Nonpharmacologic Interventions for the Management of AD 4 by Anne Lennox, RN, MPH Diagnosing and Treating Alzheimer’s Disease: CT scans and donepezil 8 by Peter N. McCracken, MD, FRCPC The Occupational Therapist and Home Assessment 10 by Françoise McDonald and Andrée Tremblay Caregiver Stress: Looking After Yourself As Well 14 by the Alzheimer Society of Canada Pharmacological Treatments for Alzheimer’s disease 16 by Serge Gauthier, MD, FRCPC The Canadian Alzheimer Disease Review Volume 3, Number 1 April 1999 Memory by Jennifer Hiscox

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Nonpharmacologic Interventions for the Management of AD 4by Anne Lennox, RN, MPH
Diagnosing and Treating Alzheimer’s Disease: CT scans and donepezil 8by Peter N. McCracken, MD, FRCPC
The Occupational Therapist and Home Assessment 10by Françoise McDonald and Andrée Tremblay
Caregiver Stress: Looking After Yourself As Well 14by the Alzheimer Society of Canada
Pharmacological Treatments for Alzheimer’s disease 16by Serge Gauthier, MD, FRCPC
The Canadian
AlzheimerDisease ReviewVolume 3, Number 1 April 1999
Mem
ory
by Je
nnife
r H
iscox
CHAIRMANPeter N. McCracken, MD, FRCPC
Geriatric Medicine StaffGlenrose Rehabilitation Hospital
Past Director, Geriatric Medicine and Professor of MedicineUniversity of AlbertaEdmonton, Alberta
Paul J. Coolican, MD, CCFPFamily Physician, St. Lawrence Medical Clinic
Morrisburg, Ontario Active Staff,Winchester District Memorial Hospital
Winchester, Ontario
Shannon Daly, RN, BScNCommunity Nurse
Northern Alberta Regional Geriatric ProgramEdmonton, Alberta
Howard Feldman, MD, FRCPCClinical Associate Professor of Medicine
University of British ColumbiaDivision of Neurology UBC
Director, UBC Alzheimer Clinical Trials UnitVancouver, British Columbia
Serge Gauthier, MD, FRCPCProfessor of Neurology and Neurosurgery,Psychiatry and Medicine, McGill University
McGill Centre for Studies in AgingMontreal, Quebec
Bernard Groulx, MD, CM, FRCPCAssociate Professor, McGill UniversityChief Psychiatrist, Hôpital Ste-AnneMcGill Centre for Studies in Aging
Montreal, Quebec
Nathan Herrmann, MD, FRCPCAssistant Professor, University of Toronto
Head of the Division of Geriatric PsychiatrySunnybrook Health Science Centre
Toronto, Ontario
Kenneth J. Rockwood, MD, FRCPCProfessor, Dalhousie University
GeriatricianQueen Elizabeth II Health Sciences Centre
Halifax, Nova Scotia
The Canadian Alzheimer Disease Review is published by STA Communications Inc., through an educational grant provided by Pfizer Canada.The opinions expressedherein are those of the authors and do not necessarily reflect the views of the publisher or the sponsor. Physicians should take into account the patient’sindividual condition and consult officially approved product monographs before making any diagnosis or treatment, or following any procedure based onsuggestions made in this document.. Publications Agreement Number 1445057. Copyright 1999.All rights reserved.
Publishing StaffEditorial Board
2 • The Canadian Alzheimer Disease Review • April 1999
The editorial board has complete independence in reviewing the articles appearing in this publication and is responsible for their accuracy. Pfizer Canada exerts no influence on the selection or the content of material published.
We’d Like to Hear From You!The Canadian Alzheimer Disease Review welcomes letters from its readers. Address all correspondences to Letters, The Canadian Alzheimer Disease Review, 955 Boul. St. Jean,Suite 306, Pointe Claire, Quebec, H9R 5K3. The Review also accepts letters by fax or Internet.Letters can be faxed to 514-695-8554 and address electronic mail to [email protected]. Please includea daytime telephone number. Letters may be edited for length or clarity.
On the CoverMemory by Jennifer Hiscox
Paul F. BrandExecutive EditorAllison GandeyManaging Editor(514) 695-7623
Scott MoffattEditorial Coordinator,
Custom CommunicationsMaria Bishop
Editorial Coordinator,Journal DivisionJeff Alexander
Senior Production EditorSylvie Lahaie
Principal Editor—FrenchMaryse Annik Lamoureux
Marsha MooreAssociate EditorsIsabelle GaudreauEditor-proofreader,
Custom FrenchSherene Chen See
Trent EdwardsTherese Ho
David HodgesDebbie Ng
Brian SalisburyJunior Editors
Donna GrahamProduction Manager
Dan OldfieldDesign DirectorMark Kislingbury
Production AssistantPeggy Kallianis
Graphic DesignerJennifer Brennan
Financial ServicesKelly QuinnJamie Tolis
Accounting AssistantsBarbara Roy
Administrative AssistantIan W.D. Henderson, MD
Medical ConsultantJohn L. Liberman, QCForensic Consultant
Deborah LaBelleProject Director
Claudette CollymoreSarah Scheigetz
Anne Marie SklarProject Coordinators
Sherrie ClaridgeSales CoordinatorRachel McCreadyAccount Manager,
Custom CommunicationsGreg Passaretti
Manager, Business DevelopmentDan Léger
Kimberley PlattDirectors, CustomCommunicationsCarlo M. Viola (905) 564-7700John D. Donnet (514) 695-7623
Account ManagersRobert E. Passaretti
Publisher

The Canadian Alzheimer Disease Review • April 1999 • 3
Callout callout callout
This month’s cover art, Memory, is thesecond piece by Jennifer Hiscox to
appear in this journal; her painting Ghostgraced the cover of volume 1, number 1.Ghost so moved my colleagues and I thatwe invited Jennifer to be artist-in-residence at our clinic.
Memory is the first piece from thatcollection. It describes an encounter withan elderly woman with a memory prob-lem who was accompanied to my clinicby her son.
Like many physicians, I test long-termmemory by having patients recount past elements of theirlives: when and where they were born, where they went toschool, the birth order of their children, the names of chil-dren’s spouses, and the names of grandchildren. To useinformation in diagnosis requires the presence of a knowl-edgeable informant with whom the details can be verified.
My patient arrived with her son who, while aware thathis mother was declining, was unprepared for what hap-pened. Even though his mother could recall her weddingday, remember her childrens’ names and provide a vagueoutline of her life, in the stress of the moment, she sud-denly did not recognize her son.
I remember caring for the wife of a distinguished warveteran. I saw him on Remembrance Day, some monthsafter she had died, and I commented on his row ofmedals. “They’re something,” he acknowledged, “butwhat they really should give out medals for is when yourwife doesn’t know you anymore after forty years.”
I told this to my patient’s son now trying to patch awound I had opened.
Jennifer was with me that day and from that experienceand others, she created “Memory”. The left-hand side ofthe painting is a swirl of color. There is a circle in theupper-left-hand corner. As through a window, it frames astructure which I take to be a church, the slats of the belltower just visible. In front, still in the frame, two blurredfigures can be seen. They seem to be holding hands.
On the right hand side, there is text.Individual letters are at once obscured, butclearly visible: they are infused withmeaning even though, overall, the text isout of sequence.
“This is the night-time street. The dark-ness and confusion like the vagueness in mymind. Once I had a newborn baby. I put himto my breast, and he knew that he belonged.This man says he is that baby. Why does helook at me so sadly?”
Jennifer said, “This is what you people dofor patients with dementia. They come with a
swirl of disorganized information, and thoughts out of con-text. You find the meaning in that, even though it can meansomething terrible.”
My colleagues and I find these paintings of value inmany respects. They provide us with a perspectivewhich, while sympathetic to what we are doing, is out-side of us—another point of view. It informs our practicein a way which a hundred Quality Assurance question-naires never could.
The paintings are poignant and immediate; they arethus a useful adjunct to small group teaching. We havelong argued that Alzheimer’s disease and its impact onfamilies demands the respect of physicians. It is onething to say this is moving, it is something else to movesomeone. “Memory” does that.
And finally, though we often preach “care for thecaregiver”, it is easy for physicians and other health-careprofessionals to forget that we are caregivers too. Even inthis era of treatment, we need moments to acknowledgethe stress, grief and bewilderment that we ourselvesoccasionally feel.
As with our patients, “Memory” has many meanings.
Kenneth Rockwood
Finding Meaning in Alzheimer’s Disease
by Kenneth Rockwood, MD, FRCPC
E D I T O R I A L

4 • The Canadian Alzheimer Disease Review • April 1999
Psychiatric and behavioral problemsare present in many patients suffer-
ing from a dementia syndrome. Theseproblems can be a major factor in care-giver stress, burnout, and the decision toplace an individual in a nursing home.The level of distress for the individualmay be difficult to measure, but it isoften substantial.
Strategies for managing the behav-ioral symptoms of dementia are amajor focus of nursing activities inlong-term care. Pharmacotherapy isfrequently the first intervention soughtby nurses from the attending physician,who may see the patient infrequentlyand feel compelled to respond torequests for medication.
Psychiatric illnesses (and relatedbehavioral problems) such as depres-sion, hallucinations and delusions oftenrespond well to pharmacotherapy.However, many other behaviors com-mon in dementia such as wandering,agitation, repetitiveness, disruptiveness,hoarding and aggression, are notamenable to treatment with medica-tions. Pharmacotherapy may, in fact,worsen these behaviors and, ultimately,the quality of life for the individual,nursing staff and other residents.
The pharmacotherapy of behavioraldisturbances in dementia has alreadybeen well described by Dr. NathanHerrmann in a previous issue of TheCanadian Alzheimer Disease Review(Vol. 2, No. 2, July 1998). The purposeof this article is to present the results ofa literature review of nonpharmacologicinterventions used to manage the behav-ioral symptomatology associated withAlzheimer’s disease (AD), followed bysome practical suggestions that haveemerged from clinical experience. It isassumed that an assessment of thebehavior has occured at least to theextent that underlying medical condi-tions such as possible delirium and psy-chiatric illness have been ruled out.
The question addressed by thisresearch overview was: “what strategieswithin the scope of nursing are effectivein managing the behavioral symptoma-tology associated with Alzheimer’s dis-ease in elderly individuals?”
Forbes’ work identified a total of265 articles on the subject, with only45 meeting the following relevancecriteria:1. The article was published after 1985
and evaluated a nonpharmacologicintervention directed at individu-
NonpharmacologicInterventions for theManagement of ADThe research supporting nonpharmacologic interventions forthe treatment of behavioral symptoms of Alzheimer’sdisease (AD) is still in its very early stages of development.To reduce reliance on pharmacologic treatments, strategiescan be used in a nursing home setting to treat behavioralsymptoms associated with dementias.
by Anne Lennox RN, MPH
Anne Lennox is a clinicalspecialist in mental health andpsychogeriatrics for CommunityCare Services, Calgary, Alberta.
The Canadian Alzheimer Disease Review • April 1999 • 5
als with AD who were 65 yearsor older;
2. The intervention falls within thescope of nursing practice;
3. The article measured the effects onone of the following behaviors:• aggressive, agitated and
disruptive behaviors • social interaction • self-care abilities • day/night disturbances• wandering; and
4. The article used a control groupwith a sample size greater than one.
Aggressive, Agitated and Disruptive BehaviorFor management of aggressive, agitatedand/or disruptive behavior, severalstrategies from research articles (ratedfrom moderate to weak) showedpromise. A planned walking program,for example, was effective in reducingthe number of aggressive events by 30%on a dementia special care unit.
Simulated presence therapy, whichuses audiotapes from family members,significantly improved problem behav-iors of residents with AD. Bright-lighttreatment significantly reduced agita-tion on treatment days; calming musicsignificantly decreased agitated behav-ior during and after the music interven-tion, while classical and favorite musicdecreased the number of repetitive dis-ruptive vocalizations. The methodolo-gies for these studies was, however,rated as weak.
Many of the interventions describedin the published literature require a 1:1resident : staff ratio, which is difficult toachieve in a nursing home setting. Othersuggestions for nursing interventionsinclude:• Assess for precipitants, time of day,
and consequences of the behavior todetermine if there is a pattern.
• Adopt a structured assessment scalethat can alter the number of aggres-sive incidents independent of otherinterventions.
• Systematically document the on-going assessment of the behavior.
• Define the behavior accurately.For example, agitation can rangefrom restlessness to akithesia,depending on the observer.
• Decide for whom the behavior is aproblem and why.
• Experiment with altering the levelof stimulation for the individual.
• When possible, provide for 1:1attention by asking family to bethere or, if possible, hire a com-panion sitter to assess whether thatwhich is labeled disruptive isharmless, (i.e., unmaking/remak-ing the bed repetitively).
• Try and find activities that thepatient will associate with previoushobbies, interests, or occupations.
• Increase physical activity througha structured walking programaround a school track, in a gym orin a mall during the winter.Provide meaningful tasks that fitwith the person’s abilities.
• Limit stimulation for individualswith a history of aggression;ensuring the safety of other resi-dents is a priority. Help caregiversunderstand the behavior is illness-related. Provide respite to staffwhenever possible.
• Provide as much structure to theday as possible. To control exter-nal noise, use a walkman withfavorite music or familiar radiobroadcasts and turn off the TVunless a scheduled program is
being watched.
Social InteractionForbes reviewed studies that examinedsocial interaction enhanced by a varietyof interventions. The only strong studyin the overview demonstrated that aplanned walking program while engag-ing in conversation enhanced the func-tion of communication.
The two studies rated as moderatesuggested that an attention-focusingprogram improved participation ingroup activities and weekly visits of adog on a special care Alzheimer unitsignificantly improved social behaviors.Although methodologically weak, twostudies found that a life-review programappeared to increase social interactionand orientation.1
Other studies rated as weak demon-strated a trend towards improving socia-bility with participatory music. Smallgroup activity appeared to result inincreased walking with others, andincreased spontaneous singing.2 It isimportant to ask for who the lack ofsocial interaction is a problem. Theneed for social interaction for individu-als with AD is difficult to define andmay be imposed by observations aboutpast experience or the projections ofcaregivers. Group situations that arereliant on language skills may createanxiety rather than improve an individ-ual’s social interaction. Anecdotally, theuse of a karaoke machine on a dementiaunit has proven to be successful.
The experience of being a partici-
Table 1
Five Behaviors Associated with Alzheimer’s Disease• Aggressive, agitated and disruptive behaviors • Social interaction • Self-care abilities • Day/night disturbances• Wandering
Adapted from: Forbes’ Strategies for management of behavioral symptomatology associated with Senile Dementia Alzheimer’s Type—a systematic overview. The Canadian Journal of Nursing Research, 1998.

6 • The Canadian Alzheimer Disease Review • April 1999
pant observer of the activities on a unitcan provide for social needs, in theabsence of interpersonal interactions.Many of today’s elderly did not partici-pate in group activities; this may not bea familiar format for achieving socialinteraction. On the other hand, previousinterests, activities, and hobbies do notnecessarily predict what will interestthe individual with dementia in a nurs-ing home setting. Individuals who donot respond to interactions with otherpeople may demonstrate an affinity forpets or children where the demand forlanguage and social skills is greatlyreduced. Anecdotally, videos aboutdogs and children were observed to bevery popular on a dementia unit, unlikeolder movies, which were expected tobe entertaining, but proved to be too complex.
Self-Care AbilityForbes found four studies that examinedinterventions directed at enhancing theself-care ability of individuals with AD.Two were rated as moderate and theother two were rated as weak. Self-careability appeared to be improved by askill training program.3 Soothing musichad a statistically significant effect bothon increasing the amount of food intakeand on increasing mealtime by 22%.Additionally, the patients ate by them-selves more often and were fed signifi-cantly more often when soothing musicwas played. 4
The prompting required to improveself-care ability is generally difficult toachieve in nursing-homes because itcosts more in terms of staff time. Thefunding mechanisms for facilities andnursing workload measurements do notpromote maintenance of self-care abili-ties. The nursing-home environmentwith communal eating is not a familiarpast experience for many residents. Thenoise level, distractions, and format canresult in poor nutrition and increasedagitation. The exigencies of running afacility sometimes take precedence over
the individual’s need for more time toeat, the timing of when the meal isserved and the diet itself. Six smallmeals a day would be more in keepingwith the needs of this group. If someoneis disruptive in the dining room, eatingalone or in smaller groups should beencouraged. The individual who wishesto eat alone should be allowed to do so.
Request that family members visitduring meal times to assist with openingcontainers and making it more social forthe resident. Families often look for aconstructive activity as opposed to pas-sively sitting with a family member.
Day/Night DisturbancesThree studies examined the effect ofbright light and music on day and nightdisturbances. Two studies reported thatbright light treatment appears to normal-ize disturbed sleep during the treatmentperiod, with more severe behavioral dis-orders at baseline predicting greaterclinical improvement.5 The third studydemonstrated that music appears to
increase the number of hours of produc-tive sleep in patients with AD.6
Bright lights are costly to purchase(ranging from $300-$1,000) and areawkward to administer to an individualwith AD, who may not comprehend theneed to sit for the exposure. A familymember would have to be enlisted toarrange the treatment and to sit with theindividual, which makes this form oftreatment impractical.
Sleep architecture changes with
aging; these changes are exaggerated forindividuals with dementia. A greater tol-erance for night time wakefulnessshould, therefore, be promoted amongnursing staff. In addition to the deterio-ration in circadian rhythm of sleep-ing/waking with dementia, a number ofother factors may be involved in sleepdisturbances, such as sensory depriva-tion, pain, the effects of medications,environmental disturbances or the needto urinate. Other suggestions include:• Strengthening activity/rest cycle by
minimizing daytime napping, maxi-mizing exposure to outdoor lightand increasing daytime physicalactivity.
• Avoid use of night time sedationand diuretics. Structured bedtimeroutine is recommended and givewarm milk and cookies when theperson wakes up.
• Restrict caffeine intake, keep theindividual dressed during daytimehours and provide adequate paincontrol. A recent study compared the experi-
ence of pain and the treatment of pain ina group of cognitively impaired individ-uals with a cognitively intact group.7
Those with dementia received half thepain medication as compared to theintact control group and on objectivemeasures, experienced more severe pain.Provision of patient comfort is a basicneed and a professional obligation.
WanderingSeveral studies built on the work ofHussian and Brown (1987) examinedthe effectiveness of using visual barriersto limit hazardous exiting from a facili-ty. One study examined the use of long-term memory cueing to reduce disorien-tation in individuals with AD. Hussianand Brown’s study concluded that afloor grid pattern in front of a door lim-ited wandering. Hewawasam’s (1996)research, the only study rated as moder-ate, supported these findings for partici-pants who were diagnosed with AD and
The nursing-home envi-ronment with communaleating is not a familiarpast experience for manyresidents. The noise level,distractions, and formatcan result in poor nutritionand increased agitation.

The Canadian Alzheimer Disease Review • April 1999 • 7
Parkinson’s Disease. This strategywas not, however, found to be effec-tive with subjects diagnosed withother forms of dementia.
Namazi, Rosner, and Calkings(1989) demonstrated that a cloth panelthat concealed the doorknob was moreeffective than the tape grid pattern indecreasing exiting by AD patients withsymptoms of visual agnosia. Dickinson,McLain-Kark, and Marshall-Baker(1995) supported these results by con-cluding that visual barriers serving tocamouflage the panic bar or door knobare effective controls for reducing haz-ardous exiting in patients with demen-tia. Personal memorabilia displayedoutside of patients’ bedrooms wasshown to be helpful in assisting someresidents with mild to moderate levelsof dementia to find their bedrooms.8
Concerns about wandering from afacility may result in nursing staff seek-ing medication to sedate the individual.
This is almost always counter-therapeutic, and can increase risk bycausing falls and actually increasingwandering behavior. Sometimes wan-dering can be caused by a neurolepticmedication. It is important to define thebehavior; is it goal directed (i.e., ‘I haveto go home’) or non-goal directed,(i.e., aimless wandering in search ofsomething the individual cannot identi-fy). Assess the safety risk for the resi-dent; small town versus large city, win-ter versus summer.
Other suggestions include: establisha structured walking program; encour-age family members to bring their petsto the facility for walks, if consistentwith past experience. Avoid use ofrestraints or methods that thwart wan-dering. This will increase frustrationand may provoke aggression. Installlocks that require remembering a com-bination. Mirrors on exit doors haveshown some success, as they can be dis-
tracting for the individual attempting toexit. Ensure the person is on theNational Wandering Registry and has anidentification bracelet. Platform rockers(which cannot tip backwards) or stan-dard rockers have been used effectivelyto modify wandering.
The research supporting nonphar-macologic interventions for the treat-ment of the behavioral symptoms of ADis still in its early stages. To promote lessreliance on pharmacologic treatments,strategies that can realistically be imple-mented in a nursing home setting totreat behavioral symptoms associatedwith dementias are urgently required.
Forbes’ overview of the publishedliterature on nursing interventions hasprovided us with the best availableresearch for managing the behavioralsymptoms of individuals with AD.Further substantial research is, howev-er, still required to improve both thenursing care given to individuals with
References:1. Tabourne CE: The effects of a life review
program on disorientation, social inter-action and self-esteem of nursing homeresidents. Int J of Aging and Hum Dev1995; 41(3):251-66.
2. Martichuski DK, Bell PA, Bradshaw B:Including small group activities in largespecial care units. The Journal of AppliedGerontology 1996; 15(2):224-37.
3. Tappen RM: The effect of skill trainingon functional abilities of nursing homeresidents with dementia. Res in NursHealth 1994; 17(3):159-65.
4. Ragneskog H, Brane G, Karlsson I et al:Influence of dinner music on food intakeand symptoms common in dementia.Scand J Caring Sci 1996; 10:11-7.
5. Mishima K, Okawa M, Hishikawa Y, et al:Morning bright light therapy for sleep andbehavior disorders in elderly patients withdementia. Acta Psychiatrica Scand 1994;89(1):1-7.
6. Lindenmuth CF, Patel M, Chang PK:Effects of music on sleep in healthy elder-ly and subjects with senile dementia ofthe Alzheimer type. The American Journalof Alzheimer’s Care and RelatedDisorders & Research 1992;13-20.
7. Feldt DS, Ryden MB, Miles S: Treatmentof pain in cognitively impaired comparedwith cognitively intact older patients withhip-fracture. J Am Geriatr Soc 1998;46(9):1079-85.
8. Namazi KH, Rosner TT, Rechlin L: Long-term memory cueing to reduce visuo-spatial disorientation in Alzheimer’s dis-ease patients in a special care unit. TheAmerican Journal of Alzheimer’s Careand Related Disorders & Research1991;10-15.
Suggested Readings:• Casby LA, Holm MB: The effects of
music on repetitive disruptive vocaliza-tions of persons with dementia.American Journal of OccupationalTherapy 1994; 48(10):883-89.
• Dickinson JI, Mclain-Kark J, Marshall-Baker, A: The effects of visual barriers onexiting behaviour in a dementia care unit.Gerontologist 1995; 35(1):127-30.
• Forbes DA: Strategies for management ofbehavioural symptomatology associatedwith dementia of the alzheimer type-a sys-tematic overview. The Can J Nurs Res1998; 30(2):67-86.
• Friedman R, Tappen RM: The effect ofplanned walking on communication inAlzheimer’s Disease. J Am Geriatr Soc1991; 39(7):650-4.
• Hewawasam L: Floor patterns limit wan-dering of people with Alzheimer’s. NursTimes 1996; 92(22):41-4.
• Holmberg SK: Evaluation of a clinical inter-vention for wanderers on a geriatric nurs-ing unit. Arch of Psychiatr Nurs 1997;11(1):21-8.
• Hussian RA, Brown DC: Use of two-dimensional grid patterns to limit hazardousambulation in demented patients. J Gerontol1987; 42(5):558-60.
• Kongable LG, Buckwalter KC, Stolley JM:The effects of pet therapy on the socialbehavior of institutionalized Alzheimer’sclients. Arch Psychiatr Nurs 1989;3(4):191-8.
• Lovell BB, Ancoli-Israel S, Gervitz R:Effect of bright light treatment on agi-tated behaviour in institutionalizedelderly subjects. Psychiatry Res 1995;57(1):7-12.
• Namzai KH, Rosner TT, Calkins MP: Visual
barriers to prevent ambulatory Alzheimer’spatients from exiting through an emergencydoor. Gerontologist 1989; 29(5):699-702.
• Palmistierna T, Wistedt B: Staff observationaggression scale, SOAS: presentation andevaluation. Acta Psychiatr Scand 1987;76(6):657-3.
• Ragneskog H, Kihlgren M, Karlsson I, et al:Dinner music for demented patients:analysis of video-recorded observations.Clin Nurs Res 1996; 5(3):262-77.
• Rosswurm MA: Attention-focusing pro-gram for persons with dementia. ClinicalGerontologist 1991;10(2):3-16.
• Satlin A, Volicer L, Ross V et al: Bright lighttreatment of behavioural and sleep distur-bances in patients with Alzheimer’sDisease. Am J Psychiatry 1992;149(8):1028-32.
• Smith-Marchese K: The effects of participa-tory music on the reality orientation andsociability of Alzheimer’s residents in along-term-care setting. Activities,Adaptation and Aging 1994; 18(2):41-55.
• Tabloski PA, McKinnon-Howe L,Remington R: Effects of calming music onthe level of agitation in cognitivelyimpaired nursing home residents. TheAmerican Journal of Alzheimer’s Care andManaging the Symptoms continuedRelated Disorders & Research 1995:10-15.
• Woods R, Ashley J: Simulated presencetherapy: Using selected memories to man-age problem behaviours in Alzheimer’sDisease patients. Geriatric Nursing 1995;16(1):9-14.
• Zanetti O, Frisoni GB, De Leo D, et al:Reality orientation therapy in Alzheimer’sDisease: Useful or not? A controlled study.Alzheimer Dis and Assoc Disord 1995;9(3):132-8.
When should I refer my patient with Alzheimer’s disease for a CT scan?
Response:In general, most elderly patients who present with aclear picture of this neurodegenerative dementia shouldnot require a computed tomography (CT) scan. Hence,those individuals with an insidious onset, gradual pro-gression and typical features of short-term memoryloss, followed by speech and language difficulty andproblems with activities of daily living (i.e., moneymanagement, bill paying and medication compliance)do not require this investigation.
The second Canadian Consensus Conference onDementia, held in February 1998 in Montreal, reaf-firmed recommendations for which patients require aCT scan. A cranial CT scan is recommended if one ormore of the following criteria are present:• age less than 60 years;• rapid (over one to two months) decline in cognition
or function;• dementia of short duration (less than two years);• any new localizing sign (hemiparesis or Babinski’s
reflex);• recent head trauma;• unexplained neurologic symptoms (onset of severe
headache or seizures);• history of cancer (especially in sites and types that
metastasize to the brain);• use of anticoagulants or history of a bleeding
disorder;• history of urinary incontinence and gait disorder
early in the course of dementia (as may be found innormal pressure hydrocephalus);
• gait disturbance; and/or
• unusual or atypical cognitive symptoms or presenta-tion (progressive aphasia).Central nervous system (CNS) infarctions or lacunes
should be documented with CT scan and neoplasm mustbe excluded in those individuals with focal CNS find-ings. The major reason for seeking a CT scan is to iden-tify those individuals with etiologies of their dementiaother than Alzheimer’s disease.
Neuro-imaging has a role in excluding reversiblecognitive dementia, such as tumor, N.P.H. or subduralhematoma, but it is less effective at distinguishingAlzheimer’s disease or other cortical dementias fromnormal aging. Patchy, white-matter lucencies occur inup to 10% of cognitively intact individuals and are oftenof uncertain significance.
Is it beneficial to increase the dosage of donepezil to 10 mg? If so, when is thebest time to do so?
Response:The recommendations are that all patients initiate treat-ment with donepezil at 5 mg per day. Both patients andcaregivers should be informed about the adverse effectsof the drug, including diarrhea, nausea, vomiting, mus-cle cramps, rhinitis and insomnia. The patient should beseen in follow up six weeks later. If the medication iswell tolerated, it should be increased at that point to 10 mg, whether or not symptomatic improvement hasbeen recognized by the patient or the caregiver. Thepatient should stay on the medication for a minimum ofthree months before decisions can be made about dis-continuation. Significant adverse events should indicatediscontinuation of the drug or, if they occur on the 10 mg dosage, a reduction back to 5 mg per day.
Featuring concise, practical answers to common questions about Alzheimer’s disease in everyday practice. The topics featured in this issue’s “Ask the Expert” are:
Diagnosing and treating Alzheimer’sDisease: CT scans and donepezilby Peter N. McCracken, MD, FRCPC
8 • The Canadian Alzheimer Disease Review • April 1999
A S K T H E E X P E R TA S K T H E E X P E R T
Q
Q

10 • The Canadian Alzheimer Disease Review • April 1999
Family members and caregiverstend to have many questions
about how a person with Alzheimer’sdisease (AD) is going to cope. Theywonder about the person’s ability todrive, manage money and use thestove. Family members and care-givers worry about the risks of allow-ing the person with AD to live athome. Occupational therapists are ableto assess the impact that cognitivedeficits have on the person’s day-to-day activities and they can suggestways to improve the person’s lifestyle.This article is a brief outline of ourapproach and the actions we take.1
Occupational therapists are multi-skilled health-care professionals whodeal with the daily lives of patientsexperiencing physical, psychologicaland social difficulties. They haveboth medical and social training,which gives them a more roundedview of the patient.2
The primary goal of occupationaltherapists is to enhance the patient’squality of life and, consequently, thatof caregivers by finding the appropri-ate level of stimulation that will max-imize the patient’s autonomy andimprove his or her self-esteem. Using
an assessment process, they try to dis-cover the abilities of the person withdementia, in order to adapt thepatient’s physical and social environ-ment to improve function and reducestress.3,4
Reaction to Occupational Therapists’ InterventionMultidisciplinary teams most ofteninclude occupational therapists whocan use early intervention techniquesto provide additional information andmake diagnosis easier. When a personwith mnemonic problems (the firststage of AD) is being evaluated, he orshe tends to feel humiliated. ADpatients tend to be unaware of prob-lems in their daily lives, and when theydo experience noticeable difficulty,they try to camouflage the deficit.
This is why family members, eventhose very close to the patient, are thelast to notice a loss of faculties. Theycling to the hope their parent is stilldoing well even when the person maybe unconsciously compensating foran inability to do something.
The role of the occupational ther-apist is to examine the patient’s func-tional activities in detail because a
The OccupationalTherapist and Home Assessment Signs of Alzheimer’s disease make it difficult to gaugean elderly relative’s independence. Occupationaltherapists suggest simple solutions for coping withcognitive deficiencies.
by Françoise McDonald and Andrée Tremblay
Françoise McDonald is anoccupational therapist, Côte-des-Neiges CLSC, Montréal, Québec
Andrée Tremblay is anoccupational therapist, Côte-des-Neiges CLSC, Montréal, Québec

self-evaluation often leaves some-thing to be desired and family mem-bers’ points of view can be biased.
Evaluation ToolsOccupational therapists use variouswritten tests to round out their assess-ments. They have a whole series oftests at their disposal, ranging frommini-mental and cognitive assess-ment scales for the elderly to themore sophisticated assessment ofmotor and process skills and cogni-tive competency tests.4 These testsprovide a more objective result, com-paring the person’s abilities withestablished standards (taking thepatient’s age and education intoaccount). However, it is essential forboth parts of the assessment to beconsidered when evaluating the man-agement of home risks. A patient mayfail the written tests, but retain safeperformance skills.
Apart from the formal assessment,an analysis of tasks helps us create alist of both a person’s strengths andweaknesses. By watching a patientperform a familiar task, such as prepar-ing a meal, we are able to analyze hisor her cognitive skill (memory, judg-ment, attention, sequence, visual analy-sis, etc.), physical ability (endurance,balance, strength, etc.) and psychologi-cal aptitude (significance for the person,pleasure derived, etc.). This analysisprovides a nice balance to the writtenassessment.
The patient’s activities tell usmore about the person and his or herstrengths and interests. They providea guide to the level of stimulationrequired for each individual. Ifrequirements are too demanding,there is a risk the patient will fail andbecome frustrated. Conversely, if heor she is too protected, it may lead toapathy, wandering (due to boredom)and a loss of self-esteem.
The occupational therapist’s assess-ment covers all aspects of daily activ-
ity. We have therefore chosen to dis-cuss those areas most commonlyobserved: money management, dri-ving, hygiene, dressing and mealpreparation (Table 1).
Money ManagementMoney management is one of the firstareas where difficulties occur: forget-ting to pay a bill, paying the same billtwice and compulsive or inappropriatebuying. Families often hesitate tobecome involved in money matters.Occupational therapists can thereforeevaluate this task using various tests,such as sorting through the mail,assessing recognition and ability tohandle coins, assessing knowledge ofthe value of objects, income, payingbills and writing cheques. It is impor-tant with this type of evaluation to dealwith an actual situation at home ratherthan simulate one; this is to avoid con-cepts which are too abstract or toocomplex. Based on these assessments,social workers will suggest appropriateresources or solutions.
DrivingWhen should a driver’s license betaken away? There are no hard andfast rules for determining the partic-ular stage or moment at which thisshould be done. Some people cancontinue to drive safely for yearsafter AD has been diagnosed.Others, however, will rapidly expe-rience perception problems (poorlyassessing distance) and will havedifficulty making the judgmentscrucial to driving. This decision isoften hard for caregivers and physi-cians because, in many cases, itaffects the person’s autonomy withrespect to going shopping or gettingout. When mnemonic problemsoccur, physicians sometimes won-der whether they should suspend thedriver’s license, even though thepatient has never had an accident orgotten lost.
As a guide, occupational thera-pists can perform a screening testusing standard methods to evaluatereaction time, attention, overall cog-nitive faculties and perceptual skills.
The purpose of the occupationaltherapist’s screening assessment is torefer the patient to the appropriateauthority for a final decision. Itshould be noted that regulations gov-erning automobile driving differ fromprovince to province.5,6
Personal CareWhen the patient’s hygiene and abili-ty to dress are affected, living athome tends to be re-evaluated andalternative accommodation consid-ered. Cognitive dysfunction, apraxiaand agnosia are the main difficultieswith respect to personal care.Everyday objects lose their meaning;for example, the patient will have dif-ficulty distinguishing white soap on awhite counter. He or she will alsohave problems putting clothes on inthe right order and on the correctbody parts.
The edge of a bath may be moredifficult to step over because thepatient does not perceive it as dis-tinctly as before. This type of diffi-culty can be solved by making adjust-ments such as placing a strip in a con-trasting color on the edge of the bath,installing support bars and an anti-skid covering or using a bath chair tomake it easier to wash sitting down.
To facilitate getting dressed,clothes can be organized on hangersby days or drawers identified to sim-plify choice of clothing. Physicalassistance or verbal instructions can
The Canadian Alzheimer Disease Review • April 1999 • 11
Table 1
Activities of Daily Living• Money management• Hygiene• Dressing• Driving• Meal preparation

also help. The extent of assistancemust be carefully monitored to allowthe patient to feel he or she is accom-plishing something. Incontinence canalso become a problem at a moreadvanced stage of the disease.Installing a commode is thereforeadvisable.7,8
Meal PreparationMeal preparation is a very broad areabecause it involves the ability to feedoneself, having an interest in doingso, and being able to organize the var-ious stages involved in preparing thedish. In early AD, patients frequentlyskip meals either because they forgetthem, or are subject to a severe loss ofappetite. In other cases, there may bedifficulty in preparing complicatedmeals, but the patient’s ability toreheat already-prepared meals isretained. Problems in using a stovecan be compensated for by installinga timer which turns off the elementsat a specific time. Microwave ovensare another alternative. It is a ques-tion of making kitchen access easierby not overloading refrigerators,keeping counters clear, eliminatingsuperfluous (condiments) or toxic
products. As with all functional activ-ities, it is important to know about theperson’s previous lifestyle and tastesto understand the current situation.7
Physical SurroundingsBased on functional assessmentresults, occupational therapists mustcreate a safe environment for thepatient to reduce the risk of falls andprovide conditions conducive to dailyactivities. Occupational therapiststherefore visit the patient’s home tosuggest ways to provide a stable envi-ronment. This would include remov-ing any obstacles (telephone or elec-trical wires, cumbersome furniture,sharp edges and loose mats), installingproper lighting and nightlights, adding ahandrail to staircases and avoiding rock-ers or chairs mounted on rollers or ballbearings.
When judgment is severelyimpaired, it is recommended that haz-ardous products and medication bekept under lock and key, electricaloutlets be capped and electrical tools,guns, matches, etc. be put away. If thepatient tends to wander, doors can bekept closed by adding locks, using achildren’s gate, installing a full-
length mirror on the door and analarm signal for when doors areopened. If the person is disoriented,photographs, pictures and different-colored door frames are suggested toindicate the areas to be used.Calendars, diaries, large-face clocks,notice boards, pictures and watcheswith the date are also useful. The ulti-mate goal is to create a safe, non-threatening, never-changing environ-ment to reassure the person withdementia.7,9,10
Our clinical work has shown thata better understanding of daily activ-ities helps set realistic objectives forpatients. However, efforts to com-pensate and provide the appropriatestimulation notwithstanding, we stillhave to manage the risks and definethe safety parameters acceptable tothe patient and his or her family. Inorder to maintain a smoothly func-tioning team, caregivers have toreach a consensus on the patient’sability to function at home.
In short, the desire to worktogether will help us achieve ourobjective of improving the qualityof life of our patients and theirfamilies.
12 • The Canadian Alzheimer Disease Review • April 1999
References1. Corporation professionnelle; 1996:
Pourquoi s’adresser à un ergothérapeute?Revue Québécoise d’ergothérapie.
2. Maltais D, Trickey F, Robitaille Y, et al:Promotion de l’autonomie des person-nes âgées par l’adaptation de leurdomicile. Rapport de recherche, 1991;DSC de l’Hôpital Général de Montréal.
3. Chevalier M: L’évaluation ergothérapiquede la clientèle psychogériatrique, 1995,Notes de cours, Montréal.
4. Société d’Alzheimer: ACE. Vivre àdomicile avec une démence de typeAlzheimer; publication ACE, 1998;Ottawa.
5. Dupont L: Evaluation de la conduiteautomobile chez les personnes âgéesprésentant des troubles cognitifs.Revue québécoise d’ergothérapie,1997. 6, 22-25.
6. Société d’Alzheimer: Sujets délicats,1997; Montréal.
7. Chevalier M, Archambault M:Stratégies d’intervention à domicilepour la clientèle avec déficits cognitifs,1995; Notes de cours, Montréal.
8. COTA: The safer tool. 1991; Ontario.9. CMHC, SCHL: At home with
Alzheimer’s disease, 1990; Montréal.10. Lévesque L, Roux C, Lauzon S:
Alzheimer: Comprendre pour mieuxaider. Editions du renouveau pédagogique,1990; Ottawa.

14 • The Canadian Alzheimer Disease Review • April 1999
How are you sleeping at night? Fine. How many timesdo you get up during the night? Not many. How many
times were you up last night? Oh, twelve. It’s just anothersleepless night for the Alzheimer caregiver.
For many of us, recognizing signs of stress in ourself isnot a frequent consideration. For those who provide care forindividuals with Alzheimer’s disease (AD), recognizingsigns of stress and caring for themselves is often ignoreduntil the stress takes a tremendous toll.
The Canadian Study of Health and Aging found that car-ing for a person with dementia was associated with chronichealth problems.1
For those providing care for a person with dementia inthe community, depressive symptoms were twice as com-mon as in the comparison group.
Many caregivers tend to set their own needs aside whilecaring for a person with AD, not recognizing the stress theyare under or denying its effect on their health. One possibleconclusion is that caregivers, by nature, care for others first.
Caregiver stress is a normal part of Alzheimer caregiving.There are steps caregivers can take to reduce it, but first itmust be recognized.
In an effort to provide Canadians with awareness andunderstanding of the signs of caregiver stress and what to doif there is concern, the Alzheimer Society launched “Are YouProviding Alzheimer Care? 10 Signs of Caregiver Stress” aspart of its January, 1999 awareness campaign.
Two new brochures have been created to support thisprogram. The second, “Reducing Caregiver Stress: FindingWays to Feel Better” provides information on strategies tofeel better and tells caregivers where to turn for help.
The 10 warning signs of caregiver stress include denialthat the person even has the disease, anger, emotional sensi-tivity, social withdrawal and depression. Symptoms alsoinclude lack of sleep, lack of concentration, exhaustion,anxiety and health problems.
For those exhibiting signs of caregiver stress, it is impor-tant to seek help. The person under stress should:• go to the doctor for regular check-ups;• ask family members and friends for their help
and support;• take advantage of community programs that provide
respite and relief from caregiving; • use programs that offer practical help with meals or
housework and assistance with the care of the personwith AD;
• plan ahead for both the immediate future and thelong term.These are just some of the things caregivers can do to
make their lives a bit easier. The Alzheimer Society helpscaregivers by providing services such as support groups,counseling, information resources and the AlzheimerWandering Registry.
The Society also funds research into improved methodsof caregiving and service delivery, as well as research intothe cause and cure of AD. These Alzheimer Societyresources and services are made possible by donations fromCanadians.
Reference1. Canadian Study of Health and Aging: Patterns of Caring for People
with Dementia in Canada. Cdn J on Aging 1994; 3(4):481-7.
Caregiver Stress:Looking After Yourself As WellThe Canadian Study of Health and Aging found that caring for a person withdementia was associated with chronic health problems. For those exhibiting signs of caregiver stress, it is important to seek help.
News From the AlzheimerSociety of Canada
Caregiver stress is a normal part ofAlzheimer caregiving. There are stepscaregivers can take to reduce it, butfirst it must be recognized.

The Canadian Alzheimer Disease Review • April 1999 • 15
Taking care of someone with Alzheimer’s disease(AD) can be a demanding task. It requires time and
energy and looking after someone you love can be diffi-cult. Even with youth and good health on your side, care-giving can be hard. To continue giving care, it is essentialthat you look after yourself.
Knowing and recognizing the signs of stress in yourselfor someone you care about is the first step in taking action.Finding ways to reduce the stress will help to lessen thelong-term emotional and physical toll of caregiving.
As a caregiver, you must take care of yourself; you arethe most important person in the life of someone with AD.The following is a list of common signs of caregiver stress:
1. Denial about the disease and its effect on the per-son affected: “I know Mom will get better. Theymust have made a mistake.”
2. Anger toward the person with AD and others: “Ifhe asks me that question once more I willscream!”
3. Withdrawing socially. You no longer want to stayin touch with friends or participate in activitiesyou once enjoyed: “I don’t care about gettingtogether with the neighbors anymore.”
4. Anxiety about facing another day and what thefuture holds: “I’m worried about what will happenwhen I can no longer provide care.”
5. Depression. You feel sad and hopeless much ofthe time: “I don’t care anymore.”
6. Exhaustion. You barely have the energy to completeyour daily tasks: “I don’t have the energy to do any-thing anymore.”
7. Sleeplessness.You wake up in the middle of the night orhave nightmares and stressful dreams: “I rarely sleepthrough the night, listening to hear if Dad is out of bed.”
8. Emotional reactions. You cry at minor upsets; you areoften irritable: “I cried when the grocery store was outof my favorite cereal. Then I yelled at the clerk.”
9. Lack of concentration. You have trouble focusingand you find it difficult to complete complex tasks. “Iused to do the daily crossword, now I am lucky if Ican concentrate enough to solve one quarter of it.”
10. Health problems. You may lose or gain weight, getsick more often (colds, flus), you may develop chron-ic health problems (backaches, headaches, highblood pressure): “Since the spring, I have had eithera cold or the flu. I just can’t seem to shake them.”
If you or someone you know is experiencing a num-ber of the symptoms on a regular basis, call your doctoror contact your local Alzheimer Society for help.
Adapted with permission from the Alzheimer’s Association, U.S.
To help cope with stress, see our brochure “ReducingCaregiver Stress: Finding Ways to Feel Better”, avail-able at your local Alzheimer Society or by calling theAlzheimer Society of Canada at 1-800-616-8816.
10 Warning Signs of Caregiver StressKnowing the signs is the first step in taking action to lessen the long-term emotional andphysical toll of caregiving.

16 • The Canadian Alzheimer Disease Review • April 1999
Pharmacologic Treatments forAlzheimer’s disease
A growing number of patients are developing Alzheimer’sdisease. Specific pharmacotherapy for the disease has increasedsignificantly over the past few years. It has therefore becomeimportant to gain a better understanding of the action and effectsof the various drugs available such as acetylcholinesteraseinhibitors.
by Serge Gauthier, MD, FRCPC
Dr. Gauthier, Alzheimer’s DiseaseResearch Unit, McGill Centre forStudies in Aging, Verdun, Québec
Once an accurate diagnosis ofdementia of the Alzheimer type
has been made and appropriate explana-tions of the implications of the diagno-sis and the treatment of any concomitantdiseases have been given, the physiciancan attempt treatment with an acetyl-cholinesterase (AChE) inhibitor. Toaccurately assess the therapeutic bene-fits, the patient’s cognitive, functional,behavioral and emotional levels must bedetermined before treatment begins.
Instruments developed for bothresearch and clinical practice such asthe Mini-Mental State Examination(MMSE)1 and the Clinical DementiaRating (CDR)2 can help the clinicianassess the impact of AChE inhibitors,especially during observation periodsthat exceed six months. We are opti-mistic that symptoms can be stabilizedover a 6- to 12-month period with ther-apeutic doses of AChE inhibitors.
Recent clinical experience suggeststhat antidepressants and commonlyused neuroleptics can be administeredin conjunction with AChE inhibitorswithout adverse effects.
The data presented in the literatureon AChE inhibitors are based on clinicaltrials involving patients with mild tomoderate Alzheimer’s disease (AD)
i.e., patients with a rating of 10 to 26on the MMSE scale or three to five onthe Functional Assessment Staging(FAST) scale.
Diagnosis and TherapyUsing AChE inhibitors does notnegate the need for a rigorous diag-nostic approach to assess the natureand causes of a complaint of memoryloss. A detailed anamnesis is the pri-mary tool used to diagnose dementia.
The anamnesis should be followedby a neuropsychological evaluation,which generally involves a structuredassessment tool such as the MMSE.This test, which measures overall cogni-tive functions, has several advantages: itcan be administered quickly, cliniciansare familiar with it, and it can help quan-tify a patient’s therapeutic response toan AChE inhibitor. This test is not, how-ever, a substitute for a global assessmentof a patient’s mood and functionalautonomy or of neuropsychiatric symp-toms such as agitation, apathy, delu-sions, hallucinations or aggressiveness.
This assessment of the various cat-egories of AD symptoms is relevantbecause improvements may occur inone symptom concurrently while dete-rioration occurs in another. A diagnosis

of dementia requires a series of obser-vations over a period of time, as doesthe monitoring of therapeutic responses.
The Use of AD-Specific DrugsA recent review of the history of phar-macotherapy for patients with ADhighlights the failure of the precursorsof acetylcholine (choline and lecithin),agents facilitating the release ofacetylcholine (linopirdine) and selec-tive muscarinic agonists (xanome-line).3 However, these agents weremostly assessed in a monotherapycontext, and their use in combinationwith AChE inhibitors should not beruled out, despite the added autonom-ic side effects.
The first large scale AChE inhibitorstudy was of tacrine. Because of itsshort half-life, the dosage requirementis four times per day, decreasing thelikelihood of compliance. Because ofthe gastro intestinal side effects associ-ated with its use, gradual upward titra-tion to therapeutic doses of between 120 mg and 160 mg per day is neces-sary. Moreover, a reversible level ofhepatic transaminase has been noted.Even though this agent has never beenmarketed in Canada, it has taught usabout the value of cholinergic pharma-cotherapy for AD, especially withrespect to long-term effects. Patientswho were able to tolerate only smalldoses of tacrine were admitted to long-term care institutions much earlier thanpatients treated with therapeutic doses(at least 120 mg per day) for a pro-longed period (two years or more).4
Pharmacoeconomic analyses demon-strate a positive effect of the long-termuse of AChE inhibitors such astacrine.5,6 A restrospective analysis ofpatients who have benefited from treat-ment with tacrine suggests, however,that those with the apolipoprotein E4(apo E4) genotype are less likely toshow improvement.7
Apo E4 mutation is associated witha significant reduction in cholinergicactivity and proportionally diminishes
the efficacy of AChE inhibitors such astacrine. A subsequent analysis of a larg-er number of patients treated withtacrine suggests this pharmacogeneticdistinction is apparent only in women.8
A post hoc analysis of the effica-cy results based on the MMSE andthe Alzheimer Disease AssessmentScale (ADAS) found a six-weekperiod before maximum improve-ment (as measured by the MMSEand the cognitive portion of theADAS) was attained at the maxi-mum dosage administered.9,10
A meta-analysis of 12 clinical tri-als confirmed benefits as measuredby the MMSE and improvement interms of clinical global impression,although age and severity of demen-tia had no clear influence on thetreatment effect.11 Furthermore, anopen label study and a post hocanalysis suggested positive effectson behavior.12,13
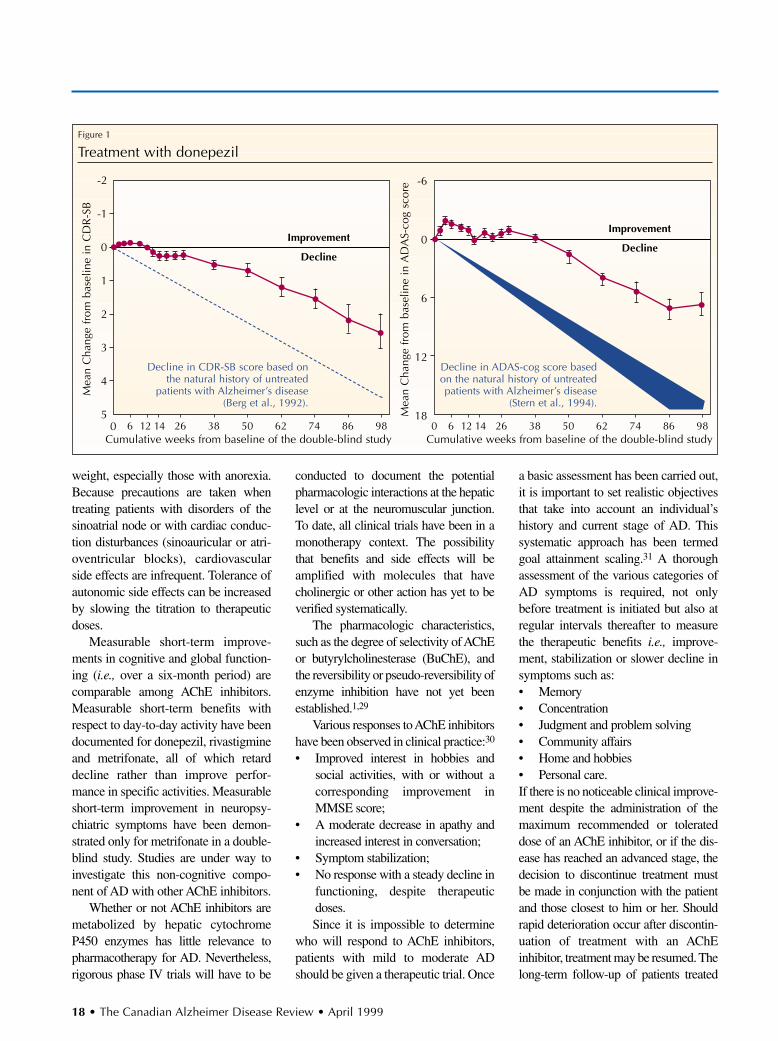
Donepezil was the first AChEinhibitor marketed in Canada.Compliance with treatment is facili-tated by a single daily dose, favorablegastro intestinal tolerability and noevidence of hepatotoxicity. Randomizeddouble-blind placebo-controlled trialshave shown that daily doses of 5 mg and10 mg are both effective on cognitiveand global functioning.14,15 However, ameta-analysis might reveal that a 10-mgdose has greater benefits. The results ofa multinational clinical trial of donepezilhave demonstrated that benefits of thedrug on day-to-day activity are statisti-
cally significant.15 The long-term follow-up of patients treated withdonepezil suggests a sustained therapeu-tic benefit.16
Pharmacoeconomic models show apositive balance sheet for donepezil.17, 18
However, that the data on which thesemodels are based are drawn from six-month studies.16 Various randomizedtrials are currently under way to assessthe longer-term (i.e., one year) effects ofdonepezil at more advanced stages ofthe disease.
Rivastigmine, for which Canadianapproval is pending, requires a dose-titra-tion period of several weeks before ther-apeutic dosage is attained. For greatergastro intestinal tolerability, it should beadministered at doses of 3 mg to 6 mgtwice daily. The results of clinical trialshave demonstrated beneficial effects oncognitive and global functioning, andday-to-day activity when administered attherapeutic doses.19,20
Metrifonate, which is still understudy, is the longest-acting AChEinhibitor and can therefore be admin-istered in a single daily dose. Thoughthe drug is well tolerated, reversiblemuscular weakness of the arms andlegs has recently been observed incertain patients receiving relativelyhigh doses.20 Phase III trials haveshown improvements proportionateto the doses administered withrespect to cognitive and global func-tions, day-to-day activity and behav-ior.21-25 The efficacy of metrifonatedoes not seem to be dependent on theapo E4 genotype.26
Galantamine, also under study,has modulatory effects on nicotinicreceptors, as well as on AChEinhibitor activity.27 The data fromphase II trials have demonstrated sig-nificant cognitive improvement.28 Thisdrug can be administered in two or threedaily doses.29
Gastro intestinal side effects are pro-portionate to dosage and may be a lim-iting factor in the use of AChEinhibitors in patients with low body
The Canadian Alzheimer Disease Review • April 1999 • 17
Donepezil was the firstAChE inhibitor marketedin Canada. Use of thedrug is facilitated by asingle daily dose, favor-able gastro intestinal tolerability and no evi-dence of hepatotoxicity.
weight, especially those with anorexia.Because precautions are taken whentreating patients with disorders of thesinoatrial node or with cardiac conduc-tion disturbances (sinoauricular or atri-oventricular blocks), cardiovascularside effects are infrequent. Tolerance ofautonomic side effects can be increasedby slowing the titration to therapeuticdoses.
Measurable short-term improve-ments in cognitive and global function-ing (i.e., over a six-month period) arecomparable among AChE inhibitors.Measurable short-term benefits withrespect to day-to-day activity have beendocumented for donepezil, rivastigmineand metrifonate, all of which retarddecline rather than improve perfor-mance in specific activities. Measurableshort-term improvement in neuropsy-chiatric symptoms have been demon-strated only for metrifonate in a double-blind study. Studies are under way toinvestigate this non-cognitive compo-nent of AD with other AChE inhibitors.
Whether or not AChE inhibitors aremetabolized by hepatic cytochromeP450 enzymes has little relevance topharmacotherapy for AD. Nevertheless,rigorous phase IV trials will have to be
conducted to document the potentialpharmacologic interactions at the hepaticlevel or at the neuromuscular junction.To date, all clinical trials have been in amonotherapy context. The possibilitythat benefits and side effects will beamplified with molecules that havecholinergic or other action has yet to beverified systematically.
The pharmacologic characteristics,such as the degree of selectivity of AChEor butyrylcholinesterase (BuChE), andthe reversibility or pseudo-reversibility ofenzyme inhibition have not yet beenestablished.1,29
Various responses to AChE inhibitorshave been observed in clinical practice:30
• Improved interest in hobbies andsocial activities, with or without acorresponding improvement inMMSE score;
• A moderate decrease in apathy andincreased interest in conversation;
• Symptom stabilization;• No response with a steady decline in
functioning, despite therapeuticdoses.Since it is impossible to determine
who will respond to AChE inhibitors,patients with mild to moderate ADshould be given a therapeutic trial. Once
a basic assessment has been carried out,it is important to set realistic objectivesthat take into account an individual’shistory and current stage of AD. Thissystematic approach has been termedgoal attainment scaling.31 A thoroughassessment of the various categories ofAD symptoms is required, not onlybefore treatment is initiated but also atregular intervals thereafter to measurethe therapeutic benefits i.e., improve-ment, stabilization or slower decline insymptoms such as:• Memory• Concentration • Judgment and problem solving• Community affairs• Home and hobbies• Personal care.If there is no noticeable clinical improve-ment despite the administration of themaximum recommended or tolerateddose of an AChE inhibitor, or if the dis-ease has reached an advanced stage, thedecision to discontinue treatment mustbe made in conjunction with the patientand those closest to him or her. Shouldrapid deterioration occur after discontin-uation of treatment with an AChEinhibitor, treatment may be resumed. Thelong-term follow-up of patients treated
18 • The Canadian Alzheimer Disease Review • April 1999
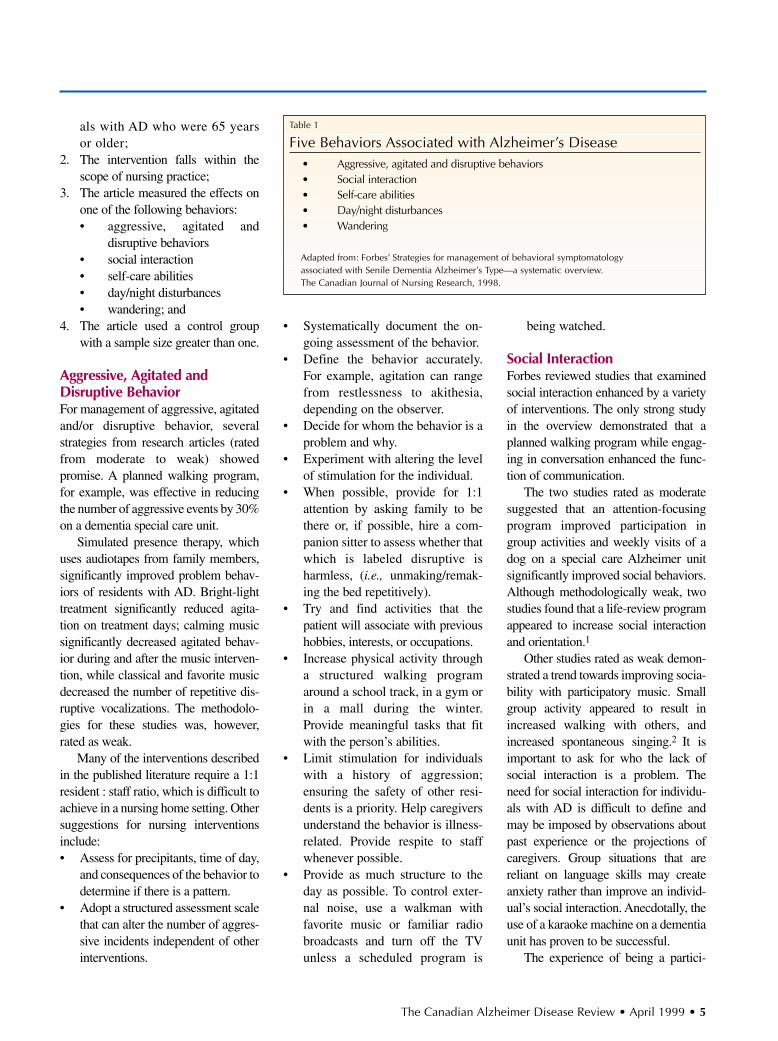
Figure 1
Treatment with donepezil
Mea
n C
hang
e fr
om b
asel
ine
in A
DA
S-co
g sc
ore -6
0
6
12
18
Improvement
Decline
Mea
n C
hang
e fr
om b
asel
ine
in C
DR
-SB
Cumulative weeks from baseline of the double-blind study
-2
-1
0
1
2
3
4
50 126 14 26 38 50 62 74 86 98
Cumulative weeks from baseline of the double-blind study0 126 14 26 38 50 62 74 86 98
Improvement
Decline
Decline in CDR-SB score based onthe natural history of untreated
patients with Alzheimer’s disease (Berg et al., 1992).
Decline in ADAS-cog score basedon the natural history of untreatedpatients with Alzheimer’s disease
(Stern et al., 1994).

The Canadian Alzheimer Disease Review • April 1999 • 19
References1. Folstein MF, Folstein SE, McHugh PR:
Mini-Mental State: a practical methodfor grading the cognitive state ofpatients for the clinician. J PsychiatrRes 1975; 12:189-98.
2. Morris JC: The Clinical DementiaRating (CDR): current version andscoring rules. Neurology 1993;43:2412-13.
3. Forette F, Boller F: Drug development inAlzheimer’s disease: a review of its history and a preview of its future. In: Gauthier S (ed): Pharmacotherapy ofAlzheimer’s disease. Martin Dunitz,London, 1998; pp. 1-15.
4. Knopman D, Schneider L, Davis K, etal: Long-term tacrine (Cognex) treat-ment: effects on nursing home place-ment and mortality. Neurology 1996;47:166-77.
5. Lubeck DP, Mazonon PD, Bowe T:Potential effect of tacrine on expendi-tures for Alzheimer’s disease. MedInterface 1994; 7:130-8.
6. Wimo A, Karlsson G, Nordberg A, etal: Treatment of Alzheimer disease withtacrine: a cost-analysis model.Alzheimer Dis Assoc Disord 1997;11:191-200.
7. Poirier J, Delisle MC, Quirion R, et al:Apolipoprotein E4 allele as a predictorof cholinergic deficits and treatmentoutcome in Alzheimer disease; ProcNatl Acad Sci USA 1995; 92:12260-64.
8. Farlow MR, Lahiri DK, Poirier J, et al:Treatment outcome of tacrine therapydepends on apolipoprotein genotypeand gender of the subjects withAlzheimer’s disease. Neurology 1998;50:669-77.
9. Rosen WG, Mohs RC, Davis KL: A newrating scale for Alzheimer’s disease.Am J Psychiatry 1984; 141:1356-64.
10. Sands LP, Katz I, Schneider L:Assessing individual patients for cognitive benefits from acetyl-cholinesterase inhibitors. AlzheimerDis Assoc Dis 1999, in press.
11. Qizilbash N, Whitehead A, Higgins J, etal: Cholinesterase inhibition for Alzheimerdisease: a meta-analysis of the tacrine trials. JAMA 1998; 280:1777-82.
12. Kaufer DI, Cummings JL, Christine D:Effects of tacrine on behavioral symptomsin Alzheimer’s disease: an open labelstudy. J Geriatr Psychiatry Neurol 1996;9:1-6.
13. Raskind MA, Sadowsky CH, SigmundWR, et al: Effects of tacrine on lan-guage, praxis and concognitive behav-ioral problems in Alzheimer’s disease.Arch Neurol 1997; 54:836-40.
14. Rogers SL, Farlow MR, Doody RS, etal: A 24-week, double-blind, placebo-controlled trial of donepezil in patientswith Alzheimer’s disease. Neurology1998; 50:136-45.
15. Gauthier S, Rossor M, Hecker J, et al:Results from a multinational phase IIIclinical trial of donepezil inAlzheimer’s disease. Presented at theFifth International Geneva–SpringfieldAlzheimer Symposium, Geneva, April 1998.
16. Rogers SL, Friedhoff: Longterm efficacyof donepezil in the treatment ofAlzheimer’s disease: an interim analy-sis of the results of a U.S. multicentreopen end extension study. Eur.Neuropsychopharmacol, 1998; 28:67-75.
17. Small GW, Donohue JA, Brooks RL: Aneconomic evaluation of donepezil inthe treatment of Alzheimer’s disease. Clin Ther 1998; 20(4):838-50.
18. O’Brien BJ, Goerce R, Kux M, et al:Economic evaluation of donepezil forthe treatment of Alzheimer’s disease inCanada. J Am Geriatr Soc, in press.
19. Corey-Bloom J, Anand R, Veach J: Arandomized trial evaluating the effica-cy and safety of ANA 713 (rivastigminetartrate), a new acetylcholinesteraseinhibitor, in patients with mild to mod-erately severe Alzheimer’s disease. Int JGeriatr Psychopharmacol 1998; 1:55-65.
20. Rosler M, Anand R, Cicin-Sain A, et al:Efficacy and safety of rivastigmine inpatients with Alzheimer’s disease:results of an international, 26-week,multicentre, randomised, placebo-controlled trial. BMJ 1999;318:633-8.
21. Schmidt BH, Heinig R: The pharmaco-logical basis for metrifonate’sfavourable tolerability in the treatmentof Alzheimer’s disease. Dement GeriatrCogn Disord 1998; 9(suppl.2):15-19.
22. Cyrus PA, Ruzicka BB, Gulanski B: Thedose-related improvement by metri-fonate of the cognitive performance ofAlzheimer’s disease patients.Neurology 1998; 50:A89.
23. Morris JC, Cyrus PA, Orazem J, etal: Metrifonate benefits cognitive,behavioral and global function inpatients with Alzheimer’s disease.Neurology 1998; 50:1222-30.
24. Gélinas I, Gauthier S, Cyrus PA, et al: The efficacy of metrifonate inenhancing the ability of Alzheimer’sdisease patients to perform basicand instrumental activities of dailyliving. Neurology 1998; 50:A91.
25. Cummings JL, Cyrus PA, RuzickaBB, et al: The efficacy of metri-fonate in improving the behavioral disturbances of Alzheimer’s disease.Neurology 1998; 50:A251.
26. Farlow MR, Lahiri DK, Brashear A, et al: Metrifonate in the sympto-matic treatment of Alzheimer’s dis-ease: influence of apolipoprotein Egenotype. Neurology 1998; 50:A88.
27. Pontecorvo MJ: Clinical develop-ment of galantamine: evaluation ofa compound with possible acetyl-cholinesterase inhibiting and nicotinic modulatory activity.Neurobiol Aging 1998; 19:57.
28. Wilcock G, Wilkinson D:Galantamine hydrobromide: interim results of a group compara-tive, placebo-controlled study ofefficacy and safety in patients witha diagnosis of senile dementia ofthe Alzheimer type, 1997. In: IqbalK, Winblad B, Nishimura T, et al(eds): Alzheimer’s Disease: Biology,Diagnosis and Therapeutics. JohnWiley & Sons, Chichester, pp. 661-4.
29. Knopman DS, Morris JC: An updateon primary drug therapies forAlzheimer’s disease. Arch Neurol1997; 54:1406-9.
30. Gauthier S: Do we have a treatmentfor Alzheimer’s disease—yes. ArchNeurol 1999; in press.
31. Rockwood K, Stolee P, Howard K, et al: Use of goal attainment scaling tomeasure treatment effects in an anti-dementia drug trial.Neuroepidemiology 1996; 15:330-8.
32. Doody RS, Pratt RD, Perdomo CA:Clinical benefits of donepezil—results from a long-term phase IIIextension trial. Presented at theAmerican Academy of NeurologyAnnual Meeting, 1999.
with an AChE inhibitor such asdonezepil has demonstrated, however,that a temporary suspension of treat-ment (from three to six weeks) resultsin a loss of observed benefits: theseare not fully recovered when treat-ment is resumed.32
The therapeutic value and safety ofcombination treatments such as an
AChE inhibitor with an antioxidantsuch as tocopherol or gingko bilboa,estrogen or a nonsteroidal anti-inflammatory have yet to be established.
ConclusionsClinicians can and should help peo-ple with AD and their families.Although cholinergic pharmacothera-
py is now part of global case management strategies, there ismuch to be learned about the clini-cal response profiles of AChEinhibitors. Systematic observa-tions, as well as post hoc analysesof randomized clinical phase III tri-als, will help refine the use of theseagents.
Lorem ipsum dolor sit amet, consectetueradipiscing elit, sed diam nonummy nibheuismod?
Duis autem vel eum iriure dolor in hendrerit in vulputatevelit esse molestie consequat, vel illum dolore eu feugiatnulla facilisis at vero eros et accumsan et iusto odio dig-nissim qui blandit praesent luptatum zzril delenit augueduis dolore te feugait nulla facilisi. Lorem ipsum dolorsit amet, consectetuer adipiscing elit, sed diam nonum-my nibh euismod tincidunt ut laore.
Lorem ipsum dolor sit amet, consectetueradipiscing elised diam?
Duis autem vel eum iriure dolor in hendrerit in vulputatevelit esse molestie consequat, vel illum dolore eu feugiatnulla facilisis at vero eros et accumsan et iusto odio dig-nissim qui blandit praesent luptatum zzril delenit augueduis dolore te feugait nulla facilisi. Lorem ipsum dolorsit amet, consectetuer adipiscing elit, sed diam nonum-my nibh euismod tincidunt ut laore.
Q
Q
20 • The Canadian Alzheimer Disease Review • April 1999
HistoryMrs. Davies is a 74-year-old, married, retired nurse wholives in a two-story house. She initially presented one yearago with an eight-month history of forgetfulness, word-finding difficulties and problems with shopping and payingbills. At that time, her neurologic exam was normal, but hermini-mental state examination (MMSE) was 22/30, withproblems in orientation to time, three-item recall, pentagondrawing and reverse spelling. Based on a comprehensiveassessment, including laboratory testing and head computedtomography (CT) scan, the diagnosis of Alzheimer’s disease(AD) was confirmed.
Physical ExaminationMrs. Davies’ husband has brought her to your office at pre-sent because, in his view, her condition has worsened in thelast two months. According to him, she is more forgetful,very repetitive, and exhibiting increasing difficulties with allactivities of daily living (ADL), including hygiene and feed-ing herself. Her husband also reports she is complainingmore of constipation, fatigue, knee and back pain, and short-ness of breath. She also seems more irritable and, at times,anxious, especially at night. Her attention span is short andinconsistent. She is increasingly refusing to go out of thehouse and mostly sits in her favorite rocking chair. Herrepeat MMSE score is 15/30, with declines in all spherescompared to one year ago.
Question• Is this deterioration characteristic of AD?
DiscussionHer subacute deterioration is highly unlikely to be exclusively a progression of her underlying AD. First,despite the individual variability in the course of mild tomoderate AD, Mrs. Davies’ husband has noticed a markedand acute change in her condition over the past few months.This is not characteristic of the gradual and insidious cogni-tive decline associated with AD. One would expect anMMSE decline of approximately 2-4 points per year.
The physician should think of the four Ds in this respect:Delirium, Depression, Diseases and Drugs. A critical role in family-practice follow-up of dementia is regular supervisionand reassessment to ensure that deterioration is in keeping
with only the progression of the underlying AD. It is alsovery important that the family physician fully educate care-givers so that any acute or subacute deterioration is notassumed to be merely a progression of AD, but is promptlybrought to the attention of the physician.
Question• What does her presentation suggest?
DiscussionThere can be a tendency to focus on a simple obvious diag-nosis, but the fundamental nature of elderly patients is thatthey can have multiple, interacting medical problems. Theinterface between medical illnesses and dementia is two-fold. First, a superimposed delirium is extremely commonbecause, by definition, all patients with dementia haveexhausted their cerebral reserve. Second, poor control ofmedical problems may make the dementia appear worse interms of cognitive and functional abilities.
This particular problem is exacerbated by the fact thatpatients with AD do not complain of symptoms, making opti-mal care of multiple medical problems more difficult for thefamily physician. Dementia, though primarily a neurologicdisorder, is secondarily a whole-body problem. Mrs. Davies’presentation would suggest the following possibilities:• Inadequate control of her arthritis, congestive heart
failure (CHF), and/or gastroesophageal reflux.• Progressive renal failure if she is over diuresed with
possible digoxin toxicity.• Occult upper gastrointestinal tract (UGI) bleed
secondary to nonsteroidal anti-inflammatory drug(NSAID) therapy.
• Central nervous system (CNS) toxicity from cimetidine,digoxin or naproxen.
• Fecal loading/impaction.• Silent myocardial infarction (MI) with increased CHF.• Increased as needed use of benzodiazepines (lorazepam)
or narcotics (Tylenol NO. 2®) resulting in a pharmacolog-ic “concussion”.
• Hyponatremia or hypernatremia.• Uncontrolled hypertension/postural hypotension.
Question• What further steps would you take?
Alzheimer’s Disease WithComorbid Medical Problems
C A S E S T U D Y
by William B. Dalziel, MD, FRCPC
The Canadian Alzheimer Disease Review • April 1999 • 21
DiscussionThe physician’s next steps would be to undertake a compre-hensive assessment of Mrs. Davies’ known medical condi-tions and to screen for the common problems that may beresponsible for her subacute decline.
In most cases, the diagnosis will be made through a his-tory and a physical examination. Additional investigations toconsider to sort out Mrs. Davies’ problems would include achest x-ray, electrocardiogram (ECG), urinalysis, urine forculture, hemoglobin and white blood count, creatinine andblood urea nitrogen (BUN), calcium, blood sugar and elec-trolytes, and serum digoxin level.
The patient’s coronary artery disease and hypertensionare strong risk factors for vascular dementia and, based onthe control of her blood pressure and any new neurologicsymptoms or signs, the physician may need to rule out asuperimposed vascular event.
Question• How could her current drug therapies be contributing
to her problems?
DiscussionIn the elderly, drug side effects commonly present as a finalcommon pathway problem, typified by the “geriatric giants”:falls, immobility, confusion, depression, incontinence anddecreased functional abilities. Although almost any drug cancause confusion in the elderly, the leading suspects in Mrs.Davies’ case would include cimetidine, digoxin, naproxen,Tylenol NO. 2® and, as needed, lorazepam. Patients withdementia, especially elderly patients, are particularly suscep-tible to CNS side effects from drugs. Any drugs, either pre-scription or over-the-counter, with anticholinergic side effectsare particularly high risk, including anti-Parkinsonian drugs,neuroleptics, tricyclic antidepressants and antihistamines.
ProgressIn terms of her medical problems, Mrs. Davies was found tohave digoxin toxicity, pre-renal failure and postural hypoten-sion secondary to dehydration, fecal loading secondary tooveruse of narcotic analgesics, and over-sedation secondaryto increased use of lorazepam for anxiety. Digoxin was dis-continued (no history or presence of atrial fibrillation, andCHF was controllable with a diuretic alone).
Diuretics were stopped short-term until her dehydrationresolved. Fecal loading was treated short-term with stimu-lant laxatives and long-term with a regimen of fluid, fiberand increased physical activity. Docusate sodium and peri-staltic stimulant were discontinued. As well, Tylenol NO. 2®
and naproxen were discontinued and her arthritic pain wascontrolled with regular doses of acetaminophen (500 mgfour times daily).
Three months later, Mrs. Davies is feeling symptomati-cally much better and her MMSE is now 19/30 (often treat-ment of concomitant medical problems will improve cogni-tion). She maintains independence in her personal ADLs.Her husband asks if she would be a candidate for the newantidementia drug, even though she has multiple medicalproblems and is on multiple medications (at this time cime-tidine, acetaminophen 500 mg qid, diltiazem HCI,hydrochlorothiazide and Milk of Magnesia®).
Question• Do her multiple medications and medical problems
preclude Mrs. Davies from consideration for donepeziltherapy?
DiscussionDonepezil has a dual elimination pathway: it is metabolizedin the liver by the cytochrome P450 enzyme system as wellas eliminated through urinary excretion. It has not beenfound to interfere with the metabolism of such drugs ascimetidine, warfarin, theophylline, digoxin, etc. It does notappear that the clearance of donepezil is significantly modi-fied in patients with moderate to severe renal impairment.Liver function testing during treatment with donepezil is notrequired. Donepezil should be used more cautiously inpatients over the age of 85, especially women with low bodyweight and in patients with significant impairment of therenal or hepatic systems. Caution is also advised in elderlypatients in terms of the peripheral cholinergic side effects ofdonepezil, particularly patients with a history of asthma,obstructive pulmonary disease, supraventricular cardiac con-duction conditions (except for right bundle branch block)and patients with peptic ulcer disease.
The most frequent side effects of donepezil seen at rateshigher than placebo are those predictable cholinergic sideeffects such as diarrhea, nausea and vomiting, which, inmost cases are mild and transient. Side effects are minimizedwhen therapy is initiated at 5 mg per day and increased aftera six-week period to the recommended 10 mg per daydosage. Mrs. Davies, despite her multiple medications andmultiple medical problems, would be an appropriate candi-date for donepezil therapy, which has been proven effectivein patients with mild to moderate dementia (MMSE between10 and 26).
Suggested Readings:
1.Drachman DA, et al: Making sure it’s really Alzheimer’s. Patient Care 1991; 13.
2.Gauthier S: Battling back against dementia. Canadian Journal ofDiagnosis 1997; 75.
3.Geldmacher DS, Whitehouse PJ: Evaluation of dementia. N Engl J Med 1996; 335:330-6.
Related Documents