THE ACQUISITION OF COORDINATE CONCEPTS IN NURSING EDUCATION A STUDY ON THE EFFECTIVENESS OF INTERACTIVE VIDEO IN CONCEPT FORMATION J. Gulmans

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THE ACQUISITION OF COORDINATECONCEPTS IN NURSING EDUCATION
A STUDY ON THE EFFECTIVENESS OF INTERACTIVE VIDEO INCONCEPT FORMATION
J. Gulmans
ii
CIP-GEGEVENS KONINKLIJKE BIBLIOTHEEK, DEN HAAG
Gulmans, J.
The acquisition of coordinate concepts in health educationThesis Universiteit Twente Enschede - With ref. - Met samenvatting in het NederlandsISBN 9036512379Subject headings: instructional technology/ concept acquisition/interactive video
All rights reserved. No part of this book may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying, recording orotherwise without the prior permission of the author.
Cover design: FEBODRUK BV, EnschedePhoto: J. JonkerPrint: FEBODRUK BV, Enschede
Copyright © 1998 J. Gulmans

iii
THE ACQUISITION OF COORDINATE CONCEPTS IN NURSING EDUCATION
A study on the effectiveness of interactive video in concept formation
PROEFSCHRIFT
ter verkrijging vande graad van doctor aan de Universiteit Twente,
op gezag van de Rector Magnificus,prof. dr. F. A. van Vught,
volgens besluit van het College voor Promotiesin het openbaar te verdedigen
op donderdag 3 december 1998 te 15.00 uur
door
Jan GulmansGeboren op 2 september 1944
te Ternaard

iv
Dit proefschrift is goedgekeurd door de promotor:
Prof.dr. S. Dijkstra

v
The narrative construal of reality is surprisingly difficult to dissect. Narrativized realities,I suspect, are too ubiquitous, their construction too habitual or automatic to be accessible toeasy inspection. We live in a sea of stories, and like the fish who will be the last to discoverwater, we have our own difficulties grasping what it is like to swim in stories. It is not that welack competence in creating our narrative accounts of reality-far from it. We are, if anything,too expert.
Jerome Bruner, (1996). The Culture of Education, Cambridge, Massachusetts: HarvardUniversity Press, page 147.
vi
vii
Acknowledgments
I would like to express my gratitude to everyone who assisted with the completion of this
study. In particular, I would like to thank my supervisor Prof. Dr. S. Dijkstra for his support. I
am indebted to him for his advice on many parts of this dissertation. I would like to thank B.
Reimerink for programming the Authorware program and J. Schmitz and R. Dieleman for the
development of the video script. Furthermore I am indebted to R. Dieleman and M. Caris for
camera-work, M. Vorwerk for the make-up work, H. Snijder and A. Veugelers for graphical
design, A. Veugelers for animation, A. R. J. van den Berg and P. A. Schmitz for montage, T.
Rijssemus for video operating, J. Oosterhuis for technical support, Telemedia GMBH
Gütersloh for laser disc production, Wim Tielen for statistical advice, and Els Bevers for
developing the graphs.
S. Tiemersma, E. Sietsma and J. Feitsma contributed much to the analysis of the medical
concepts and mechanisms. I would like to thank J. Bolster ('Lotusvereniging Nederland') for
enabling patient simulation and E. Hesp for support of 'Laméris Instrumenten BV'. I greatly
appreciate that Thyra Kamphuis-Kuijpers edited the manuscript and last but not least I
gratefully acknowledge the support of Arnd-Jan, Jelmer, Jitske and Maria.
Jan Gulmans
Enschede, December 1998

viii
ix
THE ACQUISITION OF COORDINATECONCEPTS IN NURSING EDUCATION
Table of Contents
Chapter 1 Theoretical context.
Abstract ........................................................................................................................ 11.1 Introduction....................................................................................................................... 21.2 Concepts and categories.................................................................................................... 21.3 Hypothesis formation........................................................................................................ 41.4 Paradigm shift ................................................................................................................... 41.5 Gradience and centrality ................................................................................................... 51.6 Levels of concepts............................................................................................................. 61.7 Instructional design and the acquisition of concepts ........................................................ 71.8 Tennyson’s model of concept teaching........................................................................... 101.9 The purpose of this study................................................................................................ 13References ...................................................................................................................... 14
Chapter 2 Instructional programs, authoring systems and multimedia.
Abstract ...................................................................................................................... 172.1 Introduction..................................................................................................................... 182.2 Material ...................................................................................................................... 18
2.2.1 The selection and analysis of a coordinate concept ..................................... 182.2.2 Description of the coordinate concept shock ............................................... 18
2.3 Instructional programs .................................................................................................... 222.3.1 General design of the instructional programs .............................................. 222.3.2 The first program ......................................................................................... 222.3.3 The second program..................................................................................... 232.3.4 The third program ........................................................................................ 282.3.5 Program scores............................................................................................. 36
2.4 Tests ...................................................................................................................... 362.4.1 Post-test........................................................................................................ 362.4.2 Transfer test ................................................................................................. 36
2.5 Apparatus ...................................................................................................................... 372.5.1 The first experiment..................................................................................... 372.5.2 The second and third experiment................................................................. 37
2.6 Authoring and learning environment .............................................................................. 382.6.1 The first experiment ..................................................................................... 382.6.2 The second and third experiment ................................................................. 38
References ...................................................................................................................... 43
x
Chapter 3 Instructional design for learning to categorise a disease.
Abstract ...................................................................................................................... 453.1 Introduction..................................................................................................................... 463.2 Method ......................................................................................................................48
3.2.1 Subjects ........................................................................................................ 483.2.2 Material ........................................................................................................ 483.2.3 Tests ............................................................................................................. 493.2.4 Procedure ..................................................................................................... 50
3.3 Results ...................................................................................................................... 503.4 Discussion ...................................................................................................................... 53References ...................................................................................................................... 55
Chapter 4 The effect of the presentation of best examples and attributeelaboration on the acquisition of coordinate concepts.
Abstract ...................................................................................................................... 574.1 Introduction..................................................................................................................... 58
4.1.1 The nature of examples................................................................................ 594.1.2 Attribute elaboration .................................................................................... 614.1.3 The interaction effect ................................................................................... 62
4.2 Method ......................................................................................................................634.2.1 Subjects ........................................................................................................ 634.2.2 Material ........................................................................................................ 634.2.3 Apparatus, authoring system and courseware.............................................. 664.2.4 Transfer test ................................................................................................. 684.2.5 Procedure ..................................................................................................... 694.2.6 Data and design............................................................................................ 69
4.3 Results ...................................................................................................................... 704.3.1 Program scores............................................................................................. 704.3.2 Transfer test scores....................................................................................... 73
4.4 Discussion ...................................................................................................................... 74References ...................................................................................................................... 75
Chapter 5 The effect of different modes of activation of prerequisite knowledge onthe acquisition of coordinate concepts.
Abstract ...................................................................................................................... 775.1 Introduction..................................................................................................................... 785.2 Method ......................................................................................................................84
5.2.1 Subjects ........................................................................................................ 845.2.2 Material ........................................................................................................ 845.2.3 Apparatus ..................................................................................................... 845.2.4 Implementation of the instructional-design model for interactive video..... 855.2.5 Transfer test ................................................................................................. 875.2.6 Procedure ..................................................................................................... 87
xi
5.3 Results ...................................................................................................................... 885.3.1 Program results ............................................................................................ 885.3.2 Results of the transfer test............................................................................ 90
5.4 Discussion ...................................................................................................................... 91References ...................................................................................................................... 93
Chapter 6 General discussion.
Abstract ...................................................................................................................... 956.1 Tennyson and Cocchiarella's concept teaching model.................................................... 966.2 Overall discussion of the results ..................................................................................... 996.3 Current and future research........................................................................................... 1036.4 Multimedia in nursing education .................................................................................. 104References .................................................................................................................... 106
Dutch summary (Nederlandse samenvatting).................................................................... 109
Appendices
Appendix A: Overview of (exemplary) cases for the interactive program ‘Shock’ .......... 117Appendix B: Transfer test.................................................................................................. 133Appendix C: Glossary of prerequisite knowledge ............................................................ 135Appendix D: Concept analysis of the three types of shock ............................................... 141Appendix E: Principles and strategies for multimedia ...................................................... 145Appendix F: User manuals for the interactive video ‘Shock’ .......................................... 147Appendix G: Program scores and transfer test scores ....................................................... 163Appendix H: Overview of patients.................................................................................... 167
About the author .................................................................................................................. 169
1
INSTRUCTIONAL-DESIGN MODEL FORTEACHING CONCEPTS
In this chapter the theoretical context of this study is presented. The studyaddresses the problem, how to learn the skill to categorise patients in a distinctdisease class and how instruction influences the learning. The instructionaldesign model developed by Tennyson and Cocchiarella (1986) is used to study theeffects of different instructional strategies. The model is developed to teachdifferent types of concepts. In chapter 1 a brief description of the psychology ofconcept formation is presented. Also the interpretation of concept formation as aprocess of hypothesis formation is discussed and the issues of centrality, familyresemblance, gradience and taxonomic levels are addressed. Special attention isgiven to a paradigm shift in the psychology of concept formation towards theprototype theory. Finally the purpose of this study is described. The studycomprises three experiments. The first one addresses prototype formation versusattribute listing as factors determining the acquisition of coordinate concepts. Thesecond studies the effect of the presentation of best examples and attributeelaboration on the acquisition of coordinate concepts. The third experimentaddresses the effect of different modes of refreshment of prerequisite knowledgeon the acquisition of coordinate concepts.

Chapter 1
2
1.1 Introduction
This thesis addresses the problem which instructional conditions help students to effectively
acquire coordinate concepts in a medical subject matter domain and, secondly, to learn the
skill to categorise patients in a distinct disease class. In this study the instruction for solving
categorisation problems will be varied. The effects of different presentation forms and of the
salience of attributes will be determined. The presentation forms were mainly deducted from
the instructional design model for teaching concepts as specified by Tennyson and
Cocchiarella (1986). Because the instructional design models for the acquisition of concepts
are influenced by the psychology of concept learning this topic will be briefly introduced
first. It comprises a description of concepts and the method that is used to study concept
learning. Also the theories of hypothesis formation, centrality, family resemblance, gradience
and taxonomic levels will be addressed. Then it will be shown how the interpretations
influenced Tennyson and Cocchiarella’s model. Finally the purpose of this study will be
described.
1.2 Concepts and categories
A concept is defined by one or more attributes related by a rule. The mental structure in
which a subject represents a category, is called a concept; it represents a class of things, not
any particular member of a class. A single object is referred to in terms of feature, attribute or
characteristic (for example: Peter has red hair). The concept contains the attribute (attributes)
of all objects which share the attribute(s). An attribute is a value on a certain variable or
dimension ((for example: hair has colour). Learning a concept implies to separate relevant
and irrelevant attributes. Relevant attributes define the concept. Examples of the concept,
however, will have other attributes that are unrelated to the concept. Most objects have a
large number of attributes, only some of which are relevant to the concept to which the object
is assigned. In addition to its relevant attributes, a concept is defined by a rule that combines
these attributes in a particular way. For example, a concept may require the joint presence of
two attributes. Since concepts are defined both by the relevant attributes and a rule of
combination, learning the concept requires discovering both attributes and rule. The
following rules that relate the attributes of a concept have been identified: (a) affirmation, (b)
Theoretical Context
3
negation, (c) conjunction, (d) disjunction, (e) conditional, and (f) biconditional (Bourne,
1965).
Thus a concept is a mental representation of a category, which enables a person to sort
objects into that category if they meet the rule. Categorisation is a basic activity in human
thought. Concepts are acquired by abstracting information from objects. Concepts enable one
to draw inferences and to solve problems. A concept is a categorisation rule. Categorisation is
a commonly occurring cognitive process. At the end of that process a decision is taken
whether, and if so to what degree, a certain entity (object, process, event, person, symbol) can
be assigned to a certain class. This function of concepts is characterised by Bruner, Goodnow
and Austin (1956) as follows: categorisation implies making equivalent separate entities; it
implies grouping of objects, events and persons, and to react to them in terms of their class
membership and not in terms of their uniqueness (Bruner et al., p. 1).
The skill to categorise objects correctly includes (a) the perception of objects, (b) the
development of the concept, and (c) knowledge and skills. Objects can share one or more
attributes. Whether that is the case, is perceived and described. Objects that share an attribute
can be comprised in a category (class, set). The process of learning to categorise can start
with assigning a name to entities that have one or more attributes in common. The description
based on which an entity is assigned to a category, is the concept. A distinction is made
between natural categories, formal categories and categories of designed objects. Other types
of categories are also possible. The concepts that were developed by people during centuries,
are transferred to members of new generations. That transfer takes place by categorisation of
objects and, secondly, the development of concepts. The skill comprises the application of the
identification algorithm.
There are many types of concepts, including object- and event-, concrete- and abstract
concepts, well-defined and ill-defined concepts, conjunctive- and disjunctive concepts. A
concept can include perceptual, functional and/or relational attributes. Perceptual attributes
are clearly obvious to the senses. Functional attributes are attributes of objects designed to
satisfy a need. The third type of attributes reflect a relationship between two things. Kinship
concepts are familiar examples of that type of attributes. The attributes of the objects are used
to categorise the object. Those attributes that are used for the purpose of categorisation are
labelled as relevant attributes. Those not used are irrelevant. Categories are constructed by
humans. For the description of the objects those attributes that always or often appear are

Chapter 1
4
used for categorising. If they are necessary for categorising they are labelled defining,
otherwise they are labelled characteristic attributes.
1.3 Hypotheses formation
The theory of hypotheses formation (Trabasso & Bower, 1968) states that a presumptive
concept is adopted and maintained until there is evidence for an alternative. Studies based on
the theory of hypotheses formation have resulted in the identification of three types of
concept learning processes: (a) the learning of attributes (in this case it is known what the
logical connection between the attributes are), (b) the learning of the logical connection (in
this case the attributes are known), and (c) the complete learning (in this case neither the
attributes nor the connections are known). Discovering the relevant attributes is often
depicted as a process of testing hypotheses. Assuming that the relevant attributes are within
the set of attributes a person has attended to, the person selectively tests them (practising
concept identification tasks) until the irrelevant ones have been discarded and the relevant
ones remain. The assumption that hypotheses testing is a fundamental part of learning
concepts first portrays concept learning as a constructive process, one in which the subject
generates candidate hypotheses. Second, it stresses the role of feedback in learning a concept;
without feedback, in fact, one cannot learn a concept. Finally, hypotheses testing is selective
for a certain period; it focuses on certain attributes.
1.4 Paradigm shift
About 1970 a paradigm shift took place. Neisser (1987) and Posner (1986) speak about a
revolution, which Rosch induced in the theory of concept formation. The pure hypotheses
formation was abandoned and the prototype theory was developed (Smith & Medin, 1981;
Osherson & Smith, 1981). This new paradigm, sometimes called gradience theory, assumed
that complex entities cannot be defined in a simple way. For these entities no set of necessary
and sufficient conditions can be determined based on which the entity can be assigned to a
certain category. The structure of these concepts can be characterised in terms of the
resemblance between the members of a family. Certain attributes can be found in many
family members, but there are also certain attributes that they do not have. The concept of
family resemblance is for the prototype theory (Rosch, 1978) an alternative for the necessary
Theoretical Context
5
and sufficient attributes. The prototype theory assumes that each instance shares attributes
with one or more instances within the category, but there are no attributes shared by all
instances. Rosch and Mervis (1975) assumed that concepts are organised around a best
example or a prototype. The prototype is conceived of, an "average" member of a category.
This means that the prototype contains the most frequently occurring attributes of the
members of a category. A prototype is an idealised abstraction of the members of a category.
In the studies of Posner and Keele (1968) on the identification of dot patterns they
concluded that the speed of categorisation increases depending on the deviation of the
prototype. The prototype was categorised most quickly. The speed of categorisation evidently
is a function of the distance to the prototype. Based on this evidence Posner and Keele stated
that: (a) a category is a not clearly circumscribed space, (b) the prototype is that point in this
space that has the smallest distance to the instances of the category. From these statements
follows that the prototype coincides with an "average image" of the object that has those
attributes that most frequently occur in the instances of a category (Neumann, 1977).
Depending on whether an instance is constituted from the more frequently occurring
attributes, it is a more prototypical instance of the category. One can only speak about the
degree in which examples are typical. The fact that members of a category vary as to
typicality is referred to as the graded structure of natural categories (Barsalou, 1985).
Typicality is assumed to be the central variable. This applies to the acquisition of concepts,
the retrieval of instances, and the verification of instances. The most typical instances are
acquired firstly. The typicality of an instance predicts how probable it is that the instance will
be retrieved. It is shown that if an instance is verified as a member of a category, the
typicality of an instance is positively correlated to the speed of the verification of that
instance (Smith, Shoben & Rips, 1974).
1.5 Gradience and centrality
Mervis and Rosch (1981) and Smith and Medin (1981) state that concepts frequently have
fuzzy boundaries, a gradient internal structure, and that therefore there is a family
resemblance between members of a category and the best examples. The evidence for the
existence of family resemblance is the typicality effect. Examples vary to the degree in which
they are seen as typical for a category. Typical members of a category have a greater family
resemblance, that means more common attributes, than atypical members. Typical members
Chapter 1
6
serve as cognitive reference points. Atypical members of a category commonly are "linked"
more frequently to contrasting categories than typical members. Rosch emphasises that the
non-essentialistic or analogous view of reference as is implied by the prototype theory, is
inconsistent with those theories which conceive categories as “Aristotelian in nature, that is,
that categories are logical, clearly bounded entities, whose membership is defined by a simple
set of criterial features, in which all instances possessing the criterial attributes have a full and
equal degree of membership”. Peripheral members of a category can deviate for a number of
attributes from the typical members of the category.
Objects that belong to a category often cannot be described adequately by a list of defining
attributes. More likely these objects can be recognised by attributes that have a high
probability of occurrence within the class of objects involved; the attributes enable that the
objects can be differentiated from objects from other classes. These attributes are called
characteristic attributes. In order to categorise objects the attributes have different weights,
that vary depending on goals, context and the activation of content specific prior knowledge.
Objects, comprised in a category, differ to the degree in which they can be described as a
member of the category. The typicality or centrality of an object is the degree to which an
object can be conceived as typical for its category. The continuum to which the entities can
be arranged as more or less typical is called the typicality gradient.
Within the gradience theory other assumptions can be differentiated. They differ in their
answer toward two main questions: (a) is a process of abstraction of information assumed
about instances of a category that results in a summary representation? (b) are the
characteristic attributes of instances of categories conceived as discrete or continuous
(dimensional)? The prototype theory assumes that subjects tend to abstract the characteristic
attribute information from the experience with some instances and, secondly, that they store
that attribute information as a cognitive prototype in memory. For that reason a prototype can
be conceived as an "ideal" representation of an object class. The prototype of a category
comprises a list of attributes, where the attributes have different weights according to the
degree in which they are characteristic or typical for the category. Theoretically a prototype is
situated at a higher abstraction level than concrete objects and therefore a prototype cannot be
identified with a single typical object. The perspective of Rosch (1973a, 1973b, 1975a,
1975b) is: “By prototypes of categories we have generally meant the clearest cases of
category membership defined operationally by people’s judgements of goodness of
membership in the category” (Rosch, 1978, p. 36).

Theoretical Context
7
1.6 Levels of concepts
A category is a class to which objects are assigned based on similarity. A concept contains
information (e.g., attributes or an instance) which enables a person to assign objects to
categories. A suitable method to depict the relation between concepts is to generate a
taxonomy. For this study, superordinate, coordinate and subordinate concepts are
distinguished and schematically represented. A concept with a high ranking in the taxonomy
is the most general. Concepts at lower levels are more specific. A subordinate concept always
has the attributes of the superordinate concept and also a number of other attributes. Thus
there is an inheritance of attributes from higher level concepts to lower levels concepts.
Concepts at the same level of abstraction are called coordinate concepts.
For the categorisation of natural objects Rosch (1978) distinguished the basic level, the
superordinate and the subordinate level. Also in this case it applies that a concept at a lower
level is subsumed in a concept at a higher level. Concepts at the superordinate level have few
common attributes, and, secondly, they tend to be the most general ones. The concepts at the
basic level have more common attributes (in terms of Rosch: they are more distinctive) and,
secondly, they tend to be less general. Concepts at the lowest level have hardly more
attributes than concepts at the basic level. Rosch assumes that concepts at the basic level tend
to have the most suitable degree of abstractness and distinctiveness: they are always learned
first and named fastest. For that reason, instruction has to take place at this level. The
arrangement in superordinate, basic, and subordinate levels is referred to as the vertical
dimension of categories. The horizontal dimension is formed by coordinate concepts (i.e.,
concepts at the same abstraction level).
In summary, the differentiation of basic-level categories arises because they both have a
high degree of within-category similarity and a high degree of between-category
dissimilarity. For differentiation of natural categories the similarity is a variable. It is assumed
that categories at different levels of abstraction vary in their amount of within- and between-
category similarity. Basic-level and superordinate categories have approximately equal low
amounts of between-category similarity, but basic-level categories have more within-category
similarity than superordinate categories. Basic-level and subordinate categories have
approximately equal high amounts of within-category similarity, but basic-level categories
have less between-category similarity than subordinates do.
Chapter 1
8
1.7 Instructional design and the acquisition of concepts
This paragraph contains a general overview of the rules to be applied in instructional design
for learning concepts. To learn a concept the subjects have to discover its relevant attributes
and the rule relating to them. Once the subjects have learned the relevant attributes and the
rule, they have acquired the concept and can distinguish examples of it from objects that have
some but not all of the relevant attributes. Learning a concept involves at least the following
processes: (1) discovering the relevant attributes, (2) discovering the rule that relates the
attributes, (3) testing hypotheses, and (4) using strategies, which are procedures that may be
used for learning a concept. In the first stages of learning a concept, the subjects face a
profusion of attributes. The task here is to attend to the relevant attributes and ignore the
irrelevant ones. One factor influencing attention to attributes is the salience of the attributes.
This causes that some features are noticed quickly in a concept-learning task, while others are
only noticed later if at all. When the salient attributes are relevant, learning the concept is
easy; but it is more difficult when irrelevant attributes are salient.
In their instructional design guide for teaching concepts Merrill, Tennyson and Posey
(1992) maintain the view on the teaching of concepts, as stated by Merrill and Tennyson
(1977). Merrill, Tennyson and Posey define a concept as follows: “A concept is a set of
specific objects, symbols, or events which are grouped together on the basis of shared
characteristics and can be referenced by a particular name or symbol” (p. 6). Concepts specify
the rules based on which objects can be categorised. An instance is: “A general term used to
refer to both members and non-members of concept class. There are two kinds of instances:
examples and non-examples” (p. 6). An example is an instance, which is a member of the
concept. Merrill et al. differentiate between two types of non-examples: (1) type A non-
examples: members of another concept coordinate of the concept class under consideration,
(2) type B non-examples: members of any other concept class not under consideration.
Students have learned a concept when they can correctly identify the class membership of a
specific object, or event. Classification behaviour does not occur if the subject is required to
recall memorised concept definitions or previously learned instances. According to Merrill’s
view, rule-using behaviour occurs when a subject is asked to combine objects or events from
two or more classes by means of some operation to form an object or event in a resulting
concept class. This rule-using behaviour includes pattern recognition. This term “describes
Theoretical Context
9
active cognitive processes in which the students look for patterns in the stimulus information
of newly encountered instances which correspond to patterns of a previously acquired
example of a concept class” (Merrill et al., 1992, p. 11). The basic processes underlying the
application of concepts are generalisation and discrimination. Merrill et al. define
generalisation as occurring “when learners exhibit a particular response in a stimulus situation
which they acquired in an earlier, but similar stimulus situation. When students are exposed
to a previously unencountered instance of a concept class, they generalise by looking for
common attributes which the new instance shares with previously encountered examples.” (p.
12). A discrimination “occurs when a student exhibits a particular response in one stimulus
situation, but a different response in a similar stimulus situation.” (p. 13). Thus classification
behaviour is generalisation within a class and simultaneous discrimination among classes.
For the acquisition of coordinate concepts the critical attributes have to be discriminated
and used for determining class membership. The learner can use them to generalise within a
class or to discriminate between classes (Merrill et al., p. 28). There are at least two types of
critical attributes that have relevance for the design of instruction: constant and variable. The
first type of critical attributes possesses values that are discrete and remain constant. The
second type of critical attributes (variable) have values that are represented along a continuum
or arranged on some other dimension. In many cases boundaries of their values are not exact
and are usually determined by the context (Tennyson & Cocchiarella, 1986).
In learning a concept at some moment a complete definition of the concept has to be
provided. It consists of the concept’s name, it’s critical attributes and an indication of how the
critical attributes are combined. The most common type of definition shows a conjunctive
type of relationship in which attributes are joined by an “and”. In this case all of the critical
attributes must be present for an instance to be a member of the concept class. In case of a
disjunctive concept the presence of all possible combinations of critical attributes is not
necessary.
The instructional design of concept teaching includes the use of (a) divergent examples,
(b) matched non-examples, and (c) helpful hints (Merrill et al., p. 46). The divergent example
rule assumes that concept classification performance is enhanced by exposing the student to
examples of the concept that are as divergent as possible. Obtaining divergents depends on
the concepts critical attributes. If the attributes are constant, divergents can be achieved by
changing the context. If the attributes are variable, the position within the specified range of
any of their values that exist along a continuum or other dimension can be changed. Use of

Chapter 1
10
matched non-examples means exposing the student to examples matched to an example of a
coordinate concept within the concept class. By matched, Merrill means that the attributes of
an example of concept A are explained as similar to the attributes of example of coordinate
concept B. Constant and variable critical attributes can be matched by changing the context in
which they are presented. For helpful hints an appropriate format for concept learning is
designed. Improved concept classification performance can be achieved by using attention
focusing devices to direct the learner’s attention: (1) to the critical attributes in a specific
example - to correct for undergeneralization errors, (2) to potentially confusing attributes
present in a particular example or non-example - to correct for misconceptions, and (3) to the
absence of the critical attributes in a specific non-example - to correct for overgeneralization
errors (Merrill et al., p. 90). Some useful attention focusing devices include colour, drawings,
symbols, written or audio notes, illustrations and video. Colour is one of the easiest and most
effective devices used to isolate attributes. In some concepts, attributes can be isolated by
means of drawings or breaking the instance apart into its attribute components. Often dotted
lines, underlining, italics, or other symbols can be used to focus attention on the critical
attributes. Sometimes concepts may require the use of motion to illustrate one or more of the
critical attributes. Video disc and compact disc technology are particularly suited for
application in which concept attributes can be effectively depicted through use of full motion,
slow motion, or freeze frame segments. Instructional design models often contain a
component for the activation of prior knowledge. Activating prior knowledge helps students
form a context for integrating new information provided by the instruction with an existing
knowledge base (p. 100).
Theoretical Context
11
1.8 Tennyson’s model of concept teaching
For the experiments to be described the instructional design model for the acquisition of
concepts, conceived by Tennyson and Cocchiarella (1986), is used because this instructional
design model is based on the prototype theory of concept formation. The model assumes that
the learning of concepts proceeds in two stages. In the first stage conceptual knowledge is
formed and in the second stage procedural knowledge is developed resulting from the
application of conceptual knowledge in the context of solving domain-specific problems. The
use of procedural knowledge when solving a problem elaborates the conceptual knowledge.
Tennyson and Cocchiarella suppose that any concept has two content structure qualities:
attribute characteristics and relational structure. The attribute characteristics are distinguished
in constant and variable. The relational structure of a concept to other concepts is considered
to be successive or coordinate. The combination of the design components content structure
and instructional design variables results in four instructional strategies that are shown in
Table 1.1.
Tennyson and Cocchiarella distinguish four primary instructional design variables: (a)
definition (a rule or generality encompassing the structure of the critical attributes), (b)
expository examples (examples and non-examples which organise systematically the
information in a propositional format), (c) interrogative examples (examples and non-
examples which present the information systematically in interrogatory format), (d) attribute
elaboration (analysis of critical attributes in expository instances and feedback to the critical
attributes in interrogative instances). Based on attribute characteristics and relational structure
and using the instructional design variables Tennyson and Cocchiarella distinguish between
four instructional strategies (see Table 1.1).
Relational structure.Successive concepts are characterised by a vertical relationship in that
the superordinate concept contains the subordinate concept (for example: the concept
'furniture' contains the concept 'chair'); due to inheritance the attributes of the superordinate
concept do also apply for the subordinate concept. Coordinate concepts are characterised by a
horizontal relationship in that they have a set of common attributes and at least one distinctive
attribute. For concepts with successive relationships learning is "limited primarily to the
development of generalisation within a concept class" (Tennyson & Cocchiarella, p. 42). The
production rule that will be practised, will categorise the objects into one category. For
Chapter 1
12
concepts with coordinate relationships learning includes the development of skills to
generalise with a concept class and to discriminate between concepts" (p. 42).
Attribute characteristics.The attribute characteristics of a concept are the second aspect of
the content structure component, which influences the instructional design. If concepts have
critical attributes that "remain stable across contexts" (Tennyson & Cocchiarella, p. 42), they
are termed constant dimension concepts. Concepts with critical attributes that vary across
contexts are labelled variable dimension concepts. For each of the attributes of a concept it
has to be determined whether they are constant or variable. An analysis of the perceptibility,
the complexity, the structure of a concept and the synthesis of these factors are necessary for
the classification as constant or variable (Tennyson & Cocchiarella, p. 55). The perceptibility
of a concept is related to the definition of the concept. If the definition does not change
depending on the context in which it has been learned, then the concept has constant
dimensions. A concept has variable dimensions if the definition and the examples of the
concept change from context to context.
In order to form conceptual knowledge it is necessary to link the existing knowledge, as
stored in memory, and the concept to be learned. Sometimes the existing knowledge will be
refreshed. The instruction starts with the label and one or more of the definitions of the
concept. These have to contain the defining attributes of the concept and they have to refer to
the prerequisite knowledge (Merrill & Tennyson, 1977). When concepts with variable
dimensions are involved a problem can be presented in a context or in a contextual situation
in order to provide extra information. This contextual knowledge can be applied to generate
conceptual knowledge.
Theoretical Context
13
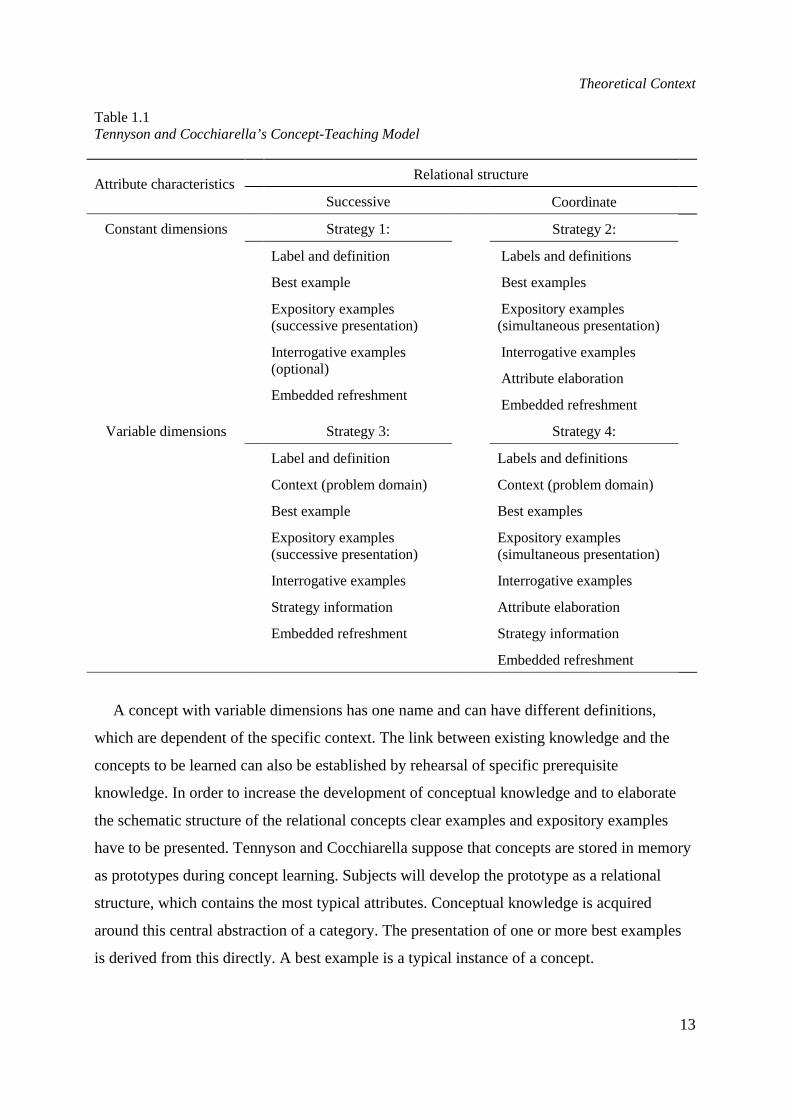
Table 1.1Tennyson and Cocchiarella’s Concept-Teaching Model
Relational structureAttribute characteristics
Successive Coordinate
Constant dimensions Strategy 1: Strategy 2:
Label and definition
Best example
Expository examples(successive presentation)
Interrogative examples(optional)
Embedded refreshment
Labels and definitions
Best examples
Expository examples(simultaneous presentation)
Interrogative examples
Attribute elaboration
Embedded refreshment
Variable dimensions Strategy 3: Strategy 4:
Label and definition
Context (problem domain)
Best example
Expository examples(successive presentation)
Interrogative examples
Strategy information
Embedded refreshment
Labels and definitions
Context (problem domain)
Best examples
Expository examples(simultaneous presentation)
Interrogative examples
Attribute elaboration
Strategy information
Embedded refreshment
A concept with variable dimensions has one name and can have different definitions,
which are dependent of the specific context. The link between existing knowledge and the
concepts to be learned can also be established by rehearsal of specific prerequisite
knowledge. In order to increase the development of conceptual knowledge and to elaborate
the schematic structure of the relational concepts clear examples and expository examples
have to be presented. Tennyson and Cocchiarella suppose that concepts are stored in memory
as prototypes during concept learning. Subjects will develop the prototype as a relational
structure, which contains the most typical attributes. Conceptual knowledge is acquired
around this central abstraction of a category. The presentation of one or more best examples
is derived from this directly. A best example is a typical instance of a concept.
Chapter 1
14
Expository examples have a double function. First subjects abstract the most relevant
attributes by comparing and by contrasting these examples. This contributes to the
completion and the elaboration of the conceptual knowledge. The expository examples have
to be presented successively when concepts with a successive relational structure are involved
and they have to be presented simultaneously when concepts with a coordinate relational
structure are addressed. The expository examples have to be combined with cues how the
clear-cut instance can be used in order to compare and to contrast. The second function of the
expository examples is to support the development of procedural knowledge. They serve as a
transition between the formation of conceptual knowledge and the development of procedural
knowledge. Procedural knowledge, in the form of production rules, is used in order to solve
domain-specific problems. This competence is developed further by the application of
conceptual knowledge when complex domain-specific problems are encountered. The
appropriate instructional design components in this context are interrogative examples,
strategic information and attribute elaboration. Interrogative examples are presented when the
students have to solve classification problems. They have to be presented cues in order to
compare each interrogative example with the example learned earlier. The presentation of
strategic information increases the development of procedural knowledge and therefore the
capabilities to provide correct classifications.
1.9 The purpose of this study
One of the four strategies (strategy two, see Table 1.1) for the teaching of concepts, as
presented by Tennyson and Cocchiarella, provides the framework of this study. Especially the
components typical example, expository instance, interrogatory instance and embedded
refreshment are applied in the design and development process. The subject matter comprises
the coordinate concept shock. The students from a nursing school will learn to categorise
videotaped patients in one of three subcategories of this concept. The effect of the following
design components will be studied.
Experiment 1: Prototype formation versus attribute listing as factors determining the
acquisition of coordinate concepts.
Theoretical Context
15
It is expected that prototype formation will lead to an increased capability to assign a
patient to a disease class. The expectation is that the development of a prototype is facilitated
by the presentation form which contains typical examples of the to be learned concept.
Experiment 2: Presentation of best examples and attribute elaboration on the acquisition of
coordinate concepts.
The expectation is that decisions on class membership are facilitated if categorisation takes
place as a process of comparison between prototype and example. Thus it is expected that a
combination of expository and interrogatory examples of a category will be more effective
compared to interrogatory examples only. Secondly, it is expected that attribute elaboration
(marking of relevant attributes) will tend to have a strengthening effect compared to no
attribute elaboration.
Experiment 3: Different modes of knowledge refreshment on the acquisition of coordinate
concepts.
It is expected that error-related activation of prerequisite knowledge will tend to increase
the program- as well as the transfer test score, compared with parallel activation and
activation in advance. The theory, design components and the expectations will be discussed
in chapters 3, 4 and 5.
References
Barsalou, L. W. (1985). Ideals, central tendency and frequency of instantiation as determinants ofgraded structure in categories.Journal of Experimental Psychology: Learning, Memory, Cognition,11, 629-654.
Bourne, L. E., Jr. (1965).Human conceptual behavior.Boston: Allyn & Bacon.Bruner, J. S., Goodnow, J., & Austin, G. (1956).A study of thinking. New York: Wiley.Merrill, M. D., & Tennyson, R. D. (1977).Teaching concepts: An instructional design guide.
Englewood Cliffs, NJ: Educational Technology Publications.Merrill, M. D., Tennyson, R. D., & Posey, L. O. (1992).Teaching concepts: an instructional design
guide.Englewood Cliffs, NJ: Educational Technology Publications.Mervis, C. B., & Rosch, E. (1981). Categorization of natural objects.Annual Review of Psychology,
32, 89-115.Neisser, U. (1987).Concepts and conceptual development: ecological and intellectual factors in
categorization.Cambridge: Cambridge University Press.Neumann, P. G. (1977). Visual prototype formation with discontinuous representation of dimensions
of variability. Memory and Cognition, 5, 2, 187-197.
Chapter 1
16
Osherson, D. N., & Smith, E. E. (1981). On the adequacy of prototype theory as a theory of concepts.Cognition, 9, 35-58.
Posner, M. I. (1986). Empirical studies of prototypes. In H. Putnam,Mind, language and reality.Cambridge: Cambridge University Press.
Posner, M. I., & Keele, S. W. (1968). On the genesis of abstract ideas.Journal of ExperimentalPsychology, 77, 353-363.
Rosch, E. (1973a). Natural categories.Cognitive Psychology,4, 328-350.Rosch, E. (1973b). On the internal structure of perceptual and semantic categories. In T. E. Moore
(Ed.),Cognitive development and the acquisition of language. New York: Academic Press.Rosch, E. (1975a). Cognitive reference points.Cognitive Psychology, 7, 532-547.Rosch, E. (1975b). Cognitive representations of semantic categories.Journal of Experimental
Psychology: General,104, 192-233.Rosch, E. (1978). Principles of categorization. In E. Rosch & B. B. Loyd (Eds.),Cognition and
categorization. Hillsdale, NJ: Erlbaum.Rosch, E., & Mervis, C. B. (1975). Family resemblances: Studies in the internal structure of
categories.Cognitive Psychology, 7, 573-605.Smith, E. E., & Medin, D. L. (1981).Categories and concepts. Cambridge, MA: Harvard University
Press.Smith, E. E., Shoben, E. J., & Rips, L. J. (1974). Structure and process in semantic memory: a featural
model for semantic decisions.Psychological Review, 81, 214-241.Tennyson, R. D., & Cocchiarella, M. F. (1986). An empirically based instructional design theory for
teaching concepts.Review of Educational Research, 56, 1, 40-71.Trabasso, T., & Bower, G. H. (1968).Attention in learning: theory and research.New York: Wiley.
2
INSTRUCTIONAL PROGRAMS, AUTHORINGSYSTEMS AND MULTIMEDIA
In this chapter the instructional content to be learned is presented as well as theauthoring system used to identify the effects of different presentation forms. Theconcept to be learned was shock. Shock is a state characterised by the inability ofthe heart and/or the peripheral circulation to maintain an adequate perfusion ofvital organs. In order to identify differential effects of different instructionalmodes to acquire the concept of shock three different instructional programs weredeveloped; they were implemented on a videodisc. The interactive video wasdeveloped in order to test the effects of variations of the instructional design.Especially the following instructional variables are studied: (a) nature ofexamples, (b) marking and contrasting of the attributes of the examples and (c)the relation between the conceptual knowledge to be developed and the existingknowledge. In order to develop the instructional program AuthorWareProfessional has been used which is appropriate for the Apple Macintosh microcomputer. In order to combine video and computer graphics AuthorWare uses aDigital Video Adaptor (DVA-4000). This Video Logic digitalises the analoguesignal of the video disc player.
Chapter 2
18
2.1 Introduction
For the three experiments of this study the same material and the same presentation facilities
were used. For that reason this chapter contains general information: (a) instructional content,
(b) instructive programs, (c) apparatus, (d) authoring environment and (e) learning
environment.
2.2 Material
2.2.1 The selection and analysis of a coordinate concept
Many coordinate concepts are found in the biological and medical domains. After consulting
three teachers of a nursing school the choice was made for the coordinate concept shock. It is
a disease category with different subcategories. Because shock can arise quickly and soon
become life threatening the recognition of the illness by nurses is extremely important and the
necessary actions to save the patient’s life have to be taken immediately.
2.2.2 Description of the coordinate concept shock
Shock is a state of the human body characterised by the inability of the heart to maintain an
adequate perfusion of vital organs. It is defined by the presence of symptoms as hypotension
(blood which is too low), tachycardia (a heart rate which is too high) , sweating, pallor,
cyanosis (a grey/blue colour due to centralisation of the blood to vital organs),
hyperventilation, and oliguria (urinary output which is not sufficient). Shock is always
secondary to some initiating event, such as myocardial infarction, trauma, haemorrhage (loss
of blood), burns or infection. The longer shock persists the more the physiological variables
merge into a pattern in which consequences of prolonged circulatory failure dominate.
Hemodynamic measurements of patients with acute myocardial infarction and, in particular,
results obtained from patients with cardiogenic shock due to myocardial infarction, provide
evidence that the mean arterial pressure is reduced.
Cardiac output is reduced in all patients who have shock. Peripheral arterial resistance is
increased. The extraction of oxygen from arterial blood is enhanced in the periphery. When
cardiac output and arterial blood pressure are reduced, being a consequence of either
haemorrhage or acute cardiac failure, blood flow to the peripheral organs is reduced. The
Instructional Programs, Authoring Systems and Multimedia
19
degree to which perfusion of any organ is reduced reflects the passive pressure-flow relation
of that organ. Blood flow during shock is characterised by a reduced perfusion to nearly all
peripheral organs, but the extent of the reduction is not uniform. Maximal decreases are
observed in the skin, in the kidney and in the intestine.
Whether shock is induced by haemorrhage or by myocardial infarction, the decrease of
cardiac output and of regional perfusion has profound effects on cellular metabolism. In part,
these changes are a direct consequence of reduced arterial perfusion. The reduction in cardiac
output that accompanies haemorrhage or myocardial infarction is highly variable. In general,
however, the decrease in cardiac output parallels the severity of blood loss in cases of
haemorrhage and the extent of myocardial damage in infarction. With modest reductions of
cardiac output the metabolic needs of peripheral tissues are met by an increase in oxygen
extraction from arterial blood. Shock can be viewed as a state of oxygen deficiency. Because
the degree of hypofusion is non-uniform, the extent of oxygen lack in various organs and
tissues is also not uniform. Although acidosis is a prominent and common manifestation of
prolonged shock, and even of early shock if it is severe, arterial blood pH is frequently normal
in early shock. The reason for this is that hyperventilation leads to a compensatory respiratory
alkalosis. If peripheral hypofusion persists or worsens, however, the rise in plasma lactate
progresses and a state of lactic acidemia ensues. A decrease in the pumping capacity of the
heart plays a prominent role in shock. In acute myocardial infarction and other cardiogenic
causes of shock, depressed myocardial performance is evident early and is the basis of
reduced cardiac output. In haemorrhage and other forms of hypovolemic shock, myocardial
performance is normal initially but becomes depressed as shock persists.
Changes in the function of the lung play a central role in the pathophysiology of shock.
They highlight a general feature of shock that initial disturbances of organ function reflect the
cause of shock and, secondly, that subsequent changes begin to merge regardless of the cause.
Haemorrhage that is sufficient to induce systemic hypotension produces immediate changes in
lung function that are attributable almost entirely to a decrease in blood volume. The decrease
in blood volume decreases venous return and cardiac output. The subject hyperventilates due
to the stimulation of peripheral chemoreceptors as a consequence of reduced blood flow. The
decrease in venous return leads to decreases in right atrial, pulmonary, and left atrial
pressures. The volume of blood within the lung is reduced, and at least initially lung
compliance is increased and the work of breathing is reduced. Cardiogenic shock differs from
Chapter 2
20
hypovolemic shock in that cardiac output fails despite a normal or elevated blood volume.
Left arterial pressure, pulmonary arterial pressure, and right atrial pressure are elevated, not
reduced, during the initial phase.
The most common attributes of shock are paleness, coldness, perspiration, fast pulse and
low pressure. The attributes of hypovolemic shock are coldness, restlessness, hypotensia,
oliguria, increased breathing. The attributes of cardiogenic shock are low perfusion, clammy
skin, low systolic pressure and urinary output less than 25 ml. The attributes of septic shock
are vasodilatation, tachycardia, and deficient perfusion and breathing. Sometimes
anaphylactic shock (characterised by irregular breathing, urticaria, vascular collapse) and
neurogenic shock (characterised by irregular peripheral vascular tonus) are distinguished
separately. In this analysis these types of shock are subsumed under the category septic shock.
The most salient attribute of shock is that all patients have a low tension. The tension is,
generally speaking, a function of two variables: (a) cardiac output, and (b) the systemic
vascular resistance. From this perspective there are two main types of shock: (a) shock due to
low cardiac output, and (b) shock resulting from low resistance. Examples of the first type
are: (a) the hypovolemic shock, and (b) cardiogenic shock, resulting from infarction or
disturbances of the rhythm. In case of an infarction or disturbances of the rhythm there is a
loss of blood, dehydration or emboly of the lung. The critical attributes of the first main type
of shock are: (a) a low cardiac output, and (b) a good microcirculation. An example of the
second main type of shock is septic shock (included anaphylactic shock and neurogenic
shock). In case of a septic shock (at least in the early stage, the so-called warm stage) the low
vascular resistance as well as the shunting are salient, resulting in an inefficient delivery of
oxygen. In case of septic shock one has to distinguish between: (a) the early septic shock, and
(b) the late septic shock. In the first case the attributes are: (a) low vascular resistance, (b) low
efficiency of the micro circulation, (c) an increased need of oxygen in the tissues, (d) if the
patient is filled well, then the cardiac output is increased; this compensates for the decreased
efficiency of the micro circulation, (e) an increased use of oxygen, and (f) no acidosis. In the
late stage (referred to as the cold stage or the irreversible stage) the vascular resistance is low,
the need for oxygen in the tissue is high, the cardiac output is low, the use of oxygen is high
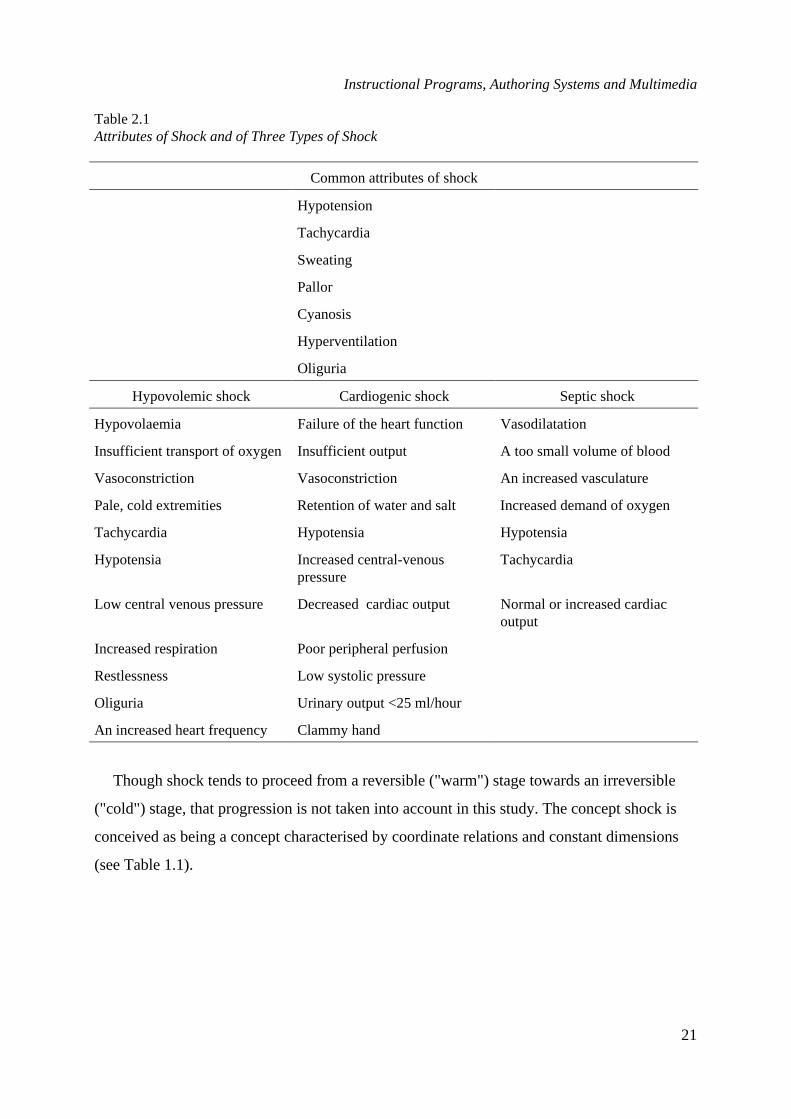
and the acidosis is high. The attributes of the three main types of shock are displayed in Table
2.1.
Instructional Programs, Authoring Systems and Multimedia
21
Table 2.1Attributes of Shock and of Three Types of Shock
Common attributes of shock
Hypotension
Tachycardia
Sweating
Pallor
Cyanosis
Hyperventilation
Oliguria
Hypovolemic shock Cardiogenic shock Septic shock
Hypovolaemia Failure of the heart function Vasodilatation
Insufficient transport of oxygen Insufficient output A too small volume of blood
Vasoconstriction Vasoconstriction An increased vasculature
Pale, cold extremities Retention of water and salt Increased demand of oxygen
Tachycardia Hypotensia Hypotensia
Hypotensia Increased central-venouspressure
Tachycardia
Low central venous pressure Decreased cardiac output Normal or increased cardiacoutput
Increased respiration Poor peripheral perfusion
Restlessness Low systolic pressure
Oliguria Urinary output <25 ml/hour
An increased heart frequency Clammy hand
Though shock tends to proceed from a reversible ("warm") stage towards an irreversible
("cold") stage, that progression is not taken into account in this study. The concept shock is
conceived as being a concept characterised by coordinate relations and constant dimensions
(see Table 1.1).
Chapter 2
22
2.3 Instructional programs
2.3.1 General design of the instructional programs
For the three experiments that will be described in detail in the next chapters three different
instructional programs were developed. Each instructional program contained both a textual
part and a number of cases (on video) that had to be categorised in one of the three coordinate
concept classes (a) hypovolemic shock, (b) cardiogenic shock and (c) septic shock. The
instructive programs are to a certain degree based on Tennyson and Cocchiarella's
prescriptions: (a) label and definition, (b) typical examples, (c) expository examples, (d)
interrogative examples, and (e) attribute elaboration (1986). The general learning goal was
solving categorisation problems.
2.3.2 The first program
For the first experiment (see Chapter 3) the program content consisted of three parts. Each of
these parts contained interrogative presentations (an interrogative presentation is a display
which presents information and solicits an overt response from the student about this
information) as well as expository presentations (an expository presentation is a display which
presents information but does not solicit an overt response from the student; mostly an
expository definition is included, i.e. a display which presents the concept label and concept
definition to the student).
The first part.The first part consisted of three expository texts about the definition of
shock. Each of these texts were followed by the presentation of a video of a typical example
in the one condition, while in the other condition a list of attributes was presented. In the first
part the instructional procedures comprised expository text, different types of questions and
feedback. In the text-only as well as in the text + video condition the instruction began with
an expository text about the generic concept of shock. This exposition was followed by one
open essay question and one multiple choice question. After feedback a videotaped, typical
case of shock was presented in the text + video condition. This information was mediated
verbally in the text-only condition. This cycle of expository text about the generic aspects of
shock, inquisitory parts and presentation (verbally or visually) of a typical case of shock was
varied twice.
Instructional Programs, Authoring Systems and Multimedia
23
The second part.The second part consisted of three expository texts about the underlying
causes and the effects of shock. Each exposition was followed by one open essay question and
one multiple-choice question.
The third part.The third part contained expository texts about different types of shock
(hypovolemic shock, cardiogenic shock, neurogenic shock, septic shock). After each
exposition interrogation followed. In the text + video condition typical cases of hypovolemic
shock, cardiogenic shock, neurogenic shock and septic shock were presented visually. The
information, contained in these typical cases, was presented verbally in the text-only
condition. During the whole instruction, after each text, two multiple-choice questions and
two open essay questions were presented to the student. The total number of questions were
twenty two.
2.3.3 The second program
For the second experiment (see Chapter four) the content of the instructional program
consisted of twenty four interrogatory examples of shock, three expository presented typical
examples of hypovolemic, cardiogenic and septic shock, and four cases of other diseases.
When an expository example is involved the example of a concept is presented and the
subjects know which concept is addressed. If an interrogatory example is involved the
example of a concept is presented and the task of the subjects is to classify this example
correctly. The function of an expository example is the presentation of all relevant attributes
in order to classify an example correctly. This implies that the most frequently occurring
symptoms of shock are presented. The function of an interrogative example is to provide an
opportunity to the students to classify an example. The subjects are encouraged to achieve this
by presenting questions about the attribute structure, the values of different attributes and so
on. If a presentation of an expository example is involved then the announcer states that a
typical example of a certain type of shock will follow. Initially the students are presented all
patient information linearly. Thereafter they get the opportunity to see the video images
repeatedly. If an interrogative example is involved the students are informed that they have to
provide a diagnosis. The students are encouraged to pay attention to the defining symptoms.
After this introduction only the patient information is presented linearly. After this
presentation the students get the opportunity to repeat parts of the presentation and to respond
to questions about symptoms. In that way the process of diagnostic reasoning is being

Chapter 2
24
maintained. After having responded to a question the students are presented informative
feedback about the quality of the response. Within and between examples, there is no fixed
sequence.
The patient information contains, except a presentation of video images, personal data, his
or her disease history and monitor data. In Table 2.2 these types of information are specified.
Table 2.2Overview of the Patient's Information
Personal data NameGenderAgeProfessional activitiesFamily circumstances
Anamnesis Disease historyNature of earlier diseasesCurrent complaints
Visual presentation FaceBellyHandFoot
Monitor Heart frequencyBlood pressureArterial-pulmonic pressureCentral-nervous pressureCardiac output
The visual material consisted of simulated patients, i.e. actors who are specialised in
imitating victims. Except expository and interrogative examples in this experiment attention
was given to marking. In the program two different screen designs were used (See Figure 2.1
and Figure 2.2).
The first screen was used to show an expository example of a shock patient. An
explanation was given what the symptoms are and what type of shock was involved. The
screen was divided in different parts; in one of these parts a set of buttons was presented. By
clicking with the mouse on one of these buttons the concomitant data was activated. The
visual materials were presented at the presentation screen. Simultaneously the announcer (a
physician) explained which symptoms the patient exhibited. These symptoms were displayed
right of the presentation screen. Using the presentation buttons a certain piece of the video
could be repeated. Two program buttons were used. The upper one was the video-button.
Instructional Programs, Authoring Systems and Multimedia
25
Using that button enabled the presentation of a visual. The lowest button was the
Stop/Proceed Button the use of which enabled to proceed from one part or button to the other.
This button was also used to proceed to the second screen.
Figure 2.1. The first screen, used in the second experiment.
The second screen was used for interrogative examples. When the students themselves
tried to determine what disease a patient had, this screen was used. This part of the instruction
also used a set of buttons. The presentation buttons were divided into three subsets. There
were buttons, which enabled the retrieval of (a) text, (b) visuals, and (c) monitor data. In order
to retrieve text three buttons were designed (P, A1, A2). These are the buttons representing
personal data, the history of the disease, and current complaints. By the use of one of these
three buttons the relevant data were accessed. These data was presented in the presentation
screen. Except from the inspection of these data, it was also possible to retrieve visuals
concerning certain tracts of the patient’s body. For that purpose seven buttons were
developed. By using such a button the students were presented one or more questions. On the
button the students could notice what part of the body was studied in the question. The
students could select the total patient, face, belly, hand or foot. Three chances were presented
Chapter 2
26
to respond correctly. After the first trial the feedback pointed to the fact whether the response
was correct, partially correct or incorrect.
Figure 2.2. The second screen, used in the second experiment.
The feedback after the second trial contained a hint. When the response after the third trial
was (partially) incorrect, then the correct answer was presented.
Also monitor data could be retrieved. For that purpose two buttons were reserved. The first
one contained heart frequency data, the blood pressure, the arterial pulmonic pressure and the
central venous pressure. The second one contained the cardiac output. In case of the
presentation of the monitor data questions were posed on what was displayed. The feedback
structure was identical to that which was used when visual data were studied. When the
students used the diagnosis button they were asked to infer the diagnosis and type the
categorisation. When the categorisation was incorrect, there were two possibilities: (a) when
not all data concerning a patient had been collected, i.e. when not all presentation buttons had
been applied, the number of trials to provide the diagnosis correctly, was unlimited. The
feedback contained an advice, which information was supposed to be still relevant in order to
provide a diagnosis; (b) when all data about a patient had been collected, i.e. when all
presentation buttons had been used, the students were presented three chances to provide a
Instructional Programs, Authoring Systems and Multimedia
27
correct diagnosis. When the diagnosis after the third trial was still incorrect, the correct
diagnosis was displayed on the screen.
In the presentation screen information was presented which was retrievable by the use of
the buttons. When the students asked for visual- or monitor information one or more questions
about the data were posed. These questions and the answers to those questions were presented
in a separate segment of the screen. The same procedure applied for the construction of a
diagnosis. With the use of the presentation buttons the student could ask for content
information. The program buttons had a navigational function. With the help button
information concerning the instructional program could be retrieved. By the use of a
presentation button for visuals the students were presented a question. When they wanted to
see the visual twice prior to responding to the question, then the video-button had to be used.
After having responded to a question or after having provided a diagnosis the students had to
close with the stop/proceed button. In this way the students could proceed through the
program.
The instructional program started with a general, verbally presented introduction. After the
students had their name and the identification number (ID) inserted, they got textual
information on the learning objectives of the program. After having completed that part the
program proceeded in two different ways, dependent on the condition to which the students
had been assigned; the condition was included in the ID-number. The instructional program
for subjects taking part of the two mixed expository/interrogatory conditions contained the
presentation of a shock patient where visually as well as textually an explanation about the
symptoms and the type of shock involved was provided (an expository presented typical
example). After that during forty minutes a set of shock patients was presented, where
students had to provide the diagnosis (interrogatory examples). This cycle was repeated
several times until each type of shock had been studied extensively. Also non-examples were
included in the program. These non-examples (collapse, hypoglycaemic coma,
hyperglycaemic coma and hyperventilation) were interwoven with the examples of shock. The
subjects from interrogative conditions got only interrogative examples. Of each patient first
the visual material was presented. Successively images of the total patient, the face, the belly,
the hand, the foot could be studied. When this search had been completed, there were three
options: (a) the collection of more data (verbal data or monitor data); (b) a repeated inspection
of certain parts of the body (visuals); (c) to provide a diagnosis using the relevant button.
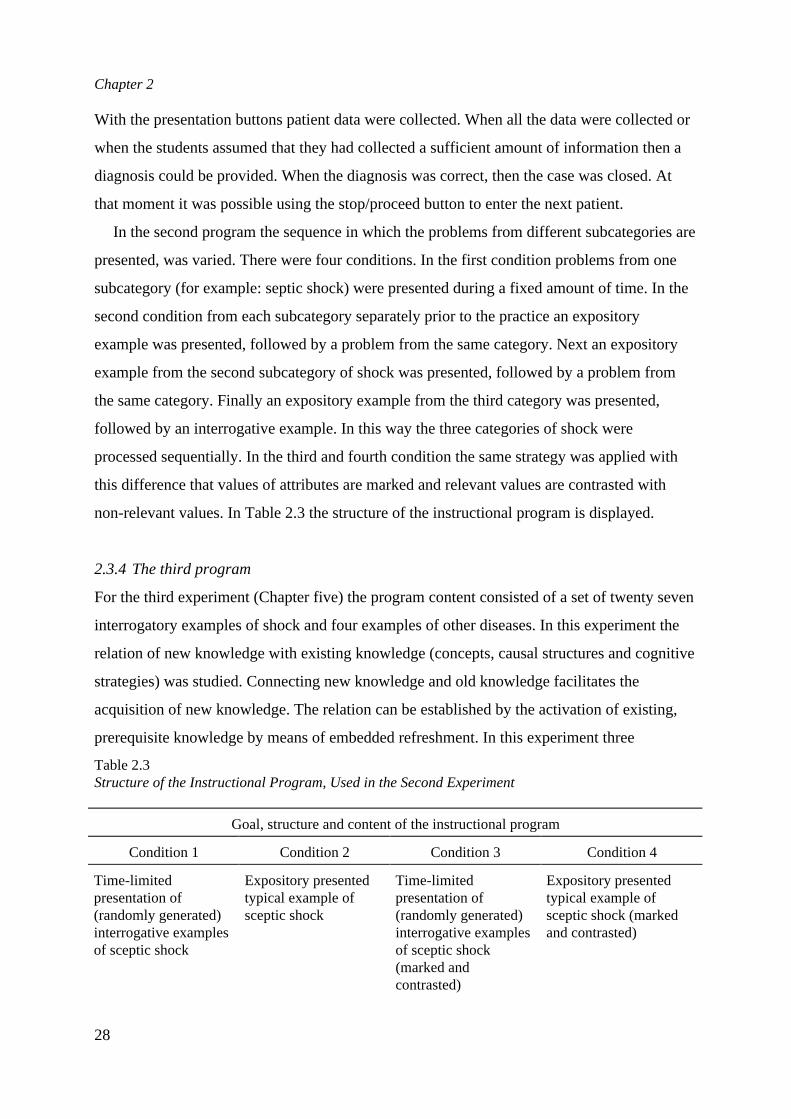
Chapter 2
28
With the presentation buttons patient data were collected. When all the data were collected or
when the students assumed that they had collected a sufficient amount of information then a
diagnosis could be provided. When the diagnosis was correct, then the case was closed. At
that moment it was possible using the stop/proceed button to enter the next patient.
In the second program the sequence in which the problems from different subcategories are
presented, was varied. There were four conditions. In the first condition problems from one
subcategory (for example: septic shock) were presented during a fixed amount of time. In the
second condition from each subcategory separately prior to the practice an expository
example was presented, followed by a problem from the same category. Next an expository
example from the second subcategory of shock was presented, followed by a problem from
the same category. Finally an expository example from the third category was presented,
followed by an interrogative example. In this way the three categories of shock were
processed sequentially. In the third and fourth condition the same strategy was applied with
this difference that values of attributes are marked and relevant values are contrasted with
non-relevant values. In Table 2.3 the structure of the instructional program is displayed.
2.3.4 The third program
For the third experiment (Chapter five) the program content consisted of a set of twenty seven
interrogatory examples of shock and four examples of other diseases. In this experiment the
relation of new knowledge with existing knowledge (concepts, causal structures and cognitive
strategies) was studied. Connecting new knowledge and old knowledge facilitates the
acquisition of new knowledge. The relation can be established by the activation of existing,
prerequisite knowledge by means of embedded refreshment. In this experiment three
Table 2.3Structure of the Instructional Program, Used in the Second Experiment
Goal, structure and content of the instructional program
Condition 1 Condition 2 Condition 3 Condition 4
Time-limitedpresentation of(randomly generated)interrogative examplesof sceptic shock
Expository presentedtypical example ofsceptic shock
Time-limitedpresentation of(randomly generated)interrogative examplesof sceptic shock(marked andcontrasted)
Expository presentedtypical example ofsceptic shock (markedand contrasted)

Instructional Programs, Authoring Systems and Multimedia
29
Randomly generatedinterrogative examplesof sceptic shock (withfeedback)
Randomly generatedinterrogative examples ofsceptic shock (withfeedback; marked andcontrasted)
Time-limitedpresentation of(randomly generated)interrogative examplesof cardiogenic shock
Expository presentedtypical example ofcardiogenic shock
Time-limitedpresentation of(randomly generated)interrogative examplesof cardiogenic shock(marked andcontrasted)
Expository presentedtypical example ofcardiogenic shock(marked and contrasted)
Randomly generatedinterrogative examplesof cardiogenic shock(with feedback)
Randomly generatedinterrogative examples ofcardiogenic shock (withfeedback; marked andcontrasted)
Time-limitedpresentation of(randomly generated)interrogative examplesof hypovolemic shock
Expository presentedtypical example ofhypovolemic shock
Time-limitedpresentation of(randomly generated)interrogative examplesof hypovolemic shock(marked andcontrasted)
Expository presentedtypical example ofhypovolemic shock(marked and contrasted)
Randomly generatedinterrogative examplesof hypovolemic shock(with feedback)
Randomly generatedinterrogative examples ofhypovolemic shock (withfeedback; marked andcontrasted)
Transfer-test
instructional strategies for activating prerequisite knowledge were used. In the first condition
the prerequisite knowledge base was presented prior to the learning of problem solving. In the
second condition the prerequisite content was presented during the learning process. In the
third condition the prerequisite knowledge base was presented after categorisation errors.
Table 2.4Structure of the Instructional Program, Used in the Third Experiment
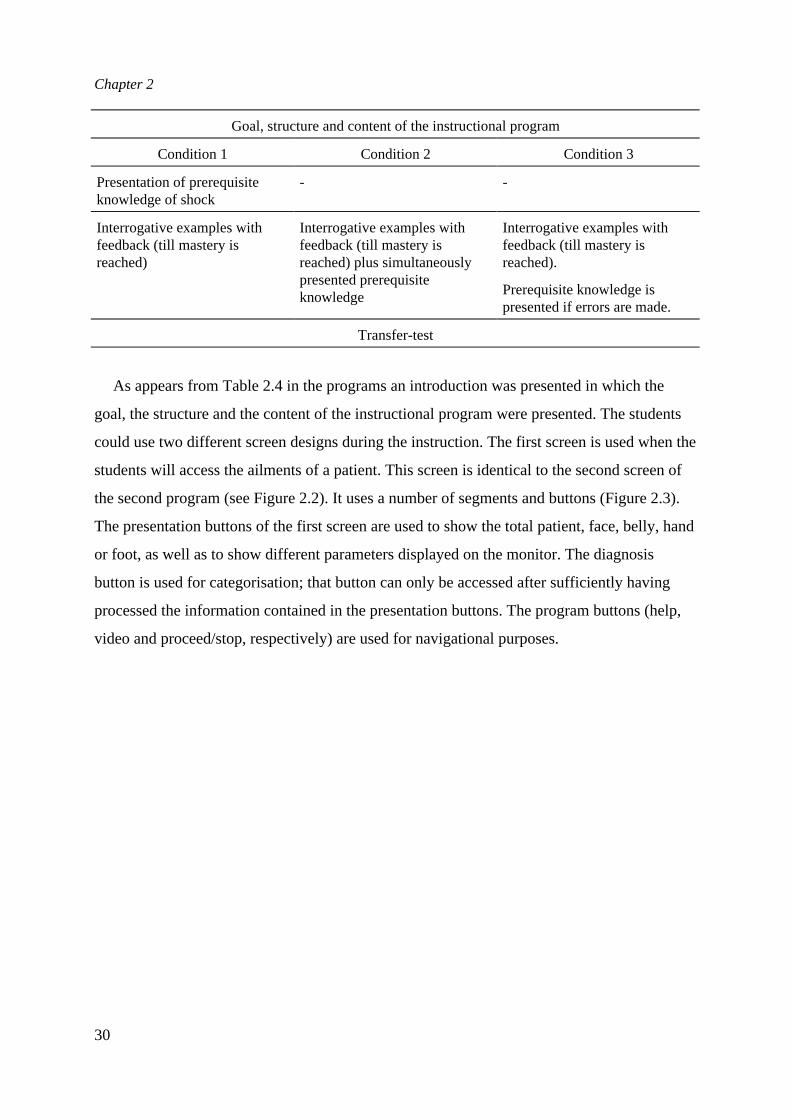
Chapter 2
30
Goal, structure and content of the instructional program
Condition 1 Condition 2 Condition 3
Presentation of prerequisiteknowledge of shock
- -
Interrogative examples withfeedback (till mastery isreached)
Interrogative examples withfeedback (till mastery isreached) plus simultaneouslypresented prerequisiteknowledge
Interrogative examples withfeedback (till mastery isreached).
Prerequisite knowledge ispresented if errors are made.
Transfer-test
As appears from Table 2.4 in the programs an introduction was presented in which the
goal, the structure and the content of the instructional program were presented. The students
could use two different screen designs during the instruction. The first screen is used when the
students will access the ailments of a patient. This screen is identical to the second screen of
the second program (see Figure 2.2). It uses a number of segments and buttons (Figure 2.3).
The presentation buttons of the first screen are used to show the total patient, face, belly, hand
or foot, as well as to show different parameters displayed on the monitor. The diagnosis
button is used for categorisation; that button can only be accessed after sufficiently having
processed the information contained in the presentation buttons. The program buttons (help,
video and proceed/stop, respectively) are used for navigational purposes.
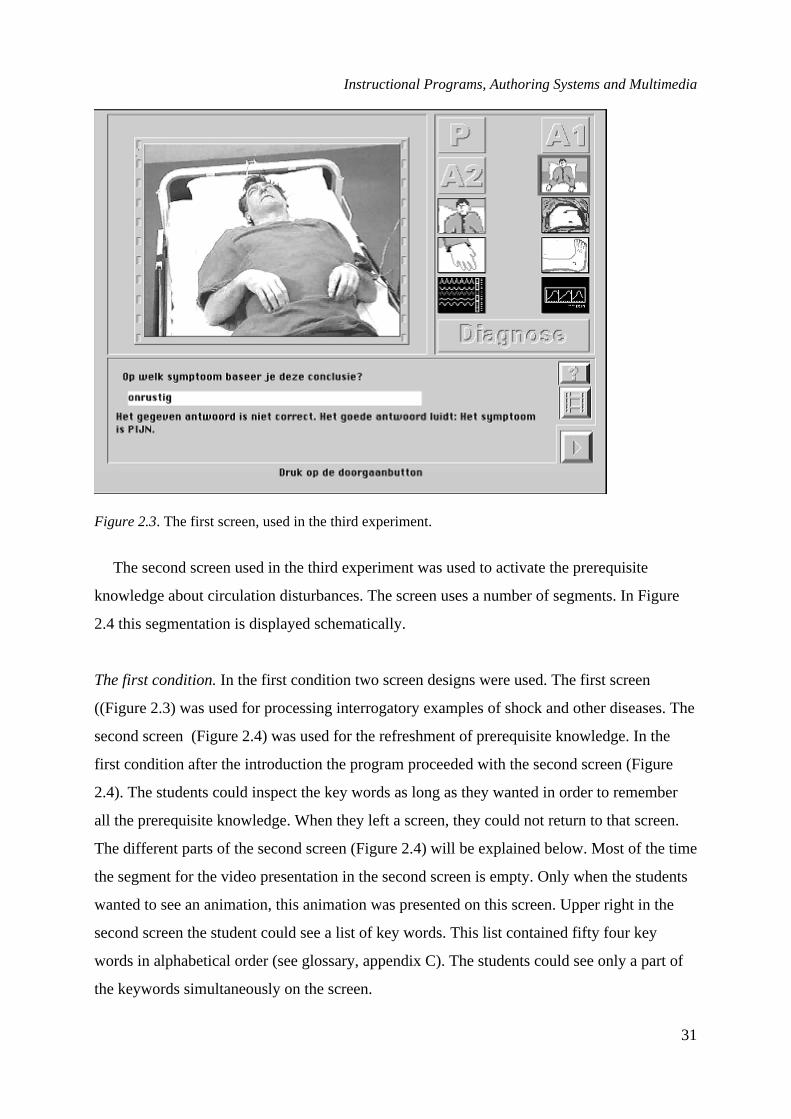
Instructional Programs, Authoring Systems and Multimedia
31
Figure 2.3. The first screen, used in the third experiment.
The second screen used in the third experiment was used to activate the prerequisite
knowledge about circulation disturbances. The screen uses a number of segments. In Figure
2.4 this segmentation is displayed schematically.
The first condition.In the first condition two screen designs were used. The first screen
((Figure 2.3) was used for processing interrogatory examples of shock and other diseases. The
second screen (Figure 2.4) was used for the refreshment of prerequisite knowledge. In the
first condition after the introduction the program proceeded with the second screen (Figure
2.4). The students could inspect the key words as long as they wanted in order to remember
all the prerequisite knowledge. When they left a screen, they could not return to that screen.
The different parts of the second screen (Figure 2.4) will be explained below. Most of the time
the segment for the video presentation in the second screen is empty. Only when the students
wanted to see an animation, this animation was presented on this screen. Upper right in the
second screen the student could see a list of key words. This list contained fifty four key
words in alphabetical order (see glossary, appendix C). The students could see only a part of
the keywords simultaneously on the screen.
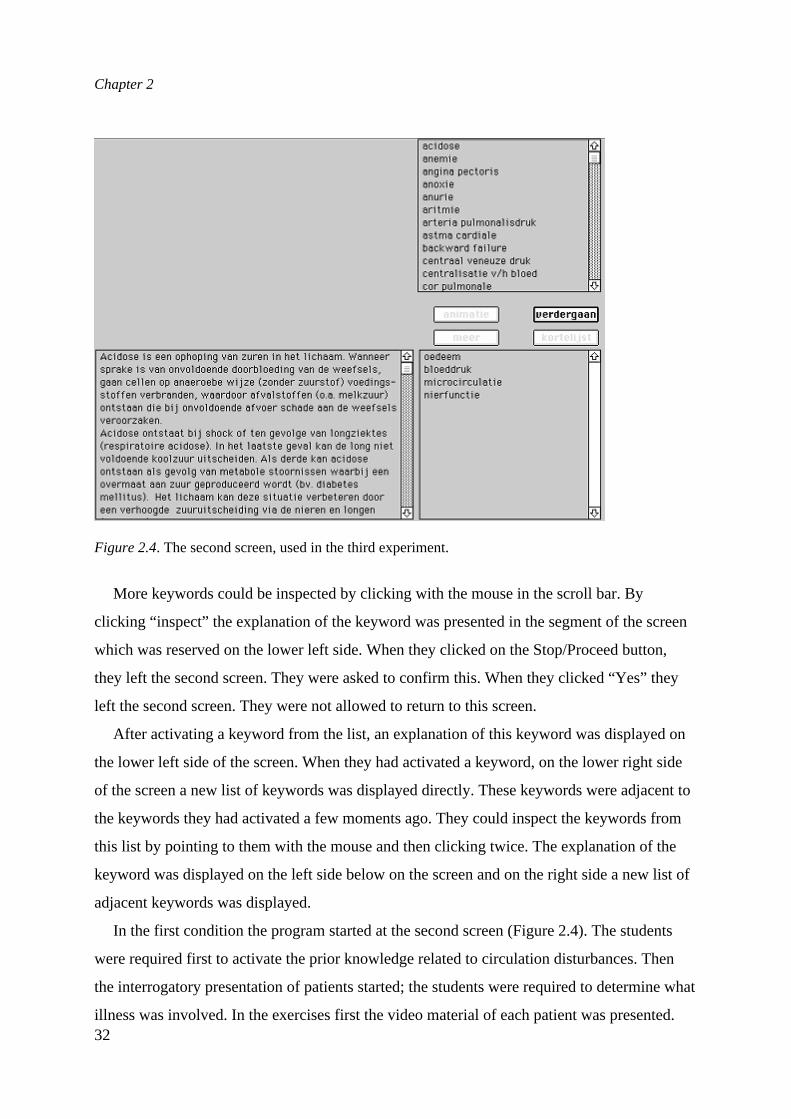
Chapter 2
32
Figure 2.4. The second screen, used in the third experiment.
More keywords could be inspected by clicking with the mouse in the scroll bar. By
clicking “inspect” the explanation of the keyword was presented in the segment of the screen
which was reserved on the lower left side. When they clicked on the Stop/Proceed button,
they left the second screen. They were asked to confirm this. When they clicked “Yes” they
left the second screen. They were not allowed to return to this screen.
After activating a keyword from the list, an explanation of this keyword was displayed on
the lower left side of the screen. When they had activated a keyword, on the lower right side
of the screen a new list of keywords was displayed directly. These keywords were adjacent to
the keywords they had activated a few moments ago. They could inspect the keywords from
this list by pointing to them with the mouse and then clicking twice. The explanation of the
keyword was displayed on the left side below on the screen and on the right side a new list of
adjacent keywords was displayed.
In the first condition the program started at the second screen (Figure 2.4). The students
were required first to activate the prior knowledge related to circulation disturbances. Then
the interrogatory presentation of patients started; the students were required to determine what
illness was involved. In the exercises first the video material of each patient was presented.

Instructional Programs, Authoring Systems and Multimedia
33
The students got visual material pertaining to the total patient, the face, the abdomen, the hand
and the foot. After having completed this, the students clicked on the “Stop/Proceed” button
in order to proceed. They had three options: (a) to collect more details; (b) to inspect once
more some parts of the patient’s body (visuals); and (c) to provide a diagnosis using the
diagnosis-button. They collected data about the patient using the presentation button. When
they had collected all data or when they assumed to have collected sufficient data, then they
could provide a diagnosis using the diagnosis button. When the correct diagnosis had been
provided, then the exercise was closed and the students could proceed to the next patient using
the “Stop/Proceed” button. The students were encouraged to proceed in their own speed, to
allocate sufficient time to each patient and to try to provide a diagnosis of as much patients as
they could. The total program lasted two hours.
The knowledge base of prerequisite concepts and principles (see glossary in Appendix C)
contained a set of fifty four keywords. These keywords were explained as succinctly as
possible. Relations between keywords were established. Each keyword referred to adjacent
ones. All keywords were associated with questions.
The interaction between students and computer was facilitated by a help-button and a short
user-manual (Appendix F). A functional segmentation of the screen-space was developed. For
that reason each of the functions as questioning, exposition and control of the computer were
localised in a separate part of the screen. The screen consisted of four parts. These four parts
are shown in Figure 2.5.
In the first part (upper left) the video-images were presented. In the second part (upper
right) the icons for controlling the videodisc were provided, while in the third part (lower left)
questions and feedback were presented. Finally in the fourth part (lower right) the icons for
help and proceeding the program were contained. In the first condition scrolling through the
list of keywords was possible. If the students wanted to inspect a keyword they had to point to
this keyword with the mouse and then an exposition of the meaning of that keyword was
presented. The text of the keyword was presented in the lower left part of the screen. When
the text was too long, scrolling was possible. Each keyword referred to adjacent keywords.
Adjacent keywords are superordinate, subordinate and possibly relevant coordinate keywords.
These adjacent keywords were presented in segment four of the screen design. If the students
wanted to inspect one or more of these keywords, they could be activated from the fourth part

Chapter 2
34
of the screen. When the icon “stop” was activated in the third screen this action had to be
confirmed. After that confirmation the presentation of interrogatory examples proceeded.
Figure 2.5. Segmentation of the screen, used in experiment 3.
The second condition. In the second condition the prerequisite knowledge (see glossary in
Appendix C) was presented parallel to the instruction. In order to achieve this the students got
the opportunity to activate the base of prerequisite knowledge at each moment. For that
purpose in the lower right segment of the screen design (Figure 2.5) an extra button “K”
(Knowledge) was presented. In the Help-menu as well as in the user manual the functioning
of K was explained. By pointing to K in the upper right segment of the screen an alphabetical
ordered list of fifty four keywords was presented in the same way as in the first condition. By
pointing to a keyword the exposition of the keyword was presented in the lower left segment,
across the current text of a question. A list of adjacent keywords was presented in the lower
right segment, similar as in the first condition.
Pointing to the icon “Stop” did not require a confirmation, but enabled to return to the
screen as it was when “K” was activated. The confirmation question was omitted because the
students in case of a misunderstanding could always return to the knowledge base of
prerequisite knowledge. During the presentation of the knowledge base of prerequisite
Instructional Programs, Authoring Systems and Multimedia
35
knowledge the video image, that was presented at the moment of activation of the “K”-button,
stayed apparent in the first segment of the screen. If computer animations were presented in
the first segment then temporarily the video image of the current patient could not be
perceived. By showing simultaneously the patient a parallel presentation of prerequisite
knowledge was enabled.
The third condition.In the third condition the prerequisite knowledge was presented when the
students responded incorrectly. When an answer was incorrect, feedback was presented
according to the format “You have responded incorrectly, please check your mastery of
prerequisite knowledge”. Successively the list of keywords, belonging to the question, was
presented in the upper right segment (Figure 2.5) of the screen design. The keywords from
this list could be activated. When a keyword was consulted, the concomitant text was
presented in the third segment and in the fourth segment a list of adjacent keywords was
presented. Due to a desirable correspondence between keyword lists the possibility existed
that the students wanted to consult a keyword that was not contained in the list. Therefore in
the second segment of the screen design, adjacent to a button “Stop”, a button “More” was
designed. When this button was activated, the alphabetical list of fifty four keywords was
presented. This list contained, compared with the second condition, an extra button “Short
list”. When this button was activated, the students returned to the short list of specific
keywords. When the button “Stop” was activated a confirmation was required and the
students returned to the instructional program. The question was presented again. When the
response to the same question was incorrect again, common feedback was presented without
the list containing prerequisite knowledge.
2.3.5 Program scores
In the first experiment during the instruction after each expository text two multiple-choice
questions and two open questions were presented. The total number of questions was twenty
two. In the second and the third experiment each interrogative example (total number: twenty
seven) contained a set of seven questions (each containing sub-questions) about the patients
attributes as well as one question about the patients diagnosis. Further data about time,
number of examples, number of correct and incorrect responses and confidence were
collected.

Chapter 2
36
2.4 Tests
2.4.1 The first experiment
Retention test.After having completed the instruction a retention test (seventeen items) was
administered. The test consisted of two parts. The first part of the test contained twelve
questions about the definition of shock and about the defining attributes of the three types of
shock. The second part of the test consisted of five questions, each of which contained a set of
relevant and irrelevant attributes. The student had to decide whether an example of shock was
involved.
Transfer test.After three weeks a transfer test was administered. This test consisted of three
parts. In the first part the student had to decide for ten patients whether shock was involved. In
the second part the student had to state the five most salient attributes of the type of shock
involved. If there was no shock involved, the student had to attach a label to the disorder. In
the third part the student had to decide which type of shock was involved, to list the most
salient attributes, and, thirdly, to identify the similarity between two cases of shock.
2.4.2 The second and third experiment
Transfer test.The reliability (Cronbach'sα) of the transfer test, used for the second and third
experiment and administered after a period of three weeks, was .34. This relative low
reliability may be attributed to the heterogeneous nature of the test. It is difficult to develop
such a test because it depends on videoing patients. Further the non-predictability of a certain
type of shock and the willingness of patients to participate play a role in developing the test.
The transfer test contained nineteen video-presented patients who had to be classified in terms
of (a) name of the disease, (b) critical symptoms and (c) the contribution of each symptom to
the diagnostic process (see list in appendix B). Students had to specify how confident they
were about the patient's illness. They had to specify the symptoms based on terms of which
they arrived at a diagnosis.
Instructional Programs, Authoring Systems and Multimedia
37
2.5 Apparatus
2.5.1 The first experiment
The video was displayed on a separate monitor by a Philips Laser Vision Videodisc. The
instructional program for the first experiment (Chapter three) was provided by a network of
Tulip-Compact computers.
2.5.2 The second and third experiment
The instructional program for the second and the third experiment (Chapters four and five)
was implemented using two systems, MacII and MacCX. Both contained the 'Videologic
DVA-4000 full motion'. The MacII was connected with a Philips Laservision Disc Drive VP
406, while the MacCX was connected with a CLD-423000 LD Player. The videodisc
contained thirty six minutes of information, as well as a video trace and two sound traces.
This implies that the disc can contain thirty six minutes stereo sound as well as seventy two
minutes mono sound. The two sound traces can be used independently and consequently for
different purposes. One second of the videodisc comprises twenty five frames. Each frame is
identical to one rotation of the videodisc, thus a still can be created by repeating this frame
continuously. A videodisc can contain, in stead of thirty six minutes of dynamic video
material, 54000 (5 x 60 x 36) stills maximally. It is possible to retain an image in the memory
of the computer while the videodisc proceeds. In this way it is possible to display a still on the
screen while the video disc player present the sound. The search time is only a few seconds if
AuthorWare is used.
In order to develop the programs for the second and third experiment AuthorWare
Professional was used, which is appropriate for the Apple Macintosh. Using AuthorWare
implies a graphical way of programming by localising different icons on a line sequentially.
When an icon is placed in the program this icon can be filled in a simple way. There are
special icons for steering a video and the audio. In order to combine video and computer
graphics AuthorWare uses a Digital Video Adaptor (DVA-4000). This Video Logic digitalises
the analogue signal of the video disc player during playing.
Chapter 2
38
2.6 Authoring and learning environment
2.6.1 The first experiment
TAIGA was used for computer-supported instruction, while video was used for the
presentation of patients. The time limit of the program was 1.30 hrs. Videotaped displays of
typical examples of shock were provided separately on the video screen.
Interactive video is a video program in which the sequence and the selection of the content
depends on the responses of the user to the content. There are different levels of interaction.
At one level the video is not controlled by a computer. This type was used in the first
experiment. The cases are presented linearly, while the students can use a stop-function to
select episodes themselves. The interactivity is similar to that of a compact-disc player. At a
second level the (second) sound channel contains elementary software instructions. At the
third level the videodisc is controlled by a computer. The users are no longer constrained by a
numerical keyboard, but they can respond to open questions. This level combines the strength
and the flexibility of a computer with the quality, the "realism" and the attractiveness of a
video.
2.6.2 The second and third experiment
In the interactive video, as used for the second and third experiment, the interaction took place
at the third level. The combination of video and computer at this level provides the
opportunity of different types of integration. The computer can be used as a pathfinder. In that
case the computer looks for the relevant episodes on the disc. The video provides the main
parts of the instruction. It is also possible to assign the instruction to video as well as to the
computer. Some parts can be taught more easily by the computer and other parts by the video.
Another possibility is where the computer is dominant. The disc is used as an external
apparatus, which provides necessary images at different moments. This mode is especially
appropriate when the instruction attends to specific video material and when the presentation
does not need to be handled by the video. The video program about shock is situated between
the last two possibilities. The instruction is mainly handled by the computer part of the
program where at certain moments examples of the concept are used from the disc. The
instruction attends especially to the visual material, which is provided. On the other part some
instruction is provided by the video part.
Instructional Programs, Authoring Systems and Multimedia
39
Based on the design a user interface had to be developed. It was assumed that it would be
appropriate that students could use the mouse as much as possible. The program had to be
user friendly as much as possible in that the users should know at each moment what they
were expected to do. In order to keep the procedures as simple as possible buttons were used.
By pointing to buttons the user can give a specific assignment to the program. Each button has
a specific function. In the context of the program shock the following buttons are of
importance: (a) proceed to a next program element, (b) jump back in text or video, (c) pause
during video, (d) stop the program, (e) activation of the knowledge base (in experiment three),
and (f) activation of help information.
In order to make the program attractive and varied an auditive presentation of the guidance
was designed to alternate with the textual information. Marking and contrasting were used in
the second experiment (third and fourth condition). The first term denotes the saliency of
some single attribute to guide the student's attention. The second term refers to the saliency of
the difference between values of attributes of a category.
The screen design comprised the following functions: presentation video, text, buttons,
presentation of questions, responses of the student and feedback. When information is
displayed consistently on one single place at the screen then transfer is supposed to be
facilitated. When an element is not used the space has to be reserved in order to maintain the
standard structure. On the screen space was reserved for the buttons on the right side. They
were vertically ordered and for their function icons were designed. The denotation of these
icons is explained prior to entering the program.
The colour green was selected for the instructional programs, used for the second and third
experiment because this colour can be varied easily. As character type "Chicago" was
selected because this type of characters is adequate and available on the Apple Macintosh.
The presentation buttons, used in the instructional programs for the second and third
experiment, can be divided in three subsets. There are buttons to access (a) text, (b) images
and (c) monitor data. The buttons can be activated in a random sequence.

Chapter 2
40
Figure 2.6. Button structure, used in the second and third experiment.
In order to access text three buttons were constructed. These are the buttons for personal
data), for anamnestic data concerning history of the disease and for the current complaints;
these buttons are contained in the upper part of Figure 2.6. By activating one of these buttons
with the mouse, the information will be accessed; the information was presented in the
presentation screen. It was possible to inspect some parts of the patient’s body. For that
purpose a number of buttons was constructed (see Figure 2.7). By clicking such a button the
students activated a part of the video. At the button they could see an icon; this icon referred
to that part of the body which will be presented in the video. They could choose from: the
total patient, face, abdomen, hand or foot. They could see the video part by activating the
video button of the program buttons. After each video presentation one or more questions
were presented about what was displayed. The students got three chances (trials) to respond to
each question. When the answer was incorrect after the third trial, then the correct answer was
presented.

Instructional Programs, Authoring Systems and Multimedia
41
Figure 2.7. Buttons, related to the patient, face, abdomen, hand or foot, as used in the second andthird experiment.
Finally the students could access monitor data (in the programs as used for the second and
third experiment). For that purpose two buttons were reserved (see Figure 2.8). The first one
(left) contained data about heart frequency, blood pressure, the pulmonic arterial pressure and
the central-venous pressure. The second button (right) presented the cardiac output (the heart-
minute volume). These data were activated by clicking the relevant button. Related to the
monitor presentation as well as the video presentation questions were presented about what
was displayed. The students got three chances (trials) to respond to each question. When the
answer was incorrect after the third trial then the correct answer was presented.
Figure 2.8. Buttons related to monitor data, used in the second and third experiment.

Chapter 2
42
For the feedback on the students responses there were three possibilities: (a) when they did
not collect all data about the patient, i.e. that they did not use all presentation buttons, they got
the advice concerning the information they had to access; (b) when they had collected all data
about a patient, i.e. when they had accessed all presentation buttons, they would get three
chances (trials) to provide the correct diagnosis. When the diagnosis was correct after the third
trial, then the correct diagnosis was given. When they accessed video- or monitor information
one or more questions about the data involved were presented. These questions were
presented in a separate segment (Figure 2.5). The answers, which they provided, were
displayed in this segment too. The same applies for the feedback as well as providing a
diagnosis. Using the presentation buttons they could access relevant information.
Figure 2.9. The help button.
When the students clicked on the Help-button on the presentation screen the program was
explained. When the students accessed video material about a part of the patient’s body by
using a presentation button then a question was presented. They could see the concomitant
video part by clicking the video button (Figure 2.10). They could repeat this as frequently as
they wanted. Also if they had given an incorrect answer after the first trial, they could see the
video part twice.
Figure 2.10. The video button.
Instructional Programs, Authoring Systems and Multimedia
43
Figure 2.11. The stop/proceed button.
When the students had answered a question, or when they had provided a diagnosis, they
had to close with the Stop/Proceed button.
Reference
Tennyson, R. D., & Cocchiarella, M. J. (1986). An empirically based instructional design theory forteaching concepts.Review of Educational Research, 56, 1, 40-71.


3
INSTRUCTIONAL DESIGN FOR LEARNING TOCATEGORISE A DISEASE 1
One of the more recent cognitive theories concerning learning concepts, referredto as prototype theory, suggests that categorisation is enhanced by priorformation of a prototype, i.e. a typical instance of a category. This chapterdescribes an experiment in which the differential effects of prototype formation onthe classificatory behaviour are assessed. The experiment is orientated tocategorisation of a disease. This is a complex phenomenon as a result of the factthat the boundaries of most diseases are fuzzy. The instructional design guide forteaching concepts, as developed by Merrill and Tennyson (1977), underlies thisexperiment. It provides prescriptions for the learning of fuzzy concepts. Theobjective to be learned is the correct identification of different types of the conceptshock, i.e. a state of circulatory insufficiency in which cellular perfusion isinadequate for normal cellular function. Data provide evidence for the validity ofthe prototype paradigm and of the utility of the instructional design model ofMerrill and Tennyson.
1 This chapter was published earlier in Gulmans, J. (1991). Instructional Design for learning to categorise adisease.Educational and Training Technology International, 28, 3, 217-223.
Chapter 3
46
3.1 Introduction
Learning to provide a diagnosis is a form of concept learning. It involves the assignment of an
object to a category by using a concept. This operation is a complex phenomenon by the fact
that (a) in many cases the boundaries of the concept are fuzzy, (b) that most diseases
encompass subcategories and c) that practising classificatory behaviour is impossible because
patients with the relevant symptoms are not available. As such, to provide a diagnosis is the
process of determining the nature of an illness. The outcome of this process is the
categorisation of the diseased condition. The diagnostic skill involved refers to the careful
examination of the symptoms or features of the disease. Because a diagnosis implies the
categorisation of a disease learning to diagnose is conceived as concept learning. Thus, the
instruction for learning to provide a diagnosis will be based on an instructional design model
for the learning of concepts.
Elstein, Shulman and Sprafka (1978) assume that the diagnostic process is based on a
hypothetical-deductive strategy. This implies that on the basis of clues a list of potential
diagnoses is formulated and that these diagnoses are successively tested until the final
hypothesis. A diagnostic decision presupposes knowledge as to the causes, the symptoms and
the course of a disease. At the end of the process the diagnostician has to decide which disease
is the case. The diagnostic process has both deductive and inductive components. In the case
of a valid deduction an inference is made in which the conclusion results logically from the
premises. The reasoning process evolves from general to specific. In the case of an inductive
reasoning the inference is based on facts. The hypotheses evolve from experience, which
becomes the basis for testing the hypotheses. The reasoning process evolves from specific to
general. The deductive component of the diagnostic process results in hypotheses, which can
be refuted by experience. The inductive component is based on sources as background
knowledge and specific experience. The diagnostic process is a process of object
identification by checking whether a symptom or combination of symptoms can be identified.
A diagnosis presupposes the acquisition of concepts. A concept is a rule for classifying
objects in two (or more) subcategories representing exemplars of the concept (Hunt, 1962;
Hovland, 1952). In order to acquire diagnostic skills conceptual knowledge is needed which is
provided by instruction. The instruction for the learning of a concept is described by Merrill
and Tennyson (1977) and Tennyson and Cocchiarella (1986). Merrill and Tennyson suppose
that the learning of concepts consists of two phases. The first one is the formation of a
prototype and the second one is the acquisition of classificatory skills. From this assumption
Prototype Formation
47
an instructional design model for the learning of concepts has been developed. This model has
two basic components: content structure variables and instructional design variables. A
rational combination of these components results in the selection of one of the four basic
instructional design strategies. These strategies consist of manipulating the primary
instructional design variables: (a) definition, i.e. a rule or generality encompassing the
structure of the critical attributes, (b) expository instances, i.e. (non-)instances which organise
the content in propositional format, (c) interrogatory instances, i.e. (non-)instances which
organise the content in interrogatory format, and 9d) attribute elaboration, i.e. analysis of
critical attributes in expository instances and feedback as to critical attributes in interrogative
instances.
Although there is confirming evidence for the applicability of this model for learning
concepts (Ok-Choon Park & Tennyson, 1980; Tennyson & Seong Ik Park, 1984) the effect of
prototype formation on generalisation to new instances and discrimination of instances from
non-instances has been investigated hardly in the medical domain. In as far as it has been
investigated (Cantor & Smith, 1980) it was found that physicians are more confident
dependent on the representativeness of the attributes of a disease. Though there is not much
evidence for the applicability of the model in the medical domain, the model of Merrill and
Tennyson (1977) and Tennyson and Cocchiarella (1986) seems also in this domain promising
for mainly two reasons. In the first place this model is based on the prototype theory (Posner
& Keele, 1968; Rosch & Mervis, 1975). This approach is suitable for medical concepts
because medical concepts, especially diseases, vary in typicality. The most typical members
share the most attributes with other members of a category. In the second place the two basic
components of the model of Merrill and Tennyson (1977) and also the model of Tennyson
and Cocchiarella (1986) are generalisation to new instances and discrimination of instances
from non-instances. These components are central in the process of differential diagnosis of a
disease.
Concept learning is the process in which subjects learn to categorise objects, processes or
events. After attaining a concept, new, un-encountered objects, processes or events,
technically labelled instances, can be categorised. Different theories of concept learning exist.
The classical theory, as formulated by Bruner, Goodnow and Austin (1956), assumes that the
world consists of entities which have fixed attributes and fixed relations between those
entities comprised in each instance of a concept. Within the classical theory defining attributes
are those which are necessary for deciding whether an instance is an example of a category.
One of the modern theories of concept learning is the prototype theory (Rosch, 1975). Within
Chapter 3
48
this theory, category-membership is determined by the resemblance to the most typical case.
This prototype encompasses the most frequently encountered attributes of a category. Merrill
and Tennyson (1977) and Tennyson and Cocchiarella (1986) have developed an instructional
design model for concept learning, which is based on prototype theory. They assume that
concept learning encompasses deductive processes. These processes are based on
classification which consists of generalisation and discrimination. This design model needs
still further confirmation. The purpose of the experiment reported here is to verify the
hypothesis that decisions on class membership are facilitated if categorisation takes place as a
matching process between prototype and instance. Consistent with the assumptions of the
prototype theory it is expected that also in the medical domain, exemplified in this experiment
by the concept shock, a differential effect will be found as a result of prototype-based
instruction.
3.2 Method
3.2.1 Subjects
A group of 106 subjects participated in the experiment. These subjects were recruited from a
school for nursing education.
3.2.2 Material
An instructional program about the concept 'shock' was developed. Shock is defined as a
reduction of amount of blood in the organism. It is a state of circulatory insufficiency arising
from shortage of blood, sepsis, cardiac irregularities, anaphylactic reactions and neurogenic
causes. In the instructional program five types of shock are differentiated:
(a) Hypovolemic shock. This is one of the most common types of shock. A great amount of
blood loss is the usual precipitating factor of this type of shock. The symptoms are coolness of
the skin, restlessness, hypotension, oliguria and increased rate and depth of respiration. The
patient may be cold and clammy with obviously poor peripheral perfusion, but can also
present a warm and well-circulated skin.
(b) Cardiogenic shock. This occurs when the heart is unable to pump enough blood to meet
the body tissues need for oxygen. The most common precipitating factor of cardiogenic shock
is myocardial infarction. The symptoms of cardiogenic shock are absent or poor peripheral
pulses, cold or clammy skin, systolic blood pressure less than 85mm Hg and urinary output
less than 25 ml.
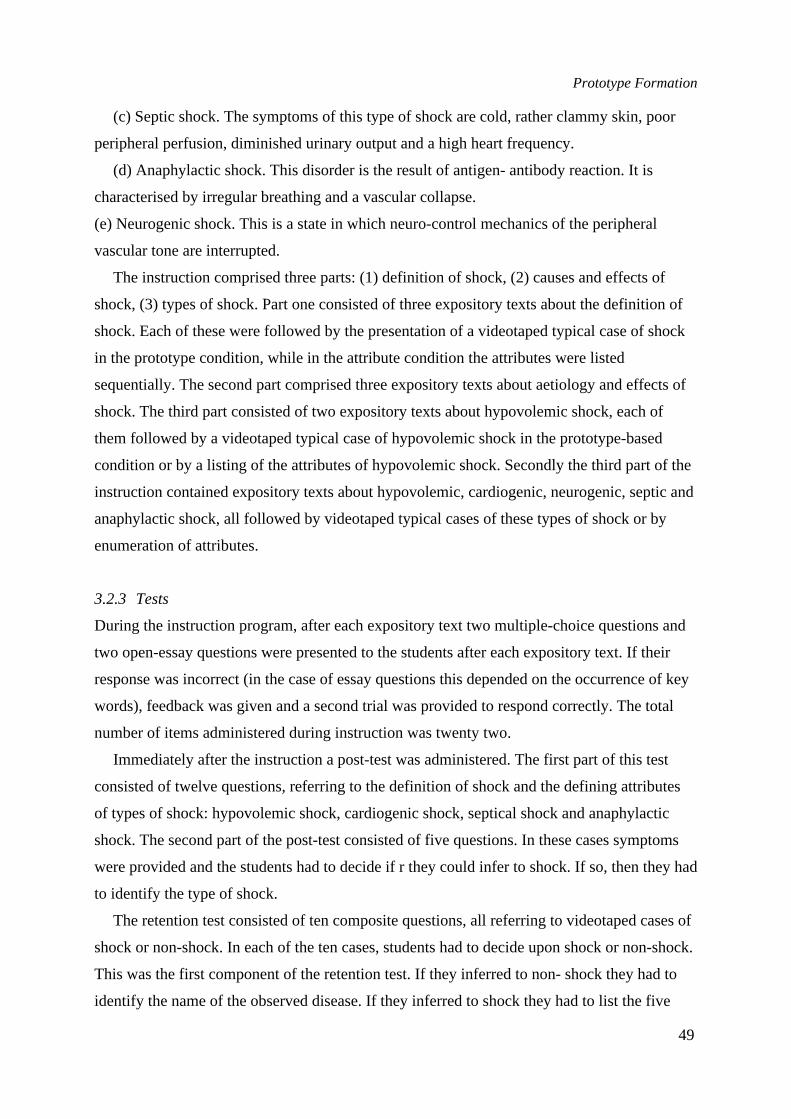
Prototype Formation
49
(c) Septic shock. The symptoms of this type of shock are cold, rather clammy skin, poor
peripheral perfusion, diminished urinary output and a high heart frequency.
(d) Anaphylactic shock. This disorder is the result of antigen- antibody reaction. It is
characterised by irregular breathing and a vascular collapse.
(e) Neurogenic shock. This is a state in which neuro-control mechanics of the peripheral
vascular tone are interrupted.
The instruction comprised three parts: (1) definition of shock, (2) causes and effects of
shock, (3) types of shock. Part one consisted of three expository texts about the definition of
shock. Each of these were followed by the presentation of a videotaped typical case of shock
in the prototype condition, while in the attribute condition the attributes were listed
sequentially. The second part comprised three expository texts about aetiology and effects of
shock. The third part consisted of two expository texts about hypovolemic shock, each of
them followed by a videotaped typical case of hypovolemic shock in the prototype-based
condition or by a listing of the attributes of hypovolemic shock. Secondly the third part of the
instruction contained expository texts about hypovolemic, cardiogenic, neurogenic, septic and
anaphylactic shock, all followed by videotaped typical cases of these types of shock or by
enumeration of attributes.
3.2.3 Tests
During the instruction program, after each expository text two multiple-choice questions and
two open-essay questions were presented to the students after each expository text. If their
response was incorrect (in the case of essay questions this depended on the occurrence of key
words), feedback was given and a second trial was provided to respond correctly. The total
number of items administered during instruction was twenty two.
Immediately after the instruction a post-test was administered. The first part of this test
consisted of twelve questions, referring to the definition of shock and the defining attributes
of types of shock: hypovolemic shock, cardiogenic shock, septical shock and anaphylactic
shock. The second part of the post-test consisted of five questions. In these cases symptoms
were provided and the students had to decide if r they could infer to shock. If so, then they had
to identify the type of shock.
The retention test consisted of ten composite questions, all referring to videotaped cases of
shock or non-shock. In each of the ten cases, students had to decide upon shock or non-shock.
This was the first component of the retention test. If they inferred to non- shock they had to
identify the name of the observed disease. If they inferred to shock they had to list the five
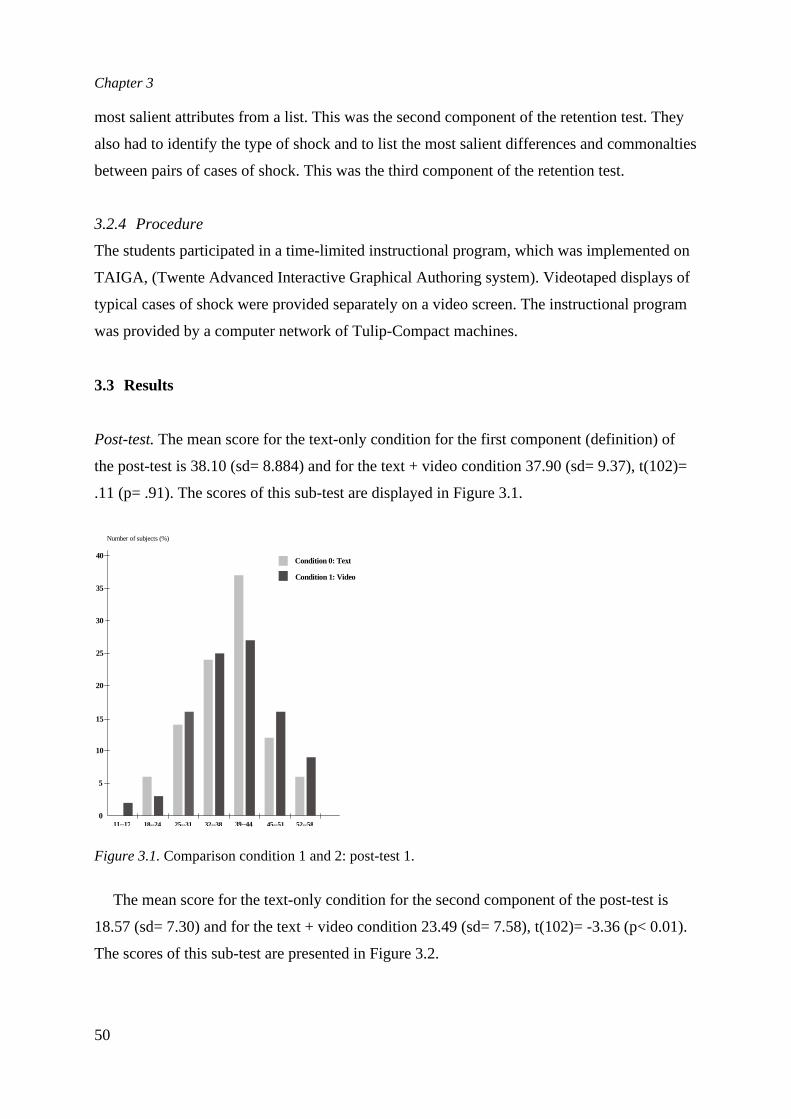
Chapter 3
50
most salient attributes from a list. This was the second component of the retention test. They
also had to identify the type of shock and to list the most salient differences and commonalties
between pairs of cases of shock. This was the third component of the retention test.
3.2.4 Procedure
The students participated in a time-limited instructional program, which was implemented on
TAIGA, (Twente Advanced Interactive Graphical Authoring system). Videotaped displays of
typical cases of shock were provided separately on a video screen. The instructional program
was provided by a computer network of Tulip-Compact machines.
3.3 Results
Post-test.The mean score for the text-only condition for the first component (definition) of
the post-test is 38.10 (sd= 8.884) and for the text + video condition 37.90 (sd= 9.37), t(102)=
.11 (p= .91). The scores of this sub-test are displayed in Figure 3.1.
Figure 3.1.Comparison condition 1 and 2: post-test 1.
The mean score for the text-only condition for the second component of the post-test is
18.57 (sd= 7.30) and for the text + video condition 23.49 (sd= 7.58), t(102)= -3.36 (p< 0.01).
The scores of this sub-test are presented in Figure 3.2.
0
5
10
15
20
25
30
35
40
11--17 18--24 25--31 32--38 39--44 45--51 52--58
Condition 0: Text
Condition 1: Video
Number of subjects (%)
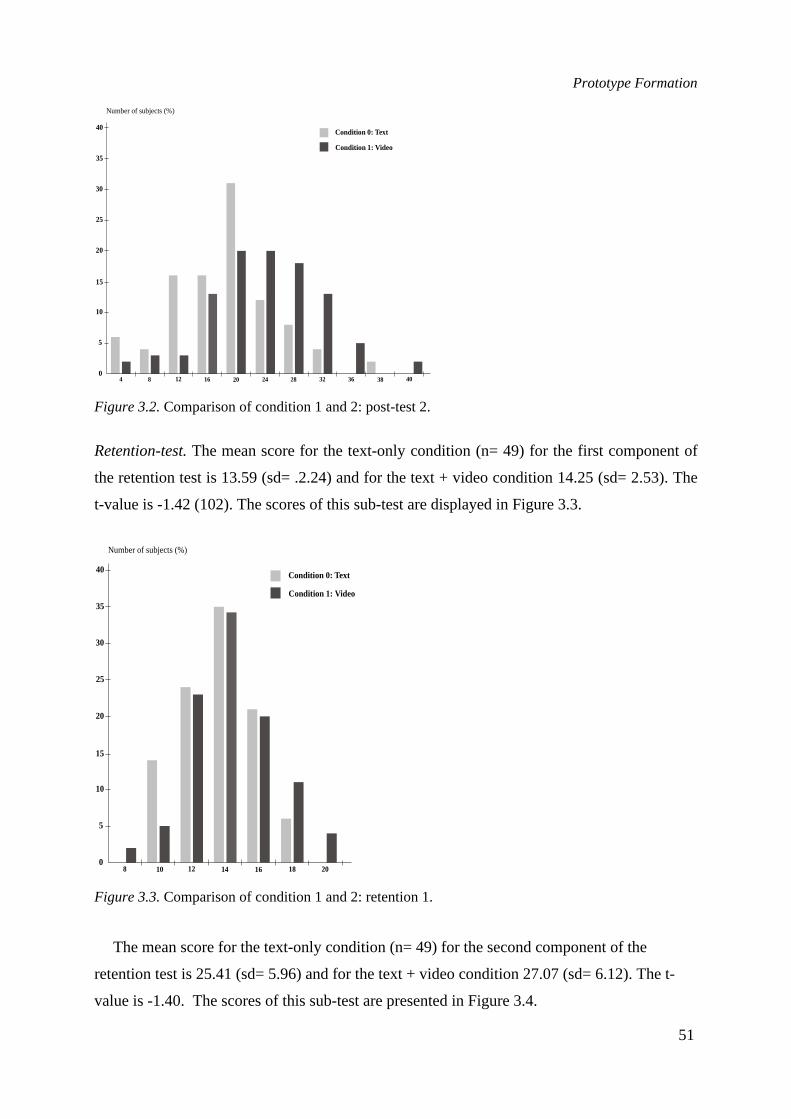
Prototype Formation
51
Figure 3.2.Comparison of condition 1 and 2: post-test 2.
Retention-test.The mean score for the text-only condition (n= 49) for the first component of
the retention test is 13.59 (sd= .2.24) and for the text + video condition 14.25 (sd= 2.53). The
t-value is -1.42 (102). The scores of this sub-test are displayed in Figure 3.3.
Figure 3.3.Comparison of condition 1 and 2: retention 1.
The mean score for the text-only condition (n= 49) for the second component of the
retention test is 25.41 (sd= 5.96) and for the text + video condition 27.07 (sd= 6.12). The t-
value is -1.40. The scores of this sub-test are presented in Figure 3.4.
0
5
10
15
20
25
30
35
40
4 8 12 16 20 24 28 32 36 38 40
Condition 0: Text
Condition 1: Video
Number of subjects (%)
0
5
10
15
20
25
30
35
40
8 10 12 14 16 18 20
Condition 0: Text
Condition 1: Video
Number of subjects (%)
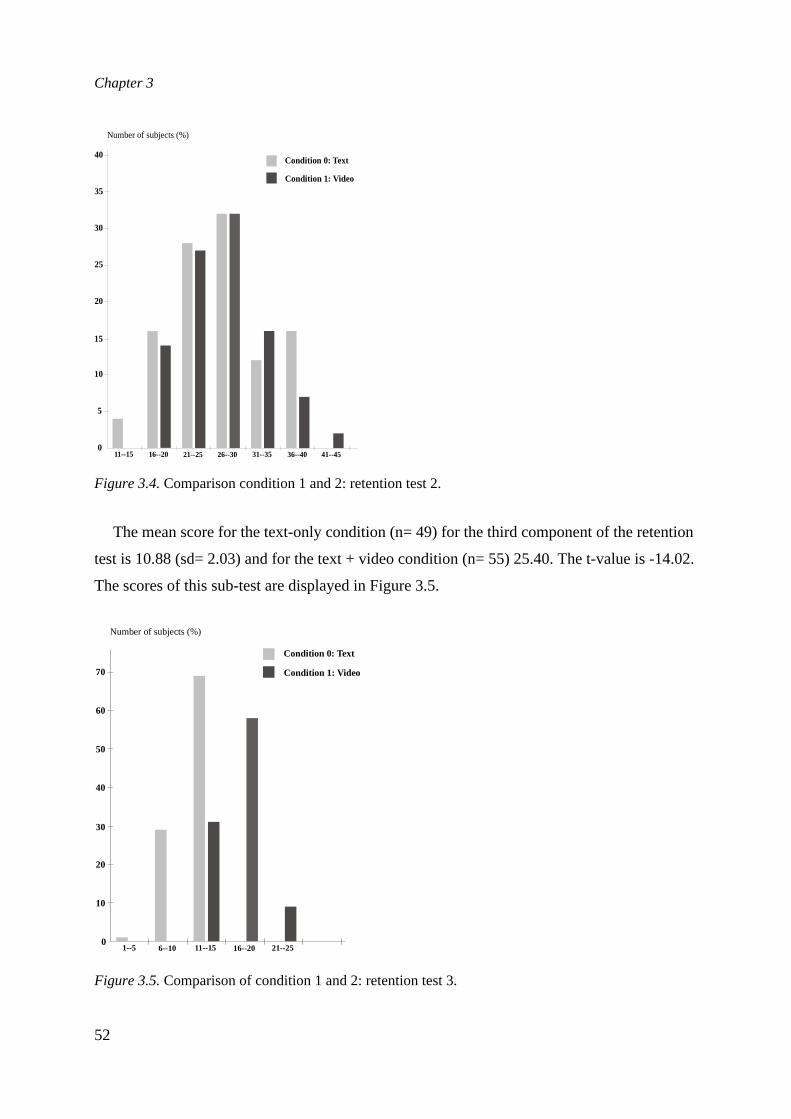
Chapter 3
52
Figure 3.4.Comparison condition 1 and 2: retention test 2.
The mean score for the text-only condition (n= 49) for the third component of the retention
test is 10.88 (sd= 2.03) and for the text + video condition (n= 55) 25.40. The t-value is -14.02.
The scores of this sub-test are displayed in Figure 3.5.
Figure 3.5.Comparison of condition 1 and 2: retention test 3.
0
5
10
15
20
25
30
35
40
11--15 16--20 21--25 26--30 31--35 36--40 41--45
Condition 0: Text
Condition 1: Video
Number of subjects (%)
0
10
20
30
40
50
60
70
1--5 6--10 11--15 16--20 21--25
Condition 0: Text
Condition 1: Video
Number of subjects (%)
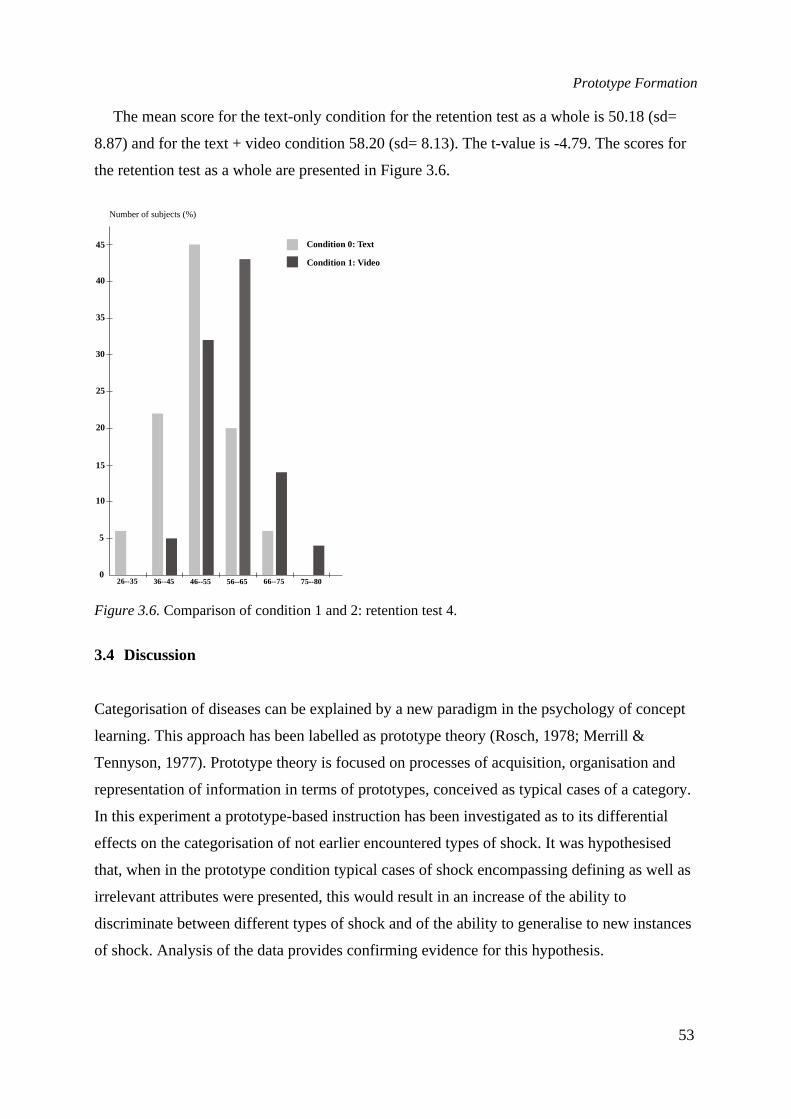
Prototype Formation
53
The mean score for the text-only condition for the retention test as a whole is 50.18 (sd=
8.87) and for the text + video condition 58.20 (sd= 8.13). The t-value is -4.79. The scores for
the retention test as a whole are presented in Figure 3.6.
Figure 3.6.Comparison of condition 1 and 2: retention test 4.
3.4 Discussion
Categorisation of diseases can be explained by a new paradigm in the psychology of concept
learning. This approach has been labelled as prototype theory (Rosch, 1978; Merrill &
Tennyson, 1977). Prototype theory is focused on processes of acquisition, organisation and
representation of information in terms of prototypes, conceived as typical cases of a category.
In this experiment a prototype-based instruction has been investigated as to its differential
effects on the categorisation of not earlier encountered types of shock. It was hypothesised
that, when in the prototype condition typical cases of shock encompassing defining as well as
irrelevant attributes were presented, this would result in an increase of the ability to
discriminate between different types of shock and of the ability to generalise to new instances
of shock. Analysis of the data provides confirming evidence for this hypothesis.
0
5
10
15
20
25
30
35
40
45
26--35 36--45 46--55 56--65 66--75 75--80
Condition 0: Text
Condition 1: Video
Number of subjects (%)
Chapter 3
54
Comparison of the post-test scores in both conditions yields that, as to definition of shock and
attributes of different types of shock the mean performance does not differ significantly. The
post-test scores as to inferring to (a type of) shock yield a significant difference between both
instructional conditions (2-tailed prob. = .001). Inspection of the scores of the retention test
yields that, as to discrimination between shock and non-shock and as to identifying the most
salient attributes of shock there is a significant difference between both conditions. Regarding
the identification of shock in terms of commonalties and differences between types of shock
the mean scores differ significantly (2-tailed prob. = .000). As a result the overall scores of the
retention test provide a significant difference (2-tailed prob. .000). In the text-only condition
the mean score is 50.18, while in the text + video condition the mean score is 58.20.
The results indicate that an instructional design model in which one assumes that members
of a category have attributes, which are separately necessary and jointly sufficient to provide a
definition of a concept, is inadequate. One has to realise that complex entities like shock can
only be defined unequivocally in terms of similarity to the most typical case of the concept.
This point of view is consistent with the hypothesis of Rosch (1975) that an item is more or
less a prototypical member of a category. The meaning of concepts is represented in
prototypes, conceived as a hypothetical construction of the most typical instance of a
category. Students are able to extract prototypes from mean values of attributes of a category.
From this perspective a prototype functions as a reference point in terms of which categorial
assignments are made by comparing the disorder to be categorised to an internal, prototypical
representation of the disease.
In forming a prototype the basic level of concepts (i.e. the level where concepts are clearly
connected to objects) play a crucial role, as has been confirmed in this experiment. Presenting
a prototype of shock does result in a mental image of the shock patient that is more resistant to
extinction than propositional information about the shock patient. This result has to be
interpreted in terms of the fact that at the basic level of concept representation a prototype
encompasses both the most frequently occurring attributes as well as irrelevant attributes. As
such the result of this experiment forms a corroboration of the model as proposed by Rosch
and of the transferability of this model to the context of an instructional design guide for
learning concepts as proposed by Merrill and Tennyson (1977).
Prototype Formation
55
References
Bruner, J. S., Goodnow, J. J., & Austin G. A. (1956).A study of thinking. New York: Wiley.Cantor, N., & Smith, E. E. (1980). Psychiatric diagnosis as prototype categorisation.Journal of
Abnormal Psychology, 89(2), 181-193.Elstein, A. S., Shulman, L. S., & Sprafka, S. (1978).Medical problem solving. Cambridge (Mass.):
Harvard University Press.Hunt, E. B. (1962).Concept learning: An information processing problem. New York: Wiley.Hovland, C. I. A. (1952). A communication analysis of concept learning.Psychological Review,
59, 461-472.Merrill, M. D., & Tennyson, R. D. (1977).Concept teaching: An instructional design guide. New
York: Englewood Cliffs.Ok-Choon Park, & Tennyson, R. D. (1980). Adaptive design strategies for selecting number and
presentation order of examples in coordinate concept acquisition.Journal of EducationalPsychology, 72,(3), 362-370.
Posner, M. I., & Keele, S. W. (1968). On the genesis of abstract ideas.Journal of ExperimentalPsychology, 77, 353-363.
Rosch, E. (1975). Cognitive representations of semantic categories.Journal of ExperimentalPsychology: General, 104, 192-233.
Rosch, E., & Mervis, C. B., (1975). Family resemblances: Studies in the internal structure ofcategories.Cognitive Psychology, 7, 573-605.
Rosch, E. (1978). Principles of categorisation. In E. Rosch & B. B. Lloyd (Eds.),Cognition andCategorisation(pp. 24-46). Hillsdale, NJ: Lawrence Erlbaum.
Tennyson, R. D., & Park, S. I. (1984). Process learning time as an adaptive design variable inconcept learning using computer-based instruction.Journal of Educational Psychology, 76,452-465.
Tennyson, R. D., & Cocchiarella, M. (1986). An empirically based instructional design theory forteaching concepts.Review of Educational Research, 56, 40-71.

4
THE EFFECT OF THE PRESENTATION OFBEST EXAMPLES AND ATTRIBUTE
ELABORATION ON THE ACQUISITION OFCOORDINATE CONCEPTS
In this chapter the effect of the presentation of best examples and attributeelaboration on the acquisition of coordinate concepts is studied. Bothinstructional design rules are contained in Tennyson and Cocchiarella's model.They defined a best example as a presentation of an example that clearlyrepresents a typical class member. In this study it involves typical examples of thethree types of shock involved (hypovolemic shock, cardial shock and septic shock).Because for the acquisition of concepts attributes have to be identified theelaboration of attributes may be helpful. Tennyson and Cocchiarella definedattribute elaboration as use of instructional devices to direct attention toimportant or salient attributes of specific expository or interrogatory examples.The model does not provide further prescriptions nor is there evidence about theeffectiveness of this component. Therefore Dwyer’s model (Dwyer, 1978) wasused. Attribute elaboration was operationalised in terms of marking andcontrasting of attributes. The instructional program contained four instructionalconditions. (a) expository-marked, (b) interrogatory-marked, (c) expository-non-marked, and (d) interrogatory-non-marked.

Chapter 4
58
4.1 Introduction
In this chapter an experiment will be described in which the effect of two instructional
variables, nature of examples and attribute elaboration, on the acquisition of coordinate
concepts were studied.
A concept is a rule to categorise a set of objects, events or processes. Based on one or more
shared attributes and the logical connectives between them the objects are grouped together
into a class. They sometimes are referred to by a label (Bourne, 1970; Eckes, 1990). A
concept acquisition process is supposed to be a problem-solving process, in which both the
conceptual rule is developed and the problem-solving procedure is learned and practised. Two
types of categorisation problems are distinguished, dependent on the number of categories to
which the objects are allocated: (a) problems where the number of categories is limited to two
for positive and negative examples, and (b) problems with different subcategories. The
resulting two types of conceptual knowledge are: (a) single or successive concept and (b)
coordinate concept. The coordinate concept comprises a set of attributes, common to all
subcategories. To categorise an object in one of the subcategories at least one critical attribute
is necessary.
For the acquisition of concepts subjects have to identify the defining attributes of the
objects and then categorise the object. Categorisation is a process in which objects, processes
or events are subsumed under a category. In education usually objects are presented to the
subjects, first as examples, later for practice and tests. They have to identify the commonalties
and differences between objects. In the categorisation process both the relevant (defining) and
the irrelevant attributes play a role.
To facilitate the acquisition of concepts instructional design models were developed. These
models differ because they are influenced by the assumptions how a concept is acquired. The
classical view of categorisation (Eckes, 1990; Medin & Smith, 1981) assumed that all
examples of a category share one or more attributes. In this view categorisation is enabled by
the decision on the existence of the defining attributes. The category boundaries are
unambiguously stated. Contrary to the classical view of concept acquisition the prototype
view also accounted for the effect of non-defining attributes. This view assumed that the
categories are represented by a “prototypical object”, that showed a combination of defining
and most often occurring non-defining attributes. The typical examples are assumed to
correspond with the prototype. The atypical examples are assumed to be in the boundary
Best Examples and Attribute Elaboration
59
region of a category. From the prototype view category membership is gradual, i.e. that
typical examples contain more characteristic attributes compared to atypical ones.
Both assumptions were used in the development of teaching models for concept
acquisition. The ideas of the classical view were applied in the model developed by Merrill
and Tennyson (1977), the assumptions of the prototype view in the model of Tennyson and
Cocchiarella (1986). The first model only attends to successive concepts. The second model
dealt with both successive and coordinate concepts. The model Tennyson and Cocchiarella
developed for the acquisition of coordinate concepts prescribes parts of the instruction and
globally sequences these parts. It encompasses six components: (a) label and definition, (b)
best example, (c) expository examples (a display which presents an example and/or non-
example to the student while simultaneously identifying its concept name) presentation), (d)
interrogatory example (a display which presents an example and/or a non-example and asks
the student to recall or match the example to the concept name), (e) attribute elaboration (uses
some attention focusing device to direct the student’s attention to important or salient
attributes present in a specific expository or interrogatory example) and (f) embedded
refreshment. There are only a few preliminary studies based on this model (e.g. Tennyson,
Youngers & Suebsonthi, 1983). To evaluate the use of the model it is important to study the
effectiveness of the model and the weight of the different components.
In case of a coordinate concept both the general conceptual rule which refers to the base
category and the rules for each subcategory have to be developed. For the general rule the
learners have to identify the relevant attributes, whereas for the specific rules the critical
attributes have to be identified in order to discriminate between the objects from the different
subcategories. Moreover the problem-solving procedure or identification algorithm has to be
learned and practised. For the identification of relevant attributes and for practising the rule
the presentation of the objects or examples are necessary (components, b, c and d of the
model).
4.1.1 The nature of examples
Tennyson and Cocchiarella defined a best example as a “presentation of (an) example(s) that
clearly represent(s) a typical class member” (p. 57). It is an example of a concept that contains
the most frequently occurring attributes. Expository examples were defined as “presentation
of complete examples with concept classification. For coordinate concepts, examples are
organised into a rational set such that examples are matched according to similarity to
Chapter 4
60
variable attributes” (p. 57, 58). They systematically present the content propositionally. They
contain a display which presents an example as well as a non-example to the student and
which identifies the concept label simultaneously. An interrogative example, finally,
systematically presents the content “within rational sets for coordinate concepts, as problems
to be solved” (p. 58). They contain a display, which presents to the student an example and/or
a non-example and which requires the student to remember the example and to match the
example with the concept name.
Tennyson and Cocchiarella (1986) assumed that the process of concept learning is at least
partially a deductive process in which the classification of examples takes into account a
typical example as a cognitive reference point. The deductive part of the process of
categorisation is the student’s combining of prototype and other examples. For the instruction
for coordinate concepts first a best example has to be found or defined. The selection or
construction of a best example depends on the structure of the taxonomy. Rosch (1978)
argued that within a taxonomy of concrete objects categories are structured such that there is
generally one level of abstraction at which the most basic category cuts can be made. In a
taxonomy this level is the base level. The objects of a category possess always some relevant
and irrelevant attributes. Because of the differences in conceptual rules (conjunction,
disjunction, conditional) the number of relevant attributes sometimes differs, whereas the
number of irrelevant attributes of objects in a category nearly always differs. Typical
examples of a category are the clearest cases of membership of a category and are supposed to
exist at the base level. A prototype is an object, which shows the most frequently occurring
relevant and irrelevant attributes. The concept's defining attributes are encapsulated into a
prototype that can be retrieved from memory and that can be used for comparison with the
new example. The selection of a best example of a coordinate concept depends on the number
of levels in a taxonomy. If the taxonomy has two levels the general category corresponds with
the base level whereas the subcategories are located at the lowest or subordinate level. For
example furniture is located at a base level, whereas chair is found at a subordinate level. In
case of a three level taxonomy the labels superordinate, base and subordinate category are
used (Rosch, 1978). If the taxonomy comprises more levels the three labels are used for those
objects which are indicated in the discourse, which means that for some objects the level
indication can change during the discourse. At all levels in a taxonomy the attributes of the
objects are used for their categorisation. Defining or relevant attributes are used to decide
whether an object belongs to a category. The label critical attributes is used to distinguish
Best Examples and Attribute Elaboration
61
between objects from different coordinate categories.
Because the coordinate concept that will be used in this study has two levels the best
example is chosen from the subordinate level. For each of the three coordinate concepts to be
acquired a best example was selected by experts. They were expository presented and
followed by interrogatively presented examples and non-examples. Information about
relevant and frequently occurring irrelevant attributes was presented by key-words, spoken
text and attention focusing devices. Interrogatory examples contained a set of questions
related to the relevant and irrelevant attributes of the object to be categorised. The prediction
was that expository presented best examples will have a facilitating effect on concept
acquisition because the subjects can easily construct (develop) a cognitive reference point that
encompasses both defining and frequently occurring irrelevant attributes. If a new example is
presented interrogatory the student will compare the attributes of the new example with those
from the reference point and if these correspond, make the categorisation response. An
irrelevant attribute, if perceived, can evoke a defining attribute and the learner will check
whether this is available. The expository presented best examples were expected to result in
(a) less errors, (b) less processing time, (c) more examples to be processed in a certain time-
limit, and (d) a greater amount of confidence compared to the case that such a cognitive
reference point does not exist. Thus the first objective was to study the effect of variation of
the nature of examples on the acquisition of coordinate concepts. A comparison between a set
of best examples (expository presented) and interrogatory examples was intended.
4.1.2 Attribute elaboration
Because for the acquisition of concepts attributes have to be identified the elaboration of
attributes may be helpful. Tennyson and Cocchiarella defined attribute elaboration as “use of
instructional devices to direct attention to important or salient attributes of specific expository
or interrogatory examples. It includes attribute prompting and attribute feedback” (p. 70). The
model does not provide further prescriptions nor is there evidence about the effectiveness of
this component. Therefore Dwyer’s model (Dwyer, 1978) was consulted. In his studies on
concept learning it was found that the saliency of attributes facilitated the acquisition of the
conceptual rule (Dwyer & Arnold, 1976). For this study it was supposed that the elaboration
of attributes will draw the learner’s attention to those attributes. Several techniques for
attribute elaboration are known ((Dwyer, 1978): contrast, underlining, complexity, intensity,
labelling, magnitude, circle, colour, ambiguity, question, optical effect, shadow effect, novelty
Chapter 4
62
and repetition. In this experiment some of them were used in order to mark the relevant
attributes and to contrast them with other attributes. Marking is the elaboration of relevant
values on a dimension from irrelevant ones. The technique is assumed to facilitate the search,
the selection and the coding of visual information. Contrasting is defined by Dwyer as a
technique to increase the saliency of the differences between two (values of) a dimension. It
was supposed that marking the relevant attributes will further facilitate concept acquisition. It
was predicted that expository presented best examples (followed by interrogatory examples
and non-examples), combined with an attention focusing device (marking and contrasting)
will result in a differential effect compared to the presentation with interrogatory examples
(with or without attribute elaboration). This differential effect was expected to hold for
responses, time and confidence.
4.1.3 The interaction effect
The predicted difference in learning efficiency and effectiveness between expository
presentation of best examples (followed by interrogatory examples) and the interrogatory
presentation of examples probably is dependent on attribute elaboration. It is supposed that in
case of expository presentation attribute elaboration will further increase the speed of
processing of information, because the search procedure for the attributes is structured. All
the relevant attributes are processed in the sequence in which they are presented and the
learners’ attention is directed to these attributes.
Moreover the elaboration of attributes will enhance the development of a cognitive
reference point, because the learners’ attention is explicitly directed to the defining attributes
and to those attributes that are strongly supporting the categorisation of the object. The
development of the reference point may foster retention of the concept and help the student to
categorise new objects. Interrogatory examples require the learners to first find the relevant
attributes.
If these are not marked first the learners need to find the defining and the most frequently
occurring attributes. This process requires more effort from the learners. If the categorisations
are correct the feedback then will strengthen the attributes' inclusion in the conceptual rule
and support retention. Because of the invested effort in the development of the concept and
the strengthening of it, the retention will not differ from the retention of the concept in the
marked condition in which probably less effort has to be invested. The result of the
investment in the non-marked condition will possibly neutralise the learning effect of the
Best Examples and Attribute Elaboration
63
saliency in the marked condition.
If the attributes are marked the speed of processing the information may be enhanced
somewhat, but because the sequence of presentation of the attributes is uncontrolled, the
learners need time to search and no interaction effect is expected.
4.2 Method
4.2.1 Subjects
The subjects were recruited from a nursing college (N= 62). Forty female and twenty two
male students participated - on an obligatory basis - in the context of the school curriculum.
As freshmen they took introductory courses in anatomy, physiology and internal medicine.
Because all students passed the prerequisite knowledge tests in the first year they were
randomly assigned to one of the four instructional conditions.
4.2.2 Material
Content.The content of the instructive program was the concept shock of which three
coordinate subtypes were used: (a) cardiogenic shock, (b) hypovolemic shock and (c) septical
shock (Perry & Potter, 1983). A detailed description of the content is presented in Chapter
two.
Shock is a disease which refers to a reduction of amount of blood in the organism. It is a
state of circulatory insufficiency in which cellular perfusion is inadequate for normal cellular
function. Based on critical attributes the coordinate types received a label: (a) hypovolemic
shock, resulting from hypovolaemia (loss of blood or liquid, (b) septic shock, resulting from
sepsis and (c) cardiogenic shock, resulting from cardiac failures. The relevant attributes of the
superordinate concept shock are: (a) paleness; (b) coldness; (c) perspiration; (d) fast pulse
rate; (e) low blood pressure and (f) reduced urinary output. The concept shock encompasses
three coordinate concepts:
(1) Hypovolemic shock. The critical attributes of this type of shock are: (a) restlessness;
(b) hypotension; (c) oliguria, i.e. decreased urinary output and (d) increased rate of
respiration. Often occurring irrelevant attributes are: (a) age (children, adults, elderly people)
and (b) accident (car accident, burns).
(2) Cardiogenic shock. The critical attributes of this type of shock are: (a) poor peripheral
pulses; (b) clammy skin; (c) low systolic blood pressure and (d) urinary output lower than 25
Chapter 4
64
ml/hr. Often occurring irrelevant attributes are: (a) age (children, adults, elderly people) and
(b) weight (obesity).
(3) Septic shock. The critical attributes of this type of shock are: (a) warm skin; (b)
clammy skin; (c) poor peripheral perfusion; (d) diminished urinary output; (e) tachycardia
(i.e. a high heart rate) and (f) tachypnoea (a high respiration rate). Often occurring irrelevant
attributes are: (a) age (children, adults, elderly people) and (b) alcohol addiction.
Based on verbal and visual information the students had to categorise twenty eight
videotaped, simulated patients in one of three subcategories. This number was supposed to be
sufficient to acquire the categorisation skill. A number of three simulated patients were
presented expository. The prescriptions for the simulation of the thirty one patients were
given by five medical experts. Their expertise varied from internal medicine to general
practitioner. They were selected based on their involvement in medical and nursing education.
Conditions.The instructional program contained four instructional conditions (see Chapter
two). Each condition contained twenty four interrogatory examples and four interrogatory
non-examples of the concept shock. Two of these conditions contained also one expository
presented typical example of the three types of shock. The students were free to decide upon
the number of patients to process in a fixed amount of time (two hours). The first condition
was labelled as expository-marked (exposition of a typical case of each of the three
subcategories of shock at the base level, combined with elaboration of the relevant attributes).
The second was labelled as interrogatory-marked (randomly selected interrogatory examples,
combined with elaboration of the relevant attributes). The third was labelled as expository-
non-marked (exposition of a typical case of each of the three subcategories of shock at the
base level, without attribute elaboration). The fourth was labelled as interrogatory-non-
marked (interrogatory examples, without attribute elaboration). Prior to entering one of the
four instructional conditions students were informed about the relevant attributes of shock as
well as about the critical attributes of the three types of shock. The instruction proceeded as
follows:
(1) Expository-marked. This condition started with the expository presentation of a typical
example of cardiogenic shock. The typicality had been assessed by medical experts dependent
on the co-occurrence of the relevant attributes. The example was characterised by the
following relevant attributes: (a) clammy skin; (b) perspiration; (c) 'dyspnoea en repos', i.e.
respiration disorders in rest; (d) cyanosis; (e) reduced systolic and diastolic blood pressure; (f)
Best Examples and Attribute Elaboration
65
increased arterial-pulmonic pressure; (g) increased central-venous pressure and (h) reduced
cardiac output. During the exposition the student’s attention was drawn to these attributes by
marking (a, b, c, d) and contrasting (e, f, g, h). After the exposition of this typical example
during forty minutes a set of randomly selected interrogatory examples (examples of one of
the three subtypes of shock or a non-example) were presented. The structure of the
interrogatory examples was: (a) initial visual presentation of the patient; (b) information about
name, age, professional activities, disease history and present status; (c) questions about the
location of the illness and about characteristics of the face, breath, hand, foot, heart frequency,
blood pressure, and cardiac output. At any time the student could choose to classify the
example. After forty minutes a typical example of hypovolemic shock was presented. Forty
minutes were used for practising the categorisation skill at the level of one subcategory. The
example was characterised by the following relevant attributes: (a) clammy skin; (b) paleness;
(c) increased breathing; (d) increased pulse rate; (e) reduced systolic and diastolic blood
pressure; (f) decreased arterial-pulmonic pressure; (g) decreased central-venous pressure; (h)
reduced cardiac output and (i) burns on chest and abdomen. During the exposition the
student’s attention was drawn to these attributes by marking (a, b, d, i) and contrasting (e, f, g,
h). After the exposition of this typical example of hypovolemic shock during forty minutes a
set of randomly selected interrogatory examples (examples of one of the three subtypes of
shock or a non-example) were presented. The structure of these interrogatory examples was
identical as in the first episode. Finally a typical example of septic shock was presented. The
example was characterised by the following relevant attributes: (a) a red chest; (b) a red face;
(c) irregular breathing; (d) cyanosis; (e) reduced systolic and diastolic blood pressure; (f)
decreased arterial-pulmonal pressure; (g) decreased central-venous pressure; (h) reduced
cardiac output and (i) increased pulse rate. During the exposition the student’s attention was
drawn to these attributes by marking (a, b, d) and contrasting (e, f, g, h). After the exposition
of this typical example of septic shock again during forty minutes a set of randomly selected
interrogatory examples (examples of one of the three subtypes of shock or a non-example)
were presented. The structure of these interrogatory examples was identical as in the first and
second episode.
(2) Expository-non-marked. This condition was identical to the prototypical-marked
condition except that no attention was drawn to the relevant attributes by using marking and
contrasting.
Chapter 4
66
(3) Interrogatory-marked. This condition contained only a set of interrogatory examples,
which could be accessed randomly. The examples could pertain to one of the three subtypes
of shock or to a non-example (hyperglycaemia, hypoglycaemia or collapse, having a certain
family-resemblance to shock). The structure of these interrogatory examples was again: (a)
initial visual presentation of the patient; (b) information about name, age professional
activities, disease history and present status; (c) questions about the location of the illness and
about characteristics of the face, breath, hand, foot, heart frequency, blood pressure, and
cardiac output. At any time the student could choose to classify the example. In this condition
relevant attributes were marked or contrasted with normal values.
(4) Interrogatory-non-marked. This condition again contained only a set of interrogatory
examples, which could be accessed randomly. The examples could pertain to one of the three
subtypes of shock or to a non-example (hyperglycaemia, hypoglycaemia or collapse, having a
certain family-resemblance to shock). The structure of these interrogatory examples was
identical to the structure of interrogatory examples in the other three conditions. Again the
student could choose to classify the example at any moment.
4.2.3 Apparatus, authoring system and courseware
The instructive program was delivered as interactive video. Three configurations, each
containing (a) a video disc player (Philips), (b) a Video Logic Card DVA 4000 and (c) a
Macintosh computer were used simultaneously for data collection. The instructions were
written in AuthorWare (AuthorWare Manual, 1990). The videodisk contained 31 simulated
patients which had to be categorised into one of the three shock categories. The video screen
was partitioned into a fixed number of segments and buttons. The video screen for the
presentation of interrogatory examples is shown in Figure 4.1.
The presentation buttons comprised three subsets: (a) buttons to access written
information; (b) buttons to access images and (c) buttons to access monitor data. The buttons
could be activated in a random sequence. In order to access written information three buttons
were constructed. These were the buttons 1 (for personal data), 2 (for anamnestic data
concerning history of the disease) and 3 (for the current complaints). By activating one of
these buttons the data could be used. The data were presented in the presentation screen. It
was possible to inspect relevant attributes of a part of the patient’s body. For that purpose a
number of buttons (numbers 4, 5, 6, 7 and 8) were available. By clicking a button the student
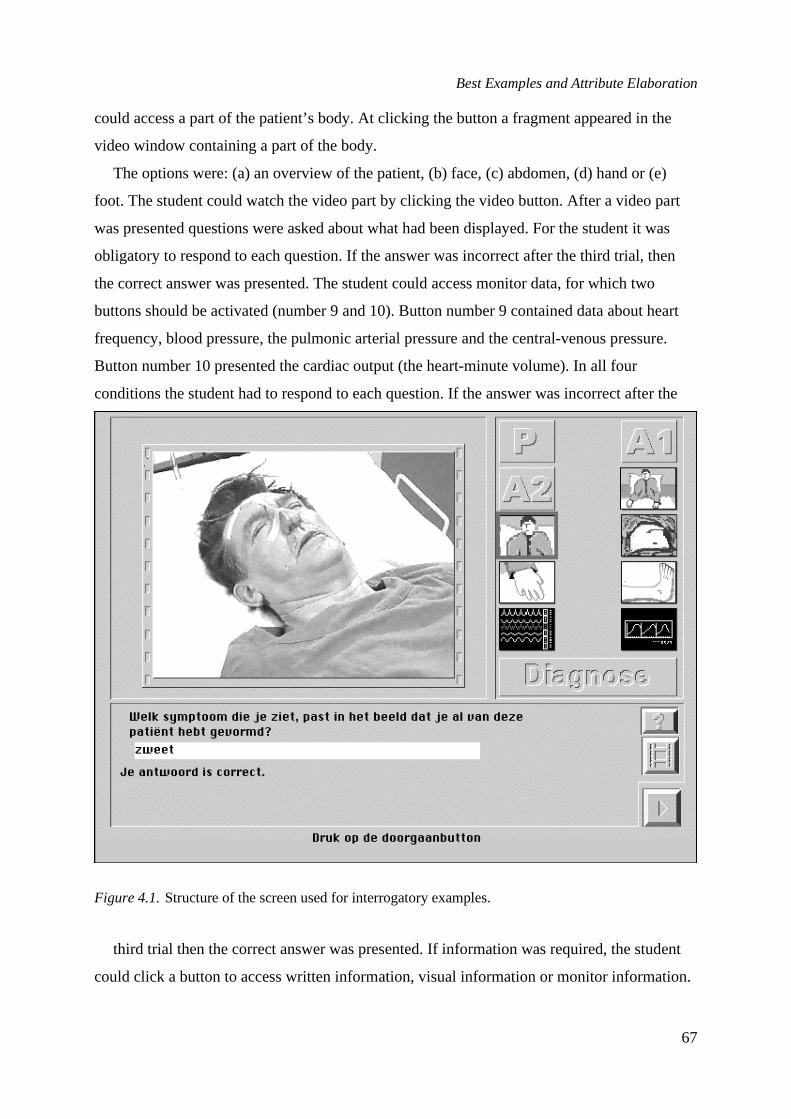
Best Examples and Attribute Elaboration
67
could access a part of the patient’s body. At clicking the button a fragment appeared in the
video window containing a part of the body.
The options were: (a) an overview of the patient, (b) face, (c) abdomen, (d) hand or (e)
foot. The student could watch the video part by clicking the video button. After a video part
was presented questions were asked about what had been displayed. For the student it was
obligatory to respond to each question. If the answer was incorrect after the third trial, then
the correct answer was presented. The student could access monitor data, for which two
buttons should be activated (number 9 and 10). Button number 9 contained data about heart
frequency, blood pressure, the pulmonic arterial pressure and the central-venous pressure.
Button number 10 presented the cardiac output (the heart-minute volume). In all four
conditions the student had to respond to each question. If the answer was incorrect after the
Figure 4.1.Structure of the screen used for interrogatory examples.
third trial then the correct answer was presented. If information was required, the student
could click a button to access written information, visual information or monitor information.
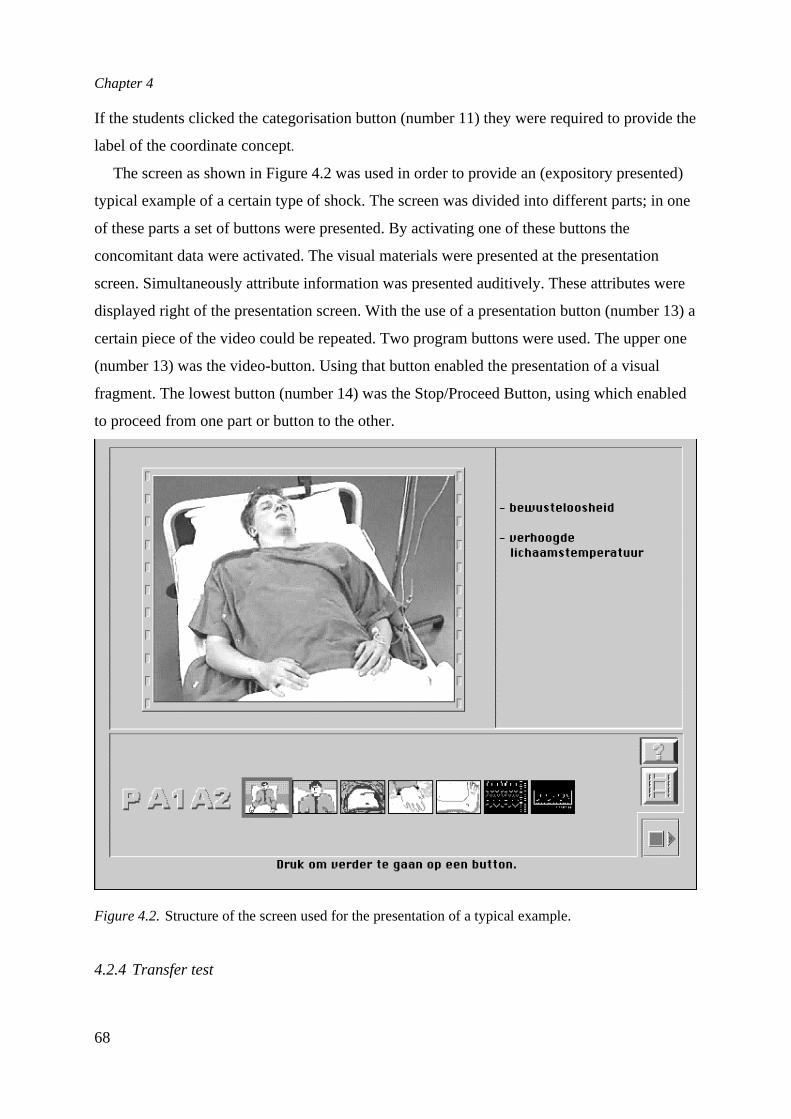
Chapter 4
68
If the students clicked the categorisation button (number 11) they were required to provide the
label of the coordinate concept.
The screen as shown in Figure 4.2 was used in order to provide an (expository presented)
typical example of a certain type of shock. The screen was divided into different parts; in one
of these parts a set of buttons were presented. By activating one of these buttons the
concomitant data were activated. The visual materials were presented at the presentation
screen. Simultaneously attribute information was presented auditively. These attributes were
displayed right of the presentation screen. With the use of a presentation button (number 13) a
certain piece of the video could be repeated. Two program buttons were used. The upper one
(number 13) was the video-button. Using that button enabled the presentation of a visual
fragment. The lowest button (number 14) was the Stop/Proceed Button, using which enabled
to proceed from one part or button to the other.
Figure 4.2.Structure of the screen used for the presentation of a typical example.
4.2.4 Transfer test
Best Examples and Attribute Elaboration
69
The transfer test contained nineteen examples and non-examples. Eleven of these patients had
a septic shock, five patients had a hypovolemic shock and two patients had a cardiogenic
shock. The different number per category resulted partly from the availability of patients in
the material production phase, partly from the incidence of the type of shock. One patient of
the total set had a diabetic coma. Each patient was presented in the following way. First a
total shot of the patient was presented; this stage was supported by verbally presented
information concerning the personal data, the disease history and the current situation. Next a
monitor displayed the heart rate values, systolic and diastolic blood pressure, central venous
pressure and temperature. The video zoomed in to head, foot and hand. The following test
format was adopted: it started with general information and an example. For each patient the
same questions were posed. First the question was presented whether there was some
dysfunction identifiable, next the student was required to provide a categorisation. Next the
students had to rate on a five-point scale the confidence with which they had put forward their
categorisation and based on which attributes they had been able to infer a category. The two
most contributing attributes had to be identified.
4.2.5 Procedure
Based on teacher ratings all subjects were randomly assigned to one of the four conditions
and were presented the corresponding instructive program. Instruction time was fixed at one
hundred and twenty minutes, for each coordinate concept forty minutes. For each coordinate
concept eight examples were available. The four non-examples of shock (hyperglycaemia,
hyperventilation, diabetic coma and collapse ("syncope")) were randomly distributed across
the subtypes of shock. The presentation of the feedback on the response depended on three
variables: (a) if the students did not collect all data about the patient, they were instructed to
study these data. They could also make a second categorisation, (b) if all data about a patient
had been collected, the students had three possibilities to provide the correct categorisation. If
the category was incorrect after the third trial, then the correct one was provided. A maximum
of three trials were chosen because that number was expected to maintain the learning
process. If the students had clicked a button and studied an attribute, one or more questions
about the fragment involved were presented. These questions were presented in a separate
segment. The answers, which the student provided, were also displayed in this segment. The
same applied for the feedback and the categorisation. By clicking the presentation buttons the
students could access relevant information. If the students had studied video material about a

Chapter 4
70
part of the patient’s body, then a question was presented. They could see the corresponding
video fragment by clicking the video button and could repeat this as frequently as they
wanted. Also if they had given an incorrect answer after the first trial, they could see the
video part twice. When the students had answered a question, or when they had provided a
categorisation, they could close the program with the Stop/Proceed button. When they did not
do this, they could not proceed with the program.
4.2.6 Data and Design
A 2 x 2 factorial design containing the factors nature of examples and attribute elaboration
was chosen. Each factor contained two levels. The factor nature of examples contained the
levels typical example and interrogatory examples. The factor attribute elaboration contained
the levels marking/contrasting or not marking/contrasting.
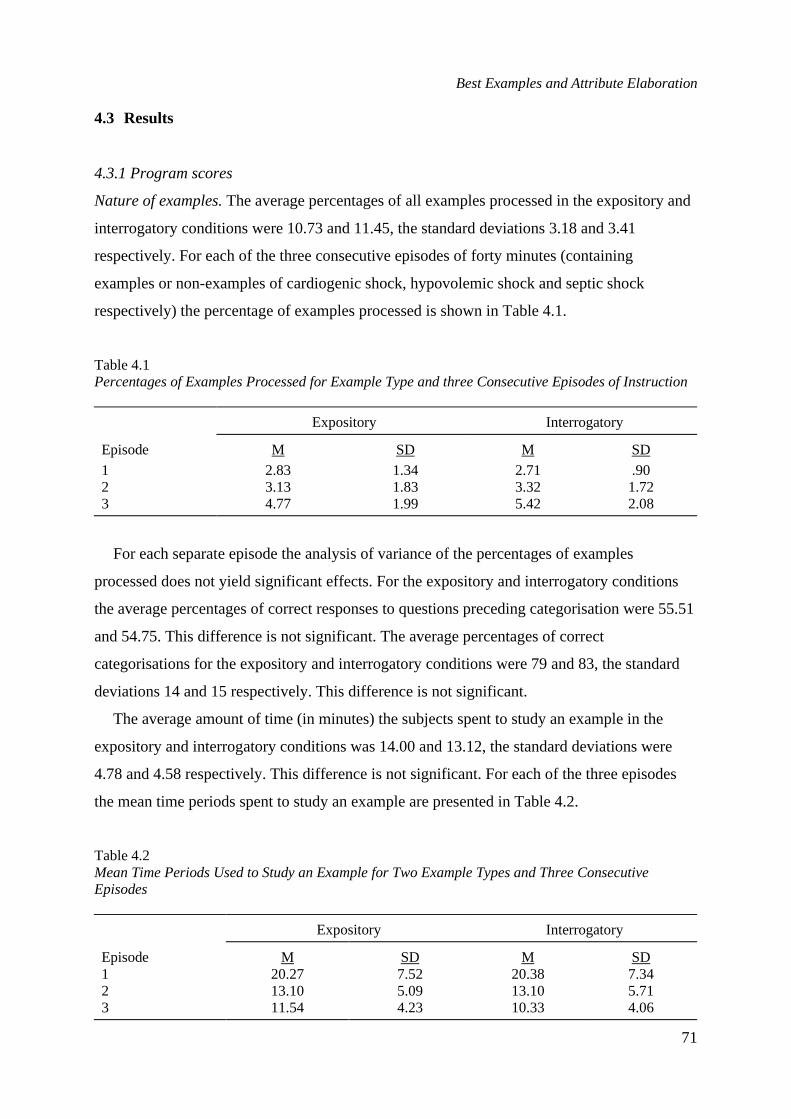
Best Examples and Attribute Elaboration
71
4.3 Results
4.3.1 Program scores
Nature of examples.The average percentages of all examples processed in the expository and
interrogatory conditions were 10.73 and 11.45, the standard deviations 3.18 and 3.41
respectively. For each of the three consecutive episodes of forty minutes (containing
examples or non-examples of cardiogenic shock, hypovolemic shock and septic shock
respectively) the percentage of examples processed is shown in Table 4.1.
Table 4.1Percentages of Examples Processed for Example Type and three Consecutive Episodes of Instruction
Expository Interrogatory
Episode M SD M SD
1 2.83 1.34 2.71 .902 3.13 1.83 3.32 1.723 4.77 1.99 5.42 2.08
For each separate episode the analysis of variance of the percentages of examples
processed does not yield significant effects. For the expository and interrogatory conditions
the average percentages of correct responses to questions preceding categorisation were 55.51
and 54.75. This difference is not significant. The average percentages of correct
categorisations for the expository and interrogatory conditions were 79 and 83, the standard
deviations 14 and 15 respectively. This difference is not significant.
The average amount of time (in minutes) the subjects spent to study an example in the
expository and interrogatory conditions was 14.00 and 13.12, the standard deviations were
4.78 and 4.58 respectively. This difference is not significant. For each of the three episodes
the mean time periods spent to study an example are presented in Table 4.2.
Table 4.2Mean Time Periods Used to Study an Example for Two Example Types and Three ConsecutiveEpisodes
Expository Interrogatory
Episode M SD M SD1 20.27 7.52 20.38 7.342 13.10 5.09 13.10 5.713 11.54 4.23 10.33 4.06
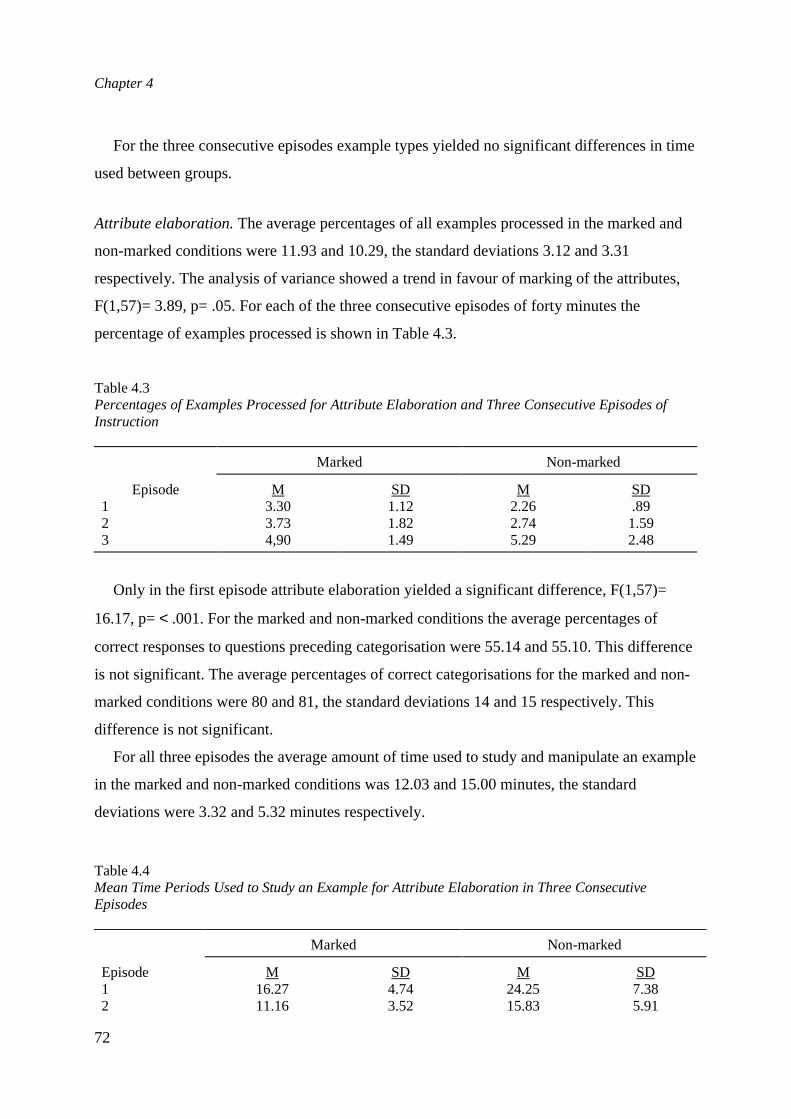
Chapter 4
72
For the three consecutive episodes example types yielded no significant differences in time
used between groups.
Attribute elaboration.The average percentages of all examples processed in the marked and
non-marked conditions were 11.93 and 10.29, the standard deviations 3.12 and 3.31
respectively. The analysis of variance showed a trend in favour of marking of the attributes,
F(1,57)= 3.89, p= .05. For each of the three consecutive episodes of forty minutes the
percentage of examples processed is shown in Table 4.3.
Table 4.3Percentages of Examples Processed for Attribute Elaboration and Three Consecutive Episodes ofInstruction
Marked Non-marked
Episode M SD M SD1 3.30 1.12 2.26 .892 3.73 1.82 2.74 1.593 4,90 1.49 5.29 2.48
Only in the first episode attribute elaboration yielded a significant difference, F(1,57)=
16.17, p=< .001. For the marked and non-marked conditions the average percentages of
correct responses to questions preceding categorisation were 55.14 and 55.10. This difference
is not significant. The average percentages of correct categorisations for the marked and non-
marked conditions were 80 and 81, the standard deviations 14 and 15 respectively. This
difference is not significant.
For all three episodes the average amount of time used to study and manipulate an example
in the marked and non-marked conditions was 12.03 and 15.00 minutes, the standard
deviations were 3.32 and 5.32 minutes respectively.
Table 4.4Mean Time Periods Used to Study an Example for Attribute Elaboration in Three ConsecutiveEpisodes
Marked Non-marked
Episode M SD M SD1 16.27 4.74 24.25 7.382 11.16 3.52 15.83 5.91
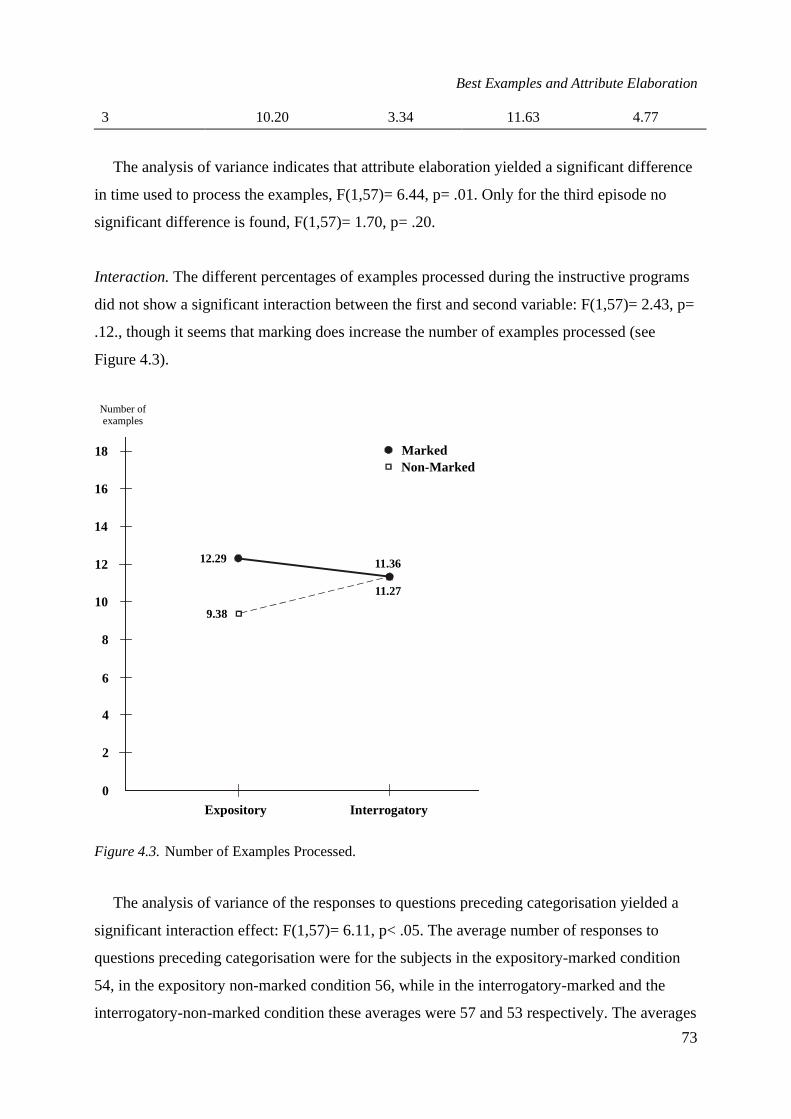
Best Examples and Attribute Elaboration
73
3 10.20 3.34 11.63 4.77
The analysis of variance indicates that attribute elaboration yielded a significant difference
in time used to process the examples, F(1,57)= 6.44, p= .01. Only for the third episode no
significant difference is found, F(1,57)= 1.70, p= .20.
Interaction.The different percentages of examples processed during the instructive programs
did not show a significant interaction between the first and second variable: F(1,57)= 2.43, p=
.12., though it seems that marking does increase the number of examples processed (see
Figure 4.3).
Figure 4.3.Number of Examples Processed.
The analysis of variance of the responses to questions preceding categorisation yielded a
significant interaction effect: F(1,57)= 6.11, p< .05. The average number of responses to
questions preceding categorisation were for the subjects in the expository-marked condition
54, in the expository non-marked condition 56, while in the interrogatory-marked and the
interrogatory-non-marked condition these averages were 57 and 53 respectively. The averages
0
2
4
6
8
10
12
14
16
18
12.29 11.36
11.27
9.38
Expository Interrogatory
Number ofexamples
MarkedNon-Marked
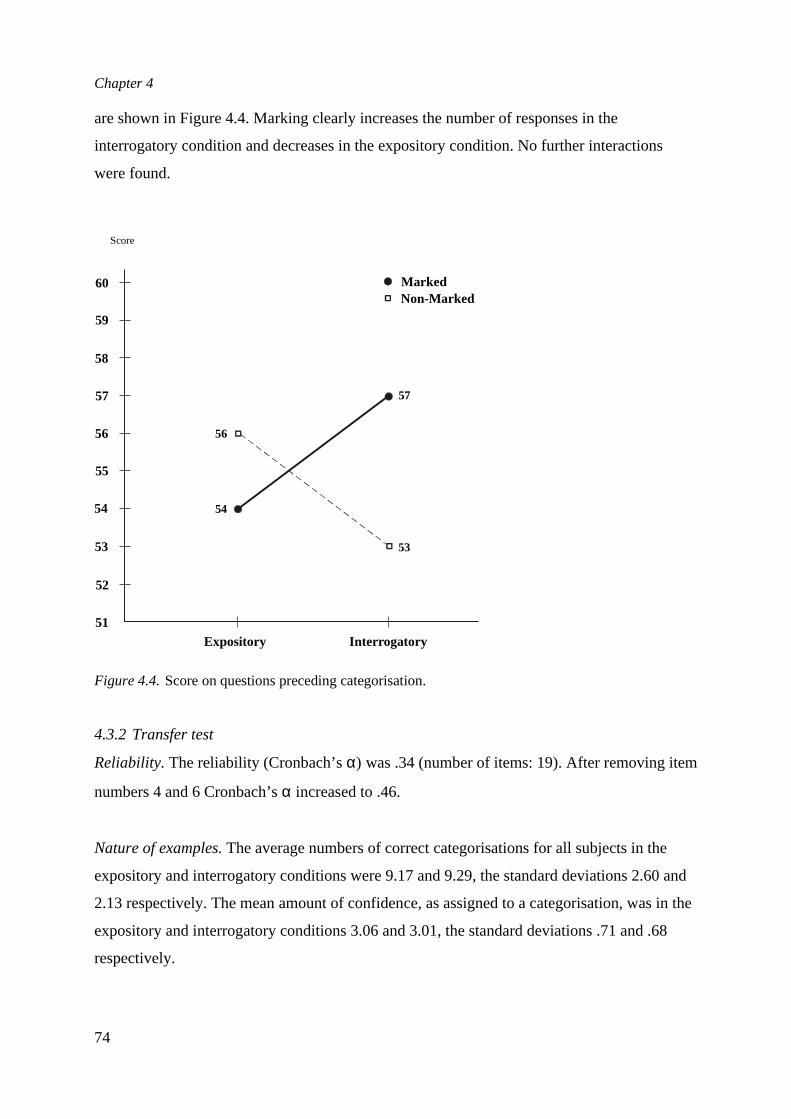
Chapter 4
74
are shown in Figure 4.4. Marking clearly increases the number of responses in the
interrogatory condition and decreases in the expository condition. No further interactions
were found.
Figure 4.4.Score on questions preceding categorisation.
4.3.2 Transfer test
Reliability.The reliability (Cronbach’sα) was .34 (number of items: 19). After removing item
numbers 4 and 6 Cronbach’sα increased to .46.
Nature of examples.The average numbers of correct categorisations for all subjects in the
expository and interrogatory conditions were 9.17 and 9.29, the standard deviations 2.60 and
2.13 respectively. The mean amount of confidence, as assigned to a categorisation, was in the
expository and interrogatory conditions 3.06 and 3.01, the standard deviations .71 and .68
respectively.
51
52
53
54
55
56
57
58
59
60
56
57
53
54
Expository Interrogatory
Score
MarkedNon-Marked
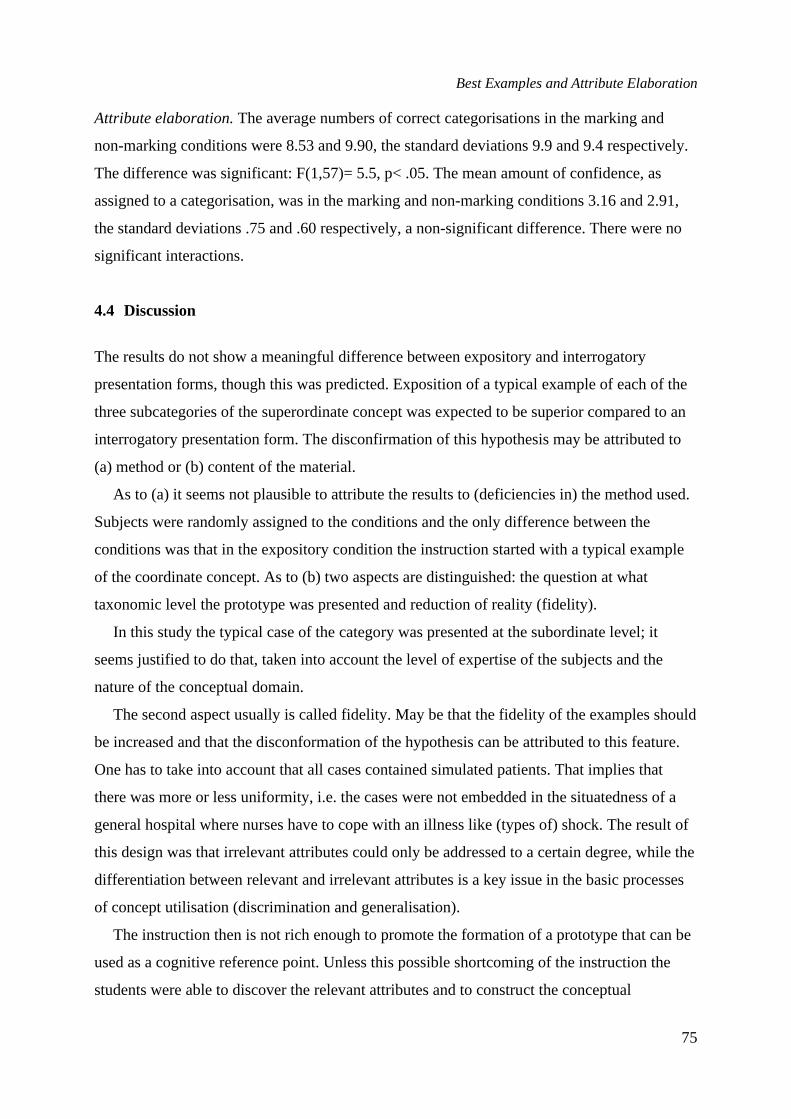
Best Examples and Attribute Elaboration
75
Attribute elaboration.The average numbers of correct categorisations in the marking and
non-marking conditions were 8.53 and 9.90, the standard deviations 9.9 and 9.4 respectively.
The difference was significant: F(1,57)= 5.5, p< .05. The mean amount of confidence, as
assigned to a categorisation, was in the marking and non-marking conditions 3.16 and 2.91,
the standard deviations .75 and .60 respectively, a non-significant difference. There were no
significant interactions.
4.4 Discussion
The results do not show a meaningful difference between expository and interrogatory
presentation forms, though this was predicted. Exposition of a typical example of each of the
three subcategories of the superordinate concept was expected to be superior compared to an
interrogatory presentation form. The disconfirmation of this hypothesis may be attributed to
(a) method or (b) content of the material.
As to (a) it seems not plausible to attribute the results to (deficiencies in) the method used.
Subjects were randomly assigned to the conditions and the only difference between the
conditions was that in the expository condition the instruction started with a typical example
of the coordinate concept. As to (b) two aspects are distinguished: the question at what
taxonomic level the prototype was presented and reduction of reality (fidelity).
In this study the typical case of the category was presented at the subordinate level; it
seems justified to do that, taken into account the level of expertise of the subjects and the
nature of the conceptual domain.
The second aspect usually is called fidelity. May be that the fidelity of the examples should
be increased and that the disconformation of the hypothesis can be attributed to this feature.
One has to take into account that all cases contained simulated patients. That implies that
there was more or less uniformity, i.e. the cases were not embedded in the situatedness of a
general hospital where nurses have to cope with an illness like (types of) shock. The result of
this design was that irrelevant attributes could only be addressed to a certain degree, while the
differentiation between relevant and irrelevant attributes is a key issue in the basic processes
of concept utilisation (discrimination and generalisation).
The instruction then is not rich enough to promote the formation of a prototype that can be
used as a cognitive reference point. Unless this possible shortcoming of the instruction the
students were able to discover the relevant attributes and to construct the conceptual
Chapter 4
76
knowledge. In both conditions they are able to categorise the patients into the three disease
categories.
Though the best examples of the three coordinate concepts may facilitate the construction
of knowledge if they are followed by interrogative examples it is found that the interrogative
examples only are as effective. This finding means that the knowledge construction process
benefits from the interrogative examples as such.
The results do show meaningful differences between the marked and non-marked
presentation forms. These differences involve (a) the number of responses to questions and
(b) the number of examples processed. The marked condition shows that students process
more examples, need less time and address more questions. The subjects in the marked
condition provide less correct categorisations compared to the subjects from the non-marked
condition. So attribute elaboration reduces the amount of time and facilitates the processing of
the information provided by the examples. Attribute elaboration fosters the efficiency of the
instruction, but does not improve the categorisation. The results show that the students in the
non-marked condition perform better. This might be caused by the increase of effort
necessary to find the relevant attributes in the non-marked condition and therefore to a
possibly better retention of the attributes. The student’s own activity in interpreting the
examples, thus to invest effort to construct the conceptual knowledge, seems important here.
References
Bourne, L. E. (1970). Knowing and using concepts.Psychological Review, 77, 546-556.Dwyer, F. M. (1978).Strategies for improving visual learning.Pennsylvania: State College, Learning
Services.Dwyer, F. M., & Arnold, T. A. (1976). The instructional effect of verbal/visual feedback in visualised
instruction.Journal of Psychology, 94, 39-41.Eckes, T. (1990).Psychologie der Begriffe: Strukturen des Wissens und Prozesse der Kategorisierung.
Berlin: Hogrefe.Medin, E. E., & Smith, D. L. (1981).Categories and concepts. Cambridge: Harvard University Press.Merrill, M. D., & Tennyson, R. D. (1977).Teaching concepts: An instructional design guide.
Englewood Cliffs, NJ: Educational Technology Publications.Perry & Potter, (Eds.). (1983).Shock: Comprehensive nursing management. St. Louis: The Mosby
C.V. Company.Rosch, E. (1978). Principles of categorization. In E. Rosch & B.B. Lloyd (Eds.),Cognition and
categorisation. Hillsdale, NJ: Lawrence Erlbaum Associates.Tennyson, R. D., & Cocchiarella, M. J. (1986). An empirically based instructional design theory for
teaching concepts.Review of Educational Research, 56(1), 40-71.Tennyson, R. D., Youngers, J., & Suebsonthi, P. (1983). Concept learning by children using
instructional presentation forms for prototype formation and classification-skill development.Journal of Educational Psychology, Vol. 75, No. 2, 280-291.

Best Examples and Attribute Elaboration
77
5
THE EFFECT OF DIFFERENT MODES OFACTIVATION OF PREREQUISITE
KNOWLEDGE ON THE ACQUISITION OFCOORDINATE CONCEPTS
In this chapter the influence of different modes of refreshment of prerequisiteknowledge on the acquisition of coordinate concepts is addressed. Three modes ofrefreshment are studied in an explorative way: (a) refreshment prior to theinstruction of new knowledge, (b) refreshment during instruction of newknowledge, and (c) refreshment dependent upon students' errors. Differenttheories are available to explain the facilitative effect of the prerequisiteknowledge during the learning process. Two of these theories, the elaborationtheory and the selective attention theory, were used. Elaboration, i.e. theenrichment of information due to the identification of relations between concepts,will possibly result in more easy retrieval processes. From a selective-attentionperspective it is argued that subjects with much prerequisite knowledge willattend selectively to knowledge-relevant parts of the learning content, which willbe processed more deeply. Consistent with Tennyson and Cocchiarella's view onembedded refreshment it is possible that refreshment will support new learningbut it is unclear when to practice the refreshment.

Chapter 5
78
5.1 Introduction
In this chapter the influence of different modes of refreshment of prerequisite knowledge on
the acquisition of coordinate concepts will be addressed. Refreshment of prerequisite
knowledge is one of the instructional design strategies contained in the instructional design
theory for teaching concepts of Tennyson and Cocchiarella (1986, p. 43). This theory assumes
that embedded refreshment is associated with the process of making connections in memory
between existing knowledge and the to-be-learned concepts (p. 42, 43). Embedded
refreshment is used during the instruction to help the student make connections with specific
prerequisite information that is supposed to be already in the student's memory (p. 43).
Prerequisite knowledge comprises the whole of a student's knowledge that needs to be used
for the acquisition of new knowledge and skills or that supports that acquisition. This type of
knowledge, sometimes called pre-knowledge, stored knowledge, pre-stored knowledge, prior
knowledge, archival memory, or declarative knowledge, is defined as the student’s current
knowledge that is available for the acquisition of the new knowledge. It is supposed that
prerequisite knowledge is structured in schemas, declaratively and procedurally. It contains
content knowledge and metacognitive knowledge and is of a dynamical nature (Dochy, 1993,
p. 100). Prerequisite knowledge tends to influence the following cognitive processes:
perception of new information, capacity of the student's short-term-memory, number of
elaborations and the nature of these elaborations, encoding of new information and
construction of mental representations, and retrieval and representation of new information
(see also Biemans, 1997, p. 9). In contrast to a frequently occurring practice (where the
teacher reviews prerequisite knowledge in advance) Tennyson and Cocchiarella state that
prior refreshment seems to contribute minimally to learning. First, the knowledge retrieved in
a review is not maintained in working memory once instruction begins, because of limited
storage capacity. And secondly, the presentation of prerequisite knowledge reviews the
necessary knowledge without benefit of the connections to the new information (p. 63). In
embedded refreshment the prerequisite information is presented only if the student is unable
to solve an interrogatory problem. It helps the student to recognise, recall and use the
prerequisite knowledge at the moment of acquiring the new concept. It offers help in recalling
prerequisite knowledge by placing it in working memory and by making connections between
existing knowledge and the to-be-learned information. Tennyson and Cocchiarella do not
specify how and when this can be realised and they do not predict specific effects of
Embedded Refreshment
79
embedded refreshment. For that reason this study is explorative, addressing a twofold
question: (a) when to refresh prerequisite knowledge, and (b) what effect of refreshment of
prerequisite knowledge can be found.
The activation of prerequisite knowledge is assumed to have a facilitative effect on the
learning of new material. In this study prerequisite knowledge is expected to have a
facilitative effect on the learning of the coordinate concept shock. It comprises knowledge of
the blood circulation, the heart, lungs, etc. To find a facilitative effect of prerequisite
knowledge depends on the moment at which this knowledge is presented and of the
possibilities which students are presented to refresh this knowledge. The following
possibilities are available: (a) presentation of prerequisite knowledge prior to the learning of
new knowledge (program-controlled or student-controlled), and (b) presentation of prior
knowledge during the learning process (program-controlled after students' errors, or student-
controlled simultaneous refreshment). In this study the following three conditions were
selected: (a) student-controlled refreshment in advance, (b) student-controlled simultaneous
refreshment, and (c) program-controlled error-related refreshment. In case of refreshment in
advance (student-controlled or program-controlled) the effect is studied (a) during the
learning process, and (b) after the learning process. In the first case the question is addressed
whether the learning process proceeds more efficiently, i.e. whether the students, who have
refreshed their prior knowledge, need less time for the instruction. Possibly they need less
time because they make less errors during instruction. The effectiveness of the mode of
refreshment is assessed ultimately by administering a transfer test.
The learning content to be acquired in this study was the concept 'shock'. Shock is a state
of circulatory disfunction in which tissue oxygen delivery is less than required. Based on the
cause shock can be classified into three coordinate categories: hypovolaemic, cardiogenic and
septic (see Chapter two). The clinical attributes of shock include tachycardia, hypotension -
particularly decreased diastolic blood pressure, gallop rhythm, oliguria, and altered
consciousness. Shock may be hypovolemic (insufficient intravascular volume), cardiogenic
(inadequate cardiac function), septic or vasodilatory, or due to combinations of these factors.
There is a relationship between prerequisite knowledge and the knowledge about shock
that had to be acquired. For that reason in this study different instructional strategies for the
activation of prerequisite knowledge were explored. Under different modes of refreshment
students had to verify whether the circulatory system was normal or pathologic. In the last
case they had to decide whether shock was involved; if so, they had to differentiate between
Chapter 5
80
different types of shock.
For the acquisition of new knowledge the availability of prerequisite knowledge is a
relevant variable in instruction. Prerequisite knowledge influences the acquisition of new
knowledge. During the last decades different explanations on the use, activation and effect of
prerequisite knowledge were published. Dochy (1992; 1993) categorised these explanations
into eight theories, all of them claiming to provide an explanation for the facilitative effect of
what he called prior knowledge. A few of these theories are similar or overlap. Often, as
Dochy stated, the theories explain the information processing that is necessary for learning.
For the description of the processing Mayer's (1989) model was used. This model is shown in
Figure 5.1. This model specified the components that are supposed to be the parts of the
information processing system: sensory storage, short term memory, working memory and
long term memory. The cognitive processes involved in learning were: (1) selecting
information in order to focus attention to that information; (2) organising of the entering
information in the short term memory system; (3) integrating of prerequisite knowledge from
long term memory with the new information, and (4) storage of the resulting learning
outcomes (encoding and storing) in long term memory. The availability and quality of
prerequisite knowledge influences the speed of information processing and will prevent the
students from making errors during learning.
Existing knowledge influences the acquisition of new knowledge. It seems that a well-
organised knowledge-base conceived as a set of items which are interrelated to form a
organised whole is more important than the amount of knowledge a subject has. Accessibility
of knowledge is a function of the strength of the associative links. Often, for the acquisition of
new knowledge, existing knowledge is prerequisite, else it can be supportive or it may even
inhibit the acquisition of new knowledge. It is possible that the prerequisite knowledge is
(partly) forgotten and has to be refreshed.
When students learn a new category, the learning is influenced by prerequisite knowledge.
The prerequisite knowledge can comprise knowledge of related categories but also knowledge
of a causal nature that underlies the features of a category. For example the knowledge
comprising the cause of the symptoms of a certain disease. What a person learns about a new
category is influenced by and dependent on what this person knows about other, related
categories as well as causal principles. Previous knowledge structures are re-used. It is easy to
learn a new category when it is similar to a previously known category. People's belief about
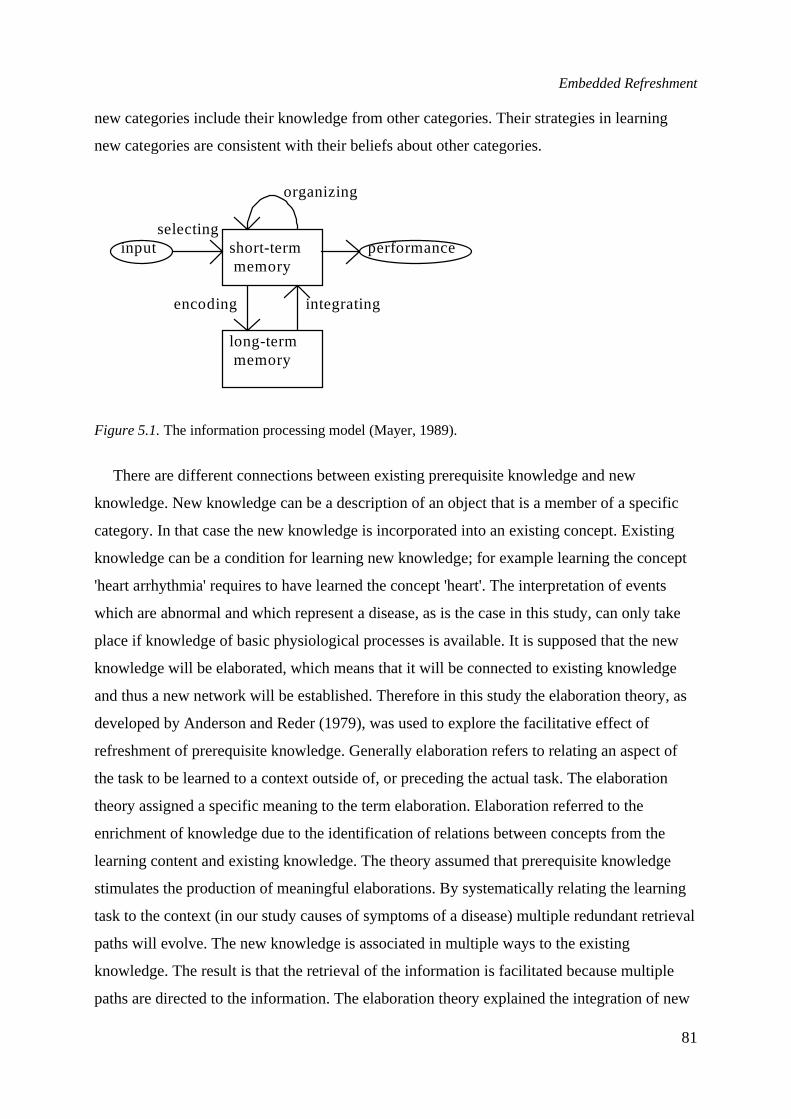
Embedded Refreshment
81
new categories include their knowledge from other categories. Their strategies in learning
new categories are consistent with their beliefs about other categories.
organizing
selectinginput short-term performance
memory
encoding integrating
long-termmemory
Figure 5.1.The information processing model (Mayer, 1989).
There are different connections between existing prerequisite knowledge and new
knowledge. New knowledge can be a description of an object that is a member of a specific
category. In that case the new knowledge is incorporated into an existing concept. Existing
knowledge can be a condition for learning new knowledge; for example learning the concept
'heart arrhythmia' requires to have learned the concept 'heart'. The interpretation of events
which are abnormal and which represent a disease, as is the case in this study, can only take
place if knowledge of basic physiological processes is available. It is supposed that the new
knowledge will be elaborated, which means that it will be connected to existing knowledge
and thus a new network will be established. Therefore in this study the elaboration theory, as
developed by Anderson and Reder (1979), was used to explore the facilitative effect of
refreshment of prerequisite knowledge. Generally elaboration refers to relating an aspect of
the task to be learned to a context outside of, or preceding the actual task. The elaboration
theory assigned a specific meaning to the term elaboration. Elaboration referred to the
enrichment of knowledge due to the identification of relations between concepts from the
learning content and existing knowledge. The theory assumed that prerequisite knowledge
stimulates the production of meaningful elaborations. By systematically relating the learning
task to the context (in our study causes of symptoms of a disease) multiple redundant retrieval
paths will evolve. The new knowledge is associated in multiple ways to the existing
knowledge. The result is that the retrieval of the information is facilitated because multiple
paths are directed to the information. The elaboration theory explained the integration of new
Chapter 5
82
information with existing knowledge by assuming that the more prerequisite knowledge is
available the more elaborations can be produced.
Anderson and Reder studied the problem of relating new, potentially meaningful material
to an assimilative context of existing knowledge in terms of elaboration. They argue that "the
variation in memory with depth of processing is a result of the number of elaborations
subjects produce while studying the material, that these elaborations establish more redundant
encodings of the to-be-remembered information, and that elaboration is what is critical,
especially for long-term retention" (p. 385). They predicted that subjects engaged in deep
processing will perform better and they hypothesised that processing information at various
depths results in different types of traces being left in memory. Instructional processes
designed to affect the depth of processing will have effect dependent on the number and type
of elaborations. The underlying assumption of Anderson and Reder was that they conceived
the long-term memory as a network of interconnected propositions and, secondly, that the
subject adds propositions to that network. At the minimum, the learner adds propositions
encoding the memory items. If the learner encodes multiple propositions that are partially
redundant with the to-be-remembered information, the learner will have a better chance of
recalling it later.
Anderson and Reder developed a reconstructive interpretation of memory. A memory
episode is assumed to be encoded as a set of propositions. This set of propositions can vary in
richness and redundancy. For recall only a subset of the propositions will be activated. The
richer the original set, the richer the subset. Memory for any proposition depends on the
subjects' ability to reconstruct it from propositions that are active (p. 388). A learner's
elaborative capabilities are a function of the cognitive procedures to develop elaborations;
these procedures come into existence through real-world experience with objects. So a
learner's prior practice at making elaborations about various types of information and practice
at interpreting the previously stored elaborations is important. The better processing is that
which generates more elaborations of the input (p. 390). Anderson and Reder assumed that
the enrichment of information with prerequisite-knowledge based elaborations results in
multiple redundant retrieval paths in the cognitive representation. The existence of these
retrieval paths is assumed to facilitate coded information at recall. The same applies for
inferences based on prerequisite knowledge. These inferences facilitate to make the incoming
information meaningful and will function as expectations about information that has still to be
processed.

Embedded Refreshment
83
The elaboration theory does not provide instructional design rules. If elaborations will help
to connect new to existing knowledge it is plausible to activate the knowledge in advance and
to prevent the student from making errors. But the knowledge can be forgotten or not
contained in the working memory at the right moment. Thus embedded refreshment seems
better in case of having made errors. The conclusion is that it is unclear when activation has
the most effect. Exploration is necessary.
Separate from the elaboration theory a second theory, the selective attention theory
(Dochy, 1993, p. 108), will be used to explore the refreshment of prerequisite knowledge.
From the selective-attention theory it was assumed that subjects with much prerequisite
knowledge will attend selectively to prerequisite knowledge-relevant parts of the learning
content, which will be processed deeply. Thus activation of prerequisite knowledge has
mainly a controlling function, in that relevant information gets more attention to the expense
of the study of less relevant information. The selective attention theory stated that subjects
with much prerequisite knowledge focus their attention selectively on prerequisite knowledge
that is relevant for learning. The learning content will be processed meaningfully. The process
of selecting new information will be influenced by salient features of the learning content. If
the prerequisite knowledge is incorrect the wrong information will be selected. In case of
incorrect prerequisite knowledge misconceptions are involved. Students connect the new
information to these misconceptions or store new information fragmentally (Ali, 1990). Then
a ‘corpus alienum’ will emerge: new knowledge forms a separate record, which will be
attached to an existing record, but will not be integrated therein. Ali concluded that the
activation of prerequisite knowledge prior to the instruction is not sufficient to produce
facilitative effects of prerequisite knowledge. This is consistent with the assumption of
Tennyson and Cocchiarella (1986). They proposed embedded refreshment. However it is
unclear how to do this. Consistent with their view on embedded refreshment it might be
expected that simultaneous refreshment and error-related refreshment of prerequisite
knowledge will produce better transfer results (in terms of number correct responses,
processing time) compared to the advance refreshment. Simultaneous refreshment and error-
related refreshment make a direct connection between the attributes of shock and the
knowledge of the circulatory system. In case of refreshment of prerequisite knowledge during
instruction and in case of error-related activation of prerequisite knowledge elaboration and
attention focussing were expected to take place more easily. The refreshment of prerequisite
Chapter 5
84
knowledge prior to the instruction will possibly contribute less to the learning process due to
not directly linking the causes and the symptoms of the disease shock.
In order to assess the effect of variation of refreshment of prerequisite knowledge an
instructional program was developed. This program was an interactive video about the
categorisation of shock (see Chapter two). Within the experiment three different conditions
were designed: (1) refreshment prior to the instruction, (2) presenting new information and
simultaneously refreshment of prerequisite knowledge which was student-controlled and (3)
error-related refreshment of prerequisite knowledge. The results of the exploration will be
explained within the theories discussed.
5.2 Method
5.2.1 Subjects
Sixty-two second year students from a school for nursing education participated in the
experiment. Because all students passed the prerequisite knowledge tests in the first year they
were randomly assigned to the different instructional conditions. Seventeen students were
male, forty five were female. The age of the students varied from 19 to 24 years. Before
entering the nursing school all students finished either a school for Senior Secondary
Vocational Education, a school for Senior General Secondary Education, or a school for Pre-
University Education. Participation was obligatory and the program was part of the nursing
curriculum.
5.2.2 Material
The coordinate concept shock, that is described in chapter two, formed the content of the
instructional programs. The students had to acquire the concept and to categorise videos of
shock patients into three coordinate categories of shock. The program contained twenty eight
interrogative examples or non-examples. Each interrogative example or non-example
contained twelve to fourteen questions about the relevance for categorisation of more or less
salient attributes of the patient. Each interrogative example contained one question about the
nature of the patient’s illness (see for further information Chapter 2). The prerequisite
knowledge about the vascular system, circulation, heart system and (the measurement of)
relevant variables was described in a glossary, which is contained in Appendix C.
Embedded Refreshment
85
5.2.3 Apparatus
The instructions which were partly student-controlled and partly program-controlled, were
presented with an Apple Macintosh II computer. All data were stored automatically. The
videos of the patients were stored on a videodisk and presented together with the written
instructions. For the presentation of the videos a videodisk player (Video Logic DVA 4000)
was used which was computer-controlled.
5.2.4 Implementation of the instructional-design model for interactive video
For the presentation of the instructional material two screen lay outs were used, the standard
screen and a special screen that was designed for the refreshment of prerequisite knowledge.
Screen dumps of both screens are included in chapter two. A schematic representation of the
special screen is shown in Figure 5.2. In the condition advance refreshment of prerequisite
knowledge, the program started with this screen. In the simultaneous refreshment condition
this screen was provided simultaneous with the instruction, whereas in the error-related
refreshment condition this screen was presented dependent on the type of categorisation error.
Advance refreshment.In this condition the glossary with fifty four keywords was presented on
the upper right-hand side. Scrolling through this list was at the students' own decision. If the
students wanted to inspect a keyword they had to point to that keyword with the mouse and
then an exposition of the meaning of that keyword was presented. The text of the keyword
was presented on the lower left-hand side of the screen. In case of too long texts scrolling was
possible. Each keyword referred to adjacent keywords. Adjacent keywords could be
superordinate-, subordinate-, and possibly relevant coordinate keywords. These adjacent
keywords were presented on the lower right-hand side of the screen. If the students wanted to
inspect one or more of these keywords, these keywords could be activated from the lower
right-hand side of the screen. When the icon “Stop” was activated this action had to be
confirmed. After that confirmation the presentation of interrogatory examples proceeded.
Simultaneous refreshment.In this condition the prerequisite knowledge was presented parallel
to the instruction. In order to achieve this the students got the opportunity to activate the base
of prerequisite knowledge at each moment. For that purpose on the lower right-hand side of
the screen an (extra) button “K” (Knowledge) was presented (see Figure 2.5). In the Help-
menu as well as in the User Manual the function of “K” was explained. By clicking the button
an alphabetically ordered list of keywords was presented in the same way as in the advance
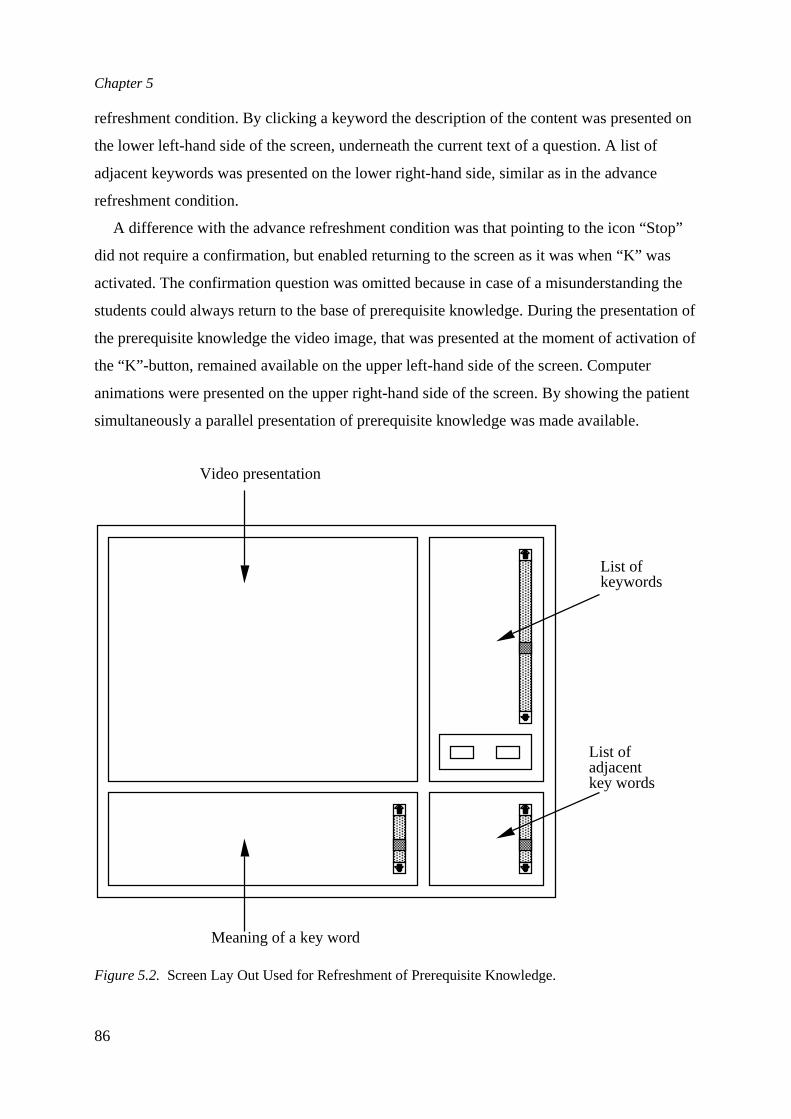
Chapter 5
86
refreshment condition. By clicking a keyword the description of the content was presented on
the lower left-hand side of the screen, underneath the current text of a question. A list of
adjacent keywords was presented on the lower right-hand side, similar as in the advance
refreshment condition.
A difference with the advance refreshment condition was that pointing to the icon “Stop”
did not require a confirmation, but enabled returning to the screen as it was when “K” was
activated. The confirmation question was omitted because in case of a misunderstanding the
students could always return to the base of prerequisite knowledge. During the presentation of
the prerequisite knowledge the video image, that was presented at the moment of activation of
the “K”-button, remained available on the upper left-hand side of the screen. Computer
animations were presented on the upper right-hand side of the screen. By showing the patient
simultaneously a parallel presentation of prerequisite knowledge was made available.
List ofkeywords
Video presentation
Meaning of a key word
List ofadjacentkey words
Figure 5.2. Screen Lay Out Used for Refreshment of Prerequisite Knowledge.
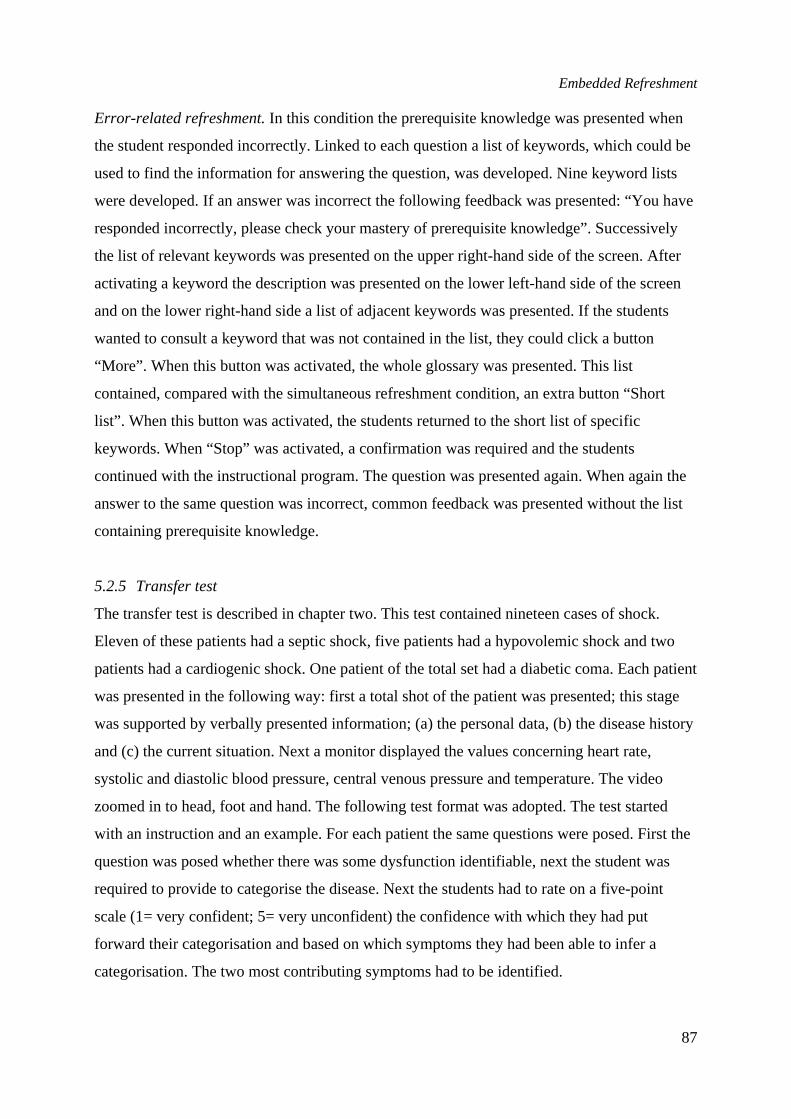
Embedded Refreshment
87
Error-related refreshment.In this condition the prerequisite knowledge was presented when
the student responded incorrectly. Linked to each question a list of keywords, which could be
used to find the information for answering the question, was developed. Nine keyword lists
were developed. If an answer was incorrect the following feedback was presented: “You have
responded incorrectly, please check your mastery of prerequisite knowledge”. Successively
the list of relevant keywords was presented on the upper right-hand side of the screen. After
activating a keyword the description was presented on the lower left-hand side of the screen
and on the lower right-hand side a list of adjacent keywords was presented. If the students
wanted to consult a keyword that was not contained in the list, they could click a button
“More”. When this button was activated, the whole glossary was presented. This list
contained, compared with the simultaneous refreshment condition, an extra button “Short
list”. When this button was activated, the students returned to the short list of specific
keywords. When “Stop” was activated, a confirmation was required and the students
continued with the instructional program. The question was presented again. When again the
answer to the same question was incorrect, common feedback was presented without the list
containing prerequisite knowledge.
5.2.5 Transfer test
The transfer test is described in chapter two. This test contained nineteen cases of shock.
Eleven of these patients had a septic shock, five patients had a hypovolemic shock and two
patients had a cardiogenic shock. One patient of the total set had a diabetic coma. Each patient
was presented in the following way: first a total shot of the patient was presented; this stage
was supported by verbally presented information; (a) the personal data, (b) the disease history
and (c) the current situation. Next a monitor displayed the values concerning heart rate,
systolic and diastolic blood pressure, central venous pressure and temperature. The video
zoomed in to head, foot and hand. The following test format was adopted. The test started
with an instruction and an example. For each patient the same questions were posed. First the
question was posed whether there was some dysfunction identifiable, next the student was
required to provide to categorise the disease. Next the students had to rate on a five-point
scale (1= very confident; 5= very unconfident) the confidence with which they had put
forward their categorisation and based on which symptoms they had been able to infer a
categorisation. The two most contributing symptoms had to be identified.
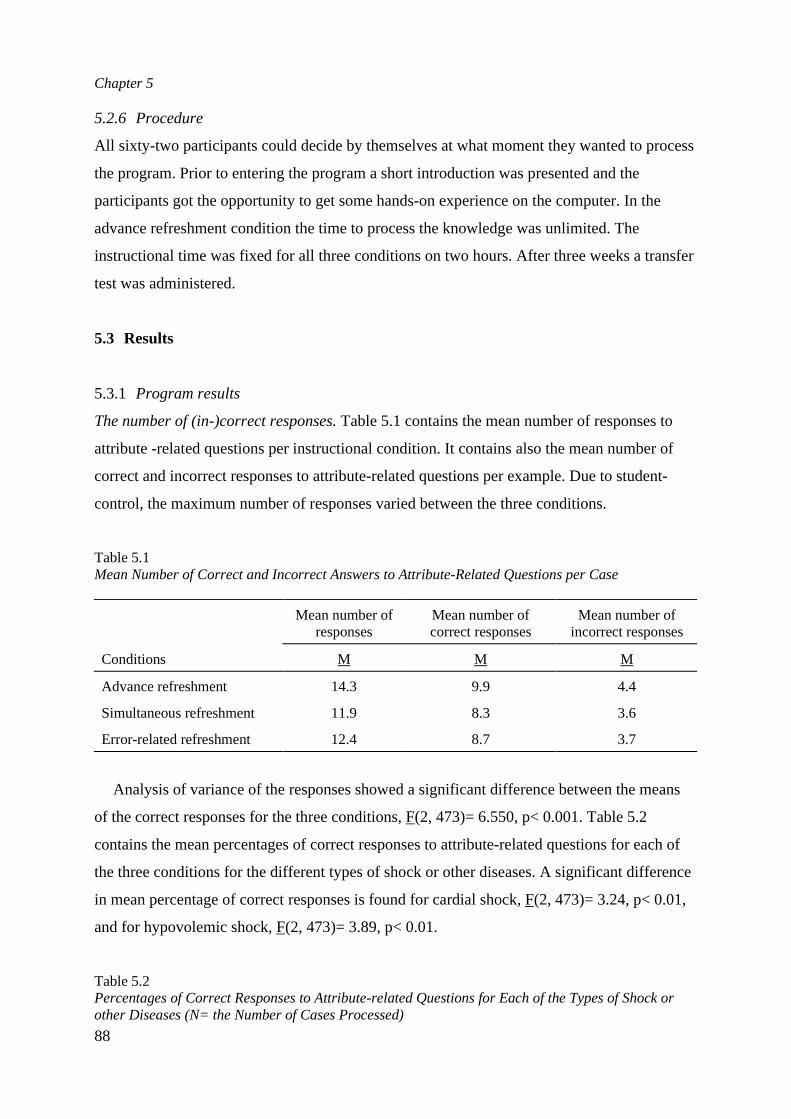
Chapter 5
88
5.2.6 Procedure
All sixty-two participants could decide by themselves at what moment they wanted to process
the program. Prior to entering the program a short introduction was presented and the
participants got the opportunity to get some hands-on experience on the computer. In the
advance refreshment condition the time to process the knowledge was unlimited. The
instructional time was fixed for all three conditions on two hours. After three weeks a transfer
test was administered.
5.3 Results
5.3.1 Program results
The number of (in-)correct responses.Table 5.1 contains the mean number of responses to
attribute -related questions per instructional condition. It contains also the mean number of
correct and incorrect responses to attribute-related questions per example. Due to student-
control, the maximum number of responses varied between the three conditions.
Table 5.1Mean Number of Correct and Incorrect Answers to Attribute-Related Questions per Case
Mean number ofresponses
Mean number ofcorrect responses
Mean number ofincorrect responses
Conditions M M M
Advance refreshment 14.3 9.9 4.4
Simultaneous refreshment 11.9 8.3 3.6
Error-related refreshment 12.4 8.7 3.7
Analysis of variance of the responses showed a significant difference between the means
of the correct responses for the three conditions, F(2, 473)= 6.550, p< 0.001. Table 5.2
contains the mean percentages of correct responses to attribute-related questions for each of
the three conditions for the different types of shock or other diseases. A significant difference
in mean percentage of correct responses is found for cardial shock, F(2, 473)= 3.24, p< 0.01,
and for hypovolemic shock, F(2, 473)= 3.89, p< 0.01.
Table 5.2Percentages of Correct Responses to Attribute-related Questions for Each of the Types of Shock orother Diseases (N= the Number of Cases Processed)
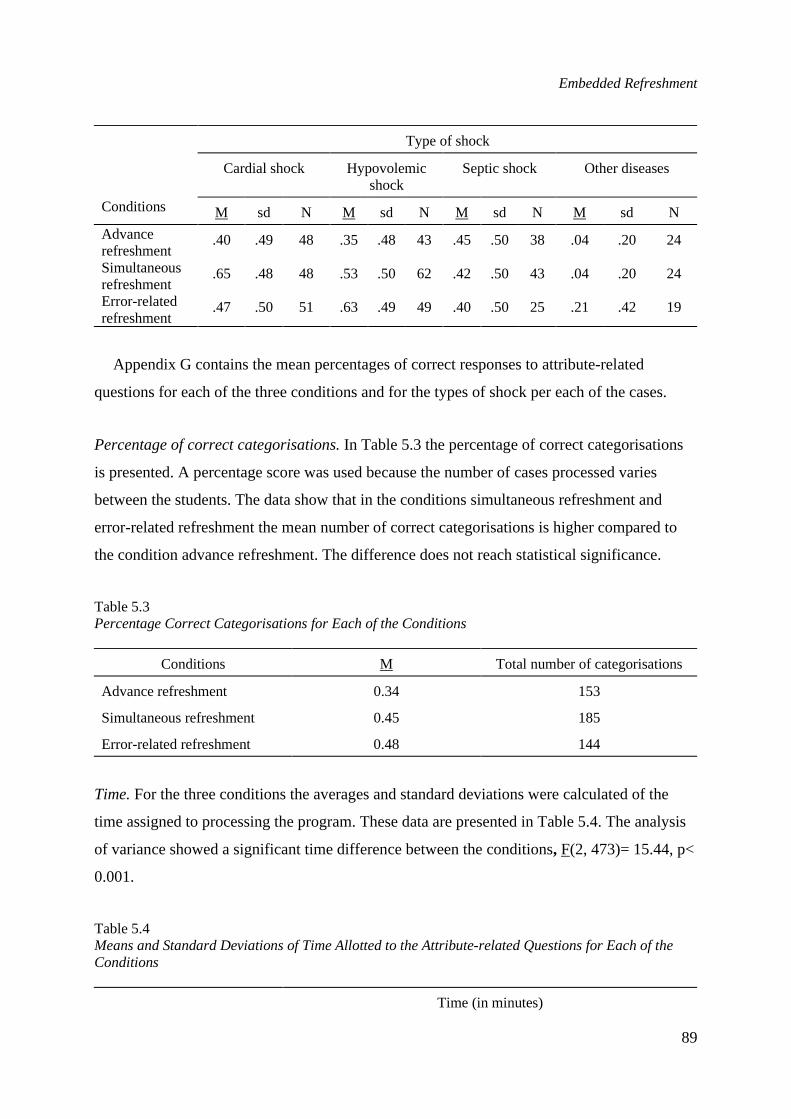
Embedded Refreshment
89
Type of shock
Cardial shock Hypovolemicshock
Septic shock Other diseases
Conditions M sd N M sd N M sd N M sd N
Advancerefreshment
.40 .49 48 .35 .48 43 .45 .50 38 .04 .20 24
Simultaneousrefreshment
.65 .48 48 .53 .50 62 .42 .50 43 .04 .20 24
Error-relatedrefreshment
.47 .50 51 .63 .49 49 .40 .50 25 .21 .42 19
Appendix G contains the mean percentages of correct responses to attribute-related
questions for each of the three conditions and for the types of shock per each of the cases.
Percentage of correct categorisations.In Table 5.3 the percentage of correct categorisations
is presented. A percentage score was used because the number of cases processed varies
between the students. The data show that in the conditions simultaneous refreshment and
error-related refreshment the mean number of correct categorisations is higher compared to
the condition advance refreshment. The difference does not reach statistical significance.
Table 5.3Percentage Correct Categorisations for Each of the Conditions
Conditions M Total number of categorisations
Advance refreshment 0.34 153
Simultaneous refreshment 0.45 185
Error-related refreshment 0.48 144
Time.For the three conditions the averages and standard deviations were calculated of the
time assigned to processing the program. These data are presented in Table 5.4. The analysis
of variance showed a significant time difference between the conditions, F(2, 473)= 15.44, p<
0.001.
Table 5.4Means and Standard Deviations of Time Allotted to the Attribute-related Questions for Each of theConditions
Time (in minutes)
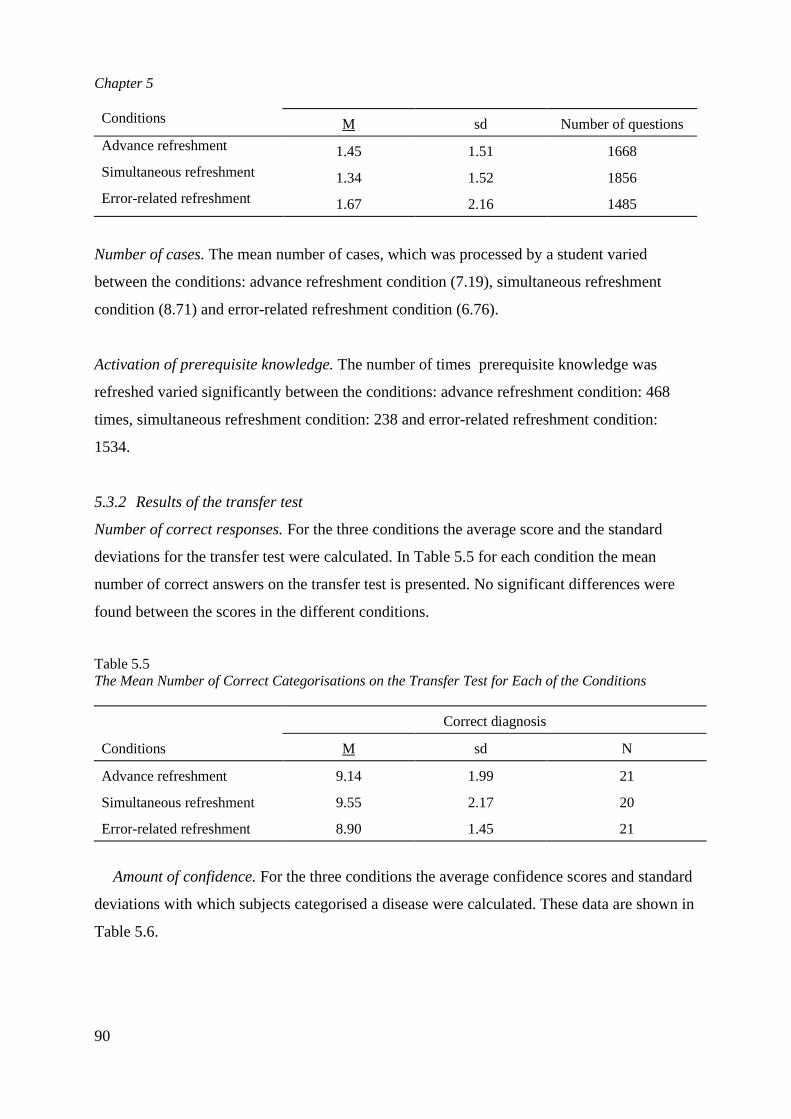
Chapter 5
90
Conditions M sd Number of questions
Advance refreshment 1.45 1.51 1668
Simultaneous refreshment 1.34 1.52 1856Error-related refreshment 1.67 2.16 1485
Number of cases.The mean number of cases, which was processed by a student varied
between the conditions: advance refreshment condition (7.19), simultaneous refreshment
condition (8.71) and error-related refreshment condition (6.76).
Activation of prerequisite knowledge.The number of times prerequisite knowledge was
refreshed varied significantly between the conditions: advance refreshment condition: 468
times, simultaneous refreshment condition: 238 and error-related refreshment condition:
1534.
5.3.2 Results of the transfer test
Number of correct responses.For the three conditions the average score and the standard
deviations for the transfer test were calculated. In Table 5.5 for each condition the mean
number of correct answers on the transfer test is presented. No significant differences were
found between the scores in the different conditions.
Table 5.5The Mean Number of Correct Categorisations on the Transfer Test for Each of the Conditions
Correct diagnosis
Conditions M sd N
Advance refreshment 9.14 1.99 21
Simultaneous refreshment 9.55 2.17 20
Error-related refreshment 8.90 1.45 21
Amount of confidence.For the three conditions the average confidence scores and standard
deviations with which subjects categorised a disease were calculated. These data are shown in
Table 5.6.
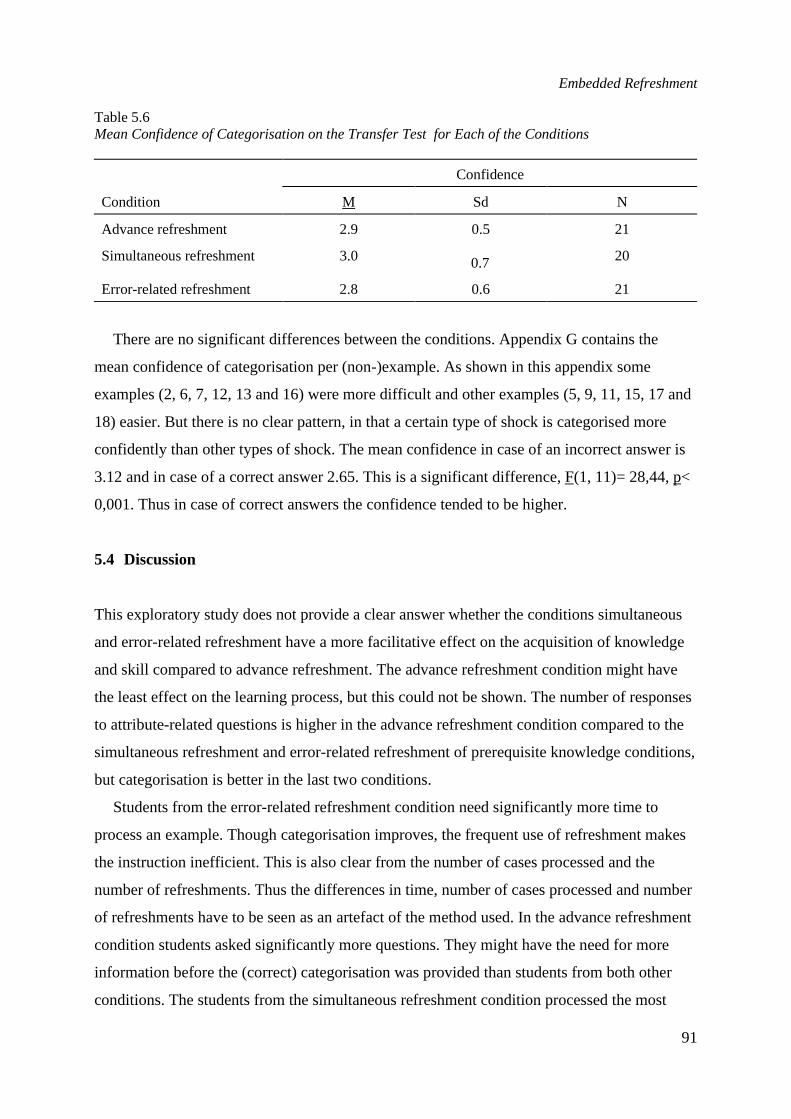
Embedded Refreshment
91
Table 5.6Mean Confidence of Categorisation on the Transfer Test for Each of the Conditions
Confidence
Condition M Sd N
Advance refreshment 2.9 0.5 21
Simultaneous refreshment 3.0 0.7 20
Error-related refreshment 2.8 0.6 21
There are no significant differences between the conditions. Appendix G contains the
mean confidence of categorisation per (non-)example. As shown in this appendix some
examples (2, 6, 7, 12, 13 and 16) were more difficult and other examples (5, 9, 11, 15, 17 and
18) easier. But there is no clear pattern, in that a certain type of shock is categorised more
confidently than other types of shock. The mean confidence in case of an incorrect answer is
3.12 and in case of a correct answer 2.65. This is a significant difference, F(1, 11)= 28,44, p<
0,001. Thus in case of correct answers the confidence tended to be higher.
5.4 Discussion
This exploratory study does not provide a clear answer whether the conditions simultaneous
and error-related refreshment have a more facilitative effect on the acquisition of knowledge
and skill compared to advance refreshment. The advance refreshment condition might have
the least effect on the learning process, but this could not be shown. The number of responses
to attribute-related questions is higher in the advance refreshment condition compared to the
simultaneous refreshment and error-related refreshment of prerequisite knowledge conditions,
but categorisation is better in the last two conditions.
Students from the error-related refreshment condition need significantly more time to
process an example. Though categorisation improves, the frequent use of refreshment makes
the instruction inefficient. This is also clear from the number of cases processed and the
number of refreshments. Thus the differences in time, number of cases processed and number
of refreshments have to be seen as an artefact of the method used. In the advance refreshment
condition students asked significantly more questions. They might have the need for more
information before the (correct) categorisation was provided than students from both other
conditions. The students from the simultaneous refreshment condition processed the most

Chapter 5
92
cases. There is no evidence that the condition error-related refreshment condition has more
effect on the acquisition of knowledge and skills than the conditions advance refreshment and
simultaneous refreshment. The data also show that the number of responses was higher in the
advance refreshment condition compared to the simultaneous refreshment condition and the
condition error-related refreshment. The data show that in the condition error related
refreshment less correct responses to attribute-related questions were provided compared to
the other two conditions, while the mean percentage of correct categorisations were higher in
this condition compared to both other conditions.
The research question underlying this exploration was at what moment, in the instructional
process is the refreshment of prerequisite knowledge most effective. In order to provide an
answer to this question data collected during the instruction, the categorisation, the
refreshment of prerequisite knowledge and the transfer test are used. In the condition error-
related refreshment a more frequent use of prerequisite knowledge is found, because this is
simply based on errors. At the moment that students provide an incorrect answer they are
referred to the (list of) keywords. During the instruction students in the condition
simultaneous refreshment tend to process more examples (M= 8.71) than in the conditions
advance refreshment (M= 7.19) and error-related refreshment (M= 6.76). In the simultaneous
refreshment condition they tend to assign less time to answer the questions for each example.
In case of student-control the students only refresh the knowledge if necessary. Making an
error sometimes reminds the students already what is correct.
In the condition advance refreshment more questions are answered than in the conditions
simultaneous and error-related refreshment. But in the conditions simultaneous refreshment
and error-related refreshment more questions are answered correctly, though the results are
not significant. This finding can be explained from the point of view that the students from
the conditions simultaneous refreshment and error-related refreshment can respond more
focused because they had the possibility to attend to those keywords which were linked to the
instructional content at a certain moment. Students in the condition advance refreshment
possibly guess more easily in responding to a question because the keywords were no longer
available. The time allotted to categorisation is longer in the condition advance refreshment.
But in the simultaneous refreshment and error-related conditions the time used is more or less
similar. In the condition error-related refreshment the categorisation during the instructional
part is more frequently correct compared to the condition simultaneous refreshment. This
difference however does not reach significance. On the transfer test students from the
Embedded Refreshment
93
condition simultaneous refreshment perform a little better than students from the conditions
prior refreshment and error-related refreshment. This is mirrored in more confidence in the
correctness of the answer.
The results from this exploration provide only some support for Tennyson and
Cocchiarella’s assumption that embedded refreshment of prerequisite knowledge is more
effective in comparison with refreshment of prerequisite knowledge in advance. Which form
of embedded refreshment is more effective (student-controlled as in the condition
simultaneous refreshment or program-controlled as in the condition error-related refreshment)
cannot be inferred from the data. What is more clear is that error-related refreshment is time
consuming and inefficient.
The findings support the elaboration theory. Practising retrieval paths has a facilitative
effect on categorisation. Simultaneous refreshment is more efficient. Error-related
refreshment of prerequisite knowledge is less efficient but tends to provide a correct
categorisation earlier than other kinds of refreshment, probably because the possible retrieval
paths are practised.
The mean number of responses to attribute-related questions is significantly higher in the
advance refreshment condition compared to simultaneous refreshment and error-related
refreshment, but the percentage of correct categorisations in the conditions simultaneous
refreshment and error-related refreshment is higher compared to the advance refreshment
condition. The findings show that advance refreshment causes the student to ask more
questions. This means that in the activation of prerequisite knowledge in advance does not
guide the students to the most relevant information of the content to be learned. Thus the
advance refreshment does not foster the selective attention. It is argued that the content of the
glossary of prerequisite knowledge is processed more deeply in the conditions simultaneous
refreshment and error-related refreshment, though no specific techniques for attention
focussing (e.g. contrast, underlining, and so on) were used in this study.
Summarising, the direction of the results is that the refreshment of prerequisite knowledge,
based on Tennyson and Cocchiarella' s embedded refreshment, is more effective than
refreshment prior to the instruction, but more research is needed to find at what moment
during the instruction is the refreshment of prerequisite knowledge the most effective.
Chapter 5
94
References
Ali, K. S. (1990).Instructiestategieën voor het activeren van preconcepties.Helmond: Wibro.Anderson, J. R., & Reder, L. M. (1979). An elaborative processing explanation of depth of processing.
In S. Cermak & F .I. M. Craik (Eds.),Levels of processing in human memory. Hillsdale, NJ:Lawrence Erlbaum Associates.
Biemans, H. J. A. (1997). Fostering activation of prior knowledge and conceptual change. Nijmegen:Catholic University Nijmegen. Doctoral Dissertation.
Dochy, F. J. R. C. (1992).Assessment of prior knowledge as a determinant for future learning; the useof prior knowledge state tests and knowledge profiles.Heerlen: Centre for Educational Technologyand Innovation. Open University of the Netherlands.
Dochy, F. J. R. C. (1993). De invloed van voorkennis op het leerresultaat en het leerproces. In W.Tomic & P. Span (Eds.),Onderwijspsychologie; Beïnvloeding, verloop en resultaten vanleerprocessen.Utrecht: Lemma B.V.; Open Universiteit Heerlen.
Mayer, R. E. (1989). Elaboration techniques that increase the meaningfulness of technical text: anexperimental test of the learning strategy hypothesis.Journal of Educational Psychology, 72,770-784.
Tennyson, R. D., & Cocchiarella, M. (1986). An empirically based instructional design theory forteaching concepts.Review of Educational Research, 56,40-71.



6
GENERAL DISCUSSION
This chapter contains a reflection on this study. The theory and the model arediscussed in terms of the data. The concept teaching model of Tennyson andCocchiarella (1986) was developed based on the concept formation theory ofRosch (1978). In that period Lakov (1987) developed his ideas aboutexperientialism and objectivism, also based on the concept formation theory ofRosch. The work of Lakov was used by Jonassen (1992) to discuss theapplicability of constructivistic ideas in instructional design. Knowledgeconstruction is necessary if the concept teaching model of Tennyson andCocchiarella is used. Some design variables of that teaching model weremanipulated in this study and their effect on program scores as well as on transferscores was studied. A medical concept was used. This concept was presentedusing videotaped, simulated patients. For the transfer test videotaped real patientswere used. For the second and third experiment a multimedia environment wasdeveloped. The instruction was for students of a nursing college, who are requiredto recognise shock as quickly as possible. It is concluded that the conceptteaching model of Tennyson and Cocchiarella is an adequate context to designinstruction for learning concepts.
Chapter 6
96
6.1 Tennyson and Cocchiarella's Concept Teaching Model
This study is based on the concept teaching model of Tennyson and Cocchiarella (1986). The
model was developed in a period of growing criticism on existing instructional-design
models, because they were often insufficiently grounded in cognitive learning theory and did
not make explicit the epistemological assumptions of the authors explicit. Tennyson and
Cocchiarella based their model on the concept formation theory of Rosch (1978). This theory
thoroughly influenced the reflection on knowledge acquisition. One year after Tennyson and
Cocchiarella published their concept teaching model Lakov (1987) published his ideas on
experientialism and objectivism. According to Lakov, who's view is based on the studies of
Rosch, the traditional view sees reason as primarily about propositions that can be
objectively either true or false. Lakov's view takes mental imagery as central to reason. In the
traditional account meaningful concepts exist abstractly, independent of any particular
embodiment. In the new view, meaning is a matter of what is meaningful to thinking,
functioning beings. According to Lakov categories on the objectivistic view are characterised
solely by the attributes shared by the members. This view is tied to the theory that categories
are defined in terms of common attributes of their members. In the objectivistic view, all
rational thought involves the manipulation of abstract symbols. To a very large extent, the
objectivist view of language and thought rests on the nature of categories. Things are in the
same category if and only if they have certain attributes in common. Those attributes are
necessary and sufficient conditions for defining the category. Lakov's view, called
experiential realism or experientialism, is that (a) thought is embodied, i.e. the structures
used to put together our conceptual systems grow out of experience and make sense in terms
of it, (b) thought is imaginative, in that many concepts go beyond mirroring or representation
of external reality, (c) thought is not atomistic, (d) thought has an ecological structure, (d)
conceptual structure can be described using cognitive models, (e) the theory of cognitive
models incorporates what was right about the traditional view of categorisation, meaning and
reason, while accounting for the empirical data on categorisation and fitting the new view.
Using the term experiential realism Lakov emphasises what experientialism shares with
objectivism. According to Lakov prototype theory is changing our idea of the most
fundamental of human capacities and with it, our idea of what the human mind and human
reason are like.
In Lakov's work the results of the research Rosch has done are used as convincing
evidence for his epistemology. A few years later Lakov's ideas were used by Jonassen
General Discussion
97
(1991), who changed the label experientialism into constructivism, a label which already was
used in epistemology.
Though Tennyson and Cocchiarella do not make explicit their epistemological
assumptions it becomes clear from their description of the model that the students should
induce and construct concepts by solving categorisation problems. This means that they have
to perceive and study the attributes of objects and then categorise them. Construction of
knowledge is also necessary if the concept teaching model of Tennyson and Cocchiarella is
applied. A number of components of this model can be conceived as constant (like
label/definition), while other components (like type of example, number of examples of a
certain type, the moment of refreshment of prior knowledge, saliency of attributes) can be
conceived as design variables. These design variables were manipulated in this study and
their effect on program scores and transfer scores were studied. A medical concept was
taught, using videotaped and simulated patients. For the transfer test videos of real patients
were used. For the experiments described in the chapters four and five a multimedia
environment was designed. The instruction was for nurses who are required to recognise
patients with circulation disorders as quickly as possible in order to refer them to a medical
specialist.
Tennyson and Cocchiarella view concept learning as a two-phase process: (a) formation of
conceptual knowledge, and (b) development of procedural knowledge. The two main
components of the model are: (a) content structure variables and (b) instructional design
variables. There are four instructional design strategies. These are intended to avoid the three
kinds of classification errors: (a) overgeneralisation, (b) undergeneralisation, and (c)
misconception. The use of the concept teaching model of Tennyson and Cocchiarella requires
that the domain's content structure should be analysed according to two conditions: (a) the
relational structure between concepts, and (b) the variability of the attribute characteristics of
each concept. The relational structure between concepts is based on their production rules
(associated with generalisation and discrimination). Successive and coordinate relations
determine the domain's structure (Tennyson & Cocchiarella, 1986, p. 42).
The learning content to be acquired in this study comprised three coordinate concepts.
Content structures which include coordinate relationships, primarily develop procedural
knowledge, which improves the formation of connections between concepts (Tennyson &
Cocchiarella, p. 42). The instructional design variables of label/definition, context and
embedded refreshment are associated with the process of making connections in memory
Chapter 6
98
between existing knowledge and the to-be-learned concepts (Tennyson & Cocchiarella, p.
42, 43). The variables of label and definition usually are attempts to make initial connections
with prerequisite knowledge by direct reference in the definition to appropriate prerequisite
information (p. 43). The context variable establishes additional connections with associative
and background knowledge (p. 43). Embedded refreshment, unlike the first two design
variables, is used during the instruction to help the learner make connections with specific
prerequisite information that is assumed to be already in the learner's memory (p. 43). Best
examples and expository examples are primarily concerned with storage of the to-be-learned
information (p. 43). Interrogatory examples, strategy information and attribute elaboration
deal directly with development of production rules for (retrieval in) problem solving (p. 43).
The process of concept teaching is threefold: (a) establish a connection in memory
between to-be-learned concepts and specific necessary knowledge, (b) improve formation of
conceptual knowledge and elaborate the schematic structure of relational concepts, and (c)
improve the development of procedural knowledge (classification rule using (p. 43, 44). The
first phase is improved by the instructional variables of (a) best examples and (b) directions
to use the best example with expository examples (p. 47). The second phase is improved
through the practice of comparing and contrasting the coded conceptual knowledge with
newly encountered interrogatory examples (p. 47). With coordinate concepts, it is important
to present the concepts simultaneously. Concepts organised as coordinate require procedural
knowledge to discriminate between newly encountered examples as well as the ability to
generalise (p. 52). Typically, refreshing necessary knowledge is done in a review prior to the
instruction. From a cognitive view prior refreshment of necessary knowledge seems to
contribute minimally to learning. First, the knowledge is retrieved in a review is not
maintained in working memory once instruction begins, because of limited storage capacity.
And second, reviewing the necessary knowledge in advance does not result in a benefit of
the connections to the new information (p. 63). Embedded refreshment presents the
prerequisite information only if the student is unable to solve an interrogatory problem. It
helps the student recognise, recall and use the prerequisite knowledge at the moment of
acquiring the new concept. It offers help in recalling prerequisite knowledge by placing it in
working memory and by making connections between existing knowledge and the to-be-
learned information.
The concept teaching model of Tennyson and Cocchiarella has four main concept
teaching strategies of which Strategy 2 (see Chapter one, Table 1.1) was used in this study.
General Discussion
99
This strategy has the following components: (a) labels and definitions, (b) best examples, (c)
expository examples (simultaneous presented), (d) interrogatory examples, (e) attribute
elaboration, and (d) embedded refreshment. Some components are fixed whereas others can
vary during instruction. The effect of the following variable components of the model was
studied in three experiments: (a) best examples, (b) expository/interrogatory examples and
attribute elaboration, and (c) embedded refreshment.
6.2 Overall discussion of the results
First experiment.In the first study (see Chapter three) the component 'best examples' is
varied. The results of this first experiment show that only enumeration of attributes does not
enable learning to categorise. There is clear evidence that prototype formation has a
facilitative effect. It is necessary that for categorisation (representations of) objects are
available. An enumeration of defining attributes does not suffice. The results of the post-test
indicate that students from the text-only condition performed a little better on the definition
component of this test. On the categorisation component students from the text + video
component performed markedly better. This may be attributed to the development of a
prototype. The results of the retention test indicate that on the component labelling students
from the text + video condition performed better; the same applies for the inference
component and the classification component. The mean scores on the retention test as a
whole differed markedly. There is an indication that students benefit from the typical
examples presented by video. Thus if in the prototype condition (text + video) typical cases of
shock encompassing defining as well as irrelevant attributes were presented, this resulted in
an increase of the capability to discriminate between different types of shock and of the
capability to generalise to new examples of shock. Data-analysis of the post-test scores do not
yield differences in performance on definition and attributes of different types of shock. A
significant difference is found in inferring type of shock. The retention test yields that
discrimination between shock and other diseases and identifying the most salient attributes of
shock yields a significant difference. The mean scores differ significantly on identification of
shock in terms of commonalties and differences between types of shock. The overall scores of
the retention test provide a significant difference in favour of prototype -based instruction.
Second experiment. In the second study (see Chapter four) the components 'expository and/or
interrogatory examples' as well as 'attribute elaboration' are varied. The results of the second

Chapter 6
100
experiment do not provide clear answers for the use of best expository examples. Only a few
weak trends are found In the expository condition the average percentage of all examples
processed is less than in the interrogatory condition. For the expository condition the average
percentage of correct responses to questions preceding categorisation is only slightly higher
compared to the interrogatory condition and does not reach significance. The average
percentage of correct categorisations for the expository condition is lower, though this
difference also is not significant. The average amount of time the subjects spent to study an
example in the expository condition is slightly higher compared to the interrogatory
condition. This difference is not significant. The average percentage of all examples
processed in the marked condition is higher compared to the non-marked condition. A trend
in favour of marking of the attributes is found. This result shows the effectiveness of attention
focussing devices. For the marked condition the average percentages of correct responses to
questions preceding categorisation is slightly higher compared to the non-marked condition,
though this difference is not significant. The average percentage of correct categorisations for
the marked condition is a little less, though this difference is not significant. The analysis of
variance indicates that attribute elaboration contributes significantly to processing examples
efficiently. Marking does increase the number of examples processed. The students elaborate
the relevant attributes. The results show that students in the expository-marked condition
perform better on questions preceding categorisation. A significant interaction effect is found.
Marking increases the number of responses in the interrogatory condition and decreases it in
the expository condition.
The average numbers of correct categorisations in the interrogatory condition is somewhat
higher than the expository condition. The mean amount of confidence in the expository
condition is a little bit higher compared to the interrogatory condition. The average number of
correct categorisations in the marking condition is lower compared to the non-marking
condition. The difference is significant. The mean amount of confidence is in the marking
condition somewhat higher, though this is a non-significant difference. The results do show
meaningful differences between the marked and non-marked presentation forms. These
differences involve (a) the number of responses to questions and (b) the number of examples
processed. The marked condition shows that students process more examples, need less time
and address more questions. The subjects in the marked condition however provide less
correct categorisations compared to the subjects from the non-marked condition. So attribute
elaboration reduces the amount of time and facilitates the processing of the information
General Discussion
101
provided by the examples. Attribute elaboration contributes to the efficiency of the
instruction, but does not improve the categorisation. The results show that the students in the
non-marked condition perform better. This might be caused by the increase of effort
necessary to find the relevant attributes in the non-marked condition and therefore to a
possibly better retention of the attributes. The student’s own activity in interpreting the
examples, thus to invest effort to construct the conceptual knowledge, seems important here.
The results of the second experiment show that attention focussing (by enhancing the
saliency of the attributes) does result in an increase of the efficiency of the learning process;
there is no evidence that it necessarily results in a an increase of transfer scores. This
experiment does not provide evidence that the combination of expository and interrogatory
examples is superior to interrogatory examples only. Interrogatory instruction as such does
not result in a clear benefit on the transfer test. The relation expository-interrogatory needs
further study, as well as a decision, not discussed by Tennyson and Cocchiarella, about what
the basic level of concept formation really is.
Rosch, Mervis, Gray, Johnson and Boyes-Braam (1976) stated that a basic level of
abstraction has a special meaning for categorisation. The basic level is the most inclusive
level on which some form of category exemplars is identifiable. Rosch et al. predicted that
basic level categories would be the classifications when objects are perceived for the first
time. She provided evidence that students categorised objects at the basic level faster
compared to the superordinate level or the subordinate level and she interpreted this by
claiming that subjects tend to categorise objects at the basic level and proceed successively by
accessing the subordinate and the superordinate level. Is it possibly dependent on expertise to
change the structure of classification hierarchies? This is of importance because somebody’s
knowledge has influence on the conceptual structure. Rosch suggested that the number of
attributes, which is added at the subordinate level, will increase expertise. Level of expertise
probably changes the structure of categories.
From an instructional point of view learning to provide a diagnosis of the shock disease
raises some specific problems. At what level the instruction has to take place: (a) the
superordinate level, (b) the basic level, or (c) the subordinate level? On the one side
superordinate categories are very distinctive but not very informative; on the other side
subordinate categories are very informative but not very distinctive (Tanaka & Taylor, 1991).
This difference has implications for the instruction. In the literature about concept formation a
distinction is made between categorisation on three levels: (a) superordinate, (b) basic, and (c)
Chapter 6
102
subordinate. What does this distinction in three levels mean in the context of the application
of the concept shock and, secondly, what is the basic level of this concept? Subjects tend to
provide basic level labels when they are required to give a name for an object. Second, they
can verify the class membership of a category in the shortest amount of time on the basic
level. This can be interpreted as a consequence of the differentiation of basic level categories.
When experts know many attributes, which are distinctive at the subordinate level, possibly
they are more capable to identify objects at the subordinate level compared to novices. That
implies that an internist immediately can identify a shock patient with a subordinate name
(cardiogenic shock) in stead of the basic level name (shock). The increased differentiation of
subordinate categories is expected to have influence on the speed experts are capable to verify
category membership at this subordinate level. There is evidence (Tanaka & Taylor, 1991)
that experts tend to use subordinate level names for the identification of objects. This finding,
called the 'downward shift hypothesis', contradicts the fact that novices first tend to apply
basic level names. Experts are better informed about the specific attributes, which
differentiate examples at the subordinate level and, secondly, experts access more easily the
information needed to provide a name for the object.
Perhaps the distinctions of superordinate level, basic level and subordinate level of
categorisation apply only to natural categories and cannot be generalised to a disease class as
shock. In the experiments of this study the decision was taken to search for a typical example
for each of the three coordinate categories, because each coordinate category has a number
of typical attributes.
Third experiment.In the third exploratory study (see Chapter five) the component 'embedded
refreshment' was varied. The mean number of responses to attribute-related questions is
significantly higher in the advance refreshment condition compared to simultaneous
refreshment and error-related refreshment, but the percentage of correct categorisations in
the conditions simultaneous refreshment and error-related refreshment is higher compared to
the advance refreshment condition. The percentage of correct categorisations is the highest
under the error-related refreshment. Because the purpose of the instruction is to correctly
categorise refreshment during instruction will be preferred.
Error-related refreshment and advance refreshment do not seem to be very efficient. The
time allotted to questions is the highest in these conditions. In the simultaneous refreshment
condition the least amount of time is assigned to a case and in the error-related refreshment

General Discussion
103
condition the most time. In the simultaneous refreshment condition the least amount of time
is assigned to video and in the advance refreshment condition the most time. The mean
number of cases processed by a student varies also between the conditions: it was the highest
in the simultaneous refreshment condition. On the transfer test the subjects from the
simultaneous refreshment condition perform only a little bit better compared to students from
both other conditions. The mean score of students from the error-related refreshment
condition is the lowest. Because of the inefficiency of this method, they probably need more
practice. The confidence data show that, if the answer is incorrect, subjects in error-related
refreshment condition tended to be more confident compared to subjects from the advance
refreshment and simultaneous refreshment conditions, though this is not a significant
difference. There is a significant difference in confidence if the correct and incorrect
diagnoses are analysed separately. In case of correct answers the confidence tended to be
higher.
This study had an explorative character. Due to the constraints, imposed by the college of
nursing and taken into account the relative small number of subjects, this study is
incomplete. For studying the effect of advance refreshment a program controlled refreshment
group is missing. Moreover a control group, the participants of which should receive no
refreshment, is missing. Nevertheless, the results are somewhat in favour of embedded
refreshment, thus during instruction. That means that in learning the different types of shock
conceptual and (prerequisite) causal knowledge have to be linked, possibly still more tightly
than it was possible in this study. In that case, as described by Anderson and Reder, retrieval
paths will be practised.
6.3 Future Research
Based on the instructional design rules discussed a summary set of instructional prescriptions
is presented, for the pre-instructional phase, the instructional phase and the evaluation phase
(Table 6.1). Future studies can use this set of prescriptions. The main questions to be
addressed in the future studies of concept learning (Dempsey, 1986) are: (a) whether concepts
are represented in different ways and how examples of a concept are organised, (b) what the
basis is for organising examples, (c) how concepts are interrelated and the basis for those
relationships, (d) how conceptual organisation develop. Dempsey proposed a model structure
that accommodates successive and coordinate relationships, as described by Tennyson and
Cocchiarella.. His contribution can be seen as a further elaboration of Tennyson and
Chapter 6
104
Cocchiarella's concept teaching model. Since in our study coordinate concepts were
addressed, the focus will be on that type of concepts.
Coordinate concepts have one or more, common critical attributes and different variable
attributes. Dempsey argued that since coordinate concepts emphasise both generalisation and
discrimination, they are better learned through the use of matched sets of examples and non-
examples. In our study the constraints imposed on the experiments were such that the use of
matched sets of examples and non-examples could not be realised. This should be done in
future research.
Dempsey provided a matrix as a useful model structure that can provide for increasing
discrimination along one axis and increasing generalisation along the other axis. Presenting a
'rational set' of matched examples (i.e. a design strategy for selecting matched examples and
non-examples based on the critical and variable attributes of the concept involved) seems the
best prescription for learning coordinate concepts. This method enables the creation of
examples with a range of difficulty. The 'Rational Set Generator', proposed by Driscoll and
Tessmer (1985a; 1985b), is an adequate device to realise such a procedure. Model matrices,
such as the "The Rational Set Generator", are able to expand and contract depending on the
number of concepts or rules in the rational set. The difficulty (generalisation) levels are also
highly variable. There is no requirement for an equal number of concepts and levels of
generalisation. The matrix structure, being pliable, is open to schemes to establish the number
and difficulty levels of the relevant skills (Lichfield, Driscoll & Dempsey, 1989). In Table 6.1
a summary set of prescriptions to design instructional systems for concept learning is
presented. Combined with Dempsey's procedure for a design strategy for selecting matched
examples and non-examples based on the critical and variable attributes of the concept
involved, future studies can address some components in Tennyson and Cocchiarella's
concept teaching model (see Table 1.1), that badly need further experimentation: (a)
simultaneous versus successive presentation of expository examples, (b) context, (c)
interrogatory and expository examples, and (d) strategy information.
6.4 Multimedia in nursing education
Multimedia are very useful in nursing education for the demonstration of patients. The
demonstration has to carefully show the practices in the hospital. Instructional multimedia-
based simulations, which are developed based on prescriptions similar as those of Park and

General Discussion
105
Hannafin (1993) (Appendix E), have the potential to transfer the knowledge to the real
situation in the hospital. Such simulations imply a type of teaching complex mental and
procedural tasks in an environment that resembles a real world setting. It presupposes that
students engage in meaningful, interactive learning environments from which they are
expected to construct the relevant knowledge. Asking questions about patients with
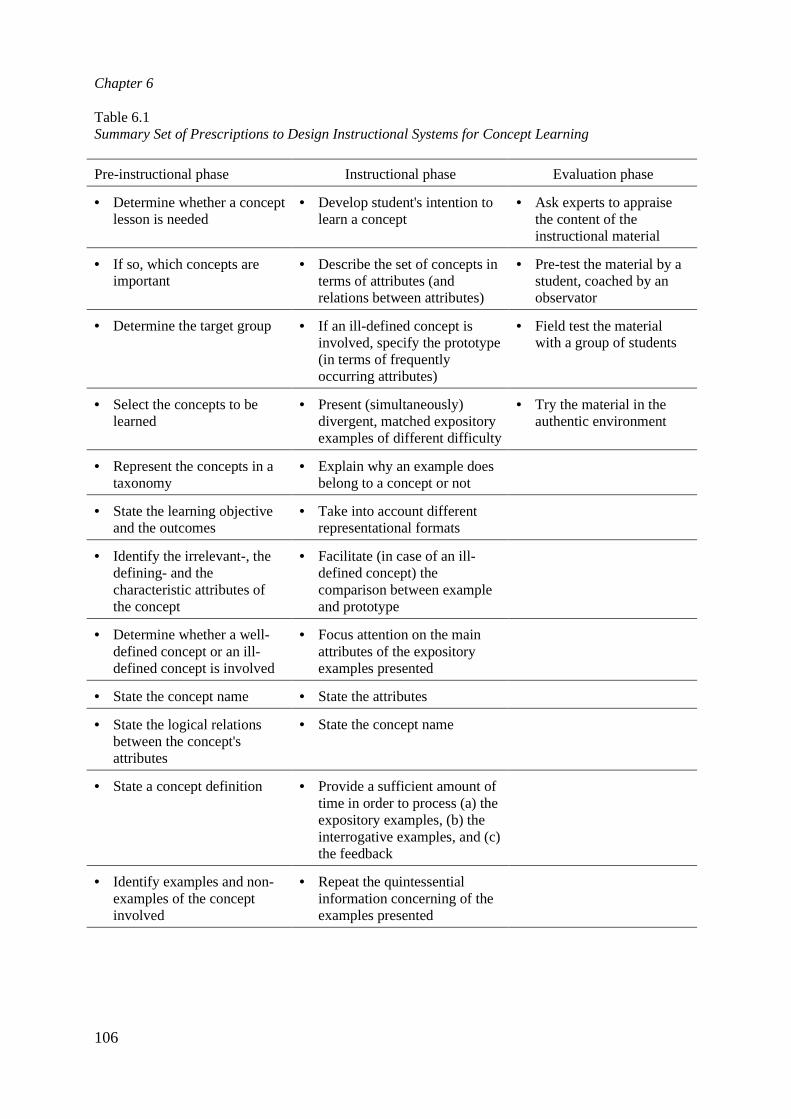
Chapter 6
106
Table 6.1Summary Set of Prescriptions to Design Instructional Systems for Concept Learning
Pre-instructional phase Instructional phase Evaluation phase
• Determine whether a conceptlesson is needed
• Develop student's intention tolearn a concept
• Ask experts to appraisethe content of theinstructional material
• If so, which concepts areimportant
• Describe the set of concepts interms of attributes (andrelations between attributes)
• Pre-test the material by astudent, coached by anobservator
• Determine the target group • If an ill-defined concept isinvolved, specify the prototype(in terms of frequentlyoccurring attributes)
• Field test the materialwith a group of students
• Select the concepts to belearned
• Present (simultaneously)divergent, matched expositoryexamples of different difficulty
• Try the material in theauthentic environment
• Represent the concepts in ataxonomy
• Explain why an example doesbelong to a concept or not
• State the learning objectiveand the outcomes
• Take into account differentrepresentational formats
• Identify the irrelevant-, thedefining- and thecharacteristic attributes ofthe concept
• Facilitate (in case of an ill-defined concept) thecomparison between exampleand prototype
• Determine whether a well-defined concept or an ill-defined concept is involved
• Focus attention on the mainattributes of the expositoryexamples presented
• State the concept name • State the attributes
• State the logical relationsbetween the concept'sattributes
• State the concept name
• State a concept definition • Provide a sufficient amount oftime in order to process (a) theexpository examples, (b) theinterrogative examples, and (c)the feedback
• Identify examples and non-examples of the conceptinvolved
• Repeat the quintessentialinformation concerning of theexamples presented
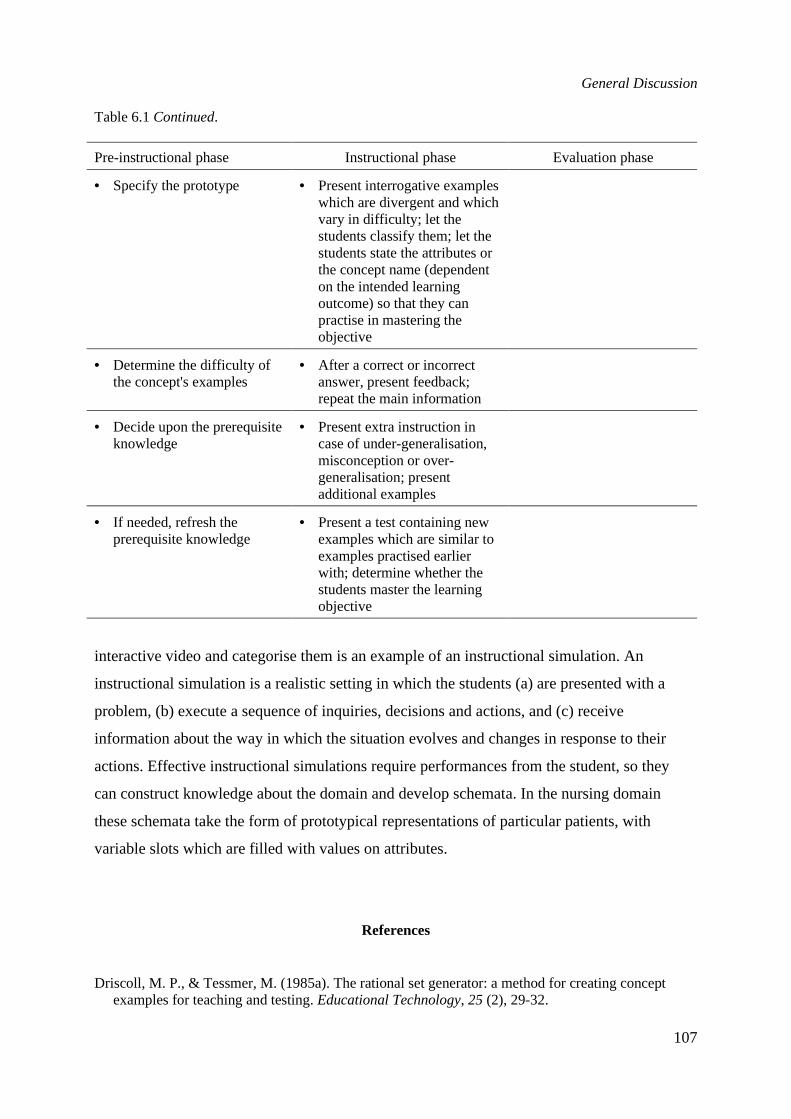
General Discussion
107
Table 6.1Continued.
Pre-instructional phase Instructional phase Evaluation phase
• Specify the prototype • Present interrogative exampleswhich are divergent and whichvary in difficulty; let thestudents classify them; let thestudents state the attributes orthe concept name (dependenton the intended learningoutcome) so that they canpractise in mastering theobjective
• Determine the difficulty ofthe concept's examples
• After a correct or incorrectanswer, present feedback;repeat the main information
• Decide upon the prerequisiteknowledge
• Present extra instruction incase of under-generalisation,misconception or over-generalisation; presentadditional examples
• If needed, refresh theprerequisite knowledge
• Present a test containing newexamples which are similar toexamples practised earlierwith; determine whether thestudents master the learningobjective
interactive video and categorise them is an example of an instructional simulation. An
instructional simulation is a realistic setting in which the students (a) are presented with a
problem, (b) execute a sequence of inquiries, decisions and actions, and (c) receive
information about the way in which the situation evolves and changes in response to their
actions. Effective instructional simulations require performances from the student, so they
can construct knowledge about the domain and develop schemata. In the nursing domain
these schemata take the form of prototypical representations of particular patients, with
variable slots which are filled with values on attributes.
References
Driscoll, M. P., & Tessmer, M. (1985a). The rational set generator: a method for creating conceptexamples for teaching and testing.Educational Technology, 25 (2), 29-32.
Chapter 6
108
Driscoll, M. P., & Tessmer, M. (1985b). Applications of the concept tree and rational set generator forcoordinate concept learning. Paper presented at the Annual Meeting of the American EducationalResearch Association. Chicago.
Dempsey, J. (1986). Using the rational set generator with computer-based instruction for creatingconcept examples: a template for instructors.Educational Technology, 26 (4), 43-46.
Jonassen, D. H. (1992). Objectivism versus constructivism; do we need a new philosophicalparadigm?Educational Technology and Development, 39 (3), 5-14.
Lichfield, B. C., Driscoll, M. D., & Dempsey, J. V. (1989). Presentation sequence and exampledifficulty: their effect on concept and rule learning in computer-based instruction. Journal ofComputer-based Instruction, 17, (1), 35-40.
Lakov, G. (1987).Women, Fire, and Dangerous Things: What Categories Reveal about the Mind.Chicago: University of Chicago Press.
Park, I., & Hannafin, M. J. (1993). Empirically-based guidelines for the design of interactivemultimedia.Educational Technology Research & Development, 41,3, 63-85.
Rosch, E. (1978). Principles of categorization. In E. Rosch & B. L. Lloyd (Eds.),Cognition andcategorisation(pp. 27-48). Hillsdale, NJ: Lawrence Erlbaum Associates.
Rosch, E., Mervis, C., Gray, W. D., Johnson, D. M., & Boyes-Braam, P. (1976). Basic objects innatural categories,Journal of Cognitive Psychology,382-439.
Tanaka, J. W., & Taylor, M. (1991). Object categories and expertise: Is the basic level in the eye of thebeholder?Cognitive Psychology, 23, 457-482.
Tennyson, R. D., & Cocchiarella, M. J. (1986). An empirically based instructional design theory forteaching concepts.Review of Educational Research, 1, 40-71.
Samenvatting(Dutch Summary)
Het onderzoek waarvan in deze dissertatie verslag wordt gedaan, betreft het beproeven van
(componenten van) het model voor het onderwijzen van concepten van Tennyson en
Cocchiarella. In het bijzonder is nagegaan hoe vanuit de instructietheorie effectief onderwijs
kan worden ontwikkeld over het leren toepassen van medische concepten in de opleiding
verpleegkunde. Aan de studenten werd gevraagd verschillende typen van circulatiestoornissen
te categoriseren. Het te leren materiaal werd met interactieve video aangeboden. Tevens is
bekeken welke instructievormen hierbij het meest effectief zijn.
In hoofdstuk 1 wordt de prototype-theorie als theoretisch kader voor het onderzoek
geschetst. Deze theorie gaat uit van een prototype als hypothetische constructie van het meest
typische voorbeeld van een categorie. Een prototype heeft in ieder kenmerk van de leden van
de categorie de gemiddelde waarde. De mate van gelijkenis in relatie tot het prototype bepaalt
volgens de prototypetheorie de mate van toebehoren aan de categorie. Een ziekteklasse is
volgens de prototype-theorie een vaag concept.
Het uitgevoerde onderzoek is geënt op het instructie-ontwerpmodel van Tennyson en
Cocchiarella. Dit model wordt geplaatst in het kader van een paradigma-verschuiving in de
richting van de prototype-theorie. Het model van Tennyson en Cocchiarella bestaat uit twee
ontwerpcomponenten, de inhoudelijke structuur van een domein en de instructie-
ontwerpvariabelen. De combinatie van de ontwerpcomponenten levert vier instructie-
ontwerpstrategieën op. Eén daarvan, te weten de ontwerpstrategie voor coördinate concepten
met constante dimensies, ligt aan de basis van de drie uitgevoerde experimenten. De gebruikte
Dutch Summary
110
ontwerpstrategie omvat de componenten: naam en definitie, duidelijke voorbeelden, exposito-
rische instanties (gelijktijdige presentatie), interrogatieve instanties, attribuutelaboratie en
herhaling.
In hoofdstuk 2 wordt een beschrijving gegeven van de te leren concepten en de gebruikte
media. In alle drie de experimenten staat het categoriseren van (typen van) shock centraal.
Shock is een circulatiestoornis die gekarakteriseerd wordt door een vrijwel acute
vermindering van de effectieve capillaire weefselperfusie met daardoor een verstoring van het
celmetabolisme. Het is een levensbedreigende stoornis. Er worden drie typen shock
beschreven. Het eerste type is de hypovolemische shock. Als gevolg van groot bloed- of
vochtverlies wordt de hoeveelheid bloed te klein om de weefsels van voldoende zuurstof te
voorzien; de kenmerken van dit type shock zijn: koude huid, rusteloosheid, hypotensie,
oligurie, versnelde ademhaling. Het tweede type is de septische shock. Septische shock
ontstaat wanneer bepaalde bacteriën in de bloedsomloop doordringen. De kenmerken van dit
type shock zijn: klamme warme huid, geringe perifere doorbloeding, verminderde productie
van urine, versneld hartritme, versnelde ademhaling. Bij het derde type shock, cardiale shock,
staat de vermindering van de hoeveelheid bloed dat door het hart wordt vervoerd (de zgn.
cardiac output) centraal. De kenmerken van dit type shock zijn: geringe perifere
doorbloeding, klamme huid, lage , urineproductie < 25 ml/uur.
In hoofdstuk 2 wordt verder een beschrijving gegeven van de interactieve video, die ten
behoeve van het uitgevoerde onderzoek is ontwikkeld. De interactieve video "Shock" is
primair ontwikkeld om de effecten van variaties in het instructie-ontwerp te kunnen testen. In
het onderzoek werden de volgende instructievariabelen onderzocht: (a) variaties in
voorbeelden (oefenproblemen), (b) de volgorde van de presentatie van problemen en de
aanwezigheid van markering en contrastering in de attributen van de voorbeelden en (c) de
relatie tussen de te ontwikkelen conceptuele kennis en reeds bestaande kennis.
Het doel van het experiment dat beschreven wordt in hoofdstuk 3 is om de hypothese te
verifiëren, of beslissingen aangaande klasse-lidmaatschap worden vergemakkelijkt indien de
categorisatie plaatsvindt als een proces van matching van een prototype en een voorbeeld van
een categorie. De veronderstelling is dat een benadering die uitgaat van de prototype-theorie
effectiever zal blijken dan een benadering gebaseerd op opsomming van eigenschappen. Op
grond van de prototype-theorie wordt verwacht dat een significant verschil in correct
categoriseren gevonden zal worden als resultaat van een prototype-gebaseerde instructie.
Dutch Summary
111
In hoofdstuk 4 wordt het effect van het presenteren van prototypische voorbeelden van het
ziektebeeld shock (wel of niet in combinatie met markering/contrast) onderzocht. Er wordt
aangenomen dat concepten zijn georganiseerd rond een beste voorbeeld. Dat prototype is een
geïdealiseerde abstractie van de leden van een categorie. Het wordt opgevat als een gemiddeld
lid van een categorie. Dit betekent dat het prototype de meest frequente attributen van de
leden van de categorie bevat. Uit onderzoek blijkt dat wanneer de deelnemers een reeks
(typische) voorbeelden aangeboden krijgen, de informatie over de afzonderlijke voorbeelden
sneller vergeten wordt dan de centrale tendens van de voorbeelden.
De hoeveelheid informatie die een individu tegelijkertijd kan verwerken is beperkt. Een
mogelijkheid om de effectiviteit van visualisatie te vergroten, is de hoeveelheid informatie die
de aandacht vraagt te reduceren door middel van markeringstechnieken. Uit onderzoek is
gebleken dat het leren in verschillende instructietaken vergemakkelijkt wordt door het gebruik
van markeringsstrategieën. De instructieboodschap kan dan sneller worden overgedragen.
Markeren wordt gedefinieerd als het proces waarin de aandacht van de lerende wordt gericht
op afzonderlijke gegevens in het visuele beeld.
In het in hoofdstuk 4 beschreven experiment werden vier instructiecondities op
differentiële effecten onderzocht. In de eerste conditie worden de problemen uit één
subcategorie (bijv. septische shock) gedurende een bepaalde tijd geoefend. Daarna de
problemen uit de tweede subcategorie, en vervolgens die uit de derde subcategorie. In de
tweede conditie wordt uit elke subcategorie afzonderlijk vooraf eerst een (typisch)
expositorisch voorbeeld aangeboden, gevolgd door een probleem uit dezelfde categorie.
Vervolgens wordt een (typisch) expositorisch voorbeeld uit de volgende categorie
aangeboden, gevolgd door een interrogatief voorbeeld. Op deze manier worden de drie
categorieën beurtelings doorlopen. In de derde en vierde conditie wordt dezelfde
instructiestrategie aangehouden als in de eerste respectievelijk de tweede conditie, maar met
dit verschil, dat hierbij waarden van attributen gemarkeerd worden en relevante waarden
gecontrasteerd worden met niet-relevante waarden.
In hoofdstuk 5 staat de exploratie van de relatie van nieuwe kennis met bestaande kennis
centraal. Het leggen van een relatie tussen nieuwe kennis en bestaande kennis bevordert het
onthouden van nieuwe kennis. De relatie kan gelegd worden door een 'glossary' te presenteren
in de vorm van "embedded refreshment". De theorie van Tennyson en Cocchiarella geeft niet
aan hoe de voorkennis geactiveerd kan worden door middel van 'embedded refreshment'. In de
literatuur onderscheidt men verschillende benaderingen ter verklaring van het faciliterend effect
Dutch Summary
112
van voorkennis. Twee van die benaderingen, de elaboratie-benadering en de selectieve-attentie
benadering liggen mede ten grondslag aan het explorerend onderzoek dat in hoofdstuk 5 wordt
beschreven. De elaboratie-benadering gaat er vanuit dat voorkennis de productie van elaboraties
stimuleert. Elaboratie is het verrijken van informatie door het bedenken van relaties tussen
voorkennis en de in de instructie aangeboden informatie. Dit verrijken van informatie door
elaboratie leidt tot de ontwikkeling van 'multiple redundant retrieval paths' in de cognitieve
representatie. Mogelijk is dat de aanwezigheid van deze retrieval-paden het leren
vergemakkelijkt doordat het ophalen van al aanwezige kennis eenvoudiger wordt. De selectieve-
attentie benadering veronderstelt dat mensen met meer voorkennis hun aandacht selectief richten
op informatie die relevant is voor de te leren kennis. Dit leidt ertoe dat de nieuwe informatie
dieper verwerkt wordt. Het activeren van voorkennis vervult binnen de selectieve-attentie
benadering een sturende rol. Relevante informatie krijgt meer aandacht (uitgedrukt in studietijd)
ten koste van informatie die niet relevant is voor het probleem of onderwerp.
In het explorerend onderzoek zijn drie condities uitgewerkt: (a) aan het begin van de instructie
activeren van voorkennis (vooraf), (b) tegelijkertijd met het aanbieden van instructie activeren
van voorkennis (parallel) en (c) voorkennis activeren wanneer een fout wordt gemaakt tijdens de
instructie (fout-gerelateerd). Tijdens het doornemen van de programma's zijn (a) aantal
responsen, waarbij een onderscheid wordt gemaakt tussen button-vragen en diagnose-vragen, (b)
aantal correcte responsen op button-vragen en diagnose-vragen, (c) tijd, (d) aantal geraadpleegde
kernwoorden en (e) aantal geraadpleegde voorbeelden vastgelegd. Na afloop van het doornemen
van het programma is een transfer-toets afgenomen.
De resultaten die gevonden zijn in de drie experimenten kunnen als volgt worden
samengevat. Het eerste experiment (hoofdstuk drie) toont dat de resultaten op de post-test uit
de tekst-alleen conditie iets hoger zijn op het gedeelte 'definitie' van deze test. Op het gedeelte
'categorisatie' presteren studenten uit de tekst plus video-conditie aanmerkelijk beter. De
resultaten van de retentie-test geven aan dat op het onderdeel 'naam geven' studenten uit de
tekst plus video-conditie beter presteren; hetzelfde geldt voor de onderdelen
'gevolgtrekkingen' en 'classificatie'. De gemiddelde scores op de retentie-test als geheel
verschillen aanmerkelijk. Er is een sterke aanwijzing dat de studenten profijt hebben van de
typische voorbeelden, zoals gepresenteerd bij de videobeelden. Dus als in de prototype-
conditie (tekst plus video) typische voorbeelden van het ziektebeeld shock, die zowel
definiërende als irrelevante attributen bevatten, werden gepresenteerd, dan resulteerde dit in

Dutch Summary
113
een toename van de vaardigheid om te onderscheiden tussen verschillende typen van shock en
in een toename van de vaardigheid om te generaliseren naar nieuwe voorbeelden van shock.
Data-analyse van de scores op de post-test geeft aan dat wat betreft de definitie van shock en
de attributen van verschillende typen van shock de gemiddelde prestatie niet significant
verschilt. Wel verschillen de post-test scores significant op het onderdeel 'gevolgtrekking'. De
retentie-test laat zien dat de scores op discriminatie tussen shock en niet-shock en het
identificeren van de meest opvallende attributen van shock significant verschillen. De
gemiddelde scores verschillen significant op het onderdeel identificatie van shock in termen
van overeenkomsten en verschillen tussen typen van shock. De overall scores op de retentie-
test laten een significant verschil zien ten gunste van de prototype-gebaseerde instructie.
De resultaten gevonden in het tweede experiment (hoofdstuk vier) laten het volgende beeld
zien. Het gemiddelde percentage van alle doorlopen voorbeelden is in de expositorische
conditie geringer dan in de interrogatieve conditie. Voor de expositorische conditie is het
gemiddeld percentage van correcte responsen op vragen voorafgaand aan de categorisering
iets hoger vergeleken met de interrogatieve conditie, maar dit verschil is niet significant. Het
gemiddeld percentage van correcte categoriseringen is in de expositorische conditie lager dan
in de interrogatieve conditie, hoewel dit verschil niet significant is. De gemiddelde
hoeveelheid tijd die de studenten uit de expositorische conditie besteden aan het bestuderen
van een voorbeeld van shock is nauwelijks hoger dan de interrogatieve conditie. Het
gemiddeld percentage van alle doorlopen voorbeelden in de gemarkeerde conditie is groter
vergeleken met de niet-gemarkeerde conditie. Er is sprake van een trend ten voordele van het
markeren van attributen. In de gemarkeerde conditie is het gemiddeld percentage correcte
responsen op vragen voorafgaand aan de categorisatie iets hoger vergleken met de niet-
gemarkeerde conditie, maar dit verschil is niet significant. Het gemiddeld percentage correcte
categoriseringen is in de gemarkeerde conditie nauwelijks minder. De variantie-analyse geeft
aan dat attribuut-elaboratie significant bijdraagt aan het efficiënt doorlopen van voorbeelden.
Het schijnt dat markeren het aantal doorlopen voorbeelden verhoogt. De variantie-analyse
geeft aan dat studenten uit de expositorische-gemarkeerde conditie beter presteren op vragen
voorafgaand aan de categorisering. Er is sprake van een significant interactie-effect. Markeren
verhoogt het aantal responsen in de interrogatieve conditie en verlaagt dat in de expositorische
conditie.
Dutch Summary
114
Wat betreft de transfer test zijn de volgende resultaten gevonden. De betrouwbaarheid van
de transfer test is relatief laag. Het gemiddeld aantal correcte categoriseringen is in de
interrogatieve conditie hoger dan in de expositorische conditie. De gemiddelde zekerheid is in
de expositorische conditie iets hoger vergeleken met de interrogatieve conditie. Het
gemiddeld aantal correcte categoriseringen in de gemarkeerde conditie is lager dan in de niet-
gemarkeerde conditie. Dit verschil is significant. De gemiddelde zekerheid is in de
gemarkeerde conditie hoger, hoewel dit verschil niet significant is.
De resultaten laten betekenisvolle verschillen zien tussen gemarkeerde - en niet-
gemarkeerde presentaties op (a) het aantal responsen op vragen voorafgaand aan
categorisering, en (b) het aantal doorlopen voorbeelden. De gemarkeerde conditie laat zien dat
studenten meer voorbeelden verwerken, dat ze minder tijd nodig hebben en dat ze meer
vragen beantwoorden. De personen uit de gemarkeerde conditie geven minder correcte
categoriseringen vergeleken met de personen uit de niet-gemarkeerde conditie. Dus attribuut-
elaboratie reduceert de hoeveelheid tijd en vergemakkelijkt het verwerken van informatie
zoals die geboden wordt in de voorbeelden. Attribuut-elaboratie bevordert de efficiëntie van
de instructie, maar verbetert de categorisatie niet. Dit is wellicht veroorzaakt door de toename
van inspanning die noodzakelijk is teneinde de relevante attributen te vinden in de niet-
gemarkeerde conditie, resulterend in een mogelijk betere retentie van de attributen. De eigen
activiteit van de student bij het interpreteren van de voorbeelden en zo inspanning te
investeren teneinde de conceptuele kennis te construeren, schijnt belangrijk in dit verband.
De resultaten van het explorerend onderzoek (hoofdstuk vijf) tonen dat het gemiddeld
aantal responsen op attribuut-gerelateerde vragen hoger is in de activatie-vooraf conditie dan
in de simultane activatie- en de fout-gerelateerde activatie conditie. De variantie-analyse laat
een significant conditie-effect zien waar het gaat om het aantal correct beantwoorde vragen
voorafgaand aan de categorisering. Het percentage correcte responsen op attribuut-
gerelateerde vragen is het hoogst in de fout-gerelateerde activatie conditie. Wat betreft het
percentage correcte categorisaties laat de data-analyse zien dat in de condities simultane
activatie en fout-gerelateerde activatie het gemiddeld aantal correcte categorisaties hoger is
dan in de conditie activatie-vooraf. De variantie-analyse laat zien dat er een significant
conditie-effect is voor wat betreft verwerkingstijd. Als de tijd per casus wordt vergeleken met
de gemiddelde tijd besteed aan de video-gedeelten zoals die in een casus zijn opgenomen, dan
Dutch Summary
115
is er sprake van een significant effect. In de simultane activatie-conditie wordt de minste
hoeveelheid tijd besteed aan een casus en in de fout-gerelateerde conditie de meeste tijd. In de
conditie simultane activatie wordt de minste tijd besteed aan video, terwijl daar in de conditie
activatie-vooraf de meeste tijd aan wordt besteed. Het aantal keren dat een prerequisiet
concept werd opgefrist varieerde over de instructiecondities. Dat geldt ook voor het aantal
casussen dat doorlopen wordt door een student(e); dat aantal is het hoogst in de conditie
simultane activatie van voorkennis.
De resultaten op de transfer test geven aan dat de studenten uit de simultane activatie
conditie beter presteren dan de studenten uit beide andere condities. De gemiddelde score van
studenten uit de fout-gerelateerde activatie conditie is het laagst. Verder blijkt dat, als het
antwoord incorrect is, studenten in de fout-gerelateerde conditie ertoe neigen meer zeker te
zijn dan studenten uit de condities activatie-vooraf en simultane activatie, hoewel dit verschil
niet significant is. Er is sprake van een significant verschil in zekerheid als de correcte en
incorrecte categoriseringen afzonderlijk worden geanalyseerd. In geval van correcte
antwoorden is de zekerheid hoger. Als het antwoord incorrect is, dan neigen studenten uit de
fout-gerelateerde activatie conditie ertoe meer zeker te zijn.
Samenvattend kan worden gesteld, dat het model voor het onderwijzen van concepten van
Tennyson en Cocchiarella een bruikbaar model blijkt. Vervolgens is het zo, dat uit deze
dissertatie blijkt dat prototypevorming, markering en activatie van voorkennis belangrijke
ontwerpregels zijn, maar dat het onderzoek naar de effectiviteit ervan op onderdelen moet
worden voortgezet.
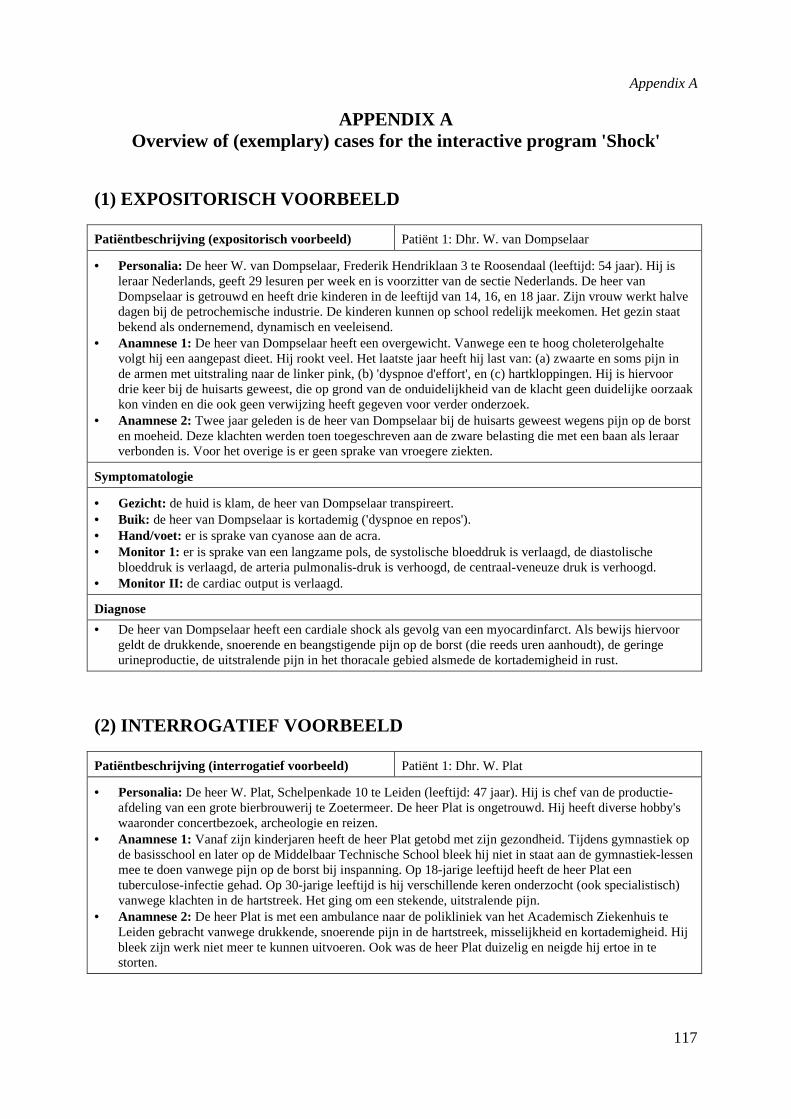
Appendix A
117
APPENDIX AOverview of (exemplary) cases for the interactive program 'Shock'
(1) EXPOSITORISCH VOORBEELD
Patiëntbeschrijving (expositorisch voorbeeld) Patiënt 1: Dhr. W. van Dompselaar
• Personalia:De heer W. van Dompselaar, Frederik Hendriklaan 3 te Roosendaal (leeftijd: 54 jaar). Hij isleraar Nederlands, geeft 29 lesuren per week en is voorzitter van de sectie Nederlands. De heer vanDompselaar is getrouwd en heeft drie kinderen in de leeftijd van 14, 16, en 18 jaar. Zijn vrouw werkt halvedagen bij de petrochemische industrie. De kinderen kunnen op school redelijk meekomen. Het gezin staatbekend als ondernemend, dynamisch en veeleisend.
• Anamnese 1:De heer van Dompselaar heeft een overgewicht. Vanwege een te hoog choleterolgehaltevolgt hij een aangepast dieet. Hij rookt veel. Het laatste jaar heeft hij last van: (a) zwaarte en soms pijn inde armen met uitstraling naar de linker pink, (b) 'dyspnoe d'effort', en (c) hartkloppingen. Hij is hiervoordrie keer bij de huisarts geweest, die op grond van de onduidelijkheid van de klacht geen duidelijke oorzaakkon vinden en die ook geen verwijzing heeft gegeven voor verder onderzoek.
• Anamnese 2:Twee jaar geleden is de heer van Dompselaar bij de huisarts geweest wegens pijn op de borsten moeheid. Deze klachten werden toen toegeschreven aan de zware belasting die met een baan als leraarverbonden is. Voor het overige is er geen sprake van vroegere ziekten.
Symptomatologie
• Gezicht: de huid is klam, de heer van Dompselaar transpireert.• Buik: de heer van Dompselaar is kortademig ('dyspnoe en repos').• Hand/voet: er is sprake van cyanose aan de acra.• Monitor 1: er is sprake van een langzame pols, de systolische bloeddruk is verlaagd, de diastolische
bloeddruk is verlaagd, de arteria pulmonalis-druk is verhoogd, de centraal-veneuze druk is verhoogd.• Monitor II: de cardiac output is verlaagd.
Diagnose
• De heer van Dompselaar heeft een cardiale shock als gevolg van een myocardinfarct. Als bewijs hiervoorgeldt de drukkende, snoerende en beangstigende pijn op de borst (die reeds uren aanhoudt), de geringeurineproductie, de uitstralende pijn in het thoracale gebied alsmede de kortademigheid in rust.
(2) INTERROGATIEF VOORBEELD
Patiëntbeschrijving (interrogatief voorbeeld) Patiënt 1: Dhr. W. Plat
• Personalia:De heer W. Plat, Schelpenkade 10 te Leiden (leeftijd: 47 jaar). Hij is chef van de productie-afdeling van een grote bierbrouwerij te Zoetermeer. De heer Plat is ongetrouwd. Hij heeft diverse hobby'swaaronder concertbezoek, archeologie en reizen.
• Anamnese 1:Vanaf zijn kinderjaren heeft de heer Plat getobd met zijn gezondheid. Tijdens gymnastiek opde basisschool en later op de Middelbaar Technische School bleek hij niet in staat aan de gymnastiek-lessenmee te doen vanwege pijn op de borst bij inspanning. Op 18-jarige leeftijd heeft de heer Plat eentuberculose-infectie gehad. Op 30-jarige leeftijd is hij verschillende keren onderzocht (ook specialistisch)vanwege klachten in de hartstreek. Het ging om een stekende, uitstralende pijn.
• Anamnese 2:De heer Plat is met een ambulance naar de polikliniek van het Academisch Ziekenhuis teLeiden gebracht vanwege drukkende, snoerende pijn in de hartstreek, misselijkheid en kortademigheid. Hijbleek zijn werk niet meer te kunnen uitvoeren. Ook was de heer Plat duizelig en neigde hij ertoe in testorten.
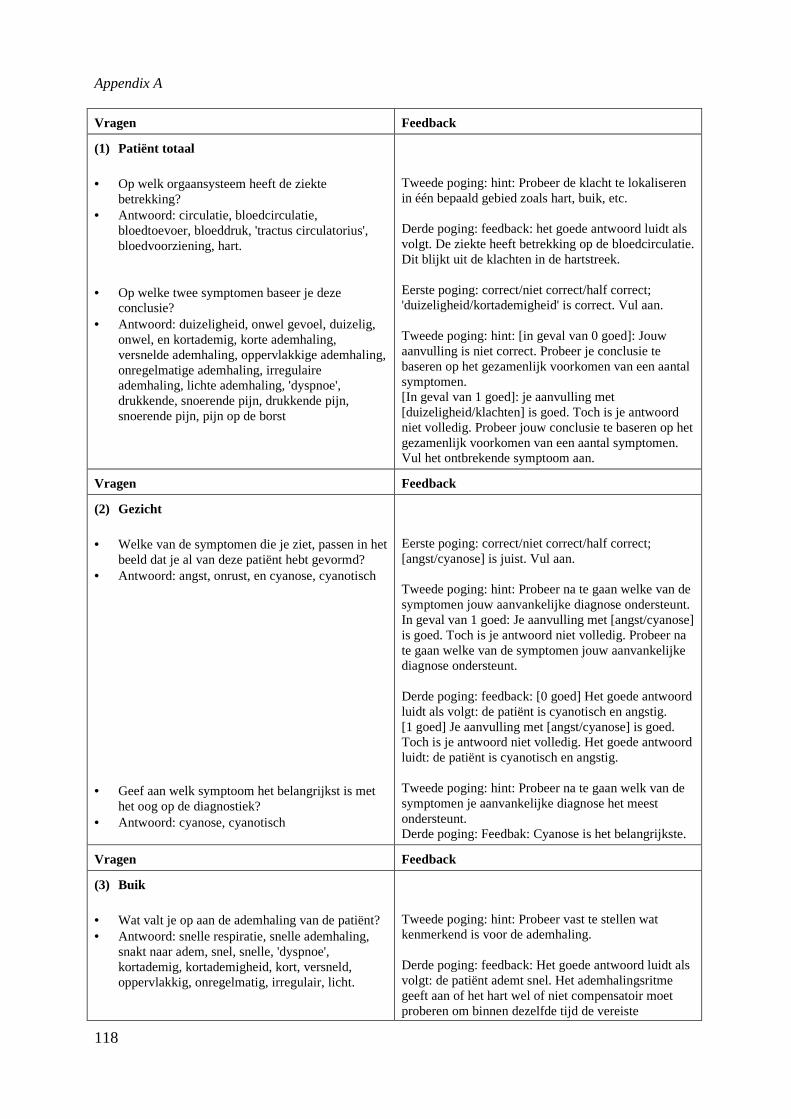
Appendix A
118
Vragen Feedback
(1) Patiënt totaal
• Op welk orgaansysteem heeft de ziektebetrekking?
• Antwoord: circulatie, bloedcirculatie,bloedtoevoer, bloeddruk, 'tractus circulatorius',bloedvoorziening, hart.
• Op welke twee symptomen baseer je dezeconclusie?
• Antwoord: duizeligheid, onwel gevoel, duizelig,onwel, en kortademig, korte ademhaling,versnelde ademhaling, oppervlakkige ademhaling,onregelmatige ademhaling, irregulaireademhaling, lichte ademhaling, 'dyspnoe',drukkende, snoerende pijn, drukkende pijn,snoerende pijn, pijn op de borst
Tweede poging: hint: Probeer de klacht te lokaliserenin één bepaald gebied zoals hart, buik, etc.
Derde poging: feedback: het goede antwoord luidt alsvolgt. De ziekte heeft betrekking op de bloedcirculatie.Dit blijkt uit de klachten in de hartstreek.
Eerste poging: correct/niet correct/half correct;'duizeligheid/kortademigheid' is correct. Vul aan.
Tweede poging: hint: [in geval van 0 goed]: Jouwaanvulling is niet correct. Probeer je conclusie tebaseren op het gezamenlijk voorkomen van een aantalsymptomen.[In geval van 1 goed]: je aanvulling met[duizeligheid/klachten] is goed. Toch is je antwoordniet volledig. Probeer jouw conclusie te baseren op hetgezamenlijk voorkomen van een aantal symptomen.Vul het ontbrekende symptoom aan.
Vragen Feedback
(2) Gezicht
• Welke van de symptomen die je ziet, passen in hetbeeld dat je al van deze patiënt hebt gevormd?
• Antwoord: angst, onrust, en cyanose, cyanotisch
• Geef aan welk symptoom het belangrijkst is methet oog op de diagnostiek?
• Antwoord: cyanose, cyanotisch
Eerste poging: correct/niet correct/half correct;[angst/cyanose] is juist. Vul aan.
Tweede poging: hint: Probeer na te gaan welke van desymptomen jouw aanvankelijke diagnose ondersteunt.In geval van 1 goed: Je aanvulling met [angst/cyanose]is goed. Toch is je antwoord niet volledig. Probeer nate gaan welke van de symptomen jouw aanvankelijkediagnose ondersteunt.
Derde poging: feedback: [0 goed] Het goede antwoordluidt als volgt: de patiënt is cyanotisch en angstig.[1 goed] Je aanvulling met [angst/cyanose] is goed.Toch is je antwoord niet volledig. Het goede antwoordluidt: de patiënt is cyanotisch en angstig.
Tweede poging: hint: Probeer na te gaan welk van desymptomen je aanvankelijke diagnose het meestondersteunt.Derde poging: Feedbak: Cyanose is het belangrijkste.
Vragen Feedback
(3) Buik
• Wat valt je op aan de ademhaling van de patiënt?• Antwoord: snelle respiratie, snelle ademhaling,
snakt naar adem, snel, snelle, 'dyspnoe',kortademig, kortademigheid, kort, versneld,oppervlakkig, onregelmatig, irregulair, licht.
Tweede poging: hint: Probeer vast te stellen watkenmerkend is voor de ademhaling.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: de patiënt ademt snel. Het ademhalingsritmegeeft aan of het hart wel of niet compensatoir moetproberen om binnen dezelfde tijd de vereiste

Appendix A
119
hoeveelheid bloed te transporteren.
Vragen Feedback
(4) Hand
• Geef met 'ja' of 'nee' aan, of er een verschil istussen de hand van de patiënt (e) en de hand vande arts.
• Antwoord: ja
• Wat is de oorzaak van dit verschil?• Antwoord: centralisatie, vasoconstrictie,
constrictie, vernauwing, vaatvernauwing,verminderde toevoer.
Tweede poging: hint: Probeer vast te stellen of dehand er normaal uitziet, dan wel in een bepaaldopzicht afwijkend is.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: Ja, er is verschil.
Tweede poging: hint: Is er sprake van een ontregeldebloedsomloop?
Derde poging: Feedback: Het goede antwoord luidt:Een cyanotische hand wijst erop dat er sprake is vancentralisatie van het bloed naar de hersenen, longen enhart.
Vragen Feedback
(5) Voet
• Geef met 'ja' of 'nee' aan, of er circulatieprobleemis
• Antwoord: ja
• Geef met 'ja' of 'nee' aan of het beeld van de voethet antwoord op de vorige vraag bevestigt.
• Antwoord: Ja
Tweede poging: hint: Denk eraan dat het bloed, als ereen circulatiestoornis is, altijd stroomt naar hersenen,longen en hart. Dit betekent dat de perifere organenminder bloed krijgen.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: Ja, er is een circulatiestoornis; een gezwollenvoet wijst erop dat er sprake is van centralisatie vanhet bloed naar hersenen, longen en hart.
Tweede poging: hint: Ga na of er sprake is vancentralisatie van bloed naar hersenen, hart en longen.Let op de kleur van de voet.
Derde poging: feedbak: Het goede antwoord luidt: Ja,want de voet is gezwollen.
Vragen Feedback
(6) Monitor [1]
• Is de hartfrequentie verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: verhoogd, hoog, snel, versneld.
• Is de systolische bloeddruk verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: verhoogd/hoog.
Tweede poging: hint: Wat is het effect op dehartfrequentie, als er sprake is van cyanose en/ofversnelde ademhaling?
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De hartfrequentie is verhoogd. Indien dehartfrequentie verhoogd is, is er sprake vancompensatie om toch de benodigde hoeveelheid bloedte transporteren.
Tweede poging: hint: Wat is het effect op desystolische bloeddruk, als er sprake is van cyanoseen/of versnelde ademhaling?
Derde poging: feedbak: De systolische bloeddruk is
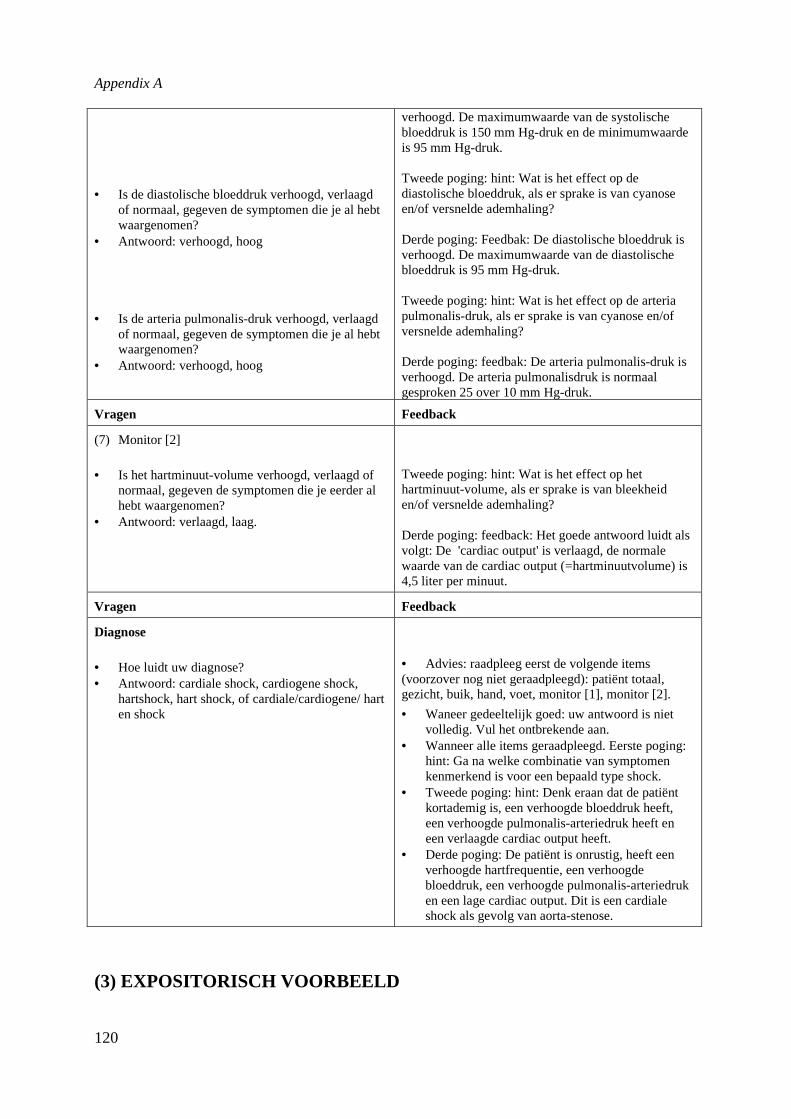
Appendix A
120
• Is de diastolische bloeddruk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: verhoogd, hoog
• Is de arteria pulmonalis-druk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: verhoogd, hoog
verhoogd. De maximumwaarde van de systolischebloeddruk is 150 mm Hg-druk en de minimumwaardeis 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op dediastolische bloeddruk, als er sprake is van cyanoseen/of versnelde ademhaling?
Derde poging: Feedbak: De diastolische bloeddruk isverhoogd. De maximumwaarde van de diastolischebloeddruk is 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op de arteriapulmonalis-druk, als er sprake is van cyanose en/ofversnelde ademhaling?
Derde poging: feedbak: De arteria pulmonalis-druk isverhoogd. De arteria pulmonalisdruk is normaalgesproken 25 over 10 mm Hg-druk.
Vragen Feedback
(7) Monitor [2]
• Is het hartminuut-volume verhoogd, verlaagd ofnormaal, gegeven de symptomen die je eerder alhebt waargenomen?
• Antwoord: verlaagd, laag.
Tweede poging: hint: Wat is het effect op hethartminuut-volume, als er sprake is van bleekheiden/of versnelde ademhaling?
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De 'cardiac output' is verlaagd, de normalewaarde van de cardiac output (=hartminuutvolume) is4,5 liter per minuut.
Vragen Feedback
Diagnose
• Hoe luidt uw diagnose?• Antwoord: cardiale shock, cardiogene shock,
hartshock, hart shock, of cardiale/cardiogene/ harten shock
• Advies: raadpleeg eerst de volgende items(voorzover nog niet geraadpleegd): patiënt totaal,gezicht, buik, hand, voet, monitor [1], monitor [2].
• Waneer gedeeltelijk goed: uw antwoord is nietvolledig. Vul het ontbrekende aan.
• Wanneer alle items geraadpleegd. Eerste poging:hint: Ga na welke combinatie van symptomenkenmerkend is voor een bepaald type shock.
• Tweede poging: hint: Denk eraan dat de patiëntkortademig is, een verhoogde bloeddruk heeft,een verhoogde pulmonalis-arteriedruk heeft eneen verlaagde cardiac output heeft.
• Derde poging: De patiënt is onrustig, heeft eenverhoogde hartfrequentie, een verhoogdebloeddruk, een verhoogde pulmonalis-arteriedruken een lage cardiac output. Dit is een cardialeshock als gevolg van aorta-stenose.
(3) EXPOSITORISCH VOORBEELD
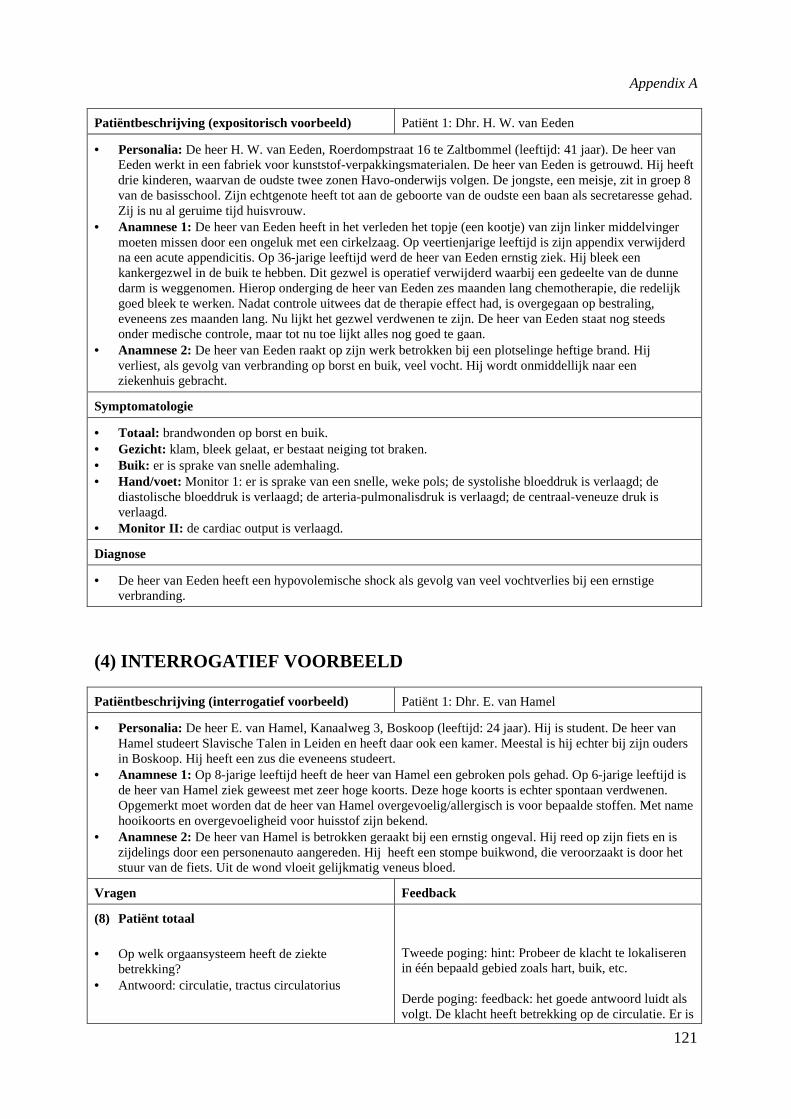
Appendix A
121
Patiëntbeschrijving (expositorisch voorbeeld) Patiënt 1: Dhr. H. W. van Eeden
• Personalia:De heer H. W. van Eeden, Roerdompstraat 16 te Zaltbommel (leeftijd: 41 jaar). De heer vanEeden werkt in een fabriek voor kunststof-verpakkingsmaterialen. De heer van Eeden is getrouwd. Hij heeftdrie kinderen, waarvan de oudste twee zonen Havo-onderwijs volgen. De jongste, een meisje, zit in groep 8van de basisschool. Zijn echtgenote heeft tot aan de geboorte van de oudste een baan als secretaresse gehad.Zij is nu al geruime tijd huisvrouw.
• Anamnese 1:De heer van Eeden heeft in het verleden het topje (een kootje) van zijn linker middelvingermoeten missen door een ongeluk met een cirkelzaag. Op veertienjarige leeftijd is zijn appendix verwijderdna een acute appendicitis. Op 36-jarige leeftijd werd de heer van Eeden ernstig ziek. Hij bleek eenkankergezwel in de buik te hebben. Dit gezwel is operatief verwijderd waarbij een gedeelte van de dunnedarm is weggenomen. Hierop onderging de heer van Eeden zes maanden lang chemotherapie, die redelijkgoed bleek te werken. Nadat controle uitwees dat de therapie effect had, is overgegaan op bestraling,eveneens zes maanden lang. Nu lijkt het gezwel verdwenen te zijn. De heer van Eeden staat nog steedsonder medische controle, maar tot nu toe lijkt alles nog goed te gaan.
• Anamnese 2:De heer van Eeden raakt op zijn werk betrokken bij een plotselinge heftige brand. Hijverliest, als gevolg van verbranding op borst en buik, veel vocht. Hij wordt onmiddellijk naar eenziekenhuis gebracht.
Symptomatologie
• Totaal: brandwonden op borst en buik.• Gezicht: klam, bleek gelaat, er bestaat neiging tot braken.• Buik: er is sprake van snelle ademhaling.• Hand/voet: Monitor 1: er is sprake van een snelle, weke pols; de systolishe bloeddruk is verlaagd; de
diastolische bloeddruk is verlaagd; de arteria-pulmonalisdruk is verlaagd; de centraal-veneuze druk isverlaagd.
• Monitor II: de cardiac output is verlaagd.
Diagnose
• De heer van Eeden heeft een hypovolemische shock als gevolg van veel vochtverlies bij een ernstigeverbranding.
(4) INTERROGATIEF VOORBEELD
Patiëntbeschrijving (interrogatief voorbeeld) Patiënt 1: Dhr. E. van Hamel
• Personalia:De heer E. van Hamel, Kanaalweg 3, Boskoop (leeftijd: 24 jaar). Hij is student. De heer vanHamel studeert Slavische Talen in Leiden en heeft daar ook een kamer. Meestal is hij echter bij zijn oudersin Boskoop. Hij heeft een zus die eveneens studeert.
• Anamnese 1:Op 8-jarige leeftijd heeft de heer van Hamel een gebroken pols gehad. Op 6-jarige leeftijd isde heer van Hamel ziek geweest met zeer hoge koorts. Deze hoge koorts is echter spontaan verdwenen.Opgemerkt moet worden dat de heer van Hamel overgevoelig/allergisch is voor bepaalde stoffen. Met namehooikoorts en overgevoeligheid voor huisstof zijn bekend.
• Anamnese 2:De heer van Hamel is betrokken geraakt bij een ernstig ongeval. Hij reed op zijn fiets en iszijdelings door een personenauto aangereden. Hij heeft een stompe buikwond, die veroorzaakt is door hetstuur van de fiets. Uit de wond vloeit gelijkmatig veneus bloed.
Vragen Feedback
(8) Patiënt totaal
• Op welk orgaansysteem heeft de ziektebetrekking?
• Antwoord: circulatie, tractus circulatorius
Tweede poging: hint: Probeer de klacht te lokaliserenin één bepaald gebied zoals hart, buik, etc.
Derde poging: feedback: het goede antwoord luidt alsvolgt. De klacht heeft betrekking op de circulatie. Er is
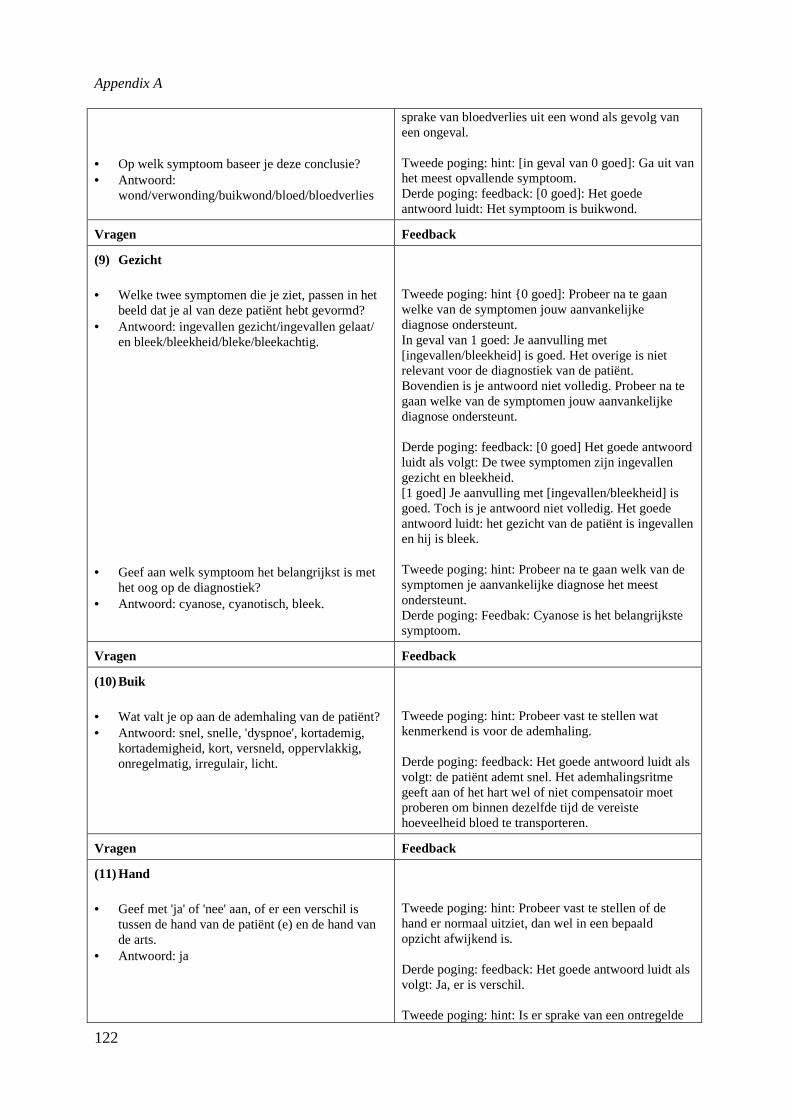
Appendix A
122
• Op welk symptoom baseer je deze conclusie?• Antwoord:
wond/verwonding/buikwond/bloed/bloedverlies
sprake van bloedverlies uit een wond als gevolg vaneen ongeval.
Tweede poging: hint: [in geval van 0 goed]: Ga uit vanhet meest opvallende symptoom.Derde poging: feedback: [0 goed]: Het goedeantwoord luidt: Het symptoom is buikwond.
Vragen Feedback
(9) Gezicht
• Welke twee symptomen die je ziet, passen in hetbeeld dat je al van deze patiënt hebt gevormd?
• Antwoord: ingevallen gezicht/ingevallen gelaat/en bleek/bleekheid/bleke/bleekachtig.
• Geef aan welk symptoom het belangrijkst is methet oog op de diagnostiek?
• Antwoord: cyanose, cyanotisch, bleek.
Tweede poging: hint {0 goed]: Probeer na te gaanwelke van de symptomen jouw aanvankelijkediagnose ondersteunt.In geval van 1 goed: Je aanvulling met[ingevallen/bleekheid] is goed. Het overige is nietrelevant voor de diagnostiek van de patiënt.Bovendien is je antwoord niet volledig. Probeer na tegaan welke van de symptomen jouw aanvankelijkediagnose ondersteunt.
Derde poging: feedback: [0 goed] Het goede antwoordluidt als volgt: De twee symptomen zijn ingevallengezicht en bleekheid.[1 goed] Je aanvulling met [ingevallen/bleekheid] isgoed. Toch is je antwoord niet volledig. Het goedeantwoord luidt: het gezicht van de patiënt is ingevallenen hij is bleek.
Tweede poging: hint: Probeer na te gaan welk van desymptomen je aanvankelijke diagnose het meestondersteunt.Derde poging: Feedbak: Cyanose is het belangrijkstesymptoom.
Vragen Feedback
(10) Buik
• Wat valt je op aan de ademhaling van de patiënt?• Antwoord: snel, snelle, 'dyspnoe', kortademig,
kortademigheid, kort, versneld, oppervlakkig,onregelmatig, irregulair, licht.
Tweede poging: hint: Probeer vast te stellen watkenmerkend is voor de ademhaling.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: de patiënt ademt snel. Het ademhalingsritmegeeft aan of het hart wel of niet compensatoir moetproberen om binnen dezelfde tijd de vereistehoeveelheid bloed te transporteren.
Vragen Feedback
(11) Hand
• Geef met 'ja' of 'nee' aan, of er een verschil istussen de hand van de patiënt (e) en de hand vande arts.
• Antwoord: ja
Tweede poging: hint: Probeer vast te stellen of dehand er normaal uitziet, dan wel in een bepaaldopzicht afwijkend is.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: Ja, er is verschil.
Tweede poging: hint: Is er sprake van een ontregelde
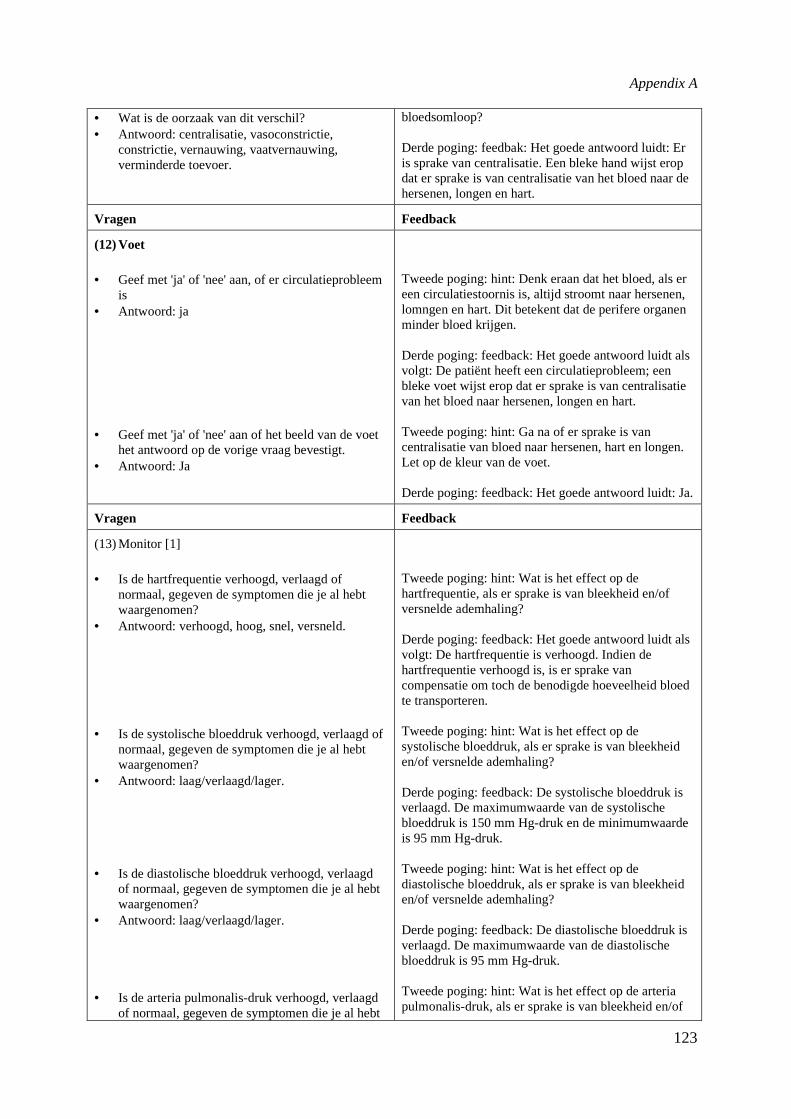
Appendix A
123
• Wat is de oorzaak van dit verschil?• Antwoord: centralisatie, vasoconstrictie,
constrictie, vernauwing, vaatvernauwing,verminderde toevoer.
bloedsomloop?
Derde poging: feedbak: Het goede antwoord luidt: Eris sprake van centralisatie. Een bleke hand wijst eropdat er sprake is van centralisatie van het bloed naar dehersenen, longen en hart.
Vragen Feedback
(12) Voet
• Geef met 'ja' of 'nee' aan, of er circulatieprobleemis
• Antwoord: ja
• Geef met 'ja' of 'nee' aan of het beeld van de voethet antwoord op de vorige vraag bevestigt.
• Antwoord: Ja
Tweede poging: hint: Denk eraan dat het bloed, als ereen circulatiestoornis is, altijd stroomt naar hersenen,lomngen en hart. Dit betekent dat de perifere organenminder bloed krijgen.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De patiënt heeft een circulatieprobleem; eenbleke voet wijst erop dat er sprake is van centralisatievan het bloed naar hersenen, longen en hart.
Tweede poging: hint: Ga na of er sprake is vancentralisatie van bloed naar hersenen, hart en longen.Let op de kleur van de voet.
Derde poging: feedback: Het goede antwoord luidt: Ja.
Vragen Feedback
(13) Monitor [1]
• Is de hartfrequentie verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: verhoogd, hoog, snel, versneld.
• Is de systolische bloeddruk verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: laag/verlaagd/lager.
• Is de diastolische bloeddruk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: laag/verlaagd/lager.
• Is de arteria pulmonalis-druk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebt
Tweede poging: hint: Wat is het effect op dehartfrequentie, als er sprake is van bleekheid en/ofversnelde ademhaling?
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De hartfrequentie is verhoogd. Indien dehartfrequentie verhoogd is, is er sprake vancompensatie om toch de benodigde hoeveelheid bloedte transporteren.
Tweede poging: hint: Wat is het effect op desystolische bloeddruk, als er sprake is van bleekheiden/of versnelde ademhaling?
Derde poging: feedback: De systolische bloeddruk isverlaagd. De maximumwaarde van de systolischebloeddruk is 150 mm Hg-druk en de minimumwaardeis 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op dediastolische bloeddruk, als er sprake is van bleekheiden/of versnelde ademhaling?
Derde poging: feedback: De diastolische bloeddruk isverlaagd. De maximumwaarde van de diastolischebloeddruk is 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op de arteriapulmonalis-druk, als er sprake is van bleekheid en/of
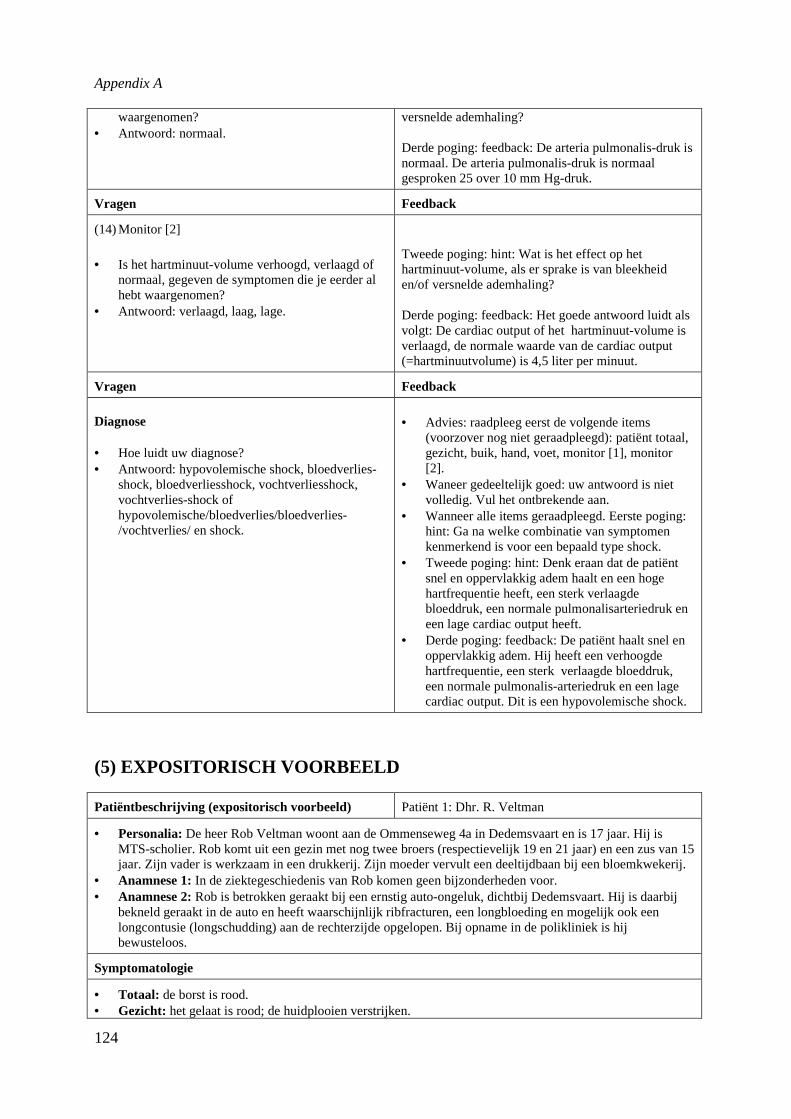
Appendix A
124
waargenomen?• Antwoord: normaal.
versnelde ademhaling?
Derde poging: feedback: De arteria pulmonalis-druk isnormaal. De arteria pulmonalis-druk is normaalgesproken 25 over 10 mm Hg-druk.
Vragen Feedback
(14) Monitor [2]
• Is het hartminuut-volume verhoogd, verlaagd ofnormaal, gegeven de symptomen die je eerder alhebt waargenomen?
• Antwoord: verlaagd, laag, lage.
Tweede poging: hint: Wat is het effect op hethartminuut-volume, als er sprake is van bleekheiden/of versnelde ademhaling?
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De cardiac output of het hartminuut-volume isverlaagd, de normale waarde van de cardiac output(=hartminuutvolume) is 4,5 liter per minuut.
Vragen Feedback
Diagnose
• Hoe luidt uw diagnose?• Antwoord: hypovolemische shock, bloedverlies-
shock, bloedverliesshock, vochtverliesshock,vochtverlies-shock ofhypovolemische/bloedverlies/bloedverlies-/vochtverlies/ en shock.
• Advies: raadpleeg eerst de volgende items(voorzover nog niet geraadpleegd): patiënt totaal,gezicht, buik, hand, voet, monitor [1], monitor[2].
• Waneer gedeeltelijk goed: uw antwoord is nietvolledig. Vul het ontbrekende aan.
• Wanneer alle items geraadpleegd. Eerste poging:hint: Ga na welke combinatie van symptomenkenmerkend is voor een bepaald type shock.
• Tweede poging: hint: Denk eraan dat de patiëntsnel en oppervlakkig adem haalt en een hogehartfrequentie heeft, een sterk verlaagdebloeddruk, een normale pulmonalisarteriedruk eneen lage cardiac output heeft.
• Derde poging: feedback: De patiënt haalt snel enoppervlakkig adem. Hij heeft een verhoogdehartfrequentie, een sterk verlaagde bloeddruk,een normale pulmonalis-arteriedruk en een lagecardiac output. Dit is een hypovolemische shock.
(5) EXPOSITORISCH VOORBEELD
Patiëntbeschrijving (expositorisch voorbeeld) Patiënt 1: Dhr. R. Veltman
• Personalia:De heer Rob Veltman woont aan de Ommenseweg 4a in Dedemsvaart en is 17 jaar. Hij isMTS-scholier. Rob komt uit een gezin met nog twee broers (respectievelijk 19 en 21 jaar) en een zus van 15jaar. Zijn vader is werkzaam in een drukkerij. Zijn moeder vervult een deeltijdbaan bij een bloemkwekerij.
• Anamnese 1:In de ziektegeschiedenis van Rob komen geen bijzonderheden voor.• Anamnese 2:Rob is betrokken geraakt bij een ernstig auto-ongeluk, dichtbij Dedemsvaart. Hij is daarbij
bekneld geraakt in de auto en heeft waarschijnlijk ribfracturen, een longbloeding en mogelijk ook eenlongcontusie (longschudding) aan de rechterzijde opgelopen. Bij opname in de polikliniek is hijbewusteloos.
Symptomatologie
• Totaal: de borst is rood.• Gezicht: het gelaat is rood; de huidplooien verstrijken.
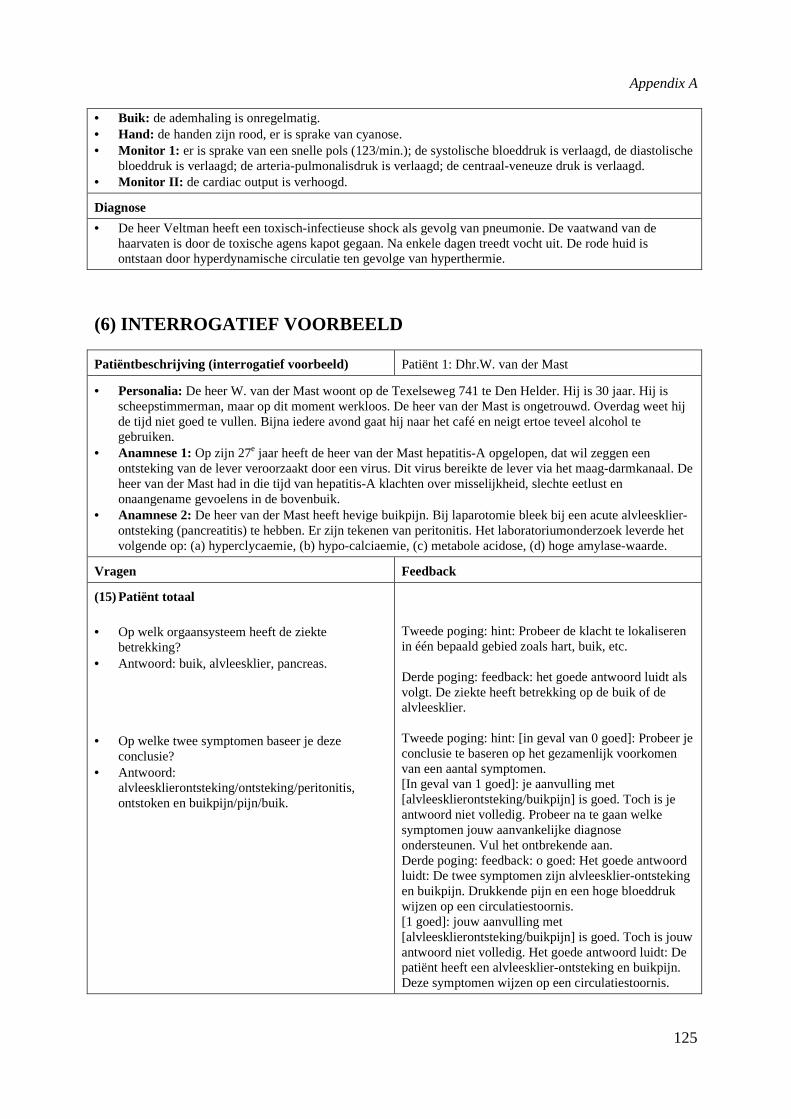
Appendix A
125
• Buik: de ademhaling is onregelmatig.• Hand: de handen zijn rood, er is sprake van cyanose.• Monitor 1: er is sprake van een snelle pols (123/min.); de systolische bloeddruk is verlaagd, de diastolische
bloeddruk is verlaagd; de arteria-pulmonalisdruk is verlaagd; de centraal-veneuze druk is verlaagd.• Monitor II: de cardiac output is verhoogd.
Diagnose
• De heer Veltman heeft een toxisch-infectieuse shock als gevolg van pneumonie. De vaatwand van dehaarvaten is door de toxische agens kapot gegaan. Na enkele dagen treedt vocht uit. De rode huid isontstaan door hyperdynamische circulatie ten gevolge van hyperthermie.
(6) INTERROGATIEF VOORBEELD
Patiëntbeschrijving (interrogatief voorbeeld) Patiënt 1: Dhr.W. van der Mast
• Personalia:De heer W. van der Mast woont op de Texelseweg 741 te Den Helder. Hij is 30 jaar. Hij isscheepstimmerman, maar op dit moment werkloos. De heer van der Mast is ongetrouwd. Overdag weet hijde tijd niet goed te vullen. Bijna iedere avond gaat hij naar het café en neigt ertoe teveel alcohol tegebruiken.
• Anamnese 1:Op zijn 27e jaar heeft de heer van der Mast hepatitis-A opgelopen, dat wil zeggen eenontsteking van de lever veroorzaakt door een virus. Dit virus bereikte de lever via het maag-darmkanaal. Deheer van der Mast had in die tijd van hepatitis-A klachten over misselijkheid, slechte eetlust enonaangename gevoelens in de bovenbuik.
• Anamnese 2:De heer van der Mast heeft hevige buikpijn. Bij laparotomie bleek bij een acute alvleesklier-ontsteking (pancreatitis) te hebben. Er zijn tekenen van peritonitis. Het laboratoriumonderzoek leverde hetvolgende op: (a) hyperclycaemie, (b) hypo-calciaemie, (c) metabole acidose, (d) hoge amylase-waarde.
Vragen Feedback
(15) Patiënt totaal
• Op welk orgaansysteem heeft de ziektebetrekking?
• Antwoord: buik, alvleesklier, pancreas.
• Op welke twee symptomen baseer je dezeconclusie?
• Antwoord:alvleesklierontsteking/ontsteking/peritonitis,ontstoken en buikpijn/pijn/buik.
Tweede poging: hint: Probeer de klacht te lokaliserenin één bepaald gebied zoals hart, buik, etc.
Derde poging: feedback: het goede antwoord luidt alsvolgt. De ziekte heeft betrekking op de buik of dealvleesklier.
Tweede poging: hint: [in geval van 0 goed]: Probeer jeconclusie te baseren op het gezamenlijk voorkomenvan een aantal symptomen.[In geval van 1 goed]: je aanvulling met[alvleesklierontsteking/buikpijn] is goed. Toch is jeantwoord niet volledig. Probeer na te gaan welkesymptomen jouw aanvankelijke diagnoseondersteunen. Vul het ontbrekende aan.Derde poging: feedback: o goed: Het goede antwoordluidt: De twee symptomen zijn alvleesklier-ontstekingen buikpijn. Drukkende pijn en een hoge bloeddrukwijzen op een circulatiestoornis.[1 goed]: jouw aanvulling met[alvleesklierontsteking/buikpijn] is goed. Toch is jouwantwoord niet volledig. Het goede antwoord luidt: Depatiënt heeft een alvleesklier-ontsteking en buikpijn.Deze symptomen wijzen op een circulatiestoornis.
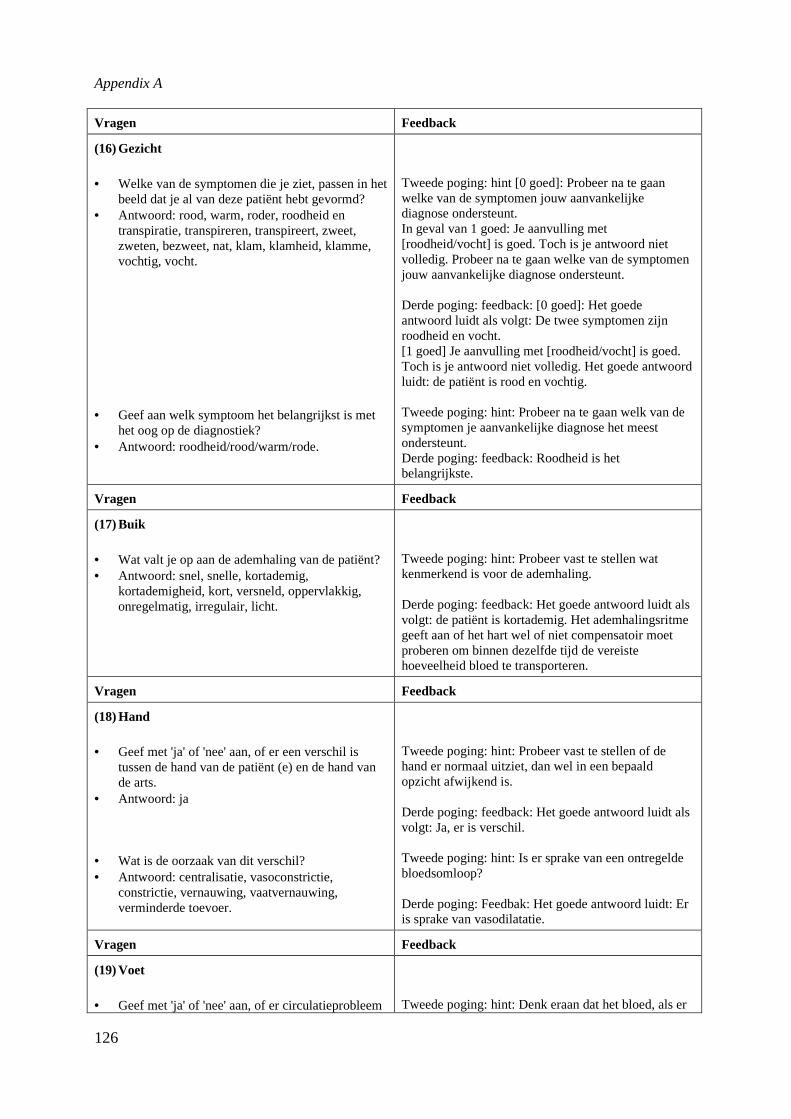
Appendix A
126
Vragen Feedback
(16) Gezicht
• Welke van de symptomen die je ziet, passen in hetbeeld dat je al van deze patiënt hebt gevormd?
• Antwoord: rood, warm, roder, roodheid entranspiratie, transpireren, transpireert, zweet,zweten, bezweet, nat, klam, klamheid, klamme,vochtig, vocht.
• Geef aan welk symptoom het belangrijkst is methet oog op de diagnostiek?
• Antwoord: roodheid/rood/warm/rode.
Tweede poging: hint [0 goed]: Probeer na te gaanwelke van de symptomen jouw aanvankelijkediagnose ondersteunt.In geval van 1 goed: Je aanvulling met[roodheid/vocht] is goed. Toch is je antwoord nietvolledig. Probeer na te gaan welke van de symptomenjouw aanvankelijke diagnose ondersteunt.
Derde poging: feedback: [0 goed]: Het goedeantwoord luidt als volgt: De twee symptomen zijnroodheid en vocht.[1 goed] Je aanvulling met [roodheid/vocht] is goed.Toch is je antwoord niet volledig. Het goede antwoordluidt: de patiënt is rood en vochtig.
Tweede poging: hint: Probeer na te gaan welk van desymptomen je aanvankelijke diagnose het meestondersteunt.Derde poging: feedback: Roodheid is hetbelangrijkste.
Vragen Feedback
(17) Buik
• Wat valt je op aan de ademhaling van de patiënt?• Antwoord: snel, snelle, kortademig,
kortademigheid, kort, versneld, oppervlakkig,onregelmatig, irregulair, licht.
Tweede poging: hint: Probeer vast te stellen watkenmerkend is voor de ademhaling.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: de patiënt is kortademig. Het ademhalingsritmegeeft aan of het hart wel of niet compensatoir moetproberen om binnen dezelfde tijd de vereistehoeveelheid bloed te transporteren.
Vragen Feedback
(18) Hand
• Geef met 'ja' of 'nee' aan, of er een verschil istussen de hand van de patiënt (e) en de hand vande arts.
• Antwoord: ja
• Wat is de oorzaak van dit verschil?• Antwoord: centralisatie, vasoconstrictie,
constrictie, vernauwing, vaatvernauwing,verminderde toevoer.
Tweede poging: hint: Probeer vast te stellen of dehand er normaal uitziet, dan wel in een bepaaldopzicht afwijkend is.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: Ja, er is verschil.
Tweede poging: hint: Is er sprake van een ontregeldebloedsomloop?
Derde poging: Feedbak: Het goede antwoord luidt: Eris sprake van vasodilatatie.
Vragen Feedback
(19) Voet
• Geef met 'ja' of 'nee' aan, of er circulatieprobleemTweede poging: hint: Denk eraan dat het bloed, als er
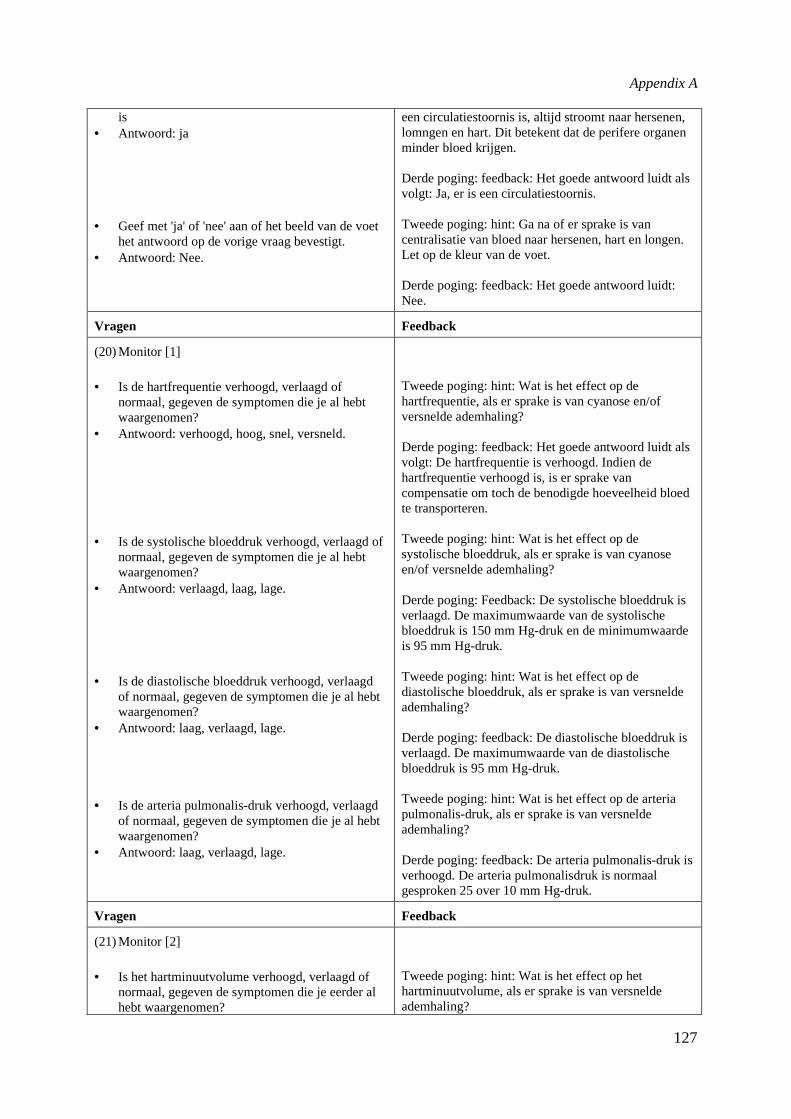
Appendix A
127
is• Antwoord: ja
• Geef met 'ja' of 'nee' aan of het beeld van de voethet antwoord op de vorige vraag bevestigt.
• Antwoord: Nee.
een circulatiestoornis is, altijd stroomt naar hersenen,lomngen en hart. Dit betekent dat de perifere organenminder bloed krijgen.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: Ja, er is een circulatiestoornis.
Tweede poging: hint: Ga na of er sprake is vancentralisatie van bloed naar hersenen, hart en longen.Let op de kleur van de voet.
Derde poging: feedback: Het goede antwoord luidt:Nee.
Vragen Feedback
(20) Monitor [1]
• Is de hartfrequentie verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: verhoogd, hoog, snel, versneld.
• Is de systolische bloeddruk verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: verlaagd, laag, lage.
• Is de diastolische bloeddruk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: laag, verlaagd, lage.
• Is de arteria pulmonalis-druk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: laag, verlaagd, lage.
Tweede poging: hint: Wat is het effect op dehartfrequentie, als er sprake is van cyanose en/ofversnelde ademhaling?
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De hartfrequentie is verhoogd. Indien dehartfrequentie verhoogd is, is er sprake vancompensatie om toch de benodigde hoeveelheid bloedte transporteren.
Tweede poging: hint: Wat is het effect op desystolische bloeddruk, als er sprake is van cyanoseen/of versnelde ademhaling?
Derde poging: Feedback: De systolische bloeddruk isverlaagd. De maximumwaarde van de systolischebloeddruk is 150 mm Hg-druk en de minimumwaardeis 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op dediastolische bloeddruk, als er sprake is van versneldeademhaling?
Derde poging: feedback: De diastolische bloeddruk isverlaagd. De maximumwaarde van de diastolischebloeddruk is 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op de arteriapulmonalis-druk, als er sprake is van versneldeademhaling?
Derde poging: feedback: De arteria pulmonalis-druk isverhoogd. De arteria pulmonalisdruk is normaalgesproken 25 over 10 mm Hg-druk.
Vragen Feedback
(21) Monitor [2]
• Is het hartminuutvolume verhoogd, verlaagd ofnormaal, gegeven de symptomen die je eerder alhebt waargenomen?
Tweede poging: hint: Wat is het effect op hethartminuutvolume, als er sprake is van versneldeademhaling?
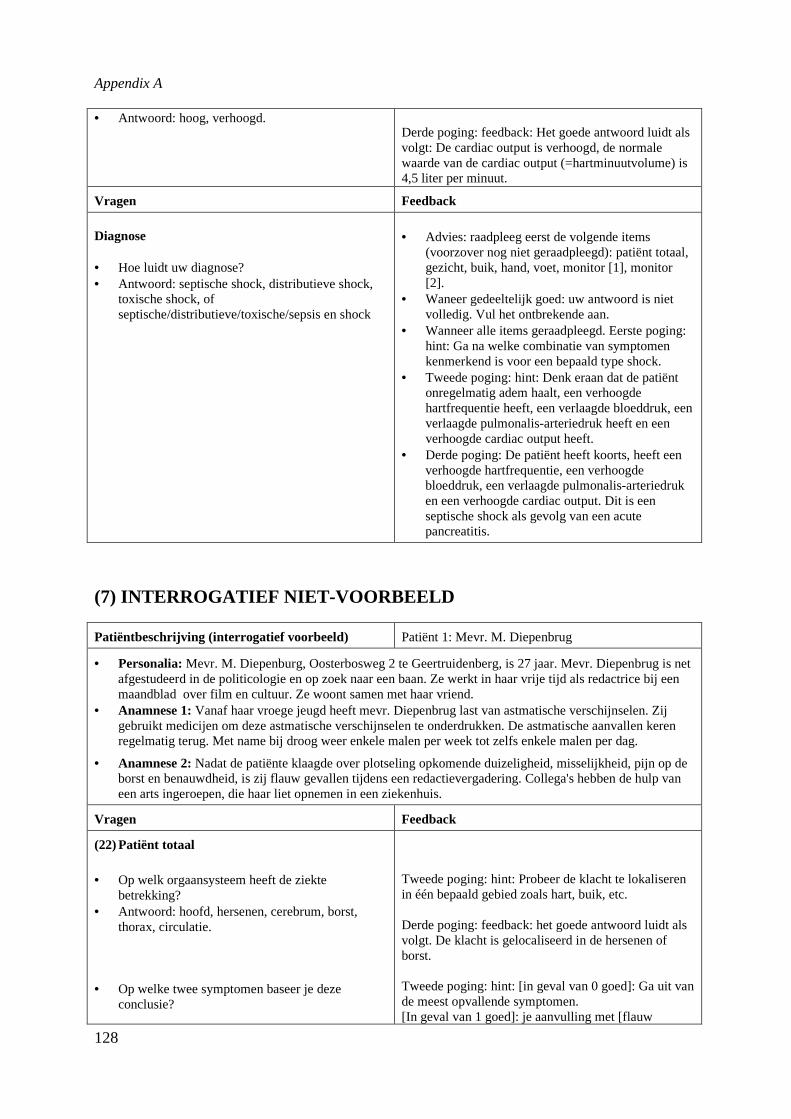
Appendix A
128
• Antwoord: hoog, verhoogd.Derde poging: feedback: Het goede antwoord luidt alsvolgt: De cardiac output is verhoogd, de normalewaarde van de cardiac output (=hartminuutvolume) is4,5 liter per minuut.
Vragen Feedback
Diagnose
• Hoe luidt uw diagnose?• Antwoord: septische shock, distributieve shock,
toxische shock, ofseptische/distributieve/toxische/sepsis en shock
• Advies: raadpleeg eerst de volgende items(voorzover nog niet geraadpleegd): patiënt totaal,gezicht, buik, hand, voet, monitor [1], monitor[2].
• Waneer gedeeltelijk goed: uw antwoord is nietvolledig. Vul het ontbrekende aan.
• Wanneer alle items geraadpleegd. Eerste poging:hint: Ga na welke combinatie van symptomenkenmerkend is voor een bepaald type shock.
• Tweede poging: hint: Denk eraan dat de patiëntonregelmatig adem haalt, een verhoogdehartfrequentie heeft, een verlaagde bloeddruk, eenverlaagde pulmonalis-arteriedruk heeft en eenverhoogde cardiac output heeft.
• Derde poging: De patiënt heeft koorts, heeft eenverhoogde hartfrequentie, een verhoogdebloeddruk, een verlaagde pulmonalis-arteriedruken een verhoogde cardiac output. Dit is eenseptische shock als gevolg van een acutepancreatitis.
(7) INTERROGATIEF NIET-VOORBEELD
Patiëntbeschrijving (interrogatief voorbeeld) Patiënt 1: Mevr. M. Diepenbrug
• Personalia:Mevr. M. Diepenburg, Oosterbosweg 2 te Geertruidenberg, is 27 jaar. Mevr. Diepenbrug is netafgestudeerd in de politicologie en op zoek naar een baan. Ze werkt in haar vrije tijd als redactrice bij eenmaandblad over film en cultuur. Ze woont samen met haar vriend.
• Anamnese 1:Vanaf haar vroege jeugd heeft mevr. Diepenbrug last van astmatische verschijnselen. Zijgebruikt medicijen om deze astmatische verschijnselen te onderdrukken. De astmatische aanvallen kerenregelmatig terug. Met name bij droog weer enkele malen per week tot zelfs enkele malen per dag.
• Anamnese 2:Nadat de patiënte klaagde over plotseling opkomende duizeligheid, misselijkheid, pijn op deborst en benauwdheid, is zij flauw gevallen tijdens een redactievergadering. Collega's hebben de hulp vaneen arts ingeroepen, die haar liet opnemen in een ziekenhuis.
Vragen Feedback
(22) Patiënt totaal
• Op welk orgaansysteem heeft de ziektebetrekking?
• Antwoord: hoofd, hersenen, cerebrum, borst,thorax, circulatie.
• Op welke twee symptomen baseer je dezeconclusie?
Tweede poging: hint: Probeer de klacht te lokaliserenin één bepaald gebied zoals hart, buik, etc.
Derde poging: feedback: het goede antwoord luidt alsvolgt. De klacht is gelocaliseerd in de hersenen ofborst.
Tweede poging: hint: [in geval van 0 goed]: Ga uit vande meest opvallende symptomen.[In geval van 1 goed]: je aanvulling met [flauw
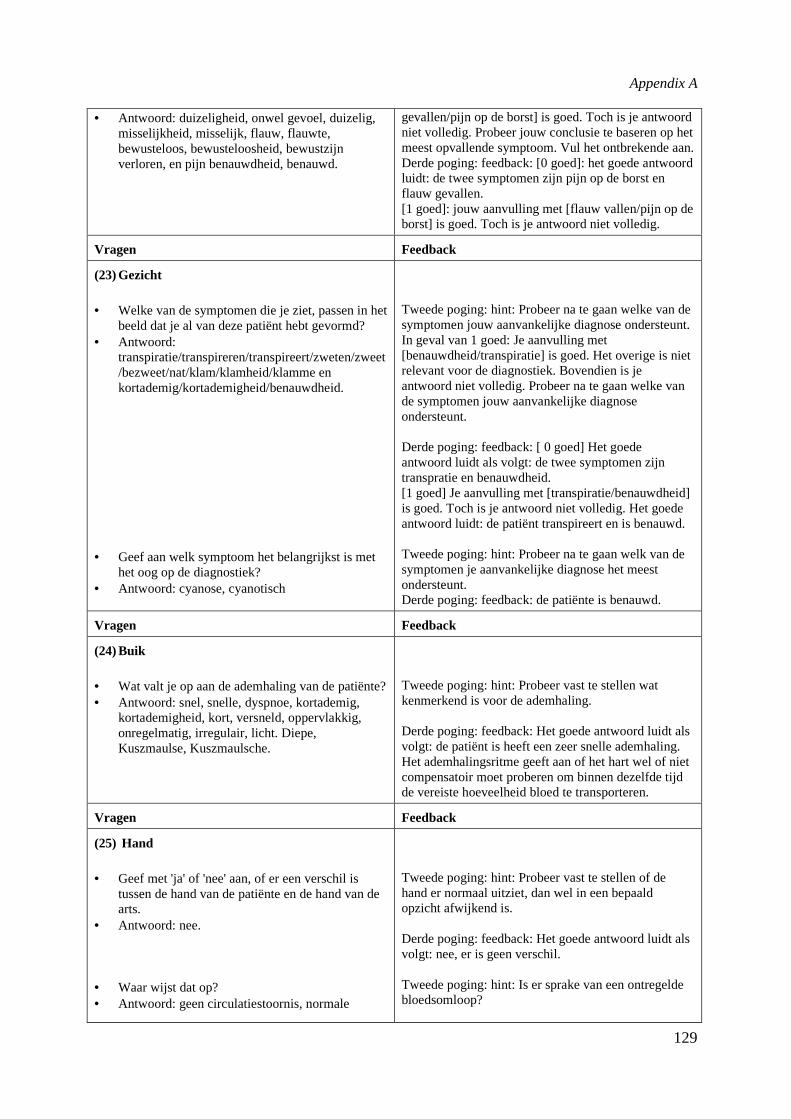
Appendix A
129
• Antwoord: duizeligheid, onwel gevoel, duizelig,misselijkheid, misselijk, flauw, flauwte,bewusteloos, bewusteloosheid, bewustzijnverloren, en pijn benauwdheid, benauwd.
gevallen/pijn op de borst] is goed. Toch is je antwoordniet volledig. Probeer jouw conclusie te baseren op hetmeest opvallende symptoom. Vul het ontbrekende aan.Derde poging: feedback: [0 goed]: het goede antwoordluidt: de twee symptomen zijn pijn op de borst enflauw gevallen.[1 goed]: jouw aanvulling met [flauw vallen/pijn op deborst] is goed. Toch is je antwoord niet volledig.
Vragen Feedback
(23) Gezicht
• Welke van de symptomen die je ziet, passen in hetbeeld dat je al van deze patiënt hebt gevormd?
• Antwoord:transpiratie/transpireren/transpireert/zweten/zweet/bezweet/nat/klam/klamheid/klamme enkortademig/kortademigheid/benauwdheid.
• Geef aan welk symptoom het belangrijkst is methet oog op de diagnostiek?
• Antwoord: cyanose, cyanotisch
Tweede poging: hint: Probeer na te gaan welke van desymptomen jouw aanvankelijke diagnose ondersteunt.In geval van 1 goed: Je aanvulling met[benauwdheid/transpiratie] is goed. Het overige is nietrelevant voor de diagnostiek. Bovendien is jeantwoord niet volledig. Probeer na te gaan welke vande symptomen jouw aanvankelijke diagnoseondersteunt.
Derde poging: feedback: [ 0 goed] Het goedeantwoord luidt als volgt: de twee symptomen zijntranspratie en benauwdheid.[1 goed] Je aanvulling met [transpiratie/benauwdheid]is goed. Toch is je antwoord niet volledig. Het goedeantwoord luidt: de patiënt transpireert en is benauwd.
Tweede poging: hint: Probeer na te gaan welk van desymptomen je aanvankelijke diagnose het meestondersteunt.Derde poging: feedback: de patiënte is benauwd.
Vragen Feedback
(24) Buik
• Wat valt je op aan de ademhaling van de patiënte?• Antwoord: snel, snelle, dyspnoe, kortademig,
kortademigheid, kort, versneld, oppervlakkig,onregelmatig, irregulair, licht. Diepe,Kuszmaulse, Kuszmaulsche.
Tweede poging: hint: Probeer vast te stellen watkenmerkend is voor de ademhaling.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: de patiënt is heeft een zeer snelle ademhaling.Het ademhalingsritme geeft aan of het hart wel of nietcompensatoir moet proberen om binnen dezelfde tijdde vereiste hoeveelheid bloed te transporteren.
Vragen Feedback
(25) Hand
• Geef met 'ja' of 'nee' aan, of er een verschil istussen de hand van de patiënte en de hand van dearts.
• Antwoord: nee.
• Waar wijst dat op?• Antwoord: geen circulatiestoornis, normale
Tweede poging: hint: Probeer vast te stellen of dehand er normaal uitziet, dan wel in een bepaaldopzicht afwijkend is.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: nee, er is geen verschil.
Tweede poging: hint: Is er sprake van een ontregeldebloedsomloop?
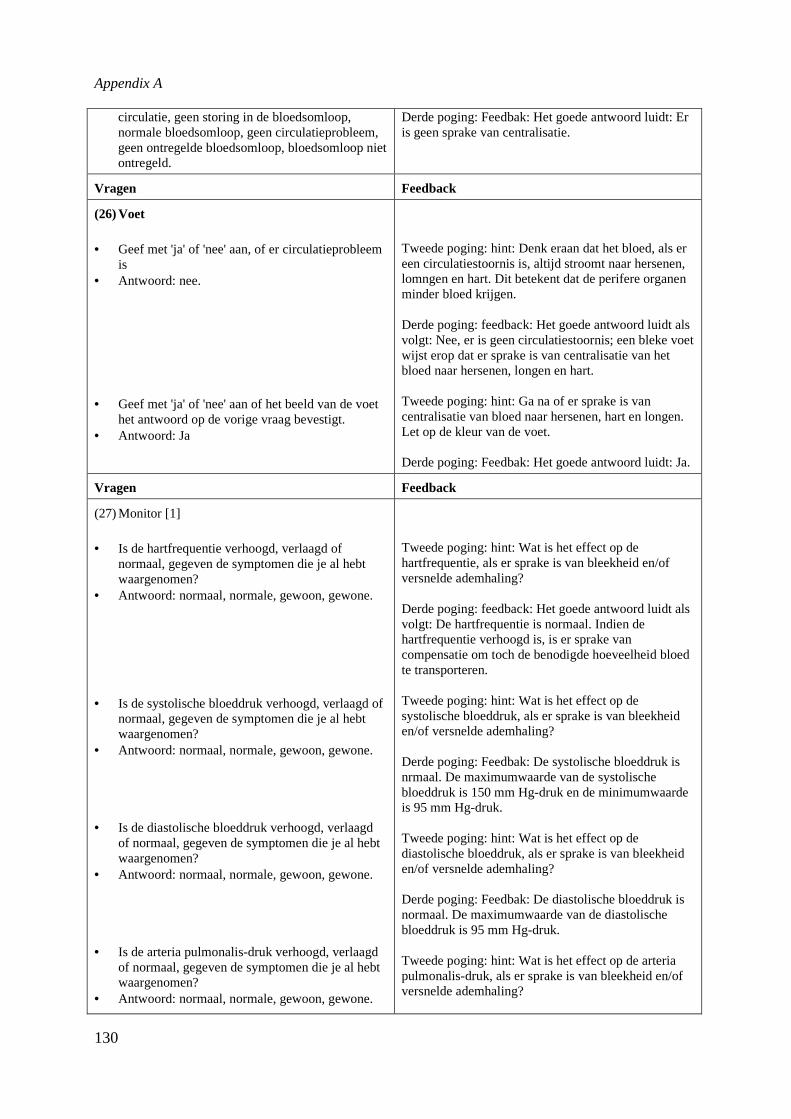
Appendix A
130
circulatie, geen storing in de bloedsomloop,normale bloedsomloop, geen circulatieprobleem,geen ontregelde bloedsomloop, bloedsomloop nietontregeld.
Derde poging: Feedbak: Het goede antwoord luidt: Eris geen sprake van centralisatie.
Vragen Feedback
(26) Voet
• Geef met 'ja' of 'nee' aan, of er circulatieprobleemis
• Antwoord: nee.
• Geef met 'ja' of 'nee' aan of het beeld van de voethet antwoord op de vorige vraag bevestigt.
• Antwoord: Ja
Tweede poging: hint: Denk eraan dat het bloed, als ereen circulatiestoornis is, altijd stroomt naar hersenen,lomngen en hart. Dit betekent dat de perifere organenminder bloed krijgen.
Derde poging: feedback: Het goede antwoord luidt alsvolgt: Nee, er is geen circulatiestoornis; een bleke voetwijst erop dat er sprake is van centralisatie van hetbloed naar hersenen, longen en hart.
Tweede poging: hint: Ga na of er sprake is vancentralisatie van bloed naar hersenen, hart en longen.Let op de kleur van de voet.
Derde poging: Feedbak: Het goede antwoord luidt: Ja.
Vragen Feedback
(27) Monitor [1]
• Is de hartfrequentie verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: normaal, normale, gewoon, gewone.
• Is de systolische bloeddruk verhoogd, verlaagd ofnormaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: normaal, normale, gewoon, gewone.
• Is de diastolische bloeddruk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: normaal, normale, gewoon, gewone.
• Is de arteria pulmonalis-druk verhoogd, verlaagdof normaal, gegeven de symptomen die je al hebtwaargenomen?
• Antwoord: normaal, normale, gewoon, gewone.
Tweede poging: hint: Wat is het effect op dehartfrequentie, als er sprake is van bleekheid en/ofversnelde ademhaling?
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De hartfrequentie is normaal. Indien dehartfrequentie verhoogd is, is er sprake vancompensatie om toch de benodigde hoeveelheid bloedte transporteren.
Tweede poging: hint: Wat is het effect op desystolische bloeddruk, als er sprake is van bleekheiden/of versnelde ademhaling?
Derde poging: Feedbak: De systolische bloeddruk isnrmaal. De maximumwaarde van de systolischebloeddruk is 150 mm Hg-druk en de minimumwaardeis 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op dediastolische bloeddruk, als er sprake is van bleekheiden/of versnelde ademhaling?
Derde poging: Feedbak: De diastolische bloeddruk isnormaal. De maximumwaarde van de diastolischebloeddruk is 95 mm Hg-druk.
Tweede poging: hint: Wat is het effect op de arteriapulmonalis-druk, als er sprake is van bleekheid en/ofversnelde ademhaling?
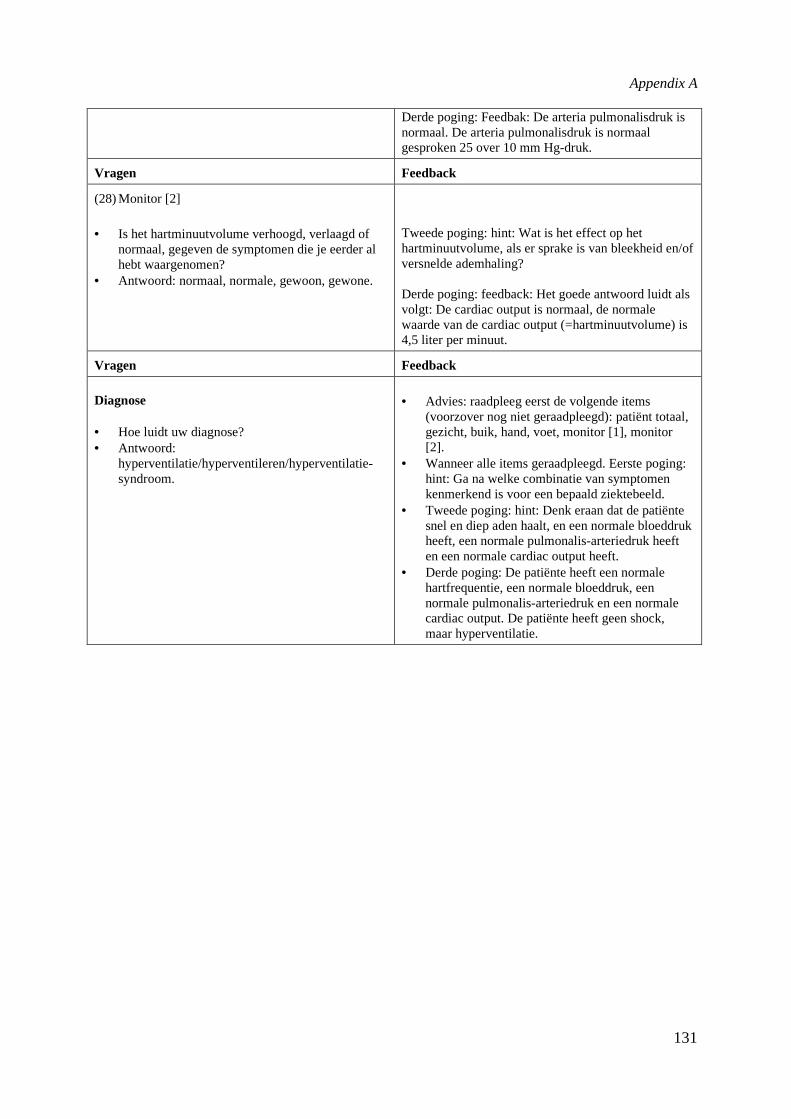
Appendix A
131
Derde poging: Feedbak: De arteria pulmonalisdruk isnormaal. De arteria pulmonalisdruk is normaalgesproken 25 over 10 mm Hg-druk.
Vragen Feedback
(28) Monitor [2]
• Is het hartminuutvolume verhoogd, verlaagd ofnormaal, gegeven de symptomen die je eerder alhebt waargenomen?
• Antwoord: normaal, normale, gewoon, gewone.
Tweede poging: hint: Wat is het effect op hethartminuutvolume, als er sprake is van bleekheid en/ofversnelde ademhaling?
Derde poging: feedback: Het goede antwoord luidt alsvolgt: De cardiac output is normaal, de normalewaarde van de cardiac output (=hartminuutvolume) is4,5 liter per minuut.
Vragen Feedback
Diagnose
• Hoe luidt uw diagnose?• Antwoord:
hyperventilatie/hyperventileren/hyperventilatie-syndroom.
• Advies: raadpleeg eerst de volgende items(voorzover nog niet geraadpleegd): patiënt totaal,gezicht, buik, hand, voet, monitor [1], monitor[2].
• Wanneer alle items geraadpleegd. Eerste poging:hint: Ga na welke combinatie van symptomenkenmerkend is voor een bepaald ziektebeeld.
• Tweede poging: hint: Denk eraan dat de patiëntesnel en diep aden haalt, en een normale bloeddrukheeft, een normale pulmonalis-arteriedruk heeften een normale cardiac output heeft.
• Derde poging: De patiënte heeft een normalehartfrequentie, een normale bloeddruk, eennormale pulmonalis-arteriedruk en een normalecardiac output. De patiënte heeft geen shock,maar hyperventilatie.

Appendix A
154
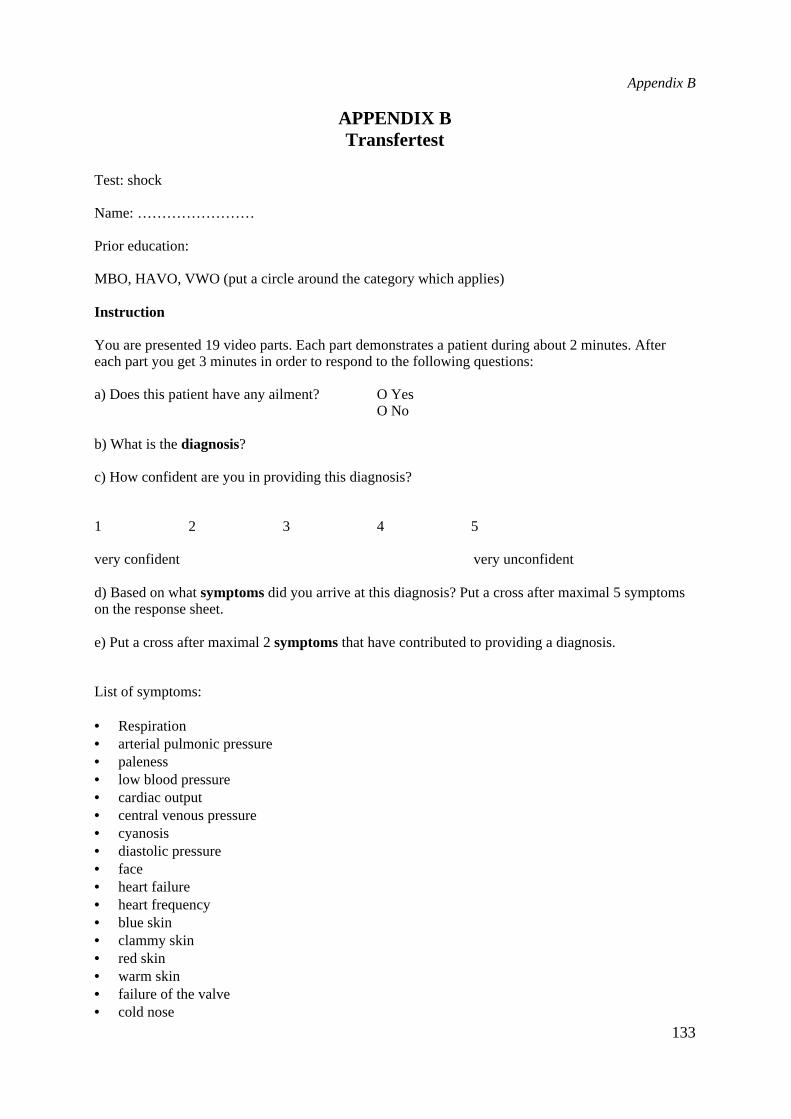
Appendix B
133
APPENDIX BTransfertest
Test: shock
Name: ……………………
Prior education:
MBO, HAVO, VWO (put a circle around the category which applies)
Instruction
You are presented 19 video parts. Each part demonstrates a patient during about 2 minutes. Aftereach part you get 3 minutes in order to respond to the following questions:
a) Does this patient have any ailment? O YesO No
b) What is thediagnosis?
c) How confident are you in providing this diagnosis?
1 2 3 4 5
very confident very unconfident
d) Based on whatsymptomsdid you arrive at this diagnosis? Put a cross after maximal 5 symptomson the response sheet.
e) Put a cross after maximal 2symptomsthat have contributed to providing a diagnosis.
List of symptoms:
• Respiration• arterial pulmonic pressure• paleness• low blood pressure• cardiac output• central venous pressure• cyanosis• diastolic pressure• face• heart failure• heart frequency• blue skin• clammy skin• red skin• warm skin• failure of the valve• cold nose
Appendix B
134
• oedema• peripheral vessel resistance• fast pulse• rhythmic disturbances of the heart• systolic pressure• temperature• perspiration• urinary output• dizziness• liquid balance• wedge pressure• use of oxygen
Appendix C
135
APPENDIX CGlossary of prerequisite knowledge
The prerequisite knowledge base contains the full text for each key word.
Acidosis is an increase of acids in the human body. If there is an insufficient perfusion of the tissues,cells tend to combust anaerobically (without oxygen) nutrients due to which debris (lactic acid)emerges which tends to cause damage to the tissues if there is insufficient outlet. Acidosis emergesin case of shock or is caused by respiratory diseases (respiratory acidosis). In the last case the lungcannot produce sufficiently carbonic acid. Thirdly acidosis can emerge due to metabolicdisturbances where a surplus of acid is produced (for example diabetes mellitus). The body canameliorate the situation where the acidosis occurs by an increased production of acid via the kidneyand lungs (carbonic acid) or by an increased production of bicarbonate in the kidney (such that theacid neutralizes). Also the blood has a buffer capacity.
Anemia is shortage of blood, a disease characterized by paleness (due to a too low Hb and/or ashortage of circulating erytrocytes), shortage of breath in case of effort, dizziness and fatigue. TheHb normally is about 140 g/l.
Angina pectoris refers to the symptoms which occur due to a shortage of oxygen in the heart. Shortageof oxygen in the myocardial muscle occurs in case of constriction of the coronary arteries due toarteriosclerosis. Or spasm in these vessels and in case of rhythm disturbances of the heart. Strictlyspeaking angina pectoris is not a vessel disease but, because the heart has to cope with the directconsequences of the constriction, angina pectoris is subsumed under heart diseases. Symptoms are:(a) constricting pain at the sternum, (b) fear, (c) radiation of the pain to the leg, hand, little finger orjaw (mostly at the left side).
Anoxia is a shortage of oxygen in the tissues. This can be caused due to a too low amount of oxygen inthe blood or in the inhaled air. If this situation persists too long, irreversible damage emerges to thetissues.
Anuria is the (temporary) incapability of the kidneys to produce urine (less than 0,3 l /24 hour). Due toless perfusion of the kidneys and/or due to a too low pressure of blood, the kidneys are incapable toproduce urine.
Arithmia is the common term for an irregular working of the heart. Under others in case of fibrillationand-fladdering., ventricle fibrillation, tachycardia and bradycardia there is arrhythmia. The mostdeviations in heart frequencies show also an abnormal pattern at the ECG-monitor.
Arteria pulmonalis pressure is the pressure in the pulmonal arteria. This pressure is measured using acatheter in the lung arteria. The catheter is put in via an arteria in the collum area and is directed viathe right chamber and right atrium in the arteria pulmonalis. The arteria pulmonalis pressurenormally is 25mmHg. If the arteria pulmonalis pressure is increased, a cor pulmonale can emerge.If the arteria pulmonalis is decreased, it can be a sign of right decompensation.
Astma cardiale is an impediment in the permeability of the minor breath due to left decompensation.Therefore liquid can excudate from the lung capillaries (lung oedema). There is now less blood-oxygen contact, due to which the substitution of oxygen and carbonic acid tends to decrease.
Backward failure refers to the consequences of a venous congestion behind the failing heart chamber.The arterial blood is insufficiently processed. In case of backward failure the consequences of afailure of the circulation are manifested backwardly. Due to a decreased perfusion the kidneys willtend to produce less liquid and salt, due to which oedema will emerge. One differentiates betweenbackward failure of the left half of the heart (left decompensation) and of the right half of the heart(right decompensation). Symptoms are: (a) congestion in the veins, (b) increased central venouspressure, (c) decrease of the heart minute volume, (d) decrease of the blood pressure, (e) a fast andweak pulse, (f) breathlessness and tickling cough, and (g) the emergence of oedema.
Blood pressure is the pressure of the blood at the arterial valve. The blood pressure is a derivative oftwo factors: the flow and the resistance. Think of Ohm's Law. The flow in our body is the heartminute volume. The resistance is the pressure of the blood on the arterial valve. The blood pressuredepends on the elasticity of the arterial valve, the tone (tension state) of the arterial valve, the
Appendix C
136
circulating volume and the viscosity of the blood, the resistance in the peripheral blood circulationand the power of the heart action.
Body circulation or grand circulation is a system which provides: a) the supply of oxygen towards thetissues, b) the outlet of carbonic acid from the tissues, c) transport of the cell's products ashormones and nutrition, d) transport of debris to organs which take care of the outlet. The bodycirculation goes from the left atrium via the aorta to the tissues and from the tissues via the venacava to the right atrium.
Bradycardia is involved if there is an abnormally decreased heart with a pulse of less than 60 beats perminute. This occurs in case of brain-, heart-, and abdominal diseases, toxication die to digitalis etc.
Burns result in that much liquid from the body evaporates or is given of (exude). Due to too lessliquid, the volume of plasma decreases in the blood and therefore the circulating blood volume.
Cardiac output per minute is equal to the heart minute volume. It refers to the average amount of bloodprocessed by the heart in a minute.
Central venous pressure is the pressure in both concave arteries and the right chamber. The bloodpressure in the body circulation decreases to the degree that the blood flows further from the rightventricle. Especially in the venous system the pressure tends to decrease, to about 4-mmHg when itenters the right chamber. The central venous pressure is normally 4-8 mmHg.
Centralisation of the blood means that the blood tends to centralize in the vital organs as heart, lungsand brain. This occurs if there is too less circulating blood volume in the body in order to provideblood to all organs.
Cor pulmonale refers to an overload of the right heart due to lung deviations, where there is noprimary heart disturbance. If the pressure in the lung circulation is increased, then a cor pulmonalewill emerge (heavily pumping and insufficient contraction).
Cyanosis refers to situation in which the skin and mucous membranes tend to be blue due to the factthat dark red blood (insufficiently oxygen bounded hemoglobine in the blood) gleams through thedark, pink skin (compare a blue stain). Normally blood contains 140 g/l hemoglobine. If minimally50 g/l of hemoglobine is not bounded to oxygen, then cyanosis will emerge. When the strength ofperfusion in the blood vessels is low (low pressure) an extra amount of oxygen will be taken fromthe blood; cyanosis will therefore emerge. If the body takes too less oxygen (due to a lung problem)if arterial and venous blood merge (due to an inherited deviation of the heart), or if there ispoisoning, then cyanosis will emerge.
Diastolic phase is the phase in which the chambers relax due to which blood flows from the atriums tothe chambers. At the end of the diastole the contraction of the bossom takes place. The diastolicblood pressure is determined by the peripheral resistance and the degree of filling of the peripheralsystem. The diastolic blood pressure is normally about 40 mmHg lower than the systolic bloodpressure. Normal value for the diastolic blood pressure is 70 to 80 mmHg. Increased normally isthe pressure 90 mmHg. A too high diastolic blood pressure is or can be very damaging for the heartand blood vessels.
Electrocardiogram (ECG) is used for the monitoring of patients. A normal monitor ECG is attainedwith the use of 3 to 4 elektrodes which are placed upon the body. The norma rithm is called thesinus rithm. This rithm is regulated by the sinus node.
Excitatory-transductory system comprises multiple parts: a) the sinus node normally produces astimulus. This stimulus is transducted via the fibers in the atria. The frequency of the sinus node isabout 72 times per minute; b) the atrioventricular node receives the stimulus and delays it (bloodrequires time to flow from the atriums towards the ventricles). The frequency of the AV-node, ifthe sinus node drops out, is about 50 to 60 times per minute; c) the Bundle of His receives thestimulus from the AV-node and the stimulus proceeds towards the bundles and the Purkinje fibers.The Bundle of His has, when also the AV-node does no longer produce a stimulus, a frequency ofabout 40 stimuli per minute. After the fibers of Purkinje, a chain reaction of depolarization of heartmuscle fibers and the ventricles tend to contract. The frequency of the fibers of Purkinje is about 20to 40 times per minute. The influence exerted upon the heart frequency is mediated through thesinus node.
Fibrillation of the atrium is a form of heart arrhythmia in the atrium. Due to this the … producesuncoordinated movements. The chamber pulses irregularly, because not all stimuli reach the
Appendix C
137
chambers, but coordinated. The chamber's ouput depends on the filling which strongly varies dueto differences in the bosom beats.
Fladdering of the atrium is a form of heart arrhythmia where the bosoms contract rhythmically veryfast (300 per minute).
Forward failure refers to symptoms due to a decreased heart minute volume. An insufficient amount ofblood is pumped into the aorta; therefore the blood pressure decreases and the tissues like thekidneys get a too less amount of blood. Causes can be cardiopathy, myocard infarction, a strongacute loss of blood or liquid or an acute dilatation of the vessels. If the symptoms emerge slowly, abackward failure will be caused. The effects of forward failure are manifested forwardly. Thekidneys have to cope with that problem; a less amount of liquid is produced, due to which thecirculating volume is increased, the load on the heart is increased and the heart minute volumetends to decrease. Symptoms of forward failure are: (a) decrease of heart minute volume, (b)decrease of systolic blood pressure, (c) insufficient perfusion of the tissues, (d) decrease of theurinary output.
Heart frequency of a normal, calm heart amounts to 70 beats a minute, with a variation of about 60 to100 beats a minute. Extreme low heart activity occurs if the sinus node can no longer provide anadequate stimulus. If the heart is required to supply a greater demand of blood then the sympaticactivity will tend to increase and the parasympatic activity will decrease, due to which the heartfrequency will increase.
Heart is constituted from: a) the endocard which covers the inner side of the atriums and chambers; b)the myocard wich is constituted from muscle fiber with a specific construction; c) the pericardiumwhich covers the heart at the outer side; d) the excitatory - and transductory system. This isconstituted from the sinus node, the AV-node, the bundle of His, and both branch blocks.
Heart minute volume is the amount of blood in liters which is processed by the heart in a minute. Incase of normal adults the heart minute volume is 4.5 to 5.5 liter per minute.
Heart tamponade is an acute compression of the heart due to the fact that the pericadium is filled withblood. Due to a great infarction gangrene of the heart's valve occurs. Due to the high pressure in theheart the valve of the heart muscle is ruptured and blood flows in the pericardium. Most of the timethis is preceded by shock, an increase of the central venous pressure and a decrease of the bloodpressure. In case of a heart tamponade the effectiveness of the heart is impeded severely.
Infections may cause a massive vasodilatation, a high fever, shivering and insufficiency of the kidney.Infliction implies a damaged tissue, due to which blood is excudated from the circulation. One
differentiates between inner and outer inflictions. Also in case of an inner wound (abdominal, at thechest) a huge amount of blood can be lost.
Kidney will produce less or none urine, due to a decrease of the blood pressure as caused byinsufficient filling of the tissue system, or by a shortage of oxygen in the cells. Due to that themetabolic process is impeded. In case of less than 25 ml urinary output per hour there is oliguria;this is a serious state if it persists. In case of less than 5 ml urinary output per hour there is anuria.In case of a persistence of a too low blood pressure a part of the kidney can die back.
Left decompensation means that the pump function of the left chamber falls short. Insufficient blood ispumped towards the aorta, the heart minute volume decreases and the pressure in the left halve ofthe heart increases due to the fact that blood stays in the heart. Dilatation of the left part of the heartoccurs and blood stays in the lungs (backward failure). Astma cardiale due to lung oedema canresult from left decompensation. If insufficient blood is pumped into the aorta, insufficient bloodwill flow towards the tissues (under which the kidneys) and oliguria and oedema will emerge(forward failure). Symptoms are: a) dyspnoe in rest, b) tickling cough, c) fast and weak pulse, d)low blood pressure, e) cold skin, f) fatigue, g) cyanotic extremities and oedema, h) rattlingrespiration.
Loss of body liquid occurs in case of dehydration due to vomiting or diarrhoea, heath or burns. Due toa shortness of liquid, the circulating volume will decrease.
Lung emboly is a congestion of the lung artery due to a embolus from another part of the body. Due tothis the supply of blood towards the left part of the heart is impeded and the circulation tends todecrease. The transport of oxygen decreases or stops. If this situation persists for longer than 3
Appendix C
138
minutes vital organs will be damaged severely. Eventually the patient will pass away. Because theblood cannot enter the lungs, an acute right decompensation can emerge.
Lung oedema emerges if the pressure in the left part of the heart increases and the blood cannot enterin that part of the heart. Because of this pulmonary congestion emerges. Due to the pulmonarycongestion the pressure in the veins of the lungs increases. In case of a high pressure in the veins ofthe lungs oedema will evolve in the lungs. Apart from an increasing pressure in the left part of theheart oedema of the lung can evolve due to insufficiency of the kidney.
Mean arterial pressure (MAP) is equal to the heart minute volume (HMV) times the total peripheralresistance (TPR). So MAP=HMV * TPR. MAP = 2/3 diastolic pressure + 1/3 systolic pressure.The Mean Arterial Pressure is about 90 mmHg. It is an indicator of the perfusion of the vitalorgans. With an average arterial pressure of less than 50 mmHg the perfusion of vital organs tendsto decrease.
Micro-circulation takes place at the pre-capillary -, the capillary -, and the post-capillary level. Theper-capillary vessels can be opened or not. The perfusion is determined by the opening of the pre-capillary sphincters. The capillaries have as their function to supply oxygen and nutrients to the celland, at the venous side, to take in carbonic acid and debris. If due to insufficient filling of thevessels the peripheral circulation decreases, the micro-circulation falls short. Processes occurwhich, if the state does not change, can result in irreversible disturbances as badly healing littlesores, gangrene and ulcus cruris.
Myocardinfarction means the occlusion of a little or a great branch of the coronary artery. Thesymptoms of the heart infarction are: a) pain at the chest, b) transpiration, c) emesis and nausea
Oedema is an abnormal increase of liquid in the tissues. This is caused by a general or localcongestion or by changes in the composition of the blood. Due to a decrease of the amount ofprotein in the blood the oncotic pressure decreases, due to which the liquid of the issue isinsufficiently taken in.
Ortho-sympathical system is a part of the autonomous or vegetative nervous system. The sympaticusis active when we are active. The muscle tone increases, as well as the perfusion of the organs. Theconsciousness and the responsiveness are increased. The frequency and strength of the heartincrease. The metabolism decreases. The respiration becomes faster.
Pale skin is a consequence of too less blood in the capillaries of the skin. If there is too less circulatingblood in order to provide sufficiently blood to all tissues, the blood vessels in the tissues which canfunction without a temporary supply of blood, for example the skin, will tend to constrict(vasoconstriction). Also if the body tends to loose too much warmth, the blood disappears from theskin's surface. People with a too low amount of hemoglobine tend to look pale, especially theirmucous membranes.
Parasympathetical system is a part of the autonomous - or vegatative nervous system. Theparasympaticus is active if we are in rest. The parasympaticus takes care of the relaxation of themuscles, a decrease of the perfusion and outlet of lactic acid. The frequency and strength of theheart decreases and the metabolism is increased.
Red colour and becoming warm result from the opening of arterio-venous anastomosis in the skin, dueto which the perfusion of the skin increases.
Respiration implies that the inhaled air flows via the nose or the mouth, through the larynx and thetrachea towards the pulmonary alveoli. Here the oxygen is taken from the air and carbonic acid itput away. Carbonic acid is put away by the exhalation. Inhalated air is saturated with vapour.Adults have a respiration of 16-20 times per minute. The ratio between the number of respiratoryacts and the pulse is commonly 1:4.
Right decompensation is an insufficient functioning of the right chamber. The central venous pressureincreases and a congestion of the venous system results. Due to that oedema evolves at the rightankle (backward failure). Due to dilatation of the right part of the heart less blood enters the lungsand also less blood enters the aorta. Due to that less blood flows towards the tissues and oliguriaemerges and also a forward failure. If right decompensation results from left decompensation thepatient is temporary less breathless.
Small circulation or lung circulation is the system that guarantees the perfusion of the lungs. Thefunction of it is to take in oxygen and to outlet carbonic acid at the capillary level. From the right
Appendix C
139
chamber the blood flows via the arteria pulmonalis (lung artery), the capillaries of the lung and thevenae pulmonales to the left atrium. In the lungs the blood takes in oxygen and outlets carbonicacid. The arteries contain less oxygenous blood (hypoxia), the veins have a high saturation withoxygen. The blood pressure in the lung circulation is lower than that in the body circulation. Ifthere is a disturbance in the lung circulation, that will result in that the body cells receiveinsufficient supply of oxygen. In order to increase the amount of oxygen, the patient will tend tobreathe faster. If during a longer period a too less amount of oxygen is taken in and thus aninsufficient saturation will emerge, the body will tend to produce more red cells (secundarypolycythemia).
Systolic phase is the phase in which the chambers contract, due to which blood enters the arteries. Thesystolic blood pressure (upper pressure) is the blood pressure during the systolic phase. Thesystolic blood pressure is determined by the strength of the heart and the elasticity of the vessel'svalve. Normally the systolic blood pressure amounts to 120mmHg-150mmHG. Growing older thevessel's valve becomes less elastic, resulting in an increase of the systolic blood pressure. Due toinsufficient filling of the vasculature the systolic blood pressure will decrease. If this systolic bloodpressure decreases beneath 80mmHg an alarming situation emerges.
Tachycardia is an abnormally increased heart with a pulse of more than 100 beats per minute. Thisoccurs in case of strong emotions, strong effort, heart diseases, fever and toxication, pain andunderfilling of the vasculature.
Transpiration (perspiration) means that liquid is produced by the sweat glands in the skin. Normallythat amounts to 1 litter per 24 hrs. The goal of transpiration is to maintain the body's temperatureby evaporation. Under the influence of sympathetical activity the transpiration is increased. Coldsweat occurs with shock, collapse in case of dying.
Vasoconstriction refers to constriction of the blood vessels. To the degree that there is moresympathetical excitation, more contraction of the vessels will occur. Due to that the total peripheralresistance of the vessels will increase and especially the diastolic pressure will increase.Vasoconstriction results thus in an increased blood pressure. Remember the formula: MAP=CO*TPR (see blood pressure). Due to a low pressure in the arteries the sympathetical system isactivated via the Baroreflex. Therefore the peripheral blood vessels contract.
Vasodilatation refers to expansion of the vessels. This can occur due to the influence of certain factorswhich decrease the sympathetical activity. Vasodilatation results in a decrease of the totalperipheral resistance and therefore in a decrease of the blood pressure.
Ventricle fibrillation is a serious situation. Parts of the ventricle contract incoherently. A systole doesnot come and thus there is no sensible pulse. The heart minute volume is very low, comparablewith a heart block.
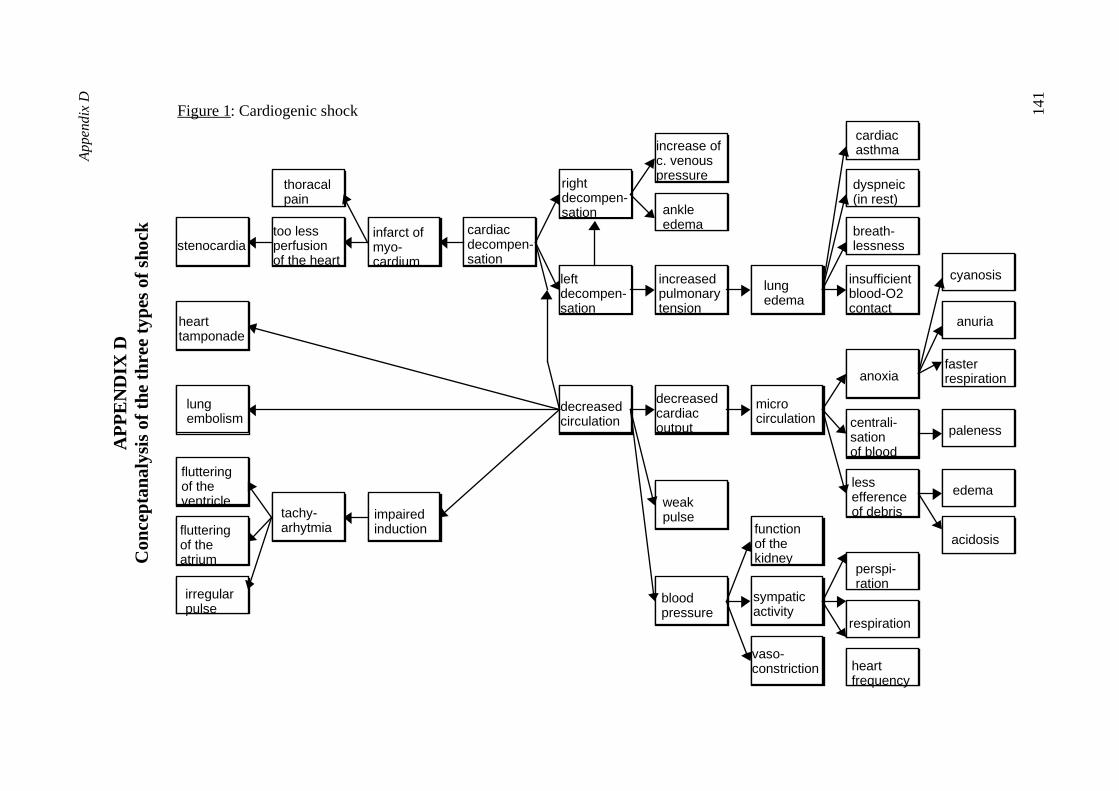
Ap
pe
nd
ixD
141
AP
PE
ND
IXD
Con
cept
anal
ysis
ofth
eth
ree
type
sof
shoc
k
too lessperfusionof the heart
infarct ofmyo-cardium
cardiacdecompen-sation
thoracalpain
rightdecompen-sation
leftdecompen-sation
ankleedema
increase ofc. venouspressure
increasedpulmonarytension
lungedema
cardiacasthma
dyspneic(in rest)
breath-lessness
insufficientblood-O2contact
hearttamponade
lungembolism
impairedinduction
decreasedcirculation
stenocardia
tachy-arhytmiafluttering
of theatrium
flutteringof theventricle
decreasedcardiacoutput
weakpulse
bloodpressure
microcirculation
functionof thekidney
sympaticactivity
vaso-constriction
paleness
respiration
heartfrequency
perspi-ration
anoxia
centrali-sationof blood
lessefferenceof debris
edema
acidosis
fasterrespiration
anuria
cyanosis
irregularpulse
Figure 1: Cardiogenic shock
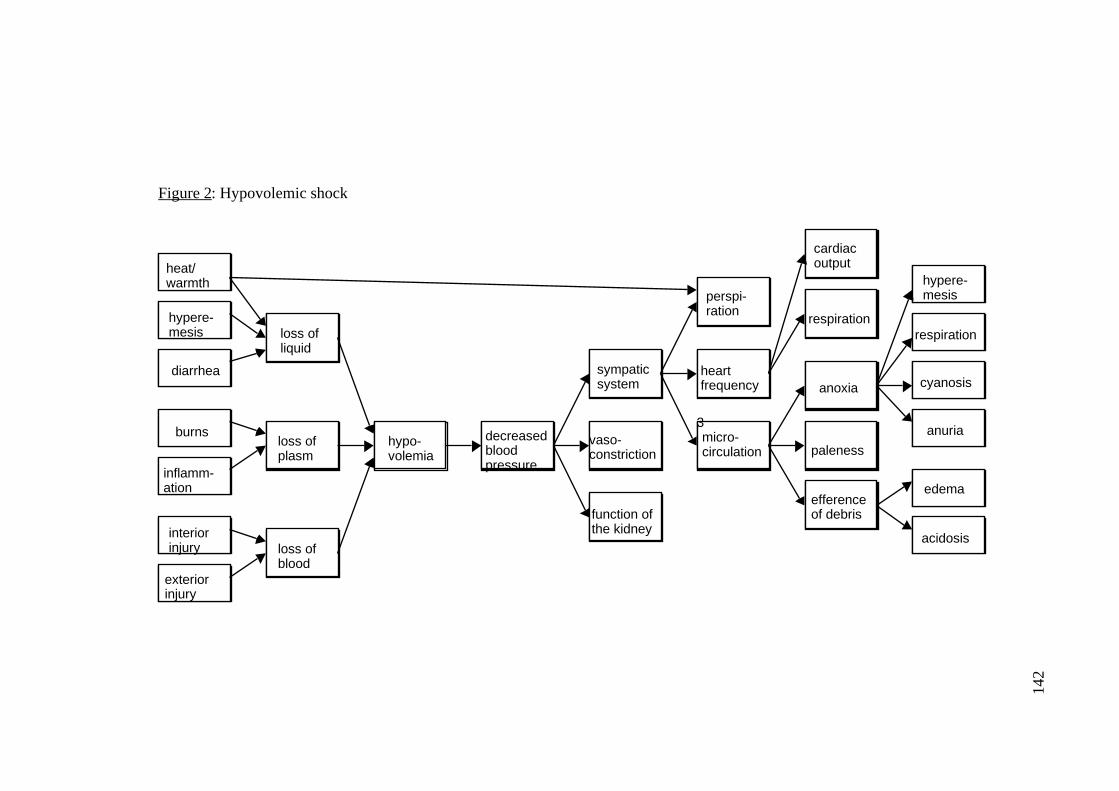
142
heat/warmth
hypere-mesis
diarrhea
burns
inflamm-ation
interiorinjury
exteriorinjury
loss ofliquid
loss ofplasm
loss ofblood
hypo-volemia
vaso-constriction
function ofthe kidney
perspi-ration
heartfrequency
micro-circulation
cardiacoutput
respiration
decreasedbloodpressure
sympaticsystem
efferenceof debris
paleness
anoxia
hypere-mesis
respiration
cyanosis
anuria
edema
acidosis
3
Figure 2: Hypovolemic shock
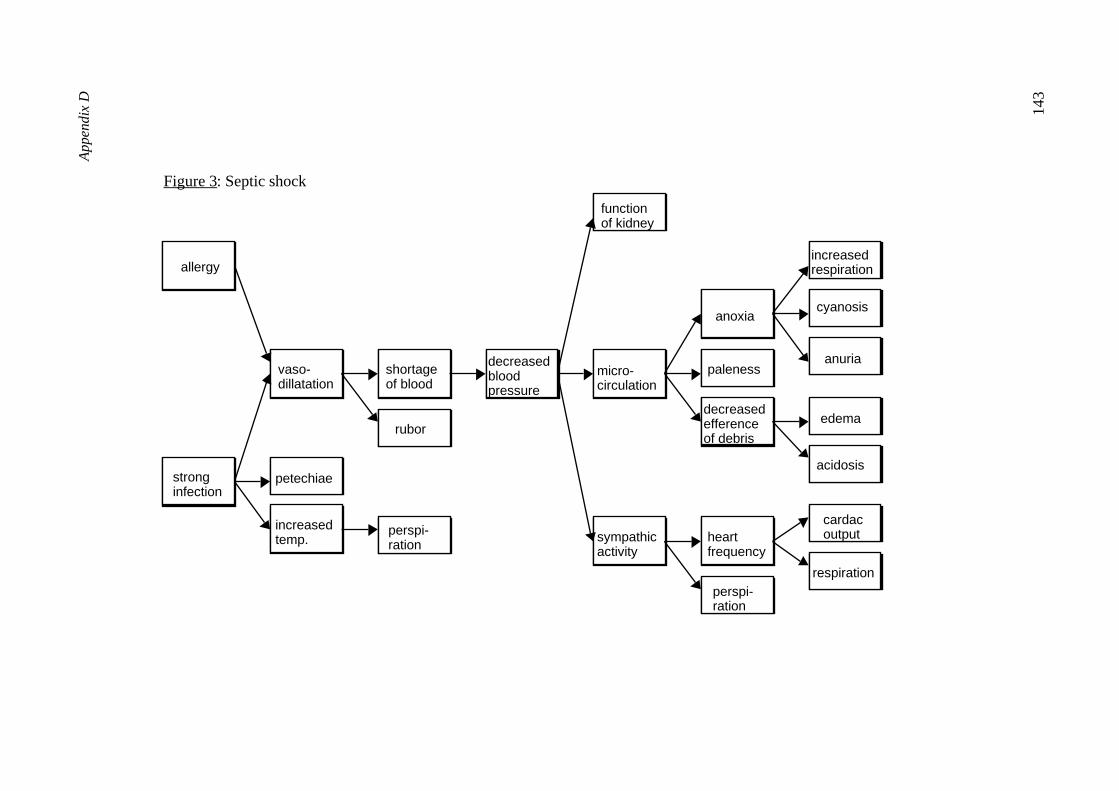
Ap
pe
nd
ixD
143
Figure 3: Septic shock
allergy
rubor
stronginfection
vaso-dillatation
increasedtemp.
petechiae
shortageof blood
decreasedbloodpressure
perspi-ration
functionof kidney
micro-circulation
sympathicactivity
heartfrequency
perspi-ration
anoxia
paleness
cardacoutput
decreasedefferenceof debris
respiration
increasedrespiration
cyanosis
anuria
edema
acidosis

166
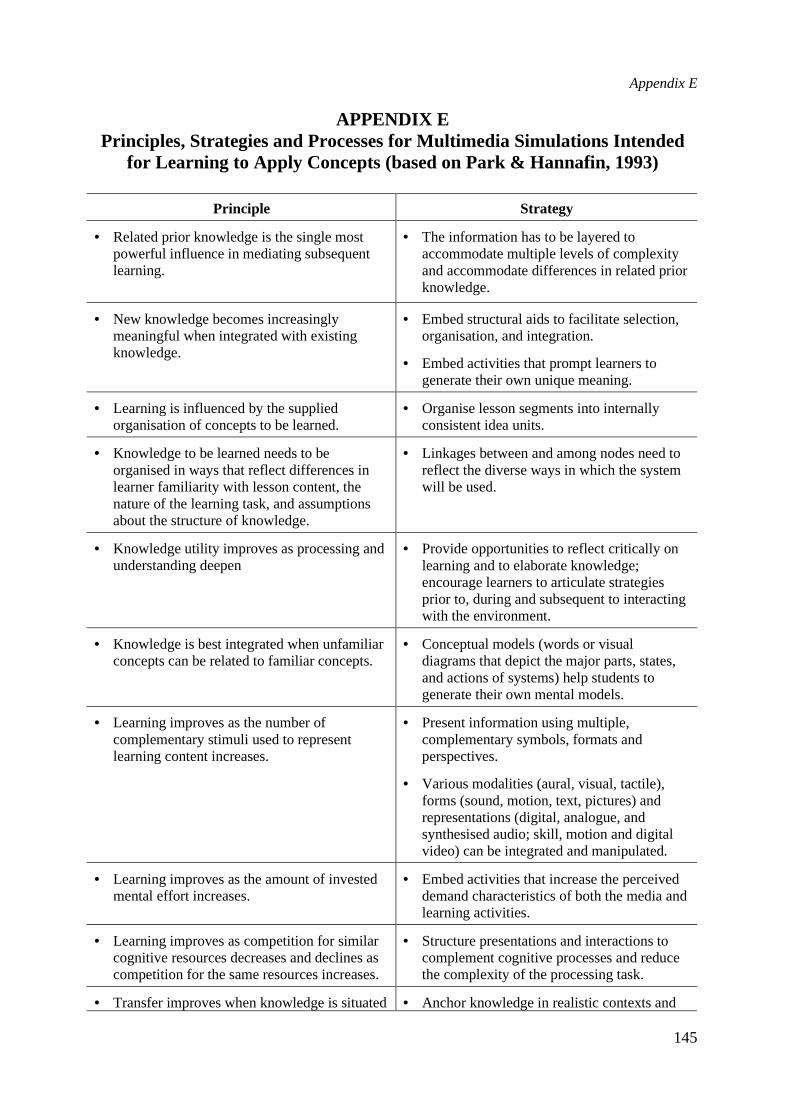
Appendix E
145
APPENDIX EPrinciples, Strategies and Processes for Multimedia Simulations Intended
for Learning to Apply Concepts (based on Park & Hannafin, 1993)
Principle Strategy
• Related prior knowledge is the single mostpowerful influence in mediating subsequentlearning.
• The information has to be layered toaccommodate multiple levels of complexityand accommodate differences in related priorknowledge.
• New knowledge becomes increasinglymeaningful when integrated with existingknowledge.
• Embed structural aids to facilitate selection,organisation, and integration.
• Embed activities that prompt learners togenerate their own unique meaning.
• Learning is influenced by the suppliedorganisation of concepts to be learned.
• Organise lesson segments into internallyconsistent idea units.
• Knowledge to be learned needs to beorganised in ways that reflect differences inlearner familiarity with lesson content, thenature of the learning task, and assumptionsabout the structure of knowledge.
• Linkages between and among nodes need toreflect the diverse ways in which the systemwill be used.
• Knowledge utility improves as processing andunderstanding deepen
• Provide opportunities to reflect critically onlearning and to elaborate knowledge;encourage learners to articulate strategiesprior to, during and subsequent to interactingwith the environment.
• Knowledge is best integrated when unfamiliarconcepts can be related to familiar concepts.
• Conceptual models (words or visualdiagrams that depict the major parts, states,and actions of systems) help students togenerate their own mental models.
• Learning improves as the number ofcomplementary stimuli used to representlearning content increases.
• Present information using multiple,complementary symbols, formats andperspectives.
• Various modalities (aural, visual, tactile),forms (sound, motion, text, pictures) andrepresentations (digital, analogue, andsynthesised audio; skill, motion and digitalvideo) can be integrated and manipulated.
• Learning improves as the amount of investedmental effort increases.
• Embed activities that increase the perceiveddemand characteristics of both the media andlearning activities.
• Learning improves as competition for similarcognitive resources decreases and declines ascompetition for the same resources increases.
• Structure presentations and interactions tocomplement cognitive processes and reducethe complexity of the processing task.
• Transfer improves when knowledge is situated• Anchor knowledge in realistic contexts and

Appendix E
146
in authentic contexts. settings.
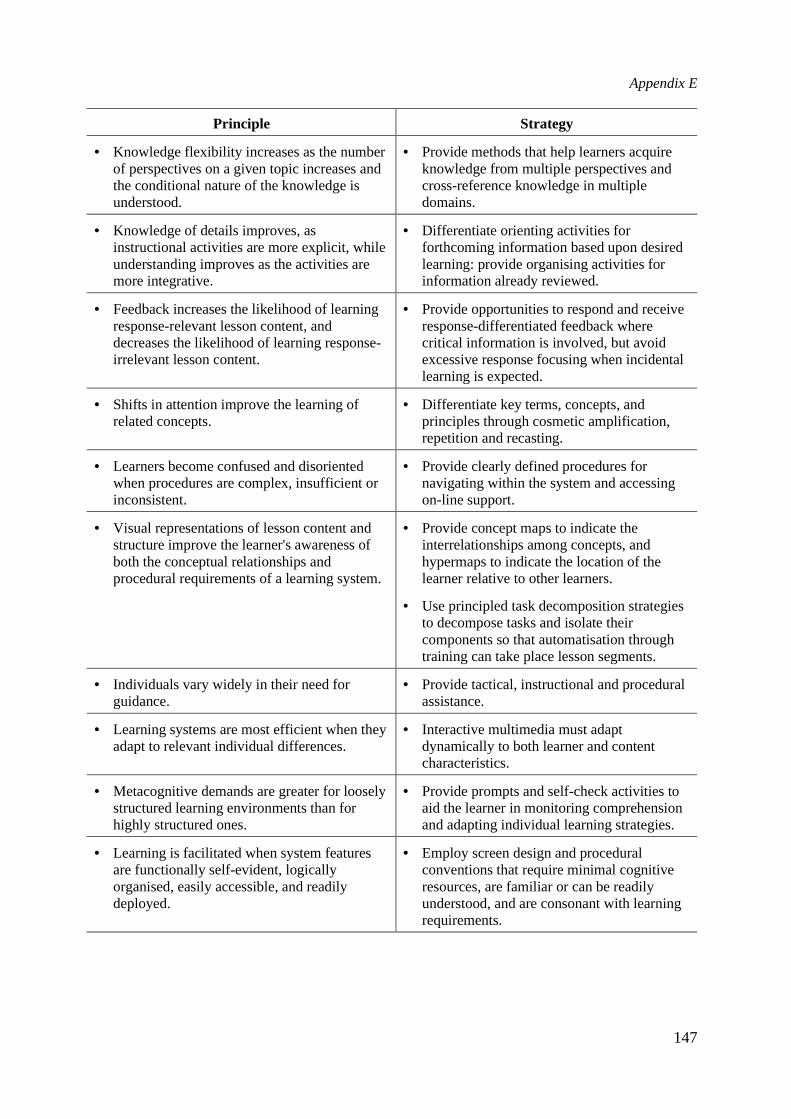
Appendix E
147
Principle Strategy
• Knowledge flexibility increases as the numberof perspectives on a given topic increases andthe conditional nature of the knowledge isunderstood.
• Provide methods that help learners acquireknowledge from multiple perspectives andcross-reference knowledge in multipledomains.
• Knowledge of details improves, asinstructional activities are more explicit, whileunderstanding improves as the activities aremore integrative.
• Differentiate orienting activities forforthcoming information based upon desiredlearning: provide organising activities forinformation already reviewed.
• Feedback increases the likelihood of learningresponse-relevant lesson content, anddecreases the likelihood of learning response-irrelevant lesson content.
• Provide opportunities to respond and receiveresponse-differentiated feedback wherecritical information is involved, but avoidexcessive response focusing when incidentallearning is expected.
• Shifts in attention improve the learning ofrelated concepts.
• Differentiate key terms, concepts, andprinciples through cosmetic amplification,repetition and recasting.
• Learners become confused and disorientedwhen procedures are complex, insufficient orinconsistent.
• Provide clearly defined procedures fornavigating within the system and accessingon-line support.
• Visual representations of lesson content andstructure improve the learner's awareness ofboth the conceptual relationships andprocedural requirements of a learning system.
• Provide concept maps to indicate theinterrelationships among concepts, andhypermaps to indicate the location of thelearner relative to other learners.
• Use principled task decomposition strategiesto decompose tasks and isolate theircomponents so that automatisation throughtraining can take place lesson segments.
• Individuals vary widely in their need forguidance.
• Provide tactical, instructional and proceduralassistance.
• Learning systems are most efficient when theyadapt to relevant individual differences.
• Interactive multimedia must adaptdynamically to both learner and contentcharacteristics.
• Metacognitive demands are greater for looselystructured learning environments than forhighly structured ones.
• Provide prompts and self-check activities toaid the learner in monitoring comprehensionand adapting individual learning strategies.
• Learning is facilitated when system featuresare functionally self-evident, logicallyorganised, easily accessible, and readilydeployed.
• Employ screen design and proceduralconventions that require minimal cognitiveresources, are familiar or can be readilyunderstood, and are consonant with learningrequirements.
Appendix F
147
APPENDIX F
User Manuals for the interactive video 'SHOCK'
Condition 1: Prior activation of prerequisite knowledge
Contents
1) What is the goal of the program?
2) What can be seen on the screen?
2.1 The first screen
2.1.1 Presentation buttons
2.1.2. Presentation screen
2.1.3. Button for the diagnosis
2.1.4. Questions and answers
2.1.5. Program buttons
2.2. The second screen
2.2.1. Image presentation
2.2.2. List of key words
2.2.3. Explanation of a key word
2.2.4. Adjacent key words
3) How does the program proceed?
The interactive video program "SHOCK".
1) What is the goal of this program?
The goal of this video program is to learn to provide a correct diagnosis of different types of shock.
Due to the circumstance that you will not quite frequently be confronted with shock patients, it is an
interesting expansion of your knowledge to get acquainted with this disease at least by the use of video
images. Moreover you will be trained intensively in diagnostic reasoning.
2) What do you see on the screen?
In this program two different screen designs are used.
Appendix F
148
2.1. The first screen
The first screen is used when you will access the ailments of a patient. This screen uses a number of
segments and buttons. The different parts of the first screen will now be handled successively.
Presentation buttons
The presentation buttons can be divided in three subsets. There are buttons to access a) written data, b)
images and c) monitor data. The buttons can be activated in a random sequence.
Written Data
In order to access written data three buttons have been constructed. These are the buttons P (for
personal data), A1 (for anamnestic data concerning history of the disease) and A2 (for the current
complaints). By activating one of these buttons with the mouse, the data will be accessed; they will be
presented in the presentation screen.
Visual data
It is possible to inspect some parts of the patient's body. For that purpose a number of buttons has been
constructed. By activating such a button you activate a part of the video. At the button you can see an
icon; this icon refers to the part of the body which will be resented at the video. You can choose from:
the total patient, face, abdomen, hand or foot. You can see the video partly activating at the video
button of the program buttons.
After each video presentation one or more questions are presented about what was displayed. You
get three chances (trials) to respond to each question. When the answer is incorrect after the third trial,
then the correct answer is presented.
Monitor Data
Finally you can access monitor data. For that purpose two buttons are reserved. The first one (left)
contains data about heart frequency, blood pressure, the pulmonic arterial pressure and the central-
venous pressure. The second button (right) presents the cardiac output (the heart-minute volume).
These data are activated by clicking the relevant button.
As to the monitor presentation as well as the video presentation questions are presented about what
is displayed. You will get three chances (trials) to respond to each question. When the answer is
incorrect after the third trial then the correct answer is presented.
2.1.2. Presentation screen

Appendix F
149
In this segment the information is presented which can be accessed by using a button. This can be
written data, visuals or monitor data.
Appendix F
150
2.1.3. Diagnosis button
When you click the diagnosis button the question is asked what diagnosis you will provide. You can
respond to that question by typing your diagnosis. Note that it can be that the patient does not have
shock, but another disease.
Concerning the feedback on your response there are three possibilities:
a) if you did not collect all data about the patient, i.e. that you did not use all presentation buttons, you
will get the advice what information you have to access. You can (of course) make another
endeavour to provide a diagnosis.
b) if you have collected all data about a patient, i.e. when you have got all presentation buttons, you
will get three chances (trials) to provide the correct diagnosis. When the diagnosis is incorrect
after the third trial, then the correct diagnosis is given.
2.1.4. Questions and answers
When you access video- or monitor information one or more questions about the data involved are
presented. These questions are presented in a separate segment. The answers which you provide, will
be displayed in this segment too. The same applies for the feedback as well as providing a diagnosis.
2.1.5. Program buttons
Using the presentation buttons you can access relevant information. The program buttons have another
function. This function will be explained below.
The Help button
When you click on this button on the presentation screen the program is explained.
The Video button
When you access video material about a part of the patient's body by using a presentation button, then
a question is presented. You can see the concomitant video part by clicking the video button. You can
repeat this as frequently as you want. Also if you have given an incorrect answer after the first trial,
you can see the video art twice.
The Stop/Proceed button
When you have answered a question, or when you have provided a diagnosis, close with the
Stop/Proceed button. When you do not do this, then you cannot proceed with the program.
Appendix F
151
2.2. The second screen
The second screen design is used in order to activate your prerequisite knowledge about circulation
disturbances. This screen uses a number of segments. In Figure 2 this is displayed schematically.
The program starts with this screen. You can see or inspect the key words as long as you want in
order to remember all the prior knowledge. When you leave a screen, you cannot return to that screen.
The different parts of the second screen will be explained successively below.
2.2.1. Video presentation
Most of the time this screen is empty. Only when you want to see an animation, this animation will be
presented on this screen.
2.2.2. List of key words
Right above in this screen you see a list of key words. This list contains 54 key words in alphabetical
order. You see only a part of the keywords simultaneously on the screen. More keywords you can
insect by clicking with the mouse in the scroll bar. When you click above the square, the list of
keywords will move downward. When you click under the square then the same list moves upward.
You can also click the arcs above and below of the scroll bar.
With the mouse you can click the keywords what you want to see. By clicking "inspect" the
explanation of the keyword is presented in the segment of the screen which has been reserved on the
left side (below).
When you click on the Stop/Proceed button, you leave the second screen.
You are asked to confirm this. When you click "Yes" you have left the second screen. You cannot
return to this screen.
2.2.3. Explanation of the keyboard
When you have activated a keyword from the list, then an explanation of this keyword is displayed in
the screen (left side, below). When the explanation is longer than the screen, then you can read the rest
of the text by clicking in the scroll bar below the square. The text moves upwards, so that you can read
further.
2.2.4. Adjacent keywords
Appendix F
152
When you have activated a keyword, on the right side (below) a new list of keywords is displayed
directly. These keywords are similar/adjacent to the keywords you have activated a few moments ago.
You can inspect the keywords from this list by pointing to them with the mouse and then clicking
twice. The explanation of the keyword is displayed on the left side below on the screen and on the
right side a new list of adjacent keywords is displayed.
3) How does the program proceed?
The program starts at screen 2. You can first activate your prior knowledge concerning circulation
disturbances. After that the presentation of patients starts; you have to determine what illness the
patient has.
In the practices first the video material of each patient is presented. You get visual material
pertaining to the total patient, the face, the abdomen, the hand and the foot. After having completed
this, click on the "Stop/Proceed" button in order to proceed. You have three options:
a) to collect more details about written data or monitor data;
b) to inspect once more some parts of the patient's body (visuals);
c) to provide a diagnosis using the diagnosis-button.
You collect data about the patient using the presentation button. When you have collected all data
or when you think to have collected sufficient data, then you can provide a diagnosis using the
diagnosis button. Note that it is possible that the patient involved has no shock! When the correct
diagnosis has been provided, then the case is closed and you can proceed to the next patient using the
"Stop/Proceed" button.
The goal is not that you will complete all 31 cases. Proceed in your own speed, allocate sufficient
time to each patient and try to provide a diagnosis of as much patients as you can.
The total program lasts two hours.
Appendix F
153
Condition 2: Simultaneous activation of prerequisite knowledge
Contents
1) What is the goal of the program?
2) What can be seen on the screen?
2.1 The first screen
2.1.1 Presentation buttons
2.1.2. Presentation screen
2.1.3. Button for the diagnosis
2.1.4. Questions and answers
2.1.5. Program buttons
2.2. The second screen
2.2.1. Image presentation
2.2.2. List of key words
2.2.3. Explanation of a key word
2.2.4. Adjacent key words
3) How does the program proceed?
The interactive video program "SHOCK".
1) What is the goal of this program?
The goal of this video program is to learn to provide a correct diagnosis of different types of shock.
Due to the circumstance that you will not quite frequently be confronted with shock patients, it is an
interesting expansion of your knowledge to get acquainted with this disease at least by the use of video
images. Moreover you will be trained intensively in diagnostic reasoning.
2) What do you see on the screen?
In this program two different screen designs are used.
2.1. The first screen

Appendix F
154
The first screen is used when you will access the ailments of a patient. This screen uses a number of
segments and buttons. The different parts of the first screen will now be handled successively.
Appendix F
155
Presentation buttons
The presentation buttons can be divided in three subsets. There are buttons to access a) written data, b)
images and c) monitor data. The buttons can be activated in a random sequence.
Written Data
In order to access written data three buttons have been constructed. These are the buttons P (for
personal data), A1 (for anamnestic data concerning history of the disease) and A2 (for the current
complaints). By activating one of these buttons with the mouse, the data will be accessed; they will be
presented in the presentation screen.
Visual data
It is possible to inspect some parts of the patient's body. For that purpose a number of buttons has been
constructed. By activating such a button you activate a part of the video. At the button you can see an
icon; this icon refers to a part of the body which will be presented in the video. You can choose from:
the total patient, face, abdomen, hand or foot. You can see the video part by activating at the video
button of the program buttons.
After each video presentation one or more questions are presented about what was displayed. You
get three chances (trials) to respond to each question. When the answer is incorrect after the third trial,
then the correct answer is presented.
Monitor Data
Finally you can access monitor data. For that purpose two buttons are reserved. The first one (left)
contains data about heart frequency, blood pressure, the pulmonic arterial pressure and the central-
venous pressure. The second button right) presents the cardiac output (the heart-minute volume).
These data are activated by clicking the relevant button.
As to the monitor presentation as well as the video presentation questions are presented about what
is displayed. You will get three chances (trials) to respond to each question. When the answer is
incorrect after the third trial then the correct answer is presented.
2.1.2. Presentation screen
In this segment the information is presented which can be accessed by using a button. This can be
written data, visuals or monitor data.
2.1.3. Diagnosis button.
Appendix F
156
When you click the diagnosis button the question is asked what diagnosis you will provide. You can
respond to that question by typing your diagnosis. Note that it can be that the patient does not have
shock, but another disease.
Concerning the feedback on your response there are three possibilities:
a) if you did not collect all data about the patient, i.e. that you did not use all presentation buttons, you
will get the advice what information you have to access. You can (of course) make another
endeavour to provide a diagnosis.
b) if you have collected all data about a patient, i.e. if you have got all presentation buttons, you will
get three chances (trials) to provide the correct diagnosis. When the diagnosis is incorrect after the
third trial, then the correct diagnosis is given.
2.1.4. Questions and answers
When you access video- or monitor information one or more questions about the data involved are
presented. These questions are presented in a separate segment. The answers which you provide, will
be displayed in this segment too. The same applies for the feedback as well as providing a diagnosis.
2.1.5. Program buttons
Using the presentation buttons you can access relevant information. The program buttons have another
function. This function will be explained below.
The Help button
When you click on this button on the presentation screen the program is explained.
The Video button
When you access video material about a part of the patient's body by using a presentation button, then
a question is presented. You can see the concomitant video part by clicking the video button. You can
repeat this as frequently as you want. Also if you have given an incorrect answer after the first trial,
you can see the video art twice.
The Stop/Proceed button
When you have answered a question, or when you have provided a diagnosis, close with the
Stop/Proceed button. When you do not do this, then you cannot proceed with the program.
The 'K'-Button
Appendix F
157
When you click this button the second screen is activated.
2.2. The second screen
The second screen design is used in order to activate your prerequisite knowledge about circulation
disturbances. This screen uses a number of segments. In Figure 2 this is displayed schematically.
Near the program buttons you see the 'K'-button. When you use this button you will enter the
second screen. You can repeat this as often as you want.
The different parts of the second screen will be explained successively below.
2.2.1. Video presentation
In this screen you see the video images which you are handling at the moment of clicking the 'K'-
button. Also animations are presented in this screen
2.2.2. List of key words
Right above in this screen you see a list of key words. This list contains 54 key words in alphabetical
order. You see only a part of the keywords simultaneously on the screen. More keywords you can
insect by clicking with the mouse in the scroll bar. When you click above the square, the list of
keywords will move downward. When you click under the square then the same list moves upward.
You can also click the arcs above and below of the scroll bar.
With the mouse you can click the keywords what you which to see. By clicking "inspect" the
explanation of the keyword is presented in the segment of the screen which has been reserved on the
left side (below).
When you click on the Stop/Proceed button, you leave the second screen.
2.2.3. Explanation of the keyboard
When you have activated a keyword from the list, then an explanation of this keyword is displayed in
the screen (left side, below). When the explanation is longer than the screen, then you can read the rest
of the text by clicking in the scroll bar below the square. The text moves upwards, so that you can read
further.
2.2.4. Adjacent keywords
Appendix F
158
When you have activated a keyword, on the right side (below) a new list of keywords is displayed
directly. These keywords are similar/adjacent to the keywords you have activated a few moments ago.
You can inspect the keywords from this list by pointing to them with the mouse and then clicking
twice. The explanation of the keyword is displayed on the left side below on the screen and on the
right side a new list of adjacent keywords is displayed.
3) How does the program proceed?
The program starts at screen 2. You can first activate your prior knowledge concerning circulation
disturbances. After that the presentation of patients starts; you have to determine what illness the
patient has.
In the practices first the video material of each patient is presented. You get visual material
pertaining to the total patient, the face, the abdomen, the hand and the foot. After having completed
this, click the on the "Stop/Proceed" button in order to proceed. You have three options:
a) to collect more details about written data or monitor data;
b) to inspect once more some parts of the patient's body (visuals);
c) to provide a diagnosis using the diagnosis-button.
You collect data about the patient using the presentation button. When you have collected all data
or when you think to have collected sufficient data, then you can provide a diagnosis using the
diagnosis button. Note that it is possible that the patient involved has no shock! When the correct
diagnosis has been provided, then the case is closed and you can proceed to the next patient using the
"Stop/Proceed" button.
The goal is not that you will complete all 31 cases. Proceed in your own speed, allocate sufficient
time to each patient and try to provide a diagnosis of as much patients as you can.
The total program lasts two hours.
Appendix F
159
Condition 3: Error-related activation of prerequisite knowledge
Contents
1) What is the goal of the program?
2) What can be seen on the screen?
2.1 The first screen
2.1.1 Presentation buttons
2.1.2. Presentation screen
2.1.3. Button for the diagnosis
2.1.4. Questions and answers
2.1.5. Program buttons
2.2. The second screen
2.2.1. Image presentation
2.2.2. List of key words
2.2.3. Explanation of a key word
2.2.4. Adjacent key words
3) How does the program proceed?
The interactive video program "SHOCK".
1) What is the goal of this program?
The goal of this video program is to learn to provide a correct diagnosis of different types of shock.
Due to the circumstance that you will not quite frequently be confronted with shock patients, it is an
interesting expansion of your knowledge to get acquainted with this disease at least by the use of video
images. Moreover you will be trained intensively in diagnostic reasoning.
2) What do you see on the screen?
In this program two different screen designs are used.
2.1. The first screen
Appendix F
160
The first screen is used when you will access the ailments of a patient. This screen uses a number of
segments and buttons. The different parts of the first screen will now be handled successively.
Appendix F
161
2.1.1. Presentation buttons
The presentation buttons can be divided in three subsets. There are buttons to access a) written data, b)
images and c) monitor data. The buttons can be activated in a random sequence.
Written Data
In order to access written data three buttons have been constructed. These are the buttons P (for
personal data), A1 (for anamnestic data concerning history of the disease) and A2 (for the current
complaints). By activating one of these buttons with the mouse, the data will be accessed; they will be
presented in the presentation screen.
Visual data
It is possible to inspect some parts of the patient's body. For that purpose a number of buttons has been
constructed. By activating such a button you activate a part of the video. At the button you can see an
icon; this icon refers to a part of the body which will be presented in the video. You can choose from:
the total patient, face, abdomen, hand or foot. You can see the video partly activating at the video
button of the program buttons.
After each video presentation one or more questions are presented about what was displayed. You
get three chances (trials) to respond to each question. When the answer is incorrect after the third trial,
then the correct answer is presented.
Monitor Data
Finally you can access monitor data. For that purpose two buttons are reserved. The first one (left)
contains data about heart frequency, blood pressure, the pulmonic arterial pressure and the central-
venous pressure. The second button (right) presents the cardiac output (the heart-minute volume).
These data are activated by clicking the relevant button.
As to the monitor presentation as well as the video presentation questions are presented about what
is displayed. You will get three chances (trials) to respond to each question. When the answer is
incorrect after the third trial then the correct answer is presented.
2.1.2. Presentation screen
In this segment the information is presented which can be accessed by using a button. This can be
written data, visuals or monitor data.
2.1.3. Diagnosis button
Appendix F
162
When you click the diagnosis button the question is asked what diagnosis you will provide. You can
respond to that question by typing your diagnosis. Note that it can be that the patient does not have
shock, but another disease.
Concerning the feedback on your response there are three possibilities:
a) if you did not collect all data about the patient, i.e. that you did not use all presentation buttons, you
will get the advice which information you have to access. You can (of course) make another
endeavour to provide a diagnosis.
b) if you have collected all data about a patient, i.e. if you have got all presentation buttons, you will
get three chances (trials) to provide the correct diagnosis. When the diagnosis is incorrect after the
third trial, then the correct diagnosis is given.
2.1.4. Questions and answers
When you access video- or monitor information one or more questions about the data involved are
presented. These questions are presented in a separate segment. The answers that you provide, will be
displayed in this segment too. The same applies for the feedback as well as providing a diagnosis.
2.1.5. Program buttons
Using the presentation buttons you can access relevant information. The program buttons have another
function. This function will be explained below.
The Help button
When you click on this button on the presentation screen the program is explained.
The video button
When you access video material about a part of the patient's body by using a presentation button, then
a question is presented. You can see the concomitant video part by clicking the video button. You can
repeat this as frequently as you want. Also if you have given an incorrect answer after the first trial,
you can see the video art twice.
The Stop/Proceed button
When you have answered a question, or when you have provided a diagnosis, close with the
Stop/Proceed button. When you do not do this, then you cannot proceed with the program.
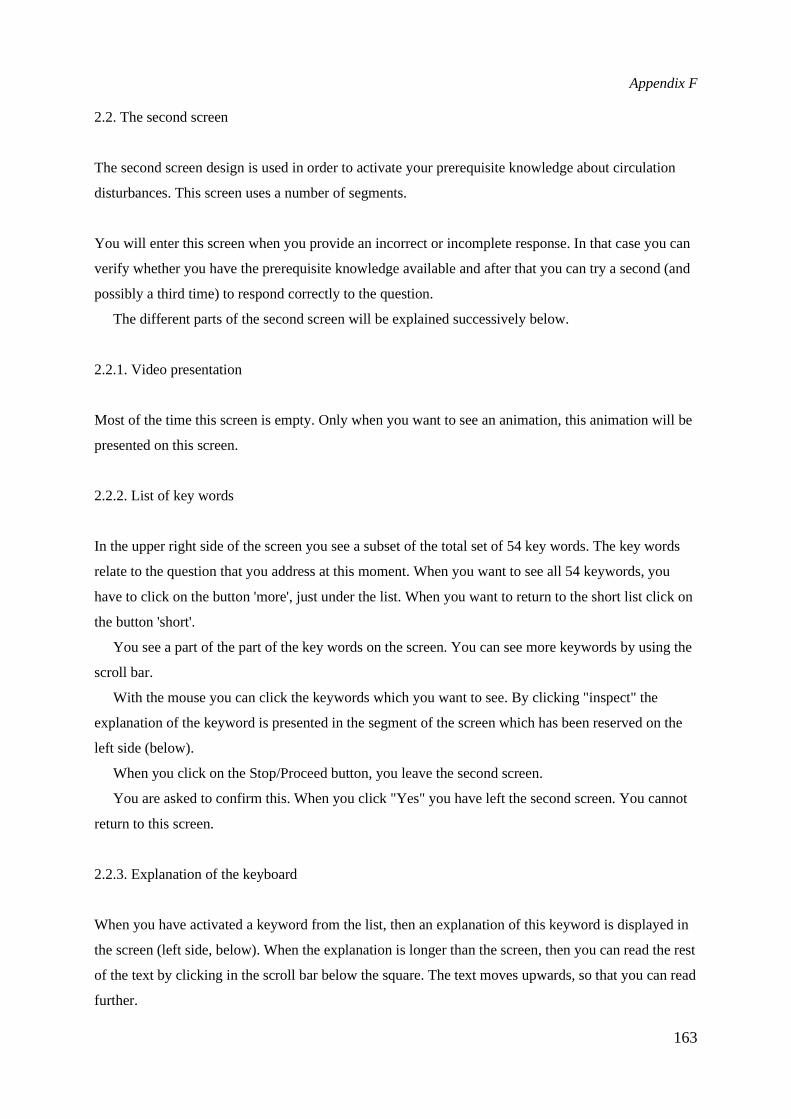
Appendix F
163
2.2. The second screen
The second screen design is used in order to activate your prerequisite knowledge about circulation
disturbances. This screen uses a number of segments.
You will enter this screen when you provide an incorrect or incomplete response. In that case you can
verify whether you have the prerequisite knowledge available and after that you can try a second (and
possibly a third time) to respond correctly to the question.
The different parts of the second screen will be explained successively below.
2.2.1. Video presentation
Most of the time this screen is empty. Only when you want to see an animation, this animation will be
presented on this screen.
2.2.2. List of key words
In the upper right side of the screen you see a subset of the total set of 54 key words. The key words
relate to the question that you address at this moment. When you want to see all 54 keywords, you
have to click on the button 'more', just under the list. When you want to return to the short list click on
the button 'short'.
You see a part of the part of the key words on the screen. You can see more keywords by using the
scroll bar.
With the mouse you can click the keywords which you want to see. By clicking "inspect" the
explanation of the keyword is presented in the segment of the screen which has been reserved on the
left side (below).
When you click on the Stop/Proceed button, you leave the second screen.
You are asked to confirm this. When you click "Yes" you have left the second screen. You cannot
return to this screen.
2.2.3. Explanation of the keyboard
When you have activated a keyword from the list, then an explanation of this keyword is displayed in
the screen (left side, below). When the explanation is longer than the screen, then you can read the rest
of the text by clicking in the scroll bar below the square. The text moves upwards, so that you can read
further.
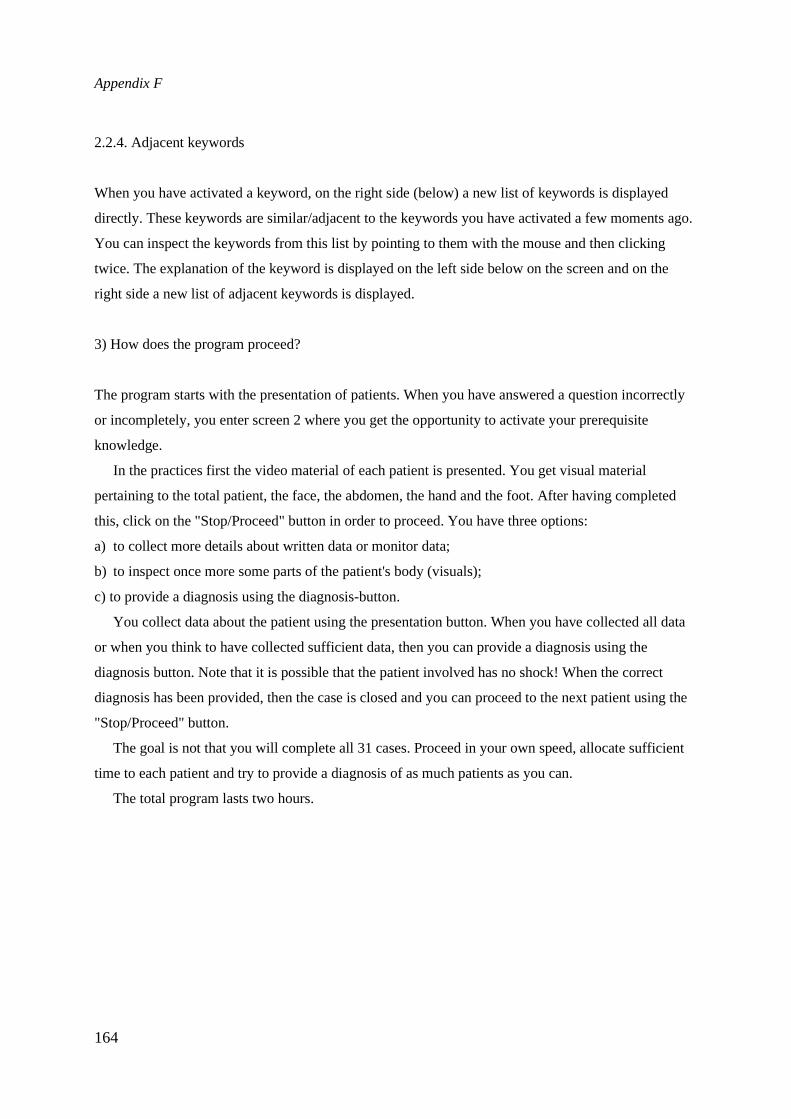
Appendix F
164
2.2.4. Adjacent keywords
When you have activated a keyword, on the right side (below) a new list of keywords is displayed
directly. These keywords are similar/adjacent to the keywords you have activated a few moments ago.
You can inspect the keywords from this list by pointing to them with the mouse and then clicking
twice. The explanation of the keyword is displayed on the left side below on the screen and on the
right side a new list of adjacent keywords is displayed.
3) How does the program proceed?
The program starts with the presentation of patients. When you have answered a question incorrectly
or incompletely, you enter screen 2 where you get the opportunity to activate your prerequisite
knowledge.
In the practices first the video material of each patient is presented. You get visual material
pertaining to the total patient, the face, the abdomen, the hand and the foot. After having completed
this, click on the "Stop/Proceed" button in order to proceed. You have three options:
a) to collect more details about written data or monitor data;
b) to inspect once more some parts of the patient's body (visuals);
c) to provide a diagnosis using the diagnosis-button.
You collect data about the patient using the presentation button. When you have collected all data
or when you think to have collected sufficient data, then you can provide a diagnosis using the
diagnosis button. Note that it is possible that the patient involved has no shock! When the correct
diagnosis has been provided, then the case is closed and you can proceed to the next patient using the
"Stop/Proceed" button.
The goal is not that you will complete all 31 cases. Proceed in your own speed, allocate sufficient
time to each patient and try to provide a diagnosis of as much patients as you can.
The total program lasts two hours.


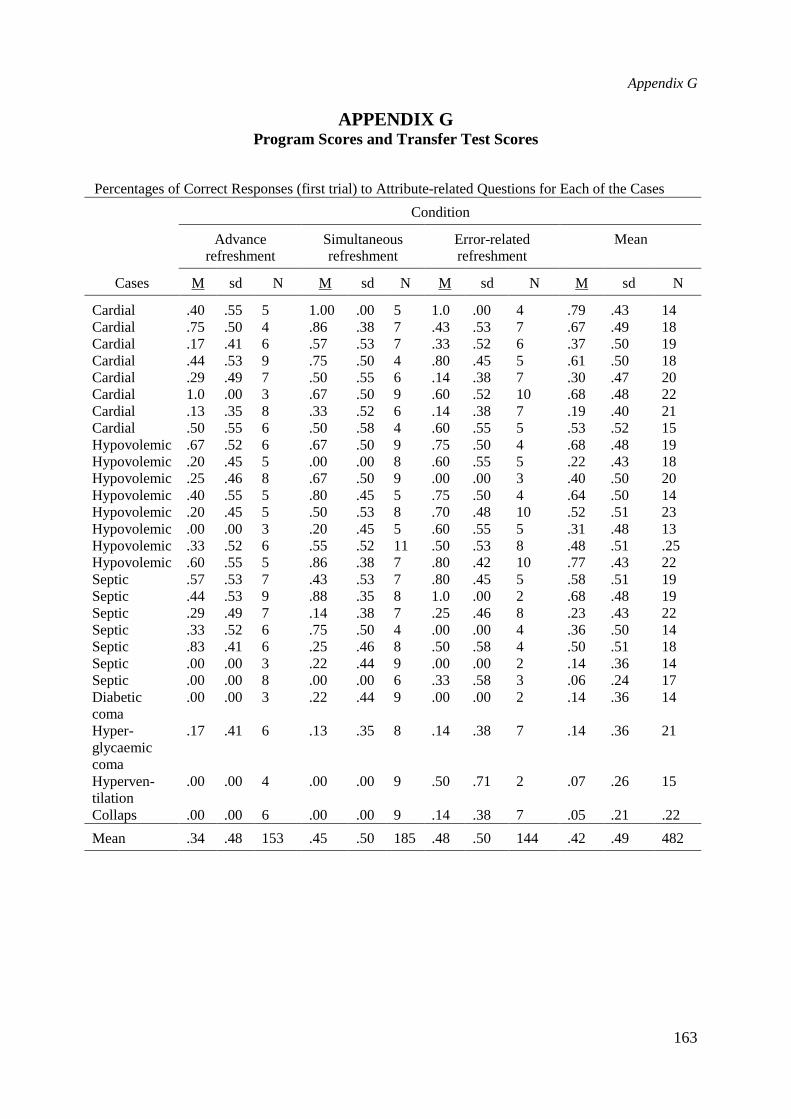
Appendix G
163
APPENDIX GProgram Scores and Transfer Test Scores
Percentages of Correct Responses (first trial) to Attribute-related Questions for Each of the Cases
Condition
Advancerefreshment
Simultaneousrefreshment
Error-relatedrefreshment
Mean
Cases M sd N M sd N M sd N M sd N
Cardial .40 .55 5 1.00 .00 5 1.0 .00 4 .79 .43 14Cardial .75 .50 4 .86 .38 7 .43 .53 7 .67 .49 18Cardial .17 .41 6 .57 .53 7 .33 .52 6 .37 .50 19Cardial .44 .53 9 .75 .50 4 .80 .45 5 .61 .50 18Cardial .29 .49 7 .50 .55 6 .14 .38 7 .30 .47 20Cardial 1.0 .00 3 .67 .50 9 .60 .52 10 .68 .48 22Cardial .13 .35 8 .33 .52 6 .14 .38 7 .19 .40 21Cardial .50 .55 6 .50 .58 4 .60 .55 5 .53 .52 15Hypovolemic .67 .52 6 .67 .50 9 .75 .50 4 .68 .48 19Hypovolemic .20 .45 5 .00 .00 8 .60 .55 5 .22 .43 18Hypovolemic .25 .46 8 .67 .50 9 .00 .00 3 .40 .50 20Hypovolemic .40 .55 5 .80 .45 5 .75 .50 4 .64 .50 14Hypovolemic .20 .45 5 .50 .53 8 .70 .48 10 .52 .51 23Hypovolemic .00 .00 3 .20 .45 5 .60 .55 5 .31 .48 13Hypovolemic .33 .52 6 .55 .52 11 .50 .53 8 .48 .51 .25Hypovolemic .60 .55 5 .86 .38 7 .80 .42 10 .77 .43 22Septic .57 .53 7 .43 .53 7 .80 .45 5 .58 .51 19Septic .44 .53 9 .88 .35 8 1.0 .00 2 .68 .48 19Septic .29 .49 7 .14 .38 7 .25 .46 8 .23 .43 22Septic .33 .52 6 .75 .50 4 .00 .00 4 .36 .50 14Septic .83 .41 6 .25 .46 8 .50 .58 4 .50 .51 18Septic .00 .00 3 .22 .44 9 .00 .00 2 .14 .36 14Septic .00 .00 8 .00 .00 6 .33 .58 3 .06 .24 17Diabeticcoma
.00 .00 3 .22 .44 9 .00 .00 2 .14 .36 14
Hyper-glycaemiccoma
.17 .41 6 .13 .35 8 .14 .38 7 .14 .36 21
Hyperven-tilation
.00 .00 4 .00 .00 9 .50 .71 2 .07 .26 15
Collaps .00 .00 6 .00 .00 9 .14 .38 7 .05 .21 .22
Mean .34 .48 153 .45 .50 185 .48 .50 144 .42 .49 482
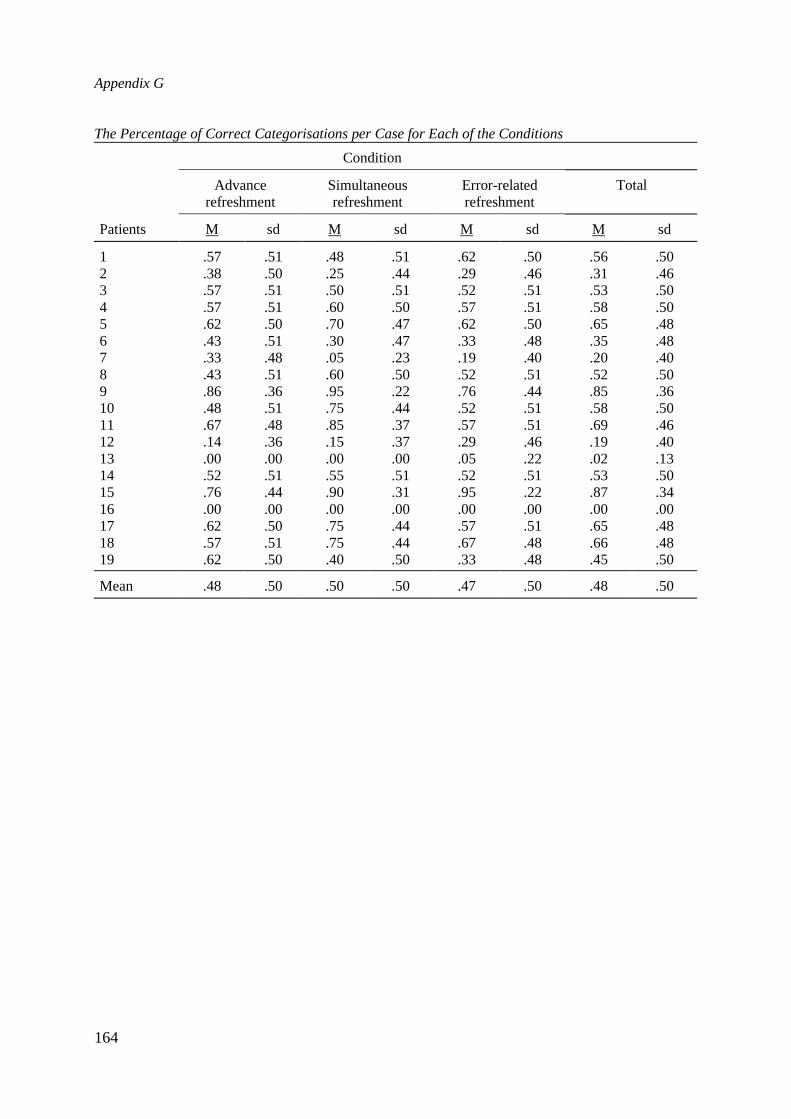
Appendix G
164
The Percentage of Correct Categorisations per Case for Each of the Conditions
Condition
Advancerefreshment
Simultaneousrefreshment
Error-relatedrefreshment
Total
Patients M sd M sd M sd M sd
1 .57 .51 .48 .51 .62 .50 .56 .502 .38 .50 .25 .44 .29 .46 .31 .463 .57 .51 .50 .51 .52 .51 .53 .504 .57 .51 .60 .50 .57 .51 .58 .505 .62 .50 .70 .47 .62 .50 .65 .486 .43 .51 .30 .47 .33 .48 .35 .487 .33 .48 .05 .23 .19 .40 .20 .408 .43 .51 .60 .50 .52 .51 .52 .509 .86 .36 .95 .22 .76 .44 .85 .3610 .48 .51 .75 .44 .52 .51 .58 .5011 .67 .48 .85 .37 .57 .51 .69 .4612 .14 .36 .15 .37 .29 .46 .19 .4013 .00 .00 .00 .00 .05 .22 .02 .1314 .52 .51 .55 .51 .52 .51 .53 .5015 .76 .44 .90 .31 .95 .22 .87 .3416 .00 .00 .00 .00 .00 .00 .00 .0017 .62 .50 .75 .44 .57 .51 .65 .4818 .57 .51 .75 .44 .67 .48 .66 .4819 .62 .50 .40 .50 .33 .48 .45 .50
Mean .48 .50 .50 .50 .47 .50 .48 .50
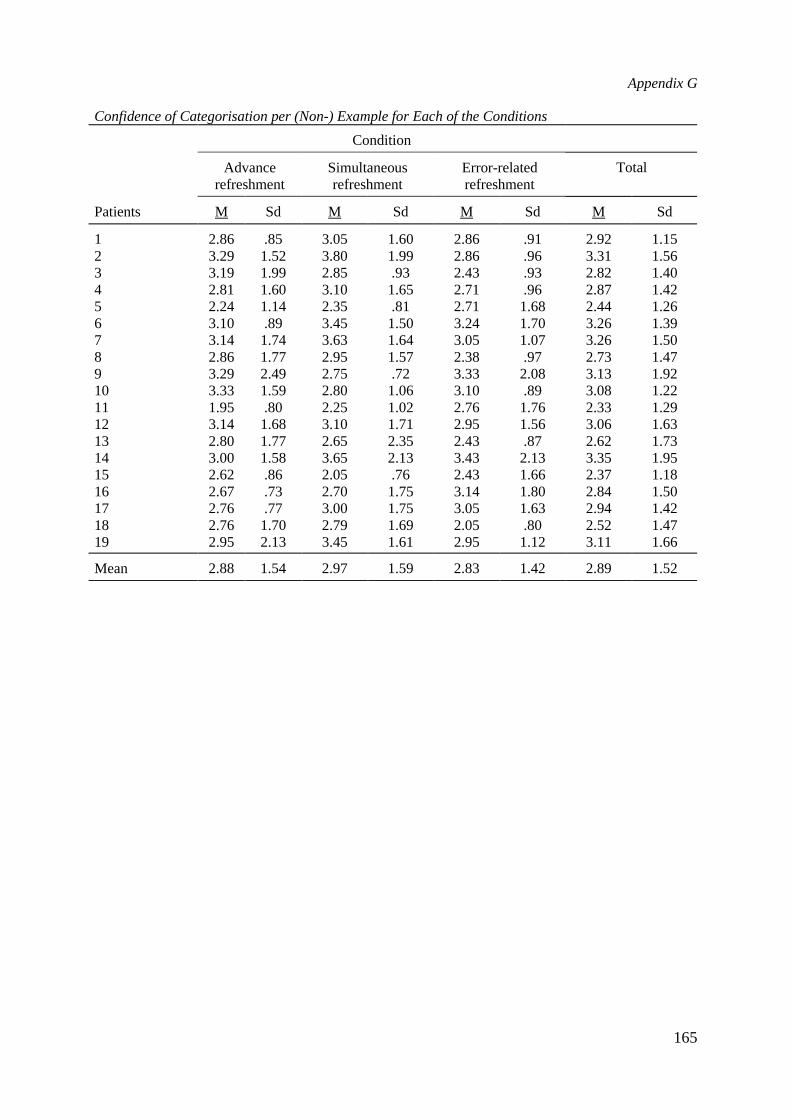
Appendix G
165
Confidence of Categorisation per (Non-) Example for Each of the Conditions
Condition
Advancerefreshment
Simultaneousrefreshment
Error-relatedrefreshment
Total
Patients M Sd M Sd M Sd M Sd
1 2.86 .85 3.05 1.60 2.86 .91 2.92 1.152 3.29 1.52 3.80 1.99 2.86 .96 3.31 1.563 3.19 1.99 2.85 .93 2.43 .93 2.82 1.404 2.81 1.60 3.10 1.65 2.71 .96 2.87 1.425 2.24 1.14 2.35 .81 2.71 1.68 2.44 1.266 3.10 .89 3.45 1.50 3.24 1.70 3.26 1.397 3.14 1.74 3.63 1.64 3.05 1.07 3.26 1.508 2.86 1.77 2.95 1.57 2.38 .97 2.73 1.479 3.29 2.49 2.75 .72 3.33 2.08 3.13 1.9210 3.33 1.59 2.80 1.06 3.10 .89 3.08 1.2211 1.95 .80 2.25 1.02 2.76 1.76 2.33 1.2912 3.14 1.68 3.10 1.71 2.95 1.56 3.06 1.6313 2.80 1.77 2.65 2.35 2.43 .87 2.62 1.7314 3.00 1.58 3.65 2.13 3.43 2.13 3.35 1.9515 2.62 .86 2.05 .76 2.43 1.66 2.37 1.1816 2.67 .73 2.70 1.75 3.14 1.80 2.84 1.5017 2.76 .77 3.00 1.75 3.05 1.63 2.94 1.4218 2.76 1.70 2.79 1.69 2.05 .80 2.52 1.4719 2.95 2.13 3.45 1.61 2.95 1.12 3.11 1.66
Mean 2.88 1.54 2.97 1.59 2.83 1.42 2.89 1.52
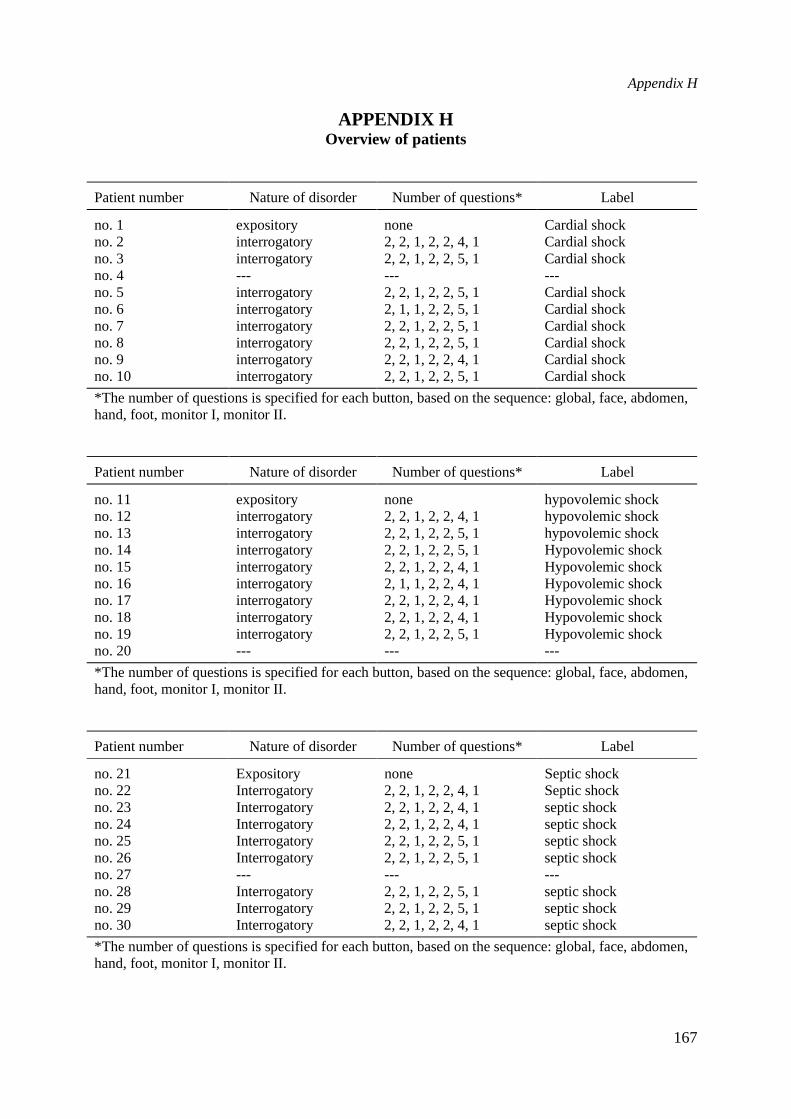
Appendix H
167
APPENDIX HOverview of patients
Patient number Nature of disorder Number of questions* Label
no. 1 expository none Cardial shockno. 2 interrogatory 2, 2, 1, 2, 2, 4, 1 Cardial shockno. 3 interrogatory 2, 2, 1, 2, 2, 5, 1 Cardial shockno. 4 --- --- ---no. 5 interrogatory 2, 2, 1, 2, 2, 5, 1 Cardial shockno. 6 interrogatory 2, 1, 1, 2, 2, 5, 1 Cardial shockno. 7 interrogatory 2, 2, 1, 2, 2, 5, 1 Cardial shockno. 8 interrogatory 2, 2, 1, 2, 2, 5, 1 Cardial shockno. 9 interrogatory 2, 2, 1, 2, 2, 4, 1 Cardial shockno. 10 interrogatory 2, 2, 1, 2, 2, 5, 1 Cardial shock
*The number of questions is specified for each button, based on the sequence: global, face, abdomen,hand, foot, monitor I, monitor II.
Patient number Nature of disorder Number of questions* Label
no. 11 expository none hypovolemic shockno. 12 interrogatory 2, 2, 1, 2, 2, 4, 1 hypovolemic shockno. 13 interrogatory 2, 2, 1, 2, 2, 5, 1 hypovolemic shockno. 14 interrogatory 2, 2, 1, 2, 2, 5, 1 Hypovolemic shockno. 15 interrogatory 2, 2, 1, 2, 2, 4, 1 Hypovolemic shockno. 16 interrogatory 2, 1, 1, 2, 2, 4, 1 Hypovolemic shockno. 17 interrogatory 2, 2, 1, 2, 2, 4, 1 Hypovolemic shockno. 18 interrogatory 2, 2, 1, 2, 2, 4, 1 Hypovolemic shockno. 19 interrogatory 2, 2, 1, 2, 2, 5, 1 Hypovolemic shockno. 20 --- --- ---
*The number of questions is specified for each button, based on the sequence: global, face, abdomen,hand, foot, monitor I, monitor II.
Patient number Nature of disorder Number of questions* Label
no. 21 Expository none Septic shockno. 22 Interrogatory 2, 2, 1, 2, 2, 4, 1 Septic shockno. 23 Interrogatory 2, 2, 1, 2, 2, 4, 1 septic shockno. 24 Interrogatory 2, 2, 1, 2, 2, 4, 1 septic shockno. 25 Interrogatory 2, 2, 1, 2, 2, 5, 1 septic shockno. 26 Interrogatory 2, 2, 1, 2, 2, 5, 1 septic shockno. 27 --- --- ---no. 28 Interrogatory 2, 2, 1, 2, 2, 5, 1 septic shockno. 29 Interrogatory 2, 2, 1, 2, 2, 5, 1 septic shockno. 30 Interrogatory 2, 2, 1, 2, 2, 4, 1 septic shock
*The number of questions is specified for each button, based on the sequence: global, face, abdomen,hand, foot, monitor I, monitor II.
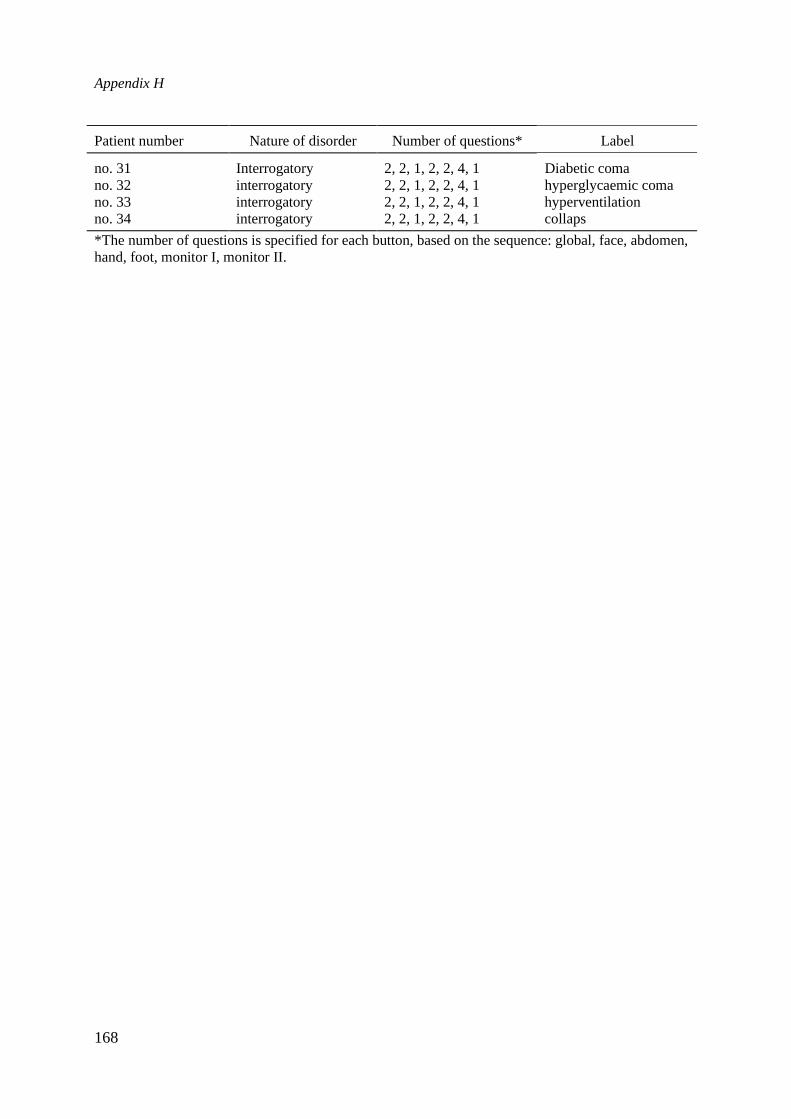
Appendix H
168
Patient number Nature of disorder Number of questions* Label
no. 31 Interrogatory 2, 2, 1, 2, 2, 4, 1 Diabetic comano. 32 interrogatory 2, 2, 1, 2, 2, 4, 1 hyperglycaemic comano. 33 interrogatory 2, 2, 1, 2, 2, 4, 1 hyperventilationno. 34 interrogatory 2, 2, 1, 2, 2, 4, 1 collaps
*The number of questions is specified for each button, based on the sequence: global, face, abdomen,hand, foot, monitor I, monitor II.

169
ABOUT THE AUTHOR
Jan Gulmans was born on September 2, 1944 in Ternaard, Friesland (The Netherlands). Heobtained his high school education at 'Oostergoo' in Dokkum (Gymnasium-α). In 1965, hestarted his study Social Sciences at the University of Groningen. He completed this study atthe University of Leyden in 1972. From 1972 till 1976 he worked as an educationalist at the'Educational Center for Vocational Education and Industry' (PCBB) in 's-Hertogenbosch.From 1976 till 1978 he worked as head of the project involved in exams for vocationaleducation at the 'Central Institute of Test Development' (CITO) in Arnhem. From 1978 till1982 he was leader of a research project of the University of Twente which identified actualand desirable educational objectives in vocational education (MBO). Since 1982, he is anassistant professor of Instructional Technology at the Faculty of Educational Technology ofthe University of Twente. His publications are about instructional technology, conceptacquisition, (para-) medical education and multimedia.
Related Documents











