TBI & Glasgow Coma Scale Mandy Freeman March 2010

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

TBI & Glasgow Coma
Scale
Mandy Freeman
March 2010

Aims
Highlight types of traumatic brain injuries (TBI)
Highlight the importance of Glasgow Coma
Scale
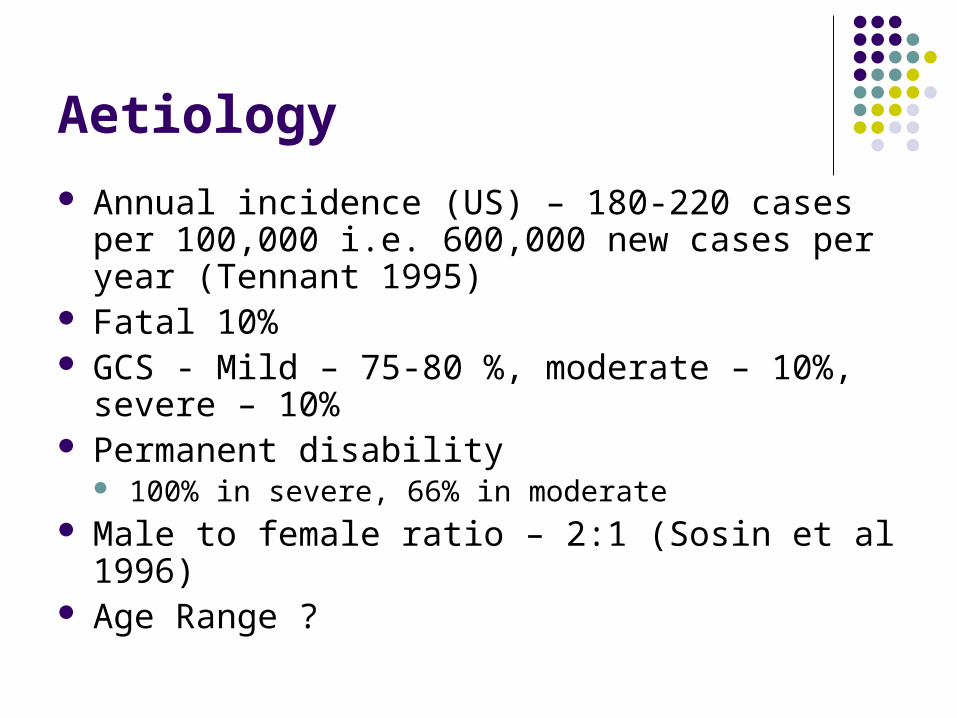
Aetiology Annual incidence (US) – 180-220 cases per
100,000 i.e. 600,000 new cases per year (Tennant 1995)
Fatal 10% GCS - Mild – 75-80 %, moderate – 10%,
severe – 10% Permanent disability
100% in severe, 66% in moderate Male to female ratio – 2:1 (Sosin et al 1996) Age Range ?

Most common causes??
(Royal College of Surgeons of England 2007)

Pathophysiology
Skull – rigid, inelastic container = Vol (Brain) + Vol (CSF) + Vol (Blood) = 80% + 10% + 10% Monro-Kellie Doctrine – states that total
intracranial volume is fixed because of the inelastic nature of the skull
Intracranial compliance – change in the pressure due to the change in volume
Cushings Triad -Sign of ICP
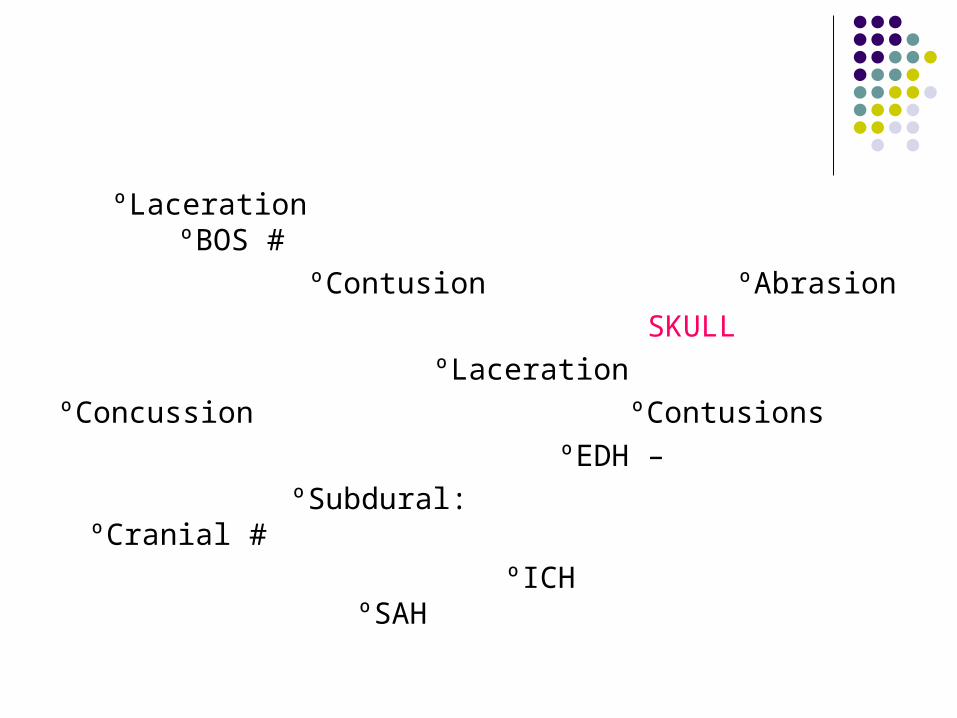
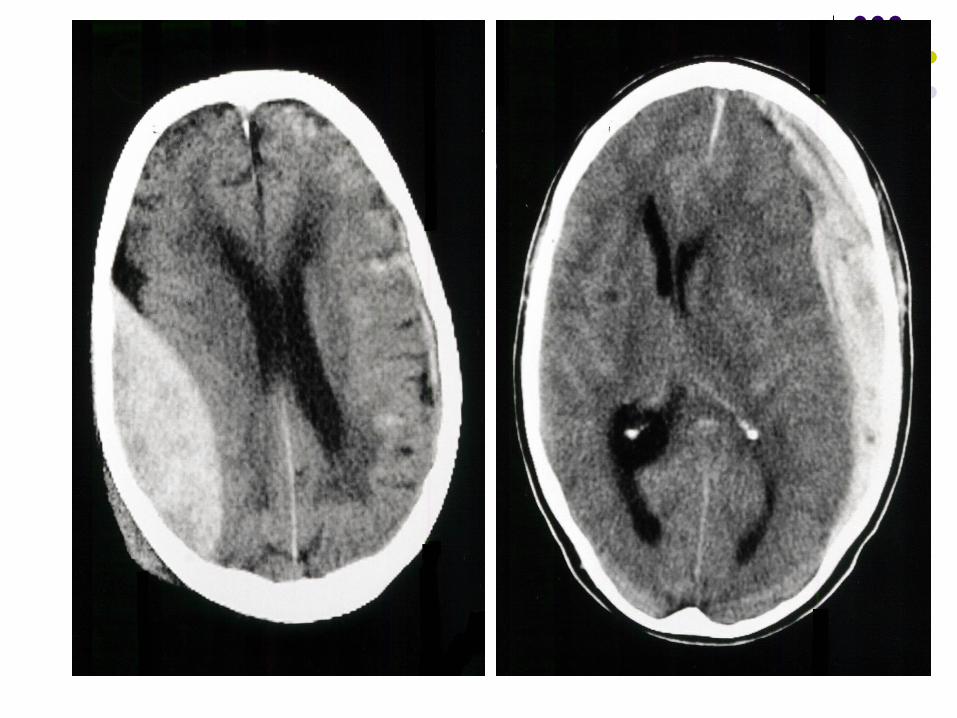
ºLaceration ºBOS # ºContusion ºAbrasion SKULL ºLacerationºConcussion ºContusions ºEDH – ºSubdural: ºCranial # ºICH ºSAH

EDH
Extradural hematomas Between inner table of skull and dura Biconvex Arterial injury – enlarge rapidly Venous in around 10% Classic example – temporal EDH by fracture
through course of middle meningeal artery Lucid interval before deteriorating If tackled early – good prognosis for isolated
lesion

SDH
Subdural hematoma Between dura and brain Outer edge – convex, inner – concave Not limited by suture lines Usually venous – bridging veins (cortex to
dura) In elderly brain more common due to
cerebral atrophy

Management
Mild Head Injury 3% will progress to more serious injuries Concussion – majority have concussion –
physiological injury to brain without structural alteration
Monitored Would require neurological observations When discharged instructed to seek medical
attention if severe headache, persistent nausea and vomiting, seizure,
confusion, unusual behaviour, watery discharge from ear or nose

Contusions
Most common and evident in minor and major head injuries
Can present with GCS 15/15 worsening over day 3 to 5
Strict fluid balance 2 litre restriction
4hrly Observations

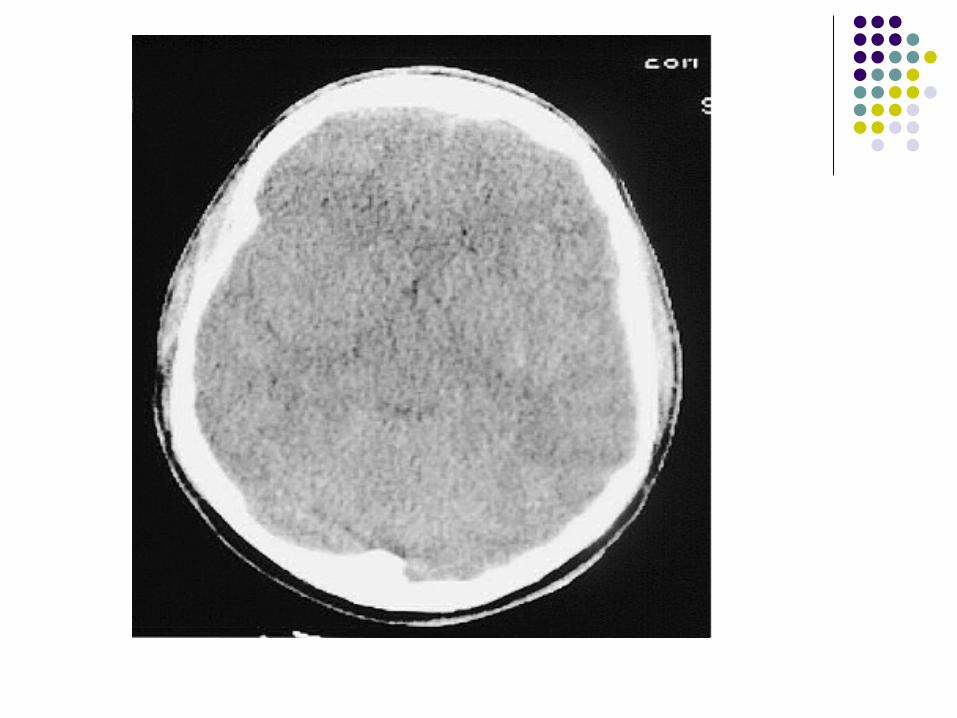
Diffuse Axonal Injury
Neuronal injury in subcortical gray matter or brain stem due to rotation or deceleration injury
Patients with severely depressed level of consciousness
CT – no significant injury ICP – within reference range Prognosis - poor

GCS
Severity of Head Injury Mild head injury – GCS 15 - 13 Moderate head injury – GCS 12 – 9 Severe head injury – GCS 8 and below

Developed by Jennett and Teasdale (1974)
Assess level of consciousness 3 categories
Eye opening – E Motor response – M Verbal response – V

Glasgow Coma Scale
Eye opening4 – spontaneously3 – to verbal
commands2 – to pain1 – No response
Best Motor responseBest Motor response6 – obeys commands6 – obeys commands5 – Localizes to pain5 – Localizes to pain4 – flexion withdrawal4 – flexion withdrawal3 – abnormal flexion3 – abnormal flexion2 – extension 2 – extension 1 – no response1 – no response
Best Verbal response5 – oriented and converses
4 – disoriented and converses
3 – inappropriate words
2 – incomprehensible sounds
1 – No response
Best – 15
Worst - 3

Poor Outcome
Age older than 60 years GCS of <5 Presence of fixed pupil Prolonged hypotension or hypoxia Presence of surgical treatable mass
lesion



NAI Children
Child with head injury – NAI must be excluded
HI is most common cause of morbidity and mortality in NAI
Multiple bilateral skull fractures, subdural hematomas of different ages, cortical contusions and shear injuries, cerebral ischaemia, retinal haemorrhages
Dunn L, Henry J, Beard D. Social deprivation and adult head injury: a
national study. (2003) J Neurol Neurosurg Psychiatry. 74:1060–1064 National Institute for Clinical Excellence. (2007) Triage, assessment
Investigation and early management of head injury in infants, children and adults Clinical Guidelines CG56. NICE;
Swann IJ, Walker A. (2001) Who cares for the patient with head injury now? Emerg Med.18:352–357.
Sosin DM, Sniezek JE, Thurman DJ. (1991) Incidence of mild and moderate brain injury in the United States. Brain Injury. 1996;10:47–54.
Thornhill S, Teasdale G, Murray GD, McEwen J, Yoy CW, Penny KI. Disability in young people and adults one year after head injury: prospective
cohort study. BMJ. 2000;320:1631–5

Tennant A. Epidemiology of head injury. (1995) In: Chamberlain MA, Neumann VC, Tennant A, editor. Traumatic Brain Injury Rehabilitation: Services, treatments and outcomes. London: Chapman & Hall
Related Documents