Background and rationale Variability in the quality of acute stroke care in hospitals has a direct impact on patient outcomes. The inability to routinely and systematically monitor processes of clinical care impacts on the ability of clinicians and decision- makers to know where to focus efforts to improve care because reliable information on gaps in care is unavailable. Clinical quality registries such as the Australian Stroke Clinical Registry (AuSCR) are important mechanisms for facilitating standardised monitoring to inform improvements to the safety, effectiveness, appropriateness and quality of healthcare. The value of a national clinical quality registry is having a meaningful minimum dataset collected on all eligible patients which can be used to improve patient care. Health services participating in the AuSCR submit their data via a web tool. This is either done directly by reviewing patient medical records and entering this information into the online system, or it is initially captured on a paper- based form whereby the data is later entered into the AuSCR. Hospital staff can either export their data or generate predefined benchmarked live reports of their data. This enables local quality assurance activities and organisational improvements for acute stroke care to be readily undertaken as needed. Data collected includes patient demographic/administrative data (such as age, gender, address, contact details and GP details), processes of clinical care and health outcome (in-hospital outcomes and at 90–180 days) data. Much of the demographic data already exists in hospital patient administration systems and clinical information systems, and a subset of this data is routinely provided to the Victorian Department of Health and Human Services. Without an automated extract from existing hospital information systems, contribution to the AuSCR result is data double-entry, with hospital staff ‘re-keying’ the demographic data into the AuSCR web tool. The VSCN Registry Initiative project for stroke In 2014, recognising that Victorian health services required sustainable and efficient systems to support data collection for the purpose of monitoring the quality of patient care, the Victorian Stroke Clinical Network (VSCN) successfully applied for funding from the Innovation, EHealth and Technology Fund coordinated by the then Department of Health’s Office of the Chief Information Officer. A grant of $450,000 was awarded for 2015 to help health services establish or improve implementation of enhanced technological solutions to the AuSCR data collection processes. An additional $200,000 was made available from within the department to augment the potential outcomes of this innovation project. The ultimate objective was to reduce the amount of manual data entry required in the AuSCR by creating tailored solutions to ‘pull’ demographic, clinical (such as stroke type) or in-hospital outcome (such as discharge destination) data from existing hospital databases that could be reliably uploaded into the AuSCR. Once in an appropriate format, clinician time could then be used to input any outstanding data not captured in the existing hospital databases. This process would reduce duplication of data collection or two-step procedures needed for data capture and submission. Other anticipated benefits include improved data completeness and accuracy. Since input is occurring in real time it becomes part of usual clinical processes and a further advantage is that the data can be used for other purposes (including discharge summaries and GP letters), which will encourage more sites to participate in the AuSCR. Technology solutions to encourage participation in the Australian Stroke Clinical Registry Methods Health services responded to an expression of interest whereby they submitted a proposal for funding a technology solution for improved data capture and importing of data into the AuSCR. Priority was given to health services not currently participating in the AuSCR and to those with higher numbers of patients admitted with acute stroke (> 100 per year). All submissions required involvement of health service IT staff, as well as clinical staff. Consideration was given to solutions being created for different patient administration systems to ensure experience and solutions could then be shared with other hospitals using these same systems for further rollout. The VSCN established a selection panel that reported to the program steering committee. The selection panel initially individually assessed the submissions and subsequently collectively weighed each application against key selection criteria. The selected sites were provided program support to oversee the development of the local hospital electronic data collection systems. These systems should: • automatically extract demographic and contact variables from hospital patient information management systems • enable live entry of clinical variables measuring quality of stroke care • provide the ability to export the data in the correct format for upload into the AuSCR. A project planning workshop involving clinical and technology staff was provided to successful sites. All sites were represented and participants were encouraged to share ideas. The aim of the workshop was to ensure all projects would meet achievable outcomes and that the objectives were understood. Support was provided from the AuSCR office throughout the process. To ensure learnings and resources from the various developments and projects were shared across Victoria, all sites were requested to present at a workshop for sites interested in applying for a second round of funding and at a national conference. Results Six hospitals collectively managing close to 3,000 stroke admissions annually were awarded funds and began their projects in 2015. Only one of these sites was already contributing data to the AuSCR. All hospitals have started sending automated extracts to the AuSCR. A further four hospitals will begin to develop automation solutions in July 2016. Hospital Automation developed Description A Cerner Millennium power form • Cerner Millennium power form developed • Data capture is performed in a clinical area via desktop or laptop • AuSCR screens are auto-populated with demographic data received from the patient administration system • Transmission of the data to AuSCR is triggered monthly B BOSSnet e-form • A dynamic e-form accessible from the clinical information system (BOSSnet) developed • Data capture form is accessed by clinical staff logging onto the CIS from a clinical area via tablet or desktop • Data captured in a ‘real time’ capacity at the patient bedside • e-form is auto-populated with some relevant administrative data from the patient information system • Prompts stroke clinical data collection throughout the patient journey in BOSSnet C Mobile app • A device agnostic mobile app developed • App accessible via a tablet or other mobile device enabling real-time data capture during stroke unit ward rounds • Automated import of demographic, clinical and diagnostic information developed • A minor subset of this data (enough to identify the patient) auto-populates the mobile app D Filemaker Pro Data Base • Purpose-built Filemaker Pro Data Base accessible via a tablet from a patient’s bedside • The database is auto-populated with demographic data and selected clinical information from the hospital’s patient administration system (PAS) • A clinical nurse enters the AuSCR-specific fields that are not auto-populated E Bespoke data feed • The health service used its patient management system to capture many of the AuSCR data fields, with the remaining AuSCR-specific data entered manually • Manual data capture is performed in a clinical area via desktop or laptop • A data extract from the PAS is made available to the stroke nurse (the primary collector of AuSCR data) in report format F Mobile app and emerging systems assessment forms • AuSCR-specific screens developed within the Emerging Health Systems Clinical Information System to capture AuSCR data • Data capture is performed via a tablet using a mobile app or standard PC/ laptop where these devices are at bedside locations • The AuSCR screens are auto-populated with demographics received from the PAS and pre-existing clinical data in Emerging Health. To receive this publication in an accessible format phone (03) 9096 1771, using the National Relay Service 13 36 77 if required, or email <[email protected]>. Authorised and published by the Victorian Government, 1 Treasury Place, Melbourne. © State of Victoria, Department of Health and Human Services, July 2016 (1606018) PARAMEDIC AMBULANC E Stroke patient arrives at hospital Department of Health and Human Services Victorian Admitted Episodes Dataset (Length of Stay, Discharge Destination) Clerical data entry % of Health services not participating in AuSCR % of Health services participating in AuSCR Stroke specific clinical data entry Generic data set Generic export AS IS scenario SINGLE SITE PERSPECTIVE STATE WIDE PERSPECTIVE Patient Information Management System Stroke patient arrives at hospital Department of Health and Human Services Department of Health and Human Services Biannual State wide and site specific reports VSCN support for system wide quality initiatives Clerical data entry Clinician data entry Automated data transfer % of Health services not participating in AuSCR % of Health services participating in AuSCR Stroke specific data Patient Information Management System TO BE scenario SINGLE SITE PERSPECTIVE STATE WIDE PERSPECTIVE PARAMEDIC AMBULANC E Sonia Denisenko,* 1 Paulette Kelly, 1 Dominique Cadilhac, 2,3 Brenda Grabsch, 2 Benjamin Clissold, 4 Anna Burgess, 1 Peter Hand 1 Feedback from health services participating in this initiative has been universally positive, with one health service summing up the time efficiency and quality improvements as: ‘This tool makes it quicker to load and enter information. The real-time capability should ensure our data is more accurate … it was more that we missed patients who were 1. under a different team with a stroke (especially in-hospital stroke); 2. we did not provide consult; 3. nor were they transferred to our team. These patients will enter our list after coding because they are recognised electronically.’ Heather Smith, Barwon Health Conclusion The VSCN Registry Initiative project for stroke has strategically enabled Victorian acute care hospitals to develop locally appropriate technology solutions to reduce their data collection efforts and support enhanced participation in the AuSCR. Many have chosen to develop solutions accessible from mobile devices for data capture at the bedside. This initiative is producing new technology solutions that will lead to more complete clinical quality data that can be used to reliably monitor and improve patient care. The Stroke Clinical registry mobile app is accessed by the stroke liaison nurse and stroke services team members via a tablet or other mobile device enabling real-time data capture during stroke unit ward rounds. A dynamic e-form accessible from the clinical information system (BOSSnet) to enable capture of the AuSCR specific data fields. References 1. Department of Health and Human Services, Melbourne, Victoria 2. Stroke Division, Florey Institute of Neuroscience and Mental Health, Heidelberg, Victoria 3. Department of Medicine, School of Clinical Sciences, Monash University, Clayton, Victoria 4. Barwon Health, Geelong, Victoria Data that can be extracted from the patient information systems Data that needs to be entered by clinicians (sample only) • name • date of birth • gender • ethnic/Aboriginal status • address • telephone number • contact details of next of kin or health contact person • Medicare number • hospital identification number • name of the hospital • type of stroke • medical treatment and care in hospital • complications, if any • living arrangements after discharge from hospital. Items highlighted in bold indicate which items may be automatically uploaded from the patient information systems. 1606018_Technology solutions to encourage participation in the Australian Stroke Clinical Registry AO poster V1.indd 1 4/07/2016 2:56 pm

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Background and rationaleVariability in the quality of acute stroke care in hospitals has a direct impact
on patient outcomes. The inability to routinely and systematically monitor
processes of clinical care impacts on the ability of clinicians and decision-
makers to know where to focus efforts to improve care because reliable
information on gaps in care is unavailable. Clinical quality registries such as
the Australian Stroke Clinical Registry (AuSCR) are important mechanisms
for facilitating standardised monitoring to inform improvements to the safety,
effectiveness, appropriateness and quality of healthcare. The value of a
national clinical quality registry is having a meaningful minimum dataset
collected on all eligible patients which can be used to improve patient care.
Health services participating in the AuSCR submit their data via a web tool.
This is either done directly by reviewing patient medical records and entering
this information into the online system, or it is initially captured on a paper-
based form whereby the data is later entered into the AuSCR. Hospital staff
can either export their data or generate predefined benchmarked live reports
of their data. This enables local quality assurance activities and organisational
improvements for acute stroke care to be readily undertaken as needed. Data
collected includes patient demographic/administrative data (such as age,
gender, address, contact details and GP details), processes of clinical care
and health outcome (in-hospital outcomes and at 90–180 days) data. Much
of the demographic data already exists in hospital patient administration
systems and clinical information systems, and a subset of this data is routinely
provided to the Victorian Department of Health and Human Services. Without
an automated extract from existing hospital information systems, contribution
to the AuSCR result is data double-entry, with hospital staff ‘re-keying’ the
demographic data into the AuSCR web tool.
The VSCN Registry Initiative project for strokeIn 2014, recognising that Victorian health services required sustainable and
efficient systems to support data collection for the purpose of monitoring
the quality of patient care, the Victorian Stroke Clinical Network (VSCN)
successfully applied for funding from the Innovation, EHealth and Technology
Fund coordinated by the then Department of Health’s Office of the Chief
Information Officer. A grant of $450,000 was awarded for 2015 to help health
services establish or improve implementation of enhanced technological
solutions to the AuSCR data collection processes. An additional $200,000
was made available from within the department to augment the potential
outcomes of this innovation project.
The ultimate objective was to reduce the amount of manual data entry
required in the AuSCR by creating tailored solutions to ‘pull’ demographic,
clinical (such as stroke type) or in-hospital outcome (such as discharge
destination) data from existing hospital databases that could be reliably
uploaded into the AuSCR. Once in an appropriate format, clinician time could
then be used to input any outstanding data not captured in the existing
hospital databases. This process would reduce duplication of data collection
or two-step procedures needed for data capture and submission. Other
anticipated benefits include improved data completeness and accuracy. Since
input is occurring in real time it becomes part of usual clinical processes and
a further advantage is that the data can be used for other purposes (including
discharge summaries and GP letters), which will encourage more sites to
participate in the AuSCR.
Technology solutions to encourage participation in the Australian Stroke Clinical Registry
MethodsHealth services responded to an expression of interest whereby they
submitted a proposal for funding a technology solution for improved
data capture and importing of data into the AuSCR. Priority was given to
health services not currently participating in the AuSCR and to those with
higher numbers of patients admitted with acute stroke (> 100 per year). All
submissions required involvement of health service IT staff, as well as clinical
staff. Consideration was given to solutions being created for different patient
administration systems to ensure experience and solutions could then be
shared with other hospitals using these same systems for further rollout.
The VSCN established a selection panel that reported to the program steering
committee. The selection panel initially individually assessed the submissions
and subsequently collectively weighed each application against key selection
criteria. The selected sites were provided program support to oversee the
development of the local hospital electronic data collection systems. These
systems should:
• automatically extract demographic and contact variables from hospital
patient information management systems
• enable live entry of clinical variables measuring quality of stroke care
• provide the ability to export the data in the correct format for upload into
the AuSCR.
A project planning workshop involving clinical and technology staff was provided
to successful sites. All sites were represented and participants were encouraged
to share ideas. The aim of the workshop was to ensure all projects would meet
achievable outcomes and that the objectives were understood. Support was
provided from the AuSCR office throughout the process. To ensure learnings
and resources from the various developments and projects were shared across
Victoria, all sites were requested to present at a workshop for sites interested in
applying for a second round of funding and at a national conference.
ResultsSix hospitals collectively managing close to 3,000 stroke admissions annually
were awarded funds and began their projects in 2015. Only one of these sites
was already contributing data to the AuSCR. All hospitals have started sending
automated extracts to the AuSCR. A further four hospitals will begin to develop
automation solutions in July 2016.
HospitalAutomation developed
Description
A Cerner Millennium power form
• Cerner Millennium power form developed
• Data capture is performed in a clinical area via desktop or laptop
• AuSCR screens are auto-populated with demographic data received from the patient administration system
• Transmission of the data to AuSCR is triggered monthly
B BOSSnet e-form • A dynamic e-form accessible from the clinical information system (BOSSnet) developed
• Data capture form is accessed by clinical staff logging onto the CIS from a clinical area via tablet or desktop
• Data captured in a ‘real time’ capacity at the patient bedside
• e-form is auto-populated with some relevant administrative data from the patient information system
• Prompts stroke clinical data collection throughout the patient journey in BOSSnet
C Mobile app • A device agnostic mobile app developed
• App accessible via a tablet or other mobile device enabling real-time data capture during stroke unit ward rounds
• Automated import of demographic, clinical and diagnostic information developed
• A minor subset of this data (enough to identify the patient) auto-populates the mobile app
D Filemaker Pro Data Base
• Purpose-built Filemaker Pro Data Base accessible via a tablet from a patient’s bedside
• The database is auto-populated with demographic data and selected clinical information from the hospital’s patient administration system (PAS)
• A clinical nurse enters the AuSCR-specific fields that are not auto-populated
E Bespoke data feed • The health service used its patient management system to capture many of the AuSCR data fields, with the remaining AuSCR-specific data entered manually
• Manual data capture is performed in a clinical area via desktop or laptop
• A data extract from the PAS is made available to the stroke nurse (the primary collector of AuSCR data) in report format
F Mobile app and emerging systems assessment forms
• AuSCR-specific screens developed within the Emerging Health Systems Clinical Information System to capture AuSCR data
• Data capture is performed via a tablet using a mobile app or standard PC/laptop where these devices are at bedside locations
• The AuSCR screens are auto-populated with demographics received from the PAS and pre-existing clinical data in Emerging Health.
To receive this publication in an accessible format phone (03) 9096 1771, using the National Relay Service 13 36 77 if required, or email <[email protected]>.
Authorised and published by the Victorian Government, 1 Treasury Place, Melbourne.
© State of Victoria, Department of Health and Human Services, July 2016 (1606018)
PARAMEDIC
AMBULANCE
Stroke patientarrives at hospital Department
of Healthand Human
Services
Victorian AdmittedEpisodes Dataset
(Length of Stay,Discharge Destination)
Clerical data entry
% of Health servicesnot participating inAuSCR
% of Health servicesparticipating inAuSCR
Stroke specificclinical dataentry
Genericdata set
Genericexport
AS IS scenarioSINGLE SITE PERSPECTIVE
STATE WIDE PERSPECTIVE
PatientInformation
ManagementSystem
Stroke patientarrives at hospital
Departmentof Health
and HumanServices
Departmentof Health
and HumanServices
Biannual State wideand site specificreports
VSCNsupport forsystem widequalityinitiatives
Clerical data entry
Clinician data entry
Automated datatransfer
% of Health services not participating in AuSCR
% of Health servicesparticipating in AuSCR
Stroke specificdata
PatientInformation
ManagementSystem
TO BE scenario SINGLE SITE PERSPECTIVE
STATE WIDE PERSPECTIVE
PARAMEDIC
AMBULANCE
Sonia Denisenko,*1 Paulette Kelly,1 Dominique Cadilhac,2,3 Brenda Grabsch,2 Benjamin Clissold,4 Anna Burgess,1 Peter Hand1
Feedback from health services participating in this initiative has been
universally positive, with one health service summing up the time efficiency
and quality improvements as:
‘This tool makes it quicker to load and enter information. The real-time capability should ensure our data is more accurate … it was more that we missed patients who were 1. under a different team with a stroke (especially in-hospital stroke); 2. we did not provide consult; 3. nor were they transferred to our team. These patients will enter our list after coding because they are recognised electronically.’
Heather Smith, Barwon Health
ConclusionThe VSCN Registry Initiative project for stroke has strategically enabled
Victorian acute care hospitals to develop locally appropriate technology
solutions to reduce their data collection efforts and support enhanced
participation in the AuSCR. Many have chosen to develop solutions accessible
from mobile devices for data capture at the bedside. This initiative is
producing new technology solutions that will lead to more complete clinical
quality data that can be used to reliably monitor and improve patient care.
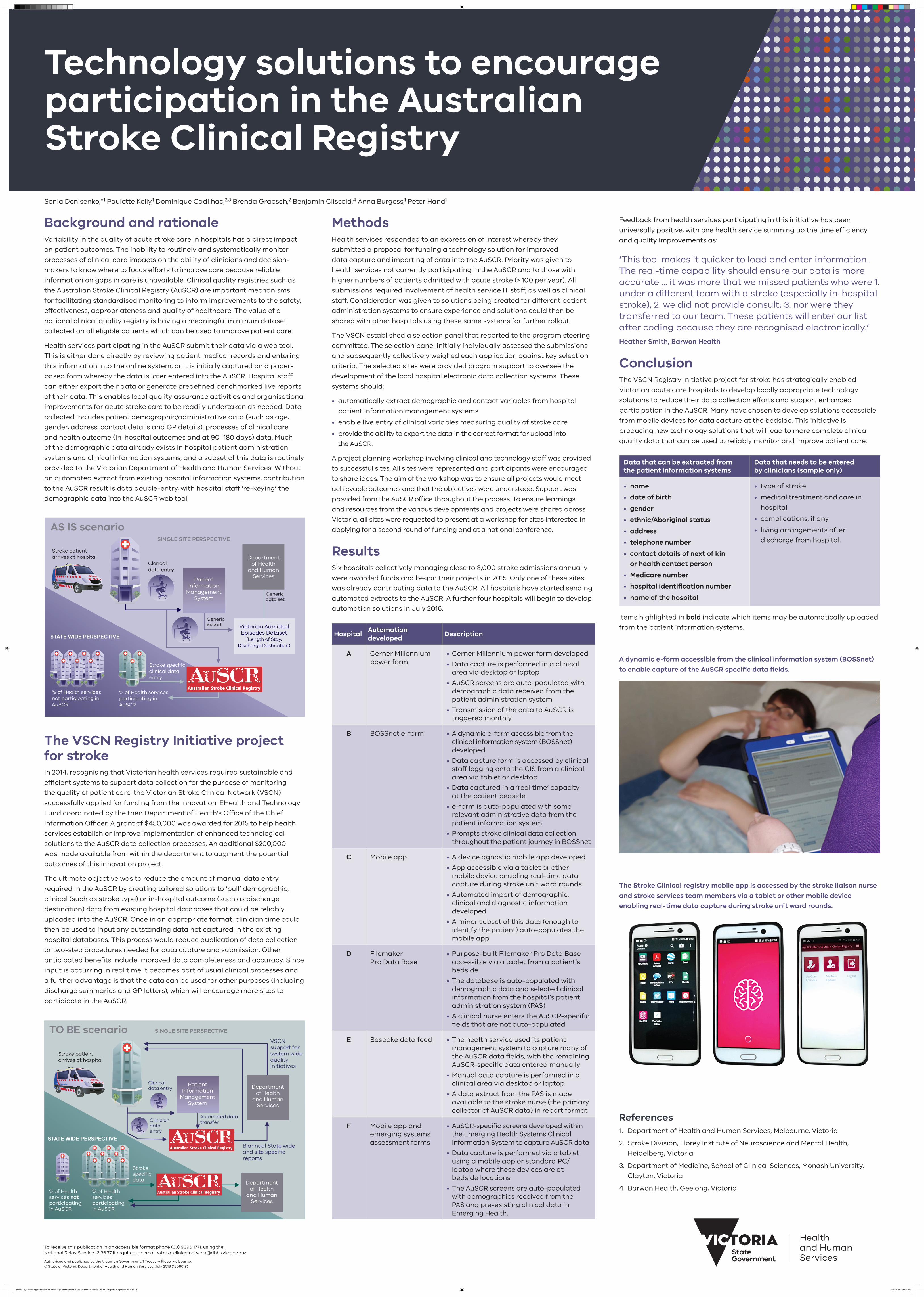
The Stroke Clinical registry mobile app is accessed by the stroke liaison nurse
and stroke services team members via a tablet or other mobile device
enabling real-time data capture during stroke unit ward rounds.
A dynamic e-form accessible from the clinical information system (BOSSnet)
to enable capture of the AuSCR specific data fields.
References1. Department of Health and Human Services, Melbourne, Victoria
2. Stroke Division, Florey Institute of Neuroscience and Mental Health,
Heidelberg, Victoria
3. Department of Medicine, School of Clinical Sciences, Monash University,
Clayton, Victoria
4. Barwon Health, Geelong, Victoria
Data that can be extracted from the patient information systems
Data that needs to be entered by clinicians (sample only)
• name
• date of birth
• gender
• ethnic/Aboriginal status
• address
• telephone number
• contact details of next of kin
or health contact person
• Medicare number
• hospital identification number
• name of the hospital
• type of stroke
• medical treatment and care in
hospital
• complications, if any
• living arrangements after
discharge from hospital.
Items highlighted in bold indicate which items may be automatically uploaded
from the patient information systems.
1606018_Technology solutions to encourage participation in the Australian Stroke Clinical Registry AO poster V1.indd 1 4/07/2016 2:56 pm
Related Documents











