Teratogenic Effects Minimization of Norfloxacin in Pregnant and Breast feeding Female Bose Anannya , Paul Susanta Department Of Pharmaceutics Calcutta Institute Of Pharmaceutical Technology & A.H.S Banitabla, Uluberia, Howrah-711316 , West Bengal ,India ABSTRACT: Norfloxacin significantly decreased the number of viable fetuses, increased the number of resorbed fetuses, and induced retardation in growth of viable fetuses; some visceral and skeletal defects in these fetuses were seen and these effects were dose dependant. Conclusively, norfloxacin caused some fetal defects and abnormalities, so it is advisable to avoid using this drug during pregnancy. Over ten million women are either pregnant or lactating in the world at any time. The risks of medication use for these women are unique. In addition to normal physiologic changes that alter the pharmacokinetics of drugs, there is the concern of possible teratogenic and toxic effects on the developing fetus and newborn. This article reviews the risks and pharmacokinetic considerations for broad-spectrum antibiotics instead of norfloxacin that can be used to treat routine and life-threatening infections during pregnancy and lactation. KEY WORDS : Pregnancy, Teratogenicity, Norfloxacin, Drug therapy, Lactation. INTRODUCTION: Teratology, the study of abnormal prenatal development and congenital malformations induced by exogenous chemical or physical agents, is a growing area of medical research in the quest for the eradication of preventable birth defects. Birth defects are known to occur in huge numbers; roughly 710% of all children require extensive medical care to diagnose or treat a birth defect; this compromises the quality of life of millions of people worldwide . Almost all therapeutic agents cross placental barrier and enter fetal circulation. Every agent given during pregnancy therefore has a tendency to produce some sort of structural abnormality in the neonate at birth until proved otherwise. A birth defect or a congenital malformation is a structural abnormality of any type present at birth. It may be macroscopic or microscopic, on the surface or within the body. During the past few decades, it has become increasingly evident that human and animal embryos are subjected to the toxic effects of many drugs, such as the use of some antibiotics in the treatment of serious diseases occurring during pregnancy. Fluoroquinolones are

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Teratogenic Effects Minimization ofNorfloxacin in Pregnant and Breast feeding
Female Bose Anannya , Paul Susanta
Department Of Pharmaceutics
Calcutta Institute Of Pharmaceutical Technology& A.H.S
Banitabla, Uluberia, Howrah-711316 , West Bengal ,India
ABSTRACT: Norfloxacin significantly decreased the number of viable fetuses, increased the number of resorbed fetuses, and induced retardation in growth of viable fetuses; some visceral and skeletal defects in these fetuses were seen and these effects were dose dependant. Conclusively, norfloxacin caused some fetal defects and abnormalities, so it is advisable to avoid usingthis drug during pregnancy.Over ten million women are either pregnant or lactating in the world at any time. The risks of medication use for these women are unique. In addition to normal physiologic changes that alter the pharmacokinetics of drugs, there is the concern of possible teratogenic and toxic effects on the developing fetus and newborn. This article reviews the risks and pharmacokinetic considerationsfor broad-spectrum antibiotics instead of norfloxacin that can be used to treat routine and life-threatening infections during pregnancy and lactation.KEY WORDS : Pregnancy, Teratogenicity, Norfloxacin, Drug therapy, Lactation.
INTRODUCTION: Teratology, the study of abnormal prenatal development and congenital malformations induced by exogenous chemical or physical agents, is a growing area of medical research in the quest for the eradication of preventable birth defects. Birth defects are known to occur in huge numbers; roughly 710% of all children require extensive medical care to diagnose or treat a birth defect; this compromises the quality of life of millions of people worldwide . Almost all therapeutic agents cross placental barrier and enter fetal circulation. Every agent given during pregnancy therefore has a tendency to produce some sort of structural abnormality in the neonate at birth until proved otherwise. A birth defect or a congenital malformation is astructural abnormality of any type present at birth. It may be macroscopic or microscopic, on the surface or within the body. During the past few decades, it has become increasingly evident that human and animal embryos are subjectedto the toxic effects of many drugs, such as the use of some antibiotics in thetreatment of serious diseases occurring during pregnancy. Fluoroquinolones are
one of the main classes of antimicrobials used in treatment of many infectionsincluding urinary, respiratory, gastrointestinal tract, skin, bone, and joint infections .
The popularity of fluoroquinolone antibiotics has increased because of their broad antimicrobial spectrum, multiple approved indications, and favorable pharmacokinetics.
Norfloxacin is synthetic antimicrobial agent of the fluoroquinolones class. Like other fluoroquinolones, norfloxacin acts principally by inhibition of DNAgyrase, an enzyme required for the proper supercoiling of bacterial chromosomes. Norfloxacin is active mainly against Gram-negative and Gram-positive pathogens. It has a wide spectrum of activity and is rapidly bactericidal at low concentration .Norfloxacin is mainly used for the treatment of urinary tract infections whichhave high incidence during pregnancy especially in the first trimester.Antibiotics are among the most commonly prescribed prescription medications for pregnant and lactating women.1 More than 10 million women are either pregnant or lactating in the world at any one time, and they are administeredantibiotics for many reasons.2 Because of the special considerations associated with fetal and newborn development, these women constitute a uniquely vulnerable population for which the risks of medication use must be separately assessed. In addition to the pharmacokinetic and pharmacodynamic changes that may occur during pregnancy and lactation that can alter the effectiveness of drugs,3 there is the added concern of the possible teratogenic and toxic effects that medications may have on thedeveloping fetus and newborn. In general, there is a dearth of pharmacokineticand pharmacodynamic information regarding the use and proper dosing of Food and Drug Administration (FDA)–approved drugs in pregnant and lactating women, as well aslimited data pertaining to the teratogenic potential and the fetal or neonataltoxicity of these marketed medications. Accordingly, sparse information must sometimes be assembled from diverse sources to address these issues.Recently, the threat of bioterrorism has expanded the context in which the potential use of antibioticmedications may be needed.4 Although the possibility of a large-scale bioterrorist attack in the United States is unlikely, the potential for widespread antibiotic use in this situation emphasizes the need for health care professionals to be familiar with the risks and benefits of administeringantibiotics to pregnant and lactating women. This article reviews the available information concerning the risks and special circumstances to be considered in pregnant and lactating women for a group of 11 broad-spectrum antibiotics (amoxicillin, chloramphenicol, ciprofloxacin, clindamycin, doxycycline, gentamicin, levofloxacin, penicillin G, penicillin VK, rifampin, and vancomycin). By using this information, better choices can be made for thetreatment of different types of bacterial pathogens in these particularly vulnerable populations. With this objective in view, the present paper was done to demonstrate the teratogenic effects of norfloxacin in pregnant females

and the use of other antibiotics instead of norfloxacin to reduce the teratogenic activity of norfloxacin.
Norfloxacin Pregnancy Warnings: Norfloxacin has been assigned to pregnancy category C by the FDA. High-dose animal studies have revealed evidence of embryolethality. There are no controlled data in human pregnancy. Surveillance studies have not reported an increased risk of major birth defects. However, cartilage damage and arthropathies have been reported in immature animals giving rise to concern over effects on fetal bone formation.
Because safer alternatives are generally available, some experts consider norfloxacin contraindicated during pregnancy, especially during the first trimester. The manufacturer only recommends use of norfloxacin during pregnancy when benefit outweighs risk.
Of 549 cases reported by the European Network of Teratology Information Services involving fluoroquinolone exposure (including norfloxacin), congenital malformations were reported in 4.8%; however, this was not higher than the background rate. In the Michigan Medicaid study, major birth defects were reported in 5 of 139 exposed neonates. Berkovitch et al. reviewed 35 pregnancies in women who received norfloxacin or ciprofloxacin during the first trimester for the treatment of urinary tract infections. No malformations were reported among these infants. When compared to infants not exposed to quinolones, there was no difference in the acquisition of developmental milestones and no joint problems or walking delays.
Norfloxacin Breastfeeding Warnings : It is not known whether norfloxacin is excreted into human milk. However, since other fluoroquinolone antibiotics are excreted into human milk, it is likely that norfloxacin is also. Quinolone-induced cartilage erosion and arthropathies that have been observed in juvenile animals render some concern over its possible toxic effects on the developing joints of nursing infants. Because of the potential for serious adverse reactions in nursing infants, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
Norfloxacin Levels and Effects while Breastfeeding :

Summary of Use during Lactation
Fluoroquinolones such as norfloxacin have traditionally not been used in infants because of concern about adverse effects on the infants' developing joints. However, recent studies indicate little risk.[1][2] In addition, the calcium in milk might prevent absorption of the small amounts of fluoroquinolones in milk,[3] but insufficient data exist to prove or disprove this assertion. The serum and milk levels and oral bioavailability of norfloxacin are the lowest of any of the fluoroquniolones, so the risk to the infant should be minimal. Short-term use of norfloxacin is acceptable in nursing mothers.
CLINICAL PROFILE OF NORFLOXACIN :
Pharmacokinetic data : “Absorption of norfloxacin is rapid following single doses of 200 mg, 400 mg and 800 mg. At the respective doses, mean peak serum and plasma concentrations of 0.8, 1.5 and 2.4 μg/mL are attained approximately one hour after dosing. The effective half-life of norfloxacin in serum and plasma is 3–4 hours. Steady-state concentrations of norfloxacin will be attained within two days of dosing. Renal excretion occurs by both glomerular filtration and tubular secretion as evidenced by the high rate of renal clearance (approximately 275 mL/min). Within 24 hours of drug administration, 26 to 32% of the administered dose is recovered in the urine as norfloxacin with an additional 5-8% being recovered in the urine as six active metabolites of lesser antimicrobial potency. Only a small percentage (less than 1%) of thedose is recovered thereafter. Fecal recovery accounts for another 30% of the administered dose. Two to three hours after a single 400-mg dose, urinary concentrations of 200 μg/mL or more are attained in the urine. In healthy volunteers, mean urinary concentrations of norfloxacin remain above30 μg/mL for at least 12 hours following a 400-mg dose. The urinary pH may affect the solubility of norfloxacin. Norfloxacin is least soluble at urinary pH of 7.5 with greater solubility occurring at pHs above and below this value. The serum protein binding of norfloxacin is between 10 and 15%.” Quoting from the 2009 package insert for Noroxin. Biotransformation is via the liver and kidneys, with a half-life of 3–4 hours.
Mode of action: Norfloxacin is a broad-spectrum antibiotic that is active against both Gram-positive and Gram-negative bacteria. It functions by inhibiting DNA gyrase, a type II topoisomerase, and topoisomerase IV
enzymes necessary to separate bacterial DNA, thereby inhibiting cell division.
Mechanism of resistance : Because of the unique mechanism of action,plasmid mediated transferable resistance probably does not occur. Resistance noted so far is due to chromosomal mutation producing a DNA gyrase or topoisomerase IV with reduced affinity for norfloxacin, or due toreduced permeability/increased efflux of these drugs across bacterial membranes. In contrast to nalidixic acid which selects single step resistant mutants at high frequency, Norfloxacin resistant mutants are not easily selected. Therefore, resistance to Norfloxacin has been reported among salmonella, pseudomonas, staphylococci, gonococci, and pneumococci
USES: Norfloxacin is used to treat a variety of bacterial infections. This the kidneys and infect them.medication belongs to a class of drugs called quinolone antibiotics. It works by stopping the growth of bacteria.This antibiotic treats only bacterial infections. It will not workfor virus infections (e.g., common cold, flu). Unnecessary use or overuse of any antibiotic can lead to its decreased effectiveness.Norfloxacin is anantibiotic used to treat some bacterial infections, such as:
urinary tract infections. infections of the stomach or intestines, such as traveller's
diarrhoea.
Norfloxacin is also used for patients who get frequent urinary tract infections. Norfloxacin may help stop these infections from coming back.Urinary tract infections are caused bythe presence of bacteria in the urinarysystem. The bacteria often comefrom the intestines where they arenecessary for normal function.In women, the most common infection involvesthe bladder and is called cystitis. In men, the infection may involve the prostate, which is called prostatitis. In both men andand women, the bacteriamay travel up to the kidneys and infect them.Norfloxacin belongs to a group of antibiotics calledquinolones. Norfloxacin works by killing the bacteria causing the infection.
DOSE STUDIES: Single-Dose Studies:In clinical trials involving 82 healthy subjects and 228 patients with gonorrhea, treated with a single dose of norfloxacin, 6.5% reported drug-related adverse experiences. However, the following incidence figures were calculated without reference to drug relationship.

The most common adverse experiences ( > 1.0%) were: dizziness (2.6%), nausea (2.6%), headache (2.0%), and abdominal cramping (1.6%).
Additional reactions (0.3%-1.0%) were: anorexia, diarrhea, hyperhidrosis,asthenia, anal/rectal pain, constipation, dyspepsia, flatulence, tingling of the fingers, and vomiting.
Laboratory adverse changes considered drug-related were reported in 4.5% of patients/subjects. These laboratory changes were: increased AST (SGOT) (1.6%), decreased WBC (1.3%), decreased platelet count (1.0%), increased urine protein (1.0%), decreased hematocrit and hemoglobin (0.6%), and increased eosinophils (0.6%).
Multiple-Dose Studies:
In clinical trials involving 52 healthy subjects and 1980 patients with urinary tract infections or prostatitis treated with multiple doses of norfloxacin, 3.6% reported drug-related adverse experiences. However, the incidence figures below were calculated without reference to drug relationship.
The most common adverse experiences ( > 1.0%) were: nausea (4.2%), headache (2.8%), dizziness (1.7%), and asthenia (1.3%).
Additional reactions (0.3%-1.0%) were: abdominal pain, back pain, constipation, diarrhea, dry mouth, dyspepsia/heartburn, fever, flatulence, hyperhidrosis, loose stools, pruritus, rash, somnolence, and vomiting.
Less frequent reactions (0.1%-0.2%) included: abdominal swelling, allergies, anorexia, anxiety, bitter taste, blurred vision, bursitis, chest pain,
chills, depression, dysmenorrhea, edema, erythema, foot or hand swelling, insomnia, mouth ulcer, myocardial infarction, palpitation, pruritus ani, renalcolic, sleep disturbances, and urticaria.
Abnormal laboratory values observed in these patients/subjects were:eosinophilia (1.5%), elevation of ALT (SGPT) (1.4%), decreased WBC and/orneutrophil count (1.4%), elevation of AST (SGOT) (1.4%), and increased alkaline phosphatase (1.1%). Those occurring less frequently included increased BUN, increased LDH, increased serum creatinine, decreased hematocrit, and glycosuria.
WHILE TAKING NORFLOXACIN:Do not take norfloxacin if:
• you have an allergy to the active ingredient, norfloxacin, other quinolone antibiotics (for example ciprofloxacin or ofloxacin or any of the ingredientslisted at the end of this leaflet.Symptoms of an allergic reaction may include itchiness, hives, swelling of the face, lips, tongue, and/or throat (which may cause difficulty in breathing or swallowing), muscle pain or tenderness, or joint pain.
• you are pregnant or breastfeeding. Your baby may absorb this medicine in the womb or from breast milk and therefore there is a possibility of harm to the baby.
Do not give norfloxacin to children or to growing teenagers, unless advisedby the doctor. The safety of norfloxacin has not been adequately studied in these people. If you are not sure whether you should start taking norfloxacin, talk to your doctor.the packaging is torn or shows signs of tampering.
How much to take: Take norfloxacin only when prescribed by your doctor. Your doctor will tell you how many tablets you need to take each day. This
depends on your condition and whether or not you are taking any other medicines. The usual dose of norfloxacin 400mg tablets is one tablet twice a day.
When to take it:
Taking norfloxacin at evenly spaced times ensures that there is a reasonably constant amount in the blood and urine This means that the medicine will fight the infection more effectively.Take norfloxacin on an empty stomach, atleast one hour before food or 2 hours after food or after taking milk and/or other dairy products.This will make sure the tablets will have a better chance of fighting the infection, because food can interfere with the absorption of norfloxacin.Do not take norfloxacin at the same time as taking iron or zinc supplements (or multivitamins containing them), antacids, sucralfate, or didanosine (ddI).Taking norfloxacin at the same time or even within 2 hours of taking these can interfere with the absorption norfloxacin,so that the chance of norfloxacin fighting the infection won't be as good.
Taking other medicines:
Some medicines and norfloxacin may interfere with each other. These include:
• nitrofurantoin, another antibiotic used to treat urinary tract infections.
• theophylline and other methylxanthines, medicines used to treat asthma. Caffeine is also a methylxanthine.
• warfarin, phenindione and other medicines used to prevent blood clots.
• cyclosporin, a medicine commonly used in patients who have received organ transplants.
• glibenclamide, a medicine used to treat diabetes.
• non-steroidal anti- inflammatory medicines, used to treat muscular problemsand arthritis. The combination of these medicines with norfloxacin may cause convulsions.
• erythromycin, another antibiotic used to treat and in some cases prevent infection.
• cisapride, a medicine used to treat discomfort due to the stomach acid flowing the wrong way up the oesophagus (also called the food pipe).
These medicines may be affected by norfloxacin, or may affect how well it works. You may need different amounts of your medicine, or you may need to take different medicines.
Some medicines may interfere with the absorption of norfloxacin. These include:
• iron or zinc supplements, and multivitamins containing them.
• antacids used for indigestion.
• sucralfate, a medicine used to ulcers.
• didanosine, a medicine used to treat HIV infection.
You can still take these medicines while you are taking norfloxacin. However,you must take norfloxacin at least 2 hours before or 2 hours after taking anyof these medicines to make sure there is no problem with absorption.
If you take too much:(Over dose)
Immediately telephone your doctor or Poisons Information Centre for advice ifyou think that you or anyone else may have taken too much norfloxacin. Do this even if there are no signs of discomfort or poisoning. Keep telephone numbers of these places handy.

While you r taking it:
Things you must do: If you become pregnant while taking norfloxacin, tell your doctor immediately.If you develop severe diarrhoea, tell your doctor or pharmacist immediately. Do this even if it occurs several weeks after norfloxacin has been stopped.Diarrhoea may mean that you have a serious condition affecting your bowel. You may need urgent medical care. Do not takeany diarrhoea medicine without first checking with your doctor.This will helpto prevent crystals forming in the urine, which can cause kidney problems. However, this is not a common problem.
Things you must not do: Do not stop taking your tablets because you are feeling better, unless advised by your doctor.If you do not complete the fullcourse prescribed by your doctor, some of the bacteria causing your infectionmay not be killed. These bacteria may continue to grow and multiply so that your infection may not clear completely or it may return.
SIDE EFFECTS of NORFLOXACIN:
• Chest pain or discomfort
• chills
• diarrhea
• discouragement
• fast, irregular, pounding, or racing heartbeat or pulse
• feeling sad or empty
• fever
• flushing or redness of the skin
• hives or welts
• increased sweating
• irritability
• irritation or soreness of the mouth
• itching of the rectal area
• itching skin
• lack of appetite
• loss of interest or pleasure
• nausea
Other drug affects of norfloxacin :
• cisapride, cyclosporine, erythromycin, nitrofurantoin, probenecid, ropinirole, tacrine, theophylline, tizanidine.
• a diuretic or "water pill".
• heart rhythm medication--amiodarone, disopyramide, dofetilide, dronedarone,procainamide, quinidine, sotalol, and others.
• medicine to treat depression or mental illness--amitriptylline, clomipramine, clozapine, desipramine, duloxetine, iloperidone, imipramine, nortriptyline, thioridazine, ziprasidone, and others; or
• NSAIDs (nonsteroidal anti-inflammatory drugs)--aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve), celecoxib, diclofenac, indomethacin, meloxicam, and others.
This list is not complete. Other drugs may interact with norfloxacin, including prescription and over-the-counter medicines, vitamins, and herbal products. Not all possible interactions are listed in this medication guide.
The possible food and drug interaction associated with this medication: If Norfloxacin is taken with certain other drugs, the effects of either could be increased, decreased, or altered. It is especially important to check with your healthcare provider before combining Norfloxacinwith any of the following: antacids containing aluminum or magnesium, antidepressants, nonsteroidal anti-inflammatory drugs (NSAIDs) (such as ibuprofen), blood thinners (such as warfarin), caffeine, cisapride, clozapine, corticosteroids, cyclosporine, didanosine, diuretics (water pills), erythromycin, heart rhythm medications (such as amiodarone, procainamide, quinidine, or sotalol), insulin or oral diabetes medications (such as glyburide), nitrofurantoin, probenecid, ropinirole, sucralfate, tacrine, theophylline, tizanidine, or multivitamins or other products containing iron or zinc.
Effect on pregnancy: Norfloxacin has been reported to rapidly cross the blood-placenta and blood-milk barrier, and is extensively distributed into
the fetal tissues. For this reason norfloxacin and other fluoroquinolones arecontraindicated during pregnancy due to the risk of spontaneous abortions andbirth defects. The fluoroquinolones have also been reported as being present in the mother’s milk and are passed on to the nursing child, which may increases the risk of the child suffering an adverse reaction even though thechild had never been prescribed or taken any of the drugs found within this class. As safer alternatives are generally available norfloxacin is contraindicated during pregnancy, especially during the first trimester. The manufacturer only recommends use of norfloxacin during pregnancy when benefitoutweighs risk.
It has long been observed that pregnancy may influence the development and course of urinary tract disorders.The physiological and anatomical changes inherent in normal pregnancy and the changing hormonal environment are generally assumed to play a role in the pathogenesis of urinary tract symptomatology. The purpose of this review is to examine the reported effect(s) of pregnancy on the lower urinary tract and to evaluate the possible role of pregnancy and delivery in lower urinary tract dysfunction.
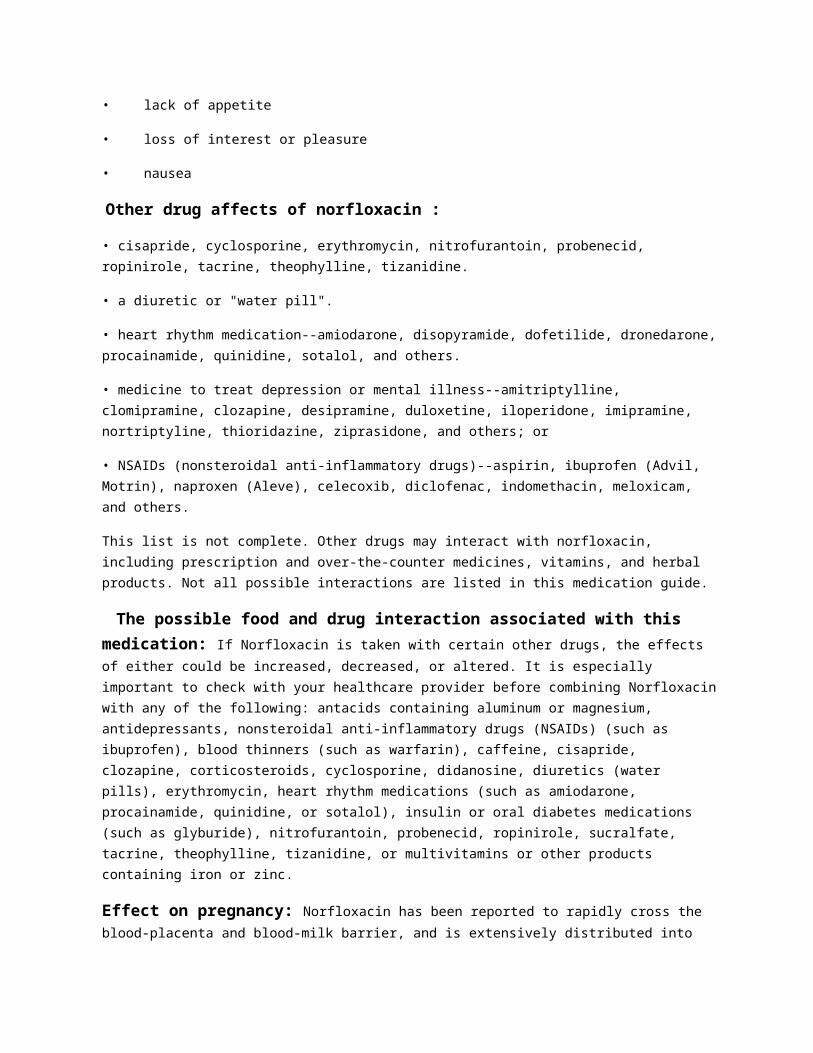
Mohamed Aboubakr, Mohamed Elbadawy, Ahmed Soliman, Mohamed El-Hewaity have
showed Embryotoxic and Teratogenic Effects of Norfloxacin in Pregnant Female
Albino Rats.
Fig 1 : Pulmonary hypoplasia with cardiac enlargement
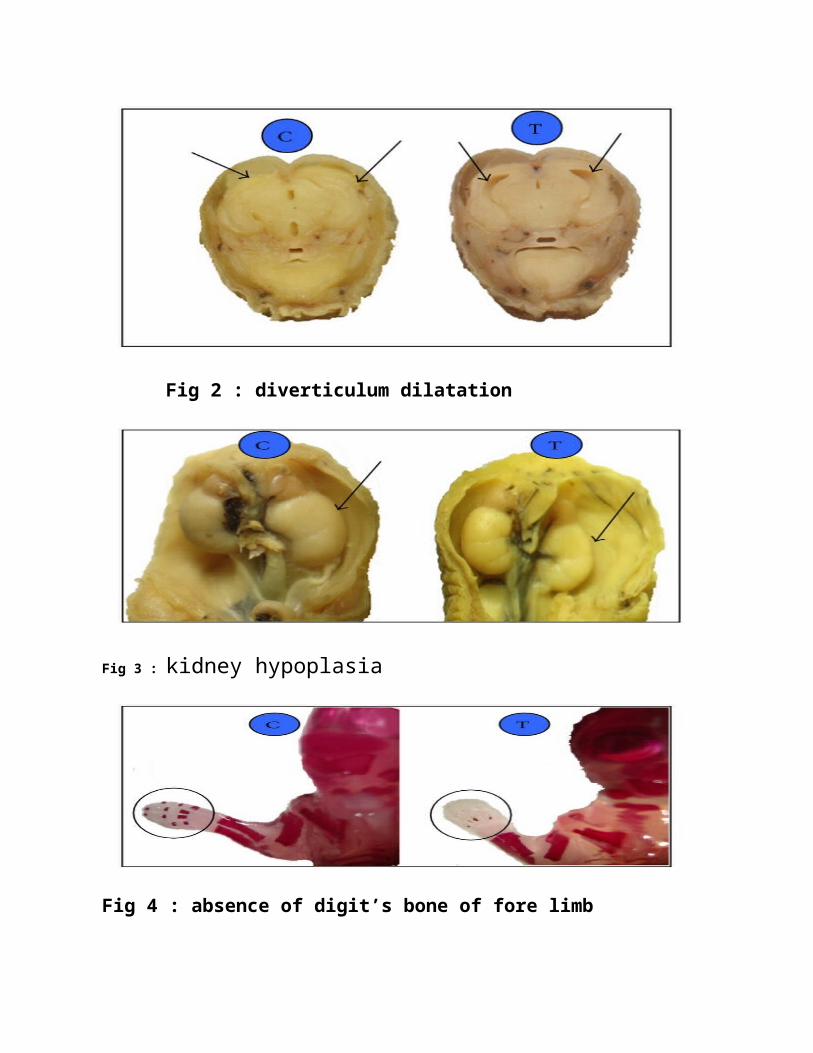
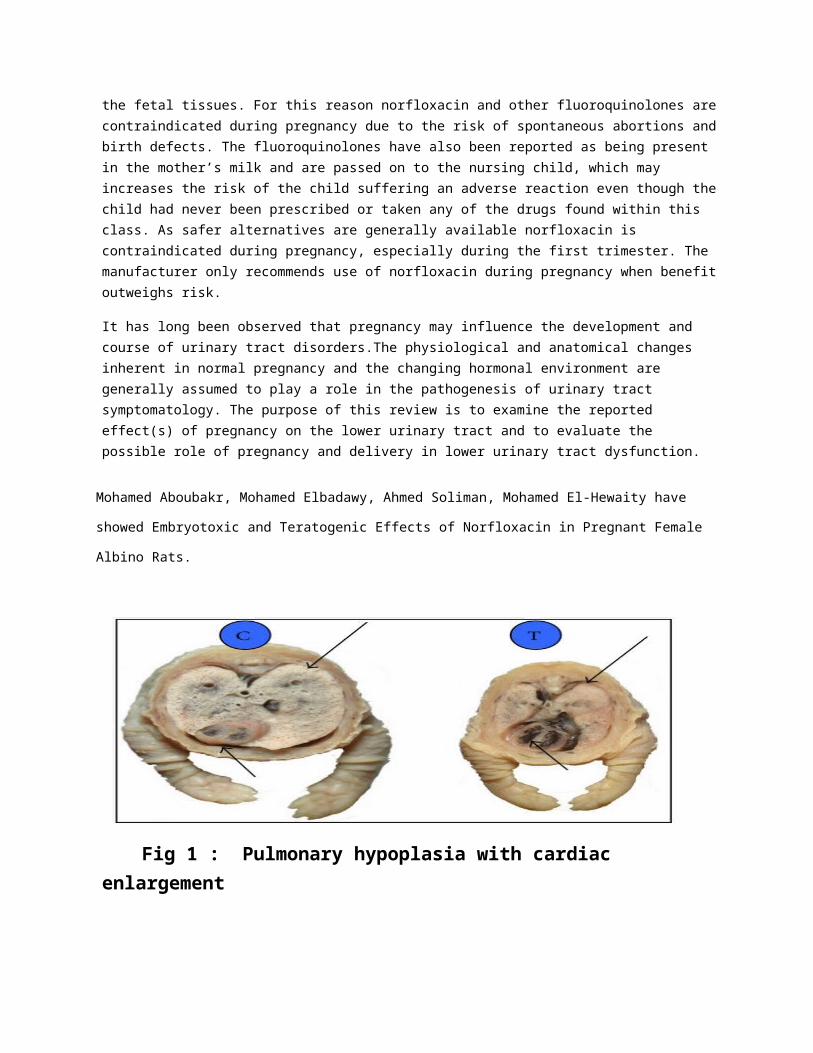
Fig 2 : diverticulum dilatation
Fig 3 : kidney hypoplasia
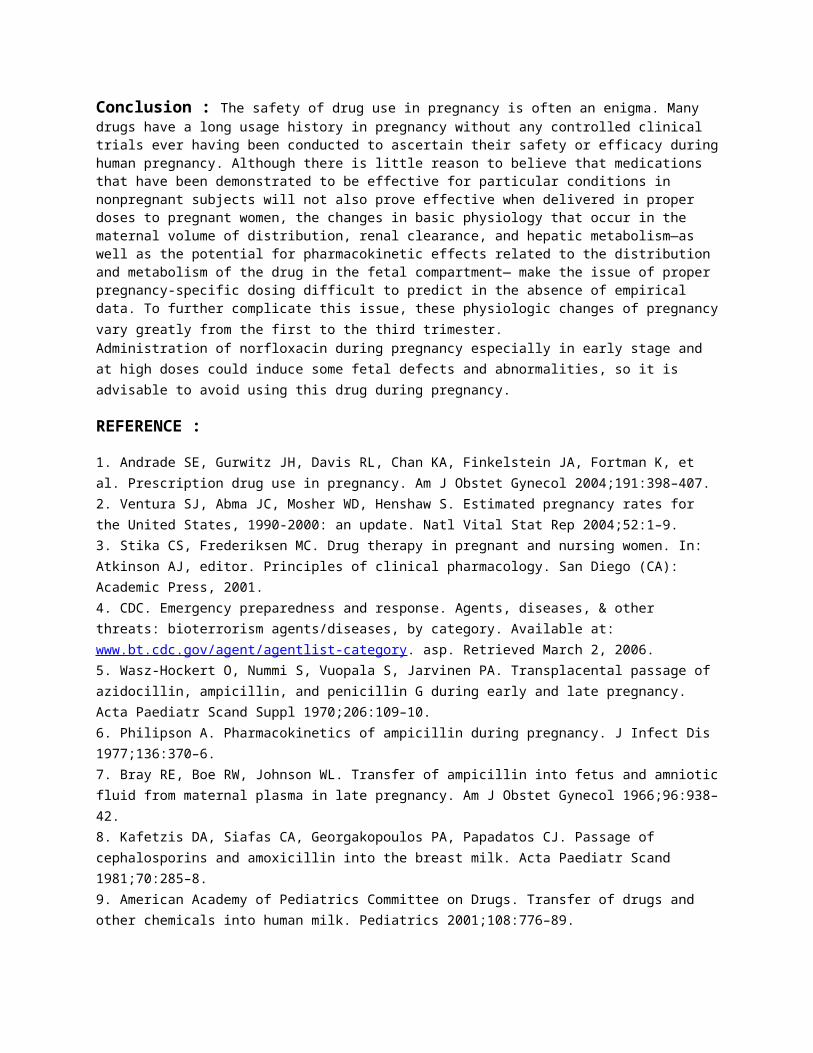
Fig 4 : absence of digit’s bone of fore limb

Fig 5 : Partial absence of caudal vertebrae
Fig 6 : irregular and short ribs of a fetuses obtained from pregnant rats after repeated oral administration
Important warning: Taking norfloxacin increases the risk that you will develop tendinitis (swelling of a fibrous tissue that connects a bone to a muscle) or have a tendon rupture (tearing of a fibrous tissue that connects abone to a muscle) during your treatment or for up to several months afterward. These problems may affect tendons in your shoulder, your hand, theback of your ankle, or in other parts of your body. Tendinitis or tendon rupture may happen to people of any age, but the risk is highest in people over 60 years of age. Tell your doctor if you have or have ever had a kidney,heart, or lung transplant; kidney disease; a joint or tendon disorder such asrheumatoid arthritis (a condition in which the body attacks its own joints, causing pain, swelling, and loss of function); or if you participate in regular physical activity. Also tell your doctor if you have ever had any tendon problems during or after your treatment with norfloxacin or another quinolone or fluoroquinolone antibiotic. Tell your doctor and pharmacist if you are taking oral or injectable steroids such as dexamethasone (Decadron, Dexpak), methylprednisolone (Medrol), or prednisone (Sterapred). If you experience any of the following symptoms of tendinitis, stop taking

norfloxacin, rest, and call your doctor immediately: pain, swelling, tenderness, stiffness, or difficulty in moving a muscle. If you experience any of the following symptoms of tendon rupture, stop taking norfloxacin and get emergency medical treatment: hearing or feeling a snap or pop in a tendonarea, bruising after an injury to a tendon area, or inability to move or bearweight on an affected area.
Taking norfloxacin may worsen muscle weakness in people with myasthenia gravis (a disorder of the nervous system that causes muscle weakness) and cause severe difficulty breathing or death. Tell your doctor if you have myasthenia gravis. Your doctor may tell you not to take norfloxacin. If you have myasthenia gravis and your doctor tells you that you should take
norfloxacin, call your doctor immediately if you experience muscle weakness or difficulty breathing during your treatment.Fluoroquinolones, including
Norfloxacin, are associated with an increased risk of tendinitis and tendon rupture in all ages. This risk is further increased in older patients usually over 60 years of age, in patients taking corticosteroid drugs, and inpatients with kidney, heart or lung transplants.
Fluoroquinolones, including norfloxacin, may exacerbate muscle weakness in persons with myasthenia gravis. Avoid Norfloxacin in patients with known
history of myasthenia gravis.
Precauation when taking norfloxacin: Before taking norfloxacin, tell your doctor or pharmacist if you are allergic to it; or to other quinolone antibiotics such as ciprofloxacin, gemifloxacin, levofloxacin, moxifloxacin, or ofloxacin; or if you have any other allergies. This product may contain inactive ingredients, which can cause allergic reactions or other problems. Talk to your pharmacist for more details.
Before using this medication, tell your doctor or pharmacist your medical history, especially of: certain metabolic disorder (G6PD deficiency), diabetes, heart problems (e.g., recent heart attack), joint/tendon problems (e.g., tendonitis, bursitis), kidney disease, myasthenia gravis, nerve problems (such as peripheral neuropathy), seizure disorder, conditions that increase your risk of seizures .
Antibiotics used during Pregnancy : Antibiotics which is approved by FDA should be used during pregnancy instead of

norfloxacin. A table is shown below of listed antibiotics with their mechanism of action.
Antibiotic Description Year of InitialFDA
ApprovalAmoxicillin Semi-synthetic beta-lactam antibiotic.
Inhibits the final stage ofbacterial cell wall synthesis, leading to celllysis.
1974
Chloramphenicol Broad-spectrum antibiotic isolated from Streptomyces venezuela in1947, now synthetically available. Binds to the 50S subunit ofbacterial ribosomes, inhibiting peptide bond formation andprotein synthesis
1950
Ciprofloxacin Fluoroquinolone antibiotic. Exerts its bactericidal effect bydisrupting DNA replication, transcription, recombination, andrepair by inhibiting bacterial DNA gyrase.
1987
Clindamycin Antibiotic derived from lincomycin that has wide-rangingantimicrobial activity. Binds to the 50S ribosomal subunit,thereby inhibiting bacterial protein synthesis
1970
Doxycycline Broad-spectrum antibiotic that binds to the 30S bacterial ribosomalsubunit. Blocks the binding of transfer-RNA tomessenger-RNA,thereby disrupting protein synthesis.
1967
Levofloxacin Fluoroquinolone antibiotic. L-isomer of ofloxacin, which providesits principal antibiotic effect. Inhibits bacterial DNA replication,transcription, recombination, and repair by inhibiting bacterialtype II topoisomerases
1996
Penicillin G Beta-lactam antibiotic that is primarily bactericidal. Inhibits thefinal stage of bacterial cell wall synthesis, leading to cell lysis.
1943
Table 1 : Description of the FDA approved Broad-Spectrum Antibiotics whichcan be use during pregnancy.
Conclusion : The safety of drug use in pregnancy is often an enigma. Many drugs have a long usage history in pregnancy without any controlled clinical trials ever having been conducted to ascertain their safety or efficacy duringhuman pregnancy. Although there is little reason to believe that medications that have been demonstrated to be effective for particular conditions in nonpregnant subjects will not also prove effective when delivered in proper doses to pregnant women, the changes in basic physiology that occur in the maternal volume of distribution, renal clearance, and hepatic metabolism—as well as the potential for pharmacokinetic effects related to the distribution and metabolism of the drug in the fetal compartment— make the issue of proper pregnancy-specific dosing difficult to predict in the absence of empirical data. To further complicate this issue, these physiologic changes of pregnancyvary greatly from the first to the third trimester. Administration of norfloxacin during pregnancy especially in early stage and at high doses could induce some fetal defects and abnormalities, so it is advisable to avoid using this drug during pregnancy.
REFERENCE :
1. Andrade SE, Gurwitz JH, Davis RL, Chan KA, Finkelstein JA, Fortman K, et al. Prescription drug use in pregnancy. Am J Obstet Gynecol 2004;191:398–407.2. Ventura SJ, Abma JC, Mosher WD, Henshaw S. Estimated pregnancy rates for the United States, 1990-2000: an update. Natl Vital Stat Rep 2004;52:1–9.3. Stika CS, Frederiksen MC. Drug therapy in pregnant and nursing women. In: Atkinson AJ, editor. Principles of clinical pharmacology. San Diego (CA): Academic Press, 2001.4. CDC. Emergency preparedness and response. Agents, diseases, & other threats: bioterrorism agents/diseases, by category. Available at: www.bt.cdc.gov/agent/agentlist-category. asp. Retrieved March 2, 2006.5. Wasz-Hockert O, Nummi S, Vuopala S, Jarvinen PA. Transplacental passage of azidocillin, ampicillin, and penicillin G during early and late pregnancy. Acta Paediatr Scand Suppl 1970;206:109–10.6. Philipson A. Pharmacokinetics of ampicillin during pregnancy. J Infect Dis 1977;136:370–6.7. Bray RE, Boe RW, Johnson WL. Transfer of ampicillin into fetus and amnioticfluid from maternal plasma in late pregnancy. Am J Obstet Gynecol 1966;96:938–42.8. Kafetzis DA, Siafas CA, Georgakopoulos PA, Papadatos CJ. Passage of cephalosporins and amoxicillin into the breast milk. Acta Paediatr Scand 1981;70:285–8.9. American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics 2001;108:776–89.

10. Nau H. Clinical pharmacokinetics in pregnancy and perinatology. II. Penicillins. Dev Pharmacol Ther 1987;10:174–98.11. Heikkila AM, Erkkola RU. The need for adjustment of dosage regimen of penicillin V during pregnancy. Obstet Gynecol 1993;81:919–21.12. Scott WC, Warner RF. Placental transfer of chloramphenicol (chloromycetin). J Am Med Assoc 1950;142:1331–2.13. Havelka J, Hejzlar M, Popov V, Viktorinova D, Prochazka J. Excretion of chloramphenicol in human milk. Chemotherapy 1968;13:204–11.14. J. C. Kim, S. H. Kim, D. H. Shin et al., “Developmental toxicityassessment of the new fluoroquinolone antibacterial DW-116 inrabbits,” Journal of Applied Toxicology, vol. 25, no. 1, pp. 52–59, 2005.15.M. M. Hall, J. T. Finnoff, and J. Smith, “Musculoskeletal complications offluoroquinolones: guidelines and precautions for usage in the athleticpopulation,” Journal of Injury, Function and Rehabilitation, vol. 3, no. 2,pp. 132–142, 2011.16.R. Stahlmann, “Children as a special population at risk-quinolones as anexample for xenobiotics exhibiting skeletal toxicity,” Archives of Toxicology,vol. 77, no. 1, pp. 7–11, 2003.17.N. K. Arora, “Are fluoroquinolones safe in children?” Indian Journal ofPediatrics, vol. 61, no. 6, pp. 601–603, 1994.
Related Documents











