449 The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder* STEPHEN J. O’BRIEN,†‡ MD, MANUEL C. NEVES,† MD, STEVEN P. ARNOCZKY,§ DVM, S. ROBERT ROZBRUCK,† EDWARD F. DICARLO, † MD, RUSSELL F. WARREN,† MD, ROBERT SCHWARTZ,† MD, AND THOMAS L. WICKIEWICZ, † MD From the † Department of Sports Medicine and the § Laboratory for Comparative Orthopaedic Research, The Hospital for Special Surgery, New York, New York ABSTRACT The gross and histologic anatomy of the inferior glenohumeral ligament was studied in 11 fresh frozen cadaver shoulders. Arthroscopic observations of the joint capsule through the normal range of motion re- vealed that the inferior glenohumeral ligament is actually a complex of structures consisting of an anterior band, a posterior band, and an interposed axillary pouch. While these components of the inferior glenohumeral ligament complex were present in all 11 specimens, they were best demonstrated in some shoulders by placing the humeral head in internal or external rotation in varying degrees of abduction. Histologic examination of the joint capsule revealed that the anterior and posterior bands of the inferior glenohumeral ligament complex were readily identifiable as distinct structures comprised of thickened bands of well-organized colla- gen bundles. Although slight variations were noted in the attach- ment sites of the anterior and posterior bands to the glenoid, the inferior glenohumeral ligament complex was observed to attach to the humeral neck in one of two distinct configurations. A collar-like attachment, in which the entire inferior glenohumeral ligament complex attaches just inferior to the articular edge of the humeral head, was observed in six specimens. In the remaining five specimens, the attachment was in the shape of a "V," with the anterior and posterior bands attaching adjacent to the articular edge of the humeral head and the axillary pouch attaching at the apex of the "V" distal to the articular edge. The orientation and design of the inferior glenohu- meral ligament complex supports the functional con- cept of this single structure as an important anterior and posterior stabilizer of the shoulder joint. The treatment of shoulder instability has long been a topic of debate among orthopaedic surgeons. A variety of operative techniques have been advocated for this problem.4-7, 9, 10, 13, 16 However, although the results of surgical treatment of an- terior shoulder dislocations have been satisfactory,4-6,16 a 50% recurrence rate has been reported for posterior dislo- cations following repair.’ This poor success rate may stem from an incomplete understanding of the anatomy of the glenohumeral joint and its static stabilizers. The glenohumeral ligaments (superior, middle, and infe- rior) were first described as mere thickenings in the joint capsule of the shoulder.2,11 However, clinical and experimen- tal studies have demonstrated the functional importance of these structures in maintaining joint stability.8, 12,14, 15, 17 While the superior and middle glenohumeral ligaments play a limited role in joint stability, the inferior glenohumeral ligament has been shown to be the primary check against anterior dislocation of the humeral head when the shoulder was abducted 90°.ls This observation has stressed the im- portance of replacing or reestablishing the functional integ- rity of this structure when treating anterior dislocations. A recent study, however, has shown that the inferior gleno- humeral ligament is the primary check against both anterior and posterior dislocation of the humeral head in the ab- *Presented at the intenm meeting of the AOSSM, Las Vegas, Nevada, February 1989, and the meeting of the Amencan Shoulder and Elbow Surgeons, Las Vegas, Nevada, 1989, at which it won the Charles S Neer award for excellence in basic science research. ~ Address correspondence and reprnt requests to Stephen J. O’Bnen, MD, The Hospital for Special Surgery, 535 East 70th Street, New York, NY 10021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
449
The anatomy and histology of the inferiorglenohumeral ligament complex of theshoulder*
STEPHEN J. O’BRIEN,†‡ MD, MANUEL C. NEVES,† MD,STEVEN P. ARNOCZKY,§ DVM, S. ROBERT ROZBRUCK,†EDWARD F. DICARLO, † MD, RUSSELL F. WARREN,† MD,
ROBERT SCHWARTZ,† MD, AND THOMAS L. WICKIEWICZ, † MD
From the † Department of Sports Medicine and the § Laboratory for Comparative OrthopaedicResearch, The Hospital for Special Surgery, New York, New York
ABSTRACT
The gross and histologic anatomy of the inferior
glenohumeral ligament was studied in 11 fresh frozencadaver shoulders. Arthroscopic observations of thejoint capsule through the normal range of motion re-vealed that the inferior glenohumeral ligament is actuallya complex of structures consisting of an anterior band,a posterior band, and an interposed axillary pouch.While these components of the inferior glenohumeralligament complex were present in all 11 specimens,they were best demonstrated in some shoulders byplacing the humeral head in internal or external rotationin varying degrees of abduction. Histologic examinationof the joint capsule revealed that the anterior and
posterior bands of the inferior glenohumeral ligamentcomplex were readily identifiable as distinct structurescomprised of thickened bands of well-organized colla-gen bundles.Although slight variations were noted in the attach-
ment sites of the anterior and posterior bands to theglenoid, the inferior glenohumeral ligament complexwas observed to attach to the humeral neck in one oftwo distinct configurations. A collar-like attachment, inwhich the entire inferior glenohumeral ligament complexattaches just inferior to the articular edge of the humeralhead, was observed in six specimens. In the remainingfive specimens, the attachment was in the shape of a
"V," with the anterior and posterior bands attachingadjacent to the articular edge of the humeral head andthe axillary pouch attaching at the apex of the "V" distalto the articular edge.The orientation and design of the inferior glenohu-
meral ligament complex supports the functional con-cept of this single structure as an important anteriorand posterior stabilizer of the shoulder joint.
The treatment of shoulder instability has long been a topicof debate among orthopaedic surgeons. A variety of operativetechniques have been advocated for this problem.4-7, 9, 10, 13, 16However, although the results of surgical treatment of an-terior shoulder dislocations have been satisfactory,4-6,16 a50% recurrence rate has been reported for posterior dislo-cations following repair.’ This poor success rate may stemfrom an incomplete understanding of the anatomy of theglenohumeral joint and its static stabilizers.The glenohumeral ligaments (superior, middle, and infe-
rior) were first described as mere thickenings in the jointcapsule of the shoulder.2,11 However, clinical and experimen-tal studies have demonstrated the functional importance ofthese structures in maintaining joint stability.8, 12,14, 15, 17While the superior and middle glenohumeral ligaments playa limited role in joint stability, the inferior glenohumeralligament has been shown to be the primary check againstanterior dislocation of the humeral head when the shoulderwas abducted 90°.ls This observation has stressed the im-portance of replacing or reestablishing the functional integ-rity of this structure when treating anterior dislocations. Arecent study, however, has shown that the inferior gleno-humeral ligament is the primary check against both anteriorand posterior dislocation of the humeral head in the ab-
*Presented at the intenm meeting of the AOSSM, Las Vegas, Nevada,February 1989, and the meeting of the Amencan Shoulder and Elbow Surgeons,Las Vegas, Nevada, 1989, at which it won the Charles S Neer award forexcellence in basic science research.
~ Address correspondence and reprnt requests to Stephen J. O’Bnen, MD,The Hospital for Special Surgery, 535 East 70th Street, New York, NY 10021

450
ducted shoulder.&dquo; The same study also suggested that theanatomy of the inferior glenohumeral ligament is more
complex than originally described and that this anatomy isdirectly related to the function of the inferior glenohumeralligament as a stabilizing structure.Our purpose, therefore, was to investigate the gross and
histologic anatomy of the inferior glenohumeral ligament inan effort to describe this structure in detail.
MATERIALS AND METHODS
Eleven fresh frozen cadaver shoulders (seven right, four left)were used for this study. Information regarding the sex andage of the specimens was unavailable. The shoulders weregrossly normal except for the presence of a rotator cuff tearin one specimen. All tissues except the joint capsule werecarefully dissected away and the shoulders mounted to atable stand by rigidly clamping the scapula. Arthroscopicexamination of the glenohumeral joint was then performedon each specimen.A 30° arthroscope was placed through the superior aspect
of the capsule in the area between the acromion and coracoidprocess and the joint was examined without any distensionwith liquid or air. This was done to preserve the inherentrelationship of the capsular structures. The shoulder wasexamined through the range of motion and the glenohumeralligaments were identified. The anterior and posterior bandsof the inferior glenohumeral ligament were identified withthe joint in internal or external rotation in varying degreesof abduction. These bands were then labeled with India inkfor later identification.
After arthroscopic examination, the joint capsule wasopened by an incision parallel to the biceps tendon. Thecapsule was examined and assigned to one of six anatomicalcategories described by De Palma et aLl that are based onthe topographic arrangement of the synovial recesses inrelation to the glenohumeral ligaments. In addition, thelocation and shape of the attachments of the inferior gle-nohumeral ligament complex (IGHLC) to the glenoid andhumerus were recorded for each specimen.The entire joint capsule was then completely detached
from the glenoid and humerus and mounted as a single, flatspecimen on a cork board. The specimen was fixed in 10%buffered formalin for 3 days, after which sections of thejoint capsule were cut in either the sagittal or coronal planesthrough the IGHLC and adjacent capsule (Fig. 1). Thespecimens were then embedded in paraffin and 5 ~m thicksections were cut and mounted on glass slides. The sectionswere stained with hematoxylin and eosin and examinedusing light and polarized light microscopy.
RESULTS
Gross anatomy
Based on the classification system of DePalma et al/ the 11 1specimens examined were categorized as follows: Type 1
(two specimens), Type 2 (none), Type 3 (four specimens),
Type 4 (two specimens), Type 5 (one specimen), and Type6 (two specimens) (Fig. 2). Although there was considerablevariation in the presence and structural thickness of thesuperior and middle glenohumeral ligaments, the inferiorglenohumeral ligament (IGHL) was easily identified in all11 specimens (Fig. 3).
Arthroscopic examination of the joint capsule through thenormal range of motion revealed that the IGHL was actuallya complex of structures consisting of an anterior band, aposterior band, and a diffuse thickening of the capsulebetween these bands that was termed the axillary pouch(Figs. 4 and 5). These components of the IGHLC werepresent in all 11 specimens, but were best demonstratedwith the shoulder in specific positions. The anterior andposterior bands of the IGHLC were most prominent whenthe humerus was internally or externally rotated in 90° ofabduction. In internal rotation, the posterior band of theIGHLC appeared to fan out and, along with the axillarypouch, provide support for the humeral head posteriorly(Fig. 6). In external rotation, the opposite occurred, with the
Figure 1. Schematic drawing of a shoulder specimen showingthe location and orientation of the histologic sections. A,anterior; P, posterior; a, sagittal section through anterior jointcapsule; b, sagittal section through anterior band of theIGHLC; c, sagittal section through axillary pouch of IGHLC;d, sagittal section through posterior band of the IGHLC; e,sagittal section through posterior joint capsule; f, coronalsection through posterior band of the IGHLC.

451
Figure 2. Drawings of the six types of joint capsule variationsas described by DePalma et al.’ The following percentagesof incidence are noted for each type and compared to thepercentage noted in their study (in parentheses). Type I,18.1 % (30.2%); Type II, 0% (2.04%); Type III, 36.3% (40.6%);Type IV, 18.1% (9.03%); Type V 9.9% (5.1 %); and Type Vi,18.1 % (11.4%).
Figure 3. Arthroscopic photograph of one of the specimensillustrating the posterior band (PB) of inferior glenohumeralligament. H, humeral head; G, glenoid.
Figure 4. Schematic drawing of the shoulder capsule illus-trating the location and extent of the IGHLC. A, anterior; P,posterior; B, biceps tendon; SGHL, superior glenohumeralligament; MGHL, middle glenohumeral ligament; AB, anteriorband; AP, axillary pouch; PB, posterior band; and PC, pos-terior capsule.
Figure 5. Cadaveric specimen illustrating the IGHLC. AB,anterior band; AP, axillary pouch; PB, posterior band; G,glenoid; H, humeral head.

452
Figure 6. Top, arthroscopic photograph of the posterior band(PB) of the IGHLC with the arm in external rotation. Note howthe posterior band (PB) appears more cord-like. Bottom, withthe arm in internal rotation the IGHLC &dquo;fans out&dquo; to supportthe humeral head (H). G, glenoid.
anterior band and axillary pouch supporting the humeralhead anteriorly.The IGHLC originated from the glenoid, the labrum, or
the neck of the glenoid just adjacent to the labrum. Thisvariation occurred between as well as within individual
specimens, and a precise classification was not possible. Theanatomical location of the origins of the anterior and pos-terior bands of the IGHLC on the glenoid also demonstratedsome slight variability although, in general, the origins werelimited to two distinct areas (Fig. 7). Describing the locationof these origins in terms of the face of a clock, the anteriorband was found to originate in an area between 2 and 4o’clock, whereas the posterior band originated in the 7 to 9o’clock position.The IGHLC inserted on the humerus just below the
articular margin of the humeral head (anatomical neck ofthe humerus) in one of two distinct configurations (Fig. 8).A collar-like attachment, in which the entire IGHLC at-taches just inferior to the articular edge of the humeral head,
Figure 7. Schematic drawing of the glenoid illustrating theattachment sites of the anterior and posterior bands of theIGHLC in the specimens examined. If viewed as the face of aclock the anterior attachments range from 2 to 4 o’clock,whereas the posterior attachments range from 7 to 9 o’clock.
Figure 8. Drawings of the proximal humerus illustrating thecollar-like (a) and &dquo;V&dquo;-shaped (b) attachments of the IGHLC.

453
was observed in six specimens. In the remaining five speci-mens, the attachment was in the shape of a &dquo;V&dquo; with theanterior and posterior bands attaching adjacent to the artic-ular edge of the humeral head and the axillary pouch attach-ing at the apex of the &dquo;V&dquo; distal to the articular edge.
Microscopic anatomy
The joint capsule in the area of the IGHLC consists of asynovial lining and three well-defined layers of collagenfibers (Fig. 9). The fibers of the inner and outer layersextend in a coronal axis from the glenoid to the humerus,whereas those of the middle layer are oriented at 90° to theinner and outer layers. The inner and middle layers of thecapsule are the thickest and most prominent. The outerlayer is the least prominent. However, the relative thicknessof these structures depends on the portion of the capsulestudied. The India ink markings of the joint capsule labelingthe arthroscopically identified bands of the IGHLC corre-lated directly with histologically distinguishable structuresin the joint capsule. The anterior and posterior bands of theIGHLC were actually abrupt thickenings in the inner layerof the joint capsule. On cross-section, these thickened areaswere found to be collections of well-organized, coarse colla-gen bundles running in the coronal plane from the glenoidto the humerus (Figs. 10 and 11). Although some variabilityin the size and density of these bands was noted betweenspecimens, the bands were always easily identified as dis-tinct histological structures within the capsule.The histologic appearance of the axillary pouch revealed
that although this area of the capsule appeared to be thethickest, the orientation of the collagen fibers was less
organized than that observed in the anterior and posteriorbands. There was a great deal of intermingling of the colla-gen fibers of the inner and middle layers in this area, and itwas difficult to delineate between the two (Fig. 12). Theouter layer of the capsule was virtually nonexistent in thisarea.
The capsule posterior to the IGHLC appeared to be thin-ner than the anterior capsule but retained the well-defined,three-layered histologic appearance previously described.The capsule anterior to the IGHLC was qualitatively thickerthan the posterior capsule because of an increase in therelative thickness of the middle layer (see Fig. 9). In addition,there appeared to be a great deal of intermingling of thecollagen fibers of the middle and outer layers. This coales-cence of fibers made it difficult to distinguish a separateouter layer in this area.
DISCUSSION
The IGHL has been described as a triangular-shaped thick-ening of the anterior-inferior joint capsule of the shoulderwith its apex at the glenoid labrum and its base blendingwith the capsule in an area between the subscapularis andtriceps.~ This anatomical description was expanded upon by
Figure 10. Schematic representation of the histology of theposterior band (A) and axillary pouch (B) of the joint capsuleas seen in the light and polarized light photomicrograph. Notehow layers one and two blend together in the axillary pouch.1, 2, 3 = layers of the capsule. (H & E x40)
Figure 9. Schematic drawing of a sagittal section of the IGHLC illustrating the three layers of the capsule and the location andorientation of the capsular structures.

454
Figure 11. &dquo;A&dquo; portion depicted in schematic in Figure 10. Histology of the posterior band as seen in the light (left) and polarizedlight (right) photomicrographs. S, synovium; 1, 2, 3 = layers of the capsule.
Figure 12. &dquo;B&dquo; portion depicted in schematic in Figure 10. Histology of the axillary pouch as seen in the light (left) and polarizedlight (right) photomicrographs. S, synovium; 1, 2, 3 = layers of the capsule.
455
another study that called attention to the anterior-superioredge of this especially thickened &dquo;ligament.&dquo;15 This promi-nent structure was termed the superior band of the IGHLand the area immediately posterior to this band called theposterior axillary pouch of the IGHL.15
Although these initial anatomical descriptions helped de-lineate the individual components of the anterior joint cap-sule, the examinations have been approached through thegross dissection of the posterior aspect of the capsule or bycomplete detachment of the humeral head. Such an ap-proach offers complete exposure of the anterior joint capsulebut disrupts the normal anatomical arrangement of thecapsular structures. With an arthroscope, the joint capsule
can be examined in situ, thus preserving the normal, func-tional anatomical relationship of the anterior capsular struc-tures.
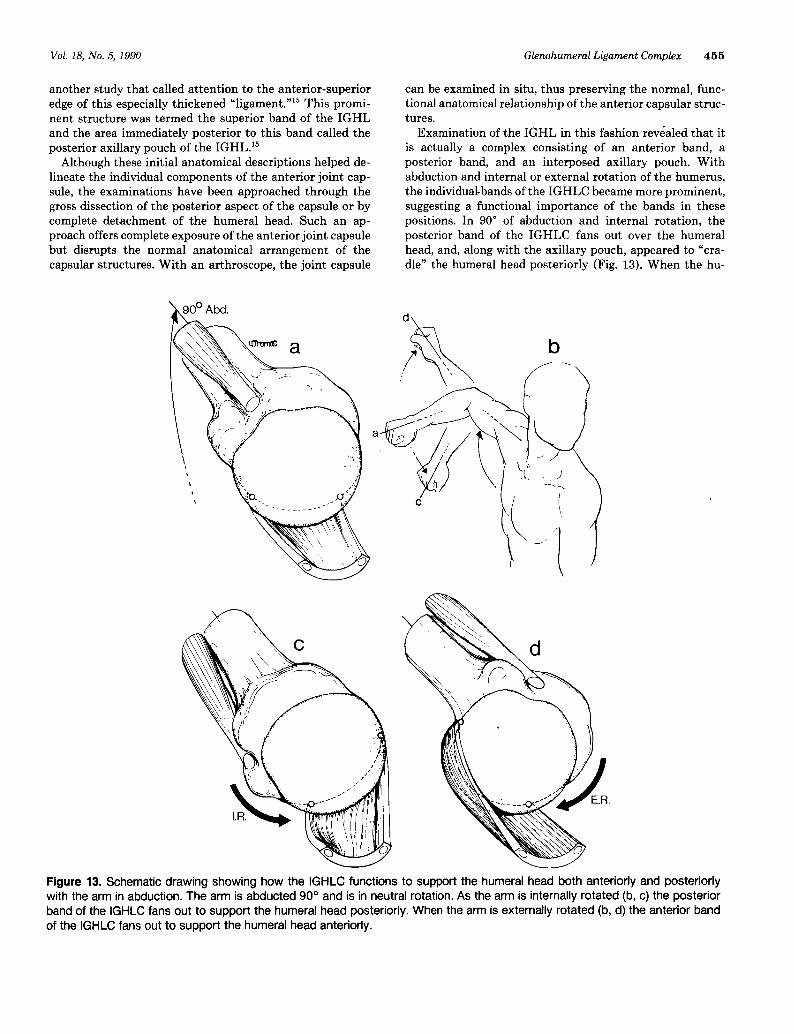
Examination of the IGHL in this fashion revealed that itis actually a complex consisting of an anterior band, aposterior band, and an interposed axillary pouch. Withabduction and internal or external rotation of the humerus,the individual-bands of the IGHLC became more prominent,suggesting a functional importance of the bands in thesepositions. In 90° of abduction and internal rotation, theposterior band of the IGHLC fans out over the humeralhead, and, along with the axillary pouch, appeared to &dquo;cra-dle&dquo; the humeral head posteriorly (Fig. 13). When the hu-
Figure 13. Schematic drawing showing how the IGHLC functions to support the humeral head both anteriorly and posteriorlywith the arm in abduction. The arm is abducted 90° and is in neutral rotation. As the arm is internally rotated (b, c) the posteriorband of the IGHLC fans out to support the humeral head posteriorly. When the arm is externally rotated (b, d) the anterior bandof the IGHLC fans out to support the humeral head anteriorly.

456
merus was externally rotated, the anterior band of theIGHLC appeared to fan out, and together with the axillarypouch support the humeral head anteriorly. In this regard,the IGHLC supports the humeral head much like a ham-mock, with the bands reciprocally tightening as the head isrotated in the abducted position.This functional anatomical concept is supported by a
biomechanical analysis of shoulder joint stability whichdemonstrated that in the abducted shoulder, the IGHLC isthe main static stabilizer to both anterior and posteriormotion.&dquo; The origins of the anterior and posterior bands ofthe IGHLC demonstrated some variability between speci-mens in terms of their specific location on the glenoid. Thesignificance of this variation is unknown. It may reflect afunctional adaptation to individual joint geometry or merelyfurther represent the anatomical variability of the capsuleas described by DePalma et aLl Further investigation isneeded to clarify the significance of this finding.While the IGHLC was present in all 11 specimens exam-
ined, there was considerable variation in the presence andsize of the superior and middle glenohumeral ligaments. Inthree of the specimens (27%), the middle glenohumeralligament was totally absent and, in another specimen, thesuperior glenohumeral ligament was almost nonexistent.Although the limited number of specimens in this studyprecludes direct comparison to the incidence of anatomicalvariations observed by DePalma et al.,l the considerablevariation in the presence, size, and location of the superiorand middle glenohumeral ligaments noted in these studiessuggests that these structures have little functional signifi-cance. However, additional study of the anatomy and func-tion of the superior and IGHL is needed to confirm thishypothesis.
In the precise anatomical definition, the glenohumeralligaments are not actually ligaments but rather thickeningsin the joint capsule. Histologic examination of the IGHLCrevealed a distinct collagen distribution and orientation thatdirectly reflected the location of the various components ofthe complex (anterior band, axillary pouch, posterior band)as observed grossly. This precise histologic pattern impliesthat although joint position does accentuate their grossappearance, the components of the IGHLC are distinctanatomical structures and not merely reflections of posturalchanges in the joint capsule. These findings have, we feel,significant clinical implications. For the first time, a distinctanatomical structure is outlined that may provide the keyto understanding both anterior and posterior stability in theshoulder.
CONCLUSIONS
In conclusion, the gross and microscopic structure of theinferior glenohumeral ligament complex reveals a distinct,functional, anatomical arrangement that appears to providesupport of the abducted humeral head in both internal andexternal rotation. This finding suggests that reestablishing
the normal anatomical integrity of the entire inferior gle-nohumeral ligament complex may be an important consid-eration in treating anterior and posterior shoulder instabil-ity.
REFERENCES
1. DePalma AF, Callery G, Bennett GA: Variational anatomy and degenerativelesions of the shoulder joint Instr Course Lect 6: 255-281, 1949
2. Flood V Discovery of a new ligament of the shoulder joint. Lancet 1. 672-673, 1829
3. Hawkins RJ, Koppert G, Johnston G: Recurrent posterior Instability (sub-luxation) of the shoulder. J Bone Joint Surg 66A: 169-174, 1984
4 Hovelius L, Thorling J, Fredin H: Recurrent antenor dislocation of theshoulder Results after the Bankart and Putti-Platt operations. J Bone JointSurg 61A. 566-569, 1979
5. Matsen FA: Glenohumeral instability, in Evarts CM (ed): Surgery of theMusculoskeletal System. New York, Churchill Livingstone, 1983, pp 349-75
6 Matsen FA, Zuckerman JD Anterior glenohumeral mstability Clin SportsMed 2. 319-338, 1983
7. Morrey BF, Janes JM: Recurrent antenor dislocation of the shoulder: Long-term follow-up of the Putti-Platt and Bankart procedures. J Bone JointSurg 58A: 252, 1976
8 Moseley HF, Overgaard B: The antenor capsular mechanism in recurrentanterior dislocation of the shoulder. J Bone Joint Surg 44B: 913-927, 1962
9 O’Bnen SJ, Warren RF, Schwartz E: Anterior shoulder Instability. OrthopClin North Am 18(3): 395-408, 1987
10. Rothman RH, Marvel JP Jr, Heppenstall RB: Recurrent antenor dislocationof the shoulder Orthop Clin North Am 6(2): 415-422, 1975
11 Schlemm F: Veber die Verstarkungsbander am Schultergelerk. Arch Anat.45-48, 1853
12 Schwartz RE, O’Bnen SJ, Torzilli PA, Warren RF: Capsular restraints toanterior-posterior motion of the shoulder. Trans Orthop Res Soc 12: 78,1987
13. Schwartz E, Warren RF, O’Bnen SJ, et al: Postenor shoulder instability.Orthop Clin North Am 18(3): 409-419, 1987
14. Thomas TT Post-hemiplegic shoulder pain. New York J Med 57. 1377-1380,1957
15. Turkel SJ, Panio MW, Marshall JL, et al. Stabilizing mechanisms preventingantenor dislocation of the glenohumeral joint. J Bone Joint Surg 63A:1208-1217, 1981
16. Warren RF: Subluxation of the shoulder in athletes. Clin Sports Med 2(2):339-354,1983
17 Warren RF, Kornblatt IB, Marchand R: Static factors affecting postenorshoulder stability. Orthop Trans 8(1): 89, 1984
DISCUSSION
Glenn C. Terry, MD, Columbus, Georgia: I think we areprogressing in a way with the shoulder that is very similarto the way in which thought concerning the knee hasevolved. We are moving toward understanding the subtletiesof shoulder anatomy. Strain gage analysis helps to delineateinjury patterns, but an understanding of normal functioncomes first.This paper was an excellent anatomical study of the
inferior glenohumeral ligament complex. The collagen workis beautiful and demonstrates the layering effect that I thinkcan be seen clinically. The authors’ work raises some intui-tive questions regarding the etiology of the &dquo;frozen&dquo; shoulderwith some kind of aberration in the sliding of those layers.Their work also emphasizes empirically the harmony be-tween the anterior and the posterior capsular structures.
I commend these authors for an excellent paper and
encourage them to continue with this work.
Related Documents











