286 Revista Românª de Anatomie funcþionalª ”i clinicª, macro- ”i microscopicª ”i de Antropologie Vol. IX - Nr. 3 - 2010 ORIGINAL PAPERS THE ANATOMICAL LESIONS OF CERVICAL ABRASION AND GINGIVAL RECESSION SIDE-EFFECTS OF TOOTHBRUSHING Dorelia Cªlin 1 , L. Frâncu 2 University of Medicine and Pharmacy Gr.T. Popa, Ia”i 1. Discipline of Cariology and Restorative Odontotherapy 2. Discipline of Anatomy THE ANATOMICAL LESIONS OF CERVICAL ABRASION AND GINGIVAL RECESSION SIDE-EFFECTS OF TOOTHBRUSHING (Abstract): The increased incidence of cervical abra- sion associated with gingival abrasion or recession, encouraged us to pursue the incidence, the characteristics and factors favoring the occurrence of these lesions. The clinical study evaluated 132 patients, of which 5.63% presented cervical abrasion lesions due to an inadequate tooth- brushing, the association with gingival recession meeting in the rate of 4.22%. The cases were of both sexes, all from urban areas and the age between 16 and 40 years, on which we evaluated the location, shape, size and sensitivity of the lesions. The highest incidence of lesions was found in the canines and premolars, especially on the mandibular arch. Canines, because of the anatomical alveolar bone defects and buccal location, are more susceptible to gingival recession. In all cases, the abrasion lesions and gingival recession are in a more advanced stage at the quadrant where begins the initial placement of the brush, in the opposite area of the hand which holds the brush. Key words: CERVICAL ABRASION OF TOOTH, DENTAL ANATOMY, GINGIVAL ABRA- SION, GINGIVAL RECCESION, TOOTHBRUSHING INTRODUCTION The natural cleaning of the teeth is insuffi- cient because the natural physiological forces cannot clean the oral cavity and remove all dental plaque. The physical methods are abso- lutely necessary to control the dental plaque. The toothbrushing is the main mean of pre- vention of oral cavity diseases. Because of the many benefits it has on oral health, the adverse effects and the damage of the hard and soft oral tissues are usually regarded as insignificant. Tooth cleaning devices date back thousands years. The Chinese used chewing sticks, which are considered primitive configurations of the toothbrush. The toothbrush itself was used by the Chinese in about 1000 years ago and is believed to have been made of hogs bristle. The toothbrush began to be used in Europe in the late 18 th century and early 19 th century but were too expensive to be used by anyone. In the late 1930s, nylon filaments have re- placed the natural hair and the handle was made of plastic or wood. They have become cheaper to reach by everyone, leading to a improved oral health of the population. Although manual brushing is the main way to maintain the oral hygiene, the majority of the people do not clean their teeth properly or for an adequate period of time. Thus, electric powered toothbrushes were invented in order to overcome these barriers and to maintain a proper oral hygiene. In the 1960s, the electric powered toothbrushes were used especially for patients with physical disabilities or for those who had limited manual dexterity. The toothbrush in combination with den- tifrice possesses some level of abrasivity, the reason for their use to remove deposits from the teeth may create undesirable effects on dental hard tissues and gingival. In the oral cavity, four tissues can be da- maged by the abrasive effect of toothbrushing: the enamel, dentine, gingival tissues and al- veolar mucosa. The most common injuries are: epithelial abrasion, gingival recession with root surface exposure in the oral cavity, cervical

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

286
Dorelia Cãlin, L. FrâncuRevista Românã de Anatomie funcþionalã ºi clinicã, macro- ºi microscopicã ºi de Antropologie
Vol. IX - Nr. 3 - 2010 ORIGINAL PAPERS
THE ANATOMICAL LESIONS OF CERVICAL ABRASION AND GINGIVALRECESSION � SIDE-EFFECTS OF TOOTHBRUSHING
Dorelia Cãlin1, L. Frâncu2
University of Medicine and Pharmacy �Gr.T. Popa�, Iaºi1. Discipline of Cariology and Restorative Odontotherapy
2. Discipline of Anatomy
THE ANATOMICAL LESIONS OF CERVICAL ABRASION AND GINGIVAL RECESSION �SIDE-EFFECTS OF TOOTHBRUSHING (Abstract): The increased incidence of cervical abra-sion associated with gingival abrasion or recession, encouraged us to pursue the incidence, thecharacteristics and factors favoring the occurrence of these lesions. The clinical study evaluated132 patients, of which 5.63% presented cervical abrasion lesions due to an inadequate tooth-brushing, the association with gingival recession meeting in the rate of 4.22%. The cases were ofboth sexes, all from urban areas and the age between 16 and 40 years, on which we evaluated thelocation, shape, size and sensitivity of the lesions. The highest incidence of lesions was found inthe canines and premolars, especially on the mandibular arch. Canines, because of the anatomicalalveolar bone defects and buccal location, are more susceptible to gingival recession. In all cases,the abrasion lesions and gingival recession are in a more advanced stage at the quadrant wherebegins the initial placement of the brush, in the opposite area of the hand which holds the brush.Key words: CERVICAL ABRASION OF TOOTH, DENTAL ANATOMY, GINGIVAL ABRA-SION, GINGIVAL RECCESION, TOOTHBRUSHING
INTRODUCTIONThe natural cleaning of the teeth is insuffi-
cient because the natural physiological forcescannot clean the oral cavity and remove alldental plaque. The physical methods are abso-lutely necessary to control the dental plaque.
The toothbrushing is the main mean of pre-vention of oral cavity diseases. Because of themany benefits it has on oral health, the adverseeffects and the damage of the hard and soft oraltissues are usually regarded as insignificant.
Tooth cleaning devices date back thousandsyears. The Chinese used chewing sticks, whichare considered primitive configurations of thetoothbrush. The toothbrush itself was used bythe Chinese in about 1000 years ago and isbelieved to have been made of hog�s bristle.
The toothbrush began to be used in Europein the late 18th century and early 19th centurybut were too expensive to be used by anyone.
In the late 1930s, nylon filaments have re-placed the natural hair and the handle was madeof plastic or wood. They have become cheaper
to reach by everyone, leading to a improvedoral health of the population.
Although manual brushing is the main wayto maintain the oral hygiene, the majority ofthe people do not clean their teeth properly orfor an adequate period of time. Thus, electricpowered toothbrushes were invented in orderto overcome these barriers and to maintain aproper oral hygiene. In the 1960s, the electricpowered toothbrushes were used especially forpatients with physical disabilities or for thosewho had limited manual dexterity.
The toothbrush in combination with den-tifrice possesses some level of abrasivity, thereason for their use to remove deposits fromthe teeth may create undesirable effects ondental hard tissues and gingival.
In the oral cavity, four tissues can be da-maged by the abrasive effect of toothbrushing:the enamel, dentine, gingival tissues and al-veolar mucosa. The most common injuries are:epithelial abrasion, gingival recession with rootsurface exposure in the oral cavity, cervical
287
The Anatomical Lesions of Cervical Abrasion and Gingival Recession
abrasion of cementum and dentine.The aim of our study is to continue the
previous research (1) on the effects of incorrecttooth brushing, with inadequate products, onthe soft and hard oral tissues.
MATERIALS AND METHODSOur study included the assessment of the
dentition and of the effects of toothbrusing onthe hard and soft oral tissues in 132 pacients inthe dental office of discipline of Cariology andRestorative Odontotherapy of University of Medi-cine ºi Pharmacy �Gr. T. Popa� Iaºi.
The selected patients for the clinical studywere of both sexes and between 16 and 72years old. They were from both rural and urbanareas. All the patients hadn�t presented associa-ted diseases of oral mucosa and general diseases.
The selected cases were presented dentaland gingival lesions caused by toothbrushingassessed after a systematic and accurate dentalhistory. The assessment of the lesions was madeafter the removing of the debris, dental plaquefrom the surface of the lesions, using the mirrorand dental probe. We aimed to detect if thereare present concomitant cervical lesions andgingival lesions or gingival recession in the sameindividual and the topography of the lesions.
RESULTS AND DISCUSSIONSThe study of our personal casuistry allowed
us to detect eight cases of cervical abrasioncaused by toothbrushing which represents 5.63%.The both sexes were interested, three caseswere found in male persons and five in femalepersons, all the cases were in people fromurban areas.
At six of the eight cases, the cervical lesionsof abrasion were accompanied by gingival re-cession (75%), which represents 4.22% of allexamined patients. The gingival recession waslocated most frequently at the cervical abrasionlesions of the mandibullary and maxillary ca-nines (8 teeth), then the premolars (5 teeth)and incisors (1 tooth). In one patient wererevealed lesions of type I gingival abrasion.
In all cases, the abrasion lesions and gin-gival recession are in a more advanced stage atthe quadrant where begins the initial placementof the brush, in the opposite area of the handwhich holds the brush.
We will present the lesional characteristicsaspects in the detected cases.
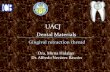
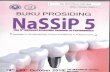
Case no 1: C.D., 38 years, presents type Igingival lesion, a patch-like surface defect cau-sed by toothbrushing at 22 tooth (fig. 1) andtype I gingival lesion, a ribbon-like surfacedefect and gingival recession localized to 33caused by the abnormal position in the dentalarch (fig. 2).
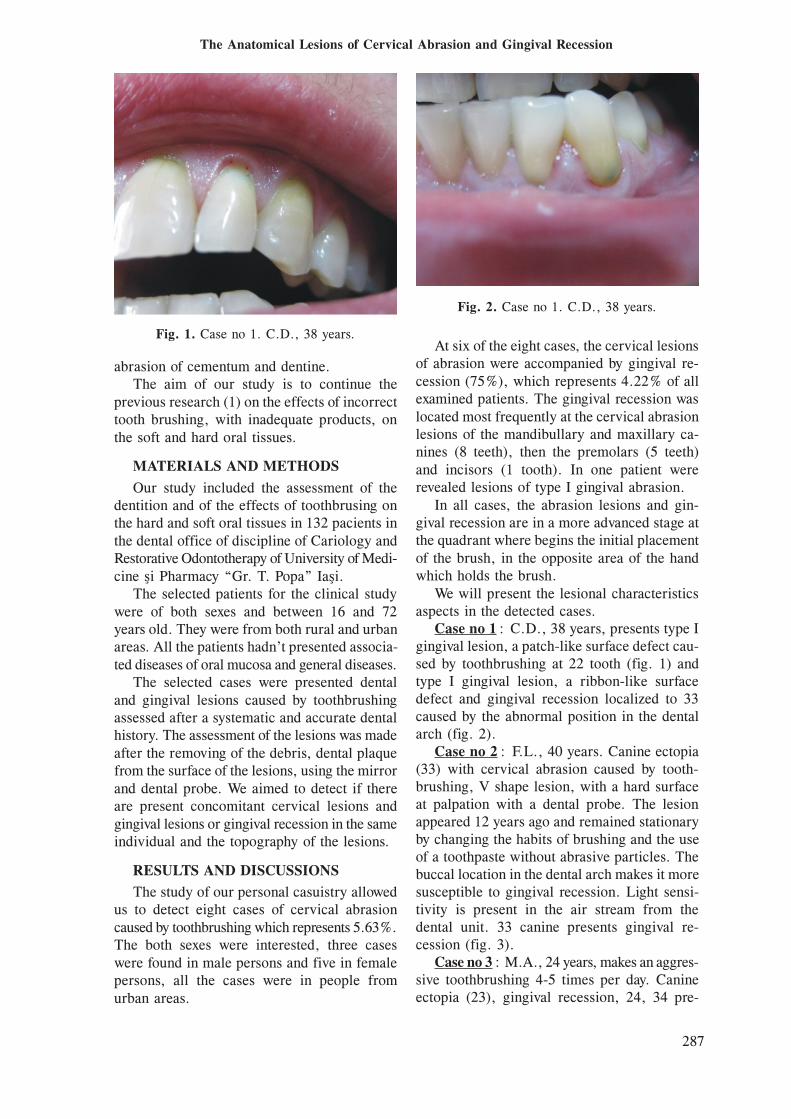
Case no 2: F.L., 40 years. Canine ectopia(33) with cervical abrasion caused by tooth-brushing, V shape lesion, with a hard surfaceat palpation with a dental probe. The lesionappeared 12 years ago and remained stationaryby changing the habits of brushing and the useof a toothpaste without abrasive particles. Thebuccal location in the dental arch makes it moresusceptible to gingival recession. Light sensi-tivity is present in the air stream from thedental unit. 33 canine presents gingival re-cession (fig. 3).
Case no 3: M.A., 24 years, makes an aggres-sive toothbrushing 4-5 times per day. Canineectopia (23), gingival recession, 24, 34 pre-
Fig. 1. Case no 1. C.D., 38 years.
Fig. 2. Case no 1. C.D., 38 years.
288
Dorelia Cãlin, L. Frâncu
sents gingival recession caused by inappro-priate toothbrushing and buccal location in thedental arch. Light sensitivity is present.
Case no 4: L.A., 23 years, toothbrushingmanually performed 2-3 times per day. Cer-vical abrasion lesion at 43 accompanied bygingival recession (fig. 4)
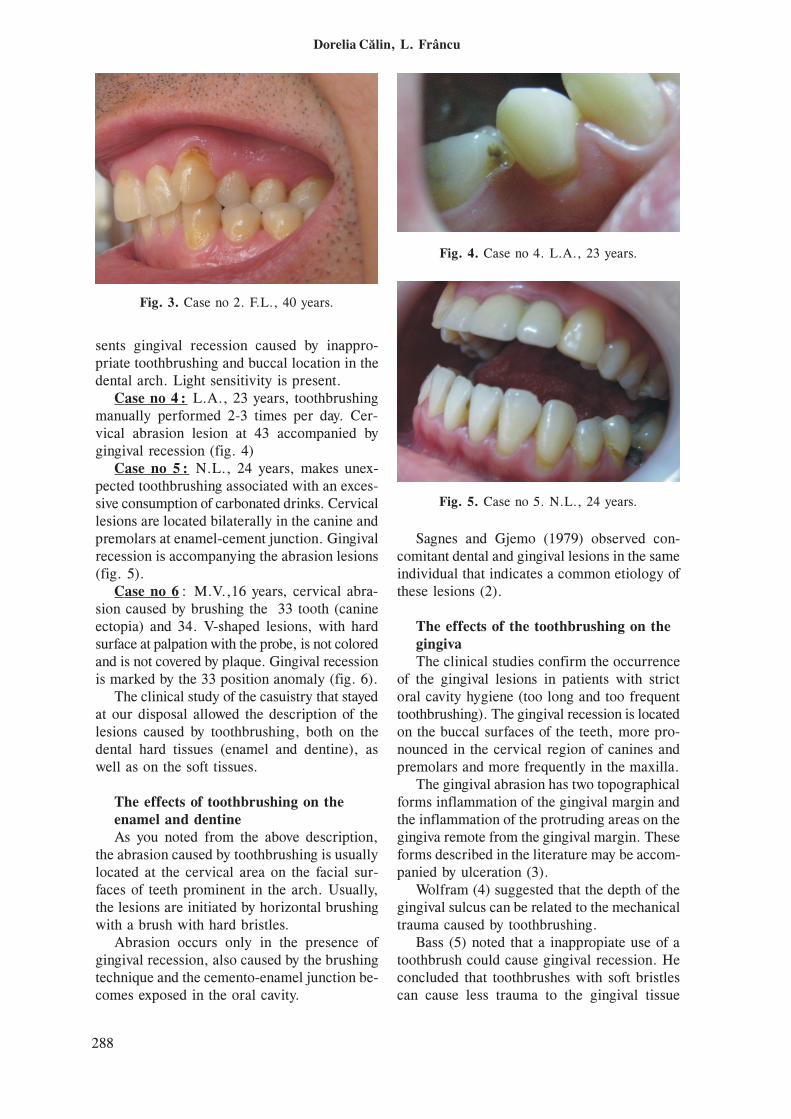
Case no 5: N.L., 24 years, makes unex-pected toothbrushing associated with an exces-sive consumption of carbonated drinks. Cervicallesions are located bilaterally in the canine andpremolars at enamel-cement junction. Gingivalrecession is accompanying the abrasion lesions(fig. 5).
Case no 6: M.V.,16 years, cervical abra-sion caused by brushing the 33 tooth (canineectopia) and 34. V-shaped lesions, with hardsurface at palpation with the probe, is not coloredand is not covered by plaque. Gingival recessionis marked by the 33 position anomaly (fig. 6).
The clinical study of the casuistry that stayedat our disposal allowed the description of thelesions caused by toothbrushing, both on thedental hard tissues (enamel and dentine), aswell as on the soft tissues.
The effects of toothbrushing on theenamel and dentineAs you noted from the above description,
the abrasion caused by toothbrushing is usuallylocated at the cervical area on the facial sur-faces of teeth prominent in the arch. Usually,the lesions are initiated by horizontal brushingwith a brush with hard bristles.
Abrasion occurs only in the presence ofgingival recession, also caused by the brushingtechnique and the cemento-enamel junction be-comes exposed in the oral cavity.
Sagnes and Gjemo (1979) observed con-comitant dental and gingival lesions in the sameindividual that indicates a common etiology ofthese lesions (2).
The effects of the toothbrushing on thegingivaThe clinical studies confirm the occurrence
of the gingival lesions in patients with strictoral cavity hygiene (too long and too frequenttoothbrushing). The gingival recession is locatedon the buccal surfaces of the teeth, more pro-nounced in the cervical region of canines andpremolars and more frequently in the maxilla.
The gingival abrasion has two topographicalforms inflammation of the gingival margin andthe inflammation of the protruding areas on thegingiva remote from the gingival margin. Theseforms described in the literature may be accom-panied by ulceration (3).
Wolfram (4) suggested that the depth of thegingival sulcus can be related to the mechanicaltrauma caused by toothbrushing.
Bass (5) noted that a inappropiate use of atoothbrush could cause gingival recession. Heconcluded that toothbrushes with soft bristlescan cause less trauma to the gingival tissue
Fig. 3. Case no 2. F.L., 40 years.
Fig. 4. Case no 4. L.A., 23 years.
Fig. 5. Case no 5. N.L., 24 years.

289
The Anatomical Lesions of Cervical Abrasion and Gingival Recession
compared to those with hard bristles and recom-mended that each filament tip should be end--rounded to minimize tissue trauma.
Since 1953 the researches of the Stahl (6)shows that toothbrusing increases the kerati-nisation degree of the gingiva, natural hairbrushes are more traumatic compared to thoseof nylon. More recently, demonstrated that thetoothbrushing is a traumatic procedure for theperiodontal tissues. The soft tissue trauma maylead to gingival abrasion (7) and to gingivalrecession (8, 9).
The gingival recession is localized on thefacial surfaces of the teeth and is attributed toan improper toothrushing technique (7). Thelesions are more pronounced in the cervicalareas of the incisors, canines and premolars(2). The lesions are more common in the ma-xilla compared with the mandible. Subjectswith a thin gingival tissue are more susceptibleto gingival recession compared to those with athick gingival tissue (10).
The gingival recession is more frequent inpeople that cleans their teeth with hard bristletoothbrush. It occurs more often in older peoplebut is not related to the physiological effect ofageing, but shows that the toothbrusing wasmade for a longer period of time (11). Theincrease of the frequency of the gingival recessionas a result of an aggressive toothbrushing canlead in time to an increased incidence of theroot surface caries.
Gillette and van House (3) have described aclassification of the lesions which result fromimproper oral hygiene measures. This classi-fication is based upon source of injury, site ofoccurence and potential side-effects. Thus, thegingival lesions caused by toothbrushing areclassified in three groups:� Laceration which is an acute mechanical
trauma� Gingival recession� Hyperkeratinization and hyperplasia, the last
two being characteristic of chronic lesions.Sandholm (1982) (7) used scanning electron
microscopy to describe these lesions and des-cribed 3 types:� Type I- erosion of the epithelial surface at
the gingival margin with the appearance ofa ribbon or patch-like surface defect or adiffuse border at the gingiva-tooth interfacecaused by bleeding or oozing of tissue fluid
from the eroded areas;� Type II- epithelial, surface flap rolled up
leaving the underlying tissue uncovered;� Type III- rupture or fenestration of the sur-
face epithelium in the middle of the promi-nent but healthy gingival area.Breitenmoser (1979) (12) found that the use
of a disclosing agent such as that used for dentalplaque may result in an excellent staining of theselesions and they could be easily distinguishedfrom normal gingiva. The small lesions of abra-sion are not visible on clinical evaluation (13).
Several factors must be considered in theetiopathogenesis of the cervical abrasion le-sions and gingival recession which can be sys-tematized as:� Individual factors: such as inappropriate
toothbrushing technique, the frequencyof toothbrushing, the force used duringbrushing;
� Factors related to the material: the use of ahard bristle toothbrush, the quality of thetoothbrush, the dentifrice abrasiveness;
� The position of the teeth in the arch.
The force used during toothbrushingNumerous clinical and experimental studies
support the assumption that the use of an ex-cessive force during toothbrushing is respon-sible in part for the trauma caused to the softand hard dental tissues (14).
Previously, numerous studies have evaluatedthe force during toothbrushing and showed sig-nificant variations in force magnitude (15, 16).Differences appear to be related to toothbru-shing technique, toothbrush design,research me-thods.
McLey ºi Zahradnik (1994) (17) investigatingthe force used during the power toothbrushingcompared with the manual toothbrushing de-monstrated that the force used during manualbrushing is significantly higher compared withthat of the electric brush. Van der Weijden(1996) (18) obtained similar results. The re-sults of these studies may be relevant in termsof maintaininig the long-term integrity of oralsoft and hard tissues exposed to various brushingdevices.
An inadequate toothbrushing is the mainfactor responsible for a repetitive gingivaltrauma leading to tissue distruction and gingivalrecession.

290
Dorelia Cãlin, L. Frâncu
Dentifrice abrasivenessDepends on the toothpaste properties. They
contain many ingredients, but the most com-mon are detergents and abrasives which cancause loss of tooth substance.
Beyeler ºi Mooser (1960) (19), during astudy of patients with a so called �perfecthygiene�, showed that the cervical abrasion andgingival lesions can be caused by the abrasivecomponents of the dentifrices. In addition, theamount of applied dentifrice may increase itsabrasive potential (20), and the cervical abra-sion is closely linked to the use of undilutedtoothpaste that is places in the same area of theoral cavity (21). It is useful to advise patientsto use decreased quantities of dentifrice andbegin brushing on the occlusal surfaces in orderto dilute the toothpaste. Also, it is recom-mended to alternate the initial placement of thepaste between quadrants in order to distributethe abrasive effect.
The end of the bristlesSince 1948, Bass recommended that each
filament should be end-rounded to minimiyetissue trauma. Studies that assessed the effectof the end of the bristles on the gingival surface(12), showed that manual brushes with pointedbristles produce greater gingival lesions com-pared with end-rounded bristles.
Force control during brushingLately, manual and electric toothbrushes
manufacturers have introduced designs whichsould limit the force used to reduce the chanceof hard and soft dental tissue damage (22).
CONCLUSIONS1. The toothbrushing is the main mean of pre-
vention of oral cavity diseases, but oral hygieneproducts should be evaluated for safety.
2. Cervical abrasion lesions and gingival lesionshave a common and multifactorial etiology.
3. There are many predisposing factors: ana-tomical, physiological and pathologicalwhich potentiate the effects of an inadequatebrushing.
4. The abrasive effect of toothbrushing candamage four tissues in the oral cavity: theenamel, dentine, gingival tissue and alveolarmucosa.
5. Both conditions are developing in a longperiod of time and in incipient forms aredifficult to detect clinically.
6. Cervical abrasion occurs in 5.63% of allexamined patients, while the association withgingival recession accurs in a proportion of4.22%.
7. These associated lesions occurs morefrequently on canines and premolars, onteeth with abnormal position, the mandi-bullary arch is more frequently interested.
8. The abrasion lesions and gingival recessionare in a more advanced stage at the quadrantwhere begins the initial placement of thebrush, in the opposite area of the hand whichholds the brush.
REFERENCES1. Cãlin D, Frâncu L. Modificarea anatomiei dentare în abrazia cervicalã cauzatã de periajul dentar.
Revista Românã de Anatomie funcþionalã ºi clinicã, macro- ºi microscopicã ºi de Antropologie, 2010;9(1):44-50.
2. Sangnes G, Gjermo P. Prevalence of oral soft and hard tissue lesions related to mechanical tooth--cleansing procedures. Community Dent Oral Epidemiol 1976, 4:77-83
3. Gillette WB, van House RL. Ill effects of improper oral hygiene procedures. J Am Dent Assoc 1980,101:476-81.
4. Wolfram K, Egelberg J, Hornbuckle C, Oliver R, Rathbun E. Effect of tooth cleaning procedures ongingival sulcus depth. J Periodont Res 1974, 9:44-9.
5. Bass C. The optimum characteristics of toothbrushes for personal oral hygiene. Dent Items of Interest1948, 70:697-718.
6. Stahl SS, Wachtel N, De Castra C, Pelletier G. The effect of toothbrushing on the keratinization of thegingiva. J periodontol 1953, 24:20-1.
7. Sandholm L, Niemi ML, Ainamo J. Identification of soft tissue brushing lesion. A clinical andscanning electron microscopic study. J Clin Periodontol 1982, 9:397-401.
8. Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severityand extent of gingival recession. J Periodontol 1992, 63:489-95.
291
The Anatomical Lesions of Cervical Abrasion and Gingival Recession
9. Serino G, Wennstrom JL, Lindhe J, Eneroth L. The prevalence and distribution of gingival recessionin subjects with a high standard of oral hygiene. J Clin Periodontol 1994, 21:57-63.
10.Olsson M, Lindhe J. Periodontal characteristics in individuals with varying form of upper centralincisors. J Clin Periodontol 1991, 18:78-82.
11. Joshipura Kj, Kent RL, DePaola PF. Gingival reccesion: intraoral distribution and associated factors.J Periodont 1994, 65:864-71.
12.Breitenmoser J, Mörmann W, Mühlermann HR. Damaging effects of toothbrush bristle end form ongingiva. J periodontol 1979, 50:212-6.
13.Danser MM, Timmernan MF, Ijzerman Y, Van der Velden U, Warren PR, Van der Weijden GA. Acomparison of electric toothbrushes in their potenþial to cause gingival abrasion of oral soft tissues. AmJ Dent 1998, 11:S35-S39.
14.Niemi M-L, Ainamo J, Etemadzadeh H. The effect of toothbrushing grip on gingival abrasion andplaque removal during toothbrushing. J Clin Periodontol 1987, 14:19-21.
15.Phaneuf EA, Harrington JH, Asland I. Automatic toothbrush: a new reciprocating action. J Am DentAssoc 1962, 65:12-25.
16.Fraleight CM, McElhaney JH, Heiser RA. Toothbrushing force study. J Dent Res 1967, 46(pt.2):209-14.
17.McLey L, Boyd RL, Sarker S. Clinical and laboratory evaluation of powered electric toothbrushes:relative degree of bristle end-rounding. J Clin Dent 1994, 8(3):86-90.
18.Van der Weijden GA, Timmerman MF, Reijerse E, Snoek CM, Van der Velden U. Toothbrushing forcein relation to plaque removal. J Clin Periodontol 1996, 23:724-9.
19.Beyeler K, Mooser M. Recherches à propos du nettoyage des dents des brases à bien naturels et enmatières synthétiques. Pouvoir abrasif du brossage avec et sans pates dentifrices. Schweiz MschrZahnhk, 1960, 70:123-52.
20.Harte DB, Manly RS. Four variables affecting magnitude of dentifrice abrasiveness. J Dent Res 1976,55:322-7.
21.Radentz WH, Barnes GP, Cutright DE. A survey of factors possibly associated with cervical abrasionof tooth surfaces. J Periodontol 1976, 47:148-55.
22.Van der Weijden GA, Timmerman MF, Reijerse E, Snoek CM, Van der Velden U. Comparison of 2electric toothbrushes in plaque-removing ability. Professional and supervising brushing. J ClinPeriodontol 1995, 22:648-52.
Related Documents
![Effects of Adjunctive Daily Blue Light Toothbrushing on ...dental plaque and maintaining a healthy gingivae [5]. Studies have shown that persistent gingival inflammation is a risk](https://static.cupdf.com/doc/110x72/5f098adc7e708231d427539b/effects-of-adjunctive-daily-blue-light-toothbrushing-on-dental-plaque-and-maintaining.jpg)