REVIEW ARTICLE The association between health care professional attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of patients with low back pain: A systematic review B. Darlow 1,2, , B.M. Fullen 3 , S. Dean 4 , D.A. Hurley 3 , G.D. Baxter 2 , A. Dowell 1 1 Department of Primary Health Care and General Practice, University of Otago, Wellington, PO Box 7343, Wellington South 6242, New Zealand 2 Centre for Physiotherapy Research, School of Physiotherapy, University of Otago, PO Box 56, Dunedin 9054, New Zealand 3 School of Public Health, Physiotherapy and Population Science, University College Dublin, Belfield, Dublin 4, Ireland 4 Peninsula College of Medicine and Dentistry, Universities of Exeter and Plymouth, Exeter EX2 4SG, United Kingdom Correspondence Ben Darlow Department of Primary Health Care and General Practice, University of Otago, Wellington, PO Box 7343, Wellington South 6242, New Zealand. Tel.: +64 4 385 5995; fax: +64 4 385 5539. E-mail: [email protected] Funding sources None Conflicts of interests None declared Accepted for publication 5 June 2011 doi:10.1016/j.ejpain.2011.06.006 Abstract Background: It has been suggested that health care professional (HCP) attitudes and beliefs may negatively influence the beliefs of patients with low back pain (LBP), but this has not been systematically reviewed. This review aimed to investigate the association between HCP attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of this patient population. Methods: Electronic databases were systematically searched for all types of studies. Studies were selected by predefined inclusion criteria. Methodological quality was appraised and strength of evidence was determined. Results: Seventeen studies from eight countries which investigated the attitudes and beliefs of general practitioners, physiotherapists, chiropractors, rheumatologists, orthopaedic surgeons and other paramedical therapists were included. There is strong evidence that HCP beliefs about back pain are associated with the beliefs of their patients. There is moderate evidence that HCPs with a biomedical orientation or elevated fear avoidance beliefs are more likely to advise patients to limit work and physical activities, and are less likely to adhere to treatment guidelines. There is moderate evidence that HCP attitudes and beliefs are associated with patient education and bed rest recommendations. There is moderate evidence that HCP fear avoidance beliefs are associated with reported sick leave prescription and that a biomedical orientation is not associated with the number of sickness certificates issued for LBP. Conclusion: HCPs need to be aware of the association between their attitudes and beliefs and the attitudes and beliefs and clinical management of their patients with LBP. Cite this article as: Ben Darlow, Brona Fullen, Sarah Dean, Deirdre A. Hurley, G. David Baxter, Anthony Dowell. The association between health care pro- fessional attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of patients with low back pain: A systematic review. Eur J Pain 16 (2011) 3–17 [doi:10.1016/j.ejpain. 2011.06.006] 1. Introduction Low back pain (LBP) is a significant and expensive health condition, with direct and indirect costs repre- senting an important financial burden (Dagenais et al., 2008). LBP has been estimated to cost 2% of gross domestic product in developed countries (van Tulder et al., 1995; Wieser et al., 2010). 3 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

REVIEW ARTICLE
The association between health care professional attitudes andbeliefs and the attitudes and beliefs, clinical management, andoutcomes of patients with low back pain: A systematic reviewB. Darlow1,2,, B.M. Fullen3, S. Dean4, D.A. Hurley3, G.D. Baxter2, A. Dowell1
1 Department of Primary Health Care and General Practice, University of Otago, Wellington, PO Box 7343, Wellington South 6242, New Zealand
2 Centre for Physiotherapy Research, School of Physiotherapy, University of Otago, PO Box 56, Dunedin 9054, New Zealand
3 School of Public Health, Physiotherapy and Population Science, University College Dublin, Belfield, Dublin 4, Ireland
4 Peninsula College of Medicine and Dentistry, Universities of Exeter and Plymouth, Exeter EX2 4SG, United Kingdom
CorrespondenceBen Darlow
Department of Primary Health Care and
General Practice, University of Otago,
Wellington, PO Box 7343, Wellington South
6242, New Zealand.
Tel.: +64 4 385 5995;
fax: +64 4 385 5539.
E-mail: [email protected]
Funding sourcesNone
Conflicts of interestsNone declared
Accepted for publication5 June 2011
doi:10.1016/j.ejpain.2011.06.006
Abstract
Background: It has been suggested that health care professional (HCP)attitudes and beliefs may negatively influence the beliefs of patients withlow back pain (LBP), but this has not been systematically reviewed. Thisreview aimed to investigate the association between HCP attitudes andbeliefs and the attitudes and beliefs, clinical management, and outcomes ofthis patient population.Methods: Electronic databases were systematically searched for all typesof studies. Studies were selected by predefined inclusion criteria.Methodological quality was appraised and strength of evidence wasdetermined.Results: Seventeen studies from eight countries which investigatedthe attitudes and beliefs of general practitioners, physiotherapists,chiropractors, rheumatologists, orthopaedic surgeons and otherparamedical therapists were included. There is strong evidence that HCPbeliefs about back pain are associated with the beliefs of their patients.There is moderate evidence that HCPs with a biomedical orientation orelevated fear avoidance beliefs are more likely to advise patients to limitwork and physical activities, and are less likely to adhere to treatmentguidelines. There is moderate evidence that HCP attitudes and beliefs areassociated with patient education and bed rest recommendations. There ismoderate evidence that HCP fear avoidance beliefs are associated withreported sick leave prescription and that a biomedical orientation is notassociated with the number of sickness certificates issued for LBP.Conclusion: HCPs need to be aware of the association between theirattitudes and beliefs and the attitudes and beliefs and clinical managementof their patients with LBP.
Cite this article as: Ben Darlow, Brona Fullen, SarahDean, Deirdre A. Hurley, G. David Baxter, AnthonyDowell. The association between health care pro-fessional attitudes and beliefs and the attitudesand beliefs, clinical management, and outcomes ofpatients with low back pain: A systematic review.Eur J Pain 16 (2011) 3–17 [doi:10.1016/j.ejpain.2011.06.006]
1. Introduction
Low back pain (LBP) is a significant and expensivehealth condition, with direct and indirect costs repre-senting an important financial burden (Dagenais et al.,2008). LBP has been estimated to cost 2% of grossdomestic product in developed countries (van Tulderet al., 1995; Wieser et al., 2010).
3Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

LBP treatment guidelines acknowledge the impor-tance of psychosocial factors on the outcome of LBP(Kendall et al., 1997). A recent systematic reviewfound patient depression, psychological distress,passive coping strategies and fear avoidance beliefs tobe independently associated with poor LBP outcome(Ramond et al., 2011); other reviews have also high-lighted the importance of pain self-efficacy beliefs andcatastrophising (Main et al., 2010).
A number of tools have been developed or adaptedto assess the attitudes and beliefs of health care pro-fessionals (HCP) (Bishop et al., 2007) and it has beensuggested that HCP attitudes and beliefs may nega-tively influence the beliefs of their patients (Vlaeyenand Linton, 2006). Although factors which affectgeneral practitioner (GP) attitudes and beliefs regard-ing acute LBP management have been previouslyinvestigated (Fullen et al., 2008), the associationbetween HCP attitudes and beliefs and patient-relatedfactors has not been systematically reviewed.
Parsons et al. (2007) investigated the interactionof patients’ and primary care practitioners’ beliefsand expectations on the process of care for chronicmusculoskeletal pain. This systematic review demon-strated that HCP beliefs influenced patient manage-ment and the patient’s satisfaction with care; however,it did not specifically address LBP, was limited tochronic pain, and only included qualitative studiesrelating to GPs (Parsons et al., 2007).
The aim of this study was to systematically reviewthe evidence regarding the association between HCPattitudes and beliefs and patient-related factors forLBP of any duration. We hypothesised that therewould be an association between HCPs’ attitudes andbeliefs and (i) patient attitudes and beliefs, (ii) patientclinical management, and (iii) patient outcome.
2. Methods
2.1 Search strategy
Electronic searches of Medline, EMBASE, CINAHL,AMED, PsycINFO, and the Cochrane Central Registerof Controlled Trials (January 1990–March 2010) wereconducted in late March 2010.
The search strategy was developed in consultationwith a medical librarian and used a combination ofMeSH terms and keywords. All MeSH terms weremapped to subject headings and checked for othercontexts to ensure inclusion of all appropriate terms; aseparate strategy was developed for each database toaccount for variations in MeSH terms. The final strate-gies were independently checked by two reviewers
(BD, BF). The strategies had four components whichwere combined: (1) attitudes and beliefs, (2) healthcare professionals, (3) low back pain, and (4) patientattitudes and beliefs, management, or outcomes. Thecomplete search strategy for Medline via Ovid is avail-able online (Table S1, see the online version at10.1016/j.ejpain.2011.06.006). Hand searches for rel-evant articles were also conducted on the bibliogra-phies of identified articles and related systematicreviews.
2.2 Study selection and inclusion criteria
Studies relating to LBP (all types and categories) thatinvestigated an association between HCP attitudesand beliefs and patient attitudes and beliefs, clinicalmanagement, or outcomes were included. Originalempirical studies (both quantitative and qualitativemethodologies), written in English, publishedbetween January 1990 and March 2010 were eligible.Studies were excluded if they primarily related to HCPattitudes about outcome expectation, race/ethnicity,gender, or narcotic medications and the relationship toLBP, or to patient satisfaction as an outcome. Titles andabstracts of citations retrieved by the literature searchwere independently scrutinised for eligibility by tworeviewers (BD, BF). Full papers were retrieved andevaluated if the paper appeared to fulfil inclusion cri-teria, if eligibility was unclear based upon the contentof the abstract, or if the abstract was not available.Disagreement regarding eligibility was resolved byconsensus between the two reviewers.
2.3 Data extraction
Potentially relevant papers were independently scru-tinised by two reviewers (BD, BF) using a standardiseddata extraction sheet. The categories of data extractedwere: study characteristics; study population characte-ristics; HCP attitudes and beliefs investigated; and theassociation with patients with LBP. Following dataextraction a final decision on the eligibility of paperswas made by consensus between the two reviewers.
2.4 Quality assessment
Two appraisal systems were chosen for this review; theEpidemiological Appraisal Instrument (EAI) was usedto appraise quantitative studies (Genaidy et al., 2007),and the Critical Appraisal Skills Programme (CASP)system for qualitative studies (Public Health ResourceUnit, 2006). Two reviewers independently appraisedthe articles (SD, DH); all disagreements regarding
The association between health care professional attitudes and outcomes of patients with low back pain B. Darlow et al.
4 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

ratings were resolved by consensus between these tworeviewers. One article was rated by a third reviewer(DB) as SD is the first author; SD was not involved inany decision regarding this study (Dean et al., 2005).No guidelines have been developed to rate researchas of low, moderate or high quality within thesetwo systems [personal communication]. We designatedresearch fulfilling less that 50% of criteria as being oflow quality, 50–75% as being of moderate quality andmore than 75% as being of high quality. Studies of lowquality were excluded from analysis.
2.5 Synthesis of evidence
The strength of evidence according to the gradingsystem used in the Agency for Healthcare and PolicyResearch (AHCPR) guidelines was the primaryoutcome measure (Bigos et al., 1994). The quality ofevidence according to the Grading of Recommenda-tions Assessment, Development and Evaluation(GRADE) guidelines was the secondary outcomemeasure (Guyatt et al., 2008).
2.6 Thematic analysis and generalizability
Two reviewers (BD and TD) independently analysedthemes related to (i) study results and (ii) study popu-lation characteristics which might be used to assessgeneralizability, before an agreed collation by thosereviewers.
3. Results
Study identification and selection for analysis is sum-marised in Fig. 1. In total, 20 studies fulfilled the inclu-sion criteria. Results of one study were reported in twoseparate publications, which met the inclusion criteriawhen combined (Buchbinder et al., 2001a,b); this wastreated as one study in the review process. Five studieswere rated as being of high quality and 12 were ratedas moderate quality (Tables S2 and S3, see the onlineversion at 10.1016/j.ejpain.2011.06.006). Threestudies were rated as low quality (Brynhildsen et al.,1995; Rupert, 2000; Houben et al., 2004) and wereexcluded from analysis. All decisions regarding studyinclusion and quality rating were reached by consen-sus, although a third reviewer was appointed toresolve disagreements, this was not required.
Table 1 summarises the characteristics of the 17included studies, more detailed information is avail-able online (Table S4, see the online version at10.1016/j.ejpain.2011.06.006). Studies were of cross-sectional, longitudinal, concurrent cohort, and quali-
tative methodologies. They were conducted in the UK,France, the Netherlands, Australia, Germany, Norway,Sweden, and the USA. Studies were based in primarycare, secondary care, or in settings including patientsor practitioners from both primary and secondarycare. The attitudes and beliefs of GPs, physiotherapists,
1937 records identified through electronic database search
106 AMED322 CINAHL138 Cochrane905 EMBASE351 Medline115 PsychINFO
14 records identified through bibliography scan
1416 records screened for inclusion
535 duplicates removed
17 studies included for qualitative synthesis
1337 excluded on title & abstract
59 excluded after obtaining full text16 had no measure of HCP attitude or belief19 had no measure of patient attitudes & beliefs/management/outcome18 did not relate HCP attitude or belief to patient beliefs/management/outcome 2 studied attitudes to narcotics1 patient satisfaction study 1 studied students not HCPs1 was another publication from same trial 1 review article
20 studies included for quality appraisal
3 excluded following quality appraisal
79 full text articles assessed for eligibility
Figure 1 Flow of studies through the review process.
B. Darlow et al. The association between health care professional attitudes and outcomes of patients with low back pain
5Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

Tab
le1
Sum
mar
yof
incl
uded
stud
ies.
Stud
yTy
pe
Cou
ntry
Sett
ing
HC
Psp
ecia
lity
Patie
ntty
pe
Res
ults
Pap
er
qua
lity
Att
itud
e/b
elie
fofH
CP
(sca
le)
Ass
ocia
tion
with
pat
ient
-rel
ated
fact
or
Bis
hop
and
Fost
er(2
005)
C-S
UK
Maj
ority
2°ca
reP
T(n
=45
3)
inM
/Sfie
ld
Thre
evi
gnet
tes
with
acut
eN
SLB
PB
iom
edic
alvs
bio
psy
cho
soci
alo
rien
tati
on
Pati
ent
man
agem
ent
Wo
rkre
com
men
da
tio
ns:
bas
ed
upon
BM
view
–th
egr
eate
rth
e
per
ceiv
edp
atho
logy
the
mor
e
likel
yth
ere
com
men
dat
ion
not
to
wor
k
M
Bis
hop
etal
.
(200
8)
C-S
UK
Maj
ority
1°ca
reG
P(n
=44
2)
PT
(n=
580)
Vig
nett
ew
ithac
ute
NSL
BP
Bio
med
ical
vsb
iop
sych
oso
cial
ori
enta
tio
n(P
AB
S)
Pati
ent
man
agem
ent
Wo
rkre
com
men
da
tio
ns:
advi
ceto
rem
ain
offw
ork
asso
ciat
edw
ith
high
erB
Msc
ores
&lo
wer
BP
S
scor
es
Gu
idel
ine
ad
her
ence
:su
bgr
oup
with
high
BM
/low
BP
Ssc
ores
mor
e
likel
yto
pro
vid
ere
com
men
dat
ions
not
alig
ned
with
guid
elin
es
M
Buc
hbin
der
etal
.
(200
1a,b
)
C-C
Aus
tral
ia1°
care
GP
(n=
2556
)Tw
ovi
gnet
tes
with
acut
e/su
b-a
cute
NSL
BP
Att
itu
des
toLB
Pp
atie
nts
&m
anag
emen
tA
ttitu
des
follo
win
gm
edia
inte
rven
tion
Pati
ent
man
agem
ent
Gu
idel
ine
ad
her
ence
:in
terv
entio
n
grou
pm
ore
likel
yto
be
alig
ned
with
guid
elin
es
M
Cou
dey
reet
al.
(200
6)
C-S
Fran
ce1°
care
GP
(n=
887)
Rep
orte
db
ehav
iour
with
acut
e/ch
roni
cLB
P
Fear
avo
idan
ceb
elie
fs(F
AB
Q)
Pati
ent
man
agem
ent
Hig
hG
PFA
BQ
Phy
sas
soci
ated
with
mor
esi
ckle
ave
pre
scri
ptio
n&
mor
ere
stri
ctiv
eac
tivity
advi
ce;l
ow
GP
FAB
QP
hys
asso
ciat
edw
ith
pro
vid
ing
mor
esp
ecifi
cLB
P
info
rmat
ion
&re
ferr
alto
spin
e
spec
ialis
t/b
ack
scho
ol
Gu
idel
ine
ad
her
ence
:hig
hG
PFA
BQ
scor
esne
gativ
ely
asso
ciat
edw
ith
follo
win
ggu
idel
ines
for
phy
sica
l&
occu
pat
iona
lact
iviti
es
H
Cou
dey
reet
al.
(200
7)
C-S
Fran
ce1°
care
GP
(n=
709)
Patie
nts
with
acut
eN
SLB
P(n
=27
27)
Fear
avo
idan
ceb
elie
fs(F
AB
Q)
Pati
ent
atti
tud
es&
bel
iefs
Wea
kco
rrel
atio
nb
etw
een
GP
s’&
pat
ient
s’fe
arav
oid
ance
bel
iefs
M
The association between health care professional attitudes and outcomes of patients with low back pain B. Darlow et al.
6 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

Tab
le1
(co
nti
nu
ed)
Stud
yTy
pe
Cou
ntry
Sett
ing
HC
Psp
ecia
lity
Patie
ntty
pe
Res
ults
Pap
er
qua
lity
Att
itud
e/b
elie
fofH
CP
(sca
le)
Ass
ocia
tion
with
pat
ient
-rel
ated
fact
or
Day
kin
and
Ric
hard
son
(200
4)
SSI
UK
2°ca
reP
T(n
=6)
in
NH
S
outp
atie
nts
Patie
nts
with
chro
nic
NSL
BP
(n=
12)
Att
itu
des
toLB
Pp
atie
nts
&m
anag
emen
tB
elie
fsab
out
&p
erce
ptio
nsof
chro
nic
LBP
Pati
ent
atti
tud
es&
bel
iefs
Bel
iefs
ab
ou
tb
ack
pa
in:
exp
lana
tions
may
chan
gep
atie
nt
bel
iefs
H
Pati
ent
man
agem
ent
Edu
cati
on
&g
uid
elin
ea
dh
eren
ce:
BM
view
refle
cted
inst
ruct
ure
orie
ntat
edp
ain
attr
ibut
ions
,
exp
lana
tions
&tr
eatm
ent
stra
tegi
es
Dea
net
al.
(200
5)
SSI
UK
2°ca
reP
T(n
=8)
in
NH
S
outp
atie
nts
Patie
nts
with
acut
e/su
b-a
cute
NSL
BP
(n=
9)
Att
itu
des
toLB
Pp
atie
nts
&m
anag
emen
tA
ttitu
des
to
ther
apeu
ticex
erci
se
Pati
ent
atti
tud
es&
bel
iefs
PTs
try
&ch
ange
pat
ient
s’b
elie
fsto
pro
mot
ead
here
nce
toan
exer
cise
regi
me.
Patie
nts
acce
pt
thei
rla
ck
ofad
here
nce
asre
ason
for
not
imp
rovi
ng
H
Hou
ben
etal
.
(200
5)
C-S
NL
Mix
edPa
ram
edic
al
ther
apis
ts
inP
P
(n=
295)
Thre
evi
gnet
tes
with
chro
nic
NSL
BP
aB
iom
edic
alvs
bio
psy
cho
soci
alo
rien
tati
on
(PA
BS)
Pati
ent
man
agem
ent
Wo
rk&
act
ivit
yre
com
men
da
tio
ns:
BM
orie
ntat
ed
ther
apis
tsvi
ewed
activ
ities
as
mor
eha
rmfu
l&ad
vise
dp
atie
nts
to
limit
dai
lyac
tivity
&w
ork
M
Laek
eman
etal
.
(200
8)
C-S
Ger
man
yM
ixed
PT
(n=
220)
bTh
ree
vign
ette
sw
ithch
roni
cN
SLB
Pa
Bio
med
ical
vsb
iop
sych
oso
cial
ori
enta
tio
n(P
AB
S)
Pati
ent
man
agem
ent
Wo
rk&
act
ivit
yre
com
men
da
tio
ns:
Cor
rela
ted
with
BM
orie
ntat
ion
M
Lint
onet
al.
(200
2)
C-S
Swed
enM
ixed
GP
(n=
60)P
T
(n=
71)
Rep
orte
db
ehav
iour
Fear
avo
idan
ceb
elie
fs(it
ems
from
TSK
,FA
BQ
,PA
IRS)
Pati
ent
man
agem
ent
Wo
rk&
act
ivit
yre
com
men
da
tio
ns:
thos
ew
ith
high
leve
lsof
fear
avoi
dan
ceb
elie
fs
pro
vid
edle
ssin
stru
ctio
nsab
out
activ
ities
M
Sic
knes
sce
rtifi
cati
on
:tho
sew
ith
high
leve
lsof
fear
avoi
dan
ceb
elie
fs
rep
orte
dsi
ckce
rtifi
cate
sto
be
a
good
trea
tmen
t
B. Darlow et al. The association between health care professional attitudes and outcomes of patients with low back pain
7Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

Tab
le1
(co
nti
nu
ed)
Stud
yTy
pe
Cou
ntry
Sett
ing
HC
Psp
ecia
lity
Patie
ntty
pe
Res
ults
Pap
er
qua
lity
Att
itud
e/b
elie
fofH
CP
(sca
le)
Ass
ocia
tion
with
pat
ient
-rel
ated
fact
or
McI
ntos
han
d
Shaw
(200
3)
SSI & FG
UK
1°ca
reG
P(n
=15
)Pa
tient
sw
ithLB
P(n
=37
)A
ttit
ud
esto
LBP
pat
ien
ts&
man
agem
ent
Info
rmat
ion
pro
visi
on&
The
Bac
kB
ook
Pati
ent
man
agem
ent
Edu
cati
on
:som
eG
Ps
relu
ctan
tto
dis
trib
ute
info
rmat
ion
mat
eria
ls
resu
lting
inin
equa
litie
sfo
rp
atie
nts
inte
rms
ofw
hat
mat
eria
lsth
ey
rece
ive.
Patie
nts
rep
orte
dre
ceiv
ing
little
orno
info
rmat
ion
from
thei
r
GP
s
H
Poir
aud
eau
etal
.
(200
6a)
C-S
Fran
ce2°
care
RH
(n=
266)
Patie
nts
with
acut
e/su
b-a
cute
LBP
(n=
443)
Fear
avo
idan
ceb
elie
fs(F
AB
Q)
Pati
ent
atti
tud
es&
bel
iefs
Fea
ra
void
an
ceb
elie
fs:
high
RH
FAB
QP
hys
scor
esi
gnifi
cant
ly
incr
ease
dri
skof
the
pat
ient
havi
ng
high
FAB
QP
hys
M
Poir
aud
eau
etal
.
(200
6a)
LFr
ance
2°ca
reR
H(n
=26
6)R
epor
ted
beh
avio
urac
ute/
chro
nic
LBP
Patie
nts
with
acut
e/su
b-a
cute
LBP
(n=
440)
Fear
avo
idan
ceb
elie
fs(F
AB
Q)
Pati
ent
man
agem
ent
Hig
hR
HFA
BQ
Phy
sas
soci
ated
with
mor
eb
edre
stp
resc
rip
tion
and
mor
ere
stri
ctiv
ew
ork
&ac
tivity
reco
mm
end
atio
ns;l
ess
likel
yto
cons
ider
mai
nob
ject
ive
of
phy
siot
hera
pyfo
rLB
Pw
asto
rein
forc
em
uscl
est
reng
thor
end
uran
ce;d
idno
td
iffer
inp
atie
nt
refe
rral
orsi
ckle
ave
pre
scri
ptio
n
Pati
ent
ou
tco
me
No
asso
ciat
ion
bet
wee
nR
HFA
BQ
scor
e&
pai
np
ersi
sten
ceat
3
mon
ths
M
Rai
nvill
eet
al.
(200
0)
C-S
USA
Mix
edG
P(n
=41
)
OS
(n=
41)
Thre
evi
gnet
tes
with
chro
nic
NSL
BP
aFe
arav
oid
ance
bel
iefs
(PA
IRS)
Pati
ent
man
agem
ent
Wo
rk&
act
ivit
yre
com
men
da
tio
ns:
corr
elat
ed
with
PAIR
Ssc
ores
M
The association between health care professional attitudes and outcomes of patients with low back pain B. Darlow et al.
8 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

Tab
le1
(co
nti
nu
ed)
Stud
yTy
pe
Cou
ntry
Sett
ing
HC
Psp
ecia
lity
Patie
ntty
pe
Res
ults
Pap
er
qua
lity
Att
itud
e/b
elie
fofH
CP
(sca
le)
Ass
ocia
tion
with
pat
ient
-rel
ated
fact
or
Sieb
enet
al.
(200
9)
LN
L1
care
GP
(n=
42)
3vi
gnet
tes
with
chro
nic
NSL
BP
a22
2
pat
ient
sw
ithac
ute
NSL
BP
Fear
avo
idan
ceb
elie
fs(P
AIR
S
&TS
K)
Pati
ent
man
agem
ent
Wo
rk&
act
ivit
yre
com
men
da
tio
ns:
(vig
nett
e)
high
erPA
IRS
&TS
Ksc
ores
asso
ciat
edw
ithre
stri
ctiv
eac
tivity
reco
mm
end
atio
ns
Ref
erra
l:(a
ctua
l)no
asso
ciat
ion
bet
wee
nPA
IRS/
TSK
scor
es&
trea
tmen
tb
ehav
iour
(dia
gnos
tic
test
s,d
rug
pre
scri
ptio
n,re
ferr
als)
Pati
ent
ou
tco
me
No
asso
ciat
ion
bet
wee
nG
P
PAIR
S/TS
Ksc
ores
&lo
ng-t
erm
(mea
n1.
9ye
ars)
pat
ient
pai
n/d
isab
ility
M
Wat
son
etal
.
(200
8)
C-S
UK
1°ca
reG
P(n
=83
)Pa
tient
sw
ithN
SLB
PB
iom
edic
alvs
bio
psy
cho
soci
alo
rien
tati
on
(PA
BS)
Pati
ent
man
agem
ent
Sic
knes
sce
rtifi
cati
on
:no
rela
tions
hip
bet
wee
nth
eB
Mor
BP
Ssc
ore
&th
enu
mb
erof
cert
ifica
tes
issu
edfo
rN
SLB
P
H
Wer
ner
etal
.
(200
5)
C-S
Nor
way
Mix
edG
P(n
=19
3)
PT
(n=
255)
CP
(n=
21)
Mem
ber
sof
the
gene
ralp
ublic
(n=
1502
)
Att
itu
des
toLB
Pp
atie
nts
&m
anag
emen
tB
elie
fsab
out
bac
kp
ain
reco
very
&su
rger
yam
ongs
tG
Ps,
PTs
&
CP
s
Pati
ent
atti
tud
es&
bel
iefs
Bel
iefs
ab
ou
tb
ack
pa
in:
pat
ient
bel
iefs
abou
tb
ack
pai
nre
cove
ry
corr
elat
edw
ithb
elie
fsof
the
HC
P
grou
pw
ithw
hom
they
had
cons
ulte
d
Key:
1,p
rim
ary;
2,se
cond
ary;
HC
P,he
alth
care
pro
fess
iona
l;C
-Cco
ncur
rent
coho
rt;C
-S,c
ross
-sec
tiona
l;FG
,foc
usgr
oup
s;L,
long
itud
inal
;SSI
,sem
i-str
uctu
red
inte
rvie
ws;
NL,
The
Net
herl
and
s;U
K,U
nite
d
King
dom
;U
SA,
Uni
ted
Stat
esof
Am
eric
a;C
P,ch
irop
ract
or;
GP,
gene
ral
pra
ctiti
oner
;M
/S,
mus
culo
skel
etal
;N
HS,
Bri
tish
Nat
iona
lH
ealth
Serv
ice;
OS,
orth
opae
dic
surg
eon;
PT,
phy
siot
hera
pis
t;
RH
,rhe
umat
olog
ist;
LBP,
low
bac
kp
ain;
NSL
BP,
non-
spec
ific
low
bac
kp
ain;
CLB
P,ch
roni
clo
wb
ack
pai
n;B
M,b
iom
edic
al;B
PS,
bio
psy
chos
ocia
l;FA
BQ
,Fea
rA
void
ance
Bel
iefs
Que
stio
nnai
re–
Phy
s,p
hysi
cal
sub
scal
e;PA
BS,
Pain
Att
itud
es&
Bel
iefs
Scal
e;PA
IRS,
Pain
&Im
pai
rmen
tR
elat
ions
hip
Scal
e;TS
K,T
amp
aSc
ale
for
Kine
siop
hob
ia;H
,hig
h;M
,mod
erat
e;L,
low
.a Id
entic
alse
tof
vign
ette
sd
evel
oped
by
Rai
nvill
eet
al.(
2000
).bTh
isst
udy
also
incl
uded
60p
hysi
othe
rapy
stud
ents
,thi
sis
not
rep
orte
das
this
revi
ewon
lyre
late
dto
qua
lified
heal
thca
rep
rofe
ssio
nals
.
B. Darlow et al. The association between health care professional attitudes and outcomes of patients with low back pain
9Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

chiropractors, rheumatologists, orthopaedic surgeons,and other paramedical therapists were investigated.These included biomedical vs biopsychosocial treat-ment orientation, fear avoidance beliefs, and attitudesto LBP patients and their management.
The association between HCP attitudes and beliefsand patientrelated factors was investigated using HCPself-reported behaviour, patient vignettes, patientquestionnaires or interviews, treatment observation oraudit, or a combination of measures. The studiesincluded acute, sub-acute and chronic LBP, as well asparticipants from the general population with previ-ous experiences of LBP. No specific LBP diagnosis wasreported by any study.
Results are described relating to the associationbetween HCP attitudes and beliefs and (i) patients’attitudes and beliefs, (ii) patient clinical management,and (iii) patient outcomes (Table 2). Strength of evi-dence is reported according to the AHCPR system(Bigos et al., 1994) (GRADE quality of evidence ratingin brackets (Guyatt et al., 2008)). Key findings aresummarised in Fig. 2.
3.1 Patient attitudes and beliefs
There is strong evidence (GRADE low quality) thatHCP beliefs about back pain are associated with thebeliefs of their patients (Daykin and Richardson, 2004;Dean et al., 2005; Werner et al., 2005), and moderateevidence (GRADE high quality) that high levels of fearavoidance beliefs in HCPs are associated with highlevels of fear avoidance beliefs in their patients(Poiraudeau et al., 2006a; Coudeyre et al., 2007).
3.2 Patient management
3.2.1 Education
There is moderate evidence (GRADE low quality) thatHCP attitudes and beliefs are associated with the typeand content of education provided to patients (McIn-tosh and Shaw, 2003; Daykin and Richardson, 2004;Coudeyre et al., 2006).
3.2.2 Work and activity recommendations
There is moderate evidence (GRADE moderatequality) that HCPs with a biomedical orientation(Bishop and Foster, 2005; Houben et al., 2005; Bishopet al., 2008; Laekeman et al., 2008) or high fear avoid-ance beliefs (Rainville et al., 2000; Coudeyre et al.,2006; Poiraudeau et al., 2006b; Sieben et al., 2009)
are more likely to advise patients with acute andchronic LBP to limit work and physical activities.
There is moderate evidence (GRADE moderatequality) that HCPs with high fear avoidance beliefs aremore likely to recommend bed rest during sick leavefor acute LBP (Coudeyre et al., 2006; Poiraudeauet al., 2006b), and that a change in HCP beliefs follow-ing a media campaign is associated with them beingless likely to prescribe bed rest (Buchbinder et al.,2001a, b).
There is moderate evidence (GRADE moderatequality) that high HCP fear avoidance beliefs are asso-ciated with increased reported sick leave prescriptionfor acute and chronic LBP (Linton et al., 2002;Coudeyre et al., 2006). There is moderate evidence(GRADE low quality) that a biomedical orientation isnot associated with the number of sickness certificatesprescribed (Watson et al., 2008).
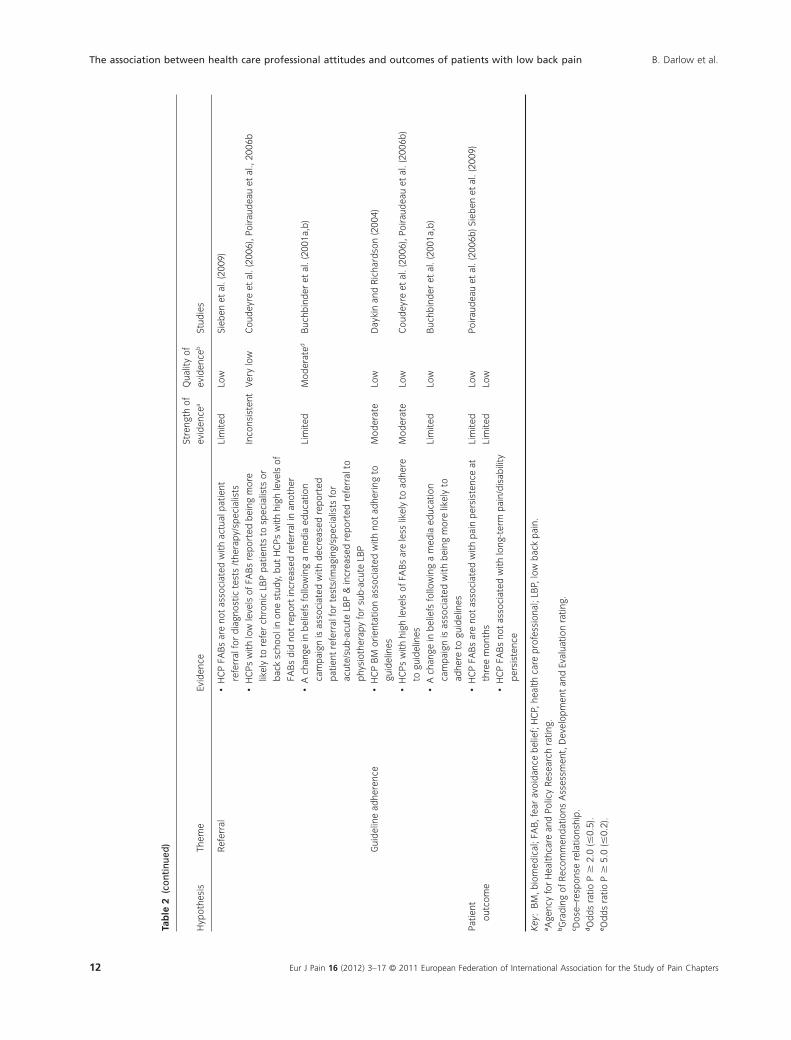
3.2.3 Referral
There is inconsistent evidence regarding the associa-tion between HCP attitudes and beliefs and patientreferral, as outlined in Table 2 (Coudeyre et al., 2006;Poiraudeau et al., 2006b).
3.2.4 Guideline adherence
There is moderate evidence (GRADE low quality) thatHCPs with a biomedical orientation (Daykin andRichardson, 2004) or high levels of fear avoidancebeliefs (Coudeyre et al., 2006; Poiraudeau et al.,2006b) are less likely to adhere to LBP treatmentguidelines.
3.3 Patient outcome
There is limited evidence (GRADE low quality) thatHCP fear avoidance beliefs are not associated with thepersistence of LBP at three months (Poiraudeau et al.,2006b) or long-term pain/disability (Sieben et al.,2009).
3.4 Generalizability
Table S5, see the online version at 10.1016/j.ejpain.2011.06.006 summarises study design andpopulation characteristics related to each finding.
4. Discussion
This systematic review demonstrates strong evidencethat the attitudes and beliefs of patients with LBP are
The association between health care professional attitudes and outcomes of patients with low back pain B. Darlow et al.
10 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

Tab
le2
Sum
mar
yof
evid
ence
.
Hyp
othe
sis
Them
eEv
iden
ce
Stre
ngth
of
evid
ence
a
Qua
lity
of
evid
ence
bSt
udie
s
Patie
ntat
titud
es
and
bel
iefs
Fear
avoi
dan
ceb
elie
fs•
Hig
hle
vels
ofFA
Bs
inH
CP
sas
soci
ated
with
high
leve
ls
ofFA
Bs
inth
eir
pat
ient
s
Mod
erat
eH
ighe
Cou
dey
reet
al.(
2007
),Po
irau
dea
uet
al.(
2006
a)
Bel
iefs
abou
tb
ack
pai
n•
HC
Pb
elie
fsab
out
bac
kp
ain
are
asso
ciat
edw
ithth
e
bel
iefs
ofth
eir
pat
ient
s
Stro
ngLo
wD
ayki
nan
dR
icha
rdso
n(2
004)
,Dea
net
al.(
2005
),W
erne
r
etal
.(20
05)
Patie
nt
man
agem
ent
Educ
atio
nre
ceiv
edb
yp
atie
nt•
HC
Ps’
BM
orie
ntat
ion
istr
ansl
ated
into
the
exp
lana
tion
give
nto
pat
ient
sab
out
the
sour
ceof
LBP
Mod
erat
eLo
wD
ayki
nan
dR
icha
rdso
n(2
004)
•H
CP
sw
ithlo
wle
vels
ofFA
Bs
mor
elik
ely
top
rovi
de
spec
ific
LBP
info
rmat
ion
Mod
erat
eLo
wC
oud
eyre
etal
.(20
06)
•H
CP
s’ne
gativ
eat
titud
eto
info
rmat
ion
mat
eria
ls
resu
ltsin
pat
ient
sno
tre
ceiv
ing
adeq
uate
info
rmat
ion
&b
eing
frus
trat
edb
yth
is
Mod
erat
eLo
wM
cInt
osh
and
Shaw
(200
3)
Wor
kan
dac
tivity
reco
mm
end
atio
ns•
HC
Ps
with
aB
Mor
ient
atio
nap
pra
ise
mov
emen
tas
bei
ngm
ore
harm
ful
Lim
ited
Low
Hou
ben
etal
.(20
05)
•H
CP
sw
ithhi
ghle
vels
ofFA
Bs
app
rais
em
ovem
ent
as
bei
ngm
ore
harm
ful
Lim
ited
Low
Sieb
enet
al.(
2009
)
•H
CP
sw
ithB
Mor
ient
atio
nad
vise
pat
ient
sto
limit
wor
k
&p
hysi
cala
ctiv
ities
Mod
erat
eM
oder
atec
Bis
hop
and
Fost
er(2
005)
,Bis
hop
etal
.(20
08),
Hou
ben
etal
.(20
05),
Laek
eman
etal
.(20
08)
•H
CP
sw
ithhi
ghle
vels
ofFA
Bs
advi
sep
atie
nts
tolim
it
wor
k&
phy
sica
lact
iviti
es
Mod
erat
eM
oder
atec
Cou
dey
reet
al.(
2006
),Po
irau
dea
uet
al.(
2006
b),
Rai
nvill
eet
al.(
2000
),Si
eben
etal
.(20
09)
•H
CP
BM
orie
ntat
ion
not
corr
elat
edw
ithnu
mb
erof
sick
ness
cert
ifica
tes
issu
ed
Mod
erat
eLo
wW
atso
net
al.(
2008
)
•H
CP
sw
ithhi
ghle
vels
ofFA
Bs
rep
ort
issu
ing
mor
e
sick
ness
cert
ifica
tes
(ass
ocia
tion
not
foun
db
yon
e
stud
y)
Mod
erat
eM
oder
ated
Lint
onet
al.(
2002
),C
oud
eyre
etal
.(20
06),
(Poi
raud
eau
etal
.,20
06b
)
•H
CP
sw
ithhi
ghle
vels
ofFA
Bs
mor
elik
ely
to
reco
mm
end
bed
rest
dur
ing
sick
leav
efo
rac
ute
LBP
Mod
erat
eLo
wC
oud
eyre
etal
.(20
06),
Poir
aud
eau
etal
.(20
06b
)
•A
chan
gein
HC
Pb
elie
fsfo
llow
ing
am
edia
cam
pai
gnis
asso
ciat
edw
ithb
eing
less
likel
yto
pre
scri
be
bed
rest
Mod
erat
eM
oder
ated
Buc
hbin
der
etal
.(20
01a,
b)
•H
CP
sw
ithhi
ghle
vels
ofFA
Bs
pro
vid
ele
ssin
stru
ctio
ns
abou
tac
tiviti
es
Lim
ited
Low
Lint
onet
al.(
2002
)
B. Darlow et al. The association between health care professional attitudes and outcomes of patients with low back pain
11Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters
Tab
le2
(co
nti
nu
ed)
Hyp
othe
sis
Them
eEv
iden
ce
Stre
ngth
of
evid
ence
a
Qua
lity
of
evid
ence
bSt
udie
s
Ref
erra
l•
HC
PFA
Bs
are
not
asso
ciat
edw
ithac
tual
pat
ient
refe
rral
for
dia
gnos
ticte
sts
/the
rapy
/sp
ecia
lists
Lim
ited
Low
Sieb
enet
al.(
2009
)
•H
CP
sw
ithlo
wle
vels
ofFA
Bs
rep
orte
db
eing
mor
e
likel
yto
refe
rch
roni
cLB
Pp
atie
nts
tosp
ecia
lists
or
bac
ksc
hool
inon
est
udy,
but
HC
Ps
with
high
leve
lsof
FAB
sd
idno
tre
por
tin
crea
sed
refe
rral
inan
othe
r
Inco
nsis
tent
Ver
ylo
wC
oud
eyre
etal
.(20
06),
Poir
aud
eau
etal
.,20
06b
•A
chan
gein
bel
iefs
follo
win
ga
med
iaed
ucat
ion
cam
pai
gnis
asso
ciat
edw
ithd
ecre
ased
rep
orte
d
pat
ient
refe
rral
for
test
s/im
agin
g/sp
ecia
lists
for
acut
e/su
b-a
cute
LBP
&in
crea
sed
rep
orte
dre
ferr
alto
phy
siot
hera
pyfo
rsu
b-a
cute
LBP
Lim
ited
Mod
erat
edB
uchb
ind
eret
al.(
2001
a,b
)
Gui
del
ine
adhe
renc
e•
HC
PB
Mor
ient
atio
nas
soci
ated
with
not
adhe
ring
to
guid
elin
es
Mod
erat
eLo
wD
ayki
nan
dR
icha
rdso
n(2
004)
•H
CP
sw
ithhi
ghle
vels
ofFA
Bs
are
less
likel
yto
adhe
re
togu
idel
ines
Mod
erat
eLo
wC
oud
eyre
etal
.(20
06),
Poir
aud
eau
etal
.(20
06b
)
•A
chan
gein
bel
iefs
follo
win
ga
med
iaed
ucat
ion
cam
pai
gnis
asso
ciat
edw
ithb
eing
mor
elik
ely
to
adhe
reto
guid
elin
es
Lim
ited
Low
Buc
hbin
der
etal
.(20
01a,
b)
Patie
nt
outc
ome
•H
CP
FAB
sar
eno
tas
soci
ated
with
pai
np
ersi
sten
ceat
thre
em
onth
s
Lim
ited
Lim
ited
Low
Low
Poir
aud
eau
etal
.(20
06b
)Sie
ben
etal
.(20
09)
•H
CP
FAB
sno
tas
soci
ated
with
long
-ter
mp
ain/
dis
abili
ty
per
sist
ence
Key:
BM
,bio
med
ical
;FA
B,f
ear
avoi
dan
ceb
elie
f;H
CP,
heal
thca
rep
rofe
ssio
nal;
LBP,
low
bac
kp
ain.
a Age
ncy
for
Hea
lthca
rean
dPo
licy
Res
earc
hra
ting.
bG
rad
ing
ofR
ecom
men
dat
ions
Ass
essm
ent,
Dev
elop
men
tan
dEv
alua
tion
ratin
g.c D
ose–
resp
onse
rela
tions
hip
.dO
dd
sra
tioP
�2.
0(�
0.5)
.e O
dd
sra
tioP
�5.
0(�
0.2)
.
The association between health care professional attitudes and outcomes of patients with low back pain B. Darlow et al.
12 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

associated with the attitudes and beliefs of the HCPwith whom they have consulted. This finding comesfrom consistent evidence from varied research meth-odologies, primary and secondary care, and a range ofspecialities, geographical locations, and cultures. It isdemonstrated in participants with acute, sub-acute,chronic, and previous experiences of LBP.
There is also moderate evidence that patient educa-tion, work and activity recommendations (includingbed rest), and guideline adherence are associated withHCP attitudes and beliefs. Finally, there is moderateevidence that HCP fear avoidance beliefs are associ-ated with reported sick leave prescription, whereasHCP biomedical orientation is not associated with thenumber of sickness certificates issued to patients withLBP.
Parsons et al. (2007) found that GPs providedpathology-based explanations for patients’ chronicmusculoskeletal pain which were grounded in a bio-medical model, and that the education provided topatients was influenced by the beliefs of the GP. Thecurrent study demonstrates similar influences on theeducation provided to LBP patients and that theseinfluences are consistent across HCP disciplines.
Studies included in this review demonstrate thatmany HCPs hold elevated fear avoidance beliefs(Linton et al., 2002; Coudeyre et al., 2006; Poiraudeau
et al., 2006b; Sieben et al., 2009), and that these beliefsare associated with higher levels of fear avoidancebeliefs in their patients, but not persistent pain anddisability. A systematic review has found patient fearavoidance beliefs to be independently associated withpersistent disability, but not pain (Ramond et al.,2011). Poiraudeau et al. (2006b) investigated only painpersistence, while Sieben et al., 2009 investigated painand disability persistence as a unidimensional con-struct. It must also be noted that Sieben et al., (2009)exluded 25 patients with the highest fear-avoidancescores and calculated Graded Chronic Pain Scale scoresbased on other measures taken at baseline, rather thanusing the scale itself (Sieben et al., 2005). This raisesquestions about the suitability of the outcome measure,especially as it is designed and validated in populationswith chronic pain (Underwood et al., 1999; Elliot et al.,2000), as opposed to their very acute sample. It is alsopossible that HCP fear avoidance beliefs may influencethe degree of these beliefs in their patients, but thestrength of this association may not be sufficient toproduce a significant effect on patient outcome, or thatsuch an association does not exist.
The contrasting findings with regards to sicknesscertification may be due to this behaviour being asso-ciated with fear avoidance beliefs rather than a bio-medical treatment orientation, or a difference between
Low quality evidence of NO association
Moderate quality evidence of associationModerate evidence of association
Strong evidence of association
Moderate evidence of NO association X
AHCPR assessment of strength of evidence
Low quality evidence of association
High quality evidence of association
GRADE assessment of quality of evidence
Health Care Professional Attitudes and Beliefs
Biomedical orientation High fear avoidance beliefs
Beliefs about back painNegative attitude to
information materialsPatient beliefs about
back painPatients less likely to receive information
Structure orientated LBP explanations
Bed rest recommended during acute LBP
High patient fear avoidance beliefs
X
Guideline non-adherence
Increased reportedsickness certification
Number of sickness certificates issued
Advice to limit work and physical activities
Figure 2 Summary of strong and moderate evidence of the association between HCP attitudes and beliefs and patient-related factors for LBP.
B. Darlow et al. The association between health care professional attitudes and outcomes of patients with low back pain
13Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

reported and actual behaviour. Actual treatmentbehaviour may be influenced by case specific factors,such as patient preferences, relationship maintenance,time pressure, and funding issues, or the GP’s generalpropensity to issue sickness certificates, thus maskingany association with HCP attitudes and beliefs(Watson et al., 2008; Sieben et al., 2009).
4.1 Strengths and limitations
A strength of this study is that it included studies ofboth quantitative and qualitative methodologies. Thisapproach provided a much richer perspective, and haspreviously been used in a related systematic review(Fullen et al., 2008). High quality quantitative andqualitative studies were considered to contributeequally to the evidence (Tomlin and Borgetto, 2011).The two methodologies produced consistent conclu-sions, and therefore strengthened the study’s conclu-sions. Although qualitative research is often notperformed with the aim of generalising to other popu-lations, by reporting the characteristics of study popu-lations and setting, judgements can be made as towhether the findings are applicable to another setting(Lincoln and Guba, 1985). Similar to the findings ofFullen et al. (2008), the majority of the quantitativestudies included were only of moderate methodologi-cal quality. In general the findings were consistentacross studies of different quality, however, thestrength of evidence generated was diminished by themodest overall quality. Three studies were excludedbased upon their low quality rating; these studies didnot contradict the review’s conclusions and had lowexternal validity.
This review used the AHCPR strength of evidenceassessment as the primary outcome measure as itallowed the integration of quantitative and qualitativeresearch evidence (Bigos et al., 1994). This gradingsystem has also been utilised in three recent LBP sys-tematic reviews (Fullen et al., 2008; Bigos et al., 2009;Kelly et al., 2011). The GRADE quality of evidenceassessment was used as a secondary outcome measureto provide consistency with Cochrane reviews (Guyattet al., 2008). The GRADE rating was generally lowerthan the AHCPR rating due to there not being amechanism to increase the GRADE based upon con-sistent findings across multiple high quality observa-tional studies.
We took several steps to minimise potential sourcesof bias in this review. We explicitly stated our hypo-theses at the outset, allowing the influence of anypossible preconceptions to be evaluated. Two review-ers independently completed each stage of the review
process, notably article screening, data extraction,quality appraisal, and thematic analysis. This reviewwas also conducted by a collaboration of reviewersfrom a number of institutions, countries, and back-grounds with different research interests, experience,and funding sources.
In this review we combined findings from studiesusing the Fear Avoidance Beliefs Questionnaire(FABQ), Tampa Scale of Kinesiophobia (TSK) and Painand Impairment Relationship Scale (PAIRS) into thecategory of Fear Avoidance Beliefs. This is analogousto the composite survey tool created by Linton et al.(2002). This allowed us to combine several relatedstudies when making strength of evidence assess-ments. These instruments provided consistent findingswhile measuring slightly different aspects of the sameconstruct, thereby increasing the external validity ofthe review’s conclusions.
Studies included in this review used a variety ofmethods to measure the association between HCP atti-tudes and beliefs and patient-related factors. Theseranged from HCP reported behaviour, to patientvignettes, measures taken directly from patients ortheir notes, and direct observation of the treatmentinteraction. Patient vignettes are easy to manipulate,and there is a reduced impact of social desirability,observer bias and Hawthorne effect; however, theymay elicit attitudes and opinions rather than actualbehaviour in real situations (Bishop and Foster, 2005).Measures taken directly from patients may be morerelevant to clinical situations; however, as patientswere recruited by participating HCPs in the studies ofpatient outcome, this may have introduced a source ofbias. A major limitation of this review is that althoughit demonstrates a strong association between the atti-tudes and beliefs of patients with LBP and those of theHCP with whom they have consulted, a causal linkcannot be implied due to the observational nature ofthe majority of studies included. An alternate expla-nation may be that patients choose their HCP accord-ing to beliefs they have already (Werner et al., 2005).
4.2 Practice and research implications
The biopsychosocial model was proposed over 30years ago (Engel, 1977), and is the basis of many LBPtreatment guidelines (Koes et al., 2001), however, anumber of relatively recent studies found that manyHCPs continue to manage their patients within a bio-medical framework. A biomedical orientation has anegative association with patient education, adher-ence to treatment guidelines, and reported work andactivity recommendations. Physiotherapists often
The association between health care professional attitudes and outcomes of patients with low back pain B. Darlow et al.
14 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

recommend activity and exercise programmes that fitwell within the biopsychosocial model; however, theyjustify these recommendations using a tissue-based(biomedical) explanatory model (Daykin and Richard-son, 2004; Dean et al., 2005). GPs acknowledge theimportance of psychosocial factors, but feel they mustprioritise screening for medical pathology, and thatthey lack the time and training to integrate psychoso-cial assessment (Crawford et al., 2007; Parsons et al.,2007). It appears that biomedical and psychosocialfactors are often viewed as being from separateschema, rather than being part of the same model.Patients experience similar difficulties to HCPs in rec-onciling the two explanatory models; they desire amedical diagnosis despite understanding that psycho-social factors influence their pain (McIntosh andShaw, 2003; Toye and Barker, 2010). Pain of psycho-social origin is often seen as being not real or thepatient’s fault (Toye and Barker, 2010). The challengeis to make the biopsychosocial model more relevant toHCPs, and less stigmatising to patients, withoutunhelpfully reinforcing the already strong biomedicalbeliefs and related behaviours of HCPs. One waywould be to place more emphasis on the bio-component of the model and the biological (neuro-physiological) processes by which psychosocial factorsinfluence pain perception and disability.
The finding that HCPs with a biomedical orientationare less likely to adhere to treatment guidelines maybe unsurprising given their biopsychosocial basis(Koes et al., 2001). The finding that HCPs withelevated fear avoidance beliefs are less likely to adhereto these guidelines is more novel and important. HCPbehaviour is often inconsistent with LBP treatmentguidelines (Foster et al., 1999; Swinkels et al., 2005;Somerville et al., 2008) despite evidence that guide-line adherence improves outcomes and decreaseshealth care utilisation (Rutten et al., 2010). ChangingHCP behaviour is a difficult and complex task; theassociation between attitudes and beliefs and behav-iour demonstrated by this review may provide afoundation for the development of complex cognitive-behaviour interventions for HCPs, similar to thosebeing developed for patients with LBP (Ammendoliaet al., 2009). Given the association between HCP atti-tudes and beliefs and patient attitudes and beliefs,such interventions may have a double benefit of opti-mising management of patients with LBP as well aspositively influencing the attitudes and beliefs of thesepatients.
The two higher quality quantitative studies includedin this review were differentiated from the otherstudies by the participation rates they achieved, their
consideration of losses and unavailable records duringanalysis, their reporting of outcomes relative to expo-sure level and the applicability of their findings(Table S2). We recommend that further longitudinalstudies be performed to investigate the associationbetween HCP attitudes and beliefs and persistent LBPdisability, using appropriate standardised outcomemeasures and researcher recruitment of patient par-ticipants. Developing a causal model for such an asso-ciation would be challenging, although it may bepossible to pre-screen HCPs for attitudes and beliefs,and then randomly allocate patients. Further qualita-tive research may also be useful to investigate causallinks.
4.3 Conclusions
This review demonstrates that HCP attitudes andbeliefs are associated with those of their patients, aswell as their clinical management of patients withLBP; HCPs need to be cognisant of this during consul-tations. The findings of this review may help informthe development of cognitive-behaviour change inter-ventions for HCPs involved in the management of LBP.
Funding
This study received no external funding. All authorshad full access to all of the data (including statisticalreports and tables) in the study and can take respon-sibility for the integrity of the data and the accuracy ofthe data analysis. Dr Sarah Dean’s time is supported byfunding from the National Institute for HealthResearch UK, in connection with her role within thePeninsula Collaboration for Leadership in AppliedHealth Research and Care.
Acknowledgements
We gratefully acknowledge the assistance of RachelEsson, Head of Research and Learning, Victoria Uni-versity of Wellington, NZ in developing the databasesearch strategies.
References
Ammendolia C, Cassidy D, Steensta I, Soklaridis S, Boyle E,Eng S, et al. Designing a workplace return-to-workprogram for occupational low back pain: an interventionmapping approach. BMC Musculoskelet Disord 2009;10:65.
Bigos SJ, Bowyer RO, Braen GR, Brown K, Deyo R, Halde-man S et al. Acute low back problems in adults. Clinical Prac-
B. Darlow et al. The association between health care professional attitudes and outcomes of patients with low back pain
15Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

tice Guideline No. 14. AHCPR Publication No. 95-0642.Rockville, MD. Agency for Health Care Policy andResearch, Public Health Service, US Department of Healthand Human Services. 1994.
Bigos SJ, Holland J, Holland C, Webster JS, Battie M,Malmgren JA. High-quality controlled trials on preventingepisodes of back problems: systematic literature review inworking-age adults. Spine J 2009;9(2):147–68.
Bishop A, Foster NE. Do physical therapists in the UnitedKingdom recognize psychosocial factors in patients withacute low back pain? Spine 2005;30(11):1316–22.
Bishop A, Thomas E, Foster NE. Health care practitioners’attitudes and beliefs about low back pain: a systematicsearch and critical review of available measurement tools.Pain 2007;132(1–2):91–101.
Bishop A, Foster NE, Thomas E, Hay EM. How does theself-reported clinical management of patients with lowback pain relate to the attitudes and beliefs of health carepractitioners? A survey of UK general practitioners andphysiotherapists. Pain 2008;135(1–2):187–95.
Brynhildsen J, Ekblad S, Hammar M. Oral contraceptivesand low back pain. Attitudes among physicians, midwivesand physiotherapists. Acta Obstet Gyn Scan 1995;74(9):714–7.
Buchbinder R, Jolley D, Wyatt M. 2001 Volvo award winnerin clinical studies: effects of a media campaign on backpain beliefs and its potential influence on management oflow back pain in general practice. Spine 2001a;26(23):2535–42.
Buchbinder R, Jolley D, Wyatt M. Population based interven-tion to change back pain beliefs and disability: three partevaluation. BMJ: Brit Med J 2001b;322(7301):1516–20.
Coudeyre E, Rannou F, Tubach F, Baron G, Coriat F, Brin S,et al. General practitioners’ fear-avoidance beliefs influ-ence their management of patients with low back pain.Pain 2006;124(3):330–7.
Coudeyre E, Tubach F, Rannou F, Baron G, Coriat F, Brin S,et al. Fear-avoidance beliefs about back pain in patientswith acute LBP. Clin J Pain 2007;23(8):720–5.
Crawford C, Ryan K, Shipton E. Exploring general practitio-ner identification and management of psychosocial YellowFlags in acute low back pain. N Z Med J 2007;120(1254):U2536.
Dagenais S, Caro J, Haldeman S. A systematic review of lowback pain cost of illness studies in the United States andinternationally. Spine J 2008;8(1):8–20.
Daykin A, Richardson B. Physiotherapists’ pain beliefs andtheir influence on the management of patients with lowback pain. Spine 2004;29(7):783–95.
Dean SG, Smith JA, Payne S, Weinman J. Managing time: aninterpretative phenomenological analysis of patients’ andphysiotherapists’ perceptions of adherence to therapeuticexercise for low back pain. Disabil Rehabil 2005;27(11):625–36.
Elliott AM, Smith BH, Smith WC, Chambers WA. Changes inchronic pain severity over time: the chronic pain grade asa valid measure. Pain 2000;88(3):303–8.
Engel GL. The need for a new medical model: a challenge forbiomedicine. Science 1977;196(4286):129–36.
Foster NE, Thompson KA, Baxter GD, Allen JM. Manage-ment of nonspecific low back pain by physiotherapists inBritain and Ireland. A descriptive questionnaire of currentclinical practice. Spine 1999;24(13):1332–42.
Fullen BM, Baxter GD, O’Donovan BG, Doody C, Daly L,Hurley DA. Doctors’ attitudes and beliefs regarding acutelow back pain management: a systematic review. Pain2008;136(3):388–96.
Genaidy AM, Lemasters GK, Lockey J, Succop P, Deddens J,Sobeih T, et al. An epidemiological appraisal instrument –a tool for evaluation of epidemiological studies. Ergonom-ics 2007;50(6):920–60.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y,Alonso-Coello P, et al. GRADE: an emerging consensus onrating quality of evidence and strength of recommenda-tions. BMJ 2008;336(7650):924–6.
Houben RMA, Ostelo RWJG, Vlaeyen JWS, Wolters PMJC,Peters M, Stomp-van Den Berg SGM. Health care provid-ers’ orientations towards common low back pain predictperceived harmfulness of physical activities and recom-mendations regarding return to normal activity. Euro JPain 2005;9(2):173–83.
Houben RMA, Vlaeyen JWS, Peters M, Ostelo RWJG,Wolters PMJC, Stomp-Van Den Berg SGM. Health careproviders’ attitudes and beliefs towards common low backpain: factor structure and psychometric properties of theHC-PAIRS. Clin J Pain 2004;20(1):37–44.
Kelly GA, Blake C, Power CK, O’Keeffe D, Fullen BM. Theassociation between chronic low back pain and sleep: asystematic review. Clin J Pain 2011;27(2):169–81.
Kendall NA, Linton SJ, Main CJ. Guide to assessing psycho-social yellow flags in acute low back pain: risk factors forlong-term disability and work loss, October 2004 ed. Well-ington, New Zealand: Accident Compensation Corporationand the New Zealand Guidelines Group; 1997.
Koes BW, van Tulder MW, Ostelo R, Kim Burton A, WaddellG. Clinical guidelines for the management of low backpain in primary care: an international comparison. Spine2001;26(22):2504–13.
Laekeman MALE, Sitter H, Basler HD. The pain attitudes andbeliefs scale for physiotherapists: psychometric propertiesof the German version. Clin Rehabil 2008;22(6):564–75.
Lincoln YS, Guba EG. Naturalistic inquiry. Beverly Hills,California: Sage Publications; 1985.
Linton SJ, Vlaeyen J, Ostelo R. The back pain beliefs ofhealth care providers: are we fear-avoidant? J OccupRehabil 2002;12(4):223–32.
Main CJ, Foster N, Buchbinder R. How important are backpain beliefs and expectations for satisfactory recovery fromback pain? Best Pract Res Clin Rheumatol 2010;24(2):205–17.
McIntosh A, Shaw CF. Barriers to patient information pro-vision in primary care: patients’ and general practitioners’experiences and expectations of information for low backpain. Health Expectations 2003;6(1):19–29.
The association between health care professional attitudes and outcomes of patients with low back pain B. Darlow et al.
16 Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters

Parsons S, Harding G, Breen A, Foster N, Pincus T, Vogel S,et al. The influence of patients’ and primary care practi-tioners’ beliefs and expectations about chronic musculosk-eletal pain on the process of care: a systematic review ofqualitative studies. Clin J Pain 2007;23(1):91–8.
Poiraudeau S, Rannou F, Baron G, Henanff AL, Coudeyre E,Rozenberg S, et al. Fearavoidance beliefs about back painin patients with subacute low back pain. Pain 2006a;124(3):305–11.
Poiraudeau S, Rannou F, Le Henanff A, Coudeyre E, Rozen-berg S, Huas D, et al. Outcome of subacute low back pain:influence of patients’ and rheumatologists’ characteristics.Rheumatology 2006b;45(6):718–23.
Public Health Resource Unit. 10 questions to help you make sense ofqualitative research 2006. <http://www.phru.nhs.uk/Doc_Links/Qualitative%20Appraisal%20Tool.pdf> (accessed14.02.10).
Rainville J, Carlson N, Polatin P, Gatchel RJ, Indahl A, VolinnE. Exploration of physicians’ recommendations for activi-ties in chronic low back pain. Spine 2000;25(17):2210–20.
Ramond A, Bouton C, Richard I, Roquelaure Y, Baufreton C,Legrand E, et al. Psychosocial risk factors for chronic lowback pain in primary care – a systematic review. Fam Pract2011;28:12–21.
Rupert RL. A survey of practice patterns and the healthpromotion and prevention attitudes of US chiropractors.Maintenance care: Part I. J Manip Physiol Therap 2000;23(1):1–9.
Rutten GM, Degen S, Hendriks EJ, Braspenning JC, HartingJ, Oostendorp RA. Adherence to clinical practice guide-lines for low back pain in physical therapy: do patientsbenefit? Phys Ther 2010;90(8):1111–22.
Sieben JM, Vlaeyen JW, Portegijs PJ, Verbunt JA, van Riet-Rutgers S, Kester AD, et al. A longitudinal study on thepredictive validity of the fear-avoidance model in low backpain. Pain 2005;117(1–2):162–70.
Sieben JM, Vlaeyen JWS, Portegijs PJM, Warmenhoven FC,Sint AG, Dautzenberg N, et al. General practitioners’ treat-ment orientations towards low back pain: influence ontreatment behaviour and patient outcome. Eur J Pain2009;13(4):412–8.
Somerville S, Hay E, Lewis M, Barber J, van der Windt D, HillJ, et al. Content and outcome of usual primary care forback pain: a systematic review. Br J Gen Pract 2008;58(556):790–7.
Swinkels IC, van den Ende CH, van den Bosch W, Dekker J,Wimmers RH. Physiotherapy management of low backpain: does practice match the Dutch guidelines? Aust JPhysiother 2005;51(1):35–41.
Tomlin G, Borgetto B. Research pyramid: a new evidence-based practice model for occupational therapy. Am JOccup Ther 2011;65(2):189–96.
Toye F, Barker K. ‘Could I be imagining this?’ – the dialecticstruggles of people with persistent unexplained back pain.Disabil Rehabil 2010;32(21):1722–32.
van Tulder MW, Koes BW, Bouter LM. A cost-of-illnessstudy of back pain in The Netherlands. Pain 1995;62(2):233–40.
Underwood MR, Barnett AG, Vickers MR. Evaluation of twotime-specific back pain outcome measures. Spine1999;24(11):1104–12.
Vlaeyen JW, Linton SJ. Are we “fear-avoidant”? Pain2006;124(3):240–1.
Watson PJ, Bowey J, Purcell-Jones G, Gales T. General prac-titioner sickness absence certification for low back pain isnot directly associated with beliefs about back pain. Eur JPain 2008;12(3):314–20.
Werner EL, Ihlebaek C, Skouen JS, Laerum E. Beliefs aboutlow back pain in the Norwegian general population: arethey related to pain experiences and health professionals?Spine 2005;30(15):1770–6.
Wieser S, Horisberger B, Schmidhauser S, Eisenring C,Brugger U, Ruckstuhl A, et al. Cost of low back pain inSwitzerland in 2005. Eur J Health Econ; 2010.
Supporting information
Additional Supporting Information may be found inthe online version of this article:
Table S1 Medline via Ovid Search Strategy.Table S2 Quality appraisal of quantitative studiesusing the Epidemiological appraisal Instrument(Genaidy et al., 2007).Table S3 Quality appraisal of qualitative studies usingthe Critical Appraisal Skills Programme (CASP) system(Public Health Resource Unit, 2006).Table S4 Extended summary of included studies.Table S5 Summary of findings including externalvalidity information.
Please note: Wiley-Blackwell are not responsible forthe content or functionality of any supporting mate-rials supplied by the authors. Any queries (other thanmissing material) should be directed to the corre-sponding author for the article.
B. Darlow et al. The association between health care professional attitudes and outcomes of patients with low back pain
17Eur J Pain 16 (2012) 3–17 © 2011 European Federation of International Association for the Study of Pain Chapters
Related Documents











