed amounts of ~alI that have been found to be effective. However, recent publi- cations, particularly from Maxon et al have shown that basing the administered laq on the individual lesion radiation dosage can be very successful. 48 During diagnostic 131I scanning, serial conjugate images of the lesion are obtained over several days. From the uptake of activity, its turnover, and lesion size (or mass), the absorbed radiation dosage per mCi administered can be calculated. Maxon et al and O'Connell et al showed that absorbed radiation dosages above 8,000 to 10,000 rad are likely to eradicate metastatic thyroid cancer. 49,5~ Similarly, radiation dosages greater than 30,000 rad will usually ablate a thyroid remnant. 49,5~ Single admin- istrations of lalI achieving these levels will be effective in over 80% of thyroid cancer metastases and 94% of thyroid remnants. 48
Basing mI therapy on lesion dosimetry has several advantages. One is that patients are not over-treated and their overall radiation exposure is
RADIOIODINE MANAGEMENT OF THYROID CANCER
Table 4. Comparison of n~l end ~ l n Pentetrentide Imaging of Residual or Recurrent Thyroid Carcinoma as Described In the Report by Beudin 4e
159
Thyroid True Cancer Posit ive Sensitivity 1311 + lSll + 1Sll _ 1311 -
Author Comparison N Pent + Pent - Pent + Pent - ThCa+ ThCa 0 1311 Pent 1Sll Pent
Baudin (1886) Patients 25 8 1 12 4 25 0 9 20 0.36 0.80
Abbreviations: N, number of subjects; ThCa +, active thyroid cancer; ThCa-, no evidence of thyroid cancer; FP, false positive.
kept as low as possible. Another is that it can be determined whether mI therapy will be effective. If not, then other forms of treatment, external radia- tion or surgery can be pursued. But the most important reason for basing ~3~I therapy on lesion dosimetry is that this gives the highest probability that the lesion will be eradicated. As an example, Maxon showed in a series of patients that the average amount of ~31I needed to effectively treat metastatic disease was 156 mCi. 5~ Thus, if 150 mCi was given as a standard amount, more than 50% would have been undertreated. On the other hand, over 80% of the tumors were eradicated when the ~3~I was administered to give an absorbed radiation dose of more than 8,000 rad. Because current information suggests that the stunning effect occurs with incomplete or inadequate therapy and may be permanent, 19,21.22 the most effective treatment strat- egy is to attempt to eradicate a lesion with a single 131I administration.
Sometimes data for precise dose estimates are not available. In these instances, a simplification of the standard dosimetry equation can help in deter- mining how much mI uptake is needed for therapy. 5! The equation for absorbed radiation dose, D is:
Ao D = ~ - 1.443- Teff . 0.433 (1)
(where Ao is the peak activity in the lesion, Tef f the effective half-life, M the mass of the tumor or remnant, 1.443 the integral for a single exponential, and 0.433 the physical constant for 1 3 1 I , gm-rad/uCi-hr). If we substitute (At*Uptake/100) for Ao where At is the total 1311 activity we plan to administer and then
rearrange the equation, we obtain:
%Uptake D . 100 M �9 Teff = A t . 1.443 (2)
We can simplify further by substituting numerical values for D and At. For D, we can use 30,000 or 8,000 rad depending on the tissue we are treating. For At, the amount of 131I administered to the patient, we can start with a value of 100mCi (100 • 103 laCi). This gives us the following. For thyroid remnant:
%Uptake - - . Teff~m) = 48.0 (3)
gram
and for metastatic thyroid cancer:
%Uptake �9 Teff(~s)= 12.8 (4)
gram
Some examples show the use of these equations. If we treat a thyroid remnant with 100 mCi of 13q and estimate the effective haif-life to be 100 hours, the percent uptake per gram to achieve. 30,000 rad must be 0.48% per gram. If we use 30 mCi, then the percent uptake per gram must be 1.58% (0.48 x 3.3). If the percent uptake per gram is 0.75%, then about 60 mCi will be needed to give 30,000 rad.
To use these equations, values for the effective half-life and tumor or remnant mass are needed. Estimates of effective 13~I half-life can be obtained from the literature. 49,52 As an example, Maxon and Smith 4s found an average effective half-life of 103 hours in thyroid remnants that were successfully
Table 5. Disease Prevalence, Sensitivity, Specificity, and Positive and Negative Predictive Values of Imaging of Thyroid Carcinoma
nil =~ NmTc MIBI leF-FDG
Disease Spec.= 1.0 Sens= .750 Spat. = .882 Sens= .878 Spec. = .853 Sens= .733 Spec. = .968 Sena= .833 Prevalence PPV NPV PPV NPV PPV NPV PPV NPV
0.35 1.00 0.88 0.76 0.84 0.73 0.86 0.91 0.91 0.10 1.00 0.97 0.39 0.96 0.36 0.97 0.68 0.98
Imaging Methods: 1311, Z~ Chloride, UmTc sestamibi (MIBI); lSF-FDG. Abbreviations: Spec., specificity; Sens, sensitivity; PPV, positive predictive value; NPV, negative predictive value.

160 REYNOLDS AND ROBBINS
treated. In those where therapy was unsuccessful the average effective half-life was 56 hours. 48 In 48 successfully treated metastatic lesions of papillary thyroid carcinoma the average effective half-life was 79 hours. But in 6 lesions where therapy was unsuccessful the average effective half-life was 46 hours. Estimates of tumor mass or remnant size are sometimes difficult to obtain but can be made with computed tomography, MRI or ultrasound. How- ever, when lesions are small and not visible by one of these methods, a conservative approach for calculating absorbed radiation dosage is to use a value of 1 g. Hurley and Becker have suggested the use of arbitrary values for pulmonary metastases. 53 Those that are diffuse and not visible on a chest radiograph are considered to be 10 g. Metastases that are just visible are "assigned a mass" of 50 g.53 Two other factors are important. First, the distribu- tion of activity in large tumors is likely to be heterogeneous so that, compared with average theoretical values, areas of increased and decreased tumor radiation occur. Second, when tumors are very small, the fraction of radiation deposited within them is less than predicted with standard formulae. 54
If we want to treat a patient with elevated thyroglobulin and a negative diagnostic 131I scan, will there be enough activity in lesions for our treatment to be effective? In gamma camera :imag- ing, two elements that affect whether a lesion can be identified are the amount of accumulated activ- ity and the volume in which it is distributed. When accumulated activity is low, we may not be able to distinguish it from background. When the volume is smaller than the resolution of the camera, only a fraction of the activity is recorded, "the partial volume effect," reducing the apparent count level. Arnstein et al showed that when a constant amount of activity is imaged in progressively smaller volumes, the recorded counts decline to a level where the activity is no longer visible. 55 However, the smaller volumes contain higher concentrations of activity that potentially give larger radiation dosages. Activity in a very small volume may be sufficient for therapy even though it cannot be identified by gamma camera imaging. 55 In Arn- stein's experiments, the smallest source of 131I was 10 laL. Approximately 70% of the 13 radiation from 131I will be deposited in this volume. 54 About 50% will be deposited in 0.5 pL, approximately 1,000 ~rn in diameter. 54 From 1,000 to 100 pm, the
percentage of absorbed radiation diminishes to 7.7%. 54 Thus, 1311 therapy may be effective in very small lesions that are not visible by diagnostic scanning but it likely will be ineffective in isolated microscopic lesions less than 100 pm diameter.
Hypothyroidism and the Evaluation of Recurrent or Residual Thyroid Carcinoma
It seems to have been forgotten over the years that hypothyroidism during thyroid hormone with- drawal affects the whole body retention of 1311. At the 1948 Laurentian Conference, Keating and Al- bert described 131I kinetic studies in patients with various thyroid states and showed that the renal clearance of 131I was reduced by about one third in hypothyroid patients. 56 In 1955, Bricker et al showed that the reduced renal clearance of 1311 occurring with hypothyroidism was caused by a reduction in glomerular filtration rate and not an alteration in fluid volume. 57 Since renal excretion is the major route of 1311 clearance, prolonged whole body retention of 131I is to be expected with hypothyroidism. At the National Institutes of Health, paired studies during euthyroid and hypothyroid conditions showed that whole body 131I retention increased by about 50% during hypothyroidism. 58 What might result from this prolonged retention? On the one hand, the prolonged circulation of 13!I might increase the absorbed radiation dose particu- larly to the bone marrow. On the other hand, the greater whole body and blood retention may aug- ment 131I uptake by tumors, increasing the possibil- ity that they will be visualized 51 or adequately treated. Historically, thyroid hormone withdrawal has been an important step in preparing patients for 131I scanning and therapy. Beierwaltes stated that optimal scanning and therapy were only possible when thyroid hormone (thyroxine) was withdrawn for a period of 6 weeks. 59 Thus, thyroid hormone withdrawal and hypothyroidism may not only raise the TSH but also alter 131I kinetics augmenting the uptake of 131I.
Because the 131I radiation dose to bone marrow will be less during the euthyroid state, this is a distinct advantage of using rhTSH. On the other hand, remnant or tumor 131I uptake could be somewhat lower after rhTSH, leading to a different imaging or therapy result than is expected when based on conventional dosage of 131I. To date, the reported imaging results with rhTSH have been extremely promising even though whole body

RADIOIODINE MANAGEMENT OF THYROID CANCER 161
retention and thyroidal uptake were less than with hypothyroidism. 8,ss The differences in whole body retention present some interesting questions about therapy that may require reevaluation of the empiri- cally established doses that are currently in use.
Lithium as an Adjuvant to t~1I Treatment of Thyroid Cancer
Unsuccessful treatment with 131I is often related to poor retention of the isotope in the tumor. Maxon found that in 54 tumors, 48 responded to 131I, and that the effective half-life was nearly twice as long as in nonresponders. 49 Indeed, as shown by O'Connell et al, a shortened biological and effec- tive half-life may be the primary finding after ineffective therapy, s~ Because it inhibits thyroid hormone secretion and 131I release from prelabeled glands without affecting ~3~I uptake, lithium has been proposed as an adjuvant to 131I therapy. 6~ Studies in which lithium has been used in patients with differentiated thyroid cancer showed that it retarded the release of t31I from tumors and when used with ~31I therapy augmented the amount of radiation delivered. 61-6s In two of the studies, lithium was shown to augment the accumulation of J31I, an effect which likely is secondary to the blockade of iodine release. Movius et al studied the effects of lithium in 7 patients with differentiated thyroid cancer and found a median increase in the biologic half-life of 52%. 63 An important finding was that the effective half-life (and radiation dos- age to the tumor) increased by more than 25% only when the initial biological half-life was less than 6 days. 6s As expected, lithium is more effective in metastases that have rapid t31I turnover. We have used lithium carbonate in selected patients and have found it to prolong the effective half-life and increase 131I accumulation in lesions in over 50% of these patients. ~ One could argue that lithium should be given to every high-risk patient, but it would be preferable to give it to patients known to have rapid ~3~I turnover.
Lithium is administered orally as lithium carbon- ate, 300 mg three times daily. 6~ Blockade of thyroidal iodine release occurs when serum levels are between 0.6 and 1.2 mEq/L, the same concentra- tions that are used in treating patients with manic- depressive disorder. 6~ Side effects occur when serum concentrations are greater than 1.5 mEq/L and can be serious when levels approach 2.0 mEq/L. 6~ Because of this narrow therapeutic index,
serum levels are measured daily in the morning. Target concentrations are usually achieved within 2 to 3 days at which time the patient is treated with 131I. After administration of the 131I, lithium carbon- ate is continued for about 5 days, but during this time, the level cannot be measured because of radiation safety considerations.
The patients have had no significant lithium side effects probably because they were treated for only short periods of time. But because lithium is excreted almost entirely in the urine and itself can cause nephrogenic diabetes insipidus, we evaluate the patient's renal function and overall level of hydration before beginning therapy. The first pa- tient that we treated with lithium, (1975) did have an unexpectedly high-level of whole body radiation with ~3q therapy.61 This was caused by the release of a large amount of 131I-labeled Tg and other proteins from the tumor. However, the calculated tumor-absorbed radiation during therapy was not significantly different than had been predicted with tracer studies. 61 It is likely then that the uptake of 131I in this patient's massive cancer was heteroge- neous and the radiation to one area was unexpect- edly high, an effect that more likely was related to characteristics of the tumor and not to the use of lithium.
CONCLUSION
With treatment currently available, a high propor- tion of patients with differentiated thyroid carci- noma can be cured. So modification of conven- tional practice must be based on clear and rational goals. The principal reason for using rhTSH to prepare patients for 131I scanning is to avoid the disturbing symptoms, potential hazard, and loss of productive time associated with hypothyroidism. As expected, symptoms experienced by clinical trial patients were markedly less in the euthyroid/ rhTSH phase than during hypothyroidism, s.9 More importantly, diagnostic 131I scanning detected as many lesions following rhTSH as with the hypothy- roid preparation. 8 During hypothyroidism retention of 131I in the whole body and blood was increased. While this did not appear to affect the results of diagnostic imaging, s it may alter therapy with ~3q. It is likely that the amount of 131I administered will need to be increased by as much as 50% in patients who are prepared with rhTSH, ss Further informa- tion is needed and this will require careful lesion dosimetry studies. At this time, administration of

162 REYNOLDS AND ROBBINS
rhTSH has proven to be effective preparation for diagnostic scanning. However, its optimal use during therapy will need further study.
The rationale for administering 1311 therapy to patients with abnormal thyroglobulin and normal nonlocalizing diagnostic scans is to eliminate the disease at a t ime when it is small. When 131I therapy has been given in this way, follow-up studies have shown decreases of thyroglobulin and disappear- ance of 131I posit ive areas in the posttherapy scans. The long-term benefit of this treatment and its effect on recurrence and survival is unknown. A possible negative feature of this approach is that extremely small tumor deposits may be under- treated making them less susceptible to later therapy either because of stunning or cell selection. A common result of treating microscopic disease in the lung is long-term remission or cure, so there should be opt imism that this treatment will be effective. However, more experience and longer follow-up data are needed.
It is clear that scanning dosages of 131I can alter the function of thyroid remnant and metastatic tumor, making them less able to accumulate 1311
and probably less susceptible to therapy. Lowering the diagnostic dose of 1311, substituting 1231, using
another imaging radiopharmaceutical or eliminat- ing low dose 131I imaging altogether are possible solutions to this problem. Because of its extremely high specificity, scanning with 1311 (or 123I) provides
diagnostic information as well as the location o f the tumor. Lowering the amount of 131I used for
pretherapy imaging reduces the l ikelihood of stun- ning but makes the study less sensitive. To date, 123I has not been proven to be as accurate as 131I for recurrent disease or distant metastases, but these studies used only 300 laCi of 1231.24 A larger amount of 123I, such as 2 to 3 mCi, should increase the sensitivity of imaging, but, of course, will be more expensive. The lower specificity of 2~ and 99mTc sestamibi makes it necessary to use these agents in selected situations and with supporting corrobora- tive information. Initial studies suggest that 18- FDG has a relatively high sensitivity and specificity when used in patients with differentiated thyroid carcinoma. With the development of SPECT cam- eras for positron emitting radiopharmaceuticals, imaging with 18-FDG may become important in this area, as it has in the evaluation of other tumors. 67
As discussed earlier, the principal reasons for basing 1311 therapy on actual lesion radiation are to lessen the chance of undertreatment and to decide if 13q will be effective at all. Formal lesion dosimetry is cumbersome and time consuming but if we are to give optimal 1311 therapy then information about its uptake and turnover is needed. Rapid tumover of 1311 appears to be responsible for failure of response in some tumors. For these, l i thium can be used to prolong the retention of 1311.
REFERENCES
1. Kaplan MM (ed): Thyroid Carcinoma. Endocrinol Metab Clin NorthAm 19:3, 1990
2. Burman KD (ed): Thyroid Cancer. Endocrino ! Metab Clin North Am 24:4, 1995
3. Wondisford FE, Radovick S, Moates, JM, et al: Isolation and characterization of human thyrotropin beta-subunit gene. J Biol Chem 263:12538-12542, 1988
4. Thotakura NR, Desal RK, Bates LG, et al: Biologic activity and metabolic clearance of a recombinant human thyrotropin in Chinese Hamster ovary cells. Endocrinology 128:341-348, 1991
5. Huber GK, Fon P, Concepcion ES, Davies TF: Recombi- nant human thyroid-stimulating hormone-Initial bioactivity as- sessment using human fetal thyroid cells. J Clin Endocrinol Metab 72:1328-1331, 1991
6. Cole ES, Lee K, Lauziere K, et al: Recombinant human thyroid stimulating hormone: development of a biotechnology product for detection of metastatic lesions of thyroid carcinoma. Biotechnology 11:1014-1024, 1993
7. Braverman LE, Pratt BM, Ebner S, et al: Recombinant human thyrotropin stimulates thyroid function and radioactive iodine uptake in the Rhesus monkey. J Clin Endocrinol Metab 74:1135-1139, 1992
8. Meier CA, Braverman LE, Ebner SA, et al: Diagnostic use
of human recombinant thyrotropin in patients with thyroid carcinoma (phase I/II study). J Clin Endocrinol Metab 78:181- 196, 1994
9. Szkudlinski MW, Thotakura NR, Bucci R, et al: Purifica- tion and characterization of recombinant human thyrotropin (TSH) isoforms produced by Chinese hamster ovary cells. The role of sialylation and sulfation in TSH bioactivity. Endocrinol- ogy 133:1490-1503, 1993
10. Spencer CA, Wang C-C: Thyroglobulin Measurements: Techniques, Clinical Benefits, and Pitfalls. Endocrinol Metab Clin North Am 24:841-863, 1995
11. Nemec J, Rohling S, Zamrazil V, et al: Comparison of the distribution of diagnostic and thyroablative I-131 in the evalua- tion of differentiated thyroid cancers. J Nucl Med 20:92-97, 1979
12. Pacini F, Lippi F, Formica N, et al: Therapeutic doses of iodine-131 reveal undiagnosed metastases in thyroid cancer patients with detectable serum thyroglobulin levels. J Nucl Med 28:1888-1891, 1987
13. Schlumberger M, Tubiana M, De Vathaire F, et al: Long-term results of treatment of 283 patients with lung and bone metastases from differentiated thyroid carcinoma. J Clin Endocrinol Metab 63:960-967, 1986
14. Schlumberger M, Arcangioli O, Piekarski JD, et al:

RADIOIODINE MANAGEMENT OF THYROID CANCER 163
Detection and treatment of lung metastases of differentiated thyroid carcinoma in patients with normal chest X-rays. J Nucl Med 29:1790-1794, 1988
15. Pineda JD, Lee T, Ain K, et al: Iodine-131 Therapy for thyroid cancer patients with elevated thryoglobulin and negative scan. J Clin Endocrinol Metab 80:1488-1492, 1995
16. Rudavsky AZ, Freeman LM: Treatment of scan negative, thyrogiobulin positive metastatic thyroid cancer using radioio- dine 1-131 and recombinant human thyroid stimulating hor- mone. J Clin Endocrinol Metab 82:11-14, 1997
17. Ozata M, Suzuki S, Miyamoto T, et al: Serum thyroglobu- lin in the follow-up of patients with treated differentiated thyroid cancer. J Clin Endocrinol Metab 79:98-105, 1994
18. Sherman SI, Tielens ET, Sostre S, et al: Clinical utility of posttreatment radioiodine scans in the management of patients with thyroid carcinoma. J Clin Endocrinol Metab 78:629-634, 1994
19. Rawson RW, Rail JE, Peacock W; Limitations and indications in the treatment of cancer of the thyroid with radioactive iodine. J Clin Endocrinol 11:1128-1142, 1951
20. Hurley JR, Beeker DV: The use of radioiodine in the management of thyroid cancer, in Freeman LM, Weissman HS (eds): Nuclear Medicine Annual. New York, NY, Raven 1983, pp 329-384
21. Jeevanram RK, Shah DH, Sharma SM, et al: Influence of initial large dose on subsequent uptake of therapeutic radioio- dine in thyroid cancer patients. Nucl Med Binl 13:277-279, 1986
22. Park HM, Perkins OW, Edmondson JW, et al: Influence of diagnostic radioiodines on the uptake of ablation iodine- 131. Thyroid 4:49-54, 1994
23. Kim CK, Tse K, San Pedro E, et al: Influence of various scanning doses on subsequent 1-131 ablation of thyroid rem- nants. J Nucl Med 35:14, 1994
24. Park H-M, Park Y-H, Zhou X-H: Detection of thyroid remnant/metastasis without stunning: An ongoing dilemma-The diagnostic accuracy of 1231 and 1311 as scanning agents and their
effect on the outcome of radioablation therapy. Thyroid 7:277- 280, 1997
25. Tonami N, Hisada K: 2~ Scintigraphy in post operative detection of thyroid cancer; A comparative study with 1-131. Radiology 136:461-464, 1980
26. Varma V, Reba R: Comparative study of TI-201 and I-13 l scintigraphy in postoperative metastatic thyroid carcinoma, in Raynard C (ed): Nuclear Medicine and Biology. Proceedings 3rd World Congress of Nuclear Medicine and Biology (vol I). Paris, France, Pergamon, 1982, pp 103-104
27. Nemec J, Zamrazil V, Pohunkova D, et al: The rational use of 2~ scintigraphy in the evaluation of differentiated thyroid cancer. Eur J Nucl Med 9:261-264, 1984
28. Hoefnagel CA, Delprat CC, Marcuse HR, et al: Role of Thallium-201 total-body scintigraphy in follow up of thyroid cancer. J Nucl Med 27:1854-1857, 1986
29. Brendel AJ, Guyot M, Jeanot R, et al: Thallium-201 imaging in the follow-up of differentiated thyroid carcinoma. J Nucl Med 29:1515-1520, 1988
30. Charkes DN, Vitti RA, Brooks K: Thallium-201 SPECT increases detectability of thyroid cancer metastases. J Nucl Med 31:147-153, 1990
31. Ramanna L, Waxman A, Braunstein G: Thallium-201 scintigraphy in differentiated thyroid cancer; comparison with
radioiodine scintigraphy and serum thyroglobulin determina- tions. J Nucl Med 32:441-446, 1996
32. Dadparvar S, Krishna L, Brady LW, et al: The role of Iodine- 131 and Thallium-201 imaging and serum thyroglobulin in the management of differentiated thyroid carcinoma. Cancer 71:3767-3773, 1993
33. Yen T-C, Lin HD, Lee CH, et al: The role of technetium- 99m sestamibi whole-body scans in diagnosing metastatic Hurthle cell carcinoma of the thyroid gland after total thyroidec- tomy: a comparison with iodine-131 and thallium-201 whole- body scans. Eur J Nucl Med 21:980-983, 1994
34. Dadparvar S, Chevres A, Tulchinsky M, et al: Clinical utility of Technetium-99m Methoxyisobutylisonitrile imaging in differentiated thyroid carcinoma: comparison with Thalliuni- 201 and Iodine-131 scintigraphy, and serum thyroglobulin quantitation. Eur J Nucl Med 22:1330-1338, 1995
35. Russo R, Col A, Cappaglig M, et al: 99mTc-Sestamibi scan in the follow-up of differentiated thyroid carcinoma. Eur J Nucl Med 23:55, 1996
36. Meyer G, Kleine U, Tiling R, et al: Tc-99m-Sestamibi whole body scintigraphy: An useful tool in the follow-up of patients with differentiated thyroid carcinoma. Eur J Nucl Med 23:$5, 1996 (abstr)
37. Nemec J, Nyvitova O, Blazek T, et al: Positive thyroid cancer scintigraph using technetium-99m methoxyisobutylisoni- trile. Eur J Nucl Med 23:69-71, 1996
38. Joensuu H, Ahonen A: Imaging of metastases of thyroid carcinoma with Fluorine-18 fluorodeoxyglucose. J Nucl Med 28:910-914, 1987
39. Sisson JC, Ackerman RJ, Meyer MA, et al: Uptake of 18 fluoro-2-deoxy-D-glucose by thyroid cancer: Implications for diagnosis and therapy. J Clin Endo Med 77:1090-1095, 1993
40. Blahd WH, Khonsary SA, Brown CV, et al: Thyroid cancer imaging with PET FDG. J Nucl IVied 34:12, 1993
41. Scott CG, Meier DA, Dickinson CZ: Cervical lymph node metastasis of thyroid papillary carcinoma imaged with Fluorine-18-FDG, Technetium-99m Pertechnetate and Iodine- 131 Sodium Iodine. J Nucl Med 36:1843-1845, 1995
42. Fridrich L, Messa C, Landoni C, et al: PET/[F-18]FDG and I-131 scintigraphy in patients with thyroid carcinoma. Eur J Nucl MOd 21:780, 1994
43. Feine U, Lietzemayer R, Hanke JP, et al: lg FDG whole body PET in differentiated thyroid carcinoma: Flip flop in uptake patterns of 18-FDG and I-131. Nuklearrnedizin 34: ! 27- 134, 1995
44. Grunwald F, Schomburg A, Bender H, et al: Fluorine-18 fluorodeoxyglucose positron emission tomography in the fol- low-up of differentiated thyroid cancer. Eur J Nucl Med 23:312-319, 1996
45. Baudin E, Schlumberger M, Lumbroso J, et al: Oetreo- tide scintigraphy i n patients with differentiated thyroid carci- noma: Contribution for patients with negative radioiodine scan. J Clin Endocrinol Metab 81:2541-2544, 1966
46. McNeil B J, Rutter CM: Methods for Evaluating New Tests, in Harbert JC, Eckelman WC, Neumanh RD, (eds): Nuclear Medicine: Diagnosis and Therapy. New York, NY, Thieme, 1996, pp 939-947
47. Maxon RH, Smith HS: Radioiodine-131 in the diagnosis and treatment of metastatic well differentiated thyroid cancer. Endocrinol Metab Clinics North Am 19:685-718, 1990
48. Maxon HR, Angler EE, Thomas SR, et al: Radioiodine- 131 therapy for well-differentiated thyroid cancer--a quantita-

164 REYNOLDS AND ROBBINS
tive radiation dosimetric approach: outcome and validation in 85 patients. J Nucl Med 33:1132-1136, 1992
49. Maxon HR, Thomas SR, Hertzberg VS, et al: Relation between effective radiation dose and outcome of radioiodine therapy for thyroid cancer. N Engl J Med 309:937-941, 1983
50. O'Connell ME, Flower MA, Hinton PJ, et al: Radiation dose assessment in radioiodine therapy. Dose-response relation- ships in differentiated thyroid carcinoma using quantiiatix~e scanning and PET. Radiother Onco128:16-26, 1993
51. Reynolds JC: Percent 1-131 uptake and post therapy 1-131 scans: their role in the management of thyroid cancer. Thyroid 7:281-284, 1997
52. Schlesinger T, Flower MA, McCready VR: Radiation dose assessments in radioiodine (1311-131) therapy. 1. The necessity for in vivo quantitation and dosimetry in the treatment of carcinoma of the thyroid. Radiother Oncol 14:35-41, 1989
53. Hurley JR, Becker DV: Treatment of Thyroid Carcinoma with Radioiodine, in Gottschalk A, Hoffer PB, Potchen EJ, et al (eds): Diagnostic Nuclear Medicine, Baltimore, Williams & Wilkins, 1989, pp 792-814
54. Quimby EH, Feitelberg S, Gross W: Radioactive Nu- clides in Medicine and Biology: Basic Physics and Instnimenta- tion. Philadelphia, PA, Lea & Febiger, 1970, p 114
55. Arnstein NB, Carey JE, Spaulding SA, et al: Determina- tion of Iodine-131 diagnostic dose for imaging metastatic thyroid cancer. J Nucl Med 27:1764-1769, 1986
56. Keating FR, Albert A: The metabolism of iodine in man as disclosed with the use of radioiodine. Recent Prog Hormone Res 4:429-481, 1949
57. Bricker NS, Hlad CJ: Observations on the mechanism of the renal clearance of 1TM. J Clin Invest 34:1057-1072, 1955
58. Park S-G, Reynolds JC, Brucker-Davis F, et al: Iodine kinetics during 1-131 scanning in patients with thyroid cancer: comparison of studies with recombinant human TSH (rhTSH) vs. hypothyroidism. J Nucl Med 37:15, 1996
59. Beierwaltes WH: The treatment of thyroid carcinoma with radioactive iodine. Semin Nucl Med 8:79-94, 1978
60. Temple R, Berman M, Carlson HE, et al: The use Of lithium in Graves' disease. Mayo Clin Proc 47:872-879, 1972
61. Gersheng0rn MC, Izumi M, Robbins J: Use of lithium as an adjunct to radioiodine therapy of thyroid carcinoma. J Clin Endocrinol Metab 42:105-111, 1976
62. Briere J, Pousse G, Darsy P, et al: Tile advantage of lithium in association with iodine 131 in the treatment of functiOning metastasis of thyroid cancer. Ann Endocrino135:281: 282, 1974
63. Rasmusson B, Olsen K, Rygard J: Lithium as adjunct to 1-131 therapy of thyroid carcinoma. Acta Endocrinologica 74:252(s), 1983
64. Pons F, Carrio I, Estorch M, et al: Lithium as an adjuvant of Iodine-131 when treating patients with Well-differentiated thyroid carcinoma. Clin Nucl Med 12:644-647, 1987
65. Movius EG, Robbins J, Pierce LR, et al: The value of lithium in radioiodine therapy of thyroid carcinoma, in Medeiros~ Neto G, Gaitan E (eds): Frontiers in Thyroidology. New York, NY, Plenum, 1986, pp 1269-1272
66. Konng S-S, Movius EG, Keenan AM, et al: The effect of lithium in radioiodine therapy of metaStatic well differentiated thyroid Carcinoma. J Nucl Med 36:15, 1995 (abstr)
67. Strauss LG, Conti PS: The applications of PET in clinical oncology. J Nucl Med 32:623-628, 1991
Related Documents











