TREATMENT GUIDELINES TUBERCULOSIS Dr. Aswini Kumar Mohapatra Professor and Head Dept. of Pulmonary Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TREATMENT GUIDELINES TUBERCULOSIS
Dr. Aswini Kumar Mohapatra Professor and Head Dept. of Pulmonary Medicine
AIMS OF TREATMENT –
1. To cure the patient of TB2. To prevent death from active TB3. To prevent death from relapse of TB4. To decrease transmission of TB to others5. To prevent development of acquired drug
resistance
INITIAL / INTENSIVE PHASE (2 months)
CONTINUATION PHASE (4 - 6MONTHS)
NEW CASES
SMEAR POSITIVE SMEAR NEGATIVE
1.Tuberculosis suspect- Any person who presents with symptoms
or signs suggestive of TB2.Definite case of TB- Patient with M.TB complex identified from
a clinical specimen, either by culture or by a newer method such as molecular line probe assay
One or more initial sputum smear examinations positive for AFB is also considered to be a ‘definite’ case
3. Case of TB- A definite case of TB or one in which a
health worker has diagnosed TB and has decided to treat the patient with a full course of TB treatment
Cases of TB also classified according to the- a. anatomical site of the disease b. bacteriological results c. history of previous treatment d. HIV status of the patient
4. Smear negative PTB cases- Smear negative PTB cases should
either:A. Sputum smear negative but culture
positive for M. tuberculosis
OR
B. meet the following diagnostic criteria : decision by a clinician to treat with a full
course of anti TB therapy; and
radiographic abnormalities consistent with active pulmonary TB and either:
-laboratory or strong clinical evidence of HIV infection
or:
- if HIV negative and no improvement in response to a course of broad spectrum antibiotics
A. FIRST LINE DRUGS:-
Isoniazid (H) Rifampicin (R) Pyrazinamide (Z) Streptomycin (S) Ethambutol (E)
B. SECOND LINE DRUGS:-
Para-amino salicylic Acid Ethionamide Cycloserine Kanamycin / Amikacin / Capreomycin Macrolides Fluroquinolones
Second line ATT are used in the treatment of MDRTB
INHRifampicinPyrazinamideStreptomycinEthambutolThioacetazone
1.Group1- first line oral agents pyrazinamide ethambutol rifabutine2.Group2- injectable agents kanamycin amikacin capreomycin streptomycin
3.Group3- fluroquinolones levofloxacin moxifloxacin ofloxacin4.Group 4-Oral bacteriostatic 2nd line drugs PAS cycloserine ethionamide protionamide5.Group 5-unclear role clofazimine linezolid clarithromycin thioacetazone amoxy –clavulinic acid high dose of INH
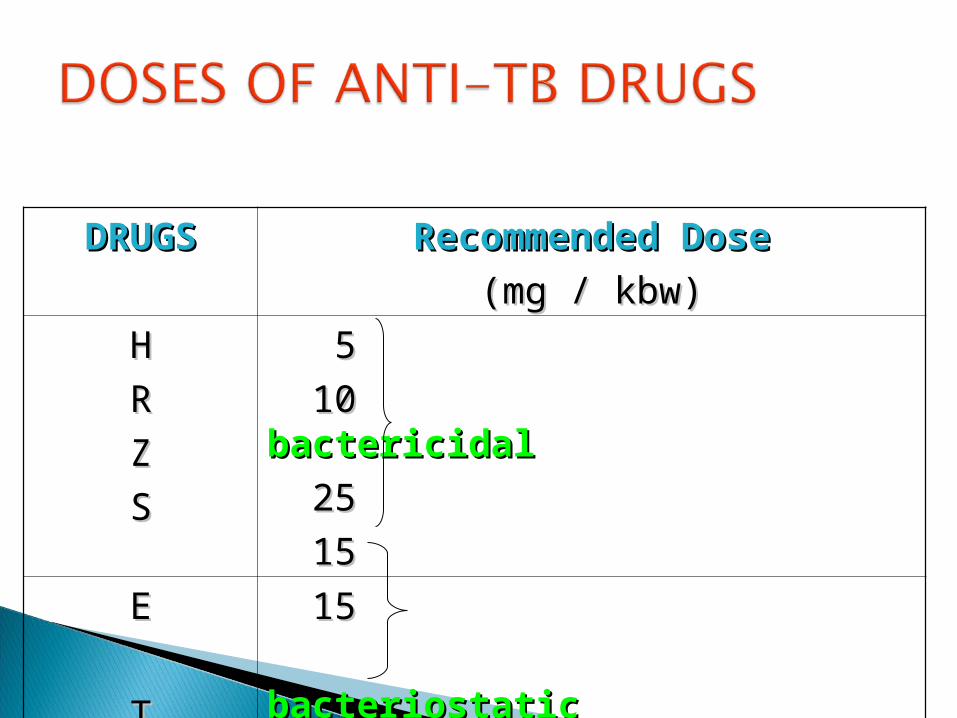
DRUGSDRUGS Recommended DoseRecommended Dose
(mg / kbw)(mg / kbw)
HH
RR
ZZ
SS
55
10 10 bactericidalbactericidal
2525
1515
EE
TT
15 15
bacteriostaticbacteriostatic
33
Three properties:
1. Bactericidal activity2. Sterilizing activity3. Ability to prevent resistance (bacteriostatic activity)
INH and Rifampicin-
Most powerful bactericidal drugs
active against all population of TB bacilli
Rifampicin -most potent sterilizing drug
Pyrazinamide - bactericidal- active only in acidic
environment Streptomycin -
Bactericidal- against rapidly multiplying bacilli
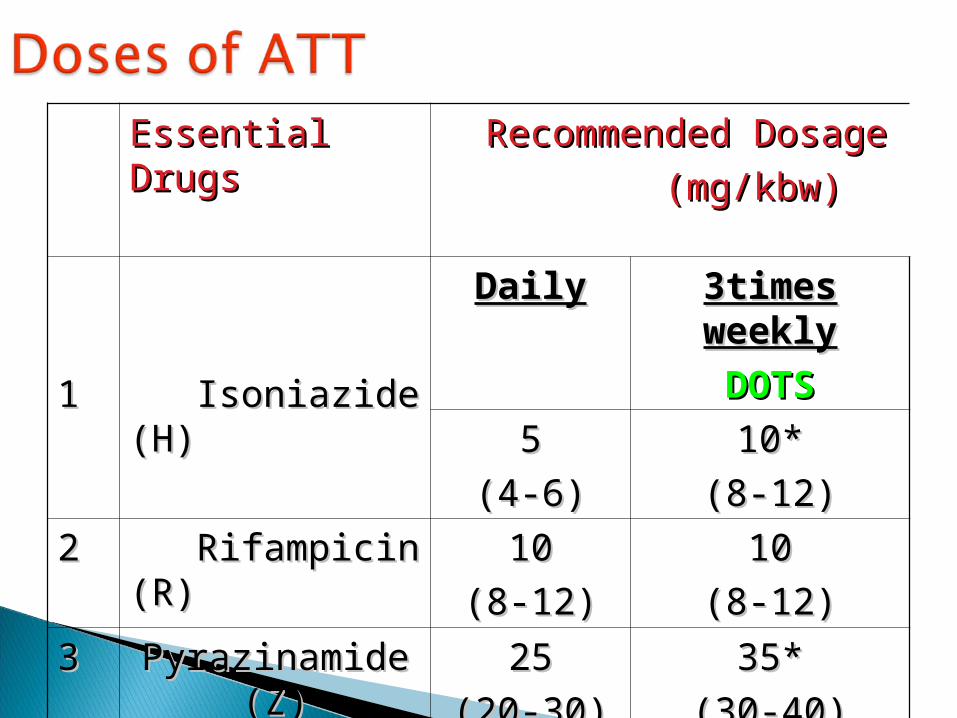
Essential Essential DrugsDrugs
Recommended Dosage Recommended Dosage
(mg/kbw) (mg/kbw)
11 Isoniazide Isoniazide (H)(H)
DailyDaily 3times 3times weeklyweekly
DOTSDOTS
55
(4-6)(4-6)10*10*
(8-12)(8-12)
22 Rifampicin Rifampicin (R)(R)
1010
(8-12)(8-12)1010
(8-12)(8-12)
33 Pyrazinamide Pyrazinamide (Z)(Z)
2525
(20-30)(20-30)35*35*
(30-40)(30-40)
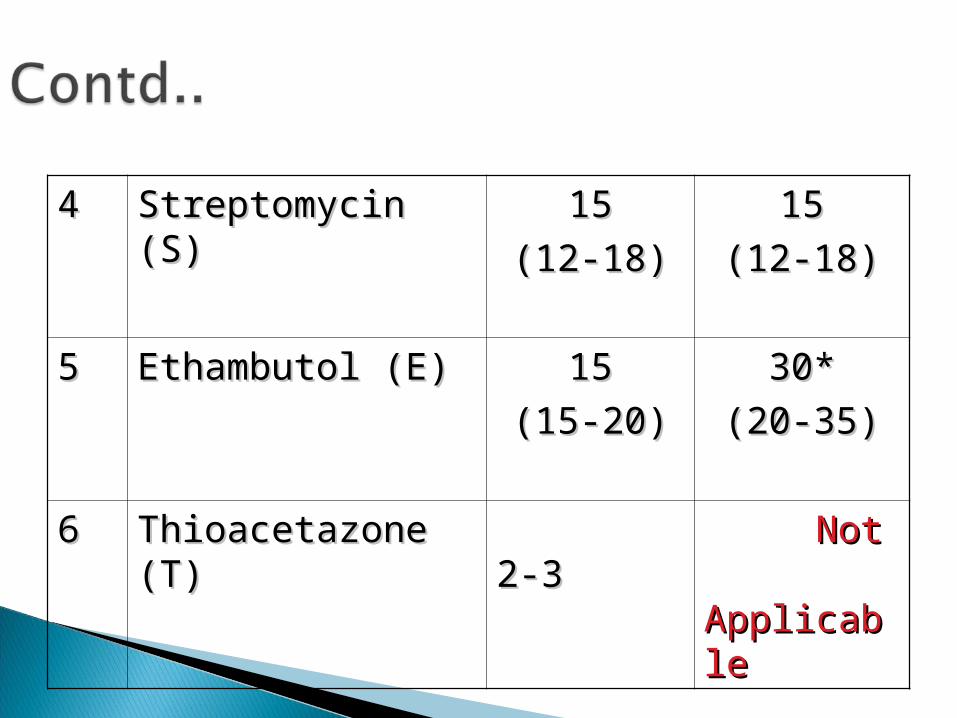
44 Streptomycin (S)Streptomycin (S) 1515
(12-18)(12-18)1515
(12-18)(12-18)
55 Ethambutol (E)Ethambutol (E) 1515
(15-20)(15-20)30*30*
(20-35)(20-35)
66 Thioacetazone (T)Thioacetazone (T) 2-32-3 Not Not ApplicablApplicablee
1. NEW CASE- A patient who has never had treatment for TB OR
Who has taken ATT <1 month
2. REPALSE-A patient previously treated for TB declared cured / treatment completed
Subsequently diagnosed with bacteriologically positive (smear or culture) tuberculosis
3. TREATMENT FAILURE- A patient who while on treatment,
remained or became again smear positive five months or later after commencing treatment
ORInitially smear negative before starting
treatment and became smear positive after the second month of treatment
4. DEFAULTER- A patient who returns to treatment, positive bacteriogically, following interruption of treatment for 2 months or more
5. OTHERS- All cases that do not fit the above difinitions.
Chronic Case A patient who is sputum positive at the end of a retreatment regimen
6. TRANSFER IN- A patient who has been transferred from another TB register to continue treatment
Recommended treatment regimens are similar irrespective of site of the disease
A patient with both pulmonary and extra pulmonary TB
Classified as a case of PTB
CAT- 1 CAT- 2 Chronic cases (CAT- 4)
TB TB
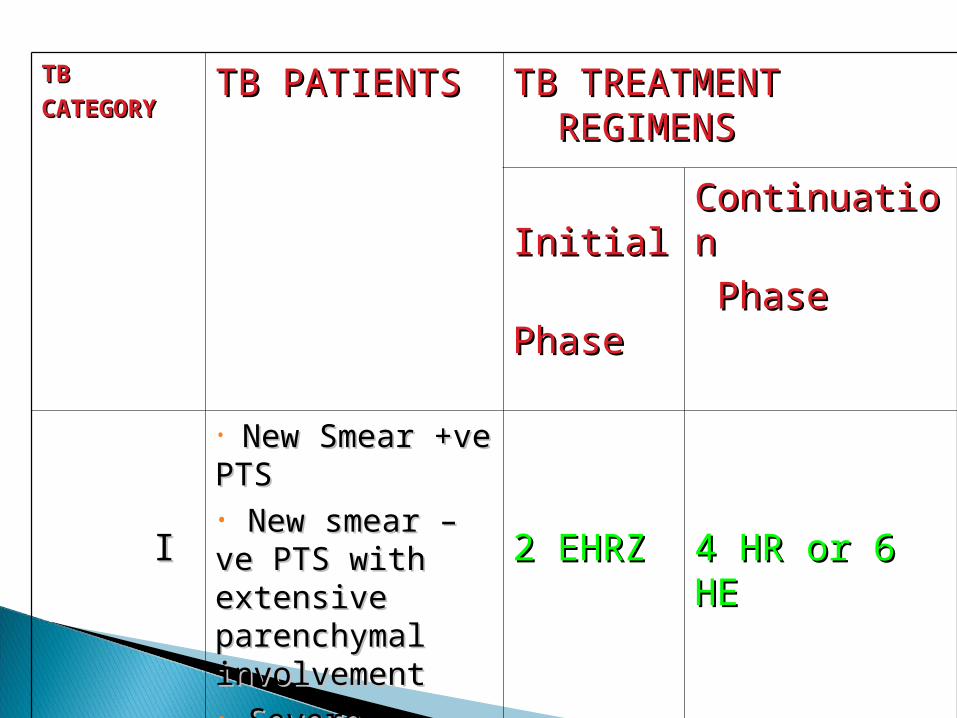
CATEGORYCATEGORYTB PATIENTSTB PATIENTS TB TREATMENT TB TREATMENT
REGIMENSREGIMENS
Initial Initial
Phase Phase
ContinuationContinuation
PhasePhase
II
• New Smear New Smear +ve PTS+ve PTS• New smear –ve New smear –ve PTS with PTS with extensive extensive parenchymal parenchymal involvementinvolvement• Severe Severe concomitant HIV concomitant HIV diseasedisease• Severe forms Severe forms of extra of extra pulmonary TBpulmonary TB
2 EHRZ2 EHRZ 4 HR or 6 4 HR or 6 HEHE
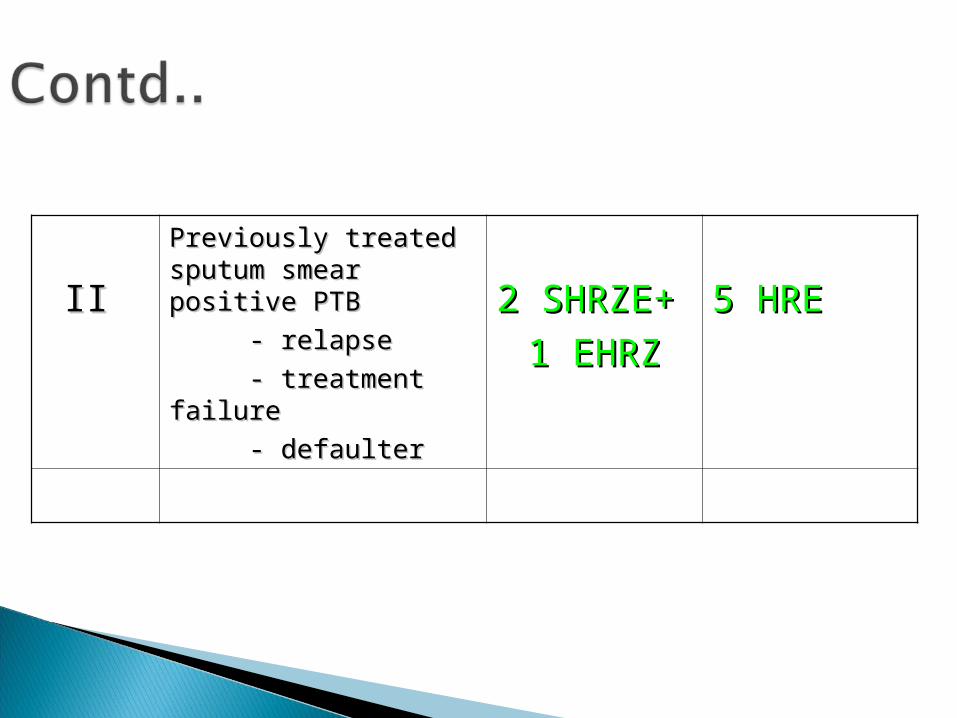
IIII
Previously treated Previously treated sputum smear positive sputum smear positive PTBPTB
- relapse- relapse
- treatment failure- treatment failure
- defaulter- defaulter
2 2 SHRZE+SHRZE+
1 EHRZ1 EHRZ
5 HRE5 HRE
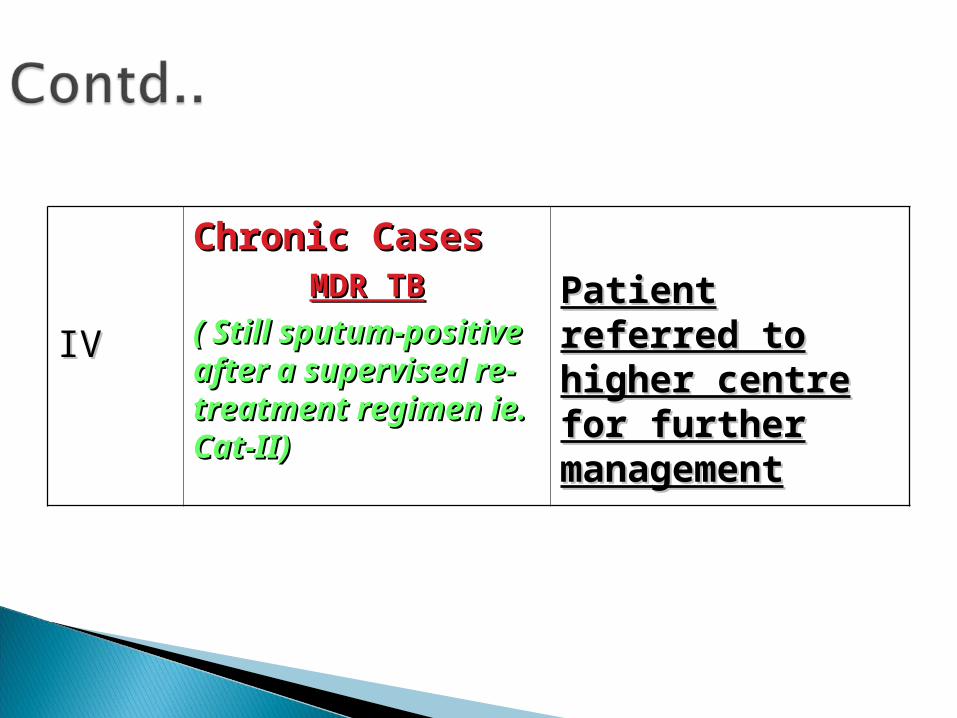
IVIV
Chronic CasesChronic CasesMDR TBMDR TB
( Still sputum-( Still sputum-positive after a positive after a supervised re-supervised re-treatment regimen treatment regimen ie. Cat-II)ie. Cat-II)
Patient referred Patient referred to higher centre to higher centre for further for further managementmanagement
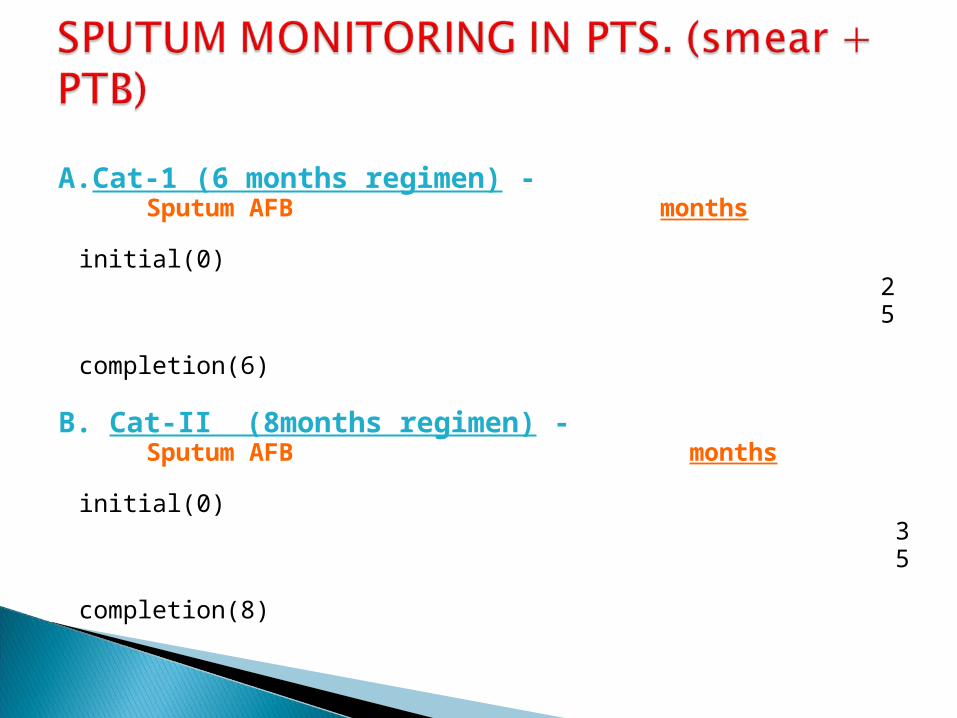
A.Cat-1 (6 months regimen) - Sputum AFB months initial(0) 2 5 completion(6)
B. Cat-II (8months regimen) - Sputum AFB months initial(0) 3 5 completion(8)
PERSONS FOR WHOM RECOMMENDED ??
Determined by Tuberculin test
I Persons with HIV infection / Close contacts of infectious cases
≥ 5mm - positiveII At risk persons
≥ 10 mm - positiveIII Persons not in a high risk category / not
exposed to high risk environment Cut off limit ≥ 15mm – positive
1. Persons with HIV infection or risk factors for HIV infection
2. Close contacts of persons with newly diagnosed infectious tuberculosis
3. Recent tuberculin skin test converters ≥ 10mm within a 2year period, age < 35years ≥ 15mm within a 2year period, age > 35
years4. Persons with medical conditions-reported to have
risk of tuberculosis. i. Diabetes mellitus ii. Prolonged therapy with steroids. iii. Immunosuppressive therapy.
iv. Hematological / reticulo endothelial disease Leukemia, Hodgkin’s disease
v. End stage renal disease vi. I.V drug abusers.
5. Foreign-borne persons from high prevalence countries - Latin America, Asia, Africa.
Given in single dose Adults - 300mg/day Children - 10- 15mg /kbw/day
(Dose should not exceed 300mg/day)
Total duration – 12 months (minimum = 6 months)
Related Documents











