The Art of Medical Prophylaxis, Impacting the Patient Early Anna Falanga, MD Hemostasis and Thrombosis Center Hematology-Oncology Dept Ospedali Riuniti Bergamo, Italy Satellite Symposium “Guidelines on Prevention and Treatment of Cancer-Associated Thrombosis” Stockholm, September 16, 2008

The Art of Medical Prophylaxis, Impacting the Patient Early Anna Falanga, MD Hemostasis and Thrombosis Center Hematology-Oncology Dept Ospedali Riuniti.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Art of Medical Prophylaxis, Impacting the Patient Early
Anna Falanga, MDHemostasis and Thrombosis Center
Hematology-Oncology DeptOspedali Riuniti Bergamo, Italy
Satellite Symposium
“Guidelines on Prevention and Treatment of Cancer-Associated Thrombosis”
Stockholm, September 16, 2008

Adapted from: 1. ACCP 2004. 1.Geerts WH, et al. Chest. 2004;126:S338–S400, 2. Cohen A et al. Lancet 2008:371;387-394.
Medical Conditions
• Although VTE is most often considered to be associated with recent surgery or trauma, 50 to 70% of symptomatic thromboembolic (TE) events and 70 to 80% of fatal pulmonary embolism (PE) occur in non-surgical patients1
• PE accounts for 5-10% of deaths in hospitalized patients, making VTE the most common preventable cause of in-hospital death2

Venous Thromboembolism (VTE) Risk
• Hospitalized medical cancer patients are at increased risk for VTE
• Out of hospital cancer patients receiving therapy are at risk for VTE
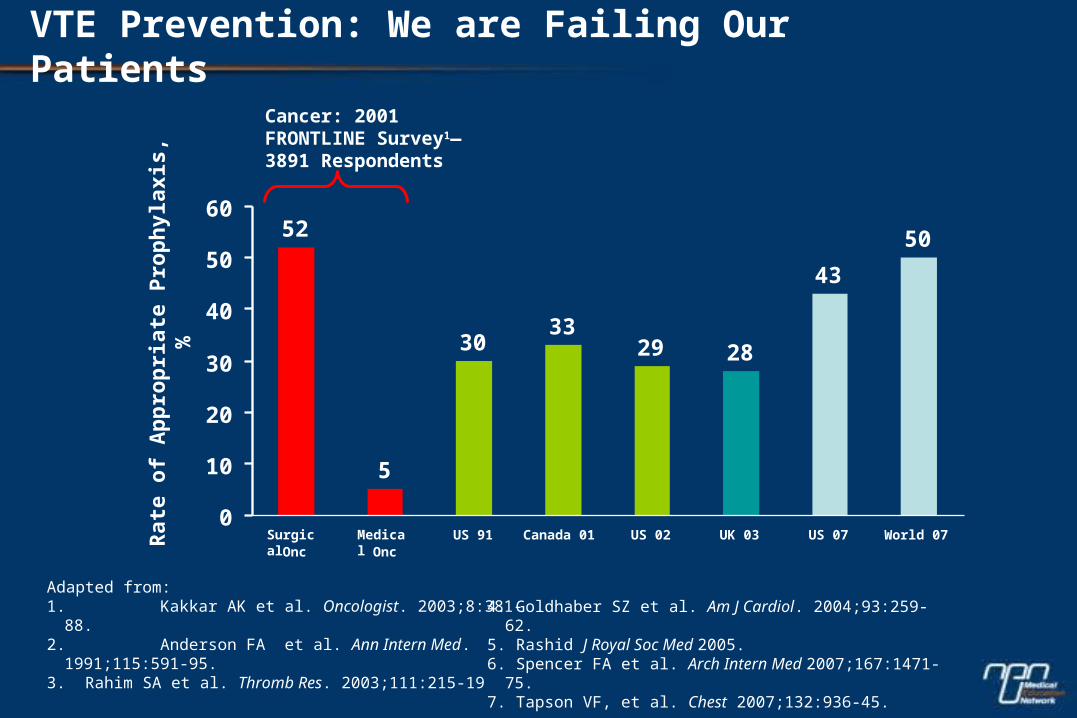
VTE Prevention: We are Failing Our Patients
Adapted from:1. Kakkar AK et al. Oncologist. 2003;8:381-88.2. Anderson FA et al. Ann Intern Med. 1991;115:591-95. 3. Rahim SA et al. Thromb Res. 2003;111:215-19
Cancer: 2001FRONTLINE Survey1— 3891 Respondents
Rat
e o
f A
pp
rop
riat
e P
rop
hyl
axis
, %
4. Goldhaber SZ et al. Am J Cardiol. 2004;93:259-62.5. Rashid J Royal Soc Med 2005.6. Spencer FA et al. Arch Intern Med 2007;167:1471-75.7. Tapson VF, et al. Chest 2007;132:936-45.
5
3033
29 28
43
5052
0
10
20
30
40
50
60
SurgicalOnc
MedicalOnc
US 91 Canada 01 US 02 UK 03 US 07 World 07

Recommendations for VTE Prophylaxis in Patients with Cancer Released by International Medical Oncology Societies
• AIOM (Italian Medical Oncology Society) - 2006
• ASCO (American Society of Clinical Oncology) - 2007
• NCCN (National Comprehensive Cancer Network) - 2007, 2008
• ESMO (European Society of Medical Oncology) - 2008

Recommendations for VTE Prophylaxis in Hospitalized Patients with Cancer
• Hospitalized patients with cancer should be considered candidates for VTE prophylaxis in the absence of bleeding or other contraindications to anticoagulation
Contraindications to Anticoagulation
• Active, uncontrollable bleeding• Active cerebrovascular hemorrhage• Dissecting or cerebral aneurysm• Bacterial endocarditis• Pericarditis, active peptic or other GI ulceration• Severe, uncontrolled or malignant hypertension• Severe head trauma• Pregnancy (warfarin)• Heparin-induced thrombocytopenia (heparin, LMWH) • Epidural catheter placement.

Prophylaxis in Acutely Ill Medical Patients
• No randomized clinical trials designed a priori for hospitalized medical cancer patients
• Randomized, placebo-controlled trials in acutely ill hospitalized medical patients
– MEDENOX1- enoxaparin 40 mg daily
– PREVENT2 - dalteparin 5000U daily
– ARTEMIS3 - fondaparinux 2.5 mg daily
Adapted from:1. Samama et al. N Engl J Med 1999;341:793-800;2. Leizorovicz et al. Circulation 2004;110:874-79;3. Cohen et al. Blood 2003; 102(11): 15.
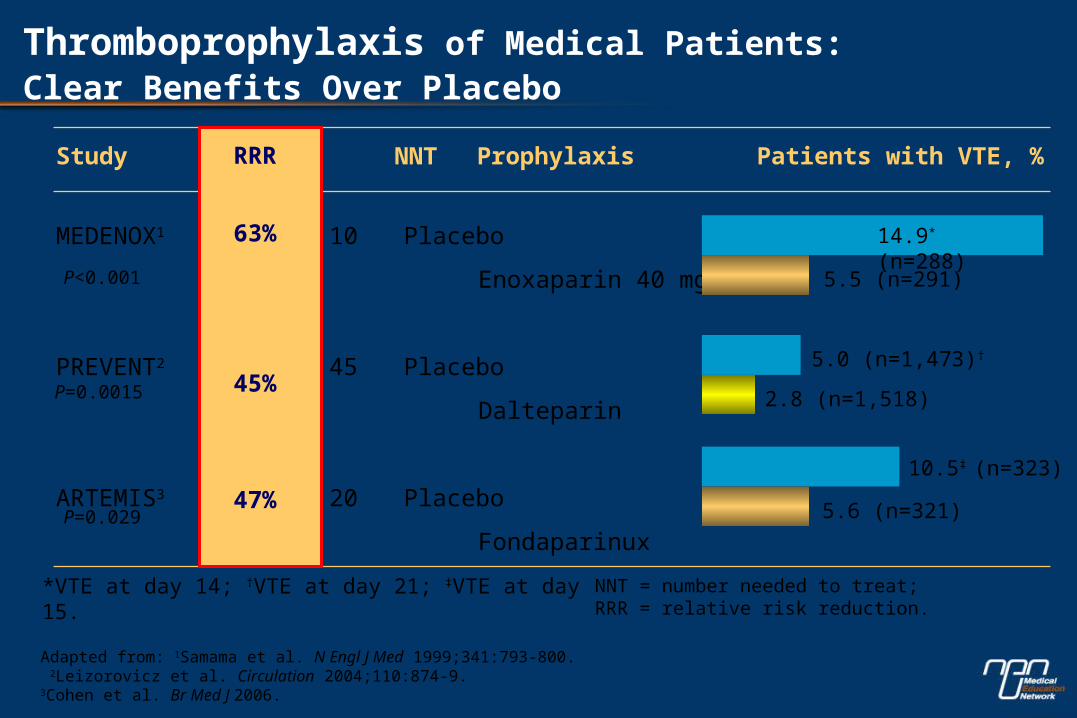
MEDENOX1 63% 10 Placebo
Enoxaparin 40 mg
PREVENT2 49% 45 Placebo
Dalteparin
ARTEMIS3 47% 20 Placebo
Fondaparinux
Study RRR NNT Prophylaxis Patients with VTE, %
Adapted from: 1Samama et al. N Engl J Med 1999;341:793-800. 2Leizorovicz et al. Circulation 2004;110:874-9.3Cohen et al. Br Med J 2006.
P<0.001
P=0.0015
P=0.029
NNT = number needed to treat; RRR = relative risk reduction.
RRR
63%
45%
47%
14.9* (n=288)
5.5 (n=291)
5.0 (n=1,473)†
2.8 (n=1,518)
10.5‡ (n=323)
5.6 (n=321)
*VTE at day 14; †VTE at day 21; ‡VTE at day 15.
Thromboprophylaxis of Medical Patients: Clear Benefits Over Placebo

MEDENOX PREVENT ARTEMIS
Enox. 2.1 %
Placebo 6.6 %
Dalte. 2.6 %
Placebo 5.0 %
Fond. 1.5 %
Placebo 3.4 %
P = 0.002 P = 0.085P = 0.037
Proximal DVT + Symptomatic VTE at D14-21
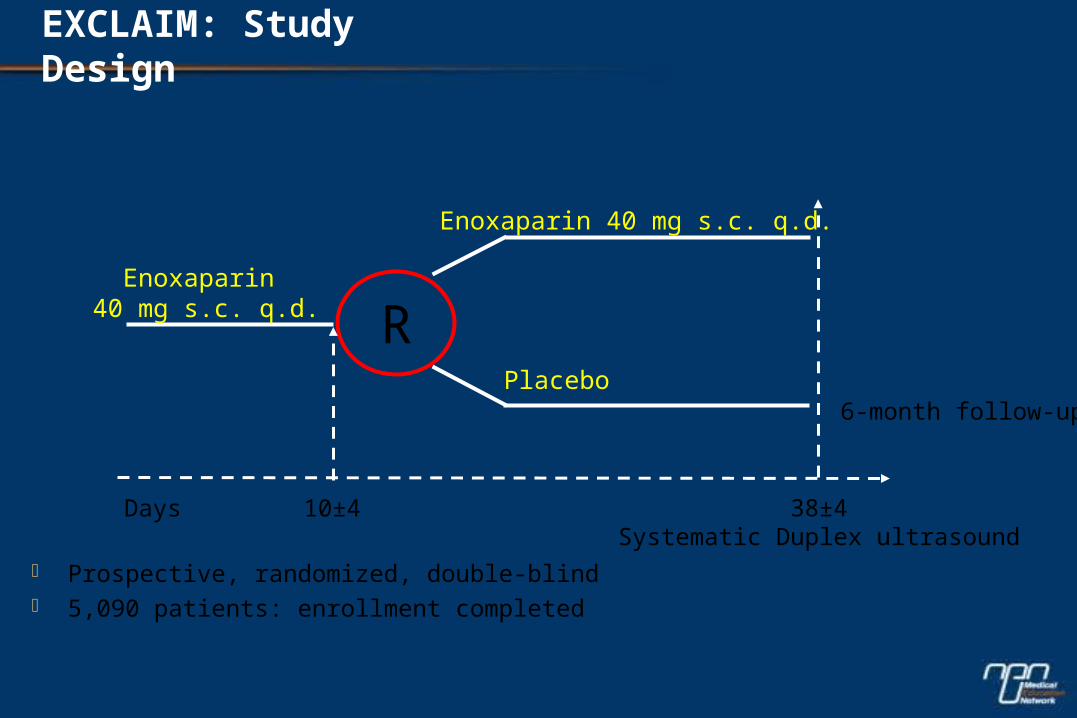
REnoxaparin
40 mg s.c. q.d.
Enoxaparin 40 mg s.c. q.d.
Placebo
10±4 38±4Systematic Duplex ultrasound
Days
6-month follow-up
EXCLAIM: Study Design
Prospective, randomized, double-blind 5,090 patients: enrollment completed
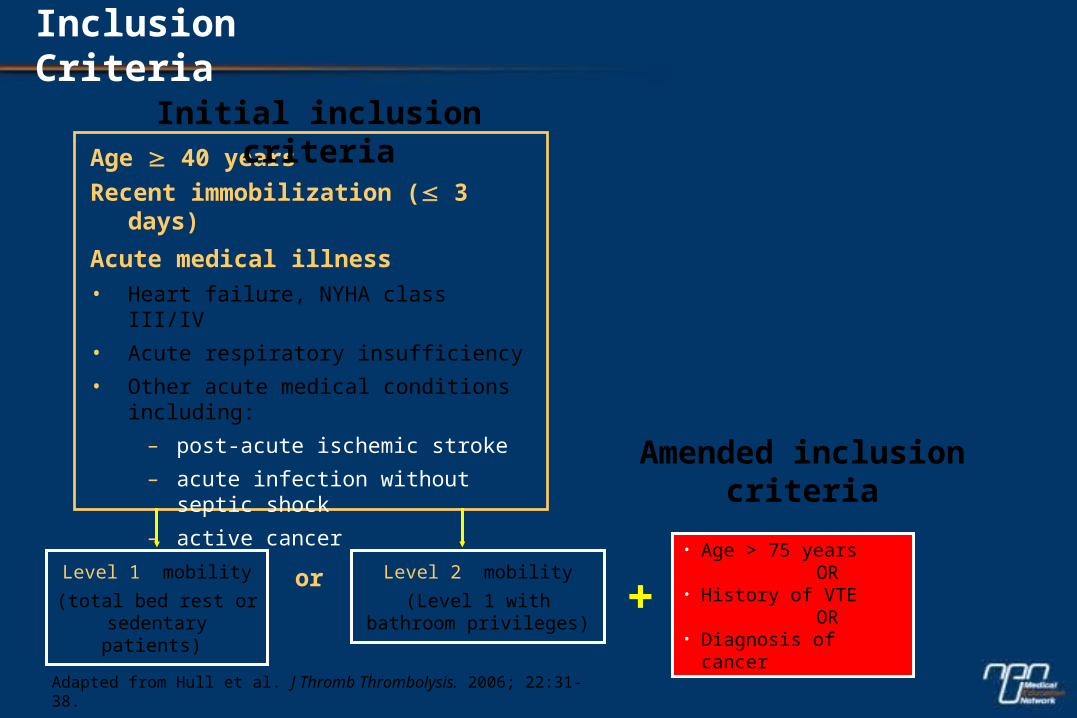
Inclusion Criteria
Adapted from Hull et al. J Thromb Thrombolysis. 2006; 22:31-38.
• Age > 75 years OR• History of VTE OR • Diagnosis of cancer
+
Age 40 years
Recent immobilization ( 3 days)
Acute medical illness• Heart failure, NYHA class III/IV
• Acute respiratory insufficiency
• Other acute medical conditions including:
– post-acute ischemic stroke
– acute infection without septic shock
– active cancer
Level 1 mobility
(total bed rest or sedentary patients)
Level 2 mobility
(Level 1 withbathroom privileges)
or
Initial inclusion criteria
Amended inclusion criteria
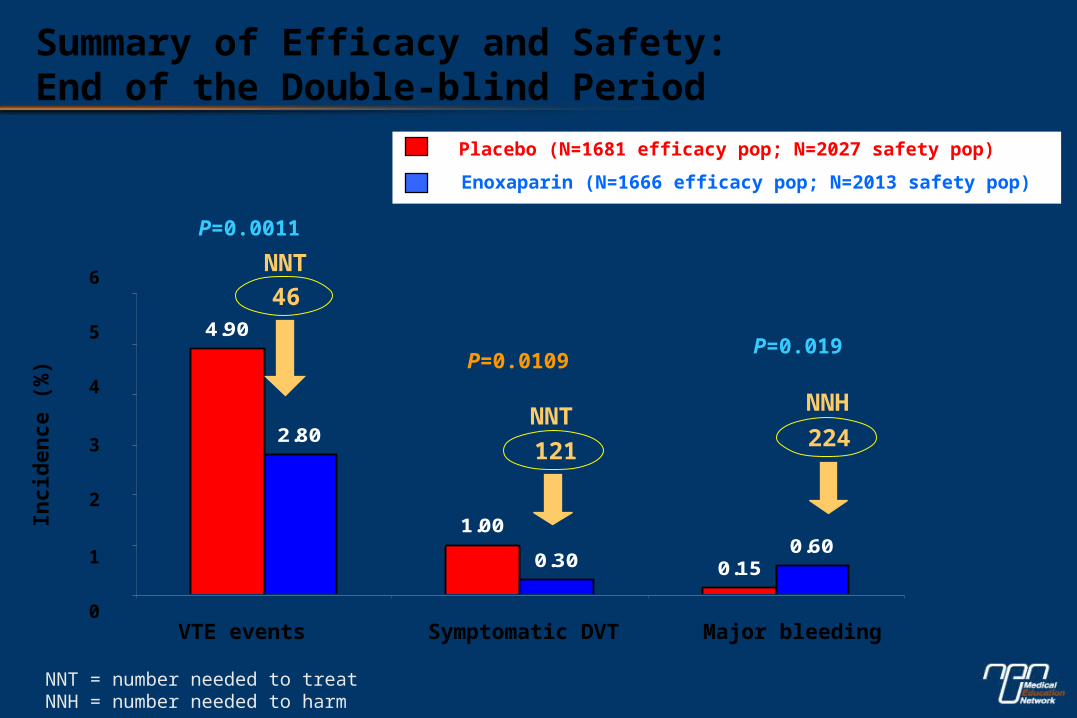
4.90
1.00
0.15
2.80
0.300.60
VTE events Major bleeding
P=0.0011
P=0.019
Symptomatic DVT
P=0.0109
121
NNT
NNT = number needed to treat NNH = number needed to harm
0
1
2
3
4
5
6
Inci
den
ce (
%)
224
NNH
46
NNT
Summary of Efficacy and Safety:End of the Double-blind Period
Placebo (N=1681 efficacy pop; N=2027 safety pop)
Enoxaparin (N=1666 efficacy pop; N=2013 safety pop)
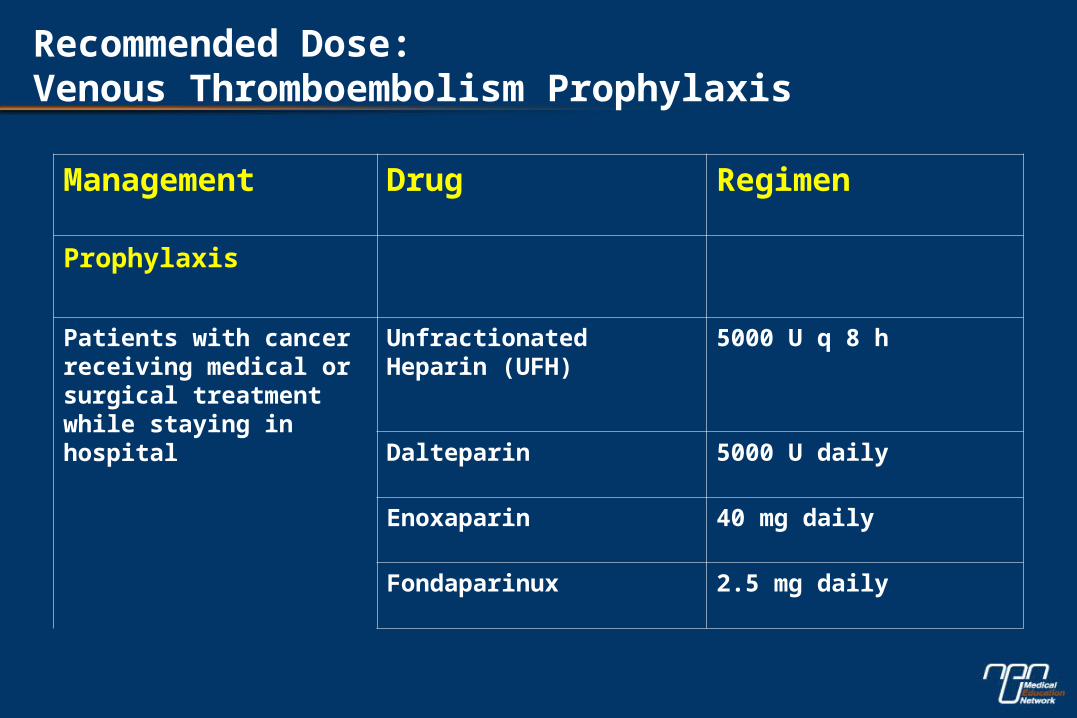
Recommended Dose: Venous Thromboembolism Prophylaxis
Management Drug Regimen
Prophylaxis
Patients with cancer receiving medical or surgical treatment while staying in hospital
Unfractionated Heparin (UFH)
5000 U q 8 h
Dalteparin 5000 U daily
Enoxaparin 40 mg daily
Fondaparinux 2.5 mg daily

Prophylaxis in Medical Patients: Ambulatory Cancer Patients
• The role of thromboprophylaxis in ambulatory cancer patients during chemotherapy and hormone therapy is not established.
• One double-blind placebo-controlled RCT demonstrated the efficacy of low-intensity warfarin (INR 1.3-1.9) in patients receiving chemotherapy for metastatic breast cancer (Levine MN et al, Lancet 1994).

Patients * Warfarin Placebo p=n=152 n=159
Thromboembolicevents 1 7 0.031
relative risk reduction = 85%
* women receiving chemotherapy for metastatic breast cancer
Adapted from Levine et al., Lancet 1994.
Double Blind Randomized Trial of Very-low-dose Warfarin (INR 1.3-1.9) for Prevention of Thromboembolism in Stage IV Breast Cancer
Warfarin Prophylaxis: Limitations
• Very difficult schedule
• Interaction with cytotoxics
• Tested only in breast cancer
Prophylaxis of VTE in Medical Cancer Patients
• LMWH benefits
– Predictable anticoagulant effect
– Single daily administration
– Reduced toxicity (thrombocytopenia, osteoporosis)
– Acceptable safety profile in oncological patient (long term use in recent studies: FAMOUS, CLOT)
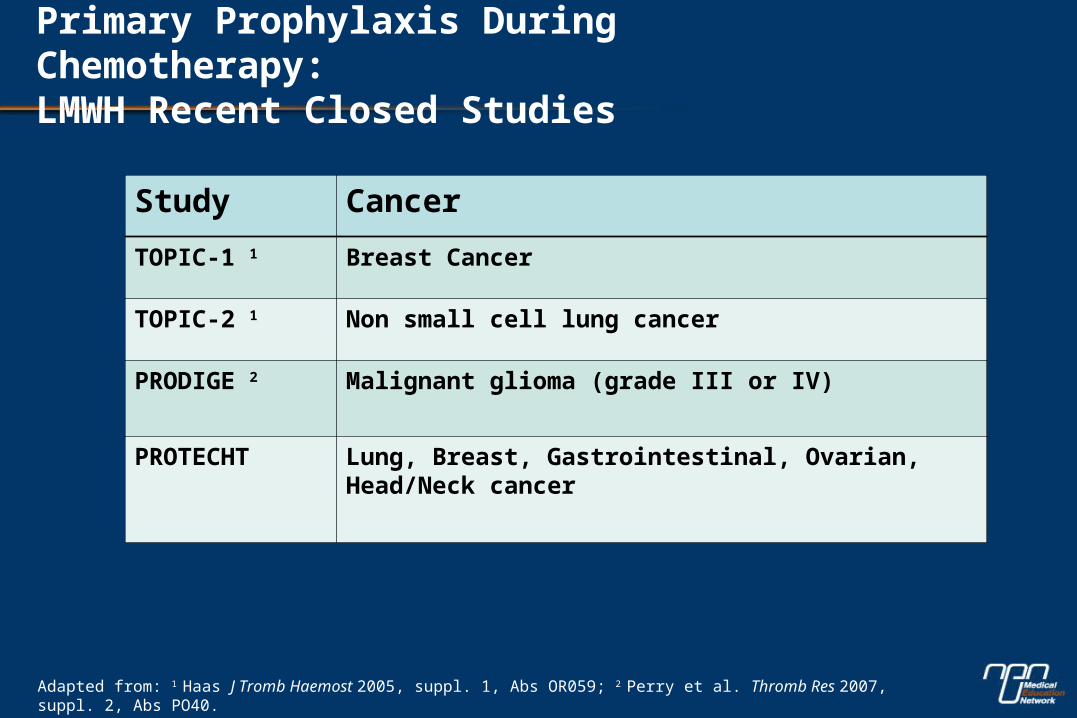
Primary Prophylaxis During Chemotherapy: LMWH Recent Closed Studies
Study Cancer
TOPIC-1 1 Breast Cancer
TOPIC-2 1 Non small cell lung cancer
PRODIGE 2 Malignant glioma (grade III or IV)
PROTECHT Lung, Breast, Gastrointestinal, Ovarian, Head/Neck cancer
Adapted from: 1 Haas J Tromb Haemost 2005, suppl. 1, Abs OR059; 2 Perry et al. Thromb Res 2007, suppl. 2, Abs PO40.
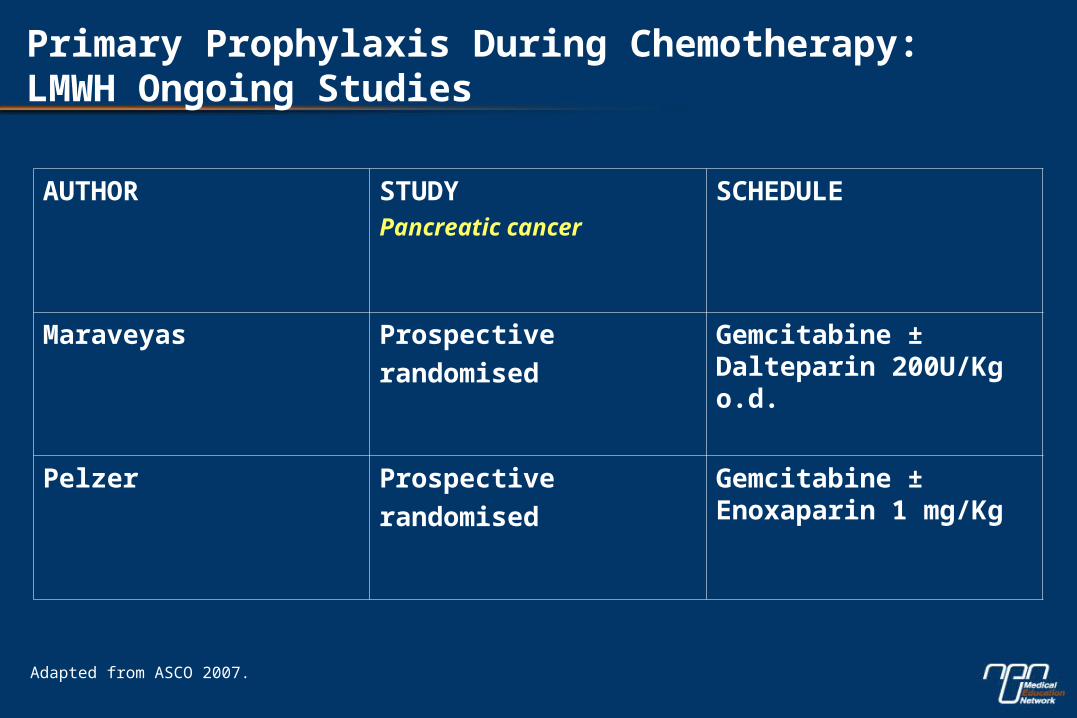
Primary Prophylaxis During Chemotherapy:LMWH Ongoing Studies
AUTHOR STUDYPancreatic cancer
SCHEDULE
Maraveyas Prospective
randomised
Gemcitabine ± Dalteparin 200U/Kg o.d.
Pelzer Prospective
randomised
Gemcitabine ± Enoxaparin 1 mg/Kg
Adapted from ASCO 2007.
Recommendations for Primary VTE Prophylaxis in Ambulatory Patients with Cancer
• Current guidelines do not recommend:
– Routine prophylaxis with an antithrombotic agent in ambulatory cancer patients

Special consideration: Prophylaxis in Multiple Myeloma patients
• Prophylaxis with LMWH or adjusted dose warfarin (INR~1.5) is recommended in multiple myeloma patients receiving thalidomide or lenalidomide + chemotherapy or dexamethasone (high VTE risk).
• However:– No RCTs available – Recommendation is based on extrapolation from non-
randomized trials or randomized studies in other similar high-risk categories
– Well-designed RCTs are urgently needed
Adapted from ASCO Guidelines, JCO 2007.

Central Venous Catheter (CVC) – Related Thrombosis
Prophylaxis of CVC - Related Thrombosis
• The presence of CVC is a risk factor for VTE.
• Three recent clinical trials have assessed that the incidence of CVC-related symptomatic thrombosis is approximately 3% to 4%.
• These trials failed to show a significant effect of prophylaxis with 1 mg fixed dose warfarin, or LMWH dalteparin, or LMWH enoxaparin in reducing symptomatic and asymptomatic thrombosis in patients with cancer.
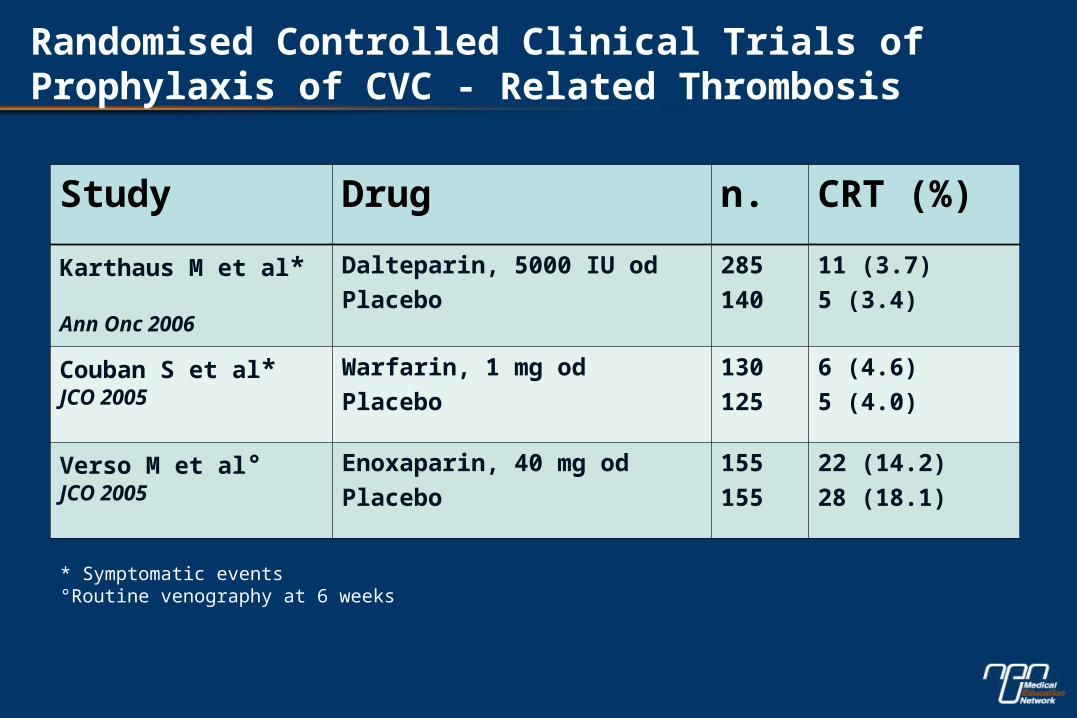
Randomised Controlled Clinical Trials of Prophylaxis of CVC - Related Thrombosis
Study Drug n. CRT (%)
Karthaus M et al* Ann Onc 2006
Dalteparin, 5000 IU od
Placebo
285
140
11 (3.7)
5 (3.4)
Couban S et al*JCO 2005
Warfarin, 1 mg od
Placebo
130
125
6 (4.6)
5 (4.0)
Verso M et al° JCO 2005
Enoxaparin, 40 mg od
Placebo
155
155
22 (14.2)
28 (18.1)
* Symptomatic events°Routine venography at 6 weeks

• Current guidelines agree that extensive, routine prophylaxis to prevent CVC-related VTE is not recommended. To date prophylaxis might be tailored according to individual risk level.
Recommendations for Prophylaxis for CVC – Related Thrombosis
Conclusion
• Evidence from epidemiological and clinical studies demonstrates that not only surgical patients but also medical patients with acute medical conditions and predisposing risk factors are at significant risk of VTE.
• Hospitalized cancer patients should be assessed for risk of VTE and given appropriate thromboprophylaxis.
• Early intervention with thromboprophylaxis (i.e. LMWH) will impact cancer patient outcome.
Related Documents











