UC SF Telehealt h “You cannot separate the technology from the process.”

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
UCSF
Telehealth“You cannot separate the technology from the process.”

UCSFThree legs of Telehealth
• Live-Video
– Cisco gives us a very strong position
• Store & Forward
– Asynchronous consultations such as
eConsult/eReferral, Tele-Derm and
Tele-Ophthamology
– PACs and EHR integration
• Remote Patient Monitoring
– Enabling the Ubiquitous vs. Episodic care paradigm

UCSFTelehealth’s Organizational Position
• Governance
– The Telehealth Resource Center reports to the
Telehealth Steering Committee
• Strategic tool that allows UCSF to:
– Build an extended referral network
– Export UCSF’s expertise and brand via remote
consultation and education
• Tactical tool that allows UCSF to:
– Collaborate intra-campus/intra-specialty
– Create dispersed yet integrated teams
– Expand our research coverage

UCSFSenator Tom Daschle visits UCSF
• Senator Daschle: “Health care in any society looks like a pyramid. The base of the pyramid comprises basic health care delivery involving wellness and prevention. It is the least costly. As we move up the pyramid, the care becomes more sophisticated and technologically advanced. At the peak are the most costly and technologically advanced applications, such as organ transplants, available in modern medicine today.”
• “Every country begins at the base of the pyramid and works its way up until the money runs out. However, in the U.S., we start at the top of the pyramid and work our way down until the money runs out. This is our fundamental problem.”
Oct 3rd 2012
UCSFUCSF Telehealth develops
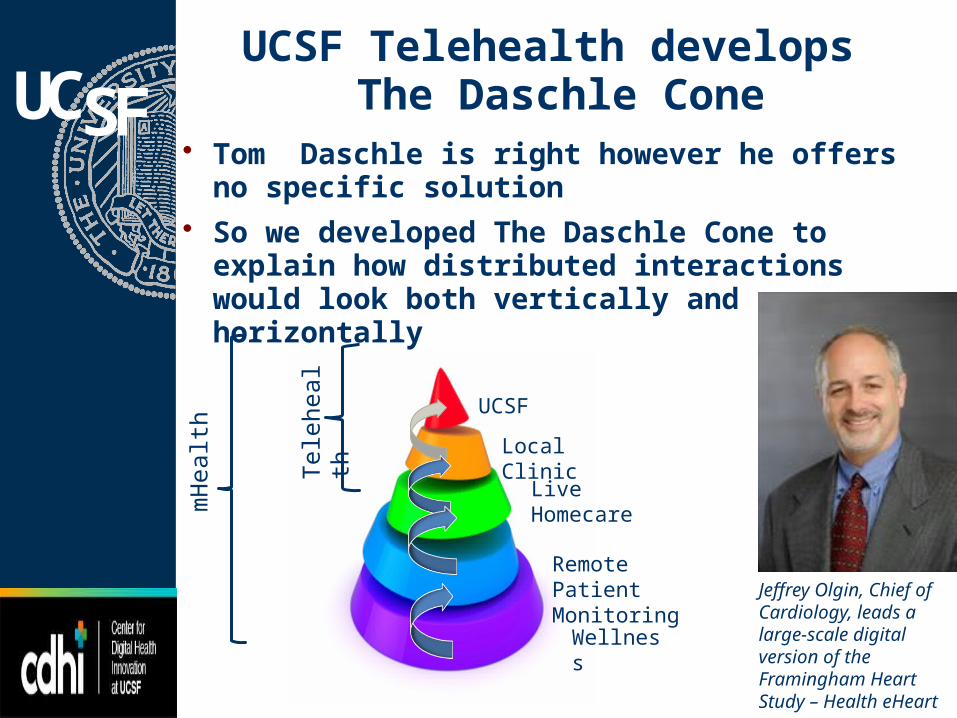
The Daschle Cone• Tom Daschle is right however he offers no specific
solution
• So we developed The Daschle Cone to explain how distributed interactions would look both vertically and horizontally
Jeffrey Olgin, Chief of Cardiology, leads a large-scale digital version of the Framingham Heart Study – Health eHeart
UCSF
Local Clinic
Live Homecare
Remote Patient Monitoring
Wellness
Tele
heal
th
mH
ealth

UCSFA patient’s journey through
the Daschle Cone
UCSF
Local Clinics
Live Homecare
Remote Patient Monitoring
Wellness
Pro-Active
In Patient Specialized Care and Education
Tracking conditions
TriageTracking issues
Follow up New NormalConsult
UCSFDr. Mault CMO Qualcomm Life

UCSF

UCSFAgrees with Eric Dishman of Intel

UCSF

UCSF

UCSFHands-on, high touch

UCSF 25X improvement?
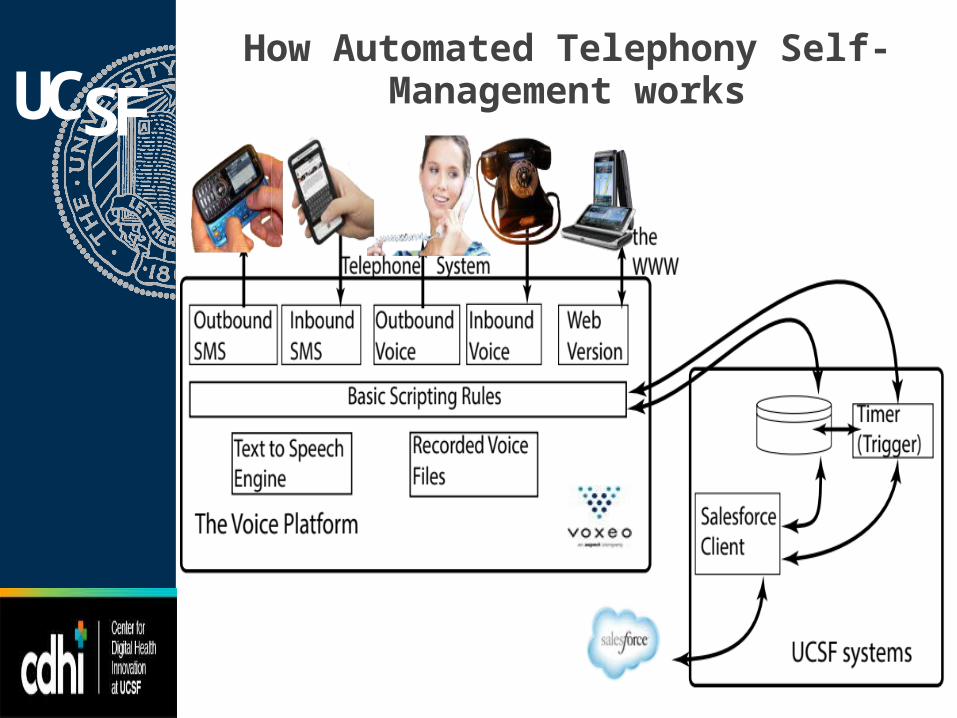
UCSFHow Automated Telephony Self-
Management works

UCSF

UCSF This is why ATSM is important

UCSFThe big picture

UCSF Telehealth Focus Areas
• Mission Bay– Intra-campus consultations (MB, M/L, Mt Z.)
– Intra-campus & inter-facility case conferences
• Telehealth Outreach– Inter-facility consultations
• Kaiser: Heart & Lung Transplant
• Pediatrics: CHO, CHCC Madera, Washington, Mad River, Marin General
• Neurology: Contra Costa
• ED: San Joaquin General

UCSF Beware the hype
• “Physicians at UC Davis began practicing telemedicine in 1992” (http://www.ucdmc.ucdavis.edu/ucdavishealth/issues/spring2014/telemedicine-leading-a-revolution.html)
• So why hasn’t UCD blanketed California?
• Factors:– Technology
– Integration
– Adoption
UCSFAdoption
• Dis-rup-tive: – innovative or groundbreaking;
– troublesome, undisciplined, unmanageable, uncontrollable, obstreperous;
• Normalisation Process Theory (Carl R. May PhD)– Four factors of success:
• Local and/or National Policy sponsor
• Structural/Technical integration
• Enrollment of cohesive, cooperative groups
• Integration at the level of professional knowledge and practice, where clinicians are able to accommodate technology through the development of new procedures and protocols
Related Documents











