A Harborside Press Publication Editor-in-Chief, James O. Armitage, MD ASCOPost.com VOLUME 2, ISSUE 1 JANUARY 1, 2011 continued on page 4 continued on page 22 MORE IN THIS ISSUE Oncology Meetings Coverage 52nd ASH Annual Meeting ................1, 12 52nd ASTRO Annual Meeting...........3, 10 Chemotherapy Foundation Symposium XXVIII ................................ 6 35th ESMO Congress............................... 21 Direct from ASCO...................................... 14 MRI-based screening for breast cancer ....... 32 T he discussion about cancer treatment in the United States has changed from the hope and promise of new innovations to con- siderations of whether a treatment is worth the personal and societal cost. is philosophical shiſt coincides with the aggressive applica- tion of comparative effectiveness evaluations of cancer care under the American Recovery and Reinvestment Act (AR, 2009) and the Affordable Care Act (ACA, 2010), which are the cornerstones of U.S. health-care reform. To meet cost-containment criteria, the Afford- able Care Act included $500 billion of cuts to Medicare over 10 years. In 2012, the Affordable Care Act will create the Independent Payment Advisory Board to “recommend payment policy revisions to con- tain Medicare cost growth” while the Medi- 52nd ASH Annual Meeting Health-care Policy Health-care Reform and the Treatment of Metastatic Cancer T he sustainable growth rate (SGR) is the method used by the Centers for Medicare & Medicaid Services (CMS) to control Medicare’s spending on physician services. Generally, the SGR was designed to ensure that the cost per Medicare beneficiary does not exceed the growth in real gross domestic product (GDP). If yearly expenditures exceed the SGR target amount, the conversion factor will decrease physi- cian fee schedules accordingly for the following year. On March 1 of each year, the physician fee schedule is updated and adjusted to meet the SGR target, which can be suspended or adjusted by Congress, as has been done in the past. On March 23, 2010, President Obama signed the Patient Protection and Affordable Care Act (PPACA) into law. During that period of sweeping reform, the The Sustainable Growth Rate’s Unsustainable Impact on Oncology Practice By Ronald Piana continued on page 2 Cancer survivorship and QOL 8 | Head & neck cancer controversy 25 | FDA drug updates 34 I n a comparison of patients with asymptomatic stage II, III, or IV follicular lymphoma, results of a randomized trial demonstrated that rituximab (Rituxan) maintenance therapy can delay the time to treatment for patients with nonbulky disease. e results of an Intergroup randomized trial of ritux- imab vs a watch-and-wait strategy were presented at a plenary session during the 52nd Annual Meeting of the American Society of Hematology (ASH). 1 “Rituximab mainte- nance therapy significant- ly delays time to treat- ment in asymptomatic patients. Delaying che- motherapy may become a popular option for pa- tients with asymptom- atic follicular lymphoma and could become the standard of care in the future,” stated lead author Maintenance Rituximab Delays the Need for Chemotherapy or Radiotherapy in Asymptomatic Follicular Lymphoma By Alice Goodman Dr. Janjan is Senior Fellow in Healthcare Policy and Dr. Goodman is President and CEO, National Cen- ter for Policy Analysis, Dallas. e National Center for Policy Analysis is a nonprofit conservative think tank established in 1983 and headquartered in Dal- las, Texas. Disclosure: Dr. Janjan served as a consultant to Dendreon prior to the Medicare Evidence Development & Coverage Advisory Commiee meeting on sipuleucel-T (Provenge). Months from randomization Proportion of patients without initiation of new therapy 0.0 0.2 0.4 0.6 0.8 1.0 0 6 12 Arm A Arm B Arm C 18 24 42 48 36 30 0.1 0.3 0.5 0.7 0.9 Fig. 1: Time to initiation of new therapy. Arm A = watchful waiting, Arm B = rituximab induction thera- py; Arm C = rituximab maintenance therapy. Courtesy of Kirit M. Ardeshna, MD. Used with permission of American Society of Hematology (ASH), from Ardeshna KM et al. 1 Permission conveyed through Copyright Clearance Center, Inc. By Nora Janjan, MD, MPSA, MBA, and John Goodman, PhD Editor’s note: As e ASCO Post went to press, both houses of Congress approved a measure to postpone the SGR-driven Medicare physician fee cuts scheduled for January 1st. Upward of 23%, the payment cuts would have had dire consequences for community oncology practices. According to Joseph S. Bailes, MD, the SGR game is not over, simply postponed. “e flawed formula remains and it will require substantial ‘pay for’ to fix. It will also require substantial political will.” Watch for continued coverage of this impor- tant issue in future editions of e ASCO Post.

TAP Vol 2 Issue 1
Mar 20, 2016
By Alice Goodman A Harborside Press Publication By Nora Janjan, MD, MPSA, MBA, and John Goodman, PhD By Ronald Piana 52nd ASH Annual Meeting stage II, III, or IV follicular lymphoma, results of a randomized trial demonstrated that rituximab 52nd ASH Annual Meeting ................ 1, 12 52nd ASTRO Annual Meeting........... 3, 10 VOLUME 2, ISSUE 1 Health-care Policy Months from randomization Editor-in-Chief, James O. Armitage, MD continued on page 22 continued on page 4 continued on page 2 0.4
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A Harborside Press Publication
Editor-in-Chief, James O. Armitage, MD ASCOPost.com
VOLUME 2, ISSUE 1
JANUARY 1, 2011
continued on page 4
continued on page 22
MORE IN THIS ISSUE
Oncology Meetings Coverage52nd ASH Annual Meeting ................1, 1252nd ASTRO Annual Meeting ...........3, 10Chemotherapy Foundation Symposium XXVIII ................................635th ESMO Congress ...............................21
Direct from ASCO ......................................14MRI-based screening for breast cancer .......32
The discussion about cancer treatment in the United States has changed from the
hope and promise of new innovations to con-siderations of whether a treatment is worth the personal and societal cost. This philosophical shift coincides with the aggressive applica-tion of comparative effectiveness evaluations of cancer care under the American Recovery and Reinvestment Act (ARRA, 2009) and the Affordable Care Act (ACA, 2010), which are the cornerstones of U.S. health-care reform. To meet cost-containment criteria, the Afford-able Care Act included $500 billion of cuts to Medicare over 10 years.
In 2012, the Affordable Care Act will create the Independent Payment Advisory Board to “recommend payment policy revisions to con-tain Medicare cost growth” while the Medi-
52nd ASH Annual Meeting
Health-care Policy
Health-care Reform and the
Treatment of Metastatic Cancer
The sustainable growth rate (SGR) is the method used by the Centers for Medicare & Medicaid
Services (CMS) to control Medicare’s spending on physician services. Generally, the SGR was designed to ensure that the cost per Medicare beneficiary does not exceed the growth in real gross domestic product (GDP). If yearly expenditures exceed the SGR target amount, the conversion factor will decrease physi-cian fee schedules accordingly for the following year. On March 1 of each year, the physician fee schedule is updated and adjusted to meet the SGR target, which can be suspended or adjusted by Congress, as has been done in the past.
On March 23, 2010, President Obama signed the Patient Protection and Affordable Care Act (PPACA) into law. During that period of sweeping reform, the
The Sustainable Growth Rate’s Unsustainable Impact on Oncology PracticeBy Ronald Piana
continued on page 2
Cancer survivorship and QOL 8 | Head & neck cancer controversy 25 | FDA drug updates 34
In a comparison of patients with asymptomatic stage II, III, or IV follicular lymphoma, results
of a randomized trial demonstrated that rituximab
(Rituxan) maintenance therapy can delay the time to treatment for patients with nonbulky disease. The results of an Intergroup randomized trial of ritux-
imab vs a watch-and-wait strategy were presented at a plenary session during the 52nd Annual Meeting of the American Society of Hematology (ASH).1
“Rituximab mainte-nance therapy significant-ly delays time to treat-ment in asymptomatic patients. Delaying che-motherapy may become a popular option for pa-tients with asymptom-atic follicular lymphoma and could become the standard of care in the future,” stated lead author
Maintenance Rituximab Delays the Need for Chemotherapy or Radiotherapy in Asymptomatic Follicular LymphomaBy Alice Goodman
Dr. Janjan is Senior Fellow in Healthcare Policy and Dr. Goodman is President and CEO, National Cen-ter for Policy Analysis, Dallas. The National Center for Policy Analysis is a nonprofit conservative think tank established in 1983 and headquartered in Dal-las, Texas.
Disclosure: Dr. Janjan served as a consultant to Dendreon prior to the Medicare Evidence Development & Coverage Advisory Committee meeting on sipuleucel-T (Provenge).
Months from randomization
Prop
ortio
n of
pat
ient
s w
ithou
t ini
tiatio
n of
new
ther
apy
0.0
0.2
0.4
0.6
0.8
1.0
0 6 12
Arm AArm BArm C
18 24 42 483630
0.1
0.3
0.5
0.7
0.9
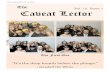
Fig. 1: Time to initiation of new therapy. Arm A = watchful waiting, Arm B = rituximab induction thera-py; Arm C = rituximab maintenance therapy. Courtesy of Kirit M. Ardeshna, MD. Used with permission of American Society of Hematology (ASH), from Ardeshna KM et al.1 Permission conveyed through Copyright Clearance Center, Inc.
By Nora Janjan, MD, MPSA, MBA, and John Goodman, PhD
Editor’s note: As The ASCO Post went to press, both houses
of Congress approved a measure to postpone the SGR-driven Medicare physician fee cuts scheduled for January 1st. Upward of 23%, the payment cuts would have had dire consequences for community oncology practices. According to Joseph S. Bailes, MD, the SGR game is not over, simply postponed. “The flawed formula remains and it will require substantial ‘pay for’ to fix. It will also require substantial political will.”
Watch for continued coverage of this impor-tant issue in future editions of The ASCO Post.

PAGE 2 The ASCO Post | JANUARY 1, 2011
Opinion
care population swells with the baby boomer generation. As described by a Centers for Medicare & Medicaid Ser-vices (CMS) document entitled, “Af-fordable Care Act Update: Implement-ing Medicare Cost Savings,” almost $24 billion in Medicare cost savings is projected by 2019. These cost savings are assured, as the “Independent Pay-ment Advisory Board’s proposals on how to improve care and control pro-gram expenditures are binding when Medicare cost projections exceed cer-tain targets, unless Congress acts to reduce expenditures in other ways.” The law also stipulates that the Inde-pendent Payment Advisory Board will publically report system-wide health-care costs, patient access to care, utili-zation, and quality of care.
Recently, various Federal agen-cies have scrutinized treatment with biologic agents for metastatic dis-ease resulting from three of the most common malignancies in the United States—colorectal, breast, and pros-tate cancers.
In January 2010, the Agency for Healthcare Research and Quality (AHRQ) initiated evaluation of the “real world” benefits and harms of the FDA-approved regimen of cetuximab (Erbitux) and bevacizumab (Avastin) for the treatment of metastatic colorec-tal cancer.
In July 2010, the FDA Oncologic Drugs Advisory Committee (ODAC) recommended against full FDA ap-proval for bevacizumab as a first-line treatment of metastatic HER2-nega-tive breast cancer.
In November 2010, the CMS Medi-care Evidence Development & Cover-age Advisory Committee (MEDCAC) evaluated the use of autologous cellu-lar immunotherapy with sipuleucel-T (Provenge) for metastatic hormone-refractory prostate cancer.
Cetuximab and Bevacizumab in Colorectal Cancer
Acknowledging on its website that “clinical trials support the efficacy of the biologic therapies cetuximab and bevacizumab for the treatment of met-astatic colorectal cancer,” the AHRQ began an evaluation of the “real-world effectiveness in diverse populations” in January 2010. This study, using can-cer registries, the Medicare program, National Comprehensive Cancer Net-work (NCCN) data sources, NCI’s Cancer Care Outcomes Research
and Surveillance Consortium, and a phase IV industry-sponsored registry, is measuring the size of the “imple-mentation gap.”
As defined by the Agency for Healthcare Research and Quality, the implementation gap is the difference between efficacy and effectiveness in clinical trials and in the nonexperi-mental setting. The AHRQ further de-fines these terms as follows: “Efficacy trials [explanatory trials] determine whether an intervention produces the expected result under ideal circum-stances,” whereas “effectiveness trials [pragmatic trials] measure the degree of beneficial effect under ‘real world’ clinical settings.”
The implementation gap will be evaluated by this registry-based data analysis for patients with attributes similar to clinical trial participants, and among populations that were either excluded or underrepresented in the clinical trials. The degree of beneficial effect is broader than overall survival, and, in terms of comparative effective-ness research, relates also to functional and symptomatic outcomes, including the burden of therapy.
Bevacizumab in Breast CancerThe importance of quality-of-life
measures and outcomes featured prominently in the ODAC recommen-dation against full FDA approval for bevacizumab as a first-line treatment of metastatic HER2-negative breast can-cer. Although the FDA does not gener-ally use quality-of-life measures in the approval process, the importance of quality-of-life outcomes was noted in public testimony and in ODAC mem-ber decision-making.
In public testimony, members of a breast cancer advocate group—SHARE Leaders—made the follow-ing three arguments: First, “trials sub-sequent to accelerated approval failed to demonstrate a clinically meaningful benefit that is either an improvement in overall survival, or a sufficient mag-nitude of progression-free survival to-gether with improved quality of life.” Next, the advocates challenged the merit of progression-free survival as a credible endpoint, noting, “Overall survival, without compromising qual-ity of life, must remain as a primary goal of research.” Third, the advocates argued, “a meaningful, progression-free survival time frame combined with few toxic side effects and a better quality of life could be an acceptable endpoint, particularly in metastatic disease.”
During the voting regarding beva-cizumab in metastatic breast cancer, many ODAC members subsequently cited the lack of quality-of-life mea-sures and outcomes data. Comments included:
“Even with the 2.9 months of pro-gression-free survival, there’s still no overall survival benefit to the patient, there’s very significant risk to the pa-tient, and there’s no demonstrated positive patient outcome in terms of quality-of-life measures.”
“What we are here to judge is whether or not there is a clinically meaningful—from a patient’s point of view—quality-of-life benefit.”
The burden of therapy was ad-dressed by one ODAC member who commented: “We keep talking about quality of life. But we haven’t ad-dressed the quality of life [and] what’s required when you’re on an agent like this [bevacizumab].”
Beneficial effect, defined by qual-ity-of-life outcomes, again took the forefront in the assessment of biologic agents for metastatic disease.
Sipuleucel-T in Prostate CancerIn November 2010, the Medicare
Evidence Development & Coverage Advisory Committee (MEDCAC) considered on-label and off-label use of sipuleucel-T for asymptomatic or minimally symptomatic metastatic, hormone-refractory prostate cancer. Although not explicitly discussed by the Committee, media coverage of the Medicare Committee meeting high-lighted the $93,000 cost of the course of sipuleucel-T therapy relative to the 4-month increase in overall survival.
The Committee was asked to evalu-ate the evidence that sipuleucel-T “significantly improves” overall sur-vival and control of disease-related symptoms, and avoids or minimizes “the burdens associated with antican-cer therapy while maintaining overall survival and control of disease-related symptoms.” The panel gave the agent an intermediate confidence score in overall survival. Despite the FDA’s re-quirement to perform a postmarket-ing study of sipuleucel-T to evaluate the risk of stroke, the Committee also turned in an intermediate confidence vote that treatment-related symptoms were avoided. However, there was low confidence in the ability of sipuleucel-T to control disease-related symptoms. No confidence was related in the off-label use of sipuleucel-T in metastatic prostate cancer for moderate to severe
Health-care Reformcontinued from page 1
symptoms, in hormone-responsive metastatic prostate cancer, and when prostate cancer has not metastasized.
Like the experience with bevaci-zumab in metastatic breast cancer, the sipuleucel-T clinical trials offered little quality-of-life data.
ConclusionsFollowing the mandates of the
American Recovery and Reinvestment Act, the Institute of Medicine detailed comparative effectiveness research priorities in 2009. These three evalua-tions of biologic agents for metastatic disease in 2010 fulfill the Institute’s priorities. Each of these evaluations involves a biologic agent for incurable metastatic cancer, a lack of quality-of-life measures and outcomes data, and the implicit issue of cost. Clinical ben-efit is no longer defined by an increase in overall or progression-free survival. Now clinical benefit is defined by the AHRQ as efficacy and effectiveness, and, especially for metastatic disease, improved quality-of-life outcomes. Comparative effectiveness assess-ments that include quality-adjusted life-year (QALY) calculations will increasingly influence practice guide-lines and reimbursement.
These three evaluations were per-formed by the three most powerful agencies in the Department of Health and Human Services: AHRQ (which spearheads the Federal comparative effectiveness efforts), the FDA, and CMS. Despite originating in differ-ent agencies within the Department of Health and Human Services, each one of the evaluations has consistent language regarding clinical benefit and effectiveness. These three high-profile examples respond to increasing economic pressures and set expecta-tions for the evidence required from ongoing and future clinical trials to merit FDA approval and Medicare re-imbursement of novel agents. Those expectations include validated quality-of-life measures and outcomes data that meet QALY criteria.
In response to these clear mes-sages, clinical trials should determine symptom burden from cancer and its treatment early on in clinical tri-als. Quality-adjusted life-year calcula-tions performed early in the course of a clinical trial will provide insight into clinical benefit beyond survival, help determine the clinical trial course, and avoid restrictions in the use and reim-bursement of the agent following FDA approval. ■

ASCOPost.com | JANUARY 1, 2011 PAGE 3
52nd ASTRO Annual Meeting
The final 5-year analysis of the four-arm HD11 multicenter ran-
domized clinical trial reveals that four cycles of ABVD (doxorubicin, bleo-mycin, vinblastine, and dacarbazine) plus 30-Gy involved-field radiotherapy (IFRT) is the treatment of choice for patients with early unfavorable Hodg-kin lymphoma, according to a presen-tation by the German Hodgkin Study Group at the plenary session of the 52nd Annual Meeting of the American Society for Radiation Oncology (AS-TRO), held October 31–November 4 in San Diego.1
Study SpecificsIn the European trial, 1,395 patients
with early, intermediate-stage Hodgkin lymphoma from 328 medical centers and five countries received a regimen of 4 × ABVD plus 20- or 30-Gy IFRT; or 4 × BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vin-cristine, procarbazine, and prednisone) plus 20- or 30-Gy IFRT. Results re-vealed that while patients who received the more intensive chemotherapy and
radiotherapy regimens more often suf-fered grade 3 or 4 toxicity, the efficacy of the standard 4 × ABVD plus 30-Gy IFRT regimen was equivalent to that of both 4 × BEACOPP regimens.
Overall, the complete remission rate was 94.1%, and the freedom from treat-ment failure rate was 85% in the trial—and those complete remission and free-dom from treatment failure rates did not differ among the two BEACOPP regimens and the 4 × ABVD plus 30-Gy IFRT arm. However, four cycles of ABVD followed by 20-Gy IFRT was inferior to the other three arms, with a 5-year freedom from treatment failure difference of 5.7% (P = .052).
“Our study shows that four cycles of ABVD chemotherapy plus 30-Gy involved-field radiotherapy remains the standard treatment for early unfavor-able Hodgkin lymphoma,” said Hans Theodor Eich, MD, PhD, lead author of the study and a radiation oncologist at the University of Cologne, Germany. “Prior to the study, it was unclear what the optimal chemotherapy regimen and the most effective dose of radiation was,” he added.
Acute ToxicitiesCompared with early favorable
disease, the outcome in early unfavor-able Hodgkin lymphoma—with up to 80% long-term tumor control—still leaves room for improvement, the authors of the trial said. Thus, HD11 was begun with the aim of optimizing patient outcomes.
With a median follow-up of 91 months, 105 patients in the HD11 tri-al had died. The most frequent events were Hodgkin lymphoma, secondary neoplasias, and cardiovascular mor-tality. The investigators found no dif-ference in overall survival among the four treatments or modalities. How-ever, acute toxicities varied accord-ing to treatment regimen. Compared to those who received ABVD, more patients treated with BEACOPP de-veloped grade 3/4 toxicity (51.5% vs 73.8%, P < .001).
The most common side effects were hematologic toxicities such as leukopenia and hair loss. Acute toxicities were also more frequent among patients who received 30-Gy radiotherapy than among those who were treated with 20 Gy (12%
vs 5.7%, P < .001). The most com-mon toxicities during radiotherapy were dysphagia and mucositis.
The authors’ final conclusions included a recommendation that IFRT dose should be reduced to 20 Gy in patients with early unfavorable Hodgkin lymphoma only if accom-panied by intensified chemotherapy. They also noted that 4 × ABVD plus 30-Gy IFRT should remain the stan-dard treatment for these patients outside of clinical trials. ■Reference
1. Eich HT, Mueller RP, Diehl V, et al: Intensified chemotherapy and dose-reduced involved field radiotherapy in patients with early unfavorable Hodgkin lymphoma: Final analysis of the Ger-man Hodgkin Study Group (GHSG) randomized HD11 trial. 52nd ASTRO Annual Meeting. Abstract 2. Presented November 1, 2010.
More Intense Chemotherapy with Less Radiation No More Effective than Standard Treatment for Hodgkin LymphomaBy Barbara Boughton
Expert Point of View
The HD11 randomized clinical trial is the lat-est in a series of seminal clinical trials from the
German Hodgkin Lymphoma Study Group that has helped shaped the treatment of Hodgkin dis-ease, said Anthony Zietman, MD, Past President of ASTRO and Professor of Radiation Oncology at Massachusetts General Hospital, Boston.
Dr. Zietman noted that the HD11 trial illustrates why randomized clinical trials are needed even when there’s an established standard treatment in oncology. Although 4 × ABVD plus 30-Gy radio-
therapy is accepted as treatment for early unfavorable Hodgkin lymphoma, questions about whether it provided optimal outcomes remained.
“With three different experimental arms, you would think that one of the experimental arms would be better than the standard arm, but this didn’t prove to be the case. Although we sometimes think that new treatments are better, and giving more treatment is better, that isn’t necessarily true,” he said. “Randomized clinical trials such as HD11 help us move beyond bias,” he said.
‘Best We Have Right Now’Dr. Zietman commented that because patients with Hodgkin lymphoma
often fare very well with treatment, the emphasis has been on minimizing toxicities while still achieving the same outcomes. “The HD11 trial shows us that we can’t back off on the radiation yet for patients with early unfavorable Hodgkin disease, and more intensive chemotherapy doesn’t get you better re-sults,” he said.
Dr. Zietman added that because patients in the HD11 trial were followed for such a lengthy time, the trial’s results can be considered definitive—at least for now. “It consolidates the evidence behind what has been the standard of care,” he said, adding that “It confirms that what we’ve been doing is the best we have right now.” ■
■ Final analysis of the HD11 randomized clinical trial by the German Hodgkin Study Group showed that four cycles of ABVD followed by 30-Gy IFRT should remain the standard of care for patients with early unfavorable Hodgkin lymphoma.
■ Efficacy outcomes for patients who received 4 × ABVD + 30-Gy IFRT was equivalent to outcomes for patients treated in both BEACOPP arms of the trial, but 4 × ABVD + 20-Gy IFRT was clearly inferior to other treatments.
■ Acute toxicities were more frequent among patients receiving BEACOPP and 30-Gy IFRT. The most frequent grade 3/4 chemotherapy toxicities were hematologic effects and hair loss, and the grade 3/4 toxicities that occurred most frequently with radiotherapy were dysphagia and mucositis.
■ Patients with early unfavorable Hodgkin lymphoma should receive 20-Gy IFRT only when accompanied by intensified chemotherapy regimens.
Standard of Care in Unfavorable Hodgkin Lymphoma
Anthony Zietman, MD
Hans Theodor Eich, MD, PhD
Hematology
See page 33

PAGE 4 The ASCO Post | JANUARY 1, 2011
52nd ASH Annual Meeting
Kirit M. Ardeshna, MD, University College London Hospitals.
The average lifespan of patients di-agnosed with follicular lymphoma was 8 to 10 years, before the introduction of rituximab, Dr. Ardeshna told listeners. “Previous studies showed no improved survival for early treatment with che-motherapy vs watchful waiting in as-ymptomatic patients. Most physicians employ watchful waiting, which can de-fer the need for chemotherapy for about 2.5 years,” he continued.
Study DesignThe investigators sought to deter-
mine whether a strategy of B-cell deple-tion with rituximab could further delay the time to treatment with chemothera-py. The study enrolled 463 patients with asymptomatic stage II, III, or IV follicu-lar lymphoma. Median age was 60 years (range, 27–67 years); 54% were female; 89% had grade 1 or 2 disease; 21% had stage II, 40% had stage III, and 39% had stage IV; 42% had bone involvement.
Patients were randomly assigned in a
1:1:1 ratio to one of three arms: watch-ful waiting (arm A, n = 186); rituximab at 375 mg/m2 once a week for 4 weeks (arm B, induction therapy, n = 84); or the same induction therapy with rituximab followed by rituximab maintenance ev-ery 2 months for 2 years (arm C, n = 192).
The study was originally designed to enroll about 600 patients, but 3 years into the trial the second arm of the study was discontinued based on the efficacy of the maintenance therapy arm. At a median follow-up of 32 months, far fewer patients required chemotherapy or radiotherapy (the primary endpoint) in the rituximab maintenance arm vs watchful waiting. At 3 years after ran-domization, no new therapy was re-quired by 49% of patients in the watchful waiting arm, 80% of patients in the in-duction therapy arm, and 91% of those treated with rituximab maintenance therapy. At the time of the ASH Annual Meeting, 95% of patients were alive and no differences in overall survival were evident among the three arms.
Maintenance Rituximabcontinued from page 1
James O. Armitage, MD Editor-in-Chief
Elizabeth Reed, MD Deputy Editor Division of Hematology & Oncology University of Nebraska Medical Center Omaha, Nebraska
ASSOCIATE EDITORS
Joseph S. Bailes, MD Texas Oncology
Richard R. Barakat, MD Memorial Sloan-Kettering Cancer Center
Charles L. Bennett, MD, PhD, MPP University of South Carolina, Columbia
Douglas W. Blayney, MD Stanford University Medical Center
Philip D. Bonomi, MD Rush University Medical Center
Richard Boxer, MD University of Miami
Harold J. Burstein, MD Dana-Farber Cancer Institute
Robert W. Carlson, MD Stanford University Medical Center
Barrie R. Cassileth, PhD Memorial Sloan-Kettering Cancer Center
Jay S. Cooper, MD Maimonides Medical Center
John Cox, DO Texas Oncology
Nancy E. Davidson, MD University of Pittsburgh Cancer Institute
George D. Demetri, MD Dana-Farber Cancer Institute
Paul F. Engstrom, MD Fox Chase Cancer Center
David S. Ettinger, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
Jimmie C. Holland, MD Memorial Sloan-Kettering Cancer Center
Nora Janjan, MD, MPSA, MBA National Center for Policy Analysis
Theodore S. Lawrence, MD, PhD University of Michigan Comprehensive Cancer Center
Stephen J. Lemon, MD, MPH Oncology Associates, PC, Omaha
Michael P. Link, MD Stanford University Medical Center
John L. Marshall, MD Ruesch Center for the Cure of GI Cancer at Georgetown University
William T. McGivney, PhD, National Comprehensive Cancer Network
James L. Mulshine, MD Rush University Medical Center
Derek Raghavan, MD, PhD Taussig Cancer Center at Cleveland Clinic
Richard L. Schilsky, MD University of Chicago Comprehensive Cancer Center
Andrew D. Seidman, MD Memorial Sloan-Kettering Cancer Center
George W. Sledge, MD Indiana University
Thomas J. Smith, MD Virginia Commonwealth University
Jamie H. Von Roenn, MD Robert H. Lurie Comprehensive Cancer Center at Northwestern University
Lynn D. Wilson, MD Yale University School of Medicine
Stanley H. Winokur, MD Singer Island, Florida
INTERNATIONAL EDITORSClement Adebamowo, BM, ChB (Hons), ScD University of Ibadan Ibadan, Nigeria
Eduardo Cazap, MD, PhD International Union Against Cancer (UICC) Buenos Aires, Argentina
Mary Gospodarowicz, MD Princess Margaret Hospital Toronto, Ontario, Canada
Jacek Jassem, MD Medical University of Gdansk Gdansk, Poland
David Khayat, MD Pitie-Salpetriere Hospital Paris, France
Tony Mok, MD The Chinese University of Hong Kong Shatin, Hong Kong
Eliezer Robinson, MD National Council for Oncology Israeli Cancer Association Haifa, Israel
Nagahiro Saijo, MD, PhD Kinki University School of Medicine Osaka, Japan
Daniel A. Vorobiof, MD Sandton Oncology Centre Johannesburg, South Africa
Conor Lynch, Executive Editor [email protected]
Cara H. Glynn, Director of Editorial [email protected]
Andrew Nash, Associate Director of Editorial [email protected]
Sarah McGullam, Assistant Editor [email protected]
Michael Buckley, Graphic Designer [email protected]
Wendy McGullam, Director of Production [email protected]
Leslie Dubin, Vice-President, Director of Sales [email protected]
Anthony Cutrone, President [email protected]
John A. Gentile, Jr., Chairman [email protected]
Editorial Board
Harborside Press Publishing Staff
Contributing Writers: Charlotte Bath, Barbara Boughton, Jo Cavallo, Margot J. Fromer, Alice Goodman, Caroline Helwick, Ronald Piana, Matthew Stenger, Marian Wiseman
Contributing Artists: Portraits by Keith Witmer, Keith Witmer Illustrations
Financial disclosure information available at ASCOPost.com.
See page 33
Expert Point of View
I believe that it is too early for this important study to be practice-changing. The primary endpoint of the
study was the time until chemotherapy or radiotherapy was required. This endpoint is subjective, and it will be important to know the reasons patients “required” ther-apy and that this was consistent between the groups.
Not surprisingly, a high response rate to ritux-imab was observed. Rituximab was also very effec-tive at delaying next treatment. The observation group had a median time to treatment of 34 months, very similar to prior studies. At 36 months, 91% of the rituximab maintenance group had not required further therapy. But is this the best overall strategy for asymptomatic patients? Important issues include safety, quality of life, and response to next treatment.
The rituximab-treated groups need to be followed for their response to their next treatment (likely rituximab plus chemotherapy). Rituximab resistance can emerge following rituximab treatment, and it is likely that this will impact the subsequent response to chemoimmunotherapy. Patients will need to have a high overall response rate and complete response rate, and a long duration of remission to their treatment. Thus, longer follow-up is required to assess the overall strategy of early upfront treatment, including impact on survival.
On the positive side, the treatment appeared to be well tolerated, and it is possible that early treatment with rituximab may increase the percentage of patients who never require additional treatment.
Lastly, the U.S.-based ECOG 4402 Intergroup trial is evaluating rituximab maintenance vs rituximab retreatment in a similar population. The results of this study are anticipated shortly and may provide additional information on the optimal utilization of rituximab in this setting. ■
—David Maloney, MD, PhD Fred Hutchinson Cancer Research Center
University of Washington, Seattle
David Maloney, MD, PhD

ASCOPost.com | JANUARY 1, 2011 PAGE 5
52nd ASH Annual Meeting
Significant ResultsTime to initiation of new therapy was
significantly longer in the rituximab arm (P < .001 for each of the rituximab arms vs watchful waiting; see Fig. 1 on page 1). Overall median time to initiation of new therapy in the watchful waiting arm was 34 months, similar to a previous trial of watchful waiting by the same group of investigators.2 Median time to initiation of new therapy had not yet been reached in the two rituximab arms at the time of the ASH meeting. The rate of pro-gression-free survival was significantly greater in both rituximab-containing arms (P < .001 for each of the arms vs watchful waiting).
Rituximab was well tolerated. The investigators reported seven infections (all grade 3), five allergic reactions, and four cases of neutropenia.
Looking AheadDr. Ardeshna said the investigators
plan to follow the patients for about 7 more years to evaluate their response to chemotherapy or radiotherapy when further treatment is initiated. “A variety of regimens will be used, and most of them will probably include rituximab. Whether treating patients upfront with rituximab will ultimately impact on their survival is unknown,” he com-mented. He emphasized that the inves-tigators want to assess whether previous exposure to rituximab will affect re-sponse to chemotherapy (with or with-out rituximab).
“Watchful waiting is not dead. Ten years after diagnosis, 20% of asymptom-atic patients with follicular lymphoma will not require therapy, but we need to identify who those patients are,” he noted.
Results of a quality-of-life analysis of this trial will be forthcoming.
The study was funded by Cancer Re-search UK and sponsored by University College London. Roche provided free rituximab for the study. ■References
1. Ardeshna KM, Qian W, Smith P, et al: An intergroup randomized trial of rituximab versus a watch and wait strategy in patients with stage II, III, and IV, asymp-tomatic, non-bulky follicular lymphoma (grades 1, 2, and 3a): A preliminary analy-sis. 52nd ASH Annual Meeting. Abstract 6. Presented December 5, 2010.
2. Ardeshna KM, Smith P, Norton A, et al: Long-term effect of a watch and wait pol-icy versus immediate systemic treatment for asymptomatic advanced-stage non-Hodg-kin lymphoma: A randomised controlled trial. Lancet 362:516-522, 2003.
Expert Point of View
The trial presented by Dr. Ar-deshna for his international
collaborators asks an important question: Can rituximab delay the need for chemotherapy compared to observation? The results demon-
strated that time to next therapy was significantly longer for pa-tients treated with either r i t u x i m a b
weekly × 4 or rituximab weekly × 4 followed by rituximab maintenance once every 2 months for 2 years.
However, the critical question is whether time to next therapy is the most informative endpoint? Ultimately, the essential question
continued on page 6Andrew Zelenetz, MD
© Centocor Ortho Biotech Inc. 2010 4/10 08ADA10011
Other pathways can contribute to prostate cancer promotion.5
References: 1. Montgomery RB, Mostaghel EA, Vessella R, et al. Maintenance of intratumoral androgens in metastatic prostate cancer: a mechanism for castration-resistant tumor growth. Cancer Res. 2008;68(11):4447-4454. 2. Locke JA, Guns ES, Lubik AA, et al. Androgen levels increase by intratumoral de novo steroidogenesis during progression of castration-resistant prostate cancer. Cancer Res. 2008;68(15):6407-6415. 3. Stanbrough M, Bubley GJ, Ross K, et al. Increased expression of genes converting adrenal androgens to testosterone in androgen-independent prostate cancer. Cancer Res. 2006;66(5):2815-2825. 4. Titus MA, Schell MJ, Lih FB, Tomer KB, Mohler JL. Testosterone and dihydrotestosterone tissue levels in recurrent prostate cancer. Clin Cancer Res. 2005;11(13):4653-4657. 5. Pienta KJ, Bradley D. Mechanisms underlying the development of androgen-independent prostate cancer. Clin Cancer Res. 2006;12(6):1665-1671.
46252ALT_TabIsland_v2 1 5/6/10 12:35 PM

PAGE 6 The ASCO Post | JANUARY 1, 2011
Chemotherapy Foundation Symposium XXVIII
Important Questions
Commenting on this presentation, Leonard Saltz, MD, Head of the Colorectal Oncology
Section in the Department of Medicine at Memorial Sloan-Kettering Cancer Center in New York, noted that the issue of drug resistance is a central one in oncology.
Once a drug is working, why would it eventually stop doing so? What changes occur in the tumor? What genes are turned on and off, and what mech-anisms do they control? These are the important questions, Dr. Saltz noted.
“If we could understand what defenses are coming into play on the part of the cancer—and when—we could start to develop ways to use that informa-tion to our patients’ advantage,” he said. “The work that Dr. Abbruzzese and his colleagues have presented represents an important step toward understanding what happens when bevacizumab stops working. This is early work and does not guide treatment today, but it has the potential to help us figure out how to get the most out of bevacizumab, and possibly similar drugs, in the future.” ■
■ Although it is effective in colorectal cancer, bevacizumab is associated with the development of resistance.
■ Early studies are ongoing to identify mechanisms of resistance to bevacizumab.
■ Hopefully, these studies will lead to potential approaches to patients who experience disease progression on this angiogenesis inhibitor.
Countering Bevacizumab Resistance
Bevacizumab (Avastin) has become an established component of com-
bination chemotherapy for metastatic colorectal cancer, but several questions remain regarding use of this angiogenesis inhibitor, said James Abbruzzese, MD, The University of Texas MD Anderson Cancer Center, Houston. Speaking at the Chemotherapy Foundation Symposium, Dr. Abbruzzese said that studies are ongo-ing to identify potential mechanisms that drive resistance to bevacizumab. The hope is that identifying these mechanisms can help inform rational approaches to patients whose disease progresses on this drug.
Factors identified thus far as potentially predictive of progression include placen-tal growth factor (PlGF), basic fibroblast growth factor (bFGF), and hepatocyte growth factor (HGF). These markers are increased in patients prior to progression
on a bevacizumab-containing regimen.“PlGF also increased just after exposure
to single-agent bevacizumab and peaked prior to progression, so it may be a poten-tial predictive factor,” Dr. Abbruzzese told listeners. “There is considerable hetero-geneity and variation in the magnitude of these changes [in the identified growth fac-tors] between patients,” he continued.
Myeloid lineage activators—recruit-ment of cells from the bone marrow and peripheral blood monocytes—are also in-creased prior to progression, as are media-tors of these activators and chemotactic cytokines, he added.
The hope is that at least some, if not all, of these markers can be used for early detection of resistance to bevacizumab. The identification of these markers pro-vides therapeutic targets for the develop-ment of agents that can reverse resistance to bevacizumab-containing regimens. Such markers may allow individualiza-tion of continued antiangiogenic therapy after progression, he explained.
Strategies for Combating Resistance
Potential approaches to resistance to bevacizumab might include inhibition of PlGF signaling by vascular endothe-lial growth factor (VEGF) tyrosine ki-
nase inhibitors and tyrosine kinase inhi-bition of bFGF, he explained.
“The absence of alternative angiogenic signaling at progression may represent an opportunity for continued benefit from bevacizumab,” Dr. Abbruzzese stated.
Bevacizumab has been shown to improve progression-free survival, he continued, but the drug has variable ef-fects on overall response rates and over-all survival. The Bevacizumab Regimens Investigation of Treatment and Effects (BRITE) trial was a prospective observa-tional study with “provocative” findings, he said.1 Patients with metastatic colorec-tal cancer who continued on treatment with bevacizumab but switched the che-motherapy backbone had improved out-comes compared with those who did not continue bevacizumab.
“In both arms, patients eventually progressed on bevacizumab, suggesting that there are important mechanisms of resistance we can learn about to help develop therapies for patients whose disease progresses on antiangiogenic therapies,” Dr. Abbruzzese commented.
Finding the Underlying Mechanisms
Increased numbers of proangiogenic substances have been identified, and these can exert secondary proangiogenic effects in the absence of VEGF, he continued. Placental growth factors and other factors that recruit macrophages and monocytes influence the endothelial milieu.
“Numerous mechanisms may come into play [in the development of resis-
Mechanisms of Resistance to Bevacizumab ExploredBy Alice Goodman
James Abbruzzese, MD
Colorectal Cancer
continued on page 7
Leonard Saltz, MD
is whether early intervention is as-sociated with prolonged survival. However, this is a long-term end-point and will not be available for a number of years. Another highly informative endpoint would be time to initiation of second therapy. This would provide balance be-tween the arms. If early interven-tion delays time to second therapy, it would be a strong indication that cytoreduction at diagnosis is clinically meaningful.
Another important issue con-cerns time to rituximab resistance, although the design of this trial is not optimally suited to answer this question. Time to rituximab resis-tance is more directly addressed in the ECOG RESORT trial, which has fully accrued, and preliminary analysis may be available in 2011.
One of the critical outstanding questions is whether or not one can identify patients in whom observa-tion is appropriate. A preliminary report by Kedmi et al, “Low pro-liferation index may be associated
with longer time to first therapy in low grade follicular lymphoma,” suggests that intrafollicular prolifer-ation of less than 30% is associated with a delayed time to first therapy (approximately 60 months vs ap-proximately 19 months). If this is validated in an independent data-set, we may have an easy, low-cost method for identifying patients in whom observation would still be appropriate.
In the United States, the Lym-phoCare study by Friedberg et al ( J Clin Oncol 27:1202, 2009) report-
ed that 17.7% of newly diagnosed patients with follicular lymphoma are being observed, and 13.9% of patients are receiving rituximab monotherapy. It is likely that the re-sults presented by Ardeshna may in-crease the use of single-agent ritux-imab among observable patients with the goal of delaying initiation of chemotherapy. Further follow-up will determine if that is indeed the best choice. ■
—Andrew Zelenetz, MD Memorial Sloan-Kettering Cancer Center, New York
Expert Point of Viewcontinued from page 5

ASCOPost.com | JANUARY 1, 2011 PAGE 7
Chemotherapy Foundation Symposium XXVIII
tance]. Studies are ongoing to identify these,” he said.
To that end, Scott Kopetz, MD, Dr. Abbruzzese, and colleagues at MD Anderson Cancer Center conducted a phase II study of 40 patients in whom treatment with the combination of FOL-FIRI (leucovorin, fluorouracil, irinote-can) plus bevacizumab failed. The in-vestigators measured proangiogenic and primary cytokine levels after initiation of systemic FOLFIRI and bevacizumab, and again at distant time points when the disease progressed.2 The factors mea-sured included PlGF, bFGF, HGF, plate-let-derived growth factor (PDGF), stem cell growth factor (SCGF), interleukin (IL)-1, IL-8, and eotaxin.
“After exposure to bevacizumab alone, a heterogeneous and perhaps interesting response was observed in terms of cir-culating growth factors,” Dr. Abbruzzese said. PlGF and eotaxin increased after bevacizumab and FOLFIRI, whereas other factors decreased after initial expo-sure to bevacizumab and exposure to che-motherapy plus bevacizumab. No chang-es in PDGF were observed, for example.
“The hypothesis is that resistance mechanisms should precede clinical progression. We should be able to mea-sure these changes just prior to emer-gence of clinical resistance. Indeed that is what we found,” he continued.
Exploratory AnalysisPlGF showed a steady increase after
exposure to chemotherapy plus bevaci-zumab; bFGF showed a marked increase after exposure to bevacizumab and che-motherapy just prior to progression. In some individuals, very substantial in-creases in both of these circulating cy-tokines were observed, suggesting that serial assays of these cytokines might be able to identify patients who are showing signs of progression during continual ex-posure to bevacizumab.
An exploratory analysis showed that other cytokines are increased that medi-ate myeloid cell activation as well as re-cruitment. These include IL-8 (a second-ary proangiogenic factor), and patients with high levels of IL-8 had worse out-comes in this phase II study. Monocyte recruitment factors were also elevated as patients progressed clinically, he said.
“This small preliminary study opens the door to a number of possi-bilities and raises questions. After pro-gression on CT, there may be a subset of patients who benefit from continu-ing bevacizumab or alternating thera-
pies. Our greatest challenge would be to identify this subset and try to apply alternative strategies,” he stated.
The phase II study had several limita-tions, including the fact that mechanisms associated with resistance are not neces-sarily causative. More study is needed to prove causality, Dr. Abbruzzese noted. Further, plasma levels of these factors
may not reflect the tumor microenviron-ment. The investigators are continuing their studies to determine which of the changes in proangiogenic factors might be the most clinically relevant. ■References
1. Grothey A, Sugrue MM, Purdie DM, et al: Bevacizumab beyond first progression
is associated with prolonged overall survival in metastatic colorectal cancer: Results from a large observational study (BRITE). J Clin Oncol 26:5326-5334, 2008.
2. Kopetz S, Hoff PM, Morris JS, et al. Phase II trial of infusional fluorouracil, irinote-can, and bevacizumab for metastatic colorec-tal cancer: efficacy and circulating angiogenic biomarkers associated with therapeutic resis-tance. J Clin Oncol 28:453-459, 2010.
Bevacizumab Resistancecontinued from page 6
© Centocor Ortho Biotech Inc. 2010 9/10 08ADA10027
References: 1. Gregory CW, Johnson RT Jr, Mohler JL, French FS, Wilson EM. Androgen receptor stabilization in recurrent prostate cancer is associated with hypersensitivity to low androgen. Cancer Res. 2001;61:2892-2898. 2. Holzbeierlein J, Lal P, LaTulippe E, et al. Gene expression analysis of human prostate carcinoma during hormonal therapy identifies androgen-responsive genes and mechanisms of therapy resistance. Am J Pathol. 2004;164(1):217-227. 3. Yu S-Q, Lai K-P, Xia S-J, Chang H-C, Chang C, Yeh S. The diverse and contrasting effects of using human prostate cancer cell lines to study androgen receptor roles in prostate cancer. Asian J Androl. 2009;11(1):39-48. 4. Corey E, Quinn JE, Buhler KR, et al. LuCaP 35: a new model of prostate cancer progression to androgen independence. Prostate. 2003;55(4):239-246. 5. Loberg RD, St. John LN, Day LL, Neeley CK, Pienta KJ. Development of the VCaP androgen-independent model of prostate cancer. Urol Oncol. 2006;24(2):161-168.
47318ALT_DSA_Asize_NB_v1 1 10/12/10 7:07 PM

PAGE 8 The ASCO Post | JANUARY 1, 2011
Expert’s Corner
Earlier detection, better diagnostic tools, and more effective treat-
ments are resulting in long-term can-cer survivorship, with 62% of adults and 77% of pediatric cancer patients now living more than 5 years beyond their initial diagnosis. What’s more, for many people cancer can be treat-ed as a chronic illness, extending pa-tients’ lives for many years.
While survival rates are rising— according to the National Cancer Institute there are nearly 12 mil-lion cancer survivors in the United States—the challenge now facing many cancer survivors is how to achieve long-term quality of life after treatment has ended. According to the National Action Plan for Cancer Survivorship, fully one-third of sur-vivors say they experience ongoing physical, psychological, or financial consequences of their cancer diagno-sis and treatment.
Recognizing the need for a com-prehensive approach to long-term survivorship care, many academic medical centers, community hospi-tals and oncologists in private prac-tices are developing survivorship care programs to manage the ongoing care of their patients.
The ASCO Post talked with Mary S. McCabe, RN, MA, Director, Can-cer Survivorship Initiative at Memo-rial Sloan-Kettering Cancer Center in New York, about the various models of long-term survivorship care and how such programs can be tailored to fit both the needs of survivors and the staffing and financial resources of in-dividual hospitals and oncologists in private practice.
DefinitionsWhen is a person with cancer deter-
mined to be a cancer survivor?Mary S. McCabe: Patients should
be able to self-identify when they feel the term is appropriate and decide if they even want to use it, because for some individuals and family mem-bers, “cancer survivor” is not a term they see as relevant to their future lives. That said, a number of defi-nitions for the term have been put forward by different organizations. Starting with Fitzhugh Mullen, MD [cofounder of the National Coalition for Cancer Survivorship], who many years ago coined the term cancer sur-vivor, the definition has evolved to in-clude current patients, as well as fam-ily members, beginning at the time of diagnosis.
In planning survivorship servic-es, however, we need to delineate survivorship from other periods of care, so we take a pragmatic ap-proach and define survivorship as the period in which patients treated with curative intent have completed their initial therapy and require fol-low-up care.
GoalsWhat are the goals and components of
long-term care that need to be considered for adult cancer survivors?
Ms. McCabe: First of all, the goals ought to be comprehensive in scope yet tailored to the specific individual in terms of age, previous health prob-lems, type of cancer treatment, and length of time since treatment was completed. That said, there are impor-tant components of care that all sur-vivors need. In addition to the usual surveillance for recurrence and sec-ond cancers, we need to educate sur-vivors about the importance of cancer screening. There also needs to be a fo-cus on the long-term and late effects of treatment and any interventions that may be useful in reducing or eliminat-ing these problems. And in addition to medical problems, we need to as-sess the psychosocial problems people might have—particularly anxiety and depression.
In all our survivorship clinics, we also emphasize healthy living, includ-ing diet, exercise, and smoking cessa-tion, as well as physical rehabilitation
needs, which are often overlooked. Another important component of
survivorship care is communication. We work with survivors to be their own advocates, not only by identifying unmet needs with us, but also in com-municating with their other health-care providers.
Models of CareTalk about the cancer survivorship
program and models of care currently in practice at Memorial Sloan-Kettering Cancer Center.
Ms. McCabe: This is a large can-cer center, so our intention from the beginning was to offer survivorship programs and services across all age groups, from pediatric patients to the adult survivors of pediatric cancers, and to individuals with adult-onset cancers.
We’ve been fortunate to have long-standing, multidisciplinary follow-up clinics for our pediatric patients, but recently our focus has been on devel-oping and evaluating models of care for individuals with adult-onset can-cers. We now have a nurse practitioner (NP) care model for this population, in which the patient is transitioned at a specific time post-treatment from the oncologist to the NP. The care is then shared between the community pri-mary care provider and the NP. There is no separate survivorship clinic but rather an integrated clinic where the NP practices as part of the treatment team. For the patient, it offers seam-less care. In setting up these NP clinics, we’ve focused initially on individuals with the most common cancers, in-cluding breast, colorectal, and prostate cancers as well as some unique malig-nancies such as thoracic and thyroid cancers.
Are there other models of care, and could you discuss some of the benefits and limitations inherent in these models?
Ms. McCabe: I think it’s very im-portant that many cancer centers, community hospitals, and private practices are beginning to evalu-ate different models of care because there’s no one-size-fits-all model. What works at a big cancer center like Memorial, where the clinics are disease-specific, is certainly not going to be successful in a community prac-tice or at a local hospital. The multi-
disciplinary model is most often used in pediatrics and includes physicians, nurse practitioners, clinical psycholo-gists, and social workers who come together to see patients, as they often require follow-up by different special-ists. However, this model is resource-intensive, depends on a low volume of patients, and is not needed by every cancer survivor.
Another approach that can be very useful is the consult model, where ei-ther a physician or an NP sees patients when they finish their treatment or at a later time. The clinician pulls together all the information these patients need for planning their care going into the future. It’s often at this post-treatment visit that a treatment summary and care plan is prepared for patients and their health-care providers, includ-ing their primary care physician. This model is common and relatively easy to establish.
Our nurse practitioner model that I described is considered an in-tegrated model. This approach offers the value of moving patients to an appropriate provider and freeing up treating physicians to bring in new pa-tients, so they can focus their exper-tise on the newly diagnosed patient or the patient with late-stage disease. This model offers an easy transition for patients because they remain in the same clinic.
Role of Primary Care Physicians and Hospitals
I’ve seen studies showing that pri-mary care physicians aren’t sure what to do with cancer patients that have come back to their practice, because they don’t know what to look for in terms of late effects. Given those find-ings, I wonder how willing they are to participate in shared care survivorship programs.
Ms. McCabe: I think we’re still learning about the information needs of primary care physicians. We know that survivors are already being seen in their practices, so I think we need to be doing a lot more in terms of en-gaging professional societies in plans for education and training. We need to develop strategies for doing this at the community level, where it’s going to be the most successful.
How expensive is it to implement
A Conversation with Mary S. McCabe, RN, MAHow Cancer Survivorship Programs Enhance Quality of LifeBy Jo Cavallo
Mary S. McCabe, RN, MA
Survivorship

ASCOPost.com | JANUARY 1, 2011 PAGE 9
Expert’s Corner
hospital survivorship programs, and how feasible is it for cash-strapped hos-pitals already faced with limited finan-cial and staff resources to take on such programs?
Ms. McCabe: The financial sup-port for any new program looms large today and is an important issue. One always has to have a business plan, and this is true whether you are in a cancer center, community hospital, or oncol-ogy practice. When beginning to plan a survivorship program, one should first think about what services and re-sources already exist and how to maxi-mize their utility.
I also always try to encourage groups to see what resources are available in their community. What could you knit together in terms of a collaboration to offer cancer survivors? There are often many resources such as gym subscrip-tions and support groups that we don’t think about until we sit down and re-
view the needs of our cancer survivors.
Concluding ThoughtsIs there any advice or guidance you’d
like to share with ASCO members who are seeking to assist their patients in tran-sitioning from cancer patient to cancer survivor?
Ms. McCabe: It’s important to do a review of who needs what. We often talk about cancer survivors as if they are all the same. Many cancer survi-vors do very, very well post-treatment, and they need and want very little as-sistance in the long-term. But then there are those individuals who have
psychological difficulties in recovering from the cancer experience or who are at risk for long-term and late effects. We want to focus on these individuals and think about whether we have the resources to provide the kind of care they need or how to get them to appro-priate care. ■
Page 1 Dr. Nora Janjan and Dr. John Goodman address the personal and
societal costs of cancer treatment and in particular evaluate the role of comparative effectiveness evaluations in health-care reform.
Page 35 Dr. Stanley Winokur offers his perspective on the importance of
sharing difficult news with patients in candid yet compassionate ways.
Plus:
Page 7 Mary S. McCabe, RN, MA, speaks with The ASCO Post about long-term cancer survivorship and goals to achieve long-term quality of life once treatment has ended.
Page 25 Should Induction Chemotherapy Be Considered Standard of Care for Local-Regional Head and Neck Cancer? Dr. Marshall Posner and Dr. William Lydiatt debate this controversial yet important issue.
Inside The ASCO Post – Don't miss these important
perspectives:
References: 1. Morote J, Orsola A, Planas J, et al. Redefining clinically significant castration levels in patients with prostate cancer receiving continuous androgen deprivation therapy. J Urol. 2007;178:1290-1295. 2. Zlotta A, Debruyne FMJ. Expert opinion on optimal testosterone control in prostate cancer. Eur Urol Suppl. 2005;4:37-41. 3. Oefelein MG, Feng A, Scolieri MJ, Ricchiutti D, Resnick MI. Reassessment of the definition of castrate levels of testosterone: implications for clinical decision making. Urology. 2000;56(6):1021-1024. 4. Perachino M, Cavalli V, Bravi F. Testosterone levels in patients with metastatic prostate cancer treated with luteinizing hormone-releasing hormone therapy: prognostic significance? BJU Int. 2009;105:648-651. © Centocor Ortho Biotech Inc. 2011 1/11 08A10006
47728ALT_Island_v1 1 11/30/10 5:47 PM

PAGE 10 The ASCO Post | JANUARY 1, 2011
52nd ASTRO Annual Meeting
In the largest randomized study to test chemoradiotherapy against ra-
diation alone in muscle-invasive blad-der cancer, chemoradiotherapy with fluorouracil (5-FU) and mitomycin was associated with a 34% reduction in risk of locoregional recurrence, ac-cording to research presented at the plenary session of the 52nd Annual Meeting of the American Society for Therapeutic Radiology and Oncology (ASTRO).1 In the multicenter ran-domized trial conducted in the United Kingdom, 82% of patients were free of invasive bladder cancer 2 years after treatment with chemoradiotherapy, compared to 68% who received radia-tion alone, according to study authors led by Nicholas James, MD, an oncol-ogist at the University of Birmingham in Birmingham, England.
UK Trial“The hazard ratio for invasive blad-
der recurrence among patients receiv-ing chemoradiotherapy in our study was 0.53—recurrences were almost halved. We feel the results of the trial should impact treatment options in the United Kingdom as well as other countries,” Dr. James said. “In the U.S.A., very few patients get offered radiotherapy, and we feel these results should change that practice,” he added.
In the UK trial, 459 patients with in-vasive bladder cancer from 45 different medical centers were were randomly as-signed to receive standard-volume radio-therapy (to the tumor and whole bladder with a 1.5-cm margin) or reduced high-dose volume radiotherapy (to the tumor plus 1.5-cm margin treated to 100% [±5%] of the target dose and remaining bladder to 80% of the target dose), with and without synchronous chemother-apy with 5-FU and mitomycin. Results indicated that at 2 years the locoregional disease-free survival was 82% among those who received chemoradiotherapy,
compared to 68% among those who re-ceived radiation alone (P = .008). The investigators found no significant dif-ferences in overall survival at 2 years, although they reported a trend toward improved survival after that time.
Toxicity FindingsReducing the radiation dose to the
uninvolved bladder had minimal effect on local control or toxicity. There was also no statistically significant increase in late toxicity during follow-up (start-ing at 6 months after treatment and up to 3 months before a recurrence). Dr. James noted that survival data are rela-tively immature beyond 3 years and will be revisited after longer follow-up.
“Acute toxicity was only slightly in-creased by the addition of chemotherapy, and there was no effect from additional chemotherapy on late toxicity,” Dr. James said. “Seventy-five percent of patients re-ported no late side effects at all.”
Dr. James noted that the investiga-tors also measured bladder capacity after treatment, and the average fall in bladder volume was less than 10%. “That’s a reduction that patients are not likely to notice. Although there’s a wide-spread perception that radiotherapy leaves patients with a small shrunken useless bladder, this was not borne out at all by our patient-reported data,” he said. “Coupled with the reduced locore-gional recurrence rate seen in our trial, we feel this should make clinicians re-appraise the rela-tive roles of bladder preservation and surgery, especially in the U.S.A., where very few patients are offered bladder preservation,” he added.
Therapeutic AlternativesDr. James noted that in the UK,
radiotherapy is widely used for treat-ment of bladder cancer as an alterna-tive to surgery, especially in older, frail patients. However, the failure rate from radiotherapy alone is quite high, and about 1 in 3 patients who receive radiation alone end up with a salvage cystectomy.
Dr. James and fellow investigators are now planning a randomized clini-cal trial that will evaluate outcomes from adding the targeted agent cetux-imab (Erbitux) to chemoradiotherapy in bladder cancer treatment. “EGFR is an adverse prognostic marker in blad-der cancer, and cetuximab has a prov-
en track record as a radiosensitizer in other EGFR-positive tumor sites such as the head and neck,” he said. Results of this trial should be available in sev-eral years, Dr. James added. ■Reference
1. James N, Hussain S, Hall E, et al: Re-sults of a 2 x 2 phase III randomized trial of synchronous chemo-radiotherapy com-pared to radiotherapy alone and standard versus reduced high volume RT in muscle invasive bladder cancer. 52nd ASTRO An-nual Meeting. Abstract 4. Presented No-vember 1, 2010.
Expert Point of View
The UK trial on chemoradiotherapy for muscle-invasive bladder cancer informs clinical practice
by showing that this therapy may control the disease for a sustained period of time, and may even cure it, said Derek Raghavan, MD, PhD, Director of the Taussig Cancer Institute at the Cleveland Clinic. Chemoradiotherapy may be a good option for pa-tients who refuse to undergo cystectomy or are too frail to undergo the surgery. Yet outside the UK, radi-cal cystectomy is still likely to remain the standard of care, Dr. Raghavan said.
“The risk of local recurrence is lower with surgery, and the cure rate is high-er,” Dr. Raghavan said. “Americans, Canadians, and Australians are more heavily focused on surgical interventions than in Britain—partly because we have ad-opted more enthusiastically the surgical technology to replace the bladder with an artificial one created from the intestine,” he said.
Dr. Raghavan noted that while most patients in the UK bladder cancer study were aged 70 to 79, the average patient with muscle-invasive bladder cancer who undergoes radical cystectomy in the United States is younger. And while most patients in the UK trial had an Eastern Cooperative Oncology Group (ECOG) status of 1 or 2, those who undergo cystectomy in the U.S. are likely to have an ECOG status of 0. “So you can’t really make a head-to-head comparison in terms of outcomes,” Dr. Raghavan said.
Not a New ConceptDr. Raghavan also noted that the concept of combining chemotherapy and
radiotherapy in muscle-invasive bladder cancer is not new; the first randomized international trials combining chemotherapy and radiotherapy in this disease were published 20 years ago. “Dr. James and his colleagues have done an in-teresting and important study, but papers published 20 years ago had similar results,” Dr. Raghavan said.
“The trial confirms that chemotherapy plus radiation is better than radiation alone, and for the patient who isn’t fit to undergo cystectomy, it’s a reasonable alternative,” he said. Yet Dr. Raghavan noted that with only 2 years of follow-up, it’s difficult to appreciate whether the results regarding the effects of reducing radiotherapy dose will stand the test of time. Although the authors found no significant difference between the two approaches to radiotherapy, the small numbers of cases in each arm and the possible confounding effect of adding chemotherapy make this conclusion open to question, Dr. Raghavan added.
“I think the data regarding radiotherapy need to mature—it’s a little bit early to claim anything too dramatic. But their chemotherapy data are pretty clear, even at 2 years,” he said. ■
Chemoradiotherapy Reduces Recurrence Risk in Bladder CancerBy Barbara Boughton
■ The largest randomized trial to date shows that chemoradiotherapy with 5-FU/mitomycin is associated with a 34% reduction in risk of locoregional recurrence in muscle-invasive bladder cancer compared to radiation alone.
■ Reducing the radiotherapy dose to the uninvolved bladder had mini-mal effect on local control or toxicity.
■ There was no significant effect on late toxicity with the addition of che-motherapy to radiation treatment, and little effect on acute toxicity.
Chemoradiotherapy for Muscle-invasive Bladder Cancer
Derek Raghavan, MD, PhD,
Genitourinary Cancer
See page 33
Halaven™ is a trademark used by eisai Inc. under license from eisai R&D Management Co., ltd. © 2010 eisai Inc. all rights reserved. eRI 65
www.halaven.com
Now
AvAilAble

Halaven™ is a trademark used by eisai Inc. under license from eisai R&D Management Co., ltd. © 2010 eisai Inc. all rights reserved. eRI 65
www.halaven.com
Now
AvAilAble

PAGE 12 The ASCO Post | JANUARY 1, 2011
52nd ASH Annual Meeting
The investigational monoclonal antibody conjugate brentux-
imab vedotin (formerly called SGN-35) achieved dramatic responses in patients with relapsed or refractory Hodgkin lymphoma (HL) who had few if any other treatment options. The investigators, as well as other experts, were excited by these findings of a phase II single-arm study presented at the 52nd Annual Meeting of the Amer-ican Society of Hematology (ASH),1 which was held December 4–7 in Or-lando, Florida. Based on these study results, Seattle Genetics and Millen-nium (a wholly owned subsidiary of Takeda Pharmaceutical Company Limited) plan to seek regulatory ap-proval in early 2011 for both HL and anaplastic large cell lymphoma.
Three-quarters of the 102 high-risk patients with refractory or re-lapsed HL enrolled at 26 study centers achieved an objective response (great-er than 50% of tumor shrinkage), and 34% achieved complete remission. Overall, 94% of patients had some de-gree of tumor reduction, according to lead investigator Robert Chen, MD, Assistant Professor, Hematology and Hematopoietic Cell Transplantation at the City of Hope, Duarte, California.
“Despite responding to front-line combination chemotherapy, up to 30% of all Hodgkin lymphoma pa-tients will relapse. These patients have limited treatment options beyond au-tologous stem cell transplantation and represent a significant unmet medical need,” Dr. Chen told listeners. “Based on these data, brentuximab vedotin has the potential to change the treat-ment paradigm for relapsed or refrac-tory Hodgkin lymphoma patients, and could be the first treatment approved for these patients in more than 20 years.”
Brentuximab vedotin is an anti-body-drug conjugate consisting of an anti-CD30 monoclonal antibody and monomethyl auristatin E (MMAE), a potent antitubulin agent. The tech-nology delivers MMAE directly into CD30-expressing cells, prompting apoptosis, and appears to spare non-CD30 cells from toxicity.
Study DetailsThe single-arm study enrolled 102
patients with relapsed/refractory HL with a median age of 31 years (range, 15–77 years); 53% were female. All patients previously underwent autolo-gous stem cell transplant, and more
than 70% had primary refractory dis-ease, failing to achieve complete remis-sion or progressing within 3 months of completing front-line therapy. Also, 39% were refractory to the most recent salvage therapy (excluding autologous transplantation). The median num-ber of prior treatment regimens was 4 (range, 1–13).
Patients were treated with an outpa-tient infusion of brentuximab vedotin at 1.8 mg/kg every 3 weeks for up to 16 total doses. The primary endpoint was objective response rate as assessed by independent central review.
Median duration of brentuximab vedotin treatment was 29 weeks (range, 3–54 weeks), and the median num-ber of cycles delivered was 9 (range, 1–16). Among patients achieving a complete remission, median duration of response had not yet been reached at the time of the ASH meeting, with a median follow-up of about 1 year.
Toxicity and Response RatesSide effects (grade 1 or 2) with the
investigational drug were manageable and included peripheral sensory neu-ropathy (47%, most common), fatigue (46%), nausea (42%), upper respira-tory tract infection (37%), and diar-rhea (36%). The most common grade 3 or higher adverse events included neutropenia (20%), peripheral senso-ry neuropathy (8%), thrombocytope-nia (8%), and anemia (6%).
Dr. Chen acknowledged that pe-
ripheral neuropathy was an issue, but said few patients had grade 3 or 4 neuropathy. “Overall, two-thirds of the patients with neuropathy showed improvement or resolution of the side effect during the course of treatment,” he commented.
In addition to the impressive 75% objective response rate and 34% com-plete remission rate, 22% of patients had stable disease, 3% had progressive disease, and 1 patient was not evalu-able for response. Progression-free survival among all patients was 25 weeks by independent review and 39 weeks by investiga-tor assessment. At the time of the ASH meeting, progres-sion-free survival had not yet been reached in patients who achieved complete remission.
“Brentuximab vedotin achieves high response rates, has low toxicity, and because of these qualities, outpa-tient treatment allows patients to con-tinue their daily routine. It has few side effects and most are reversible,” Dr. Chen said. ■Reference
1. Chen R, Gopal AK, Smith SE, et al: Results of a pivotal phase 2 study of bren-tuximab vedotin (SGN-35) in patients with relapsed or refractory Hodgkin lym-phoma. 52nd ASH Annual Meeting. Ab-stract 283. Presented December 6, 2010.
Brentuximab Vedotin Offers Hope for Patients with Relapsed/Refractory Hodgkin LymphomaBy Alice Goodman
Expert Point of View
This promising drug offers a new treatment option for patients with re-lapsed/refractory Hodgkin lymphoma who have no other options,” stat-
ed Ginna Laport, MD, Associate Professor of Medicine, Division of Blood & Marrow Transplantation, Stanford University School of Medicine, Stanford, California. Dr. Laport moderated an official American Society of Hematol-ogy (ASH) press conference, where these data were released at the 52nd ASH Annual Meeting.
“The results are very exciting, with a 34% complete response rate and 75% objective response rate. Peripheral neuropathy is an issue, but it is tolerable. Several of my patients have received this agent. It is administered intrave-nously every 3 weeks or on an outpatient basis, and I have seen both partial and complete responses. This novel antibody-drug conjugate also has activity in other CD30+-positive expressing lymphomas such as anaplastic large cell lymphoma,” she said. ■
■ Patients with relapsed or refractory Hodgkin lymphoma have few curative treatment options other than autologous stem cell transplant.
■ Brentuximab vedotin achieved high objective response rates and complete remission rates in a heavily pretreated, high-risk group of patients with Hodgkin lymphoma.
■ The drug will be submitted to the FDA for regulatory approval based on results of the phase II trial reported at ASH.
Brentuximab Vedotin, Breakthrough Drug for Hodgkin Lymphoma
Hematology
Visit The ASCO Post website at:
ASCOPost.com
New!
See page 33

DEADLINE FOR ABSTRACT SUBMISSION IS FEBRUARY 2nd, 2011 For the 47th Annual Meeting of the American Society of Clinical Oncology
Submit your abstract to be considered for presentation or publication at the 47th Annual Meeting, to be held June 3-7, 2011, at McCormick Place, Chicago, Illinois.
Contribute to the premier oncology Meeting by submitting your original research abstract of 300-350 words today. Visit the Call for Abstracts section of ASCO’s Annual Meeting website, asco.org/cfa, for a complete list of this year’s scientific tracks. There, you’ll also find detailed information on Annual Meeting abstract policies, submission requirements, and the abstract selection process, as well as Coauthor Disclosure Forms and Frequently Asked Questions.
Deadline for submission is February 2, 2011 at 11:59 PM (EST).
June 3-7, 2011 | McCormick Place | Chicago, IL

PAGE 14 The ASCO Post | JANUARY 1, 2011
Direct from ASCO
As part of its mission to fight can-cer around the world, ASCO
collaborates in many activities with regional and international cancer so-cieties. ASCO’s International Affairs Committee takes the lead in recom-mending educational partnerships to benefit the global oncology commu-nity at large and patients with cancer worldwide.
The brief reports that follow provide examples of the challenges and activities of oncology societies in four countries, and ways in which ASCO interacts with these societies to advance their missions.
Nigerian Society Addresses Need for Knowledge among Professionals, Public
In Nigeria, lack of awareness and understanding of cancer—among both the public and professionals—is one of the biggest barriers to effective cancer care, according to Clement A. Adebamowo, MD, ScD, an onco-logic surgeon who is President of the Society of Oncology and Cancer Re-search of Nigeria (SOCRON).
Dr. Adebamowo explains that patients with cancer don’t present with signs and symptoms like the classic cases in medical textbooks, in part because the Nigerian popula-tion is comparatively young. “A can-cer diagnosis is often last on the list of differential diagnoses. The high prevalence of infectious diseases also lulls clinicians into a reduced index of suspicion.” In addition, following diagnosis, patients with cancer are often treated inappropriately, he says.
The lack of early diagnosis and ap-propriate treatment then leads peo-ple to doubt the efficacy of “West-ern” treatment. “The entire situation reinforces notions about alternative explanations for the etiology of can-cer and shifts the preference toward ‘traditional’ or ‘spiritual’ treatments,” Dr. Adebamowo says.
Nigeria’s lack of organized and ad-equate health-care financing is also a major barrier to cancer care. Not able to afford care, patients do not present when the disease is at an early stage, hoping it will go away. “They try to raise funds from friends and family, causing further delay. The advanced stage of disease leads to poor out-
comes, making people unwilling to support treatment of future patients because of a perceived futility of such efforts in the past.”
In 2003, Dr. Adebamowo, who is currently the Chair of ASCO’s Inter-national Affairs Committee, received an International Development and Education Award (IDEA) from The ASCO Cancer Foundation®. The IDEA program identifies early-career oncologists in developing countries and offers experiences and mentor-ing in leadership development. As an IDEA recipient, Dr. Adebamowo recognized the power a professional organization could have in advo-cacy, education, and research, and he worked with colleagues in Nigeria to create SOCRON in 2005.
“Without ASCO, there would be no SOCRON—period,” he com-ments. “The ASCO leaders we in-teracted with were tremendously supportive and have remained en-gaged—traveling to Nigeria to give presentations, mentoring Nigerian oncologists, and opening doors for SOCRON to take advantage of op-portunities.”
Now with 400 members, SOCRON provides education and information for both professionals and patients on its website, and in 2008 held its first International Con-ference on Modern Cancer Manage-ment, which was standing room only at all of its sessions. SOCRON will hold a second conference in Febru-ary 2011. “You guessed it—ASCO is already supporting the meeting by providing international faculty,” Dr. Adebamowo comments.
Oncology training is still “fairly ru-dimentary” in Nigeria, with only a few centers offering training of reasonable quality, Dr. Adebamowo says. Some physicians have received medical on-
cology training out of the country, but very few return to Nigeria to practice. Chemotherapy is given by hematolo-gists as well as radiation, surgical, gy-necologic, and pediatric oncologists, complemented and supported by the patient’s primary care physician.
Chinese Society Focuses on Medical Education, Research
Shukui Qin, MD, the President of the Chinese Society of Clinical On-cology (CSCO), says that CSCO’s goals encompass the development of continuing medical education, en-hancement of multidisciplinary col-laboration and academic exchange, encouragement of multicenter re-search, and promotion of standard-ized tumor diagnosis and treatment so as to benefit patients with cancer in all of China.
Founded in 1997, the 10,000-mem-ber society has several robust educa-tional programs in addition to its an-nual meeting, which last year attracted 15,000 people. In one such program, expert oncologists travel to western China and outlying communities to give presentations on the latest devel-opments in tumor diagnoses, radio-therapy, molecular target therapy, and other fields. “So far, tens of thousands of physicians have benefited from lec-tures, and their clinical and research ability has been boosted as well,” Dr. Qin reports.
Another educational activity is CSCO’s thematic academic forums, which include presentations by in-ternational experts on specific topics. Thematic forums have been presented on lymphoma; gastrointestinal, lung, and breast cancers: molecular target-ed therapy; and biologic therapy.
CSCO has also created a charitable foundation. In 2002 it founded the Science Foundation of China Clinical Oncology, which supports clinical re-search, continuing medical education, professional training, and internation-al academic communication.
Currently, lung and stomach cancer are the two most frequent types of cancer in China for both sexes combined, although among women breast cancer has the high-est incidence. An increase in cancer rates looms in China because of the
high use of tobacco in the country. With 20% of the world’s population, China consumes 30% of the world’s cigarettes, according to the American Cancer Society website.
The interaction between ASCO and CSCO becomes stronger every year. For example, attendance at the Best of ASCO conference grew from 600 in 2009, the first year it was held in China, to nearly 900 participants a year later—one of the largest Best of ASCO meetings in the world.
ASCO’s IDEA program is an-other strong tie between the two or-ganizations. The IDEA grant covers expenses for an individual to attend the ASCO Annual Meeting and visit a cancer center, and it establishes a scientific mentoring relationship be-tween leading oncologists in ASCO and the award recipients. China has consistently had the highest or second-highest number of IDEA ap-plications, and 14 awards have been given to Chinese oncologists.
Dr. Qin notes, “While constantly improving itself, CSCO pays atten-tion to the introduction of foreign advanced technology and scientific management experience.”
Advancing Research a Goal of Latin American Society
Founded in 2004, SLACOM—the Latin American and Caribbean Soci-ety of Medical Oncology—already has 2,000 members. It includes all of South and Central America as well as the Caribbean. As might be expected in such a huge area, the prevalence of cancers varies widely. SLACOM’s founder and President, Eduardo Cazap, MD, a medical oncologist and cancer researcher in Buenos Aires, de-scribes some of these variations:
The cancer incidence and mortal-
Oncology Societies Advance Cancer Care around the WorldASCO Is Partner in Education, Leadership Development
Eduardo Cazap, MD
Clemente Adebamowo, MD, ScD
continued on page 17

ASCOPost.com | JANUARY 1, 2011 PAGE 15
Direct from ASCODirect from ASCO
Vol 28, No 34 December 1, 2010
OURNAL OFLINICALNCOLOGY
Official Journal of the American Society of Clinical Oncology www.jco.org
JCO
JCO
Impact of Androgen-Deprivation Therapy on Cognitive Function in Men WithNonmetastatic Prostate Cancer. S.M.H. Alibhai et al
Impact of Androgen-Deprivation Therapy on Physical Function and QOL inMen With Nonmetastatic Prostate Cancer. S.M.H. Alibhai et al
Optimizing Collection of Adverse Event Data in Cancer Clinical TrialsSupporting Supplemental Indications. L.D. Kaiser et alEditorial: D.J. Sargent et al
Availability of Experimental Therapy Outside of Randomized Clinical Trials inOncology. E.P. Hamilton et al
Survival Patterns in Patients With Hodgkin’s Lymphoma With a Pre-ExistingAutoimmune Disease. O. Landgren et al
Prospective Analysis of Hepatitis B Virus Reactivation in Patients With DiffuseLarge B-Cell Lymphoma After Rituximab Combination ChemotherapyN. Niitsu et al
Bortezomib-Melphalan-Prednisone-Thalidomide Followed by ContinuousTreatment With Bortezomib-Thalidomide Compared With Bortezomib-Melphalan-Prednisone for Initial Treatment of Multiple Myeloma: ARandomized Controlled Trial. A. Palumbo et al
Phase I Study of Everolimus Plus Weekly Paclitaxel and Trastuzumab inPatients With Metastatic Breast Cancer Pretreated With TrastuzumabF. Andre et al
Review Article: Strategies for Prolonged Therapy in Patients With AdvancedNon–Small-Cell Lung Cancer. P. Fidias et al
Art of Oncology: Stand and Wait. G.F. Blackall
What’s Hot in JCO OnlineTop 10 most-accessed articles recently published in Journal of Clinical Oncology
JCO.org
1. Stand and Wait George F. Blackall 28(34):5124
2. Another Step Toward the Cure of Metastatic Renal Cell Carcinoma? Nicholas J. Vogelzang 28(34):5017
3. Strategies for Prolonged Therapy in Patients With Advanced Non–Small-Cell Lung Cancer Panos Fidias, et al 28(34):5116
4. Clinical Trials Data Collection: When Less Is More Daniel J. Sargent 28(34):5019
5. Favorable Response to Gefitinib Treatment of Lung Adenocarcinoma With Coexisting
Germline and Somatic Epidermal Growth Factor Receptor Mutations Kuei-Pin Chung, et al 28(34):e701
6. Bortezomib-Melphalan-Prednisone-Thalidomide Followed by Maintenance With Bortezomib-Thalidomide Compared With Bortezomib-Melphalan-Prednisone for Initial Treatment of Multiple Myeloma: A Randomized Controlled Trial Antonio Palumbo, et al 28(34):5101
7. Phase I Study of Everolimus Plus Weekly Paclitaxel and Trastuzumab in Patients With Metastatic Breast Cancer Pretreated With Trastuzumab
Fabrice Andre, et al 28(34):5110
8. Miliary Brain Metastases in Lung Cancer Anne-Marie Ruppert, et al 28(34):e714
9. Pilot Study Using Molecular Profiling of Patients’ Tumors to Find Potential Targets and Select Treatments for Their Refractory Cancers Daniel D. Von Hoff, et al 28(33):4877
10. Bisphosphonate Risks and Benefits: Finding a Balance Julie R. Gralow 28(33):4873
The oncology community con-tinues to experience shortages
of many critical therapies, including but not limited to doxorubicin, leu-covorin, cisplatin, etoposide, nitro-gen mustard, vincristine, propofol and morphine. As ASCO continues to provide its members and oncology professionals with the most current information on these shortages and progress toward potential solutions, it is crucial that the Society hears how these shortages are affecting your practices.
“I would encourage oncology pro-
fessionals to please report the short-ages they are experiencing to ASCO, the FDA, or to the American Soci-ety of Health-System Pharmacists (ASHP),” said ASCO President-Elect Michael P. Link, MD. “The more physicians report, the bet-ter idea the FDA has of the current scope of the shortages. “
Oncology professionals can in-form ASCO on how these shortages are affecting their practices by con-tacting the Society at [email protected] or 571-483-1368. Also, please inform the FDA of these
shortages at [email protected] or ASHP at http://www.ashp.org/DrugShortages/Report/.
In November, ASCO co-con-vened a summit on drug shortages with the ASHP, the American So-ciety of Anesthesiologists, and the Institute for Safe Medication Prac-tices. The summit, which represent-ed a first step in initiating dialog on potential solutions, also included key stakeholders from pharmaceuti-cal manufacturers, supply chain en-tities, and the FDA. While there is no single reason or solution for the shortages, summit participants de-veloped several recommendations, including:
1. Improve rapid communication between the pharmaceutical supply
chain and providers, so providers have more advanced notice to better anticipate and manage shortages
2. Remove the barriers faced by drug manufacturers and the FDA to minimize the impact of drug short-ages, such as establishing processes for potentially extending the expira-tion date of a drug in short supply if it still meets safety requirements
3. Clarify the definition of “medi-cally necessary,” which is the term that prompts notifications to the FDA related to drug shortages, to ensure the FDA is aware of short-ages in a more timely manner. ASCO is working with summit par-ticipants on solutions to ensure our patients have access to vital cancer therapies. ■
Oncology Drug Shortages: ASCO Working to Provide Information and Solutions
Save the Date2011 Genitourinary Cancers Symposium
February 17-19, 2011Orlando World Marriott
Orlando, Florida

PAGE 16 The ASCO Post | JANUARY 1, 2011
Direct from ASCO
In July 2010, the American Society of Clinical Oncology launched its
social networking site, ASCOcon-nection.org, along with its revamped member magazine of the same
name. Since the launch, the number of bloggers featured on the site has climbed to 11, including such lead-ers in the field as ASCO President George Sledge, MD; Immediate Past
President Douglas Blayney, MD; and ASCO Connection Editor-in-Chief and gynecologic cancer expert Jona-than S. Berek, MD, MMS.
“ASCO Connection allows
ASCO leaders to talk directly with ASCO’s membership (both domes-tic and international) on issues of the day,” says Dr. Sledge. “As more phy-sicians adopt social media, it’s vital for ASCO to have an online meeting place for member-to-member com-munication, and ASCO Connection is that forum.”
The blogs, which continue to be the star attraction on the site, pro-vide insider insight on such topics as end-of-life care, the politics and policies affecting the practice of on-cology, the growing challenges of cancer care worldwide, physicians’ use of social media, and, of course, the science and research affecting the future of cancer care. When Dr. Sledge posts a blog (“Smart Tumors Need Smart Systems”) about an article that altered his “view of the cancer world,” people take notice.
Other featured bloggers on the site include ASCO International Affairs Committee Chair Clement Adebamowo, MD, ScD; Director of the Yale Breast Center at Smilow Cancer Hospital Anees Chagpar, MD; Journal of Oncology Prac-tice Editor-in-Chief John V. Cox, DO, MBA, FACP; Immediate Past Chair of the Integrated Technology Committee L. Michael Glodé, MD; CME Chair for the Association of Physician Assistants in Oncology Heather Hylton, MS, PA-C; Journal of Oncology Practice and Cancer.Net Editorial Board Member Rob-ert Miller, MD; Professor of Medi-cine at Northwestern University’s Feinberg School of Medicine Jamie Von Roenn, MD; and ASCO Board of Directors Member Peter Yu, MD.
Opportunities for Member Networking
The opportunities for conversa-tion, networking, and debate extend beyond the featured blogs. The dis-cussion Forums on ASCOconnec-tion.org give ASCO members and registered guests an online platform for making contacts, asking a quick question, or starting discussion threads on oncology-related topics of their choice.
The member Magazine page fea-tures an interactive digital edition of the latest issue as well as exclu-
Top Oncology Leaders Blog on ASCO’s Social Networking Site
continued on page 17

ASCOPost.com | JANUARY 1, 2011 PAGE 17
Direct from ASCODirect from ASCO
ity rates in some countries, such as Uruguay and Argentina, are similar to those in the United States, with breast, lung, colon, and prostate cancers in the lead. In contrast, in countries on the Pacific side of South America, including Chile, Peru, and Ecuador, gastric and gallbladder can-cers are more prevalent.
Even within the same country, can-cer epidemiology can vary widely, Dr. Cazap explains. Big cities in Argentina and Brazil, for example, have differ-ent cancer rates than those found in the Argentina’s northern provinces or the Brazilian jungle. Each country’s health-care strategy and cancer con-trol plans must be adapted to the local and regional realities, he points out.
The incidence and mortality for many cancers is rising in most Latin American countries, largely due to the aging of the population, urban-ization, and the westernization of lifestyles. Two barriers to effective cancer care are the lack of organized strategies for primary and second-ary prevention and the limitations in access to care, Dr. Cazap says. Con-tributing to these obstacles is the fact that research is poor at the local and regional level, so the population data available are scarce or fragmented.
ASCO is furthering research in less-developed countries through its International Clinical Trials Workshop, which features research education that is adapted to local issues of accrual, informed consent, and regulation. Re-search nurses and data managers par-ticipate in the workshop along with physicians. In 2009, Argentina was the
site of ASCO’s first International Clini-cal Trials Workshop. Dr. Cazap, who is an ASCO Board of Directors Member and liaison to ASCO’s International Affairs Committee, says that the Ar-gentina workshop served as a pilot that has led to improvements in later work-shops, now slated for Egypt, Romania, and Uruguay in 2011.
“ASCO was instrumental in the organizational development of SLA-COM,” Dr. Cazap states, noting that ASCO helped support the organi-zational training and mentoring for SLACOM senior staff. ASCO and SLACOM continue to collaborate in a number of ways, presenting four Best of ASCO meetings in the region annu-ally and planning additional Interna-tional Clinical Trials Workshops after the one in Uruguay in 2011.
“ASCO and SLACOM are ideal partners,” Dr. Cazap notes. “ASCO can provide scientific and organi-zational expertise, well-developed programs, and prototypes for SLA-COM’s own future programs. For its part, SLACOM can provide local and regional advice, collaboration in edu-cation, and promotion of ASCO in Latin America. As ASCO expands its international program, Latin Ameri-can experiences and pilots serve as examples that can be duplicated in other regions of the world.”
Japanese Oncology Societies Advance Oncology Training, Standards
Cancer is the primary cause of death in Japan, where incidence of the disease is growing. Two oncol-ogy societies—the Japanese Society of Medical Oncology ( JSMO) and the Japan Society of Clinical Oncol-
ogy ( JSCO)—have worked together to educate oncologists and influence health-care regulation to improve cancer care. Most of JSMO’s approxi-mately 8,000 members are medical oncologists, whereas surgical oncol-ogists represent over half of JSCO’s more than 17,000 members.
Yoshihiko Maehara, MD, Chief Director of JSCO, notes that smok-ing rates are much higher and cancer screening rates are much lower in Ja-pan than in the United States. Public education about cancer prevention is inadequate, and JSCO is intensifying its public outreach and cancer pre-vention activities.
Both Dr. Maehara and Kazuo Tamura, MD, JSMO President, point to a shortage of qualified oncology spe-cialists as a barrier to cancer care in Ja-pan. Accordingly, a number of the two organizations’ activities focus on on-cology training, continuing education, and promoting high standards of care.
In 2007, JSCO and JSMO joined forces with several other cancer-related organizations in Japan to form the Jap-anese Board of Cancer Therapy, which has certified nearly 8,000 physicians who have basic knowledge of oncology. But only 451 medical oncologists have been certified by JSMO so far, and Dr.
Tamura says he would like to see up to 4,000 certified medical oncologists. He reports that only about half of Japan’s medical schools have an independent department of neoplastic diseases, and JSMO is urging academic centers to es-tablish medical oncology departments.
ASCO has strong ties with both JSCO and JSMO as well as Japanese oncologists individually, many of whom are ASCO members. In fact, ASCO has more members from Ja-pan than from any country outside the United States. Japan is also well represented at the ASCO Annual Meeting. Among international at-tendees at the 2010 Annual Meeting, the number from Japan was second only to the number from Germany.
ASCO partners with both JSCO and JSMO to hold joint symposia at their annual meetings. In addi-tion, ASCO holds the Best of ASCO meeting in Japan each year in collab-oration with JSMO. Dr. Tamura and Dr. Maehara both value ASCO’s col-laborations with their organizations. Dr. Maehara comments, “ASCO is the world’s leading organization for cancer care. We recognize that it is highly significant for us to interact with ASCO.” ■
© 2011. American Society of Clinical Oncology. All rights reserved.
Yoshihiko Maehara, MD
Kazuo Tamura, MD
Receiving a diagnosis of cancer can be overwhelming for your
patients. To help them navigate the road ahead, Cancer.Net (www.cancer.net), ASCO’s patient web-site, features the guidance for those who have been newly diagnosed. As a starting point, encourage your
Help Your Newly Diagnosed Patients Know Where to Start sive interviews with State Affiliate
leaders and past award winners. The Member News column highlights ASCO member career changes, publications, and awards, as well as behind-the-scenes articles on how various members pursue a work-life balance—for some it’s golf; for oth-ers it’s white water rafting or bungee jumping, to name a few.
Plans are also underway to create group functionality on the site and enable direct member-to-member messaging.
It’s Easy to Join the Discussion
ASCO members who log in to the site with their ASCO.org username and password have immediate access to read and comment on all content. Nonmembers who register a guest account with ASCO.org can read and post on selected topics.
Visit the site today at ASCOcon-nection.org. For questions and com-ments or for Member News sub-missions, please send an e-mail to [email protected]. ■© 2011. American Society of Clinical Oncology. All Rights Reserved.
patients to read about first steps to take (www.cancer.net/firststeps), including learning about the diag-nosis, finding medical care and sup-port, and getting organized. In addi-tion, they can find comprehensive information about more than 120 specific types of cancer and cancer-related syndromes (www.cancer.net/cancer). ■© 2011. American Society of Clinical Oncology. All Rights Reserved.
Oncology Leaders Blogcontinued from page 16
Oncology Societiescontinued from page 14




ASCOPost.com | JANUARY 1, 2011 PAGE 21
35th ESMO Congress
New biologic therapies are a mixed blessing, said participants in a
debate on whether access to these new drugs will improve survival. The new drugs are quite costly, and although some of them may significantly im-prove progression-free survival (PFS), with few exceptions, they have yet to show a substantial benefit in overall survival (OS).
“We are here because treatment costs have skyrocketed for innovative therapies and there will be new rules for the game. In different countries it can take up to 1 year for access to these drugs as well as reimbursement,” said Thomas Szucs, MD, University of Ba-sel, Switzerland, who moderated the debate during the 35th ESMO Con-gress, held recently in Milan, Italy.
Ivar S. Kristiansen, MD, of the University of Oslo, Norway, assumed the Pro position and Franz Porzsolt, MD, University of Ulm, Germany, ar-gued the Con position. However, there was less disagreement than agreement between these participants.
Lesson from Cardiovascular Investigations
Dr. Kristiansen pointed out that clinical trials of ACE inhibitors and statins demonstrated only small im-provements in survival, yet 2 decades after their introduction, mortality in Norway declined more than 50%.
“Clinical trials [of cardiovascular drugs] at the time showed only modest survival gains, yet overall, these drugs have made a big difference,” he said. “This could be the case with the new biologics,” he suggested.
“Various trials of biologic thera-pies demonstrate a prolongation of 0.1 to 0.4 years in OS, which critics call a
Debate on Whether Novel Agents Will Improve Survival Revealed Little Difference between Pro and Con PositionsBy Alice Goodman
modest gain. However, this is similar to the cardiovascular clinical trials,” Dr. Kristiansen stated.
Clinical trials of new cancer drugs tend to show bigger differences in PFS compared to older drugs but only small, if any, differences in OS.
Dr. Kristiansen took issue with use of PFS as an endpoint in clinical trials. “Most trials [of new biologics] focus on PFS, but oncologists should require data on OS for new drugs, not a surro-gate endpoint of PFS,” he stated.
Cost-Benefit ConsiderationsEven though novel agents are avail-
able, many patients in different coun-tries don’t have access to these drugs because the governments are not will-ing to pay for them, Dr. Kristiansen re-minded listeners.
Two novel agents have fared differ-ently with regard to reimbursement in Norway, he continued. Trastuzumab (Herceptin) was found to prolong life by 2.7 years in one study of HER2-pos-itive breast cancer, at an estimated cost of €19,000 per quality-adjusted life-year (QALY). Bevacizumab (Avastin) was found to prolong life expectancy by 0.41 years in a study of metastatic colorectal cancer, at an estimated cost of €83,000 per QALY. The threshold for cost-effectiveness in Norway is €62,500 per QALY, so the government will pay for trastuzumab but not for bevacizum-ab in metastatic colorectal cancer.
“The cost of novel treatments should reflect the benefit,” he stated. “If patients are denied access because of cost, the drug prices may be too high. We need a reasonable balance between cost and benefits,” he told listeners.
Although he believes that all pa-tients should have the opportunity to attain their full health potential, worry-ing inequalities exist in the European Union countries with regard to levels of cancer control and care, he stated.
Endpoints ReconsideredTaking the Con position, Dr. Porz-
solt said that an unpublished study he was involved in found that out of 106 clinical trials using time to progression (TTP) as an endpoint, only 43 showed a significant difference in TTP, and of those only 44% also demonstrated a statistically significant difference in OS. Out of 74 studies using PFS as an end-point, 31 showed a statistical difference in PFS, and of these, only 50% had a significant OS benefit.
These studies had inconsistent defi-nitions of TTP and PFS. More than one-third (37%) did not define TTP, 37% used PFS as an endpoint but claimed TTP findings, and 26% had a definition of TTP. This paper will be submitted for publication in a peer-review journal, Dr. Porzsolt said.
“The totality of evidence from these studies suggests that if a novel drug pro-longs TTP/PFS, the chance of the drug also prolonging OS is 50%. If a novel drug does not prolong TTP/PFS, the chance that it won’t prolong survival is around 90%,” he stated.
Perceived ValueThe perceived value of treatment ap-
pears to be different for physicians and patients, he continued. “Studies show that doctors and patients care about different things. In general, doctors are focused on disease control, while pa-
tients are more concerned about qual-ity of life,” he told listeners.
In addition to differences in per-ceived values, information from doc-tors may be confusing to patients. For example, physicians often present relative risk reductions with a new treatment, whereas patients generally want to know the absolute risks and benefits.
Another issue is the connection be-tween cost and effectiveness in doctors’ minds. Dr. Porzsolt cited a study of 82 medical students randomly assigned to what they were told was an expensive or cheap painkiller, but they all actually received placebo.1 All participants re-ceived electric shocks before and after taking the pill. A greater reduction in pain was observed among those ran-domly assigned to the so-called expen-sive drug.
“This study should go in every med-ical textbook. This demonstrates the power of information. An expensive treatment can generate hope and per-ceived safety, as well as somatic effects like reduction in pain,” he stated.
Bottom LineThe major issue with novel thera-
pies is whether cost is in line with the benefit. The bottom line is that novel drugs don’t necessarily improve sur-vival, he summarized.
“If it were possible to identify pa-tients with the highest chance of re-sponse to a new therapy, economic risks could be reduced. But this hap-pens so far only in ‘Wonderland,’” he said, “unfortunately not yet within the current health-care systems.” ■Reference
1. Waber RL, Shiv B, Carmon Z, et al: Commercial features of placebo and thera-peutic efficacy. JAMA 299:1016-1017, 2008.
Ivar S. Kristiansen, MD
Thomas Szucs, MD
Franz Porzsolt, MD
■ For the most part, new biologic therapies prolong progression-free survival but not overall survival.
■ The cost of novel agents is quite high, and reimbursement may be denied, depending on the country.
■ Access to novel agents could be broadened if survival gains could be demonstrated for subpopulations of patients.
Impact of Novel Agents on Survival and Cost of Care
See page 33

PAGE 22 The ASCO Post | JANUARY 1, 2011
Health-care Policy
policy experts feel that legislators will attempt to put a longer-term “patch” in place, possibly 3 to 5 years. However, many in Congress want to wash their hands of the SGR altogether by hand-ing control of Medicare issues over to an independent entity. Joseph S. Bailes, MD, Past Chair of ASCO’s Government Relations Council, told The ASCO Post, “In the health-care reform bill, there’s an Independent Medicare Payment Ad-visory Board, known as IPAB, which is broadly charged with reviewing Medi-care with an eye toward increasing effi-ciencies and reducing costs, etc, without
harming services. In my view, an inde-pendent group with authority to make recommendations that Medicare could implement without Congressional ac-tion is worrisome. We’ve always worked with Congress on oncology issues, such as equitable reimbursement for practice services and therapeutics. Losing politi-cal interaction with legislators is prob-lematic, not just for oncology but for
medicine in general.”Dr. Bailes said that a lack of knowl-
edge about the true costs of providing cancer care is one of the underlying problems. “Over the years, trying to convey actual oncology practice costs to policymakers has been a contentious process. At ASCO, we commissioned a survey by the Gallup Organization to provide evidence of actual practice expenses to Congress. That survey was used in 2004 to revamp some chemo-therapy administration codes. How-ever, as a general rule, the costs that Medicare uses are determined by a sur-vey conducted by the AMA, in which community oncology is underrepre-sented by data that do not capture the true costs and complexity involved in delivering high-value cancer care.”
The SGR Cost-Control MythEnacted in 1997, the Congressional
Budget Office (CBO) and Congress originally expected the SGR to lower physician payments below levels of the previous method, the Medicare Vol-ume Performance Standard (MVPS). At first, payment rates for physicians kept pace, but by 2002, the increase in volume and complexity of services pro-duced a larger-than-expected cut in pay-ment rates, 4.8%. And, as we now know, that was only the beginning.
“The SGR has not worked in con-trolling costs, and we’re left holding this giant bill that no one wants to pay. Congress continues to ‘patch’ the SGR, but it refuses to fix it. Now we’re left with the worst of both worlds—you’ve not controlled costs and you’ve placed the entire Medicare program on the precipice of collapse,” said ASCO CEO Allen S. Lichter, MD.
Dr. Lichter pointed out that Medi-care’s SGR problem has a disproportion-ate effect on the oncology community. “The current challenges in Medicare re-imbursement affect every specialty, but they hit oncology especially hard. For one thing, almost 50% of all cancer pa-tients are Medicare beneficiaries, so we are vastly overrepresented in the CMS payer model. Second, Medicare bun-
Medicare fee schedule was once again kicked aside, a political football that most policymakers acknowledge is fatal-ly flawed but few want to tackle, especial-ly when the price tag for what’s known on Capitol Hill as the “doctor fix” would cost taxpayers in excess of $200 billion. Although the SGR ticks up and down by percentage points, one reality remains: a physician fee cut of more than 21% looms unless Congress acts to avert it.
The SGR Oncology ProblemThe SGR is more than another
wonky term in the lexicon of health-care reform—leaders in oncology warn it portends a fiscal crisis for the cancer care community with no solution at hand. According to David Eagle, MD, President of the Community Oncology Alliance (COA), additional cuts to al-ready financially challenged oncology practices will sharply reduce access to care. “COA’s Components of Care sur-vey found that in 2008, Medicare paid only 57% of actual infusion costs. That is a huge payment shortfall, one of the reasons practices across the country are joining hospital groups, closing satellite facilities, and cutting staff, or closing al-together. If the SGR cuts go through, this trend will accelerate with disas-trous results,” Dr. Eagle said.
Asked whether the SGR needs to be fixed or eliminated, Dr. Eagle re-sponded, “It needs to be scrapped. The concept behind SGR is wrong, it holds physicians responsible for the overall growth in health-care spending even though the vast majority of costs input are far beyond our control, such as new and expensive technologies that to-day’s well-informed patients demand as part of their care.”
Independent Commission?After Congress voted in 2010 to in-
crease the federal debt ceiling, most
The SGR Oncology Problemcontinued from page 1
Allen S. Lichter, MDJoseph S. Bailes, MDDavid Eagle, MD
dles oncology services and drug reim-bursement in related fee codes, so when the agency has these several week sus-pensions between the next SGR patch, it costs community oncology practices around the country hundreds of thou-sands of dollars in lost drug reimburse-ments. No other specialty is affected in that manner,” he said.
“Studies show that the United States has the best cancer care delivery system in the world. But, to be fair, costs of pro-viding oncology services are rising at an unsustainable rate, and we cannot carry on with a business-as-usual mentality. However, the government cannot ad-dress the cost issue with a sledgeham-mer approach, bashing oncology with a 20% to 30% cut in payment. That will end the Medicare program as we know it,” Dr. Lichter added. ■
The flawed formula remains and it will require substantial ‘pay for’ to fix. It will also require substantial political will.
–Joseph S. Bailes, MD
■ SGR’s target spending path is based on growth in physician costs, total Medicare enrollment, and real GDP per beneficiary.
■ The price tag for the “doc fix” is more than $200 billion.
■ Oncology is disproportionately affected; ~50% of oncology patients are Medicare beneficiaries.
■ Studies (ASCO, COA) indicate that if implemented, SGR cuts would drastically reduce access to cancer care, especially for Medicare patients
■ In December 2010 both houses of Congress approved a measure to postpone the SGR-driven Medicare physician fee cuts that were scheduled for January 1st, 2011.
The Sustainable Growth Rate Problem
Contact The ASCO Post
Editorial CorrespondenceJames O. Armitage, MD
Editor-in-Chief email: [email protected]
Cara H. Glynn, Director of Editorial email: [email protected]
Phone: 631.935.7654
Andrew Nash, Assoc. Director of Editorial email: [email protected]
Phone: 631.935.7657
Advertising Rates, reprints, or supplements
Leslie Dubin email: [email protected]
Phone: 631.935.7660
Rights and Permissionsemail: [email protected]
Editorial OfficeHarborside Press
37 Main Street Cold Spring Harbor, NY 11724
Phone: 631.692.0800 Fax: 631.692.0805
ASCOPost.com HarborsidePress.com

Concerned about CYP2D6 in breast cancer?Fareston® may be the answer.
For more information about Fareston call 1-877-362-7595 or visit www.fareston.com
© 2010 GTx, Inc., Memphis, TN 38103. All rights reserved. FAR-071R0 June 2010
FARESTON (toremifene citrate) 60 mg Tablets: indicated for the treatment of metastatic breast cancer in postmenopausal women with estrogen receptor positive or unknown tumors.
Fareston helps reduce the guess work
500,000 PATIENT YEARS Proven clinical profileEfficacy comparable to tamoxifen in head to head trials
ALREADY ACTIVEParent compound binds to and blocks estrogen receptors
UNIQUE METABOLISMMetabolized principally by CYP3A4 CYP2D6 does not play a significant role in the activity of FARESTONNo known drug interactions with SSRI antidepressants
PATIENT SAVINGSSavings coupons offer up to $50 off each prescription for eligible patientsPatient Assistance Program available for Medicare Part D and uninsured patients who qualify
Please see full prescribing information on the following page.
FARESTON is contraindicated in patients with known hypersensitivity to the drug. FARESTON has been shown to prolong the QTc interval in a dose and concentration dependent manner. FARESTON should not be prescribed to patients with congenital/acquired QT prolongation, uncorrected hypokalemia or uncorrected hypomagnesemia. The administration of FARESTON with agents that are strong CYP3A4 inhibitors (e.g., ketoconazole, grapefruit juice and others) increases the steady-state concentration in serum and should be avoided. Patients with a history of thromboembolic diseases should generally not be treated with FARESTON. In general, patients with preexisting endometrial hyperplasia should not be given long-term FARESTON treatment. As with other antiestrogens, tumor flare, hypercalcemia, and vaginal bleeding have been reported in some breast cancer patients being treated with FARESTON. During clinical trials involving 1157 patients treated with FARESTON or tamoxifen, the incidence of serious side effects were as follows: cardiac events (2.03% vs. 2.42%), ocular events (10.30% vs. 9.38%), thromboembolic events (3.21% vs. 3.28%), and elevated liver tests (26.2% vs. 23.7%), respectively.References: FARESTON® Prescribing Information, 2004. Data on file, GTx, Inc.
Important safety information:

FARESTON® (toremifene citrate) tablets
DESCRIPTION FARESTON (toremifene citrate) Tablets for oral administration each contain 88.5 mg of toremifene citrate, which is equivalent to 60 mg toremifene. FARESTON is a nonsteroidal antiestrogen. The chemical name of toremifene is: 2-{p-[(Z)-4-chloro-1,2-diphenyl-1-butenyl]phenoxy}-N,N-dimethylethylamine citrate (1:1). The structural formula is:
and the molecular formula is C26
H28
CINO • C6H
8O
7. The molecular weight of toremifene citrate is
598.10. The pKa is 8.0. Water solubility at 37˚C is 0.63 mg/mL and in 0.02N HCI at 37˚C is 0.38 mg/mL.
FARESTON is available only as tablets for oral administration. Inactive ingredients: colloidal silicon dioxide, lactose, magnesium stearate, microcrystalline cellulose, povidone, sodium starch glycolate, and starch.
CLINICAL PHARMACOLOGY Mechanism of Action: Toremifene is a nonsteroidal triphenylethylene derivative. Toremifene binds to estrogen receptors and may exert estrogenic, antiestrogenic, or both activities, depending upon the duration of treatment, animal species, gender, target organ, or endpoint selected. In general, however, nonsteroidal triphenylethylene derivatives are predominantly antiestrogenic in rats and humans and estrogenic in mice. In rats, toremifene causes regression of established dimethylbenzanthracene (DMBA)-induced mam-mary tumors. The antitumor effect of toremifene in breast cancer is believed to be mainly due to its antiestrogenic effects, ie, its ability to compete with estrogen for binding sites in the cancer, blocking the growth-stimulating effects of estrogen in the tumor. Toremifene causes a decrease in the estradiol-induced vaginal cornification index in some postmenopausal women, indicative of its antiestrogenic activity. Toremifene also has estrogenic activity as shown by decreases in serum gonadotropin concentrations (FSH and LH).
Pharmacokinetics: The plasma concentration time profile of toremifene declines biexponentially after absorption with a mean distribution half-life of about 4 hours and an elimination half-life of about 5 days. Elimination half-lives of major metabolites, N-demethyltoremifene and (deaminohydroxy) toremifene were 6 and 4 days, respectively. Mean total clearance of toremifene was approximately 5L/h.
Absorption and Distribution: Toremifene is well absorbed after oral administration and absorption is not influenced by food. Peak plasma concentrations are obtained within 3 hours. Toremifene displays linear pharmacokinetics after single oral doses of 10 to 680 mg. After multiple dosing, dose proportionality was observed for doses of 10 to 400 mg. Steady-state concentrations were reached in about 4-6 weeks. Toremifene has an apparent volume of distribution of 580 L and binds extensively (>99.5%) to serum proteins, mainly to albumin.
Metabolism and Excretion: Toremifene is extensively metabolized, principally by CYP3A4 to N-demethyltoremifene, which is also antiestrogenic but with weak in vivo antitumor potency. Serum concentrations of N-demethyltoremifene are 2 to 4 times higher than toremifene at steady state. Toremifene is eliminated as metabolites predominantly in the feces, with about 10% excreted in the urine during a 1-week period. Elimination of toremifene is slow, in part because of enterohepatic circulation.
Special Populations: Renal insufficiency: The pharmacokinetics of toremifene and N-demethyltoremifene were similar in normals and in patients with impaired kidney function. Hepatic insufficiency: The mean elimination half-life of toremifene was increased by less than twofold in 10 patients with hepatic impairment (cirrhosis or fibrosis) compared to subjects with normal hepatic function. The pharmacokinetics of N-demethyltoremifene were unchanged in these patients. Ten patients on anticonvulsants (phenobarbital, clonazepam, phenytoin, and carbamazepine) showed a twofold increase in clearance and a decrease in the elimination half-life of toremifene. Geriatric patients: The pharmacokinetics of toremifene were studied in 10 healthy young males and 10 elderly females following a single 120 mg dose under fasting conditions. Increases in the elimination half-life (4.2 versus 7.2 days) and the volume of distribution (457 versus 627 L) of toremifene were seen in the elderly females without any change in clearance or AUC. Race: The pharmacokinetics of toremifene in patients of different races has not been studied. Drug-drug interactions: No formal drug-drug interaction studies with toremifene have been performed.
CLINICAL STUDIES Three prospective, randomized, controlled clinical studies (North American, Eastern European, and Nordic) were conducted to evaluate the efficacy of FARESTON for the treatment of breast cancer in postmenopausal women. The patients were randomized to parallel groups receiving FARESTON 60 mg (FAR60) or tamoxifen 20 mg (TAM20) in the North American Study or tamoxifen 40 mg (TAM40) in the Eastern European and Nordic studies. The North American and Eastern European studies also included high-dose toremifene arms of 200 and 240 mg daily, respectively. The studies included postmenopausal patients with estrogen-receptor (ER) positive or estrogen-receptor (ER) unknown metastatic breast cancer. The patients had at least one measurable or evaluable lesion. The primary efficacy variables were response rate (RR) and time to progression (TTP). Survival (S) was also determined. Ninety-five percent confidence intervals (95% CI) were calculated for the difference in RR between FAR60 and TAM groups and the hazard ratio (relative risk for an unfavorable event, such as disease progression or death) between TAM and FAR60 for TTP and S. Two of the 3 studies showed similar results for all effectiveness endpoints. However, the Nordic Study showed a longer time to progression for tamoxifen (see table).
Clinical Studies Study North American Eastern European NordicTreatment Group FAR60 TAM20 FAR60 TAM40 FAR60 TAM40No. Patients 221 215 157 149 214 201ResponsesCR1 + PR2 14+33 11+30 7+25 3+28 19+48 19+56RR3 (CR + PR)% 21.3 19.1 20.4 20.8 31.3 37.3Difference in RR 2.2 -0.4 -6.095% CI4 for Difference in RR -5.8 to 10.2 -9.5 to 8.6 -15.1 to 3.1Time to Progression (TTP)Median TTP (mo.) 5.6 5.8 4.9 5.0 7.3 10.2Hazard Ratio (TAM/FAR) 1.01 1.02 0.8095% CI4 for Hazard Ratio (%) 0.81 to 1.26 0.79 to 1.31 0.64 to 1.00Survival (S)Median S (mo.) 33.6 34.0 25.4 23.4 33.0 38.7Hazard Ratio (TAM/FAR) 0.94 0.96 0.9495% CI4 for Hazard Ratio (%) 0.74 to 1.24 0.72 to 1.28 0.73 to 1.221CR = complete response; 2PR = partial response; 3RR = response rate; 4CI = confidence interval The high-dose groups, toremifene 200 mg daily in the North American Study and 240 mg daily in the Eastern European Study, were not superior to the lower toremifene dose groups, with response rates of 22.6% AND 28.7%, median times to progression of 5.6 and 6.1 months, and median
survivals of 30.1 and 23.8 months, respectively. The median treatment duration in the three pivotal studies was 5 months (range 4.2-6.3 months).
INDICATION AND USAGE FARESTON is indicated for the treatment of metastatic breast cancer in postmenopausal women with estrogen-receptor positive or unknown tumors.
CONTRAINDICATIONS FARESTON is contraindicated in patients with known hypersensitivity to the drug.
WARNINGS Hypercalcemia and Tumor Flare: As with other antiestrogens, hypercalcemia and tumor flare have been reported in some breast cancer patients with bone metastases during the first weeks of treatment with FARESTON. Tumor flare is a syndrome of diffuse musculoskeletal pain and erythema with increased size of tumor lesions that later regress. It is often accompanied by hypercalcemia. Tumor flare does not imply failure of treatment or represent tumor progression. If hypercalcemia occurs, appropriate measures should be instituted and if hypercalcemia is severe, FARESTON treatment should be discontinued.
Tumorigenicity: Since most toremifene trials have been conducted in patients with metastatic disease, adequate data on the potential endometrial tumorigenicity of long-term treatment with FARESTON are not available. Endometrial hyperplasia has been reported. Some patients treated with FARESTON have developed endometrial cancer, but circumstances (short duration of treatment or prior antiestrogen treatment or premalignant conditions) make it difficult to establish the role of FARESTON. Endometrial hyperplasia of the uterus was observed in monkeys following 52 weeks of treatment at ≥1 mg/kg and in dogs following 16 weeks of treatment at ≥3 mg/kg with toremifene (about 1/4 and 1.4 times, respectively, the daily maximum recommended human dose on a mg/m2 basis).
Pregnancy: FARESTON may cause fetal harm when administered to pregnant women. Studies in rats at doses ≥1.0 mg/kg/day (about 1/4 the daily maximum recommended human dose on a mg/m2 basis) administered during the period of organogenesis, have shown that toremifene is embryotoxic and fetotoxic, as indicated by intrauterine mortality, increased resorption, reduced fetal weight, and fetal anomalies; including malformation of limbs, incomplete ossification, misshapen bones, ribs/spine anomalies, hydroureter, hydronephrosis, testicular displacement, and subcutaneous edema. Fetal anomalies may have been a consequence of maternal toxicity. Toremifene has been shown to cross the placenta and accumulate in the rodent fetus. In rodent models of fetal reproductive tract development, toremifene produced inhibition of uterine development in female pups similar to diethylstilbestrol (DES) and tamoxifen. The clinical relevance of these changes is not known. Embryotoxicity and fetotoxicity were observed in rabbits at doses ≥1.25 mg/kg/day and 2.5 mg/kg/day, respectively (about 1/3 and 2/3 the daily maximum recommended human dose on a mg/mt basis); fetal anomalies included incomplete ossification and anencephaly. There are no studies in pregnant women. If FARESTON is used during pregnancy, or if the patient becomes pregnant while receiving this drug, the patient should be apprised of the potential hazard to the fetus or potential risk for loss of the pregnancy.
PRECAUTIONS General: Patients with a history of thromboembolic diseases should generally not be treated with FARESTON. In general, patients with preexisting endometrial hyperplasia should not be given long-term FARESTON treatment. Patients with bone metastases should be monitored closely for hypercalcemia during the first weeks of treatment (see Warnings). Leukopenia and thrombocytopenia have been reported rarely; leukocyte and platelet counts should be monitored when using FARESTON in patients with leukopenia and thrombocytopenia.
Information for Patients: Vaginal bleeding has been reported in patients using FARESTON. Patients should be informed about this and instructed to contact their physician if such bleeding occurs. Patients with bone metastases should be informed about the typical signs and symptoms of hypercalcemia and instructed to contact their physician for further assessment if such signs or symptoms occur.
Laboratory Tests: Periodic complete blood counts, calcium levels, and liver function tests should be obtained.
Drug-drug Interactions: Drugs that decrease renal calcium excretion, eg, thiazide diuretics, may increase the risk of hypercalcemia in patients receiving FARESTON. There is a known interaction between antiestrogenic compounds of the triphenylethylene derivative class and coumarin-type anticoagulants (eg, warfarin), leading to an increased prothrombin time. When concomitant use of anticoagulants with FARESTON is necessary, careful monitoring of the prothrombin time is recommended. Cytochrome P450 3A4 enzyme inducers, such as phenobarbital, phenytoin, and carbamazepine increase the rate of toremifene metabolism, lowering the steady-state concentration in serum. Metabolism of toremifene may be inhibited by drugs known to inhibit the CYP3A4-6 enzymes. Examples of such drugs are ketoconazole and similar antimycotics as well as erythromycin and similar macrolides. This interaction has not been studied and its clinical relevance is uncertain.
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Conventional carcinogenesis studies in rats at doses of 0.12 to 12 mg/kg/day (about 1/100 to 1.5 times the daily maximum recommended human dose on a mg/m2 basis) for up to 2 years did not show evidence of carcinogenicity. Studies in mice at doses of 1.0 to 30.0 mg/kg/day (about 1/15 to 2 times the daily maximum recommended human dose on a mg/m2 basis) for up to 2 years revealed increased incidence of ovarian and testicular tumors, and increased incidence of osteoma and osteosarcoma. The significance of the mouse findings is uncertain because of the different role of estrogens in mice and the estrogenic effect of toremifene in mice. An increased incidence of ovarian and testicular tumors in mice has also been observed with other human antiestrogenic agents that have primarily estrogenic activity in mice. Toremifene has not been shown to be mutagenic in in vitro tests (Ames and E. coli bacterial tests). Toremifene is clastogenic in vitro (chromosomal aberrations and micronuclei formation in human lymphoblastoid MCL-5 cells) and in vivo (chromosomal aberrations in rat hepatocytes). No significant adduct formation could be detected using 32P post-labeling in liver DNA from rats administered toremifene when compared to tamoxifen at similar doses. A study in cultured human lymphocytes indicated that adducting activity of toremifene, detected by 32P post-labeling, was about 1/6 that of tamoxifen at approximately equipotent concentrations. In addition, the DNA adducting activity of toremifene in salmon sperm, using 32P post-labeling, was 1/6 and 1/4 that observed with tamoxifen at equivalent concentrations following activation by rat and human microsomal systems, respectively. However, toremifene exposure is fourfold the exposure of tamoxifen based on human AUC in serum at recommended clinical doses. Toremifene produced impairment of fertility and conception in male and female rats at doses ≥25.0 and 0.14 mg/kg/day, respectively (about 3.5 times and 1/50 the daily maximum recommended human dose on a mg/m2 basis). At these doses, sperm counts, fertility index, and conception rate were reduced in males with atrophy of seminal vesicles and prostate. In females, fertility and reproductive indices were markedly reduced with increased pre- and post-implantation loss. In addition, offspring of treated rats exhibited depressed reproductive indices. Toremifene produced ovarian atrophy in dogs administered doses ≥3 mg/kg/day (about 1.5 times the daily maximum recommended human dose on a mg/m2 basis) for 16 weeks. Cystic ovaries and reduction in endometrial stromal cellularity were observed in monkeys at doses ≥1 mg/kg/day (about 1/4 the daily maximum recommended human dose on a mg/m2 basis) for 52 weeks.
Pregnancy: Pregnancy Category D: (see WARNINGS). Nursing mothers: Toremifene has been shown to be excreted in the milk of lactating rats. It is not known if this drug is excreted in human milk. (See WARNINGS and PRECAUTIONS). Pediatric use: There is no indication for use of FARESTON in pediatric patients. Geriatric use: The median ages in the three controlled studies ranged from 60 to 66 years. No significant age-related differences in FARESTON effectiveness or safety were noted.
Race: Fourteen percent of patients in the North American Study were non-Caucasian. No significant race-related differences in FARESTON effectiveness or safety were noted.
ADVERSE REACTIONS Adverse drug reactions are principally due to the antiestrogenic hormonal actions of FARESTON and typically occur at the beginning of treatment. The incidences of the following eight clinical toxicities were prospectively assessed in the North American Study. The incidence reflects the toxicities that were considered by the investigator to be drug related or possibly drug related. North American Study FAR60 TAM20 n = 221 n = 215
Hot Flashes 35% 30% Sweating 20% 17% Nausea 14% 15% Vaginal Discharge 13% 16% Dizziness 9% 7% Edema 5% 5% Vomiting 4% 2% Vaginal Bleeding 2% 4%
Approximately 1% of patients receiving FARESTON (n = 592) in the three controlled studies discontinued treatment as a result of adverse events (nausea and vomiting, fatigue, thrombophlebitis, depression, lethargy, anorexia, ischemic attack, arthritis, pulmonary embolism, and myocardial infarction). Serious adverse events occurring in patients receiving FARESTON in the three major trials are listed in the table below.Adverse Events North American Eastern European Nordic FAR60 TAM20 FAR60 TAM40 FAR60 TAM40 n=221(%) n=215(%) n=157(%) n=149(%) n=214(%) n=201(%)CardiacCardiac Failure 2 (1) 1 (<1) - 1 (<1) 2 (1) 3 (1.5)Myocardial Infarction 2 (1) 3 (1.5) 1 (<1) 2 (1) - 1 (<1)Arrhythmia - - - - 3 (1.5) 1 (<1)Angina Pectoris - - 1 (<1) - 1 (<1) 2 (1)Ocular*Cataracts 22 (10) 16 (7.5) - - - 5 (3)Dry Eyes 20 (9) 16 (7.5) - - - -Abnormal Visual Fields 8 (4) 10 (5) - - - 1 (<1)Corneal Keratopathy 4 (2) 2 (1) - - - - Glaucoma 3 (1.5) 2 (1) 1 (<1) - - 1 (<1)Abnormal Vision/Diplopia - - - - 3 (1.5) -ThromboembolicPulmonary Embolism 4 (2) 2 (1) 1 (<1) - - 1 (<1)Thrombophlebitis - 2 (1) 1 (<1) 1 (<1) 4 (2) 3 (1.5)Thrombosis - 1 (<1) 1 (<1) - 3 (1.5) 4 (2)CVA/TIA 1 (<1) - - 1 (<1) 4 (2) 4 (2)Elevated Liver Tests**SGOT 11 (5) 4 (2) 30 (19) 22 (15) 32 (15) 35 (17)Alkaline Phosphatase 41 (19) 24 (11) 16 (10) 13 (9) 18 (8) 31 (15)Bilirubin 3 (1.5) 4 (2) 2 (1) 1 (<1) 2 (1) 3 (1.5)Hypercalcemia 6 (3) 6 (3) 1 (<1) - - -
* Most of the ocular abnormalities were observed in the North American Study in which on-study and biannual opthalmic examinations were performed. No cases of retinopathy were observed in any arm.** Elevated defined as follows: North American Study: SGOT >100 IU/L; alkaline phosphatase >200 IU/L; bilirubin > 2 mg/dL. Eastern European and Nordic studies: SGOT, alkaline phosphatase, and bilirubin – WHO Grade 1 (1.25 times the upper limit of normal).
Other adverse events of unclear causal relationship to FARESTON included leukopenia and thrombocytopenia, skin discoloration or dermatitis, constipation, dyspnea, paresis, tremor, vertigo, pruritis, anorexia, reversible corneal opacity (corneal verticulata), asthenia, alopecia, depression, jaundice, and rigors. In the 200 and 240 mg FARESTON dose arms, the incidence of SGOT elevation and nausea was higher. Approximately 4% of patients were withdrawn for toxicity from the high-dose FARESTON treatment arms. Reasons for withdrawal included hypercalcemia, abnormal liver function tests, and one case each of toxic hepatitis, depression, dizziness, incoordination, ataxia, blurry vision, diffuse dermatitis, and a constellation of symptoms consisting of nausea, sweating, and tremor.
OVERDOSAGE Lethality was observed in rats following single oral doses that were ≥1000 mg/kg (about 150 times the recommended human dose on a mg/m2 basis) and was associated with gastric atony/dilatation leading to interference with digestion and adrenal enlargement. Vertigo, headache, and dizziness were observed in healthy volunteer studies at a daily dose of 680 mg for 5 days. The symptoms occurred in two of the five subjects during the third day of the treatment and disappeared within 2 days of discontinuation of the drug. No immediate concomitant changes in any measured clinical chemistry parameters were found. In a study in postmenopausal breast cancer patients, toremifene 400 mg/m2/day caused dose-limiting nausea, vomiting, and dizziness, as well as reversible hallucinations and ataxia in one patient. Theoretically, overdose may be manifested as an increase of antiestrogenic effects, such as hot flashes; estrogenic effects, such as vaginal bleeding; or nervous system disorders, such as vertigo, dizziness, ataxia, and nausea. There is no specific antidote and the treatment is symptomatic.
DOSAGE AND ADMINISTRATION The dosage of FARESTON is 60 mg, once daily, orally. Treatment is generally continued until disease progression is observed.
HOW SUPPLIED FARESTON Tablets, containing toremifene citrate in an amount equivalent to 60 mg of toremifene, are round, convex, unscored, uncoated, and white, or almost white.FARESTON Tablets are identified with TO 60 embossed on one side.FARESTON Tablets are available as:NDC 11399-005-30 bottles of 30NDC 11399-005-01 bottles of 100
Store at 25°C (77°F)excursions permitted to 15-30°C (59-86°F)[see USP Controlled Room Temperature].Protect from heat and light.
Distributed by GTx, Inc.Memphis, TN 38163, USAProduct covered by Orion Product Patents and related patent numbers.© 2004 GTx, Inc.All rights reserved.
1E Rev. 12/2004
OCH2CH2NCH3
CH3
CH2
CH2COOH
CH2COOHCH2Cl
C CC COOHHO

ASCOPost.com | JANUARY 1, 2011 PAGE 25
TAP Caucus
Should Induction Chemotherapy Be Considered Standard of Care for Local-Regional Head and Neck Cancer?
continued on page 27
CON The use of induction chemother-apy with TPF (docetaxel, cispla-
tin, and fluorouracil [5-FU]) prior to concurrent chemoradiotherapy in the treatment of squamous cell head and neck cancer is gradually becoming commonplace in academic and community can-cer centers. The trend is concerning. At this time, clinical trial data do not support TPF induction as standard of care in most patients with local–region-ally advanced head and neck cancer. Although TPF induction is included in the National Comprehen-sive Cancer Network (NCCN) practice guidelines,
it is noted to be only an alternative to the preferred option of concurrent chemoradiotherapy with high-dose cisplatin alone or surgery followed by ra-diation therapy (RT) with or without chemotherapy.1 In fact, the category 3 designation that NCCN gives to induction chemotherapy reflects the serious disagreement among multiple panel members about whether TPF induction should be included in the guidelines at all.
Key Clinical TrialsRandomized trials from the 1980s and early 1990s set the stage for three
recent trials investigating the treatment of locally advanced head and neck can-cer with induction chemotherapy as a study arm.2-5 The investigators found no improvement in overall survival or local-regional control. However, the rate of distant metastasis was decreased in some trials, suggesting a possible role for induction in the control of distant disease. These trials suggested that equi-poise existed and additional research was warranted.
The Radiation Therapy Oncology Group (RTOG) 91-11 trial compared induction using cisplatin and 5-FU (PF) vs radiation alone vs concurrent radiation with cisplatin. The data show no survival advantage for any group. However, local-regional control was better in the concurrent arm vs the induc-tion arm vs radiation alone (88% vs 75% vs 70%).6 The fundamental impor-tance of local-regional control cannot be overstated in head and neck cancer. In addition, no difference was seen in high-grade toxic effects between the two
chemotherapy arms (82% vs 81%). This trial developed the level 1 evidence used to support concurrent radiation with cisplatin chemotherapy as the pre-ferred NCCN option.
Recently, two trials have examined which induction regimen is superior—PF or TPF. These trials clearly demonstrate that TPF is better than PF as an induction regimen when followed by radiation with weekly low-dose carbo-platin (3-year overall survival of 62% vs 48%; 3-year progression-free survival of 49% vs 37%).7,8 It is important to note, however, that these trials do not compare induction chemotherapy with the current NCCN-recommended radiation plus concurrent cisplatin; they demonstrate which of these two in-duction chemotherapy regimens is superior.
Two subsequent multicenter randomized controlled trials have been in-stituted (the PARADIGM study led by Dana-Farber Cancer Institute, and DeCIDE study led by the University of Chicago). Unfortunately, both have closed without meeting accrual goals.9,10 Due to what appears to be an un-
PRO In an age of evidence-based medi-cine, ample data support the stan-
dard inclusion of induction chemotherapy and sequential therapy as options for treatments in the multimodality management of patients with locally advanced squamous cell cancer of the head and neck. Many investigators have taken a position op-posed to the use of induction chemotherapy for any patient with head and neck cancer outside of a clini-cal trial. This opinion is not based on the data from clinical trials in head and neck cancer.
Head and neck cancer is a complex, difficult tumor site for clinical man-agement. Patients with the disease are difficult to treat, frequently have co-morbidities, and have complex staging. Tumors from different sites within the head and neck respond differentially to therapy. Thus, many head and neck–specific subtleties exist in therapeutic decision-making.
Reviewing the EvidenceBefore I address these clinical considerations, we need to review therapy
based on the specific evidence. First, multiple meta-analyses over almost 10 years have consistently shown that cisplatin/fluorouracil (PF) induction che-motherapy significantly improves survival in patients with head and neck can-cer compared to radiotherapy or radiotherapy plus surgery in studies with a
survival endpoint.1,2 Two large randomized phase III clinical trials done in the modern age of trial management by cooperative groups show a significant sur-vival improvement with PF compared with radiotherapy and surgery. These trials and randomized organ-preservation trials provide unequivocal level 1 evidence that PF is superior to the prior standard of radiotherapy and surgery for survival 4,5 and organ preservation.6,7
Also of importance, and contrary to commonly held beliefs, induction chemotherapy improved local-regional control and reduced metastases in the two randomized advanced disease trials compared to radiotherapy and surgery alone. Thus, the beliefs that induction chemotherapy only selects patients for whom radiation would work, does not improve local-regional control, and only impacts distant metastases is contradicted by the data from these and other randomized controlled trials (RCTs). When we examine the three RCTs with large enough patient numbers that compare PF induction chemotherapy to platinum-based chemoradiotherapy—the two modern age trials in the organ-preservation setting and the single trial in advanced tu-mors—all demonstrate that induction therapy and chemoradiotherapy pro-duce identical outcomes for survival and for organ preservation.6,8,9 Thus, PF and chemoradiotherapy are equivalent for organ preservation and survival when compared head to head, and importantly, induction chemotherapy is less toxic, based on late chemoradiotherapy-related mortality as reported in at least two of the trials.6,8
Newer Induction RegimensImprovements in induction chemotherapy and an analysis of failures in in-
duction and chemoradiotherapy trials has led to new regimens that have been continued on page 26
Pro/Con
Increases in toxicity and cost to the patient and society must be justified by commensurate improvement in outcome. This has not been demonstrated for TPF induction.
If PF and chemoradiotherapy are equivalent and TPF is very significantly better than PF, then TPF is highly likely to be better than chemoradiotherapy.
Marshall Posner, MD William M. Lydiatt, MD, FACS

PAGE 26 The ASCO Post | JANUARY 1, 2011
TAP Caucus
studied in RCTs. Recently, three RCTs have shown that docetaxel/cisplatin/fluorouracil (TPF) induction chemo-therapy significantly and meaningfully improves survival and organ preserva-
tion in locally advanced head and neck cancer compared to PF, with less con-sequent toxicity.10-12
Logically, if PF and chemoradio-therapy are equivalent and TPF is very significantly better than PF, then TPF is highly likely to be better than chemoradiotherapy. Because biologic systems frequently defy logic, RCTs
are necessary for conclusive proof. However, at least until randomized comparisons are available, TPF should be considered an acceptable treatment for appropriate patients. We can safely say that induction chemotherapy and sequential therapy are not merely ex-perimental therapies to be limited to clinical trials. They are, in fact, tools we
can use to treat and cure patients and should be considered standard therapy for appropriate patients.
Selection CriteriaWhat is an “appropriate” patient?
Every therapy has clinical “inclusion” and “exclusion” parameters. Based on the data we have from multiple trials, I believe that patients who have a good performance status (ECOG 0-1), good renal and cardiac function, and are psychologically suited should be con-sidered for sequential treatment if they have stage III or IV head and neck can-cer. I am comfortable treating patients with stage III hypopharynx and larynx cancers with this approach, based on the results of RCTs. All patients with stage IV disease should be considered for TPF sequential therapy, although oral cavity cancers are best treated with surgery if possible.
It is apparent from the TAX 324 trial and chemoradiotherapy trials that local-regional failure remains the ma-jor problem for patients with head and neck cancer. We should consider TPF as part of a sequential therapy plan in which chemoradiotherapy and surgery can further increase local-regional control and decrease morbidity. As new agents and improvements in sup-portive care and technology are added to our therapeutic armamentarium, we will cure more patients with less hu-man cost. ■References
1. Pignon J, Bourhis J, Domenge C, et al: Chemotherapy added to locoregional treatment for head and neck squamous-cell cancer: Three meta-analysis of updated in-dividual data. Lancet 355:949-955, 2000.
2. Pignon JP, le Maitre A, Maillard E, et al: Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 pa-tients. Radiother Oncol 92:4-14, 2009.
3. Munro A: An overview of random-ized controlled trials of adjuvant chemo-therapy in head and neck cancer. Br J Can-cer 71:83-91, 1995.
4. Domenge C, Hill C, Lefebvre J, et al: Randomized trial of neoadjuvant chemo-therapy in oropharyngeal carcinoma. Br J Cancer 83:1594-1598, 2000.
5. Zorat PL, Paccagnella A, Cavaniglia G, et al: Randomized phase III trial of neo-adjuvant chemotherapy in head and neck cancer: 10-year follow-up. J Natl Cancer Inst 96:1714-1717, 2004.
6. Forastiere A, Maor M, Weber R, et al: Long term results of Intergroup RTOG 91-11: A phase III trial to preserve the
Sequential and Induction Chemotherapy Are Effective Standard Therapiescontinued from page 25
To register and reserve housing, visit www.gicasym.org
The 2011 Gastrointestinal Cancers Symposium will showcase important advances in research and emerging
therapies for gastrointestinal cancers through a variety of sessions designed for a multidisciplinary audience.
Tailored to be a discussion-based meeting, the Symposium is intended to foster dialogue among oncologists,
surgeons, radiation oncologists, gastroenterologists, and other members of the cancer care community. The
educational sessions will feature presentations on the latest science and its applicability to optimizing
treatment of patients with gastrointestinal cancers.
January 20-22, 2011The Moscone West BuildingSan Francisco, California
2011 Gastrointestinal Cancers Symposium
Science and Multidisciplinary Management of GI Malignancies
Join the Discussion
This activity has been approved for AMA PRA Category 1 Credit.™
• NEW: Posters will be displayed for all-day viewing
• NEW: e-Q&A: text, tweet, or e-mail your questions
in selected sessions
• NEW: Abstracts in the 2011 Gastrointestinal
Cancers Symposium Proceedings are citable as
an online supplement to the Journal of Clinical
Oncology
• NEW: Virtual Meeting included in Registration Fee
• Meet the Professor Sessions - Breakfast and
evening events, four concurrent sessions*
• Translational Research Sessions - Daily lunch
event
• Fellows, Residents, and Junior Faculty Networking
Luncheon*
Highlights of this year’s Symposium include:
T A R G E T I N G C A N C E R C A R E
*Tickets Required
To register and reserve housing, visit www.gicasym.org
The 2011 Gastrointestinal Cancers Symposium will showcase important advances in research and emerging
therapies for gastrointestinal cancers through a variety of sessions designed for a multidisciplinary audience.
Tailored to be a discussion-based meeting, the Symposium is intended to foster dialogue among oncologists,
surgeons, radiation oncologists, gastroenterologists, and other members of the cancer care community. The
educational sessions will feature presentations on the latest science and its applicability to optimizing
treatment of patients with gastrointestinal cancers.
January 20-22, 2011The Moscone West BuildingSan Francisco, California
2011 Gastrointestinal Cancers Symposium
Science and Multidisciplinary Management of GI Malignancies
Join the Discussion
This activity has been approved for AMA PRA Category 1 Credit.™
• NEW: Posters will be displayed for all-day viewing
• NEW: e-Q&A: text, tweet, or e-mail your questions
in selected sessions
• NEW: Abstracts in the 2011 Gastrointestinal
Cancers Symposium Proceedings are citable as
an online supplement to the Journal of Clinical
Oncology
• NEW: Virtual Meeting included in Registration Fee
• Meet the Professor Sessions - Breakfast and
evening events, four concurrent sessions*
• Translational Research Sessions - Daily lunch
event
• Fellows, Residents, and Junior Faculty Networking
Luncheon*
Highlights of this year’s Symposium include:
T A R G E T I N G C A N C E R C A R E
*Tickets Required

ASCOPost.com | JANUARY 1, 2011 PAGE 27
TAP Caucus
larynx—induction cisplatin/5-FU and ra-diation therapy versus concurrent cispla-tin and radiation therapy versus radiation therapy. J Clin Oncol 24(18S):Abstract 5517, 2006.
7. Lefebvre J, Chevalier D, Luboinski B, et al: Larynx preservation in pyriform sinus cancer: Preliminary results of a European organization for research and treatment of cancer phase III trial. J Natl Cancer Inst
fortunate early adoption of TPF induc-tion into standard practice, the oppor-tunity may have been lost for reliable clinical trial evaluation of the relative toxicities and benefits of TPF induc-tion compared to standard cisplatin/RT alone.
Drawbacks of Induction Chemotherapy
Given a lack of direct evidence to support that there is any clinical ben-efit to induction chemotherapy, what are the disadvantages to adopting this as standard of care? The most obvi-ous is that this paradigm doubles the time of treatment from 7 to 14 weeks. Depression is known to adversely af-fect outcomes in patients with head and neck cancer and correlates with increased length and toxicity of ther-apy.11-13 Thus, prolongation of therapy through the addition of a high-toxicity induction chemotherapy regimen may be expected to increase the frequency and severity of depression in patients.
Induction chemotherapy prior to chemoradiotherapy is unlikely to de-crease toxicities compared to chemo-radiotherapy alone. In concurrent chemoradiotherapy, RT is the base curative modality, significantly poten-tiated by the chemotherapy. Delay in starting curative-intent RT is known to adversely affect outcomes. The poten-tial benefits of induction chemothera-py, therefore, must be balanced against the potential harm of delay in starting definitive RT. In addition, the random-ized trials establishing standard cispla-tin/RT alone show that approximately 40% of patients do not receive all three
planned cycles of cisplatin. This num-ber can only be expected to worsen with the addition of high-toxicity, lengthy induction chemotherapy.
With all else being equal, it is axi-omatic that TPF induction markedly increases the cost of therapy. In the current health-care cost crisis, we as physicians cannot consider treatment regimens as equivalent standard of care when one is nearly twice as ex-pensive. Increases in toxicity and cost to the individual patient and society must be justified by commensurate improvement in outcome. This has not been demonstrated for TPF induction.
Changing EpidemiologyFinally, TPF induction must also
be considered in the context of the epidemic increase in the incidence of human papillomavirus (HPV)-related oropharynx cancers. Data continue to accumulate that these patients have dramatically improved outcomes com-pared to those with HPV-unrelated disease when treated with standard cisplatin/RT (overall survival of 82% vs 57%).14-16 With outcomes progres-sively improving due to an increasing proportion of HPV-related disease, historic comparisons of survival be-come moot. Faced with this changing epidemiology, it is all the more impor-tant to be judicious in the adoption of new therapies, particularly those that potentially increase toxicity and clearly increase the duration and cost of therapy.
For the present, TPF induction chemotherapy cannot and should not be considered standard of care in local-regional head and neck cancer, and should not be used outside of the clini-cal trial setting or highly selected clini-cal situations. ■
References1. National Comprehensive Cancer
Network: NCCN Clinical Practice Guide-lines in Oncology: Head and neck cancers, v.2.2010. Available at www.nccn.org. Ac-cessed November 8, 2010.
2. Adjuvant chemotherapy for advanced head and neck squamous carcinoma. Final report of the Head and Neck Contracts Pro-gram. Cancer 60:301-311, 1987.
3. Laramore GE, Scott CB, al-Sarraf M, et al: Adjuvant chemotherapy for resect-able squamous cell carcinomas of the head and neck: Report on Intergroup Study 0034. Int J Radiat Oncol Biol Phys 23:705-713, 1992.
4. Paccagnella A, Orlando A, Marchiori C, et al: Phase III trial of initial chemo-therapy in stage III or IV head and neck cancers: A study by the Gruppo di Studio sui Tumori della Testa e del Collo. J Natl Cancer Inst 86:265-272, 1994.
5. Pignon JP, Bourhis J, Domenge C, et al: Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. MACH-NC Col-laborative Group. Meta-analysis of chemo-therapy on head and neck cancer. Lancet 355:949-955, 2000.
6. Forastiere AA, Goepfert H, Maor M, et al: Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 349:2091-2098, 2003.
7. Vermorken JB, Remenar E, van Her-pen C, et al: Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med 357:1695-1704, 2007.
8. Posner MR, Hershock DM, Blajman CR, et al: Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med 357:1705-1715, 2007.
9. Haddad RI, Tishler RB, Adkins D, et al: The PARADIGM trial: A phase III
study comparing sequential therapy (ST) to concurrent chemoradiotherapy (CRT) in locally advanced head and neck cancer (LAHNC): Preliminary toxicity report. J Clin Oncol 28(15S):Abstract 5563, 2010.
10. Docetaxel based chemotherapy plus or minus induction chemotherapy to decrease events in head and neck cancer (DeCIDE). Available at www.clinicaltrials.gov. Accessed November 8, 2010.
11. Lydiatt WM, Denman D, McNeilly DP, et al: A randomized, placebo-con-trolled trial of citalopram for the preven-tion of major depression during treatment for head and neck cancer. Arch Otolaryn-gol Head Neck Surg 134:528-535, 2008.
12. Lauzure KE, Lydiatt WM, Denman D, et al: Association between depression and survival or disease recurrence in pa-tients with head and neck cancer (HNC) enrolled in a depression prevention trial. Head Neck 31:888-892, 2009.
13. Lydiatt WM, Moran J, Burke WJ: A review of depression in the head and neck cancer patient. Clin Adv Hematol Oncol 7:397-403, 2009.
14. Ang KK, Harris J, Wheeler R, et al: Human papillomavirus and survival of pa-tients with oropharyngeal cancer. N Engl J Med 363:24-35, 2010.
15. Rischin D, Young RJ, Fisher R, et al: Prognostic significance of p16INK4A and human papillomavirus in patients with oropharyngeal cancer treated on TROG 02.02 phase III trial. J Clin Oncol 28:4142-4148, 2010.
16. Shi W, Kato H, Perez-Ordonez B, et al: Comparative prognostic value of HPV16 E6 mRNA compared with in situ hybridization for human oropharyn-geal squamous carcinoma. J Clin Oncol 27:6213-6221, 2009.
Dr. Lydiatt is Professor and Division Chief, Head and Neck Surgical Oncology, Univer-sity of Nebraska Medical Center, Omaha.
Induction Chemotherapy Should Not Be Considered Standard of Carecontinued from page 25
88:890-898, 1996.8. Taylor S, Murthy A, Vannetzel J, et al:
Randomized comparison of neoadjuvant cisplatin and fluorouracil infusion followed by radiation versus concomitant treatment in advanced head and neck cancer. J Clin Oncol 12:385-395, 1994.
9. Lefebvre JL, Rolland F, Tesselaar M, et al: Phase 3 randomized trial on larynx preservation comparing sequential vs alter-
nating chemotherapy and radiotherapy. J Natl Cancer Inst 101:142-152, 2009.
10. Pointreau Y, Garaud P, Chapet S, et al: Randomized trial of induction chemo-therapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx pres-ervation. J Natl Cancer Inst 101:498-506, 2009.
11. Posner MR, Hershock DM, Blajman CR, et al: Cisplatin and fluorouracil alone
or with docetaxel in head and neck cancer. N Engl J Med 357:1705-1715, 2007.
12. Vermorken JB, Remenar E, van Her-pen C, et al: Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med 357:1695-1704, 2007.
Dr. Posner is Medical Director, Head and Neck Cancer Center, The Tisch Cancer Insti-tute, Mount Sinai Medical Center, New York.
What Do You Think About Induction Chemotherapy for Local-Regional Head and Neck Cancer?Whether induction chemotherapy should be considered standard of care in local-regional head and neck cancer is a controversial issue, as noted in the discussions above by Marshall Posner, MD, of the Mount Sinai Medical Center in New York and William Lydiatt, MD, of the University of Nebraska Medical Center in Omaha. Write to The ASCO Post at [email protected] to share your thoughts about this important issue in managing patients with head and neck cancer.

TORISEL—Significant overall survival benefit as first-line therapy1
Kaplan-Meier curves for overall survival (OS)*—TORISEL vs IFN�1
• Live vaccinations and close contact with those who received live vaccines should be avoided.• Patients and their partners should be advised to avoid pregnancy throughout treatment and for 3 months after TORISEL
therapy has stopped.• The most common (incidence ≥30%) adverse reactions observed with TORISEL are: rash (47%), asthenia (51%), mucositis (41%),
nausea (37%), edema (35%), and anorexia (32%). The most common laboratory abnormalities (incidence ≥30%) are anemia (94%), hyperglycemia (89%), hyperlipemia (87%), hypertriglyceridemia (83%), elevated alkaline phosphatase (68%), elevated serum creatinine (57%), lymphopenia (53%), hypophosphatemia (49%), thrombocytopenia (40%), elevated AST (38%), and leukopenia (32%).
• In the randomized, phase 3 trial, complete blood counts (CBCs) were checked weekly, and chemistry panels were checked every 2 weeks. Laboratory monitoring for patients receiving TORISEL may need to be performed more or less frequently at the physician’s discretion.
• Most common grades 3/4 adverse events and laboratory abnormalities included asthenia (11%), dyspnea (9%), hemoglobin decreased (20%), lymphocytes decreased (16%), glucose increased (16%), phosphorus decreased (18%), and triglycerides increased (44%).
• Strong inducers of CYP3A4/5 (eg, dexamethasone, rifampin) and strong inhibitors of CYP3A4 (eg, ketoconazole, atazanavir) may decrease and increase concentrations of the major metabolite of TORISEL, respectively. If alternatives cannot be used, dose modifications of TORISEL are recommended.
• St. John’s Wort may decrease TORISEL plasma concentrations, and grapefruit juice may increase plasma concentrations of the major metabolite of TORISEL, and therefore both should be avoided.
• The combination of TORISEL and sunitinib resulted in dose-limiting toxicity (Grade 3/4 erythematous maculopapular rash, and gout/cellulitis requiring hospitalization).
Please see the brief summary of the full Prescribing Information on the next page.
References: 1. TORISEL® Kit (temsirolimus) Prescribing Information, Wyeth Pharmaceuticals Inc. 2. Data on file, Pfizer Inc. 3. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: kidney cancer. V.2.2010.
Change expectations
• Studied first-line in patients with ≥3 of 6 preselected prognostic risk factors1
The advanced RCC pivotal study included patients with2
• Clear-cell or non–clear-cell tumor histologyII • Any nephrectomy status
Median duration of treatment was 17 weeks (range 1-126 weeks) for the TORISEL arm and 8 weeks (range 1-124 weeks) for the IFN� arm.1
Results from a phase 3, multicenter, 3-arm, randomized, open-label study conducted in 626 previously untreated patients with advanced RCC.1
mTOR=mammalian target of rapamycin.IFN�=interferon alpha.CI=confidence interval.* Time from randomization to death.1† A comparison is considered statistically significant
if the P-value is <.0159 (O’Brien-Fleming boundary at 446 deaths).1
‡ Based on log-rank test stratified by prior nephrectomyand region.1
§ Based on Cox proportional hazard model stratified by prior nephrectomy and region.1
II 82% and 82.5% of patients had known clear-cell histology for TORISEL and IFN�, respectively.2
¶ NCCN Category 1 recommendations are based on high-level evidence (eg, randomized controlled trials) and uniform NCCN consensus.3
# TORISEL was approved by the FDA in 2007.1
• Category 1 NCCN recommendation—first-line for poor-prognosis patients3¶
• >3 years experience since FDA approval#
Important Safety Information• TORISEL is contraindicated in patients with bilirubin >1.5 x ULN and should be used with caution when treating patients with mild
hepatic impairment (bilirubin >1–1.5 x ULN or AST >ULN but bilirubin ≤ULN). If TORISEL must be given to patients with mild hepatic impairment, reduce the dose of TORISEL to 15 mg/week. In a phase 1 study, the overall frequency of ≥grade 3 adverse reactions and deaths, including deaths due to progressive disease, was greater in patients with baseline bilirubin >1.5 x ULN.
• Hypersensitivity reactions manifested by symptoms, including, but not limited to anaphylaxis, dyspnea, flushing, and chest pain have been observed with TORISEL.
• Serum glucose, serum cholesterol, and triglycerides should be tested before and during treatment with TORISEL. – The use of TORISEL is likely to result in hyperglycemia and hyperlipemia. This may result in the need for an increase in
the dose of, or initiation of, insulin and/or oral hypoglycemic agent therapy and/or lipid-lowering agents, respectively.• The use of TORISEL may result in immunosuppression. Patients should be carefully observed for the occurrence of
infections, including opportunistic infections.• Cases of interstitial lung disease, some resulting in death, have occurred. Some patients were asymptomatic and others presented
with symptoms. Some patients required discontinuation of TORISEL and/or treatment with corticosteroids and/or antibiotics.• Cases of fatal bowel perforation occurred with TORISEL. These patients presented with fever, abdominal pain, metabolic
acidosis, bloody stools, diarrhea, and/or acute abdomen.• Cases of rapidly progressive and sometimes fatal acute renal failure not clearly related to disease progression occurred
in patients who received TORISEL.• Due to abnormal wound healing, use TORISEL with caution in the perioperative period.• Patients with central nervous system tumors (primary CNS tumor or metastases) and/or receiving anticoagulation therapy
may be at an increased risk of developing intracerebral bleeding (including fatal outcomes) while receiving TORISEL.
portant Safety Information
Change expectationsfor overall survival
With the fi rst and only IV mTOR inhibitor indicated for advanced renal cell carcinoma (RCC)1...
TUP100027_ASCO Post_Tabloid_FNL.indd 1-2 8/12/10 4:38 PM

TORISEL—Significant overall survival benefit as first-line therapy1
Kaplan-Meier curves for overall survival (OS)*—TORISEL vs IFN�1
• Live vaccinations and close contact with those who received live vaccines should be avoided.• Patients and their partners should be advised to avoid pregnancy throughout treatment and for 3 months after TORISEL
therapy has stopped.• The most common (incidence ≥30%) adverse reactions observed with TORISEL are: rash (47%), asthenia (51%), mucositis (41%),
nausea (37%), edema (35%), and anorexia (32%). The most common laboratory abnormalities (incidence ≥30%) are anemia (94%), hyperglycemia (89%), hyperlipemia (87%), hypertriglyceridemia (83%), elevated alkaline phosphatase (68%), elevated serum creatinine (57%), lymphopenia (53%), hypophosphatemia (49%), thrombocytopenia (40%), elevated AST (38%), and leukopenia (32%).
• In the randomized, phase 3 trial, complete blood counts (CBCs) were checked weekly, and chemistry panels were checked every 2 weeks. Laboratory monitoring for patients receiving TORISEL may need to be performed more or less frequently at the physician’s discretion.
• Most common grades 3/4 adverse events and laboratory abnormalities included asthenia (11%), dyspnea (9%), hemoglobin decreased (20%), lymphocytes decreased (16%), glucose increased (16%), phosphorus decreased (18%), and triglycerides increased (44%).
• Strong inducers of CYP3A4/5 (eg, dexamethasone, rifampin) and strong inhibitors of CYP3A4 (eg, ketoconazole, atazanavir) may decrease and increase concentrations of the major metabolite of TORISEL, respectively. If alternatives cannot be used, dose modifications of TORISEL are recommended.
• St. John’s Wort may decrease TORISEL plasma concentrations, and grapefruit juice may increase plasma concentrations of the major metabolite of TORISEL, and therefore both should be avoided.
• The combination of TORISEL and sunitinib resulted in dose-limiting toxicity (Grade 3/4 erythematous maculopapular rash, and gout/cellulitis requiring hospitalization).
Please see the brief summary of the full Prescribing Information on the next page.
References: 1. TORISEL® Kit (temsirolimus) Prescribing Information, Wyeth Pharmaceuticals Inc. 2. Data on file, Pfizer Inc. 3. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: kidney cancer. V.2.2010.
Change expectations
• Studied first-line in patients with ≥3 of 6 preselected prognostic risk factors1
The advanced RCC pivotal study included patients with2
• Clear-cell or non–clear-cell tumor histologyII • Any nephrectomy status
Median duration of treatment was 17 weeks (range 1-126 weeks) for the TORISEL arm and 8 weeks (range 1-124 weeks) for the IFN� arm.1
Results from a phase 3, multicenter, 3-arm, randomized, open-label study conducted in 626 previously untreated patients with advanced RCC.1
mTOR=mammalian target of rapamycin.IFN�=interferon alpha.CI=confidence interval.* Time from randomization to death.1† A comparison is considered statistically significant
if the P-value is <.0159 (O’Brien-Fleming boundary at 446 deaths).1
‡ Based on log-rank test stratified by prior nephrectomyand region.1
§ Based on Cox proportional hazard model stratified by prior nephrectomy and region.1
II 82% and 82.5% of patients had known clear-cell histology for TORISEL and IFN�, respectively.2
¶ NCCN Category 1 recommendations are based on high-level evidence (eg, randomized controlled trials) and uniform NCCN consensus.3
# TORISEL was approved by the FDA in 2007.1
• Category 1 NCCN recommendation—first-line for poor-prognosis patients3¶
• >3 years experience since FDA approval#
Important Safety Information• TORISEL is contraindicated in patients with bilirubin >1.5 x ULN and should be used with caution when treating patients with mild
hepatic impairment (bilirubin >1–1.5 x ULN or AST >ULN but bilirubin ≤ULN). If TORISEL must be given to patients with mild hepatic impairment, reduce the dose of TORISEL to 15 mg/week. In a phase 1 study, the overall frequency of ≥grade 3 adverse reactions and deaths, including deaths due to progressive disease, was greater in patients with baseline bilirubin >1.5 x ULN.
• Hypersensitivity reactions manifested by symptoms, including, but not limited to anaphylaxis, dyspnea, flushing, and chest pain have been observed with TORISEL.
• Serum glucose, serum cholesterol, and triglycerides should be tested before and during treatment with TORISEL. – The use of TORISEL is likely to result in hyperglycemia and hyperlipemia. This may result in the need for an increase in
the dose of, or initiation of, insulin and/or oral hypoglycemic agent therapy and/or lipid-lowering agents, respectively.• The use of TORISEL may result in immunosuppression. Patients should be carefully observed for the occurrence of
infections, including opportunistic infections.• Cases of interstitial lung disease, some resulting in death, have occurred. Some patients were asymptomatic and others presented
with symptoms. Some patients required discontinuation of TORISEL and/or treatment with corticosteroids and/or antibiotics.• Cases of fatal bowel perforation occurred with TORISEL. These patients presented with fever, abdominal pain, metabolic
acidosis, bloody stools, diarrhea, and/or acute abdomen.• Cases of rapidly progressive and sometimes fatal acute renal failure not clearly related to disease progression occurred
in patients who received TORISEL.• Due to abnormal wound healing, use TORISEL with caution in the perioperative period.• Patients with central nervous system tumors (primary CNS tumor or metastases) and/or receiving anticoagulation therapy
may be at an increased risk of developing intracerebral bleeding (including fatal outcomes) while receiving TORISEL.
portant Safety Information
Change expectationsfor overall survival
With the fi rst and only IV mTOR inhibitor indicated for advanced renal cell carcinoma (RCC)1...
TUP100027_ASCO Post_Tabloid_FNL.indd 1-2 8/12/10 4:38 PM

TUP100027_ASCO Post_Tabloid_FNL.indd 3-4 8/12/10 4:38 PM


PAGE 32 The ASCO Post | JANUARY 1, 2011
In the News
Long-term results of a breast can-cer screening study found that
that intensive surveillance that in-cludes magnetic resonance imaging (MRI) in addition to mammography and physical examination is more ef-fective in detecting breast cancer early in women at high-risk of the disease due to BRCA1/BRCA2 mutations or family history. Among the significant points raised by the study is the idea that “a program of careful screening with physical examination, mam-mography, and MRI, can be a rational and reasonable alternative” to pro-phylactic mastectomy for women at high risk of breast cancer, Andrew D. Seidman, MD, attending physician and medical oncologist at Memo-rial Sloan-Kettering Cancer Center in New York, said in an interview with The ASCO Post.
The Dutch MRI Screening Study involved 2,157 women with a cumula-tive lifetime risk of breast cancer ≥ 15% due to familial or genetic predisposi-tion. This included one subgroup of 599 women with an estimated cumu-lative lifetime risk of 50% to 85% due to BRCA1/BRCA2 or other gene mu-tations, and two other subgroups of women with high (30%–50%) or mod-erate (15%–30%) cumulative lifetime risk but without documented gene mutations. All received biannual clini-cal breast examinations and annual, si-multaneous mammography and MRI.
“MRI sensitivity was superior to that of mammography for invasive cancers (77.4% vs 35.5%; P < .00005), but not for ductal carcinoma in situ [DCIS],” the investigators reported. Among the 75 breast cancers (including 13 cases of
DCIS and 9 inter-val cancers) found with results of both MRI and mammog-raphy, the sensitiv-ity was 70.7% for
MRI vs 41.3% for mammography and 20.6% for clinical breast examination. “Strikingly, the sensitivity of MRI was much higher than that of mammogra-phy in BRCA1 (n = 24; 66.7% vs 25%; P = .0129) and only slightly higher (n = 13; 69.2% vs 61.5%; P = 1.0) in BRCA2 mutation carriers,” the inves-tigators stated. The study results were published in the Journal of Clinical On-cology1 and reported online and in the press, including The New York Times.2
Potentially Practice-changing “The investigators have conducted
the largest such trial of MRI screen-ing in high-risk individuals, and their new report that MRI screen-ing appears to be preferentially use-ful in BRCA1 mutation carriers as compared to BRCA2 has potentially practice-changing implications,” Dr. Seidman commented.
Mortality in the Dutch study was low, with four deaths at a median of 5 years after diagnosis, all among women with BRCA1/BRCA2 muta-tions. Overall survival 6 years after diagnosis was 93% among the 42 BRCA1/BRCA2 mutations carriers who developed invasive breast cancer, which compares favorably to a 74% overall survival in 26 previous studies with a median follow-up of 5 years.
“The favorable overall survival in all high-risk groups reported sug-gests that careful MRI screening is not only superior to mammography alone, but may be an attractive alter-native to risk-reducing prophylactic mastectomy for some women,” ac-cording to Dr. Seidman. “A woman who has to make a life-altering de-cision about having prophylactic bilateral mastectomy shouldn’t feel that the prophylactic mastectomy is absolutely the only option.”
Nearly 36% of the invasive tumors detected in women with BRCA1 muta-
Is MRI-based Screening a Reasonable Alternative to Prophylactic Mastectomy for Women at High Risk of Breast Cancer?By Charlotte Bath
In the News focuses on media re-ports that your patients may have questions about at their next visit. This continuing column will pro-vide summaries of articles in the popular press that may prompt such questions, as well as com-ments from colleagues in the field.
Expect Questions from Your PatientsDoes the Dutch study mean that MRI should be part of standard screening for breast cancer?
No. The Dutch breast cancer screening study involved only women at high risk of breast cancer due to genetic or familial factors and did not assess MRI as standard breast cancer screening for all women. The study authors state that the ability of MRI to detect breast cancers not detected by either mam-mography or clinical breast examination and at a favorable tumor stage “sup-port the recommendation of the American Cancer Society to use annual MRI screening not only for BRCA1/2 mutation carriers, but for all women with approximately 20% to 25% or greater cumulative lifetime risk of breast cancer due to familial predisposition. However, the cost-effectiveness of MRI screen-ing should be evaluated for all risk groups separately.”
How do these study results affect the options for women at high risk of breast cancer?
Currently, women with a family history of breast cancer that includes close relatives who have died of the disease “often chose prophylactic surgery,” Dr. Seidman said. “The other option for prevention is use of selective estrogen receptor modulators such as tamoxifen and raloxifene, and these have been shown to reduce the risk of developing breast cancer by about half. What the Dutch study offers is yet another option. For women who can live with the anxiety of having frequent scans and undergoing a biopsy if there is something suspicious—and who find the idea of prophylactic surgery to be very unat-tractive or repulsive—the Dutch study offers some reassurance that a screen-ing program of biannual physical examination, mammography, and MRI, may not be an unreasonable choice.”
Can these options be switched?Yes. Choosing the screening program option and taking tamoxifen or ral-
oxifene are “not mutually exclusive,” Dr. Seidman added. “So certainly one can use ‘chemoprevention’ as well as MRI and mammographic screening as a way to either avoid or delay the use of prophylactic surgery.” In addition, a woman who initially decides against prophylactic surgery may later decide not to deal with the anxiety anymore and have the surgery.
Is prophylactic mastectomy still the most effective preventive measure?Yes, but “prophylactic mastectomy is not 100% preventive of breast cancer,”
Dr. Seidman noted. “It is the most effective preventive measure that we know, but even in published series, as many as 5% or so of patients—despite prophy-lactic mastectomy—may still develop breast cancer in breast tissue that is left behind on the chest wall.” ■
Andrew D. Seidman, MD
tions were larger than 2 cm, compared to about 8% in the BRCA2 group. This indicated that the cancers found in the women with BRCA1 mutations “probably have a different biologic behavior, such that morphologically what happens in the breast translates to a stealthy pattern of growth, one that is harder to detect with imaging,” Dr. Seidman said. “This study shows us that BRCA1- and BRCA2-associat-ed breast cancers are distinct entities.”
More Frequent MRI?The Dutch study “strengthens
the argument that particularly for BRCA1-related breast cancers, MRI increases sensitivity significantly over mammography,” Dr. Seidman said. Even so, he continued, “there was a much higher incidence of interval cancers—cancers that were diag-nosed in between screening imag-ing—in the BRCA1 group, suggesting that we might need to consider either more frequent MRI scanning or some other improved or supplemental im-aging modality.”
The study’s authors suggest that a “modification of the screening sched-See page 33

ASCOPost.com | JANUARY 1, 2011 PAGE 33
In the News
ule for BRCA1 mutations carriers (eg, biannual MRI)” as well as other mea-sures may be necessary “in order to further improve results on survival, which seem promising with the cur-rent schedule.” These newer measures could include PARP inhibitors. “We are all hopeful that the PARP inhibitor class may represent a class of drugs that have unique relevance to BRCA-mu-tated breast cancers, but that remains to be seen in large randomized trials,” Dr. Seidman said. ■
What about Ultrasound?
Not addressed in the Dutch study, Dr. Seidman noted,
but used in many clinical prac-tices—at least in the New York metropolitan area where he is based—is the use of ultrasound as yet another imaging modality. Many women who fit the high-risk categories in the Dutch study, he said, “are having triple imag-ing—mammography, MRI, and ultrasound.”
Triple imaging tests are often staggered, but with mammogra-phy and ultrasound usually done together. “Doing certain breast evaluations together as a package may be more powerful than doing them in isolation,” Dr. Seidman said. “Also within that package, of course, is the clinical breast ex-amination. Findings on physical examination or mammography might direct ultrasound, so that it is more of a directed test, rather than a screening test. But what we really lack are good, rigorous trials to determine how much, if any, ul-trasound will improve the predic-tive value in these patients at high risk.” ■References
1. Rijnsburger AJ, Obdeijn I-M, Kaas R, et al: BRCA1-associated breast cancers present differently from BRCA-associated and famil-ial cases: Long-term follow-up of the Dutch MRISC Screening Study. J Clin Oncol. November 15, 2010 (early release online).
2. Grady D: M.R.I.’s help fight high risk of cancer. New York Times, November 15, 2010.
What’s this?
Simply text the word “scan” to 43588.
Go to www.getscanlife.com on your phone’s Web browser. The application will attempt to determine which model phone you have. If it’s successful, simply select “Download”.
Visit the application store for your smartphone (such as the iTunes Store or the Android Market).
1 2 3
Using 2D BarcodesThe 2D barcodes found in this issue of The ASCO Post will connect readers to further information about the articles they are reading using the ScanLife application.
Getting the ApplicationThere are three ways to download the ScanLife application:
PHASE III TRIAL CURRENTLY RECRUITING

PAGE 34 The ASCO Post | JANUARY 1, 2011
FDA Update
FDA Recommends Removing Breast Cancer Indication from Bevacizumab Label
The FDA has announced that the agency is recommending removing the breast cancer indication from the label
for bevacizumab (Avastin) because the drug has not been shown to be safe and effective for that use.
The agency is making this recommendation after reviewing the results of four clinical
studies of bevacizumab in women with breast cancer. According to the agency, the data indicate that the drug does not pro-long overall survival in breast
cancer patients or provide a sufficient
benefit in slowing disease progres-sion to outweigh the significant risk to patients. These risks include se-vere high blood pressure; bleeding and hemorrhage; the development of perforations in the body, including in the nose, stomach, and intestines; and heart attack or heart failure.
In July 2010, an independent advi-sory committee, composed primarily of oncologists, voted 12–1 to remove the breast cancer indication from the drug’s label.
The FDA’s recommendation is the first step in a process. The drug is not being removed from the market, and the action will have no immediate im-pact on its use in treating breast cancer. The action will not affect the drug’s ap-proval in colon, kidney, brain, and lung cancers. Oncologists currently treating patients with bevacizumab for metastat-ic breast cancer should use their medi-cal judgment when deciding whether a patient should continue treatment with the drug or consider other options.
The FDA is open to working with Genentech, the drug’s manufacturer, on proposals to conduct additional studies of bevacizumab in patients with meta-static breast cancer designed to identify a population of patients in which the drug’s benefits exceed the risks.
ODAC Opposes Dutasteride, Finasteride for Prostate Cancer Risk Reduction
The FDA Oncologic Drugs Advisory Committee (ODAC) recently voted against approval of supplemental New Drug Applications (sNDAs) for dutas-teride (Avodart, GlaxoSmithKline) and finasteride (Proscar, Merck & Co) for reduction in prostate cancer risk in men at increased risk of developing the disease. When asked if the dutasteride risk- benefit profile is favorable for risk reduction, ODAC voted 14 against, 2 in favor, and 2 abstentions. The vote on finasteride was 17–0, with 1 abstention.
The ODAC panel noted that, al-though studies of both dutasteride and finasteride showed they reduced the overall risk of developing prostate can-cer, the drop was driven by a decline in low-grade, slow-growing cancers that typically aren’t life-threatening. The reviewers also raised the concern that healthy people taking these drugs could increase their risk for high-grade tumors.
Both drugs are currently approved to treat symptomatic benign prostatic hypertrophy. ■
Oncology Drug News
Join us before the conference!Preconference Workshops on 17 February 2011 featuring Jimmie Holland MD, William Breitbart MD, Donna Greenberg MD, Matthew Loscazlo LCSW, and more experts on topics such as
• Getting Your Work Published • Meaning Centered Psychotherapy • Creating Tomorrow’s Leaders Today • Psycho-Pharmacology • Patient Centered Communication• Patient-Reported Outcomes Measurement Information System (PROMIS)• Therapeutic Work with Children and Adolescents When a Parent has Cancer• The Bright IDEAS System• Creating a Culture of Screening through Interactive Teams
Patricia Ganz MDUCLA Jonsson Comprehensive Cancer Center
Visit www.apos-society.org/apos2011 for conference details!
The American Psychosocial Oncology Society (APOS) invites you to join us at the APOS 8th Annual Conference in Anaheim, CA, USA, 17 - 19 February 2011.
Barbara Sourkes PhDStanford University School of Medicine
Keynote Presentations by
APOS • 154 Hansen Rd. Ste. 201, Charlottesville, VA 22911 USA Ph: +1.434.293.5350 • Fax: +1 434.977.1856 • [email protected]
Quality Cancer Care Across the Lifespan: Psychosocial Research and Practice Across DisciplinesJointly Sponsored By
Mission San Juan Capistrano, Orange County
www.apos-society.org/apos2011

ASCOPost.com | JANUARY 1, 2011 PAGE 35
Lessons Learned
When I started practicing oncol-ogy in 1973, I was frequently
asked by my patients, “What’s my prognosis, what can I expect?” At first, I was reluctant to tell the patient very much, especially when I knew the prognosis wasn’t good. I wanted to spare the patient the details of the inevitable outcome of his cancer, so I downplayed the truth. Some may call it sugarcoating the information. I just wanted to do anything I could to protect my patient from learning that not only didn’t we have a cure for his cancer, we didn’t even have a treatment to extend his life. The best we could do was to maybe improve the quality of his life for as long as possible.
Now, 37 years later, not much has changed. Today, most patients with cancer never receive information from their physicians about their prognosis or even imminent death. According to a recent article in The Journal of the American Medical Association, not tell-ing patients their prognosis leads to a worse quality of life for both patients and their caregivers.
Why are physicians so reluctant to give their patients truthful an-swers regarding their prognosis? When asked, most oncologists say that they don’t want to take away their patients’ hope of recovery. Oth-ers say they are afraid that if they tell them the truth, the patients will stop treatment. Some worry that their pa-tients will leave and seek the advice of another physician.
Evidence to the ContraryRecently, I read a study showing
that hope is maintained when patients with advanced cancer are given truth-ful prognostic and treatment informa-tion, even when the news is bad. The study, performed at the VCU Massey Cancer Center, surveyed 27 patients with advanced cancers, including breast, lung, colon, and prostate malig-nancies, about their feelings regarding their cancer and their future. The re-searchers used the Herth Hope Index to assess the impact of giving the study participants accurate information about their prognosis.1
Why We Avoid Telling Patients the TruthBy Stanley Winokur, MD
After reading the results of this study, I wondered why the practice of not being totally honest with our pa-tients still exists, especially when other studies also support the Massey find-ings. Rather than fearing that our pa-tients may give up and stop treatment if they knew the truth, I wondered if the real reason we avoid telling our pa-tients the truth was because, as physi-cians, we can’t admit to ourselves that we can’t cure our patients or even ex-tend their lives.
I know it was difficult for me to face that reality. Patients and their family members seek us out to solve their problem, and yet we are limited in our knowledge of how to do that. After several years in practice, I fi-nally found the balance between tell-ing my patients the truth about their prognosis and maintaining their hope. Finding that balance is what I have come to believe is the “art of medicine.”
Patients want us to be truthful, compassionate, and clear about their prognosis and want to know that we will be there with them every step of the way. Rather than taking away hope, being honest with our patients provides them with the necessary in-formation to help them redefine hope, even if cure is not possible. ■Reference
1. Smith TJ, Dow LA, Virago E, et al: Giving honest information to patients with advanced cancer maintains hope. On-cology (Williston Park) 24:521-525, 2010.
Dr. Winokur is a retired oncologist who lives with his family in Singer Island, Florida. He is the author of Grandfathered In: A Memoir, a book about finding balance between having a career in medicine and having a family.© Robert Mankoff/The New Yorker Collection/www.cartoonbank.com
The ASCO Post (ISSN 2154-3283) is published semi-monthly, except monthly in February, April, June, August, October and December, by Harborside Press, 37 Main Street, Cold Spring Harbor, NY 11724, under a license arrangement with the American Society of Clinical Oncology, Inc. (ASCO®). Application to mail at Periodicals Prices is Pending at Cold Spring Harbor, NY, and additional mailing offices.
Change of Address: Postmaster send address changes to The ASCO Post, c/o Harborside Press, 37 Main Street, Cold Spring Harbor, NY 11724. ASCO Members: If you would like to cancel your subscription to The ASCO Post or need to update your mailing address, please visit your personalized page on ASCO.org. For personalized service, please contact ASCO Member Services at (888) 282-2552, (703) 299-0158, or via email at [email protected]. Non ASCO Members: To initiate or cancel a subscription or to update your mailing address, please email [email protected] or fax (631) 692-0905.
Copyright ©2011 by Harborside Press, LLC. All rights reserved. Reproduction in whole or in part, in any form, without pri-or written permission of the publisher is prohibited. For permission inquiries, contact [email protected].
Editorial Mission: The ASCO Post communicates timely information to a broad audience of oncology specialists, helping to advance the highest quality multidisciplinary cancer care. The ASCO Post publishes highly validated coverage of cancer research and policy news, patient care and clinical practice issues, and thoughtful commentary from leaders in the field and others with an interest in clinical oncology.
Circulation: The ASCO Post is sent free of charge to approximately 26,000 physicians and nurses, including all US-based ASCO members. Medical, surgical, pediatric, and gynecologic oncologists, hematologists, and hematologist/oncologists in the United States who are not members of ASCO will be eligible for a complimentary subscription. ASCO members outside of the United States receive complimentary access to The ASCO Post online at www.ASCOPost.com. Paid subscriptions to The ASCO Post are available for all other interested individuals. Individual Domestic: $225; Individual International: $275; Institutional Domestic: $275; Institutional International $350. Contact [email protected].
Correspondence: Address general inquiries to Harborside Press, 37 Main Street, Cold Spring Harbor, NY 11724. Phone: 631.692.0800; Fax: 631.692.0805. Address editorial correspondence to James O. Armitage, MD, Editor-in-Chief, c/o Cara Glynn, phone: 631.935.7654; e-mail: [email protected].
Advertising: For information on advertising rates, reprints, or supplements, contact Leslie Dubin, phone: 631.935.7660; e-mail: [email protected].
Notice to Advertisers: Advertiser and advertising agency recognize and accept that the following language appears within the publication: “All statements, including product claims, are those of the person or organization making the statement or claim. Neither the publisher nor ASCO adopts any such statement or claim as its own, and any such state-ment or claim does not necessarily reflect the opinion of the publisher or ASCO.”
Advertiser and advertising agency accept and assume liability for all content (including text, representations, illustra-tions, opinions, and facts) of advertisements printed, and also assume responsibility for any claims made against the publisher or ASCO arising from or related to such advertisements. In the event that legal action or a claim is made against the publisher or ASCO arising from or related to such advertisements, advertiser and advertising agency agree to fully defend, indemnify, and hold harmless the publisher and ASCO, and to pay any judgment, expenses, and legal fees incurred by the publisher and by ASCO as a result of said legal action or claim. The publisher reserves the right to reject any advertising that it believes is not in keeping with the publication’s standards.
The publisher is not liable for delays in delivery and/or non-delivery in the event of Act of God, action by any government or quasi-governmental entity, fire, flood, insurrection, riot, explosion, embargo, strikes (whether legal or illegal), labor or material shortage, transportation interruption of any kind, work slow-down, or any condition beyond the control of the publisher affecting production or delivery in any manner.
Disclaimer: The ideas and opinions expressed in The ASCO Post™ do not necessarily reflect those of Harborside Press, LLC, HSP News Service, LLC, or the American Society of Clinical Oncology, Inc. (ASCO®). The mention of any product, service, or therapy in this publication should not be construed as an endorsement of the products mentioned. It is the responsibility of the treating physician or other health-care provider, relying on independent experience and knowledge of the patient, to determine the appropriate treatment for the patient. Readers are advised to check the appropriate medical literature and the product information currently provided by the manufacturer of each product or therapy to be administered to verify the dosage, method, and duration of administration, or contraindications. Readers are also encouraged to contact the manufacturer with questions about the features or limitations of any products. Harborside Press, HSP News Service, LLC, and ASCO® assume no responsibility for any injury or damage to persons or property arising out of or related to any use of material contained in this publication or to any errors or omissions.
Patients want us to be truthful, compassionate, and clear about their prognosis

To meet this unmet need, Novartis Oncology has undertakenthe largest Phase III clinical trial program of targetedtherapy in advanced NET, enrolling more than 800 patients.2
The trials have investigated patients with carcinoid (GI andlung) and pancreatic NET.2 Novartis Oncology has a strongheritage of leadership in developing cancer therapies thathave enriched and improved the lives of patients living withmany types of cancer. We are dedicated to developingeffective treatment options for patients with diverse types ofadvanced NET.
References: 1. Yao JC, Hassan M, Phan A, et al. One hundred years after “carcinoid”:epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 casesin the United States. J Clin Oncol. 2008;26:3063-3072. 2. Data on file. NovartisPharmaceuticals Corporation.
The options are limited for treating thispotentially aggressive diseaseProgressive neuroendocrine tumor (NET) presents a seriouschallenge: The median duration of survival among patientswith metastatic NET is 33 months.1
The median duration of survival among patients withmetastatic neuroendocrine tumor is 33 months.1
NET is a complex disease affecting many organ systems,including the gastrointestinal (GI) tract, lungs, andpancreas.1 These types of NET are unique in biology andpathogenesis. The GI tract and lungs are the most commonsites of origin for NET, giving rise to carcinoid tumors thatoccur in a total of 85% of all NET patients.1 Advancedpancreatic NET can be aggressive, with a median survivaltime of only 27 months.1 There is no currently approvedtherapy to address the need for tumor control for theseNETs of diverse origin.
No current therapy addresses the need for tumor controlfor neuroendocrine tumors of diverse origin: GI, lung, and pancreatic NET.
We’re committed to finding a path forward
When a patient’s neuroendocrine tumor progresses...
Novartis Pharmaceuticals Corporation East Hanover, NJ 07936 ©2010 Novartis Printed in U.S.A. 09/10 ONC-901380
Safety:9.5”Safety:13”
Trim:10.5”Trim
:14”
Bleed:10.75”Bleed:14.25”
103310_Afinitor_Advert_King.v1.indd 1 12/6/10 4:22 PM
Related Documents