28/5/21 1 Aryeh Shander, MD, FCCM, FCCP, FASA Director, TeamHealth Research Institute Emeritus Chief Department of Anesthesiology, Critical Care and Hyperbaric Medicine Englewood Hospital and Medical Center, Englewood, New Jersey Courtesy Clinical Professor UF College of Medicine Adjunct Clinical Professor of Anesthesiology, Medicine and Surgery Icahn School of Medicine at Mount Sinai, New York Clinical Professor of Anesthesiology Rutgers Medical School, New Jersey THE BURDEN OF BLEEDING DISCLOSURE 1 SPEAKERS BUREAU: Merck CONSULTANT/SPEAKER: Masimo Corporation, CSL Behring, Gauss Surgical, Vifor Pharma, Octapharma and Pharmaniaga GRANT/RESEARCH: CSL Behring, Masimo, HbO2 Therapeutics, LLC 2 DISCLOSURE 2 CONSULTANT: USDOD, USDOJ AND USDHHS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

28/5/21
1
Aryeh Shander, MD, FCCM, FCCP, FASADirector, TeamHealth Research Institute
Emeritus Chief Department of Anesthesiology, Critical Care and Hyperbaric MedicineEnglewood Hospital and Medical Center, Englewood, New Jersey
Courtesy Clinical Professor UF College of Medicine
Adjunct Clinical Professor of Anesthesiology, Medicine and SurgeryIcahn School of Medicine at Mount Sinai, New York
Clinical Professor of Anesthesiology Rutgers Medical School, New Jersey
THE BURDEN OF BLEEDING
DISCLOSURE 1SPEAKERS BUREAU: MerckCONSULTANT/SPEAKER: Masimo Corporation, CSL Behring, Gauss Surgical, Vifor Pharma, Octapharma and PharmaniagaGRANT/RESEARCH: CSL Behring, Masimo, HbO2 Therapeutics, LLC
2
DISCLOSURE 2CONSULTANT: USDOD, USDOJ AND USDHHS

28/5/21
2
OBJECTIVES AND OVERVIEW• Discuss the real burden of bleeding in surgery• Conditions associated with increased bleeding during
surgery• Accurate assessment of blood loss leads to appropriate
interventions• Discuss ways to avoid unneeded transfusions by use of
hemostatic agents and sealants• Introduce the VIBe scale tool for intraoperative bleeding
management
HEALTHCAREHealthcare System Expectations:
• Clinical:o Outcome – Survival vs. well-being
• Administrative:o Cost (expenditure), efficiency, regulations
• Evolving concept of “Value-based” vs. current ”Volume-based” payment systemo Concept of surgical bleeding as a quality measure!

28/5/21
3
A STRATEGY FOR HEALTH CARE REFORM — TOWARD A VALUE-BASED SYSTEM• Move towards a Value-Based System• Our system rewards those:
o Those who bill for more serviceso Not those who deliver the most value (care?)
• A Value-Based System will provide (reward):o Achieving and maintaining good health vs. dealing with poor health*o Decreasing the cost and resource consumption**
* Important** More important
Porter ME. Et al. N Engl J Med. 2009
HOW TO ACHIEVE A VALUE-BASED DELIVERY SYSTEM*
• Mandatory measurement and dissemination of health outcomes• Reexamining the organization of the services• Reorganizing care delivery around medical conditions• A reimbursement system based on improving value for patients• Providers to compete for patients, based on value at the medical –
condition level • EMRs• Consumers to become much more involved – ‘shared decision’• * Safety is inherent
Porter ME. Et al. N Engl J Med. 2009

28/5/21
4
ENDLESS GRID OF HEALTHCARE
Cost HIGH LOW NEUTRAL
Quality HIGH LOW NEUTRAL
§ BEST§ Neutral§ Worst
ASSESSMENT OF BLEEDING

28/5/21
5
CAUSES OF INTRAOPERATIVE AND POSTOPERATIVE HEMORRHAGE
Intraoperative Delayed postoperative (days 2–7)
Structural/technical defects Thrombocytopenia
Disseminated intravascular coagulation Acquired platelet disorders (aspirin or NSAID)
Heparin overdose Vitamin K deficiency
Hyperfibrinolysis Multiorgan failure
Early postoperative (days 0–2) Acquired immune coagulopathy
Structural/technical defects Operator mishap
Thrombocytopenia Operator poor decision making
Inherited or acquired platelet disorders
Mild to moderate inherited/acquired coagulation disorder -
Marietta M. et al. Transplant Proc. 2006
BLEEDING MANAGEMENT IN THESURGICAL PATIENT• Unanticipated surgical bleeding
o Expensiveo Risk to patiento Associated with poor outcome
• Anticipated surgical bleedingo Requires planningo Addresses need for resourceso Implements a clinical pathway

28/5/21
6
FACTORS THAT IMPACT BLEEDING-RELATED COMPLICATIONS
1The progressively widespread use of anticoagulant and
antiplatelet therapeutics
2Technological
advances that enable complex and lengthy surgical procedures
3The advancing age of the general population
with associated comorbidities that
predispose to bleeding related complications
Shander A, et al. JACS 2014
CONDITIONS ASSOCIATED WITH INCREASED BLEEDING RISKS• Advanced age• Serious co-morbid conditionso Liver diseaseo Renal diseaseo HBP
• History of significant GI bleeding• History of CVA• Additional medication or substance abuse• Labile INR

28/5/21
7
ESTIMATED BLOOD LOSS DURING SURGERY IS OFTEN OVERSTATED
Physician estimate of Blood Loss was 40% higher than
actual blood loss
Hill SJ et al. ASA. 201160 spine surgery patients
60 practitioners participated: 17 anesthesia providers, 22 surgeons, and 21 nurses and technicians
ESTIMATION OF BLOOD LOSS IS INACCURATE AND UNRELIABLELuke D. Rothermel, MD, MPH and Jeremy M. Lipman, MD, Cleveland, OH
Surgery. 2016

28/5/21
8
DOES ANYONE GRADE THE BLEEDING?
WHO Classification
Grade 1Minor
Blood Loss
Grade 2Mild
Blood Loss
Grade 3Gross
Blood Loss
Grade 4Debilitating Blood Loss
WHO Classification

28/5/21
9
VALIDATED INTRAOPERATIVE BLEEDING SCALE (VIBE SCALE)Grade Visual presentation Anatomic appearance Qualitative
descriptionVisual estimated rate of blood loss (mL/min)
0 No bleeding No bleeding No bleeding ≤ 1.0
1 Ooze or intermittent flow Capillary-like bleeding Mild >1.0–5.0
2 Continuous flow Venule and arteriolar-like bleeding Moderate >5.0–10.0
3 Controllable spurting and/or overwhelming flow
Noncentral venous and arterial-like bleeding Severe >10.0–50.0
4Unidentified or inaccessible spurting or gush
Central arterial- or venous-like bleeding Life threatening* >50.0
*Systemic resuscitation is required (e.g., volume expanders, vasopressors, blood products, etc.).
Kevin Lewis, Qing Li, Drew Jones et al. Surgery. 2017 Mar;161(3):771-781.
UNIVERSAL DEFINITION OF PERIOPERATIVE BLEEDING IN ADULT CARDIAC SURGERY
Cornelius Dyke, Md, Solomon Aronson, MD, Wulf Dietrich, MD, PhD, Axel Hofmann, ME, Keyvan Karkouti, MD,Marcel Levi, MD, PhD, Gavin J. Murphey, MD, FRCS, Frank W. Sellke, MD, Linda Shore-Lesserson, MD, Christian von Heymann, MD, and Marco Ranucci, MD
J Thorac Cardiovasc Surg 2014

28/5/21
10
WEIGHT OF THE BLEEDING IMPACT ON EARLY AND LATE MORTALITY AFTER PERCUTANEOUS CORONARY INTERVENTION
Gjin Ndrepepa, Elena Guerra, Stefanie Schultz, Massimiliano Fusaro, Salvatore Cassese, Adnan Kastrati
J Thromb Thrombolysis. 2015
Study includes 14,180
patients
Fig. 1 Landmark analysis showing probability of death at 30 days and from 30 days — 1 year in patients with and without bleeding within the 30 days after PCI
TOP 10 MOST COSTLY, FREQUENT MEDICAL COMPLICATIONS IN THE US
http://www.soa.org/files/pdf/research-econ-measurement.pdf
Error type % of injuriesthat are errors
Count of injuries (2008)
Count of Errors (2008)
Medical costper Error
In HospitalMortality Cost per Error
STD Cost Error
Total Cost per Error
Total Cost of Error Millions
Pressure Ulcer (Medicare Never Event)
>90% 394,669 374,964 $8,730 $1,133 $425 $10,288 $3858
Postoperative infection >90% 265,995 252,695 $13,312 $- $1,236 $14,548 $3,676
Mechanical complication of device, implant or graft
10-35% 268,353 60,380 $17,709 $426 $636 $18,771 $1,133
Postlaminectomy syndrome 10-35% 505,881 113,823 $8,739 $- $1,124 $9,863 1,123
Hemorrhage complicating a procedure 35-65% 156,433 78,216 $8,665 $2,838 $778 $12,272 $960
Infection following infusion, injection, transfusion, vacc
>90%9,321 8,855 $63,911 $14,172 $- $78,083 $691
Pneumothorax 35-65% 51,119 25,256 $22,256 $- $1,876 $24,132 $617
Infection due to central venous catheter >90% 7,434 7,062 $83,365 $- $- $83,365 $589
Other complications of internal biological, synthetic
<10% 535,666 26,783 $14,851 $1,768 $614 $17,233 $462
Ventral hernia w/o mention of obstruction or gangrene
10-35% 239,156 53,810 $6,359 $260 $1,559 $8,178 $440

28/5/21
11
The "All-patient" cohort comprised 21,429 patients: 213 "significant bleeding"; 2,780 "non-significant bleeding"; and 18,436 "no bleeding"
THE CLINICAL AND ECONOMIC BURDEN OF SIGNIFICANT BLEEDING DURING LUNG RESECTION SURGERY: A RETROSPECTIVE MATCHED COHORT ANALYSIS OF REAL-WORLD DATASudip K. Ghosh, Sanjoy Roy, Mehmet Daskiran, Andrew Yoo, Gang Li and Elliott J. Fegelman
J Med Econ. 2016
IMPACT OF BLEEDING-RELATED COMPLICATIONS AND/OR BLOOD PRODUCT TRANSFUSIONS ON HOSPITAL COSTS IN INPATIENT SURGICAL PATIENTS
• Overall, the rate of bleeding-related complications was 29.9%
• Overall, incremental LOS associated with bleeding-related complications or transfusions was 6.0 days
• The incremental cost per hospitalization associated with bleeding-related complications and adjusted for covariates was:
• Highest for spinal surgery ($17,279) followed by vascular ($15,123), solid organ ($13,210), non-cardiac thoracic ($13,473), cardiac ($10,279), general ($4,354), knee/hip replacement ($3,005), and reproductive organ ($2,805)
• The study supports implementation of blood-conservation strategies
Michael E Stokes, Xin Ye, Manan Shah, Katie Mercaldi, Mathew W Reynolds, Marcia FT Rupnow and Jeffrey Hammond
BMC Health Serv Res 2011

28/5/21
12
MEAN TOTAL ADJUSTED HOSPITAL COSTS (95% CIS) IN 2007 $US BY SURGICAL COHORT
BMC Health Serv Res 2011
Surg
ical c
ohor
t
$38,112.00
$9,295.00
$18,255.00
$19,063.00
$31,959.00
$37,047.00
$31,461.00
$39,050.00
$20,833.00
$6,490.00
$15,250.00
$14,709.00
$18,749.00
$23,574.00
$16,338.00
$28,771.00
$0.00 $10,000.00 $20,000.00 $30,000.00 $40,000.00 $50,000.00
Spinal (N=107,185)
Repro duct ive (N=384,131)
Knee/ hip (N=246,815)
General (N=362,507)
Solid organ (N=45,687)
Non-car diac thoracic (N=142,533)
Vascular (N=216,191)
Cardiac (N=130,806)
Mean total hospital costs(2007)
Non bleeding-related conseq uencesBleeding-related con sequences
N = 2991 patients identified with a hospital associated bleed
RELATIONSHIP OF HOSPITAL-ASSOCIATED BLEEDING WITH LENGTHOF STAY AND TOTAL HOSPITALIZATION COSTS IN PATIENTS HOSPITALIZED FOR ATRIAL FIBRILLATIONAlpesh N. Amin, Scott B. Robinson, Bruce D. Bowdy, Yonghua Jing, Bernadette H. Johnson and Daniel P. Wiederkehr
J Med Econ. 2016

28/5/21
13
THE THERAPY
TRANSFUSION PRACTICE• Not scientific/rational
o Corwin HL, et al. Chest. 1995;108:767-71.• Lots of action little knowledge• Salem-Schatz SR, Avorn J, Soumerai S B. JAMA
1990:25;264(4):476-83• “Cultural” vs. evidence based
o Goodnough LT et al. J.A.M.A. 1991• Stover PE ANESTHESIOLOGY 1998
• Guidelines unknown or ignored

28/5/21
14
When to Transfuse: Is It Any Surprise That We Still Don’t Know?Jacob T. Gutsche, MD
To Transfuse or Not to Transfuse: Is It Really a Question?George N. Thalmann
To Transfuse or Not to Transfuse in Upper Gastrointestinal Hemorrhage? That is the Question.Don C. Rockey, MD
OBSERVED VARIATION IN HOSPITAL-SPECIFIC TRANSFUSION RATES FOR PRIMARY ISOLATED CABG SURGERY WITH CARDIOPULMONARY BYPASS DURING 2008 (N = 798 SITES)
• Variation in transfusion rates due to:• Local culture and practice• Physician preference re: hemoglobin “trigger”
• Variation in transfusion rates not due to differences in patient acuity • Transfused patients not necessarily that different
than those not transfused• Some of the variation is due to differences in
how patients’ blood is “managed”: anemia treatment, avoiding blood loss, inappropriate transfusion threshold
Bennett-Guerrero, E. et al. JAMA 2010;304:1568-1575.

28/5/21
15
POTENTIAL RISKS OF BLOOD TRANSFUSIONINFECTIOUS§ Infectious agents – for example, hepatitis
viruses, HIV, West Nile virus, bacteria, cytomegalovirus, syphilis, dengue fever virus, malaria, new variant Creutzfeldt-Jakob disease
NONINFECTIOUS§ Transfusion reactions
§ Medical errors (wrong blood given because of mislabeled specimen or patient misidentification)
§ TRALI
§ TACO
§ Iron overload§ Immunomodulation§ Clinical effects due to storage of blood
Murphy MF et al. Transfus Clin Biol. 2015
0 USD
500 U SD
1,000 USD
1,500 USD
2,000 USD
2,500 USD
3,000 USD
3,500 USD
EH MC RIH CHUV AKH LinzMean RBC produc t cost Mean cost per RBC txn Mean txn cost per surg ical pt txed
COST OF RBC TRANSFUSION
COBCON - Shander et al., Transfusion 2010
28/5/21
16
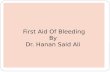
COST OF PLASMA TRANSFUSION
COBCON – Shander et al. Vox Sang 2016
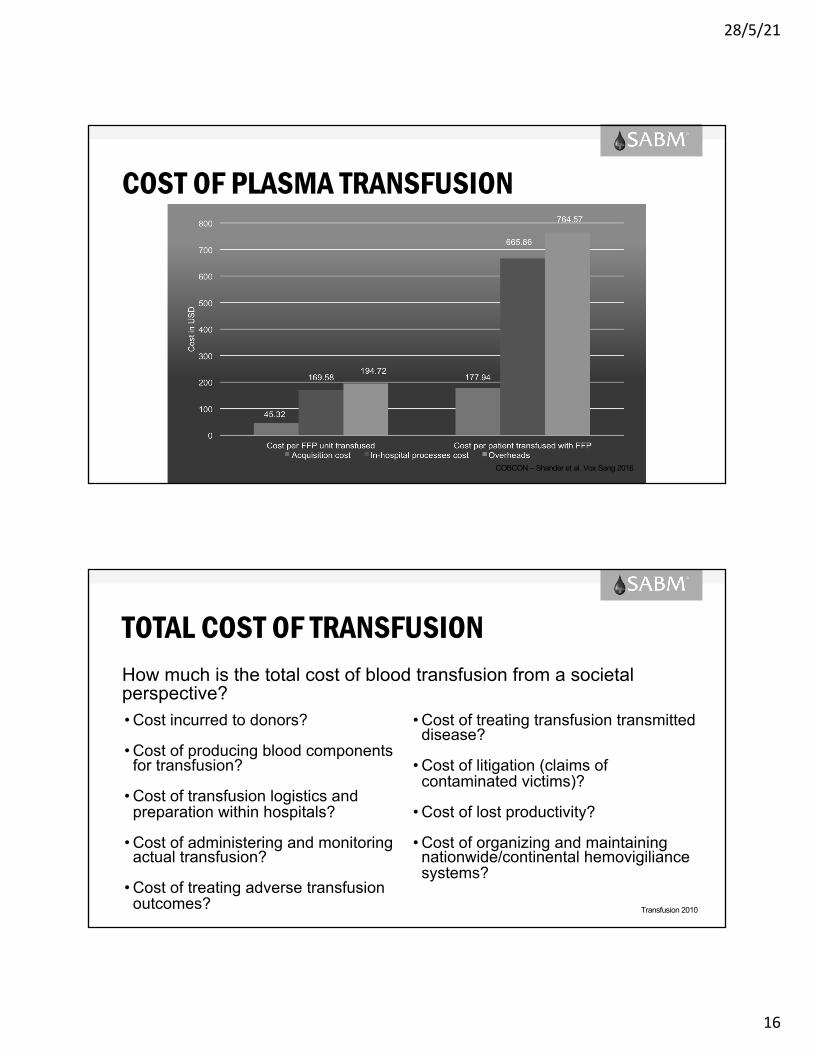
TOTAL COST OF TRANSFUSIONHow much is the total cost of blood transfusion from a societalperspective?
Transfusion 2010
• Cost incurred to donors?
• Cost of producing blood componentsfor transfusion?
• Cost of transfusion logistics andpreparation within hospitals?
• Cost of administering and monitoringactual transfusion?
• Cost of treating adverse transfusionoutcomes?
• Cost of treating transfusion transmitteddisease?
• Cost of litigation (claims ofcontaminated victims)?
• Cost of lost productivity?
• Cost of organizing and maintainingnationwide/continental hemovigiliancesystems?

28/5/21
17
Menitove JE. 2018
THE CONFUSION CONTINUES: RESULTS FROM AN AMERICAN ASSOCIATION FOR THE SURGERY OF TRAUMA SURVEY ON MASSIVE TRANSFUSION PRACTICES AMONG UNITED STATES TRAUMA CENTERS
• Most institutions regularly activate recently implemented MTPs for trauma and nontrauma indications; however, few use validated scoring systems for MTP activation
• MTP content is highly variable. Few institutions use VET, while most have incorporated tranexamic acid into their protocol
• The lack of consistent practices underscores the need for outcome-based studies to guide transfusion
Eric Etchill, Jason Sperry, Brian Zuckerbraum, Lous Alarcon, Joshua Brown, Kevin Schuster, Lewis Kaplan, Greta Piper, Andrew Peitzman and Matthew D. Neal
Transfusion. 2016

28/5/21
18
RATIO VS GOAL DIRECTEDMassive Transfusion Packages (1:1:1)Pro: additional volume effectCon: side effects of plasma, time delay, prophylactic, transfusion, efficacy . . .
Individualized target controlled coagulation management and transfusionPro: no prophylactic transfusion, less side effects of transfusion related complications, efficacyCon: additional demand of colloids/crystalloids, close POC monitoring . . .
SUMMARY• Bleeding is a major concerno Impacts patient outcomeo Increases resource consumptiono Is costly for hospitalso Is costly for healthcareo Increases demand of resources
§ That made add to the overall negative outcome§ That adds to an already expensive complication

28/5/21
19
EARLY AND ACCURATE RECOGNITON LEADS TO EARLY INTERVENTION AND IMPROVED OUTCOME

Related Documents