The McCaughey Centre VicHealth Centre for the Promotion of Mental Health and Community Wellbeing Policy Signpost # 2 Universities Working with and for Communities: Strategies for Collaborative Community Research and Knowledge Exchange Sarah MacLean, Deborah Warr and Priscilla Pyett Knowledge for Common Good July 2008 The McCaughey Centre: VicHealth Centre for the Promotion of Mental Health and Community Wellbeing, Melbourne School of Population Health, The University of Melbourne

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The McCaughey CentreVicHealth Centre for the Promotion of Mental Health and Community Wellbeing
Policy Signpost #2
Universities Working with and for Communities: Strategies for Collaborative Community Research and Knowledge Exchange
Sarah MacLean, Deborah Warr and Priscilla Pyett
Knowledge forCommon Good
July 2008
Published by The McCaughey Centre: VicHealth Centre for the Promotion of Mental Health and Community WellbeingMelbounre School of Population Health, The University of Melbourne, Level 5, 207 Bouverie Street, Victoria 3010 AustraliaTelephone: +61 (3) 8344 9101 Facsimile: +61 (3) 9348 2832
http://www.mccaugheycentre.unimelb.edu.au
© McCaughey Centre 2008
Policy Signpost #1Community Wellbeing in an Unwell World: Trends, Challenges and Opportunitieshttp://www.mccaugheycentre.unimelb.edu.au/pdf_library/Policy_signpost_1.pdf
ISBN 978-0-9804620-3-6
The McCaughey Centre: VicHealth Centre for the Promotion of Mental Health and Community Wellbeing,Melbourne School of Population Health,The University of Melbourne
The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
1
The authors
Sarah MacLean1Deborah Warr1Priscilla Pyett2
1 McCaughey Centre, School of Population Health, University of Melbourne2 Onemda VicHealth Koori Health Unit, School of Population Health, University of Melbourne
Abbreviated terms
ARC Australian Research CouncilARCSHS Australian Research Centre for Sex, Health and SocietyCP community partnerCPR collaborative participatory researchCLO community liaison officerDW Dr Deborah WarrDEST Commonwealth Department of Education, Science and Training DHS Department of Human ServicesGARDS Gippsland Asbestos Related Diseases SupportMOU memorandum of understandingRA research assistantRQF Research Quality FrameworkTLM Associate Professor Tony LaMontagneNHMRC National Health and Medical Research CouncilPP Dr Priscilla PyettVACCHO Victorian Aboriginal Community Controlled Health Organisation
Acknowledgments
This report draws on opinions and experiences of many people involved in research in Victoria. We would like to thank all the interview participants for their generosity in sharing their experiences of research collaboration with us. Special thanks to: Angela Clarke, Vicki Hamilton, Lynne Hillier, Anne Kavanagh, Tony LaMontagne, Maureen Leahy, Kellie Loughron, Shelley Mallett, Anne Mitchell, John Parker, Dorothy Roberts, Ben Rossiter, Marie Smith, Paul Stewart, Amanda Tattam, Deb Vallance, Peter Waples-Crowe and Sue West.
The project was funded by a small grant from the University of Melbourne’s Faculty of Medicine, Dentistry and Health Sciences. Dr Warr and Dr Pyett are funded by VicHealth Public Health Fellowships. Additional funding was contributed by the McCaughey Centre: VicHealth Centre for the Promotion of Mental Health and Community Wellbeing.
Knowledge forCommon Good
Knowledge forCommon Good
Contents
2
Summary 3Recommendations 41. Introduction 6
Collaborative participatory research 6Knowledge exchange 7Research at universities 8Summary 9
2. Research method 10Participants 10Interviews and thematic analysis 10Case studies 11Research limitations 11
3. Case studies of models for community engagement and research exchange 123.1 Centre-based models 12The Australian Research Centre for Sex, Health and Society 12Research with same-sex attracted youth 13Key Centre for Women’s Health in Society 14
Project i 14Onemda VicHealth Koori Health Unit 15
Community-based collaborative research at VACCHO 173.2 Research project models 18Developing a social and public health response to asbestos disease in the Latrobe Valley 18Social processes for health: understanding the links between place and social connection 19Trajectories of identity for injecting drug users 20
4. Strategies for community engagement and knowledge exchange 22Initiating projects 22Finding a community partner and spending time in the community 23Establishing an advisory or reference group 24Developing memoranda of understanding or partnership agreements 25Employing community liaison staff 26Community reports, newsletters, presentations and seminars 27Websites and media 28Challenges encountered by researchers 29
5. Challenges for effective CPR 29Challenges encountered by community partners 32Challenges encountered in relation to employing community liaison staff 33
6. Suggestions for supporting CPR 36Sympathetic approaches by researchers 36Dedicated CPR funding 37Measuring CPR as academic activity and output 39Supportive faculty and centre governance 40Encouraging knowledge exchange 40Enhancing capacity for community liaison in universities 42
7. Conclusions 45References 47Appendix 1 Template for a project agreemen 51

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
While aimed primarily at an audience within the University of Melbourne, it is hoped that the information and recommendations presented here will be of interest to a wider audience.
3
Summary
This is a study of university-based collaborative and participatory strategies for health and welfare research conducted with and for communities experiencing various forms of disadvantage. It draws on interviews with 23 people involved in collaborative participatory research (CPR) in Victoria. Of these, seven were researchers, seven were employed as community liaison or community development officers within universities and nine were community members or representatives. Three research centres and three additional research project models are described as case studies.
Various mechanisms for community engagement and knowledge exchange were described by research participants. These included identifying community partners, establishing reference or advisory groups, developing project agreements or memoranda of understanding and employing community liaison staff. Knowledge exchange strategies included community reports, presentations and seminars, websites and media promotions.
Researchers involved in the study mentioned four main difficulties in conducting CPR and ensuring knowledge exchange, which were:
n the sensitivities of working in communities;n time-requirements and diverse non-academic tasks involved; n funding shortfalls; andn a perception that their careers had suffered as a result of
missed publication opportunity.
Community partners identified a different set of challenges, including:
n unequal power within the research relationship;n concern that their involvement might be used only to legitimate
research; andn having to fit research tasks into busy schedules.
Some of the challenges for community liaison officers and those who employed them were described as:
n lack of clarity about the role;n managing conflicting demands of researchers and
communities; and n career structure, performance assessment and sense of value.
This report suggests various means of enhancing CPR including sympathetic approaches by researchers, provision of dedicated funding for CPR, measuring CPR as academic activity, supportive governance, and enhancing capacity for knowledge exchange and community liaison. While aimed primarily at an audience within the University of Melbourne, it is hoped that the information and recommendations presented here will be of interest to a wider audience.
Knowledge forCommon Good
4
Collaborative participatory research is a methodological approach well suited to studies involving disadvantaged communities. Collaborative and participatory research with communities experiencing disadvantage entails diverse tasks and novel approaches to knowledge exchange which should be recognised as legitimate academic work and resourced by universities and research funding bodies. The following processes are recommended to enable and support collaborative and participatory approaches to research:
n Researchers undertaking community-engaged research should be prepared to invest time in building relationships and should seek ways to ensure that participants benefit from involvement.
n Advisory or reference groups should be established where real input to a research project is desired by the community and respected by the researcher.
n Memoranda of understanding or partnership agreements are recommended to clarify roles and expectations of all research partners. Research centres should develop template documents for adaptation by researchers (see Appendix 1).
n Researchers should consider engaging communities in the initial planning of projects as a means of optimising opportunities for input and knowledge exchange.
n Research negotiations should include consideration of appropriate and respectful ways of acknowledging community partners, participants and co-authors and, with the approval of community partners, the placing of relevant logos on reports and other publications.
n Research proposals should include funding to reimburse community participants who are not undertaking their role as part of paid employment.
n Funding bodies should consider establishing specific CPR funding programs to include the time requirements for research establishment, implementation and dissemination and to reimburse communities for their participation.
n The University of Melbourne should consider establishing research fellowships specifically for collaborative and participatory research.
Knowledge exchange is a critical aspect of collaborative and participatory research. The following recommendations suggest ways to strengthen the reach and impact of research outcomes:
n The University of Melbourne should adopt the term ‘knowledge exchange’ in preference to ‘knowledge transfer’ to convey the importance of respecting the knowledge and understanding that both university and community partners bring to research.
n Research projects addressing health and social disadvantage should include plans for knowledge exchange involving communities and community representatives.
n Universities should ensure that support staff with electronic
Recommendations
The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
5
media skills are available to assist researchers to profile their work and to regularly update web pages.
n Ongoing positions at University or Centre level would facilitate and support more effective community engagement and knowledge exchange.
The following recommendations support collaborative research activities to be recognised as academic work:
n Academic performance appraisal tools utilised by universities and funding bodies should include metrics for community engagement activities related to negotiating and conducting partnership research and participating in knowledge exchange.
n The University of Melbourne should advocate that community reports and other forms of knowledge exchange be counted as academic outputs under the new Excellence in Research for Australia system and that measures be developed to assess the impact of CPR research with disadvantaged communities.
n Research centres should develop flexible administrative systems to facilitate community engagement in research.
n University award schemes should continue to recognise and encourage innovative forms of knowledge exchange.
Community liaison is critical for collaborative participatory research and requires a broad range of highly-developed communication skills. Community liaison officers require a clear role and sense of value within universities to work effectively. The following recommendations would assist in achieving this:
n Skilled community liaison work requires funding at university, centre or project level.
n Research funding bodies should recognise the need for community liaison support in projects that entail extensive community involvement.
n A network of community liaison staff and researchers who work with them should be established at the University of Melbourne to clarify the role, develop performance indicators and explore options for career development.

Knowledge forCommon Good
1. Introduction
6
The process of making research findings available to those who might use them has become known as knowledge transfer, research transfer, dissemination, diffusion or, more reciprocally, as knowledge exchange.
This is a small exploratory study of strategies currently used within five Victorian university research centres to promote the engagement of communities in research and to share research findings with those communities. Universities engage with diverse communities, from industry to policy and professional groups. We focus here on health and welfare research involving communities that experience disadvantage or disenfranchisement; for instance, Indigenous communities, same-sex attracted young people, homeless young people or people living in areas of socio-economic marginality.
Various methodologies for research involving partnerships between researchers and communities are described in the literature, most notably collaborative participatory research (CPR) or community-based participatory research, where projects are located and managed outside universities. We use the term CPR to refer to any methodology where collaboration and participation of communities or their representatives (beyond simply being involved as research subjects) is critical to the conduct of the project and where the aim of research is to achieve some benefit for communities concerned. The process of making research findings available to those who might use them has become known as knowledge transfer, research transfer, dissemination, diffusion or, more reciprocally, as knowledge exchange. Knowledge uptake or utilisation refers to the employment of research findings in policy or practice. In this report we use the term ‘knowledge exchange’ because it conveys the importance of respecting the understandings that both university and community partners bring to research.
This report begins by introducing some considerations for CPR and knowledge exchange, and then provides a brief overview of the context of health research at universities. Section 2 outlines the research method. Section 3 provides descriptive case studies of three centre-based and three CPR project models. Sections 4, 5 and 6 comprise discussion of mechanisms to facilitate community engagement and research exchange, impediments or difficulties experienced by researchers, community liaison officers (CLOs) and community representatives engaged in CPR, and suggestions about how CPR could be better supported at universities. A brief conclusion is at Section 7.
Collaborative participatory research The hallmark of collaborative and participatory approaches to research is an insistence on the importance of research subjects’ input to research (Pyett, 2002). Nonetheless, actual community involvement in collaborative research varies significantly. The present research is concerned with models that include some significant component of community participation, often involving individuals acting as representatives of community groups and advocacy bodies. These people are unlikely to be involved in all research components and very often have an advisory and linkage role. Australian health research is primarily investigator-driven and structured community involvement is relatively rare (National Health and Medical Research

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
7
Community-university research partnerships present an opportunity to involve disadvantaged communities in developing strategies to address social and health inequality and facilitate knowledge exchange.
Council & Consumers’ Health Forum of Australia, 2004; Street, Baum, & Anderson, 2007).
CPR is believed to be particularly suited to contexts of social and economic disadvantage. Proponents of CPR have argued that it is an ethically sound approach which may empower, rather than simply provide advice to communities (Flicker & Savan, 2006; Israel, Schultz, & Parker, 1998; Pyett, 2002; Sapienza, Corbie-Smith, Keim, & Fleischman, 2007). Methodological advantages of collaborative research involving communities can include ensuring the relevance of research and the appropriateness of measurement tools (Viswnanathan et al., 2004). Collaborative approaches may be a useful way of accessing populations that are marginalised and hard to reach. These approaches have also been used with Indigenous and other marginalised communities who have previously had negative experiences of involvement in research (Cochran et al., 2007; Pyett, 2002). Community-university research partnerships present an opportunity to involve disadvantaged communities in developing strategies to address social and health inequality and facilitate knowledge exchange. A review of collaborative research to prevent HIV infection found that such an approach ‘often facilitates technology transfer and implementation of interventions and can result in improved methodology, enhanced quality of data, and increased effectiveness of data dissemination’ (Roussel, Fan, & Fulmer, 2002: 3).
A substantial and growing literature considers both collaborative research and knowledge dissemination. Much of the writing on CPR emerges from North America, particularly Canada. Nonetheless, specific models and practices for engaging disadvantaged communities and knowledge exchange are rarely documented and research centre staff lack accessible information about the merits and weaknesses of available strategies. The National Health and Medical Research Council (NHMRC) has provided a model framework and resources pack for researchers and community partners engaged in participatory projects (National Health and Medical Research Council, 2004; National Health and Medical Research Council & Consumers’ Health Forum of Australia, 2004) as well as the Keeping Research on Track resource kit specifically developed for Indigenous communities engaging with research (National Health and Medical Research Council, 2005).
Knowledge exchangeIt is generally argued that active strategies are essential to effective knowledge transfer and knowledge exchange, regardless of the audience (Gano, Crowley, & Guston, 2007; Mitchell & Walsh, 2003; Nutley, Walter, & Davies, 2007). Huberman (1994) has proposed that ‘sustained interactivity’ between researchers and potential users of research or their representatives is the key to ensuring research relevance and maximising research utilisation. Parkin (2004) argues that dissemination is facilitated by consulting and involving potential research users at the planning and development stage of a project.

Knowledge forCommon Good
8
University researchers internationally are under pressure to demonstrate that their research has ‘real world’ impact.
The involvement of relevant communities as collaborative partners in the development and implementation of research projects is therefore likely also to support subsequent knowledge exchange.
The literature considers knowledge transfer and knowledge exchange involving three groups: policy makers (Jacobs & Barnett, 2000; Nutley et al., 2007), practitioners and clinicians (Lang, Wyer, & Haynes, 2007), and communities (Matthews, Frommer, Tjhin, & Rubin, 2001). Literature which focuses on knowledge exchange with disadvantaged communities tends to provide general principles on how to best to approach and establish collaboration rather than detailing specific strategies or models. The Cooperative Research Centre for Aboriginal Health has, however, developed a set of tools and resources to assist researchers to plan and conduct research transfer (see http://www.crcah.org.au/research/researchtransfer.html#RT_tools).
Research at universitiesContradictory forces within research funding both support and hinder community engagement in research. On the positive side is the increasing value ascribed to ‘evidence-based’ health and welfare policy and practice (Nutley et al., 2007). University researchers internationally are under pressure to demonstrate that their research has ‘real world’ impact. In the context of public health research this means that research which demonstrably influences health and well-being policy or practice, or even better, contributes to improved health outcomes, is considered important and fundable.
Funding bodies in Australia emphasise the importance of building structures to ensure that research evidence translates to improvements in policy and practice and community participation is seen as a way to enhance the relevance, conduct and dissemination of research (Anderson, 2006). Both the NHMRC and the Australian Research Council (ARC) funding guidelines indicate that projects with clear national benefit are preferred. Since 2005 NHMRC grant applications require researchers to stipulate and report on how consumer or community participation will be incorporated into their projects (National Health and Medical Research Centre & Consumers’ Health Forum of Australia, 2004)
The importance of demonstrating the relevance of research has been recognised by universities (Winter, Wiseman, & Muirhead, 2005). The University of Melbourne’s ‘Growing Esteem’ strategy identifies a new focus on knowledge transfer to complement its traditional research and teaching activities. As part of its commitment to making research findings available to people and institutions that might put them to use, the university undertakes to ‘serve public ends’ and ‘to deepen the relevance and impact of its academic mission’ (The University of Melbourne, 2005: 7).
Yet despite encouragement to undertake work of social value and incorporate community participation, the capacity to undertake CPR depends on securing funding to do so and on appropriate recognition

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
9
Despite the acknowledged value of community participation, it can be difficult for researchers to secure funding for collaborative participatory research. Public health funding bodies are often unfamiliar with collaborative participatory research and prefer to provide resources for studies using more established scientific methods.
of CPR as academic work. Funding allocated to universities is increasingly tied to performance. Australian universities have two principal funding sources. The Commonwealth Government allocates research funding to universities through various schemes and on the basis of three measures: higher degree by research completions, nationally competitive grants and recognised publications (Butler, 2003). As we shall discuss through this report, decisions about what kinds of publications may be counted as academic output through performance metrics have important implications for the viability of CPR within universities.
Nationally competitive research grants are another important source of university funding and academic prestige. Academics develop research proposals for submission to bodies such as the ARC and NHMRC. Despite the acknowledged value of community participation, it can be difficult for researchers to secure funding for CPR. Public health funding bodies are often unfamiliar with CPR and prefer to provide resources for studies using more established scientific methods (Israel et al., 1998). Time-limited competitive grant funding of research projects also makes sustained community engagement problematic (Winter et al., 2005). Funding bodies, furthermore, encourage research involving corporate or industry partners which are required to contribute funding or in-kind resources. Researchers thus have less incentive to work with local or disadvantaged communities which cannot contribute financially to research projects.
Universities operate in an environment of competition, commercialisation and scarce research funding (Pick, 2006). As others have summarised the problem: ‘there is a risk that the educational, social and economic benefits of community engagement will be undermined by higher education policies which emphasise competitiveness, commercialisation and cutbacks’ (Winter et al., 2005: 6).
SummaryIncorporating CPR processes in research involving disenfranchised communities promises to maximise the value of research by improving the quality of data that are collected and the uptake of associated interventions, and by facilitating the dissemination of findings and other outcomes. Involving communities in the processes of research is also endorsed by key funding bodies. There remain, however, many barriers for adopting CPR and the difficulties are heightened when potential research partners are disenfranchised communities. Despite the challenges, some researchers are incorporating CPR approaches in their research projects. This study discusses these efforts and provides insights into the difficulties and benefits of CPR approaches across a range of research projects concerned with aspects of health and health-related issues.
Knowledge forCommon Good
2. Research method
10
The aim of the study was to explore strategies currently employed by university researchers to engage with communities experiencing various forms of disadvantage, in order to conduct collaborative and participatory health research projects.
This project uses a qualitative approach and a critical reflexive methodology (Fook, 1996; Hertz, 1997; Reason, 1994). Two of the investigators are included as key informants and their experiences as community researchers have informed the analysis. The aim of the study was to explore strategies currently employed by university researchers to engage with communities experiencing various forms of disadvantage, in order to conduct collaborative and participatory health research projects. The methods involved a literature review, key informant interviews, and a review of information available on the relevant university websites and in annual reports. Ethical approval was obtained from the School of Population Health Human Research Ethics Committee. Participants provided informed consent and were offered the opportunity to review drafts of sections of the report referring to their contribution prior to its being made public.
ParticipantsThe starting points for sample selection were three university research centres known by the investigators to engage in collaborative research with disadvantaged communities. Key researchers or community liaison staff in each of these centres were contacted and all agreed to participate in the project. Representatives of community organisations who had engaged in research with each of the three centres were subsequently recruited via referrals from these researchers and CLOs.
Twenty-three participants took part in research interviews comprising:n seven research staff;n seven community liaison, community development or project
staff employed in research centres (these staff are all referred to as CLOs in the report); andn nine community members or employees of community
agencies (referred to as community participants or CPs in the report).
Interviews and thematic analysisInterviews were of 30-70 minutes duration and utilised a conversational approach (Bourdieu, 1996). Interviews were focused around the following questions:
n How do university researchers engage with communities?n What processes exist for engagement and collaboration? n What have been the outcomes of collaborative research?n What are some of the difficulties encountered in collaborative
research?n What measures support effective collaborative research?
Interviews were conducted either in person or on the phone, depending on the preference of the interviewee. Most interviews were tape-recorded (with permission from participants) and subsequently transcribed. The researcher took detailed notes during those interviews that were not recorded. All interview transcripts and research notes were coded using the qualitative software package

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
11
In investigating case studies we aimed to identify what Jack (2005) has characterised as ‘promising approaches’ to a social issue, in this instance the strategies developed by university-based researchers and university research centres to engage disadvantaged communities in research and knowledge exchange.
NVivo. A thematic analysis (Huberman & Miles, 1994) was used to structure the coding and the report findings. Data from all interviews were analysed and integrated into the findings and discussion, although not all the projects described by participants were included as individual case studies.
Case studies Three research centre models and three individual research projects were selected as case studies. Case studies were not chosen to be representative of health or social research practice in Victoria but rather because they would offer a range of insights into both the practice of CPR and the contexts in which research is conducted (Stake, 1998). In investigating case studies we aimed to identify what Jack (2005) has characterised as ‘promising approaches’ to a social issue, in this instance the strategies developed by university-based researchers and university research centres to engage disadvantaged communities in research and knowledge exchange.
Research limitationsThis is a small exploratory study. The majority of research centre models and projects involved are based at the University of Melbourne. Community representatives interviewed were referred to the study by researchers or CLOs in the respective centres, with the obvious limitation that selection bias may have produced only assessments of collaborations with universities that were generally positive. All participants were advised that the research was not intended to evaluate either their work context or the individual research projects; rather, the research goal was to identify the strengths of a range of approaches to university-based CPR that are actually in operation in Victoria at the present time and difficulties or impediments to conducting CPR in a university context.

Knowledge forCommon Good
3. Case studies of models for community engagement and research exchange
12
Researchers maintain responsibility for disseminating findings in academic contexts through journal articles, teaching or conference papers. Community liaison officers, on the other hand, disseminate findings to research participants and relevant communities including policy makers, clinicians and educators, and populations of people from whom participants are drawn.
The following section briefly outlines research projects which have entailed significant collaboration between university-based researchers and disadvantaged communities. Models described here are grouped as centre-based (where CLOs are employed within a centre to work with researchers) and project based (where researchers undertake community liaison either on their own or in conjunction with a project or research officer employed specifically on the project concerned).
3.1 Centre-based modelsThe Australian Research Centre for Sex, Health and SocietyThe Australian Research Centre for Sex, Health and Society (ARCSHS) was established in 1992 within the Faculty of Health Sciences at La Trobe University in Victoria. ARCSHS conducts multidisciplinary research on sexual health. The applied nature and sensitivity of this research made the need for mechanisms to engage those who might put the research into practice apparent from the outset. From the time of ARCSHS’s establishment one CLO was employed from core funding. Since then, a number of other CLO staff have been employed through specific research project budgets (Mitchell & Walsh, 2003). CLOs were selected for their expertise in community development, health promotion and adult education. Six to eight (mainly part-time) staff were employed in CLO roles at the Centre in late 2007.
The role of CLOs at the Centre has evolved over time. Initially they focused on building relationships with communities and potential research users, and consulting with communities to inform the Centre’s research agenda. Community liaison staff also consulted with research users (such as policy makers) prior to the commencement of a project to ensure research would meet their needs, and facilitated the recruitment, training and support of community representatives as research assistants and co-researchers. As ARCSHS’s research profile developed, the CLOs’ role assumed a new focus on disseminating research outcomes. Researchers maintain responsibility for disseminating findings in academic contexts through journal articles, teaching or conference papers. CLOs, on the other hand, disseminate findings to research participants and relevant communities including policy makers, clinicians and educators, and populations of people from whom participants are drawn. This is done through writing community reports and articles for industry magazines, holding workshops and discussions, and developing booklets or comics (see Hillier, Mitchell, Besley, & Lavin, n.d.; Walsh, 1998). CLO activities also include liaising with media, commenting on government policies and initiating meetings with bureaucrats to discuss the significance and potential uses of research (Mitchell & Walsh, 2003). CLO activities are funded through research budgets; however, staff have also obtained funding specifically to produce evidence-based educational or resource materials (Mitchell & Walsh, 2003).
Staff at ARCSHS argue that the presence of CLOs has altered the culture of their organisation:

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
13
‘I would be very surprised if there was a researcher at ARCSHS who doesn’t recognise the value of having that sort of community work happening hand-in-hand beside them ...’
I would say now that I would be very surprised if there was a researcher at ARCSHS who doesn’t recognise the value of having that sort of community work happening hand-in-hand beside them and most of them now do their own community work because they’ve been taught a particular style of operation, and they’ve embedded it. (CLO)
Over the last decade and a half ARCSHS projects have engaged with a wide range of communities including: sex workers, homeless young people, teenage mothers, people with STIs (sexually transmissible infections), people living with HIV/AIDS and same-sex attracted youth.
Research with same-sex attracted youthARCSHS has conducted a series of research and research transfer projects concerned with understanding and addressing same-sex attracted young people’s experiences at school, much of it led by Dr Lynne Hillier. Major national surveys were undertaken in 1998 and 2004 (Hillier et al., 1998; Hillier, Turner, & Mitchell, 2005). Same-sex attracted young people are often hidden and hard to access. By targeting these young people as research participants, researchers feared they might inadvertently divulge young people’s sexual preference to their parents. As a project team member said ‘there’s that additional layer with them that their safety depends on us not exposing them’. Rather than attempting to access this group directly, ARCSHS used a range of advertising strategies alerting young people who were sexually attracted to people of their own sex, or to both sexes, to the study. Participants then completed a survey on the internet or could request it be mailed to them. In the first study roughly equal proportions of participants completed the survey on line and by post; by the time of the second survey the majority were filled in on line.
Once findings of the first study provided tangible evidence of serious discrimination and harm faced by same-sex attracted young people in schools, the ARCSHS team found it easy to generate interest in developing a response:
We did progressively develop a group of people who got behind us and worked with us to advocate … of course now we’ve got a community of same-sex-attracted young people who are also working with us. (CLO)
Surveys of same-sex attracted youth have led to other projects and a range of dissemination activities. ARCSHS also supports other broader resources for the gay, lesbian, bisexual, transgender and intersex (GLBTI) communities. ARCSHS manages Gay and Lesbian Health Victoria (which provides health information and resources for GLBTI people) and the Rainbow Network (which supports people working with GLBTI young people in the community or school-based settings). ARCSHS’s work with same-sex attracted young people is described in more detail on their website: http://www.latrobe.edu.au/ssay/ .
Knowledge forCommon Good
14
A community liaison officer developed a protocol for interviews including procedures for dealing with critical incidents (such as threats of harm to self or others), and a list of services which might assist in participant recruitment.
Separately funded resources produced by ARCSHS’s CLOs (often in conjunction with researchers) include information and a checklist for schools outlining measures to counteract homophobia (Ollis, Mitchell, Watson, Hillier, & Walsh, n.d.) and Outsmarting Homophobia, a booklet for young people (based on qualitative interviews) describing how young people have dealt with homophobic beliefs (Hillier et al., n.d.). A community partner interviewed told us that working with ARCSHS over many projects had been beneficial to his agency: ‘the data feeds back to us to inform us of best practice of how to target our service’. He also observed that young people he works with are extremely enthusiastic about Outsmarting Homophobia: ‘they love that, love it’.
Key Centre for Women’s Health in SocietyThe Key Centre for Women’s Health in Society (KCWHS) within the School of Population Health at the University of Melbourne received funding from VicHealth to employ a half-time CLO for three years from 2004-2007, inspired by the model operating at ARCSHS. CLOs were also employed through budgets of funded projects at KCWHS, including Project i (documented below) and the VicLANES project (Kavanagh et al., 2007). CLO activities at KCWHS documented in a report to VicHealth include research dissemination, media liaison, managing web pages and uploading documents, organising briefings for policy staff, managing relationships with local government officials and writing newsletters (Tattam, 2006).
Project i
Project i was an international study initiated by two senior researchers and funded by the National Institute of Mental Health in the United States for five years. It operated in Melbourne and Los Angeles, through the Center for Community Health at the University of California. In Melbourne Project i was initially conducted at ARCSHS and then, for most of its duration, was located at the KCWHS.
The Project i team surveyed 496 experienced homeless young people and tracked 165 newly homeless young people in Melbourne using in-depth open-ended interviews. In-depth interviews were also conducted with service providers from housing, mental health, juvenile justice, child protection, Centrelink and mediation services.
The Project i team included a 0.8 to full-time CLO, with three staff engaged in this role over three years. CLO activities were diverse. A CLO developed a protocol for interviews including procedures for dealing with critical incidents (such as threats of harm to self or others), and a list of services which might assist in participant recruitment. Workers from the service sector were trained and employed as research interviewers and the CLO was responsible for liaising with these staff. Meetings were arranged at potential participating services, initially to speak with managers and then with staff groups. These meetings dealt with issues such as where to conduct interviews, and processes for dealing with disclosures or critical incidents. During data collection the CLO carried a mobile phone in case of critical incidents. CLOs

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
15
maintained a website (http://www.projecti.org.au/), kept data bases up-to-date and wrote three-monthly reports on the project which were distributed to hundreds of services.
The involvement of services in assisting with recruitment to the study was crucial. As a researcher told us ‘it was essential we have service providers on board because they would be a critical way of recruiting participants into the study and also because we wanted the research to have an impact in the sector’. The research team focused much energy on maintaining linkages, regularly reporting findings and ensuring the relevance of research to the sector (Rossiter, 2000). Project i staff developed a communication protocol with each participating service. Throughout the project services received regular phone calls and visits from an allocated interviewer. The team ran regional community information forums and engaged with a network of refuges. A service provider from a participating service reported that her agency’s contribution had been valued and respected by the team ‘I felt that there was a genuine partnership with Project i’.
Project i staff were able to engage in activities not usually considered part of research work to reinforce service links, for instance sitting on agency boards of management. The project also fed directly into policy-making processes. Project i staff sat on a steering committee for a key state government policy on homelessness and their research provided the evidence base for the development of this policy.
Project outcomes included a range of refereed publications (i.e. Keys, Mallett, & Rosenthal, 2006), reports (i.e. Mallett, Edwards, Keys, Myers, & Rosenthal, 2003), broadsheets and resource books for young people living on the streets (Mallett, Keys, & Rosenthal, 2005; Rosenthal, Mallett, Keys, & Edwards, n.d.).
Onemda VicHealth Koori Health UnitOnemda was established in 1999 with core funding from VicHealth and the Commonwealth Department of Health and Ageing to focus on Koori health issues in south-east Australia. Koori communities and agencies were consulted prior to funding Onemda, and from the outset the Unit has operated on an innovative model where community development (as opposed to simply liaison) is a central activity, alongside research and teaching: ‘Our teaching and research activities were also framed by community development principles and practices’ (Onemda VicHealth Koori Health Unit, 2008a). Onemda has a clearly articulated community development plan, with the following goals:
1. Respect and strengthen Koori knowledge on health and well-being by: n Sharing knowledge and learning with Koori Communities and
stakeholders. n Affirming and enhancing the role of Koori Community
organisations in health research and evaluation. n Promoting Koori methodologies in health research and
evaluation.
The involvement of services in assisting with recruitment to the study was crucial. As a researcher told us ‘it was essential we have service providers on board because they would be a critical way of recruiting participants into the study and also because we wanted the research to have an impact in the sector’.
Knowledge forCommon Good
16
2. Define, strengthen and promote Koori community development principles and processes within Onemda by:
n Evaluating Koori Community Development using Koori terms of reference. n Developing appropriate and valid measures.
3. Ensure Koori community values, knowledge and priorities shape Onemda’s teaching, research and community development activities by:
n Integrating Koori community development principles into teaching and research. n Holding annual Talkin’ Strong days, community development
workshops and community visits (Onemda VicHealth Koori Health Unit, 2008b).
In 1999, Onemda held a workshop for Koori researchers to discuss their work and for community members to express their concerns about Aboriginal health research. Community Elders and young community members contributed to the discussions at this workshop, which were written up as a report (VicHealth Koori Health Research and Community Development Unit, 2000). Much of the discussion concerned how Koori communities could increase community control of research and ensure research would benefit community members. Onemda staff told us that findings of this workshop have guided the Unit’s subsequent work.
Three staff members are employed on the Onemda community development team, two of whom also undertake other activities at the Unit. As one staff member explained, the primary role of the community development team is to listen to community members and then work out what the Unit can do to work with community on issues of concern:
From this listening we develop a research project which then we feed back to community as community reports, which we then inject back into our teaching … collaborating with other units here or outside of the university. (CLO)
Community development workers also see their role as helping communities to make informed decisions about participating in research. They are committed also to bringing Koori community members into the university, for instance to contribute to teaching. Contact with community members is maintained informally through their own networks and through reference groups. The team also produces regular newsletters and disseminates community reports. Staff also respond to requests from non-Indigenous people for information on how to conduct research involving Koori communities and field numerous requests from students for information on Koori health: ‘We fill a void not just for the Aboriginal community but for the non-Aboriginal community too, who don’t know where to go and they get on the net and they come across Onemda’. Onemda has established a number of memoranda of understanding (MOUs) to formalise its relationships with other agencies.
Onemda provides a unique model for CPR. As a researcher from another centre told us: ‘Onemda has been an inspiration for people
Community development workers also see their role as helping communities to make informed decisions about participating in research. They are committed also to bringing Koori community members into the university, for instance to contribute to teaching.

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
working in other contexts of disadvantage’. Onemda has a website at http://www.onemda.unimelb.edu.au/index.html.
Community-based collaborative research at VACCHO
Dr Priscilla Pyett (PP) has a VicHealth Public Health Research Fellowship and is employed at Onemda. To further her work on community collaboration in health research and provide a resource to the Aboriginal community, PP suggested to the Victorian Aboriginal Community Controlled Health Organisation (VACCHO) that she base herself one day a week at their office in order to work with them or provide advice on research projects of their choosing. Previously funded by an NHMRC post-doctoral research fellowship, PP has now worked as VACCHO’s researcher-in-residence for over five years and has recently increased her role within the organisation to at least two days per week. VACCHO is the peak body providing policy advice, advocacy and support to the 25 Aboriginal Community Controlled Health Organisations around Victoria. Neither VACCHO nor its member organisations have any dedicated funding for research except through short-term project funding.
It took some time for the researcher to establish a role within VACCHO. She found she needed to be flexible about her role, offering to help with non-research activities to build relationships with staff.
Having a researcher on site has assisted VACCHO’s staff to become involved in a range of research activities. One of these was a Department of Human Services (DHS) funded project to develop information resources for the Koori community on alcohol use in pregnancy, to prevent the occurrence of fetal alcohol syndrome. VACCHO workers consulted with their community over the research while the researcher wrote a literature review (Pyett, 2007), drafted research questions and analysed data with the project team. The team encountered difficulties in negotiating with DHS around the format of the resources and around copyright ownership of Koori art for the project. These challenges prolonged the project but also helped to affirm the community’s trust in the researcher. The team eventually developed a suite of resources for the benefit of the Koori community that they were all extremely proud of. DHS has supported VACCHO to disseminate the resources with a specific training program to over 500 workers in mainstream and Aboriginal organisations, and the research team has also presented on the research findings at seven national conferences. After five years of the research partnership, VACCHO staff members said that they have learnt valuable skills and the organisation has increased credibility as a research provider. In addition, VACCHO is currently in the process of developing a Public Health Unit which will have dedicated funding to employ an Indigenous researcher within the organisation. Peter Waples-Crowe, a VACCHO staff member, and PP have co-authored a report that outlines ten steps for effective models for partnerships between Indigenous and mainstream organisations (Waples-Crowe & Pyett, 2005).
After five years of the research partnership, VACCHO staff members said that they have learnt valuable skills and the organisation has increased credibility as a research provider.
17

Knowledge forCommon Good
VACCHO staff advised that motivations of individual researchers are critical in determining which people are likely to be able to forge constructive research relationships with Indigenous communities:
Harms come in a lot of shapes and forms, especially around research …You want someone who’s going to work there and have an understanding of social justice. I think it’s really about what person you get. You need someone who cares about the community. (CP)
3.2 Research project modelsDeveloping a social and public health response to asbestos disease in the Latrobe ValleyIn 2002 Associate Professor Tony LaMontagne (TLM) initiated a program of research into asbestos disease in the Latrobe Valley area of Victoria. TLM initially made contact by attending collective or public memorial services for people who had died of asbestos-related disease, such as International Workers’ Memorial Day, and meeting members of the local community. The Gippsland Asbestos Related Diseases Support group (GARDS) subsequently became a central partner in a series of research projects. GARDS representatives were keen to be involved in research from the start, seeing research in which they could have a say as critical in their struggle to make governments fund appropriate services. A GARDS member stated that ‘that’s what the university’s there for, in my view … so we can get knowledge that empowers us to drive issues forward’. Community participants noted that they had used research to successfully argue for the funding of a regional cancer treatment ward.
On commencing this work TLM was employed in the Centre for Health and Society, later moving to the McCaughey Centre for the Promotion of Mental Health and Community Wellbeing, both within the School of Population Health at the University of Melbourne. Much of the work was supported by a VicHealth Senior Research Fellowship awarded to TLM to undertake community-based research into health promotion involving blue-collar workers. Projects in the Latrobe Valley have included a qualitative analysis of community perspectives on asbestos disease in the Valley (LaMontagne & Walker, 2005; Walker & LaMontagne, 2004) and a history of responses to the issue (Hunter & LaMontagne, in press). Community partners have published transcripts of public addresses on asbestos disease alongside an academic journal article by TLM and co-researchers (Hamilton, in press; LaMontagne, Hunter, Vallance, & Holloway, in press; Swayne, in press). In 2006 an NHMRC grant was awarded to TLM and Dr Anthony Holloway of the Peter MacCallum Cancer Institute, with GARDS as a partner, to research potential markers for asbestos-related diseases in former and current power industry workers in the Latrobe Valley.
A research officer has been employed to liaise with unions and GARDS on the NHMRC-funded project. This worker’s primary role on the project has been negotiating with unions and other agencies that
‘That’s what the university’s there for, in my view … so we can get knowledge that empowers us to drive issues forward’.
18

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
19
are active partners in recruiting research participants and processing blood samples. The research officer also acts as a contact point for research participants themselves. TLM continues to liaise with community members and in research exchange activities, often in collaboration with the research officer.
TLM believes that working in collaboration has broadened his approach to public health research through identifying ‘things that I would not have arrived at from a straight public health perspective’. His collaborative experience in this area has led him to propose that a ‘comprehensive social and public health’ response is needed to fully address the asbestos disease legacy (LaMontagne et al., in press).
Social processes for health: understanding the links between place and social connection Dr Deborah Warr (DW) has a long-standing research interest in exploring health and well-being for people living in disadvantaged communities. This project (funded by the NHMRC) explored the social networks of people living in two socially and economically marginalised localities in Victoria. The place-based projects required sustained on-site community engagement and thus relied on developing links with people who were willing to support long-term ethnographic research.
In each of the sites, DW was able to develop ongoing partnerships with key community-based workers: a health promotion/community development worker and the coordinator of an early-learning centre attached to a primary school. In both sites she spent considerable periods of time in community settings, talking with parents and workers and participating in activities that were taking place.
It was important to give something back to the communities from the research and in each of the sites DW prepared plain language reports outlining key findings from the research. In response to local issues, the reports had different emphases. One of the reports focused on the role of the early-learning centre and documented the centre’s innovative efforts to improve educational outcomes in contexts of intersecting disadvantages (Warr, 2007). The early-learning centre coordinator had struggled for many years to secure funding for her program. She believes the report was one of a number of factors involved in her eventual success in doing so: ‘having a published report does more than just inform - it provides a framework for others to see where you’re going’. Working with a researcher also offered her and other staff opportunities to think about their work in new ways and made them feel their work was valued:
For me, having [the researcher] in the room, allowed us to reflect on what we do. Having another pair of hands and eyes allowed us to reflect in a different way. It gave a legitimacy to the work that we were doing. (CP)
This report was timely because plans are underway to amalgamate and build new schools in the area. The local community and service
‘Having a published report does more than just inform - it provides a framework for others to see where you’re going’.

Knowledge forCommon Good
providers were concerned to promote understanding of the needs of the community, show these needs are currently being met and to make the case for additional resources that were needed.
The other community report (Warr, 2004) focussed on a set of issues that had been consistently raised in the interviews conducted with residents. The report was widely disseminated in the area and was used as a training tool for professional development with police. Among other issues, the report presented residents’ accounts of problems related to neighbourhood stigmatisation. In response to these issues, a community-initiated project called ‘Northern Exposure’ was established to develop positive images of the northern suburbs of Geelong. Strategies included working with a journalist at the regional newspaper and obtaining funding from a wide variety of sources to develop a ‘digital stories’ project run by the Australian Centre for Moving Images. This project culminated in a special screening of completed stories at a cinema in Geelong followed by a ‘question and answer’ session with guests and film-makers exploring the links between the stories of people and places that were portrayed and problems of stigma. Some of the residents involved in this project participated in a forum at the University of Melbourne organised by DW, where they reported on their experiences in the digital stories project.
Trajectories of identity for injecting drug users An ARC grant was awarded to Associate Professor John Fitzgerald from the School of Population Health and Dr Kevin McDonald, then in the School of Sociology at the University of Melbourne, to study the social experience of drug use. Additional DHS funding was also secured to undertake research into Hepatitis C in regional Victoria, which the researchers linked with the ARC project. Researchers decided to locate the study in the city of Bendigo. The ARC funding period was from 2002-2005, although researchers continued to disseminate findings after this period.
The project involved collaboration with diverse groups, from health centre executives and police to injecting drug users. Staff maintained contact with 15-20 drug users in Bendigo over a period of three years, often visiting people in their homes and meeting with them both individually and collectively. The project was fluid in structure and researchers changed direction as new opportunities or constraints emerged. A Project Officer with a background in the youth and drug treatment service system was employed in a CLO role to manage relationships with participants and partners in Bendigo. This person arranged appointments and accompanied the researchers to meetings and interviews. As the research methodology was ethnographic - requiring long periods of time in the research setting - the researchers remained actively involved in liaison with project participants.
Staff focused a great deal of energy on knowledge exchange. A website was maintained through the project, with drug users who
Strategies included working with a journalist at the regional newspaper and obtaining funding from a wide variety of sources to develop a ‘digital stories’ project run by the Australian Centre for Moving Images.
20

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
21
In accordance with the community’s wishes, the team devised a careful media strategy and used this to promote debate without generating wider negative publicity about drug use in the area concerned.
had skills in web management employed to undertake this role (see http://www.bodydrugsworld.unimelb.edu.au/info.html). Community members were consulted about research recommendations through a series of forums and meetings and research conclusions were refined during this process. A report (Fitzgerald, McDonald, & Klugman, 2004) was distributed and also downloaded from the internet by over 1200 unique users. In accordance with the community’s wishes, the team devised a careful media strategy and used this to promote debate without generating wider negative publicity about drug use in the area concerned. One research outcome was an invitation from DHS to develop a policy response to the issues raised in the report for the region. The project involved the researchers in activities far outside the usual academic role: ‘it was a lot of non-research work; it was actually political work and policy work’.

Knowledge forCommon Good
22
Researchers also observed that the quality of their work benefited from sustained interaction within communities. Some pointed out that they could only do the kinds of research that interested them with the cooperation and support of communities and community representatives.
As this report shows, CPR projects were established and conducted in different ways. Large projects entailing teams of researchers and multiple project partners required more formal arrangements than small or one-off interactions between communities and researchers.
Initiating projectsThe researchers and CLOs interviewed gave, in the main, strongly altruistic aims for their work and were often motivated by social justice concerns. For instance,
We all have a belief that you’ve got to give back to communities. But it’s more than that. Your research needs to make a difference … we have a dream for a different world, that’s social change. (R)
We had a commitment to not just feeding back to the sector but to try to make a contribution in whatever way we could. (CLO)
Everybody that’s in the Unit is motivated for the betterment of the community. (CLO)
Researchers also observed that the quality of their work benefited from sustained interaction within communities. Some pointed out that they could only do the kinds of research that interested them with the cooperation and support of communities and community representatives.
Community partners, as indicated in the case studies above, were keenly aware of the value of research in advocating for improved service delivery and understanding of marginalised groups. They entered into research partnerships because they believed stories needed to be told, they felt that useful resources for community members might be developed as a result, and also because they anticipated they would be able to use findings to support funding claims. Research provided community agencies and members with opportunities to have a broader influence than they felt to be possible through their day-to-day activities:
In some ways agencies like us where we’re small, we rely on those avenues to be able to articulate and contribute to ideas and solutions. (CP)
Other studies of CPR advise that community partners should ideally be involved in the initial planning and design of projects, not just at the time researchers wish to commence data collection and need to access participants (Community-Campus Partnerships for Health, 2007; Israel et al., 1998; Roussel et al., 2002). Nonetheless, the reality of the research environment is that this is often difficult for researchers to achieve. In many instances researchers lack time to consult with community partners over proposals that may or may not be successful in gaining funding or else are responding to funding opportunities offered by government departments rather than expressed community needs.
Many of the research projects described above were initiated by researchers, rather than communities or community representatives.
4. Strategies for community engagement and knowledge exchange

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
23
Many of the community representatives interviewed stated that they neither wanted nor expected to be involved in all aspects of a research project. They did, however, expect their involvement and contributions to be acknowledged and to feel valued and respected by the researchers.
One researcher involved said that asking people to commit to projects with an already-formulated methodology was difficult because it constrained the nature of the contributions partners were able to make. Some researchers acknowledged that their work was investigator-initiated and they offered carefully delineated partnerships to community members or agencies. Most felt that they were able to adapt aspects of their projects in accordance with partners’ wishes. People working in Aboriginal health, on the other hand, were very clear that the community must be consulted about any proposed project and must ultimately have control over the direction of Indigenous health research.
Involving community partners in research does not necessarily mean that consensus will be achieved on research conclusions or recommendations. One researcher spoke of involving community agencies in an iterative process of research discussion and reformulation. Some participants (such as police) contributed to the research process and to subsequent discussions but did not support all eventual research recommendations.
Comments reported above on community participants’ motivations for engagement in CPR indicate that their primary concern is to generate information or findings that may benefit the communities they come from or work for. Many of the community representatives interviewed stated that they neither wanted nor expected to be involved in all aspects of a research project. They did, however, expect their involvement and contributions to be acknowledged and to feel valued and respected by the researchers. In this case community involvement from early project development may not be critical to their willingness to participate. Involving community partners when research projects are already formulated does, however, clearly limit the kinds of input participants are able to have and their sense of ownership of research.
Finding a community partner and spending time in the communityResearch projects described above included a range of community partners, from members of a disadvantaged or disenfranchised community to paid employees in community groups or advocacy organisations. Many researchers and CLOs found that it was essential in gaining entry to a community to establish rapport and common purpose with particular influential or well-connected individuals who were prepared to be active partners in the research. Identifying key informants who facilitate access to communities is well-recognised as a research strategy within the discipline of ethnography (Atkinson & Hammersley, 1998). Israel and colleagues (1998) review community-based research projects and conclude that respected and well-integrated community members must be involved. They also argue that when research is concerned with understanding a ‘community of identity’, such as a group defined by ethnicity or race, community members as well as paid employees (who may or may not be community members themselves) must also be engaged as participants.

Knowledge forCommon Good
24
The establishment of any advisory group raises difficult questions about who is able to represent the views or interests of any community. Representatives of community groups, rather than community members themselves, often sit on advisory groups.
Research partnerships appear to blossom where there is a genuine liking and mutuality of interest between community partners and researchers. Mutual trust is also essential (Pyett, 2002). A research participant told us that partnerships work best where people know each other well enough to voice disagreement and to spend the time required for reaching consensus on issues.
Researchers in the present study believed that having community participation greatly enhances the impact of research. This is because community partners actively disseminate and advocate for the implementation of research recommendations: ‘you’ve basically got study ambassadors. It’s not just somebody else’s work. It’s their work’. One researcher observed that change was most likely to occur after a report was released where a community representative or agency took it upon themselves to act as an advocate and lobbyist.
Face-to-face contact is clearly crucial in establishing research partnerships. All projects entailed visits to meet with representatives of communities. A community participant involved with a very large research project stated that she appreciated having one identified person to liaise with who visited her service regularly. One community worker interviewed argued that it is critical for researchers to spend time themselves in community settings to really understand what is going on:
If you’re going to have an interaction with another person then you have to sit in their landscape.
Researchers using ethnographic methods obviously spent significantly more time immersed in communities than those who used survey methods. For one such researcher, interaction in community settings provided a ‘depth of insight otherwise unavailable’.
Establishing an advisory or reference groupAdvisory or reference groups are frequently used as participatory mechanisms in health research. Advisory or reference groups vary from a true forum for partnership where important decisions are made, to a uni-directional opportunity for researchers to advise community representatives about their work.
The establishment of any advisory group raises difficult questions about who is able to represent the views or interests of any community. Representatives of community groups, rather than community members themselves, often sit on advisory groups. Particularly in the case of disadvantaged populations, community representatives may differ from community members in terms of income and education (Israel et al., 2003).
There were mixed reports on the usefulness of establishing formal advisory or reference groups as a means of ensuring input to projects. One project initially began by establishing two reference groups, one for service providers and another for policy professionals, but found that discussion at both groups overlapped significantly. A couple of participants commented that funding bodies

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
25
Community consultation is particularly critical in Aboriginal health research. People working in Koori health who were interviewed for the study saw reference groups as a very important part of their commitment to community engagement.
like to see reference groups as evidence of collaboration and that they are sometimes used by researchers as legitimating strategies rather than as genuine strategies for collaboration. Researchers on smaller projects tended to liaise with a key community member, rather than set up a formal structure.
Community consultation is particularly critical in Aboriginal health research (Matthews et al., 2001; VicHealth Koori Health Research and Community Development Unit, 2000). People working in Koori health who were interviewed for the study saw reference groups as a very important part of their commitment to community engagement. Reference groups also enable researchers to develop research findings cooperatively with others so a broader range of views might be represented, as a staff member told us:
And the bottom line is I don’t want to be making decisions on a project without having consensus from a group. And that’s about valuing people’s opinions and giving them a voice around the table. (CLO)
Participants in our research agreed that reference groups were only of use where researchers were committed to incorporating community views and able to adjust projects accordingly. For instance, one project had a complex methodology and the researchers found that they were unable to incorporate many of the reference group’s suggestions due to the demands of the already established research protocol.
Recommendation: Advisory or reference groups should be established where real input to a research project is desired by the community and respected by the researcher.
Developing memoranda of understanding or partnership agreementsNorris and colleagues (2007) argue that developing an MOU aids in establishing an equitable relationship between university and community partners. Some research projects profiled in this study, particular larger ones, developed and agreed upon MOUs with partner agencies and individuals. In other research centres MOUs are very detailed and subject to legal overview. These documents tend to be used to formalise relationships between agencies. In these instances smaller-scale partnership agreements might be developed to agree on research. A sample research partnership agreement is attached at Appendix 1. Another MOU pro forma is included in a journal article (Norris et al., 2007) and an example is provided in a report by Waples-Crowe and Pyett (2005).
Israel and colleagues (1998) advise that jointly agreeing on research principles and approaches, for instance around confidentiality and data access, facilitates effective partnerships between researchers and communities. Some of our research participants insisted that while written agreements are a good safeguard against personnel changes in organisations, the real value of this approach is in the discussions which occur over the development of agreements.

Knowledge forCommon Good
26
Little has been written on the employment of dedicated community liaison staff in universities. A US report suggests that staff familiar with both research and community settings can play a ‘translational’ role between partners in research.
Many small or short-term projects adopt a more informal approach to agreeing on terms of reference. Some researchers participating in our project felt that short collaborations did not necessitate MOUs or that, in the case of qualitative or exploratory studies, such documents were impossible to draft because the exact nature of the arrangement would evolve over time and thus could not be stipulated at the outset.
On the other hand most community representatives interviewed emphasised the importance of these documents, particularly because some felt they had less bargaining power than researchers when disputes arose. A community representative suggested a standard MOU could be developed detailing confidentiality agreements, data ownership and use of agency logos on ensuing reports. A service provider interviewed reported feeling very reassured by the offer of a detailed MOU outlining roles and responsibilities of all partners. Another community representative believed developing a MOU prior to submitting for research funding would have averted subsequent conflict:
I will never do another project unless I actually see the project in writing, who actually the players are and what actually we are achieving and it all written down prior to going for funding ... It creates all sorts of problems.
Recommendation: Memoranda of understanding or partnership agreements are recommended to clarify roles and expectations of all research partners. Research centres should develop template documents for adaptation by researchers (see Appendix 1).
Employing community liaison staffLittle has been written on the employment of dedicated community liaison staff in universities. A US report suggests that staff familiar with both research and community settings can play a ‘translational’ role between partners in research (Community-Campus Partnerships for Health, 2007: 6). Israel and colleagues (1998: 186) recommend the employment on research staff of a ‘community organiser’, ‘who is able to bring together people in the community, who has a history of community involvement, and who is respected and perceived as a leader in the community’. In Australia, Mitchell and Walsh (2003) argue that academic staff face institutional and professional impediments to establishing and maintaining relationships with community partners. They suggest therefore that dedicated intermediaries such as CLOs are required to maximise the value of social research. Mitchell and Walsh provide examples of how CLOs employed through core centre funding have enhanced research activities by negotiating with stakeholders over research questions and research utilisation.
The case studies described above include three research centre models where dedicated CLOs or community development staff are employed at universities to facilitate community engagement. Individual research projects described include a range of mechanisms for liaison with communities such as employment of a project or research officer or instances where the researcher performs a

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
27
Academic publications are notoriously slow to appear, usually requiring long lead times between submission, revision and eventual publication. Community reports written in plain language and in a readable format are frequently used to share information with communities.
community liaison role him or herself.
The nature of CLO roles appears to be largely influenced by employees’ existing strengths and the stage which research projects were at. One CLO did some research interviewing; others focused on managing relationships with project partners or media liaison. Where they were employed late in a project, much of the CLO’s focus was on research dissemination. Community development staff at Onemda, profiled above, saw part of their role as educating Indigenous communities on how to make decisions about research participation, and also advising them of complaints mechanisms where communities were unhappy about research involvement.
Recommendation: Skilled community liaison work requires funding at university, centre or project level. Ongoing positions at University or Centre level would facilitate and support more effective community engagement and knowledge exchange.
Community reports, newsletters, presentations and seminarsStrategies for sharing research findings must be tailored to meet the needs of specific audiences whose knowledge, policies or practice the research findings are intended to influence (Lavis, Robertson, Woodside, McLeod, & Abelson, 2003). For example, systematic literature reviews accessed through central registries may facilitate evidence-based policy decision-making (Lavis, Lomas, Hamid, & Sewamkambo, 2006) but are unlikely to be read by many community members. Research institutes are becoming aware of the need to target communication of findings to specific audiences. In Canada, for instance, one third of research organisations responding to a large survey produced specific messages for targeted clinical or policy audiences from their research (Lavis et al., 2003).
Various articles advocate imaginative formats for sharing research, for instance through video making (Brannen, 2002), scripting a DVD (Sandelowski, Trimble, Woodard, & Barroso, 2006), holding interactive workshops, developing websites (Lavis et al., 2003) or sending text messages (Tattam, 2006). Researchers and CLOs involved in our research spoke of using many different formats for disseminating research findings. Approaches to knowledge exchange included designing and delivering training packages for professional staff, producing visual educational materials such as posters and leaflets, producing podcasts for download from the internet, posting PowerPoint slides on the internet, resourcing support groups and making contributions to government policy.
Academic publications are notoriously slow to appear, usually requiring long lead times between submission, revision and eventual publication. Community reports written in plain language and in a readable format are frequently used to share information with communities. An advantage of these reports is that they may be produced and disseminated far more quickly than academic publications (Mitchell & Walsh, 2003). ARCSHS and Onemda make

Knowledge forCommon Good
28
Face-to-face meetings with researchers where issues could be discussed were the preferred knowledge exchange mechanism for most community representatives interviewed. Communities also generally said that they preferred to hear directly from the researchers rather than other project staff.
it a priority to publish community reports to disseminate findings promptly and in a readable format (Mitchell & Walsh, 2003). In some instances community newsletters were also used to disseminate research findings.
Researchers and CLOs also frequently present research findings verbally, at meetings, forums and conferences. Face-to-face meetings with researchers where issues could be discussed were the preferred knowledge exchange mechanism for most community representatives interviewed. Communities also generally said that they preferred to hear directly from the researchers rather than other project staff. Only a few efforts have been made to investigate ways that community members can publish or have a voice alongside researchers. DW arranged a forum where research participants shared their views with university staff. As previously noted, TLM facilitated the publication in an academic journal of public addresses made by community partners.
Researchers found it difficult to provide the right amount of information in reports and presentations. One researcher commented that she had presented too much information at an early meeting to explain research. In retrospect she felt she would have been better to have focused on the probable benefits of the research for communities.
Websites and mediaWeb pages and downloadable documents are cost-efficient options for knowledge exchange, offering an excellent medium for disseminating information about research projects and research findings. As well as disseminating research, posting research reports on the internet offers academics the opportunity to demonstrate research usage by counting the number of times that documents are downloaded (Thelwell, 2002). Researchers told us of hundreds of unique users having accessed project sites and downloaded reports. Website maintenance requires, however, a significant investment of time and energy and a level of computing expertise that is beyond most researchers.
Publicity in mainstream media is an effective means of communicating with the mainstream community (National Health and Medical Research Centre & Consumers’ Health Forum of Australia, 2004). Launching community reports provides a good opportunity to publicise research findings though media releases. Participants were, however, ambivalent about the utility of involving the media in disseminating complex and often sensitive research findings regarding disadvantaged communities. Many research participants commented that it was difficult to manage how media represented their findings (see also Tattam, 2006). Some projects entailed carefully planned media strategies and targeted press releases to appeal to outlets most likely to treat research findings with sensitivity.
Recommendation: Universities should ensure that support staff with electronic media skills are available to assist researchers to profile their work and to regularly update web pages.

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
29
In practice, actual community involvement in collaborative research varies considerably, although researchers generally retain ultimate control of the process, community representatives can often play a significant role.
There are many challenges for researchers and community representatives wishing to undertake CPR from within a university. Truly equal research partnerships are difficult to achieve. While laudable in its intent, putting ideals of equality into practice is not easy, (Chataway, 1997; Maguire, 1987; Petras & Porpora, 1993). It is naïve to assume that larger social power differences will become irrelevant or disappear simply because of the goodwill of participants (Chataway, 1997; Croft & Beresford, 1992; Marshall & McLean, 1988). All partners in CPR may find their desires to work as equals fraught by the social and political context in which they operate, where academic expertise is afforded greater legitimacy than community experience (Israel et al., 1998; 2003). In communities that are experiencing economic disadvantage, ‘social difference’ between community members and professional research staff may lead to problems with communication and mutual understanding (Cawson, Mercer, & Barbour, 2007). Researchers and communities may have different ambitions for the research, particularly where researchers are required to produce scholarly outcomes that are of little direct benefit to communities. Indeed, researchers have found that the time demanded by collaboration interferes with their career prospects through limiting their capacity to produce academic publications (Israel et al., 1998). At the same time researchers are unlikely to maintain collaboration with community partners unless their joint work also benefits the communities involved (Cochran et al., 2007; Volker, 2002). Research must be rigorous while at the same time consistent with community values (Street et al., 2007).
In practice, actual community involvement in collaborative research varies considerably, although researchers generally retain ultimate control of the process, community representatives can often play a significant role (Norris et al., 2007; Seifer & Green-Morton, 2007). Service providers tend to be mostly involved in advocacy and research dissemination and community partners frequently have the least active roles (Flicker & Savan, 2006).
Participants in this research reported grappling with these and other problems, as outlined below.
Challenges encountered by researchersResearchers involved in the study mentioned four main difficulties in conducting CPR and ensuring knowledge exchange. These were:
n the sensitivities of working in communities;n time requirements and diverse non-academic tasks involved; n funding shortfalls; andn an associated perception that their careers had suffered as a
result of missed publication opportunity, and that academic performance measurement failed to recognise the demands of CPR and non-academic research outputs.
Working with communities frequently entails sensitive negotiations. The literature identifies determining who is able to represent the views of community members through acting as a research partner as a key concern for CPR (Israel et al., 1998; 2003). Researchers
5. Challenges for effective CPR

Knowledge forCommon Good
30
At times researchers found dealing with the complex politics of community work stressful and distressing. They felt that some community group members’ lack of understanding of the research process occasionally led to unrealistic expectations and dissatisfaction with research.
in the present study struggled with conflicts within communities over who ought to be consulted or who was qualified to represent whom. This was particularly problematic when university processes such as ethical approval require they demonstrate community involvement. Yet they were aware also that some peak bodies or organisations were not actually representative of the communities concerned. At times researchers found dealing with the complex politics of community work stressful and distressing. They felt that some community group members’ lack of understanding of the research process occasionally led to unrealistic expectations and dissatisfaction with research. Researchers were also wary of providing too little or too much information to communities, fearing alternatively insulting them by oversimplifying findings or presenting material in language that was too obtuse.
CPR is notoriously slow work (Israel et al., 1998). Extensive time for consultation and negotiation is required from project conception to implementation and eventual research dissemination. Effective data collection would only occur, in some instances, after researchers were well-known in the community. A researcher spent six months working directly in a community group before some members felt comfortable participating in research interviews with her.
Researchers engaged in CPR must be prepared to respond to diverse community needs. Many noted that in order to gain entry to a community they often needed to offer whatever expertise they could, rather than focusing solely on research tasks. Negotiating a role could be an awkward period of uncertainty for researchers. As one researcher told us:
To begin with I felt shy, like a fish out of water. I just sat around I didn’t know what to do at lunch. I was waiting for people to realise that I could be useful… until people found things to ask me to do.
Researchers also found they spent significant time providing input to policy processes or giving advice to community partners subsequent to conducting research. Another requirement of CPR is to produce plain language reports for communities and policy professionals and reports to funding bodies, which, as we shall go on to discuss, count for little within current Commonwealth Department of Education, Science and Training (DEST) systems of academic performance measurement.
Research funding for CPR is difficult to secure. As we have observed, funding bodies may be reluctant to provide grants for less established research methodologies, such as CPR with long lead-times, uncertain outcomes and additional resourcing requirements (Israel et al., 1998). The benefits of CPR and related approaches are often diffuse and difficult to measure. Perspectives on the effectiveness of any collaboration are likely to vary and few rigorous evaluations of research collaborations have been undertaken (Lavis et al., 2003; Roussel et al., 2002), although some efforts have been made to develop procedures for evaluating these collaborations (Maurrasse, 2002; Viswnanathan et al., 2004).

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
31
A community liaison officer commented that building ongoing relationships with communities was made difficult by the fact that so many university staff are employed on short contracts: ‘How are people going to be committed to doing knowledge transfer from work when [they’re] not going to be around?’
It was widely argued by participants in this project that research funding rarely provides sufficient resources to enable academics to engage communities and to conduct research exchange. Two researchers told us that:
Funding is a key issue obviously. Funding rarely is sufficient for time taken. Funding needs to recognise the time taken out of researchers.
It’s very hard to get money and when you do it’s typically underfunded. It doesn’t recognise time for relationship building and relationship maintenance … That’s totally not recognised or appreciated in the funding. Research transfer is also time-consuming and frequently involves travel.
A CLO commented that building ongoing relationships with communities was made difficult by the fact that so many university staff are employed on short contracts: ‘How are people going to be committed to doing knowledge transfer from work when [they’re] not going to be around?’ A researcher complained that the university policy of taking 35% on costs made it no longer viable for her to tender to undertake research consultancies.
Closely related to concerns over the time spent on developing and maintaining community partnerships was a parallel anxiety among researchers about lost opportunity to produce peer reviewed academic publications. The NHMRC has suggested that more incentives are needed to encourage academics to communicate their findings in lay language (National Health and Medical Research Council, 2004). A DEST Publication Category system has been used in Australia to assess a component of each university’s funding allocation (Butler, 2003). From 2007, the Research Quality Framework (RQF) was introduced in Australia as a system for assessing not only the volume of research output, but also quality and benefit to the community of academic research. The federal Labour Government announced in early 2008 that the RQF will be replaced with a new system, titled ‘Excellence in Research for Australia’ (Carr, 2008). Under the DEST publication system, universities were required to report on four kinds of publications: authored books, chapters in research books, refereed journal articles and refereed conference papers, but not community reports. DEST publications are valued by universities because they are counted in funding allocations and are likewise an important measure of success for academics.
Concern about the impact on academic careers of time spent on community engagement or writing community reports was frequently raised through interviews conducted for this study. Although researchers often felt that CPR was valued within their research centre or by some colleagues, they were keenly aware that outputs from this research were not counted in academic performance metrics under the DEST system, and that findings are difficult to publish in prestigious ‘high impact’ journals. Time spent on research dissemination was also difficult to account for and poorly valued within the university, as a number of researchers explained:
Knowledge forCommon Good
32
‘We do our booklets, our posters, we have all of our time out in the field, which we feel is just as important as the research but we have no incentive to do that at all – it doesn’t count. That’s the biggest impediment to doing community work.’
We really suffered in terms of publications in doing this … There’s a huge personal cost for me and for some of the other members of staff.
We do our booklets, our posters, we have all of our time out in the field, which we feel is just as important as the research but we have no incentive to do that at all – it doesn’t count. That’s the biggest impediment to doing community work.
Our community work doesn’t count. So the default is not to do good community dissemination.
Places where you can publish reports on community work have very low impact factors.
We need a way of counting community reports and community liaison as academic work.
An experienced researcher told us they were only able to undertake community research because, nearing retirement age, they no longer felt the need to promote their own career. Nonetheless, a couple of researchers also argued that CPR brought recognition if researchers were able to actively promote their work within the university. One way this had been done was by tracking numbers of unique users downloading community reports.
Challenges encountered by community partnersDifficulties reported by community partners participating in this research included:
n having unequal power within the research relationship;n concern that their involvement might be used only to legitimate
research; andn having to fit research tasks into busy schedules.
There are many barriers to effective collaboration between researchers and communities. Communities may distrust researchers. In some instances community willingness to participate in research may be marred by previous experiences. Indigenous peoples frequently argue that researchers take data from communities and build their own careers without offering any tangible benefit in return (Cochran et al., 2007; O’Donaghue cited in Matthews et al., 2001: 1; VicHealth Koori Health Research and Community Development Unit, 2000).
Many of the difficulties reported by community partners were associated with their unequal position within research partnerships and reliance on researchers to offer opportunities for inclusion and to feed back information to them. Some felt that their expertise and contribution were not as valued as that of researchers.
Employees of an Indigenous community-based agency noted that they are constantly asked by researchers to comment on research proposals or to support research, with universities hoping to use their logo to lend credibility to their projects. Along with other community members interviewed, they also find that when projects do not go as envisaged or community members are unhappy with
The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
33
Community partners also commented on the sensitivity of some research projects and that sometimes researchers were unaware of politics around issues they were researching in local communities: ‘researchers don’t understand and don’t particularly want to know about the politics and that’s where they blunder in’.
research, they are left in the difficult position of either defending research or withdrawing involvement:
They’ll use you to say they’ve got the Aboriginal community on side. And if things go wrong, you cop it.
Community partners also commented on the sensitivity of some research projects and that sometimes researchers were unaware of politics around issues they were researching in local communities: ‘researchers don’t understand and don’t particularly want to know about the politics and that’s where they blunder in’.
Individuals acting as community partners often find it difficult to secure organisational time and commitment for involvement in research (Community-Campus Partnerships for Health, 2007). Research participation can be difficult to fit into a work schedule where service delivery is the priority. A community representative interviewed appreciated researchers’ efforts to minimise time required to assist researchers recruit for a study: ‘They really recognised that we were under the gun with day-to-day work.’
From the perspectives of community members, the time between data collection and release of findings can be frustrating (Community-Campus Partnerships for Health, 2007). Community partners interviewed for this project also expressed some frustration about the extensive time that it took to get research off the ground, conduct it and eventually receive findings.
Challenges encountered in relation to employing community liaison staffSome of the challenges for CLOs and those who employed them were:
n lack of clarity about the role;n managing conflicting demands of researchers and
communities; and n issues relating to performance assessment, career structure and
sense of value.
CLOs undertake diverse activities which include contacting agencies, coordinating project staff, developing research resources and protocols, organising and attending forums and meetings and maintaining web pages. CLOs are also frequently responsible for knowledge exchange, including writing community reports and media liaison. While they do not usually undertake research themselves, CLOs require a good understanding of research and its potential uses. Tattam (2006) has suggested that CLOs need a personality and approach which will enable them to work with many different people. CPs agreed that these positions are difficult to fill with appropriately skilled staff.
Relatively few CLOs are employed in universities and so the nature of this already diverse role is frequently ill-defined. CLOs spoke about a period of difficulty during the early period of their employment while the team worked out their various responsibilities. A researcher

Knowledge forCommon Good
34
Community liaison officers may be subject to competing expectations or demands from communities and researchers.
in a centre employing staff to undertake community liaison spoke similarly of having only gradually become comfortable about working with community liaison staff. She told us that initially she was anxious that the CLO would take over her work. A few projects later this had changed and the researcher now feels extremely comfortable with the community liaison approach, so much so that she regards herself as ‘almost part of the community liaison team’. She believes strongly in the importance of employing dedicated CLOs but also cautions that researchers should remain engaged in community work:
I think if all you do is just hand over your research at the end, it deskills you, it disconnects you from the community … I think what you need to do is – there’s some middle ground – where you are using the strengths of the community liaison while not absolving yourself of the responsibility or your connections.
Curiously, researchers who had worked with a CLO were sometimes ambivalent about the wisdom of employing specific staff in this role. One researcher found it difficult to relinquish the liaison role and wondered whether employing a research assistant (RA) in a more junior role, along with additional administrative support might have been a better choice:
Having had [a] CLO, I’m not sure that I would do it again. I’d certainly have people doing some of the administrative work. I’d probably employ a RA to do some of that engagement. What I found was that it was far easier to do that engagement if I was doing it myself, if I actually made the links. It was particularly critical as we began to disseminate because I knew the research in a way that the CLO really didn’t. And I knew the theoretical field and I also was very clear about what I wanted to achieve in those relationships … it can be difficult.
CLOs may be subject to competing expectations or demands from communities and researchers. Although they are employed to liaise between researchers and communities, CLOs are employed and situated in research centres and therefore more closely aligned with universities than with disadvantaged groups. Liaison staff employed in US institutions indicate that this can be a difficult role and staff may lose respect within their communities if they are perceived to be accountable to universities rather than communities (Community-Campus Partnerships for Health, 2007). Some staff interviewed for the present study also found their conflicting allegiances very difficult to balance, as one CLO explained:
Of course we had terrible struggles working out then what I could do. I thought the idea would be that I would consult the community and then we’d do what the community wanted. Instead there was a bunch of researchers with their own ideas about what they wanted to do.
Likewise, some community representatives felt that liaison staff should be based in communities and not in universities so that their

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
35
Like academics, community liaison staff were concerned that much of their workload was not measurable through performance appraisal systems at universities. They felt that valuable aspects of their work were very much under-recognised.
first loyalty would be to communities and not to researchers or universities:
The liaison role person should be a community development type of person. Community groups really struggle with professional jargon. You need someone who’s used to dealing with communities, like a community development officer. You can’t just put an academic in there.
In some instances CLOs complained about a lack of career structure and felt that their expertise was undervalued by academics. An academic expressed concern that CLOs are employed on contract and there are no established career structures or performance measurement tools for their work. One CLO was emphatic that she would never again take on a similar role because it became a de facto administrative role:
That’s the reason I’m not interested in applying for any community liaison jobs. I don’t want to spend hours organising catering for an event or standing in front of a photocopier.
Like academics, community liaison staff were concerned that much of their workload was not measurable through performance appraisal systems at universities. They felt that valuable aspects of their work were very much under-recognised:
I know that if I had to tick a box on the academic work that I’ve done, most of them would be empty … As a staff member you’re judged on your performance by journal articles and what you’ve written. There’s nowhere [on the forms] where it really values the networks that we have and the brokerage that we do. I think it might be recognised within the unit but not more broadly within the university.

Knowledge forCommon Good
36
A meaningful role for community workers in the research, and mutually trusting relationships must be established. It is important also to build the research skills of community participants in the research process.
The literature describes a range of elements common to successful research collaborations between communities and researchers (see Community-Campus Partnerships for Health, 2007; Israel et al., 1998; National Health and Medical Research Council & Consumers’ Health Forum of Australia, 2001; Pyett, 2002; Roussel et al., 2002; Winter et al., 2005). Firstly, research partners should be involved from the very beginning of the project. Extensive negotiation and consultation is likely to be required prior to the commencement of any project to formulate and agree on common goals. Respective roles of all partners should be clearly defined. Mutual respect for each other’s strengths and contributions are also required (Community-Campus Partnerships for Health, 2007). All parties must maintain an awareness of the political context of any research project. Partners must be sufficiently flexible to renegotiate arrangements if required and decision-making should be democratic (Israel et al., 1998). A meaningful role for community workers in the research, and mutually trusting relationships must be established. It is important also to build the research skills of community participants in the research process (Pyett & VicHealth Koori Health Research and Community Development Unit, 2002). The literature stresses that developing and maintaining research partnerships requires major investments of time from both community participants and researchers.
Sympathetic approaches by researchersThe approach of individual researchers is critical for effective CPR. Support for research partnership must be genuine and should be demonstrated to the satisfaction of the community both in words and in action. Trust is essential to any research partnership and must be earned over time by sensitive and considerate interaction with the community (Pyett, 2002). It is important also that research be conducted in an ethical manner if all parties are to remain committed to the process (Parkin, 2004).
Some researchers have far better skills in community liaison than others and thus find it easy to work with CLOs or to undertake the role themselves (Tattam, 2006). People bring their other work and life experience to research and having worked with disadvantaged communities in the past is clearly an advantage in CPR, as a CLO told us:
Basically some people are better at it than others. Better at talking to people outside academia. Academics that have worked somewhere else like the community sector understand why you need to adjust the way you present and the way you talk, or how you communicate it, and the need for it to be applied.
Researchers, community representatives and CLOs participating in this study advised that some researchers require training in effective CPR. When approaching a new or unfamiliar community, and particularly when approaching Indigenous organisations, researchers should do some background reading to save community partners time informing them of the community’s history or of particular sensitivities around research within that community. A community
6. Suggestions for supporting CPR

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
37
Community members emphasised the importance of researchers having a respectful attitude to community partners and willingness to adjust the project in accordance with community needs.
representative advised that researchers should draft a clear and concise statement of their aims when approaching any agency seeking support for research. Some community representatives also suggested that researchers would benefit from training in communicating research findings to a non-specialist audience.
Other participants noted the importance of researchers ‘giving back’ to communities, not just through knowledge exchange but also in practical ways. These might be writing letters of support, providing references, offering training, or sitting on agency boards. Community members emphasised the importance of researchers having a respectful attitude to community partners and willingness to adjust the project in accordance with community needs, as outlined above.
One community worker whose agency had contributed significantly to research projects said that the organisation concerned would appreciate more than a mention in the acknowledgement section of reports. This worker did not believe that the agency should be credited with the same responsibility for the report as the research body, but wondered whether the agency’s logo might be included on future publications to which they had contributed significantly.
North American community partners have called to be paid for their contribution to research projects (Community-Campus Partnerships for Health, 2007). The NHMRC has advised that research funding should cover sitting fees for community members as well as reimbursing participation costs (such as transport) (National Health and Medical Research Council & Consumers’ Health Forum of Australia, 2004). Many community representatives interviewed for this study were in paid positions and these workers did not believe they needed to be financially reimbursed for contribution. Community volunteers, however, felt strongly that they should be given some recompense for their input, as did workers in non-government agencies who felt that participating in research was not part of their core funded business.
Recommendation: Researchers undertaking community-engaged research should be prepared to invest time in building relationships and should seek ways to ensure that participants benefit from involvement.
Recommendation: Research negotiations should include consideration of appropriate and respectful ways of acknowledging community partners, participants and co-authors and, with the approval of community partners, the placing of relevant logos on reports and other publications.
Recommendation: Research proposals should include funding to reimburse community participants who are not undertaking their role as part of paid employment.
Dedicated CPR funding Funding bodies should adopt policies that support community engagement where this is relevant or necessary for ethical and effective research (Israel et al., 1998). Policies to support CPR might

Knowledge forCommon Good
38
Some writers have argued that community members without academic credentials should be recognised by funding bodies as legitimate principal investigators on research projects, and that funding should be made available to train and mentor community members in grant writing and research
entail dedicated funding streams, provision of seeding funding, and awards schemes for CPR (Flicker & Savan, 2006). Grant assessment procedures may need to be adapted to ensure a fair hearing for CPR projects. Funding assessment processes have included community members as reviewers on grant applications for collaborative research (Saunders, Crossing, Girgis, Butow, & Penman, 2007; Seifer & Green-Morton, 2007; Street et al., 2007) or on funding research priority decision making bodies (National Health and Medical Research Council, 2004). In order to track the proportion of research funding going to support CPR, funding bodies should report how many successful grants incorporate community collaboration (Seifer & Green-Morton, 2007). Some writers have argued that community members without academic credentials should be recognised by funding bodies as legitimate principal investigators on research projects, and that funding should be made available to train and mentor community members in grant writing and research (Maurrasse, 2002; Seifer & Green-Morton, 2007; Street et al., 2007). Seifer and Green-Morton (2007) also argue that the usual funding periods of two to five years are insufficient for research involving community partners. They note that the National Institute of Health National Center on Minority Health and Health Disparities provides three year planning grants, five year implementation grants and additional three year dissemination grants.
CPR has specific resourcing requirements. As mentioned above, reimbursement should be available for expenses incurred by research participants (National Health and Medical Research Centre & Consumers’ Health Forum of Australia, 2004). This may include money for childcare, meeting sitting fees, translation of project materials and catering (Flicker & Savan, 2006).
Participants in this project offered recommendations for Australian research funding bodies. One researcher suggested that NHMRC and ARC submission forms might include a section asking whether the project will require additional funding for any particular reason due to requirement for community engagement or the sensitivity of the research environment. This could be used to justify requests for funding to employ a CLO.
Some funding schemes encourage co-contribution to research projects. For instance, the ARC Linkage Projects scheme requires researchers to identify industry partners that can pledge contributions. A researcher interviewed argued that it is difficult to secure funding for research partnerships involving non-government agencies and that hence we ‘need more relaxed rules for some of these smaller agencies’.
It is striking how many of the projects sampled were made possible by the award of a VicHealth Public Health or Senior Health Fellowship to a key researcher. These five year fellowships support researchers to undertake a sustained program of research in communities or settings of particular need. Fellowship recipients acknowledged that these awards enabled them to invest time in building relationships

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
39
It is timely therefore to argue for the importance of counting community reports and other forms of knowledge exchange as legitimate forms of academic output ...
through the early phases of research, sometimes with little short-term research output to show for this work:
Without a VicHealth five year fellowship I never could have done what I’m doing. If I were to try to do what I’m doing under ARC or NHMRC [funding] I couldn’t have done it – no way.
Recommendation: Research funding bodies should recognise the need for community liaison support in projects that entail extensive community involvement.
Recommendation: Funding bodies should consider establishing specific CPR funding programs to include the time requirements for research establishment, implementation and dissemination and to reimburse communities for their participation.
Measuring CPR as academic activity and outputResearchers and CLOs interviewed for this study argued that undertaking CPR disadvantaged them in two ways. First, they believed that community engagement should be recognised as part of an academic workload within performance appraisal mechanisms for both academics and CLOs. Participants argued that university-based performance assessment tools should measure CPR activities such as attending community meetings, providing research feedback and conducting negotiations over new projects. Researchers argued also that measures should be included to assess the impact of academic work on policy, practice or communities:
We do need to account for our activity … Indicators need to cut across from activities to outputs to outcomes.
Second, participants argued that community reports or other forms of knowledge dissemination should be counted as academic outputs. We noted above that the Federal Government has announced plans to dismantle the RQF and introduce a new mechanism for assessing academic output and research quality, to be called ‘Excellence for Research in Australia’. Specific measures have not been announced at the time of writing but will include assessment evaluation by leading researchers in disciplinary clusters. The system ‘will assess research quality using a combination of metrics and expert review by committees comprising experienced, internationally-recognised experts’ (Carr, 2008). Metrics for assessing research performance may vary across disciplines within this system. It is timely therefore to argue for the importance of counting community reports and other forms of knowledge exchange as legitimate forms of academic output and to include measures within academic performance metrics that assess the impact of CPR on disadvantaged communities.
Recommendation: Academic performance appraisal tools utilised by universities and funding bodies should include metrics for community engagement activities related to negotiating and conducting partnership research and participating in knowledge exchange.

Knowledge forCommon Good
40
Universities must also adopt supportive policies if researchers are to be encouraged to conduct collaborative community research.
Recommendation: The University of Melbourne should advocate that community reports and other forms of knowledge exchange be counted as academic outputs under the new Excellence in Research for Australia system, and that measures be developed to assess impact of CPR research with disadvantaged communities.
Supportive faculty and centre governance Universities must also adopt supportive policies if researchers are to be encouraged to conduct collaborative community research. University promotion committees must recognise the challenges of CPR and the different kinds of research outcomes (such as community reports and training materials) produced through community engagement (Norris et al., 2007). Education should be provided for researchers on the benefits of collaborative approaches to research and how to initiate and conduct it (Flicker & Savan, 2006; Norris et al., 2007).
Research participants advised that many practical measures can be and have been taken within faculties and research centres to support CPR. Complex administrative arrangements can be an impediment when researchers require access to funds (sometimes cash) to pay research participants. Other resources such as availability of pool cars can be of great value to researchers who are frequently required to travel to visit community partners or share research findings. Working with communities can entail significant administrative workloads for researchers; for instance, issuing invitations or mailing out reports. In the absence of administrative capacity within research centres, researchers and CLOs frequently undertook these roles themselves. Additional administrative assistance was therefore recommended by study participants. The NHMRC and Consumers’ Health Forum recommend that research teams or organisations encourage community participation by posting web pages describing opportunities for input, involving community members in planning and priority setting mechanisms, establishing a community advisory committee and allocating funds for participation (National Health and Medical Research Council & Consumers’ Health Forum of Australia, 2004).
Emotional and interpersonal support for CPR is also important. Researchers frequently spoke of appreciation for their research centre colleagues’ interest in their work and willingness to tolerate their frequent absence from the office while on community visits. Fostering a culture within universities where CPR is a valued methodological approach is one means of encouraging this form of research.
Recommendation: Research centres develop flexible administrative systems to facilitate community engagement in research.
Encouraging knowledge exchangeAs we observed above, active strategies are most effective in ensuring knowledge exchange (Huberman, 1994). Research projects

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
41
Community liaison officers can help create a culture within research centres of commitment to conducting knowledge exchange with relevant communities, policy makers and practitioners.
which have the broadest range of impacts are often those which have used multiple methods for knowledge exchange (Nutley et al., 2007). Case studies outlined in Section 3 of this report provide examples of researchers’ and CLOs’ strong commitment to knowledge exchange.
Some participants in this research advised that knowledge exchange is facilitated by involving community partners in the initial planning of the project. This way the research would be more likely to be relevant to community needs and others besides the researchers would feel ownership of findings:
To me that role is about relationship developing at the beginning, because if you’ve got people working with you they’re ‘busting’ for the research results. We never had to disseminate this stuff ... People say to us ‘When will the report be out? I really need it!’ (CLO)
Involving community partners in the initial and subsequent phases of research is not always practical but should be practised wherever possible.
Mitchell and Walsh (2003) argue that community liaison staff are well placed to disseminate research findings. Nutley and colleagues (2007) recommend similarly that dedicated ‘knowledge brokers’ – individuals or agencies – be funded to work with researchers and agencies to translate research findings for practitioners and communicate research needs to universities. Lomas advocates for employment of ‘retailers’ who are credible to both academic staff and community members to actively disseminate research findings (Lomas, 1993 cited in Mitchell & Walsh, 2003). CLOs can help create a culture within research centres of commitment to conducting knowledge exchange with relevant communities, policy makers and practitioners (Mitchell & Walsh, 2003; Tattam, 2006).
Participants noted that experienced CLOs are able to help researchers plan a strategic approach to knowledge exchange, for instance through proactively arranging meetings with government officials (Mitchell & Walsh, 2003). A couple of researchers commented that CLOs were really useful in helping them pitch their research messages effectively to interest specific people or groups.
Some research participants suggested that CLOs should be conceptualised as knowledge exchange specialists. Knowledge exchange is an important part of the role which CLOs have developed at ARCSHS. Employees of the University of Melbourne interviewed for this project believed that the University’s interest in knowledge transfer might be used as leverage to secure funding to employ CLOs in research centres. The case studies described in this report show, however, that some CLOs are employed specifically to maintain relationships during research data generation and collection phases, and that research exchange is not always central to the CLO role. While the CLO role must be broader than knowledge exchange, this function is increasingly understood as important within universities and offers opportunities to demarcate an area of expertise for these staff.

Knowledge forCommon Good
42
A couple of interviewees objected to the university’s use of the term ‘knowledge transfer’ preferring ‘knowledge exchange’ as implying a more equitable relationship where all parties have important information to share.
Funding bodies and universities can develop strategies to support researchers to engage in knowledge exchange. Appropriate research dissemination resources are difficult to secure though funding bodies (Flicker & Savan, 2006; Israel et al., 1998; Norris et al., 2007; Parkin, 2004). In Canada, funds provided by Health Canada for communication activities are quarantined from expenditure on other items (Parkin, 2004).
A number of our research participants commented that knowledge exchange activities must be funded through the university or built into funding proposals to ensure that they occur: ‘knowledge transfer falls to the bottom of the pile because there’s no money [for it]’. A CLO argued also that staff should be employed on an ongoing basis rather than on short-term contracts so that they would still be around after research projects conclude to ensure knowledge transfer occurs:
Otherwise the work stops when the grant runs out. And that is the time that you really need to do the research transfer.
A couple of interviewees objected to the university’s use of the term ‘knowledge transfer’ preferring ‘knowledge exchange’ as implying a more equitable relationship where all parties have important information to share. This term is consistent with a partnership approach to conducting research.
Recommendation: Research projects addressing health and social disadvantage should include plans for knowledge exchange involving communities and community representatives.
Recommendation: The University of Melbourne should adopt the term ‘knowledge exchange’ in preference to ‘knowledge transfer’ to convey the importance of respecting the knowledge and understanding that both university and community partners bring to research.
Recommendation: Researchers should consider engaging communities in the initial planning of projects as a means of optimising opportunities for input and knowledge exchange.Recommendation: University award schemes should continue to recognise and encourage innovative forms of knowledge exchange.
Enhancing capacity for community liaison in universitiesThree main suggestions were made for enhancing community liaison at universities: establishing a centre for CPR, employing additional CLOs, and setting up CPR fellowships.
Many participants advocated that central university support for CPR is required. A couple of participants suggested that some kind of centre for community engagement and research exchange would help to ensure these processes remain a priority within the university and to develop CPR as a respected research methodology:
It would go an enormous distance to improving the situation if they acknowledge that this was a critical part of research and what research is for. Just like they’ve got a research and graduate

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
43
Where community liaison officers are employed, it is critical that roles be carefully defined, work be acknowledged and recognised, and moves be initiated to develop a career structure.
studies office and a magazine. If they actually supported some central capacity for this kind of thing or supported a few positions in key research areas. Maybe if some process like the RQF starts to attach federal funding to those kind of runs on the board, that might happen. But at the moment I’ve never really seen much acknowledgement that this is a legitimate activity for a university to engage in ... There’s more the idea that research will just diffuse itself into the community rather than somebody will actively play that role. (CLO)
Much of the discussion generated at interviews for this research centred on experiences of employing CLOs or working as a CLO. Community liaison works well where it receives high level support from centre directors and where a distinct role has been established (Mitchell & Walsh, 2003; Tattam, 2006). Participants frequently referred to community liaison at ARCSHS and community development at Onemda as models they would like to see replicated elsewhere. Community development or liaison staff have been employed at both ARCSHS and Onemda since their inception and each body now has teams of workers. At Onemda community engagement is seen as essential to research and so community development staff are in no doubt as to their importance within the Unit. At ARCSHS the community liaison team is similarly well-established and researchers have come to value community engagement. CLOs have been awarded independently sourced funding and work relatively autonomously on some projects. This suggests that a critical mass of CLOs employed in a centre or unit over a number of years may help to establish respect for the role and develop clear and recognised functions within research centres or faculties.
Challenges for CLOs described above (at Section 5) include lack of clarity about the role, managing conflicting demands of researchers and communities, and issues relating to performance assessment, career structure and sense of value. Researchers seeking funding to employ CLOs should ensure that, as much as possible, the tasks to be allocated are functions they are happy to hand over and are not predominantly administrative. Where CLOs are employed, it is critical that roles be carefully defined, work be acknowledged and recognised, and moves be initiated to develop a career structure. If their employment is ongoing, CLOs should be encouraged to seek funding for discrete projects in cooperation with researchers. Because of the risks of isolation for staff in community liaison roles, we believe that CLOs should be employed in teams wherever possible. Establishing a professional network of CLOs and researchers who work closely with these staff might assist people to address issues around CLO roles, performance assessment, career structure and sense of value.
The question of whether centres should appoint community liaison staff to work across multiple projects is a difficult one. For instance, the McCaughey Centre within the School of Population Health has diverse research interests and engages with a correspondingly heterogeneous set of communities. A researcher doubted that one

Knowledge forCommon Good
44
This suggests that there are currently opportunities to develop community liaison within universities and to seek funding to employ additional staff in these roles.
CLO could work across the centre: ‘we don’t have a unified work agenda at the McCaughey Centre so we would require multiple people [as CLOs]’. Nonetheless other research participants observed that CLOs at both ARCSHS and KCWHS were required to engage with many different communities and issues:
It was not uncommon for me to working on homelessness one day, IVF another day and obesity later in the week. (CLO)
A researcher suggested that another way to enhance CPR would be to employ professional researchers with expertise in CPR methodologies to lead CPR research within faculties or research centres, for instance as research chairs or research fellows. These people would advise other researchers and develop a focus for CPR: ‘we need someone to take some leadership in this methodological skill’. Professional researchers may well be more able than CLOs to develop a focus for CPR in universities.
Mitchell and Walsh (2003) have argued that dedicated funding lines are required to demonstrate an institution’s commitment to community liaison. The NHMRC recommends that funding organisations provide resources for ‘consumer participation facilitators’ in key research agencies for at least several years’ duration (National Health and Medical Research Council & Consumers’ Health Forum of Australia, 2004: 26). La Trobe University now contributes to funding a CLO position at ARCSHS. This suggests that there are currently opportunities to develop community liaison within universities and to seek funding to employ additional staff in these roles.
Recommendation: A network of community liaison staff and researchers who work with them should be established at the University of Melbourne to clarify the role, develop performance indicators and explore options for career development.
Recommendation: The University of Melbourne should consider establishing research fellowships specifically for collaborative and participatory research.

The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
45
The literature suggests that collaborative participatory research is an excellent means to actively support research exchange, particularly with communities experiencing marginality or discrimination.
This report has described some of the mechanisms used within universities to promote the engagement of disadvantaged communities in health research. We have outlined difficulties faced by those attempting CPR and made suggestions as to how CPR might be supported. Only a small number of directly health-related community research activities within five research centres have been considered here. If we were to look more broadly we would find CPR models operating in centres and faculties outside the health arena. Further research might investigate how CPR at universities is differently conceptualised and implemented across disciplinary boundaries and how these approaches could be supported by funding bodies and university administrations.
Even within health research, however, CPR embraces diverse approaches. Community research partners varied widely between projects. Some researchers built links with local members of the community concerned, such as injecting drug users, while others focused on forging partnerships with service providers or employees of peak bodies working within disadvantaged communities. Researchers in some case studies described here maintained long-term relationships with community partners over a series of projects while other engagements were for a specific project. Most approaches to CPR in this report are investigator-driven. This means that they are instigated by researchers and – although they incorporate community consultation and participation – university partners retain ultimate control. Aboriginal health research agencies are notable for their dedication to developing equal relationships with community partners (National Health and Medical Research Council, 2004). Supporting Aboriginal self-determination is for instance part of Onemda’s vision statement and staff are committed to ensuring that research is conducted with strong community support, involvement and input.
The literature suggests that CPR is an excellent means to actively support research exchange, particularly with communities experiencing marginality or discrimination. The University of Melbourne has endorsed a ‘triple helix’ commitment to supporting knowledge transfer as an integral strand of its role, alongside research and teaching. This offers an opportunity to advocate for greater recognition of CPR as a means of promoting research exchange. Moreover, the introduction by the Federal Government of a new system of research output measurement makes it an excellent time to argue for recognition of community reports and other forms of non-peer reviewed publications as legitimate academic outputs.
A key issue in institutional arrangements to support CPR is whether to fund and employ dedicated CLOs. This has worked well in centres where teams of CLOs are employed and where their role is understood and valued by researchers. Other options that might be explored for supporting community liaison would be establishing research chair or fellow positions with a focus on CPR or networks for university staff engaged in community liaison.
7. Conclusions

Knowledge forCommon Good
46
Participants in this research observed a contradiction between moves toward making universities more entrepreneurial and competitive and, at the same time, encouragement from funding bodies for researchers to incorporate mechanisms for community participation. This tension must be negotiated if researchers and universities are to work successfully with communities that are experiencing disadvantage.
The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
47
Anderson, Warwick P. (2006). Working to build a healthy Australia: a new era for the NHMRC. Medical Journal of Australia, 185(11/12), 613-615.
Atkinson, P., & Hammersley, M. (1998). Ethnography and participant observation. In N. K. Denzin & Y. S. Lincoln (Eds.), Strategies of Qualitative Inquiry (pp. 110–137). Thousand Oaks, CA: Sage.
Bourdieu, P. (1996). Understanding. Theory, Culture and Society, 13(2), 17-37.
Brannen, Julia. (2002). The use of video in research dissemination: children as experts on their own family lives. International Journal of Social Research Methodology, 5(2), 173-180. Retrieved 18 December 2007 from http://search.ebscohost.com/login.aspx?direct=true&db=a9h&AN=6814374&site=ehost-live.
Butler, Linda. (2003). Modifying publication practices in response to funding formulas. Research Evaluation, April, 39-46.
Carr, Kim. (2008). New era for research in quality: announcement of Excellence in Research for Australia. Canberra: Innovation, Industry, Science and Research: Ministers and Parliamentary Secretary. Retrieved 3 April 2008 from http://www.minister.industry.gov.au/senatorthehonkimcarr/pages/neweraforresearchquality.aspx.
Cawson, Peter G., Mercer, Stewart W., & Barbour, Rosaline S. (2007). Involving deprived communities in improving the quality of primary care services: does participatory action research work? BMC Health Services Research, 7(1), 88-96.
Chataway, Cynthia J. (1997). An examination of the constraints on mutual inquiry in a participatory action research project. Journal of Social Issues, 53(4), 747-765.
Cochran, Patricia A.L., Marshall, Catherine A., Garcia-Downing, Carmen, Kendall, Elizabeth, Cook, Doris, McCubbin, Laurie, & Gover, Reva Mariah S. (2007). Indigenous ways of knowing: implications for participatory research and community. American Journal of Public Health, 98(1), 8-13.
Community-Campus Partnerships for Health. (2007). Achieving the Promise of Authentic Community-Higher Education Partnerships: Community Partners Speak Out! Seattle, WA: Community-Campus Partnerships for Health. Retrieved 25 February 2007 from www.ccph.info.
Croft, Suzy, & Beresford, Peter. (1992). The politics of participation. Critical Social Policy, 12(35), 20-44.
Fitzgerald, John L., McDonald, Kevin, & Klugman, Matthew. (2004). Unspoken But Ever Present:
Hepatitis C in a Regional Setting. Melbourne: The University of Melbourne.
Flicker, Sarah, & Savan, Beth. (2006). A Snapshot of CBR in Canada: Wellesley Institute. Retrieved 20 December 2007 from http://wellesleyinstitute.com/files/CBR_snapshot.pdf.
Fook, Janis (Ed.). (1996). The Reflective Researcher: social workers’ theories of practice research. St Leonards, NSW: Allen & Unwin.
Gano, G.L., Crowley, J.E., & Guston, D. (2007). “Shielding” the knowledge transfer process in human service research. Journal of Public Administration Research and Theory, 17(1), 39-90.
Hamilton, V. (in press). Voices from the field. Address at the launch of ‘Work and Health in the Latrobe Valley: Community Perspectives on Asbestos Issues’, September 2004. New Solutions: A Journal of Environmental and Occupational Health Policy.
Hertz, Rosanna (Ed.). (1997). Reflexivity and Voice. Thousand Oaks: Sage.
Hillier, Lynne, Dempsey, Deborah, Harrison, Lyn, Beale, Lisa, Matthews, Lesley, & Rosenthal, Doreen. (1998). Writing Themselves In: A National Report on the Sexuality, Health and Well-being of Same-Sex Attracted Young People. Melbourne: National Centre in HIV Social Research and Australian Research in Sex, Health and Society.
Hillier, Lynne, Mitchell, Anne, Besley, Nicole, & Lavin, Andrew. (nd). Outsmarting Homophobia. Melbourne: Australian Research Centre for Sex, Health and Society.
Hillier, Lynne, Turner, Alina, & Mitchell, Anne. (2005). Writing Themselves In Again: 6 Years On. Melbourne: Australian Research Centre in Sex, Health and Society.
Huberman, A.M., & Miles, M.B. (1994). Data management and analysis methods. In N.K. Denzin & Y.S. Lincoln (Eds.), Handbook of Qualitative Inquiry (pp. 428–444). Thousand Oaks: Sage.
Huberman, Michael. (1994). Research utilization: the state of the art. Knowledge and Policy, 7(4), 13-33.
Hunter, Cecily, & LaMontagne, Anthony D. (in press). Work and illness in the Latrobe Valley: investigating ‘community’ through a history of responses to asbestos-related disease in an Australian industrial region. Social History of Medicine, (accepted 18 Jan 2008).
Israel, Barbara A., Schultz, Amy J., & Parker, Edith A. (1998). Review of community-based research: assessing partnership approaches to improve
References
Knowledge forCommon Good
48
public health. Annual Review of Public Health, 19, 173-202.
Israel, Barbara A., Schultz, Amy J., Parker, Edith A., Becker, Adam B., Allen, Alex J., & Guzman, J. Ricardo. (2003). Critical issues in developing and following community based participatory research principles. In M. Minkler & N. Wallerstein (Eds.), Community-Based Participatory Research for Health (pp. 53-76). San Francisco: Jossey-Bass.
Jack, G. (2005). Assessing the impact of community programmes working with children and families in disadvantaged areas. Child and Family Social Work, 10, 293-304.
Jacobs, Kerry, & Barnett, Pauline. (2000). Policy transfer and policy learning: A study of the 1991 New Zealand Health Services Taskforce. Governance, 13(2), 185. Retrieved 19 December 2007 from http://search.ebscohost.com/login.aspx?direct=true&db=a9h&AN=3171472&site=ehost-live.
Kavanagh, Anne, Thornton, Lukar, Tattam, Amanda, Thomas, Lyndal, Jolley, Damian, & Turrell, Gavin. (2007). Place Does Matter for Your Health: A Report of the Victorian Lifestyle and Neighbourhood Environment Study. Melbourne: University of Melbourne.
Keys, Deb, Mallett, Shelley, & Rosenthal, Doreen. (2006). Giving up on drugs: homeless young people and self-reported problematic drug use. Contemporary Drug Problems(33), 63-98.
LaMontagne, A.D., Hunter, C., Vallance, D., & Holloway, A.J. (in press). Asbestos disease in Australia: looking forward and looking back. New Solutions: A Journal of Environmental and Occupational Health Policy.
LaMontagne, Anthony D., & Walker, Hannah H. (2005). Community views on responding to a local asbestos disease epidemic: implications for policy and practice. Policy and Practice in Health and Safety, 3(1), 69-84.
Lang, Eddy S., Wyer, Peter C., & Haynes, R. Brian. (2007). Knowledge translation: closing the evidence-to-practice gap. Annals of Emergency Medicine, 49(3), 355-363. Retrieved 12 October 2007 from http://www.sciencedirect.com/science/article/B6WB0-4M8775P-3/2/92aa1487e1371dd01c73ac5b4544e9a0.
Lavis, John N., Lomas, Jonathan, Hamid, Maimunah, & Sewamkambo, Nelson K. (2006). Assessing country-level efforts to link research to action. Bulletin of the World Health Organization, 84(8), 620-628.
Lavis, John N., Robertson, Dave, Woodside, Jennifer M., McLeod, Christopher B., & Abelson, Julia. (2003). How can research organizations more effectively transfer research knowledge to decision makers? Milbank Quarterly, 81(2), 221-248. Retrieved 20 December 2007 from http://search.ebscohost.com/login.aspx?direct=true&db=a9h&AN=9751023&site=ehost-live.
Maguire, Patricia. (1987). Doing Participatory Research: a feminist approach. Amherst: University of Massachusetts.
Mallett, S., Edwards, J., Keys, D., Myers, P., & Rosenthal, D. (2003). Disrupting Stereotypes: Young People, Drug Use and Homelessness. Melbourne: The Key Centre for Women’s Health in Society.
Mallett, Shelley, Keys, Deb, & Rosenthal, Doreen. (2005). 674 A pocket guide to keeping well on the streets. Melbourne: Key Centre for Women’s Health in Society.
Marshall, Judi, & McLean, Adrian. (1988). Reflection in action: exploring organizational culture. In P. Reason (Ed.), Human Inquiry in Action: developments in new paradigm research (pp. 199-220). London: Sage.
Matthews, Sally, Frommer, Michael, Tjhin, Michelle, & Rubin, George. (2001). When research reports and academic journals are clearly not enough: strengthening links between Aboriginal health research and health outcomes. Darwin: Cooperative Research Centre for Aboriginal and Tropical Health.
Maurrasse, David J. (2002). Higher education-community partnerships: assessing progress in the field. Nonprofit and Voluntary Sector Quarterly, 31(1), 131-139.
Mitchell, Anne, & Walsh, Jenny. (2003). The community liaison model of research transfer. In V. Lin & B. Gibson (Eds.), Evidence-Based Health Policy: Problems and Possibilities (pp. 263-271). Melbourne: Oxford University Press.
National Health and Medical Research Centre, & Consumers’ Health Forum of Australia. (2004). A Model Framework for Consumer and Community Participation in Health and Medical Research. Canberra: Commonwealth of Australia.
National Health and Medical Research Council. (2004). Resource Pack for Consumer and Community Participation in Health and Medical Research. Canberra: Commonwealth of Australia. Retrieved 14 April 2008 from http://www.nhmrc.gov.au/publications/synopses/_files/r34.pdf.
The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
49
National Health and Medical Research Council (2005). Keeping research on track: a guide for Aboriginal and Torres Strait Islander peoples about health research ethics. Canberra, AGPS.
National Health and Medical Research Council, & Consumers’ Health Forum of Australia. (2001). Statement on Consumer and Community Participation in Health and Medical Research. Canberra: Commonwealth of Australia. Retrieved 14 April 2007 from http://www.nhmrc.gov.au/publications/synopses/_files/r22.pdf.
National Health and Medical Research Council, & Consumers’ Health Forum of Australia. (2004). A Model Framework for Consumer and Community Participation in Health and Medical Research. Canberra: Commonwealth of Australia.
Norris, Keith C., Brusuelas, Rebecca, Jones, Loretta, Miranda, Jeanne, Duru, Kenrik, & Mangione, Carol M. (2007). Partnering with community-based organizations: an academic institution’s perspective. Ethnicity and Disease, 17(Winter), S127-S132.
Nutley, Sandra M., Walter, Isabel, & Davies, Huw T.O. (2007). Using Evidence: How Research Can Inform Public Services. Bristol: The Policy Press.
Ollis, Debbie, Mitchell, Anne, Watson, Jan, Hillier, Lynne, & Walsh, Jenny. (nd). Safety in Our Schools: Strategies for Responding to Homophobia. Melbourne: Australian Research Centre for Sex, Health and Society.
Onemda VicHealth Koori Health Unit. (2008a). About us: history. Retrieved 27 February 2008 from http://www.onemda.unimelb.edu.au/about/history.html.
Onemda VicHealth Koori Health Unit. (2008b). Community Development. Retrieved 27 February 2008 from http://www.onemda.unimelb.edu.au/community/.
Parkin, Rebecca T. (2004). Communications with research participants and communities: foundations for best practices. Journal of Exposure Analysis and Environmental Epidemiology, 14, 516-523.
Petras, Elizabeth McLean, & Porpora, Douglas V. (1993). Participatory research: three models and an analysis. American Sociologist, 24(1), 107-126.
Pick, David. (2006). The re-framing of Australian higher education. Higher Education Quarterly, 60(3), 229-241.
Pyett, P. (2002). Working together to reduce health inequalities: reflections on a collaborative participatory approach to health research.
Australian and New Zealand Journal of Public Health, 26, 332–336.
Pyett, Priscilla. (2007). Fetal Alcohol Syndrome: A Literature Review for the ‘Healthy Pregnancies, Healthy Babies for Koori Communities’ Project. Melbourne: State of Victoria.
Pyett, Priscilla, & VicHealth Koori Health Research and Community Development Unit. (2002). Towards reconciliation in Indigenous health research: the responsibilities of the non-Indigenous researcher. Contemporary Nurse, 14(1), 56-65.
Reason, Peter. (1994). Three approaches to participative inquiry. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of Qualitative Research (pp. 324-339). Thousand Oaks, CA: Sage.
Rosenthal, Doreen, Mallett, Shelley, Keys, Deb, & Edwards, Judy. (nd). Young People’s True Stories. Melbourne: Key Centre for Women’s Health in Society, University of Melbourne.
Rossiter, Ben. (2000). The place of research. Parity, 13(9). Retrieved 11 February 2008 from http://www-test.kcwh.unimelb.edu.au/projecti/research/article01.pdf.
Roussel, Amy E., Fan, Nancy L., & Fulmer, Erika. (2002). Identifying Characteristics of Successful Researcher/Community-based Organization collaboration in the Development of Behavioural Interventions to Prevent HIV Infection. Research Triangle Park, NC: Health, Social and Economics Research. Retrieved 21 December 2007 from http://ctsi.ucsf.edu/documents/Lit_Smry_2002.pdf.
Sandelowski, Margarete, Trimble, Frank, Woodard, Elizabeth K., & Barroso, Julie. (2006). From Synthesis to script: transforming qualitative research findings for use in practice. Qualitative Health Research, 16(10), 1350-1370. Retrieved 18 December, 2007 from http://qhr.sagepub.com/cgi/content/abstract/16/10/1350
Sapienza, Jessica N., Corbie-Smith, Giselle, Keim, Sarah, & Fleischman, Alan R. (2007). Community engagement in epidemiological research. Ambulatory Pediatrics, 7(3), 247-252.
Saunders, Carla, Crossing, Sally, Girgis, Afaf, Butow, Phyllis, & Penman, Andrew. (2007). Operationalising a model framework for consumer and community participation in health and medical research. Australian and New Zealand Health Policy, 4(13), 1-6.
Seifer, Sarena D., & Green-Morton, Ella. (2007). Realizing the promise of community-based participatory research: community partners
Knowledge forCommon Good
50
get organized! Progress in Community Health Partnerships: Research, Education and Action, 1.4(Winter), 291-294.
Stake, R.E. (1998). Case studies. In Y. S. Lincoln & N. K. Denzin (Eds.), Strategies of Qualitative Inquiry (pp. 86–106). Thousand Oaks, CA: Sage Publications.
Street, Jackie, Baum, Fran, & Anderson, Ian. (2007). Developing a collaborative research system for Aboriginal health. Australian and New Zealand Journal of Public Health, 31(4), 372-378.
Swayne, G. (in press). Voices from the field. Address at the dedication of an asbestos disease memorial for waterside workers at Melbourne Docks, 24 November 2004. New Solutions: A Journal of Environmental and Occupational Health Policy.
Tattam, Amanda. (2006). Translating Research Ways of Working. Melbourne: Key Centre for Women’s Health, University of Melbourne.
The University of Melbourne. (2005). Growing Esteem... the University of Melbourne. Melbourne: University of Melbourne.
Thelwell, Mike. (2002). Research dissemination and invocation on the web. Online Information Review, 26(6), 413-420.
VicHealth Koori Health Research and Community Development Unit. (2000). We don’t like research...but in Koori hands it could make a difference. Melbourne: VicHealth Koori Health Research and Community Development Unit, University of Melbourne. Retrieved 9 April 2008 from http://www.onemda.unimelb.edu.au/docs/CR1-WeDontLike%20Research.pdf.
Viswnanathan, Meera, Ammerman, Alice, Eng, Eugenia, Gartlehner, Gerald, Lohr, Kathleen N., Griffith, Derek, Rhodes, Scott, Samuel-Hodge, Carmen, Maty, Siobhan, Lux, Linda, Webb, Lucille, Sutton, Sonya F., Swinson, Tammeka, Jackman,
Anne, & Whitener, Lynn. (2004). Community-based Participatory Research: Assessing the Evidence. Rockville, MD: RTI International - University of North Carolina. Retrieved 18 December, 2007 from http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat1a.chapter.44133.
Volker, Thomas. (2002). Conducting research with community agencies: meeting recruitment and collaboration challenges. Journal of Marital and Family Therapy, 28(1), 9-14.
Walker, Hannah, & LaMontagne, Anthony D. (2004). Work and Health in the Latrobe Valley: Community Perspectives on Asbestos Issues. Melbourne: Centre for the Study of Health and Society, University of Melbourne.
Walsh, Jenny. (1998). Keep it Simple Guide to Safe Sex. Canberra: Australian National Council on AIDS, Hepatitis C and Related Diseases.
Waples-Crowe, Peter, & Pyett, Priscilla. (2005). The Making of a Great Relationship: A Review of a Healthy Partnership Between Mainstream and Indigenous Organisations. Melbourne: Victorian Aboriginal Community Controlled Health Organisation.
Warr, Deborah. (2007). Outside the School Gates: A Model for Tackling Disadvantage and Promoting Participation in Preschool Education at the Meadowbank Early Learning Centre. Melbourne: Centre for Health and Society, University of Melbourne.
Warr, Deborah. (2004). ‘There’s good and bad everywhere you go’: Exploring local contexts for social capital. Melbourne: Centre for Health and Society, University of Melbourne.
Winter, Alexandra, Wiseman, John, & Muirhead, Bruce. (2005). Beyond Rhetoric: University-Community Engagement in Victoria. Brisbane: Eidos.
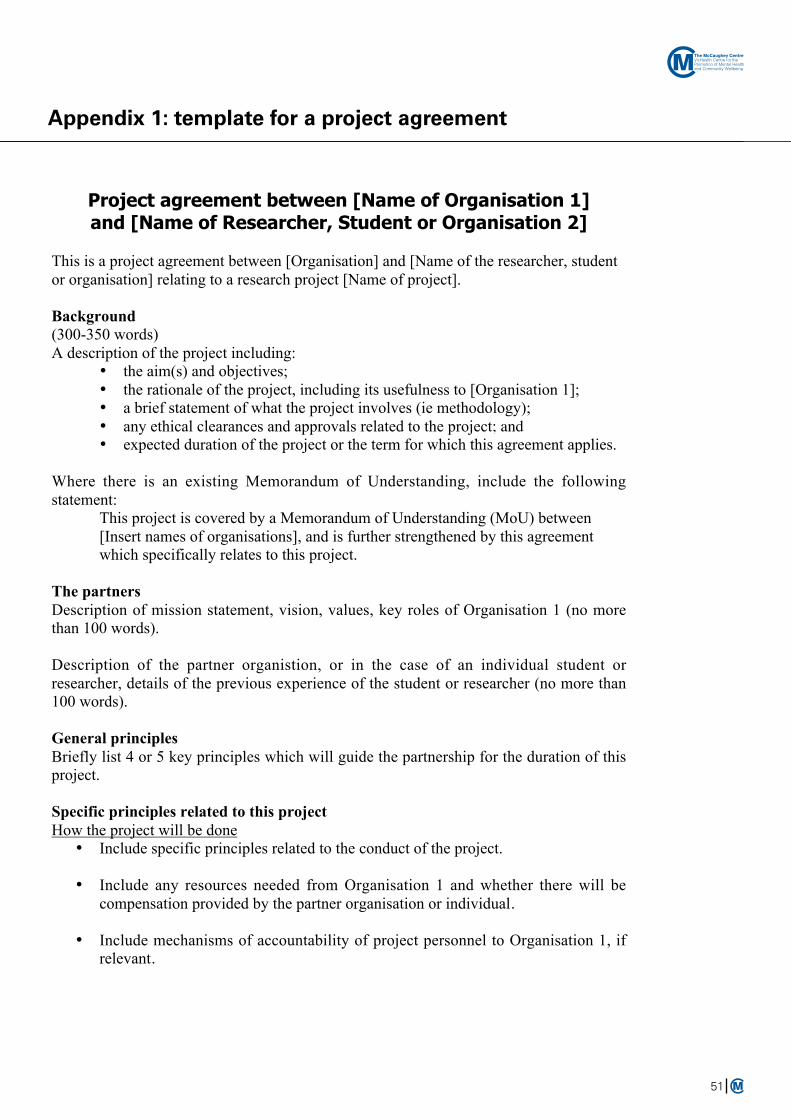
The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
51
Appendix 1: template for a project agreement
Project agreement between [Name of Organisation 1]and [Name of Researcher, Student or Organisation 2]
This is a project agreement between [Organisation] and [Name of the researcher, student
or organisation] relating to a research project [Name of project].
Background
(300-350 words)
A description of the project including:
• the aim(s) and objectives;
• the rationale of the project, including its usefulness to [Organisation 1];
• a brief statement of what the project involves (ie methodology);
• any ethical clearances and approvals related to the project; and• expected duration of the project or the term for which this agreement applies.
Where there is an existing Memorandum of Understanding, include the following
statement:
This project is covered by a Memorandum of Understanding (MoU) between
[Insert names of organisations], and is further strengthened by this agreement
which specifically relates to this project.
The partners
Description of mission statement, vision, values, key roles of Organisation 1 (no more
than 100 words).
Description of the partner organistion, or in the case of an individual student or
researcher, details of the previous experience of the student or researcher (no more than
100 words).
General principles
Briefly list 4 or 5 key principles which will guide the partnership for the duration of this
project.
Specific principles related to this project
How the project will be done
• Include specific principles related to the conduct of the project.
• Include any resources needed from Organisation 1 and whether there will be
compensation provided by the partner organisation or individual.
• Include mechanisms of accountability of project personnel to Organisation 1, if
relevant.
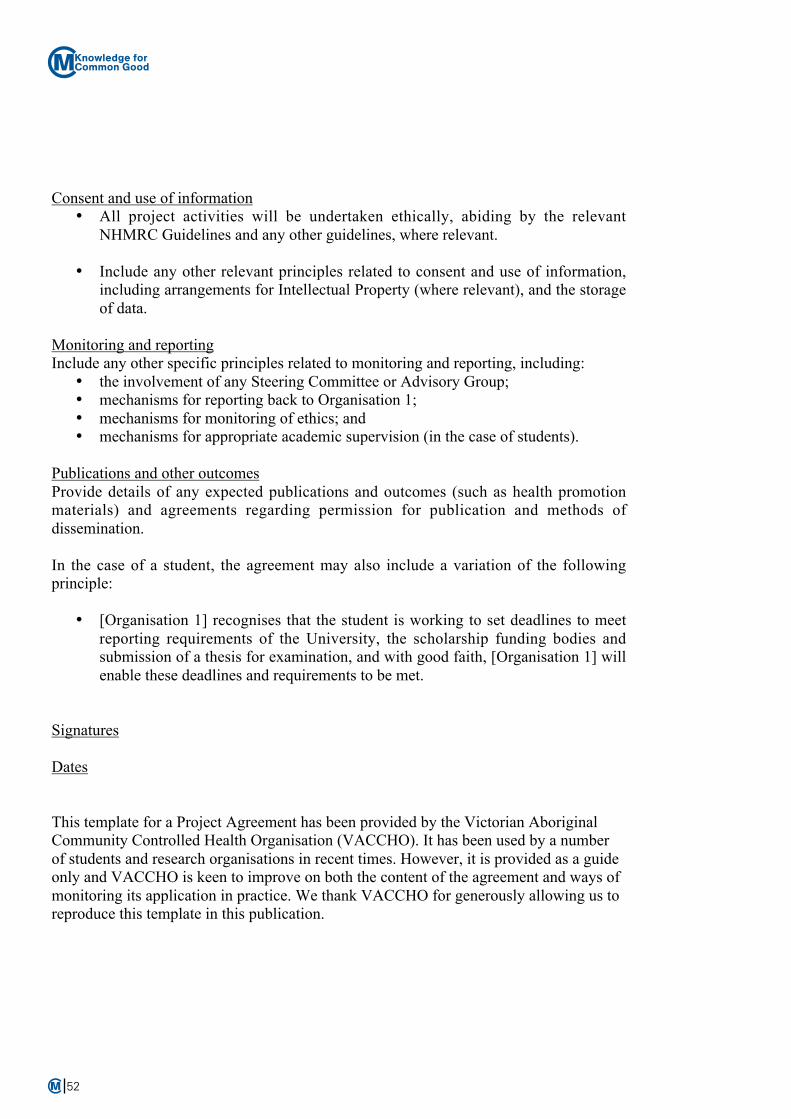
Knowledge forCommon Good
The McCaughey CentreVicHealth Centre for the Promotion of Mental Healthand Community Wellbeing
52
Consent and use of information
• All project activities will be undertaken ethically, abiding by the relevant
NHMRC Guidelines and any other guidelines, where relevant.
• Include any other relevant principles related to consent and use of information,
including arrangements for Intellectual Property (where relevant), and the storage
of data.
Monitoring and reporting
Include any other specific principles related to monitoring and reporting, including:
• the involvement of any Steering Committee or Advisory Group;
• mechanisms for reporting back to Organisation 1;
• mechanisms for monitoring of ethics; and
• mechanisms for appropriate academic supervision (in the case of students).
Publications and other outcomes
Provide details of any expected publications and outcomes (such as health promotion
materials) and agreements regarding permission for publication and methods of
dissemination.
In the case of a student, the agreement may also include a variation of the following
principle:
• [Organisation 1] recognises that the student is working to set deadlines to meet
reporting requirements of the University, the scholarship funding bodies and
submission of a thesis for examination, and with good faith, [Organisation 1] will
enable these deadlines and requirements to be met.
Signatures
Dates
This template for a Project Agreement has been provided by the Victorian Aboriginal
Community Controlled Health Organisation (VACCHO). It has been used by a number
of students and research organisations in recent times. However, it is provided as a guide
only and VACCHO is keen to improve on both the content of the agreement and ways of
monitoring its application in practice. We thank VACCHO for generously allowing us to
reproduce this template in this publication.

The McCaughey CentreVicHealth Centre for the Promotion of Mental Health and Community Wellbeing
Policy Signpost #2
Universities Working with and for Communities: Strategies for Collaborative Community Research and Knowledge Exchange
Sarah MacLean, Deborah Warr and Priscilla Pyett
Knowledge forCommon Good
July 2008
Published by The McCaughey Centre: VicHealth Centre for the Promotion of Mental Health and Community WellbeingMelbounre School of Population Health, The University of Melbourne, Level 5, 207 Bouverie Street, Victoria 3010 AustraliaTelephone: +61 (3) 8344 9101 Facsimile: +61 (3) 9348 2832
http://www.mccaugheycentre.unimelb.edu.au
© McCaughey Centre 2008
Policy Signpost #1Community Wellbeing in an Unwell World: Trends, Challenges and Opportunitieshttp://www.mccaugheycentre.unimelb.edu.au/pdf_library/Policy_signpost_1.pdf
ISBN 978-0-9804620-3-6
The McCaughey Centre: VicHealth Centre for the Promotion of Mental Health and Community Wellbeing,Melbourne School of Population Health,The University of Melbourne
Related Documents











