© ACoRN Neonatal Society – 2006 The ACoRN Process Problem List Respiratory Cardiovascular Neurology Surgical conditions Fluid & glucose Thermoregulation Infection Support Respiratory Laboured respiration* Respiratory rate > 60/min* Receiving respiratory support* Surgical Conditions Anterior abdominal wall defect Vomiting or inability to swallow Abdominal distension Delayed passage of meconium or imperforate anus Thermoregulation T < 36.3 or > 37.2ºC axillary* Increased risk for temperature instability Fluid & Glucose Management Blood glucose < 2.6 mmol/L At risk for hypoglycemia Not feeding or should not be fed Neurology Abnormal tone* Jitteriness Seizures* Cardiovascular Pale, mottled, or grey* Weak pulses or low BP* Cyanosis unresponsive to O 2 Heart rate > 220 bpm Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Sequences Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Infection Risk factor for infection ACoRN alerting sign with * Clinical deterioration Consider transport

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© ACoRN Neonatal Society – 2006
The ACoRN Process
Problem List Respiratory
Cardiovascular Neurology Surgical conditions Fluid & glucose Thermoregulation Infection
Support
Respiratory Laboured respiration* Respiratory rate > 60/min* Receiving respiratory support*
Surgical Conditions Anterior abdominal wall defect Vomiting or inability to swallow Abdominal distension Delayed passage of meconium or imperforate anus
Thermoregulation T < 36.3 or > 37.2ºC axillary*
Increased risk for temperature instability
Fluid & Glucose ManagementBlood glucose < 2.6 mmol/L
At risk for hypoglycemia Not feeding or should not be fed
Neurology Abnormal tone* Jitteriness Seizures*
CardiovascularPale, mottled, or grey*
Weak pulses or low BP* Cyanosis unresponsive to O2 Heart rate > 220 bpm
Baby at risk Unwell
Risk factors Post-resuscitation requiring stabilization
Sequences
Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis
Infection Risk factor for infection ACoRN alerting sign with * Clinical deterioration
Consider transport

The Resuscitation Sequence
© ACoRN Neonatal Society – 2006
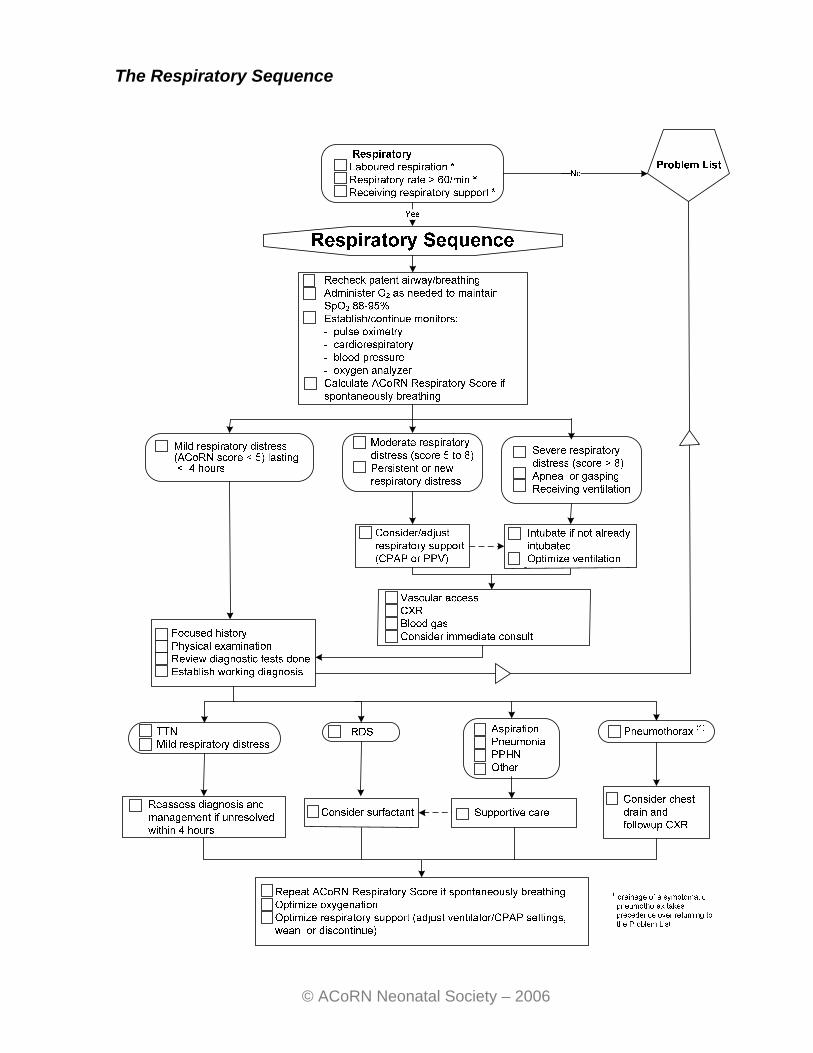
The Respiratory Sequence
© ACoRN Neonatal Society – 2006

© ACoRN Neonatal Society – 2006
The Respiratory Score: Score 0 1 2
Respiratory rate 40 to 60/minute 60 to 80/minute > 80/minute
Oxygen requirement1 None ≤ 50% > 50%
Retractions None Mild to moderate Severe
Grunting None With stimulation Continuous at rest
Breath sounds on auscultation
Easily heard throughout
Decreased Barely heard
Prematurity > 34 weeks 30 to 34 weeks < 30 weeks 1 A baby receiving oxygen prior to the setup of an oxygen analyzer should be assigned a score of “1” Adapted from Downes JJ, Vidyasagar D, Boggs TR Jr, Morrow GM 3rd. Respiratory distress syndrome of newborn infants. I. New clinical scoring system (RDS score) with acid-base and blood-gas correlations. Clin Pediatr 1970; 9(6):325-31.
Total score:
Mild respiratory distress Respiratory Score < 5, starting at birth and lasting < 4 hours.
Moderate respiratory distress (Babies are at risk of progressing to respiratory
failure.) Respiratory Score of 5 to 8 mild respiratory distress (Respiratory Score < 5), but persisting over 4 hours babies who were previously well but develop new respiratory distress.
Severe respiratory distress
Respiratory Score > 8 babies with severe apnea or gasping babies who are already receiving ventilation due to respiratory failure
(initiated during the Resuscitation Sequence or a previous passage through the Respiratory Sequence).
Note:
Babies with persistent or new respiratory distress may be symptomatic due to other causes such as infection.

The Cardiovascular Sequence
© ACoRN Neonatal Society – 2006

Assuming a normal hemoglobin level and adequate cardiac output, how are various degrees of desaturation (hypoxemia) tolerated? SpO2 Degree of desaturation Tolerance
> 75%
mild to moderate usually well tolerated
65 to 75% marked may be less well tolerated
if baby otherwise sick < 65% severe poorly tolerated Clinical signs of cardiovascular instability:
Stable Unstable
alert, active and looking well, normal tone
listless or lethargic and/or distressed, decreased tone
capillary refill < 3 seconds centrally and peripherally
capillary refill > 3 seconds
pulses palpable and full pulses weak
heart sounds normal gallop
no edema or signs of third space
fluid edema or signs of other third space fluid
clear lungs and normal-sized heart on chest radiograph
congested lungs or pleural effusions, and/or enlarged heart on chest radiograph
© ACoRN Neonatal Society – 2006

The Neurology Sequence
© ACoRN Neonatal Society – 2006

The Surgical Conditions Sequence
© ACoRN Neonatal Society – 2006
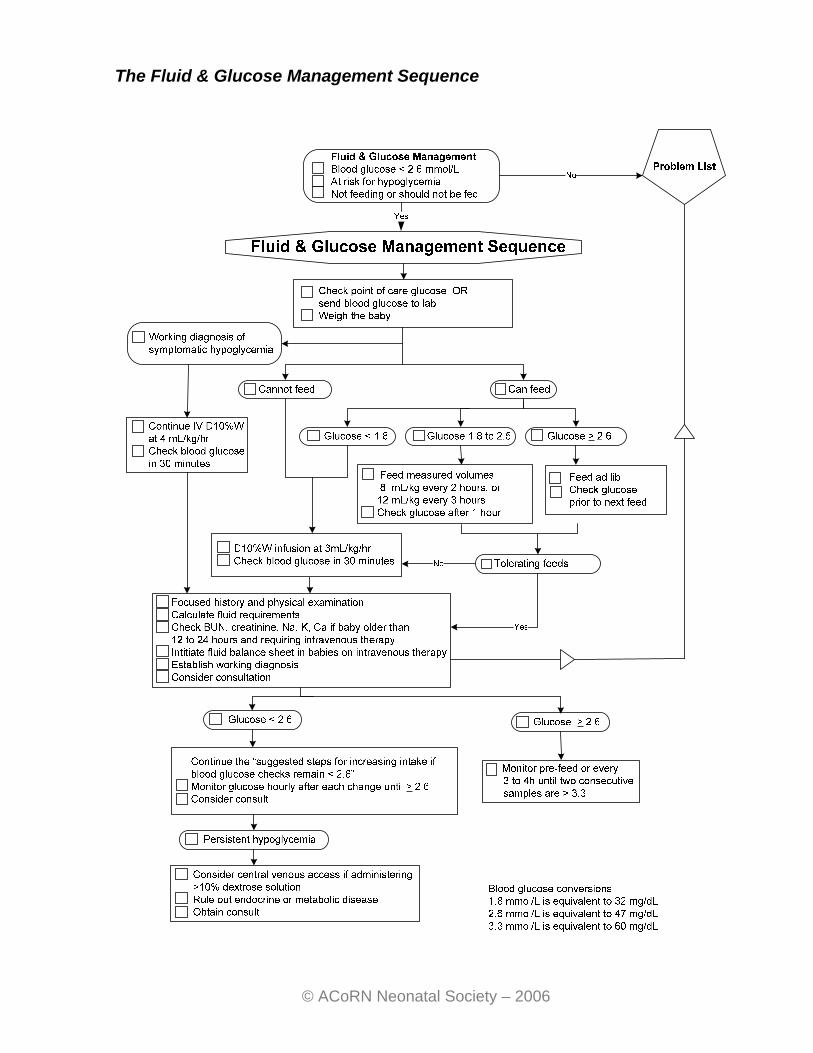
The Fluid & Glucose Management Sequence
© ACoRN Neonatal Society – 2006

© ACoRN Neonatal Society – 2006
Maintenance fluid
Postnatal age
Baseline oral intake (if not breastfed on cue)
Baseline intravenous intake (if not feeding)
Day 1 Up to 12 mL/kg every 3 hours
D10%W at 3 mL/kg/hour
Day 2 Up to 12 mL/kg every 3 hours
D10%W at 4 mL/kg/hour
Day 3 Up to 15 mL/kg every 3 hours
D10%W with 20 mmol/L of NaCl at 5 mL/kg/hour
≥ Day 4 Up to 18 to 20 mL/kg every 3 hours
D10%W with 20 mmol/L of NaCl at 6 mL/kg/hour (other electrolytes may be needed)
Glucose monitoring guidelines to ensure normal values are achieved after treatment is initiated:
Blood glucose level Monitoring guideline
< 2.6 mmol/L (< 47 mg/dL)
One hour after enteral feed and prior to the next feed, or 30 minutes after an IV bolus or starting an IV infusion.
2.6 to 3.3 mmol/L (47 to 60 mg/dL)
Prior to feeds; or every 4 to 6 hours if on an IV infusion
> 3.3 mmol/L (> 60 mg/dL)
Every 2nd to 3rd feed or every 6 to 8 hours if on an IV infusion. Transition to enteral feeds: discontinue monitoring after two consecutive glucose levels > 3.3 mmol/L (> 60 mg/dL).
Suggested steps for increasing glucose intake if blood glucose checks remain < 2.6 mmol/L (< 47 mg/dL)
Steps Enterally fed IV dextrose infusion
Baseline Breastfeed on cue, or Feed every 2 to 3 hours
D10%W, 3 mL/kg/hour (= 5 mg/kg/minute of glucose)
Step 1 Feed measured volume 8 mL/kg every 2 hours or 12 mL/kg every 3 hours, or Start IV dextrose infusion at baseline
D10%W, 4 mL/kg/hour (= 6.7 mg/kg/minute of glucose)
Step 2 Go to IV dextrose infusion step 1, and proceed from there
D12.5%W, 4 to 5 mL/kg/hour (= 8.3 to 10.4 mg/kg/minute of glucose) Obtain consultation and investigations Consider central access Consider glucagon or other pharmacological intervention

The Thermoregulation Sequence
© ACoRN Neonatal Society – 2006

The Infection Sequence
© ACoRN Neonatal Society – 2006

© ACoRN Neonatal Society – 2006
Transport Neonatal Pre-Transport Information Sheet
Date of call: Time of call:
Local facility physician’s name: Tel number:
Consultant physician/ Transport coordinator’s name:
Tel number:
Information about the baby
Name: Diagnosis/reason for consult: Birth date Time Sex Birth wt. Gestation Apgar score Eye prophylaxis?
1 min: 5 min: Vitamin K given?
Resuscitation:
Respiration Compressions Medications Spontaneous: Yes ( ) No ( ) Bag ventilation: Yes ( ) No ( ) O2: Yes ( ) % No ( ) Intubated: Time ETT size ______ Suction meconium below cords: Yes ( ) No ( )
Yes ( ) No ( ) Time initiated: Time stopped:
ETT: IV:
Congenital anomalies: Postnatal course:
Heart rate: RR: BP: Perfusion: SaO2: FiO2: IPPV:
Current status:
Physical exam: Feeding/intravenous: X-rays – results: Laboratory – results: Cord/other blood gases: Information about the mother Name: Age: G: P: LMP/EDC: / Blood group Rh VDRL Rubella HBsAG TB HIV Group B Strep: Pos ( ) Neg ( ) Unknown/not done ( ) Date / / Past obstetric history: Labour & delivery Fetal monitoring: Yes ( ) No ( ) Internal ( ) External ( ) Auscultation ( ) Scalp pH _________ Length of labour: 1st stage 2nd stage ______ AROM ( ) SROM ( ) Date Time Colour Amount __________ Medications: Anesthesia/analgesia: Type of delivery: C. Section ( ) Vaginal ( ) Forceps ( ) Vacuum ( ) Presentation Complications:
Date: / / Signature and title:
Adapted from: PPPESO. Neonatal Transport. Perinatal Nursing Guidelines (3rd Ed). Ottawa, ON: Perinatal Partnership Program of Eastern and Southeastern Ontario, 2001.

© ACoRN Neonatal Society – 2006
Related Documents