J Neural Transm [P-DSect] (1990) 2:249-264 Journal of, Neural Transmission by Springer-Verlag1990 The auditory P 300 correlates with specific cognitive deficits in Parkinson's disease S. Pang 1, J. C. Borod 1' 2, A. Hernandez 1' 2, I. Bodis-Wollner 1' 3, S. Raskin 2, L. Mylin l, L. Coscia 2, and M. D. Yahr 1 l Department of Neurology, Mount Sinai School of Medicine; 2Department of Psychology, Queens College of the City University of New York; 3Department of Ophthalmology, Mount Sinai School of Medicine, New York, U.S.A. Accepted June 15, 1990 Summary. An abnormally prolonged latency of the P 300 event-related potential has been reported in several types of dementing illnesses, including Parkinson's disease (PD). While some PD patients have dementia, a significant number of PD patients have less severe cognitive impairments. We examined the relation- ship between the auditory P 300 and a neuropsychological battery of 11 tasks in 43 PD patients. The quantitative relationship between the individual neu- ropsychological measures and the P 300 was examined using partial correlation and analysis of covariance techniques which controlled for age, education, and illness duration. The strongest correlations were between P 300 and both short- term memory and visual perception. Global cognitive deficits do not appear to relate to the abnormal P 300 responses in PD: instead, specific aspects of cog- nitive decline accounted for the electrophysiological abnormalities. An abnor- mally long or absent P300 correlated with deficits on select cognitive tasks: those involving memory, visual perception, and abstract reasoning. The inter- actions between anatomical and neurochemical abnormalities in PD are dis- cussed in light of the pattern of deficits seen in this study. Keywords: Parkinson's disease, P300, evoked potential, neuropsychological measures, cognition. Introduction Over 20 years ago, Sutton etal. (1965) described a late positive polarity en- dogenous component of the scalp evoked potential which occurs approximately 300 milliseconds after the eliciting event and reflects on cognitive functioning. Since its original description, considerable literature has emerged supporting the concept that P 300 reflects cognitive processes involved in stimulus evalu-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

J Neural Transm [P-DSect] (1990) 2:249-264 Journal of,
Neural Transmission
�9 by Springer-Verlag 1990
T h e a u d i t o r y P 3 0 0 c o r r e l a t e s w i t h s p e c i f i c c o g n i t i v e d e f i c i t s
in P a r k i n s o n ' s d i s e a s e
S. Pang 1, J. C. Borod 1' 2, A. Hernandez 1' 2, I. Bodis-Wollner 1' 3, S. Raskin 2, L. Mylin l, L. Coscia 2, and M. D. Yahr 1
l Department of Neurology, Mount Sinai School of Medicine; 2 Department of Psychology, Queens College of the City University of New York; 3 Department of Ophthalmology,
Mount Sinai School of Medicine, New York, U.S.A.
Accepted June 15, 1990
Summary. An abnormally prolonged latency of the P 300 event-related potential has been reported in several types of dementing illnesses, including Parkinson's disease (PD). While some PD patients have dementia, a significant number of PD patients have less severe cognitive impairments. We examined the relation- ship between the auditory P 300 and a neuropsychological battery of 11 tasks in 43 PD patients. The quantitative relationship between the individual neu- ropsychological measures and the P 300 was examined using partial correlation and analysis of covariance techniques which controlled for age, education, and illness duration. The strongest correlations were between P 300 and both short- term memory and visual perception. Global cognitive deficits do not appear to relate to the abnormal P 300 responses in PD: instead, specific aspects of cog- nitive decline accounted for the electrophysiological abnormalities. An abnor- mally long or absent P300 correlated with deficits on select cognitive tasks: those involving memory, visual perception, and abstract reasoning. The inter- actions between anatomical and neurochemical abnormalities in PD are dis- cussed in light of the pattern of deficits seen in this study.
Keywords: Parkinson's disease, P300, evoked potential, neuropsychological measures, cognition.
Introduction
Over 20 years ago, Sutton etal. (1965) described a late positive polarity en- dogenous component of the scalp evoked potential which occurs approximately 300 milliseconds after the eliciting event and reflects on cognitive functioning. Since its original description, considerable literature has emerged supporting the concept that P 300 reflects cognitive processes involved in stimulus evalu-

250 S. Pang et al.
ation and task relevant decisions by the observer. A P 300 can be generated in a range of tasks, most easily perhaps in an "odd-ball paradigm" when the observer discriminates two differing stimuli. It occurs to the limited random presentation of a rare target within presentations of more frequent foils.
In most experimental paradigms, P 300 amplitude inversely correlates with the subjective probability of the event to be categorized when the subject has to decide on the event's task relevance. Hence, it was suggested that the P 300 is a marker of stimulus encoding categorization and evaluation time (and not of response execution) (Mulder et al., 1984). There is, in fact, supportive evi- dence, using the Sternberg (and not the routine odd-ball) paradigm that P 300 latency expresses time taken to evaluate the presence or absence of a target.
While the latency of the P 300 component increases with normal aging (Goodin etal., 1978a; Kraiuhin etal., 1986), in demented patients there is a significant exaggeration of this trend (Goodin et al., 1978b). Recent studies have shown that prolonged P 300 latency is found in several types of dementing disorders: Huntington's disease (Homberg etal., 1986), Alzheimer's disease (Goodin et al., 1978b), Korsakofffs disease (Goodin and Aminoff, 1987), and PD (Bodis-Wollner et al., 1984; Goodin and Aminoff, 1987; Hansch et al., 1982; O'Donnell et al., 1987; Polich et al., 1986). In general, these studies demonstrated a prolongation of P 300 latency which paralleled the decline in patients' mental status. As a result of these clinical studies, it is generally assumed that the abnormal latency increase of P 300 reflects generalized cognitive decline (Polich etal., 1986). Whether or not specific rather than global cognitive deficits may be correlated with an abnormal P 300 was not examined in most studies. How- ever, there is reason to look for a more specific correlation between P 300 and certain cognitive deficits. It has been suggested that the P 300 may be dependent on short-term memory (STM) processing of normal observers (Fabiani et al., 1986). Thus, P 300 could have clinical relevance as an indicator of STM memory deficit, which can occur without dementia in Parkinson's disease (PD).
While PD is predominantly marked by motor disabilities, a significant number of patients have cognitive impairments (e.g., Pirozzolo etal., 1982). The reported incidence of "dementia" in PD varies widely, ranging from 10% to 90%. In PD patients who do not exhibit dementia, the most consistently reported cognitive deficits are in visuospatial perception (Bowen etal., 1972; Huber et al., 1986; Pirrozolo et al., 1982; Raskin et al., 1990), abstract reasoning (Taylor etal., 1986), short-term effortful memory (Wilson etal., 1980), and verbal fluency (Taylor et al., 1986). At this point, it is unknown whether or not an abnormal P 300 correlates with global dementia or with some subset of cognitive dysfunction in Parkinson's disease.
The current study was designed to explore whether or not there is a rela- tionship between the auditory P 300 and a number of neuropsychological func- tions most often reported to be impaired in PD patients (see review above). These functions are visuospatial abilities, abstract reasoning skills, initiation and set shifting skills, and short-term memory. In addition, we evaluated whether

The auditory P 300 correlates with specific cognitive deficits in PD 251
general cognitive functioning, per se, is correlated with the P 300 in this patient group, and if not, whether or not abnormalities in the P 300 are a reflection of discrete cognitive deficits. In light of the above considerations, 43 PD patients were tested with the auditory P300 and a neuropsychological battery of 11 tasks, and the relationship between electrophysiological and neuropsychological measures was quantitatively examined. Our data will demonstrate that there is a subset of cognitive functions which are affected in PD. Secondly, generalized cognitive decline does not explain the abnormal P 300 responses in PD, Instead, one must consider specific aspects of cognitive dysfunction in correlation with these electrophysiological abnormalities.
Materials and methods
Subjects
Forty-three patients with an established diagnosis of PD, who were admitted to our Clinical Research Center. served as subjects in this study. Patients selected for study had no history of thalamotomy nor other previous or concurrent neurological disease. Patients who could not understand the evoked potential task and or the behavioral tasks were not included for study. Clinical assessment of dementia was performed via the neurologist's mental status examination, and clinically demented patients were excluded from this study. Each patient had a complete neurological evaluation prior to the electrophysiological and neuropsy- chological testing. Only patients with the diagnosis of idiopathic Parkinson's disease were included. Clinically-manifested depression and or use of anti-depressant medication were also exclusionary criteria. The data of patients whose N 1 component of the auditory evoked potential was not identifiable or appeared distorted were excluded from the analysis. Hearing was assessed by clinical neurological testing, i.e., whisper and tuning fork at 256 C; those with hearing impairments were excluded. There were 26 males and 17 females. Handedness, as determined by self-report, was right-sided for 38 subjects and left-sided for five subjects. The mean age was 63.0 (s.d. + 10.0, range = 38 79); the mean years of education were 13.2 (s.d. = 3.3, range = 6-18); the mean duration of illness was 114.6 months (s.d. 4- 81.5, range = 6 300); and the mean duration of L-dopa treatment was 109.7 months (s.d. + 65.4, range = 14-226). All patients were on dopaminergic medication (e.g., Sinemet). Sixteen percent of patients were on anti-cholinergic medication. Our subjects were in stage II (n -- 7), III (n = 23), or IV (n = 10) o f P D (Hoehn and Yahr, 1967). Those patients who experienced on/off phenomena were always tested during the "on" phase.
Electrophysiological recording
To elicit the AP 300, an auditory "odd-ball" stimulus paradigm was used. A series of 1.5 K (target) and 1 K (nontarget) tones was presented binaurally through Telephonic model TDH-39 P headphones at 70 db SPL with a 9.9 msec. rise/fall time and a 20 msec. plateau time at a 1.1 per second stimulus rate. The filter bandpass was set at 0.3 and 50 hz. The artifact-rejection criterion was set at 152 microvolts. Target tones (1.5 K) were presented 10% of the time and were randomly interspersed among the higher probability nontarget (1 K) tones, which were presented 90% of the time. Subjects were asked to keep a running mental count of the low probability target tones. A practice trial to ensure understanding was given prior to the actual test trials. If during the test it appeared that a patient had forgotten the instructions, the test was discontinued. During the test, when it appeared that the patient kept falling asleep and did not follow instructions to look at the screen,

252 S. Pang et al.
the test was discontinued, and the patient was rescheduled. As stated above, there were 43 patients who met all criteria for having their results included in our study. Tones were presented until at least 46 artifact-free responses to target tones were collected. This resulted in the presentation of approximately 462 frequent tones. In order to measure reproducibility, two independent test trials (Trial I and Trial II) were presented. Between Trial I and II, a control trial was inserted. In the control condition, both tones had the frequency of 1 K. The EEG was recorded with Grass gold cup electrodes affixed at Cz, Fz, and linked mastoids which served as reference. The forehead was grounded. Eye movements were recorded with electrodes placed above and below one orbit. Additionally, in selected patients, horizontal eye movement channels were added. The EEG and EOG responses were averaged for 800msec. post-stimulus onset separately for target and nontarget tones. The N 100 was measured as the maximum-amplitude negative waveform occurring within 80-150msecs. of the nontarget stimulus onset. The N 200 and P 300 responses were designated as the maximum-amplitude negative and positive waveforms, respectively, occurring within 200-500 msecs, of the rare stimulus onset. Amplitude was measured for specific latencies from the baseline, representing the average voltage of the first 50 msecs, of the trace. Latencies were measured using the cursors of the eight-channel averaging equipment (Dantec and Evomatic). P 300 measures were taken for the Cz and Fz electrode. Traces were plotted and also stored on diskettes for later analysis. Filters were set for 0.3 and 50 Hz. During the recording, accumulating averages were monitored on line by the authors. For further analysis, the number of target tones counted and latency values measured (in msec.) for N 1, N 2, and P 300 of the averaged evoked potential were recorded. The data of patients whose N 1 component of the auditory evoked potential was not identifiable or exceeded 130 msecs, were excluded from the analysis.
Neuropsychological assessment
A battery of neuropsychological tests covering a wide range of cognitive functions was administered to patients within one week of the evoked potential testing. The following cognitive functions were assessed: general intellectual ability- Information subtest of the Wechsler Adult Intelligence Scale-Revised (WAIS-R) (Wechsler, 1981); atten- tion- Attention subtest of the Mattis Dementia Rating Scale (MDRS) (Mattis, 1976); f luency- Controlled Word Association Test (F-A-S) (Benton and Hamsher, 1976), Initiation subtest of the MDRS; memory- Memory subtest of the MDRS, Logical Memory subtest of the Wechsler Memory Scale (Wechsler, 1945); visualperception-Visual Form Discrim- ination Test (Benton et al., 1983); visuospatial organization- Line Orientation Test (Benton etal., 1983), Facial Recognition Test (Benton etal., 1983); and abstract reason- ing- Conceptualization subtest of the MDRS, Raven's Progressive Matrices Test (Raven, 1960). For the data analyses to follow, the total raw score was used for each of the neuropsychological tests. An exception was made for the Information subtest of the WAIS- R, where the age-corrected scaled score was used.
Statistical evaluation
This section outlines our plan for statistical analysis. First, means and standard deviations for electrophysiological and neuropsychological variables were calculated and presented. As a preliminary measure to control for patient/subject variables that might confound performance on the measures of electrophysiological and neuropsychological functioning, analyses of variance or Pearson product-moment correlations were conducted. Six patient/ subject variables (i.e., gender, handedness, anti-cholinergic medication, age, education, illness duration) were examined against the l 1 neuropsychological measures and the six electrophysiological measures. For significant relationships found, patient/subject variables
The auditory P 300 correlates with specific cognitive deficits in PD 253
were controlled. Alpha level for significance was set at the standard level of 0.05 for this and subsequent analyses. Since this was an exploratory study, trends (p < 0.10) also were indicated in any tabular presentation of the results.
For the experimental analysis of our data, the relationship between measures of elec- trophysiological and neuropsychological functioning was studied using two separate anal- yses. Because this was an exploratory study and there were no specific a priori hypotheses, all variables were included in the analyses. First, Pearson product-moment correlation coefficients were calculated between the neuropsychological tests and electrophysiological measures. Second, to look more specifically at the relationship between P 300 abnormalities and neuropsychological deficits, analysis of variance was utilized. For each electrophy- siological measure, subjects were categorized into three groups: (a) those with a normal evoked potential response, (b) those with an abnormal (i.e., delayed) evoked potential response, and (c) those with an absent evoked potential response. One-way analyses of variance were conducted on the Group (3) variable for each neuropsychological task. Significant correlations and significant F-values are reported and discussed. Finally, we attempted to evaluate whether or not potential relationships between electrophysiological measures and neuropsychological tests were due to globally impaired cognitive performance, as operationalized by patient performance on the Dementia Rating Scale (DRS) (Mattis, 1976). The experimental analyses described above were repeated: (a) for the correlational analysis, separate analyses were conducted for subjects nonimpaired on the DRS, for those mildly impaired on the DRS, and for those moderately impaired on the DRS; and (b) for the analyses of variance, two-way ANOVAs (3 X 3) were conducted for Group (3) by Cognitive Status (3). In the case of the correlation analyses, patterns of significant coef- ficients were compared across the three groups (as defined by global cognitive status); in the case of the analyses of variance, significant interactions between the two factors were reported.
Results
Means and standard deviations
The means and s tandard deviations for each electrophysiological and neuro- psychological variable are displayed in Table 1. In some instances, the bat tery o f neuropsychologica l tests was curtailed. Fai lure to complete the entire bat tery was not related to a subject 's inability to pe r fo rm these tests but to scheduling difficulties.
All 43 patients had no rma l N 1 latency. Of the 43 patients, six had unmea- surable P 300 latency as the P 300 could not be identified with certainty; if it were present, it must have had a longer la tency than our analysis window (800 msec.) or had an ampl i tude lower than 2 microvolts. We accepted these results as represent ing abnorma l P 300. The norma l m e a n for 63 year-olds (the average age o f our patients) is 362 4- 18msec. W h e n classifying norma l or abnorma l results, we adjusted the n o r m for the age o f each individual pat ient by + 1.8 msec. per year plus 2 s tandard deviations. Of the remain ing 37 patients, 15 had a la tency outside the no rma l mean. Each of the patients with abnorma l P 300 had a present N 2. Of those whose P 300 could not be measured, only one had a clearly defined N 2. The m e a n age o f patients with abnormal P 300 was 65 years (range 54 to 74), compared to the m e a n age o f all patients which was 63 years.

254 S. Pang et al.
Table 1. Means and standard deviations for electrophysiological 1 and neuropsychological variables 2
Type of data Variable N 3 Mean S.D.
Electrophysiological
Neuropsychological
N1 Trial I 43 100.5 12.7 N1 Trial II 43 103.1 13.7 N2 Trial I 33 263.8 64.0 N2 Trial II 33 262.7 54.4 P300 Trial I 34 369.9 70.2 P300 Trial IX 34 371.1 68.3
Information (WAIS-R) 37 10.8 3.4 Attention (MDRS) 4 38 35.2 3.1 Generative Naming 23 41.3 15.3 Initiation (MDRS) 38 32.3 7.0 Memory (MDRS) 38 21.2 5.4 Logical Memory (WMS) 5 25 9.9 6.0 Vis. Form Discrimin. 33 26.5 6.5 Line Orientation 31 21.3 6.9 Facial Recognition 33 38.5 10.8 Conceptual (MDRS) 38 33.6 5.5 Progressive Matrices 24 15.8 6.9
1 Means for N1, N2, and P300 are for the average of Trial I and Trial II 2 All values are raw scores, except for the WAIS-R Information subtest which is an
age-corrected scaled score 3 N is not equal since not all patients completed the full battery 4 MDRS -- Mattis Dementia Rating Scale 5 WMS = Wechsler Memory Scale
The relationship of patient~subject variables to electrophysiological and neuropsychological functioning
To control for pat ient variables that might con found pe r fo rmance on the de- pendent measures of electrophysiological and neuropsychological functioning, analyses o f variance (ANOVA) were conduc ted or Pearson p r o d u c t - m o m e n t correlat ions were computed . Fo r each analysis, the neuropsychological measures (N = 11) included the 11 test scores, and the electrophysiological measures (N = 6) included the latency values (in msec.) for N 1, N 2, and P 300, separately, on Trial I and on Trial II. W h e n one-way A N O V A s (2) were conduc ted (using a between-subjects design) separately for the pat ient /subject variables of gender (male versus female), handedness (right versus left), and anti-cholinergic med- ication (present versus absent) on each of the 17 dependent variables specified above, none of 51 A N O V A s yielded significant results. However , when age (in years), educat ion (in years), and illness dura t ion (in months) were correlated

The auditory P 300 correlates with specific cognitive deficits in PD 255
separately with each of the 17 dependent variables, 12 of the 51 correlation coefficients (3 patient variables x 17 dependent variables) were significant (p ~< 0.05). Since there were more significant correlations than would be expected by chance for each of these patient variables, age, education, and illness duration were controlled for in the statistical analyses to follow through the use of partialling and covariate procedures.
Correlations
The relationship between quantitative measures of electrophysiological and neuropsychological functioning was estimated by the Pearson product-moment correlation coefficient. For the evoked potential data, mean scores of the two independent trials were entered into the correlation computations, since Trial I was significantly (p<0.001) correlated with Trial II for N2 (r = 0.84) and P300 (r = 0.88). The mean for N2 was 270.0 + 60.2 (N = 37), and the mean for P 300 was 375.4 • 68.6 (N = 37). Since several patients did not have values for both Trials I and II, the mean values reported here are not exactly the average of the means for each trial reported in Table 1.
Table 2 displays the correlation coefficients between the two evoked poten- tials measures (N2 Mean, P 300 Mean) and the 11 neuropsychological tests. Of the 22 correlation coefficients computed, seven (32%) were significant (p < 0,05). As can be seen in Table 2, there were three significant findings (out of 11) for N2 and four significant findings (out of 11) for P 300. There were four significant findings (out of four) for memory, two significant findings (out of two) for visual perception, and one significant finding (out of four) for visuospatial organization. In these cases, the longer the evoked potential latency, the greater the degree of cognitive impairment.
Analyses of variance
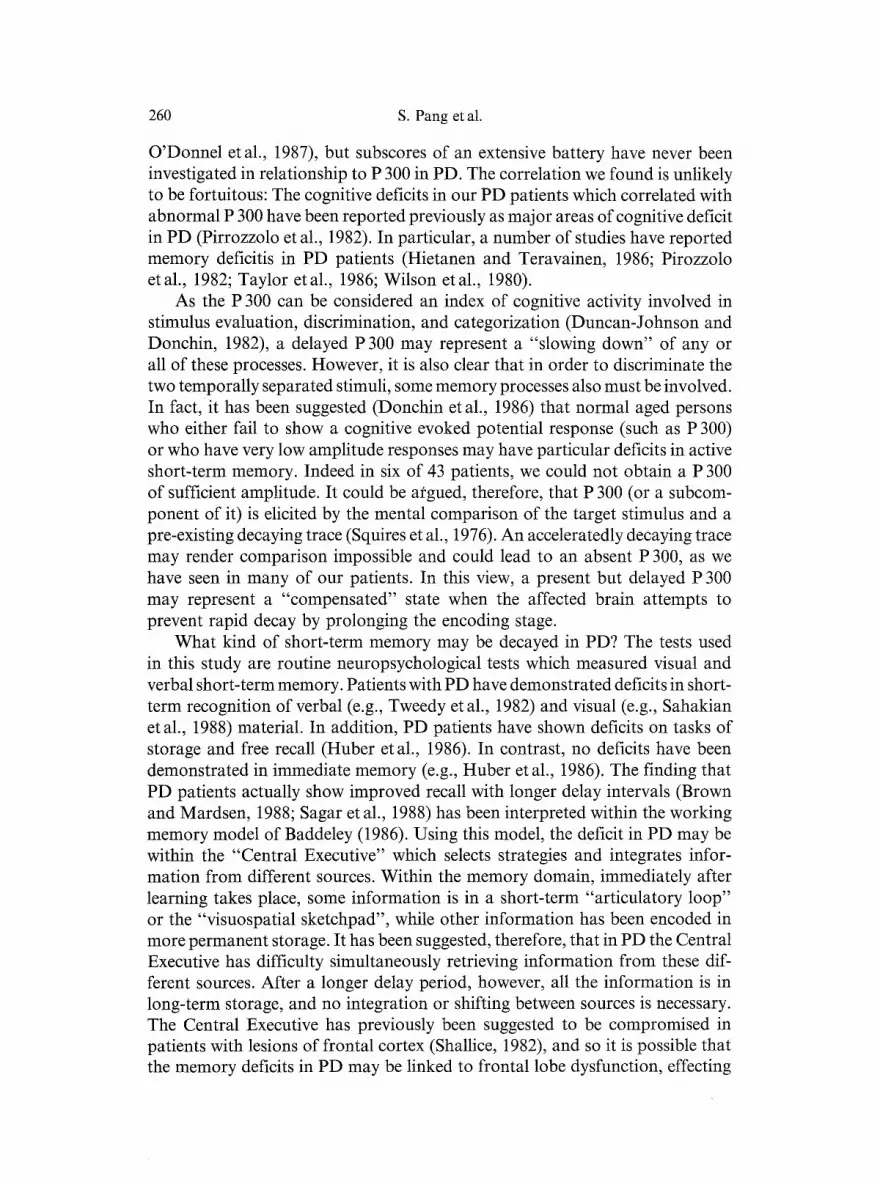
To study the relationship between electrophysiological and neuropsychological measures in PD, subjects were categorized into three groups depending upon the nature of their evoked potential response: those subjects with a normal evoked potential response, those with an abnormal evoked potential response, and those with an absent evoked potential response. Figure 1 presents typical P 300 waveforms for subjects with normal, abnormal (delayed), and absent P 300 responses.
As summarized earlier, the categorization of normal versus abnormal P 300 was based on age-related normative data of our laboratory, which are consistent with other published data (Goodin etal., 1978 a; Kraiuhin etal., 1986). One- way analyses of covariance (ANCOVAs) were conducted on the Group (3) variable using a between-subjects design for each neuropsychological task, sep- arately for N 2 on Trial 1, N 2 on Trial II, P 300 on Trial I, and P 300 on Trial II. (Trial I and Trial II were not averaged in order to evaluate the possible

256 S. Pang et al.
Table 2. Pearson Product-Moment correlation coefficients are presented for the neuro- psychological versus the electrophysiological variables t. Significant values and trends are
indicated. The number of observations for each coefficient appears in parentheses
Neuropsychological variables Electrophysiological variables
Category Measure N2 mean P300 mean
General Information - 0.33 + - 0.19 Intellectual Subtest (27) (27) Ability WAIS-R
Attention Attention - 0.35 + - 0.29 Subtest (MDRS) (28) (28)
Fluency Generative - 0.26 - 0.20 Naming (F-A-S) (15) (14)
Initiation 0.18 - 0.09 Subtest (MDRS) (28) (28)
Memory Memory - 0.42* - 0.37* Subtest (MDRS) (28) (28)
Logical Memory - 0.70*** - 0.62** Subtest (WMS) (17) (16)
Visual Visual Form - 0.54** - 0.44* Perception Discrimination (24) (24)
Visuospatial Line Orientation - 0.32 - 0.44* Organization (23) (22)
Facial - 0.34 + - 0.22 Recognition (24) (23)
Abstract Conceptualization - 0.30 - 0.24 Reasoning Subtest (MDRS) (33) (28)
Progressive - 0.35 - 0.45 + Matrices Test (18) (17) Ravens
t With partialling Rating Scale; W M S ***p<0.001
for age, education, and illness duration; M D R S Mattis Dementia Wechsler Memory Scale; +p<0 .10 ; *p<0.05; **p<0.01;
inf luence o f changes in the pa t i en t ' s clinical s ta tus due to t h e r a p y or prac t ice effects.) The G r o u p var iable was compr i s ed o f the three subg roups o f subjects
(subjects wi th a n o r m a l evoked po ten t i a l response , subjects wi th an a b n o r m a l evoked po ten t i a l response, a n d subjects wi th an absen t evoked po t en t i a l re- sponse) . F o r each analysis , a covar ia te p rocedu re was used, s i mu l t a n e o u s l y con t ro l l ing for age, educa t ion , a n d illness du ra t ion .

The auditory P 300 correlates with specific cognitive deficits in PD 257
AP300 LATENCY
N I Normal A.
Z63-LRm ~ F r e q u e n t
Z 6 3 - k R m 1 Rare
~"~ ~ ~ S u b t r a ti n , ~ . ~ ~ ,v ~ c o
5 jJVID I l I I
0 200 400 600 800 N i Delayed B.
2~WD raction
I I I I
0 200 400 600 800
E NI Absent C
Z63-LRm ~ Frequent
Z63-LRm Rare
S u b t r a c t i o n 2~V/D
I I i I 0 200 400 600 800
msec
Fig. 1. Auditory EPs to auditory stimuli are shown for three different representative patients. (A) Patient A, stage III, has a normal P 300 (356 msec.) and N 2 (225 msec.) latency. The amplitude of P3, measured from baseline, is 15.3 microvolts. The top trace in this figure and in others is the response to the frequent non-target, and the third trace represents subtraction between the two traces. (B) Shows a delayed P 300 (444msec.) and reduced amplitude (4.62 microvolts) in a patient with Stage III PD. (C) Shows uncertain, probably absent P 300. The trace to the target contains two deflections in the time window when P 300 should occur. At 444 msec. the deflection measures 2.37 microvolts, while at 536 msec. it has an amplitude of 3 microvolts. However, due to preceding and following deflections (which are only present in the target trace), the presence of P 300 is questionable. Never- theless, if either positive deflection represents P 300, it is clearly attenuated and delayed.
This patient also had been characterized as Stage III
Table 3 displays the F-values for the G r o u p variable f rom the A N C O V A s for each o f the four late evoked potent ial measures (N 2 Trial I, N 2 Trial II, P 300 Trial I, P 300 Trial II) on each o f the 11 neuropsychological variables. Of the 44 A N C O V A s conducted, twelve (27%) yielded significant (p<0 .05) main effects for the G r o u p variable. There were seven significant findings (out

258 S. Pang et al.
Table 3. The numerical values represent the F-values for the Group Variable from the one- way analyses of covariance (ANCOVA). t Significant values and trends are indicated, The
number of observations for each ANCOVA appears in parentheses
Neuropsychological variables Electrophysiological variables
N2 P300
Category Measure TR I TR II TR I TR II
General Information 1.07 3.43* 1.23 0.18 Intellectual Subtest (36) (36) (36) (36) Ability (WAIS-R)
Attention Attention 2.06 0.82 2.17 1.47 Subtest (MDRS) (37) (37) (37) (37)
Fluency Generative 0.27 0,64 1.08 0.41 Naming (F-A-S) (23) (23) (23) (23)
Initiation 4.11" 1.50 1.69 1.25 Subtest (MDRS) (37) (37) (37) (37)
Memory Memory 6.05* 1.56 4.33* 1.61 Subtest (MDRS) (37) (37) (37) (37)
Logical Memory 5.44* 2.09 3.06 + 2.63 + Subtest (WMS) (24) (24) (24) (24)
Visual Visual Form 1.79 3.47* 3.81" 0.28 Perception Discrimination (32) (32) (32) (32)
Visuospatial Line Orientation 1.12 3.29* 0.88 1.30 Organization (30) (30) (30) (30)
Facial 2.10 0.01 0.48 0.98 Recognition (32) (32) (32) (32)
Abstract Conceptualization 4.56* 1.04 7.11"* 5.29** Reasoning Subtest (MDRS) (37) (37) (37) (37)
Progressive 2.33 0.94 3.64* 0.65 Matrices Test (23) (23) (23) (23) Ravens
t Covariate analysis of variance with simultaneous control of age, education, and illness duration; TR Trial; MDRS Mattis Dementia Rating Scale; WMS Wechsler Memory Scale; + p<0.10; *p<0.05; **p<0.01; *** p<0.001
of 22) for N 2 and five significant findings (out of 22) for P 300. The majority of these significant findings occurred for analyses involving abstract reasoning (four out of eight), visual perception (two out of four), and memory (three out of eight). When subgroup adjusted means for the 12 significant ANCOVAs were examined, in most cases, subjects with normal evoked potential responses

The auditory P 300 correlates with specific cognitive deficits in PD 259
showed the least, subjects with normal evoked potential responses showed middle-level, and subjects with absent evoked potential responses showed the most impairment on the neuropsychological tasks.
Controlling for global cognitive deficits
Further analyses were performed to evaluate whether or not the relationship between electrophysiological and neuropsychological measures was due solely to impaired cognitive performance. The total score from the Mattis Dementia Rating Scale was employed as an index of cognitive functioning. The distribution of scores on this test was divided into three relatively equal groups: (a) a non- impaired group, consisting of those patients with scores between 137 and 144 (n -- 12) (median -- 142); (b) a mildly impaired group, consisting of those pa- tients with scores between 130 and 136 (n-- 13) (median-- 133); and (c) a moderately impaired group, consisting of those patients with scores less than 129 (n = 12) (median = 117).
Correlations between the two electrophysiological variables (N2 Mean, P 300 Mean) and the 11 neuropsychological variables were recomputed, sep- arately, for each of the three groups. Sixty-six correlation coefficients were calculated (3 groups x 22 coefficients). The patterns of correlation did not differ systematically between the groups. More importantly, exclusion of the mod- erately impaired group did not substantially alter the magnitude of the cor- relations. To reexamine the analysis of covariance data, two-way ANCOVAs (3 x 3) were conducted using a between-subjects design for Group (normal evoked potential response, abnormal evoked potential response, absent evoked potential response) and Cognitive Status (non-impaired, mildly impaired, mod- erately impaired) on each of the 11 neuropsychological variables, separately for N 2 Trial I, N 2 Trial II, P 300 Trial I, and P 300 Trial II. Again, for each ANCOVA, the covariates of age, education, and illness duration were entered simultaneously. Of the 44 ANCOVAs conducted, only one of the 44 interactions between Group and Cognitive Status was significant, not more than would be expected by chance. Thus, the results suggest no significant effect of cognitive status on the relationship between electrophysiological and neuro- psychological functioning in our data.
Discussion
This is the first study, to our knowledge, which demonstrates correlations between cognitive evoked potentials and a subset of neuropsychological dys- functions in Parkinson's disease. We found a correlation between an abnormal auditory P 300 and impaired memory function and to a lesser degree between P 300 and visuospatial processing in patients with Parkinson's disease.
In previous studies, P 300 changes in PD were examined with respect to a limited number of preselected neuropsychological tests (e.g., Hansch et al., 1982;
260 S. Pang et al.
O'Donnel et al., 1987), but subscores of an extensive battery have never been investigated in relationship to P 300 in PD. The correlation we found is unlikely to be fortuitous: The cognitive deficits in our PD patients which correlated with abnormal P 300 have been reported previously as major areas of cognitive deficit in PD (Pirrozzolo et al., 1982). In particular, a number of studies have reported memory deficitis in PD patients (Hietanen and Teravainen, 1986; Pirozzolo etal., 1982; Taylor etal., 1986; Wilson etal., 1980).
As the P 300 can be considered an index of cognitive activity involved in stimulus evaluation, discrimination, and categorization (Duncan-Johnson and Donchin, 1982), a delayed P 300 may represent a "slowing down" of any or all of these processes. However, it is also clear that in order to discriminate the two temporally separated stimuli, some memory processes also must be involved. In fact, i t has been suggested (Donchin et al., 1986) that normal aged persons who either fail to show a cognitive evoked potential response (such as P 300) or who have very low amplitude responses may have particular deficits in active short-term memory. Indeed in six of 43 patients, we could not obtain a P 300 of sufficient amplitude. It could be argued, therefore, that P 300 (or a subcom- ponent of it) is elicited by the mental comparison of the target stimulus and a pre-existing decaying trace (Squires et al., 1976). An acceleratedly decaying trace may render comparison impossible and could lead to an absent P 300, as we have seen in many of our patients. In this view, a present but delayed P 300 may represent a "compensated" state when the affected brain attempts to prevent rapid decay by prolonging the encoding stage.
What kind of short-term memory may be decayed in PD? The tests used in this study are routine neuropsychological tests which measured visual and verbal short-term memory. Patients with PD have demonstrated deficits in short- term recognition of verbal (e.g., Tweedy et al., 1982) and visual (e.g., Sahakian etal., 1988) material. In addition, PD patients have shown deficits on tasks of storage and free recall (Huber etal., 1986), In contrast, no deficits have been demonstrated in immediate memory (e.g., Huber et al., 1986). The finding that PD patients actually show improved recall with longer delay intervals (Brown and Mardsen, 1988; Sagar et al., 1988) has been interpreted within the working memory model of Baddeley (1986). Using this model, the deficit in PD may be within the "Central Executive" which selects strategies and integrates infor- mation from different sources. Within the memory domain, immediately after learning takes place, some information is in a short-term "articulatory loop" or the "visuospatial sketchpad", while other information has been encoded in more permanent storage. It has been suggested, therefore, that in PD the Central Executive has difficulty simultaneously retrieving information from these dif- ferent sources, After a longer delay period, however, all the information is in long-term storage, and no integration or shifting between sources is necessary. The Central Executive has previously been suggested to be compromised in patients with lesions of frontal cortex (Shallice, 1982), and so it is possible that the memory deficits in PD may be linked to frontal lobe dysfunction, effecting

The auditory P 300 correlates with specific cognitive deficits in PD 261
a "memory hold" operation. Further studies should employ measures to directly confront the working memory model (e.g., procedural learning, incidental learn- ing, enhanced cued recall, frequency of occurrence, etc.).
While at the present there is little general agreement on the functional significance of the P 300 component or components, it is worth considering some relevant recent neuroanatomical and neurophysiological data. Regional depletion of dopamine in the area of the frontal cortex, where neurons exhibit mnemonic coding of visual space (Funahashi etal., 1989), leads to cognitive deficits in the monkey. It is now recognized that PD is accompanied by de- generation of both nigrostriatal and mesocorticolimbic dopaminergic systems (Graybiel, 1986). Indeed, PD patients demonstrate certain cognitive deficits similar to those observed in patients with frontal lobe damage (Levin etal., 1988; Taylor etal., 1986). Reciprocal pathways connect the dorsolateral pre- frontal cortex with the hippocampal formation and parahippocampal cortex (Goldman-Rakic etal., 1984). Several investigators have suggested that the hippocampus and associated brain sites may be among the important P 300 generator sites (Okada etal., 1983). Thus, abnormal P 300 may occur in PD because of a deficiency in the striatal-dorsolateral prefrontal-hippocampal net- work. We are not implying, however, that the electrophysiological/neuropsy- chological correlation necessarily represents the lesion of a common single anatomic site. Rather, a common lesion could affect distributed but intercon- nected sites with reciprocal dopaminergic connections, such as the dorsolateral prefrontal cortex and other structures involved in P 300 generation (Wood et al., 1984.).
Is there a relationship between P 300 and dopamine replacement therapy in PD? Some studies have shown that fluctuations in dopamine levels are associated with selective changes in verbal memory (e.g., Mohr et al., 1987) and that PD patients who have on/off phenomena show deficits in verbal memory during periods of sub-optimum dopamine response (off-periods) as compared with response during on-periods (e.g., Mohr et al., 1987). Gotham etal. (1988) assessed PD patients, both on and off levodopa treatment, on a range of tests selected from the human and animal experimental literature as being sensitive to disruption of prefrontal cortex. A variable pattern of results was obtained, one based on the effects of dopamine depletion and the other based on the adverse effects of dopamine overstimulation. The results also suggested that different areas of prefrontal cortex are involved in the different tasks employed and that the relationship between dopamine and cognitive function in the frontal system is complex. Studies in the monkey with a Parkinsonian syndrome (char- acterized by rigidity, tremor, and bradykinesia), induced by the neurotoxin 1-methyl-4-phenyl-l,2,5,6-tetrahydropyridine (MPTP), suggest that MPTP does also disrupt auditory P 300 generation. However, while levodopa does improve all motor symptoms, it does not restore the cognitive potential (Glover et al., 1988). In this study, all patients were receiving dopaminergic agents, yet ab- normalities in P 300 still occurred.

262 S. Pang et al.
In summary, then we have demonstrated correlations between abnormal cognitive potentials and select neuropsychological functions in Parkinson's dis- ease. In light of our results and the literature on STM deficits in PD and on memory deficits in frontal lobe lesioned patients, we speculate that the high rate of P 300 abnormalities shown by the PD patients in our study may reflect a faulty STM process. Whether or not this represents an accelerated form of age-associated degeneration of dopaminergic pathways (Goldman-Rakic and Brown, 1981) overlaid by the dopaminergic dysfunction in the basal ganglia and mesolimbic system currently associated with PD, remains to be seen.
Acknowledgements
This paper was supported, in part, by NIH Grants Nos. NS 11631, RR71, and EY 1708 to the Mount Sinai Medical Center and by NIH Biomedical Research Support Grant No. RR07064 to Queens College. The authors thank Martin Sliwinski for performing statistical analyses and Dr. Carol Bodian for comments on the manuscript. A portion of this paper was presented at the annual meeting of the American Academy of Clinical Neurophysiology, Boston, July, 1988.
References
Baddeley A (1986) Working memory. Oxford University Press, Oxford Benton A, Hamsher K (1976) Multilingual aphasia examination. University of Iowa, Iowa
City Benton A, Hamsher K, Varney N, Spreen O (1983) Contributions to neuropsychological
assessment: a clinical manual. Oxford University Press, New York Bodis-Wollner I, Yahr MD, Mylin LH (1984) Nonmotor functions of the basal ganglia.
In: Hassler RG, Christ JR (eds) Advances in neurology. Raven Press, New York, pp 289-297
Bowen F, Burns M, Brady E, Yahr MD (1972) A note on alterations of personal orientation in Parkinsonism. Neuropsychologia 14:425429
Brown R, Marsden C (1988) Internal versus external cues and the control of attention in Parkinson's disease. Brain 111:323-345
Donchin E, Miller GA, Farwell LA (1986) The endogenous components of the event-related potential: a diagnostic tool? In: Swaab DF, Fliers E, Mirmiran M, van Gool WA, van Haaren F (eds) Progress in brain research. Elsevier Science Publishers, Amsterdam, pp 87-102
Duncan-Johnson CC, Donchin E (1982) The P 300 component of the event-related brain potential as an index of information processing. Biol Psychol 14:1-52
Fabiani M, Karis B, Donchin E (1986) P 300 and recall in an incidental memory paradigm. Psychophysiology 23:298-308
Funahashi S, Bruce CJ, Goldman-Rakic PS (1989) Mnemonic coding of visual space in the monkey's dorsolateral prefrontal cortex. J Neurophysiol 61:331-349
Glover A, Ghilardi M, Bodis-Wollner I, Onofrj M (1988) Alterations in event-related potentials of MPTP-treated monkeys. Electroencephalogr Clin Neurophysiol 71: 461-468
Goldman-Rakic PS, Brown RM (1981) Regional changes of monoamines in cerebral cortex and s,bcortical structures of aging rhesus monkeys. Neuroscience 6:177-187
Goldma. Rakic PS, Selemon LD, Schwartz ML (1984) Dual pathways connecting the dorsolateral prefrontal cortex with the hippocampal formation and parahippocampal cortex in the rhesus monkey. Neuroscience 12:719-743

The auditory P 300 correlates with specific cognitive deficits in PD 263
Goodin D, Aminoff MJ (1987) Electrophysiological differences between demented and nondemented patients with Parkinson's disease. Ann Neurol 21:9~94
Goodin D, Squires K, Henderson B, Starr A (1978a) Age-related Variations in evoked potentials to auditory stimuli in normal human subjects. Electroencephalogr Clin Neu- rophysiol 44:447-458
Goodin D, Squires K, Starr A (1978b) Long latency event-related components of the auditory potential in dementia. Brain 101:635-648
Gotham AM, Brown RG, Marsden CD (!988) "Frontal" cognitive function in patients with Parkinson's disease "on" and "off" Levodopa. Brain 111:299-321
Graybiel AM (1986) DA-containing innervation of the striatum: subsystem and their striatal correspondents. In: Fahn S, Marsden CD, Jenner P (eds) Recent developments in Parkinson's disease. Raven Press, New York, pp 1-16
Hansch E, Syndulko K, Cohen S, Goldberg Z, Potvin A, Tourrellotte W (1982) Cognition in Parkinson's disease: an event-related perspective. Ann Neurol 11:599-607
Hietanen M, Terevainen H (1986) Cognitive performance in early Parkinson's disease. Acta Neurol Scand 73:151-159
Hoehn M, Yahr M (1967) Parkinsonism: onset, progression, and mortality. Neurology 17: 427-442
Homberg V, Hefter H, Granseyer G, Strauss W, Lange H, Hennerici M (1986) Event- related potentials in patients with Huntington's disease and relatives at risk in relation to detailed psychometry. Electroencephalogr Clin Neurophysiol 63:552-569
Huber S, Shuttleworth E, Paulson G (1986) Dementia in Parkinson's disease. Arch Neurol 43:987-990
Kraiuhin C, Gordon E, Stamfield P, Meares R, Howson A (1986) P 300 and the effects of aging: relevance to the diagnosis of dementia. Exp Aging Res 12:187-192
Levin BE, Llabre MM, Weiner WJ (1988) Neuropsychological correlates of early Parkin- son's disease: evidence for frontal lobe dysfunction. In: Kalivas PW, Nemeroff CB (eds) The mesocorticolimbic dopamine system. Ann NY Acad Sci 537:518-520
Mattis S (1976) Mental Status Examination for organic mental syndrome in the elderly patient. In: Bellak L, Karasu T (eds) Geriatric psychiatry. Grune and Stratton, New York
Mohr E, Fabrini G, Ruggieri S, Fedio P, Chase T (1987) Cognitive concomitants of dopamine system stimulation in Parkinsonian patients. Neurol Neurosurg Psychiatry 50:1192-1196
Mulder G, Gloerich ABM, Brookhuis KA, van Dellen HJ, Mulder LJM (1984) Stage analysis of the reaction time process using brain event-related potentials and reaction time. Psychol Rev 46:15-32
O'Donnel B, Squires N, Martz M, Chen J, Phay A (1987) Evoked potential changes and neuropsychological performance in Parkinson's disease. Biol Psychol 24:23-37
Okada Y, Kaufman L, Williamson S (1983) The hippocampal formation as a source of the slow endogenous potentials. Electroencephalogr Clin Neurophysiol 55:417-426
Pirozzolo F J, Hansch EC, Mortimer JA, Webster DD, Kuskowski DD (1982) Dementia in Parkinson's disease: a neuropsychological analysis. Brain Cogn 1:71-83
Polich J, Ehlers C, Otis S, Mandell A, Bloom F (1986) P 300 latency reflects the degree of cognitive decline in dementing illness. Electroencephalogr Clin Neurophysiol 63: 138-144
Raskin SA, Borod JC, Wasserstein J, Bodis-Wollner I, Coscia L, Yahr MD (1990) Vis- uospatial orientation in Parkinson's disease. Int J Neurosci 51:9-18
Raven J (1960) Guide to the standard progressive matrices. Lewis, London Sagar H, Sullivan E, Gabrieli J, Corkin S, Growdon J (1988) Temporal ordering and short-
term memory deficits in Parkinson's disease. Brain 111:525-539

264 S. Pang et al.: The auditory P 300 correlates with specific cognitive deficits in PD
Sahakian B, Morris R, Evendon J, Heald A, Levy R, Philpot M, Robbins T (1988) A comparative study of visuospatial memory and learning in Alzheimer-type dementia and Parkinson's disease. Brain 111:695-718
Shallice T (1982) Specific impairments in planning. Phil Trans Royal Soc Lond 298:199-209 Squires KC, Wickens N, Squires N, Donchin E (1976) The effect of stimulus sequence on
the waveform of the cortical event-related potential. Science 193:1142-1146 Sutton S, Braren M, Zubin J, John ER (1965) Evoked potential correlates of stimulus
uncertainty. Science 150:1187-1188 Taylor AE, Saint-Cyr AJ, Lang AE (1986) Frontal lobe dysfunction in Parkinson's disease:
the cortical focus of neostriatal outflow. Brain 109:845-883 Tweedy J, Langer K, McDowell F (1982) The effect of semantic relations on the memory
deficits associated with Parkinson's disease. J Clin Neuropsychol 4:235-247 Wechsler D (1945) A standardized memory scale for clinical use. J Psychol 19:87-95 Wechsler D (1981) Wechsler Adult Intelligence Scale-Revised. Psychological Corporation,
New York Wilson RS, Kaszniak AW, Klawans HL, Garron DC (1980) High speed memory scanning
in Parkinsonism. Cortex 16:67-72 Wood CC, McCarthy G, Squires NK, Vaughan HG, Woods DL, McCallum WC (1984)
Anatomical and physiological substrates of event-related potentials. In: Kanner R, Cohen J, Tueting P (eds) Brain and information: event related potentials. New York, pp 681-721
Author's address: Dr. J. C. Borod, Department of Psychology, NSB-E318, Queens College, Flushing, New York 11367, U.S.A.
Received January 31, 1990
Related Documents











