ORIGINAL PAPER Tc-99m sestamibi single photon emission computed tomography for guiding percutaneous coronary intervention in patients with multivessel disease: a comparison with quantitative coronary angiography and fractional flow reserve Stefan Fo ¨rster Johannes Rieber Christopher U ¨ bleis Mayo Weiss Peter Bartenstein Paul Cumming Volker Klauss Marcus Hacker Received: 14 April 2009 / Accepted: 1 September 2009 / Published online: 16 September 2009 Ó Springer Science+Business Media, B.V. 2009 Abstract To evaluate the accuracy of myocardial perfusion SPECT (MPI) in the detection and allocation of vessel specific perfusion defects (PD) using standard distribution territories in a routine clinical procedure of patients with multivessel disease (MVD). Combined quantitative coronary angiography and fractional flow reserve (QCA/FFR) measurements were used as inva- sive reference standard. 216 vessels in 72 MVD patients (67 ± 10 years, 28 female) were investigated using MPI and QCA. FFR of 93 vessels with interme- diate stenoses was determined. MPI detected signifi- cant stenoses according to QCA/FFR findings with a sensitivity of 85%. However, vessel-based evaluation using standard myocardial distribution territories delivered a sensitivity of only 62% (28 MPI? out of 45 (QCA/FFR)? findings), with specificity, PPV and NPV of 90, 62 and 90%. 7/17 false positive and 7/17 false negative findings (41%) could be attributed to incorrect allocation of reversible PD to their respective coronary arteries. 6/17 (35%) perfusion territories were classified as false negative when additional fixed PD were present. MPI had reasonable sensitivity for the detection of significant coronary artery disease in patients with multivessel disease. However, sensitivity decreased markedly, when the significance of each individual stenosis was evaluated using standard myocardial supplying territories. In this setting, 41% of false negative and false positive MPI findings resulted from incorrect allocation of reversible perfu- sion defects to their determining supplying vessel. Keywords Myocardial perfusion SPECT Á Fractional flow reserve Á Multivessel disease Á Percutaneous coronary intervention Á Coronary angiography Introduction Based on an extensive body of data, myocardial perfusion single photon emission tomography (MPI) is widely used for risk stratification and assessment of both ischemia and viability in patients with coronary artery disease (CAD) [4]. However, given that MPI is an imaging technique measuring flow enhancement in S. Fo ¨rster Á C. U ¨ bleis Á M. Weiss Á P. Bartenstein Á P. Cumming Á M. Hacker Department of Nuclear Medicine, University of Munich, Munich, Germany J. Rieber Á V. Klauss Department of Cardiology, Medizinische Poliklinik- Innenstadt, University of Munich, Munich, Germany M. Hacker (&) Klinik und Poliklinik fu ¨r Nuklearmedizin der LMU, Marchioninistr. 15, 81377 Mu ¨nchen, Germany e-mail: [email protected] 123 Int J Cardiovasc Imaging (2010) 26:203–213 DOI 10.1007/s10554-009-9510-x

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL PAPER
Tc-99m sestamibi single photon emission computedtomography for guiding percutaneous coronary interventionin patients with multivessel disease: a comparisonwith quantitative coronary angiographyand fractional flow reserve
Stefan Forster Æ Johannes Rieber Æ Christopher Ubleis ÆMayo Weiss Æ Peter Bartenstein Æ Paul Cumming ÆVolker Klauss Æ Marcus Hacker
Received: 14 April 2009 / Accepted: 1 September 2009 / Published online: 16 September 2009
� Springer Science+Business Media, B.V. 2009
Abstract To evaluate the accuracy of myocardial
perfusion SPECT (MPI) in the detection and allocation
of vessel specific perfusion defects (PD) using standard
distribution territories in a routine clinical procedure of
patients with multivessel disease (MVD). Combined
quantitative coronary angiography and fractional flow
reserve (QCA/FFR) measurements were used as inva-
sive reference standard. 216 vessels in 72 MVD
patients (67 ± 10 years, 28 female) were investigated
using MPI and QCA. FFR of 93 vessels with interme-
diate stenoses was determined. MPI detected signifi-
cant stenoses according to QCA/FFR findings with a
sensitivity of 85%. However, vessel-based evaluation
using standard myocardial distribution territories
delivered a sensitivity of only 62% (28 MPI? out of
45 (QCA/FFR)? findings), with specificity, PPV and
NPV of 90, 62 and 90%. 7/17 false positive and 7/17
false negative findings (41%) could be attributed to
incorrect allocation of reversible PD to their respective
coronary arteries. 6/17 (35%) perfusion territories
were classified as false negative when additional fixed
PD were present. MPI had reasonable sensitivity for
the detection of significant coronary artery disease in
patients with multivessel disease. However, sensitivity
decreased markedly, when the significance of each
individual stenosis was evaluated using standard
myocardial supplying territories. In this setting, 41%
of false negative and false positive MPI findings
resulted from incorrect allocation of reversible perfu-
sion defects to their determining supplying vessel.
Keywords Myocardial perfusion SPECT �Fractional flow reserve � Multivessel disease �Percutaneous coronary intervention �Coronary angiography
Introduction
Based on an extensive body of data, myocardial
perfusion single photon emission tomography (MPI)
is widely used for risk stratification and assessment of
both ischemia and viability in patients with coronary
artery disease (CAD) [4]. However, given that MPI is
an imaging technique measuring flow enhancement in
S. Forster � C. Ubleis � M. Weiss � P. Bartenstein �P. Cumming � M. Hacker
Department of Nuclear Medicine, University of Munich,
Munich, Germany
J. Rieber � V. Klauss
Department of Cardiology, Medizinische Poliklinik-
Innenstadt, University of Munich, Munich, Germany
M. Hacker (&)
Klinik und Poliklinik fur Nuklearmedizin der LMU,
Marchioninistr. 15, 81377 Munchen, Germany
e-mail: [email protected]
123
Int J Cardiovasc Imaging (2010) 26:203–213
DOI 10.1007/s10554-009-9510-x

diverse myocardial beds based on changes in relative
radiotracer uptake [26], there arise distinct limitations
in its use in the evaluation of patients with multivessel
disease (MVD) [7, 10]. In particular, the allocation of
perfusion defects to their determining coronary arter-
ies or specific coronary lesions—a precondition for
performing appropriate percutaneous coronary inter-
vention (PCI) [15, 16, 36]—is frequently hampered
when morphological correlation is not available [7,
10, 35, 41, 23, 40]. Additionally, the detection of
ischemic myocardial regions might be compromised
in patients with fixed perfusion defects due to the
presence of myocardial scaring or chronic hypo
perfusion, as has been shown in a recent study [32].
In a clinical cardiology setting, two-dimensional
quantitative coronary angiography (QCA), although
often underestimating or overestimating a lesion‘s
functional severity, is still the standard technique for
guiding PCI in patients with multivessel CAD [14, 39].
Initial results from the Fractional Flow Reserve
versus Angiography for Multivessel Evaluation
(FAME) study, however, reported in 1,005 patients
with multivessel CAD a significant reduction of the
composite end point of death, non-fatal myocardial
infarction (MI), and repeated revascularization during
a 1 year follow-up, when additional measurements of
fractional flow reserve (FFR) were performed [38].
FFR is defined as the ratio of maximum achievable
coronary blood flow in a stenotic coronary artery
relative to the maximal blood flow in the same vessel
in the absence of all epicardial obstructions [11].
Initial studies compared FFR with MPI as a reference
standard in patients both with single-vessel and
multivessel disease [5, 7, 8, 12, 21, 25, 29, 43]. On
the basis of various clinical studies, an FFR cut-off
value\0.75 was established for the detection of flow-
limiting or functionally significant coronary artery
stenoses. Recent publications confirmed the validity
of the cut-off value of 0.75 also in comparison to
H215O positron emission tomography blood flow
measurements in patients with chronic MI [24], as
well as after revascularization therapy and during
long-term follow up [3, 31].
The aim of the present study was to evaluate MPI
for the detection and allocation of flow-limiting
stenoses in patients with multivessel disease, com-
pared to an invasive reference standard of QCA/FFR.
We hypothesized that the accuracy of MPI is limited
for vessel-based evaluation using standard myocardial
distribution territories due to the uncertainty of
allocating perfusion defects to particular coronary
arteries without knowledge of individual coronary
vascular anatomy.
Methods
Patient Selection
Patients were included in the study if they had
multivessel coronary artery disease, which was
defined as coronary artery stenoses of at least 50%
of the vessel diameter in at least two of the three
major epicardial coronary arteries. Patients who had
had a myocardial infarction were included if the
infarction had occurred at least 10 days before study
inclusion. Patients who had undergone previous PCI
were also included in the study. Patients who had
angiographically significant left main coronary artery
disease, previous coronary-artery bypass surgery, or
patients who were pregnant were excluded.
QCA with FFR measurements and MPI were
performed in all patients.
The study was approved by the local ethics
committee and written informed consent was obtained
from all patients.
Quantitative Coronary Angiography (QCA) and
FFR measurements
All patients were instructed to abstain from caffeine
and chocolate for 12 h prior to catheterization. At
least two orthogonal views were obtained, and the
projection showing the most severe narrowing was
used for quantitative coronary measurements (Philips
DCI, The Netherlands). Using the guiding catheter as
a scaling device, measurements of the minimal lumen
diameter as well as proximal and distal reference
diameters were made [36].
FFR was measured in all vessels with intermediate
stenoses, i.e. in the range C50 and B75%. Vessels with
severe ([75%) or low-grade stenoses (\50%) were not
investigated for pressure measurements. After crossing
the target lesion with a dedicated sensor-tipped 0.014-
inch angioplasty guidewire (WaveWireWaveMap,
Volcano Therapeutics, Rancho Cordova, CA, USA;
or PressureWire, Radi Medical Uppsala, Sweden)
while under angiographic guidance, the pressure
204 Int J Cardiovasc Imaging (2010) 26:203–213
123

sensor was positioned beyond the stenosis in the distal
portion of the artery. Phasic and mean aortic pressure
as well as phasic and mean coronary pressure distal to
the stenoses were then measured under maximum
coronary hyperemia, which was induced by intrave-
nous administration of 140 lg/kg min-1 of adenosine
(Adrecar, Sanofi, Munich, Germany). FFR was defined
as the ratio of mean poststenotic pressure and mean
aortic pressure measured during maximum hyperemia.
Significance of a stenosis was classified by dicho-
tomous criteria (significant or non-significant), accord-
ing to the composite of the QCA and FFR findings. A
lesion was classified as significant if severe stenosis
was detected in QCA, or if FFR measurement yielded a
value of\0.75. Occluded vessels or those who could
not be assessed by FFR due to subtotal occlusions were
also rated as significant. A lesion was classified as non-
significant if QCA showed no abnormality, stenosis
\50%, or if FFR was C0.75.
Myocardial Perfusion SPECT (MPI)
When appropriate, physical or pharmacological stress/
rest MPI was performed according to a one-day
protocol with Tc-99m sestamibi, as follows; before
the termination of the stress test, a dose of 4 MBq/kg of
Tc-99m sestamibi (at least 300 MBq) was adminis-
tered intravenously. For the subsequent resting study, a
dose of 10 MBq/kg of Tc-99m sestamibi (at least
700 MBq) was injected. If systolic blood pressure was
greater than 120 mm Hg, 0.8 mg nitroglycerine was
sublingually administered to the patients before injec-
tion of the radiopharmaceutical for the rest image.
Image acquisition was performed with a triple-
headed camera system (Philips [formerly Picker]
Prism 3000 XP, Cleveland, Ohio). Possible attenuation
artefacts were corrected by applying an attenuation
correction based on a simultaneous transmission
measurement with 153Gd (STEP�), with 360� rotation
in continuous mode, or alternately by performing gated
SPECT acquisition for wall motion analyses, as
described previously [19]. Images were reconstructed
over 360� with 20 slices along the short axis, the long
axis, and the four-chamber view for each study. A
standardized filter (Low Pass 4th power, cut-off-
frequency 0.26) was used. Quantitative analysis of
MPI perfusion studies was carried out using QPS
processing software (Cedars-Sinai Medical Center,
Los Angeles, California).
Image analysis was performed by agreement of two
experienced observers (M.H. and S.F.) blinded to the
results of QCA/FFR, the coronary distribution type, or
the presence of coronary normal variants such as
ramus intermedius, or the location of stenoses. A
commonly used 20 segment model was employed for
division of the left ventricular myocardium images
[6]. Each of the 20 segments was scored according to
the guideline for semiquantitative analysis (‘‘Semi-
quantitative Scoring System: The Fivepoint Model’’:
0 = normal; 1 = mildly reduced—not definitely
abnormal; 2 = moderate reduced—definitely abnor-
mal; 3 = severely reduced; 4 = absent radiotracer
distribution) [1]. Segmental scores were summed for
the three main coronary arteries (LAD, RCA, LCx)
according to standard myocardial perfusion territo-
ries, as described elsewhere [8], resulting in regional
perfusion scores under stress (SSSr, regional Summed
Stress Score) and rest (SRSr, regional Summed Rest
Score) conditions. The difference of SSSr and SRSr
was defined as the regional Summed Difference Score
(SDSr). On the basis of previously published results,
stenoses and their respective supplying territories with
an SDSr C 1 were considered significant, while
stenoses and their respective supplying territories
with an SDSr = 0 were considered as non-significant
[18]. SRSr C 1 was defined as fixed perfusion defect.
Evaluation of the allocation process
In addition to the above territorial mapping, allocation
of ischemic myocardial regions to appropriate target
vessels was evaluated. Wrong allocation was assumed
for the following combinations of disagreement:
(1) MPI suggested ischemia of a target vessel with
non-significant stenosis (\50% or an FFR C
0.75); and at the same time significant stenosis
(between 50 and 75% with an FFR \ 0.75 or
stenosis [ 75%) was present in another vessel,
which (according to standard distribution terri-
tories) did not show ischemia on MPI ((MPI)?/
(QCA/FFR)-).
(2) MPI did not suggest ischemia, but significant
stenosis was nonetheless present in the respec-
tive distribution territory, and at the same time
MPI detected ischemia in another vessel with
non-significant stenosis ((MPI)-/(QCA/
FFR)?)).
Int J Cardiovasc Imaging (2010) 26:203–213 205
123

Statistical analysis
Descriptive analysis for categorical and continuous
parameters was performed using SPSS version 13.0
(SPSS, Chicago, IL, USA). Results are presented as
mean ± standard deviation (SD) and range, unless
stated otherwise. Paired and unpaired t-tests were
used when appropriate. Statistical significance was
tested on the 5% level.
Results
Seventy two consecutive patients (28 female, mean
age 67 ± 10 years) with multivessel disease (32
patients with two- and 40 patients with three-vessel
disease) were eligible for the study.
QCA with FFR measurements and MPI were
performed in each patient within an interval of
13 ± 43 days. QCA/FFR was performed before MPI
in 13 and after MPI in 59 patients.
Ergometric stress was performed in 17 patients,
whereas pharmacological stress or a combined stress
protocol was applied in 55 patients. Patient charac-
teristics are summarized in Table 1.
Quantitative coronary angiography and FFR
measurements
About 216 vessels in 72 patients were investigated
with QCA, morphological characteristics are sum-
marized in Table 2. FFR measurements were per-
formed in 93 vessels with intermediate stenoses, i.e.
C50 and B75%. Here, the FFR values ranged from
0.42 to 1.0, with a mean FFR of 0.78 ± 0.10. There
was a significant difference detected between mean
diameter stenosis of significant lesions compared to
non-significant lesions (71.2 ± 11.5% vs. 34.8 ±
28.7%, P \ 0.001). No correlation was found
between FFR values and degree of angiographic
stenoses (n = 93) ranging between 50 and 75%.
According to QCA, 14 vessels showed severe
stenoses ([75%) and were rated as significant. Ten of
these coronary arteries showed total occlusions, six in
the proximal and four in the distal part of the artery.
However, at least partial collateral filling (Rentrop
grade 2 or higher) was present in seven (70%) of the
occluded vessels. 31 of the 93 intermediate stenoses
showed FFR \0.75, such that overall 45/216 lesions
were rated as significant by definition.
MPI in the detection of significant coronary artery
lesions using standard myocardial distribution
territories
Vessel based evaluation
A total of 216 perfusion territories were analyzed for
MPI (3 territories per patient). 64 territories were
identified as showing abnormal perfusion (any PD),
45 with reversible perfusion defects (SDSr C 1) and
Table 1 Clinical characteristics of study cohort (n = 72)
Clinical parameters
Sex (m/f) 44/28
Age years ± SD 67 ± 8.5
Diabetes mellitus (%) 26 (36)
Hypertension (%) 53 (74)
Hypercholesterolemia (%) 47 (65)
Current smoker (%) 34 (47)
Family predisposition (%) 22 (31)
First-pass LVEFrest % 53 ± 10
2-vessel disease (%) 32 (44)
3-vessel disease (%) 40 (56)
Table 2 Procedural characteristics of significant versus non-
significant lesions as defined by QCA/FFR
Significant
n = 45
Non-significant
n = 171
Morphological characteristics
QCA diameter stenosis % 71.2 ± 11.5** 34.8 ± 28.7
QCA widthprox (mm) 2.8 ± 1.6** 1.8 ± 1.6
QCA widthdist (mm) 2.7 ± 1.3** 1.7 ± 1.5
Functional characteristics
FFR (n = 93) 0.63 ± 0.1** 0.85 ± 0.1
SSSr 4.8 ± 6.6** 1.5 ± 4.0
SRSr 3.1 ± 6.2** 1.0 ± 3.4
SDSr 1.7 ± 2.5** 0.4 ± 1.5
QCA Quantitative coronary angiography, FFR fractional flow
reserve, SSSr (regional) summed stress score, SRSr (regional)
summed rest score, SDSr (regional) summed difference score.
Values are mean ± SD
** P \ 0.001
206 Int J Cardiovasc Imaging (2010) 26:203–213
123
19 with fixed perfusion defect (PD) (SRS C 1). 15
perfusion territories showed a combination of both,
reversible and fixed perfusion defects.
Considering only reversible perfusion defects on
MPI, 28 of 45 perfusion territories were rated
significant by QCA/FFR, while 17 of the 45 territo-
ries were classified as non-significant by QCA/FFR.
On the other hand, 17 of 45 coronary lesions rated as
significant by QCA/FFR showed no reversible per-
fusion defects on MPI. 154 of all 216 vessels showed
no perfusion defects in MPI and were non-significant
in QCA/FFR (‘‘true’’ negatives; see Table 3). In the
detection and allocation of myocardial ischemia by
MPI, sensitivity was 62%, specificity was 90%, ppV
was 62%, npV was 90% and accuracy was 84%.
When the presence of any perfusion defect was
taken into account, 33 of 64 myocardial supplying
territories were rated significant by QCA/FFR and 12
of 45 significant lesions showed neither reversible nor
fixed perfusion defects on MPI (Table 3). This
indicates sensitivity of 73%, specificity of 82%,
ppV of 52%, npV of 92%, and an accuracy of 80%.
Considering only the 93 vessels with intermediate
stenoses (C50 and B75%) with all individually
available FFR measurements, sensitivity was 77%,
specificity was 82%, ppV was 69%, npV was 88%
and accuracy was 81% when reversible perfusion
defects in MPI were evaluated (data not shown in
detail).
Patient based evaluation
For all patients, sensitivity was 79%, specificity was
74%, ppV was 72%, npV was 81% and accuracy was
76%, when only reversible perfusion defects were
considered and sensitivity increased to 85%, while
specificity was 54%, ppV was 61%, npV was 81%
and accuracy was 68%, when any perfusion defect
was rated as pathological (Table 4).
For the subgroup of diabetes mellitus patients,
sensitivity was 70%, specificity was 81%, ppV was
70%, npV was 81% and accuracy was 77%, when
only reversible perfusion defects were considered and
sensitivity increased to 77%, while specificity was
54%, ppV was 63%, npV was 70% and accuracy was
65%, when any perfusion defect was rated as
pathological (Table 5).
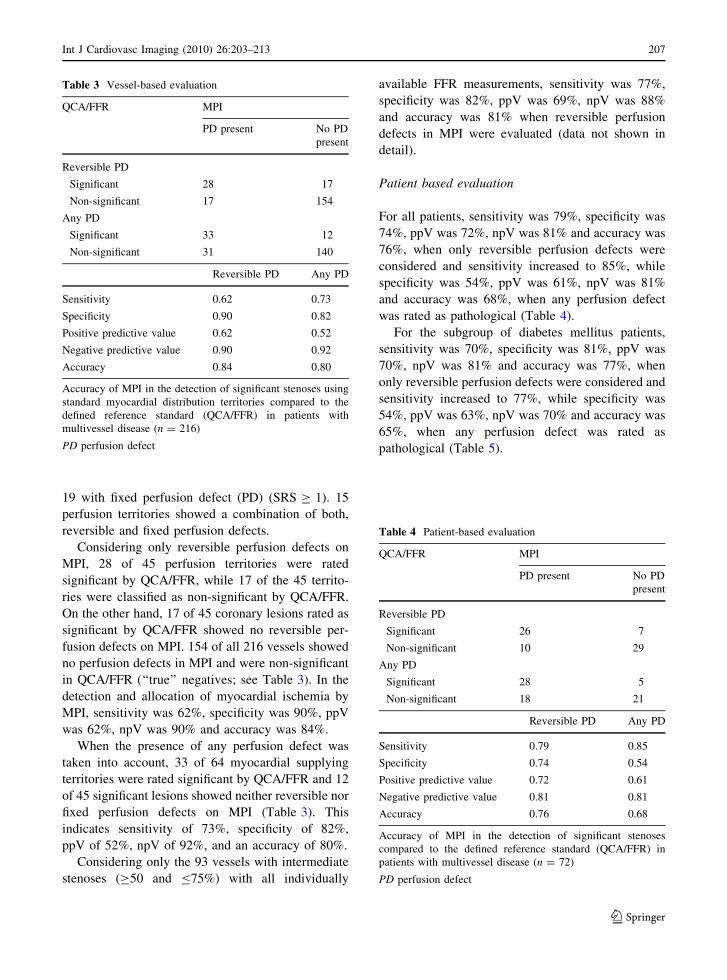
Table 3 Vessel-based evaluation
QCA/FFR MPI
PD present No PD
present
Reversible PD
Significant 28 17
Non-significant 17 154
Any PD
Significant 33 12
Non-significant 31 140
Reversible PD Any PD
Sensitivity 0.62 0.73
Specificity 0.90 0.82
Positive predictive value 0.62 0.52
Negative predictive value 0.90 0.92
Accuracy 0.84 0.80
Accuracy of MPI in the detection of significant stenoses using
standard myocardial distribution territories compared to the
defined reference standard (QCA/FFR) in patients with
multivessel disease (n = 216)
PD perfusion defect
Table 4 Patient-based evaluation
QCA/FFR MPI
PD present No PD
present
Reversible PD
Significant 26 7
Non-significant 10 29
Any PD
Significant 28 5
Non-significant 18 21
Reversible PD Any PD
Sensitivity 0.79 0.85
Specificity 0.74 0.54
Positive predictive value 0.72 0.61
Negative predictive value 0.81 0.81
Accuracy 0.76 0.68
Accuracy of MPI in the detection of significant stenoses
compared to the defined reference standard (QCA/FFR) in
patients with multivessel disease (n = 72)
PD perfusion defect
Int J Cardiovasc Imaging (2010) 26:203–213 207
123

MPI and allocation of reversible perfusion defects
Seven of the 17 patients (41%) without reversible
perfusion defects on MPI, but exhibiting significant
stenosis in QCA/FFR, showed reversible perfusion
defects in an adjacent territory with non-significant
stenosis in the respective supplying vessel ((MPI)-/
(QCA/FFR)? disagreement, Figs. 1, 2). Addition-
ally, six (MPI)-/(QCA/FFR)? findings showed fixed
perfusion defects in the respective myocardial sup-
plying territory and the remaining four (MPI)-/
(QCA/FFR)? were ‘‘true’’ false negatives without
any perfusion defect on MPI. Seven of 17 patients
(29%) with non-significant stenosis in QCA/FFR, but
with reversible perfusion defects on MPI had signif-
icant stenosis in another coronary artery ((MPI)?/
(QCA/FFR)- disagreement). The remaining 10
(MPI)?/(QCA/FFR)- were ‘‘true’’ false positives.
Overall, 14 of 34 (MPI)?/(QCA/FFR)- or (MPI)-/
(QCA/FFR)? findings (41%) occurred due to wrong
allocation of MPI reversible perfusion defects to their
determining and supplying vessel, according to stan-
dard myocardial distribution territories.
Discussion
Numerous studies have shown high overall sensitiv-
ity, up to 90%, for MPI to identify patients with two-
or three vessel disease [9, 28, 30, 42]. Particularly in
these patients, the detection of functionally signifi-
cant coronary artery stenoses is an important
precondition for adequate treatment and improved
outcome. However, as compared to intracoronary
pressure measurements, which are performed directly
in the target vessels, MPI alone has limited capacity
to detect functionally significant stenoses, and to
allocate correctly the perfusion defects to specific
vessels or even coronary lesions in patients with
MVD, as shown in the present study.
The most important result for planning and
guiding individual therapies is the limited utility of
MPI alone for allocating correctly reversible and
fixed perfusion defects to their respective coronary
artery, or even to their determining coronary artery
lesion. Indeed, 41% of our disagreements (41% of
(MPI)-/(QCA/FFR)? and 41% of (MPI)?/(QCA/
FFR)-) resulted from just such allocation problems.
These limitations of MPI are well known and
previously documented in comparison studies
between MPI and invasive coronary angiography
[2] and can be explained by previously published post
mortem analysis, reporting only 50–60% accordance
between standard myocardial perfusion territories and
supplying areas of the three main coronary arteries, a
discrepancy arising from the extensive inter-individ-
ual variability of the coronary tree [20].
However, the diagnostic accuracy of MPI was
rarely investigated using a combined morphological
and functional reference standard, which was recently
shown superior to QCA alone in patients with MVD
[38]. To ensure an objective comparison in the
present study, MPI perfusion defects were systemat-
ically assigned to one of the three main coronary
arteries (RCA, LAD and LCX).
As such, our procedure does not necessarily reflect
clinical routine diagnostics in patients with MVD.
One possible clinical scenario is to determine
whether a demonstrated anatomical abnormality is
causing flow limitation requiring intervention in the
setting of an intermediate or no diagnostic finding on
QCA, especially when revascularization may not be
straightforward for the interventionist like in the
presence of long segment of disease, nearby branches
Table 5 Patient-based evaluation
QCA/FFR MPI
PD present No PD
present
Reversible PD
Significant 7 3
Non-significant 3 13
Any PD
Significant 10 3
Non-significant 6 7
Reversible PD Any PD
Sensitivity 0.70 0.77
Specificity 0.81 0.54
Positive predictive value 0.70 0.63
Negative predictive value 0.81 0.70
Accuracy 0.77 0.65
Accuracy of MPI in the detection of significant stenoses
compared to the defined reference standard (QCA/FFR) in a
subgroup of patients with multivessel disease and diabetes
mellitus (n = 26)
PD perfusion defect
208 Int J Cardiovasc Imaging (2010) 26:203–213
123
or in the presence of poor visualization on QCA, in-
or peri-stent restenosis.
Indeed, specific limitations of the MPI method
without knowledge of patient‘s coronary anatomy
were evident in the present study, even if early
studies have demonstrated how well this method can
demonstrate a culprit lesion or draw attention to one
which may have been initially overlooked at QCA.
In a recent study of 36 patients (88 vessels) suffering
from MVD, Ragosta et al. [32] reported that 36% of all
vascular zones lacking fixed or reversible perfusion
abnormalities on MPI showed either pathological FFR
(\0.75), or total occlusions in QCA. From this
observation, it was concluded that numerous hemody-
namically significant stenoses would be overlooked if
clinical judgment were based only upon MPI. In their
interpretation, most cases of discordance between MPI
and FFR measurements were primarily due to perfu-
sion imaging correctly identifying the most severe
stenosis, but not identifying other zones subtended by
lesser, but still significant, lesions. In seven of 22
patients (32%), MPI was completely normal in all
perfusion territories, despite the occurrence of patho-
logically FFR in one or more territories.
The observed high rate of improper classification
of an individual vascular territory based on MPI using
standard myocardial distribution territories would
lead to errors in management that are clinically
unacceptable. This well known limitation has led to
the proposed use of 3-D image fusion of the coronary
arteries visualized by coronary angiography, with
myocardial perfusion maps [13], an elegant approach
that has not yet found widespread use in routine
diagnostic practice. It has to be emphasized, that
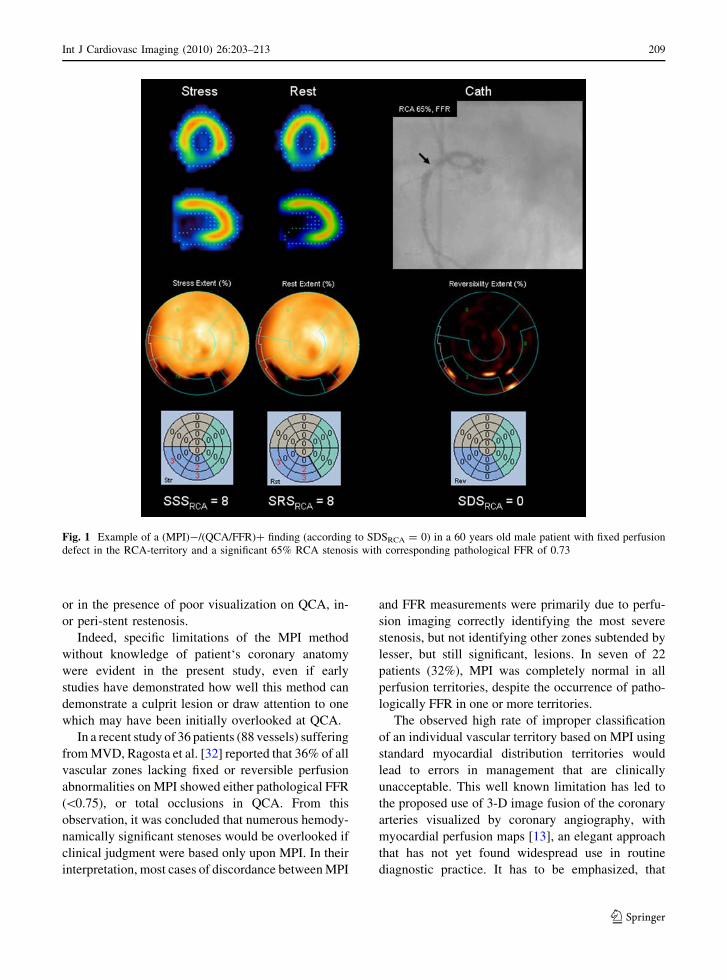
Fig. 1 Example of a (MPI)-/(QCA/FFR)? finding (according to SDSRCA = 0) in a 60 years old male patient with fixed perfusion
defect in the RCA-territory and a significant 65% RCA stenosis with corresponding pathological FFR of 0.73
Int J Cardiovasc Imaging (2010) 26:203–213 209
123
decisions regarding revascularization of specific
arteries in patients with MVD cannot be based on
MPI alone and that there is a need of proper
anatomical information (i.e. one should better rely
on incorporation of the angiogram with adjunctive
use of FFR as appropriate). Certainly, non-invasive
methods combining morphological and functional
imaging strategies using SPECT-CT or PET-CT
hybrid scanners will improve MPI as a tool for the
selection of vessel regions that are candidates for
intervention. There are already promising studies
using hybrid imaging technology [17, 27], which
were able to show improved allocation of perfusion
defects to specific coronary artery lesions and, thus,
potentially will improve therapy planning.
Assessing the diagnostic performance of MPI was
a further aspect in the present study, we found that
4/17 patients with significant stenosis in QCA/FFR
(24%) had no perfusion defect in MPI, reflecting
‘‘true’’ false negative ((MPI)-/(QCA/FFR)?) results.
This reflects a well-known limitation for MPI, which
can be attributed to the occurrence of balanced
ischemia in the absence of valid myocardial reference
areas [22, 41]. A further reason for discrepant results
in which MPI was negative while QCA/FFR positive
in the present study (6/17 patients, 35%), was the
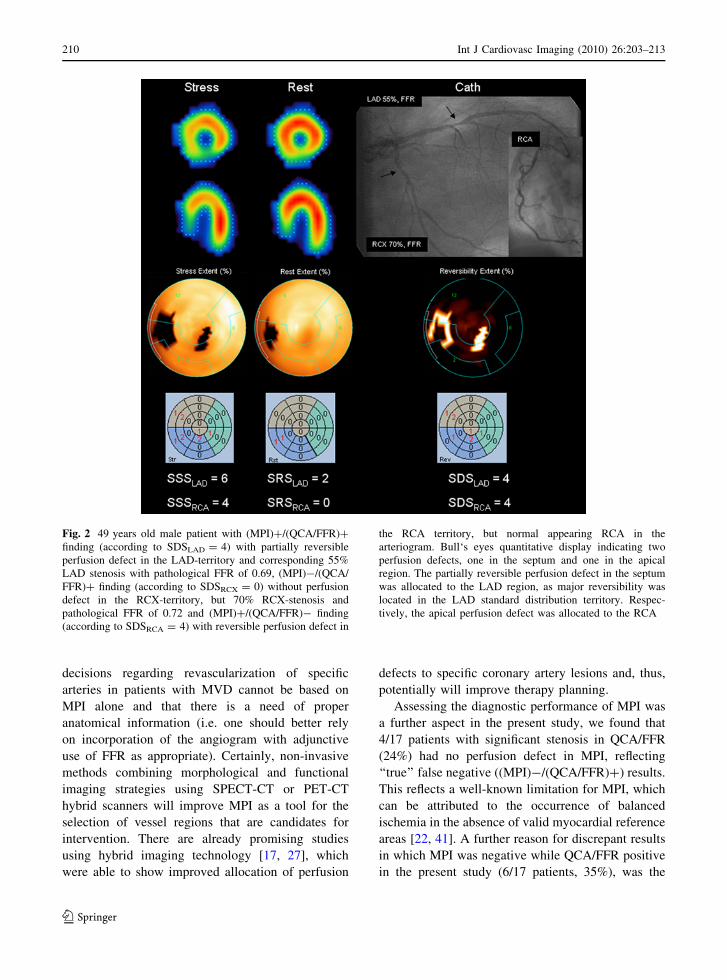
Fig. 2 49 years old male patient with (MPI)?/(QCA/FFR)?
finding (according to SDSLAD = 4) with partially reversible
perfusion defect in the LAD-territory and corresponding 55%
LAD stenosis with pathological FFR of 0.69, (MPI)-/(QCA/
FFR)? finding (according to SDSRCX = 0) without perfusion
defect in the RCX-territory, but 70% RCX-stenosis and
pathological FFR of 0.72 and (MPI)?/(QCA/FFR)- finding
(according to SDSRCA = 4) with reversible perfusion defect in
the RCA territory, but normal appearing RCA in the
arteriogram. Bull‘s eyes quantitative display indicating two
perfusion defects, one in the septum and one in the apical
region. The partially reversible perfusion defect in the septum
was allocated to the LAD region, as major reversibility was
located in the LAD standard distribution territory. Respec-
tively, the apical perfusion defect was allocated to the RCA
210 Int J Cardiovasc Imaging (2010) 26:203–213
123

occasional presence of fixed perfusion defects mask-
ing ischemia, which is also a well-known limitation
of MPI arising from an underestimation of the true
extent of myocardial viability in the standard resting
images [34]; see example Fig. 1. Some of the fixed
perfusion defects might have reflected not MI, but
rather stunned or hibernating myocardium, particu-
larly in this selective patient group with more
advanced stages of disease. For this reason, we
applied nitroglycerin before the tracer injection at
rest, so as to enhance tracer uptake in the ischemic
myocardium compared with that seen in the nonvi-
able and nonischemic myocardium. This approach
has earlier been shown to improve MPI viability
detection [37].
Study limitations
Our study has several limitations. First, FFR mea-
surement was not performed in all three coronary
arteries; therefore, the reference standard consists of a
combination of angiographic diameter stenosis mea-
surements with and without corresponding FFR
values, reflecting an approach already published by
our group [33]. A separate comparison of MPI with
FFR in intermediate stenoses delivered a sensitivity
of 77%, which was in line with previous studies,
confirming that these assumptions were appropriate.
In general, it is at present difficult to control for the
effects of perfusion derived from collateral vessels,
competitive flow, differential ischemia and other
factors [26]. Additionally, functionally relevant ste-
noses \50% as well as intramyocardial vessel
affections and peripheral stenoses, which both are
inaccessible for FFR measurements, could have lead
to false positive MPI findings. However, analysis in
the subgroup of patients with diabetes mellitus (and
therefore higher possibility of microvascular disease)
revealed similar ability for MPI in the detection of
significant stenoses when compared to the whole
patient cohort, such that the rate of microvasculature
related false positives in the current study is deemed
to be low.
Another limitation is presented by the lack of
gated SPECT in all patients, such that regional wall
motion and thickening patterns have not been imple-
mented for optimal validation of MPI for the
identification of significant stenoses.
Conclusion
Myocardial perfusion SPECT had reasonable sensi-
tivity for the detection of significant coronary artery
disease in patients with multivessel disease relative to
quantitative coronary angiography with/without addi-
tional FFR measurements. However, sensitivity
decreased markedly, when the significance of each
individual stenosis was evaluated using standard
myocardial supplying territories. In this setting,
41% of false negative and false positive MPI findings
resulted from incorrect allocation of reversible per-
fusion defects to their determining supplying vessel.
Acknowledgments We are grateful for the support and
superb technical assistance of the staff in the departments of
Nuclear Medicine and Cardiology at the University of Munich.
References
1. (1999) Imaging guidelines for nuclear cardiology proce-
dures, part 2. American Society of Nuclear Cardiology.
J Nucl Cardiol 6(2):G47–84
2. Allman KC, Berry J, Sucharski LA et al (1992) Determi-
nation of extent and location of coronary artery disease in
patients without prior myocardial infarction by thallium-
201 tomography with pharmacologic stress. J Nucl Med
33(12):2067–2073
3. Berger A, Botman KJ, MacCarthy PA et al (2005) Long-
term clinical outcome after fractional flow reserve-guided
percutaneous coronary intervention in patients with mul-
tivessel disease. J Am Coll Cardiol 46(3):438–442
4. Brindis RG, Douglas PS, Hendel RC et al (2005) ACCF/
ASNC appropriateness criteria for single-photon emission
computed tomography myocardial perfusion imaging
(SPECT MPI): a report of the American College of Car-
diology Foundation Quality Strategic Directions Commit-
tee Appropriateness Criteria Working Group and the
American Society of Nuclear Cardiology endorsed by the
American Heart Association. J Am Coll Cardiol
46(8):1587–1605
5. Caymaz O, Fak AS, Tezcan H et al (2000) Correlation of
myocardial fractional flow reserve with thallium-201
SPECT imaging in intermediate-severity coronary artery
lesions. J Invasive Cardiol 12(7):345–350
6. Cerqueira MD, Weissman NJ, Dilsizian V et al (2002)
Standardized myocardial segmentation and nomenclature
for tomographic imaging of the heart: a statement for
healthcare professionals from the Cardiac Imaging Com-
mittee of the Council on Clinical Cardiology of the
American Heart Association. Circulation 105(4):539–542
7. Chamuleau SA, Meuwissen M, Koch KT et al (2002)
Usefulness of fractional flow reserve for risk stratification
of patients with multivessel coronary artery disease and an
intermediate stenosis. Am J Cardiol 89(4):377–380
Int J Cardiovasc Imaging (2010) 26:203–213 211
123
8. Chamuleau SA, Meuwissen M, van Eck-Smit BL et al
(2001) Fractional flow reserve, absolute and relative cor-
onary blood flow velocity reserve in relation to the results
of technetium-99m sestamibi single-photon emission
computed tomography in patients with two-vessel coronary
artery disease. J Am Coll Cardiol 37(5):1316–1322
9. Chamuleau SA, Tio RA, de Cock CC et al (2002) Prog-
nostic value of coronary blood flow velocity and myocar-
dial perfusion in intermediate coronary narrowings and
multivessel disease. J Am Coll Cardiol 39(5):852–858
10. Christian TF, Miller TD, Bailey KR et al (1992) Nonin-
vasive identification of severe coronary artery disease
using exercise tomographic thallium-201 imaging. Am J
Cardiol 70(1):14–20
11. De Bruyne B, Bartunek J, Sys SU et al (1995) Relation
between myocardial fractional flow reserve calculated
from coronary pressure measurements and exercise-
induced myocardial ischemia. Circulation 92(1):39–46
12. De Bruyne B, Pijls NH, Bartunek J et al (2001) Fractional
flow reserve in patients with prior myocardial infarction.
Circulation 104(2):157–162
13. Faber TL, Santana CA, Garcia EV et al (2004) Three-
dimensional fusion of coronary arteries with myocardial
perfusion distributions: clinical validation. J Nucl Med
45(5):745–753
14. Fischer JJ, Samady H, McPherson JA et al (2002) Com-
parison between visual assessment and quantitative angi-
ography versus fractional flow reserve for native coronary
narrowings of moderate severity. Am J Cardiol 90(3):210–
215
15. Gibbons RJ, Abrams J, Chatterjee K et al (2003) ACC/
AHA 2002 guideline update for the management of
patients with chronic stable angina—summary article: a
report of the American College of Cardiology/American
Heart Association Task Force on Practice Guidelines
(Committee on the Management of Patients With Chronic
Stable Angina). Circulation 107(1):149–158
16. Gibbons RJ, Chatterjee K, Daley J et al (1999) ACC/AHA/
ACP-ASIM guidelines for the management of patients with
chronic stable angina: a report of the American College of
Cardiology/American Heart Association Task Force on
practice guidelines (Committee on management of patients
with chronic stable angina). J Am Coll Cardiol
33(7):2092–2197
17. Hacker M, Jakobs T, Hack N et al (2007) Combined use of
64-slice computed tomography angiography and gated
myocardial perfusion SPECT for the detection of func-
tionally relevant coronary artery stenoses. First results in a
clinical setting concerning patients with stable angina.
Nuklearmedizin 46(1):29–35
18. Hacker M, Rieber J, Schmid R et al (2005) Comparison of
Tc-99m sestamibi SPECT with fractional flow reserve in
patients with intermediate coronary artery stenoses. J Nucl
Cardiol 12(6):645–654
19. Hacker M, Tausig A, Romuller B et al (2005) Dobutamine
myocardial scintigraphy for the prediction of cardiac
events after heart transplantation. Nucl Med Commun
26(7):607–612
20. Kalbfleisch H, Hort W (1977) Quantitative study on the
size of coronary artery supplying areas postmortem. Am
Heart J 94(2):183–188
21. Leesar MA, Abdul-Baki T, Akkus NI et al (2003) Use of
fractional flow reserve versus stress perfusion scintigraphy
after unstable angina. Effect on duration of hospitalization,
cost, procedural characteristics, and clinical outcome.
J Am Coll Cardiol 41(7):1115–1121
22. Lima RS, Watson DD, Goode AR et al (2003) Incremental
value of combined perfusion and function over perfusion
alone by gated SPECT myocardial perfusion imaging for
detection of severe three-vessel coronary artery disease.
J Am Coll Cardiol 42(1):64–70
23. Mahmarian JJ, Mahmarian AC, Marks GF et al (1995)
Role of adenosine thallium-201 tomography for defining
long-term risk in patients after acute myocardial infarction.
J Am Coll Cardiol 25(6):1333–1340
24. Marques KM, Knaapen P, Boellaard R et al (2007)
Hyperaemic microvascular resistance is not increased in
viable myocardium after chronic myocardial infarction.
Eur Heart J 28(19):2320–2325
25. Matsuo H, Watanabe S, Kadosaki T et al (2002) Validation
of collateral fractional flow reserve by myocardial perfu-
sion imaging. Circulation 105(9):1060–1065
26. Miller DD (2002) Coronary flow studies for risk stratifi-
cation in multivessel disease. A physiologic bridge too far?
J Am Coll Cardiol 39(5):859–863
27. Namdar M, Hany TF, Koepfli P et al (2005) Integrated
PET/CT for the assessment of coronary artery disease: a
feasibility study. J Nucl Med 46(6):930–935
28. Pijls NH, De Bruyne B, Bech GJ et al (2000) Coronary
pressure measurement to assess the hemodynamic signifi-
cance of serial stenoses within one coronary artery: vali-
dation in humans. Circulation 102(19):2371–2377
29. Pijls NH, De Bruyne B, Peels K et al (1996) Measurement
of fractional flow reserve to assess the functional severity
of coronary-artery stenoses. N Engl J Med 334(26):1703–
1708
30. Pijls NH, Van Gelder B, Van der Voort P et al (1995)
Fractional flow reserve. A useful index to evaluate the
influence of an epicardial coronary stenosis on myocardial
blood flow. Circulation 92(11):3183–3193
31. Pijls NH, van Schaardenburgh P, Manoharan G et al (2007)
Percutaneous coronary intervention of functionally non-
significant stenosis: 5-year follow-up of the DEFER study.
J Am Coll Cardiol 49(21):2105–2111
32. Ragosta M, Bishop AH, Lipson LC et al (2007) Compar-
ison between angiography and fractional flow reserve
versus single-photon emission computed tomographic
myocardial perfusion imaging for determining lesion sig-
nificance in patients with multivessel coronary disease. Am
J Cardiol 99(7):896–902
33. Rieber J, Huber A, Erhard I et al (2006) Cardiac magnetic
resonance perfusion imaging for the functional assessment
of coronary artery disease: a comparison with coronary
angiography and fractional flow reserve. Eur Heart J
27(12):1465–1471
34. Sciagra R (2003) Nitrates and viability: a durable affair.
J Nucl Med 44(5):752–755
35. Shaw LJ, Peterson ED, Kesler K et al (1996) A meta-
analysis of predischarge risk stratification after acute
myocardial infarction with stress electrocardiographic,
myocardial perfusion, and ventricular function imaging.
Am J Cardiol 78(12):1327–1337
212 Int J Cardiovasc Imaging (2010) 26:203–213
123

36. Smith SC Jr, Dove JT, Jacobs AK et al (2001) ACC/AHA
guidelines for percutaneous coronary intervention (revision
of the 1993 PTCA guidelines)-executive summary: a report
of the American College of Cardiology/American Heart
Association task force on practice guidelines (Committee
to revise the 1993 guidelines for percutaneous transluminal
coronary angioplasty) endorsed by the Society for Cardiac
Angiography and Interventions. Circulation 103(24):3019–
3041
37. Tadamura E, Mamede M, Kubo S et al (2003) The effect of
nitroglycerin on myocardial blood flow in various seg-
ments characterized by rest-redistribution thallium SPECT.
J Nucl Med 44(5):745–751
38. Tonino PA, De Bruyne B, Pijls NH et al (2009) Fractional
flow reserve versus angiography for guiding percutaneous
coronary intervention. N Engl J Med 360(3):213–224
39. Topol EJ, Nissen SE (1995) Our preoccupation with cor-
onary luminology. The dissociation between clinical and
angiographic findings in ischemic heart disease. Circula-
tion 92(8):2333–2342
40. Travin MI, Dessouki A, Cameron T et al (1995) Use of
exercise technetium-99m sestamibi SPECT imaging to
detect residual ischemia and for risk stratification after
acute myocardial infarction. Am J Cardiol 75(10):665–669
41. Travin MI, Katz MS, Moulton AW et al (2000) Accuracy
of dipyridamole SPECT imaging in identifying individual
coronary stenoses and multivessel disease in women versus
men. J Nucl Cardiol 7(3):213–220
42. Usui Y, Chikamori T, Yanagisawa H et al (2003) Reli-
ability of pressure-derived myocardial fractional flow
reserve in assessing coronary artery stenosis in patients
with previous myocardial infarction. Am J Cardiol
92(6):699–702
43. Yanagisawa H, Chikamori T, Tanaka N et al (2002) Cor-
relation between thallium-201 myocardial perfusion
defects and the functional severity of coronary artery ste-
nosis as assessed by pressure-derived myocardial fractional
flow reserve. Circ J 66(12):1105–1109
Int J Cardiovasc Imaging (2010) 26:203–213 213
123
Related Documents





![[PPT]PCI VS CABG JOURNAL REVIEW REVIEW/PCI VS CABG.ppsx · Web viewCABRI TRIAL Objective: RCT CABG VS PCI N- 1054 Conclusion: In patients with multivessel coronary disease and chronic](https://static.cupdf.com/doc/110x72/5b054daa7f8b9a3c378eb5d6/pptpci-vs-cabg-journal-reviewpci-vs-cabgppsxweb-viewcabri-trial-objective-rct.jpg)





