Research Report Target-specific rCBF changes induced by 0.3-T static magnetic field exposure on the brain Seungyeon Kim a,1 , Yong-An Chung b,1 , Chang-Uk Lee c , Jeong-Ho Chae c , Rahyeong Juh d , Jaeseung Jeong a, ⁎ a Department of Bio and Brain Engineering, Korea Advanced Institute of Science and Technology (KAIST), Yuseong-gu, Kuseong-dong, 373-1 Daejeon, 305-701 South Korea b Department of Radiology, Institute of Catholic Integrative Medicine, Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Incheon, 403-720 Republic of Korea c Department of Psychiatry, College of Medicine, The Catholic University of Korea, Seoul, 150-713 Republic of Korea d Department of Biomedical Engineering, College of Medicine, The Catholic University of Korea, Seoul, 150-713 Republic of Korea ARTICLE INFO ABSTRACT Article history: Accepted 22 October 2009 Available online 30 October 2009 The magnetic field has been regarded as both harmful and beneficial for its applications on human brains including transcranial magnetic stimulation (TMS), but its effects still remain in question. Here, we determined using single photon emission computed tomography (SPECT) if 0.3-T static magnetic field could alter regional cerebral blood flow (rCBF) in target and other brain regions in healthy subjects. The permanent static magnet (0.3 T, unipolar, disk shaped, 4 cm diameter and 1 cm thick) was placed on the right frontotemporal region of the brain for each of 14 healthy subjects. Tc-99m ECD perfusion SPECT was taken to compare the CBF patterns in the subjects exposed to the static magnet field with those of the resting and sham conditions. We found that the rCBF was significantly increased in the right frontal and parietal regions and the right insula. On the other hand, rCBF was rather decreased in the left frontal and left parietal regions (P < 0.05). These results of this basic study suggest that 0.3-T static magnetic field induces an increase in rCBF in the targeted brain areas non- invasively, which may result from a decrease in rCBF in contralateral regions. © 2009 Published by Elsevier B.V. Keywords: Static magnetic field Cerebral blood flow SPECT SPM 1. Introduction Magnetic fields have long been considered as a potentially beneficial therapeutic application. When diamagnetic materi- als such as fibrin, collagen, osteoblasts and red blood cells (RBC) are exposed to static gradient magnetic fields, they align either parallel or perpendicular to the direction of the magnetic field depending on the magnetic anisotropy of the materials in question (Torbet et al., 1981). Induced magnetic fields in the brain might affect the membrane or synaptic properties of neurons, brain functions and thus behavior. Many studies have consequently applied magnetic fields to proximal areas of pain and inflammation of patients to alleviate pain and discomfort due to arthritis, headaches, sciatica, heel spurs, migraine and so forth (for example, Stuchly, 1986). The exposure to magnetic fields had opened up a new range of applications to facilitate bone growth and speed the healing of fractures. BRAIN RESEARCH 1317 (2010) 211 – 217 ⁎ Corresponding author. Fax: +82 42 350 4310. E-mail address: [email protected] (J. Jeong). 1 Both authors are equally contributed. 0006-8993/$ – see front matter © 2009 Published by Elsevier B.V. doi:10.1016/j.brainres.2009.10.057 available at www.sciencedirect.com www.elsevier.com/locate/brainres

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

B R A I N R E S E A R C H 1 3 1 7 ( 2 0 1 0 ) 2 1 1 – 2 1 7
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r . com/ loca te /b ra i n res
Research Report
Target-specific rCBF changes induced by 0.3-T static magneticfield exposure on the brain
Seungyeon Kima,1, Yong-An Chungb,1, Chang-Uk Leec, Jeong-Ho Chaec,Rahyeong Juhd, Jaeseung Jeonga,⁎aDepartment of Bio and Brain Engineering, Korea Advanced Institute of Science and Technology (KAIST), Yuseong-gu, Kuseong-dong,373-1 Daejeon, 305-701 South KoreabDepartment of Radiology, Institute of Catholic Integrative Medicine, Incheon St. Mary's Hospital, College of Medicine,The Catholic University of Korea, Incheon, 403-720 Republic of KoreacDepartment of Psychiatry, College of Medicine, The Catholic University of Korea, Seoul, 150-713 Republic of KoreadDepartment of Biomedical Engineering, College of Medicine, The Catholic University of Korea, Seoul, 150-713 Republic of Korea
A R T I C L E I N F O
⁎ Corresponding author. Fax: +82 42 350 4310E-mail address: [email protected] (J. Jeo
1 Both authors are equally contributed.
0006-8993/$ – see front matter © 2009 Publisdoi:10.1016/j.brainres.2009.10.057
A B S T R A C T
Article history:Accepted 22 October 2009Available online 30 October 2009
The magnetic field has been regarded as both harmful and beneficial for its applications onhuman brains including transcranial magnetic stimulation (TMS), but its effects still remainin question. Here, we determined using single photon emission computed tomography(SPECT) if 0.3-T static magnetic field could alter regional cerebral blood flow (rCBF) in targetand other brain regions in healthy subjects. The permanent static magnet (0.3 T, unipolar,disk shaped, 4 cm diameter and 1 cm thick) was placed on the right frontotemporal region ofthe brain for each of 14 healthy subjects. Tc-99m ECD perfusion SPECTwas taken to comparethe CBF patterns in the subjects exposed to the static magnet field with those of the restingand sham conditions.We found that the rCBF was significantly increased in the right frontaland parietal regions and the right insula. On the other hand, rCBF was rather decreased inthe left frontal and left parietal regions (P<0.05). These results of this basic study suggestthat 0.3-T static magnetic field induces an increase in rCBF in the targeted brain areas non-invasively, which may result from a decrease in rCBF in contralateral regions.
© 2009 Published by Elsevier B.V.
Keywords:Static magnetic fieldCerebral blood flowSPECTSPM
1. Introduction
Magnetic fields have long been considered as a potentiallybeneficial therapeutic application. When diamagnetic materi-als such as fibrin, collagen, osteoblasts and red blood cells(RBC) are exposed to static gradient magnetic fields, they aligneither parallel or perpendicular to the direction of themagnetic field depending on the magnetic anisotropy of thematerials in question (Torbet et al., 1981). Induced magnetic
.ng).
hed by Elsevier B.V.
fields in the brain might affect the membrane or synapticproperties of neurons, brain functions and thus behavior.Many studies have consequently applied magnetic fields toproximal areas of pain and inflammation of patients toalleviate pain and discomfort due to arthritis, headaches,sciatica, heel spurs, migraine and so forth (for example,Stuchly, 1986). The exposure to magnetic fields had openedup a new range of applications to facilitate bone growth andspeed the healing of fractures.
212 B R A I N R E S E A R C H 1 3 1 7 ( 2 0 1 0 ) 2 1 1 – 2 1 7
Particularly, magnetic stimulation has been used as apromising non-invasive modality for modulating neuralactivities in humans. Repetitive transcranial magnetic stimu-lation (rTMS) is a less painful, non-invasive method thandirect electric stimulations through surface electrodes placedon the head. Thus, rTMS has become an important toolfor modulating the functional organization of the brain inpatients with neurological or psychiatric disorders. It has beenreported to be a potentially safe and useful treatment forvarious brain disorders, such as depression and Parkinson'sdisease (Pascual-Leone et al., 1994; Chen et al., 2004; Hansen etal., 2004; Boggio et al., 2005; Alisauskiene et al., 2005; Canaveroand Bonicalzi, 2005). In addition, brain stimulation usingmagnetic fields is, so far, not known to have serious sideeffects compared with electrical stimulation.
However, the clinical utility of TMS as therapeuticapplication is only supported by isolated anecdotes, yet notfully supported by comprehensive epidemiological andclinical experimental findings (Aleman et al., 2007; Lam et
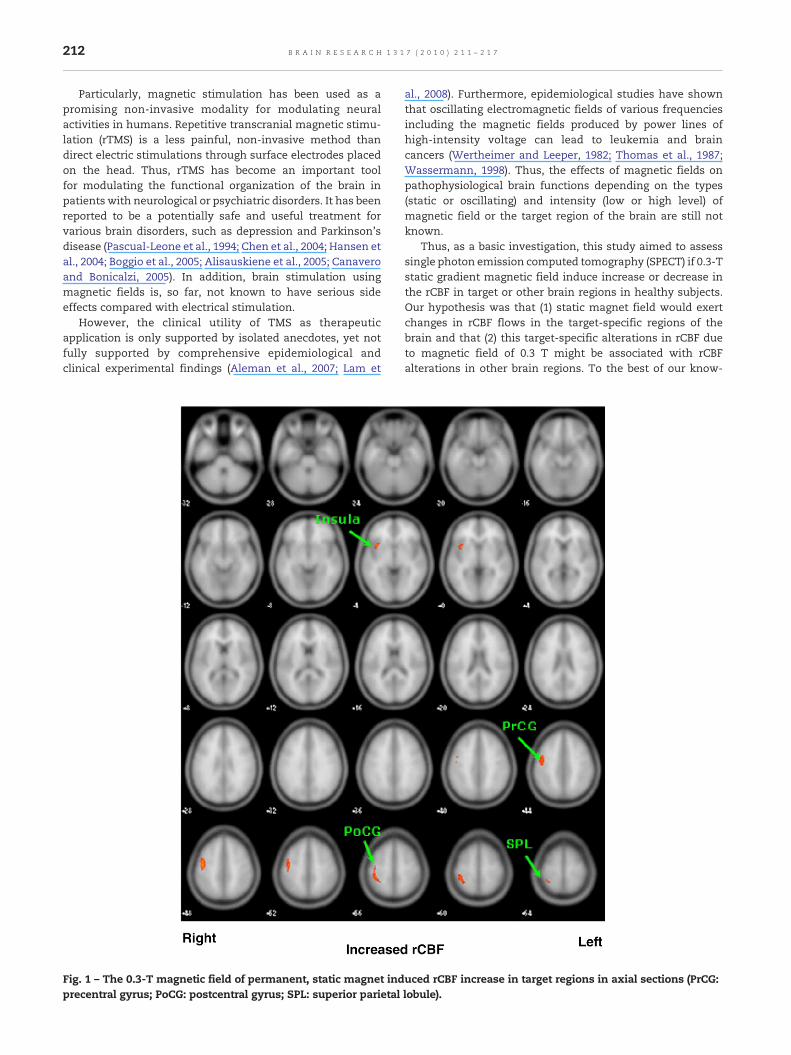
Fig. 1 – The 0.3-T magnetic field of permanent, static magnet indprecentral gyrus; PoCG: postcentral gyrus; SPL: superior parietal
al., 2008). Furthermore, epidemiological studies have shownthat oscillating electromagnetic fields of various frequenciesincluding the magnetic fields produced by power lines ofhigh-intensity voltage can lead to leukemia and braincancers (Wertheimer and Leeper, 1982; Thomas et al., 1987;Wassermann, 1998). Thus, the effects of magnetic fields onpathophysiological brain functions depending on the types(static or oscillating) and intensity (low or high level) ofmagnetic field or the target region of the brain are still notknown.
Thus, as a basic investigation, this study aimed to assesssingle photon emission computed tomography (SPECT) if 0.3-Tstatic gradient magnetic field induce increase or decrease inthe rCBF in target or other brain regions in healthy subjects.Our hypothesis was that (1) static magnet field would exertchanges in rCBF flows in the target-specific regions of thebrain and that (2) this target-specific alterations in rCBF dueto magnetic field of 0.3 T might be associated with rCBFalterations in other brain regions. To the best of our know-
uced rCBF increase in target regions in axial sections (PrCG:lobule).
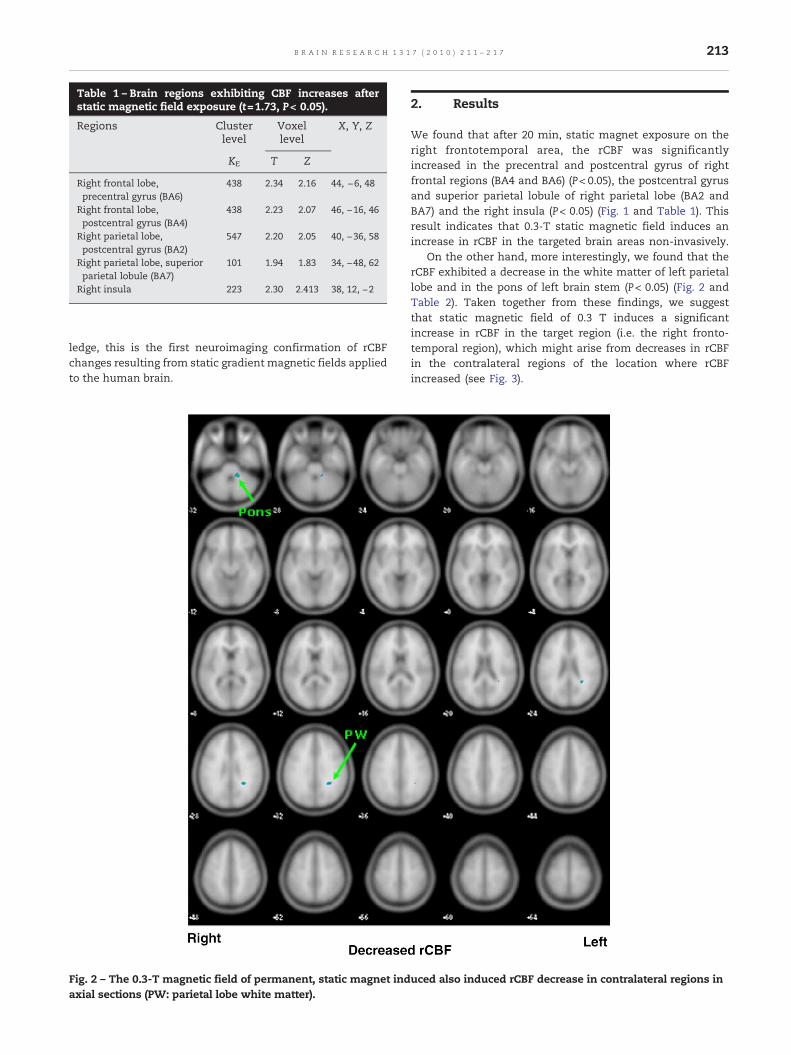
Table 1 – Brain regions exhibiting CBF increases afterstatic magnetic field exposure (t=1.73, P< 0.05).
Regions Clusterlevel
Voxellevel
X, Y, Z
KE T Z
Right frontal lobe,precentral gyrus (BA6)
438 2.34 2.16 44, −6, 48
Right frontal lobe,postcentral gyrus (BA4)
438 2.23 2.07 46, −16, 46
Right parietal lobe,postcentral gyrus (BA2)
547 2.20 2.05 40, −36, 58
Right parietal lobe, superiorparietal lobule (BA7)
101 1.94 1.83 34, −48, 62
Right insula 223 2.30 2.413 38, 12, −2
213B R A I N R E S E A R C H 1 3 1 7 ( 2 0 1 0 ) 2 1 1 – 2 1 7
ledge, this is the first neuroimaging confirmation of rCBFchanges resulting from static gradient magnetic fields appliedto the human brain.
Fig. 2 – The 0.3-T magnetic field of permanent, static magnet indaxial sections (PW: parietal lobe white matter).
2. Results
We found that after 20 min, static magnet exposure on theright frontotemporal area, the rCBF was significantlyincreased in the precentral and postcentral gyrus of rightfrontal regions (BA4 and BA6) (P< 0.05), the postcentral gyrusand superior parietal lobule of right parietal lobe (BA2 andBA7) and the right insula (P< 0.05) (Fig. 1 and Table 1). Thisresult indicates that 0.3-T static magnetic field induces anincrease in rCBF in the targeted brain areas non-invasively.
On the other hand, more interestingly, we found that therCBF exhibited a decrease in the white matter of left parietallobe and in the pons of left brain stem (P< 0.05) (Fig. 2 andTable 2). Taken together from these findings, we suggestthat static magnetic field of 0.3 T induces a significantincrease in rCBF in the target region (i.e. the right fronto-temporal region), which might arise from decreases in rCBFin the contralateral regions of the location where rCBFincreased (see Fig. 3).
uced also induced rCBF decrease in contralateral regions in
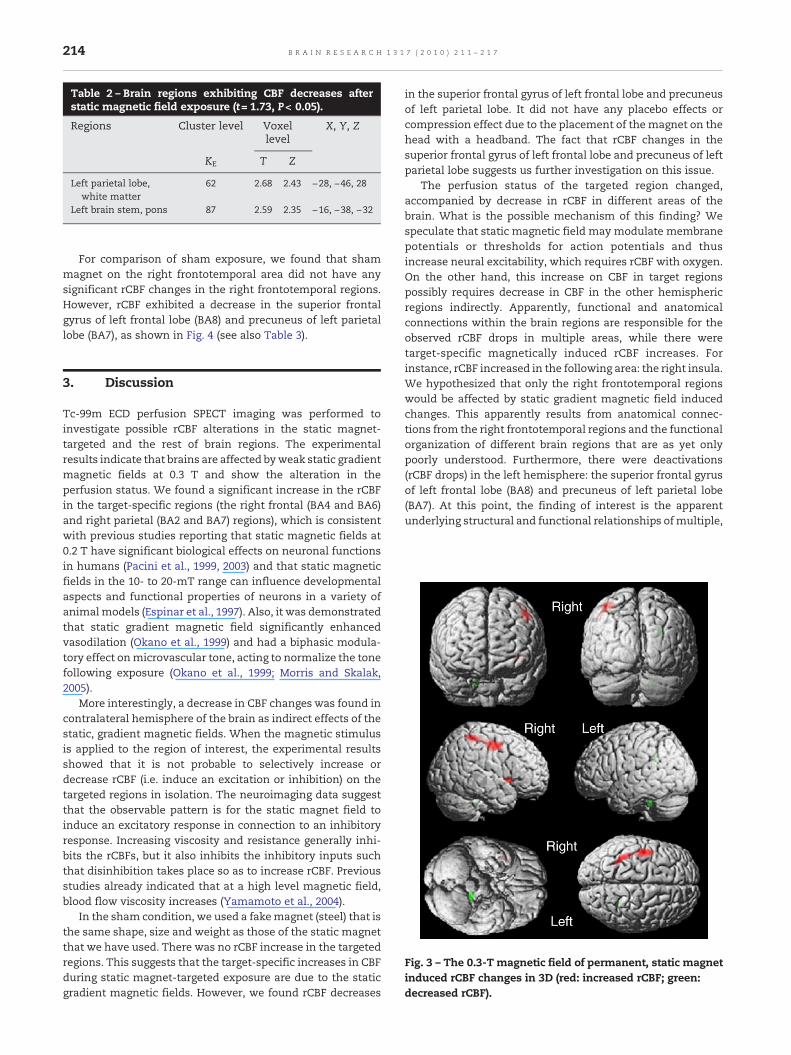
Table 2 – Brain regions exhibiting CBF decreases afterstatic magnetic field exposure (t= 1.73, P< 0.05).
Regions Cluster level Voxellevel
X, Y, Z
KE T Z
Left parietal lobe,white matter
62 2.68 2.43 −28, −46, 28
Left brain stem, pons 87 2.59 2.35 −16, −38, −32
214 B R A I N R E S E A R C H 1 3 1 7 ( 2 0 1 0 ) 2 1 1 – 2 1 7
For comparison of sham exposure, we found that shammagnet on the right frontotemporal area did not have anysignificant rCBF changes in the right frontotemporal regions.However, rCBF exhibited a decrease in the superior frontalgyrus of left frontal lobe (BA8) and precuneus of left parietallobe (BA7), as shown in Fig. 4 (see also Table 3).
Fig. 3 – The 0.3-T magnetic field of permanent, static magnetinduced rCBF changes in 3D (red: increased rCBF; green:decreased rCBF).
3. Discussion
Tc-99m ECD perfusion SPECT imaging was performed toinvestigate possible rCBF alterations in the static magnet-targeted and the rest of brain regions. The experimentalresults indicate that brains are affected byweak static gradientmagnetic fields at 0.3 T and show the alteration in theperfusion status. We found a significant increase in the rCBFin the target-specific regions (the right frontal (BA4 and BA6)and right parietal (BA2 and BA7) regions), which is consistentwith previous studies reporting that static magnetic fields at0.2 T have significant biological effects on neuronal functionsin humans (Pacini et al., 1999, 2003) and that static magneticfields in the 10- to 20-mT range can influence developmentalaspects and functional properties of neurons in a variety ofanimalmodels (Espinar et al., 1997). Also, it was demonstratedthat static gradient magnetic field significantly enhancedvasodilation (Okano et al., 1999) and had a biphasic modula-tory effect onmicrovascular tone, acting to normalize the tonefollowing exposure (Okano et al., 1999; Morris and Skalak,2005).
More interestingly, a decrease in CBF changes was found incontralateral hemisphere of the brain as indirect effects of thestatic, gradient magnetic fields. When the magnetic stimulusis applied to the region of interest, the experimental resultsshowed that it is not probable to selectively increase ordecrease rCBF (i.e. induce an excitation or inhibition) on thetargeted regions in isolation. The neuroimaging data suggestthat the observable pattern is for the static magnet field toinduce an excitatory response in connection to an inhibitoryresponse. Increasing viscosity and resistance generally inhi-bits the rCBFs, but it also inhibits the inhibitory inputs suchthat disinhibition takes place so as to increase rCBF. Previousstudies already indicated that at a high level magnetic field,blood flow viscosity increases (Yamamoto et al., 2004).
In the sham condition, we used a fakemagnet (steel) that isthe same shape, size and weight as those of the static magnetthat we have used. There was no rCBF increase in the targetedregions. This suggests that the target-specific increases in CBFduring static magnet-targeted exposure are due to the staticgradient magnetic fields. However, we found rCBF decreases
in the superior frontal gyrus of left frontal lobe and precuneusof left parietal lobe. It did not have any placebo effects orcompression effect due to the placement of themagnet on thehead with a headband. The fact that rCBF changes in thesuperior frontal gyrus of left frontal lobe and precuneus of leftparietal lobe suggests us further investigation on this issue.
The perfusion status of the targeted region changed,accompanied by decrease in rCBF in different areas of thebrain. What is the possible mechanism of this finding? Wespeculate that static magnetic field may modulate membranepotentials or thresholds for action potentials and thusincrease neural excitability, which requires rCBF with oxygen.On the other hand, this increase on CBF in target regionspossibly requires decrease in CBF in the other hemisphericregions indirectly. Apparently, functional and anatomicalconnections within the brain regions are responsible for theobserved rCBF drops in multiple areas, while there weretarget-specific magnetically induced rCBF increases. Forinstance, rCBF increased in the following area: the right insula.We hypothesized that only the right frontotemporal regionswould be affected by static gradient magnetic field inducedchanges. This apparently results from anatomical connec-tions from the right frontotemporal regions and the functionalorganization of different brain regions that are as yet onlypoorly understood. Furthermore, there were deactivations(rCBF drops) in the left hemisphere: the superior frontal gyrusof left frontal lobe (BA8) and precuneus of left parietal lobe(BA7). At this point, the finding of interest is the apparentunderlying structural and functional relationships ofmultiple,
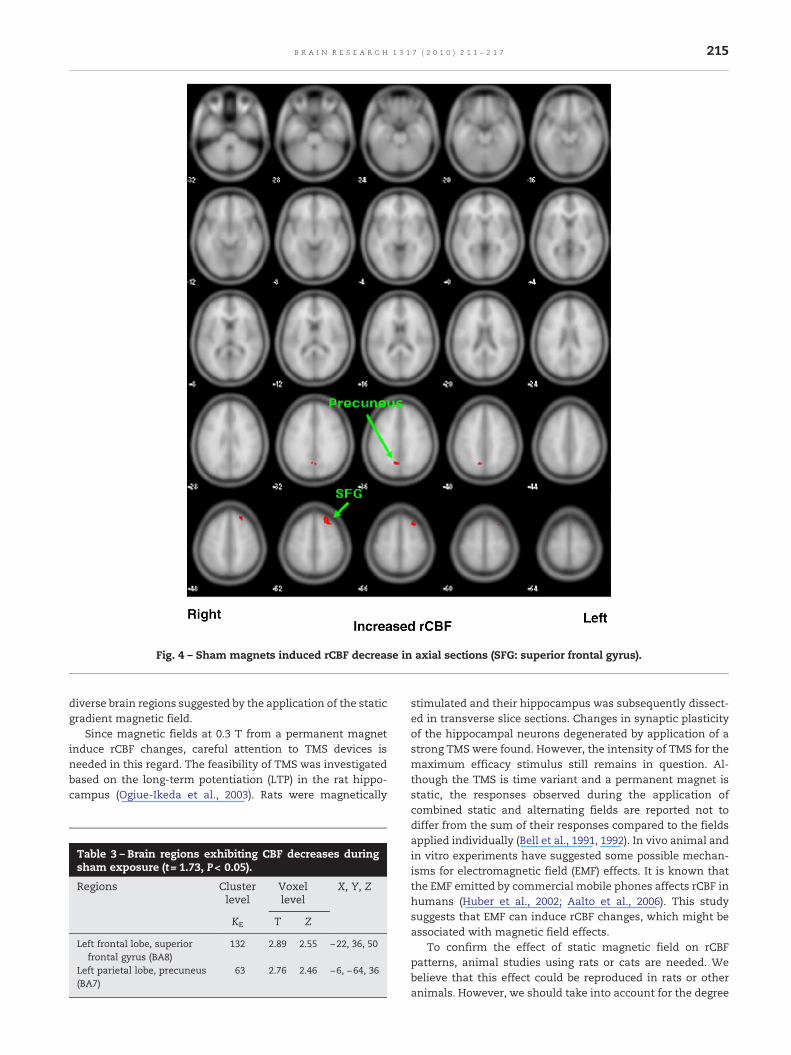
Fig. 4 – Sham magnets induced rCBF decrease in axial sections (SFG: superior frontal gyrus).
215B R A I N R E S E A R C H 1 3 1 7 ( 2 0 1 0 ) 2 1 1 – 2 1 7
diverse brain regions suggested by the application of the staticgradient magnetic field.
Since magnetic fields at 0.3 T from a permanent magnetinduce rCBF changes, careful attention to TMS devices isneeded in this regard. The feasibility of TMS was investigatedbased on the long-term potentiation (LTP) in the rat hippo-campus (Ogiue-Ikeda et al., 2003). Rats were magnetically
Table 3 – Brain regions exhibiting CBF decreases duringsham exposure (t= 1.73, P< 0.05).
Regions Clusterlevel
Voxellevel
X, Y, Z
KE T Z
Left frontal lobe, superiorfrontal gyrus (BA8)
132 2.89 2.55 −22, 36, 50
Left parietal lobe, precuneus(BA7)
63 2.76 2.46 −6, −64, 36
stimulated and their hippocampus was subsequently dissect-ed in transverse slice sections. Changes in synaptic plasticityof the hippocampal neurons degenerated by application of astrong TMS were found. However, the intensity of TMS for themaximum efficacy stimulus still remains in question. Al-though the TMS is time variant and a permanent magnet isstatic, the responses observed during the application ofcombined static and alternating fields are reported not todiffer from the sum of their responses compared to the fieldsapplied individually (Bell et al., 1991, 1992). In vivo animal andin vitro experiments have suggested some possible mechan-isms for electromagnetic field (EMF) effects. It is known thatthe EMF emitted by commercial mobile phones affects rCBF inhumans (Huber et al., 2002; Aalto et al., 2006). This studysuggests that EMF can induce rCBF changes, which might beassociated with magnetic field effects.
To confirm the effect of static magnetic field on rCBFpatterns, animal studies using rats or cats are needed. Webelieve that this effect could be reproduced in rats or otheranimals. However, we should take into account for the degree
Fig. 5 – The illustrative location of the static magnet/shammagnet on the head of the subject (i.e. the right frontotem-poral area).
216 B R A I N R E S E A R C H 1 3 1 7 ( 2 0 1 0 ) 2 1 1 – 2 1 7
of localization of the static magnet. Although static magnethas various sizes from several millimeters of the radius toseveral meters, some of the smallest magnets is still too largefor small brains of rats to focus on the target regions of ratswhich are possibly implicated as human brains.
One of the limitations we should take into account in thisstudy is a small sample size (n= 14). Although we couldobserve changes in one targeted region with small number ofsubjects, future longitudinal investigations should be per-formed to understand the effects of the duration of themagnetic fields in varying strengths, polarities of the magnetand the sham condition. Multiple locations should also betested for their associated rCBF perfusion status. In addition,static gradient magnetic field with different intensities can beused to correlate with the rCBF changes. To assess thecomplex and dynamic effects of magnetic fields, both staticand alternating, it will be necessary to test for both uniformand gradient magnetic fields in multiple areas in the brainwith different intensities in a series of carefully devisedexperiments.
4. Experimental procedures
4.1. Subjects
Fourteen healthy volunteers (M:F=7:7, age=31.6±5.5 yearswith range of 24–41 years) were recruited by an advertisementof the local community and participated in this study. Allsubjects were right-handed and had normal or corrected-to-normal vision. In the self-reported questionnaire, noneresponded as having a history of neurological or psychiatricdisorder or having previously used any magnetic therapy orbeing taking any antidepressant medications (e.g. fluoxetine,nortriptyline, amitriptyline) that might hinder with the brainperfusion status. They signed the informed consent formsapproved by IRB in the Catholic University of Korea aftercareful explanations. Institutional review boards (IRB) of theCatholic University of Korea approved all experimentalprocedures.
4.2. Magnets
The magnets used in this study were commercially available,ceramic magnets (3000 gauss, unipolar). Each was a diskshaped magnet that weighed 85 g and had a surface field of0.3 T, 4 cm diameter and 1 cm thick. The north side of themagnet was placed on the right frontotemporal regions for themagnetic stimulus as shown in Fig. 5 because the rightfrontotemporal region is the locationwhere the rTMS stimulusis usually applied in therapeutic treatments.
4.3. Paradigms and data acquisitions
The experiment was double blind and counterbalanced. TheSPECT was taken under three experimental conditions:control (n=14), magnetic (n=12) and sham (n=6). Threeconditions were randomly mixed, and SPECT images ofmagnetic stimulation, sham and control conditions weretaken 3 days apart. All SPECTs were performed with the
subject supine on a bed in an isolated, dark, quiet room. The0.3-T magnet was placed on the right frontotemporal regionfor 20 min. SPECT images were obtained after 20 min from theintravenous injection of approximately 740–925 MBq of Tc-99m ECD using amulti-detector scanner (ECAM plus; Siemens,Eriangen, Germany) equipped with a low-energy and fan-beam collimator. Tc-99m ECD SPECT images were correctedfor tissue attenuation using a standard commercial correctionroutine, which assumes a uniform attenuation with thecircular shape of the head. During tracer uptake, we let thesubjects lie down on the bed at rest without any cognitivetasks or loads in the dark, silent room to protect them exposedto other stimuli except static magnet fields. Magnets wereheld in position with a headband and the experimenters holdthe magnet in place so that the weight of the magnet did notaffect possible rCBF changes. For the shamexposure, imitationmagnet (steel) of identical weight and size was placed on thesame region for 6 subjects among 14 control subjects for20 min.
4.4. Data processing using statistical parametric mapping(SPM)
The software for image manipulation included the Matlab(version 5.3, Mathworks, Natick, MA) and SPM2 (WellcomeDepartment of Imaging Neuroscience, University College ofLondon, UK) softwares. The reconstructed SPECT data withattenuations and scatter correction were reformatted into theanalyzer (Mayo Foundation, Baltimore, MD, USA) headerformat. The header format of the SPECT data included 348bytes of header, 3.9 mm of x and y pixel size and a 3.9-mmthick slice. Image analyses were performed on an IBM PC witha Windows XP operating system. The SPECT data withattenuation and scatter correction were converted intoANALYZE format. The mean pixel intensity across all slicesof the imaging volume was calculated. Each pixel was thenthresholded at 80% of this value to eliminate backgroundnoise and the brain-edge halo effect caused by partial-volumeerror, without losing any imaging data specific to the brain.Each SPECT scan was then spatially normalized by 12-parameter affine warping and sinc-linear interpolation tothe SPECT template brain from the Montreal NeurologicalInstitute and reformatted to a 16-bit image of 79×95×68voxels, each 2×2×2 mm in size. Data were normalized to a

217B R A I N R E S E A R C H 1 3 1 7 ( 2 0 1 0 ) 2 1 1 – 2 1 7
SPECT template for a better resolution (Montreal NeurologicalInstitution Template) and smoothed with 16 mm full-width athalf-maximum (FWHM) prior to SPM statistical analysis. Thenormalized SPECT data of the 7 magnetic subjects werecompared to their corresponding normal states. Group con-trasts in rCBF were estimated at each voxel using the generallinear model of SPM99 (Ashburner and Friston, 1999).
A paired t-test model was fitted and a t-statistic image(SPM[t]) was constructed. The t-statistic image was thresholdat t>2.54, corresponding to an uncorrected p-value <0.01, inconjunction with a cluster filter of 50 voxels. And for shamcomparison, a two-sample t-test model was fitted and a t-statistic image (SPM[t]) was constructed. The t-statistic imagewas thresholded at t>1.73, corresponding to an uncorrected p-value <0.05 in conjunction with a cluster filter of 50 voxels.Combined application of a statistical threshold and clusterfilter has previously been shown to substantially reduce thefalse-positive identification of activated pixels at any giventhreshold. For the purposes of visualization and anatomiclocalization, the t-score clusters were projected onto standardhigh-resolution T1-weighted MRI templates.
Acknowledgments
The authors wish to acknowledge the financial support of theCatholic Medical Center Research Foundation made in theprogram year of 2008. This work was also supported by grantsfrom the Korea Science and Engineering Foundation (KOSEF)grant funded by the Korean government (MOST) (No.M10644000005-06N4400-00510, No. R01-2007-000-21094-0 andNo. M10644000013-06N4400-01310).
R E F E R E N C E S
Aalto, S., Haarala, C., Bruck, A., Sipila, H., Hamalainen, H., Rinne,J.O., 2006. Mobile phone affects cerebral blood flow inhumans. J. Cereb. Blood Flow Metab. 26, 885–890.
Aleman, A., Sommer, I.E., Kahn, R.S., 2007. Efficacy of slowrepetitive transcranial magnetic stimulation in the treatmentof resistant auditory hallucinations in schizophrenia: ameta-analysis. J. Clin. Psychiatry 68, 416–421.
Alisauskiene, M., Truffert, A., Vaiciene, N., Magistris, M.R., 2005.Transcranial magnetic stimulation in clinical practice.Medicina (Kaunas) 41, 813–824.
Ashburner, J., Friston, K.J., 1999. Nonlinear spatial normalizationusing basis functions. Hum. Brain Mapp. 7, 254–266.
Bell, G., Marino, A., Chesson, A., Struve, F., 1992. Electrical states inthe rabbit brain can be altered by light and electromagneticfields. Brain Res. 570, 307–315.
Bell, G.B., Marino, A.A., Chesson, A.L., Struve, F.A., 1991. Humansensitivity to weak magnetic fields. Lancet 338, 1521–1522.
Boggio, P.S., Fregni, F., Bermpohl, F., Mansur, C.G., Rosa, M., Rumi,D.O., Barbosa, E.R., Odebrecht Rosa, M., Pascual-Leone, A.,Rigonatti, S.P., Marcolin, M.A., Araujo Silva, M.T., 2005. Effect ofrepetitive TMS and fluoxetine on cognitive function in patientswith Parkinson's disease and concurrent depression. Mov.Disord. 20, 1178–1184.
Canavero, S., Bonicalzi, V., 2005. Transcranial magnetic
stimulation for central pain. Curr. Pain Headache Rep. 9,87–89.
Chen, A.C., Zhang, W.T., Han, J.S., 2004. [Transcranial magneticstimulation (TMS): physiology, psychology, brain mappingand clinical applications]. Sheng Li Ke Xue Jin Zhan 35,102–106.
Espinar, A., Piera, V., Carmona, A., Guerrero, J.M., 1997. Histologicalchanges during development of the cerebellum in the chickembryo exposed to a static magnetic field. Bioelectromagnetics18, 36–46.
Hansen, P.E., Videbech, P., Clemmensen, K., Sturlason, R., Jensen,H.M., Vestergaard, P., 2004. Repetitive transcranial magneticstimulation as add-on antidepressant treatment. Theapplicability of the method in a clinical setting. Nord. J.Psychiatry 58, 455–457.
Huber, R., Treyer, V., Borbely, A.A., Schuderer, J., Gottselig,J.M., Landolt, H.P., Werth, E., Berthold, T., Kuster, N., Buck,A., Achermann, P., 2002. Electromagnetic fields, such asthose from mobile phones, alter regional cerebral bloodflow and sleep and waking EEG. J. Sleep. Res. 11,289–295.
Lam, R.W., Chan, P., Wilkins-Ho, M., Yatham, L.N., 2008. Repetitivetranscranial magnetic stimulation for treatment-resistantdepression: a systematic review and metaanalysis. Can. J.Psychiatry 53, 621–631.
Morris, C., Skalak, T., 2005. Static magnetic fields alter arteriolartone in vivo. Bioelectromagnetics 26, 1–9.
Ogiue-Ikeda, M., Kawato, S., Ueno, S., 2003. The effect of repetitivetranscranial magnetic stimulation on long-term potentiationin rat hippocampus depends on stimulus intensity. Brain Res.993, 222–226.
Okano, H., Gmitrov, J., Ohkubo, C., 1999. Biphasic effects of staticmagnetic fields on cutaneous microcirculation in rabbits.Bioelectromagnetics 20, 161–171.
Pacini, S., Gulisano, M., Peruzzi, B., Sgambati, E., Gheri, G., GheriBryk, S., Vannucchi, S., Polli, G., Ruggiero, M., 2003. Effects of0.2 T static magnetic field on human skin fibroblasts. CancerDetect. Prev. 27, 327–332.
Pacini, S., Vannelli, G.B., Barni, T., Ruggiero, M., Sardi, I., Pacini, P.,Gulisano, M., 1999. Effect of 0.2 T static magnetic field onhuman neurons: remodeling and inhibition of signaltransduction without genome instability. Neurosci. Lett. 267,185–188.
Pascual-Leone, A., Valls-Sole, J., Brasil-Neto, J.P., Cohen, L.G.,Hallett, M., 1994. Akinesia in Parkinson's disease. I. Shorteningof simple reaction time with focal, single-pulse transcranialmagnetic stimulation. Neurology 44, 884–891.
Stuchly, M.A., 1986. Human exposure to static and time-varyingmagnetic fields. Health Phys. 51, 215–225.
Thomas, T.L., Stolley, P.D., Stemhagen, A., Fontham, E.T., Bleecker,M.L., Stewart, P.A., Hoover, R.N., 1987. Brain tumor mortalityrisk among men with electrical and electronics jobs: acase-control study. J. Natl. Cancer Inst. 79, 233–238.
Torbet, J., Freyssinet, J.M., Hudry-Clergeon, G., 1981. Oriented fibringels formed by polymerization in strong magnetic fields.Nature 289, 91–93.
Wassermann, E.M., 1998. Risk and safety of repetitive transcranialmagnetic stimulation: report and suggested guidelines fromthe International Workshop on the Safety of RepetitiveTranscranial Magnetic Stimulation, June 5–7, 1996.Electroencephalogr. Clin. Neurophysiol. 108, 1–16.
Wertheimer, N., Leeper, E., 1982. Adult cancer related to electricalwires near the home. Int. J. Epidemiol. 11, 345–355.
Yamamoto, T., Nagayama, Y., Tamura, M., 2004. Ablood-oxygenation-dependent increase in blood viscosity dueto a static magnetic field. Phys. Med. Biol. 49, 3267–3277.
Related Documents











