1998;65:137-143 Ann Thorac Surg Nistal and José M. Revuelta José M. Bernal, José M. Rabasa, Francisco Gutierrez-Garcia, Carlos Morales, J. Francisco The CarboMedics Valve: Experience With 1,049 Implants http://ats.ctsnetjournals.org/cgi/content/full/65/1/137 the World Wide Web at: The online version of this article, along with updated information and services, is located on ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1998 by The Society of Thoracic Surgeons. Print is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 2, 2013 ats.ctsnetjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1998;65:137-143 Ann Thorac SurgNistal and José M. Revuelta
José M. Bernal, José M. Rabasa, Francisco Gutierrez-Garcia, Carlos Morales, J. Francisco The CarboMedics Valve: Experience With 1,049 Implants
http://ats.ctsnetjournals.org/cgi/content/full/65/1/137the World Wide Web at:
The online version of this article, along with updated information and services, is located on
ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1998 by The Society of Thoracic Surgeons. Print
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from

The CarboMedics Valve: Experience With 1,049ImplantsJose M. Bernal, MD, Jose M. Rabasa, MD, Francisco Gutierrez-Garcia, MD,Carlos Morales, MD, J. Francisco Nistal, MD, and Jose M. Revuelta, MDDepartment of Cardiovascular Surgery, Hospital Universitario Valdecilla, Universidad de Cantabria, Santander, Spain
Background. The lack of valve rotatability, the struc-tural deterioration, and the rate of valve-related compli-cations with the standard mechanical bileaflet prosthesisled to the development of a new second-generationbileaflet valve in 1986.
Methods. Between January 1989 and March 1994, 1,049CarboMedics valves were implanted in 859 patients. Therotatability was used in 109 mitral prostheses (21.5%) andin 61 aortic prostheses (11.6%). Follow-up was 97.1%complete, with 3,049 patient-years.
Results. The hospital mortality was 6.9% for the mitralgroup, 3.4% for the aortic group, and 10.7% for thedouble-valve group (p < 0.005). The actuarial survivalcurve at 5 years was 77.3% 6 3.6%, 90.1% 6 2.5%, and79.2% 6 3.7% (p 5 0.0003), freedom from thromboembo-
lism was 89.1% 6 3.6%, 87.1% 6 3.8%, and 68.8% 6 8.2%,freedom from reoperation was 95.9% 6 1.4%, 98.9% 60.6%, and 94.9% 6 2.4%, and freedom from valve-relatedcomplications was 68.8% 6 4.1%, 79.5% 6 3.5%, and55.3% 6 5.9% after mitral, aortic, and mitral and aorticvalve replacement, respectively. There were five episodesof valve thrombosis, but no structural deterioration oc-curred.
Conclusions. The clinical performance of the Carbo-Medics valve is quite satisfactory, with a low incidenceof valve-related mortality and morbidity. The rotatabilityfeature was useful when the native valve was preservedor for repeat valve replacement.
(Ann Thorac Surg 1998;65:137–43)© 1998 by The Society of Thoracic Surgeons
The CarboMedics bileaflet prosthetic heart was intro-duced for clinical use in 1986. The CarboMedics
heart valve is a bileaflet pyrolitic carbon heart valve,different from the St. Jude Medical prosthesis in severalcharacteristics including the Biolite carbon-coveredblood contacting surface on the sewing ring, the valvepivot design with absence of pivot guards, the presenceof a titanium stiffening ring, and particularly the rotat-ability of the valve after implantation. This mechanicalprosthesis has two leaflets that sit at an angle of 25degrees in the closed position and open to 53 degreesfrom the closed to the open position, or 78 degrees fromthe plane of the ring. The hemodynamic performanceboth in vitro and in vivo has been reported earlier, withsatisfactory results similar to those of other widely usedbileaflet prostheses [1–4]. The largest clinical experiencewith this prosthesis was described by Copeland [5] andthe investigators of the international, multicenter study,with an average follow-up of 30.2 months.
The CarboMedics valve has been our mechanical pros-thesis of choice since 1989, when the first valve wasimplanted in our institution. We were encouraged by thementioned characteristics, particularly its rotatability inour patient population with a high rate of valve reopera-tions. Since then, 1,049 prostheses have been implantedin 859 patients with a total follow-up of 3,049 patient-years. The object of the present study is to analyze the
clinical experience with this second-generation bileafletvalve.
Material and Methods
Between January 1989 and March 1994, 859 consecutivepatients underwent valve replacement with a CarboMed-ics valve (CarboMedics, Inc, Austin, TX) in our institutionand have had at least 12 months of follow-up. This groupcomprised 386 women, (44.9%) and 473 men (55.1%), witha mean age of 55.2 6 10.6 years (range, 15 to 78 years).Most of the patients were in the sixth and seventh decadeof life (n 5 594, 69.2%). Mitral valve replacement (MVR)was performed in 330 patients (38.4%), aortic valve re-placement (AVR) in 349 patients (40.6%), double-valvereplacement (DVR) in 177 patients (20.6%), and isolatedtricuspid, pulmonary, or tricuspid and pulmonary valvereplacement in 3 patients (0.4%). There were 526 aortic,507 mitral, 14 tricuspid, and 2 pulmonary valves im-planted, for a total of 1,049 CarboMedics prostheses. Aprimary valve replacement was performed in 569 pa-tients (66.2%) and a repeat valve replacement in theremaining 290 patients (33.8%). A bioprosthesis wasexplanted in 227 patients, with a mean interval of 94.2 636.9 months. In our early series [6, 7] a bioprosthesis wasmainly indicated when valve repair was not feasible, dueto our patient population characteristics, not after anadequate anticoagulation regimen after valve replace-ment. Among the patients having primary valve replace-ment, 20 patients had a previous closed mitral commis-surotomy and 6 had a percutaneous mitral valvuloplasty.
Accepted for publication Aug 25, 1997.
Address reprint requests to Dr Bernal, Cirugıa Cardiovascular, HospitalUniversitario Valdecilla, 39008-Santander, Spain.
© 1998 by The Society of Thoracic Surgeons 0003-4975/98/$19.00Published by Elsevier Science Inc PII S0003-4975(97)01238-1
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
According to the New York Heart Association, 32 patientswere in functional class I (3.7%), 172 in class II (20.0%),530 in class III (61.7%), and 125 in class IV (14.6%)preoperatively. Patients in class I were operated on forsevere aortic stenosis, progressive left ventricular dys-function, or significant structural deterioration of a pre-vious bioprosthesis.
The cause of valve disease in the primary valve re-placement group was predominantly rheumatic heartvalve disease. Those 3 patients who had isolated tricus-pid, pulmonary, or tricuspid and pulmonary valve re-placement were excluded from this study.
From the repeat valve replacement group, 43 patientshad a previous open valve repair (14.8%) and 247 aprevious valve replacement (85.2%). The causes of valvedisease in the AVR, MVR, and DVR groups are shown inTable 1. Preoperative clinical data are summarized inTable 2.
All patients were operated on with standard cardiopul-monary bypass with moderate hypothermia (28° to 30°C).Myocardial protection was assured with either crystalloid
or blood cardioplegia delivered antegrade, retrograde, orboth ways. Surgical technique for valve implantation inall positions consisted in 2-0 pledget-supported U-Tycron (Ethicon Ltd, Edinburgh, UK) everting sutures (12to 15 sutures per valve).
For mitral valves, sizes 27 and 29 were most common,and for aortic valves, sizes 21 and 23 were most common.The rotation feature of the CarboMedics valve was usedin 109 mitral prostheses (21.5%) and in 61 aortic prosthe-ses (11.6%). Orientation of the mitral valve was mostcommonly in the anatomic position, whereas the orien-tation of the aortic prosthesis was most commonly trans-verse with pivots at the midpoint of the noncoronary cuspand in the commissure between the right and left cusps.
In the MVR group, the posterior mitral leaflet waspreserved in 84 patients (25.5%), the anterior in 4 (1.2%),and both (transvalvular implantation) in 19 (5.8%). Bothleaflets were resected in 172 patients (52.1%), and thisinformation was not reported in 51 instances (15.5%). Inthe DVR group, the posterior mitral leaflet was preservedin 38 patients (21.5%) and both leaflets were preserved in3 (1.7%). Nonleaflet preservation or previous valve re-placement occurred in 102 patients (57.6%), and leafletpreservation was not reported in 34 patients (19.2%).
Associated cardiac procedures are summarized in Ta-ble 3. One hundred twenty-nine patients from the MVRgroup required an associated cardiac procedure (39.1%).
Thromboembolic ProphylaxisAnticoagulation with acenocoumarol was started 48hours after the CarboMedics valve implant. No heparinwas given before the procedure. The international nor-malized ratio was maintained within a range of 2.5 to 3.5in those patients in sinus rhythm and between 3.0 and 4.5when atrial fibrillation was present. Patients undergoingcoronary artery bypass grafting received aspirin (125 to
Table 1. Cause of Valve Diseasea
Cause MVR AVR DVR
Rheumatic 161 (48.8) 115 (33.0) 85 (48.0)Degenerative/calcification 14 (4.2) 95 (27.2) 2 (1.1)Congenital 2 (0.6) 23 (6.6) . . .Ischemic 16 (4.8) . . . . . .Infective endocarditis 5 (1.5) 25 (7.2) 9 (5.1)Previous valve repair 28 (8.5) 10 (2.9) 5 (2.8)Previous valve replacement 94 (28.5) 77 (22.1) 76 (42.9)Unknown/not reported 10 (3.0) 4 (1.1) . . .
a Numbers in parentheses are percentages.
AVR 5 aortic valve replacement; DVR 5 double-valve replacement;MVR 5 mitral valve replacement.
Table 2. Preoperative Clinical Data
Variable MVR AVR DVR
Age (y)Mean 6 SD 55.4 6 10.4 55.3 6 10.9 55.1 6 9.8Range 22–75 15–78 24–75
Male/female 125/205 259/90 88/89NYHA class
I & II 15.6% 35.9% 15.7%III 67.8% 55.8% 62.0%IV 16.6% 8.3% 22.3%
Previousthromboembolism
71 (21.5%) 25 (7.2%) 31 (17.5%)
Sinus rhythm 26.9% 85.3% 30.4%Atrial fibrillation 73.1% 14.7% 69.6%Primary valve
replacement206 (62.4%) 275 (78.8%) 88 (49.7%)
Repeat valvereplacement
124 (37.6%) 74 (21.2%) 89 (50.3%)
AVR 5 aortic valve replacement; DVR 5 double-valve replacement;MVR 5 mitral valve replacement; NYHA 5 New York Heart Associ-ation; SD 5 standard deviation.
Table 3. Associated Cardiac Operations
Operation MVR AVR DVR
Tricuspid commissurotomy 3 1 3Tricuspid annuloplasty 54 3 20Mechanical TVR 9 . . . 4Bioprosthetic TVR . . . 1 3CABG 17 29 5Left atrial thrombectomy 40 . . . 13ASDa 5 . . . . . .Congenital disease 1 1 2Mitral commissurotomy . . . 10 . . .Mitral valve repair . . . 4 . . .Aortic root enlargement . . . 5 . . .Ascending aorta
aneurysmectomy. . . 14 . . .
Total 129 (39.1%) 68 (19.5%) 50 (28.2%)
a Iatrogenic after percutaneous mitral valvuloplasty.
ASD 5 atrial septal defect; AVR 5 aortic valve replacement;CABG 5 coronary artery bypass grafting; DVR 5 double-valve re-placement; MVR 5 mitral valve replacement; TVR 5 tricuspidvalve replacement.
138 BERNAL ET AL Ann Thorac SurgTHE CARBOMEDICS VALVE 1998;65:137–43
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
200 mg per day). However, this thromboembolic prophy-laxis was modified according to patient requirementduring follow-up.
Follow-upThe follow-up data were procured over a 6-month periodbetween October 1994 and April 1995. From 802 patientsdischarged, follow-up was obtained in 779 patients.Those patients were followed up directly in our outpa-tient clinic, mailed questionnaires, or contacted directlyby telephone. The completeness of follow-up during theclosing interval was 97.1%. The mean follow-up was 46.2months, ranging from 12 to 76 months. Cumulativefollow-up was 3,049 patient-years.
Statistical AnalysisAll valve-related mortality and complication definitionsfollow the guidelines approved by the Ad Hoc LiaisonCommittee for Standardizing Definitions of ProstheticHeart Valve Morbidity [8]. All continuous variables arepresented as mean 6 standard deviation. Basic methodsof univariate analysis included the x2 and Student’s t test.Actuarial curves were obtained by the life-table method.The Patient Analysis and Tracking System database,version 06.02.03 (Dendrite Clinical Systems, Inc, Port-land, OR), was used for collection and analysis of data.
Results
Hospital and Late MortalityThere were 54 hospital deaths, with a total mortality of6.3%. Mortality for the MVR group was 6.97% (23/330),for the AVR group 3.44%, (12/349), and for the DVR group10.73% (19/177) (p , 0.005). The causes of hospital mor-tality were most often related to low cardiac outputsyndrome (n 5 27) or hemorrhage (n 5 15). Other causeswere sepsis (n 5 5), respiratory insufficiency (n 5 4), andsudden unknown death (n 5 3) (postmortem examina-
tion was not allowed by the family) (Table 4). Late deathoccurred in 44 patients. Late mortality was 7.3% in theMVR group, 2.9% in the AVR group, and 5.6% in the DVRgroup (p , 0.025). The most common cause of late deathwas cardiac failure (21/44). Twenty-one patients died ofvalve-related causes (thromboembolism in 3, sudden/unknown death in 14, mitral valve thrombosis in 1, sepsisin 2, and hemorrhage in 1). Other causes are summarizedin Table 4.
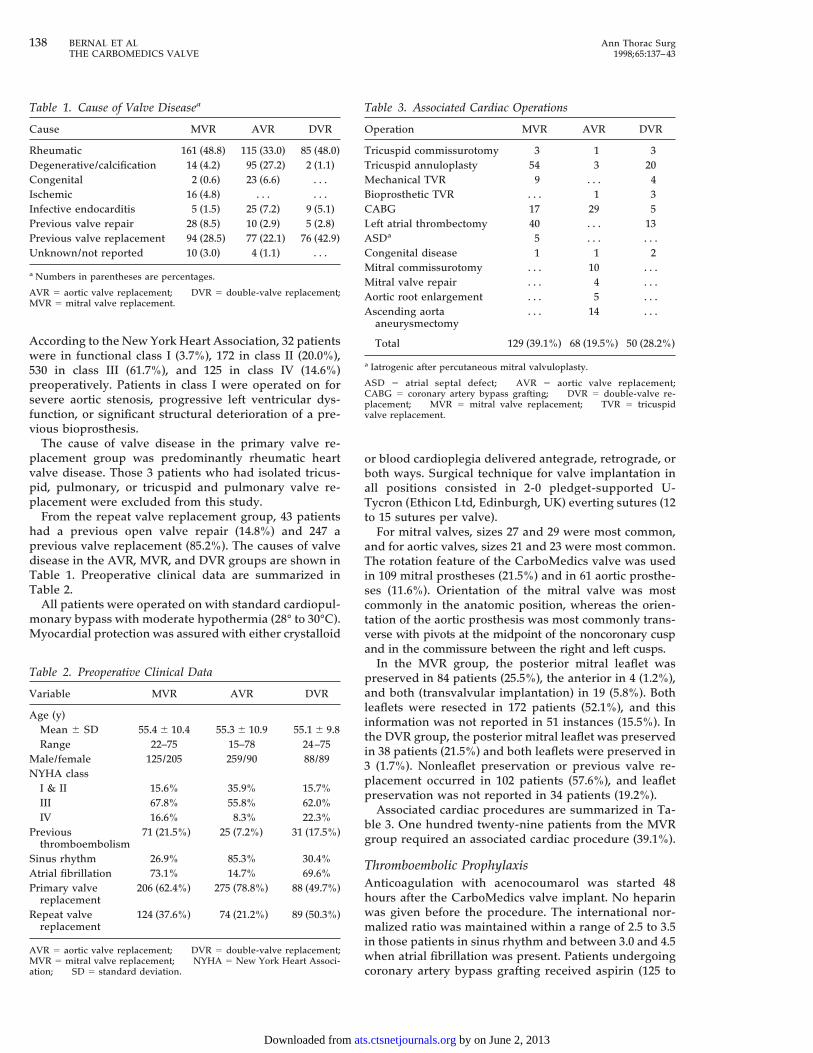
The actuarial survival curve for CarboMedics valvereplacement was 82.8% 6 1.9% at 5 years (Fig 1). Five-year survival was 77.3% 6 3.6%, 90.1% 6 2.5%, and 79.2%6 3.7% for MVR, AVR, and DVR, respectively (p 5 0.0003)(Fig 2).
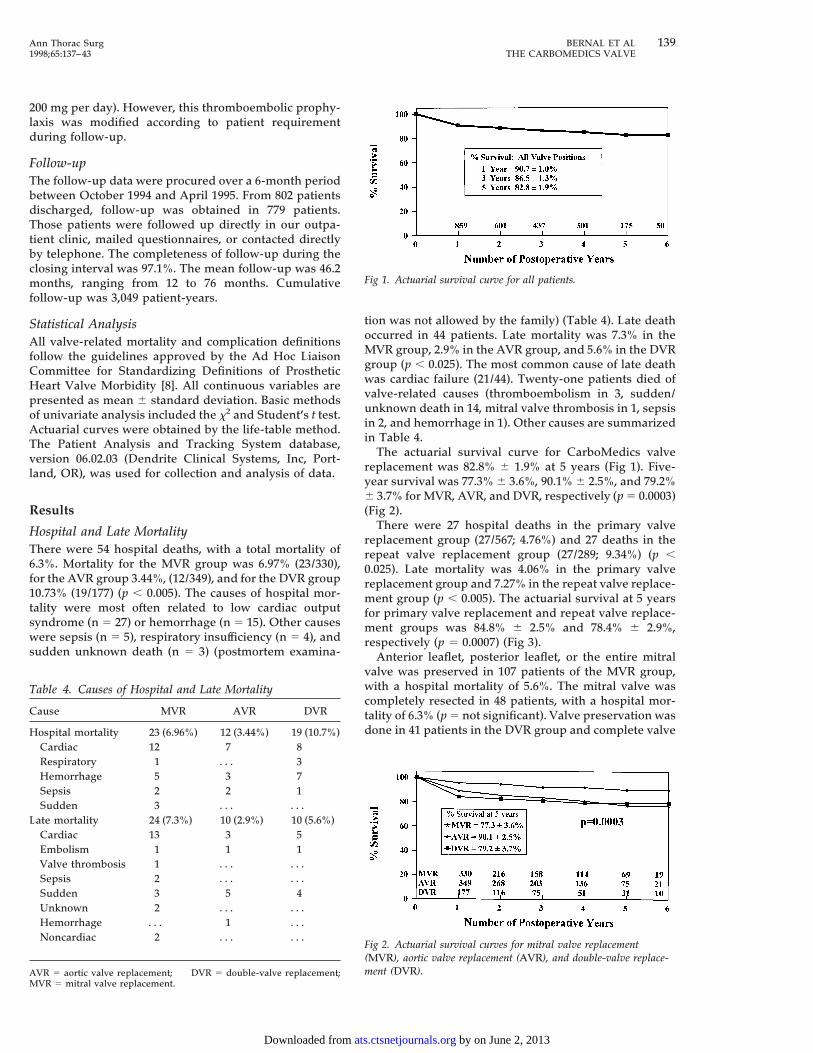
There were 27 hospital deaths in the primary valvereplacement group (27/567; 4.76%) and 27 deaths in therepeat valve replacement group (27/289; 9.34%) (p ,0.025). Late mortality was 4.06% in the primary valvereplacement group and 7.27% in the repeat valve replace-ment group (p , 0.005). The actuarial survival at 5 yearsfor primary valve replacement and repeat valve replace-ment groups was 84.8% 6 2.5% and 78.4% 6 2.9%,respectively (p 5 0.0007) (Fig 3).
Anterior leaflet, posterior leaflet, or the entire mitralvalve was preserved in 107 patients of the MVR group,with a hospital mortality of 5.6%. The mitral valve wascompletely resected in 48 patients, with a hospital mor-tality of 6.3% (p 5 not significant). Valve preservation wasdone in 41 patients in the DVR group and complete valve
Fig 1. Actuarial survival curve for all patients.
Fig 2. Actuarial survival curves for mitral valve replacement(MVR), aortic valve replacement (AVR), and double-valve replace-ment (DVR).
Table 4. Causes of Hospital and Late Mortality
Cause MVR AVR DVR
Hospital mortality 23 (6.96%) 12 (3.44%) 19 (10.7%)Cardiac 12 7 8Respiratory 1 . . . 3Hemorrhage 5 3 7Sepsis 2 2 1Sudden 3 . . . . . .
Late mortality 24 (7.3%) 10 (2.9%) 10 (5.6%)Cardiac 13 3 5Embolism 1 1 1Valve thrombosis 1 . . . . . .Sepsis 2 . . . . . .Sudden 3 5 4Unknown 2 . . . . . .Hemorrhage . . . 1 . . .Noncardiac 2 . . . . . .
AVR 5 aortic valve replacement; DVR 5 double-valve replacement;MVR 5 mitral valve replacement.
139Ann Thorac Surg BERNAL ET AL1998;65:137–43 THE CARBOMEDICS VALVE
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
resection in 13 patients, with a hospital mortality of 9.8%and 15.1%, respectively (p 5 not significant).
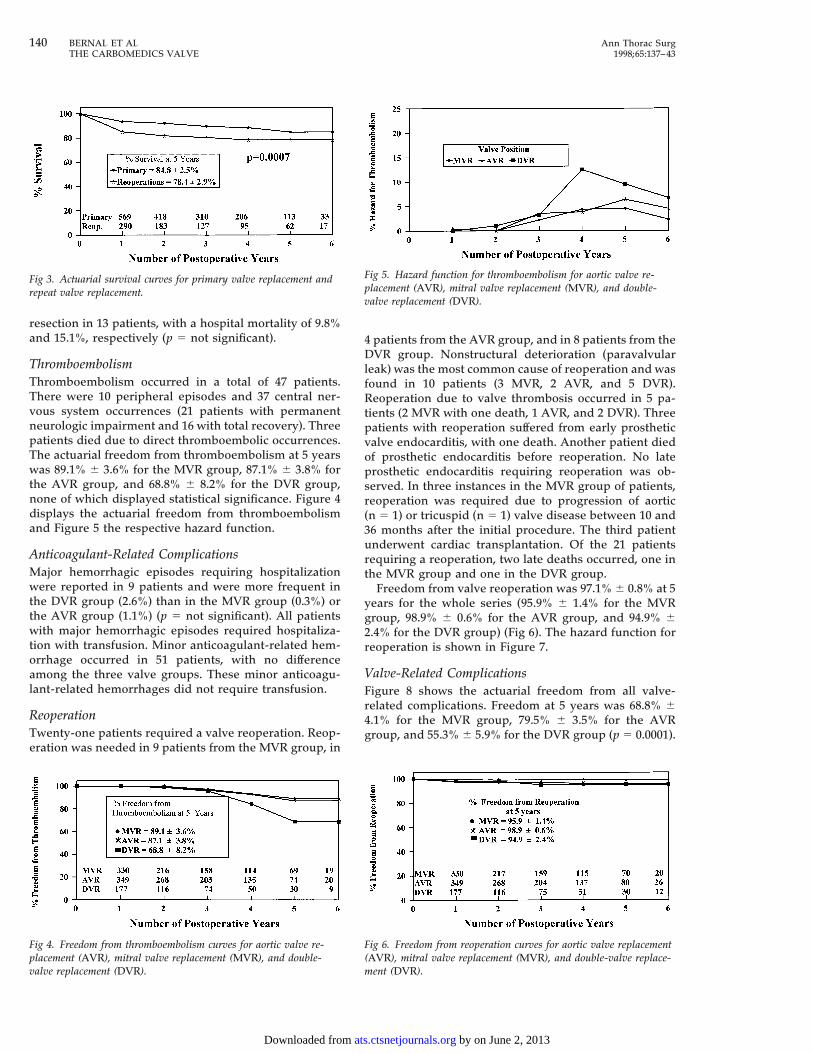
ThromboembolismThromboembolism occurred in a total of 47 patients.There were 10 peripheral episodes and 37 central ner-vous system occurrences (21 patients with permanentneurologic impairment and 16 with total recovery). Threepatients died due to direct thromboembolic occurrences.The actuarial freedom from thromboembolism at 5 yearswas 89.1% 6 3.6% for the MVR group, 87.1% 6 3.8% forthe AVR group, and 68.8% 6 8.2% for the DVR group,none of which displayed statistical significance. Figure 4displays the actuarial freedom from thromboembolismand Figure 5 the respective hazard function.
Anticoagulant-Related ComplicationsMajor hemorrhagic episodes requiring hospitalizationwere reported in 9 patients and were more frequent inthe DVR group (2.6%) than in the MVR group (0.3%) orthe AVR group (1.1%) (p 5 not significant). All patientswith major hemorrhagic episodes required hospitaliza-tion with transfusion. Minor anticoagulant-related hem-orrhage occurred in 51 patients, with no differenceamong the three valve groups. These minor anticoagu-lant-related hemorrhages did not require transfusion.
ReoperationTwenty-one patients required a valve reoperation. Reop-eration was needed in 9 patients from the MVR group, in
4 patients from the AVR group, and in 8 patients from theDVR group. Nonstructural deterioration (paravalvularleak) was the most common cause of reoperation and wasfound in 10 patients (3 MVR, 2 AVR, and 5 DVR).Reoperation due to valve thrombosis occurred in 5 pa-tients (2 MVR with one death, 1 AVR, and 2 DVR). Threepatients with reoperation suffered from early prostheticvalve endocarditis, with one death. Another patient diedof prosthetic endocarditis before reoperation. No lateprosthetic endocarditis requiring reoperation was ob-served. In three instances in the MVR group of patients,reoperation was required due to progression of aortic(n 5 1) or tricuspid (n 5 1) valve disease between 10 and36 months after the initial procedure. The third patientunderwent cardiac transplantation. Of the 21 patientsrequiring a reoperation, two late deaths occurred, one inthe MVR group and one in the DVR group.
Freedom from valve reoperation was 97.1% 6 0.8% at 5years for the whole series (95.9% 6 1.4% for the MVRgroup, 98.9% 6 0.6% for the AVR group, and 94.9% 62.4% for the DVR group) (Fig 6). The hazard function forreoperation is shown in Figure 7.
Valve-Related ComplicationsFigure 8 shows the actuarial freedom from all valve-related complications. Freedom at 5 years was 68.8% 64.1% for the MVR group, 79.5% 6 3.5% for the AVRgroup, and 55.3% 6 5.9% for the DVR group (p 5 0.0001).
Fig 3. Actuarial survival curves for primary valve replacement andrepeat valve replacement.
Fig 4. Freedom from thromboembolism curves for aortic valve re-placement (AVR), mitral valve replacement (MVR), and double-valve replacement (DVR).
Fig 5. Hazard function for thromboembolism for aortic valve re-placement (AVR), mitral valve replacement (MVR), and double-valve replacement (DVR).
Fig 6. Freedom from reoperation curves for aortic valve replacement(AVR), mitral valve replacement (MVR), and double-valve replace-ment (DVR).
140 BERNAL ET AL Ann Thorac SurgTHE CARBOMEDICS VALVE 1998;65:137–43
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
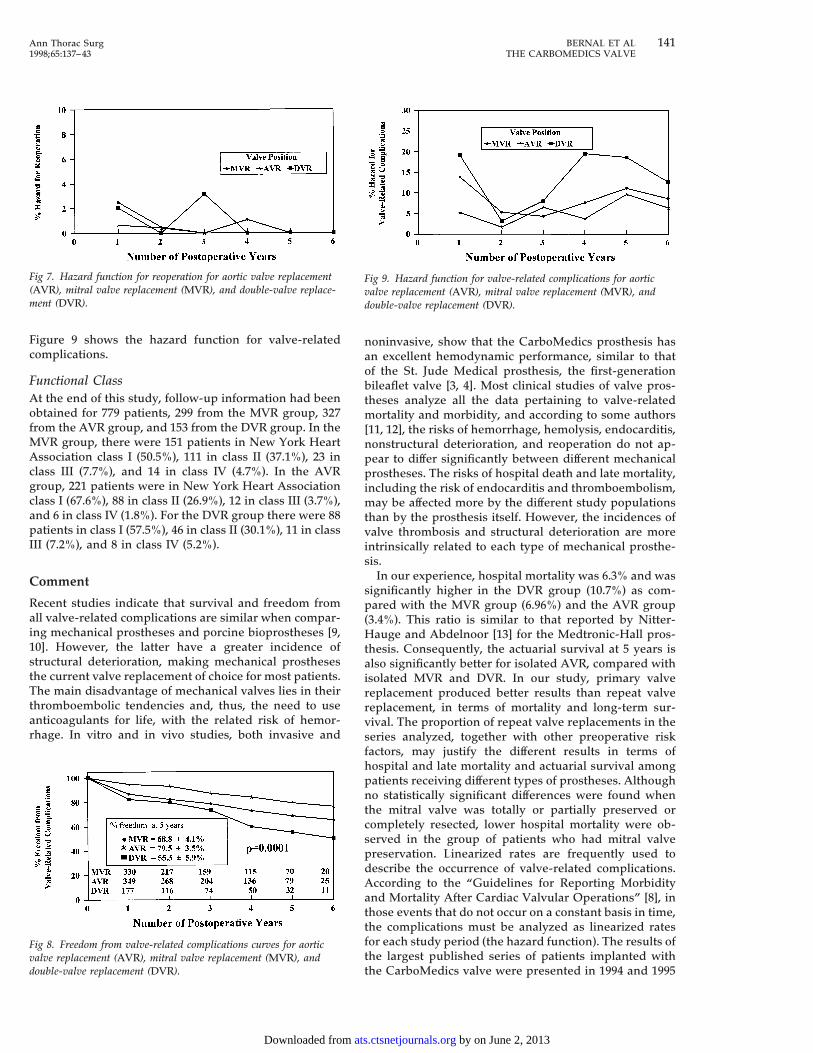
Figure 9 shows the hazard function for valve-relatedcomplications.
Functional ClassAt the end of this study, follow-up information had beenobtained for 779 patients, 299 from the MVR group, 327from the AVR group, and 153 from the DVR group. In theMVR group, there were 151 patients in New York HeartAssociation class I (50.5%), 111 in class II (37.1%), 23 inclass III (7.7%), and 14 in class IV (4.7%). In the AVRgroup, 221 patients were in New York Heart Associationclass I (67.6%), 88 in class II (26.9%), 12 in class III (3.7%),and 6 in class IV (1.8%). For the DVR group there were 88patients in class I (57.5%), 46 in class II (30.1%), 11 in classIII (7.2%), and 8 in class IV (5.2%).
Comment
Recent studies indicate that survival and freedom fromall valve-related complications are similar when compar-ing mechanical prostheses and porcine bioprostheses [9,10]. However, the latter have a greater incidence ofstructural deterioration, making mechanical prosthesesthe current valve replacement of choice for most patients.The main disadvantage of mechanical valves lies in theirthromboembolic tendencies and, thus, the need to useanticoagulants for life, with the related risk of hemor-rhage. In vitro and in vivo studies, both invasive and
noninvasive, show that the CarboMedics prosthesis hasan excellent hemodynamic performance, similar to thatof the St. Jude Medical prosthesis, the first-generationbileaflet valve [3, 4]. Most clinical studies of valve pros-theses analyze all the data pertaining to valve-relatedmortality and morbidity, and according to some authors[11, 12], the risks of hemorrhage, hemolysis, endocarditis,nonstructural deterioration, and reoperation do not ap-pear to differ significantly between different mechanicalprostheses. The risks of hospital death and late mortality,including the risk of endocarditis and thromboembolism,may be affected more by the different study populationsthan by the prosthesis itself. However, the incidences ofvalve thrombosis and structural deterioration are moreintrinsically related to each type of mechanical prosthe-sis.
In our experience, hospital mortality was 6.3% and wassignificantly higher in the DVR group (10.7%) as com-pared with the MVR group (6.96%) and the AVR group(3.4%). This ratio is similar to that reported by Nitter-Hauge and Abdelnoor [13] for the Medtronic-Hall pros-thesis. Consequently, the actuarial survival at 5 years isalso significantly better for isolated AVR, compared withisolated MVR and DVR. In our study, primary valvereplacement produced better results than repeat valvereplacement, in terms of mortality and long-term sur-vival. The proportion of repeat valve replacements in theseries analyzed, together with other preoperative riskfactors, may justify the different results in terms ofhospital and late mortality and actuarial survival amongpatients receiving different types of prostheses. Althoughno statistically significant differences were found whenthe mitral valve was totally or partially preserved orcompletely resected, lower hospital mortality were ob-served in the group of patients who had mitral valvepreservation. Linearized rates are frequently used todescribe the occurrence of valve-related complications.According to the “Guidelines for Reporting Morbidityand Mortality After Cardiac Valvular Operations” [8], inthose events that do not occur on a constant basis in time,the complications must be analyzed as linearized ratesfor each study period (the hazard function). The results ofthe largest published series of patients implanted withthe CarboMedics valve were presented in 1994 and 1995
Fig 7. Hazard function for reoperation for aortic valve replacement(AVR), mitral valve replacement (MVR), and double-valve replace-ment (DVR).
Fig 8. Freedom from valve-related complications curves for aorticvalve replacement (AVR), mitral valve replacement (MVR), anddouble-valve replacement (DVR).
Fig 9. Hazard function for valve-related complications for aorticvalve replacement (AVR), mitral valve replacement (MVR), anddouble-valve replacement (DVR).
141Ann Thorac Surg BERNAL ET AL1998;65:137–43 THE CARBOMEDICS VALVE
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from

[5, 12]. These groups differ in their mean follow-up (16.1versus 30.2 months). A significant decrease of the linear-ized rates is observable between them, even with thesmall difference in follow-up time. The incidence ofanticoagulant-related hemorrhage decreased from2.36%/patient-year in 1994 to 1.51%/patient-year in 1995,for example. The same is true for other incidence rates,that is, valve thrombosis, hemolysis, and reoperation. Inour initial experience with the CarboMedics prosthesis[14], we found that valve-related complications weremore frequent during the first years of follow-up. Fur-thermore, as observed in the different hazard functionsfor thromboembolism, reoperation, and all valve-relatedcomplications, the linearized rates for each year of fol-low-up do not remain constant.
Thromboembolism has been the most frequent valve-related complication in our series, especially in the DVRgroup. These data contrast significantly with those re-ported by Smith and associates [15] with the St. Judeprosthesis in a group of 1,184 patients averaging 59 yearsof age. This group presented actuarial freedom-from-thromboembolism curves at 10 years with values greaterthan 96% for the three patient groups. The curves re-ported by Smith and associates are probably similar tothose of the human population without prosthetic heartvalves. The results of other authors are more logical.Ibrahim and colleagues [16], in a study of 1,184 patientsimplanted with a St. Jude prosthesis, show actuarialfreedom-from-thromboembolism rates of 76% at 13 yearsfor the MVR and DVR groups. These data also corre-spond to those published by Fernandez and co-workers[17] in a study of 1,200 patients with a St. Jude prosthesis,who had an actuarial freedom-from-thromboembolismcurve of 81% at 9 years. Furthermore, the linearized rateof thromboembolism with the St. Jude prosthesis rangesfrom 0.5%/patient-year, as reported by Smith and co-workers [15], to 6.62%/patient-year, published by Horst-kotte and associates [18]. The disparity of the results forthe same prosthesis, for example, Smith and associates[15] versus Horstkotte and associates [18], indicates thatthe specific characteristics of each patient and themethod of anticoagulation may play a greater role inthromboembolism than the type of mechanical prosthe-sis. Anticoagulation-related hemorrhage is closely linkedto thromboembolism. As mentioned before [18], thosepatients maintained at a higher international normalizedratio (3.0 to 4.5) have a greater incidence of anticoagulant-related hemorrhage, whereas the thromboembolism rateis not significantly higher in groups of patients main-tained with an international normalized ratio less than3.0.
In accordance with results reported by Copeland andassociates [12], the risks of endocarditis and nonstruc-tural deterioration, such as paravalvular leak, encoun-tered in our series do not appear to be different fromthose mentioned for other types of prostheses, whethermechanical or biological. Conversely, valve thrombosisrequiring emergency reoperation or fibrinolytic treat-ment is considered to be one of the most serious compli-cations of mechanical prostheses. Although the role of
well-managed anticoagulation seems to be essential,some models of mechanical prostheses may be morethrombotic than others. The North American experiencewith the CarboMedics valve reported 10 cases of throm-bosis in 1,228 patients, with a cumulative follow-up of3,082 patient-years. In all such cases, a level of anticoag-ulation lower than that recommended was documented.In our experience, only 5 cases of thrombosis werediagnosed in 859 patients with a cumulative follow-up of3,049 patient-years, also in the presence of lowered levelsof anticoagulation. Although Smith and colleagues [15]reported just a single case of thrombosis with a St. Judeprosthesis in 3,075 patient-years, 4 cases of thrombosiswith a St. Jude prosthesis were reported by Horstkotteand associates [18] in 4,080 patient-years. Thirty events ofthrombosis are discussed in an article by Baudet andcolleagues [19] in a series of 1,112 patients. Except for themost optimistic data [15], most of the series of mechanicalbileaflet valves present similar results. The study re-ported by Baudet and colleagues [19] mentioned above isone of the largest series of patients implanted with a St.Jude bileaflet prosthetic valve. With a follow-up of 8,988patient-years, it showed actuarial curves of freedom fromeach of the valve-related complications similar to those ofour study. Based on published results of mortality, endo-carditis, thromboembolism, anticoagulant-related hem-orrhage, nonstructural deterioration, and prostheticthrombosis, we conclude that our outcomes were gener-ally comparable with those reported by other authors forthe St. Jude prosthesis.
There are two main differences between the two typesof mechanical bileaflet prosthetic valves. Although casesof structural deterioration have been described for the St.Jude prosthesis [20–23], none have been reported for theCarboMedics prosthesis. However, the worldwide expe-rience with the St. Jude Medical valve is significantlyhigher and has longer follow-up than with the Carbo-Medics valve, so a longer experience and follow-up ismandatory to find any significant differences in thebehavior of the two bileaflet prosthesis. The largestCarboMedics valve series [5, 12], plus ours, have shown atotal absence of structural deterioration. In the St. Judeprosthesis, two types of structural deterioration werereported. Leaflet fracture was reported by Orsinelli andcolleagues [20], and leaflet dislocation causing leafletembolization was described on several occasions [21–23],both for aortic and mitral prostheses. In contrast to the St.Jude prosthesis, the use of a titanium stiffening ring inthe valve housing minimizes the chance for orifice dis-tortion and likely explains the absence of structuraldeterioration in the CarboMedics prosthesis. Anotherremarkable difference is valve rotatability, which is ab-sent in the St. Jude prosthesis. In our experiment, therotatability feature of the CarboMedics valve was used inat least 21.5% of the mitral prostheses and in 11.6% of theaortic prostheses. These data correspond to those re-ported in the CarboMedics North American experience[12]. The rotation was used in many cases out of the needto improve leaflet mobility or to properly orient them,which was particularly useful when the subvalvular ap-
142 BERNAL ET AL Ann Thorac SurgTHE CARBOMEDICS VALVE 1998;65:137–43
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from

paratus was totally or partially preserved. This alsoapplied to situations where the valve was used in patientswith prior valve replacements. Not everyone agrees onthe need for mechanical prostheses to have the rotationfeature, but the recent introduction for clinical use of anew prosthesis marketed by St. Jude Medical, Inc (St.Paul, MN), which has a rotation feature, appears to givesignificant importance to this feature.
The midterm results with the CarboMedics mechanicalvalve prostheses are similar to those reported by mostauthors for other bileaflet prostheses, in terms of hospitaland late mortality and other valve-related complications,which are frequently due more to the patient than theprosthesis itself. The rate of valve thrombosis is low andalways related to inadequate anticoagulation. The greatadvantages of this second-generation, bileaflet, mechan-ical valve over its predecessor are the total absence ofstructural deterioration and, in our opinion, the rotationfeature, which is very useful when a decision is made topreserve the mitral leaflets or when a previous prosthesisis explanted.
References
1. Chambers J, Cross J, Deverall P, Sowton E. Echocardio-graphic description of the CarboMedics bileaflet prostheticheart valve. J Am Coll Cardiol 1993;21:398–405.
2. Ihlen H, Molstad P, Simonsen S, et al. Hemodynamic eval-uation of the CarboMedics prosthetic heart valve in theaortic position: comparison of noninvasive and invasivetechniques. Am Heart J 1992;123:151–9.
3. Nygaard H, Paulsen PK, Hasenkarn JM, Pedersen EM,Rovsing PE. Turbulent stress downstream of three mechan-ical aortic valve prostheses in human beings. J ThoracCardiovasc Surg 1994;107:438–46.
4. Butterfield M, Fisher J, Davies GA, Spyt TJ. Comparativestudy of the hydrodynamic function of the CarboMedicsvalve. Ann Thorac Surg 1991;52:815–20.
5. Copeland JG. An international experience with the Carbo-Medics prosthetic heart valve. J Heart Valve Dis 1995;4:56–62.
6. Bernal JM, Rabasa JM, Vilchez FG, Cagigas JC, Revuelta JM.Mitral valve repair for rheumatic disease: the flexible solu-tion. Circulation 1993;88:1746–53.
7. Bernal JM, Rabasa JM, Cagigas JC, Echevarria JR, CarrionMF, Revuelta JM. Valve-related complications with the Han-cock I porcine bioprosthesis: a twelve- to fourteen-yearfollow-up study. J Thorac Cardiovasc Surg 1991;101:871–80.
8. Edmunds LH Jr, Clark RE, Cohn LH, Grunkemeier GL,
Miller DC, Weisel RD. Guidelines for reporting morbidityand mortality after cardiac valvular operations. Ann ThoracSurg 1996;62:932–5.
9. Bloomfield P, Wheatley DJ, Prescott RJ, Miller HC. Twelve-year comparison of a Bjork-Shiley mechanical heart valvewith porcine bioprostheses. N Engl J Med 1991;324:573–9.
10. Hammermeister KE, Sethi GK, Henderson WG, Oprian C,Kim T, Rahimtoola S. A comparison of outcomes in men 11years after heart-valve replacement with a mechanical valveor bioprosthesis. N Engl J Med 1993;328:1289–96.
11. Blackstone EH, Kirklin JW. Death and other time-relatedevents after valve replacement. Circulation 1985;72:753–67.
12. Copeland JG, Sethi GK, North American team of clinicalinvestigators for the CarboMedics prosthetic heart valve.Four-year experience with the CarboMedics valve: the NorthAmerican experience. Ann Thorac Surg 1994;58:630–8.
13. Nitter-Hauge S, Abdelnoor M. Ten-year experience with theMedtronic Hall valvular prosthesis. A study of 1,104 patients.Circulation 1989;80(Suppl 1):43–8.
14. Nistal JF, Hurle A, Revuelta JM, Gandarillas M. Clinicalexperience with the CarboMedics valve: early results with anew bileaflet mechanical prosthesis. J Thorac CardiovascSurg 1996;112:59–68.
15. Smith JA, Westlake GW, Mullerworth MH, Skillington PD,Tatoulis J. Excellent long-term results of cardiac valve re-placement with the St. Jude Medical valve prosthesis. Cir-culation 1993;88(Suppl 2):49–54.
16. Ibrahim M, O’Kane H, Cleland I, Gladstone D, Sarsam M,Patterson C. The St. Jude Medical prosthesis. A thirteen-yearexperience. J Thorac Cardiovasc Surg 1994;108:221–30.
17. Fernandez J, Laub GW, Adkins MS, et al. Early and late-phase events after valve replacement with the St. JudeMedical prosthesis in 1200 patients. J Thorac CardiovascSurg 1994;107:394–407.
18. Horstkotte D, Schulte H, Bircks W, Strauer B. Unexpectedfindings concerning thromboembotic complications and an-ticoagulation after complete 10 year follow up of patientswith St. Jude Medical prosthesis. J Heart Valve Dis 1993;2:291–301.
19. Baudet EM, Puel V, McBride JT, et al. Long-term results ofvalve replacement with the St. Jude Medical prosthesis.J Thorac Cardiovasc Surg 1995;109:858–70.
20. Orsinelli DA, Becker RC, Cuenoud HF, Moran JM. Mechan-ical failure of a St. Jude Medical prosthesis. Am J Cardiol1991;67:906–8.
21. Antunes MJ. Mechanical failure of a St. Jude Medical pros-thesis. Am J Cardiol 1991;68:841–2.
22. Odell JA, Durandt J, Shama DM, Vythilingum S. Spontane-ous embolization of a St. Jude prosthetic mitral leaflet. AnnThorac Surg 1985;39:569–72.
23. Burckhardt D, Striebel D, Vogt S, et al. Heart valve replace-ment with the St. Jude medical valve prosthesis: long-termexperience in 743 patients in Switzerland. Circulation 1988;78(Suppl 1):18–24.
143Ann Thorac Surg BERNAL ET AL1998;65:137–43 THE CARBOMEDICS VALVE
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from

1998;65:137-143 Ann Thorac SurgNistal and José M. Revuelta
José M. Bernal, José M. Rabasa, Francisco Gutierrez-Garcia, Carlos Morales, J. Francisco The CarboMedics Valve: Experience With 1,049 Implants
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/65/1/137including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/65/1/137#BIBL
This article cites 23 articles, 13 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/65/1/137#otherarticles
This article has been cited by 24 HighWire-hosted articles:
Permissions & Licensing
[email protected] or email: http://www.us.elsevierhealth.com/Licensing/permissions.jsp
entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or in its
Reprints [email protected]
For information about ordering reprints, please email:
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
Related Documents











