TB Infection Control within the palliative care context Kath Defilippi 1 Patient Care Portfolio Manager Hospice Palliative Care Association of South Africa (HPCA)

TB Infection Control within the palliative care context
Feb 10, 2016
Kath Defilippi. TB Infection Control within the palliative care context. Patient Care Portfolio Manager Hospice Palliative Care Association of South Africa (HPCA). TB infection control will be discussed in relation to the disease transmission cycle - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
TB Infection Control within thepalliative care context
Kath Defilippi
Patient Care Portfolio ManagerHospice Palliative Care Association of South Africa (HPCA)

2
During this presentation:
• TB infection control will be discussed in relation to the disease transmission cycle
• Additional interventions implemented by HPCA will be shared
• Although drug resistant TB will be specifically mentioned, the focus is on general infection control iro TB in the palliative care context and includes both adults and children

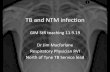
MYCOBACTERIIUMTB
1. RESERVOIR5.SUSCEPTIBLE
HOST
4. PLACE
OF ENTRY
2. PLACE OF EXIT
3. METHOD OF TRANSMISSION
Disease-producing agent
How the agent moves from place-to-place or person-to-person
Where the agent leaves the host
Place where the agent lives
Where the agent enters the next host
Person who can become infected
Adapted from JHPIEGO, 2003
Disease Transmission Cycle

4
The agent – mycobacterium tuberculosis• Has been active in humans for hundreds of years
• Acid fast slightly curved rod shaped bacillus 0.2-0.5 microns in diameter; 2-4 microns in length
• Thick lipid cell wall
• Multiplies slowly (every 18-24 hours)
• Aerobic – pulmonary TB most common variety
• One cough can release 3,000 droplet nuclei – one sneeze can release tens of thousands
• Initial infection – can remain dormant for decades as latent TB Infection (LTBI)
CDC Training, Pretoria University, August, 2010

Granuloma
Control of replication
Latent TBinadequate control of replication
ACTIVE TB
No disease(control of replication)
Bacterial replication
Immunosuppression
REACTIVATION
COURSE OF INFECTION
fibrosis
G Kaplan, CDC Training, University of Pretoria, Aug, 2010

6
Conditions that promote progression of LTBI toactive TB disease• Overcrowding• Malnutrition• Age very young – immature immune system • very old – deteriorating immune system
• HIV infection – immune suppression - A healthy person with a strong immune system has a
10% chance per lifetime of developing TB disease - An HIV+ person has a 10% chance per year of developing TB

7
“Everywhere in the world, whenever a new case of infectious tuberculosis emerges, the diagnosis and commencement of treatment are usually only made after that case has already infected one or more other persons”. JD Klausner, CDC Training , Pretoria University, August , 2010
Given the HIV/TB co-infection rate, statistics collected from HPCA member organizations suggest that there are a large number of undiagnosed TB patients already on palliative care programmes in South Africa.
In Sept 2010 out of a total of 31,685 HIV+ patients there were only 4,831 diagnosed with TB (15.2%)

8
1. Decreasing the reservoir • Screening and referral for further investigation of TB:
• all new patients admitted to the pall care programme
• all existing patients who develop any of the signs and symptoms on TB screening tool
• all staff and volunteers on appointment and thereafter at least annually
• all staff and volunteers developing any of the signs and symptoms listed on TB screening tool
NB for palliative care programmes to liaise with DOH partners

9
Contacts who are at risk of contracting TB in the home care setting where 99% of palliative care patients are to be found
• 9Health Care
Workers
Neighbours
Family*
Person with
infectiousTB
* Especially children under 5 years

10
Indicators of probable TB disease in severely immune-suppressed patients
According to studies done by Hardman and Ong the most important indicators are:
• Significant recent weight loss• Persistent low grade fever• Night sweats• Cough
Only 60% of patients had a cough in Ong study
CK Ong et al Tuberculosis -HIV Coinfection: The relationship between manifestation of tuberculosis and the degree of immune-suppression le JSME: 2(2): 17-21

11
HPCA TB Screening Tool
• All newly admitted patients to IPU and HBC programmes
• Visitors and family members
• All new staff /annual screening

12
1.1 Decreasing the reservoir iro of patients/families
• Information regarding TB disease included in the health education given to all HIV+ patients and their families
• A person-centred approach to the provision of treatment adherence support and the management of side effects of TB drugs
• Promoting the relevant rights and responsibilities from the Patients Charter for Tuberculosis Care (p15 HPCA Guidelines)
• Advocating for all HIV+ patients with TB to commence with ART asap, including those on TB treatment

13
Photo South Coast HospiceKwa-ZuluNatal
Photo St Bernard’s Hospice E Cape
Challenging environment in which infection control is implemented in HBC setting
Open air support group
Photo Msunduzi Hospice KZN

14
1.2 Decreasing the reservoir iro staff and volunteers
• Staff wellness programme to promote and maintain optimal immune status
• Mandatory training on TB including infection control, for all categories of staff and volunteers
• Creating an organisational environment conducive to disclosure of HIV and TB status
• INH preventive therapy for HIV+ staff without signs of active TB

15
Training community caregivers on infection control
Photo St Bernard’s Hospice, East London

16
2.0 Infection control linked to place of exit of MTB
COUGH HYGIENE! COUGH HYGIENE!COUGH HYGIENE! Picture – G Kaplan, CDC Training, Pretoria University, August, 2010

17
2.1 Infection control linked to place of exit• Policies in place regarding criteria for admission of TB patients
to palliative care programmes (HPCA Draft Guidelines p 12-14)
• Generally patients with TB in the lungs or larynx should be considered infectious until they have:• Completed 2 wks of TB treatment and show improvement in
clinical symptoms
• In the case of MDRTB:• Had two consecutive negative sputum smears on two
different days. At least one specimen should be an early morning specimen
• Safe sputum collection (HPCA Draft Guidelines p 23)

18
3.1 Prevention of transmission
• Good ventilation can help reduce the risk of infection by diluting and/or removing infectious particles in the air
• A well-ventilated space has air constantly entering and leaving, allowing an effective mixture of air
• This effective mixture increases the dilution of infectious particles

19
3.2 Promote good natural ventilation to prevent airborne transmission of MTB
• Keep doors and windows open especially in areas where people congregate inside a building
• Where electricity is available, use fans to blow air out of the room
• Hold support groups in the open air whenever the weather permits
• Encourage patients and family members to sit outside in the sun

20
5.1 Susceptible children
• All children who have been exposed to an adult with infectious TB must be referred for investigation
• - they should then either receive first or second line treatment or be given INH preventive therapy (IPT)
• Young children with TB are usually not a risk to other children or adults

21
4.0 Infection Control linked to place of entry - airborne mycobacterium tuberculosis
Personal Controls• Surgical masks
• No protection against infectious droplets
• May limit distribution of large particles
• Consider for coughing patients
• Respirators for caregivers• Filter >95% of infectious droplets (N95)• Fit-testing required• Valuable during aerosol-producing
procedures• May be re-used if handled properly

22
4.1 Implement universal precautions linked to the prevention of HIV infection
• Hand washing and the wearing of gloves whenever there is contact with bodily secretions
• Covering any breaks in the skin
• Effective disposal of all potentially contaminated waste
• Safe disposal of sharps

23
5.0 Protection of susceptible family membersIn the case of MDR TB • Assess home prior to admission of patient, prepare and
capacitate family to implement the necessary infection control measures
• Ensure that there are separate sleeping arrangements
• No children under 5 years in the household
• If possible no elderly relatives in the household
• Monitor response to second line treatment and liaise with MDR unit re management of side effects

24
5.1 Protection of susceptible health care workers in palliative care teams• Provide effective facial masks and monitor their use
• As far as is possible do not allow immune compromised staff and volunteers to have direct contact very ill AIDS patients who could have undiagnosed TB or with MDR TB patients
• Promote disclosure of HIV and TB status
• INH preventive therapy
• Care for the caregiver programmes

25
5.2 Personal Protective Equipment
In order for facial masks to be effective:-Must be large enough to fully cover the nose, lower face,
jaw, and facial hair-Must be made of fluid-resistant materials
All staff/volunteers caring for patients must begiven gloves and have access to aprons

26
5.3 Infection Control Plan
Designated responsibility reflected on job description/s
Includes assessment of TB infection control risks
Written policies and procedures
In-service training for all categories of staff /volunteers
Forms part of Risk Management Programme which is evaluated annually

27
5.6 Staff Training
Each staff person should understand the importance of infection control & their role in implementing infection control
Job descriptions should include specific infection control duties
Infection control should be included as part of staff orientation and in-service training, and include those not directly involved in patient care

28
Additional interventions adopted by HPCA 2nd edition of the Hospice Palliative Care Standards include criteria on:
• Screening for TB as part of initial and ongoing assessments• TB infection control and training• Inclusion of TB in risk management and quality improvement
programmesSurveys are conducted to assess compliance with the standards on a
regular basis
Infection control guidelines distributed to all members• Implementation of infection control monitored via audit tool
Development of Guidelines for providing palliative care to patients with TB
Development of a specific 5-day training course for TB in the palliative care setting

29

30
Topics included in TB master training course
Global, national and provincial overview
SA National TB programme (4 I’s)
Diagnosis and investigations (pulmonary and extra-pulmonary TB) adults and children
Palliative care principles within the context of TB
History of TBEpidemiology
Communication
Collaboration, referrals and networking
Special paediatric considerationsIPT
Monitoring evaluation and reporting
Prevention and Infection Control – adults and childrenTB as part of risk management
Treatment adherence supportPatient and family education
Drug resistant TB Integration of TB and HIV IRIS – implications for palliative careprogrammes
Providing care for TB patients, including end of life careLoss, grief and bereavement

31
Sincere thanks to:HPCA TB Task Team and the reference group of TB
experts - in particular Prof David Cameron
Open Society Institute
Worldwide Palliative Care Alliance
Related Documents