THE Anesthetic Pipeline: THE Anesthetic Pipeline: How It Will Change Your How It Will Change Your Practice Practice Steven L. Shafer, MD Steven L. Shafer, MD Professor of Anesthesia, Stanford University Professor of Anesthesia, Stanford University Adjunct Professor of Biopharmaceutical Sciences, Adjunct Professor of Biopharmaceutical Sciences, UCSF UCSF Incoming Editor in Chief, Anesthesia & Analgesia Incoming Editor in Chief, Anesthesia & Analgesia

The anesthetic pipeline
May 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
THE Anesthetic Pipeline: THE Anesthetic Pipeline: How It Will Change Your How It Will Change Your
PracticePractice
Steven L. Shafer, MDSteven L. Shafer, MDProfessor of Anesthesia, Stanford UniversityProfessor of Anesthesia, Stanford University
Adjunct Professor of Biopharmaceutical Sciences, UCSFAdjunct Professor of Biopharmaceutical Sciences, UCSFIncoming Editor in Chief, Anesthesia & AnalgesiaIncoming Editor in Chief, Anesthesia & Analgesia
DisclosureDisclosure
This is a talk about the future.This is a talk about the future. Most of the drugs discussed are not Most of the drugs discussed are not
approved.approved. I’ve consulted with AstraZeneca I’ve consulted with AstraZeneca
(Propofol), Theravance (THRX (Propofol), Theravance (THRX 918661), Cognetix (Contulakin-G)918661), Cognetix (Contulakin-G)
OutlineOutline HypnoticsHypnotics
Novel Propofol FormulationsNovel Propofol Formulations A New Rapidly Metabolized hypnoticA New Rapidly Metabolized hypnotic
Muscle RelaxantsMuscle Relaxants A new relaxantA new relaxant A new mechanism of relaxant reversalA new mechanism of relaxant reversal
AnalgesicsAnalgesics Novel opioidsNovel opioids Other centrally acting analgesicsOther centrally acting analgesics Peripherally acting analgesicsPeripherally acting analgesics
HypnoticsHypnotics
What’s New With What’s New With Propofol?Propofol?
How to improve on propofol:How to improve on propofol: Less pain on injectionLess pain on injection Less toxic lipid formulationLess toxic lipid formulation
““Propofol ICU syndrome” may be partly Propofol ICU syndrome” may be partly caused by the long chain triglyceridescaused by the long chain triglycerides
Faster offsetFaster offset Less contamination riskLess contamination risk
Propofol FormulationsPropofol Formulations
Lipuro PropofolLipuro Propofol Propofol in medium chain triglyceridesPropofol in medium chain triglycerides Identical PK/PD profileIdentical PK/PD profile Less pain on injectionLess pain on injection Unavailable in the US, perhaps because Unavailable in the US, perhaps because
of the lack of EDTAof the lack of EDTA
Propofol FormulationsPropofol Formulations
IDD-D PropofolIDD-D Propofol Propofol in medium chain triglyceridesPropofol in medium chain triglycerides 2% formulation2% formulation Slower onset than DiprivanSlower onset than Diprivan Increased pain on injectionIncreased pain on injection
Increased pain on injection makes this a Increased pain on injection makes this a nonstarter in my viewnonstarter in my view
Propofol FormulationsPropofol Formulations
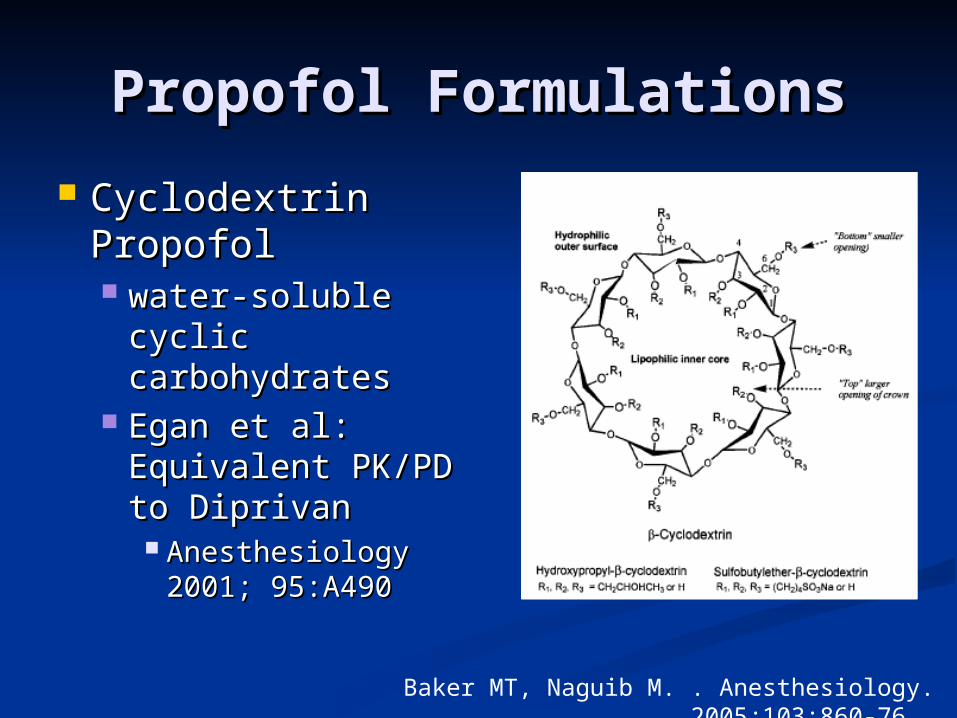
Cyclodextrin Cyclodextrin PropofolPropofol water-soluble water-soluble
cyclic cyclic carbohydratescarbohydrates
Egan et al: Egan et al: Equivalent PK/PD Equivalent PK/PD to Diprivanto Diprivan Anesthesiology Anesthesiology
2001; 95:A4902001; 95:A490
Baker MT, Naguib M. . Anesthesiology. 2005;103:860-76.
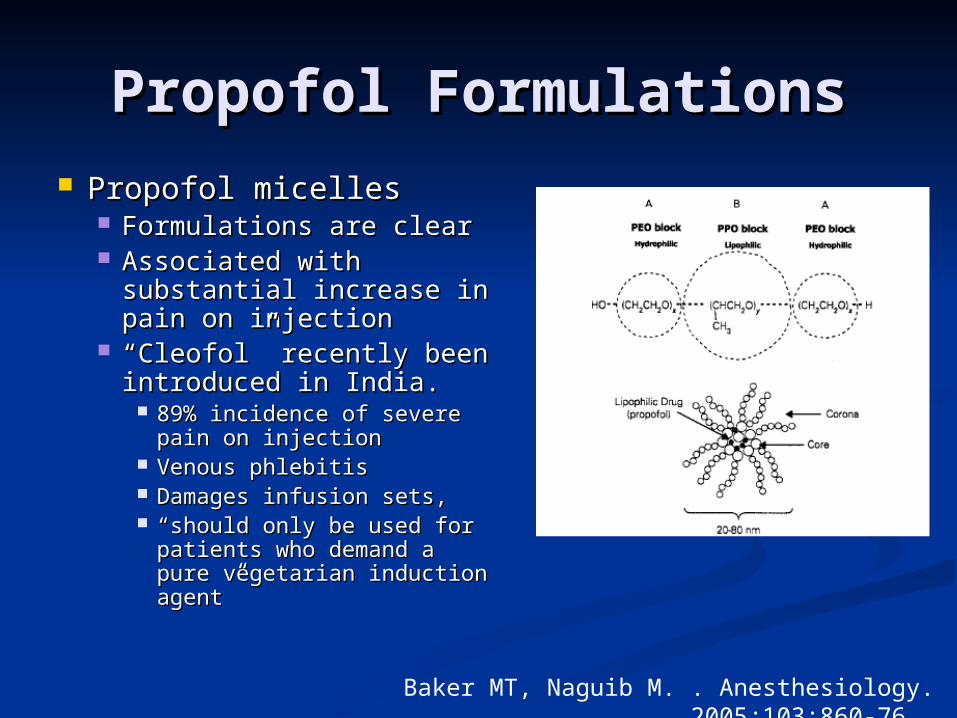
Propofol FormulationsPropofol Formulations Propofol micellesPropofol micelles
Formulations are clearFormulations are clear Associated with Associated with
substantial increase in substantial increase in pain on injectionpain on injection
““Cleofol” recently been Cleofol” recently been introduced in India.introduced in India.
89% incidence of severe 89% incidence of severe pain on injectionpain on injection
Venous phlebitisVenous phlebitis Damages infusion sets, Damages infusion sets, ““should only be used for should only be used for
patients who demand a patients who demand a pure vegetarian induction pure vegetarian induction agent”agent”
Baker MT, Naguib M. . Anesthesiology. 2005;103:860-76.
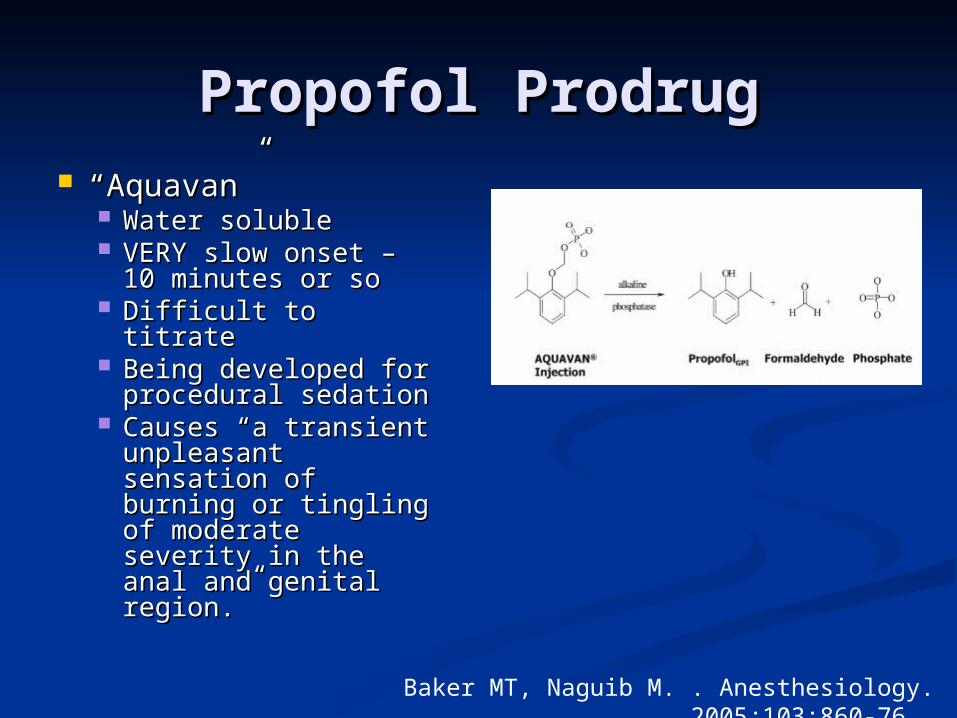
Propofol ProdrugPropofol Prodrug ““Aquavan”Aquavan”
Water solubleWater soluble VERY slow onset – VERY slow onset –
10 minutes or so10 minutes or so Difficult to titrateDifficult to titrate Being developed for Being developed for
procedural sedationprocedural sedation Causes “a transient Causes “a transient
unpleasant unpleasant sensation of burning sensation of burning or tingling of or tingling of moderate severity in moderate severity in the anal and genital the anal and genital region.”region.”
Baker MT, Naguib M. . Anesthesiology. 2005;103:860-76.
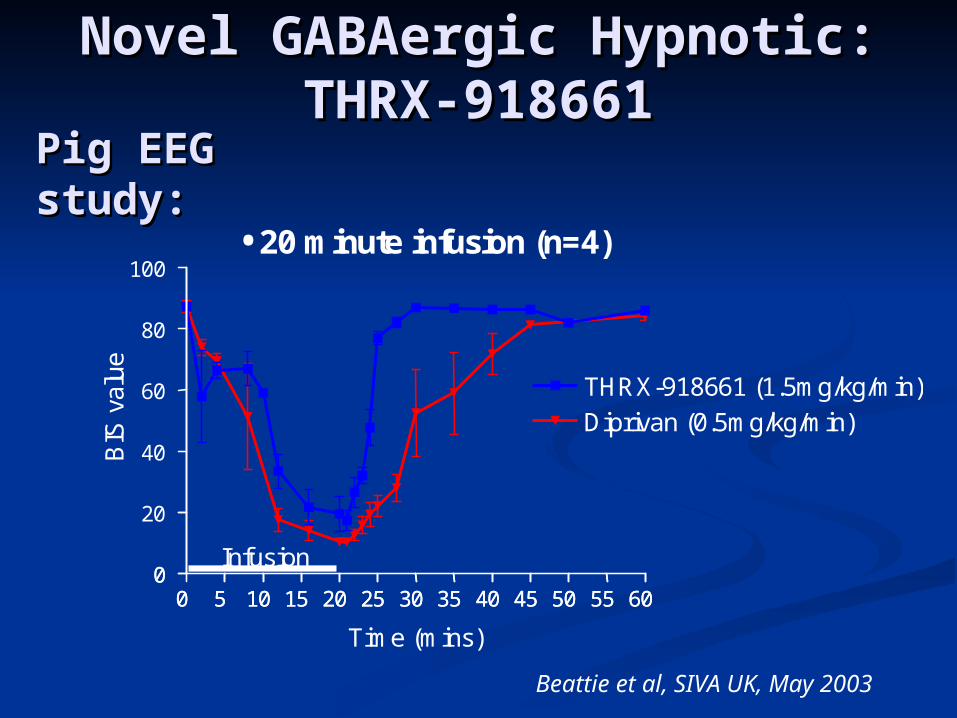
Novel GABAergic Hypnotic:Novel GABAergic Hypnotic:THRX-918661THRX-918661
0 5 10 15 20 25 30 35 40 45 50 55 6000 5 10 15 20 25 30 35 40 45 50 55 60
0
20
40
60
80
100
THRX-918661 (1.5mg/kg/min)Diprivan (0.5mg/kg/min)
Infusion
Time (mins)
BIS
val
ue
•20 minute infusion(n=4)
Beattie et al, SIVA UK, May 2003
Pig EEG Pig EEG study:study:
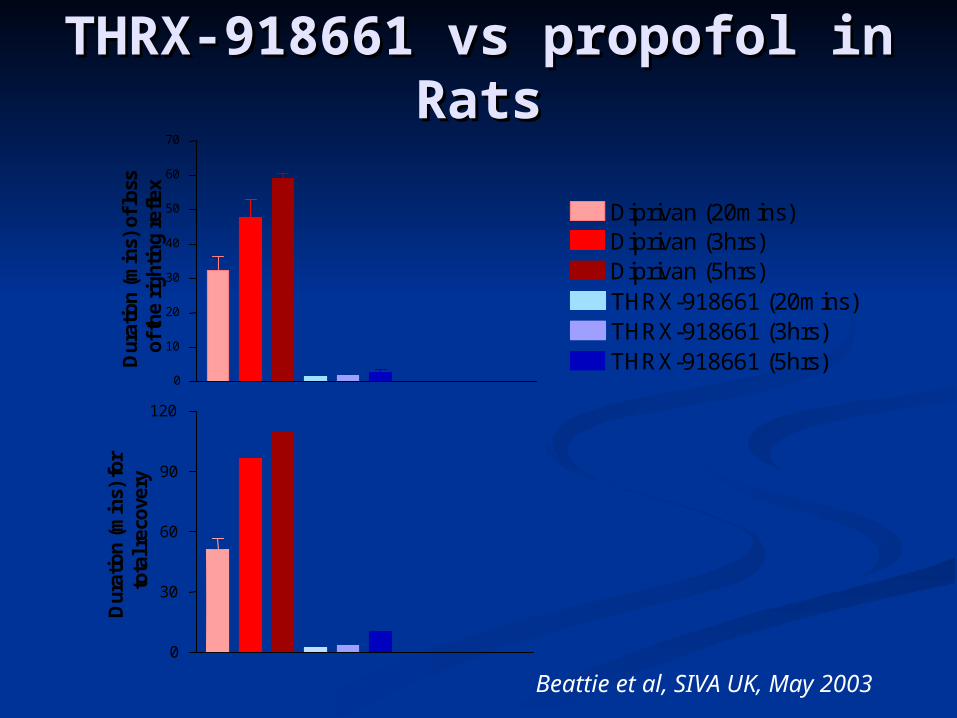
THRX-918661 vs propofol THRX-918661 vs propofol in Ratsin Rats
0
10
20
30
40
50
60
70
Diprivan (20mins)Diprivan (3hrs)Diprivan (5hrs)THRX-918661 (20mins)THRX-918661 (3hrs)THRX-918661 (5hrs)D
urat
ion
(min
s) o
f los
sof
the
right
ing
refle
x
0
30
60
90
120
Dur
atio
n (m
ins)
for
tota
l rec
over
y
Beattie et al, SIVA UK, May 2003
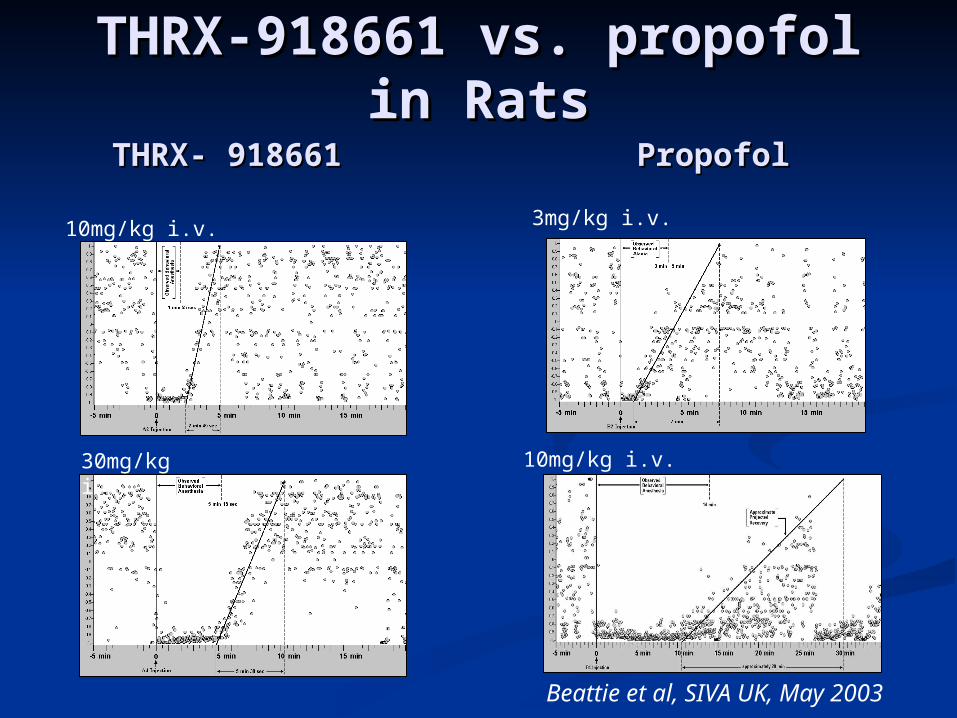
THRX-918661 vs. propofol THRX-918661 vs. propofol in Ratsin Rats
THRX- 918661THRX- 918661
10mg/kg i.v.
30mg/kg i.v.
PropofolPropofol
3mg/kg i.v.
10mg/kg i.v.
Beattie et al, SIVA UK, May 2003
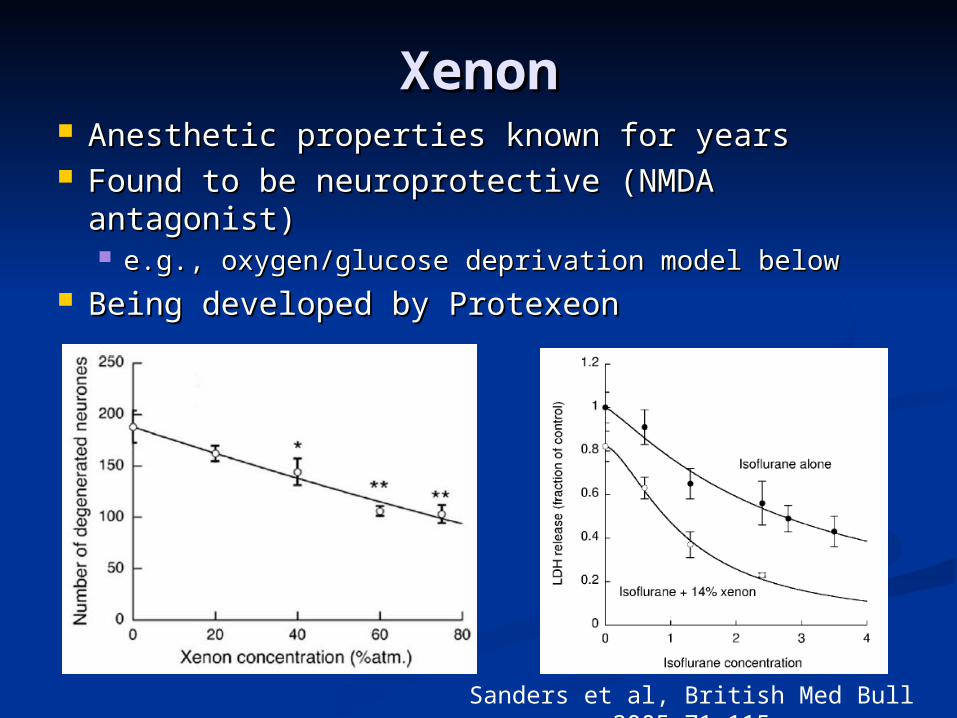
XenonXenon Anesthetic properties known for yearsAnesthetic properties known for years Found to be neuroprotective (NMDA antagonist)Found to be neuroprotective (NMDA antagonist)
e.g., oxygen/glucose deprivation model belowe.g., oxygen/glucose deprivation model below Being developed by ProtexeonBeing developed by Protexeon
Sanders et al, British Med Bull 2005 71:115
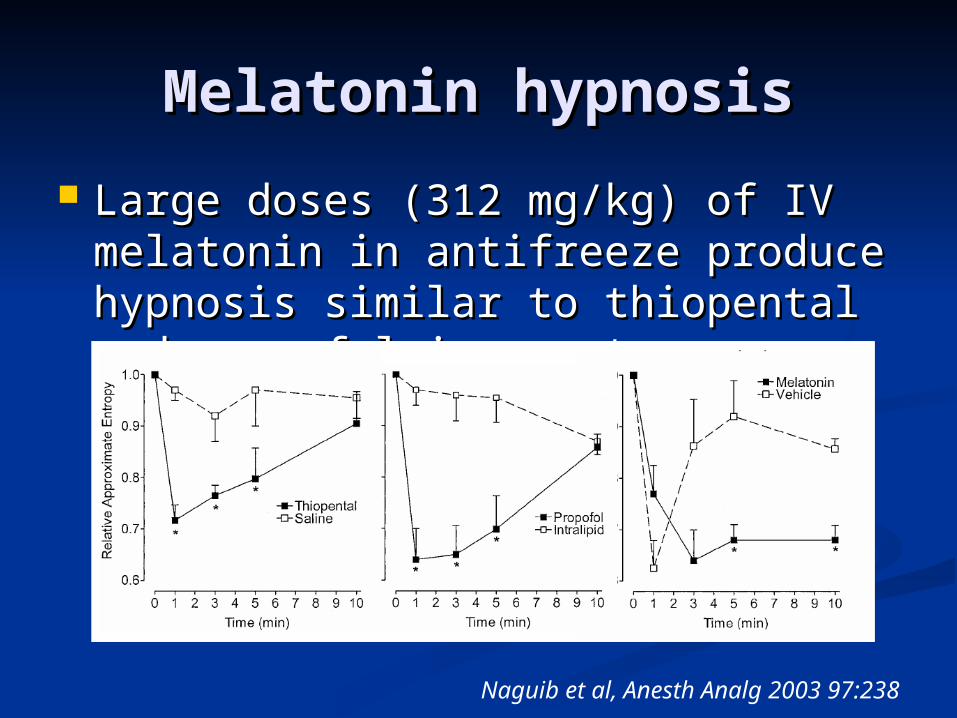
Melatonin hypnosisMelatonin hypnosis
Large doses (312 mg/kg) of IV Large doses (312 mg/kg) of IV melatonin in antifreeze produce melatonin in antifreeze produce hypnosis similar to thiopental and hypnosis similar to thiopental and propofol in a rat.propofol in a rat.
Naguib et al, Anesth Analg 2003 97:238
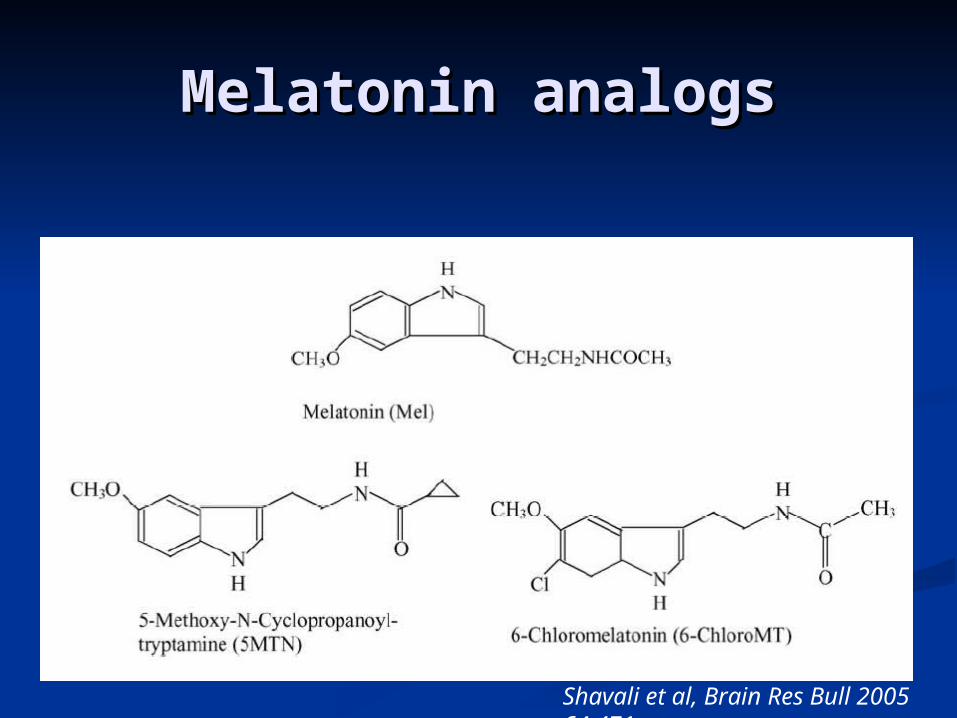
Melatonin analogsMelatonin analogs
Shavali et al, Brain Res Bull 2005 64:471
Muscle RelaxantsMuscle Relaxants
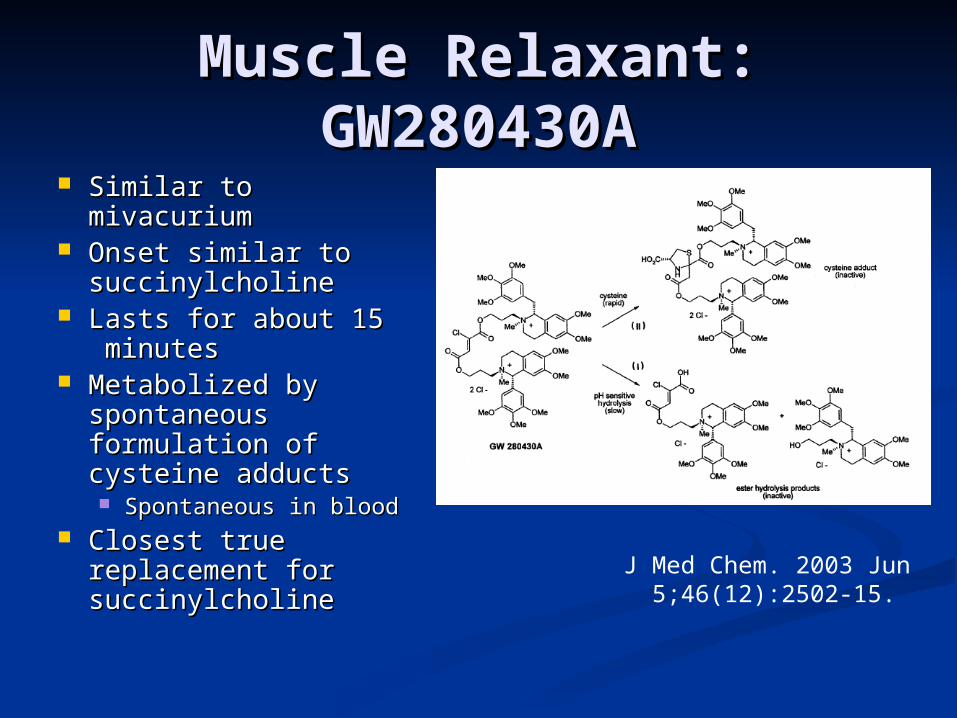
Muscle Relaxant: Muscle Relaxant: GW280430AGW280430A
Similar to Similar to mivacuriummivacurium
Onset similar to Onset similar to succinylcholinesuccinylcholine
Lasts for about 15 Lasts for about 15 minutesminutes
Metabolized by Metabolized by spontaneous spontaneous formulation of formulation of cysteine adductscysteine adducts Spontaneous in bloodSpontaneous in blood
Closest true Closest true replacement for replacement for succinylcholinesuccinylcholine
J Med Chem. 2003 Jun 5;46(12):2502-15.
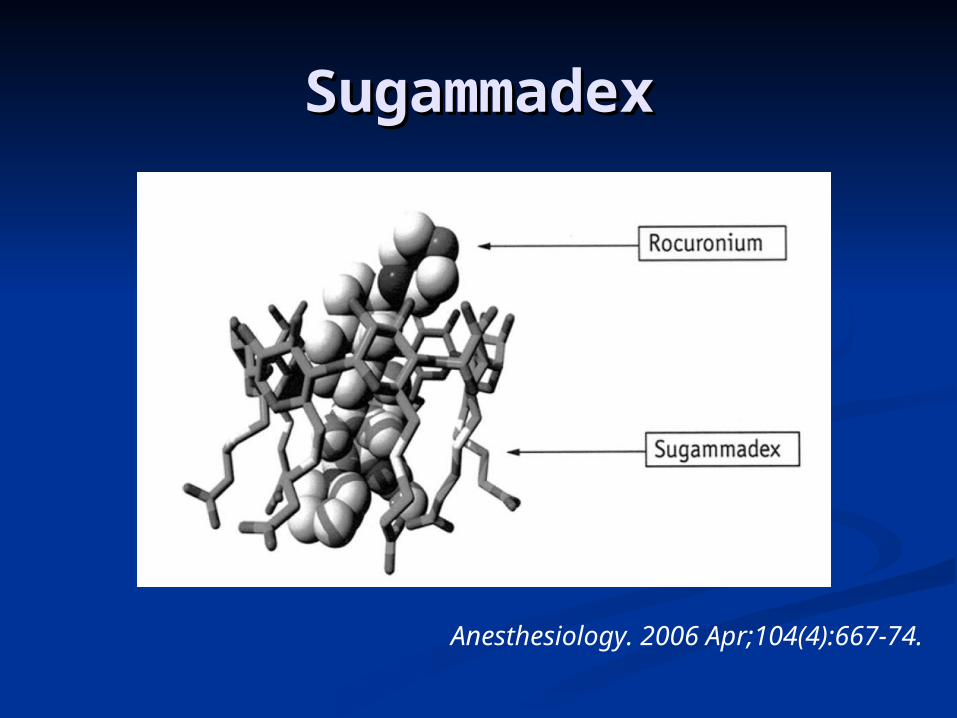
SugammadexSugammadex
Anesthesiology. 2006 Apr;104(4):667-74.
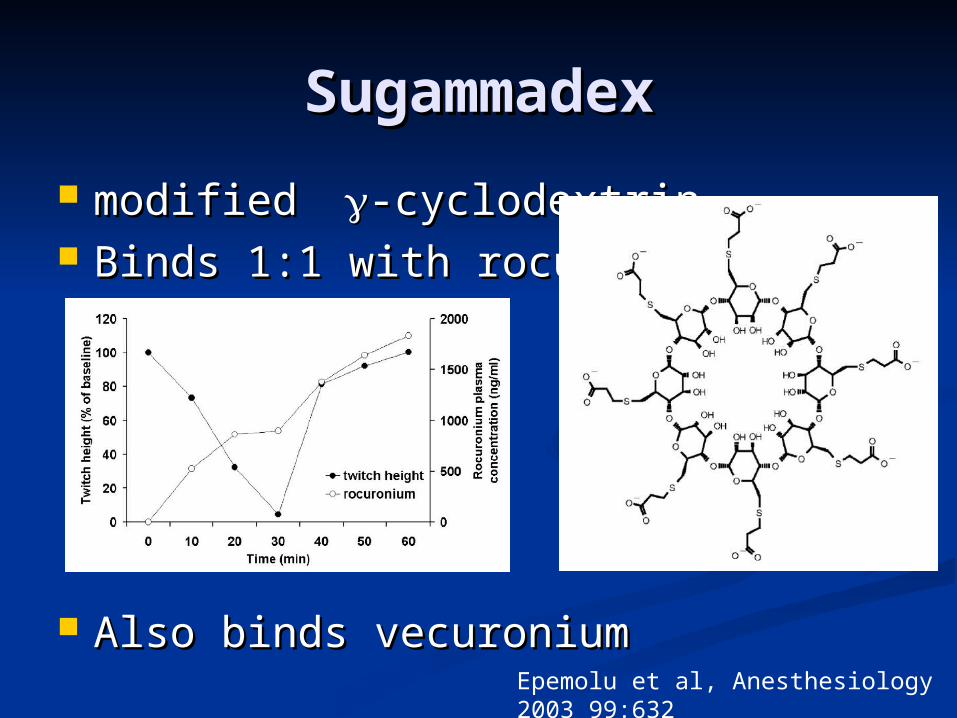
SugammadexSugammadex
modified modified -cyclodextrin-cyclodextrin Binds 1:1 with rocuroniumBinds 1:1 with rocuronium
Also binds vecuroniumAlso binds vecuroniumEpemolu et al, Anesthesiology 2003 99:632
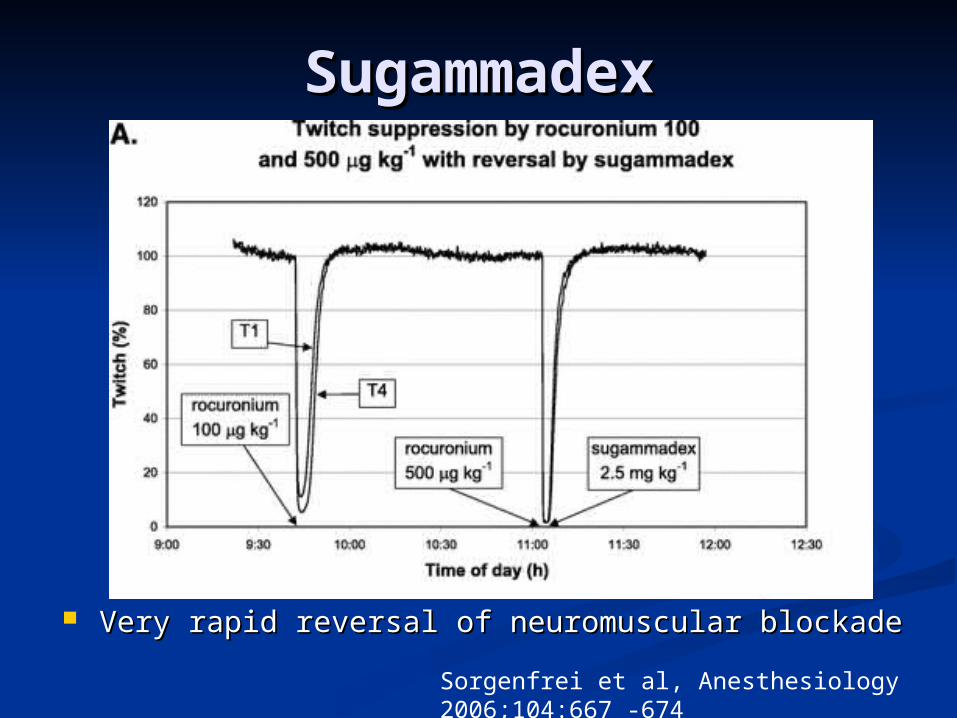
SugammadexSugammadex
Very rapid reversal of neuromuscular blockadeVery rapid reversal of neuromuscular blockade
Sorgenfrei et al, Anesthesiology 2006;104:667 -674
AnalgesicsAnalgesics
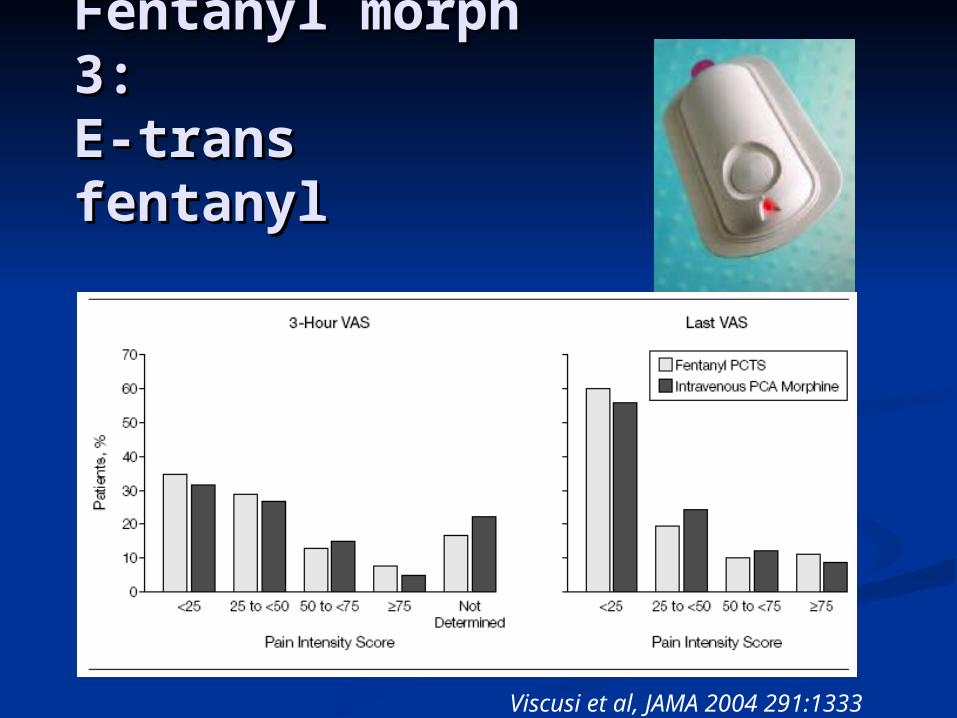
Fentanyl morph Fentanyl morph 3:3:E-trans E-trans fentanylfentanyl
Viscusi et al, JAMA 2004 291:1333
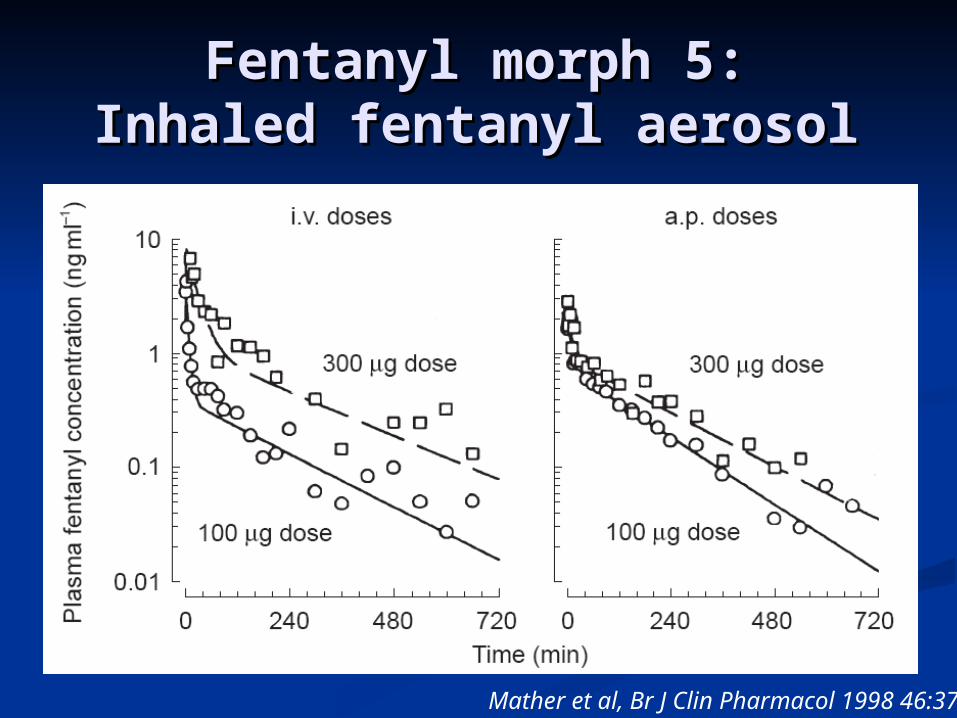
Fentanyl morph 5:Fentanyl morph 5:Inhaled fentanyl aerosolInhaled fentanyl aerosol
Mather et al, Br J Clin Pharmacol 1998 46:37
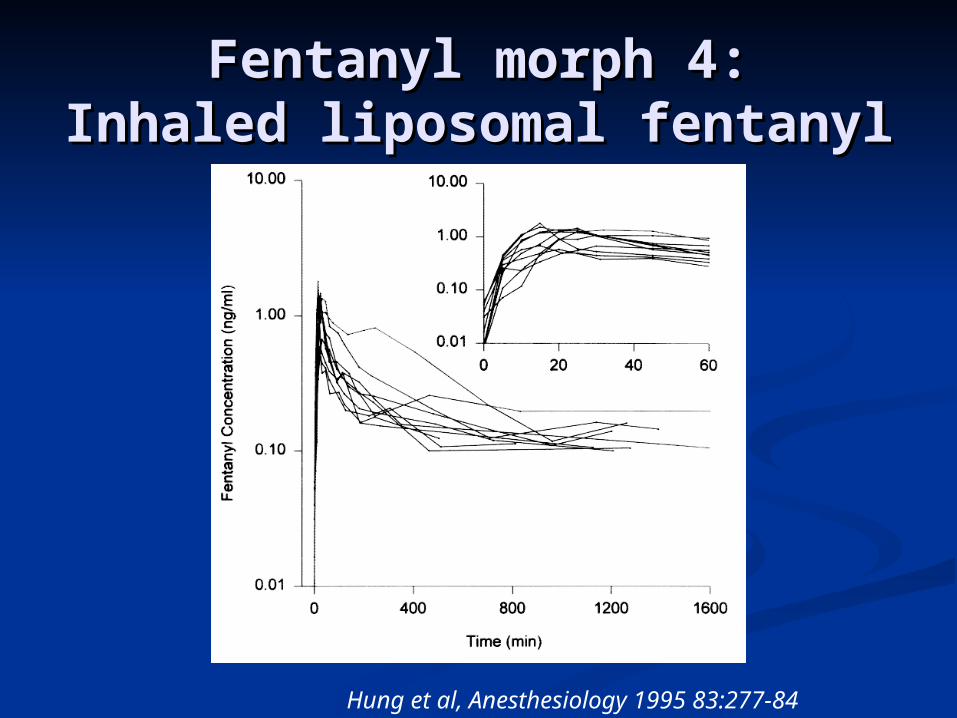
Fentanyl morph 4:Fentanyl morph 4:Inhaled liposomal fentanylInhaled liposomal fentanyl
Hung et al, Anesthesiology 1995 83:277-84
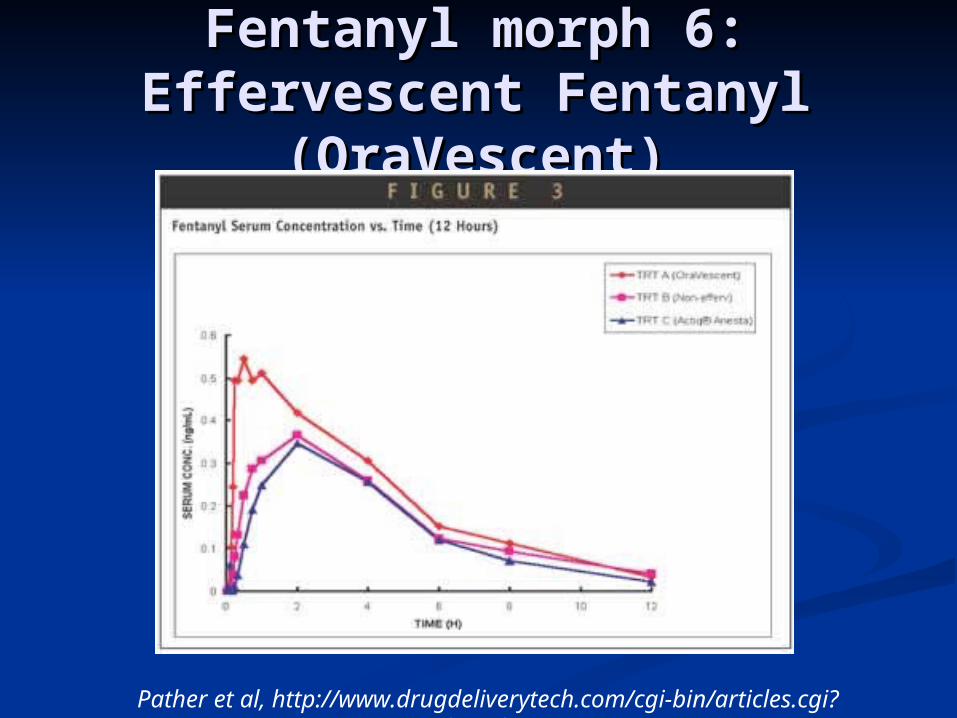
Fentanyl morph 6:Fentanyl morph 6:Effervescent Fentanyl Effervescent Fentanyl
(OraVescent)(OraVescent)
Pather et al, http://www.drugdeliverytech.com/cgi-bin/articles.cgi?
idArticle=5
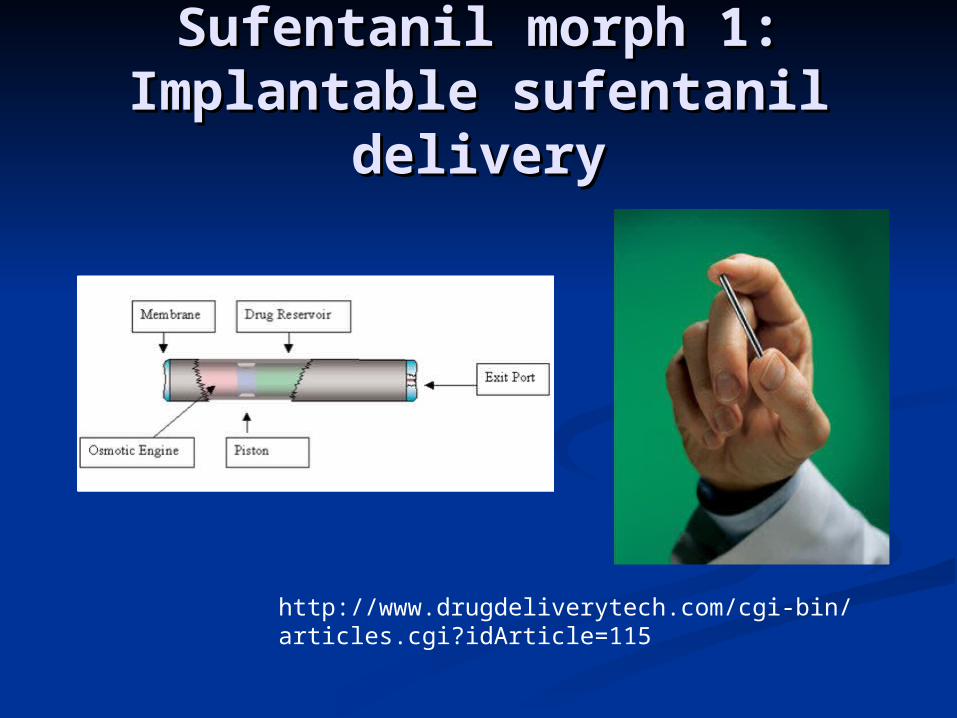
Sufentanil morph 1:Sufentanil morph 1:Implantable sufentanil Implantable sufentanil
deliverydelivery
http://www.drugdeliverytech.com/cgi-bin/articles.cgi?idArticle=115
Evidence of Evidence of opioid opioid subtypessubtypes
Only about 50% cross tolerance Only about 50% cross tolerance between morphine, methadone, fentanylbetween morphine, methadone, fentanyl
Explains why rotating opioids in chronic pain is Explains why rotating opioids in chronic pain is probably a good ideaprobably a good idea
CXBK mouse is insensitive to morphine, CXBK mouse is insensitive to morphine, but has normal response to M6G and but has normal response to M6G and fentanylfentanyl
Selective response to opioid antagonistsSelective response to opioid antagonists Morphine-6-glucuronide, the outlierMorphine-6-glucuronide, the outlier
Gavril Pasternak, Life Sciences 2001:68, 2213
NaloxonazineNaloxonazine
Selectively antagonizes morphine Selectively antagonizes morphine analgesia in animalsanalgesia in animals 11 is considered naloxonazine sensitive is considered naloxonazine sensitive
Does not antagonize morphine-Does not antagonize morphine-induced ventilatory depression or GI induced ventilatory depression or GI effectseffects 22 is considered naloxonazine is considered naloxonazine
insensitiveinsensitive
Gavril Pasternak, Life Sciences 2001:68, 2213
Morphine-6-glucuronideMorphine-6-glucuronide Active metabolite of morphine, about 100 fold Active metabolite of morphine, about 100 fold
more potent intrathecally, but enters the CNS more potent intrathecally, but enters the CNS VERY slowlyVERY slowly
Has analgesic activity in the CXBK mouse that Has analgesic activity in the CXBK mouse that is insensitive to morphineis insensitive to morphine
Actions blocked by naloxonazine (hence, Actions blocked by naloxonazine (hence, 11)) Has a unique antagonist, 3-O-methylnaxtrexoneHas a unique antagonist, 3-O-methylnaxtrexone
Also antagonizes heroin self administration, little affect on Also antagonizes heroin self administration, little affect on morphinemorphine
Subtype of Subtype of 11
MOR-1 knockout (exon 1) has normal sensitivity MOR-1 knockout (exon 1) has normal sensitivity to morphine-6-glucuronideto morphine-6-glucuronide
Gavril Pasternak, Life Sciences 2001:68, 2213
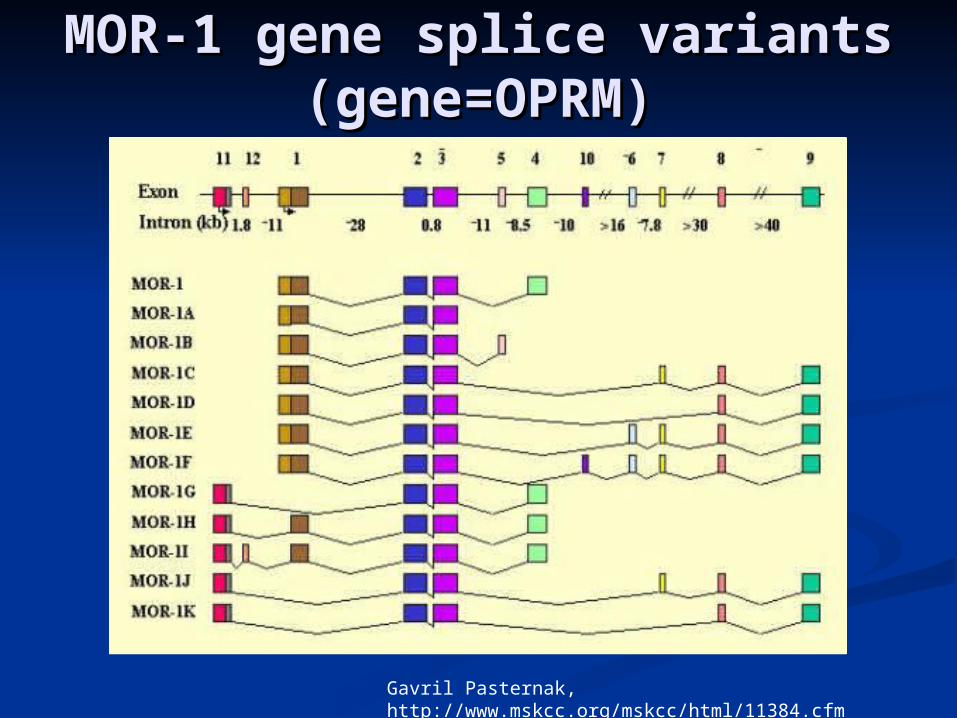
Gavril Pasternak, http://www.mskcc.org/mskcc/html/11384.cfm
MOR-1 gene splice variantsMOR-1 gene splice variants(gene=OPRM)(gene=OPRM)
Gavril Pasternak, http://www.mskcc.org/mskcc/html/11384.cfm
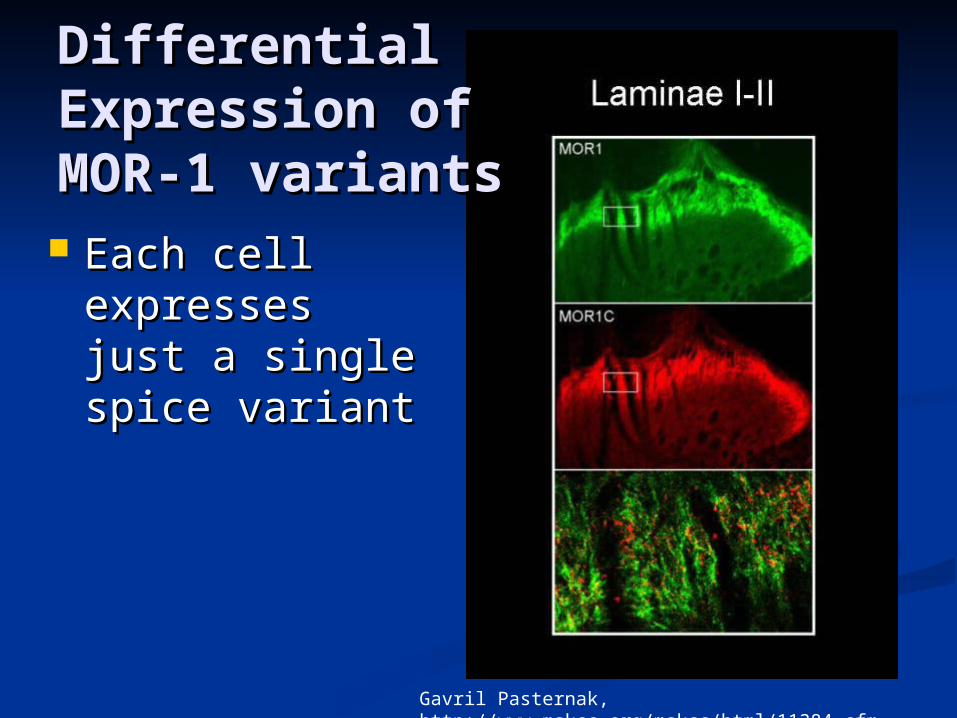
DifferentialDifferentialExpression ofExpression ofMOR-1 variantsMOR-1 variants
Each cell Each cell expresses just expresses just a single spice a single spice variantvariant
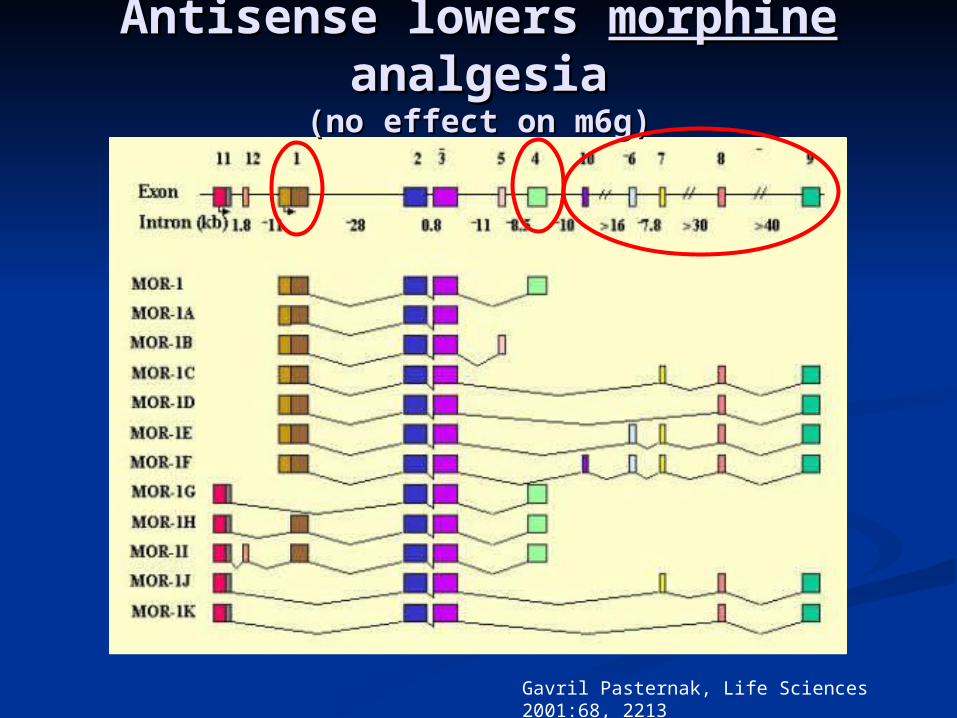
Antisense lowers Antisense lowers morphinemorphine analgesiaanalgesia
(no effect on m6g)(no effect on m6g)
Gavril Pasternak, Life Sciences 2001:68, 2213
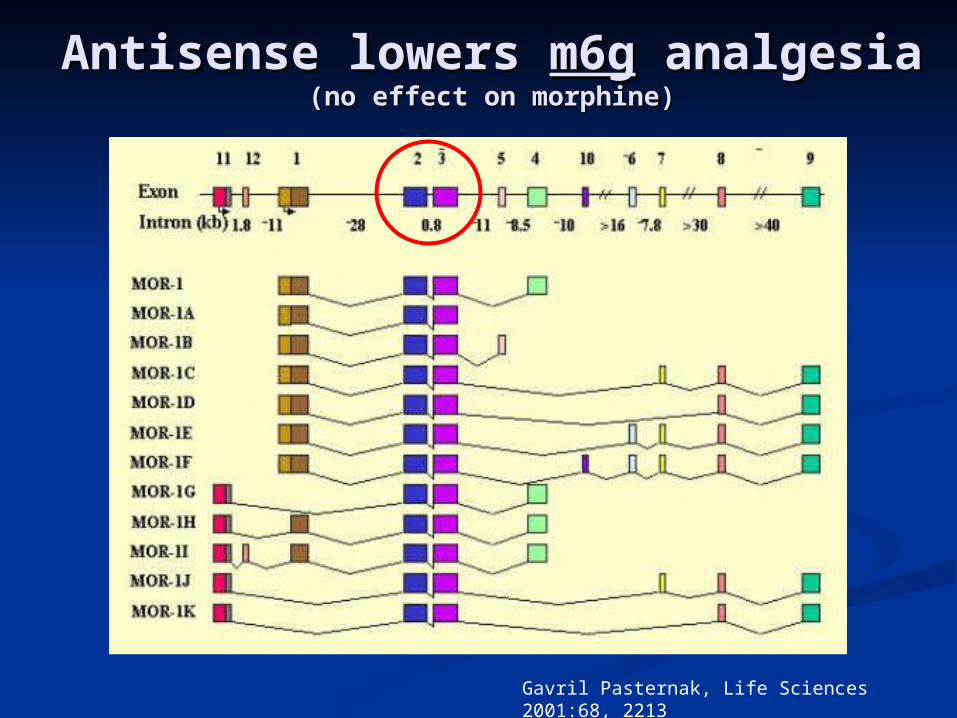
Gavril Pasternak, Life Sciences 2001:68, 2213
Antisense lowers Antisense lowers m6gm6g analgesia analgesia(no effect on morphine)(no effect on morphine)
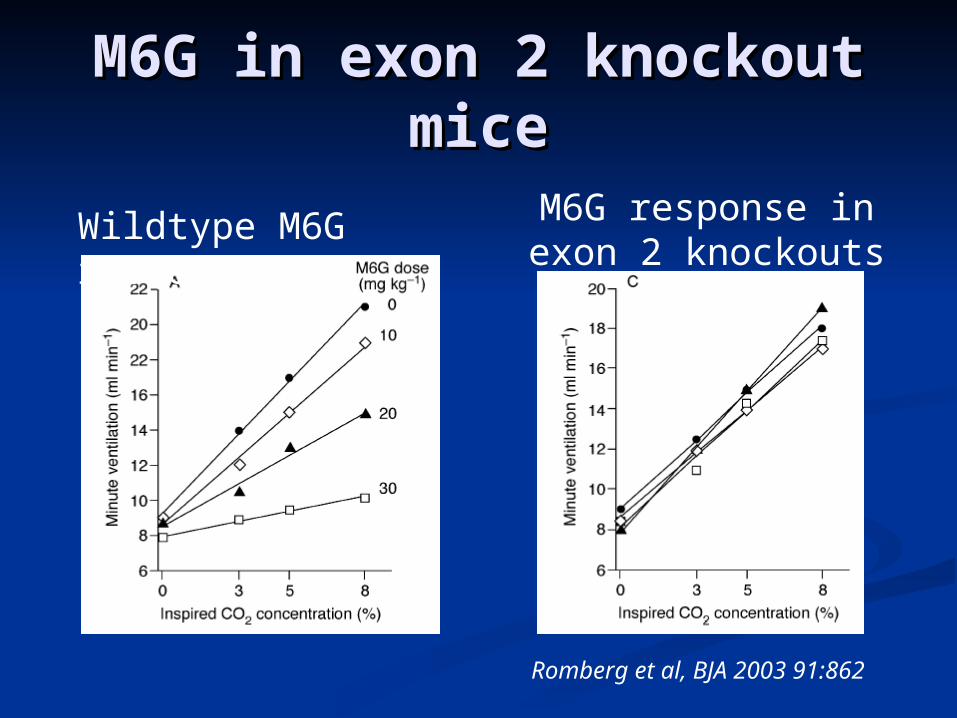
M6G in exon 2 knockout M6G in exon 2 knockout micemice
Wildtype M6G response
M6G response in exon 2 knockouts
Romberg et al, BJA 2003 91:862
Morphine-6-glucuronideMorphine-6-glucuronide Very slow transit across blood brain barrier.Very slow transit across blood brain barrier. Not a substrate for p-glycoprotein, but appears Not a substrate for p-glycoprotein, but appears
to be a substrate for probenecid inhibited to be a substrate for probenecid inhibited transporters (Anesthesiology 2004:101 1394)transporters (Anesthesiology 2004:101 1394)
Recently a peptide based carrier demonstrated Recently a peptide based carrier demonstrated 4 fold increase in uptake and potency (JPET 4 fold increase in uptake and potency (JPET 2005:12 epub).2005:12 epub).
Some data show higher affinity for Some data show higher affinity for 11, and lower , and lower affinity for affinity for 22, compared to morphine., compared to morphine.
Some suggestion that M6G is associated with Some suggestion that M6G is associated with less ventilatory depression for the amount of less ventilatory depression for the amount of analgesiaanalgesia (e.g., Romberg et al, Anesthesiology 2004 100:120) (e.g., Romberg et al, Anesthesiology 2004 100:120)
11 selective agonists? selective agonists?
Despite evidence now 25 years old of Despite evidence now 25 years old of differential response to angatonists, differential response to angatonists, nobody has found a nobody has found a 11 selective agonist selective agonist
Biggest argument against it: Paul Biggest argument against it: Paul Janssen spent years looking for one, Janssen spent years looking for one, screening over 70,000 possible ligandsscreening over 70,000 possible ligands
Reason for hope: perhaps our improved Reason for hope: perhaps our improved knowledge of MOR-1 splice variants will knowledge of MOR-1 splice variants will help identify the required pharmacoforehelp identify the required pharmacofore
Don’t hold your breath…Don’t hold your breath…
Next best thing:Next best thing:give opioids, manage side give opioids, manage side
effectseffects
Treat constipation, ileus with Treat constipation, ileus with peripheral antagonistsperipheral antagonists
Treat ventilatory depression with Treat ventilatory depression with 5HT5HT44 agonists agonists
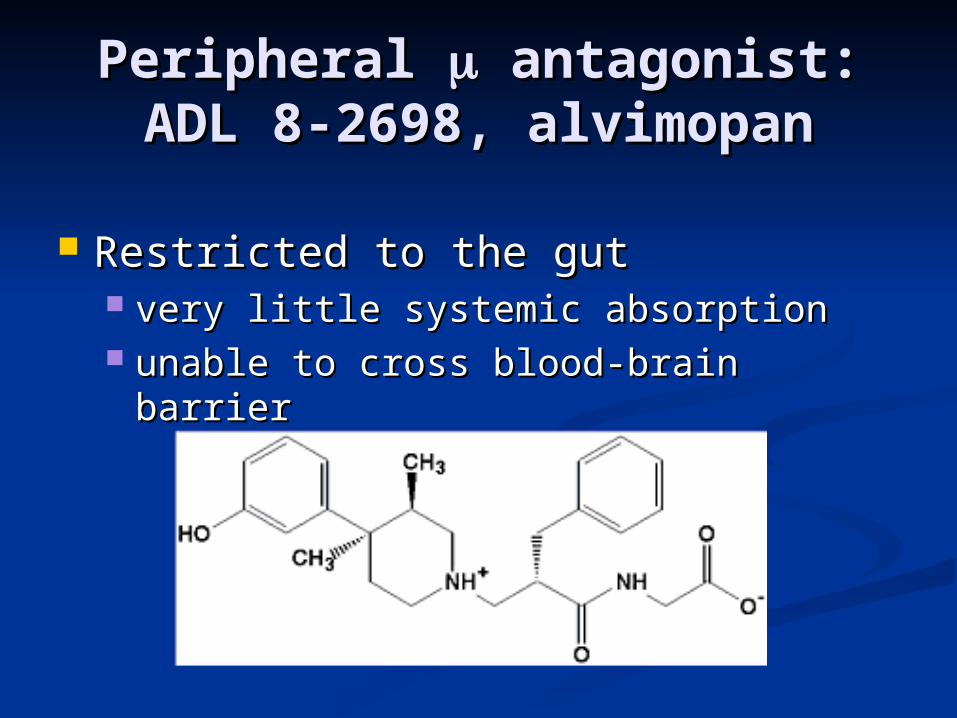
Peripheral Peripheral antagonist: antagonist:ADL 8-2698, alvimopanADL 8-2698, alvimopan
Restricted to the gutRestricted to the gut very little systemic absorptionvery little systemic absorption unable to cross blood-brain barrierunable to cross blood-brain barrier
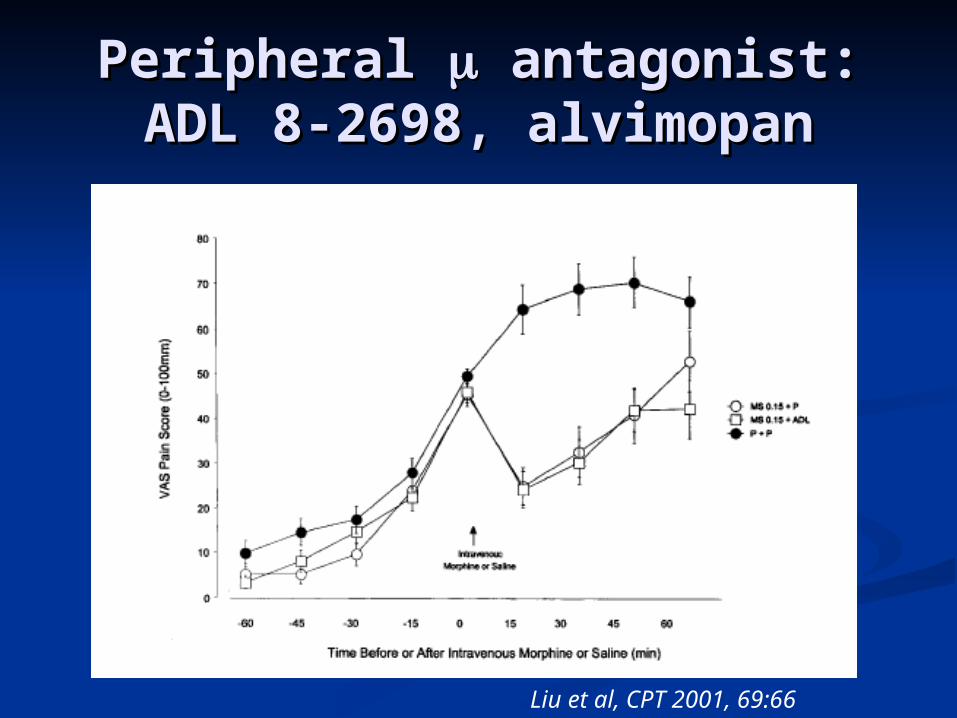
Peripheral Peripheral antagonist: antagonist:ADL 8-2698, alvimopanADL 8-2698, alvimopan
Liu et al, CPT 2001, 69:66
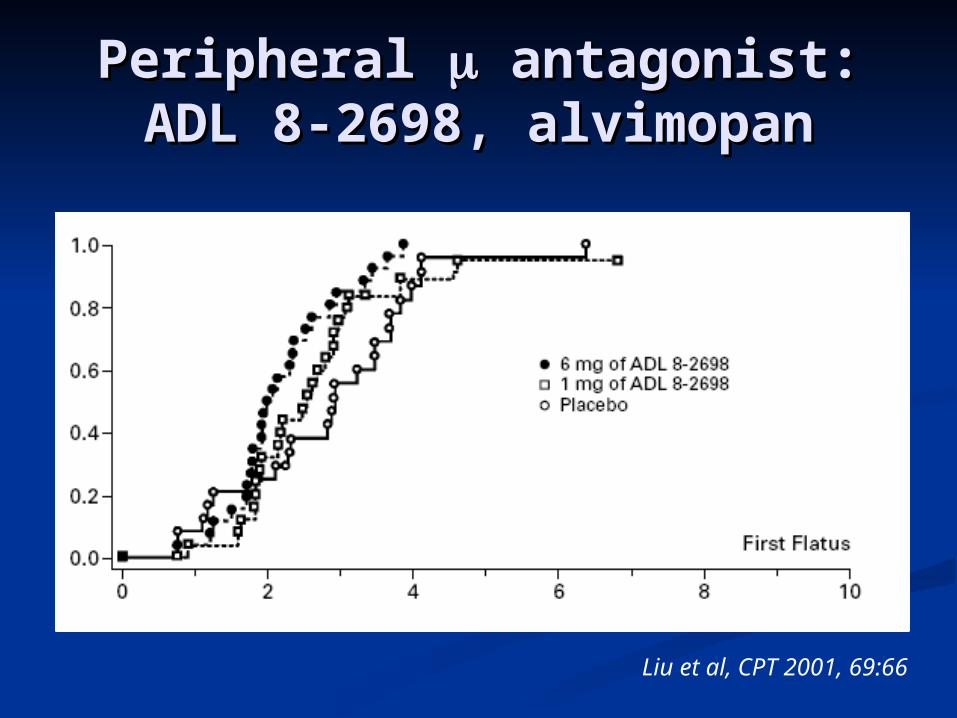
Liu et al, CPT 2001, 69:66
Peripheral Peripheral antagonist: antagonist:ADL 8-2698, alvimopanADL 8-2698, alvimopan
MethylnaltrexoneMethylnaltrexone Invented by Leon Goldberg, Invented by Leon Goldberg,
University of ChicagoUniversity of Chicago Effective for a variety of opioid Effective for a variety of opioid
side effects includingside effects including Opioid induced constipationOpioid induced constipation PruritisPruritis Post-operative ileusPost-operative ileus
Being developed for IV/SQ/OralBeing developed for IV/SQ/Oral ProgenicsProgenics
Phase III trialsPhase III trials
5HT5HT44 agonists agonists
Cisapride, prucalopride, renzapride, Cisapride, prucalopride, renzapride, tegaserod, SB207710, TC-2749tegaserod, SB207710, TC-2749
Primary development target is as a Primary development target is as a prokinetic agentprokinetic agent
Interesting that 5HTInteresting that 5HT44 agonists agonists reverse two opioid side effects: ileus reverse two opioid side effects: ileus and hypoventilation…and hypoventilation…
TD-2759 (Theravance) is a once daily TD-2759 (Theravance) is a once daily drug in developmentdrug in development
Theravance 2005 investor presentationTheravance 2005 investor presentation
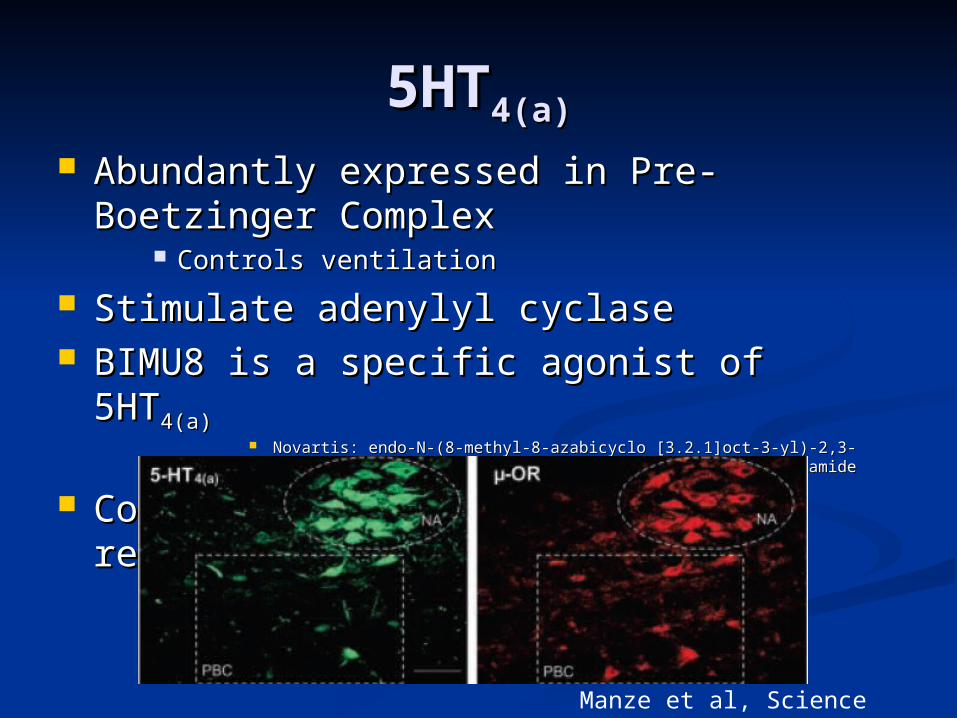
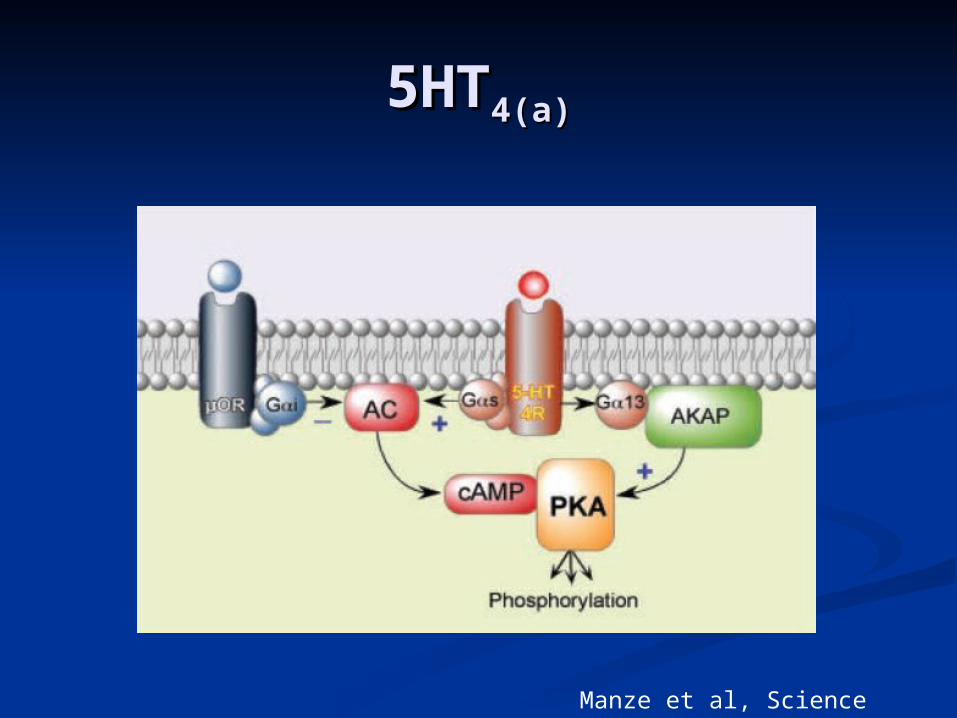
5HT5HT4(a)4(a)
Abundantly expressed in Pre-Boetzinger Abundantly expressed in Pre-Boetzinger ComplexComplex
Controls ventilationControls ventilation
Stimulate adenylyl cyclaseStimulate adenylyl cyclase BIMU8 is a specific agonist of 5HTBIMU8 is a specific agonist of 5HT4(a)4(a)
Novartis: endo-N-(8-methyl-8-azabicyclo [3.2.1]oct-3-yl)-2,3-dihydro-(1-Novartis: endo-N-(8-methyl-8-azabicyclo [3.2.1]oct-3-yl)-2,3-dihydro-(1-methyl) ethyl-2-oxo-1H-benzimidazole-1-carboxamidemethyl) ethyl-2-oxo-1H-benzimidazole-1-carboxamide
Co-locate in PBC with opioid receptorsCo-locate in PBC with opioid receptors
Manze et al, Science 2003 301:226
5HT5HT4(a)4(a)
Manze et al, Science 2003 301:226
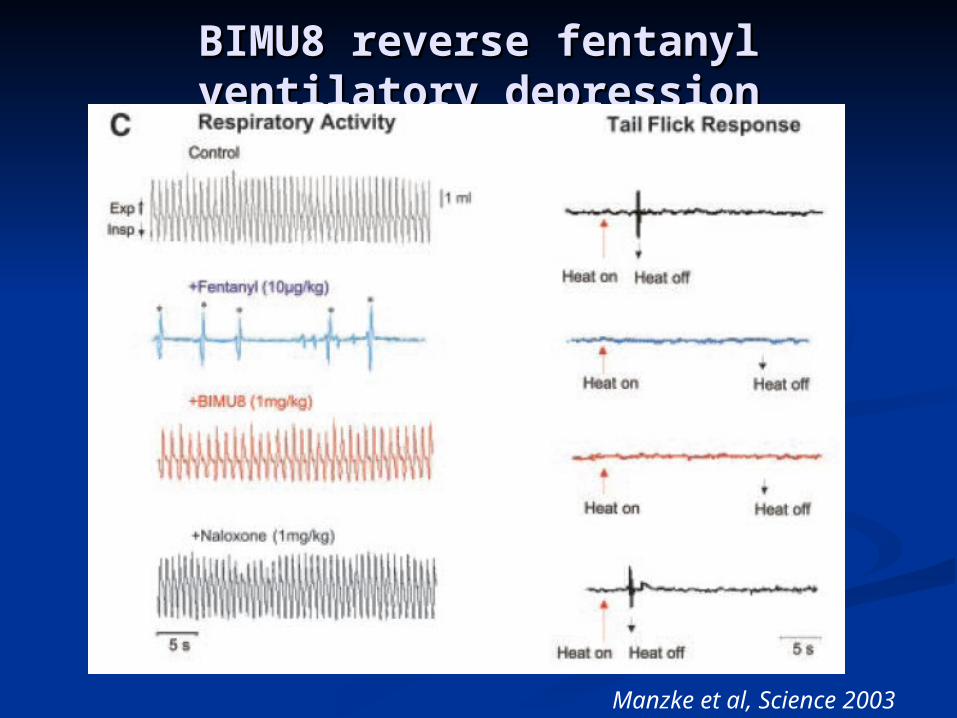
BIMU8 reverse fentanyl ventilatory BIMU8 reverse fentanyl ventilatory depressiondepression
Manzke et al, Science 2003 301:226
UnfortunatelyUnfortunately
Based on the Manzke work, the 5HTBased on the Manzke work, the 5HT44 nonspecific agonists have been tried nonspecific agonists have been tried for efficacy in reversing opioid for efficacy in reversing opioid induced ventilatory depression. induced ventilatory depression.
They don’t work.They don’t work. Need to await development of 5HTNeed to await development of 5HT4(a)4(a)
specific agonists.specific agonists.
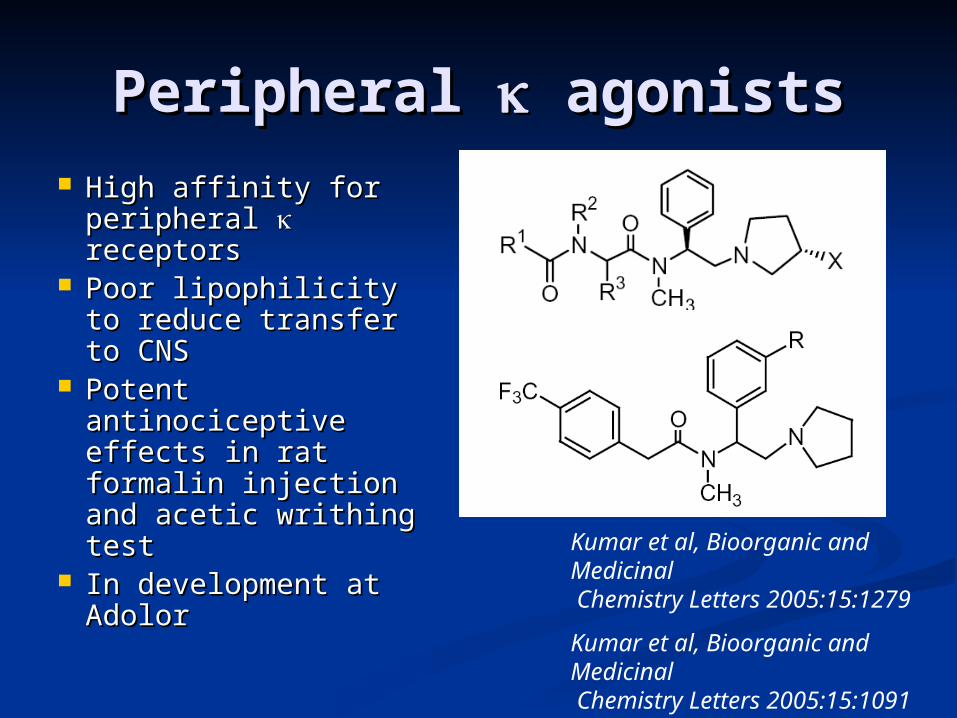
Peripheral Peripheral agonists agonists High affinity for High affinity for
peripheral peripheral receptorsreceptors
Poor lipophilicity to Poor lipophilicity to reduce transfer to reduce transfer to CNSCNS
Potent Potent antinociceptive antinociceptive effects in rat formalin effects in rat formalin injection and acetic injection and acetic writhing testwrithing test
In development at In development at AdolorAdolor
Kumar et al, Bioorganic and Medicinal Chemistry Letters 2005:15:1279
Kumar et al, Bioorganic and Medicinal Chemistry Letters 2005:15:1091
Adolor Corporation
Other centrally Other centrally actingacting
analgesic drugsanalgesic drugs
CannabinoidsCannabinoids Dronabinol has modest efficacy as an Dronabinol has modest efficacy as an
analgesic in multiple sclerosis (Svendsen et analgesic in multiple sclerosis (Svendsen et al, BMJ 2004:31:329)al, BMJ 2004:31:329)
THC has minimal analgesic activityTHC has minimal analgesic activity Ajulemic acid, novel Ajulemic acid, novel
cannabinoid with no cannabinoid with no psychotropic effectspsychotropic effects
Shown effective in Shown effective in human trial of chronic neuropathic painhuman trial of chronic neuropathic pain
Karst et al, JAMA 2003 290:1757Karst et al, JAMA 2003 290:1757
Mechanism of action appears to be anti-Mechanism of action appears to be anti-inflammationinflammation
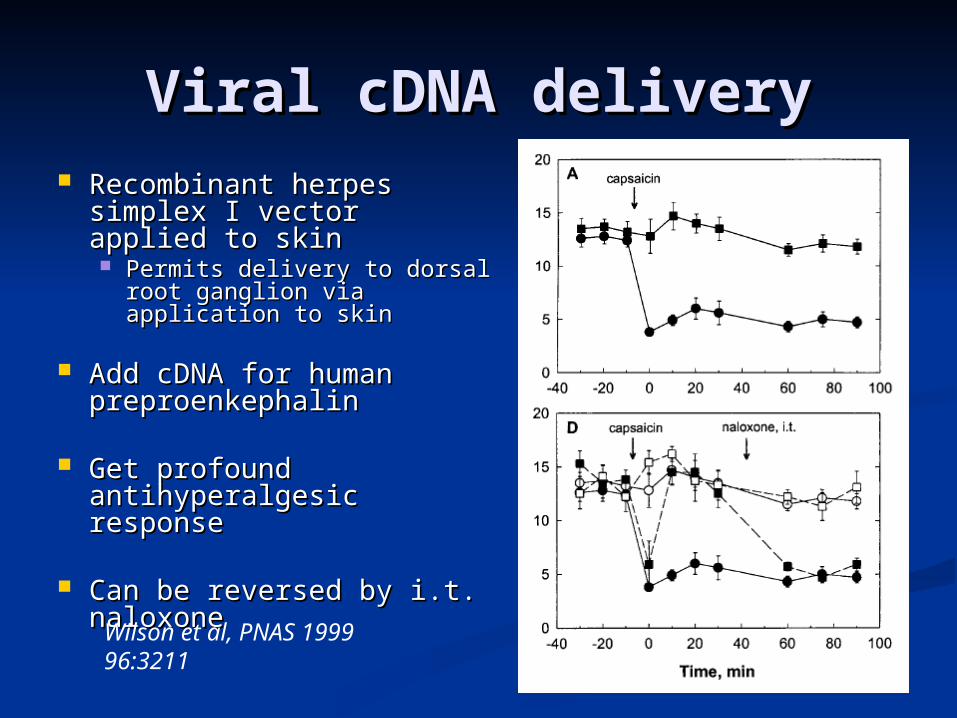
Viral cDNA deliveryViral cDNA delivery Recombinant herpes Recombinant herpes
simplex I vector applied simplex I vector applied to skinto skin Permits delivery to dorsal Permits delivery to dorsal
root ganglion via root ganglion via application to skinapplication to skin
Add cDNA for human Add cDNA for human preproenkephalinpreproenkephalin
Get profound Get profound antihyperalgesic responseantihyperalgesic response
Can be reversed by i.t. Can be reversed by i.t. naloxonenaloxoneWilson et al, PNAS 1999 96:3211
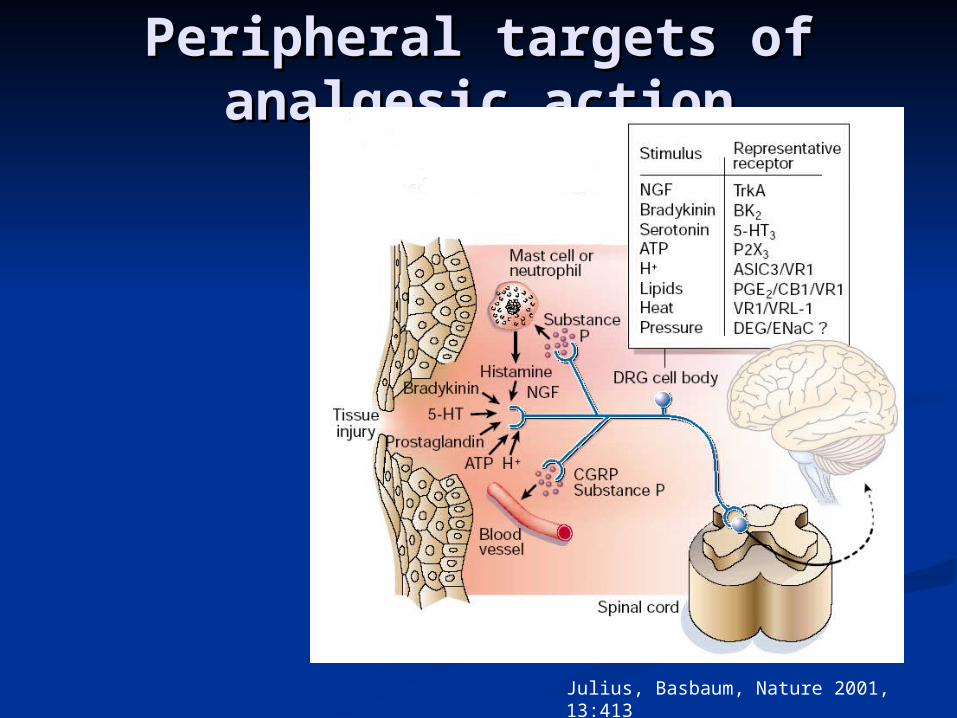
Peripheral targets of Peripheral targets of analgesic actionanalgesic action
Julius, Basbaum, Nature 2001, 13:413
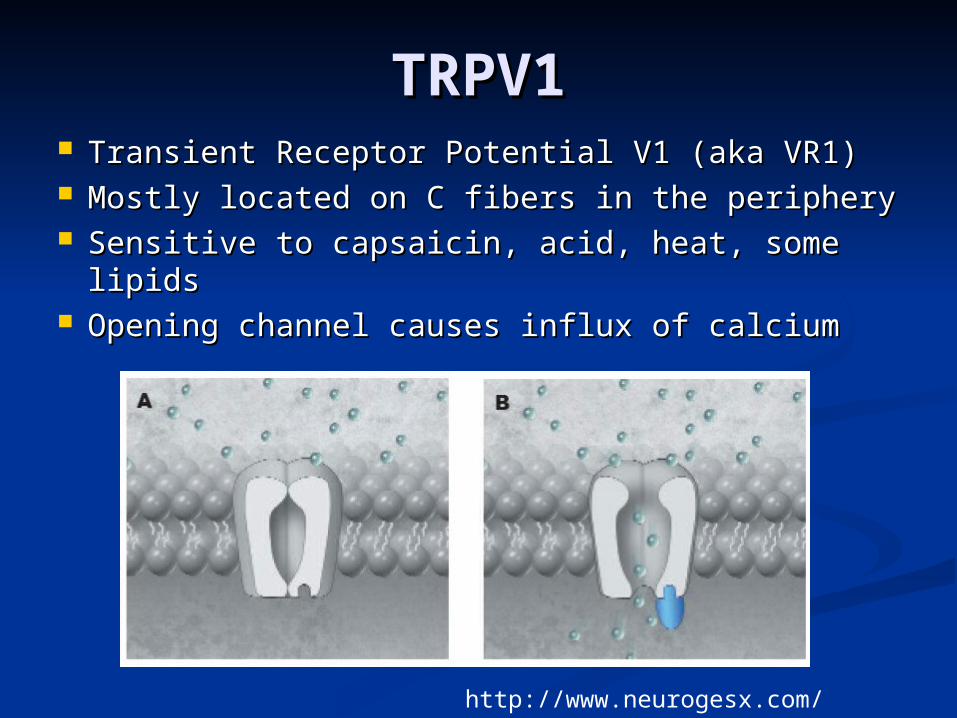
TRPV1TRPV1 Transient Receptor Potential V1 (aka VR1)Transient Receptor Potential V1 (aka VR1) Mostly located on C fibers in the peripheryMostly located on C fibers in the periphery Sensitive to capsaicin, acid, heat, some lipidsSensitive to capsaicin, acid, heat, some lipids Opening channel causes influx of calciumOpening channel causes influx of calcium
http://www.neurogesx.com/NcPnTRPV1.html
TRPV1 agonists TRPV1 agonists (capsaicin)(capsaicin)
How capsaicin works:How capsaicin works:TRPV1 kept open TRPV1 kept open Ca++ entry Ca++ entry Prolonged cell dysfunction Prolonged cell dysfunction Prolonged analgesiaProlonged analgesia
Malmberg et al, Pain 2004 111:360
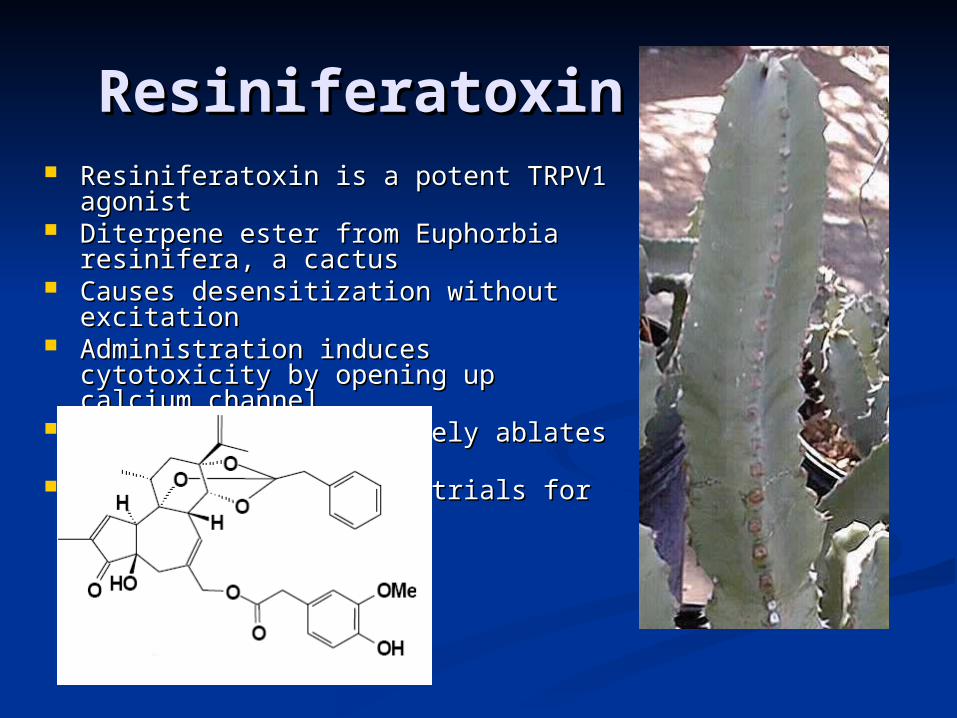
ResiniferatoxinResiniferatoxin Resiniferatoxin is a potent TRPV1 Resiniferatoxin is a potent TRPV1
agonistagonist Diterpene ester from Euphorbia Diterpene ester from Euphorbia
resinifera, a cactusresinifera, a cactus Causes desensitization without Causes desensitization without
excitationexcitation Administration induces cytotoxicity by Administration induces cytotoxicity by
opening up calcium channel.opening up calcium channel. In high doses selectively ablates In high doses selectively ablates
TRPV1 nervesTRPV1 nerves Currently in clinical trials for Currently in clinical trials for
overactive bladder overactive bladder
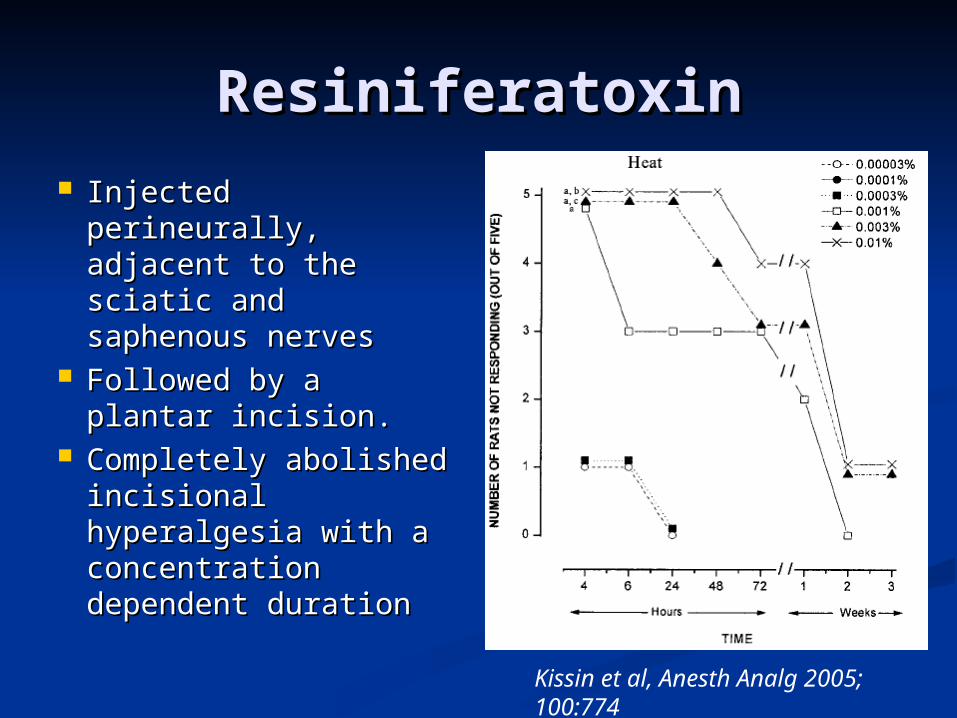
ResiniferatoxinResiniferatoxin Injected perineurally, Injected perineurally,
adjacent to the adjacent to the sciatic and sciatic and saphenous nervessaphenous nerves
Followed by a plantar Followed by a plantar incision.incision.
Completely abolished Completely abolished incisional incisional hyperalgesia with a hyperalgesia with a concentration concentration dependent durationdependent duration
Kissin et al, Anesth Analg 2005; 100:774
TRPV1 neuroablationTRPV1 neuroablation Resiniferatoxin is a potent TRPV1 agonistResiniferatoxin is a potent TRPV1 agonist Administration induces cytotoxicity by Administration induces cytotoxicity by
opening up calcium channel.opening up calcium channel. Selectively ablates TRPV1 nervesSelectively ablates TRPV1 nerves In rats and dogs, inflammatory In rats and dogs, inflammatory
hyperalgesia is blockedhyperalgesia is blocked Touch, proprioception, mechanosensitive, Touch, proprioception, mechanosensitive,
and locomotor function remain intactand locomotor function remain intact Probably requires general anesthesia!Probably requires general anesthesia!
Karai et al, J Clin Invest 2004 113:1344
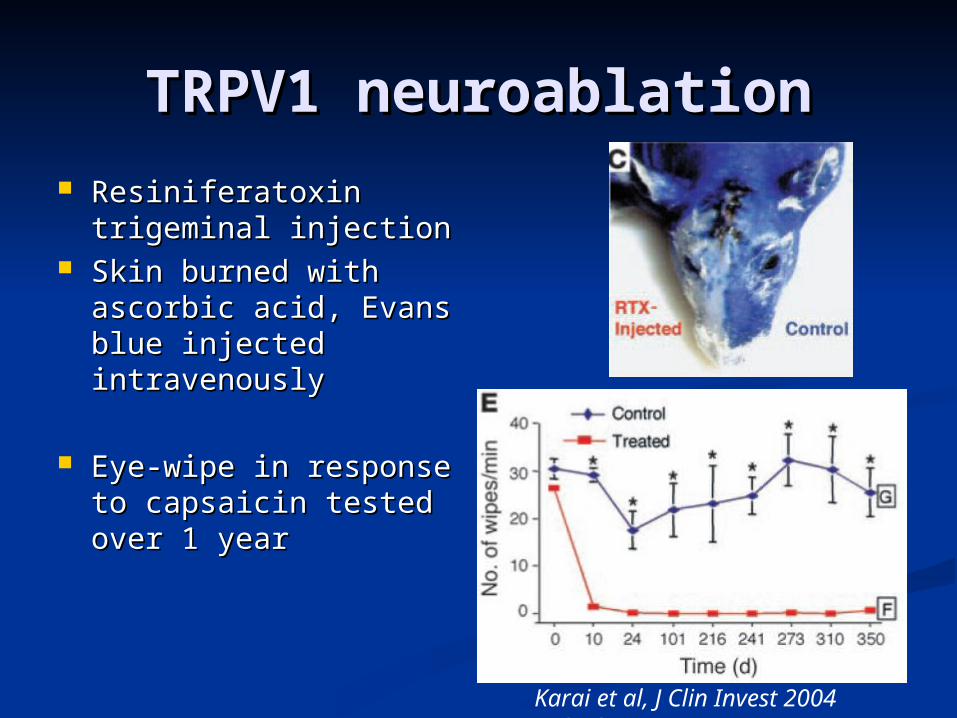
TRPV1 neuroablationTRPV1 neuroablation Resiniferatoxin Resiniferatoxin
trigeminal injectiontrigeminal injection Skin burned with Skin burned with
ascorbic acid, Evans ascorbic acid, Evans blue injected blue injected intravenouslyintravenously
Eye-wipe in response Eye-wipe in response to capsaicin tested to capsaicin tested over 1 yearover 1 year
Karai et al, J Clin Invest 2004 113:1344
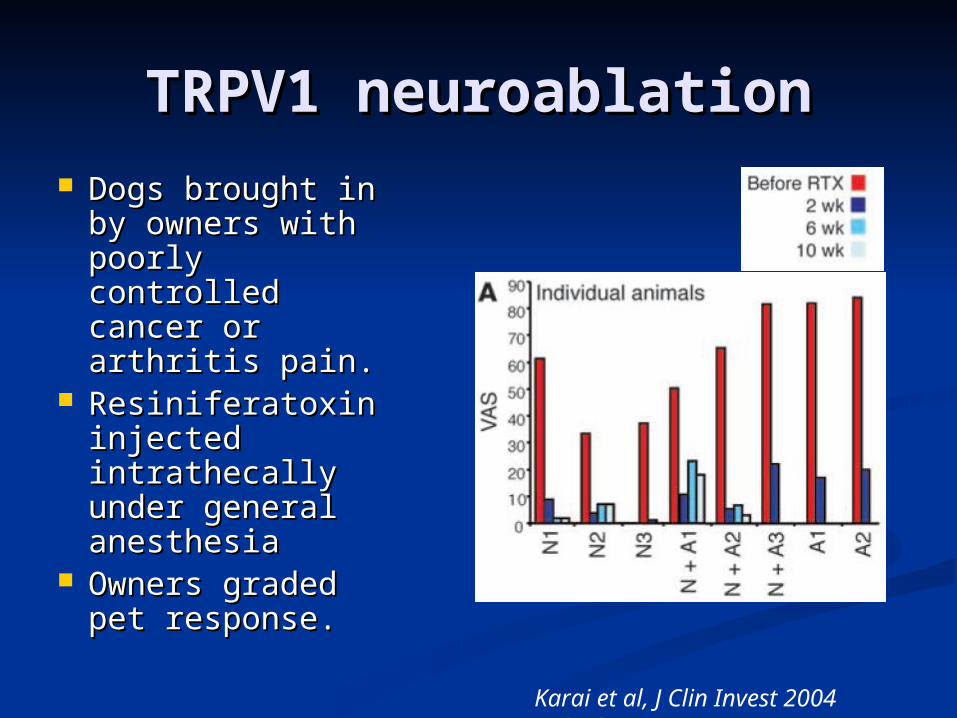
TRPV1 neuroablationTRPV1 neuroablation Dogs brought in Dogs brought in
by owners with by owners with poorly controlled poorly controlled cancer or arthritis cancer or arthritis pain.pain.
Resiniferatoxin Resiniferatoxin injected injected intrathecally intrathecally under general under general anesthesiaanesthesia
Owners graded Owners graded pet response.pet response.
Karai et al, J Clin Invest 2004 113:1344
TRPV1 agonist/antagonist TRPV1 agonist/antagonist pipelinepipeline
OlvanilOlvanil is an agonist, developed as is an agonist, developed as an oral analgesican oral analgesic
Phenylacetylrinvanil is an agonist Phenylacetylrinvanil is an agonist with picomolar potencywith picomolar potency
Addition of iodine to the phenyl ring Addition of iodine to the phenyl ring creates TRPV1 antagonistscreates TRPV1 antagonists
Appendino et al, J PET 2005 312:561
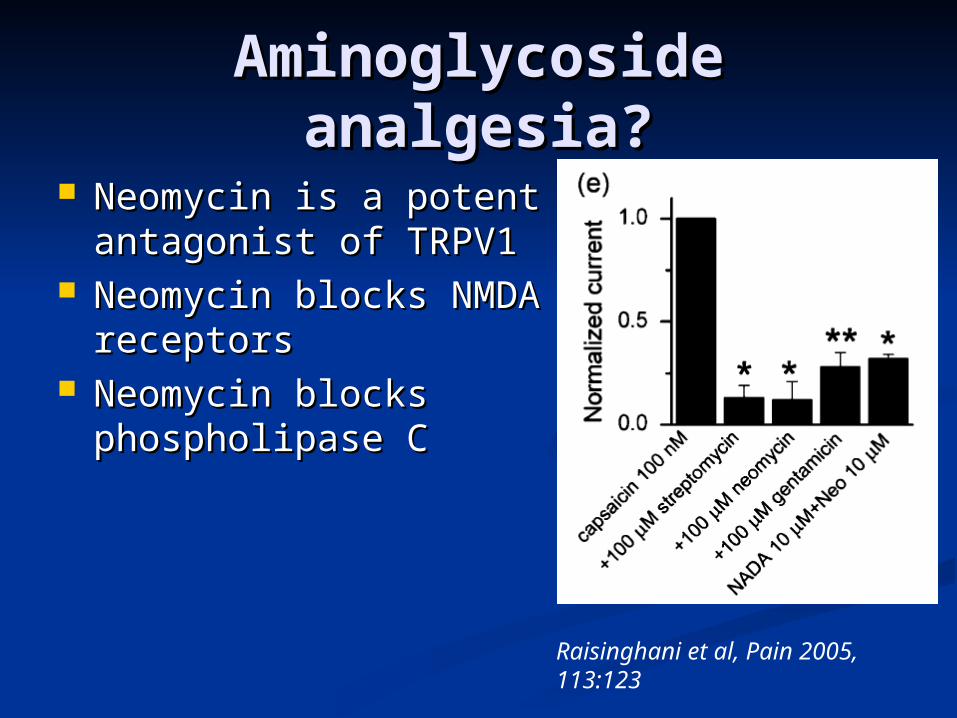
Aminoglycoside Aminoglycoside analgesia?analgesia?
Neomycin is a potent Neomycin is a potent antagonist of TRPV1antagonist of TRPV1
Neomycin blocks Neomycin blocks NMDA receptorsNMDA receptors
Neomycin blocks Neomycin blocks phospholipase Cphospholipase C
Raisinghani et al, Pain 2005, 113:123
ConotoxinsConotoxins Derived from Derived from ConusConus, a predatory snail, a predatory snail Highly potent peptides, about 2000 known Highly potent peptides, about 2000 known
so farso far -conotoxin – nicotinic antagonists-conotoxin – nicotinic antagonists
Some are neuromuscular blockersSome are neuromuscular blockers Some are central nicotinic antigonists with Some are central nicotinic antigonists with
activity in neuropathic pain in animal modelsactivity in neuropathic pain in animal models -conotoxin – calcium channel antagonists-conotoxin – calcium channel antagonists
Ziconitide (Prialt) approved for IT use in Ziconitide (Prialt) approved for IT use in chronic or neuropathic painchronic or neuropathic pain
Several others in developmentSeveral others in development Contulakin-G – Neurotensin agonistContulakin-G – Neurotensin agonist
Phase II trials, IT delivery for acute painPhase II trials, IT delivery for acute pain
ConclusionConclusion Very promising future for new Very promising future for new
hypnotics, muscle relaxants, and hypnotics, muscle relaxants, and analgesics.analgesics.
ALL OF THESE WILL CHANGE YOUR ALL OF THESE WILL CHANGE YOUR PRACTICEPRACTICE Sugammadex will revolutionize the use of Sugammadex will revolutionize the use of
muscle relaxantsmuscle relaxants The new hypnotics will be an important The new hypnotics will be an important
incremental changeincremental change Advances in analgesics will contribute to Advances in analgesics will contribute to
significant reductions in patient significant reductions in patient morbidity and mortality after surgerymorbidity and mortality after surgery
Related Documents











