The Basics of The Basics of Clinical Clinical Psychopharmacology Psychopharmacology : Pediatric : Pediatric Psychopharmacology Psychopharmacology Edition 2, Lecture 5 ASCP Model Curriculum for Medical Students

The Basics of Clinical Psychopharmacology: Pediatric Psychopharmacology Edition 2, Lecture 5 ASCP Model Curriculum for Medical Students.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Basics of Clinical The Basics of Clinical Psychopharmacology: Psychopharmacology: Pediatric Pediatric PsychopharmacologyPsychopharmacology
Edition 2, Lecture 5
ASCP Model Curriculumfor
Medical Students

AuthorsAuthors
Vishal Madaan, MD*Christopher J. Kratochvil, MD**
*University of Virginia Health System**University of Nebraska Medical Center

Objectivesfrom ADMSEP Psychiatry Learning
Objectives Taskforce, 2007
By completion of the By completion of the clerkship/medical school, the student clerkship/medical school, the student will be able to:will be able to:

ADMSEP Objectives—con’t
1. 1. Discuss the common, currently available psychotropic Discuss the common, currently available psychotropic medications with regard to clinical indications and medications with regard to clinical indications and contraindications, presumed mechanism of action and contraindications, presumed mechanism of action and relevant pharmacodynamics, common and serious relevant pharmacodynamics, common and serious adverse effects, pharmacokinetics, evidence for adverse effects, pharmacokinetics, evidence for efficacy, cost, risk of drug-drug interactions and drug-efficacy, cost, risk of drug-drug interactions and drug-disease interactions, and issues relevant to use in disease interactions, and issues relevant to use in special populations (e.g., pregnancy and lactation, special populations (e.g., pregnancy and lactation, childhood and adolescence, the elderly, persons using childhood and adolescence, the elderly, persons using herbal and over-the-counter treatments).herbal and over-the-counter treatments).
2. Propose selected psychotropic pharmacotherapy for 2. Propose selected psychotropic pharmacotherapy for designated patients and provide clinical reasoning that designated patients and provide clinical reasoning that includes discussion of factors influencing treatment includes discussion of factors influencing treatment selection (e.g.,patient-specific and drug-specific selection (e.g.,patient-specific and drug-specific variables, scientific evidence). variables, scientific evidence).

ADMSEP Objectives—con’t
3. Discuss the factors relevant to implementing, 3. Discuss the factors relevant to implementing, monitoring and discontinuing psychotropic monitoring and discontinuing psychotropic pharmacotherapy including drug dosing, treatment pharmacotherapy including drug dosing, treatment duration, and adherence, and make management duration, and adherence, and make management recommendations for dealing with an unsuccessful recommendations for dealing with an unsuccessful treatment trial (e.g., lack of efficacy, intolerability).treatment trial (e.g., lack of efficacy, intolerability).
4. Counsel patients about psychotropic 4. Counsel patients about psychotropic pharmacotherapy including risks and benefits of pharmacotherapy including risks and benefits of recommended treatment, treatment alternatives, recommended treatment, treatment alternatives, and no treatmentand no treatment
5. Identify and discuss resources to maintain an up-to-5. Identify and discuss resources to maintain an up-to-date knowledge of psychotropic pharmacotherapy date knowledge of psychotropic pharmacotherapy

ADMSEP Objectives—con’t
6. 6. Discuss special issues and concerns related to specific Discuss special issues and concerns related to specific psychotropic drug classes including metabolic, psychotropic drug classes including metabolic, hematologic, hepatic, etc.hematologic, hepatic, etc.

Objectives for MS II
At the end of this lecture, the student will:
Be able to articulate the basics of using psychotropics in children and adolescents
Be able to name the basic drugs used for children and adolescents and their clinical indications

Objectives for MS III
At the end of this lecture, the student will:
Be able to list appropriate dose ranges for at least 3 drugs used for children and adolescents
Be able to elucidate the major side effects seen in the use of the various drugs

Outline
Children are not small adults! Epidemiology 3 topics discussed:
ADHDChildhood DepressionAnxiety Disorders
Questions

Children are not small adults!
Young children may not be able to describe their internal states
Developmentally relevant vocabulary must be developed for working with children and families
Physiologically differentStart low, go slow, but higher doses may be
tolerated and required, on a mg/kg basis

Epidemiology of Common Child and Adolescent Psychiatric Disorders
ADHD: PrevalenceADHD is one of the most common mental
disorders in childhoodConservative estimates of 4-7% in grade
school children 4.4 million, 7.8%, of 4-17 y.o. U.S. children
have a history of ADHD by parent report (CDC, MMWR Weekly 54:842-847, 2005)

Pediatric Depression Epidemiology
0.3% of pre-schoolers2% of school-aged children5% of adolescents20-25% lifetime prevalence by the end of
adolescence (Kessler et al, Biological Psychiatry 2001;49:1002-1014.)
Distribution by SexApproximately equal before puberty2:1 female to male ratio after puberty

Child & Adolescent Anxiety Disorders
Among the most prevalent of child and adolescent psychiatric disorders 15.4% children in pediatric primary care sample
of 300 7-11y.o. met criteria for an anxiety disorder during a 1-year period (Benjamin et al 1990)
Of 792 eleven-year-olds, 3.5% separation anxiety d/o, 2.4% simple phobia, 2.9% overanxious d/o, 1% social phobia (Anderson et al 1987)

Autism Spectrum Disorders
Autistic Disorder Occurs in 4 out of 10,000 children Distributed equally among all socioeconomic levels Male to Female ratio 3:1 (Females affected more
severely, with greater neurological impairment) Asperger’s Syndrome
More common in boys than girls 10:1 Not associated with socioeconomic status or parental
education Prevalence was thought to be 0.6-4 per 10,000 A Swedish survey estimated 10-26 per 10,000

Attention-Deficit/Hyperactivity Disorder

ADHD: MTA Results
• Behavioral treatment alone • Community based treatment
All treatment arms found to be effective on an absolute basis
Nearly equally effective and superior to both:
Medication management alone
Medication management + behavioral treatment
(MTA Study Group, Arch Gen Psych, 1999)

Clinical Use of Stimulants
Safety and efficacy data beginning in the 1930’s, with their role in treating children well established by the 1970’s.
One of the best studied treatments in pediatric psychopharmacology
One of the most robust responses in pediatric psychopharmacology

Pharmacotherapy of ADHD
PsychostimulantsMethylphenidate (approved for > 6yrs)
Methylphenidate (in various formulations) Dexmethylphenidate
Amphetamine (approved for > 3yrs) Dextroamphetamine Mixed Amphetamine salts Lisdexamfetamine

Pharmacotherapy cont’d Non-stimulant Agents (Atomoxetine, Guanfacine
XR and Clonidine XR are FDA approved for ADHD) Atomoxetine (approved for 6yrs and up) Bupropion Desipramine Clonidine (IR and XR) Guanfacine (IR and XR)

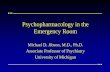
Drug release technology: “biphasic” release profile with combination of intermediate release (IR) and
extended release (ER) MPH beads
Protective membrane
20 mg
Protective membrane
Release controlmembrane
MPH
Core
ER beads
Core
MPH
IR beads
Time Release Capsules

Water
Water
During operation
Orifice/exit port
Drugcompartment #1
Drugcompartment #2
Pushcompartment
Drugovercoat
Rate-controlledmembrane
Before operation
Oros® Technology

Longer Acting Treatment Options:Stimulants
Methylphenidate Metadate CD®: Biphasic (30% immediate, 70% 3 hours
later) Ritalin LA®: Biphasic (50% immediate, 50% 4 hours later) Focalin® XR: Biphasic (50% immediate, 50% 4 hours later) Concerta®: Triphasic (overcoat of immediate release &
osmotic pump) Daytrana® patch: Transdermal patch applied to hip Quillivant XR TM: Extended release oral suspension
Amphetamine Extended release d,l-amphetamine (Adderall XR™):
biphasic (50% immediate, 50% 4 hours later) Lisdexamfetamine (Vyvanse)

Optimizing Response to Stimulants
In general, use extended-release formulations Give first dose as early as possible in AM Increase dose to ensure maximum benefit achieved Sculpt the dose: examples of potential combinations
Give immediate release TID Give Metadate CD or Ritalin LA BID Give IR early AM and Concerta/Adderall XR around
noon Give Concerta/Adderall XR early and IR around 6 PM
Greenhill LL, et al. J Am Acad Child Adolesc Psychiatry 2002;41(suppl 2):26S-49S
IR = 4 hrs Ritalin LA = 8 hrs
Metadate CD = 6-8 hrs Concerta/Adderall XR = 10-12 hrs

Adverse Effects of Stimulants
Appetite suppression Insomnia Tics Growth suppression Cardiovascular Rare: psychotic symptoms, mania,
seizures

Atomoxetine (Strattera™) Selective noradrenergic reuptake inhibitor FDA approved for age 6 and up in November,
2002 Dosed by body weight, titrated based on
tolerability and response Initiated at approximately 0.5mg/kg/day and
gradually titrated to target dose (1.2 mg/kg/day) to improve tolerability
FDA approved maximum 1.4mg/kg/day Delayed onset of action

Indications for Atomoxetine
FDA approved for the treatment of children 6 years of age and older, adolescents, and adults
Low substance abuse liability, so often seen as an option where there is a high risk of substance abuse or diversion
May be useful for those with comorbid anxiety or comorbid Tourette’s

Adverse Effects of Atomoxetine & Management
Dyspepsia Sedation Irritability Hepatic Suicidality

Aim- To test the efficacy and tolerability of methylphenidate for preschool children
N= 165 3-5 years old 12 weeks Randomized, placebo-controlled. Cross-over with
4 fixed doses plus PBO (1 week each), followed by a 4-week parallel group, and a 10-month naturalistic maintenance phase.
Preschoolers with ADHD Treatment Study (PATS)
Greenhill, Kollins, Abikoff et al, J Am Acad Child Adolesc Psychiatry, 2006, 45(11):1284-1293

PATS <10% responded to parent training alone Significant improvements noted with
methylphenidate 2.5mg TID, 5mg TID, and 7.5mg TID. Mean optimal dose 14.2 mg/d
Only 21% on best-dose MPH and 13% on PBO met remission criteria
Emotional outbursts, difficulty falling asleep, repetitive behaviors/thoughts, appetite decrease, and irritability were most frequently reported adverse effects
At 1 year mean gains in growth -1.38cm & -1.3 kg below expected

Depression

DSM-IV-TR Diagnostic Criteria Five or more symptoms present for 2
weeks (every day or nearly every day) At least one symptom is
depressed/irritable mood or anhedonia Symptoms not due to general medical
conditions or substances Significant distress or impairment in
functioning

DSM-IV-TR Diagnostic Criteria Depressed mood- or irritability in
children/adolescents Sleep- increased sleep or insomnia Interest- markedly diminished interest/pleasure Guilt- feeling worthless or inappropriate guilt Energy- fatigue or loss of energy Concentration- diminished ability to think/concentrate Appetite- sig. wt. loss or gain (e.g.. 5%), diminished
appetite, in kids failure to make expected gains Psychomotor- physically slowed or agitated Suicide- thoughts, attempts, or recurrent thoughts of
death

Clinical Presentation Young children
Physical ComplaintsDepressed or Irritable MoodWithdrawn & Sad Appearance
AdolescentsGrouchy & Sulky commonly RestlessWithdrawnPhysically Slowed Lack of enjoyment in activities

Pediatric Depression
Fluoxetine and Escitalopram are the only antidepressants FDA approved for the treatment of depression in children or adolescents

Treatment Strategies TADS: Treatment of Adolescents with
Depression Study Examined effectiveness of fluoxetine,
CBT, combination, and placebo NIMH sponsored; 12 sites nationally
Stage I: Acute treatment for 12 weeksStage II: Consolidation for 6 weeksStage III: Maintenance for 18 weeksStage IV: One year open follow-up

TADS Treatment Response with acute treatment:
Combination: 71%; Fluoxetine: 61%
CBT: 43%; Placebo: 35%
Conclusions: Combination of fluoxetine & CBT is most
effective. Fluoxetine alone is effective, but not as
effective as combination

Suicidality and Antidepressants Meta-analysis from 24 antidepressant
studies conducted in pediatric patients (Hammad 2004)
4% had suicidal thoughts/behaviors on medication, 2% on placebo; no completed suicides
Black box warning for antidepressant use in children and adolescents

Suicidality and Antidepressants 20% decline in pediatric antidepressant
use. Olfson, 2003: Inverse relationship between
regional change in antidepressant use and suicide rates (1% ↑ in antidepressant use associated with a ↓ of 0.23 suicides/100,000 adolescents/year.
CDC, Feb 2007: Child & adolescent suicide rate in 2004 rose for the first time in more that a decade (18%)

The Treatment of Resistant Depression in Adolescents Study (TORDIA) Aim: to compare the effectiveness of an alternative
antidepressants (SSRIs or venlafaxine), alone and in combination with CBT, in adolescents with depression who failed an adequate initial SSRI trial
12 weeks of Switch to 2nd, different SSRI (paroxetine, citalopram, or fluoxetine) Switch to a different SSRI + CBT Switch to venlafaxine Switch to venlafaxine + CBT
N= 326 12-18 years old 12 weeks of acute treatment followed by a 12 week
continuation Brent, Emslie, Clark et al, JAMA 2008, 299:901-913.

TORDIA The combination of CBT and a switch to another
antidepressant resulted in a higher rate of clinical response (54.8%) than did a medication switch alone (40.5%)
There was no difference in response rate between venlafaxine and a second SSRI, although venlafaxine was associated with an increase in diastolic blood pressure & pulse and more skin problems than SSRI

Pediatric Anxiety Disorders

Treatment Strategy for Anxiety Disorders
Clinical management of anxiety disorders requires 3 distinct areas of dysfunction be addressed the primary symptoms: Hyperarousal, restlessness,
anxiety, obsessions, compulsions the anticipatory anxieties—may respond to
psychotherapeutic interventions behavioral disturbances in patient or environment as a
result of the primary symptoms or anticipatory anxieties
Pharmacological interventions are clearly indicated, but often need to be combined with psychotherapeutic interventions

Child and Adolescent Anxiety Multimodal Study (CAMS) Aim: to compare sertraline and CBT,
alone and in combination, to PBO. N=488 subjects with separation anxiety
disorder, generalized anxiety disorder, or social phobia
Age: 7-17 years Duration- 12-week trial
Walkup et al, NEJM, 359(26): 2753-2766: 2008

CAMS
All 3 active treatments demonstrated efficacy
81% response to COMB, 61% CBT, 56% sertraline, 26% PBO
COMB > CBT=Sertraline > PBO

Research Units of Pediatric Psychopharmacology (RUPP) Fluvoxamine Study
Fluvoxamine (RUPP studies 2001, 2002) 50-300 mg, 8 wks, n=128mg, 8 wks, n=128 in 6-17 yrs
Generalized Anxiety Disorder, Separation Anxiety Disorder, or Social Phobia persisting after 3 wks supportive psychotherapyResponse Rates= FLVX 76% v 29% placebo Adverse effects= stomachache, motor
activation 28% v 12% placebo

6 mo open label extension-94% continued remission
Fluvox non-responders-> Fluoxetine (n=14) 20-40 mg 71% response by clinician rating and PARS
Higher level of depression, SP and severity of illness- less drug efficacy;
ES=1.1 largely because of low placebo response
Take home message: If no response from first SSRI, try a second one
Research Units of Pediatric Psychopharmacology (RUPP) Fluvoxamine Study

The Pediatric Obsessive-Compulsive Disorder Treatment Study (POTS) Aim- to test efficacy of sertraline and CBT, alone
and in combination in children with OCD, compared to PBO
OCD in Children and Adolescents: A Cognitive Behavioral Approach, JS March & K Mulle, Guilford Press
N= 112 7-17 years old 12 weeks
The Pediatric OCD Treatment Study (POTS) Team, JAMA 2004 292(16): pp 1969-76

Pediatric OCD Treatment Study (POTS) Compared efficacy of 4 different treatment options:
Sertraline alone, sertraline +CBT, CBT alone & placebo alone; n=112; 12 weeks
Randomized parallel groups Entry criteria CYBOCS=16; Mean of 24.6 with only ADHD
meds allowed Sertraline- Upward titration from 25→200 mg/d over 6
weeks Outcome measure of remission: CYBOCS <10

POTS: Outcome Mean daily dose of sertraline
With combined treatment:133 mg/day Sertraline alone: 176 mg/day
Effect sizes CBT: 0.97 Sertaline alone: 0.67 Combined treatment:1.4
Remission rates (CYBOCS=10) for combined 53.6%; CBT alone 39.3%; sertraline 21.4% and placebo 3.6%

POTS
CBT alone, sertraline alone, COMB all superior to PBO
COMB was most effective, beat sertraline alone & CBT alone
CONCLUSION: children & adolescents with OCD should begin treatment with the combination of CBT plus an SSRI or CBT alone

FDA Atypical Antipsychotic Indications in Children and Adolescents
Bipolar Disorder
(10-17 yo)
Schizophrenia
(13-17 yo)
Irritability in Autism
Clozapine
Olanzapine X (13-17 yo) X
Risperidone X X X (5-16 yo)
Quetiapine X X
Ziprasidone
Aripiprazole X X X (6-17 yo)

Discussion Questions Question 1
a. Fluoxetine
b. Sertraline
c. Fluvoxamine
d. Paroxetine
e. Citalopram
1. Which of the following antidepressants have been FDA approved for the treatment of major depressive disorder (MDD) in youth?

Question 2
2. Which of the following has been associated with the best outcomes in adolescents with depression?
a. Fluoxetine alone
b. CBT
c. Paroxetine + CBT
d. Fluoxetine + CBT

Question 3
3. Which non-stimulant is FDA approved for the treatment of ADHD?
a. Atomoxetine
b. Imipramine
c. Bupropion
d. Risperidone
e. Aripiprazole

Question 4
4. Which stimulant medication has the largest amount of data pertaining to safety & efficacy in preschool children?
a. Amphetamine
b. D-amphetamine
c. Atomoxetine
d. Methylphenidate
e. D-methylphenidate

Answers
1. A
2. D
3. A
4. D

End of Lecture
Related Documents