GENETIC COUNSELING, Vol.10, No 1, 1999, pp. 79-88 THE BEHAVIOURAL PHENOTYPE IN VELO.CARDIO.FACIA SYNDROME (VCFS): FROM INFANCY T0ADOLESCENCE By As w L L E N l KD EVRT E N DT','' u f' rrrir {oifi[l] p fi ],[i f Fli;, Summary: I'he behavioural phenotype in Velo-Cardio-Facial syndrome (VCFS): from infancy to adolescence: ln lhis contfibution the current status and recent findings of the behavioural phenotype in VCFS (22q11, dele- tion) are discussed with regard [o motor development, cognition and neurodevelopment,, and behaviour and l,emperament. Motor: hlpotonia in infancy, gross-molor milestones are delayed, prcblems with coordination andbalance frnm preschool ageon, problems with tempo/speed dufingadolescence Cognition andneurodevelopment: learning disabilities (82-100V0), intellectual disability (450/o), better verbal abilitiesthan performal abilities, poor atlention and concentra[ion, visuo-perceptual-spatial prublems, good (auditory) memory An important, subgroup of children (557o) hasa non-verbal learning disability (NLD). Behaviour and social-emotional developmen[: AD(H)D, withdrawn and shy, person-dependent, social problems in relalionships with peers, anxious, risk for child psychiatric problems as well as for the development of psy- chiatricproblems during adolescence and earlyadulthood Information on the behavioural phenotype in VCFS (22q1 1 deletion) is of grcatimportance to clinicians as an aid to s),ndrome diagnosis, bul evenmorE to parents because it offersimmense dirEct, practical valueto lhe management, of the behaviour of their child. Apprcpriate counseling and information on the long-term expecta- tions, andbetterinsight in the behaviour will lead to the development of rEalistic ways of coping with l,heir child. Key-words: Behavioural phenotype - VCFS - 22q1 .l deletion - Non-verbal learning disability IINTRODUCTION Velo-cardio-facial syndr0me, als0 known as Shprinlzen syn- drome (1978), is a multiple anomaly disorder estimated t0affec[ 1 in 4000 individuals (1). The ofiginal presen[ing symptoms lhat con- lributed [0the clinical delineation 0fthis entity were the associati0n 0f hypernasal speech, cardiac anomalies, learning disabilities, and a characteristic facial appearance. The discovery 0f a submicro- scopic deletion in chromosom e 22q11 (9)in the maiority 0fpatients confirmed that VCFS is a specific syndrome. In most patients the delelion occurs de novo, but familial occurence wi[han affected pafenI is noted in approximately 150/0 of patients (15). The clinical phenotype 0f the disofder has been broadened and includes over 40 clinical features, and patients with VCFS are being identified from manio-facial clinics, genelic clinics, pediatric cardi- ology clinics, iearning/developmental centefs, and, m0re recently, (1) Centre forHuman Gene- tics, DepartmenL of Clinical Genelics, Univers jly Hospilal Gaslhuisberg, Leuven, Belgium (2) Departmenl of EducaLional Sciences, Universily of Leuven, Leuven. Belgium 70 1 ,"I

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

GENETIC COUNSELING, Vol . 10, No 1, 1999, pp. 79-88
THE BEHAVIOURAL PHENOTYPE IN VELO.CARDIO.FACIALSYNDROME (VCFS): FROM INFANCY T0 ADOLESCENCE
By A s w L L E N l K D EVRT E N DT','' u f'
rrrir {oifi[l]
p fi ],[i f Fli ;,
Summary: I'he behavioural phenotype in Velo-Cardio-Facial syndrome (VCFS): from infancy to adolescence:ln lhis contfibution the current status and recent findings of the behavioural phenotype in VCFS (22q11, dele-tion) are discussed with regard [o motor development, cognition and neurodevelopment,, and behaviour andl,emperament.Motor: hlpotonia in infancy, gross-molor milestones are delayed, prcblems with coordination and balance frnmpreschool age on, problems with tempo/speed dufing adolescenceCognit ion and neurodevelopment: learning disabi l i t ies (82-100V0), intel lectual disabi l i ty (450/o), better verbalabilities than performal abilities, poor atlention and concentra[ion, visuo-perceptual-spatial prublems, good(auditory) memory An important, subgroup of chi ldren (557o) has a non-verbal learning disabi l i ty (NLD).Behaviour and social-emotional developmen[: AD(H)D, withdrawn and shy, person-dependent, social problemsin relalionships with peers, anxious, risk for child psychiatric problems as well as for the development of psy-chiatric problems during adolescence and early adulthoodInformation on the behavioural phenotype in VCFS (22q1 1 deletion) is of grcat importance to clinicians as anaid to s),ndrome diagnosis, bul even morE to parents because it offers immense dirEct, practical value to lhemanagement, of the behaviour of their child. Apprcpriate counseling and information on the long-term expecta-tions, and better insight in the behaviour will lead to the development of rEalistic ways of coping with l,heir child.
Key-words: Behavioural phenotype - VCFS - 22q1 .l deletion - Non-verbal learning disability
IINTRODUCTION
Velo-cardio-facial syndr0me, als0 known as Shprinlzen syn-drome (1978), is a mult iple anomaly disorder estimated t0 affec[ 1in 4000 individuals (1). The ofiginal presen[ing symptoms lhat con-lr ibuted [0 the cl inical del ineation 0f this entity were the associati0n0f hypernasal speech, cardiac anomalies, learning disabil i t ies, anda characterist ic facial appearance. The discovery 0f a submicro-scopic deletion in chromosom e 22q11 (9) in the maiority 0f patientsconfirmed that VCFS is a specif ic syndrome. In most patients thedelel ion occurs de novo, but famil ial occurence wi[h an affectedpafenI is noted in approximately 150/0 of patients (15).
The cl inical phenotype 0f the disofder has been broadened andincludes over 40 clinical features, and patients with VCFS are beingidentif ied from manio-facial cl inics, genelic cl inics, pediatr ic cardi-ology clinics, iearning/developmental centefs, and, m0re recently,
(1) Centre for Human Gene-t ics, DepartmenL of Cl in icalGenel ics, Univers j ly Hospi la lGaslhuisberg, Leuven,Belgium
(2) Departmenl of EducaLionalSciences, Universi ly ofLeuven, Leuven. Belgium
70 1, " I
GENETIC COUNSELING
als0 from chi ld psychiatf ic uni ts and psychiatr ic inst i lut ions becauseof behavioural and psychiatr ic problems.
In this contf ibul ion the cuf rent sta[us and fecenl f indings of thebehavioural phenolype in VCFS (22q1l delet ion) wi l l be discussed
I THE CONCEPT a BEHAVIOURAL PHENOTYPE >
Behavioural phenotype is a new name for an old 0bservat ion.For as long as there have been ident i f iable congenital causes 0fdevelopmental disabi l i ty, i t has been recognized that people affectedby some 0f these usyndromes,, can have typical behavioural andtempef amenlal featuf es.
In 1994, Fl inl & Yule (2) gave the fol lowing def ini t ion 0f lhe con-cept 0f behavioural phenotype: .The behavioural phenotype is acharac[er ist ic pattern ol motor, cognit ive, l inguist ic and social0bserval iOns, which is consistent ly associaled wi lh a biological /genet ic disorder. In some cases, the behavioural phenotype mayc0ns[ i lu le a psychiatr ic disorder; in 0thers, behaviours which arenot usual ly regarded as symp[0ms of psychiatr ic disorders mayOccuf >. In lhis def ini l , ion, i I is not proposed lhal the l ink betweenbehavioural phenotype and the ass0ciated biological /genel ic dis0f-der is a simple, one-t0-0ne or universal relat ionship, but more l ikelya complex and varied one.
The behavioural phenotype in VCFS (22ql1delet ion) wi l l be dis-cussed, wi lh fegard t0 (a) m0tor development, (b) cognit ion andneurodevelopment, and (c) behaviour and [emperamenl.
(A) MOTOR DEVELOPMENT
Hypotonia during childhood in VCFS is fep0rted in 760/o t0 B5%0 0[pa[ients (7, 11). Already early in infancy, babies with VCFS have dif-ficullies in developing the appropfiate musc]e strenglh and motorcoordination t0 learn basic movemen[s. In a previous study per-formed in 37 chi ldren with VCFS (14), the ma j0f i ty of chi ldren, - evenlhose wi[h a borderline to normal intelligence - were significantlyslower than the normal peers in reaching the miles[ones ncrawlingoand *walking alone, (see Table I). Most infan[s wtlh a22q11 de]elionare able to walk independent ly between 1B-24 months.
As the chi ldren grow older, the hypotonia decreases, but gfoss-motor abi l i t ies are often delayed. Chi ldren with VCFS have part icu-
THE BEHAVIOURAL PHENOTYPEIN VCFS 122U.11 DELETION)
180

A. SwttrN erar , Behavioural phenotype in VCFS I
Milestones in motor development(months)
Si t t ing alone (8. I ) 'Crawling (B 7)
Standing alone (13 4)
Walking alone (14 '1 )
Mean VCFS
96
12 0r ' ,
136
]B B'
SEM
1 064
r 633
I 208
1 447
lar ly problems with coofdinat ion and balance. During adolescence,prOblems wi[h tempo/speed are frequent ly Observed. Graphomotorperf0rmances are alsO n0ted t0 be poor (4).
Physical excefcises [0 incfease muscle streng[h and co0rdina-t i0n are therefore important in the care 0f these chi ldren, even froman early age 0n.
(B) COGNITION AND NEURODEVELOPMENT
Intelligence
In lheir in i [ ia l descr ip[ ion 0f [he syndrOme, Shprin[zen et a] . ,(10) recognized [he presence 0f leafning disabi l i t ies in al l pa[ ients.Since then, learning di f f icul t ies have been reported in 820/o (7) Lo1000/o (11)0f the pat ients wi th VCFS. Mental retardat, ion 0r in[el-lectual disabi l i ty (nol specif ical ly def ined) is reporled [o be presenIin 400/o tro 460/o.ln a previous sludy 0n 37 children and adolescentswith VCFS (14), intel lectual disabi l i ly (def ined as FSIQ < 70 or >-2 SD below [he mean) was found in 45o/o. ln the ma;or i ly 0f [hem(380/o) [he inlel lectual disabi l i ty was mi]d (FSIQ 55-69) and onlytwO pat ients had a moderate intel lectual disabi l i ty (FSIQ 40-54).Severe mental retardat, ion seems [0 be rare in VCFS. Only one chi ldwith a famil ia l delet ion and cerebel lar hypoplasia was severelyreLarded (FSIQ 24). This sludy also conf irmed the wide var iabi l i ty inintel l igence in VCFS pat ients. Unt i l now, there have been no goodexplanat ions for the var iabi l i ty in intel l igence (for example, no cor-relat, ion with the extent 0f the delet iOn). in our study (14)we did notf ind a correlat ion belween intel l igence and [he presence or absenceof a congenital heart defect: the mean FSIQ of chi ldren with a heartdefect (n=1 7) was 77.2, and the mean FSIQ of the chi ldren withOut,a heart defecl (n=20) was 68, which is not stat ist ical ly s igni f icant(Student 's , [esl , p=0.10447). The mode of inheri tance however,namely famil ia l delet ion versus de novo delet ion, seems to play arole in the var iabi l i ly 0f intel l igence in VCFS: the incidence 0f intel-lectual disabi l i ty was higher in the pat ients with a famil ia l delet ion(10/12 or 83,3%o) vefsus the pat ien[s wi[h a de novo delet ion (7/25or 2\o/o). We found a statislical significant difference in mean FSIQbetween pat ients wi th a ' fami l ia l 'delet ion (M 63.2; SD 11.08) andpa[ ien[s with a "de n0v0, dele[ i0n (M 79.8; SD 11.8) (Student r test,
Iable 1: Mileslones inmoton development, inVCFS (FSIQ > 70)
(a) mean (accordin€ [o BayleyDevelopmental Scales 2-l l0mon Ihs)(b) srgnit icant, t)<0 05.(c) signi l tcant p<0 01
q1- ' l
IGENETtC COUNSELTNG
p<0.002). In lhis analysis, 0ne patient with a famil ial deletion andsevere menml retardalron was excluded. This difference can possi-bly be explained in part by the lower educationallevelof paren[s olfamil ial cases versus parents of de novo cases. Indeed, parental IQand socio-economic status, are major determining factors 0f the IQin chi ldren, and here this was es[imaled by lhe educational levelofthe parents. In famil ialcases, also Lhe parent who did n0t, carfy Lhedelel ion, had a lower educational level compared lo parents of den0v0 cases, sugges[ing ass0rla[ ive mating.
Neuropsychological profile
Studies 0n lhe in[el l igence profi le of VCPS children afe scarse.In a sludy on 24 children and young adulls wilh VCFS, 54%o of thechildren had a signif icanI higher verbal IQ (80 t 13) than performalIQ (72 t 9) (B). We also found in 0ur s[udygroup of 37 children andadolescen[s a sta[ist ical signif icant difference be[ween [he meanverbal IQ (M=78; SD 14.7) and the mean performal IQ (M=70;SD11.3) (14). In m0st chi ldren, speci f ic cogni t ive def ic i ts i .e. v isuo-perceptual-spatial abi l i ty and planning abil i ty, could be suspecledfrom the cogni[ ive profi le. This could refer to a typical non-verballearning disabil i ty (NLD). RecenI f indings of a study on primaryschool age children with VCFS (22q1l deletion) and a borderl ine [onormal intel l igence (FSIQ > 70), show that for many neuropsycho-logical functions, chi ldren wilh VCFS (22q11 deletion) and childrenwith NLD have the same assets and deficits (16).
Poor altenl ion and concentration, an impulsive working styleand good memory have also been described in VCFS (4, 16).
As a resul[ 0f [hese neuropsychological assets and deficits, themajori[y of chi ldren with VCFS wil l have learning problems, espe-cial ly in the afeas 0f af i thmetics and reading comprehension.
VCFS children wil l therefore benefit from remedial leaching andappropria[e teaching strategies such as a struc[ured learning envi-ronmenl 0f inlefact, ive c0mpu[er based inslruction (6).
(C} BEHAVIOUR AND SOCIO.EMOTIONAL DEVELOPMENT
Behaviour and temperament
Aftef the delineation of [he syndrome, seveial common behav-ioural and temperamen[al features were observed in VCFS children,and confirmed in later studies: impulsive and disinhibi led on theone hand, withdrawn and shy 0n the other hand (4, 13). Also ADHD,ADD, emotional unstabil i ly, and anxie[y have been reporled duringchildhood (3,4). In our experience, many children with VCFS atevery attached to and dependent from the members of their family,e.g. they can not go to sleep if the m0ther is n0[ aI home; they only
182

A. Swttrv rr at., Behavioural phenotype in VCFS I
wanl [0 stay wilh a babysi[[er i f another persOn 0f the family is pre-sent (a brother 0r a sister); they can behave very differentlydepending from which pefs0n is wiLh them: [hey do very well withone [eacher/counselor, [hey underachieve wi[h anO[her teacher.Therefore [he term (pefson-dependent, should be added t0 [he l is[of typical behavioural features of VCFS.
In view 0f the reports of more severe psychopathology in olderpatien[s wilh a 22q11 de]etion (14, 3), the m0sr imporrant ques[i0nin this area is: whal is [he natural history of this behaviour, tem-perament, and social development? To answer this queslion, a longi-tudinal study 0n lhe behaviour and social cOmpelence of infants,chi ldren and adolescents wi[h VCfS was init iated in this Centre.Parents, teachers and adolescents were asked to evalua[e [hebehaviour and social development 0f theif chi ld (or of themselves)using standardized ques[ionnaires (CBCL, TRF, YSR) (17). Theseques[ionnaifes consists of 112 behaviours (problem items). Theresults from the checklist are t,ransformed f irsl int0 a [0talproblemsc0re, sec0nd into lwo subscores for respecLively intrernalising(withdrawn, somatic complainls, and anxious/depressed) and ex[er-nalising problem behaviour (delinquent and aggressive), and thirdinto a profi le of clusters with specif ic problem behaviour (wirh-drawn, somatic complainls, anxious/depressed, social problems,thought problems, a[[en[ion problems, delinquent behaviour, andaggressive behaviour). T scores (X=50, SD=10) were calculated foreach patienl. For lhe [0[al problem score, and [he internalising andexlernalising subscores, a to[al T score of63 or higher (90[h centi leor higher) is considered [0 be in the "cl inical> range. T scores (forthe seperale syndromes) higher than 70 (> g8th centi le) are foundin populations wi[h severe behavioural 0r emotional problems. For[he specif ic problem clusters, a T score of66 or higher (> 93rd cen-[ i le) ate considered t0 be 0f concern.
Unti l now, the s[udygrOup consist,s of 60 children and adoles-cents (29 boys and 31 girls) with a 22q11 delerion. sublects weredivided in[o four groups based on aSe groups:
Group 1: infan[s aged 2-3 years (n=i6)
Group 2: preschool chi ldren aged 4-6 years (n=19)
Group 3: primary school chi ldren aged 7-11 years (n=16)
Gnoup 4: adolescenls aged 1 2-18 years (n=9)
The cross-sectional data revealed the f0l lowing prel iminary f ind-lngs:
1. Parenls, teachers and adolescenls repotI more in[ernalizingproblem behaviour lhan ex[ernalizing problem behaviour, and[his difference seems t0 increase with ape.
e?l"- l
I GFNtFTtT- anl tNtqFt tNtaiuf r \ f , r ru u\JrJr \Jf ,L i l \u
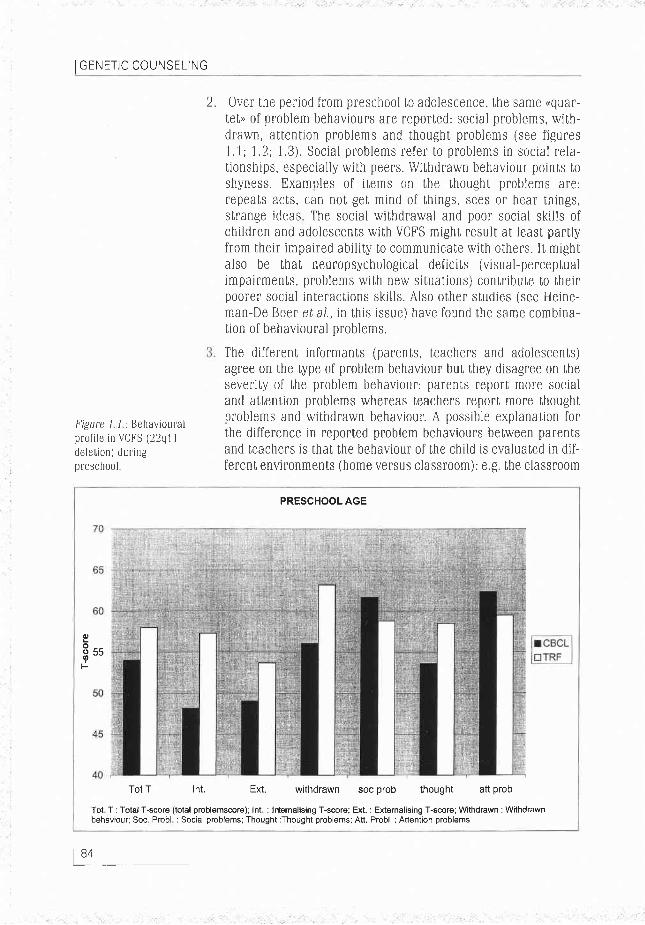
2. Over lhe period from preschool [o adolescence, the same (quar-tet> 0f problem behaviours are reported: social problems, with-drawn, atlention problems and thought problems (see f igures1.1;1.2:1.3). Social problems refer [o problems in social re la-t ionships, especial ly wi[h peers. Wi[hdrawn behaviour poin[s t0shyness. Examples 0f i [ems 0n [he th0ught pnoblems are:repea[s acts, can nOt get mind of things, sees 0r hear things,slrange ideas The social withdrawal and poor social ski l ls ofchi ldren and adolescents wi[h VCFS might result, at least, parl lyfrom their impaired abil i ty lo communica[e with others. I t mighIalso be [hat neur0psychological deficits (visual-perceptualimpairments, problems with new situa[i0ns) c0ntribute t0 theirpoorer social interactions ski l ls. Also other s[udies (see Heine-man-De Boer era1., in this issue) have fOund the same combina-[ion of behavioural problems.
The different informan[s (parenls, leachers and adolescents)agree 0n the type of problem behaviour but they disagree 0n [heseveri[y of lhe problem behaviour: pafenls report, more socialand attention problems whereas teachers report more thoughtproblems and wilhdrawn behaviour. A possible explanation forthe difference in reported problem behaviours between parentsand teachers is that the behaviour of [he child is evaluated in dif-ferenI environments (home versus classroom): e.g. the classroom
l,.igure 1 / : Behaviouralprof i le in VCt 'S (22q1 1delet ion) dur ingpreschool
PRESCHOOL AGE
Eo__!2 55
F
Tot T Int. Ext. withdrawn soc prob thought att prob
Tot T : Total T-score (total problemscore); Int : Intemalising T-score; Ext. : Externalising T-score; Withdrawn : Withdrawnbehaviour; Soc Probl i Social problems; Thought:Thought problems: Att. Probl, : Attention problems
184

A. SwrtttN rr,qr., Behavioural phenotype in VCFS I
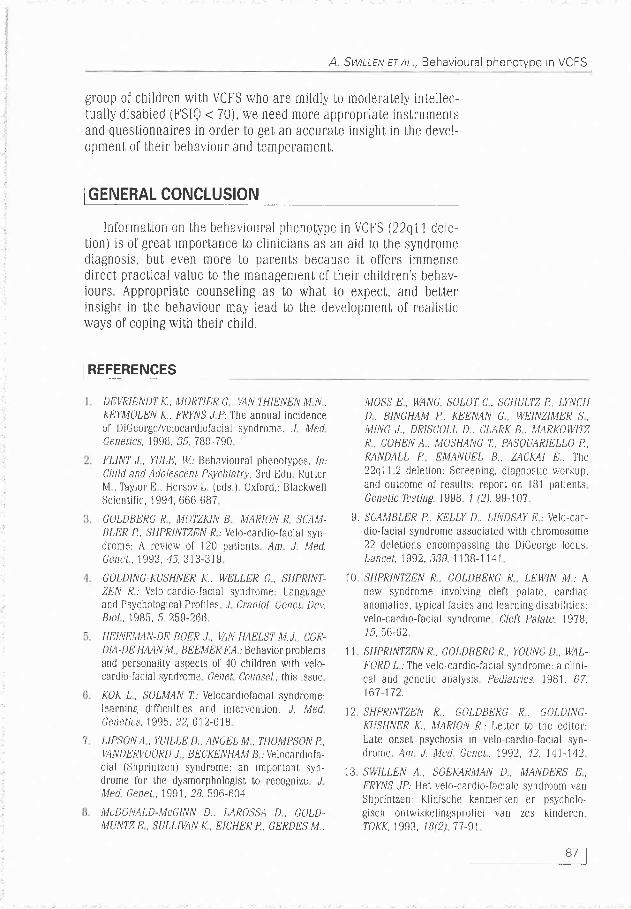
PRIMARY SCHOOL AGE
Tot T Int Ext. withdrawn soc prob thought aft prob
Tot T: Total T-score (total problemscore): Int : Internalising T-score; Ext, I Externalising T-score; Withdrawn: Withdrawnbehaviour; Soc Probl : Social problems: Thought:Thought problems; Att Probl : Attention probtems
Figure 1 2.: Behavioural prol i le in VCFS (22q1 1 dele[ i0n) during primary school
ADOLESCENCE
OU
ud
8ssqF
50
4C
40Tot T Int. Ext. withdrawn soc prob thought att prob
Tot T: Total T-score (total problemscore): Int : lnternalising T-score; Ext. : Externalising T-scorel Withdrawn : Withdrawnbehaviour; Soc Probl : Social problems; Thought: Thought problems; Att Probl : Attention problems
Figure 1 3.: Behavioural pr0f i ie in VCFS (22q1 1 delet ion) during adolescence
85 1

IGENETtC COUNSELTNG
6.
4.
is a more struclured environment than the family environment,so less attention problems, but more withdrawn behaviourbecause i l is unfamil iar ground.
According to leachers, the anxious/depression syndrome signif i-cantly incfeases wilh age. During primary school, 10%0 0f theVCFS children score wi[hin the cl inical range (T-score > 70 or> g8th pefcenti le). In puberly, lhis incfeases [0 300/0 of the ado-lescents. A l0t 0f chi ldren with VCFS are often bull ied at school,even from primary schoolage on. Most chi ldren have poor socialski l ls and do not defend themselves. A possible consequence islhat [hese children become in t ime more social]y withdrawn andmore anxious. Hormonal changes during puberty as well as agene[ic predisposit ion to anxiely and wilhdrawal may play animportant role in this process. An important question is whelher[his increase of anxiety/depression is a precursor of psy-chopathology in laler l i fe.
Over the different developmen[al periods, there is no statist icalsignif icanl difference in behaviour be[ween boys and gir ls withVCFS.
There appears to be a relation between the type of problembe-haviour and mental level ( lQ > 70 vs. IQ < 70): in [he group ofintel lectually disabled children signif icantly m0re thought prob-lems are found. A statist ical ly signif icant (0.05 level) dif ferencein behaviour for .thoughl problems, is found between the 2groups. Parents and leachers reporb signif icantly more [houghtproblems in the group of chi ldren and adolescents with an intel-lectual disabil i ty ( lQ < 70). The f inding of signif icant higherscores 0n .thOughl problemsu in the group of chi]dren with anin[el]ectual disabil i ly/menml fe[ardation (FSIQ < 70) is notunexpecled. Because of l imited cognit ive and verbal abil i t ies,chi ldren and adolescents with intel lectuaydevelopmental dis-abil i t ies cannot communicate [heir feel ings and [houghts well.These children and youngslers have less coping abil i t ies, and,when faced with difficulties, they have limited abilities to reflec[,fa[ i0nalize, inlel lectualize, and f ind appropriate slrategies tomeeI their pOals.
From these observa[ ions, i [ is c lear that a g00d fol low-up withspecial interesl for lhe development of social ski l ls and self- imageof chi ldren with VCFS (22q11 delet ion) is indispensable. Parenls,teachers and professionals musI be a]ert for behavioural changes,and if necessary, the VCFS child should be referred to a child/ado-lescent psychiatf ist
Prospect ive, longitudinal and mult i -cenler s[udies with c0ntrOlgroups are needed to conf irm these prel iminary f indings. For the
186
A SwrtttN rr nt , Behavioural phenotype in VCFS I
gfoup 0f chi ldren with VCFS who afe mildly to moderately intel lec-tually disabled (FSIQ < 70), we need more appropriale insfumenlsand questionnaires in order to gel an accurate insight in the devel-Opmenl of lheir behaviour and temperamenl.
IGENERAL CONCLUSTON
lnformation 0n [he behavioural phenotype in VCf S (22q1 I dele-t ion) is of great rmp0fbance to cl in ic ians as an aid [0 lhe syndrOmediagnosis, buI even more t0 parents because i t of fers immensedirect pract ical value t0 the managemen[ 0f their chi ldren's behav,iours. Appropriate counsel ing as t0 what [0 expect, and betterinsight in the behaviour may lead to the development 0f real ist icways of coping wi[h their chi ld.
I REFERENCES
DEVRIENDT K., MOR'IIER C , VAN THIENEN MI N ,KEYM)LEN K, FRf,ryS J P The annual incidenceol DiGeolge/velocardi0facial syndrome. J Mr.;dCenetics, 1998, 35, 789-790
t"LlNT J , YULE, W: Behavioural phenotypes. /n:Child and AtlolescenL Psychiatry,3fd Edn RuttefM , Taylor R, Hersov L. (eds ) Oxford, : Blackwel lScienti f icr, 1 994, 666-687
GOLDBERC R, MOI'ZKIN B, MAR]ON R, SCAM-BLER P, SHPRINTZEN R: Velo-cardio-facjal syn-drome: A review ol 120 pat ients An J. Med.Cener, 1993, 45, 313-319
GOLDING-KUSHNER K., IVELLER G, SHPRINT-ZEN R: Velo-cardio-facial syndrome: Languageand Psychological Profiles J Craniof. GeneL Dev.Biol , 198tt,5, 259-266
LIEINEMAN-DE BOER J, VAN HAELST M.J COR-DIA-DE H,LAN M., BHEMER Ii:A: Behavior problemsand personali ty aspec[s of 40 chi ldren with velo-cardio-facial syndrome Genet Counsel., this tssue
K?K L , SOLMAN Z: Velocardiofacial syndrome:learning dif f icult , ies and interventi0n. J. MedGenelics, 1995, 32, 61 2-61 B
LIPSON A , YU]LLE D,, ANCEL M , TI]OMPSON P.,VANDERV))RD J, BECKENHAM B : Velocardiofa-cial (Shpr intzen) syndrome: an imporLant, syn-drome for lhe dysmorphologist, to rec0gnize JL,led Genet, , 1991 , 28,596-t i04,
NIcD]NALD-McGINN D., LAR?SSA D, G)LD-MUNTZ E , SULLIUAN K., EICHER P., GERDES M ,
7
MOSS E , WANG, SOLO'I C , SCHULTZ P., LYNCHD, BINGHAM P, KEENAN G , WEINZIMER S,M]NG ,I , DR]SCOLL D,, CI,ARK B, MARKOWII'ZR, COI]EN A, MOSHANG 7., PASQUARIELLO P,RANDALL P, EMANUEL 8,, ZACMI B: ThC22q11 2 deleLion: Screening, diagnosLic workup,and ou[come of resu]ts: fep0f[ 0n IB1 pat ientsGenetic Testine, 1998, / (2), 99-107
9. SCAMBLER P.. KELLY D . LINDSAY E: Velo-car-dio-facial syndrome assoclal,ed with chromOsome22 delet ions encompassing the DiCeofge locusLa ncet, 1992. 339. 1 1 3B-1 1 41
10 SHPRINTZEN R , GOLDBERG R LEWIN IVI : Ancw syndrome involv ing c lef t palale,0ardiacan0mal ies, l ,ypical facies and learning disabi l i t ies:velo-cardio-facial syndrome Aen Pahrc, 1978.1 5,56-62
11 SHPR|NTZEN R, GOLDBERG R , YOUNG D , WAL-F)RD L;The velo-cardio-facial syndrome: a c l in i -cal and genelic analysis Pediatxics. 1981. 67,167-172.
l2,SHPRINTZEN R, GOLDBERG R, GOI,DING.KUSI]NER K., MARION R.; Le[Ier [O the ediI,Or:Lale onseI psychosis in velo-cardio-facial syn-drome ,4m J. Med Genet. 1992, 42, 141-142
13 SWILLEN 4.. SOEMRN]AN D, MANDERS E,FRYNS , lP: Het velo-cardio-facrale syndroom vanShprin[zen: K]inische kenmerken en psycholo,gisch 0ntwikkel ingsprofiel van zes kinderenT)KK, 1993, 1 B( 2 ), 7 7 -9 |
87 1

IGENETIC COUNSELING
14 SWILLEN A., DEVRIENDT K., LEGIUS 8., 17. VERHULST E, UAN DEN ENDE J., K00T H.: Hand-EYSKENS 8., DUM)ULIN M., GEWILLIG M. leiding voor de CBCU4-|8 (Nedeilandse versie).FRYNS JP: Intelligence and psychosocial adjust- Afdeling Kinder- en Jeugdpsychialrie, Sophiament in velo-cardio-facial syndrome: a sludy 0f 37 Kinderziekenhuis, Academisch Ziekenhuis Rotter-children and adolescents wilh VCFS. J. Med. dan, Erasmus Universiteit, Rotterdam, 1996,Genet., 1997, 34(6), 453-458. 2g0pp
15 SWILLEN 4., DEVRIENDT K., VANTMPPEN G.,VOGELS A., ROMMEL ,ry., EYSKENS 8.,DUMOULIN M., GEWILLIG M., FRYNS JPj LeI[eTt0 ihe edi[or: Familial deletions in chromosome22q11: Lhe Leuven experience. Am. J. Med.Genet., 1998, 80. 263-264.
16. SWILLEN 4., VANDEPUNE 1,, CMCCO J., MAES8., GHESQUIERE P., DEVRIENDT K., FRYNS JP:Neuropsych'l'gicat and learning pr'file 0f chil-
ADDRESS FjRC1RRESP)NDENCE:
dren with velo-cardio-facial syndrome: Evidence Ann Swillen, Cenlre for Human Genetics, Depart-of a Nonverbal Learning Disabil ity? J. Learning ment0fClinicalGenelics,UniversityHospitalGas-,ls., submitted, 1998. thuisberg, Herestraat4g,3000 Leuven, Belgium.
IRRt* '
Related Documents











