ORIGINAL ARTICLE Taxonomy of rare genetic metabolic bone disorders L. Masi 1 & D. Agnusdei 2 & J. Bilezikian 3 & D. Chappard 4 & R. Chapurlat 5 & L. Cianferotti 1 & J.-P. Devolgelaer 6 & A. El Maghraoui 7 & S. Ferrari 8 & M. K. Javaid 9 & J.-M. Kaufman 10 & U. A. Liberman 11 & G. Lyritis 12 & P. Miller 13 & N. Napoli 14 & E. Roldan 15 & S. Papapoulos 16 & N. B. Watts 17 & M. L. Brandi 1 Received: 10 October 2014 /Accepted: 26 May 2015 /Published online: 13 June 2015 # International Osteoporosis Foundation and National Osteoporosis Foundation 2015 Abstract Summary This article reports a taxonomic classification of rare skeletal diseases based on metabolic phenotypes. It was prepared by The Skeletal Rare Diseases Working Group of the International Osteoporosis Foundation (IOF) and includes 116 OMIM phenotypes with 86 affected genes. Introduction Rare skeletal metabolic diseases comprise a group of diseases commonly associated with severe clinical consequences. In recent years, the description of the clinical phenotypes and radiographic features of several genetic bone disorders was paralleled by the discovery of key molecular pathways involved in the regulation of bone and mineral metabolism. Including this information in the description and classification of rare skeletal dis- eases may improve the recognition and management of affected patients. Electronic supplementary material The online version of this article (doi:10.1007/s00198-015-3188-9) contains supplementary material, which is available to authorized users. * M. L. Brandi [email protected] 1 Metabolic Bone Diseases Unit, Department of Surgery and Translational Medicine, University Hospital of Florence, University of Florence, Florence, Italy 2 Eli Lilly and Co., Florence, Italy 3 College of Physicians and Surgeons, Columbia University, New York, NY, USA 4 GEROM Groupe Etudes Remodelage Osseux et bioMatériaux-LHEA, IRIS-IBS Institut de Biologie en Santé, LUNAM Université, Angers, France 5 INSERM UMR 1033, Department of Rheumatology, Université de Lyon, Hospices Civils de Lyon, Lyon, France 6 Departement de Medicine Interne, Cliniques Universitaires UCL de Saint Luc, Brussels, Belgium 7 Service de Rhumatologie, Hôpital Militaire Mohammed V, Rabbat, Morocco 8 Division of Bone Diseases, Faculty of Medicine, Geneva University Hospital, Geneva, Switzerland 9 Oxford NIHR Musculoskeletal Biomedical Research Unit, University of Oxford, Oxford, UK 10 Department of Endocrinology, Ghent University Hospital, Gent, Belgium 11 Department of Physiology and Pharmacology and the Felsenstein Medical Research Center, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel 12 Laboratory for the Research of Musculoskeletal System, University of Athens, Athens, Greece 13 Colorado Center for Bone Research, University of Colorado Health Sciences Center, Lakewood, CO, USA 14 Division of Endocrinology and Diabetes, Università Campus Bio-Medico di Roma, Rome, Italy 15 Department of Clinical Pharmacology, Gador SA, Buenos Aires, Argentina 16 Center for Bone Quality, Leiden University Medical Center, Leiden, The Netherlands 17 Mercy Health Osteoporosis and Bone Health Services, Cincinnati, OH, USA Osteoporos Int (2015) 26:2529–2558 DOI 10.1007/s00198-015-3188-9

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL ARTICLE
Taxonomy of rare genetic metabolic bone disorders
L. Masi1 & D. Agnusdei2 & J. Bilezikian3& D. Chappard4
& R. Chapurlat5 &
L. Cianferotti1 & J.-P. Devolgelaer6 & A. El Maghraoui7 & S. Ferrari8 & M. K. Javaid9&
J.-M. Kaufman10& U. A. Liberman11
& G. Lyritis12 & P. Miller13 & N. Napoli14 &
E. Roldan15& S. Papapoulos16 & N. B. Watts17 & M. L. Brandi1
Received: 10 October 2014 /Accepted: 26 May 2015 /Published online: 13 June 2015# International Osteoporosis Foundation and National Osteoporosis Foundation 2015
AbstractSummary This article reports a taxonomic classification ofrare skeletal diseases based on metabolic phenotypes. It wasprepared by The Skeletal Rare DiseasesWorking Group of theInternational Osteoporosis Foundation (IOF) and includes 116OMIM phenotypes with 86 affected genes.Introduction Rare skeletal metabolic diseases comprise agroup of diseases commonly associated with severe clinical
consequences. In recent years, the description of theclinical phenotypes and radiographic features of severalgenetic bone disorders was paralleled by the discoveryof key molecular pathways involved in the regulation ofbone and mineral metabolism. Including this informationin the description and classification of rare skeletal dis-eases may improve the recognition and management ofaffected patients.
Electronic supplementary material The online version of this article(doi:10.1007/s00198-015-3188-9) contains supplementary material,which is available to authorized users.
* M. L. [email protected]
1 Metabolic Bone Diseases Unit, Department of Surgery andTranslational Medicine, University Hospital of Florence, Universityof Florence, Florence, Italy
2 Eli Lilly and Co., Florence, Italy3 College of Physicians and Surgeons, Columbia University, New
York, NY, USA4 GEROM Groupe Etudes Remodelage Osseux et
bioMatériaux-LHEA, IRIS-IBS Institut de Biologie en Santé,LUNAM Université, Angers, France
5 INSERM UMR 1033, Department of Rheumatology, Université deLyon, Hospices Civils de Lyon, Lyon, France
6 Departement de Medicine Interne, Cliniques Universitaires UCL deSaint Luc, Brussels, Belgium
7 Service de Rhumatologie, Hôpital Militaire Mohammed V,Rabbat, Morocco
8 Division of Bone Diseases, Faculty of Medicine, Geneva UniversityHospital, Geneva, Switzerland
9 Oxford NIHR Musculoskeletal Biomedical Research Unit,University of Oxford, Oxford, UK
10 Department of Endocrinology, Ghent University Hospital,Gent, Belgium
11 Department of Physiology and Pharmacology and the FelsensteinMedical Research Center, Sackler School of Medicine, Tel AvivUniversity, Tel Aviv, Israel
12 Laboratory for the Research of Musculoskeletal System, Universityof Athens, Athens, Greece
13 Colorado Center for Bone Research, University of Colorado HealthSciences Center, Lakewood, CO, USA
14 Division of Endocrinology and Diabetes, Università CampusBio-Medico di Roma, Rome, Italy
15 Department of Clinical Pharmacology, Gador SA, BuenosAires, Argentina
16 Center for Bone Quality, Leiden University Medical Center,Leiden, The Netherlands
17 Mercy Health Osteoporosis and Bone Health Services,Cincinnati, OH, USA
Osteoporos Int (2015) 26:2529–2558DOI 10.1007/s00198-015-3188-9
caverzas
Texte tapé à la machine
B 796
caverzas
Texte tapé à la machine
caverzas
Texte tapé à la machine

Methods IOF recognized this need and formed a Skel-etal Rare Diseases Working Group (SRD-WG) of ba-sic and clinical scientists who developed a taxonomyof rare skeletal diseases based on their metabolicpathogenesis.Results This taxonomy of rare genetic metabolic bonedisorders (RGMBDs) comprises 116 OMIM phenotypes,with 86 affected genes related to bone and mineral ho-meostasis. The diseases were divided into four majorgroups, namely, disorders due to altered osteoclast, os-teoblast, or osteocyte activity; disorders due to alteredbone matrix proteins; disorders due to altered bone mi-croenvironmental regulators; and disorders due to de-ranged calciotropic hormonal activity.Conclusions This article provides the first comprehensivetaxonomy of rare metabolic skeletal diseases based onderanged metabolic activity. This classification will helpin the development of common and shared diagnosticand therapeutic pathways for these patients and also inthe creation of international registries of rare skeletaldiseases, the first step for the development of genetictests based on next generation sequencing and forperforming large intervention trials to assess efficacyof orphan drugs.
Keywords Bonemetabolism . Genetic bone diseases .
Metabolic bone diseases . Rare bone diseases . Taxonomy
Introduction
A disease or disorder is defined as rare or Borphan^ when itaffects less than 5 in 10,000 individuals or has a prevalence of<7.5/100,000 [1–3]. More than 6000 rare disorders have beendescribed affecting approximately 30 million individuals inthe USA and 27–36 million in the EU [1, 4–6; http://www.fda.gov/; http://ec.europa.eu/research/fp7/index_en.cfm;http://www.ema.europa.eu/pdfs/human/comp/29007207en.pdf), with almost half affecting children [7]. Many of theseconditions are complex, severe, degenerative, and chronicallydebilitating [1, 7], and there is a need for recognition,diagnosis, and treatment of affected individuals. Due to therarity of these disorders, international cooperation andcoordination of research and funding are essential [7–18].
Genetic disorders involving primarily the skeletal sys-tem represent a considerable portion of the recognizedrare diseases, and more than 400 different forms ofskeletal dysplasia have been described [19]. Accumulat-ing evidence of the clinical and genetic heterogeneity ofskeletal disorders has led to different classifications of
these disorders based on their clinical and radiologicalfeatures and, subsequently, their molecular and embryo-logical features [20–24]. In 2011, Warman et al. [25]proposed a classification of rare skeletal disorders basedon four criteria: (1) significant skeletal involvement,corresponding to the definition of skeletal dysplasia,metabolic bone disorders, dysostoses, and skeletal mal-formation and/or reduction syndromes; (2) publicationand/or listing in MIM (meaning that observations shouldnot find their way into the nosology before they achievepeer-reviewed publication status); (3) genetic basis prov-en by pedigree or very likely based on homogeneity ofphenotype in unrelated families; and (4) nosology au-
Fig. 1 Main English websites on rare diseases with constantly updateddatabases (as most recently accessed in January 2015)
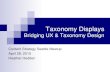
Fig. 2 The bone metabolic machinery
2530 Osteoporos Int (2015) 26:2529–2558

tonomy confirmed by molecular or linkage analysis and/or by the presence of distinctive diagnostic features andof observation in multiple individuals or families. Usingthese criteria, the authors identified 456 different condi-tions which they classified in 40 groups. Of these con-ditions, 316 were associated with one or more of 226different gene defects [25, 26]. Nowadays, severalwebsites, mainly focusing on genetics, are available(Fig. 1) and can be used as reference once a rare dis-ease is identified.
Bones are formed during embryonic developmentthrough two major mechanisms: endochondral andintramembranous ossification. This process, calledmodeling, begins in utero and continues throughout ad-olescence until skeletal maturity. Following skeletal ma-turity, bone continues to be broken down and rebuilt(remodeling) throughout life and adapts its material tothe mechanical demands. Remodeling has the functionof the control of mineral homeostasis and of maintain-ing the biomechanical competence of the skeleton. The
Fig. 3 Osteoclasts (OCs), the bone-resorbing cells, are multinucleatedcells originating from precursor cells derived from the mononuclear my-eloid lineage, which also give rise to macrophages [42]. The main regu-lators of osteoclastogenesis are cells of the osteoblastic lineage, throughthe release in the bone microenvironment of important chemokines, asmacrophage-colony stimulating factor (M-CSF) and receptor activator ofNF-κB ligand (RANKL), both active on the OC precursors (OCPs) [42].M-CSF binds to its receptor, c-fms, on OCPs and activates signalingthrough MAP kinases and ERKs during the early phase of OCP differ-entiation [43]. RANKL binds to its receptor, RANK, on the surface ofOCPs, activating signaling through NF-κB, c-Fos, phospholipase Cγ(PLCγ), and nuclear factor of activated T cells c1 (NFATc1), to inducedifferentiation of OCPs into mature osteoclasts [44]. Osteoprotegerin(OPG), also secreted by osteoblasts in response to several local and sys-temic factors, functions as a decoy receptor that binds RANKL and pre-vents it from interacting with RANK, limiting OC formation, activity, andsurvival [45]. In pathological conditions, remodeling/modeling activitycan be increased or decreased. The bone resorption process is complex;
two phases in this pathway can be recognized, namely acid secretion andproteolysis [46]. The model of bone degradation clearly depends on phys-ical intimacy between the osteoclast and bone matrix, a role provided byintegrins. Integrins, alpha beta (ανβ3) heterodimers, are the principal cellmatrix attachment molecules and they mediate osteoclastic bone recog-nition creating a sealing zone, into which hydrochloric acid and acidicproteases such as cathepsin K are secreted [47]. Acid secretion is initiatedthrough the active secretion of protons through a vacuolar type ATPase(V-ATPase) and passive transport of chloride through a chloride channel[48, 49], with a final dissolution of the inorganic bone matrix [50]. Acidproduction is accompanied by an increased chloride transport [46, 51–55]and the involvement of the enzyme carbonic anhydrase II (CAII), whichcatalyzes conversion of CO2 and H2O into H2CO3, thereby providing theprotons for the V-ATPase [56]. Proteolysis of the type I collagen matrix inbones is mainly mediated by the cysteine proteinase, cathepsin K, whichis active at low pH in the resorption lacunae [46, 50, 57, 58]. Products ofbone metabolism can be measured, with fragments of collagen type Ibeing the most direct indicators of the osteoclastic activity [59–61]
Osteoporos Int (2015) 26:2529–2558 2531

components of the metabolic bone tissue machinery aredepicted in Fig. 2. The cells involved in the metabolicactivity of the skeleton are osteoclasts (OCs), osteoblasts(OBs), and osteocytes [27]. The bone extracellular matrix(ECM), known as osteoid, is a complex of self-assembledmacromolecules composed predominantly of collagens(~90 % of the matrix proteins), noncollagenous glycopro-teins, hyaluronan, and proteoglycans. The osteoid andits local modulating factors are also primary factors inthe metabolic performance of bone tissue. The mineralis another important component of the metabolic
machinery of bone tissue. The metabolic activity ofbone is controlled by systemic and local factors andmechanical signals depicted in Figs. 3, 4, 5, 6, and 7[28–41].
The major advances in our understanding of the regu-lation of bone metabolism in recent years allow a differentapproach to the classification of rare skeletal diseasesbased on their metabolic pathogenesis. Such approachcannot only improve the recognition and diagnosis of af-fected patients but can also lead to identification of newtargets for therapeutic interventions. In addition, it can
Fig. 4 Osteoblasts (OBs) are bone-forming cells that originate frommes-enchymal stem cells (MSCs). The complexities of bone formation areimmediately apparent in the embryo, where different regions of the skel-eton arise either from intramembranous bone formation or from the en-dochondral sequence. Osteogenesis is regulated by many molecules, in-cluding transcription factors, growth factors, cytokines, and hormones,acting through paracrine, autocrine, and endocrinemechanisms [27], withaxial and appendicular-derived osteoblasts exhibiting different responsesto hormones [24, 62, 63]. Factors critical in osteoblastogenesis and inmature OBs function are represented by Runx2, Osterix, Wingless(Wnt), lipoprotein receptor-related protein 5 and 6 (Lrp5/6), and bonemorphogenetic proteins (BMPs) [27]. OBs are responsible for the depo-sition of bone extracellular matrix (osteoid), which become mineralized,by deposition of calcium hydroxyapatite, giving the bone rigidity andstrength. Biomineralization is characterized by development of matrixextracellular vesicles that are formed by polarized budding from the
surface membrane of OBs [64]. The mineralization begins with the for-mation of hydroxyapatite crystals [calcium (Ca) and inorganic phosphate(Pi)] within matrix vesicles. Ca is incorporated in vesicles by annexin Cachannel, Ca-binding phospholipids calbindins and sialoprotein. Pi is pro-vided by type III Na/Pi cotransporter, by PHOSPHO1, and from theactivity of tissue-nonspecific alkaline phosphatase that hydrolyzes pyro-phosphate (PPi) [64]. This process is followed by propagation of hy-droxyapatite through the membrane into the extracellular matrix in clus-ters around matrix vesicles and fills the space between collagen fibrils inthe skeletal matrices. PPi inhibits the formation of hydroxyapatite. Theratio of Pi to PPi that is mediated by alkaline phosphatase activity iscrucial in this step of mineralization [64]. Markers of bone formationare measurable, some being enzymes or proteins produced by osteoblasts(i.e., alkaline phosphatase and osteocalcin) [60, 65–69], while othersderive from type I collagen metabolism (i.e., procollagen type Ipropetides) [60]
2532 Osteoporos Int (2015) 26:2529–2558

provide bone specialists the background for the diagnosticevaluation of biochemical alterations in individual pa-tients and can contribute to their better understanding ofthe etiology of the disease.
The aim of the present article, resulted from the workof the members of the Skeletal Rare Diseases Working
Group (SRD-WG) of the International Osteoporosis Foun-dation (IOF), is to classify rare skeletal disorders accord-ing to alterations of specific genes encoding proteins in-volved in the activity of bone cells, bone matrix proteins,microenvironmental regulators essential for bone physiol-ogy, or response to calciotropic hormones.
Fig. 5 In the adult skeleton, osteocytes make up 90−95 % in volume ofall bone cells compared with 4–6 % osteoblasts and 1–2 % osteoclasts[70]. Osteocytes establish an extensive intercellular communicationsystem via gap-junction-coupled cell processes, also extended to OBsand OCs on the bone surface and, therefore, represent an idealmechanosensory system. Various authors have identified several transi-tional stages between osteoblasts and osteocytes. In their review article,Franz-Odendaal et al. [71] combined these observations to propose eightrecognizable transitional stages from the osteoblast to the osteocyte. The-se authors favor an embedding mechanism in which a subpopulation ofosteoblasts on the bone surface slows down matrix production relative toadjacent cells and becomes Bburied alive^ under the matrix produced byneighboring osteoblasts. Sclerostin, the SOST gene protein product, isspecifically expressed in osteocytes and inhibits osteoblast function andbone formation by antagonizing canonicalWnt signaling through bindingtoWnt coreceptor Lrp5 and Lrp6, with Sost-deficient mice being resistantto bone loss at unloading [72]. In addition, Dickkopf (in particular Dkk-1)protein, expressed in many cell types, is highly expressed in osteocytes[73] and has also been shown to bind to Lrp5/6 and a transmembraneprotein, Kremen, inhibiting canonical Wnt activation pathway [74]. Thefunction of osteocytes in bone formation is still a matter of debate. Underin vitro application of mechanical stimuli, osteocytes activate bone
formation through the release of anabolic factors [i.e., prostaglandin E2(PGE2), prostaglandin I2 (PGI2), nitric oxide (NO), cyclooxygenase-2(COX-2), and endothelial nitric oxide synthase (eNOS)] [72], with boneformation being severely inhibited after osteocyte ablation [75]. Withinthe past two decades, several markers of osteocytes have been identified[74, 76, 77]. It is known that there is a heterogeneity in gene expression inosteocytes within bone. For example, early embedding osteoid osteocytesand young osteocytes express high levels of E11/gp38 (also known aspodoplanin), while more mature, deeply embedded osteocytes expresshigh levels of sclerostin [78]. Moreover, several proteins that are osteo-cyte specific, or selectively expressed in osteocytes, play critical roles inphosphate homeostasis. These include phosphate-regulating gene withhomologies to endopeptidases on the X chromosome (PHEX), matrixextracellular phosphoglycoprotein (MEPE), dentin matrix protein 1(DMP1), and fibroblast growth factor 23 (FGF23) [79]. Compared toOBs, osteocytes also appear to be enriched in proteins associated withresistance to hypoxia [80] due to their embedded location within bone, asexpected [79]. Another important category of factors whose expression isdifferent in osteocytes compared to OBs is molecules involved in cyto-skeletal function and cell motility (destrin, CapG, cdc42, and E11/gp38)[79, 80]
Osteoporos Int (2015) 26:2529–2558 2533

Material and methods
In 2012, the IOF recognized the need for identifyingand managing patients with rare skeletal diseases andestablished a working group (SRD-WG) of experts indiseases of bone metabolism to address this issue. Themembers of the group, after reviewing existing literatureinformation and consulting other physicians involved inthe management of patients with rare skeletal diseases,concluded that classification of these diseases accordingto their metabolic pathogenesis was more appropriateand prepared the first draft of the manuscript. Thecriteria used to include different disorders were as fol-lows: skeletal involvement as linked to major alterationsof bone metabolism, publication and/or listing in theOnline Mendelian Inheritance in Man (OMIM) system,and nosologic autonomy (literature updated withPubMed database searches up to January 2015). TheSRD-WG considered abnormalities of all elementsknown to influence bone metabolism and included
disorders that are rare, metabolic, and skeletal in originwhose genetic basis is proven or suspected on the basisof the phenotype. This classification does not, therefore,include skeletal dysplasias due to altered morphogenesisduring embryonic development. In addition, we did notinclude in the classification rare diseases in which alter-ations in the actors of bone metabolism are not theprimary cause of the syndrome and bone is only sec-ondarily involved (e.g., storage disorders). This manu-script is the result of several discussions and revisionsof the original draft and represents the consensusreached by the members of the group.
Acronyms for the disorders described, phenotype, andgene/locus numbers are presented according to the no-menclature of the OMIM database, as most recentlyaccessed in January 2015 (http://www.ncbi.nlm.nih.gov/omim). An OMIM entry preceded by a number sign (#)indicates the phenotype and specific OMIM entries forthe genes/loci whose mutations have been shown asresponsible for that phenotype (http://web.udl.es/dept/
Fig. 6 Bone ECM is not only a scaffold for the cells, but also serves as areservoir for growth factors and cytokines, and modulates bone turnoverand mineral deposition [81, 82]. Type I collagen, synthesized by the OBs,is the most abundant extracellular protein of bone tissue (85–90%), beingessential for bone strength. The molecules of mature collagenspontaneously assemble into fibrils, and cross links form to increase thetensile strength of the fibrils [83]. Different cytokines, inflammatorymediators, matrix-degrading enzymes, hormones, and growth factorscan modify the synthesis and degradation of type I collagen, withinwell-orchestrated autocrine and paracrine anabolic and catabolic
pathways [81–83]. Noncollagenous proteins (NCPs) compose 10–15 %of the total bone protein content. These proteins are multifunctional, hav-ing roles in organizing the extracellular matrix, coordinating cell-matrixand mineral-matrix interaction, and regulating the mineralization process.[82]. The NCP molecules can be classified into four groups: (1) proteo-glycans, (2) glycosylated proteins, (3) glycosylated proteins with poten-tial cell adhesion properties, and (4) γ-carboxylated (gla) proteins [28,82–85]. Sincemutations in these proteins cause mainly skeletal dysplasia,they have not been considered in the proposed classification
2534 Osteoporos Int (2015) 26:2529–2558

cmb/biomatica/OMIM.PDF). The names of genes/lociare those approved by HGNC (HUGO Gene Nomencla-ture Committee, http://www.genenames.org). Diseasesfor which the OMIM classif icat ion leads to aconfounding numbering system (e.g., osteogenesisimperfecta) have been l is ted into grouping inphenotypes according recently to suggested taxonomies.Diseases for which a specific OMIM phenotype hasbeen described, but for which the genetic alterationhas not yet been detected (e.g., Gorham-Stout disease),have in any case been included in the tables. For dis-eases for which locus heterogeneity has been recognized(e.g., Camurati-Engelmann disease), the main geneticalteration has been herein reported. A brief descriptionof the phenotype and altered biomarkers, when avail-able, has been reported for each rare metabolic bonedisease, in order to focus on the metabolic phenotype,even for cases for which this latter information is indi-cated as BNR^ (not reported). In Fig. 8, the availablenondisease-specific screening/diagnostic assays, whichcould be of use to further refine the diagnosis, havebeen listed.
Some diseases/phenotypes overlap in two or more ta-bles because of multiple alterations in bone metabolism(e.g., a pure osteoblast defect can manifest into a disorderof bone matrix). Following a metabolic-based taxonomy,these specific disorders have to be indicated in more thanone table. Thus, a disease resembling a phenotype due,for example, to an alteration of collagen metabolism, butdue to a primitive alteration in osteoblast (e.g., osteogen-esis imperfecta type IV due to mutations of SP7 or PLS3)has been primarily inserted in Tables 1, 2, 3, and 4,encompassing the alterations in osteoblasts, which indeedultimately lead to collagen metabolism alteration, andsecondarily in Tables 5 and 6, since they resemble adisorder in bone matrix (and referred to as Bsee Tables 1,2, 3, and 4^).
Results
Rare genetic metabolic bone disorders (RGMBDs) wereclassified in four major groups according to their primarypathogenetic mechanism: altered osteoblast, osteoclast, orosteocyte function; altered bone matrix proteins; alteredbone microenvironmental regulators; and alteredcalciotropic hormonal activity. We report 116 disease-related OMIM phenotypes with 86 affected genes, andwe include genetic causes (germ line mutations,postzygotic somatic mutations, mitochondrial DNA)
where known, as well as general and bone-specific fea-tures and biochemical alterations.
Altered osteoblast, osteoclast, or osteocyte function
Tables 1, 2, 3, and 4 describe diseases due to an alteration inthe activity of bone cells (osteoclasts, osteoblasts, and osteo-cytes) resulting in an increase or decrease in either boneformation or bone resorption. The four main groups iden-tified include 38 different phenotypes. Disorders charac-terized by high bone resorption are shown in Table 1,while those associated with low bone resorption areshown in Table 2. These disorders are generally causedby mutations in genes encoding osteoclastic functionalproteins. Table 3 depicts disorders characterized by highbone formation. These are caused by mutations in genesencoding proteins involved in osteoblastogenesis and ma-ture osteoblast function or proteins produced by osteo-cytes involved in differentiation and life span of osteo-blasts. Finally, diseases characterized by low bone forma-tion are shown in Table 4; these are caused by mutationsin genes encoding proteins involved in the formation andfunction of osteoblasts.
Altered bone matrix proteins
Tables 5 and 6 describe diseases where the characteris-tics of matrix proteins are altered. Three major groupswere identified, with 28 different phenotypes (fiveoverlapping with the forms listed in Tables 1, 2, 3,and 4). Regarding the diseases related to proteoglycanalterations, only the forms where the large proteogly-cans are involved in the pathogenesis were included.Mutations in genes encoding type I collagen andcollagen-related bone matrix proteins have been primar-ily listed in rare skeletal disorders characterized by al-tered collagen metabolism (Table 5). Alkaline phospha-tase is one of the main enzymes involved in bone min-eralization. Disorders causing altered production of alka-line phosphatase have been described primarily inTable 6.
Altered bone microenvironmental regulators
Tables 7, 8, 9, and 10 depict diseases caused by mutation ofgenes encoding for proteins involved in the regulation of boneturnover. Four major groups were recognized with 13 differentphenotypes (12 overlapping with the forms listed in Tables 1,2, 3, and 4 or 5 and 6).
Osteoporos Int (2015) 26:2529–2558 2535

2536 Osteoporos Int (2015) 26:2529–2558

Altered calciotropic hormonal activity
Tables 11, 12, 13, and 14 describe diseases with boneinvolvement due to congenital alterations of the functionof hormones involved in the regulation of calciotropic
hormones. Four major groups were described with 54different phenotypes. Disorders due to parathyroid hor-mone excess or deficiency are listed in Table 11, whilediseases caused by altered parathyroid hormone (PTH)signaling and abnormal vitamin D metabolism and ac-tion are shown in Tables 12 and 13, respectively.Table 14 displays disorders due to altered phosphatemetabolism.
Discussion
We propose here for the first time a classification sys-tem for rare skeletal bone diseases based on a metabolicapproach, selecting from this large number of disordersthose due to an abnormality of the actors of bone me-tabolism: bone cells, bone matrix, and local and system-ic regulators. The primary aim of this taxonomy is toprovide a reference list on a metabolic basis, and onlysecondarily to help in the diagnostic workup. For thisreason, the information regarding family history, geneticevaluation, and management of the different disordersreported was not included in the classification. We ac-knowledge further that this classification is arbitrary, butit has the strength that is based on actual, known find-ings that will encourage clinicians to perform propermetabolic evaluation of patients in order to plantargeted suitable treatment. It should be also noted thatsome level of arbitrary judgment is always compatiblewith a taxonomy process, and the same criticism can beposed toward a radiological classification that does notencompass information that we consider relevant for theclinical management of such difficult patients. In addi-tion, such evaluation can be of clinical relevance intargeting appropriate treatment, when available, thatgenerally is not timely and appropriately prescribed inthe majority of patients. Finally, this metabolic taxono-my does not undermine the importance of previous classifi-cations on this subject, which still constitute a reference list forthese disorders [25].
To date, the diagnosis of rare skeletal diseases isbased on clinical phenotype and radiographic features.A classification system based on measurement of bonemineral density (BMD) or assessment of skeletal fragil-ity is not feasible because in the majority of these dis-orders, systematic evaluation of BMD by DXA has notyet been performed, and the long-term incidence offracture is unknown. Classification of Blocal^ orBsystemic^ disorders is also not feasible, because in ap-parently localized disorders, a systemic alteration in
�Fig. 7 Calciotropic hormones are defined on the basis of their capabilityto modulate Ca/Pi metabolism, and all of them directly and indirectlymodulate bone metabolism. Ca and Pi are essential to many vitalphysiological processes [29] and their regulation involves a concertedaction among the digestive system, kidneys, and skeleton via the actionof calciotropic hormones. Disturbances in calciotropic hormonehomeostasis have been linked to several pathophysiological disorders,including bone abnormalities [29, 30]. Among the hormones thatcontrol Ca and Pi metabolism, parathyroid hormone (PTH) andcalcitriol [1-25(OH)2D3] are the most documented. PTH inhibits renalPi reabsorption and increases Ca reabsorption, indirectly increasingintestinal Ca and Pi absorption by stimulating the synthesis of calcitriol.Conversely, Ca and Pi modulate the synthesis and secretion of PTH fromparathyroid cells [31]. Homeostasis of calcium is represented in a. Thesymbol orange + indicates the direct PTH stimuli and orange (+)indicates the PATH indirect stimuli. The symbol blue + indicates thevitamin D stimuli. Parathyroid cells respond to decreases inextracellular calcium concentration by means of the calcium-sensingreceptor (CaSR), a cell surface receptor that alters phosphatidylinositolturnover and intracellular calcium, ultimately determining an increase inPTH secretion [31]. In addition to parathyroid tissue, the receptor is alsoexpressed in the regions of the kidney involved in the regulation of Caand magnesium (Mg) reabsorption [32] and in many different tissuesthroughout the body [33]. Conversely, calcitriol increases both intestinalCa and Pi absorption and renal Pi reabsorption [34, 35]. In addition, PTH-related peptide (PTHrP), first discovered as the major cause of thehumoral hypercalcemia of malignancy [36], is evolutionarily andfunctionally related to PTH and also functions as mineral metabolismregulator. It is expressed by a variety of fetal and adult tissues, having aprominent role in the regulation of endochondral bone formation [37] andin the organogenesis of several epithelial tissues (i.e., skin, mammarygland, teeth) [38]. The most recently identified calciophosphotropichormones are the phosphatonins [29, 31] (b). The term phosphatoninsis used to describe factors responsible for the inhibition of Pi renalreabsorption by cotransporter and for the modulation of the 1-alpha-hydroxylase levels [29]. These molecules include FGF23, PHEX,matrix extracellular phosphoglycoprotein (MEPE), secreted frizzledrelated protein 4 (sFRP4), and fibroblast growth factor 7 (FGF7) [36,37, 76]. Most of the studies indicate FGF23 as the most importantphosphatonin. Functional in vitro studies show that FGF23 activity isregulated by proteases and its specific receptors [38]. Mature FGF23 isdegraded to two small fragments by the furin family proteases [39].Moreover, the tissue-specific activity of FGF23 can be explained on thebasis of the need for the presence of both fibroblast growth factorreceptors (FGFRs) and Klotho (KL), a coreceptor for FGF23 thatincreases the affinity of FGF23 for FGFRs [40]. In bone tissue, Ca andPi interact with cells of the bone-forming lineage and with theextracellular matrix proteins to control the osteoid mineralization [32],while deposition of minerals in soft tissues is prevented through less well-understood factors [41]. The “bone” hormones measurable in seruminclude intact PTH (iPTH), calcidiol [25(OH)D3], calcitriol [1-25(OH)2D3], intact FGF23 (iFGF23), C-terminal FGF23, and α-Klotho
Osteoporos Int (2015) 26:2529–2558 2537

bone metabolism can be present (e.g., tumoral calcino-sis) or maybe have not yet been assessed. For the ma-jority of the listed disorders, biochemical features arenot available, which underlines the need for a bettermetabolic characterization. Determination of biomarkersrelated to mineral metabolism as well as systematic as-sessment of BMD and quality of bone by improveddiagnostic tools is, therefore, needed. However, theseinvestigations are not disease-specific and are not com-monly employed, unless patients are evaluated in refer-ral centers by bone specialists with expertise in rareskeletal disorders. In selected cases, bone biopsy andin vitro assays can help to further refine the metabolicdiagnosis. Many of the bone marker tests, not availableat the time of the first description of these diseases, arenow routinely used, encouraging the biochemical/metabolic characterization of disorders potentially char-acterized by metabolic fingerprints.
The metabolic framing of a rare skeletal disease is ofparamount importance for therapeutics and can guide theclinician in the choice of the most appropriate pharmaco-logical intervention. Indeed, the characterization of a rarebone disease for the bone-forming or bone-resorbing phe-notype will lead to different therapeutic approaches (e.g.,anabolics or antiresorptives). In this respect, an exampleis hypophosphatasia, the only rare bone disease, due to aspecific metabolic enzymatic alteration, for which atargeted therapy (asfotase alpha) has recently been devel-oped and for which an antiresorptive therapy is contrain-dicated. However, other rare genetic metabolic bone dis-orders are often treated with the available antiosteoporoticagents which are given without being included in theirapproved indications (off-label prescription). In suchcases, knowledge of the bone metabolic and structuralprofile can help in choosing the most suitable therapyfor a given clinical case.
Fig. 8 Biochemical/instrumental exams and in vitro tests forcharacterizing metabolic bone diseases. Measurements of biochemicalindexes and hormones regulating mineral homeostasis can help inconfirming or excluding systemic bone metabolic disorders. Theassessment of bone turnover is important in order to plan furthertherapeutic approaches. Bone quantity and quality appraisal andprevalent vertebral fracture assessment may help to refine the metabolic
framing of the disease, manifesting with an otherwise evident bonephenotype, and is crucial in the follow-up of the treated patient. Bonebiopsy is critical in selected cases for the identification and for differentialdiagnosis. In vitro assays can be useful to identify supposed functionalabnormalities of bone cells and/or matrix proteins (e.g., in collagen-related disorders)
2538 Osteoporos Int (2015) 26:2529–2558

Tab
le1
Alteredosteoclast,osteoblast,or
osteocyteactiv
ity:low
bone
resorptio
n
Disease
OMIM
phenotype
number
OMIM
gene/
locus
number
Gene
Chrom
osom
elocatio
nPh
enotype
Mainbiochemicalalteratio
ns
Osteopetrosisdueto
altered
osteoclastfunctio
nEntities
characterizedby
anincreasedbone
density
(sclerosis)
andgeneralized
high
bone
mass,dependingon
decreasedbone
resorptio
ndueto
decreasedosteoclastfunctio
n,with
high
fracture
ratein
severe
recessiveform
s;additio
nalsigns
foreach
phenotype:
Adult/interm
ediateform
s:high
CK-BB,highbone
ALP
Infantile/severeform
s:lowCa,
high
PTH,high1,25(O
H)2D,
high
CK-BB,highAP,anem
ia
•Autosom
aldominant2
(OPTA
2)/Albers-Schonberg
disease
#166600
602727
CLCN7
16p13.3
Asymptom
atic,bonesclerosis,fractures,dentalabscesses,osteom
yelitisof
themandible
•Autosom
alrecessive1(O
PTB1)
#259700
604592
TCIRG1
11q13.2
Severe,loss
oftrabecular
structure,poor/nodefinitio
nbetweencorticaland
medullary
bone,m
acrocephaly,frontalb
ossing,blin
dness,deafness,
facialpalsy,genu
valgum
,dentald
efects,bonemarrowinsufficiency
•Autosom
alrecessive2(O
PTB2)
#259710
602642
TNFSF
1113q14.11
Interm
ediate,osteoclast-poor,fractures,genuvalgum
,hepatosplenomegaly,dentaldefects,osteom
yelitisof
themandible
•Autosom
alrecessive3(O
PTB3)
#259730
611492
CA2
8q21.2
Interm
ediate,renaltubularacidosis,early
fractures,shortstature,m
ental
retardation,dentalmalocclusion,visualim
pairment
+Metabolicacidosis
•Autosom
alrecessive4(O
PTB4)
#611490
602727
CLCN7
16p13.3
Severe,loss
oftrabecular
structure,poor/nodefinitio
nbetweencorticaland
medullary
bone,fractures,hepatosplenom
egaly,mild
optic
nerveatrophy
•Autosom
alrecessive5(O
PTB5)
#259720
607649
OST
M1
6q21
Severe,lossof
trabecular
structure,poor/nodefinitio
nbetweencorticaland
medullary
bone,hydrocephaly,microcephaly,fractures,osteosclerosis,
hepatosplenomegaly,visualim
pairment,bone
marrowinsufficiency
•Autosom
alrecessive6(O
PTB6)
#611497
611466
PLEKHM1
17q21.31
Interm
ediate,bonedeform
ities,pain,chondrolysis,dense
metaphysealbands
•Autosom
alrecessive7(O
PTB7)
#612301
603499
TNFRSF
11A
18q21.33
Severe,osteoclast-poor,hypogam
maglobulin
emia
•Autosom
alrecessive8(O
PTB8)
#615085
614780
SNX10
7p15.2
Severe,loss
oftrabecular
structure,poor/nodefinitio
nbetweencorticaland
medullary
bone,m
acrocephaly,failu
reto
thrive,opticnerveatrophy,
nasalstuffinessdueto
fully
ossified
sinuses,bone
marrowinsufficiency
•Ectodermaldysplasia,
anhidrotic,immunodeficiency,
osteopetrosis,lymphedem
a(O
LEDAID
)
#300301
300248
IKBKG
Xq28
Lym
phedem
a,anhidroticectoderm
aldysplasia,im
munologicalteratio
ns
•Os teopetrosisandinfantile
neu roaxonald
ystrophy
#600329
––
–Severe,O
PTB1phenotype,agenesisof
thecorpus
callo
sum
Osteopetrosisdueto
altered
osteoclastnumber
•Dysosteosclerosis(D
SS)
#224300
612373
SLC29A3
10q22.1
Platyspondyly
andmetaphysealosteosclerosiswith
relativ
eradiolucency
ofwidened
diaphyses,densebutb
rittleskeleton,shortstatureand
fractures,failu
reof
tootheruptio
n,developm
entald
elay,seizures,skin
findings
such
asred-violetmacularatrophy,atthehistopathological
levelp
aucity
ofosteoclasts
Low
totaland
bone
ALP,low
TRAP5b,low
UrDPD/Cr
Pycnodysostosis(PYCD)
#265800
601105
CTSK
1q21.3
Generalized
high
bone
mass,bone
fragility,shortstature,clavicular
dysplasia,obtuse
angleof
mandible,shortterminalphalanges
Low
GH,low
IGF1
Osteoporos Int (2015) 26:2529–2558 2539

Tab
le2
Alteredosteoclast,osteoblast,or
osteocyteactiv
ity:h
ighbone
resorptio
n
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype
Mainbiochemicalalteratio
ns
Cystic
angiom
atosisof
bone/Gorham-Stout
disease(G
SD)
#123880
––
–Inheritedosteolysisdisorder
characterizedby
destructionandresorptio
nof
affected
boneswith
subsequent
skeletaldeform
ities
andfunctio
nal
impairment.Early-onsetprogressiveosteolysisof
oneor
morebones
alwaysassociated
with
anangiom
atosisof
bloodvesselsandsometim
esof
lymphatics,historyof
fragility
fractures,andvascular
malform
ations
inthe
affected
bonesor
surroundingsofttissues,m
ultip
ledilatedvascular
spaces
replacingnorm
albone
marrowelem
ents,disseminated
multifocalvascular
lesionsof
theskeleton
with
possiblevisceralinvolvem
ent,bony
deform
ities,m
uscularweaknessandlocalized
pain
HighIL-6
(not
always),highserum
fibrinogen,highserum
D-dim
er,
high
ESR
,highCD105/endoglin
Cystic
angiom
atosis(CA)
#123880
––
–Multifocalhemangiom
atousand/or
lymphangiom
atouslesionsof
the
skeleton
with
possiblevisceralorganinvolvem
ent
HighOPG
,highOPN
,highIL-6
Familialhydiopatic
hyperphosphatasia/
juvenilePaget’s
diseaseof
bone
#239000
602643
TNFRSF
11B
8q24.12
Retinaldegeneratio
nin
someindividuals,angioidstreaks,muscular
weakness,deafness
ininfancy,osteoporosis,expandedlong
bones,bowed
long
bones,fragile
bones,increasedbone
form
ationanddestruction,
progressiveskeletaldeform
ity,shortstature,mild
involvem
ento
fcranial
bones,islandsof
increasedskullb
onedensity
HighPi,normalCa,markedlyhigh
ALP,high
acid
phosphatase,high
uricacid
Fam
ilialexpansile
osteolysis(FEO)
#174810
603499
TNFRSF
11A
18q21.33
Deafnessandloss
ofdentition,focalskeletalchanges,with
predom
inantly
peripheraldistributio
n,progressiveosteoclasticresorptio
naccompanied
bymedullary
expansionledto
severe,painful,disablin
gdeform
ityanda
tendency
topathologicfracture
HighALP,high
UrOHP,possible
high
Ca
2540 Osteoporos Int (2015) 26:2529–2558

Tab
le3
Alteredosteoclast,osteoblast,or
osteocyteactiv
ity:h
ighbone
form
ation
Disease
OMIM
phenotype
number
OMIM
gene/
locus
number
Gene
Chrom
osom
elocatio
nPh
enotype
Mainbiochemicalalteratio
ns
•Highbone
mass(H
BM)
#607634
603506
LRP5
11q13.2
Increasedbone
density,m
ostly
asym
ptom
atic(rarelybone
pain)
NR
•Van
Buchem
disease
type
2,autosomal
dominant(VBCH2)
#607636
603506
LRP5
11q13.2
Increasedbone
density,m
ostly
asym
ptom
atic,associatedwith
osteosclerosis
oftheskull,enlarged
andsquaredjaw(decreased
gonialangle),cranial
nervecompression,sensorineuralhearingloss
(otopharyngealexostosis)
•Osteosclerosis/endosteal
hyperostosis,autosom
aldominant
#144750
603506
LRP5
11q13.2
See
above+corticalthickening
ofthelong
bones,toruspalatin
usHighALP
•Hyperostosiscorticalis
generalisata/Van
Buchem
disease(V
BD)
#239100
605740
SOST
17q21.31
Progressiveskeletalovergrow
th(especially
skull)andcorticalthickening
and
generalized
osteosclerosis,enlargemento
fthejawwith
wideangle,flatnasal
bridge,frontalprom
inence,painof
long
bone
with
appliedpressure,no
fragility
fractures,hypertelorism,proptosis,m
ultip
lecranialn
erve
involvem
ent
with
recurrentfacialn
erve
palsy,deafness,opticatrophyfrom
narrow
ingof
cranialforam
ina,associated
with
:
Highbone
ALP,high
P1NP,
decreasedsclerostininVBD,
undetectablesclerostinin
SOST
1andCDD
•Sclerosteosis1,autosomal
recessive(SOST1)
#269500
605740
SOST
17q21.31
Symmetriccutaneoussyndactyly,excessive
height
andweight
•Sclerosteosis2,autosomal
dominant/recessive
(SOST2)
#614305
604270
LRP4
11p11.2
Syndactyly/brachyphalangy
with
naildysplasia
•Craniodiaphyseald
ysplasia,
autosomaldominant(CDD)
#122860
605740
SOST
17q21.31
Leonine
facies
Osteopathiastriata
NR
•With
outcranialsclerosis(O
S)#300373
––
–Striatio
nsin
theileum
,intestin
almalrotatio
n(rare,in
males),analstenosis(rare
inmales),analatresia(rare,in
males),gastroesophagealreflux,linearstriations
attheends
oflong
bones,bilateralfibulaaplasia(always)
•With
cranialsclerosis
(OSC
S)#300373
300647
AMER1
Xq11.2
Fem
ales:see
above+mild
learning
disabilities,macrocephaly,cleftp
alate,mild
learning
disabilities,sclerosisof
thelong
bonesandskull,cleftp
alate,long
straightclavicoleandstriations
visibleon
radiographsof
thelong
bones,pelvis,
andscapulae
Males:fetalor
neonatallethality
•Fo
cal d
ermalhypoplasia
(FDH)/Goltzsyndrome
#305600
300651
PORCN
Xp11.23
Fem
ales:h
eartdefects,gastrointestinalmalform
ations,linearareasof
derm
alhypoplasiathroughwhich
adiposetissuecanherniateandavarietyof
bone
defectsin
thelim
bs(striatedbones)
Males:u
tero
lethality
Osteopoikilo
sis/
Buschke-O
llendorff
syndrome(BOS)
#166700
607844
LEMD3
12q14.3
Asymptom
atic,disseminated
connectiv
etissuenevi
with
both
elastic-typenevi
(juvenile
elastoma)
andcollagentype
nevi
(dermatofibrosislenticularis
dissem
inate),osteosclerotic
fociin
epim
etaphysealregionsof
long
bones
NR
Melorheostosis(associated
with
osteopokilo
sis)
#155950
607844
LEMD3
unknow
ngene(s)
12q14.3
Jointcontractures,scleroderm
atousskin
lesions,muscleatrophy,hemangiom
as,
lymphedem
a,bone
deform
ities
with
linearhyperostosisof
thecortex
oflong
bonesreminiscent
ofdripping
candlewax
––
Craniom
etaphysealdysplasia,
autosomaldominant(CMD)
#123000
605145
ANKH
5p15.2
NR
Osteoporos Int (2015) 26:2529–2558 2541

Tab
le3
(contin
ued)
Disease
OMIM
phenotype
number
OMIM
gene/
locus
number
Gene
Chrom
osom
elocatio
nPh
enotype
Mainbiochemicalalteratio
ns
Impaired
vision,hearing
loss,and
facialnerveparalysis,metaphysealflaring,
hyperostosisandsclerosisof
thecranialb
ones,thick
bony
wedge
over
the
bridge
ofthenose
andglabella(firstsign)
Craniom
etaphysealdysplasia,
autosomalrecessive
(CMDR)
#218400
121014
GJA
16q22.31
Hyperostosisandsclerosisof
thecraniofacialbonesandabnorm
almodelingof
the
metaphyses,sclerosisof
theskull,asym
metry
ofthemandible,cranialn
erve
compression
with
hearingloss
andfacialpalsy
Cam
urati-Engelmann
disease(CAEND)
#131300
190180
TGFB1
unknow
ngene(s)
19q13.2
Leg
pain,m
uscularatrophyandweakness,diaphysealdysplasia,hyperostosis
oftheskullb
ase,corticalbone
thickening
andsclerosisof
thediaphysisof
the
long
tubularbonesby
both
endostealand
periostealbone
proliferation.The
extrem
evariability
inphenotypicalexpression,bothbetweenfamilies
sharing
thesamemutationandam
ongmem
bersof
thesamefamily,m
akes
itdifficult
todetectpossiblegenotype-phenotype
correlations.T
hemostseverely
affected
individualshave
progressionof
mild
skullh
yperostosisto
severe
skullthickeningandcranialn
erve
compression
Anemia,highP1N
P,N/high
bone
ALP
Cam
urati-Engelmann
diseasetype
2#606631
190180
TGFB1
19q13.2
Marfanoid
habitus,waddlinggait,
muscularweakness,intenselegpain,
flexioncontractureof
thehipandknee
joints,delayed
sexualdevelopm
ent,
corticalthickening
ofthediaphyses.Metaphysealexpansionof
thelong
bones,coarse
andthicktrabeculae
ofthelong
andshorttubular
bones,
striations
inthespinal,pelvic,andlong
bones,andcranialsclerosis
restricted
tothepetrom
astoid
regions
HighALP,high
ESD
NRnotreported
2542 Osteoporos Int (2015) 26:2529–2558

Tab
le4
Alteredosteoclast,osteoblast,or
osteocyteactiv
ity:low
bone
form
ation
Disease
OMIM
phenotype
number
OMIM
gene/
locus
number
Gene
Chrom
osom
elocatio
nPh
enotype
Mainbiochemical
alteratio
ns
Osteoporosis-pseudoglioma
syndrome,autosomal
recessive(O
PPG)
#259770
603506
LRP5
11q13.1
Blin
dness,microphthalmia,vitreoretin
alabnorm
alities,cataract,phthisisbulbi,absent
anterior
eyecham
ber,irisatrophy,pseudoglyoma,musclehypotonia,obesity,m
entalretardatio
n(insomecases),ligam
entlaxity,severeosteoporosis,m
ultip
lefractures,shortstature,
kyphoscolio
sis,hyperextensiblejoints,w
idemetaphyses
NR
Familialexudative
vitroretinopathy
(FEVR)
#601813
603506
LRP5
11q13.1
Decreased
visualacuity,b
lindness,falciform
retin
alfolds,tractio
nalretinaldetachment,
macular
ectopia,retin
alexudates,vitreous
detachment,subcapsularopacities
peripheral
retin
alavascularizatio
n,neovascularizatio
n,vitreous
hemorrhage,horizontalpendular
nystagmus,decreased
bone
mineraldensity
NR
OItype
IV,com
mon
variable
OIwith
norm
alsclerae
Moderate,somecasesindistinguishablefrom
type
III,adulth
earing
loss,variablephenotype,
osteoporosis,bonefractures,shortstature,vertebraldeform
ityandscoliosis,triangularface,
norm
alsclerae,hyperm
obility
ofthejoints,m
ilddentinogenesisim
perfectain
somecases
#613849
606633
SP7
12q13.13
NR
#300910
300131
PLS3
Xq23
NR
OItypeV,w
ithcalcificationin
interosseous
mem
branes
#610967
614757
IFITM5
11p15.5
Moderate-severe,sim
ilarto
type
IV,but
with
outd
entin
ogenesisim
perfectaandblue
sclerae,
calcificationof
intraosseusmem
branes
intheforearm
andhyperplasticcallu
sform
ation,
metaphysealbandsadjacent
togrow
thplate(distalfem
ora,proxim
altib
ia,distalradii),
histologicalmesh-lik
eor
irregularbone
pattern
HighALP,high
NTX
Cleidocranialdysplasia(CCD)
#119600
600211
RUNX2
6p21
Skeletaldysplasiacharacterizedby
abnorm
alclavicles(hypoplasticclavicles,aplasticclavicles)
shortribs,cervicalribs,patentsutures
andfontanelles,supernum
eraryteeth,shortstature,
andavarietyof
otherskeletalchanges
NR
•Formefruste,w
ithbrachydactyly
Seeabove+brachydactyly
•Formefruste,dental
anom
alyonly
See
above+delayederuptio
nof
perm
anentteeth,supernumeraryteeth
Hajdu-Cheneysyndrome
#102500
#600275
NOTCH2
1p12p11
Shortstature,coarse
anddysm
orphicfacies,bow
ingof
thelong
bones,vertebralanomalies
NR
Facialfeatures
includehypertelorism,bushy
eyebrows,micrognathia,sm
allm
outhwith
dental
anom
alies,low-setears,and
shortn
eck
Progressivefocalb
onedestruction,includingacroosteolysisandgeneralized
osteoporosis
Additionalandvariablefeatures
includehearingloss,renalcysts,andcardiovascularanom
alies
Winchester-To
rgsyndrome
#259600
#120360
MMP2
16q12.2
Torg
syndrome:multip
le,painless,subcutaneous
nodules(interphalangealjoints,knees,feet,
elbows,pretibial),m
ildtomoderateosteoporosisandosteolysisusually
limitedtothehands
andfeet,w
ideningof
themetacarpaland
metatarsalb
ones
Winchestersyndrome:subcutaneous
nodulesarecharacteristically
absent,severeosteolysisin
thehandsandfeet,and
variousadditio
nalfeaturesincludingcoarse
face,cornealopacities,
gum
hypertrophy,andEKGcoarse
face
HighANA,high
IL-6,highIL-1β
NRnotreported
Osteoporos Int (2015) 26:2529–2558 2543

Tab
le5
Alteredbone
matrixproteins:d
isordersin
collagenmetabolism
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
Osteogenesisim
perfecta(O
I)Alsoknow
nas
brittlebone
disease,itisagenetically
determ
ined
bone
disorder
inwhich
either
defectiveor
insufficient
quantitiesof
collagenmolecules
areproduced
Com
mon
clinicalsigns:increasedbone
fractures.Secondaryfeatures
such
asshortstature,
blue
sclerae,dentinogenesisim
perfectaandhearingloss
may
also
existinaffected
individuals
•Nondeform
ing,with
blue
sclerae(O
Itype
I)Mild
estform
ofOI,dueto
50%
reductionof
theam
ount
ofcollagentype
I;blue
sclerae,
jointh
yperextensibility,normaltooth(O
Itype
IA,w
ithareductionin
theam
ount
ofnorm
alcollagen)
ordentinogenesisim
perfecta(O
Itype
IB,w
ithabnorm
alcollagen),
hearingloss(onsetusually
around
20years),m
itralvalveprolapse,thinskin,increased
fracture
ratethroughout
childhood
(ensueswhenchild
begins
towalk,decreasesafter
puberty,then
increasesaftermenopause
andin
men
aged
60–80years),
biconcaveflattenedvertebrae
#166200
120150
COL1
A1
17q21.33
Nospecificalterations
inbone
markers(low
sclerostin,low
PINPandPICPhave
been
reported)
#166200
120160
COL1
A2
7q21.3
•Perinatally
lethal
(OItype
II)
Mostsevereform
ofOI,neonatallethality,bornprem
aturelyandsm
allfor
gestationalage,
multipleneonatalfractures,shortening
andbowingof
long
boneswith
severeunder
modelingleadingto
crum
pled
long
bones,allv
ertebrae
hypoplastic/crushed,hip
abducted
andkneesflexed,severeosteoporosiswith
intrauterine
fracturesandabnorm
almodeling,skullw
ithsevere
underm
ineralizationwith
wide-open
anterior
andposterior
fontanels,whiteor
blue
sclerae,deathforrespiratoryinsufficiencyandpneumonias
–Ty
peII-A
#166210
120150
COL1
A1
17q21.33
NR
#166210
120160
COL1
A2
7q21.3
NR
–Ty
peII-B
#610682
605497
CRTA
P3p22.3
NR
#610915
610339
LEPRE1
1p34.2
NR
#259440
123841
PPIB
15q22.31
NR
•Progressivelydeform
ing
(OItype
III)
Severe,progressive
with
age,born
prem
aturelyandsm
allfor
gestationalage,m
arked
impairmento
flin
eargrow
th,progressive
deform
ityof
long
bonesandspine,blue/gray
orwhitesclerae,dentinogenesisim
perfecta,severebone
dysplasia,severeosteoporosis
with
multip
lefracturesandbone
deform
ities
(morethan
3prepubertalfractures
per
annum),softandshorterlongbones,jointlaxity,chronicbone
pain,triangularfacewith
frontalb
ossing,dentin
ogenesisim
perfectain
somecases
#259420
120150
COL1
A1
17q21.33
NR
#259420
120160
COL1
A2
7q21.3
NR
#614856
112264
BMP1
8p21.3
Normalto
slightly
high
ALP;
insomepatients:lowP1
CP
and/or
high
UrDPD
/Cr
#610682
605497
CRTA
P3p22.3
NR
#610968
607063
FKBP10
17q21.2
HighAP
2544 Osteoporos Int (2015) 26:2529–2558

Tab
le5
(contin
ued)
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
#259450
607063
FKBP10
17p21.2
+Congenitaljoint
contracture(elbow
andknees)(Bruck
syndrometype
1)HighUrOHP
#610915
610339
LEPRE1
1p34.2
+Sp
ecificradiologicalsign
(Bpopcorn^
epiphyses)
NR
#609220
601865
PLO
D2
3q24
+Congenitaljoint
contracture(elbow
andknees)(Bruck
syndrometype
2)HighUrOHP
#259440
123841
PPIB
15q22.31
NR
#613982
172860
SERPINF1
17p13.3
+Sp
ecifichistologicalsign
(fish-scalelamellarappearance)
NR
#613848
600943
SERPINH1
11q13.5
NR
#615066
611236
TMEM38B
9q31.2
NR
#615220
164820
WNT1
12q13.12
+Developmentald
elay,brain
malform
ation,unilateralcerebellarhypoplasia,congenital
absenceof
theverm
is,pontin
ehypoplasia,hypoplasiaof
themesencephalictectum
,sm
allanteriorcommissure,hypoplasiaof
theoptic
chiasm
,hypoplasiaof
the
hypothalam
us,closed-lip
schizencephaly,type1Chiarim
alform
ation
NR
•Com
mon
variable
moderateOIwith
norm
alsclerae(O
Itype
IV)
Moderate,somecasesindistinguishablefrom
type
III,adulth
earing
loss,variable
phenotype,osteoporosis,bonefractures,shortstature,vertebraldeform
ityandscoliosis,
triangular
face,normalsclerae,hyperm
obility
ofthejoints,m
ilddentinogenesis
imperfectain
somecases
#166220
120150
COL1
A1
17q21.33
NR
#166220
120160
COL1
A2
7q21.3
NR
#615220
164820
WNT1
12q13.12
+Developmentald
elay,brain
malform
ation,unilateralcerebellarhypoplasia,congenital
absenceof
theverm
is,pontin
ehypoplasia,hypoplasiaof
themesencephalictectum
,sm
allanteriorcommissure,hypoplasiaof
theoptic
chiasm
,hypoplasiaof
the
hypothalam
us,closed-lip
schizencephaly,type1Chiarim
alform
ation
NR
#610682
605497
CRTA
P3p22.3
NR
#259440
123841
PPIB
15q22.31
NR
#613849
606633
SP7
12q13.13
SeeTable4
#300910
300131
PLS
3Xq23
SeeTable4
OIwith
calcificationin
interosseous
mem
branes
and/or
hypertrophiccallus
(OItype
V)
#610967
614757
IFITM5
11p15.5
SeeTable4
UnclassifiedOI-lik
edisorders:
Disorderswith
aphenotypesimilarto
OI
•Osteoporosis-pseudoglioma
syndrome(O
PPG)
#259770
603506
LRP5
11q13.1
SeeTable4
•Cole-Carpentersyndrometype
1#112240
176790
P4H
B17q25.3
Craniosynostosis,ocular
proptosis,hydrocephalus,distinctivefacialfeatures,bone
phenotypesimilarto
OItype
IVwith
recurrentd
iaphysealfractures
NR
•Cole-Carpentersyndrometype
2#616294
607186
SEC24D
4q26
Seeabove
NRnotreported
Osteoporos Int (2015) 26:2529–2558 2545

Tab
le6
Alteredbone
matrixproteins:d
isordersof
alkalin
ephosphatase
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
Hypophosphatasia(H
PP)
171760
ALPL
1p36.12
Inborn
errorof
bone
andmineralmetabolism
caused
byvariousdefectsin
tissue-nonspecificalkalin
ephosphatase(TNSA
LP(ALPL
)gene
Low
ALP
•Perinatal
#241500
Alm
ostalwaysfatal,irritability,periodicapneawith
cyanosis,bradycardia,
unexplainedfever,myelophthisicanem
ia(due
toexcess
osteoidand
unmineralized
cartilage),intracranialhemorrhage,profound
bone
hypomineralizationwith
bone
deform
ities,fractures,craniosynostosis,
osteochondralspursthatmay
pierce
theskin
andprotrude
laterally
from
midshafto
ftheulnasandfibulas,dentalabnorm
alities
with
deciduousteeth
poorly
form
ed
Seeexam
inbold
+high
Ca
•Infantile
#241500
Postnatalbutb
efore6monthsof
age,failu
reto
thrive,hypotonia,bulging
oftheanterior
fontanel,raisedintracranialpressure
andpapilledema,proptosis,
mild
hypertelorism,brachycephaly,scleramay
beblue,vitamin
B6-responsive
seizures,rickets
Seeexam
inbold+high
Ca,
high
UrCa,high
Pi(in
heterozygotes),highPi,high
UrPi
•Childhood
#241500
After
6monthsof
age,prem
atureloss
ofprim
aryteeth(before5years)with
out
toothroot
resorptio
n,nonprogressivemyopathy,rickets,radiographicfocal
defectifcartilage
thatprojectfrom
thegrow
thplates
into
themetaphyses
(tongues
ofradiolucency)
Seeexam
inbold
+norm
alCa,
high
Pidueto
high
TmP/GFR
,high
Pi,high
UrPPi
•Adult
#146300
Prem
atureloss
ofprim
aryandsecondaryteeth,severe
dentalcaries,decreased
alveolar
bone,enlargedpulp
cham
ber;osteom
alaciarecurrentfractures,long
bone
pseudofractures,calcium
pyrophosphatearthropathy,chondrocalcinosis
metatarsalstressfracture
Seeexam
inbold
+norm
alCa,
high
Pidueto
high
TmP/GFR
•Odontohypophosphatasia
#146300
Verymild
form
,early-onsetperiodontitis
NR
Hyperphosphatasia
HighALP
•Familialhydiopatic
hyperphosphatasia/juvenile
Paget’s
disease
#239000
602643
TNFRS11B
8q24.12
SeeTable2
•Hyperphosphatasiawith
mentalretardatio
nsyndrome1(H
PMRS1
)
#239300
610274
PIG
V1p36.11
Mentalretardatio
n,variousneurologicabnorm
alities
such
asseizures
and
hypotonia,facialdysm
orphism,variabledegreesof
brachytelephalangy
Seeexam
inbold+high
Pi,
norm
alCa,markedlyhigh
ALP,high
acidphosphatase,
high
uricacid
•Hyperphosphatasiawith
mentalretardatio
nsyndrome2(H
PMRS2
)
#614749
614730
PIG
O9p13.3
Moderatelyto
severely
delayedpsychomotor
developm
ent,mentalretardatio
n,variousneurologicabnorm
alities
such
asseizures
andhypotonia,hypoplasic
nails,longpalpebralfissures,facialdysm
orphism;v
ariabledegreesof
brachytelephalangy
Seeabove
•Hyperphosphatasiawith
mentalretardatio
nsyndrome3(H
PMRS3
)
#614207
615187
PGAP2
11p15.4
Mild
(insomepatients),delayed
psychomotor
developm
ent,mentalretardatio
n,severe,intellectuald
isability,hypotonia,seizures,disorder
insleeppattern
(insomepatients),cerebralatrophy
(insomepatients),m
icrocephaly
Seeabove
•Hyperphosphatasiawith
mentalretardatio
nsyndrome4(H
PMRS4
)
#615716
611801
PGAP3
17q12
Severely
delayedpsychomotor
developm
entw
ithmentalretardatio
n,seizures,
anddysm
orphicfacialfeatures
Seeabove
NRnotreported
2546 Osteoporos Int (2015) 26:2529–2558

Table 7 Mutated bone microenvironment regulators (cytokines and growth factors): disorders of the RANK/RANKL/OPG system
Disease OMIMphenotypenumber
OMIMgene/locusnumber
Gene Chromosomelocation
Phenotype (systemicand bone-specific signs)
Mainbiochemicalalterations
Hereditary familial expansile polyostoticosteolytic dysplasia (FEO)
#174810 603499 TNFRSF11A 18q21.33 See Table 2
Osteopetrosis severe #259710 602642 TNFSF11 13q14.11 See Table 1
#612301 603499 TNFRSF11A 18q21.33
Juvenile Paget’s disease #239000 602643 TNFRSF11B 8q24.12 See Table 2
Table 8 Mutated bone microenvironment regulators (cytokines and growth factors): disorders of the glycosylphosphatidylinositol biosyntheticpathway
Disease OMIMphenotypenumber
OMIMgene/locusnumber
Gene Chromosomelocation
Phenotype (systemic andbone-specific signs)
Mainbiochemicalalterations
Hyperphosphatasia with mentalretardation syndrome 1 (HPMRS1)
#239300 610274 PIGV 1p36.11 See Table 6
Hyperphosphatasia with mentalretardation syndrome 2 (HPMRS2)
#614749 614730 PIGO 9p13.3 See Table 6
Hyperphosphatasia with mentalretardation syndrome 3 (HPMRS3)
#614207 615187 PGAP2 11p15.4 See Table 6
Hyperphosphatasia with mentalretardation syndrome 4 (HPMRS4)
#615716 611801 PGAP3 17q12 See Table 6
Table 9 Mutated bone microenvironment regulators (cytokines and growth factors): disorders of the LRP5
Disease OMIMphenotypenumber
OMIMgene/locusnumber
Gene Chromosomelocation
Phenotype (systemic andbone-specific signs)
Mainbiochemicalalterations
Van Buchem disease type 2, autosomaldominant (VBCH2)
#607636 610274 LRP5 1p36.11 See Table 3
High bone mass (HBM) #607634 614730 LRP5 9p13.3 See Table 3
Osteoporosis-pseudoglioma syndrome,autosomal recessive (OPPG)
#259770 603506 LRP5 11q13.1 See Table 4
OI type III #615220 164820 WNT1 12q13.12 See Table 5
Table 10 Mutated bone microenvironment regulators (cytokines and growth factors): disorders of the bone morphogenetic protein receptor (BMPPR)
Disease OMIMphenotypenumber
OMIMgene/locusnumber
Gene Chromosomelocation
Phenotype (systemic and bone-specific signs) Mainbiochemicalalterations
Fibrodysplasiaossificansprogressiva(FOP)
#135100 102576 ACVR1 2q24.1 Sporadic episodes of painful soft tissue swellings, occur which areoften precipitated by soft tissue injury, intramuscular injections,viral infection, muscular stretching, falls or fatigue, sensorineuralhearing loss, conductive hearing loss, widely spaced teeth,mental retardation, respiratory failure, intermittently progressiveectopic ossification and malformed big toes which are oftenmonophalangic (hallux valgus, malformed first metatarsal, and/ormonophalangism), flat, broad mandibular condyles, scoliosis,small cervical vertebral bodies, proximal medial tibialosteochondromas
High ALP, highUr OHP
Osteoporos Int (2015) 26:2529–2558 2547

Tab
le11
Derangedcalciotropichorm
onalactiv
ity:p
arathyroid
horm
oneexcess
ordeficiency
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
Prim
aryhyperparathyroidism
Endocrine
disorderresulting
from
apersistenthypercalcemiasupportedby
aninadequatesecretionof
PTH;rarelyitoccursin
familialsyndromes.
System
icsigns:renal(polyuria,hypercalciuria,nephrolithiasis)skeletal,
neurom
uscular(m
yopathy,chondrocalcinosis,arthritis),centralnervous
system
(fatigue,cognitivechanges),gastrointestinal(peptic
ulcer,
pancreatitis),cardiovascular(hypertension,reductionQTinterval),
bone-specificsigns:osteoporosiswith
areductionof
bone
mineral
density
mainlyof
thecorticalbone,osteitis
fibrosacysticain
severe
cases(subperiostalresorptionof
thephalange,saltand
pepper
appearance
oftheskull,bone
cysts,brow
ntumorsof
thelong
bones)
HighCa,lowPi,high
UrPi,
high
UrCa,high
PTH:
•Multip
leendocrineneoplasia
type
I(M
EN1)
#131100
613733
MEN1
11q13.1
Enteropancreatic
endocrinetumors,anterior
pituitary
tumors
Seeexam
sin
bold
+otherpituitary
and/or
enteropancreatichorm
onealteratio
ns
•Multip
leendocrineneoplasia
type
II(M
EN2)
#171400
164761
RET
10q11.21
Medullary
thyroidcarcinom
a,pehochromocytom
aSeeexam
sin
bold
(not
always)+high
calcitonin(always),high
catecholam
ine/catecholam
ine
metabolites
•Multip
leendocrineneoplasia
type
IV(M
EN4)
#610755
600778
CDKN1B
12p13.1
Enteropancreatic
endocrinetumors,anterior
pituitary
tumors
Seeexam
sin
bold
+otherpituitary
and/or
enteropancreatichorm
onealteratio
ns
•Hereditary
hyperparathyroidism
jaw-tum
orsyndrome(H
PT-JT)
#145001
607393
HRPT
21q31.2
Fibro-osseoustumorsof
thejaw,benignand/or
malignant
lesions
overthecourse
ofthelifetim
e(m
ostcom
mon:W
ilms’tumor,
papillary
renalcarcinoma),p
olycystic
kidney
disease
Seeexam
sin
bold
•Familialisolated
prim
ary
hyperparathyroidism
(FIH
P)
#145000
613733
MEN1
11q13.1
Seeexam
sin
bold
601199
CaSR
3q21.1
607393
HRPT
21q31.2
•Neonatalsevere
hyperparathyroidism
(NSH
PT)
#239200
601199
CaSR
3q21.1
Life-threatening,severe
osteoporosis
Extremelyhigh
Ca,high
UrCa,low
Pi,highUrPi,highPT
H
•Familialhypocalciuric
hypercalcemiatype
I(H
HC1)
#145980
601199
CaSR
3q21.1
Usually
asym
ptom
atic,rarebone
involvem
ent,pancreatitisand
chondrocalcinosis
HighCa,lowUrCa,CaC
l/CrCl<0.01,
high
Mg,norm
al/highnorm
alPT
H
•Familialhypocalciuric
hypercalcemiatype
II(H
HC2)
#145981
139313
GNA11
19p13.3
Seeabove
•Familialhypocalciuric
hypercalcemiatype
III(H
HC3)
#600740
602242
AP2
S119q13.32
Seeabove
Hypoparathyroidism
Endocrine
deficiency
disorder
characterizedby
lowserum
calcium,
elevated
serum
phosphorus,and
absent
orinappropriatelylow
levelsof
parathyroidhorm
one,system
icsigns:increases
neurom
uscularirritability(cramping,tetany,seizures)ocular
(cataracts),cardiovascular
(prolongationQTinterval),softtissue
calcifications;b
one-specificsigns:increase
incancellous
bone
volume
andcorticalthickness
Low
Ca,high
Pi,low/und
etectable
PTH,low
1,25(O
H) 2D
2548 Osteoporos Int (2015) 26:2529–2558

Tab
le11
(contin
ued)
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
Isolated
hypoparathyroidism
•Autosom
aldominant
hypocalcem
iawith
hypercalciuriatype
1(H
YPO
C1)/Barttersyndrome
subtypeV
#601198
601199
CaSR
3q21.1
Mild
orasym
ptom
atichypocalcem
ia,sym
ptom
atichypocalcem
ia,
rarely
hypercalciuria,kidneystones
andnephrocalcinosis,ectopicand
basalg
angliacalcifications,ifassociated
with
Barttersyndrome:
hypokalemicmetabolicalkalosis,high
reninandaldosterone
Seeexam
sin
bold
+low-normalMg,
high-normalUrCa,lowK(rare),
high
reninandaldosterone(rare)
•Autosom
aldominant
hypocalcem
iawith
hypercalciuriatype
2(H
YPO
C2)
#615361
139313
GNA11
19p13.3
Mild
orasym
ptom
atichypocalcem
ia,sym
ptom
atichypocalcem
ia,
rarely
hypercalciuria,kidneystones
andnephrocalcinosis,
ectopicandbasalg
angliacalcifications
Seeexam
sin
bold
+low-normalMg,
high-normalUrCa
•Familialisolated
hypoparathyroidism
(FIH
),autosomaldominant/autosom
alrecessive
#146200
168450
PTH
11p15.2
Severe,early-onset(congenital),life-threateninghypocalcem
ia,
neonatalseizures,parathyroid
hypoplasia/aplasia
Seeexam
sin
bold
603716
GCMB
6p24.2
Familialisolated
hypoparathyroidism
,X-linked
recessive(H
YPX
)
#307700
–SO
X3
Xq26-q27
Severe,early-onset(congenital),life-threateninghypocalcem
ia,
neonatalseizures,parathyroid
hypoplasia/aplasia
Seeexam
sin
bold
Hypoparathyroidism
incomplex
disorders
•DiGeorgesyndrometype
1(D
GS1
)#188400
602054
TBX1
22q11.2
Thymichypoplasiawith
T-celldeficiency,often
early-onset,congenital
hypocalcem
ia,w
ithcardiacdefects,craniofacialdeform
ities
Neonates:lowCa
Adults:low
Cain
65%
ofcases,lowPT
H
•DiGeorgesyndrometype
2(D
GS2
)#601362
–NEBL
10p14-p13
Thymichypoplasiawith
T-celldeficiency,often
early-onset,
congenitalh
ypocalcemia,cardiac
defects,craniofacialdeform
ities
Seeexam
sin
bold
•Hypoparathyroidism,
sensorineurald
eafness,
renald
isease
(HDR)
#146255
131320
GATA
310p14
Early-onset,congenitaland
severe
hypocalcem
ia,deafness,renal
anom
alies
Seeexam
sin
bold
•Kenny-Caffeysyndrome
type
1(K
CS1
)#244460
604934
TBCE
1q42.3
Early-onsethypocalcem
ia,basalganglialcalcification,nanophthalmos
and
hyperopia,dentalabnorm
alities;m
edullary
stenosisof
long
bones,short
stature,osteosclerosis,corticalthickening
ofthelong
bones,delayed
closureof
theanterior
fontanel
Seeexam
sin
bold
+anem
ia,
low/normalMg
•Kenny-Caffeysyndrome
type
2(K
CS2
)#127000
615292
FAM111A
11q12.1
Seeabove
Anemia(not
always),low
Ca
(transient),high
Pi(transient),
lowPT
H,low
/normalMg
•Hypoparathyroidism,retardation,
dysm
orphism
syndrome(H
RD)
#241410
604934
TBCE
1q42.3
Early-onsethypocalcem
ia,deep-seteyes,microcephaly,thin
lips,
depressednasal,bridge,posteriorly
rotatedears,tetany,mental
retardation,grow
thretardation
Seeexam
sin
bold
•Gracilebone
dysplasia(G
CLEB)
#602361
615292
FAM111A
11q12.1
Severe
hypoparathyroidism
with
high
perinatallethality,thin
long
bones,prem
atureclosureof
basalcranialsutures,stenosisthe
medullary
cavity
ofthelong
bones,microphthalmia,triangular
face
with
frontalb
ossing
Seeexam
sin
bold
•Autoimmune
hypoparathyroidism
polyendocrinesyndrome
type
1(A
PS1)
#240300
607358
AIRE
21q22.3
Hypoparathyroidism
(100
%),chronicmucocutaneous
candidiasis,autoim
muneadrenalinsufficiency
Seeexam
sin
bold
+otherhorm
one
alteratio
ns
Osteoporos Int (2015) 26:2529–2558 2549

Tab
le11
(contin
ued)
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
•Autoimmune
hypoparathyroidism
polyendocrinesyndrome
type
2(A
PS2)
#269200
142860
HLA haplotype
DR3DR4
6p21.32
Hypoparathyroidism,autoimmuneAddison’sdisease,insulin-
dependentd
iabetes,prim
aryhypergonadotropichypogonadism
,autoim
munethyroiddisease,pernicious
anem
ia,alopecia,
vitiligochronicautoim
munehepatitis,hypophysitis,m
yasthenia
gravis,rheum
atoidarthritis,S
jögren’ssyndrome,thrombocytic
purpura
Seeexam
sin
bold
+otherhorm
one
alteratio
ns
Mito
chondriald
iseases:
Severe
multio
rgan
conditions,with
high
perinatallethality,
sometim
esassociated
with
hypoparathyroidism
Seeexam
sin
bold
+high
CSF
proteins
(>100mg/dl),lowCSF
folic
acid,
lacticacidosis,low
serum
and
musclecoenzymeQ
•Kearns-Sayresyndrome(K
SS)
#530000
–mito
c.DNA
•Mito
chondrialm
yopathy,
encephalopathy,lactic
acidosis,
andstroke-likeepisodes
(MELAS)
#540000
–mito
c.DNA
•Mito
chondrialtrifunctio
nal
proteindeficiency
(MTPD
)#609015
600890
HADHA/
HADHB
2p23.3
143450
2p23.3
Medium
chainacylCoA
dehydrogenasedeficiency
(ACADMD)
#201450
607008
ACADM
1p31.1
+Low
plasmacarnitine
levels
2550 Osteoporos Int (2015) 26:2529–2558

Tab
le12
Derangedcalciotropichorm
onalactiv
ity:abnormalparathyroidhorm
onereceptor
signaling
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPhenotype
(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
Gsα
abnorm
alities
•Pseudohypoparathyroidism
Increasedneurom
uscularirritability(spasm
s,tetany,seizures)ocular
(cataracts),cardiovascular
(prolongationQTinterval),softtissue
calcifications
Low
Ca,high
Pi,high
PTH,
low/normal
1-25(O
H) 2D3
-Ty
peIa
(PHP1
A)
#103580
139320
GNAS
(maternal)
20q13.32
Albrighth
ereditary
osteodystrophy
(obesity,round
face,m
ildmental
retardation,basaln
ucleicalcificatio
ns)with
multih
ormonal
resistance
(toTSH
,gonadotropins,G
HRH),increase
incancellous
bone
volumeandcorticalthickness,shortstature,prematureclosure
ofgrow
thplate,brachydactyly(IVmetacarpal),ectopic
ossificatio
ns
See
exam
sin
bold
+lowUr
cAMPin
response
toPTH+
multip
lehorm
oneresistance
-Ty
peIb
(PHP1
B)
#603233
603666
STX16
20q13.32
Resistanceto
PTHwith
outm
ultih
ormonalresistance
See
exam
sin
bold
+lowUr
cAMPin
response
toPTH
610540
GNASA
S120q13.32
139320
GNAS
20q13.32
-Ty
peIc
(PHPIC)
#612462
139320
GNAS
20q13.32
Resistanceto
PTHusually
notassociatedto
otherhorm
onalresistance,
hyperparathyroid
bone
disease(insomecasesosteitisfibrosacystica)
See
exam
sin
bold
+lowUr
cAMPin
response
toPTH
-Ty
peII(PHP2
)#203330
––
–Resistanceto
PTHusually
notassociatedto
resistance
toother
horm
ones
See
exam
sin
bold
+norm
alUr
cAMPin
response
toPTH
•Pseudo-
pseudohypoparathyroidism
(PPHP)
#612463
139320
GNAS
(paternal)
20q13.32
Albrighth
ereditary
osteodystrophy
(obesity,round
face,m
ildmental
retardation,basaln
ucleicalcificatio
ns)with
outm
ultih
ormonal
resistance
NormalCa,norm
alPi,norm
alPTH
•Acrodysostosis1(A
CRDYS1
)#101800
188830
PRKAR1A
17q24.2
Form
ofskeletaldysplasiacharacterizedby
brachydactyly,shortstature,
obesity,faciald
ysostosisandnasalh
ypoplasia(featuresof
Albright
hereditary
osteodystrophy)
Low
ornorm
alCaandPi,low
ornorm
alPTH,±
multip
lehorm
oneresistance
•Acrodysostosis2(A
CRDYS2
)#614613
600129
PDE4D
5q12
Seeabove
See
above
•Progressiveosseous
heteroplasia(POH)
#166350
139320
GNAS
(paternal)
20q13.32
Autosom
aldominantd
isordercharacterizedby
heterotopicossificatio
nsin
thederm
is(osteomacutis)with
possibleextensionto
deep
tissues,intramem
branousossificatio
n;rarely
Albrighth
ereditary
osteodystrophy
NormalCa,norm
alPi,norm
alPTH
•McC
une-Albright
syndrome(M
AS)
#174800
139320
GNAS
20q13.32
Disorderthataffectsthebones,skin
(café-au-laitp
igmentatio
n),and
severalendocrine
tissues
with
possibleprecocious
puberty,
hyperthyroidism,excessive
secretionof
grow
thhorm
one,
Cushing
syndrome,polyostotic
fibrousdysplasia(scar-lik
e/fibrous
tissuein
thebones,oftenconfined
tooneside
ofthebody),some
casesof
hypophosphatem
icosteom
alacia,craniofacialh
yperostosis
Normal-highCa,norm
al-low
Pi,
norm
al-highPT
H,normal/high
1-25(O
H) 2D3+otherendo-
crine
abnorm
alities
PTH/PTHrP
receptor
abnorm
alities
•chondrodysplasiaswith
mineralionhomeostasis
abnorm
alities
Chondrodysplasias
with
mineralionhomeostasisabnorm
alities
dueto
alteratio
nsof
thePTH/PTHrP
receptor
gene
(PTHR1)
gene,w
hich
usually
mediatestheactio
nsof
thetwolig
ands:P
THandPTH-related
peptide
Osteoporos Int (2015) 26:2529–2558 2551

Tab
le12
(contin
ued)
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
-Metaphyseal
chondrodysplasia
Jansen
type
(JMC)
#156400
168468
PTHR1
3p21.31
Highskullv
ault,
flattening
ofthenose
andforehead,low
-setears,
hypertelorism,higharched
palate,m
icrognathia,retrognathia,
kyphoscolio
siswith
bell-shaped
thorax
andwidened
costochondral
junctio
ns,m
etaphysealenlargem
ento
fthejoints,frontonasalhyperplasia,
shortlegsandrelativ
elylong
arms;in
youngerpatients:enlargem
ento
fmetaphyseswith
awidezone
ofirregularcalcifications
(lesions
similar
torickets)
Atp
uberty:partially
calcifiedcartilage
thatprotrude
into
diaphysis
Lateadolescence:cartilaginous
tissueinthemetaphysisdisappears,sclerosis
andthickening
ofthebase
ofskullw
ithcranialaudito
ryandopticalnerve
compression
HighCa,lowPi,highUrPi,high
UrCa,high
UrcA
MP,
suppressed/lo
w-normalPTH
-Chondrodysplasia
Blomstrand
type
(BOCD)
#215045
168468
PTHR1
3p21.31
Early
lethality,defectsof
mam
maryglandandof
toothdevelopm
ent,
hypoplasiaof
nasal,mandibularandfacialbones,shortthick
ribs,
hypoplasiaof
thevertebrae,hyperdensity
ofthewholeskeleton,
markedlyadvanced
ossificatio
nLo
ngbones:extrem
elyshortand
poorly
modeled,nozonesof
chondrocyteproliferationandof
columnform
ationarelacking
Low
Ca,high
PTH,low
UrPi,
high
UrcA
MP
-Eiken
familialskeletal
dysplasia
#600002
168468
PTHR1
3p21.31
Multip
leepiphysealdysplasia
Normal-highPT
H
-Multip
leenchondrom
atosis,
Ollier
type
#166000
168468
PTHR1
3p21.31
Softtissuehemangiom
as(M
affuccisyndrom
e),m
ultip
leenchondrom
aswith
skeletaldeform
ities
andpotentialriskformalignant
change
tochondrosarcoma
Slig
htly
high
PTH
147700
IDH1
2q34
147650
IDH2
15q26.1
2552 Osteoporos Int (2015) 26:2529–2558

Tab
le13
Derangedcalciotropichorm
onalactiv
ity:d
isordersof
vitamin
Dmetabolism
andactio
n
Disease
OMIM
phenotype
number
OMIM
gene/
locus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
Disordersof
vitamin
Dmetabolism
Alteratio
nof
vitamin
Dmetabolism
causes
defectsin
thegrow
thplateandbone
demineralizationthatiscalledricketsin
child
ren
andosteom
alaciain
adults
Low
Ca,lowPi,high
bone
ALP
•VitaminDhydroxylation-deficient
ricketstype
1A(V
DDR1A
)#264700
609506
CYP
27B1
12q14.1
Growth
retardation,muscleweakness,irritability,congenital
ricketswith
enlarged
costochondraljunctions
oftheribs,pectus
carinatum,m
etaphysealflaringof
thewristsor
ankles,genus
varus,frontalb
ossing
enlarges
suturesandfontanelsor
craniotabes,long
bone
deform
ities
See
exam
sin
bold
+low1,25(O
H) 2D,
norm
al25
OHD,slig
htlyhigh
PTH,
generalized
aminoaciduria
•VitaminDhydroxylation-deficient
ricketstype
1B(V
DDR1B
)#600081
608713
CYP
2R1
11p15.2
Hypotonia,m
uscleweakness,difficulty
inwalking,difficulty
instanding,congenitalricketswith
fractures,bone
pain,sparsebone
trabeculae,thinbony
cortex,delayed
opacificationof
theepiphyses,
widened,distorted
epiphyses,frayed,irregular
metaphyses,lower
limbdeform
ities,bow
ingof
thelegs
Seeexam
sin
bold
+norm
al1,25(O
H) 2D,decreased
25OHD
Disordersof
vitamin
Dactio
n
•Vitamin
D-dependent
rickets
type
2A(V
DDR2A
)#277440
601769
VDR
12q13.11
Growth
retardation,muscleweakness,convulsion
forhypocalcem
ia,
bone
pain
atthelower
extrem
ities
thatdelays
theirdevelopm
ent
ofwalking,dentalcariesor
hypoplasiaof
theteeth,scalpandtotal
alopecia,m
ilddeafness,congenitalricketswith
fracture
and
pseudofractures,sparse
bone
trabeculae,thinbony
cortex,delayed
opacificationof
theepiphyses,widened,distorted
epiphyses,frayed,
irregularmetaphyses,lower
limbdeform
ities,bow
ingof
thelegs,
curvatures
ofthefemur,tibia,fibula,enlargem
ento
fthewrists,
enlargem
ento
ftheankles,subperiostealerosions
dueto
secondary
hyperparathyroidism
High1,25(O
H) 2Dnorm
al25
OHD,
markedlyhigh
PTH,m
arkedlyhigh
bone
ALP
•Vitamin
D-dependent
ricketstype
2B(V
DDR2B
)#600785
––
–Seeabove
Osteoporos Int (2015) 26:2529–2558 2553

Tab
le14
Derangedcalciotropichorm
onalactivity
:disordersof
phosphatehomeostasis
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
Hypophosphatemicdisorders
Group
ofdisorderswith
similarclinicalandbiochemical
features
representedby
hypophosphatem
ia,
hyperphosphaturia
Phosphatonin-related
disorders:
HighUrP,
lowPi,lowrena
lTmP/G
FR,
norm
alCa,low-normalUrCa,no
rmal
25OH
D;low-normal
1,25(O
H) 2D,
high
bone
ALP
•Autosom
aldominant
hypophosphatem
icrickets
(ADHR)
#193100
605380
FGF23
12p13.32
Fatig
ueandmuscleweakness,shortstature,earlyonset
(1–3
years):severebowingof
lower
extrem
ities,rickets
with
enlarged
costochondraljunctions
oftheribs;lateonset
(puberty):bone
pain
(nobowingof
lower
extrem
ities)
Seeexam
sin
bold
+high
intactFG
F23,
norm
alPTH
•X-linked,dominant,
hypophosphatem
icrickets
(XLHR)
#307800
300550
PHEX
Xp22.11
Latedentition,tooth
abscessessecondaryto
poor
mineralization,bowingof
lower
extrem
ities,enlarged
costochondraljunctions
oftheribs,pectum
carinatum,
metaphysealflaringof
thewristsor
ankles,genus
varus,
frontalb
ossing
enlarges
suturesandfotanelsor
craniotabes
Seeexam
sin
bold
+high
intactFG
F23,
norm
alPTH,rarelylowGH
•Osteoglophonicdysplasia
(OGD)
#166250
136350
FGFR1
9p11.23-
p11.22
Macroglossia,hypertrophyof
thegums,severe
dwarfism
,mandibularprognathism,frontalbossing,andproptosis;
rickets/osteom
alacia,severecraniofacialabnorm
alities,
bone
dysplasia
Seeexam
sin
bold
+high/normalintact
FGF2
3,norm
alPT
H
•Autosom
alrecessive
hypophosphatem
icrickets
type
1(A
RHR1)
#241520
600980
DMP1
4q22.1
Shortstature;lim
itedmovem
ento
fspineandhip,calcification
ofthelig
amentsatthebony
insertions
sites,high
bone
density
atthebase
ofskull,clavicleandribanom
alies,
enthesopathies
Seeexam
sin
bold
+high
intactFG
F23,
norm
alPTH
•Autosom
alrecessive
hypophosphatem
icricketstype
2(A
RHR2)
#613312
173335
ENPP1
6q23.2
See
above
•Arterialcalcificatio
nof
infancy
#208000
173335
ENPP1
6q23.2
Shortstature,deafness,conductive(insomepatients),angioid
retin
alstreaks(insomepatients),coronaryandgeneralized
artery
calcification,
cardiacdysfunction,periarticular
calcification,hypophosphatem
icrickets,pseudoxanthoma
Low
Pi
•Hypophosphatemicricketswith
hyperparathyroidism
(HRH)
#612089
604824
KLOTH
O13q13.1
Kidneystones,rickets
Seeexam
sin
bold
+high
PTH
(normalintactFGF2
3)
Phosphatonin-unrelated
disorders:
HighUrP,
lowPi,lowrena
lTmP/G
FR,
norm
alcalcium,h
ighUrCa,
low/normal
PTH,n
ormal
25OH
D,
high
1,25(O
H) 2D,h
ighbo
neALP
•Hereditary
hypophosphatem
icricketswith
hypercalciuria
(HHRH)
#241530
609826
SLC34A3
(NPTIIc)
9q34.3
Kidneystone,nephrocalcinosis,rickets/osteomalacia
Seeexam
sin
bold
+norm
al/highCa,
norm
alintactFG
F23
2554 Osteoporos Int (2015) 26:2529–2558

Tab
le14
(contin
ued)
Disease
OMIM
phenotype
number
OMIM
gene/lo
cus
number
Gene
Chrom
osom
elocatio
nPh
enotype(systemicandbone-specificsigns)
Mainbiochemicalalteratio
ns
•Hypophosphatemia
nephrolithiasisosteoporosis
type
1(N
PHLOP1
)
#612286
182309
SLC34A1
(NPTIIa)
5q35.3
Kidneystones,nephocalcinosis,osteoporosis
Seeexam
sin
bold
+norm
alCa,norm
alintactFGF2
3
•Hypophosphatemia
nephrolithiasisosteoporosis
type
2(N
PHLOP2
)
#612287
604990
SLC9A
3R1
17q25.1
See
above
Hyperphosphatem
icdisorders
Tum
oralcalcinosis
•Hyperphosphatem
icfamilial
tumoralcalcinosis
(HFT
C)/hyperostosis
hyperphosphatemia
syndrome(H
HS)
#211900
605380
FGF23
12p13.32
Periarticular
cysticandsolid
tumoralcalcifications
with
hyperphosphatemiaandhypophosphaturiaandelevated
serum
ofcalcitriol,softtissuemassesaround
major
joints,
dentalabnorm
alities,ocularinvolvem
entw
ithrangefrom
angioidstreaksto
cornealcalcificatio
ndepositsandneuronal
calcifications,alteredskeletalmineralization,low/normal
bone
mass
Low
UrP,high
Pi,high
TmP/GFR
,norm
alCa,norm
alUrCa,norm
alPTH,
norm
al25
OHD,high1,25(O
H) 2D,
lowintactFGF2
3
601756
GALNT3
2q24.3
604824
KLOTH
O13q13.1
Normophosphatemicdisordersresemblinghyperphosphatemicdisorders
•Normophosphatemicfamilial
tumoralcalcinosis(N
FTC)
#610455
610456
SAMD9
7q21.2
Reddish
tohyperpigmentedskin
lesions,softtissuemasses
attheextrem
ities,severeconjunctivitis,severe
gingivitis,
noalteredskeletalmineralization
NormalPi,normalUrP
Osteoporos Int (2015) 26:2529–2558 2555

Conclusions
In conclusion, with the present report, the IOF’s SRD-WGprovides for the first time a metabolic classification forRGMBDs. Surprisingly perhaps, bone remodeling phenotypeis not known for all diseases of metabolic origin. However,knowledge of the metabolic pathway that characterizes a giv-en disorder may help in the management of such patients.Indeed, for the majority of these disorders, disease-targetedtherapies are still missing, restricting the choice betweenantiresorptive and anabolic agents in complicated syndromes,often in children. The metabolic profile may help in selectingthe most appropriate pharmacological treatment in patientsaffected by RGMBDs. It is intended that this taxonomic paperwill provide the core and the structural framework for thedevelopment of a web-based atlas for rare metabolic skeletaldiseases by the International Osteoporosis Foundation with adetailed description and a guided diagnostic workup for eachdisease, leading to a targeted therapeutic approach on the basisof the available metabolic hallmarks and structuralphenotypes.
Acknowledgments This paper was supported by the IOF.
Conflicts of interest None.
References
1. (2013) Report on the state of the art of rare disease activities in Europe;European Union Committee of Expert on Rare Disease. Overview ofrare disease activities in Europe. Part I; pp. 1–78 http://www.eucerd.eu/upload/file/Reports/2013ReportStateofArtRDActivities.pdf
2. Ayme S, Schmidtke J (2007) Networking for rare diseases: a neces-sity for Europe. Bundesgesundheitsbl GesundheitsforschGesundheitsschutz 50:1477–1483
3. Available from: National Organization for Rare Diseases (NORD)of the United States: www.rarediseases.org. Accessed Jan 2015
4. Haffner ME, Whitley J, Moses M (2002) Two decades of orphanproduct development. Nat Rev Drug Discov 10:821–825
5. BraunMM, Farag-El-Massah S, Xu K, Coté TR (2010) Emergenceof orphan drugs in the United States: a quantitative assessment ofthe first 25 years. Nature Reviews Drug Discovery 9:519–522
6. For a list of rare diseases and their prevalence, please consult theOrphanet Reports Series BPrevalence of rare diseases: bibliographicdata^, Orphanet Report Series, Rare Diseases collection, Number 1:Listed in alphabetical order of diseases, http://www.orpha.net/orphacom/cahiers/docs/GB/Prevalence_of_rare_diseases_by_alphabetical_list.pdf. Accessed Jan 2015
7. Villa S, Compagni A, Reich MR (2009) Orphan drug legislation:lessons for neglected tropical diseases. Int J Health Plann Manage24:27–42
8. (2010) 5th European conference on rare diseases. European refer-ence networks & centers of expertise for rare diseases, pp. 1–75
9. Available from: EUROPLAN website: www.europlanproject.eu.Accessed Jan 2015
10. Commission Regulation (EC) No 847/2000 of 27 April 2000; OJ L103, 28.4.2000
11. Macarthur D (2011) Orphan drugs in Europe: pricing, reimburse-ment, funding & market access issues, Edition www.justpharmareports.com
12. Inventory of Community andMember States’ incentive measures toaid the research, marketing, development and availability of orphanmedicinal products. Revision 2005, http://ec.europa.eu/health/files/orphanmp/doc/inventory_2006_08_en.pdf. Accessed Jan 2015
13. Available from: Orphabioetic foundation: www.orphanbiotec-foundation.com. Accessed Jan 2015
14. Commission Regulation (EC) No 847/2000 of 27April 2000 layingdown the provisions for implementation of the criteria for designa-tion of a medicinal product as an orphan medicinal product anddefinitions of the concepts ‘similar medicinal product’ and ‘clinicalsuperiority’. Off J Eur Commun 103/5-103/8
15. Available from: Orphanet Activity Report 2012, http://www.orpha.net/orphacom/cahiers/docs/GB/ActivityReport2012.pdf. AccessedJan 2015
16. Thorat C, Xu K, Freeman SN, Bonnel RA, Joseph F, Phillips MI,Imoisili MA (2012) What the Orphan Drug Act has done lately forchildren with rare diseases: a 10-year analysis. Pediatrics 129:516–521
17. Forman J, Taruscio D, Llera VA, Barrera LA, Coté TR, Edfjall C,Gahved D, Haffner ME, Nishimura Y, Posada M, Tambuyzer E,Groft SC, Henter J-I (2012) The need for world-wide policy andactions plans for rare diseases. Acta Pediatr 101:805–807
18. Roldán EJA (2013) Proceedings from the VIII InternationalConference on Rare Diseases and Orphan Drugs (ICORD), StPetersburg (Russia). Rare J 1(suppl 1):1–48
19. Mäkitie O (2011) Molecular defects causing skeletal dysplasias.Camacho-Hübner C, Nilsson O, SŠvendahl L (eds) Cartilage andbone development and its disorders. Endocr Dev. Basel, Karger, vol21, pp 78–84
20. (1970) International nomenclature of constitutional diseases ofbones. Ann Radiol (Paris) 13(7):455–464
21. (1971a) A nomenclature for constitutional (intrinsic) diseases ofbones. J Pediatr 78(1):177–179
22. (1971b) International nomenclature of constitutional bone diseases.Constitutional bone diseases without known pathogenesis. Arch FrPediatr 28(5):553–557
23. Nomenclature for constitutional (intrinsic) diseases of bones.(1971c) Pediatrics 47(2):431–344. Nomenclature for the constitu-tional (intrinsic) diseases of bone. Radiology. 1971d; 99(3):699–702
24. McKusick VA, Scott CI (1971) A nomenclature for constitutionaldisorders of bone. J Bone Joint Surg Am 53(5):978–986
25. Warman ML, Cormier-Daire V, Hall C, Krakow D, Lachman R,LeMerrer M, Mortier G, Mundlos S, Nishimura G, Rimoin DL,Robertson S, Savarirayan R, Sillence D, Spranger J, Unger S,Zabe B, Superti-Furga A (2011) Nosology and classification ofgenetic skeletal disorders—2010 revision. Am J Med Genet A155A(5):943–968
26. Superti-Furga A, Unger S (2007) Nosology and classification ofgenetic skeletal disorders: 2006 revision. Am J Med Genet A143(1):1–18
27. Boyce BF, Zuscik MJ, Xing L (2013) Biology of bone and carti-lage. In: Thakker RV, Whyte MP, Eisman JA, Igarashi T (eds) 1edn. Genetics of bone biology and skeletal diseases. Ch. 1 pp. 3–24
28. Pagani F, Francucci CM, Moro L (2005) Markers of bone turnover:biochemical and clinical perspectives. J Endocrinol Invest 28:8–13
29. Berndt TJ, Schiavi S, Kumar R (2005) Phosphatonins and the reg-ulation of phosphorus homeostasis. Am J Renal Physiol 289:1170–1182
30. Kumar R, Riggs R (1980) Pathologic bone physiology. In: UristMR (ed) Fundamental and clinical bone physiology. Lippincott,Philadelphia, pp 394–406
2556 Osteoporos Int (2015) 26:2529–2558

31. Schiavi SC, Moe OW (2002) Phosphatonins: a new class of phos-phate regulating proteins. Curr Opin Nephrol Hypertens 11:423–430
32. Brown EM, MacLeod RJ (2001) Extracellular calcium sensing andextracellular calcium signaling. Physiol Rev 81:239–297
33. Alfadda TI, Saleh AM, Houllier P, Gaidel JP (2014) Calcium-sensing receptor 20 years later. Am J Physiol 307(3):C221–C231
34. Kumar R (1990) Vitamin D metabolism and mechanisms of calci-um transport. J Am Soc Nephrol 1:30–42
35. Fleisch H (1980) Homeostasis of inorganic phosphate. In: Urist MR(ed) Fundamental and clinical bone physiology. Lippincott,Philadelphia, pp 268–282
36. Burtis WJ,Wu T, Bunch C,Wysolmerski JJ, Insogna KL, Weir EC,Broadus AE, Stewart AF (1987) Identification of a novel 17,000-dalton parathyroid hormone-like adenylate cyclase-stimulating pro-tein from a tumor associated with humoral hypercalcemia of malig-nancy. J Biol Chem 262:7151–7156
37. Kronenberg HM (2003) Developmental regulation of the growthplate. Nature 2423:332–336
38. Juppner H, Silve C (2013) Genetic disorders affecting PTH/PTHrPreceptor function. In: Thakker RV, Whyte MP, Eisman JA, IgarashiT (eds) Genetics of bone biology and skeletal diseases. Ch. 28, pp.441–457
39. Qin C, Baba O, Butler WT (2004) Post-translational modificationsof sibling proteins and their roles in osteogenesis anddentinogenesis. Crit Rev Oral Biol Med 15:126–136
40. Econs MJ, Drezner MK (1994) Tumor induced osteomalaciaunveiling a new hormone. N Engl J Med 330:1679–1681
41. Quarles LD (2003) FGF23, PHEX, and MEPE regulation of phos-phate homeostasis and skeletal mineralization. Am J PhysiolEndocrinol Metab 285:E1–9
42. Boyce BF, Yao Z, Zing L (2009) Osteoclasts have multiple roles inbone in addition to bone resorption. Crit Rev Eukaryot Gene Expr19:171–80
43. Fukuchi M, Fukai Y, Masuda N, Miyazaki T, Nakajima M, SohdaM, Manda R, Tsukada K, Kato H, Kuwano H (2002) High-levelexpression of the Smad ubiquitin ligase Smurf2 correlates with poorprognosis in patients with esophageal squamous cell carcinoma.Cancer Res 62:7162–7165
44. Takayanagi H (2007) Osteoimmunology: shared mechanisms andcrosstalk between the immune and bone systems. Nat Rev Immunol7:292–304
45. Hofbauer LC, Kühne CA, Viereck V (2004) The OPG/RANKL/RANK system in metabolic bone diseases. J MusculoskeletNeuronal Interact 4:268–75
46. Henriksen K, Bollerslev J, Everts V, Karsdal MA (2011) Osteoclastactivity and subtypes as a function of physiology and pathology—implications for future treatments of osteoporosis. EndocrineReviews 32:31–63
47. Ross PF (2013) Osteoclast biology and bone resorption. In: Primeron the metabolic bone diseases and disorders of mineral metabo-lism. Official publication of the American Society for Bone andMineral Research (ASBMR) 8 edn Ch. 3 pp.25–33
48. Blair HC, Teitelbaum SL, Ghiselli R, Gluck S (1989) Osteoclasticbone resorption by a polarized vacuolar proton pump. Science 245:855–857
49. Blair HC, Teitelbaum SL, Tan HL, Koziol CM, Schlesinger PH(1991) Passive chloride permeability charge coupled to H(+)-ATPase of avian osteoclast ruffled membrane. Am J Physiol 260:C1315–C1324
50. Josephsen K, Praetorius J, Frische S, Gawenis LR, Kwon TH, AgreP, Nielsen S, Fejerskov O (2009) Targeted disruption of the Cl/HCO3 exchanger Ae2 results in osteopetrosis in mice. Proc NatlAcad Sci USA 106:1638–1641
51. Baron R, Neff L, Louvard D, Courtoy PJ (1985) Cell-mediatedextracellular acidification and bone resorption: evidence for a low
pH in resorbing lacunae and localization of a 100-kD lysosomalmembrane protein at the osteoclast ruffled border. J Cell Biol 101:2210–2222
52. Frattini A, Orchard PJ, Sobacchi C, Giliani S, Abinun M, MattssonJP, Keeling DJ, Andersson AK,Wallbrandt P, Zecca L, NotarangeloLD, Vezzoni P, Villa A (2000) Defects in TCIRG1 subunit of thevacuolar proton pump are responsible for a subset of human auto-somal recessive osteopetrosis. Nat Genet 25:343–346
53. Karsdal MA, Henriksen K, Sørensen MG, Gram J, Schaller S,Dziegiel MH, Heegaard AM, Christophersen P, Martin TJ,Christiansen C, Bollerslev J (2005) Acidification of the osteoclasticresorption compartment provides insight into the coupling of boneformation to bone resorption. Am J Pathol 166:467–47
54. Henriksen K, Gram J, Schaller S, Dahl BH, Dziegiel MH,Bollerslev J, Karsdal MA (2004) Characterization of osteoclastsfrom patients harboring a G215R mutation in ClC-7 causingautosomal dominant osteopetrosis type II. Am J Pathol 164:1537–1545
55. Arnett TA (2008) Extracellular pH regulates bone cell function. JNutr 138:415S–418S
56. Tolar J, Teitelbaum SL, Orchard PJ (2004) Osteopetrosis. N Engl JMed 351:2839–2849
57. Jansen ID, Mardones P, Lecanda F, de Vries TJ, Recalde S, HoebenKA, Schoenmaker T, Ravesloot JH, van Borren MM, van EijdenTM, Bronckers AL, Kellokumpu S, Medina JF, Everts V, OudeElferink RP (2009) Ae2a, b-deficient mice exhibit osteopetrosis oflong bones but not of calvaria. FASEB J 23:3470–3481
58. Gowen M, Lazner F, Dodds R, Kapadia R, Field J, Tavaria M,Bertoncello I, Drake F, Zavarselk S, Tellis I, Hertzog P, DebouckC, Kola I (1999) Cathepsin K knockout mice develop osteopetrosisdue to a deficit in matrix degradation but not demineralization. JBone Miner Res 14:1654–1663
59. Calvo MS, Eyre DR, Gundberg CM (1996) Molecular basis andclinical application of biological markers of bone turnover. EndocrRev 17:333–368
60. Singer FR, Eyre MD (2008) Using biochemical markers of boneturnover in clinical practice. Cleveland Clinic Journal of Medicine75:739–750
61. Bergmann P, Body JJ, Boonen S, Boutsen Y, Devogelaer JP,Goemaere S, Kaufman JM, Rozenberg S, Reginster JY (2009)Evidence-based guidelines for the use of biochemical markers ofbone turnover in the selection and monitoring of bisphosphonatetreatment in osteoporosis: a consensus document of the BelgianBone Club. Int J Clin Pract 63:19–26
62. Suwanwalaikorn S, Van Auken M, Kang MI, Alex S, BravermanLE, Baran DT (1997) Site selectivity of osteoblast gene expressionresponse to thyroid hormone localized by in situ hybridization. AmJ Physiol 272(2 Pt 1):E212–217
63. Kasperk C, Wergedal J, Strong D, Farley J, Wangerin K, Gropp H,Ziegler R, Baylink DJ (1995) Human bone cell phenotypes differdepending on their skeletal site of origin. J Clin Endocrinol Metab80(8):2511–2517
64. Orimo H (2010) The mechanism of mineralization and the role ofalkaline phosphatase in health and disease. J Nippon Med Sch 77:4–12
65. Mortland M, Robison R (1929) The preparation and use of thephosphatase. Biochem J 23:237–242
66. Seibel MJ (2005) Biochemical markers of bone turnover: part I:biochemistry and variability. Clin Biochem Rev 26:97–122
67. Gundberg CM, Markowitz ME, Mizruchi M, Rosen JF (1985)Osteocalcin in human serum: a circadian rhythm. J ClinEndocrinol Metab 60:736–739
68. Delmas PD, Wilson DM, Mann KG, Riggs BL (1983) Effect ofrenal function on plasma levels of bone Gla-protein. J ClinEndocrinol Metab 57:1028–1030
Osteoporos Int (2015) 26:2529–2558 2557

69. Bergmann P, Body JJ, Boonen S, Boutsen Y, Devogelaer JP,Goemaere S, Kaufman JM, Reginster JY, Gangji V, Members ofAdvisory Board on Bone Markers (2009) Evidence-based guide-lines for the use of biochemical markers, bone turnover: biomarkersof bone turnover. Int J Clin Pract CME 63(1):19–26
70. Keen RW (2013) Sclerosing and displastic bone diseases. In:Primer on the metabolic bone diseases and disorders of mineralmetabolism. 8 edn, Wiley, Ames, section VIII, pp 767–842
71. Franz-Odendaal TA, Hall BK, Witten PE (2006) Buried alive: howosteoblasts become osteocytes. Dev Dyn 235:176–190
72. Burger EH, Klein-Nulend J (1999)Mechanotransduction in bone—role of the lacuno-canalicular network. FASEB J 13(Suppl):S101–112
73. Li X, Liu P, Liu W, Maye P, Zhang J, Zhang Y, Hurley M, Guo C,Boskey A, Sun L, Harris SE, Rowe DW, Ke HZ, Wu D, Liu LX(2005) Dkk2 has a role in terminal osteoblast differentiation andmineralized matrix formation. Nat Genet 37:945–952
74. Bonewald LF, Johson ML (2008) Osteocytes, mechanosensing andWnt signaling. Bone 42:606–615
75. Tatsumi S, Ishii K, Amizuka N, Li M, Kobayashi T, Kohno K, ItoM, Takeshita S, Ikeda K (2007) Targeted ablation of osteocytesinduces osteoporosis with defective mechanotransduction. CellMetabolism 5:464–475
76. Moriishi T, Fukuyama R, Ito M, Miyazaki T, Maeno T, Kawai Y,Komori H, Komori T (2012) Osteocyte network; a negative regu-latory system for bonemass augmented by the induction of Rankl in
osteoblasts and Sost in osteocytes at unloading. PLoS ONE 7(6):e401–443
77. Bonewald LF (2007) Osteocytes as dynamic multifunctional cells.Ann N YAcad Sci 1116:281–290
78. Kneissel M (2009) The promise of sclerostin inhibition for thetreatment of osteoporosis. IBMS BoneKEy 6:259–264
79. Dalla SL, Bonewald LF (2010) Dynamics of the transition fromosteoblast to osteocyte. Ann N YAcad Sci 1192:437–443
80. Guo D et al (2006) Identification of proteins involved in cytoskel-etal rearrangement, anti-hypoxia and membrane channels in osteo-cytes over osteoblasts. J Bone Miner Res 21:S168
81. Gentili C, Cancedda R (2009) Cartilage and bone extracellular ma-trix. Curr Pharm Des 15:1334–1348
82. Robey PG, Boskey AL. The composition of bone. In: Primer on thebone metabolic diseases and disorders of mineral metabolism.Seventh ed. Official publication of the American Society for Boneand Mineral Research Ch. 6 pp. 32–38
83. Rossert J, de Crombrugghe B (1996) Type I collagen: structure,synthesis, and regulation. In: JP Bilezikian, Raisz LC, Rodan Ga(eds) Principle of bone biology. 1st edn. Ch. 10 pp. 127–142
84. Lian JB, Stein GS (2006) The cells of bone. In: Seibel MJ, RobinsS, Bilezikian JP (eds) Dynamics of bone and cartilage metabolism.Academic, San Diego
85. Lee NK, Sowa H, Hinoi E, Ferron M, Ahn JD, Confavreux C,Dacquin R, Mee PJ, McKee MD, Jung DY, Zhang Z, Kim JK,Mauvais-Jarvis F, Ducy P, Karsenty G (2007) Endocrine regulationof energy metabolism by the skeleton. Cell 130:456–469
2558 Osteoporos Int (2015) 26:2529–2558
Related Documents