1 Tanta Scientific Nursing Journal Prof Dr Rahma Soliman Bahgat Board Director Prof Dr Rahma Soliman Bahgat Editor in chief Dr Manar Zaky Elwelely Editor Secretary Vol. 3 No. 3 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Tanta Scientific Nursing Journal
Prof Dr Rahma Soliman Bahgat
Board Director
Prof Dr Rahma Soliman Bahgat
Editor in chief
Dr Manar Zaky Elwelely
Editor Secretary
Vol. 3 No. 3
2012
2
Editorial Advisory Board
Prof Dr Farial Abdal Aziz : Community Health Nursing Alexandria University
Prof Dr Gamalat Elsaid Mansy : Pediatric Nursing, Alexandria University
Prof Dr Bassema Azat Goid : Community Health Nursing, Tanta University
Prof Dr Nazek Ebrahim AbdElghany: Community Health Nursing, Alexandria University
Prof Dr Fouada Shaban : Nursing Administrative Tanta University
Prof Dr Seham Hamoda : Nursing Administrative Tanta University
Prof Dr Rahma Soliman : Pediatric Nursing, Tanta University
Prof Dr Sanaa Abdal Aziz : Psychiatric and Mental Health Nursing , Alexandria University
Prof Dr Zeinab Loutfy: Psychiatric and Mental Health Nursing ,Ain shams University
Prof Dr Sanaa Ala eldeen: Medical Surgical Nursing, Alexandria University
Prof Dr Nahed Elsabahy: Medical Surgical Nursing, Alexandria University
Prof Dr Sanaa Nour: Obstetric and gynecological Nursing, Zagazig University
Prof Dr Magda Mourad : Obstetric and Gynecological Nursing , Alexandria University
3
Information to Authors
General policies
The Bulletin of Tanta Scientific Nursing Journal publishes concise, original articles
and contributions in the board field of nursing sciences. The Editor is responsible
for the view and statements of authors expressed in their articles.
The authors must transfer all copyright townships of the published manuscripts to
the Bulletin of Tanta Scientific Nursing Journal
The authors still retain the right to post, without permission, their own published
manuscript either as link to the online version of the manuscript on the website of
the journal
Table and figures are permitted to be used by authors
Provide the proper reference is made to the original published manuscripts and the
journal
Preparation of Manuscript:
Format: three complete copies should be submitted
- Should be printed on A4 80 gm paper, 1.5 line space with 2.5 cm margins.
Manuscripts should not exceed two column, 12 pages, and inclusive
references. CD containing the manuscripts should be enclosed
- Title of manuscripts: should be concisenot more than 15 words and include
the name of the authors(s) professional 5itle and institution affiliation
Abstract: not exceeding 200 words, should be included , ti should state the
aim of the study , subjects and methods and important findings and
conclusion
Below the abstract provide and identify 3 to 10 key words or short phrases
for indexing according to the contemporary subject headings
A list of all abbreviations: used should be provided after the abstract.
Abbreviations are not placed in parentheses at first use in the text
Introduction: It should include relevant literature related to the problem
4
of abbreviations should be spelled out the first time they are used. Symbols, others
than standard statistical symbols, should be identified the first time used
Subject and methods:
Should include setting where the study was done subjects of the study and
criteria for selection, tools for data collection and study design and procured.
Results:
Tables, figures or graphs should be typed or drawn on one page and relative
placement should be noted in the text
Discussion:
The findings with other relevant studies in the field of studies in the field of
study
Conclusion
Recommendations
References: are numbered according to order of appearance in the text and should
follow the style of the uniform requirements for manuscripts submitted to the
journals. The Vancouver style should be followed
Procedures
All papers will be reviewed by three .The final decision to publish or reject
the manuscript remains in the hand of the editor. All manuscripts will be sent
to a statistical reviewer. Proof reading of manuscripts for linguistic and
typographic sounds will be done by the editors will be returned .The initial
review process is expected to take 2 weeks time. Accepted manuscripts
become the property of the Tanta nursing scientific journal. The journal
reserves the rights to edit all manuscripts for its style and space requirements
and for the purpose of the clarity of Tanta journal of nursing will determine
in which volume and issue accepted manuscripts will appear.
Faculty of Nursing, Tanta University
5
Address:
Email: Tanta nursing [email protected]
Email: [email protected]
Three copies of the manuscripts and CD that should be sent to Tanta
Scientific Nursing Journal
Subscription information
Online access is open to all readers at no subscription fees
Print version subsection
6
Contents
Subject Page
1-Quality of Nursing Interventions Provided to Infants Receiving
Mechanical Ventilation 7
2-Infection among Women using Intrauterine Devices and Oral
Contraceptives
22
3-Whiff Test and Vaginal pH >4.5 as Rapid and Accurate Bed-side
Screening Test for Vaginal Infection 50
4-Effects of Topical Honey Dressing on Infected Wounds after
Gynecological and Obstetrical Abdominal Surgery 57
5-Effect of Nursing Intervention on the Supportive Role Played by
Peers on Glycemic Control Among Diabetic School Students in
Tanta City.
77
6-Application of Designed Orientation Program for Nurse Interns
Based on Learning Needs Assessment
7-Life Style Profile of School Age Children Suffering From
Pathological Stuttering
8- Establishing Basic Standards of Nursing care protocol at
Neonatal Intensive care unit.

7
Quality of Nursing Interventions Provided to Infants
Receiving Mechanical Ventilation
Rahma Soliman Bahgat Profssor of pediatric Nursing
Faculty of Nursing, Tanta University
Ebtisam Mohmed El-Sayed
Assistant professor of Pediatric Nursing , Tanta university
Ahmed AbdEl Basset, Assistant professor of pediatric Medicine
Faculty of Medicine , Tanta University
Shimaa Ramadan Ahmed Abd El- Sattar .B.SC.N
Faculty of nursing tanta university
Abstract
Mechanical ventilation is a complex supportive and life saving therapy for many children
with respiratory failure. Optimal outcomes for these children are achieved through the skilled
delivery of standardized nursing care include management of the airway and ventilator, physical
care, emotional support, pain and anxiety control and prevention of complications. The present
study aimed to assess the quality of nursing interventions provided to infants receiving
mechanical ventilation. The study was conducted at Pediatric Intensive Care Unit of Tanta
University Hospital. It included thirty nurses working in the previously mentioned setting and
sixty infants who received mechanical ventilation. Two tools were used for data collection: a
structure questionnaire sheet and an observational checklist. The results revealed that, more than
half of studied nurses had fair knowledge in relation to their educational level. The majority of
them had poor practice in relation to the educational level and years of experience in afternoon
shift comparing with morning shift. The study recommended that, in-service training programs
and workshops should be conducted for those nurses to improve their knowledge and
performance about standard nursing care of mechanically ventilated infants with constructive
supervision and follow up by head nurses.
8
Introduction
Advances in respiratory care have become
an integral part in the care of critically ill
patients. Support of oxygenation and/or
ventilation is an integral to the practice of
pediatric critical care nursing because the
majority of critically ill infants and
children need interventions to stabilize the
pulmonary system.(1)
Mechanical ventilation is the foundation of
resuscitation, intensive care medicine, and
anesthesia.(2)
It is an invasive life support
procedure with many effects on the
cardiopulmonary system to mechanically
assist or replace spontaneous breathing. (3,4)
Mechanical ventilators are devices that can
create a flow of gas into and out of the
lungs by the manipulation of airway
pressures. The main goal of the ventilator
may be achieved by improving alveolar
ventilation, arterial oxygenation,
increasing lung
volume and reducing work of breathing.(5)
Mechanical ventilation is indicated when
the patient is unable to maintain safe levels
of oxygen and carbon dioxide through
spontaneous breathing.(3)
It is mainly used
for patients with acute respiratory failure.(6)
Respiratory failure is a sudden and life
threatening deterioration of function of the
lung, and inability to maintain normal
arterial blood gases.(7- 9)
The number of children who are suffering
from respiratory failure increases annually
all over the world. It is estimated that the
number of children who are suffering from
respiratory failure is about 1.5 million
children. In Egypt, the annual statistical
report of the Ministry of Health and
Population in 2004 showed that, the
mortality number of infants from
respiratory distress was 11.656 from
1.849.638 live births. Meanwhile, the
mortality number of children who are five
years or less is 2708 child.(1)
There are 79,400 hospitalizations in the
United States each year for neonates
undergoing mechanical ventilation,
8,500 of whom die. Importantly, almost
40% of deaths occur in cases that never
receive care at higher level centers. (10)
Mechanical ventilation can be noninvasive,
involving various types of face masks, or
invasive, involving endotracheal
intubation. Decision to initiate mechanical
ventilation should be based on clinical
judgment that considers the entire clinical
situation and should not be delayed until
the patient is in extremis.(11)
Traditionally
mechanical ventilation divided into
negative-pressure ventilation, where air is
essentially sucked into the lungs, or
positive pressure ventilation, where air (or
another gas mix) is pushed into the trachea.
(4)
9
Mechanical ventilation is often a life-
saving intervention, but carries many
potential complications including
pneumothorax, airway injury, alveolar
damage, and ventilator-associated
pneumonia.(12)
Endotracheal suction is one
of the most common procedures carried
out in an intensive care unite. Suctioning
techniques are necessary nursing care used
to clear the airway of thick secretions. (13)
Quality of care focused on the system of
care. It is concerned with improving the
processes, so that everyone’s performance
improves. Improvement usually requires
removing the barriers in the way of the
providers who already possess the
motivation in order to established standard.
(14)
Nurses are constantly present at the
patient’s bedside, so they are the primary
healthcare for monitoring the patient’s
respiratory status. They also responsible
for notifying the respiratory therapist when
mechanical problems occur with the
ventilator, and when there are new
physician orders that call for changes in
the settings or the alarm parameters. (7, 15)
The nurse is responsible for documenting
frequent respiratory assessments. This
usually means documenting ventilator
setting and spontaneous respiratory
parameters every hour, with a full
respiratory assessment, including lung
sounds, at least every four hours. The
nurse also performs suctioning and
provides oral and site care around the
artificial airway. There is often a great deal
of teaching and reassuring that must be
done, both for the patient and their
family.(16)
Aim of the study:
This study aimed to assess the quality of
nursing interventions provided to infants
receiving mechanical ventilation.
Subject & Methods:
Research design:-
A descriptive design was used in this
study.
Setting:-
This study was conducted at Pediatric
Intensive Care Unit of Tanta University
Hospital. It contained one large room with
6 pediatric beds, 6 ventilators and 2
continuous positive airway pressure
devices.
Subjects:-
All available nurses working in the
previously mentioned setting who are
caring for mechanically ventilated infant
regardless of their years of experience,
level of education and their ages were
included in this study. The total number of
thirty nurses were classified as follows (12
nurses graduated from faculty of nursing, 5
nurses graduated from technical institute of
nursing and 13 nurses with secondary
school nursing diploma).
10
60 infants who received mechanical
ventilation are included in this study
according to the following criteria:
Their age : from one month to 12 months
Both sexes ,Acute stage of respiratory
disorder, Free from any chronic disease
Tools of the study:-
Two tools were used to collect the
required data in this study. They were
developed based on the recent literature.
Tool I: "A Structure Questionnaire
Sheet". It was constructed by the
researcher to assess nurses' knowledge
about mechanical ventilation. It consisted
of two parts:
Part (1):- Biosocial data: It was
developed to assess a- nurses' socio-
demographic data such as (age, level of
education, years of experience and
previous training). b- infant socio-
demographic data such as (age, sex,
date of admission, date of applying
mechanical ventilation, and history of
medical diagnosis).
Part (2):- Nurses' Knowledge about
mechanical ventilation. It included:-
definition, purpose, indications, types,
modes, parameters, complications, criteria
used for initiation of mechanical
ventilation and nursing management of
infants receiving mechanical ventilation
such as: (care for the tube, chest
physiotherapy, suction, hygienic care "eye,
oral, skin care", infection control strategies
and psychological support).
The questionnaire sheet contained closed
ended questions and the nurses were
asked to respond to these ones with only
one correct response for each; the nurses
who responded " correct answer" (one)
was given and the nurses who responded
"incorrect answer" or "did not give any
answer" (zero) was given. The "total
knowledge score" was 54 where it comes
from multiplying total number of
questions (54) in the correct response
score (1), and then the result is divided by
100 to be converted into percentage.
Grading of nurses' answers to
questions and checklist were converted as
follows: Total knowledge score from 50-
↓60% was graded (poor), total knowledge
score from 60-↓70% was graded (fair) and
total knowledge score from 70-100% was
graded (good).
Tool II: "An Observational Checklist":
It was developed by the researcher to
assess the quality of nursing interventions
related to the actual nursing care provided
to infants receiving mechanical ventilation.
It comprised 5 main items:
1-Provide care for the tube:
- All tubes must be secured to decrease
tube movement and accidental extubation.
- Inspect the skin, nose, and mouth for
tissue breakdown.
11
- Change tracheostomy tape or
endotracheal tube tape as needed.
- Move the oral endotracheal tube to the
opposite side of the mouth every 24 hours.
- Frequently assess the tube’s position
2-Make Suction:
- When secretions are present.
- Prepare all needed equipment before the
procedure.
- Use the appropriate catheter size.
- Duration of the suctioning.
- Apply pre-oxygenation be considered for
30–60 seconds prior.
- Physical assessment such as rate and
depth of respiration, nature of breathing
sound.
3- Provide general hygienic care: -
including: Eye care, Mouth care and Skin
care.
a) Eye care:
- Instillation of ophthalmic ointment or
drops decreases corneal drying.
- The infant's eye should be swapped with
normal saline regularly.
- Apply antibiotic drops or ointment to the
eye as ordered.
- The eyelids of the infant should be
closed to prevent corneal ulceration.
b) Mouth care:
- Mouth care at least once per shift by
using oral swab.
- lubricate lips with water-soluble ointment
to prevent drying of lips.
-Reposition or rotate the endotracheal tube
from one corner of the mouth to the
opposite side every 24 hours.
c) Skin care:
- Bath the infant daily.
- Change position every 2 hours.
- keep infants clothes clean, dry and keep
bed free from any objects.
- Lubricate the back and bony prominence
and frequent massage for the back should
be done.
4- Follow infection control strategies:
- Washing hands before handling the
infant, before and after any procedure.
- Use isolation technique of infant who has
any infectious disease away from other
infants.
- Avoid exposing the infant to persons
with upper respiratory tract infection.
- Remove or empty water that
accumulates in the ventilator tubing.
-Methods and schedules of cleaning and
disinfection of ventilator circuits should be
learned and applied.
5-Psychological support:
- Provide an emotional support to the
infant by applying distraction techniques
as: allowing the infant to listen to stories &
quiet music, providing back rub & gentle
massage and offering attractive & safe toys
for conscious infants.
Different nursing activities related
to each item were listed. A scoring system
was used to check each activity whether it
was adequately done, inadequately done or

12
not done. Scoring of (two points) was
given to adequate nursing activity; (one
point) was given to inadequate nursing
activity and (zero) for not done nursing
activity with a total score of (334) where
it comes from accumulating the number of
steps of all nursing care procedures (167)
multiplied in adequate nursing activity
score (2) then the result is divided by100
to be converted into percentage.
The total score of each item was (34
points for chest physiotherapy, 40 points for
care of the endotracheal tube, 36 points for
nasopharyngeal and oropharyngeal Suction,
38 points for endotracheal Suction, 98 points
for general hygienic care (28 points for eye
care, 38 points for mouth care, 32 points for
skin care), 62 points for infection control
strategies ( 24 points for application of
standard precautions and transmission based
precautions, 10 points for care of ventilator,
28 points for central venous catheter care) ,
and 26 points for Psychological support.
Grading of checklist nursing practice
were converted as follows: from 60-↓65 %
was graded "poor", 65-↓70% was graded
"fair", 70-100 % was graded "good".
Method
- An official permission was obtained
from the directors of hospital of the
selected setting (PICU at Tanta University
Hospital).
- Meeting with nurses before starting data
collection procedure was done to establish
a good relationship, check the availability
of conducting the research, and to explain
the purpose of the study.
- An oral consent was obtained from the
nurses to participate in the study after
explanation of the purpose and importance
of the study.
- Study tools were structured and
developed based on review of the related
literature.
- Ethical considerations:-
Nurses were informed of the privacy of
information obtained from them,
nature of the study, their right to withdraw
from the study at any time and the
confidentiality of their names.
- The pilot study: Pre-test of the used tools
was carried out at the above mentioned
setting before starting the data collection .It
was done on 10% of the study sample to
assess clarity, reliability, applicability of the
study tools, the time needed to fill each tool,
and to identify obstacles that might be faced
during data collection. The sample which
was included in the pilot study was a part of
the studied sample.
- A structure questionnaire sheet was
developed to assess the nurses' basic
information and knowledge related to
mechanical ventilation.
-The questionnaire sheet was distributed
on nurses; the content of the sheet was
explained to all of them and filled
individually. The nurses were reassured
13
that all information will be confidential
and used only for the purpose of the study
and nurses were asked to respond in the
presence of the researcher.
- The time required for answering the
questionnaire sheet was about one hour.
- Each nurse was observed twice in the
morning and afternoon shifts by the
researcher to assess her care provided to
the infant receiving mechanical ventilation
by using observational check list.
- The time required to the researcher for
checking the observational checklist for
each nurse was about 2 intermittent hours.
-Data were collected over a period of 4
months from October 2011 to January
2012.
Statistical analysis:
The collected data were organized,
tabulated and statistically analyzed using
SPSS statistical package version 19.
Numerical variables were presented as
range, mean and standard deviation for
categorical variables, the number and
percent distribution was calculated.
Statistical analysis for factors affecting the
total score of knowledge and practice was
done using Mann-Whitney test as the
small sample size for each studied
categories was small and did not guarantee
normal distribution to use the student t-
test. Comparison of mean values for chest
physiotherapy, hygiene and infection
control was performed using paired t-test
as the total cases were treated as one
group. For comparisons of observations of
items related to knowledge or practice
between morning and afternoon shifts,
Wilocxon signed rank test. The level of
significance was adopted at p<0.05.
Limitations of the study:
- Lack of interest and cooperation of
studied nurses.
- Many of nurses were too overloaded with
their work particularly in afternoon shift.
- There were many interruptions during
answering the questionnaires.
- Small sample size to make
generalization.
Results:
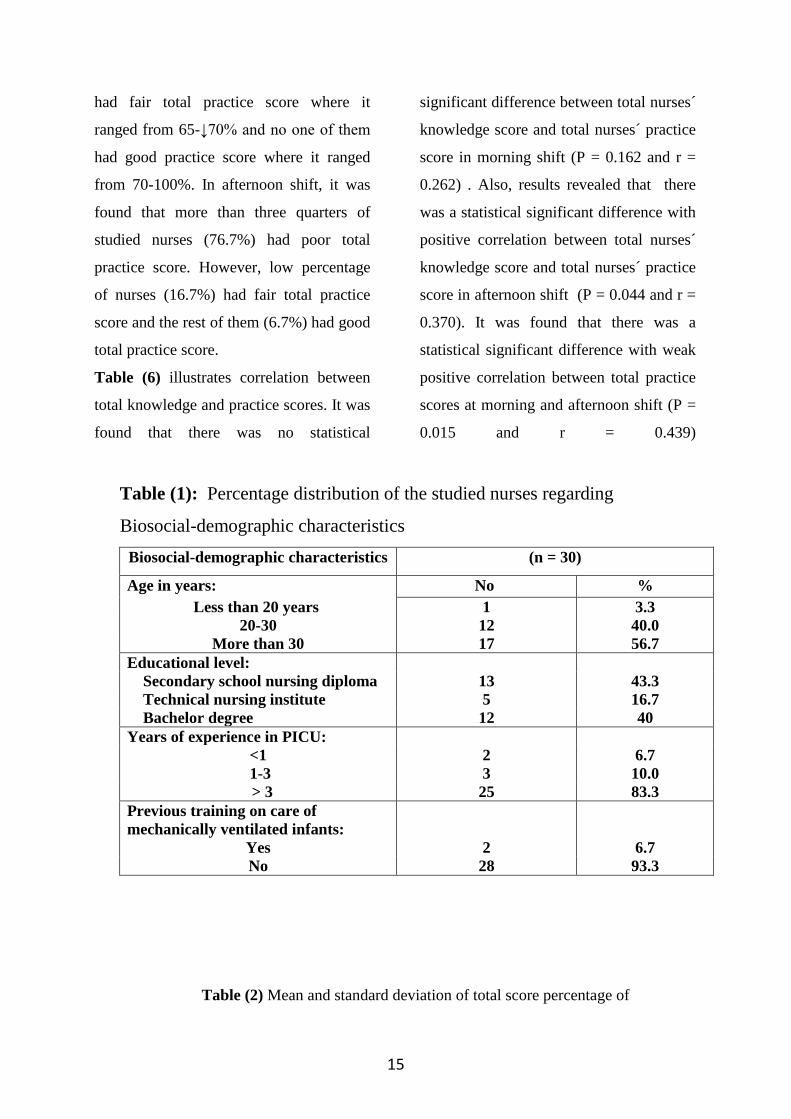
Table (1) presents the percentage
distribution of the studied nurses regarding
biosocial-demographic characteristics. It
was revealed that, more than half of
nurses' ages (56.7%) were more than 30
years while 40% of them were between the
age of 20 and 30 years and the rest of them
(3.3%) were less than 20 years. In relation
to nurses' educational level, 43.3% of
studied nurses had secondary school
nursing diploma while more than one third
of them (40%) had university education
and the rest of them (16.7%) had technical
nursing institute. Regarding years of
experience in pediatric intensive care unit,
it was clear that the majority of nurses
(83.3%) had more than 3 years of
experience. In relation to nurses' previous
14
training on care of mechanically ventilated
infants, it was found that the majority of
them (93.3%) had no previous training.
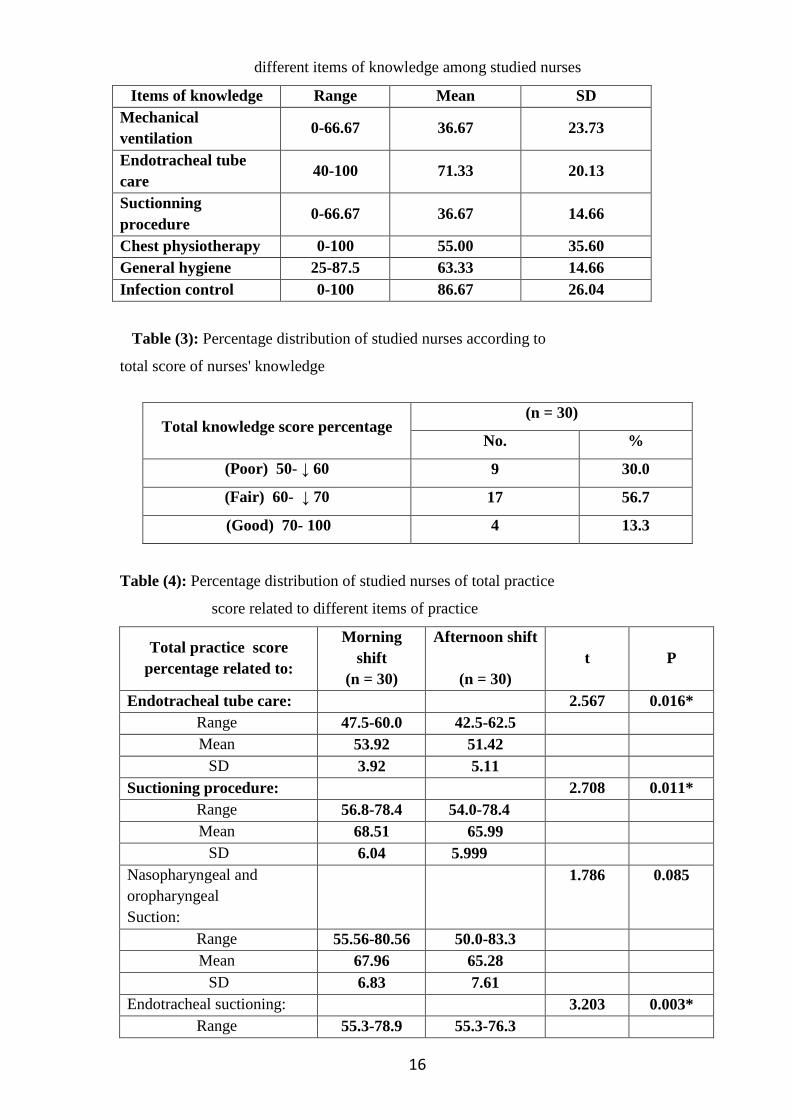
Table (2) shows mean and standard
deviation of total score percentage of
different items of knowledge among
studied nurses. It was observed that the
mean total knowledge score of nurses
regarding infection control was
(86.67±26.04) and ranged between zero
and 100%. Also, the mean total knowledge
score of nurses regarding endotracheal
tube care was (71.33±20.13) and ranged
between 40% and 100%. However, the
mean total knowledge score of nurses
regarding mechanical ventilation and
suctioning procedure was (36.67±23.73)
and ranged between zero and 66.67% for
each.
Table (3) illustrates percentage
distribution of studied nurses according to
total score of nurses' knowledge. Results
revealed that about one third of nurses
(30%) had poor total knowledge score (50-
↓60 %). However, more than half of
studied nurses (56.7%) had fair total
knowledge score (60- ↓70 %) and the rest
of them (13.3%) had good total knowledge
score (70- 100%).
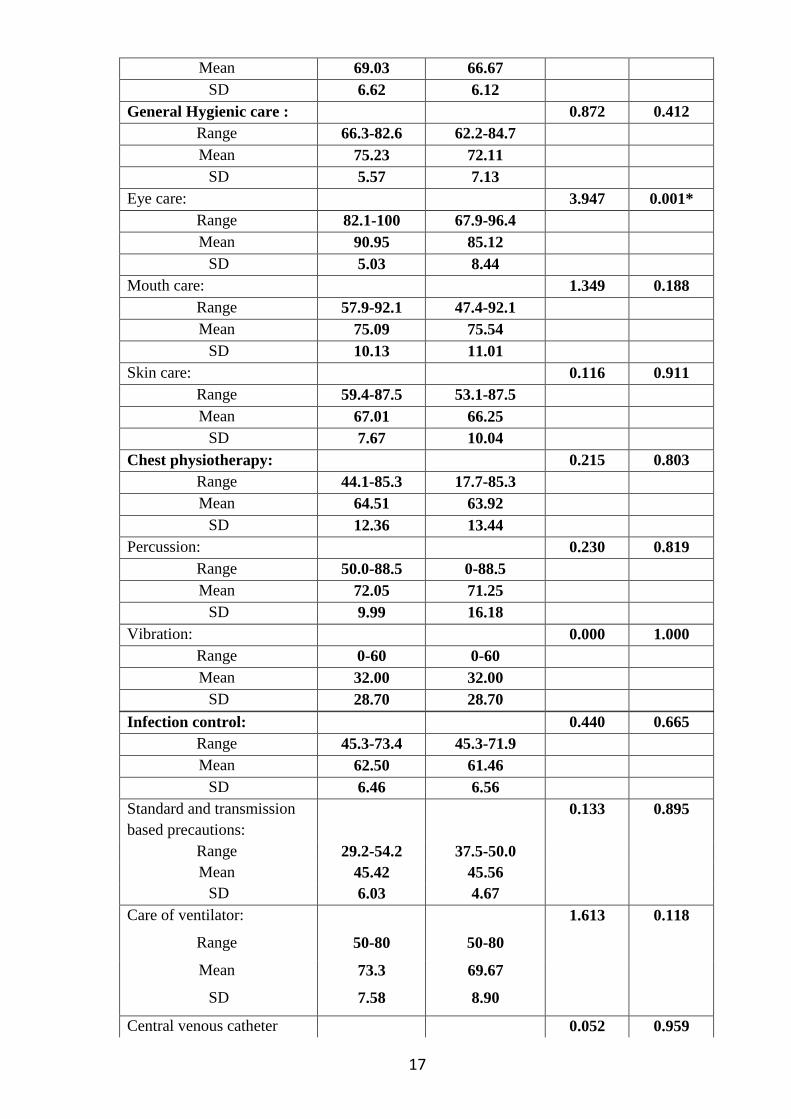
Table (4) illustrates percentage
distribution of studied nurses of total
practice score related to different items of
practice. In relation to general hygienic
care, it was found that the total practice
score percentage of general hygienic care
in the morning shift ranged between 66.3%
and 82.6% while, in the afternoon shift,
the total practice score percentage ranged
between 62.2% and 84.7%. Also, results
revealed that, the mean total practice score
percentage of general hygienic care in
morning shift (75.23±5.57) was more than
that in the afternoon shift (72.11±7.13).
However, in relation to endotracheal tube
care, it was found that the total practice
score percentage of endotracheal tube care
in the morning shift ranged between 47.5%
and 60% while in the afternoon shift, the
total practice score percentage ranged
between 42.5% and 62.5%. Also, results
revealed that the mean total practice score
percentage of endotracheal tube care in
morning shift (53.92±3.92) was more than
that in the afternoon shift (51.42±5.11).
There was a statistical significant
difference between total practice scores of
nurses in relation to "endotracheal tube
care","suctioning procedure",
"endotracheal suctioning" and "eye care"
in morning and afternoon shifts (P =
0.016, 0.011, 0.003, 0.001 respectively) .
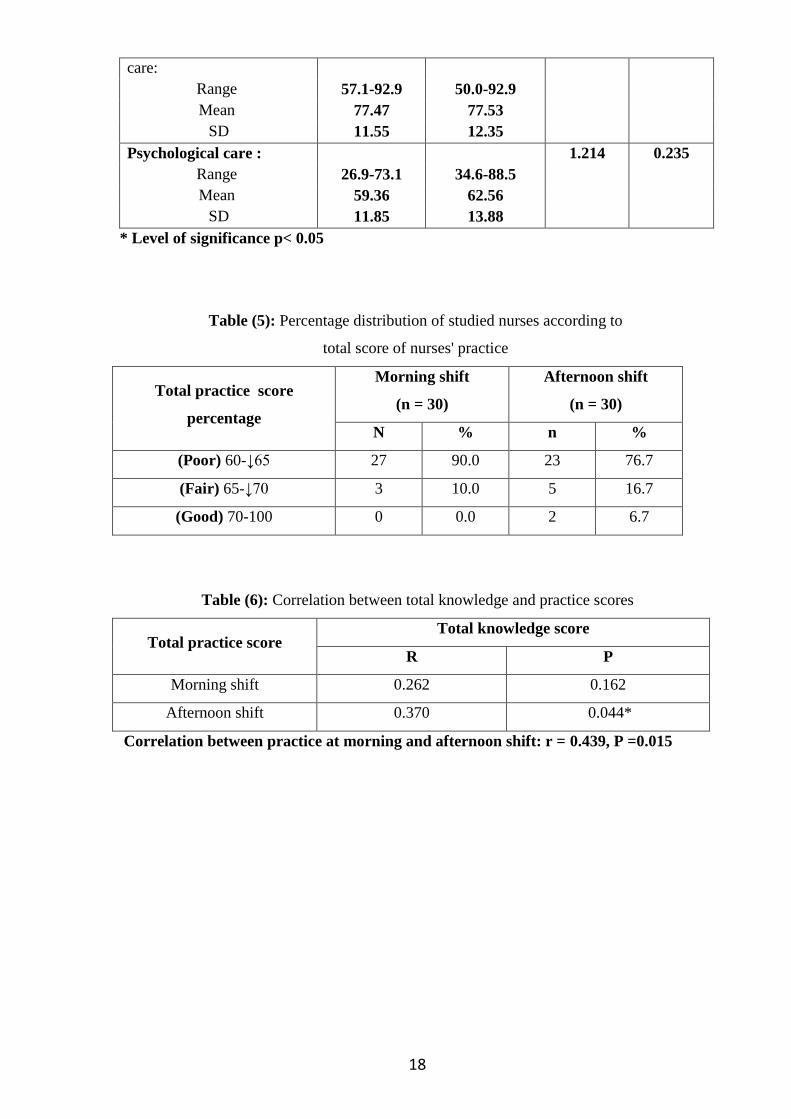
Table (5) illustrates percentage
distribution of studied nurses according to
total score of nurses' practice. In morning
shift, it was found that the majority of
studied nurses (90%) had poor total
practice score where it ranged from 60-
↓65%. Low percentage of nurses (10%)
15
had fair total practice score where it
ranged from 65-↓70% and no one of them
had good practice score where it ranged
from 70-100%. In afternoon shift, it was
found that more than three quarters of
studied nurses (76.7%) had poor total
practice score. However, low percentage
of nurses (16.7%) had fair total practice
score and the rest of them (6.7%) had good
total practice score.
Table (6) illustrates correlation between
total knowledge and practice scores. It was
found that there was no statistical
significant difference between total nurses´
knowledge score and total nurses´ practice
score in morning shift (P = 0.162 and r =
0.262) . Also, results revealed that there
was a statistical significant difference with
positive correlation between total nurses´
knowledge score and total nurses´ practice
score in afternoon shift (P = 0.044 and r =
0.370). It was found that there was a
statistical significant difference with weak
positive correlation between total practice
scores at morning and afternoon shift (P =
0.015 and r = 0.439)
Table (1): Percentage distribution of the studied nurses regarding
Biosocial-demographic characteristics
Biosocial-demographic characteristics (n = 30)
Age in years: No %
Less than 20 years 1 3.3
20-30 12 40.0
More than 30 17 56.7
Educational level:
Secondary school nursing diploma 13 43.3
Technical nursing institute 5 16.7
Bachelor degree 12 40
Years of experience in PICU:
<1 2 6.7
1-3 3 10.0
> 3 25 83.3
Previous training on care of
mechanically ventilated infants:
Yes 2 6.7
No 28 93.3
Table (2) Mean and standard deviation of total score percentage of
16
different items of knowledge among studied nurses
Items of knowledge Range Mean SD
Mechanical
ventilation 0-66.67 36.67 23.73
Endotracheal tube
care 40-100 71.33 20.13
Suctionning
procedure 0-66.67 36.67 14.66
Chest physiotherapy 0-100 55.00 35.60
General hygiene 25-87.5 63.33 14.66
Infection control 0-100 86.67 26.04
Table (3): Percentage distribution of studied nurses according to
total score of nurses' knowledge
Table (4): Percentage distribution of studied nurses of total practice
score related to different items of practice
Total practice score
percentage related to:
Morning
shift
(n = 30)
Afternoon shift
(n = 30)
t P
Endotracheal tube care: 2.567 0.016*
Range 47.5-60.0 42.5-62.5
Mean 53.92 51.42
SD 3.92 5.11
Suctioning procedure: 2.708 0.011*
Range 56.8-78.4 54.0-78.4
Mean 68.51 65.99
SD 6.04 5.999
Nasopharyngeal and
oropharyngeal
Suction:
1.786 0.085
Range 55.56-80.56 50.0-83.3
Mean 67.96 65.28
SD 6.83 7.61
Endotracheal suctioning: 3.203 0.003*
Range 55.3-78.9 55.3-76.3
Total knowledge score percentage (n = 30)
No. %
(Poor) 50- ↓ 60 9 30.0
(Fair) 60- ↓ 70 17 56.7
(Good) 70- 100 4 13.3
17
Mean 69.03 66.67
SD 6.62 6.12
General Hygienic care : 0.872 0.412
Range 66.3-82.6 62.2-84.7
Mean 75.23 72.11
SD 5.57 7.13
Eye care: 3.947 0.001*
Range 82.1-100 67.9-96.4
Mean 90.95 85.12
SD 5.03 8.44
Mouth care: 1.349 0.188
Range 57.9-92.1 47.4-92.1
Mean 75.09 75.54
SD 10.13 11.01
Skin care: 0.116 0.911
Range 59.4-87.5 53.1-87.5
Mean 67.01 66.25
SD 7.67 10.04
Chest physiotherapy: 0.215 0.803
Range 44.1-85.3 17.7-85.3
Mean 64.51 63.92
SD 12.36 13.44
Percussion: 0.230 0.819
Range 50.0-88.5 0-88.5
Mean 72.05 71.25
SD 9.99 16.18
Vibration: 0.000 1.000
Range 0-60 0-60
Mean 32.00 32.00
SD 28.70 28.70
Infection control: 0.440 0.665
Range 45.3-73.4 45.3-71.9
Mean 62.50 61.46
SD 6.46 6.56
Standard and transmission
based precautions:
0.133 0.895
Range 29.2-54.2 37.5-50.0
Mean 45.42 45.56
SD 6.03 4.67
Care of ventilator: 1.613 0.118
Range 50-80 50-80
Mean 73.3 69.67
SD 7.58 8.90
Central venous catheter 0.052 0.959
18
care:
Range 57.1-92.9 50.0-92.9
Mean 77.47 77.53
SD 11.55 12.35
Psychological care : 1.214 0.235
Range 26.9-73.1 34.6-88.5
Mean 59.36 62.56
SD 11.85 13.88
* Level of significance p< 0.05
Table (5): Percentage distribution of studied nurses according to
total score of nurses' practice
Total practice score
percentage
Morning shift
(n = 30)
Afternoon shift
(n = 30)
N % n %
(Poor) 60-↓65 27 90.0 23 76.7
(Fair) 65-↓70 3 10.0 5 16.7
(Good) 70-100 0 0.0 2 6.7
Table (6): Correlation between total knowledge and practice scores
Total practice score Total knowledge score
R P
Morning shift 0.262 0.162
Afternoon shift 0.370 0.044*
Correlation between practice at morning and afternoon shift: r = 0.439, P =0.015

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 19
Discussion:
Critically ill infants in most modern PICU
require a period of mechanical ventilation.
Mechanical ventilation is an important
supportive mode in the care of acutely and
critically ill infants in general. (17- 19)
Nursing
care is one of the essential components of
quality of care given to the infants in
PICU.(20)
Therefore, pediatric nurse must
have keen observation skills, highly trained
and qualified especially when caring for
children who are critically ill. Nurses should
also be educated in the art of recognizing
any changes in children behavior,
interpreting the observation of other and
timing intervention appropriately.(21)
This
study focused on the assessment of nurses'
knowledge about mechanical ventilation and
the quality of nursing interventions related
to the actual nursing care provided to infants
receiving mechanical ventilation which
comprised 5 main items "providing care for
the tube, making suction and chest
physiotherapy, providing general hygienic
care, following infection
control strategies and psychological
support".
The present study revealed that more than
half of nurses' ages were more than 30 years.
40% of nurses had university education. It is
considered a large percentage. So, they were
able to carry out their responsibilities, had a
heightened awareness of resource allocation,
working up on evidence-based practice and
providing advanced quality of care.
Although the majority of nurses had more
than three years of experience in PICU, only
few of them had previous training in
mechanical ventilation. This rendered them
inexperienced in pediatric critical care
practice. Meanwhile, it is stated that, there is
a clear relationship between trained
intensive care staff and quality of patient
management (22)
. Also, it is indicated that,
the agency of Health Care Research Quality
identified that in order to achieve quality of
care; nurses should keep learning and
conducting research rather than being
stagnated in their educational background.
(23)

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 20
Regarding nurses' knowledge in relation to
mechanical ventilation, the present study
indicated that, the mean total knowledge
score of nurses regarding to infection control
was the highest one. While, the mean total
knowledge score of nurses regarding to
mechanical ventilation and suctioning
procedure were the least. This may be
attributed to lack of their basic knowledge
and education programs regarding to
mechanical ventilation and ideal care
provided to mechanically ventilated infants.
These findings contradicted with Carson
(2000) who stated that about three quarters
of nurses had correct knowledge mechanical
ventilation. This could be related to the
difference in educational preparation,
continuous renewal of their license to
practice nursing, and their continuous
exposure to results of most recent researches
related to management of patient on
mechanical ventilation. (24)
Meanwhile,
these findings were consistent with
Mohumed (2005) who mentioned that there
was a gap between the rapid development in
scientific information and slow development
of knowledge of health care providers. (25)
Regarding chest physiotherapy which is
composed of two basic procedures
“percussion and vibration”. It was observed
that some nurses obtained zero the total
practice score in relation to percussion and
vibration procedures. This could be related
to those nurses thought that chest
physiotherapy was composed of percussion
or vibration only, so they provided one of
the two procedures and not both procedures.
Also may be due to unavailability of training
programs regarding to the ideal chest
physiotherapy procedure.
Concerning general hygienic care, the
results of the present study illustrated that
general hygienic care was adequately done
by about three quarters of the study nurses.
This finding was consistent with study
demonstrated by Zahran (1991) who
observed that the general care to the eye,
ear, nose, mouth and skin of the infant was
adequately done by about three quarters of
nurses in NICU of Tanta University
Hospital.(26)
Concerning following of infection control
strategies and specifically universal and
transmission based precautions for infection

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 21
control; it was revealed that these
precautions were adequately done by only
less than half of nurses. These findings of
the present study may be due to insufficient
supplies as masks and gowns in PICU and
lack of supervision and guidance by head
nurses of the unit to nurses to strictly apply
infection control strategies. Also, this could
owe to lack of in-service training programs
related to infection control strategies.
Psychological and emotional support is very
important especially in Pediatric Intensive
Care Unit during stressful situations. The
results of the present work found that more
than one third of the study nurses neglected
or did not offer emotional care to
mechanically ventilated infants. This may be
attributed to increased and continuous
workload that negatively affects the
emotional status of nurses and make
thepsychologically upset as the majority of
them spent long years of work at PICU
without psychological or financial support,
so, they will not be able to give
psychological support adequately to the
infants in Pediatric Intensive Care Unit.
Also, lack of time of the nursing staff and
overlapping of nursing activities in intensive
care unit, would make them focus mainly on
major patient issues and would not be able
to attend to minor issues as emotional
support. Furthermore, the majority of infants
were sedated most of the time to prevent
fighting the ventilator.
This finding was consistent with the finding
of Martensson et al (2004) who stated that
the majority of nurses in intensive care unit
neglect the patient’s verbal and non-verbal
communication, so the critically ill patient
may experience feeling of anger, sadness,
negative emotion and depression. It was
stated that the role of the critical care nurse
is to consider the patient's verbal and non-
verbal communication ability. It is necessary
for critical care nurse to help the patient to
feel trust and be secure when receiving
mechanical ventilation. (27)
Although more than half of studied nurses
had fair total knowledge score, the majority
of studied nurses had poor total practice
score. This finding means that the nurses did
not apply their knowledge in providing
adequate nursing care to critically ill infants.
These findings may be attributed to that all

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 22
nurses follow the hospital policy in
providing nursing care to mechanically
ventilated infants and not to follow the
standardized nursing care plan. Also, the
newly recruited nurses ask the old nurse in
the unit when they cannot perform any
procedure instead of returning to the ideal
nursing care, or may be due to lack of
resources, equipments and supplies needed
to provide standardized nursing care.
As regards of nursing performance, the
present study revealed that the nursing care
provided to infants receiving mechanical
ventilation was poor and below the accepted
level of what should have been done. This
may be due to lack of motivation, hospital
facilities, resources and lack of training
courses that enable nurses to perform
standardized nursing care. It was indicated
that the agency of Health Care Research
Quality identified that in order to achieve
quality of care; nurses should keep learning,
training and conducting research rather than
being stagnated in their educational
background (23)
.
Conclusion
Based up on the results of this study, it
could be concluded that nurses' knowledge
and practice were inadequate to provide
ideal care for mechanically ventilated
infants. It was found that more than half of
the studied nurses had fair knowledge in
relation to their educational level and the
majority of them had poor practice in
relation to the their educational level and
years of experience. This may be attributed
to lack of supervision, and lack of
motivation, resources and facilities that
affect nurses' knowledge and performance.
Recommendations
Based on the findings of the present study,
the following can be recommended:
In-service training programs and
workshops should be conducted
periodically and regularly for nurses
working in Pediatric Intensive Care
Unit to improve the nurses' knowledge
and performance about nursing care of
mechanically ventilated infants.
Protocol of care should be started on the
admission of the infant to the unit.
Newly recruited nurses in Pediatric
Intensive Care Unit are better exposed
to a sort of orientation period. During

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 23
this period new nurses have to:
Know about their expected roles.
Learn about the common infant's
problems and needs.
Complement for any deficiencies in
basic knowledge and skills.
- Provision of handouts of up- to- date
guidelines regarding standardized nursing
care of mechanically ventilated infants.
- Standardized nursing care for mechanically
ventilated infants should be prepared by
professional specialized adept nursing
staff and kept in the unit.
References
1. Hanaa A. Quality of Nursing Interventions
While Managing Children Receiving
Mechanical Ventilation, Unpublished
Master Thesis in Faculty of Nursing.
Menouphiya University 2008; 1-4
2. Anna U , Jolanta S , Ivelisse G.
Mechanical Ventilation , 3rd
ed, New
York: Raven Press Co, 2010; 11-12
3. John P, Eric C , Ann R. Manual of
Neonatal Care, 6th
ed, Philadelphia:
Lippincott Co, 2004; 331
4. Genel L. Historical Perspective on the
Development of Mechanical Ventilation,
2nd
ed, New York: McGraw-Hill Co, 2006;
978
5. Marvin K. Mechanical ventilation of
infants, Journal of American Science 2011;
7(12): 531-541
6. Witta K. New techniques for weaning
difficult patient from mechanical
ventilation. Clinical issue & critical care
nursing Journal, 1995; 1(2): 260.
7. Gehan A. Assessment of Nurses
Knowledge and Performance in Relation
to Weaning and Extubation of Patient with
Mechanical Ventilation, Unpublished
Master Thesis in Faculty of Nursing. Tanta
University 2005; 1-2
8. Clochesy J, Breu C, Cardin S, Whillaker A
, Rudy E. Critical Care Nursing, 2nd
ed,
Philadelphia: WB Saunders Co, 1996; 630-
47
9. Smeltzer S, Bare B. Text Book of Medical
Surgical Nursing, 9th
ed, Philadelphia: JB
Lippincott Co, 2000; 466-467.
10. Angus D, Griffin M, Clermont G, Clark R.
Epidemiology of neonatal respiratory
failure in the USA: projections from
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 24
California and New York. Am Journal
Respir Crit Care Med 2001; 164(7):1154–
1160
11. Merck S, Dohme C. Overview of
mechanical ventilation: Respiratory failure
and mechanical ventilation, 2009- 2010;
available at
http://www.merckmanuals.com
12. Tanıl K, Aslı K, Zahide Y, Emel D , Erdal
E. Mechanical ventilation in children,
Turkish Journal of Pediatrics
2006;48(4):323-327
13. Akgul S and Akyoluc N. Effect of normal
saline on endotracheal suctioning, Journal
clinical nurse, 2004; 11(6): 826-30
14. Institue of Medicine. Committee on quality
health care in America crossing the quality
chasm: A new health system For the 21 St
Centuries Washing DC: The National
Academies Press 2001
15. Smeltzer S, Bare B. Text Book of Medical
Surgical Nursing, 7th
ed., Philadelphia: JB
Lippincott Co 2004; 200-222.
16. Walls R, Murphy M , Luten R. Manual of
Emergency Airway Management, 3rd
ed,
Philadelphia: Lippincott Williams and
Wilkins Co, 2008; 552-565
17. Palmeri J. Developing a comprehensive
preoperative nursing documentation form,
AORN J, 2005; 44(18):77.
18. Ingersoll G. Measurement in mechanical
ventilation weaning research, The Online J
Known Synthesis Nurs, 1995; 2(12), 51.
19. Chase S. The research basis for weaning
from mechanical ventilation, The Online J
Know Synthesis Nurs, 1994; 1(7) 1-10.
20. Meade M, Guyatt G,Cook D. Weaning
from mechanical ventilation: The evidence
from clinical research, Respir Care J, 2001;
46(12): 1408-15.
21. Chinn P and Leitch C. Child Health
Maintenance, A guide to Clinical
Assessment, 6th ed., London, C.V. Mosby
Co., 2000; 28-32.
22. Wong D , Hockenberry M. Wong's
Nursing Care of Infants, 7th
ed, London,
Mosby Co., 2003.
23. Backmann U, Gillies D. Factors associated
with re-intubation in intensive care: An
analysis of causes and outcomes, Chest J,
2001; 120(2): 538-42.
24. Carson S, Ely E, Govert J, Garrett J, Hall
J. Effectiveness of medical residents,
Education in mechanical ventilation,
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 25
AHRCCM Articles in Press, 2000;(24)13,
45-8.
25. Mohumed R. Role of the nurse in counseling
parents of children with hereditary diseases,
published thesis, Faculty of Nursing,
Menoufiya University, 2005; 98.
26. Zahran S. Study of the organization and
utilization of the neonatal intensive care unit
in Tanta University Hospital, Unpublished
Master Thesis in Faculty of Nursing,
Alexandria University, 1991
27. Martensson I, Fridlund B. Patient's reports
of health care practitioner interventions that
are related to communication during
mechanical ventilation, Heart& Lung J,
2004; 33(5): 308-20.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 26
Infection among Women using Intrauterine Devices and Oral Contraceptives
Aida abd El-Razek,
Assistant Professor of Maternal and newborn Health Nursing
Faculty of Nursing, Menoufyia University
Abstract
The study was to evaluate the relationship between vaginal douching practices and
genitourinary infection in women, aged 18-49, who use an intrauterine contraceptive device
(IUCD) or oral contraceptives (OCP). This study was planned and applied as a descriptive cross-
sectional study. The study was conducted at Mother and Child Health and Family Planning
Center of El-Basher Hospital Amman Jordon. The study was conducted with 185 consenting
women (90 using OCP, 90 using IUCD). Since the number of women using condoms was
minimal, these were excluded from the study. 10 months at 2009 over the period of the study. No
inclusion criteria were taken into consideration aside from age, having used the same method in
the last 4 years, and not menstruating at the time samples were to be taken. It was found that
women taking OCP who practiced vaginal douching (VD) had higher ratios of bacteria growth in
the urine compared to women with IUCD. While there was a significant relationship seen
between the method used and the urine culture results (Χ2=5.045 df =1 p=0.01), no relationship
was observed in terms of the vaginal culture (Χ2=0.631 df=1 p=0.264). The conclusion of the
study was that the development of genitourinary infection during the use of OCP or IUCD was
associated more with lack of proper hygiene rather than with the practice of vaginal douching.
Keywords: Genitourinary infection, Intrauterine contraceptive device, Oral
contraceptive, Vaginal douching

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 27
Introduction
Vaginal douching (VD) is an old and
traditional practice that is carried out for
intra-vaginal cleansing or treatment, using
the fingers and/or substances to clean and
rinse out the vagina [1, 2]
. VD is a
widespread practice among women. Woman
practice VD generally for vaginal
cleanliness after menstruation or sex, as a
contraceptive measure, or because of
hygienic beliefs [3]
. According to hygienic
belief, body secretions flowing from or
remaining in the vagina preclude the
observance of hygienic beliefs.
Menstruating women, for example, cannot
perform the ritual prayer or read the Koran
[4]. Most women will clean the vaginal area
after sexual intercourse, either using their
fingers or by douching, removing seminal
fluid from the vagina as an act of
purification [4,5]
. Women use many different
substances when practicing VD. Among the
most frequently encountered of these are
soap, perfumes, and vinegar [6, 8]
. In
addition, some studies have reported that
women are not aware of the harmful effects
of VD [7, 8, 9]
. When the habit of washing out
the genital area with water after going to the
toilet is added to the practice of VD, the risk
of infection becomes more alarming [5]
. It
has been found that one-fifth of women
practicing VD do so after going to the
toilet.10 Women who wash the anal area
after defecation are likely to perform VD
with their contaminated hands. This causes
the transmission of many pathogenic
microorganisms into the vagina, making the
area susceptible to the development of many
health issues [11, 12]
. VD disrupts the balance
of the normal vaginal flora and prepares a
foundation for infection [10]
. The risk of
genitourinary infection increases when
women's poor hygienic habits are added to
this picture. It has been determined in
research that methods of contraception can
be trigger factors for infection. It is
recognized that among the different
contraceptive methods, the IUCD is the
method that is more likely to increase
susceptibility to genitourinary infections [13,
14]. IUCDs may change the nature of the
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 28
vaginal flora and cause an increase of
anaerobic bacteria [15, 16]
. Besides this
shortcoming, it has also been reported that a
lack of hygienic conditions during the
insertion of the IUCD and deficiencies in
information concerning its use are also
infection-triggering factors [17, 18]
.
Significant of the study
According to the reports of Jordon
Population and Health Research (JNSA), a
significant increase was seen in the use of
IUCDs as an effective method of
contraception between the years 2003-2008,
and it is striking to note that women with
IUCDs are more educated than those that
take OCPs [21]
. study reported that IUCD's
were the primary and preferred effective
method; condoms were the second
preference while taking OCPs was third [21]
.
The results of the present study are
consistent with this finding.
Studies have shown that deficiencies
in hygiene when using the various
contraceptive methods are more likely to
bring about genitourinary infection [15]
.
There is no study in the literature, however,
that examines the association between the
use of OCP and genitourinary infection.
Some studies have been reported that the
effect of OCP use on the vaginal flora is
minimal [14, 17]
. It has been reported, on the
other hand, that the estrogen contained in
OCP facilitates the population of
uropathogens in the vaginal and urogenital
cells, preparing a suitable environment for
the growth of microorganisms [15]
. In
addition to these factors, personal habits of
the individual during the use of OCPs (anal
sex, poor hygiene, low water consumption,
etc.) also trigger genitourinary infection [16]
.
The aim of the study
Evaluate the relationship between
vaginal douching practices and
genitourinary infection in women, aged 18-
49, who use an intrauterine contraceptive
device (IUCD) or oral contraceptives (OCP).
MATERIALS AND METHOD
Research design:
This study was planned and applied
as a descriptive cross-sectional study
Research Setting:
The study was conducted at Mother
and Child Health and Family Planning

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 29
Center of El-Basher Hospital Amman
Jordon.
Subjects of the study
Sample size
El-Basher Hospitals, Family
planning services in Jordon are provided by
three separate groups of institutions. These
are private and state hospitals, family
physicians, and the Child Health and Family
Planning Centers (CHFPC).
The CHFPC in the city center accepts a
monthly average of 60 women for IUD
checkups, 50 women for IUCD insertion, 70
women for OCP prescriptions, and 15
women to obtain condoms. 10 months at
2009 over the period of the study, 195
women applied to the Center and of these,
15 were using condoms. The study was
conducted with 185 consenting women (90
using OCP, 90 using IUCD). Since the
number of women using condoms was
minimal, these were excluded from the
study. No inclusion criteria were taken into
consideration aside from age, having used
the same method in the last 4 years, and not
menstruating at the time samples were to be
taken.
Type of sampleA
Convenience sample of 180 using OCP, 90
using IUCD was conveniently selected to
achieve the aim of the study.
Tools for data collection:
The data was collected by using pen-
and-paper self-report forms which included
the following: a socio-demographic data
collection form, a questionnaire inquiring
into vaginal douching behavior and data on
urine culture and vaginal culture results
based on the specimens obtained from the
women.
The data collection form consisted of
15 questions prepared by the researchers to
record the socio-demographic characteristics
of the participants and the questionnaire was
based on 13 questions from the literature 12
that were developed to inquire about
descriptive characteristics related to vaginal
douching and genital hygiene. In addition,
specimens were obtained from the women
for vaginal cultures and urine cultures.
These samples were sent to the El-Basher

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 30
Technical University Microbiology and
Pathology Labs within 1 hour.
Socio-demographic Questionnaire
This consisted of questions
developed by the researcher based on the
literature. The questions concerned
the women's ages, their work, educational
level, social security status, monthly income,
number of children and births, the duration
the method had been used and similar
information
Vaginal Douching and General Hygiene
Questionnaire
This consisted of questions about vaginal
douching practices, the method used, the
reason for practicing VD, from whom the
woman had heard about vaginal douching,
the material used in VD, how frequently it
was practiced, how many times the woman
has sex in a week, and whether or not she
had any knowledge about the harmful
effects of VD.
Ethical Considerations:
The study was carried out with co-operation
of different levels of authority. An official
letter was sent from the Dean of the Faculty
of Nursing in Philadelphia University to the
directors of El-Basher Hospitals These are
private and state hospitals, family
physicians, and the Child Health and Family
Planning Centers (CHFPC) explaining the
aim of the study and the time of data
collection seeking his permission for data
collection. An official permission through
written letters clarifying the purpose and
sitting of the study was obtained from the
directors of El-Basher Hospital As an
approval for data collection. A written
informed consent was obtained from the
participants after explaining the purposes of
the study, which include: no harm was
occurring to participant, do not contradict
with the cultural, traditional and religious
issues, human rights were reserved, data was
confidential and used mainly for the purpose
of the research and each subjects was free to
withdraw from the study at any time.
Method
Data collection Procedure:
Development of tools for data
collection after reviewing the related
literature the tools was revised for
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 31
content validity by 5 experts in the
field.
The women's was selected by A
convenient sample was used
according to the mentioned criteria.
The data were collected through a
period of 10 months at 2009. Three
days per week starting at 9am to
2pm. The researcher introduced
herself to the women and obtained
their consent to be recruited in the
study after explaining the aim of the
study.
Each woman was interviewed
individually by the researcher.
The average time for filling each
sheet was about 15 minutes
depending on the response of the
women. Consent was obtained from
each women and the interviewing
questionnaire was explained to each
women.
After that, the researcher assessed
Procedure for Obtaining Sterile
Urine Specimens. A sterile container
(red-screw-capped culture container)
was used as a urine culture container.
- Instructions as to how the culture
should be taken were given to the
women consenting to the study, as
follows: “Thoroughly wipe the outer
part of the urinary tract with the
disinfectant/antiseptic wipe before
taking the urine sample; dry the area
with the sterile gauze that's been
given to you; after discharging the
first few drops of urine, collect the
middle of the flow in the sterile
container. Do not allow the urine
container to touch anything and do
not fill up the container to the brim.”
[20].
The lids were then placed on the
urine containers, on which the names
of the patients were written; the
specimens were taken to the
laboratory in a short time by the
researcher. The samples were
evaluated after their “S”-shaped
inoculation on to blood
EMB/McConkey agar plates [20]
.
Procedure for Obtaining Vaginal
Culture: Glass culture tubes equipped with
cotton-tipped sterile swabs used only for this

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 32
purpose were employed to gather specimens.
The small-tipped sterile swab was swept
across the vaginal wall and the specimen
was placed in a closed container with the
patient's name written on it. A Nugent score
assessment of the samples was made [20]
.
Limitation of the study:
Microbiology and pathology laboratories
container is not available for sometime.
Not funded this study by the University
Research, researcher finds it difficult to test
Statistical Analysis
The Statistical Program for the Social
Sciences, version 15.0 (SPSS 15.0) was used
for data analysis. Percentages and averages
were also calculated, the Chi-square test and
t- test were performed for the statistical
analysis. The level of statistical significance
was set at p<0.05.
The logistic regression analysis model to
determine which factors affected bacterial
growth in the urine and vaginal culture. The
enter method was used in the logistic
regression analysis
RESULTS
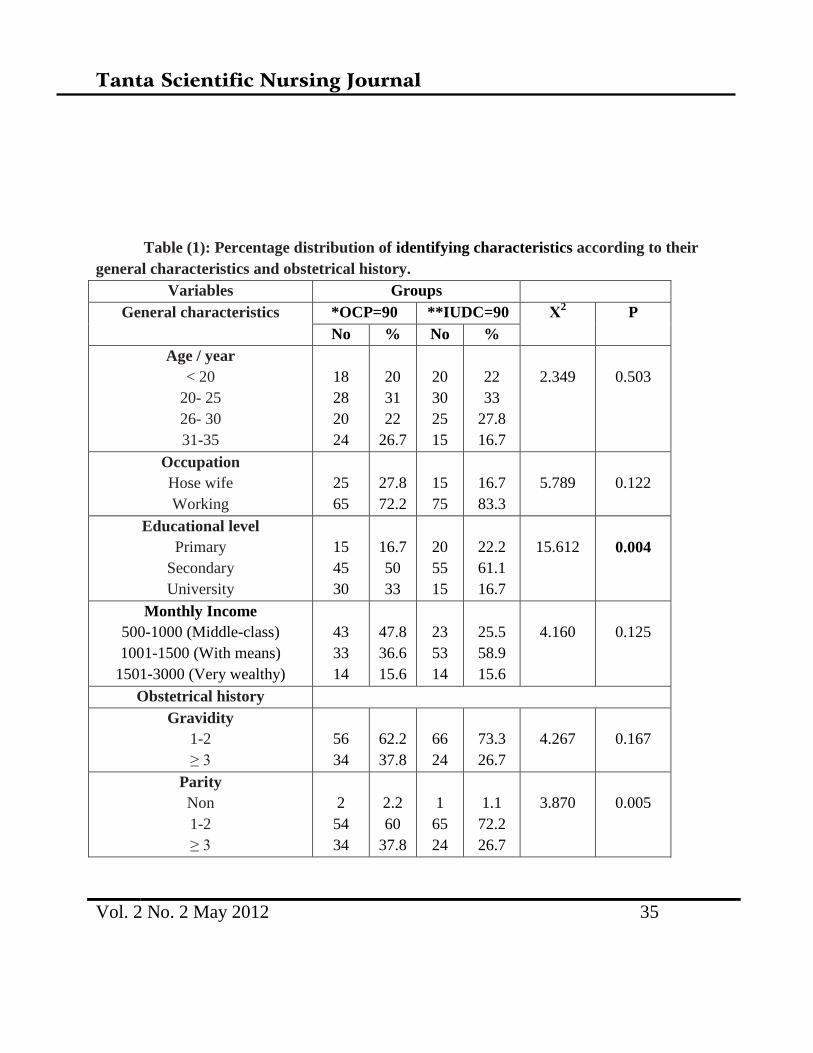
The women's age group, their working
status, educational level, social security
status and income levels are shown in Table
1. As can be seen in Table 1, no statistical
difference was observed between the two
groups except variable of educational level.
The women taking OCPs made up 70% of
the group, and those using IUCD's, 81.1%.
In the statistical analysis, there was no
significant difference between the two
groups in terms of performing vaginal
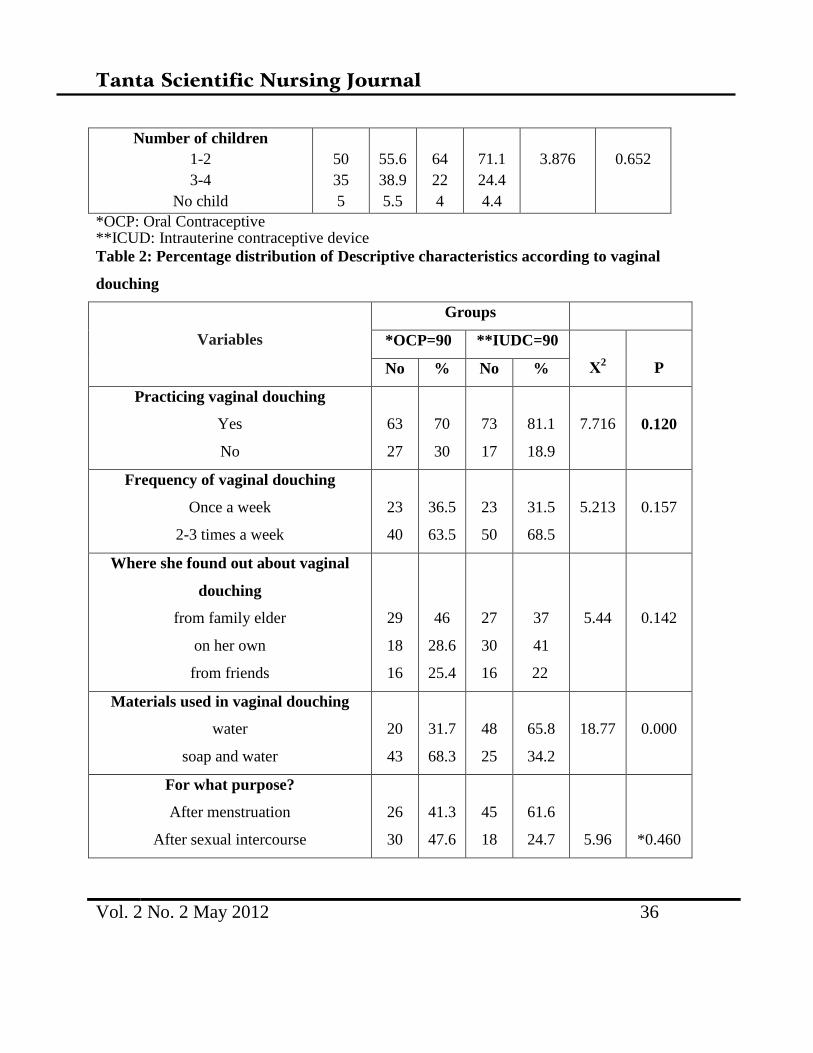
douching (Χ2=7.716 p=0.120) (Table 2). It
was found that 63.5% of the women
practicing vaginal douching who were
taking OCPs, 68.5 %of the women using
IUDs said that they practiced VD 2-3 times
a week; 41% of the women using IUCDs
said that they had made this decision on
their own; 46 % of the women using OCPs
said they had heard about VD from their
elders; 68.3% of the women taking OCPs
said that they performed vaginal douching
with soap and water, and 65.8% of the
women with IUDs said that they performed
vaginal douching with water; of the women
using OCPs, 47.6 % said they performed
VD usually after sexual intercourse; 61.6 %

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 33
of the women with IUCDs said they
performed vaginal douching after
menstruation; 60.3% of the women taking
OCPs and 65.8% of the women using
IUCDs stated that they practiced vaginal
douching regularly. Of the women taking
OCPs, 71.4%, and 68.5% of the women
using IUCDs said they didn't think VD was
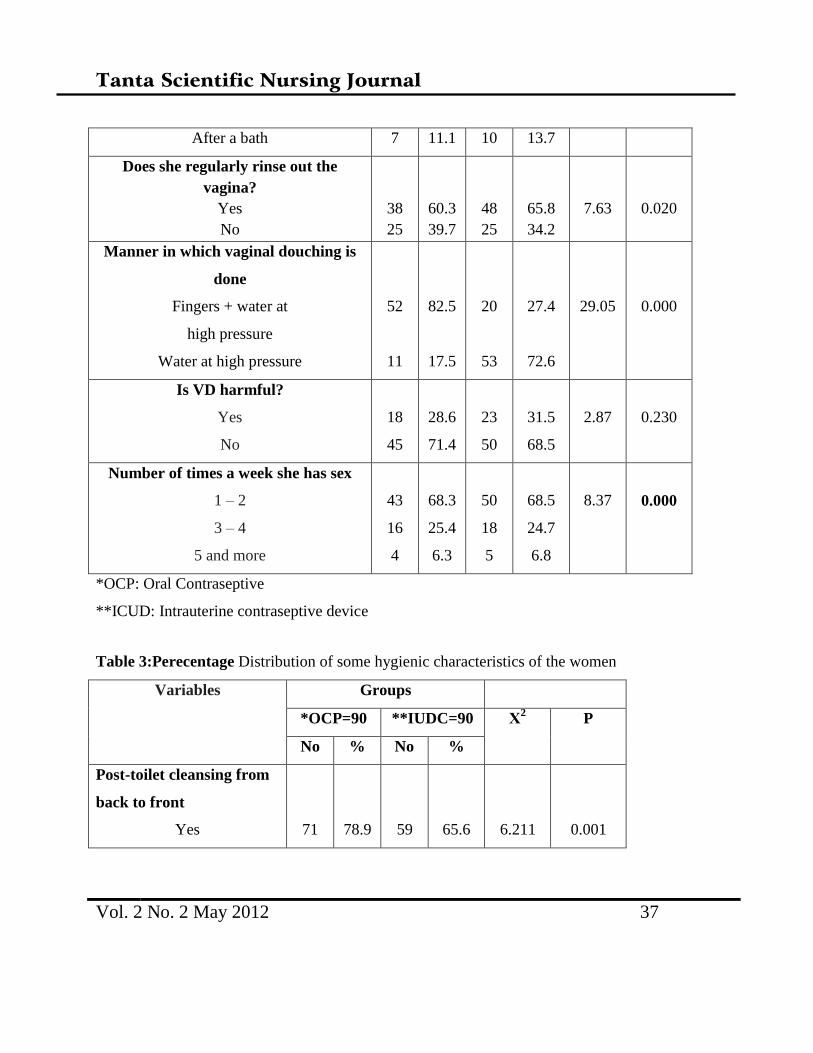
harmful (Table 2). There were significant
differences between the groups in terms of
the materials used regularly, the method of
VD and the frequency of sexual intercourse
(Χ2=18.77 p=0.000; Χ
2=7.35 p=0.020;
Χ2=29.02 p=0.000; Χ
2=8.37 p=0.000,
respectively).
Among the group taking OCPs, 78.9%, and
65.6% of the IUCD group were rinsing off
their genital area from back to front. A
statistical difference was found in this factor
between the groups (Χ2=6.211 p=0.001)
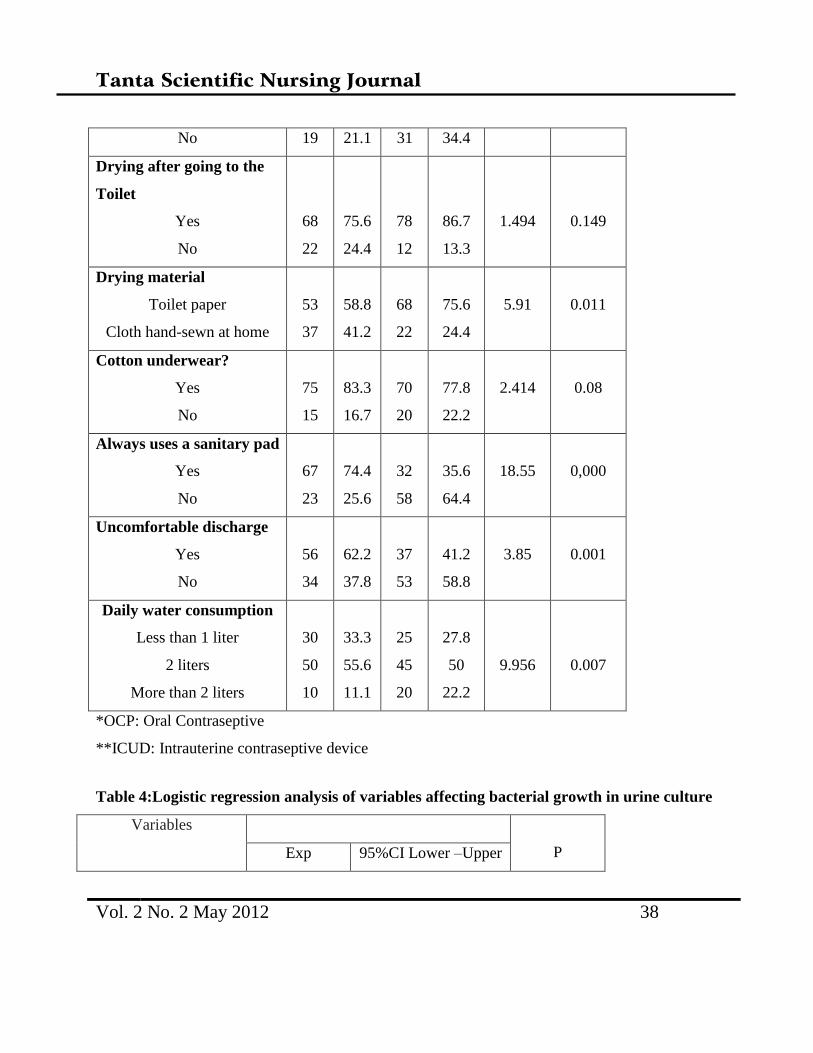
(Table 3). The two groups also exhibited
significant differences in terms of the
material used for drying off, continuously
using a sanitary pad, and the existence of a
disagreeable secretion (Χ2=5.91 p=0.011;
Χ2=18.55 p=0.000; Χ
2=2.188 p=0.000,
respectively) (Table 3). It was noted that
75.6 % of the OCP group dried off their
genitals after going to the toilet while this
percentage was 86.7% in the IUCD group.
There was no significant difference found
between the two groups (Χ2=1.494
p=0.149). Looking into whether the women
wore cotton underwear, it was seen that 83.3
% of the OCP group and 77.8% of the IUCD
group wore cotton underwear; no significant
difference was found between the two
groups (Χ2=2.414 p=0.08) (Table 3). As
regards the practice of using sanitary
protection all the time, it was revealed that
74.4 % of the OCP women and 35.6% of the
IUCD group used sanitary pads daily. A
significant difference was found between the
two groups (Χ2=18.55 p=0.00) (Table 3).
Daily water consumption of less than 2 liters
was 55.6% in the OCP group and 50. % in
the IUCD group there was a significant
difference found between the two groups in
terms of this factor (Χ2=9.956 p=0.007).
Tabe 4: While bacterial growth was
observed in the urine culture results of
53.1% of the women taking COCs, bacterial
growth was found in 35.7% of the women
with IUCDs. Escherichia coli was the
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 34
microorganism predominantly found in the
urine culture of women taking OCPs,while
Enterobacteria species were more
pronounced in women with IUCDs. The
results of the vaginal culture showed that
66.7% of the women using OCP and 60.7%
of the women using IUCD's did not display
any microbial growth. In the vaginal culture,
both groups of women displayed a
predominant growth of the microorganism
Candida albicans. While there was a
significant difference between the two
groups in the urine culture results (Χ2=5.045
p=0.01), no difference was discovered in the
vaginal culture (Χ22=0.631 p=0.264).
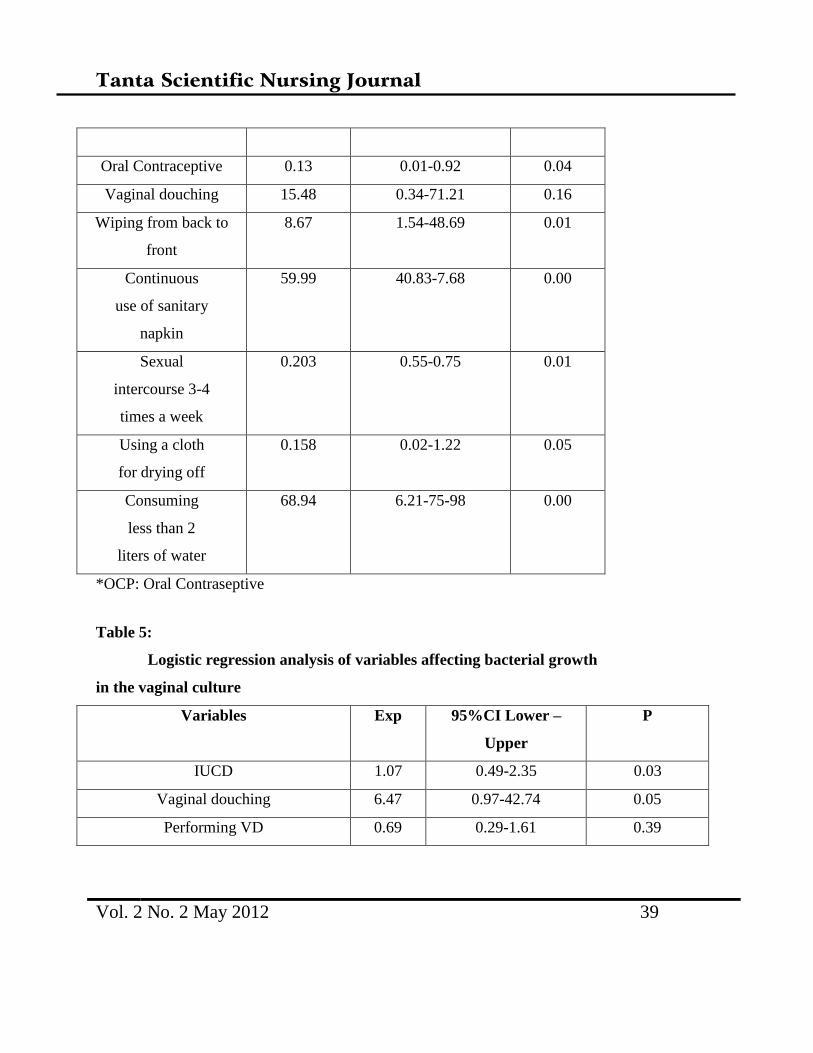
The results of the logistic regression
analysis used to determine the factors that
had an effect on the urine and vaginal
culture are shown in Tables 4 and 5. As can
be seen in Table 4, the use of OCPs (Exp:
0.12, 95% CI 0.01-0.91), wiping from back
to front (Exp: 8.66. 95% CI 1.54-48.95),
continuous use of a sanitary pad (Exp:
59.99, 95% CI 40.83-7.68), low daily water
consumption (Exp: 68.94% CI 6.21-75.98),
engaging in sexual intercourse 3-4 times a
week (Exp: 0.203, 95% CI 0.55-0.75), using
a piece of cloth hand-sewn at home as
drying material (Exp: 0.158, 95% CI 0.02-
1.22) were seen to be independent factors
that had on an effect on bacterial growth in
the urine culture, while the use of IUCDs
(Exp: 1.07, 95% CI 0.49–2.35) and
performing vaginal douching (Exp: 6.47,
95% CI 0,97-42.74) were independent
factors observed to have an effect on
bacterial growth in the vaginal culture.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 35
Table (1): Percentage distribution of identifying characteristics according to their
general characteristics and obstetrical history.
Variables Groups
General characteristics *OCP=90 **IUDC=90 Χ2
P
No % No %
Age / year
< 20
20- 25
26- 30
31-35
18
28
20
24
20
31
22
26.7
20
30
25
15
22
33
27.8
16.7
2.349
0.503
Occupation
Hose wife
Working
25
65
27.8
72.2
15
75
16.7
83.3
5.789
0.122
Educational level
Primary
Secondary
University
15
45
30
16.7
50
33
20
55
15
22.2
61.1
16.7
15.612
0.004
Monthly Income
500-1000 (Middle-class)
1001-1500 (With means)
1501-3000 (Very wealthy)
43
33
14
47.8
36.6
15.6
23
53
14
25.5
58.9
15.6
4.160
0.125
Obstetrical history
Gravidity
1-2
≥ 3
56
34
62.2
37.8
66
24
73.3
26.7
4.267
0.167
Parity
Non
1-2
≥ 3
2
54
34
2.2
60
37.8
1
65
24
1.1
72.2
26.7
3.870
0.005
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 36
Number of children
1-2
3-4
No child
50
35
5
55.6
38.9
5.5
64
22
4
71.1
24.4
4.4
3.876
0.652
*OCP: Oral Contraceptive **ICUD: Intrauterine contraceptive device
Table 2: Percentage distribution of Descriptive characteristics according to vaginal
douching
Variables
Groups
*OCP=90 **IUDC=90
Χ2
P No % No %
Practicing vaginal douching
Yes
No
63
27
70
30
73
17
81.1
18.9
7.716
0.120
Frequency of vaginal douching
Once a week
2-3 times a week
23
40
36.5
63.5
23
50
31.5
68.5
5.213
0.157
Where she found out about vaginal
douching
from family elder
on her own
from friends
29
18
16
46
28.6
25.4
27
30
16
37
41
22
5.44
0.142
Materials used in vaginal douching
water
soap and water
20
43
31.7
68.3
48
25
65.8
34.2
18.77
0.000
For what purpose?
After menstruation
After sexual intercourse
26
30
41.3
47.6
45
18
61.6
24.7
5.96
*0.460
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 37
After a bath 7 11.1 10 13.7
Does she regularly rinse out the
vagina?
Yes
No
38
25
60.3
39.7
48
25
65.8
34.2
7.63
0.020
Manner in which vaginal douching is
done
Fingers + water at
high pressure
Water at high pressure
52
11
82.5
17.5
20
53
27.4
72.6
29.05
0.000
Is VD harmful?
Yes
No
18
45
28.6
71.4
23
50
31.5
68.5
2.87
0.230
Number of times a week she has sex
1 – 2
3 – 4
5 and more
43
16
4
68.3
25.4
6.3
50
18
5
68.5
24.7
6.8
8.37
0.000
*OCP: Oral Contraseptive
**ICUD: Intrauterine contraseptive device
Table 3:Perecentage Distribution of some hygienic characteristics of the women
Variables Groups
*OCP=90 **IUDC=90 Χ2
P
No % No %
Post-toilet cleansing from
back to front
Yes
71
78.9
59
65.6
6.211
0.001
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 38
No 19 21.1 31 34.4
Drying after going to the
Toilet
Yes
No
68
22
75.6
24.4
78
12
86.7
13.3
1.494
0.149
Drying material
Toilet paper
Cloth hand-sewn at home
53
37
58.8
41.2
68
22
75.6
24.4
5.91
0.011
Cotton underwear?
Yes
No
75
15
83.3
16.7
70
20
77.8
22.2
2.414
0.08
Always uses a sanitary pad
Yes
No
67
23
74.4
25.6
32
58
35.6
64.4
18.55
0,000
Uncomfortable discharge
Yes
No
56
34
62.2
37.8
37
53
41.2
58.8
3.85
0.001
Daily water consumption
Less than 1 liter
2 liters
More than 2 liters
30
50
10
33.3
55.6
11.1
25
45
20
27.8
50
22.2
9.956
0.007
*OCP: Oral Contraseptive
**ICUD: Intrauterine contraseptive device
Table 4:Logistic regression analysis of variables affecting bacterial growth in urine culture
Variables
P Exp 95%CI Lower –Upper
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 39
Oral Contraceptive 0.13 0.01-0.92 0.04
Vaginal douching 15.48 0.34-71.21 0.16
Wiping from back to
front
8.67 1.54-48.69 0.01
Continuous
use of sanitary
napkin
59.99 40.83-7.68 0.00
Sexual
intercourse 3-4
times a week
0.203 0.55-0.75 0.01
Using a cloth
for drying off
0.158 0.02-1.22 0.05
Consuming
less than 2
liters of water
68.94 6.21-75-98 0.00
*OCP: Oral Contraseptive
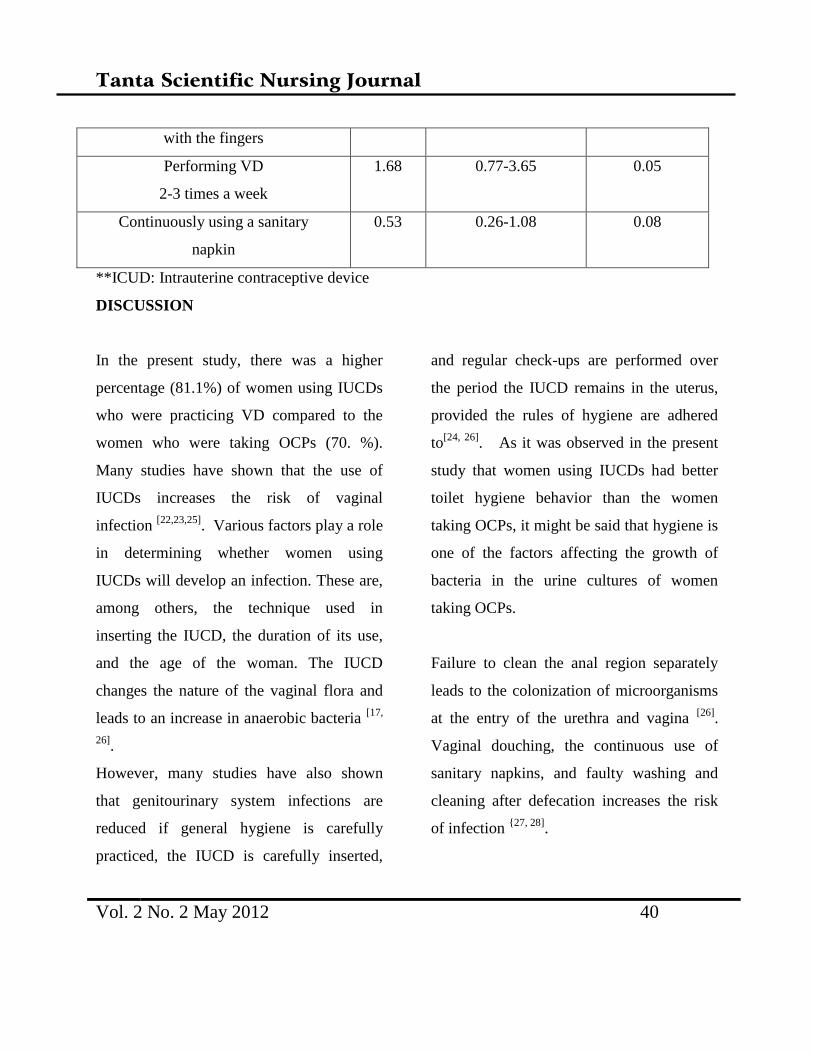
Table 5:
Logistic regression analysis of variables affecting bacterial growth
in the vaginal culture
Variables Exp 95%CI Lower –
Upper
P
IUCD 1.07 0.49-2.35 0.03
Vaginal douching 6.47 0.97-42.74 0.05
Performing VD 0.69 0.29-1.61 0.39
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 40
with the fingers
Performing VD
2-3 times a week
1.68 0.77-3.65 0.05
Continuously using a sanitary
napkin
0.53 0.26-1.08 0.08
**ICUD: Intrauterine contraceptive device
DISCUSSION
In the present study, there was a higher
percentage (81.1%) of women using IUCDs
who were practicing VD compared to the
women who were taking OCPs (70. %).
Many studies have shown that the use of
IUCDs increases the risk of vaginal
infection [22,23,25]
. Various factors play a role
in determining whether women using
IUCDs will develop an infection. These are,
among others, the technique used in
inserting the IUCD, the duration of its use,
and the age of the woman. The IUCD
changes the nature of the vaginal flora and
leads to an increase in anaerobic bacteria [17,
26].
However, many studies have also shown
that genitourinary system infections are
reduced if general hygiene is carefully
practiced, the IUCD is carefully inserted,
and regular check-ups are performed over
the period the IUCD remains in the uterus,
provided the rules of hygiene are adhered
to[24, 26]
. As it was observed in the present
study that women using IUCDs had better
toilet hygiene behavior than the women
taking OCPs, it might be said that hygiene is
one of the factors affecting the growth of
bacteria in the urine cultures of women
taking OCPs.
Failure to clean the anal region separately
leads to the colonization of microorganisms
at the entry of the urethra and vagina [26]
.
Vaginal douching, the continuous use of
sanitary napkins, and faulty washing and
cleaning after defecation increases the risk
of infection {27, 28]
.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 41
Vaginal douching has become a part of
women's general hygiene in [14,15]
. Married
women describe themselves as being soiled
when seminal fluid remains in the vagina
after sexual intercourse. Women's beliefs
cause women to regard the vagina as
contaminated after intercourse. Women
practice vaginal douching to feel clean again
and many studies have shown that women
practice vaginal douching to restore their
sense of wellness and cleanliness [10,18]
.
Other reasons reported as to why women
perform vaginal douching have been vaginal
discharge, eliminating itching or odor,
preventing or treating sexually transmitted
diseases or vaginal infections, and using the
practice as a contraceptive measure [8,10,14,29]
.
The practice is common as it is a part of the
full ablution regimen required by the
religion after sexual intercourse. 4,10In the
present study, VD was resorted to primarily
after menstruation and sexual intercourse.
Hodoğlugil et al. reported in a study they
conducted in the Black Sea Region in 2000
that VD was practiced by 64.0% of women
using IUCDs and by 64.5% of women that
were not. In the present study, our finding
was that more women with IUCDs were
practicing VD compared to women taking
OCPs; this is consistent with the literature.
In the study, the women in the OCP
and IUCD groups said that they performed
vaginal douching 2-3 times a week. In a six-
month study conducted in the US, it was
found that 22% of women practice vaginal
douching [28]
. The detergents, soaps, acetic
acid, perfumes and other agents that may be
used in vaginal douching disturb the vaginal
flora and prepare a suitable environment for
infection [10,16,29]
. Various studies have
shown that soap and water are the
substances that are most commonly used in
vaginal douching [6,14]
.
In the present study, the use of soap
and water was more pronounced in women
taking OCPs compared with those using
IUCDs. Most of the women taking OCPs
were using their fingers to wash the vagina
with soap and water whereas most of the
women with IUCDs were practicing VD by
washing out the vagina with water at high
pressure without using the fingers. IUCDs in
particular are a potential risk factor and
although the women with IUCDs, who were
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 42
using less soap than the OCP group and
refraining from using their fingers, instead
flushing out the area with water at high
pressure, exhibited more prominent bacterial
growth in the culture, both methods resulted
in the development of vaginal infection The
transport into the urinary tract of
microorganism colonies developing in the
vagina is facilitated by the fact that the
exterior one-third of the urethra, which is
short in women, is in constant contact with
intestinal flora [26]
. The regions of the body
that are conducive to the colonization of
microorganisms are the vagina, rectum, and
ureter. The type of underwear worn, the
form of cleansing, the materials used, among
other factors, are all instrumental in the
degree these three areas are protected [10]
.
Since the continuous use of a sanitary
napkin keeps the vagina moist, an
environment that allows bacteria to grow is
thus created.
In many studies it has been shown
that a large percentage of women use
sanitary pads continuously, either because of
religious beliefs or as a customary habit. It
has been proven in many studies that daily
water consumption can prevent urinary tract
infections [17,26]
. In our study, the
predominance in the OCP group of
uncomfortable vaginal discharge, cleansing
from back to front, continuous use of
sanitary napkins, daily water consumption of
under 2 liters, and the use of cloths as drying
materials after going to the toilet were the
factors that resulted in more bacterial growth
in the urine culture compared to the IUCD
group. At the same time, it is known that
estrogen facilitates the settling of
uropathogens in the vagina and urogenital
cells and that some antibiotics spoil the
vaginal flora, creating an environment where
microorganisms can grow freely [15,19]
. The
difference observed in the urine culture of
women taking OCPs in the present study
was a product of the characteristic of such
agents, a factor which was intensified by the
deficiencies in hygiene that were observed
in the study.
Conclusion and Recommendation
Women continue to practice
traditional habits that can be recognized as
VD. Changing these traditions is a difficult
task that will require time. VD is practiced,
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 43
regardless of whether the hazards to the
health are known or not. When the variety of
reasons women practice VD are considered,
it is of importance to study women's
hygienic practices and educate them about
the mistakes they are making. It is important
that members of a health team offer women
the opportunity for an exchange of
information, working to prevent the
complications that faulty technique and lack
of attention to the rules of hygiene can bring
about. The early discovery of mistakes is
essential, not only in terms of preventing
potential health problems in women but also
in treating existing problems early on.
REFERENCES
1.Martino JL, Vermund SH. Vaginal
douching 2002; Evidence for risks or
benefits to women’s health. Epidemiol.
Rev 2002.;24:109-124.
2. Mete S, Gercek E. (2005): Factors
affecting the prevalence of vaginal
douching and outcomes. JOSN;55-61.
3. Lichtenstein, B., Nansel, T.R. 2000:
Women’s douching practices and related
attitudes:findings from four focus groups.
Women & Health2000;30(4):117-131.
4. http://www.diyanet.gov.tr/ Accessed 12
February 2012
5. Ege E, Timur S, Zincir H, et alVaginal
douching practices and related attitudes
in eastern Turkey. J. Obstet. Gynaecol.
Res 2007; 33(3):353-59.
6. Demirbağ C. Risk factors for IUCD
related to hygienic habits in women. C.U.
Nurs.School J.2000; 4(2):52-58.
7. Foch BJ, McDaniel ND, Chacko MR:
Racial differences in vaginal douching
knowledge, attitude, and practices among
sexually active adolescents. JPAG
2001;14:29 –33
8. Hacıalioğlu N, Đnandı T, Pasinlioğlu T:
Incidence of genital infections and risk
factors in women presenting at the
Erzurum Mother & Child Health and
Family Planning Center. A. U, Nurs.
School J 2000;. 3(2):11-17.
9. Akın B, Erdem H, Ege E: Vaginal
douching practices in married women,
ages 15-49, and adverse effects. Life Sci.
J 2006;3 3.
10. Calıskan D, Subası N, Sarısen O.:
Vaginal douching and associated factors
among married women attending a family
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 44
planning and gynecology clinic. 4th
International Congress of Reproductive
Health & Family Planning, Bayt press
Ankara: Turkey, 2006’.201-205.
11. Martino JL, Vermund SH.Vaginal
douching: Evidence for risks or benefits
to women’s health. Epidemiol. Rev.2002;
24:109-124.
12. Simpson T, Merchant JS, Grimley DM,
et al. (2004):Vaginal douching among
adolescent and young women: more
challenges than progress. J Pediatr
Adolesc Gynecol 2004; 17:249- 258.
13. Kirchner JT.: Prevalence of vaginal
douching despite its adverse effects.
Am.Fam.Phys. 2000;61(3):849-851.
14. Calzolari E, Masciangelob R, Militea V.
et al: Bacterial vajinosis and
contraceptive methods. Int J Gynaecol
Obstet2000.;70:341-46.
15. Calıskan D, Col M, Akdur R, et al.
Study of prevalence of vaginal douching
in women, ages 15-49, in the Park
Regional Healthcare Center and
influencing factors, Ankara University
Medical School Journal2003;49(2):73-80.
16. Kalterna V, Tepes NK, Pejkovic L et al.
An intrauterine device as a possible cause
of change in the microbial flora of the
female genital system. J Obstet.
Gynaecol. Res.2011; 37(8):1035-1040.
17. Gupta K, Hiller SL, Hooton TM et al.
Effects of contraceptive method on the
vajinal microbial flora: A prospective
evaluation. J Infect. Dis. 2000;181:595-
97.
18. Anh PK, Khanh NT, Ha DT, et
al.(2003): Prevalence of lower genital
tract ınfection among women attending
maternal and child health and planning
clinics in Hanoi. Vietnam, Southeast
Asian J Trop Med Public Health;34:367-
373.
19. Oh MK, Funkhouser E, Simpson T, et al.
Early onset of vaginal douching is
associated with false beliefs and high risk
behaviour. STDs 2003;30(9):689-669.
20. Zarakolu P, Hodoglugil NS, Aydın F, et
al.: Reliability of interpretation of
gramstained vaginal smears by nugent's
scoring system for diagnosis of bacterial
vaginosis. Diagn. Microbiol. and Infect.
Dis.2004; 48(2):77-80.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 45
21. Turkish Population and Health Research
On Rapor. Tubitak Mart: Ankara, 2009.
22. Gazmararian JA, Bruce FC, Kendrick
JS, et al: Why do women douche?
Results from a qualitative study. Matern
Child Health J2001; 5(3):153-159.
23. Chiaffarino F, Parazzini F, DeBesi P:
Risk factor for bacterial vaginozis. Eur J.
Obstet. Gynecol Reprod. Bio
l2004.;117:222-226.
24. Calıskan D. Traditional intravaginal
applications: “should vaginal douching,
lavage be performed or not? CME
2005;4:15-18.
25. Ocak S, Cetin M, Hakverdi S. et
alEffects of intrauterine device and oral
contraceptive on vaginal flora and
epithelium. Saudi Med. J2007.;28:727-31.
26. Ozsut H.Urinary tract infections:
Infectious Diseases and Clinical
Microbiology2002; 1059-65. Ayse Wilke
Topcu, Guner Soyletir, Mehmet Doğanay
(Eds), Nobel medical press,
27. Hoduoglugul NS, Aslan D, Bertan M.
.Intrauterine device use and some issues
related to sexually transmitted disease
screening and occurrence. Contraception
2000;61:359-364.
28. Koumans EH, Stenberg M, Bruce C et al.
The prevalence of bacterial vaginosis in
the United States, 2001-2004; associations
with symptoms, sexual behaviors, and
reproductive health. Sex Transm.
Dis.2007;;34:864-9.
29. Pavlova SI, Tao L.In vitro inhibition of
commercial douche products against
vaginal microflora. Infect Dis Obstet
Gynecol.2002;;8:99-104.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
Whiff Test and Vaginal pH >4.5 as Rapid and Accurate Bed-side Screening Test for
Vaginal Infection
Sahar Fahmy Gawad
Lecturer of Obstetric & Gynecology Nursing,
Faculty of Nursing, South Valley University (Kena), Egypt
Abstract
Bacterial vaginosis and Trichomonas virginals infection have been associated with adverse
pregnancy and health outcomesAims of the study : To evaluate the diagnostic yield of
determination of vaginal pH considering pH>4.5 as diagnostic for vaginal infection and positive
Whiff test as rapid bed-side diagnostic tests and their applicability as screening tests for vaginal
infection in women apparently free of symptoms Materials & method: The current study
included 120 women; 60 women were complaining of vaginal discharge (Patient group) and
another 60 women have no complaint of vaginal discharge (Screening group). An un-lubricated
Cusco’s vaginal speculum was inserted into the vagina and characteristics of the discharge with
respect to amount, odor and type of discharge were evaluated. Two samples of the vaginal
discharge collected on dry sterile cotton wool tipped swabs. Secretions from the second swab
were placed on pH indicator strips with a pH range of 3.5 to 6 to determine vaginal pH. Two
drops of 10% KOH solution were added to the second and release of fishy amine odor signified a
positive whiff test.Results: Thirty-three patients (55%) complained of vaginal discharge, 5
patients (8.3%) had itching and 14 patients (23.3%) had history of recurrent discharge and past
history of treatment. Thirty-nine patients 39 (65%) had positive whiff test and 43 swabs (71.7%)
had pH>4.5. Twenty-seven patients were missed on reliance on clinical data only, while 21
patients were missed in case of whiff test and only 17 patients in case of pH>4.5. Thus, both tests
improved the diagnosis of vaginal infection with sensitivity rate of 85% and accuracy rate of 65%
compared to sensitivity rate of 58.9% and accuracy rate of 46.7% for clinical alone. Conclusion:
Determination of vaginal pH >4.5 and positive Whiff test are rapid, simple and easy to perform
as bed-side diagnostic tests and could be used as screening tests for vaginal infection in women
apparently free of symptoms.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
Introduction
Bacterial vaginosis and Trichomonas
virginals infection have been associated with
adverse pregnancy and health outcomes.
Being the most common vaginal infections
among women. BV and TV increase risk for
acquisition of other sexually transmitted
infections. In obstetrics, BV has been
implicated in causing higher rates of late
miscarriage, preterm premature rupture of
membrane, chorio-amnionitis, spontaneous
preterm labor, preterm birth, and postpartum
endometritis (1, 2, 3)
.The high prevalence of
BV and TV and the large burden of
associated disease, there is a compelling
public health need for simple and
inexpensive point-of-care diagnostic tests for
expanded screening of women especially in
poor settings (4)
.In many parts of the
developing world, laboratory diagnosis of
vaginal infections is not available outside
urban areas. Even simple and inexpensive
methods such as Gram stain of vaginal
smears or microscopic examination for
motile trichomonads are generally beyond
the reach of most primary healthcare settings
(5)Healthcare workers typically manage
vaginal infections using a syndromic
approach which bases treatment on
symptoms and signs. Unfortunately, studies
have shown low sensitivity and low
predictive values for diagnoses of
reproductive tract infections (RTI) using a
syndromic approach among women. Such an
approach not only misses asymptomatic
infections but also results in substantial
under-diagnosis and over-treatment of BV
and TV (6-9)
.The present study aimed to
evaluate the diagnostic yield of
determination of vaginal pH considering
pH>4.5 as diagnostic for vaginal infection
and positive Whiff test as rapid bed-side
diagnostic tests and their applicability as
screening tests for vaginal infection in
women apparently free of symptom
Materials & method
Research design:
The research was prospective study
Setting:
The study was conducted at the outpatient
clinic of Department of Obstetrics &
Gynecology, South Valley University
Hospital at Kena

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 89
Subject:
The subject was composed of 120 women
were enrolled in the study. Sixty women
were collected from those attending the
gynecology outpatient clinic complaining
from vaginal discharge (Patient group)
-Another 60 women collected from those
attending Family Planning Clinic requesting
for appropriate contraceptive modality and
have no complaint of vaginal discharge
(Screening group).
Tools of data collection
Structure questioner sheet was developed by
the researcher to collect the necessary data
which includes the following:
Part I: Socio demographic data: which
includes as age, marital status, educational
level, occupation, and parity were recorde
Part II
Participants were asked about their
symptoms, the nature of their complaints
concerning presence and amount of
discharge, presence of itching, past illness,
and history of treatment before enrollment.
Pregnant and menstruating women or those
who had used antibiotics and/or topical
vaginal creams within seven days prior to
the date of examination were excluded from
the study.
Tool II
An un-lubricated Cusco’s vaginal
speculum was inserted into the vagina and
characteristics of the discharge with respect
to amount, odor and type of discharge were
evaluated.
Two samples of the vaginal discharge
collected on dry sterile cotton wool tipped
swabs. Secretions from the second swab
were placed on pH indicator strips with a pH
range of 3.5 to 6 to determine vaginal pH.
Two drops of 10% KOH solution were
added to the second and release of fishy
amine odor signified a positive whiff test.
Results
As regarding sociodemogrphic data, the
study included 120 women with mean age of
34.9±3.4; ranged from 23-41 years. The
majority of studies sample were age group
of 30-40 years. Eighty-nine women were
currently married while 9 women were
single while 11 were widow and 11 were

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 90
divorced. Twenty-three women were
university graduate, As regarding
educational level , it was noticed that 41
women were high school graduate while 35
%of them were not graduated and 21% of
them were illiterate. Only 11 women were
nullipara, 21 women were primpara, 40
women were para-two, 32 women were
para-three and 16 women were para-four.
There was non-significant difference
between both groups as regards enrollment
data, (Table 1).
Thirty-three patients (55%) complained of
vaginal discharge which was profuse in 11
patients (18.3%), minimal in 15 patients
(25%) and scanty in 7 patients (11.7%). Five
patients (8.3%) had itching and 14 pa tients
(23.3%) had history of recurrent discharge
and past history of treatment.
Among studied patients 39 women (65%)
had positive whiff test and 43 swabs (71.7%)
had pH>4.5, while both tests were positive
in 22 patients. Only 10 patients had
discharge gave positive pH test, 11 patients
had discharge gave positive whiff test and
12 patients had discharge gave positive both
tests, (Table 2, Fig. 1). Considering presence
of vaginal discharge as the frequent clinical
symptom and the main complaint, 27
patients will be missed on reliance on
clinical data only. On contrary 21 patients
will be missed on reliance on whiff test and
only 17 patients in case of pH>4.5. Thus,
both tests improved the diagnosis of vaginal
infection with sensitivity rate of 85% and
accuracy rate of 65% compared to sensitivity
rate of 58.9% and accuracy rate of 46.7% for
clinical alone.Application of both tests to
screen the apparently healthy group allowed
detection of 28 cases with vaginal infection
despite the absence of complaints or clinical
findings. Fifteen women (25%) had vaginal
pH>4.5, while 13 women gave a swab
giving positive Whiff test and 5 of these
women gave both tests positive (Table 3,
Fig. 3).
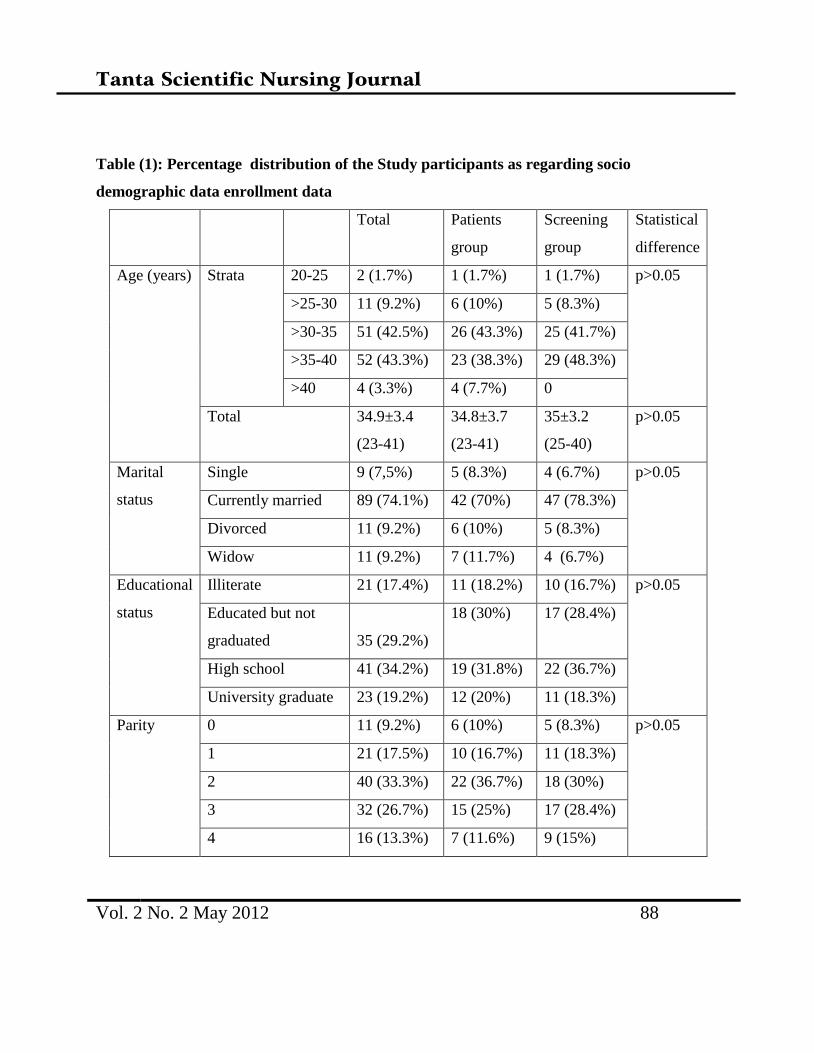
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
Table (1): Percentage distribution of the Study participants as regarding socio
demographic data enrollment data
Total Patients
group
Screening
group
Statistical
difference
Age (years) Strata 20-25 2 (1.7%) 1 (1.7%) 1 (1.7%) p>0.05
>25-30 11 (9.2%) 6 (10%) 5 (8.3%)
>30-35 51 (42.5%) 26 (43.3%) 25 (41.7%)
>35-40 52 (43.3%) 23 (38.3%) 29 (48.3%)
>40 4 (3.3%) 4 (7.7%) 0
Total 34.9±3.4
(23-41)
34.8±3.7
(23-41)
35±3.2
(25-40)
p>0.05
Marital
status
Single 9 (7,5%) 5 (8.3%) 4 (6.7%) p>0.05
Currently married 89 (74.1%) 42 (70%) 47 (78.3%)
Divorced 11 (9.2%) 6 (10%) 5 (8.3%)
Widow 11 (9.2%) 7 (11.7%) 4 (6.7%)
Educational
status
Illiterate 21 (17.4%) 11 (18.2%) 10 (16.7%) p>0.05
Educated but not
graduated 35 (29.2%)
18 (30%) 17 (28.4%)
High school 41 (34.2%) 19 (31.8%) 22 (36.7%)
University graduate 23 (19.2%) 12 (20%) 11 (18.3%)
Parity 0 11 (9.2%) 6 (10%) 5 (8.3%) p>0.05
1 21 (17.5%) 10 (16.7%) 11 (18.3%)
2 40 (33.3%) 22 (36.7%) 18 (30%)
3 32 (26.7%) 15 (25%) 17 (28.4%)
4 16 (13.3%) 7 (11.6%) 9 (15%)
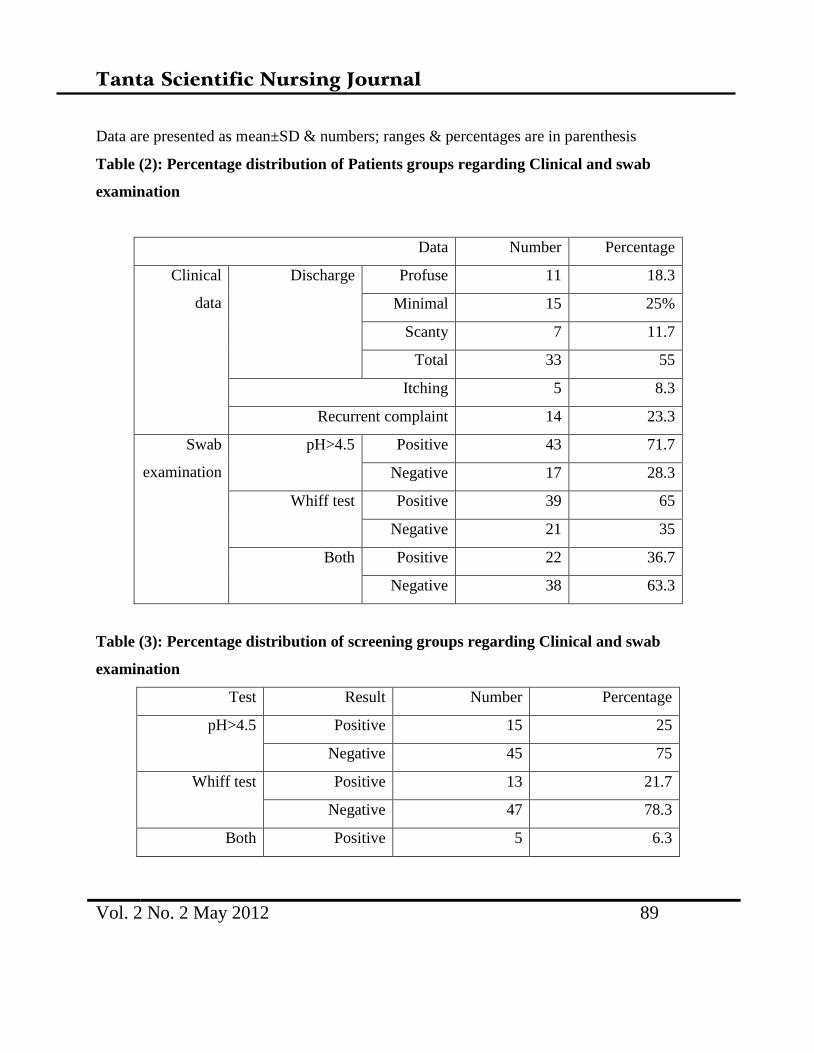
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 89
Data are presented as mean±SD & numbers; ranges & percentages are in parenthesis
Table (2): Percentage distribution of Patients groups regarding Clinical and swab
examination
Data Number Percentage
Clinical
data
Discharge Profuse 11 18.3
Minimal 15 25%
Scanty 7 11.7
Total 33 55
Itching 5 8.3
Recurrent complaint 14 23.3
Swab
examination
pH>4.5 Positive 43 71.7
Negative 17 28.3
Whiff test Positive 39 65
Negative 21 35
Both Positive 22 36.7
Negative 38 63.3
Table (3): Percentage distribution of screening groups regarding Clinical and swab
examination
Test Result Number Percentage
pH>4.5 Positive 15 25
Negative 45 75
Whiff test Positive 13 21.7
Negative 47 78.3
Both Positive 5 6.3
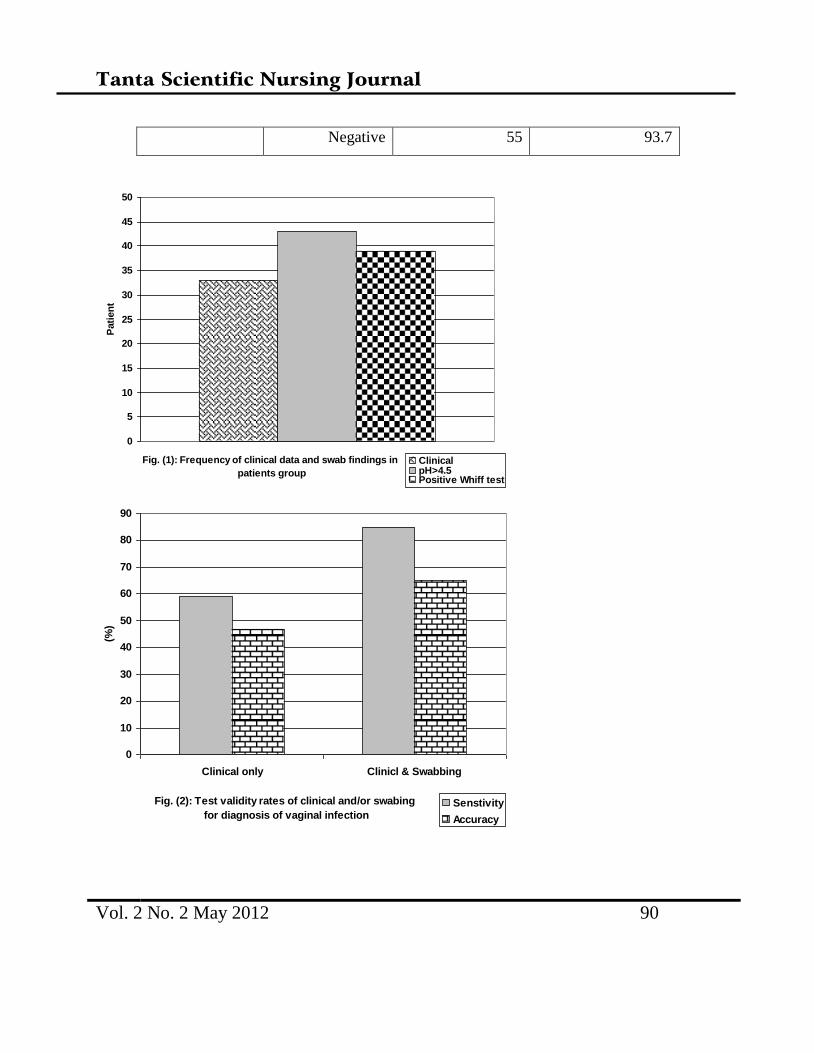
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 90
Negative 55 93.7
Fig. (1): Frequency of clinical data and swab findings in
patients group
0
5
10
15
20
25
30
35
40
45
50
Pati
en
t
ClinicalpH>4.5Positive Whiff test
Fig. (2): Test validity rates of clinical and/or swabing
for diagnosis of vaginal infection
0
10
20
30
40
50
60
70
80
90
Clinical only Clinicl & Swabbing
(%)
Senstivity
Accuracy
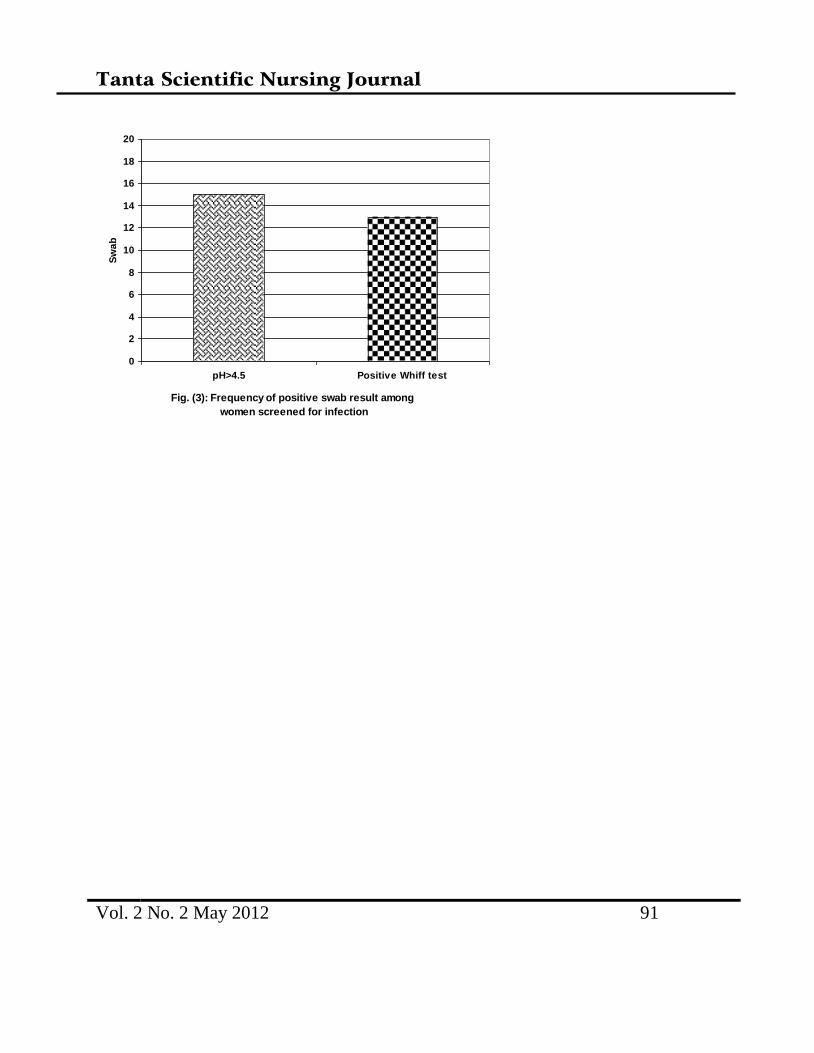
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 91
Fig. (3): Frequency of positive swab result among
women screened for infection
0
2
4
6
8
10
12
14
16
18
20
pH>4.5 Positive Whiff test
Sw
ab

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
Discussion
The frequency of vaginal discharge varied
between various populations and among
certain population; in developing countries
the frequency of vaginal infection varied
between 20 to 50% of non-pregnant women
and bacterial vaginosis was found to affect
about 70% of women (10, 11)
.
Proper diagnosis of bacterial vaginosis is
challenging. In addition to scientific
considerations, choosing a method for
laboratory diagnosis requires consideration
of complexity, cost, and the frequency of un-
interpretable specimens. Nevertheless, some
alternative diagnostic methods have been
developed, such as the polymerase chain
reaction, rapid nucleic acid hybridization
test, proline amino peptidase activity. More
recently, several point-of-care tests based on
various combinations of microbial products,
presence of RNA, or more complex
laboratory instrumentation such as sensor
arrays, have also been introduced for the
diagnosis of bacterial vaginosis. However,
most of these are expensive and their
sensitivities and specificities do not offer a
huge advantage over the classical methods
(12, 13).
Through the current study, the
dependence on clinical manifestations
allowed identification of 33 patients with
vaginal infection, while reliance on positive
Whiff test allowed detection of 39 patients
and vaginal pH>4.5 allowed detection of 43
patients. Thus, reliance on these rapid bed-
side tests raised sensitivity for presence of
vaginal infection to 89% and accuracy of
diagnosis to 65%. The diagnostic bed-side
tests were applied to non-symptomatizing
women considering themselves free of
vaginal infection and could identify 28 cases
of vaginal infection, so both tests could be
used for screening of vaginal infection
among apparently healthy women. In line
with the reliance on these both tests in
conjunction with clinical manifestations if
present; Madhivanan et al. (14)
compare the
performance of simple inexpensive point-of-
care tests; vaginal pH; and Whiff test to
laboratory diagnosis including serology for
HSV-2; cultures for TV, Candida sp., and
Neisseria gonorrhoeae; Gram stains and
found that in the absence of laboratory

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 89
diagnostics, vaginal pH; and Whiff test is
not only inexpensive and practical, but also
significantly more sensitive than the
syndromic management approach, resulting
in less over-treatment.
Quan (15)
documented that vaginitis
is one of the most common ambulatory
problems to occur in women, the medical
history and examination are an important
source of clues to the underlying diagnosis;
however, making a definitive diagnosis
requires skillful performance of office
laboratory procedures, including the vaginal
pool wet mount examination, determination
of the vaginal pH, and the whiff test and
vaginal and cervical cultures, nucleic acid
tests, and point-of-care tests are available
and may be required in selected patients.
Thulkar et al. (16)
evaluated sensitivity and
specificity of pH test and Whiff test in
diagnosis of abnormal vaginal discharge,
considering microscopic diagnosis as gold
standard and found pH ≥4.5 and positive
Whiff test had sensitivity of 94.1% and
specificity 87.5% in diagnosing vaginal
infection and concluded that pH test and
Whiff test can improve diagnostic value of
speculum examination where microscope
facilities are not available.
Hainer & Gibson (17)
stated that
bacterial vaginosis, trichomoniasis, and
vulvovaginal candidiasis are the most
common infectious causes of vaginitis and
diagnosis is commonly made using the
Amsel criteria, which include vaginal pH
greater than 4.5, positive whiff test, milky
discharge, and the presence of clue cells on
microscopic examination of vaginal fluid.
The procedure as a whole was
applied by the author, a gynecologically
qualified staff nurse without the attendance
of physician, and owing to simplicity and
good yield could be applied as training
course for nurses working in healthcare units
for widespread screening program. In hand
with this assumption, multiple studies tried
self-obtained swabs for diagnosis of
vaginitis and reported applicability.
Huppert et al. (18)
compared the accuracy of
self-performed point-of-care tests with
clinician-performed tests for trichomoniasis
in adolescent women and found that young
women performing a self-point-of-care test

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 90
detected as many trichomoniasis infections
as clinician- point-of-care tests or culture,
twice as many as wet mount and slightly
fewer than an amplified test. Incorporating
self-obtained or self-performed point-of-care
tests into routine practice could effectively
increase the identification and treatment of
trichomoniasis in this vulnerable
population.It could be concluded that
determination of vaginal pH >4.5 and
positive Whiff test are rapid, simple and
easy to perform as bed-side diagnostic tests
and could be used as screening tests for
vaginal infection in women apparently free
of symptoms.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
References
1-ElyanA, Rund N: Bacterial vaginosis and
pregnancy. ASJOG, 2004; 1: 179-84.
2-McClelland RS, Sangare L, Hassan WM:
Infection with Trichomonas vaginalis
increases the risk of HIV-1 acquisition.
Journal of Infectious Diseases, 2007; 195,
698–702.
3-Atashili J, Poole C, Ndumbe PM, Adimora
AA, Smith JS: Bacterial vaginosis and
HIV acquisition: a meta-analysis of
published studies. AIDS, 2008; 22, 1493–
501.
4-Bologno R, Díaz YM, Giraudo MC,
Fernández R, Menéndez V, Brizuela JC,
Gallardo AA, Alvarez LA, Estevao
Belchior SG: Importance of studying the
balance of vaginal content (BAVACO) in
the preventive control of sex workers.
Rev Argent Microbiol. 2011;43(4):246-
50.
5-Mullick S, Watson-Jones D, Beksinska M,
Mabey D: Sexually transmitted infections
in pregnancy, prevalence, impact on
pregnancy outcomes, and approach to
treatment in developing countries.
Sexually Transmitted Infections, 2005;
81, 294–302.
6-World Health Organization: Management
of Symptomatic STIs . RTIs Sexually
Transmitted and Other Reproductive
Tract Infections . A Guide to Essential
Practice. WHO, Geneva, 2005.
7-Tann CJ, Mpairwe H, Morison L: Lack of
effectiveness of syndromic management
in targeting vaginal infections in
pregnancy in Entebbe, Uganda. Sexually
Transmitted Infections, 2006; 82, 285–9.
8-Romoren M, Velauthapillai M, Rahman
M, Sundby J, Klouman E, Hjortdahl P:
Trichomoniasis and bacterial vaginosis in
pregnancy, inadequately managed with
the syndromic approach. Bulletin of
World Health Organisation, 2007; 85,
297–304.
9-Onyekonwu CL, Olumide YM, Oresanya
FA, Onyekonwu GC: Vaginal discharge:
aetiological agents and evaluation of
syndromic management in Lagos. Niger J
Med. 2011;20(1):155-62.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 89
10-Rivers CA, Adaramola OO, Schwebke
JR: Prevalence of bacterial vaginosis and
vulvovaginal candidiasis mixed infection
in a southeastern american STD clinic.
Sex Transm Dis. 2011; 38(7):672-4.
11-Sherrard J, Donders G, White D, Jensen
JS; European IUSTI: European
(IUSTI/WHO) guideline on the
management of vaginal discharge, 2011.
Int J STD AIDS. 2011; 22(8):421-9.
12-Menard JP, Mazouni C, Fenollar F,
Raoult D, Boubli L, Bretelle F:
Diagnostic accuracy of quantitative real-
time PCR assay versus clinical and Gram
stain identification of bacterial vaginosis.
Eur J Clin Microbiol Infect Dis. 2010;
29(12):1547-52.
13-Ram JL, Karim AS, Sendler ED, Kato I:
Strategy for microbiome analysis using
16S rRNA gene sequence analysis on the
Illumina sequencing platform. Syst Biol
Reprod Med. 2011;57(3):162-70.
14-adhivanan P, Krupp K, Hardin J, Karat
C, Klausner JD, Reingold AL:Simple and
inexpensive point-of-care tests improve
diagnosis of vaginal infections in
resource constrained settings. Trop Med
Int Health. 2009; 14(6):703-8.
15-Quan M: Vaginitis: diagnosis and
management. Postgrad Med. 2010;
122(6):117-27
16-Thulkar J, Kriplani A, Agarwal N: Utility
of pH test & Whiff test in syndromic
approach of abnormal vaginal discharge.
Indian J Med Res. 2010;131:445-8.
17-Hainer BL, Gibson MV: Vaginitis. Am
Fam Physician. 2011; 83(7):807-15.
18-Huppert JS, Hesse E, Kim G, Kim M,
Agreda P, Quinn N, Gaydos C:
Adolescent women can perform a point-
of-care test for trichomoniasis as
accurately as clinicians. Sex Transm
Infect. 2010;86(7):514-9.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
Effects of Topical Honey Dressing on Infected Wounds after Gynecological and Obstetrical
Abdominal Surgery
Mona Abd El-Haleem Ebraheem El-Agamy
Assistant lecturer Maternity and Gynecological Nursing
Faculty of Nursing, Tanta University.
Prof. Dr.Shadia Abd El-kader Hassan
Maternity and Newborn health Nursing,
Faculty of Nursing, Cairo University.
Naeim Fatoh El Far
Prof. of Microbiology,
Faculty of Medicine, Tanta University.
Iman Abd El-Azziz El-Khayat
Lecturer of Maternity and Gynecological Nursing,
Faculty of Nursing, Tanta University.
Abstract
Despite use of prophylactic antibiotics, wound infections remain common. Post operative wound
infections develop in 4% of patients following inpatient gynecologic surgery and in 5% to 7% of
patients undergoing primary cesarean section. The use of honey as a wound dressing material is
an ancient remedy that has been rediscovered. The aim of the study is to evaluate the effects of
topical honey dressing on infected wounds after obstetrical and gynecological abdominal surgery
as compared to the routine hospital wound care. This study was conducted on 60 women were
recruited from Tanta University hospitals at Obstetrical and Gynecological Department. Where
30 of them were dressed according routine wound care of the hospitals, which includes local
antiseptics, daily dressing, and antibiotic. And the others were dressed by honey (Api-care)
dressing plus the routine hospital wound care. The result of the study revealed that the mean age
of the honey group was 30.87 ± 8.41 while the other groups mean age was 35.17 ± 9.92 which
was statistically not significant (p=0.061). Results of honey dressing showed remarkable change

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 89
compared to other method. After 6 days of dressing, wound appearance among those dressed by
honey was normal among 100% of cases compared to grey or white pallor appearance for the
other group. Honey dressed group showed 100% significant improvement, mild pain, non
exudates which was significantly different from other group (p=0.001). the mean duration of
management of cases with honey was found to be 11 days compared to 20 cases for other group
which was found to be significantly different at p=0.001. The researcher concluded that topical
application of sterile topical honey cream (Api-care) could eradicate organisms within short time,
reduce period of antibiotic use, accelerate the healing process in unique and economic way, result
in minimal scar formation, prevent wound dehiscence and need for re- suturing. weight, 15.8% in
overweight, and 37.5 in obese women (4)
.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
Introduction
Hysterectomy and cesarean section are the
most commonly performed operations
among inpatients at Egyptian Hospital (1)
.
The two most frequent complications of
these surgeries are fever and surgical site
infections (SSIs). The use of prophylactic
antibiotics in hysterectomy and cesarean
section in Egyptian hospitals is not
standardized and is determined by the
consultant in charge of the case.
Inappropriate and prolonged use of
antibiotics is a serious problem. It increases
the morbidity and mortality of patients and
also increases health care costs due to
increased antibiotic resistance rates (2)
.
SSIs developed in 4% of inpatient
undergone gynecologic surgery and in 5% to
7% of patients’ undergone primary cesarean
section (1,3)
. According study In Egypt
about wound infection after Cesarean
Section and women weight; wound
infections were 11.4 % in normal Surgical
site infections (SSIs) continue to pose a
major problem for many surgery patients. Its
occurrence is associated with readmission,
repeated surgery or intervention, prolonged
hospitalization and significant clinical and
economic consequences. The risk is
particularly high in developing countries due
to mal-nutrition, illiteracy, improper surgical
technique, substandard sterilization of
operation theatres and inadequate or over
burdened health facilities (5,6,7)
. Data on SSI
rates is not available in Egypt; however,
other sources of data suggest that there is
poor compliance in aseptic techniques and
Increase the cost of the hospital stay 7 – 8
days for a SSI (7)
. In Egypt, every one
Egyptian pound spent for infection control
saves 60 Egyptian pound spent on
nosocomial infection (8)
.
Nursing care of the female surgical patient
requires an accurate understanding of the
pathophysiologic changes that occur
perioperatively. The nurse should maintain
proper environment and appropriate
interventions; the first nurse's goal during
the postoperative period is to provide
appropriate support that allows for the
maintenance of homeostasis and the
prevention of potential complications. The
second goal is to recognize unfavorable

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 89
trends in the course of recovery and respond
expeditiously to prevent further compromise.
Much information can be obtained by close
monitoring of vital signs. Changes of these
measurements reflect the patient's ongoing
condition (9)
.
The management of the incision is based
on the normal biology of the healing
process, which is conceptually divided into
three phases. Initial phase (inflammation),
second phase (fibroblast proliferation) and,
third phase (maturation). The operative
dressing can be removed after 24-48 hours.
If wound drainage is noted upon inspection,
a sterile dressing must be replaced until the
drainage ceases and closure is attained. On
the other hand, allowing sutures to stay in
place for a long period increases scar
formation at the sites of skin penetration. In
healthy individuals with an abdominal
incision, sutures can be removed on the third
postoperative day. (9.10)
. Temperature
elevation higher than (38°C) in the surgical
patient should alert the nurse of potential
complications. Evaluation and subsequent
therapy are dependent on how soon after
surgery the fever develops. Postoperative
fever in the First 24-48 hours may refer to
wound infection. Signs may include crepitus,
pain, and edematous discoloration.
Treatment consists of aggressive
intraoperative debridement and drainage and
broad-spectrum antibiotics. The use of
drains, tubes, and suction devices at the
wound site is often necessary to promote
healing. It is important to know the type of
drain or tube in use so that patency and
placement can be accurately assessed. Once
a diagnosis of wound infection has been
confirmed and antibiotic sensitivities
identified, appropriate management
regimens should be considered, with a high
priority given to reducing the risk of cross
infection. It is important to treat the patient
as a whole and not the infection alone, so
management strategies must be based on
data driven from a holistic assessment of
individual needs (11, 12,13)
.
Many researchers supported the use of
honey in managing infected wounds and
stated its prophylactic use on the wounds of
patients susceptible to infections and
antibiotic-resistant bacteria. Egyptian honey
is effective as an antibacterial agent against

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 90
different pathogenic bacteria. Most of
honey samples can completely inhibit the
growth of all bacteria. The use of honey as a
wound dressing material is an ancient
remedy that has been rediscovered. Honey is
produced from many different floral sources
and its antibacterial activity varies with
origin and processing. Honey selected for
clinical use should be evaluated on the basis
of antibacterial activity levels determined by
laboratory testing. Antibacterial properties of
honey include the release of low levels of
hydrogen peroxide and phytochemical
antibacterial components. So appropriate use
of topical honey dressing helps to reduce the
bacterial burden on the wound surface
(4,10,14).
Post operative obstetrical and gynecological
nursing professionals play a crucial role in
early detection of wound infections. Failure
to do this, can result in serious patients'
outcomes. Post operative nurses can expand
their current efforts through implementing
strategies to providing effective management
of infected surgical wound (11,12,13,15)
.
Practical guide on the use of honey in
managing infected surgical wounds, such as
amount of honey, concentration, type of
dressing, appropriate use and frequency
were considered and followed by the
researcher. So, this research was carried out
to early detection of SSIs and examines the
effects of honey dressing on optimal healing
of infected abdominal surgical wound of
obstetrical & Gynecological surgeries.
The aim the study was:-
To evaluate the effects of topical honey
dressing on infected wounds after obstetrical
and gynecological abdominal surgery as
compared to the routine hospital wound care.
Materials and Method
Subjects:
A total sample of 60 women was recruited
from the previously mentioned setting,
through the first three days after the surgery
according the following criteria:
Women are in the childbearing age (16-49
year). Post operative abdominal obstetrical
or gynecological patients. Appearance of
surgical site infection signs or symptoms
such as; redness, tenderness, infected
discharge, bad smell in the wound, fever
more than 38oC, faster pulse rate and faster
breathing. Signs and symptoms of infection

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 91
would are confirmed by wound culture.
Excluding patients who have any
medical disorder as; cardiac failure, chronic
respiratory problems, vascular disorders,
diabetes, renal and liver insufficiency and,
patients with hemoglobin ≤8 mg/ml. In
addition, patient receiving drug therapies
which may interfere with wound healing as
chronic steroid therapy, immunosuppressant
drugs, and anticoagulants were also
excluded.
Then the sample was divided into two
groups 30 women each. These subjects were
randomly divided into control group in odd
number and study group in even number.
The aim is to evaluate the effects of topical
honey dressing on surgical site infection
after obstetrical and gynecological
abdominal surgery compared to the routine
hospital wound care.
A- Control group:They were exposed to the
routine wound care of the hospital, which
include local antiseptics, daily dressing,
cultures from purulent discharge and
antibiotic policy.
B- Study group: They were exposed to
application honey dressing plus the
routine hospital wound care. The amount
of applied honey depended on the amount
of exudates. Tools of data collection
To achieve the aim of the study the
following tools were used.
I- Interview questionnaire was
developed by the researcher to collect
the required data about the study.
It was comprised of:
1- Sociodemographic data, which include:-
age, occupation, education, and family
history of medical diseases….etc
2- Patient medical history includes:- history
of the operation treatment and
complications….etc
II: An observation checklist to assess the
wound characteristics: site, size, color, odor,
amount, type of exudates and pain
assessment during hospitalization.
The findings of the current study are as
follows:-
There were significant differences in
progress of wound healing concerning skin
appearance surrounding wound. The
differences in progress started to be clear in
the 6th
day after application of honey

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 92
dressing . The skin became normal in the 9th
day in the study group.
Table (1): Represents Follow-up signs of
wound assessment (Skin appearance
surrounding wound) among the studied
subjects (study and control groups).It was
observed that, there were statistical
significant differences in progress of wound
healing concerning skin appearance
surrounding wound. In the first three days
the skin was White or gray pallor in the two
groups, But in the 6th day the difference in
progress started to be clear as (76.7%) of the
study group become pink and 23% is bright
red or blanch to touch. Gradually at the 9th
day skin become normal in the study group.
Contingency concerning control group there
was (86.7%) Skin appearance surrounding
wound was Bright red or blanches to touch
and (13.3 %) their wound was White or gray
pallor or hypo pigmented. Regarding
inflammatory response at the 9th
day of
management, there was not any response in
each case in the study group (100%) But, in
the control group there was (63.3%) their
wound was red and (13.3%) was red with
hotness. But at 21st day (86.7%) of subjects
was relived from inflammatory response
except (13.3%) of subjects) were still
suffering.
Graph (4) shows illustration of the mean
rank for the inflammatory variable for
both groups and the results was as
following:
In the first three days, there is
difference between the two
groups as the control group takes
the mean rank value (16.38) and
study group takes the mean rank
value (44.62) which means that
the treatment on the control
group has a better effect in that
earlier period.
After six days there is difference
between the two groups as the
control group takes the mean
rank value (17.43) and study
group takes the mean rank value
(43.57) which means that the
treatment on the control group
has a better effect.
After nine days there is
difference between the two
groups as the control group takes
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 93
the mean rank value (40) and
study group takes the mean rank
value (21) which means that the
treatment on the study group has
a better effect at the end of the
nine days.
Exudates disappeared in all subjects
(100%) in the study group at the 9th
day after application of honey
dressing, whereas the amount of
exudates was large in (36.3%) of
subjects and small in (36.3%) of
subjects in the control group till the
9th
day.
Concerning control group at 21st day
(13.3%) were purulent and (83.3%)
were changed to serous.
After the 6th
day, all wounds were
closed with a remarkably observed
improvement in the study group.
At the 9th
day, the pain during wound
dressing disappeared in the study
group comparing to two third (63.3%)
of subjects were complaining from a
severe pain and (36.7%) of subjects
were complaining from a mild pain in
the control group.
Graph (6) represents distribution of
the study groups according to their
wound size after 3 weeks of honey
application. It was found that the
mean of wound length was
15.83±2.45 in the study group and
16.37±2.95 in the control group.
Regarding width of wound after three
week of the application of honey,
there were significant different. As it
was 3-5 mm in the study group and 5-
8 mm in the control group with mean
4.10±0.76, and 6.63±0.96
respectively.
After 3 weeks of honey application.
Regarding width of wound , it ranged
from 3-5 mm in the study group and
from 5-8 mm in the control group
with mean 4.10±0.76, and 6.63±0.96
respectively
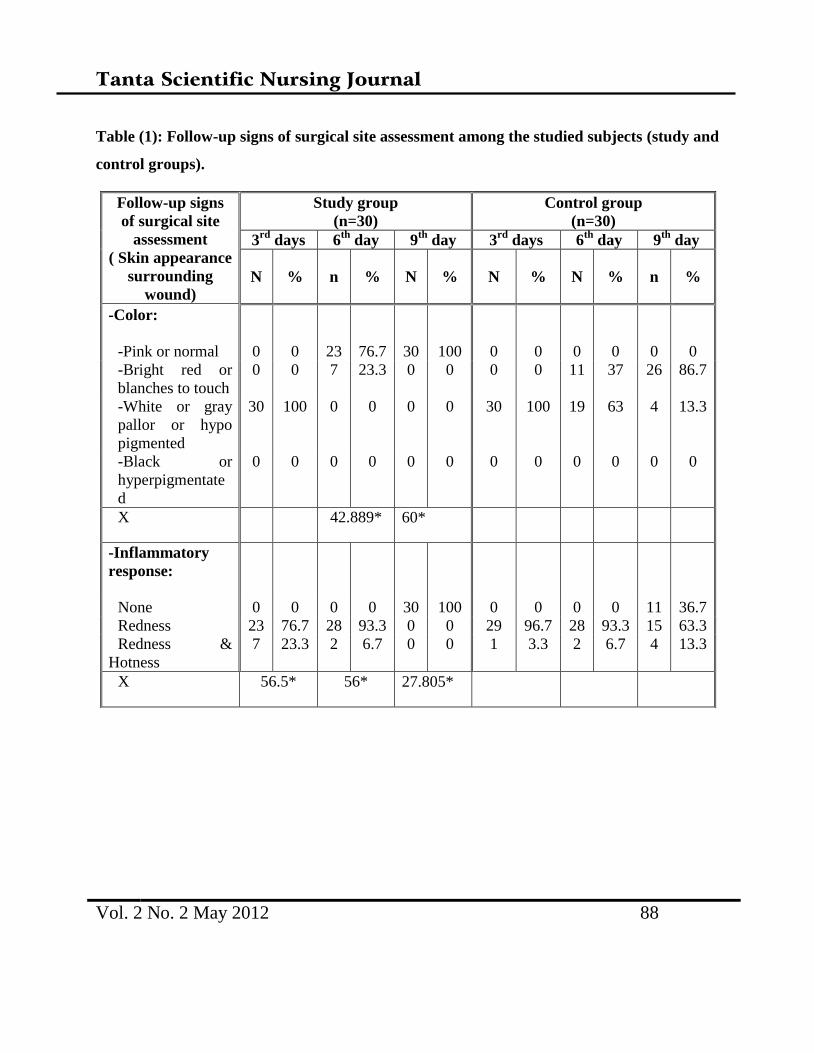
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 88
Table (1): Follow-up signs of surgical site assessment among the studied subjects (study and
control groups).
Follow-up signs
of surgical site
assessment
( Skin appearance
surrounding
wound)
Study group
(n=30)
Control group
(n=30)
3rd
days 6th
day 9th
day 3rd
days 6th
day 9th
day
N % n % N % N % N % n %
-Color:
-Pink or normal 0 0 23 76.7 30 100 0 0 0 0 0 0
-Bright red or
blanches to touch
0 0 7 23.3 0 0 0 0 11 37 26 86.7
-White or gray
pallor or hypo
pigmented
30 100 0 0 0 0 30 100 19 63 4 13.3
-Black or
hyperpigmentate
d
0 0 0 0 0 0 0 0 0 0 0 0
X 42.889* 60*
-Inflammatory
response:
None 0 0 0 0 30 100 0 0 0 0 11 36.7
Redness 23 76.7 28 93.3 0 0 29 96.7 28 93.3 15 63.3
Redness &
Hotness
7 23.3 2 6.7 0 0 1 3.3 2 6.7 4 13.3
X 56.5* 56* 27.805*
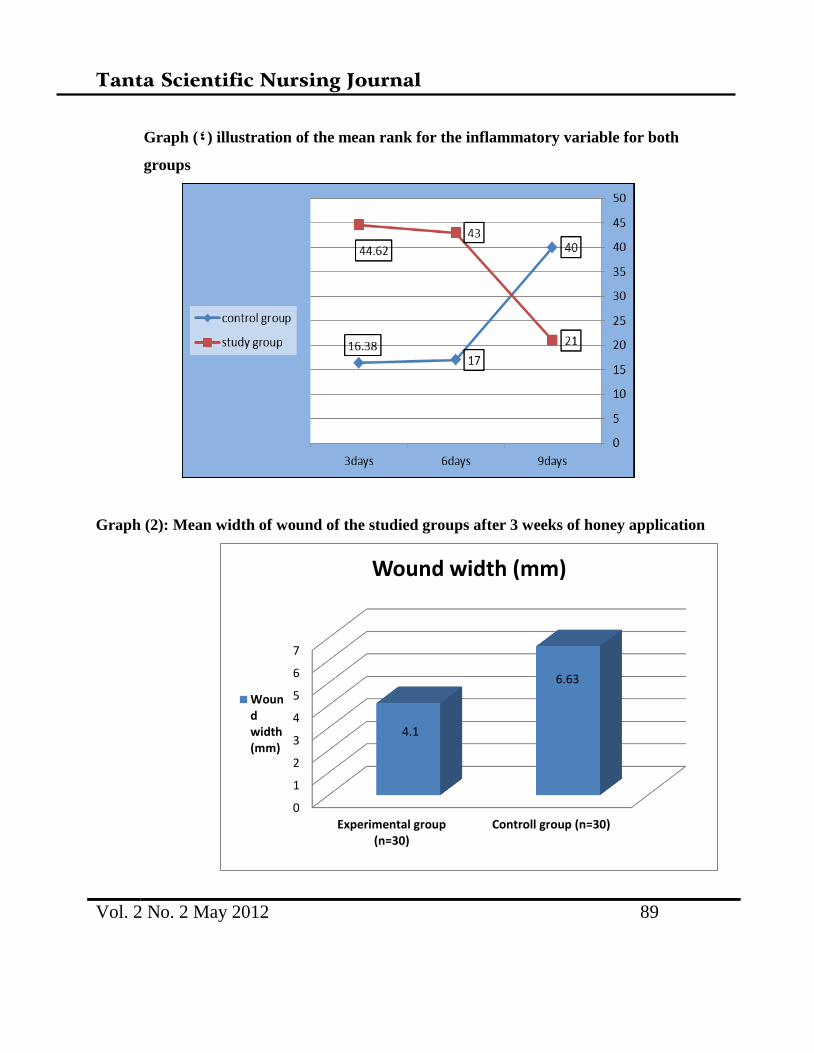
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 89
Graph (4) illustration of the mean rank for the inflammatory variable for both
groups
Graph (2): Mean width of wound of the studied groups after 3 weeks of honey application
0
1
2
3
4
5
6
7
Experimental group(n=30)
Controll group (n=30)
4.1
6.63
Wound width (mm)
Woundwidth(mm)
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 90
Discussion
Socio-demographic data include age,
education, occupation, smoking, income,
and residency. As determined in the
study criteria all women were in
childbearing period but the current study
revealed that the mean and the standard
deviation of the age were 30.87 and 8.41
years respectively for the study group
and were 35.17 and 9.92 years
respectively for the control group. Most
of study group and control group were
illiterate. As known from our previous
experience, most of the university
patients are poor and with low level of
education. This was clear in the present
study as the majority of subjects were
housewives, live in rural area and their
income was less than enough. (El-
Zanaty & Ann, 2008) (8)
.
In the present study, obesity was the most
determent grade representing about two
fifth in the study group and nearly three fifth
in the control group, with considerable
percentages of over-weight in both groups.
This finding is in accordance with
(Nahmias, 2007) (125)
, who stated that, in
2005, both the mean and the median of BMI
increased to about 28. Obesity and
overweight have been increasing in Egypt
over the last decade and are still now at
levels that are even higher than those seen in
the West. Obese women are more at risk of
postpartum complications such as infections,
hemorrhage and embolisms. Taken all
together, maternal mortality and morbidity is
significantly elevated for obese women.
In the present study concerning the
obstetrical history, about half of the two
groups were gravid 3-4, Para 3-4. In
addition to 3-4 as the number of living
children represents the highest
percentage in both groups. The majority
of subjects were not exposed to abortion.
These results approximately match with
the study carried out by Nahmias (2007)
(125). who had extracted the data from the
demographic and health Surveys
conducted in Egypt in 1992, 1995, 2000
and 2005. These are large surveys carried
out periodically and intended to be
uniform to facilitate cross-national
comparisons.
Regarding the types of undergoing
surgery, It was observed that, the
majority of both groups had under gone
cesarean section except about one third
had under gone hysterectomy and only
(3.3%) had under gone oopheroectomy in
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 91
the control group. Also in the present
study, it was observed that the majority
of women delivered vaginally in the last
delivery followed by current cesarean
section. This result is supported by
(Khawaja et al, 2009) (107)
. who reported
that, cesarean rates for hospital-based
deliveries were much higher than the
overall rates, and the rate also increased
slightly from a low level of 15.3 percent
in the 1992 survey to 18.5 percent in the
1995 survey to 20.9 percent in the 2000
survey, representing a 72 percent
increase during the study period.
Although the cesarean section rate was
slightly higher in private hospitals, the
rate also increased consistently in public
hospitals. The present study also revealed
that, only low pfannenestiel incision was
done in all the subjects.
Concerning recognition of surgical site
infections Collier et al (2004) (111)
,
reported that, There are a number of
indicators of surgical site infections;
include redness, tenderness, infected
discharge, a bad smell in the wound, and
fever. The patient may have a faster
pulse rate and faster breathing, in
addition to unexpected pain and/or
tenderness either at the time of dressing
change or reported by the patient even
when the wound dressing is in place.
After careful assessment, it is apparent
that the wound is infected, it is important
to confirm this and identify the causative
organism(s) and possible sensitivities to
antibiotics.
In the present study, the first indicator of
surgical site infections was the increase
of body temperature to 38 oC or more for
24 hours for all cases. Then positive
wound culture for all cases. The third
indicator was the local signs, it was
detected that more than half of wounds in
the study group were erythematized
compared to entire control group.
Although pain was present in all cases of
the two groups, it was different in
severity and quality. While pain was
moderate in the entire study group, it was
mild in about one quarter and moderate
in about three quarters of the subject of
the control group. Pain was intermittent
all over the time. All studied groups were
felt stabbing pain compared to the
control group, half of them were felt
stabbing pain and the other half were felt
aching pain.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 92
In addition, the researcher confirmed
diagnosis of surgical site infections
among the studied subjects (study and
control groups) by wound culture.
Regarding wound culture, it was found
that, the causativeorganisms, Gram –ve
organisms represent two fifth in the study
group and more than three fifth in the
control group while Gram +ve organisms
represent the majority in the study group
and more than a half in the control group.
On the other hand, Staff org. represents
more than three fifth and about one
quarter, Pseudomonas represents one
fifth and nearly two fifth and Proteus
represent represents about half and one
fifth in the study and control group
respectively.
Regarding sensitivity to antibiotic, in the
study group, about one quarter of the
subject was sensitive to Amoxicillin and
one quarter was sensitive to cefotax
compared to one tenth of subjects in the
control group. In addition to more than
two fifth of subjects in the study group
were sensitive to another type of
antibiotics as ciprofloxacin &
levofloxacin compared to four fifth of
subjects in the control group. This
finding is in accordance with Al-Waili’s
and Saloom’s (1999) (3)
who reported
that, Period for antibiotics use was 6.88
+/- 1.7 days in the study group and 15.45
+/- 4.37 in the control group (p <0.05).
They also stated that complete wound
healing was evident after 10.73 +/- 2.5
days in the study group and after 22.04
+/- 7.33 in the control group.
Concerning results of wounds culture, 7
days after honey application, the majority
of study group were negative and less
than two fifth were positive. on the other
hand all the control group (100%) were
positive. This finding is in accordance to
Al-Waili’s and Saloom’s (1999) (3)
who
reported that, eradication of bacterial
infections was obtained after 6 +/- 1.9
days (mean +/- SD) in the study group
using topical honey, and after 14.8 +/-
4.2 days in the control group who didn’t
not use topical honey.
This finding is ascribed to that; honey
provides a moist healing environment and
prevents bacterial growth even when wounds
are heavily infected. Honey is a very
effective mean of quickly rendering heavily
infected wounds sterile, without the side-
effects of antibiotics, and it is effective
against antibiotic-resistant strains of bacteria.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 93
Its antibacterial properties and its viscosity
also provide a barrier to cross-infection of
wounds. (Molan, 2001) (84)
.
Moreover, concerning wound size in the
present study, the wound lengths didn’t
exceed 20 cm in both groups with mean
15.83±2.45 in the study group and
16.37±2.95 in control group. Regarding
width of wound after three week of the
application of honey, it ranged from 3-5
mm in the study group and from 5-8 mm
in the control group with mean
4.10±0.76, and 6.63±0.96 respectively.
This finding is in accordance to Al-
Waili’s and Saloom’s (1999) (3)
who
reported that, Size of postoperative scar
was 3.62 +/- 1.4 mm in the study group
which used topical honey and was 8.62
+/- 3.8 mm in the control group who did
not use topical honey.
In the current study the researcher used a
follow up record to assess prognosis of
infected surgical site. the researcher
categories the time variable to three, six
and nine days, the main objective is to do
a comparison between study group(
women exposed to honey dressing +
routine hospital wound care hospital
wound care) and control group (women
exposed to routine hospital wound care
hospital wound care only) and the results
was as following:
Concerning skin appearance surround
wound. In the first three days the skin
was White or gray pallor in the two
groups, But in the 6th day the difference
in progress started to be clear as more
than three quarter of the study group
become pink and one quarter is bright
red or blanch to touch. Gradually at the
9th
day skin become normal in the study
group. Contingency concerning control
group the majority of Skin appearance
surrounding their wound was Bright red
or blanches to touch and less than one
fifth their wound was White or gray
pallor or hypo pigmented. In addition;
regarding inflammatory response at the
9th
day of management, the inflammatory
response disappeared in the entire study
group. But, most of the control group
their wound was red and less than one
fifth was red with hotness.
Regarding exudates amount there were
significance difference between study
group and control group, the in the
exudates disappeared from the majority
of the study group at the 6th of
management. On the other hand, the
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 94
exudates amounts were moderate in all
the control group. In the 9th,
the exudates
disappeared completely from the study
but still large in the most of the control
group. At the 21st of wounds
managements the amounts of exudates in
the majority of the control group were
very scant except more than one tenth
were large until the 21st of wound
managements.
When exploring the type of exudates
especially at the 9th day of management
the exudates were absent completely in
the study group. During exploring the
control group it was observed that one
third of them were foul purulent ,about
one fifth were purulent, about one fifth
were serous, one fifth were was
Serosanguieous and one tenth was
bloody. In the day 21st still more than
thirteen percentages were purulent and
the majorities were changed to serous.
This may be due to Honey provides a
supply of glucose for leucocytes, which
is essential for the respiratory burst that
produces hydrogen peroxide, which is
the dominant component of the
antibacterial activity of macrophages.
Furthermore the use of honey provides
substrates for glycolysis, which is the
major mechanism for energy production
in the macrophages, and thus allows
them to function in damaged tissues and
exudates where the oxygen supply is
often poor. In addition, the acidity of
honey (typically below pH 4) may also
assist in the antibacterial action of
macrophages, as an acid pH inside the
vacuole is involved in killing ingested
bacteria. Whether it is through this
action, or through preventing the toxic
unionized form of ammonia from
existing that is involved, topical
acidification of wounds promotes
healing. The high glucose levels that the
honey provides would be used by the
infecting bacteria in preference to amino
acids from the serum and dead cells, and
thus would give rise to lactic acid instead
of ammonia and the amines and sulphur
compounds that are the cause of
malodour in wounds. (Leveen et al,
1973) (126)
.
Regarding the wound status, it was
observed that, there were improvements
in the study group throughout six days of
honey application. On the other hand, the
deterioration started to appear in the

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 95
control group, but at the 9th
day, more
than two thirds of control group showed
a slight improvement. Also at the 21st
day, the majority of subjects in the
control group showed a significant
improvement, and less than one fifth of
them their wounds were deteriorated.
This finding is in accordance to Al-
Waili’s , Saloom (2005) (3)
. who reported
that, after using honey, (84.4%) of
patients showed complete wound healing
without wound disruption or a need for
re-suturing and only (4) patients showed
mild dehiscence. In their control group,
(50%) of patients showed complete
wound healing and (50%) of patients
showed wound dehiscence, half of them
needed re-suturing under general
anesthesia (Molan, 2005) (84)
.also
reported that honey used as a wound
dressing has been promoted the
formation of a clean healthy granulation
tissue, promoted epithelialisation of the
wound, Improvement of nutrition of
wounds has been observed, increased
blood flow has been noted in wounds,
and free flow of lymph. Another effect of
honey on wounds has been noted is, it
reduces inflammation and hastens
subsidence of passive hyperemia. It also
reduces edema and exudation, and
absorbing fluid from the wound. This may
be due to that, honey is be expected to have a
direct nutrient effect on regenerating tissue
because it contains a wide range of amino
acids, vitamins and trace elements, in
addition to large quantities of readily
assimilable sugars. The vitamin C content of
honey, which is typically more than three
times higher than that in serum, and may be
many times higher, it could be a particular
importance because of the essential role of
this vitamin in collagen synthesis. In
addition, the high osmolarity of honey causes
an outflow of lymph which serves to provide
nutrition for regenerating tissue which
otherwise can only grow around points of
angiogenesis (seen as granulation). Healing
is delayed if the circulation to an area is
poor, or if a patient is poorly nourished. Also
it has been suggested that, the decreased
turgor resulting from the application of
honey may increase oxygenation of tissues.
In addition, honey gives a fast rate of tissue
regeneration and suppression of
inflammation, oedema, exudation and
malodour in wounds. The antibacterial
properties clearing infection could alone
account for these effects by preventing the
production of the products of bacterial
metabolism which are responsible for the
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 96
contrary conditions. Furthermore, honey has
a direct trophic and anti-inflammatory effect
on wound tissues (Efem, 1988) (127)
.
Regarding pain during wound dressing in
the beginning there were no difference,
but at the 9th
day the pain disappeared in
the study group but in the control group,
there were two third of subjects
complaining from severe pain except
around two fifth of subjects whose pain
was slight. At the 21st day, concerning
the control group, thirteen percent of
subjects were having a severe pain and
the rest were having a slight pain. This
result is in accordance with Molan’s
(2005) (84)
who reported that, honey is
soothing when applied to wounds and
that honey causes no pain on dressing or
causes only momentary stinging. They
also added that honey is non-irritating,
causes no allergic reaction, and has no
harmful effects on tissues. In addition, it
has been noted that, honey dressings are
easy to apply and to remove because
there is no adhesion to cause damage to
the granulating surface of wounds.
Honey also causes no bleeding when
removing dressings. Any residual honey
is easily removed by simple bathing.
Concerning duration of wound management,
the study group did not exceed 11 days in
wound management but the control group
exceeded 21 days. All women in the two
groups were taken antibiotics and analgesics
according hospital routine. This result
matches with Efems’ et al (1988) (127)
who
reported that, the wounds become sterile in 3
- 6 days, or 7 - 10 days after clinical studies
on the usage of honey as a dressing for
infected wounds and with Molan’s who
reported that, the mean hospital stay was
9.36 +/- 1.8 days in group A (treated by
honey dressing) and 19. 91 +/- 7.35 days in
group B (treated according hospital routine).
There is also an economical advantage of
using honey as a wound dressing. This is
seen in the direct cost savings when
compared with conventional treatments
and in the savings in ongoing costs when
consideration is given to the more rapid
healing rates that are achieved. Other
observations on cost savings have been
use of antibiotics ceased, length of
hospitalization reduced by at least half.
To conclude that, various studies on the
usage of honey as a dressing for infected
wounds have reported that, the wound
become sterile in 3-10 days. Honey used as
wound dressing has been reported to
promote the formulation of clean healthy

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 97
granulation tissue. It has also been reported
to promote epithelialisation of the wound
and rapid growth of new tissue is
remarkable. Inflammation, swelling and pain
are quickly reduced, odor is reduced,
sloughing of necrotic tissue is induced, and
healing occurs rapidly with minimal
scarring. Improvement of wounds nutrition
has been noted in addition to free flow of
lymph. Finally, topical honey dressing as
alternative method of managing abdominal
surgical site infections provides a specific
desirable affects (Ahmed, 2003) (89)
.
Conclusion
Based on the findings of the present
study, the researcher can conclude that
topical application of sterile honey could
eradicate organisms within a short period of
time, reduce the period of antibiotic use,
accelerate the healing process in a unique
and an economic way, result in minimal
scar formation, prevent wound dehiscence
and the need for re-suturing
Recommendation:
-Mass media should be utilized for the
dissemination of simple, correct and
relevant information about honey
dressing for infected wound.
-The use of standardized scale for
measuring surgical wound healing must
be an integral part of surgical wound
managements
-Herbal management of surgical site
infections should be included in the
curricula of basic nursing education and
continuing education in variable nursing
educational settings.
-Appropriate and accessible public services
which include information, education
and counseling about herbal management
of surgical site infections must be
included in the health care delivery
system.
Recommendations (Suggestion) for further
studies:-
Studies to find out factors that affect the
dissemination and implementation of up
to date information about complementary
therapy for surgical site infections.
- Replication of the present study at
different settings and among different
samples of selected high risk women for
surgical site infections.
- Studies about the effect and techniques
of complementary therapy on surgical
site infections.
- The study need to be conducted on a
larger sample and be extended for a
longer period of time to allow

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 98
generalization of the results. 6- The study
can be conducted on any age of women,
any post operative abdominal obstetrical
or gynecological patients, women with
medical disorder as cardiac failure,
chronic respiratory problems, vascular
disorders, diabetes, renal and liver
insufficiency, patients with hemoglobin
≤8 mg/ml, and patient receiving drug
therapies which interfere with wound
healing as chronic steroid therapy,
imunosuppressant drugs, and
anticoagulants.
References
1-Gibbons L., Belizán J. M., Lauer J. A.,
Betrán A. P., Merialdi M. & Althabe F.
World Health Report Background Paper:
The Global Numbers and Costs of
Additionally Needed and Unnecessary
Caesarean Sections Performed per Year:
Overuse as a Barrier to Universal
Coverage, (2010). Available at
http://www.who.int/healthsystems/topics/
financing/healthreport/30C-
sectioncosts.pdf. Last accessed on 10th
Feb 2012.
2- Shetty Jyothi, Vyas Neetha M, Kumar
Pratap, Kamath Asha. Antibiotic
prophylaxis for hysterectomy and
cesarean section:Amoxicillin-clavulanic
acid versus cefazolin:J Obstet Gynecol
India Vol. 60, No. 5 : September /
October , 2010; pp 419 - 423.
3-Al waili, N., S., Saloom, K., Y. Effects of
topical honey on post-operative wound
infections due to gram positive and gram
negative bacteria following caesarean
sections and hysterectomies. European
journal of medical research, 1999 ; 4 (3):
pp 126-130.
4- Salah, R. Ahmed, Mostafa A. A. Ellah,
Osman A. Mohamed, and Hesham M.
Eid, Prepregnancy Obesity and
Pregnancy Outcome, Department of
Obstetrics & Gynecology, Sohag
University Hospital, Egypt, International
Journal of Health Sciences, 2009; Jul;
3(2)203-208.
http://www.ncbi.nlm.nih.gov/pmc/article
s/PMC3068823/
sited at 15 jul 2012
5-World Health Organization (WHO).
WHO Guidelines on Hand Hygiene in
Health Care. Geneva, Switzerland: 2009;
WHO Press. Available at:
http://whqlibdoc.who.int/publications/20
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 99
09/9789241597906_eng.pdf. Accessed
October 12, 2010.
6- Jyothi S., Neetha V., Pratap K., Asha K.
Antibiotic prophylaxis for hysterectomy
and cesarean section: Amoxicillin-
clavulanic acid versus cefazolin. J Obstet
Gynecol India, 2010; (60) 419 - 423.
7- Ministry of Health and Population Egypt
(MOHP). Standards of practice for
integrated maternal and child health and
reproductive health services, First
edition, Infection Control Department,
2005;MOHP Egypt. Available at
http://pdf.usaid.gov/pdf_docs/PNADF09
2.pdf. Last accessed on 25th January
2012.
8- El-Zanaty, F. & Ann, W. Egypt
Demographic and Health Survey. Kasr
Al-Aini Journal Of Obstetrics &
Gynecology, 2008; Egypt Ministry of
Health. Available at
http://www.measuredhs.com/pubs/pdf/F
R220/FR220.pdf. Last accessed on 26th
January 2012.
9- Spry, C. Essentials of perioperative
nursing. Jones & Bartlett Learning, 2009,
pp214
10- MOLAN, P .Mode of action, In White,
R; Molan, P; Copper, R (eds) Honey: A
modern wound management product,
Wounds UK; Aberdeen, 2005; pp 1-23.
11- Banister, E., Schreiber, R. The tyranny
of consensus: Implications for nursing
education. International Journal of
Nursing Education Scholarship, 2004;
1(1). Retrieved from
http://www.bepress.com/ijnesnaty. Last
accessed on 22/10/2011.
12- Pillitteri, A. Maternal & child health
nursing care of the childbearing and
childrearing family, 4th
ed., USA,
Lippincott Williams& Wilkins, 2003; Pp
540-49,552-57,596-98,604-6.
13- Nettina, S. Lippincott manual of
nursing practice. (9th ed. ed.). Ambler, PA:
wolters kluwer/lippincott Williams, 2010;
p.212.
14- World Health Organization (WHO).
Traditional medicine,(2008; Fact sheet
N°134
15- World Health Organization (WHO).
Prevention of hospital-acquired infections
A practical guide, 2nd edition. 2002;
Available at
http://www.who.int/csr/resources/publica
tions/whocdscsreph200212.pdf
16- Nahmias, P. Trends in the prevalence
of overweight among women in Egypt.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 100
Vol. 33, Iss. 3, 01 oct. , 2007; pp 108 -
110
17- Khawaja, M., Choueiry, N., Jurdi R.
Hospital- based caesarean section in the
Arab region: An overview. Eastern
Mediterranean health Journal, 2009;
15(2). Pp 459.
18- Collier M., Recognition and
management of wound infections,
Published: Jan 2004.
http://www.worldwidewounds.com/2004
/january/Collier/Management-of-Wound-
infections.html Last Modified: Monday,
18-Oct-2004 14:11:49 BST
19- Culligan, P., J., Kubik, K., Murphy, M.,
Blackwell, L., Snyder, J. A randomized
trial that compared povidone iodine and
chlorhexidine as antiseptics for vaginal
hysterectomy. Am J Obstet Gynecol,
2005; 192(2): pp 422-425.
20-Leveen, H.,H., Falk, G., Borek, B.,
et al. Chemical acidification of wounds:
an adjuvant to healing and the
unfavorable action of alkalinity and
ammonia. Ann Surg., 1973;178(6): pp
745–753
21- EFEM, S. E. Clinical observations on
the wound healing properties of honey
183. British Journal of Surgery, 1988;
75: 679-681. 22- Centers for Disease
Control and Prevention (CDC). (2012).
Frequently Asked Questions about
Surgical Site Infections. Available at
http://www. cdc.gov/HAI/ssi/
faq_ssi.htm l#a1. Last accessed on 25th
January 2012.
Effect of Nursing Intervention on the Supportive Role Played by Peers on Glycemic
Control Among Diabetic School Students in Tanta City.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 101
Bassima Ezat Gowayed
Community Health Nursing –Tanta University
Ikbal Fathala Elshafay
Community Health Nursing –Tanta University
Latifa Mahmod Foda
Community Health Nursing –Tanta University
Lulah Abd Elwahab Abd Elaty Hassan
Abstract:
Diabetes mellitus is one of the most common metabolic and chronic diseases of school age
children. The main aim of diabetes management for diabetic teenage is to achieve optimal
glycymic control. Peer support may help achievement of this aim. Aim: is to investigate the
effect of nursing intervention on the supportive role played by peers on glycymic control among
diabetic school students in Tanta city. Research design: Quasi-experimental research design.
Material and method: The study was conducted at the outpatient medical clinics of all school
health units (I, II, and III) affiliated to the students’ health insurance serving Tanta city as well
as governmental schools. A convenient sample of diabetic school children were selected from
the previous settings representing fifty percent of the total subjects. The study sample was
divided into two equal groups (control& study). The control group received an individual
program for glycemic control. The study group received the same glycemic control program in
addition to peer support sessions. An interview questionnaire and anthropometric measurements
sheets were used to collect data and for evaluation. They were used three times during the study
period; before the program, immediate, and three months post program. Results: the result of
this study showed that before implementation of the program the study and control groups
showed poor glycemic control, low scores of knowledge, self care practices and perceived peer
support. After implementation of the program, the two groups showed significant glycemic
control and improvement in their knowledge and self care practices. This improvement was
highly significant among the study group who received peer support than the control one.
Conclusion and recommendation: peer support approach is a predictor of glycemic control
among school age children. Therefore, the school health nurse could do her best effort to make
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 102
peer support available to every diabetic student, in particular, those with poor glycemic control
or newly diagnosed.
Introduction
Diabetes mellitus is one of the most
common metabolic and chronic diseases of
school age children (1)
. There are two main
types of diabetes mellitus. Type 1 diabetes
also called insulin dependent diabetes or
juvenile diabetes. The average age of its
onset is 10 to 14 years. It is autoimmune
disorder in which the body destroys the
insulin- producing islet cells in the
pancreases of those who are genetically
vulnerable. Environmental and genetic
factors are strongly implicated. This is the
most prevalent type among children (2, 3)
.
The International Diabetes Federation
(IDF) reported that, every day more than
200 children are diagnosed with type 1
diabetes. It is increasing at a rate of 3%
each year among children and rising even
faster in pre-school children at a rate of 5%
per year. Currently, over 500,000 children
under the age of 15 live with
diabetes(4)
.Approximately 5% of children
have a first or second degree relative with
DM type 1. In the United States, surveys
indicated the prevalence of type1 DM to be
14.9 per 100000 in 2004. The frequency
increases with age (2).
The International Diabetes Federation
(IDF) mentioned that, Egypt is in the
world's top 10 in terms of highest number
of people with diabetes in 2003 (3.9
million) and highest projected number of
people with diabetes in 2025 (7.8 million).
Also, the prevalence rate of diabetes is as
high as 20% in the United Arab Emirates,
16% in Qatar and 15% in Bahren(5). In
Egypt (2005) the prevalence of diabetes
among children aged 10 to 18 was 0.7 per
cent. The frequency was higher among
females than males and equal in urban and
rural areas. Children with fasting blood
glucose levels between 100mg and 125mg
were considered pre-diabetic; they
represented 16.4 per cent of the total
sample (6)
.
Type 1 diabetes is a challenging disease,
with a daily regimen that include multiple
insulin injections, monitoring of blood
glucose level, and a special diet and
exercise regimen. Treatment management
is very difficult, especially for school age

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 103
children who are experiencing a series of
social, psychological, emotional and
physiological changes(7,8)
. Diabetes
management is complicated because it
must occur across different settings such as
at home and in school. Consequently,
diabetes management should be facilitated
by the support of both family members and
peers(9)
.Peer support among patients with
the same chronic health problem may be a
particularly potent intervention, combining
the benefits of both receiving and
providing social support. “Peer support” is
defined as “support from a person who has
experiential knowledge of a specific
behavior or stressor and similar
characteristics as the target population”.
Peer support helps reduce problematic
health behaviors, depression, and
contribute to improve diabetes
management, including improving
behaviors related to medication adherence,
diet, exercise, and blood glucose
monitoring. The success of peer support
appears to be due to the nonhierarchical,
reciprocal relationship that is created
through the sharing of similar life experi-
ences(10)
.The child's concept of self is
shaped by relationship with others. Peers
play an important role in the approval and
critiquing of skills of school-age children.
Continuous peer relationship provide the
most important social interaction for
school age children. Valuable information
are learned from interaction with children
of their own age(11)
.
Working with groups is an important
community nursing skill. Groups are an
effective and powerful way to initiate and
implement changes for individuals,
families, organization, and community.
Moreover, groups can be used to
disseminate health information in a cost-
effective way to a number of clients who
meet together: for instance, individuals
with diabetes can brought together to
consider diet management, physical care
and to share in problem- solving
remedies(12)
. The nurse's role with this
support group is to facilitate group
interaction and to serve as a role model of
acceptance (13)
.
Aim of the study The aim of this study is
to:- Identify the effect of nursing
intervention on the supportive role played
by peers on glycym control among diabetic
school students in Tanta city.
Subjects and methods :

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 104
Study design:-This study was a quazi
experimental study.
Subjects:- A convenient sample of diabetic
school children was selected from health
units affiliated to the students' health
insurance serving Tanta city. The study
was conducted at the out patient medical
clinic of the all school health units (I, II,
and III) in Tanta city, representing half of
the diabetic students in the school health
units.
Study population and sampling: The field
work of this study was done in nine months
starting from March to November 2010.
Each student of the studied sample was
informed about the program objectives, as
well as the time schedule in order to obtain
their active participation and cooperation
during implementation of the intervention.
Then the pretest was fulfilled from each
student. The program sessions were 11
sessions for group I with two additional
sessions for group II. The duration of each
session was 30-60 minutes.
Inclusive criteria: Age from 10- 18
years, had no other chronic disease. The
child was enrolled in governmental school
in Tanta city.
The total study sample was 40 diabetic
school children. The study sample was
divided into two equal groups (20 students
each). Group I (control group):- Each
student in this group will receive an
individual program for glycemic control.
Group II (study group):- This group was
divided into 4 subgroups (5 students in
each). Each group received the glycemic
control program in addition to additional
two sessions for social group support for
each other.
Ethical consideration: 1- Official
permission to conduct the study will be
obtained from the responsible authorities
(Ministry of Education and Health
Insurance).\Consent of the diabetic
children and their parents were obtained.
The researcher meet with the diabetic
children at their schools according to the
convenient time. All participants was
informed about the purpose, benefits, and
procedure of the study.
A pilot study was carried out on four
diabetic students(10% of the study sample)
Tools of the study:-
Tool I:- An Interview Questionnaire
Schedule: It included four parts:-
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 105
Part 1: Sociodemographic characteristics
of the diabetic children: This included
three items as follows:- (a)- Personal data
about the diabetic students, (b)- Students'
parents data, and (c)- Past medical history
of students and their family.
Part 2: Diabetic Educational Assessment
Tool (DEAT):- This tool was developed
by the researcher to assess diabetic
children's knowledge and practice about
diabetes. It will cover the following areas;
definition of diabetes mellitus and its
manifestations, complications,
management such as diet, exercise,
medications, medical follow up and health
promotion, how to prevent injuries and
activities of daily living.
3Part 3: Diabetic Support Assessment
(DSA):-
This tool was adapted from "Medical
Outcomes Study Social Support Survey
Instrument", for the Advancing Diabetes
Self Management Project at the clinic of
Raza( 14)
. It assess the availability for
social support for diabetic patients. It was
modified by the researcher to suit school
children. It was used to assess children's
needs for support in dealing with diabetes.
Part 4: Self- Care Inventory (SCI):
The self care inventory, is a 13 items
self report measure. It was developed by
La Greca (1988) (15)
to assess patient
perceptions of the degree to which they
adhere to treatment recommendations for
their diabetes self care. The instrument was
subsequently revised and now consists of
14 items. The SCI is a likert type scale
ranged from 1-5. It includes items that
focus on blood glucose testing, insulin and
food regulation, exercise and emergency
precautions. The researcher translated this
scale into Arabic language to introduce it
to the study subjects.
Tool II: Measurement sheet:- This
consisted of two parts:-
Part 1: Anthropometric measurements : It
included height, and weight and then
calculation of body mass index. These
measures were done at the beginning of
the study. Then, weight was measured
every month for three months after the
application of the intervention. The body
mass index (BMI) was calculated as
follows:
Part 2: Fasting blood glucose test:- The
fasting blood glucose level of each
participant student was tested by using
him/ her own one touch apparatus.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 106
Developing the nursing intervention
program
1- Preparatory phase:-
–Rational: Studies carried out on Egyptian
diabetic adolescents at Alexandria city
revealed that, although they had a good
knowledge about DM they showed partial
adherence to diabetes self care (16,17)
. About
74.8% of diabetic students had
uncontrolled diabetes and 7.4% of them
developed complications (17)
.
-Analysis of the resources:
Human resources:- The program was
totally carried out by the researcher.
Non human resources (audiovisual
material).It included booklet, power point
sides, doll, and real material (e.g. one
touch blood glucose check apparatus and
its strips, syringe, cotton, and alcohol) to
demonstrate procedures related to DM
management like insulin injection and
blood glucose test. The booklet and power
point were prepared by the researcher
based on literature review. The booklets
were distributed to the studied sample at
the end of sessions and the power point
was presented according to students' level
during each session as needed.
2- Planning phase:-
1- General objectives:
The general goal of the nursing
intervention is to enable the diabetic
students to control their diabetes.
2- Specific objectives:-
The program sessions was 11
sessions as follows for group I with two
additional sessions for group II. Specific
objectives of the intervention and its
sessions was as follows:- Session 1:The
aim of this session was to orient the
students about the importance of the
program, its sessions and expectation of
each session. Session 2:- The aim of this
session was to increase students'
knowledge about the disease related to its
causes and manifestations. Session 3:This
session aimed to allow students to identify
steps of how to calculate the diabetic diet
and how to improve it. Session 4The goal
of this session was to increase students'
awareness about how to mange diabetes
through exercise. Session 5:- The purpose
of this session was to inform the
participants about diabetic medication, its
type and its administration. Session 6:- The
objective of this session was to enable
students manage insulin administration and
site rotation. Session 7:- The aim of this
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 107
session was to enable students practice
blood glucose testing & interpret its normal
and abnormal values. Session 8:- The goal
of this session was to increase the students'
awareness about signs and symptoms of
hypoglycemia and hyperglycemia and
proper dealing with them. Session 9:- The
aim of this session was to discuss with the
group the probable complications that may
arise from uncontrolled diabetes (short
term& long term). Session 10:- The
purpose of this session was to help the
participants to identify the behaviors and
activities that promote their health and
prevent injuries. Session 11:-The objective
of this session was to encourage the
diabetic students to deal constructively
with decisions related to their disease and
glycemic control.
The sessions for group II was as sessions
for group I, in addition to the following
two sessions. These two sessions will be
given to the students after the orientation
session.
Session 1:- The aim of this session is to
help the individual student and all group
members to establish relationship with
each other and with the researcher. Session
2:-:The purpose of it is to enable the
participants to develop social support skills
that help them to manage their diabetes
properly.
Implementation of the program:-
The implementation of the program was as
follows:-
Group I (control group):- Implementation
of the program was based on providing
individual instructions to each student and
discussing problems encountered during
management of the disease. Group II
(study group):- Instructions was provided
in a form of group discussions. Each
student in the group will be encouraged to
express oneself, share problems, concerns
and way of management. The researcher
will act as a facilitator for the group
interaction by providing support,
clarification, interpretation and positive re-
enforcement. discussion, simulation and
demonstration will be used as a teaching
strategy. Hand outs, booklets and power
point presentation will be used as a
teaching aid
Result
Table 1 showed the distribution of the
studied sample regarding to their
sociodemographic characteristics. The
table revealed that the mean age of the
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 108
study group was 15.75±1.74 years while
the mean age of control group was 14.40
±2.91 years. The table also illustrated that
50% and 55% of the study group and
control group respectively were females.
As regard to the educational level, 70% of
the study group and 50% of control group
were students at secondary schools
compared to 30% of both groups were
from preparatory schools.
Concerning birth order, the table showed
that those who were the first or the second
child in the family constituted the highest
percentage of the study and control group
70% and 60% respectively. This is
followed by 20% and 30 % respectively of
both groups who were the third on birth
order. Half of the students of the study
group had five or more siblings compared
with the majority of the control group. The
highest percentage of students (85%) of
both groups was from urban areas.
As regard fathers' education, 35% of
the study group and 25% of the control
group their fathers were university
graduates, and 30% of the students from
both groups their fathers had secondary
education. In relation to mothers’
education, the same table revealed that
(40%) of the study group their mothers
were university graduates, compared with
25% of the control group. More than half
(55%) of the control group their mothers
had secondary education, compared with
35% of the study group. About two thirds
(65%) of both groups their mothers were
housewives. In addition, the table revealed
that only one quarter (25%) of the study
group and one fifth of the control group
had consanguinity between their mothers
and fathers.
Table (2) showed the distribution of
the studied sample regarding personal and
family history of disease. It was observed
that, three quarters (75%) of both groups
had a family history of diabetes mellitus.
Concerning the duration of diabetes
mellitus among students, the mean duration
of disease among the study group was
4.20±3.05 years compared with 4.07± 2.36
years for the control group. Three quarters
(75%) of both groups admitted previously
to hospital because of diabetes mellitus.
However, one quarter (25%) of the study
group reported complications of diabetes.
Table (3) showed the mean score &
standard deviation of knowledge of the
studied sample about diabetes mellitus. It
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 109
was observed that there was a significant
improvement in the mean score of
knowledge of the study group and control
groups about diabetes mellitus (definition,
predisposing factors, manifestation,
accurate blood glucose level,
complications, hypoglycemia, and
hyperglycemia) (P˂ 0.05).The highest total
mean score of knowledge of the study and
control groups was noticed immediately
post program (42.95±6.19 and 41.45±5.86
respectively). There was a significant
difference between the two groups at three
months post program as regard the
definition, accurate blood glucose level,
and complications of diabetes, as well as
the total mean score (X2
= 2.787,
Table (4) showed the mean score and
standard deviation of knowledge of the
studied sample about management of
diabetes mellitus. There was a significant
improvement of the mean score of
knowledge of the study and control groups
for all the studied items (P˂ 0.05). There
was a significant difference between the
two groups at three months post
intervention as regard treatment of diabetes
(t=2.127), types of insulin (t=3.793),
importance of adherence to diabetic diet
(t=2.494), and the importance of exercise
(t=2.494).The study group had a higher
means score of knowledge than the control
group about diabetes management
immediately post program (25.95±2.56 and
24.55±4.65 respectively) and three months
post program (26.59±1.87 and 23.90±4.40
respectively). There was a significant
difference between the two groups through
the study (pre, immediate, and three
months post program) (P˂0.05).
Table (5) showed the total mean
score of knowledge of the studied sample
about diabetes mellitus. The table revealed
that, there was a significant improvement
in the total mean score of knowledge for
both groups through the study period.
However, the study group gained higher
mean score than the control group
immediately post program (68.9±8.75 and
65.89±10.51respectively) and three
months post program (69.14±6.43 and
62.3±12.51 respectively). There was a
significant difference between the two
groups through the study periods (pre,
immediate, and three months post program
(P˂ 0.05).
Table (6) showed the mean score & standard
deviation of the studied sample regarding self
care inventory through the study. There was a

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 110
significant improvement in the mean score of
self care items among the study and control
group in relation to blood glucose
testing(P=0.009 and P=0.010 respectively),
recording(P=0.008 and P=0.007 respectively),
changing insulin dose according to blood
glucose level (P=0.001 and P=0.006
respectively) adherence to diabetic diet
(P=0.044 and P=0.012 respectively), carrying
sweaty foods to manage hypoglycemia
(P=0.001 and P=0.017respectively), and
practicing exercise regularly (P=0.044 and
P=0.037 respectively). Moreover, the table
illustrated that, there was a significant
improvement in the mean score of the study
group regarding eating snakes
regularly(P=0.001), while the improvement of
the control group was not significant(P=0.273).
On the other hand, there was a non significant
improvement in the mean score of self care
items among the study and control group in
relation to talking accurate insulin dose
(P=0.102 and P=0.130 respectively), talking
accurate insulin dose on the right time, eating
meal at times(P=0.317 and P=0.052
respectively), medical follow up (P=0.170 and
P=0.186 respectively), and practicing exercise
strenuously(P=0.058 and P=0.141
respectively). It was also observed that there
was no significant improvement in the mean
score of ketones testing among the study and
control group (P=0.946 and P=0.530
respectively).
Moreover, there was a significant
difference between the two groups regarding
all self care inventory items three months post
program except for ketones testing (P= 0.206).
Table (7) showed the correlation between
knowledge, Self- Care Inventory, diabetic peer
support, performed steps in measuring blood
glucose level and injecting insulin by pen
among the studied sample (study and control
groups) immediately post-test. The table
illustrated that, there was positive correlation
between the knowledge of the study group and
Self- Care Inventory (P=0.019), measuring
blood glucose level(P=0.044), injecting insulin
by pen(P=0.012) and fasting blood glucose
level(P=0.04 Table (8) showed correlation
between knowledge, Self- Care Inventory,
diabetic peer support performed steps in
measuring blood glucose level and injecting
insulin by pen among the studied sample
(study and control groups) 3 months post-test.
The table revealed that, there was a significant
positive correlation between the knowledge of
the study group and Self- Care Inventory
(P=0.001), diabetic peer support (P=0.026),
measuring blood glucose level(P=0.038),
injecting insulin by pen(P=0.023) and fasting
blood glucose level(P=0.005). There was also a
positive correlation between the same group's
Self- Care Inventory and diabetic peer support
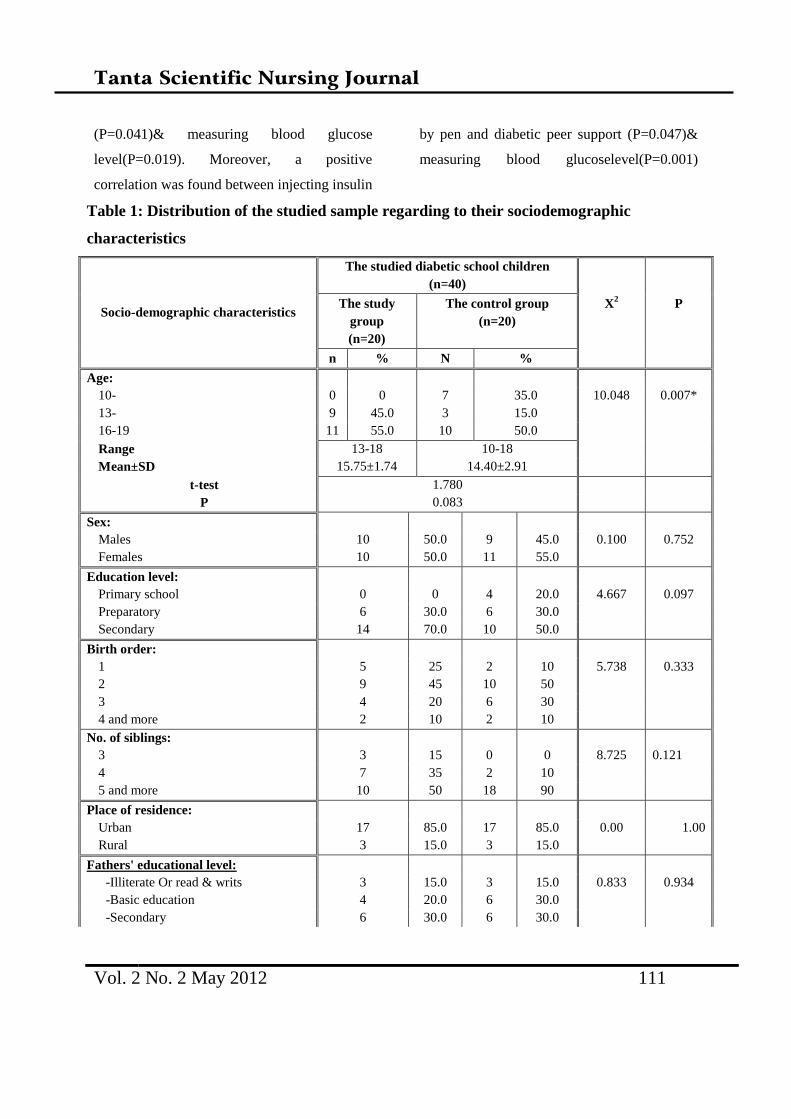
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 111
(P=0.041)& measuring blood glucose
level(P=0.019). Moreover, a positive
correlation was found between injecting insulin
by pen and diabetic peer support (P=0.047)&
measuring blood glucoselevel(P=0.001)
Table 1: Distribution of the studied sample regarding to their sociodemographic
characteristics
Socio-demographic characteristics
The studied diabetic school children
(n=40)
The study
group
(n=20)
The control group
(n=20)
X2 P
n % N %
Age:
10- 0 0 7 35.0 10.048 0.007*
13- 9 45.0 3 15.0
16-19 11 55.0 10 50.0
Range 13-18 10-18
Mean±SD 15.75±1.74 14.40±2.91
t-test 1.780
P 0.083
Sex:
Males 10 50.0 9 45.0 0.100 0.752
Females 10 50.0 11 55.0
Education level:
Primary school 0 0 4 20.0 4.667 0.097
Preparatory 6 30.0 6 30.0
Secondary 14 70.0 10 50.0
Birth order:
1 5 25 2 10 5.738 0.333
2 9 45 10 50
3 4 20 6 30
4 and more 2 10 2 10
No. of siblings:
3 3 15 0 0 8.725 0.121
4 7 35 2 10
5 and more 10 50 18 90
Place of residence:
Urban 17 85.0 17 85.0 0.00 1.00
Rural 3 15.0 3 15.0
Fathers' educational level:
-Illiterate Or read & writs 3 15.0 3 15.0 0.833 0.934
-Basic education 4 20.0 6 30.0
-Secondary 6 30.0 6 30.0
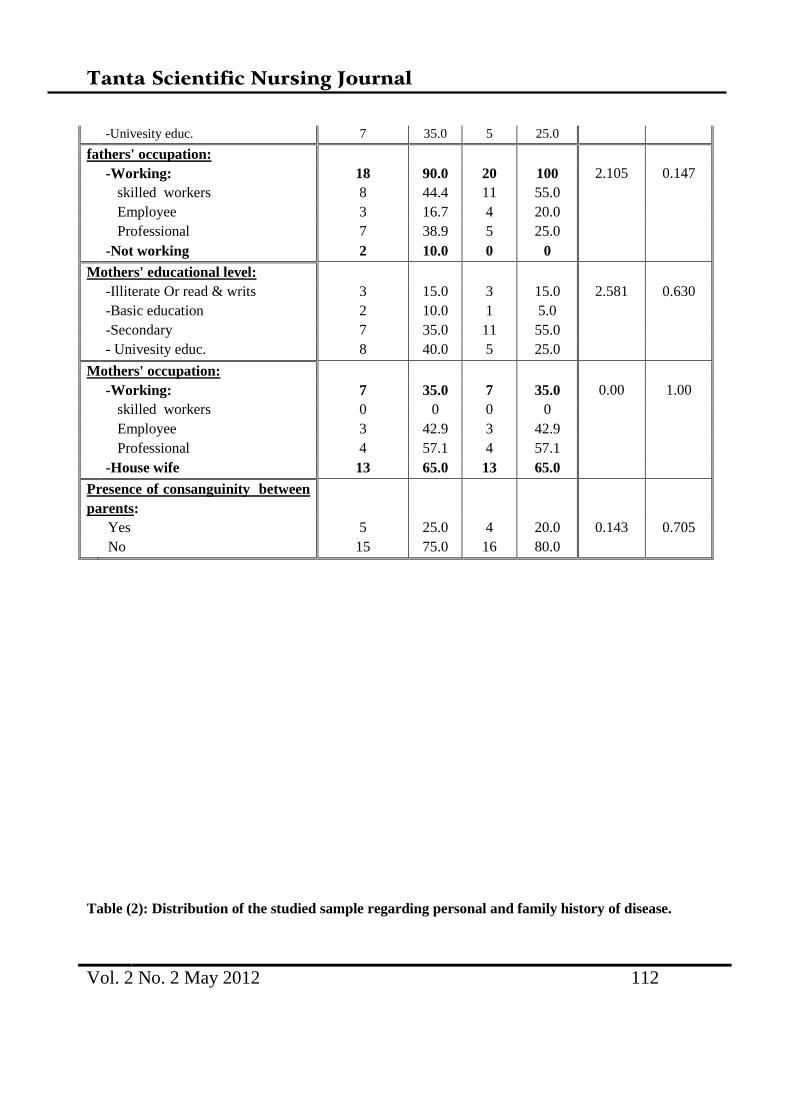
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 112
-Univesity educ. 7 35.0 5 25.0
fathers' occupation:
-Working: 18 90.0 20 100 2.105 0.147
skilled workers 8 44.4 11 55.0
Employee 3 16.7 4 20.0
Professional 7 38.9 5 25.0
-Not working 2 10.0 0 0
Mothers' educational level:
-Illiterate Or read & writs 3 15.0 3 15.0 2.581 0.630
-Basic education 2 10.0 1 5.0
-Secondary 7 35.0 11 55.0
- Univesity educ. 8 40.0 5 25.0
Mothers' occupation:
-Working: 7 35.0 7 35.0 0.00 1.00
skilled workers 0 0 0 0
Employee 3 42.9 3 42.9
Professional 4 57.1 4 57.1
-House wife 13 65.0 13 65.0
Presence of consanguinity between
parents:
Yes 5 25.0 4 20.0 0.143 0.705
No 15 75.0 16 80.0
Table (2): Distribution of the studied sample regarding personal and family history of disease.
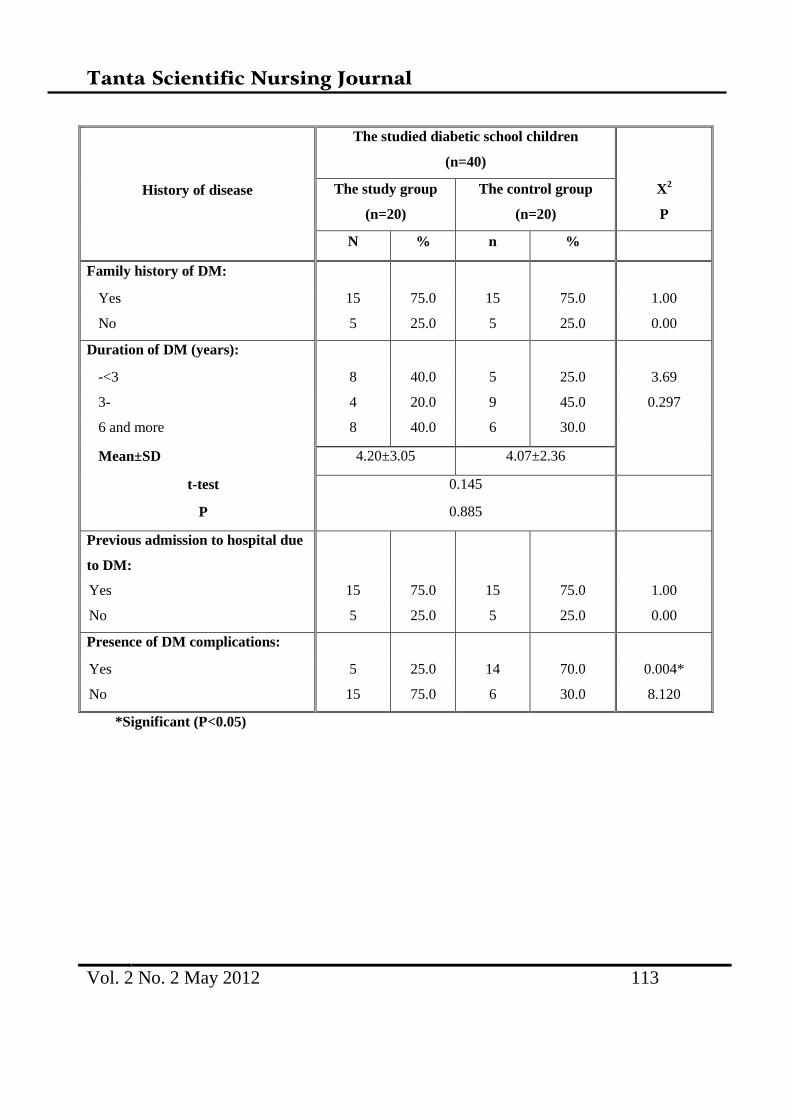
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 113
History of disease
The studied diabetic school children
(n=40)
The study group
(n=20)
The control group
(n=20)
X2
P
N % n %
Family history of DM:
Yes 15 75.0 15 75.0 1.00
No 5 25.0 5 25.0 0.00
Duration of DM (years):
-<3 8 40.0 5 25.0 3.69
3- 4 20.0 9 45.0 0.297
6 and more 8 40.0 6 30.0
Mean±SD 4.20±3.05 4.07±2.36
t-test 0.145
P 0.885
Previous admission to hospital due
to DM:
Yes 15 75.0 15 75.0 1.00
No 5 25.0 5 25.0 0.00
Presence of DM complications:
Yes 5 25.0 14 70.0 0.004*
No 15 75.0 6 30.0 8.120
*Significant (P<0.05)
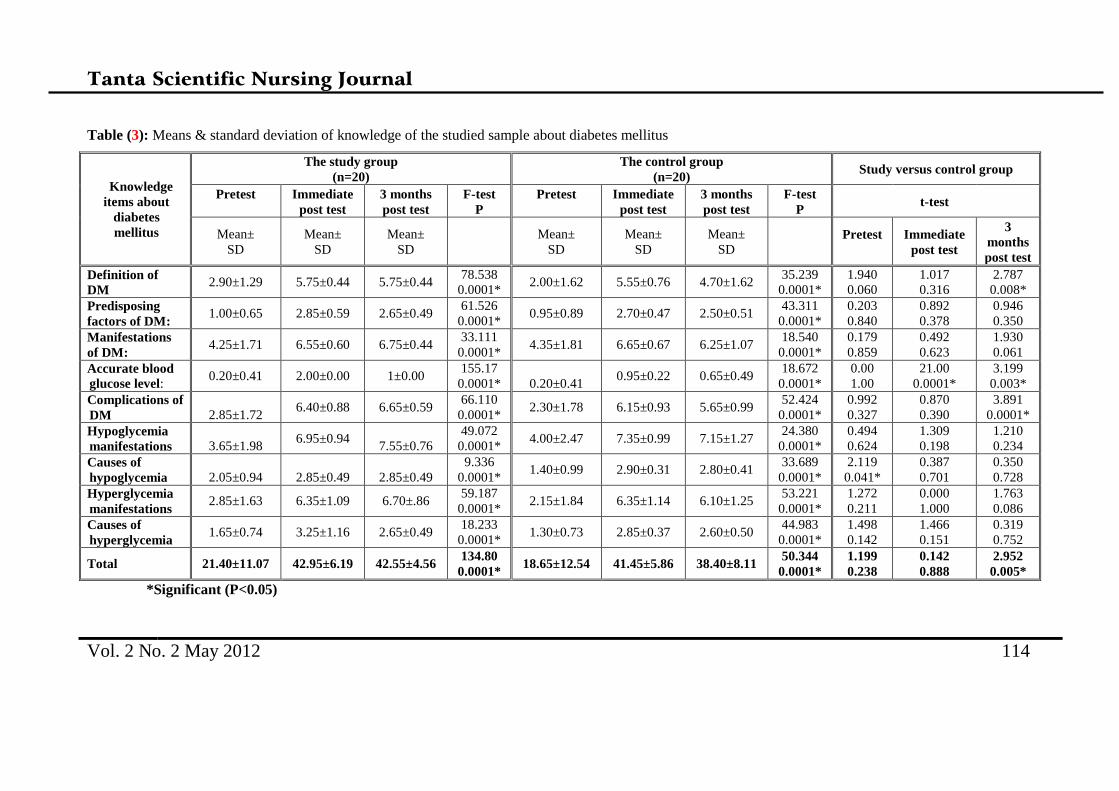
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 114
Table (3): Means & standard deviation of knowledge of the studied sample about diabetes mellitus
Knowledge
items about
diabetes
mellitus
The study group
(n=20)
The control group
(n=20) Study versus control group
Pretest
Immediate
post test
3 months
post test
F-test
P
Pretest
Immediate
post test
3 months
post test
F-test
P t-test
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Pretest
Immediate
post test
3
months
post test
Definition of
DM 2.90±1.29 5.75±0.44 5.75±0.44
78.538
0.0001* 2.00±1.62 5.55±0.76 4.70±1.62
35.239
0.0001*
1.940
0.060
1.017
0.316
2.787
0.008*
Predisposing
factors of DM: 1.00±0.65 2.85±0.59 2.65±0.49
61.526
0.0001* 0.95±0.89 2.70±0.47 2.50±0.51
43.311
0.0001*
0.203
0.840
0.892
0.378
0.946
0.350
Manifestations
of DM: 4.25±1.71 6.55±0.60 6.75±0.44
33.111
0.0001* 4.35±1.81 6.65±0.67 6.25±1.07
18.540
0.0001*
0.179
0.859
0.492
0.623
1.930
0.061
Accurate blood
glucose level: 0.20±0.41 2.00±0.00 1±0.00
155.17
0.0001*
0.20±0.41 0.95±0.22 0.65±0.49
18.672
0.0001*
0.00
1.00
21.00
0.0001*
3.199
0.003*
Complications of
DM
2.85±1.72 6.40±0.88 6.65±0.59
66.110
0.0001* 2.30±1.78 6.15±0.93 5.65±0.99
52.424
0.0001*
0.992
0.327
0.870
0.390
3.891
0.0001*
Hypoglycemia
manifestations
3.65±1.98 6.95±0.94
7.55±0.76
49.072
0.0001* 4.00±2.47 7.35±0.99 7.15±1.27
24.380
0.0001*
0.494
0.624
1.309
0.198
1.210
0.234
Causes of
hypoglycemia
2.05±0.94
2.85±0.49
2.85±0.49
9.336
0.0001* 1.40±0.99 2.90±0.31 2.80±0.41
33.689
0.0001*
2.119
0.041*
0.387
0.701
0.350
0.728
Hyperglycemia
manifestations 2.85±1.63 6.35±1.09 6.70±.86
59.187
0.0001* 2.15±1.84 6.35±1.14 6.10±1.25
53.221
0.0001*
1.272
0.211
0.000
1.000
1.763
0.086
Causes of
hyperglycemia 1.65±0.74 3.25±1.16 2.65±0.49
18.233
0.0001* 1.30±0.73 2.85±0.37 2.60±0.50
44.983
0.0001*
1.498
0.142
1.466
0.151
0.319
0.752
Total 21.40±11.07 42.95±6.19 42.55±4.56 134.80
0.0001* 18.65±12.54 41.45±5.86 38.40±8.11
50.344
0.0001*
1.199
0.238
0.142
0.888
2.952
0.005*
*Significant (P<0.05)
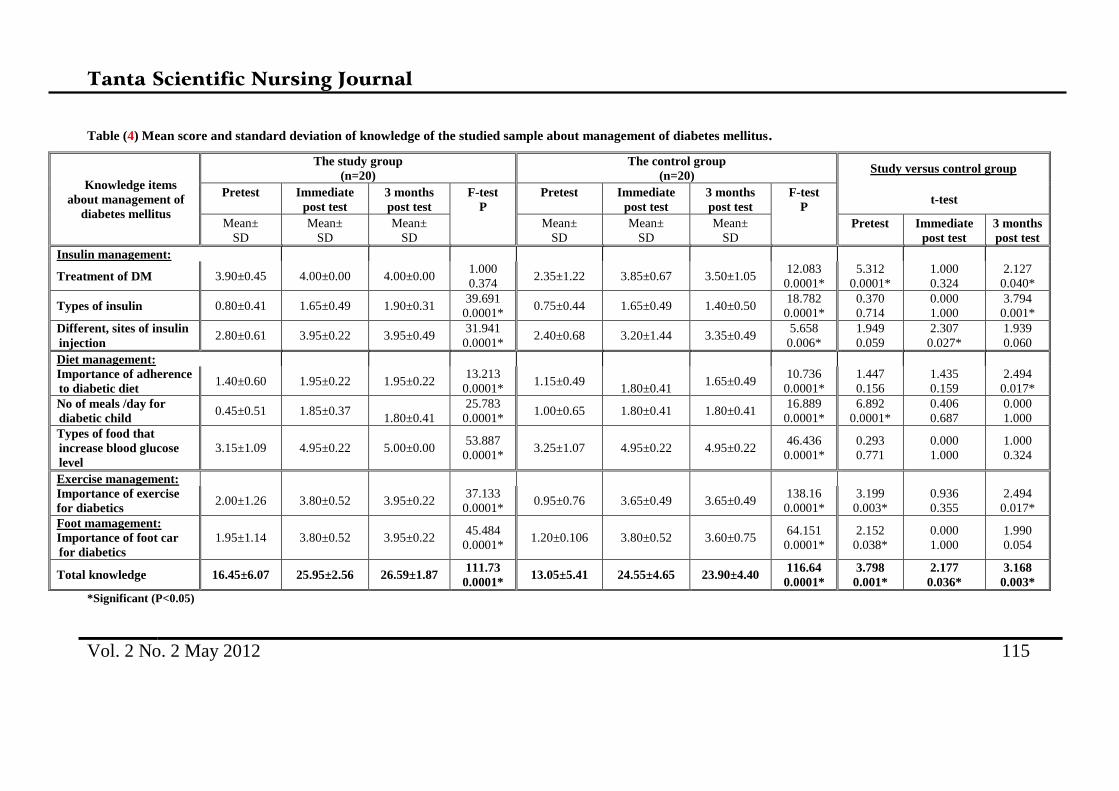
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 115
Table (4) Mean score and standard deviation of knowledge of the studied sample about management of diabetes mellitus.
Knowledge items
about management of
diabetes mellitus
The study group
(n=20)
The control group
(n=20) Study versus control group
Pretest
Immediate
post test
3 months
post test
F-test
P
Pretest
Immediate
post test
3 months
post test
F-test
P t-test
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Pretest
Immediate
post test
3 months
post test
Insulin management:
Treatment of DM 3.90±0.45 4.00±0.00 4.00±0.00 1.000
0.374 2.35±1.22 3.85±0.67 3.50±1.05
12.083
0.0001*
5.312
0.0001*
1.000
0.324
2.127
0.040*
Types of insulin 0.80±0.41 1.65±0.49 1.90±0.31 39.691
0.0001* 0.75±0.44 1.65±0.49 1.40±0.50
18.782
0.0001*
0.370
0.714
0.000
1.000
3.794
0.001*
Different, sites of insulin
injection 2.80±0.61 3.95±0.22 3.95±0.49
31.941
0.0001* 2.40±0.68 3.20±1.44 3.35±0.49
5.658
0.006*
1.949
0.059
2.307
0.027*
1.939
0.060
Diet management:
Importance of adherence
to diabetic diet 1.40±0.60 1.95±0.22 1.95±0.22
13.213
0.0001* 1.15±0.49
1.80±0.41 1.65±0.49
10.736
0.0001*
1.447
0.156
1.435
0.159
2.494
0.017*
No of meals /day for
diabetic child 0.45±0.51 1.85±0.37
1.80±0.41
25.783
0.0001* 1.00±0.65 1.80±0.41 1.80±0.41
16.889
0.0001*
6.892
0.0001*
0.406
0.687
0.000
1.000
Types of food that
increase blood glucose
level
3.15±1.09 4.95±0.22 5.00±0.00 53.887
0.0001* 3.25±1.07 4.95±0.22 4.95±0.22
46.436
0.0001*
0.293
0.771
0.000
1.000
1.000
0.324
Exercise management:
Importance of exercise
for diabetics 2.00±1.26 3.80±0.52 3.95±0.22
37.133
0.0001* 0.95±0.76 3.65±0.49 3.65±0.49
138.16
0.0001*
3.199
0.003*
0.936
0.355
2.494
0.017*
Foot mamagement:
Importance of foot car
for diabetics
1.95±1.14 3.80±0.52 3.95±0.22 45.484
0.0001* 1.20±0.106 3.80±0.52 3.60±0.75
64.151
0.0001*
2.152
0.038*
0.000
1.000
1.990
0.054
Total knowledge 16.45±6.07 25.95±2.56 26.59±1.87 111.73
0.0001* 13.05±5.41 24.55±4.65 23.90±4.40
116.64
0.0001*
3.798
0.001*
2.177
0.036*
3.168
0.003*
*Significant (P<0.05)

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 116
Table (5): Total mean score of knowledge of the studied sample about diabetes mellitus.
Total
Knowledge
scores
The studied diabetic school children
(n=40)
The study group
(n=20)
The control group
(n=20)
Pretest
Immediate
post test
3
months
post test
F-test
P
Pretest
Immediate
post test
3
months
post test
F-test
P
Range 22-61 57-76 66-74 20-61 51-76 42-74
Mean±SD 37.85±17.14 68.9±8.75 69.14±6.43 157.933 31.7±17.95 65.89±10.51 62.3±12.51 92.860
Median 40.00 71.50 71.00 0.0001* 33.50 68.00 66.00 0.0001*
Study vs
Control:
T-test
P
2.153
0.038*
2.240
0.031*
3.261
0.002*
*Significant (P<0.05)
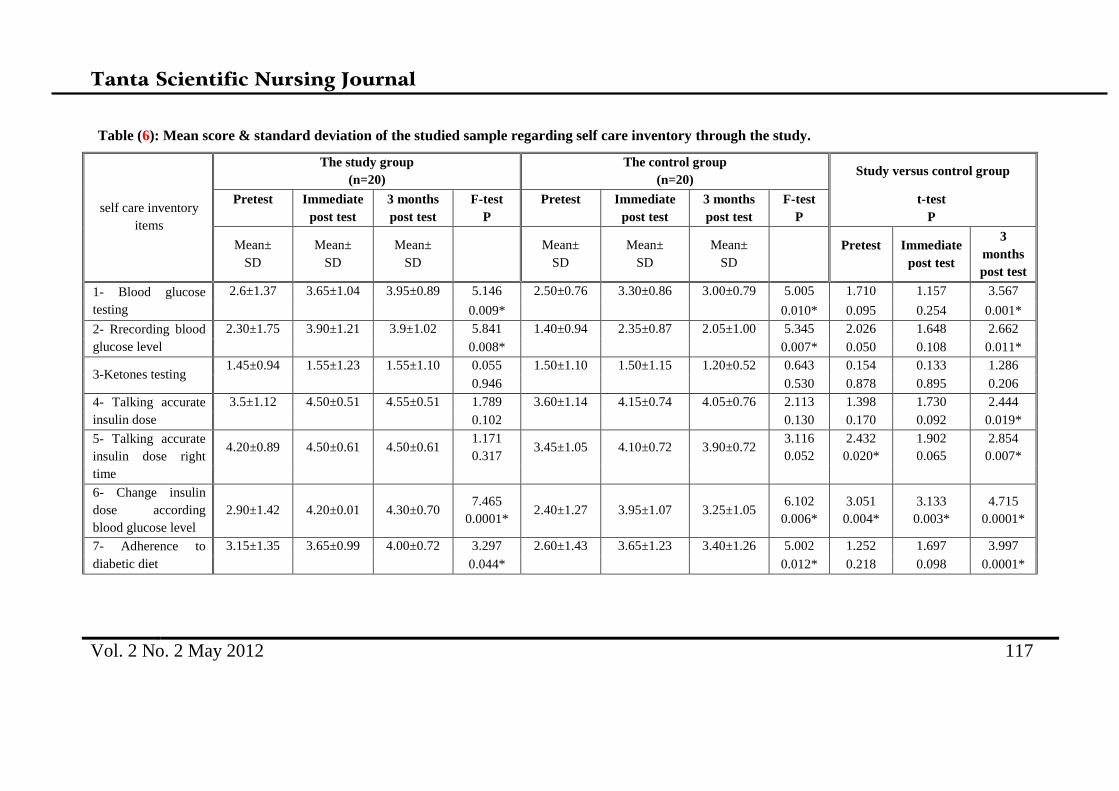
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 117
Table (6): Mean score & standard deviation of the studied sample regarding self care inventory through the study.
self care inventory
items
The study group
(n=20)
The control group
(n=20) Study versus control group
Pretest
Immediate
post test
3 months
post test
F-test
P
Pretest
Immediate
post test
3 months
post test
F-test
P
t-test
P
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Mean±
SD
Pretest
Immediate
post test
3
months
post test
1- Blood glucose
testing
2.6±1.37 3.65±1.04 3.95±0.89 5.146 2.50±0.76 3.30±0.86 3.00±0.79 5.005 1.710 1.157 3.567
0.009* 0.010* 0.095 0.254 0.001*
2- Rrecording blood
glucose level
2.30±1.75 3.90±1.21 3.9±1.02 5.841 1.40±0.94 2.35±0.87 2.05±1.00 5.345 2.026 1.648 2.662
0.008* 0.007* 0.050 0.108 0.011*
3-Ketones testing 1.45±0.94 1.55±1.23 1.55±1.10 0.055 1.50±1.10 1.50±1.15 1.20±0.52 0.643 0.154 0.133 1.286
0.946 0.530 0.878 0.895 0.206
4- Talking accurate
insulin dose
3.5±1.12 4.50±0.51 4.55±0.51 1.789 3.60±1.14 4.15±0.74 4.05±0.76 2.113 1.398 1.730 2.444
0.102 0.130 0.170 0.092 0.019*
5- Talking accurate
insulin dose right
time
4.20±0.89 4.50±0.61 4.50±0.61 1.171
0.317 3.45±1.05 4.10±0.72 3.90±0.72
3.116
0.052
2.432
0.020*
1.902
0.065
2.854
0.007*
6- Change insulin
dose according
blood glucose level
2.90±1.42 4.20±0.01 4.30±0.70 7.465
0.0001* 2.40±1.27 3.95±1.07 3.25±1.05
6.102
0.006*
3.051
0.004*
3.133
0.003*
4.715
0.0001*
7- Adherence to
diabetic diet
3.15±1.35 3.65±0.99 4.00±0.72 3.297 2.60±1.43 3.65±1.23 3.40±1.26 5.002 1.252 1.697 3.997
0.044* 0.012* 0.218 0.098 0.0001*
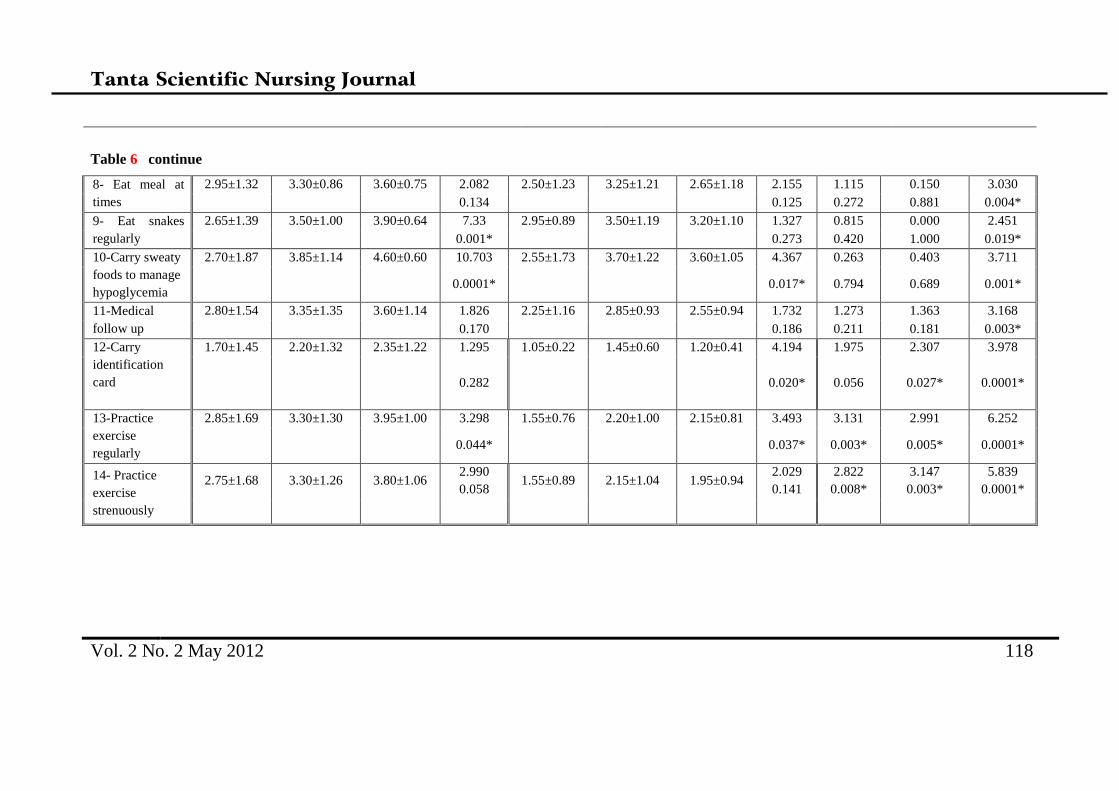
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 118
Table 6 continue
8- Eat meal at
times
2.95±1.32 3.30±0.86 3.60±0.75 2.082 2.50±1.23 3.25±1.21 2.65±1.18 2.155 1.115 0.150 3.030
0.134 0.125 0.272 0.881 0.004*
9- Eat snakes
regularly
2.65±1.39 3.50±1.00 3.90±0.64 7.33 2.95±0.89 3.50±1.19 3.20±1.10 1.327 0.815 0.000 2.451
0.001* 0.273 0.420 1.000 0.019*
10-Carry sweaty
foods to manage
hypoglycemia
2.70±1.87 3.85±1.14 4.60±0.60 10.703 2.55±1.73 3.70±1.22 3.60±1.05 4.367 0.263 0.403 3.711
0.0001* 0.017* 0.794 0.689 0.001*
11-Medical
follow up
2.80±1.54 3.35±1.35 3.60±1.14 1.826 2.25±1.16 2.85±0.93 2.55±0.94 1.732 1.273 1.363 3.168
0.170 0.186 0.211 0.181 0.003*
12-Carry
identification
card
1.70±1.45 2.20±1.32 2.35±1.22 1.295 1.05±0.22 1.45±0.60 1.20±0.41 4.194 1.975 2.307 3.978
0.282 0.020* 0.056 0.027* 0.0001*
13-Practice
exercise
regularly
2.85±1.69 3.30±1.30 3.95±1.00 3.298 1.55±0.76 2.20±1.00 2.15±0.81 3.493 3.131 2.991 6.252
0.044* 0.037* 0.003* 0.005* 0.0001*
14- Practice
exercise
strenuously
2.75±1.68 3.30±1.26 3.80±1.06 2.990
0.058 1.55±0.89 2.15±1.04 1.95±0.94
2.029
0.141
2.822
0.008*
3.147
0.003*
5.839
0.0001*
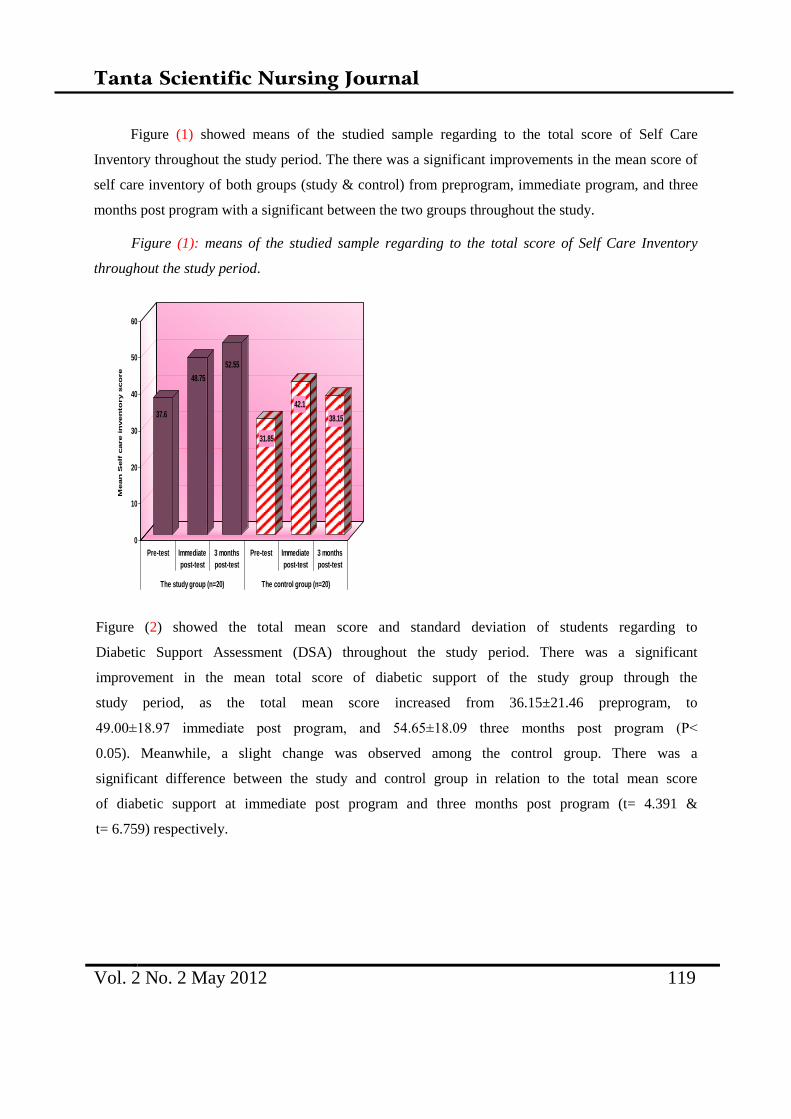
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 119
Figure (1) showed means of the studied sample regarding to the total score of Self Care
Inventory throughout the study period. The there was a significant improvements in the mean score of
self care inventory of both groups (study & control) from preprogram, immediate program, and three
months post program with a significant between the two groups throughout the study.
Figure (1): means of the studied sample regarding to the total score of Self Care Inventory
throughout the study period.
Figure (2) showed the total mean score and standard deviation of students regarding to
Diabetic Support Assessment (DSA) throughout the study period. There was a significant
improvement in the mean total score of diabetic support of the study group through the
study period, as the total mean score increased from 36.15±21.46 preprogram, to
49.00±18.97 immediate post program, and 54.65±18.09 three months post program (P˂
0.05). Meanwhile, a slight change was observed among the control group. There was a
significant difference between the study and control group in relation to the total mean score
of diabetic support at immediate post program and three months post program (t= 4.391 &
t= 6.759) respectively.
37.6
48.75
52.55
31.85
42.1
38.15
0
10
20
30
40
50
60
Mean
Self
care in
ven
to
ry s
co
re
Pre-test Immediate
post-test
3 months
post-test
Pre-test Immediate
post-test
3 months
post-test
The study group (n=20) The control group (n=20)
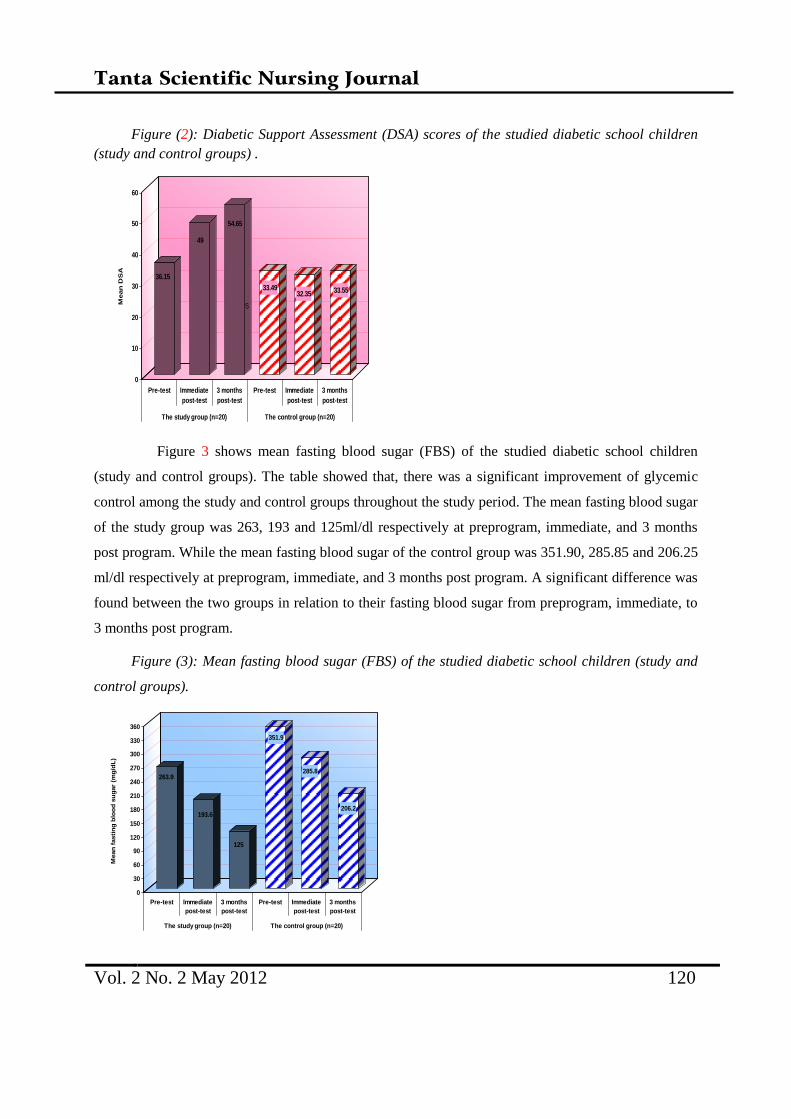
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 120
Figure (2): Diabetic Support Assessment (DSA) scores of the studied diabetic school children
(study and control groups) .
Figure 3 shows mean fasting blood sugar (FBS) of the studied diabetic school children
(study and control groups). The table showed that, there was a significant improvement of glycemic
control among the study and control groups throughout the study period. The mean fasting blood sugar
of the study group was 263, 193 and 125ml/dl respectively at preprogram, immediate, and 3 months
post program. While the mean fasting blood sugar of the control group was 351.90, 285.85 and 206.25
ml/dl respectively at preprogram, immediate, and 3 months post program. A significant difference was
found between the two groups in relation to their fasting blood sugar from preprogram, immediate, to
3 months post program.
Figure (3): Mean fasting blood sugar (FBS) of the studied diabetic school children (study and
control groups).
36.15
49
54.65
33.4932.35 33.55
0
10
20
30
40
50
60
Mean
DS
A
Pre-test Immediate
post-test
3 months
post-test
Pre-test Immediate
post-test
3 months
post-test
The study group (n=20) The control group (n=20)
S
263.9
193.6
125
351.9
285.8
206.2
0
30
60
90
120
150
180
210
240
270
300
330
360
Mean
fasti
ng
blo
od
su
gar
(mg
/dL
)
Pre-test Immediate
post-test
3 months
post-test
Pre-test Immediate
post-test
3 months
post-test
The study group (n=20) The control group (n=20)
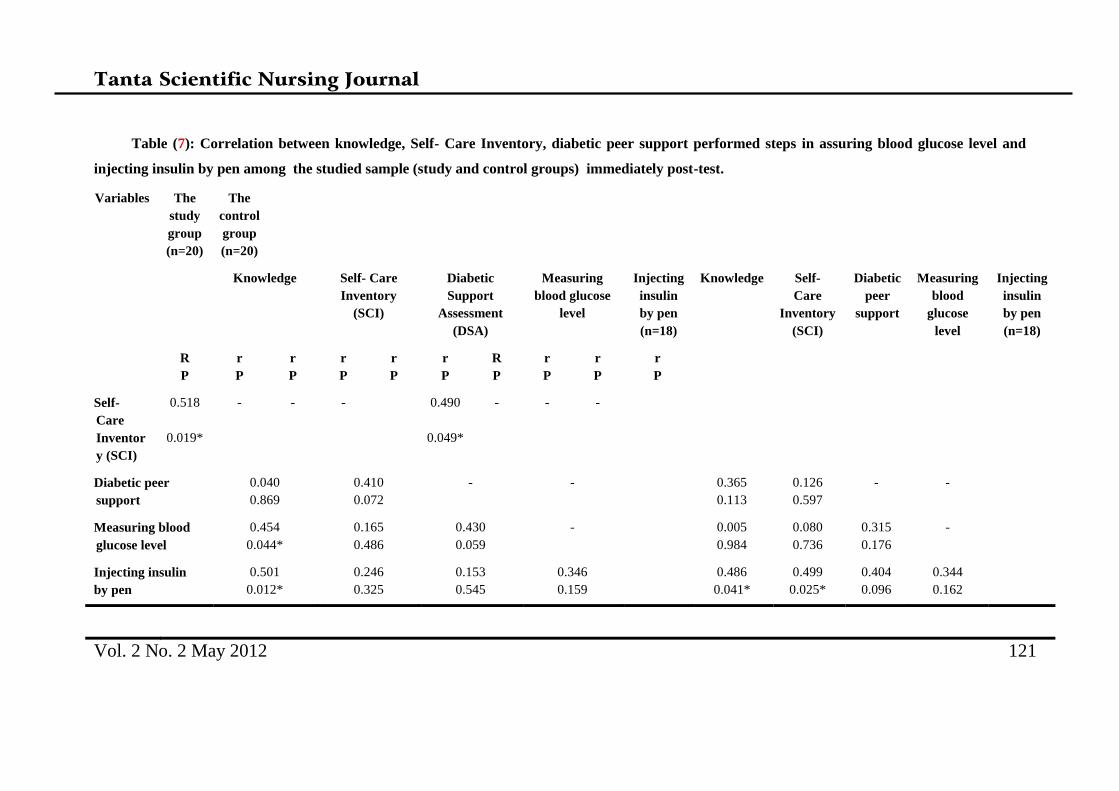
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 121
Table (7): Correlation between knowledge, Self- Care Inventory, diabetic peer support performed steps in assuring blood glucose level and
injecting insulin by pen among the studied sample (study and control groups) immediately post-test.
Variables The
study
group
(n=20)
The
control
group
(n=20)
Knowledge
Self- Care
Inventory
(SCI)
Diabetic
Support
Assessment
(DSA)
Measuring
blood glucose
level
Injecting
insulin
by pen
(n=18)
Knowledge
Self-
Care
Inventory
(SCI)
Diabetic
peer
support
Measuring
blood
glucose
level
Injecting
insulin
by pen
(n=18)
R
P
r
P
r
P
r
P
r
P
r
P
R
P
r
P
r
P
r
P
Self-
Care
Inventor
y (SCI)
0.518
0.019*
- - - 0.490
0.049*
- - -
Diabetic peer
support
0.040
0.869
0.410
0.072
- - 0.365
0.113
0.126
0.597
- -
Measuring blood
glucose level
0.454
0.044*
0.165
0.486
0.430
0.059
- 0.005
0.984
0.080
0.736
0.315
0.176
-
Injecting insulin
by pen
0.501
0.012*
0.246
0.325
0.153
0.545
0.346
0.159
0.486
0.041*
0.499
0.025*
0.404
0.096
0.344
0.162
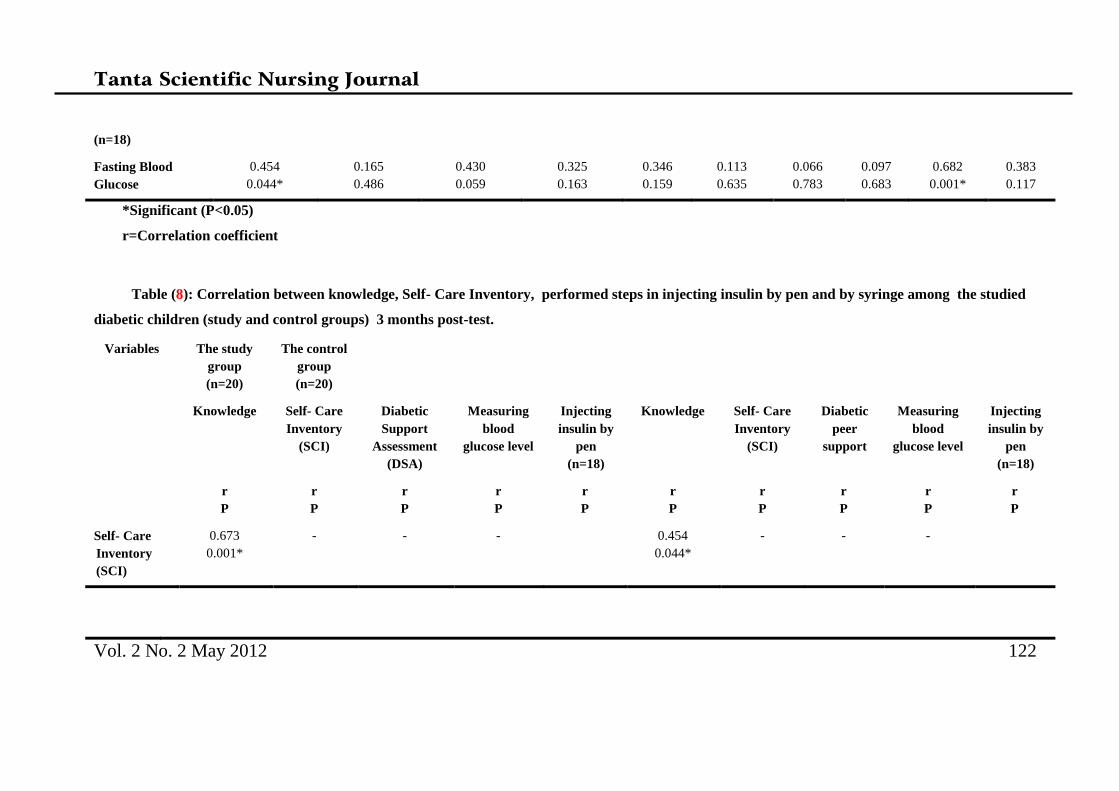
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 122
(n=18)
Fasting Blood
Glucose
0.454
0.044*
0.165
0.486
0.430
0.059
0.325
0.163
0.346
0.159
0.113
0.635
0.066
0.783
0.097
0.683
0.682
0.001*
0.383
0.117
*Significant (P<0.05)
r=Correlation coefficient
Table (8): Correlation between knowledge, Self- Care Inventory, performed steps in injecting insulin by pen and by syringe among the studied
diabetic children (study and control groups) 3 months post-test.
Variables The study
group
(n=20)
The control
group
(n=20)
Knowledge
Self- Care
Inventory
(SCI)
Diabetic
Support
Assessment
(DSA)
Measuring
blood
glucose level
Injecting
insulin by
pen
(n=18)
Knowledge
Self- Care
Inventory
(SCI)
Diabetic
peer
support
Measuring
blood
glucose level
Injecting
insulin by
pen
(n=18)
r
P
r
P
r
P
r
P
r
P
r
P
r
P
r
P
r
P
r
P
Self- Care
Inventory
(SCI)
0.673
0.001*
- - - 0.454
0.044*
- - -
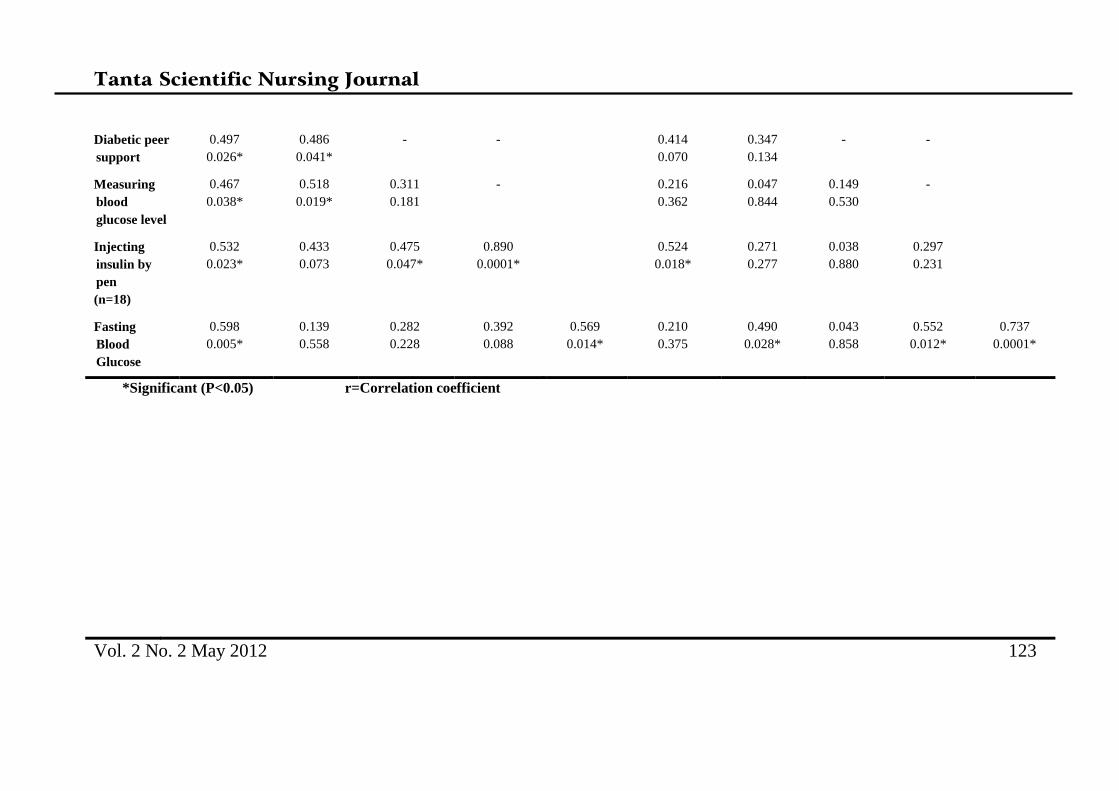
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 123
Diabetic peer
support
0.497
0.026*
0.486
0.041*
- - 0.414
0.070
0.347
0.134
- -
Measuring
blood
glucose level
0.467
0.038*
0.518
0.019*
0.311
0.181
- 0.216
0.362
0.047
0.844
0.149
0.530
-
Injecting
insulin by
pen
(n=18)
0.532
0.023*
0.433
0.073
0.475
0.047*
0.890
0.0001*
0.524
0.018*
0.271
0.277
0.038
0.880
0.297
0.231
Fasting
Blood
Glucose
0.598
0.005*
0.139
0.558
0.282
0.228
0.392
0.088
0.569
0.014*
0.210
0.375
0.490
0.028*
0.043
0.858
0.552
0.012*
0.737
0.0001*
*Significant (P<0.05) r=Correlation coefficient

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 124
Discussion
Type 1 diabetes mellitus (T1DM) is a
lifelong metabolic disorder for which no cure is
known. The management of T1DM is a complex
regimen of multiple daily insulin injections,
frequent monitoring of blood glucose level and
life style adjustment such as meal planning and
exercise. TIDM presents a unique challenge to
health care provider, diabetic school children
and their families (18,19)
.
The main aim of diabetes management of
diabetic teenage is to achieve optimal glycymic
control as it prevents long term complications.
Glycymic control usually deteriorates during
adolescence (20)
.
Peer support helps reduce problematic
health behaviors, depression, and contribute to
improve diabetes management, including
improving behaviors related to medication
adherence, diet, exercise, and blood glucose
monitoring. The success of peer support appears
to be due to the nonhierarchical, reciprocal
relationship that is created through the sharing
of similar life experiences(21)
.
At the begaining of this study, the pretest
was applied to students of both the study and
control groups to analyze their
sociodemographic data, knowledge, self care
practices, glycemic control, and availability of
peer support of the diabetic school children in
order to develop specifically targeted
comprehensive guidelines on diabetes self-
management according to their needs,
knowledge and practices deficit.
In this context, the result of this study
showed that before implementation of the
program the study and control groups showed
poor glycemic control, low scores of
knowledge, self care practices and perceived
peer support. After implementation of the
program, the two groups showed significant
glycemic control and improvement in their
knowledge score and self care practices. This
improvement was highly significant among the
study group who received peer support than the
control one.
Maintaining glycemic levels is an
extremely difficult task for most school- age
children and their families(22)
. Preprogram, the
two groups showed poor glycemic control as
they had high means of fasting blood glucose
levels. Immediately and three months after
applying the program, a significant progressive
reduction in the means of the fasting blood
glucose levels was found among the two groups.
However, the reduction was more obvious
among the study group than the control one.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 125
This could be due to that students included in
the peer support group were more motivated
and supported each other to adhere to diabetic
diet, regular exercise in the form of walking,
regular monitoring of blood glucose level and
adjust insulin injection dose according to the
results. Such support was mainly through
telephone call or meeting during school day
break to discuss daily events related to diabetes.
This result is in agreement with the result of
Deakin et. al., (2005), who reported that group
based training significantly improved fasting
blood glucose level of diabetic people at both
short- and long- term follow up(23)
.
As regard students’ knowledge about
diabetes, the present study showed that, results
of pretest showed that only a few percent of
both the study and control groups reported
correct and complete knowledge about diabetes
as well as its management. This result may be
attributed to unavailability of an organized-
structured health education program about
diabetes to those diabetic students. The present
result is in agreement with El Rafay
SS(2004)(24)
,who reported that the diabetic
children had improper knowledge of diabetes
including its meaning, types and causes.
The importance of knowledge in health
education must not be ignored as improvement
in knowledge is the first step toward health
behavior modification. After applying the
program, the two groups in this study showed a
significant improvement in their mean score of
total knowledge about diabetes, its management
and all its aspects immediately and 3 months
post program. This improvement was relatively
higher among the group who received peer
support than the control group. This reflects the
importance of continuous education of diabetics
in conjunction with peer support to refresh their
knowledge as some details may be forgotten, so
peers can review them together. In accordance
with the present study Coleman et. al., (2011)
(25) reported that peer education had a significant
increase in diabetic students' knowledge related
to diabetes. The result also is in agreement with
the finding of Hassan S(2007) (16)
, El zubier
(2001) (26)
, and Norris et. al., (2001) (27)
who
found significant improvement in knowledge of
diabetic children after health education program.
El Rafay (2004) (24)
, mentioned that diabetic
adolescent reported appropriate understanding
about the difference between the traditional and
the unfamiliar symptoms of hypoglycemia after
health education.
Concerning Self Care Inventory (SCI),
the pretest in this study revealed that the two
groups had low frequency of practicing most of

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 126
its items e.g. blood glucose testing, recording,
ketones testing, changing insulin dose according
to result of blood glucose test, eating meals at
times, having snacks regularly, carry sweaty
foods to manage hypoglycemia, medical follow
up, carrying identification card, and practicing
of exercise. This finding may be due to many
facts as lack of their knowledge about DM and
its management, negligence, as well as their
desire for not to be different from their
colleagues or friends. After applying the
program, there was a significant improvement in
all items of SCI for both groups immediately
post program except for testing of ketones,
taking accurate insulin dose, taking it at right
time, and eating meals at times. This
improvement was higher and significant among
the study group than the control one through the
study period especially three months post
intervention. Moreover, the overall score of SCI
was higher among the study than the control
with significant difference between the two
groups either, immediate, and post test. These
results may be attributed to the core element of
peer support which depends on sharing and
exchanging of experiences related to diabetes
among the study group. Peer support may
improve self-management among millions of
people with diabetes around the world(28)
.
The realization of the importance and
effectiveness of peer support among adolescents
has encouraged its implementation in various
health problems as engaging peer support to
help adolescent and child to deal with public
health problems such as smoking(29)
. A assessed
the influence of peer relationships on adjustment
to cystic fibrosis during adolescence by
D’Auiria et. al., (2000) (30)
, showed that, peer
support help adolescents to incorporating cystic
fibrosis into their developing ideas of who they
are and who they will become, gave them a
greater perspectives of illness, its consequences,
coping and the importance of believing in a
positive future.
Therapy of T1DM involves greater and
earlier use of intensive insulin regimens in order
to achieve better control of blood glucose
level(31)
. The result of the present study revealed
that, study group showed high compliance with
insulin dose and adjusting it according to results
of blood glucose test more than the control one.
This result may be attributed to their influence
by familial experiences as three quartres of the
studied sample had family history of diabetes
mellitus in particular among first degree relati
relatives (father mother, sister and brother).
Moreover, every student in the peer support
group competed to be more compliant than his

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 127
peers. In agreement with the current result, La
Greca (2004), reported that most people with
diabetes report compliance with insulin
management very often(15)
. This result is
contradicted with Abdel Gaffar (2003)(17)
who
found that only thirty percent of the diabetic
students had good self care practice scores in the
area of insulin injection therapy.
The American Diabetes Association
(ADA) (2005) (32)
recommended that patients
with DM perform self monitoring blood glucose
at least 3 times/day especially before meals. In
the present study before implementation of the
program a varied percentage of the study and
control groups used to test blood glucose level
before meals, two hours after meal, or at any
time. Immediately after applying the program,
the majority of the two groups tested their blood
glucose level before meals and two hours after
meals. At three months post program, all the
study group reported that they test their blood
glucose at such times while the control group
showed slight decrease than this percentage.
Their scores regarding recording of the result of
blood glucose test increased through the study
period especially among the study group. These
results may be explained by the role played by
peers as they reminded each other about
adherence to testing blood glucose at time
through a mobile telephone call at morning and
at night before sleeping. Moreover, the health
insurance provided each diabetic student with an
apparatus for blood glucose testing that makes
blood glucose testing available for the student at
any time.
Although insulin therapy is the
cornerstone of treatment for type 1 DM, a
dietary plan is important in maintaining near-
normoglycemia without wide swings in blood
glucose levels. Long term adherence to the
dietary plan is probably the most difficult aspect
of the diabetic regimen (33)
. The results of the
present study denoted that preprogram more
than half of the two groups showed improper
practices regarding diabetic diet (adhered to
wrong diet regimen, take no action if they want
to eat sweaty foods, had few meals /day, ate
inappropriate snacks, and did not weight body
regularly).
Poor dietary regimen adherence could be
also attributed to both inadequate patients'
knowledge of dietary management, and that
food habits are the most difficult habit to
change(34)
. Immediately post program, the
majority of the study group and more than half
of the control group showed improvement in
their practice regarding diabetic diet. This
improvement was maintained among the study

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 128
group at three months post program more than
the control group. This result as mentioned by
the study group is related to the presence of a
peer who helped them to select appropriate food
and encourage them to eat proper snacks e.g.,
one peer supporter had previous health
education sessions about diabetes and its
suitable diet at Abo El-Resh hospital and the
students usually search net wipe site for
diabeteic diet and intern they benefit their peers.
Such peers were not available to the control
group. In agreement with the present results El
Saleet (2000), assessed the effect of improving
knowlegde and practice among diabetic children
and their mothers in Tanta city and reported
improved adherence to diet control among
diabetic children(35)
. On the other hand results of
Hassan (2007) (16)
, are contradicted with this
result as it revealed that there was a significant
reduction in the mean score of adolescents’
adherence to diabetic diet after implementation
of the intervention.
Regular physical activity is associated
with immediate and long-term health
benefits(36)
. According to American Diabetic
Association (ADA) guidelines, all patients with
diabetes should be given the opportunity to
benefit from the effect of exercise(37)
. At the
pretest more than half of the study group and
only more than one tenth of the control
practiced physical exercise. This finding is in
agreement with many researches that assessed
self- care and physical practices of diabetics
which denoted poor physical exercise practices
among diabetic children(17,32,38)
. Immediately
and 3 months after implementation of the
program, there was a significant improvement in
the practice of physical exercise of the two
groups, but it was more significant among study
group than the control one. This finding may be
related to the influence of peers as peers
encouraged each other to practice exercise.
Friends' support in this study consisted primarily
of companionship behaviors, such as sharing
various activities (e.g. they go to biking or
walking together).
Although circulatory problems of the feet
are less common in children, proper foot
hygiene habits need to be established(39)
. The
current study denoted that a varied percentage
ranged from 50% to 80% of both groups had
improper practices. Immediately and 3 months
after implementation of the program, the
majority of both groups showed improvement in
all items of foot care practices, but with no
significant differences between the two groups.
This result may be attributed to improvement of
their knowledge related to foot care. The

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 129
students reported that they adhered to foot care
practices fearing of foot complications
especially diabetic foot and amputation.
Findings of El Sallet (2000)(35)
, are in agreement
with this results.
Adolescents and children tend to have
difficulty adherence to diabetic regimens(40)
.
Negative social attributions have a role in
adherence difficulties, so intensive psychosocial
support may be indicated (41)
. Peer support falls
within the social model, which is defined as the
process through which social relationships
might promote health and well-being(42)
. The
results of the present study denoted that,
preprogram, the majority of the two groups
reported that their parents were the resource
persons for diabetes social support. Immediately
and 3 months post program, the majority of the
study group reported that peers and parents were
the resource persons for diabetic social support,
while the majority of the control group reported
parents only. Furthermore, it was also observed
that, immediately and 3 months post program,
students exposed to peer support, reported peers
with high score than parents as a resource for
support. Finding of a study done by Greco P et.
al., (2001)(43)
, about peer group intervention for
adolescents with type 1 diabetes and their best
friends is in agreement with the result of the
present study and added that parents reported
that including peers in treatment has been
associated with decreased parent- child diabetes
conflict.
Concerning peer support, the present
study revealed that, pre-intervention the study
and control groups had nearly the same mean
scores on the diabetes peer support assessment
scale regarding all the studied items.
Immediately and 3 months post program, the
study group showed a significant continuous
increase in their total mean score of diabetes
peer support and for all the items. On the other
hand, the control group showed no
improvement. This result is in agreement with
Pendley et. al., (2002), who studied peer and
family support in children and adolescents with
type 1 diabetes and mentioned that adolescents
reported significantly more peer support for
various management tasks in every category of
peer support(44)
. These results may be justified
that, as adolescent experience more intimacy
and disclose information, as it is typical in
normative development, and they may also
share more disease-related information and, in
turn, perceive their peers as offering more
support for their diabetes(45)
.
The present study showed a positive
correlation between the knowledge of the study

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 130
group and Self- Care Inventory, peer support,
measuring blood glucose level, injecting insulin
by pen and fasting blood glucose level at 3
months post program Self- Care Inventory was
also correlated with peer support and injecting
insulin. This correlation may be related to the
success of peer supporters in persuading the
diabetic student to correct their diabetic
knowledge and enhance their adherence to self
care practices. In relation to the control group, a
significant positive correlation was found
between the group's knowledge and Self- Care
Inventory, and injecting insulin by pen
immediately and 3 months post program. This
correlation is similar to that of Norris et. al.,
(2001)(46)
,who reported that self management
training was associated with improvement of
knowledge, frequency or accuracy of blood
glucose self monitoring, self-reported dietary
habits and glycemic control.
Three months post program there was
also a positive correlation between Self- Care
Inventory of study group and diabetic peer
support & measuring blood glucose level.
Moreover, a positive correlation was found
between injecting insulin by pen and diabetic
peer support & measuring blood glucose level.
In addition, there was a positive correlation
between fasting blood glucose level and diabetic
knowledge & injecting insulin by pen. This
correlation is clarifying that every student in the
study group gained benefit from the practical
experience of each other which intern improve
their self care practices and glycemic control.
Continuous effort should be made to help
diabetic school students achieving gylcemic
control and adhering to the management of the
disease. This can be achieved through
organization and implementation of diabetic
peer support group within the school. Proper
glycemic control will help students enhancing
their academic performance and relations with
the outside environment.
Recommendations
1- School health nurses should be informed
about the importance of peer support for
diabetic students and encouraged to do their best
effort to make peer support available to every
diabetic student in particular those of poor
glycemic control or newly diagnosed.
2-The school health nurse should conduct
periodic and continuous training programs for
the diabetic students to enhancing their diabetes
self care and glycemic control.
3- School health insurance needs to specify a
certain day and name it “day of diabetic
student”. This day give the chance for meeting
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 131
of all diabetic students and doing recreational
and physical activities that enhance their social
support to each other.
4- School health insurance should provide every
diabetic student with a booklet with simple
instructions and diagrams about diabetes and its
management.
5- Mass media programs about type 1 diabetes
and peer support need to be prepared and
introduced by diabetic teenagers.
References
1- Ball JW and Blindler RC. Child Health
Nursing: Partnering with Children &
Families. New Jersey: Pearson Prentice
Hall Co., 2006; 1263-1275.
2- Price DL and Gwin JF. Pediatric
Nursing: An Introductory Text. 10thed.
Tokyo: Saunders Co., 2008; 291-302.
3- Towle MA and Adams ED. Maternal-
Child Nursing Care. New Jersy:
Pearson Prentice Hall Co., 2008; 753-
764.
4- International Diabetes Federation.
International Diabetes Federation calls
for global action to keep all children
with diabetes alive.2001.
5- International Diabetes Federation.
Diabetes. Diabetes is a chronic and
life- threatening condition. 2006.
6- http://weekly.ahram.org.eg/2007/853/e
g8.htm
7- Allen PA and Vessey TA. Primary
Care of a Child with Chronic
Condition. 4th ed. China: Mosby Co.,
2004; 426-444.
8- Bearman KJ and La Greca AM.
Assessing Friend Support of
Adolescents' Diabetes Care: The
Diabetes Social Support
Questionnaire- Friend Version. Journal
of Pediatric Psychology, 2002; 27(5):
417-428.
9- Pendly JS, Kasmen LJ, Miller DL,
Donze J, Senson C and Reevers G.
Peer and Family Support in Children
and Adolescents with Ttpe 1 Diabetes.
Journal of Pediatric Psychology, 2002;
27(5): 429-438.
10- Heisler M. Overview of Peer Support
Models to Improve Diabetes Self-
Management and Clinical Outcomes.
Journal of Diabetes Spectrum,
2007;20(4):214-219.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 132
11- Kyle T. Essentials of Peadiatric
Nursing. Tokyo: Lippincott Williams
Co., 2008; 957-966.
12- Boyd M. psychiatric Nursing:
Contemporary Practice. 4th ed. Tokyo:
Lippincott Williams& Wilkins Co.,
2008; 189-199.
13- Lundy K and Janes S. Community
Health Nursing: Caring for the Public's
Health. 2nd
ed. Singapore: Jones and
Bartlett Publishers Co., 2001: 391-400.
14- http://www.diabetesinitiative.org/resou
rces/tools/documents/8-LAC-
SocialSupportToolEnglish_000.pdf
15- La Greca AM. Manual for Self-Care
Inventory.
http://www.psy.miami.edu/faculty/alag
reca/SCI_manual_2004.pdf
16- Hassan SG. Quality of Life of Diabetic
Adolescents in Alexandria:
Determinants and Relation to
Glycemic Control. Unpublished
Doctoral thesis, Alexandria University,
High Institute of Public Health, 2007.
17- Abd El-Ghaffar AA. Factors Affecting
Self- Care Practices of Diabetic School
Students in Alexandria. Unpublished
Master thesis, Alexandria University,
Faculty of Nursing, 2003.
17-Schilling JA and Homles HN. Diabetes
Mellitus: A Guide to Patient Care. Tokoy:
Lippincott Williams& Wilkins Co., 2007;
53-77.
18- Gage D, Hampson S, Skinner TC, Hart
J, Storey L, Foxcroft D, Kimber A,
Cradock S and McEvilly EA.
Educational and Psychosocial
Programs for Adolescents with
Diabetes: Approaches, Outcomes and
Cost- Effectiveness. Patient Education
and Counseling. 2004;53(2): 333-346.
19- Du Pasquier-Fediaevsky L, Chwalow
AJ, Tubiana-Rufi N and PEDIAB
collaborative group. Is the Relationship
Between Adherence Behaviours and
Glycaemic Control Bidirectional at
Adolescence? A longitudinal Cohort
Study, Diabet Med (2005); 22: 427–
433.
20- Heisler M. Overview of Peer Support
Models to Improve Diabetes Self-
Management and Clinical Outcomes.
Journal of Diabetes Spectrum,
2007;20(4):214-219.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 133
21- Smelizer CS, and Bare B. Brunner and
Suddaeth Textbook of Medical
Surgical Nursing. 10th ed. Philadephia,
Congess Com., 2004; 30-40.
22- Deakin T, McSane CE, Cade JE, and
Willliams RD. Group-Based Training
for Self- Management Srategies in
people with Type 2 Diabetes Mellitus.
Cochrane Database Syst. Rev. (2)
2005.
23- Al-Rafay SS. Glycemic Control in
Adolescents with Insulin- Dependent
Diabetes IDD: Comprehensive
Guidelines for Diabetes Self-
Management. The New Egyptian
Journal of Medicine, 2004; 30(suppl.
4): 23-31.
24- Coleman KJ, Clark AY, Shordon M,
Ocana LL, Walker C, Araujo RA,
Coleman JO and Tsimikas AP. Ten
Peer Educator and Diabetes
Knowledge of Low-Income Fifth
Grade Students. Journal of Community
Health. 2011; 36(1):23-26.
25- Elzubier AG. Knowledge of
Hypoglycemia by Primary Health Care
Centers- Registered Diabetic Patient.
Saudi Medical Journal, 22(3): 219-222.
26- Norris SL, Engelgau, MM, and Venkat
Narayn KM. Effectiveness of Self –
Management Training in Type 2
Diabetes: A Systematic Review of
Randomized Controlled Trials.
Diabetes Care, 2001; 24(3): 561-587.
27- Fisher EB, Earp JA, Mamman S and
Zolotor A. Cross-Cultural and
International Adaptation of Peer
Support for Diabetes Management.
Family Practice. 2009;1-11.
http://fampra.oxfordjournals.org/cgi/co
ntent/abstract/cmp013
28- Patten C, Lopes K, Thomas J, Offord
K, Decker P, Pingree S, Dornelas E
and Ahluwalia J. Reported Willingness
Among Adolescent Nonsmokers to
Help Parents, peers, and Others to Stop
Smoking. Preventive Medicine, 2004;
39(6): 1099-1106.
29- D’Auiria J, Christian B, Hendreson Z
and Haynes B. The Company They
Keep: The Influnce of Peer
Relationships on Adjustment to Cystic
fibrosis During Adolescence. Journal
of peadiatric Nursing, 2000; 15(3):
175-182.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 134
30- Strauss K, Gols H, Hannel I, Partanen
T and Frid A. A Pan- European
Epidemiology Study of Insulin
Technique in Patient with Diabetes.
Practical Diabetes International. 2002;
19(3):71-76.
31- American Diabetes Association.
Standard of Medical Care in Diabetes.
Diabetes Care. 2005; 28(suppl. 1): S4-
36
32- Toljamo M and Hentinen M.
Adherence to Self-Care and Glycemic
Control among People with Insulin
Dependent Diabetes. Journal of
Advanced Nursing, 2001; 34(6): 780-
786.
33- Saleh S. Study on Nutrition in Non
Dependent Diabetic Subjects in
Alexandria: The Present Status, Needs
and its Impact on the Metabolic
Control. Unpublished Doctoral Thesis.
Alexandria University. High Institute
of Public Health, 1999.
34- El-Saleet GM, Bahgat RS, El-Deib A
and Sikena MH. Effect of Improving
Knowlegde and Practice among
Diabetic Children and their Mothers in
Tanta City, Gharbia Governorate. The
new Egyptian Journal of Medicine,
2000;22(suppl. 1): 7-24.
35- Ekblom B and Astrand PO. Role of
Physical Activity on Health in
Children and Adolescents. Acta
Paediatr, 2000; 89: 762-774.
36- American Diabetes Association.
Physical Activity/Exercise and
Diabetes. Diabetes Care, 2004;
27(suppl. 1): S59-S62.
37- Helmy FE and El-Shafie IF. Coping
Behaviors and Adaptation of Children
with Diabetes. The Egyptian Journal of
Diabetes. 2001; 6(1): 7-15.
38- Boaz N. Evolving Health. New York:
John Wiley &Sons, Inc., 2002; 124-
135.
39- Wysocki T, Greco P, and Buckloh LM.
Handbook of Pediatric Psychology. 3rd
ed., New York: Guilford com., 2003;
304-320.
40- Hains AA, Berlin KS and Davies WH.
Atrribution of Adolescents with Type 1
Diabetes in Social Situations:
Relationship with Expected
Adherence, Diabetes Stress, and
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 135
Metabolic Control, Diabetes Care,
2006; 29(1): 818-822.
41- Cohen S, Gottlieb B and Underwood
L. Social Relationship and Health:
Social Support Measurments and
Intervention. Oxford, Oxford
University Press, 2000; 3-28.
42- Greco P, Pendley JS, McDonell K and
Reeves G. A Peer Group Intervention
for Adolescents with Type 1 Diabetes
and Their Best Friends. Journal of
Pediatric Psychology, 2001; 26(8):
485-490.
43- Pendly JS, Kasmen LJ, Miller DL,
Donze J, Senson C and Reevers G.
Peer and Family Support in Children
and Adolescents with Ttpe 1 Diabetes.
Journal of Pediatric Psychology, 2002;
27(5): 429-438.
44- Fluigni AJ, Eccles JS, Barber BL and
Clements P. Early Adolescent Peer
Oreintation and Adjustment during
High School. Developmental
Psychology. 2001; 37(1): 28-36.
45- Norris SL, Lau J, Smith SJ, Schmid
CH and Engelgau MM. Self –
Management Education for Adults
with Type 2 Diabetes: A Meta-analysis
of the Effect of Glycemic Control.
Diabetes Care,2002; 25(7): 1159-1171.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 136
Application of Designed Orientation Program for Nurse Interns Based on Learning
Needs Assessment
Heba K. Obied, Assistant lecturer in Nursing Administration Dep, Faculty of Nursing, Tanta University
Fouada M.Shabaan, Prof. of Nursing Administration, Faculty of Nursing, Tanta University
Helmy H. Shalaby, Prof. of Plastic Surgery, Faculty of Medicine, Tanta University
Samar H. Gadiry, Lecturer of Nursing Administration, Faculty of Nursing, Tanta University
Abstract
Orientation programs based on LNA encourage nurse interns to feel safe and enable them to demonstrate
competency in the basic clinical and management skills needed for providing high quality and safe patient care.
Using LNA ensure NIs commitment to these program. This study aimed to design, implement, and evaluate an
orientation program about clinical and management skills needed for nurse interns based on the findings of
learning needs assessment tool. Material and method the study was conducted at Tanta University Faculty of
Nursing and Tanta University Emergency and Main Hospitals ICUs and obstetric and dialysis departments.
(384) nursing students passed the 4th
academic year attended the orientation program. (198) spent their
internship year at Tanta University Hospitals were included in the researcher’s observation 3 month post
program. The data collection was achieved by using LNA scale, knowledge test, NIs’ orientation program and
follow up observation sheet. RESULTS: Pre program around half (51%) of NIs assessed themselves as cannot
carryout different clinical and management skills. Majority (87%) of NIs got low knowledge level for both
skills. Post orientation program statistical significant improvement at (P≤0.05) was found in NIs’ knowledge and
practical levels for both clinical and management skills. Conclusion designing orientation programs before
starting the internship year based on nurse interns LNA is important to ensure efficient interns performance.
Recommendation conduct orientation programs based on nurse interns’ LNA and knowledge test before
starting internship year and at the beginning of each new rotation, provide nurse interns with pass booklet
include standard procedures required to be carried out in each rotation, provide them also with designed
evaluation manual based on the pass booklet and implementing nursing mentor-ship and preceptor-ship
programs during internship year.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 137
Introduction
The internship year is considered a time of
transition from undergraduate nursing students to
beginning level registered nurses. During this year
nurse interns should acquire the values, attitudes,
and goals fundamental to the nursing
profession(1,2)
. At the beginning of the internship
year many nurse interns feel uncomfortable and
inadequacy as their skill levels do not match their
expectations of the role and responsibilities of a
practicing as a registered nurse(3)
. During
internship year nurse interns are expected to work
in intensive care units (ICUs) under supervision of
experienced knowledgeable supervisors (4)
.
Today’s health care arena become complex and
suffer from severe nursing shortage and limited
budgets for continuing education programs; that
affect organization’s ability to provide
comprehensive orientation programs for new
graduates or for nurse interns(5-6)
.
In addition hospital administrators’ expect nurse
interns to be competent to function and take
responsibilities in nursing service at the time of
graduation with adequate clinical and patient
management skills to cover shortage and decrease
the workload on experienced staff. Consequently
nurse interns are imposed to the work field
responsibilities early(7-8)
. Therefore, nursing
faculties have to provide interns with a supportive
clinical environment in terms of skills, knowledge,
practice, reflection and cultural socialization to
help them to feel competent and supported (9)
.
Effective internship year should starts with
orientation program to enhance the nurse interns’
knowledge and relieve their stress. Nursing
faculties are responsible for designing and
implementing appropriate internship programs to
smooth transition from student to registered nurse.
Well designed internship program facilitate interns’
entry into clinical practice, support their growth
along the continuum of expertise, and development
of essential leadership skills within the field of
health care(10,11)
.
Orientation program encourage nurse interns
to feel welcome, safe and valued, so it eases
transition and provide them with opportunities to
develop self confidence, increase job satisfaction
and chances to demonstrate competency in the
basic skills needed for So this study aimed to assess
nurse interns’ learning needs before entering
clinical practice setting and design a suitable
orientation program for covering the gabs in their
clinical and management knowledge and skills.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 138
This study also aimed to evaluate the nurse
interns’ statistical change of clinical and
management knowledge and skills after attending
the orientation program.
Aim of the study: This study aimed to apply a
designed orientation program for nurse interns
based on learning needs assessment through:
- Design, implement, and evaluate an orientation
program about clinical and management skills
needed for nurse interns based on the findings of
using learning needs assessment tool.
Materials and Method:
Study design: Cross-sectional study design was
utilizes to achieve the aim of this study.
Setting: The study was conducted at
Tanta University Faculty of Nursing.
Tanta University Emergency and Main
Hospitals Intensive Care Unites (ICUs) include
medical, anesthetic, neurological, neonatal,
pediatric, and cardiac .In addition to obstetric
and dialysis departments.
providing high quality and safe patient care (5,12,13)
.
Orientation program ensures useful transition time
if it is based on the interns’ key learning needs and
considers teaching and learning activities
grounded in practice experience, skilled and well-
supported preceptors and structured learning
framework (14)
.
LNAs are often conducted to identify
deficiencies in knowledge, skill, behavior, or
attitude in the current teaching practices, or to
anticipate deficiencies based on expected changes
in health care needs. So orientation program based
on LNA match the nurse interns’ unique learning
needs not only nursing service needs(15-18)
.
Subject
All the nursing students (384) passed the fourth
academic year (2009-2010) attended the
designed orientation program based on their
learning needs assessment and participated in
pre and post program knowledge test.
All (198) nursing students who spent their
internship year (2010-2011) at Tanta University
Hospitals were included in post program
observation after three months. Tools of the study:
to collect the data four tools were used:
1. Learning needs assessment scale, developed by
the researcher guided by Zerwekh (2006)(53)
and Fakhry (2005)(159)
and others, to assess
nurse interns’ clinical and management
learning needs immediately before starting
internship year. The sheet contained part of
demographic data, and (150) items cover
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 139
clinical subscales (91) items and management
subscales (59). Responses were measured by
three points Likert Scale for clinical subscale
ranging from can do it by myself to can’t do it
by myself. And two points Likert scale
ranging from able to not able for management
subscale.
2. Nurse interns’ knowledge test, designed by the
researcher and used to collect data from nurse
interns. The test composed of (100) questions
cover both clinical and management subscales.
Scoring system represent knowledge levels of
nurse interns’ ranging from low (≤60%),
medium (>60%- ≤80%) to high (>80).
3. Nurse interns’ orientation program was
designed by the researcher based on the
findings of the learning needs assessment
scale and nurse interns' knowledge test tools
(1&2) (pre-test). At the end of the program, a
post-test was carried out used tool (2) for
sample (384) of nurse interns before starting
internship year to assess the extent to which
desired stated objectives and assumed needs
were achieved.
4. Follow up observation sheet, included the
same items in the learning needs assessment
5. scale to evaluate nurse interns' actual
performance of clinical and management skills
after three months of the orientation program
during their internship year. Researcher’s
observations to clinical skills were measured
by four points Likert Scale ranged from can do
it herself to not applicable. Management skills
were measured by two pointsLikert Scale
range from able to do to not able to do.
Method of data collection:
1. An official permission was obtained from
responsible authorities including Faculty of
Nursing and Hospitals of Tanta University to
conduct the study.
2. The learning needs assessment scale was
submitted to a jury of ten experts from different
nursing specialties to get their suggestions
about content validity and applicability of the
tool.
3. A pilot study was conducted on ten students
out of the proposed sample two times (two
weeks separated) to measure test-retest
reliability.
4. The content validity index was (93%), internal
consistency reliability was (0.9501) and the
test-retest reliability that was (0.9725).
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 140
5. Nurse interns’ learning needs of clinical and
management skills were assessed by (tool 1).
6. Nurse interns’ knowledge was tested by (tool
2) pre implementation of the orientation
program.
7. The nurse interns' orientation program was
designed based on the assessment data and
literature review. The program was
implemented by the researcher and started two
weeks just before internship year; it was ten
hours duration divided into five sessions each
session two hours for five days. The nurse
interns' were divided into two groups each
group attended the five sessions.
8. Nurse interns' knowledge was tested post
program by tool (2).
9. Nurse interns’ were followed up in their
clinical areas for the first three months after the
implementation of the orientation program,
then they were reevaluated using follow up
observation sheet (tool 3).
Results
Table (1) represents demographic
characteristics of nurse interns. Nurse interns
(73.2%) were in the age group ≤ 20-22. Majority
(81%) of nurse interns graduated from general
secondary school, while minorit
(6%) graduated from secondary technical nursing
school.
About two third (65%) of the subject had
graduation level very good and (7.6%) had
excellent graduation level. NIs (71.4%) did not
have previous training. While (28.6%) had
previous training, (61.9%) of them trained during
third and fourth academic years, (20.9%) trained
during all the four academic years and (17.2%)
trained during first and second academic years.
Training mean period was (3.4 + 0.45) month.
Those trained NIs (40.9%) of them had trained in
ICUs and (34.5%) trained in medical surgical
wards.
Figure (1) shows that pre program (51%) of
nurse interns assessed themselves as cannot do,
while (49%) can do both clinical and management
skills. More than half (53%) of NIs assessed
themselves as cannot do clinical skills, while
(42%) as cannot do management skills.
Table (2) represents nurse interns’ LNA total
clinical skills scales pre orientation program. Nurse
interns’ (71.3% and 69.1%) can assess vital signs
and collect patient's data respectively. Also (65.5%,
64.5%, 64.1%, 63.3% and 60.9%) can do assess

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 141
anthropometric measures, prevent immobility
complications, apply safe practice &infection
control, heat& cold therapy and perform patient
hygiene by themselves respectively. Nurse interns
(45.4 %, 43.7%, 42% and 41.8%) can not provide
by themselves elimination care, assist in diagnostic
procedures, provide gastrointestinal care and
provide cardio-respiratory care respectively.
Around one third (33.1% and 32.8%) of the nurse
interns can not provide by themselves newborn
care or apply mechanical restraining respectively.
More than quarter (29.4% and 28%) can not assess
by themselves neurological condition or provide
wound care respectively.
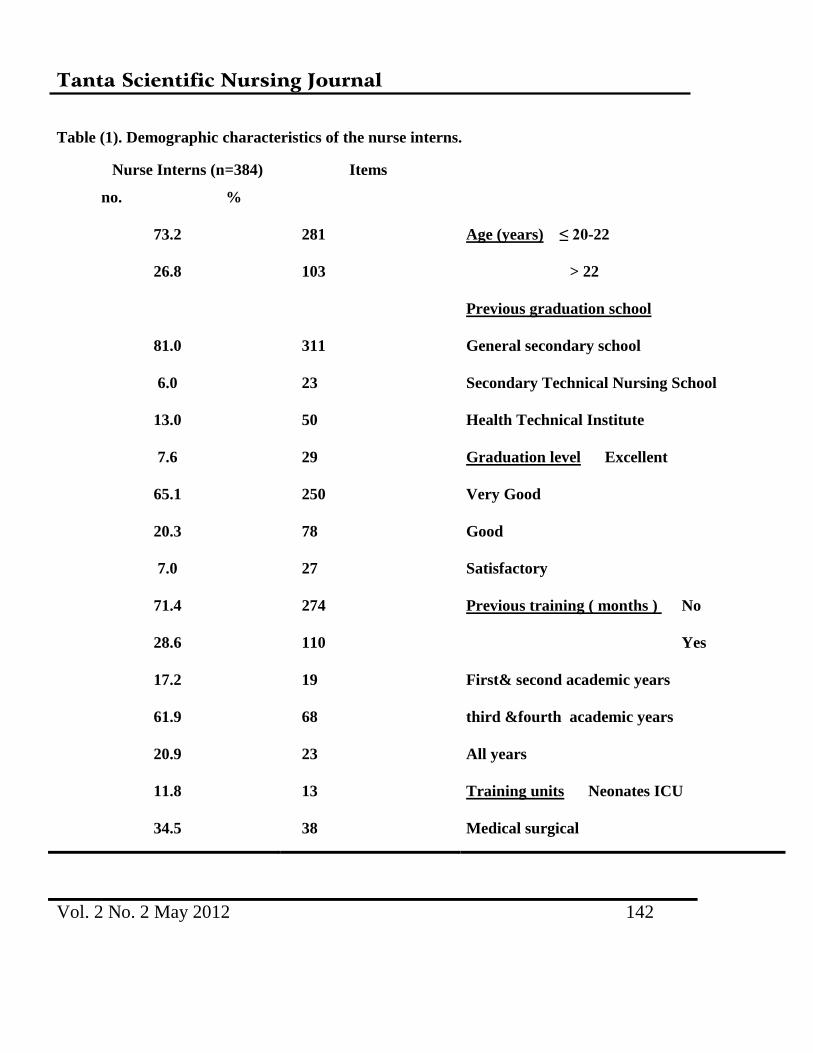
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 142
Table (1). Demographic characteristics of the nurse interns.
Nurse Interns (n=384)
no. %
Items
73.2 281 Age (years) ≤ 20-22
26.8 103 > 22
Previous graduation school
81.0 311 General secondary school
6.0 23 Secondary Technical Nursing School
13.0 50 Health Technical Institute
7.6 29 Graduation level Excellent
65.1 250 Very Good
20.3 78 Good
7.0 27 Satisfactory
71.4 274 Previous training ( months ) No
28.6 110 Yes
17.2 19 First& second academic years
61.9 68 third &fourth academic years
20.9 23 All years
11.8 13 Training units Neonates ICU
34.5 38 Medical surgical
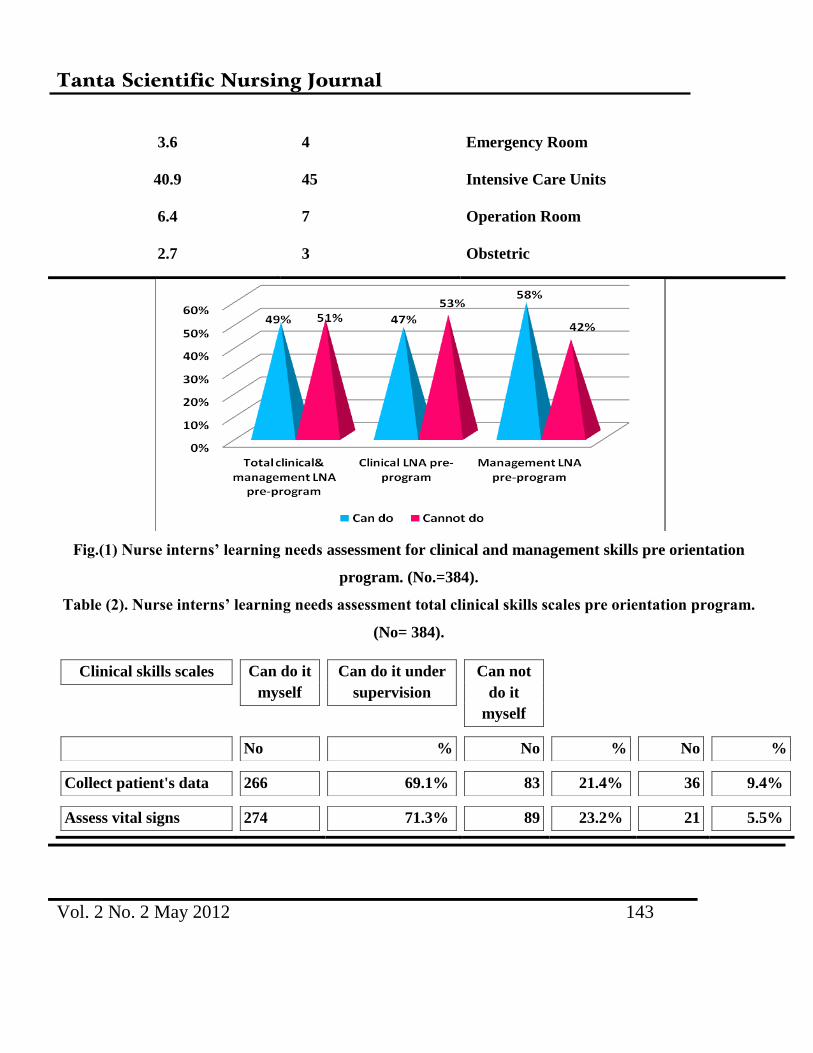
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 143
3.6 4 Emergency Room
40.9 45 Intensive Care Units
6.4 7 Operation Room
2.7 3 Obstetric
Fig.(1) Nurse interns’ learning needs assessment for clinical and management skills pre orientation
program. (No.=384).
Table (2). Nurse interns’ learning needs assessment total clinical skills scales pre orientation program.
(No= 384).
Clinical skills scales Can do it
myself
Can do it under
supervision
Can not
do it
myself
No % No % No %
Collect patient's data 266 69.1% 83 21.4% 36 9.4%
Assess vital signs 274 71.3% 89 23.2% 21 5.5%
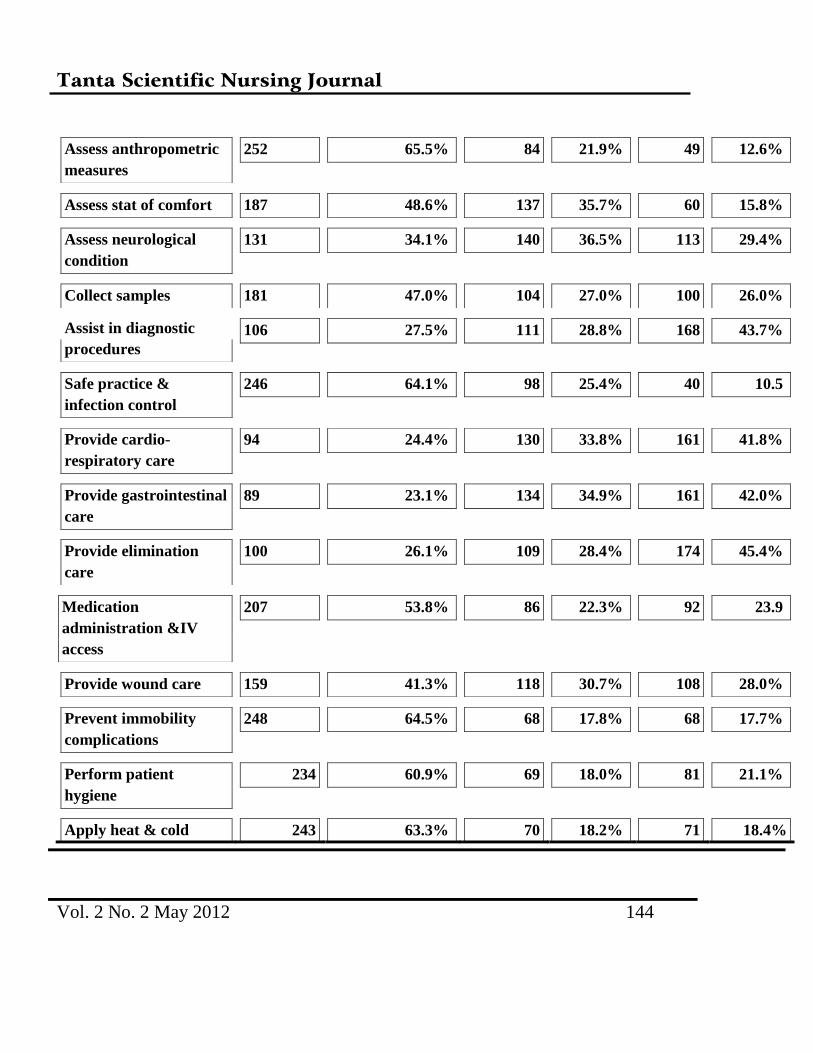
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 144
Assess anthropometric
measures
252 65.5% 84 21.9% 49 12.6%
Assess stat of comfort 187 48.6% 137 35.7% 60 15.8%
Assess neurological
condition
131 34.1% 140 36.5% 113 29.4%
Collect samples 181 47.0% 104 27.0% 100 26.0%
Assist in diagnostic
procedures
106 27.5% 111 28.8% 168 43.7%
Safe practice &
infection control
246 64.1% 98 25.4% 40 10.5
Provide cardio-
respiratory care
94 24.4% 130 33.8% 161 41.8%
Provide gastrointestinal
care
89 23.1% 134 34.9% 161 42.0%
Provide elimination
care
100 26.1% 109 28.4% 174 45.4%
Medication
administration &IV
access
207 53.8% 86 22.3% 92 23.9
Provide wound care 159 41.3% 118 30.7% 108 28.0%
Prevent immobility
complications
248 64.5% 68 17.8% 68 17.7%
Perform patient
hygiene
234 60.9% 69 18.0% 81 21.1%
Apply heat & cold 243 63.3% 70 18.2% 71 18.4%
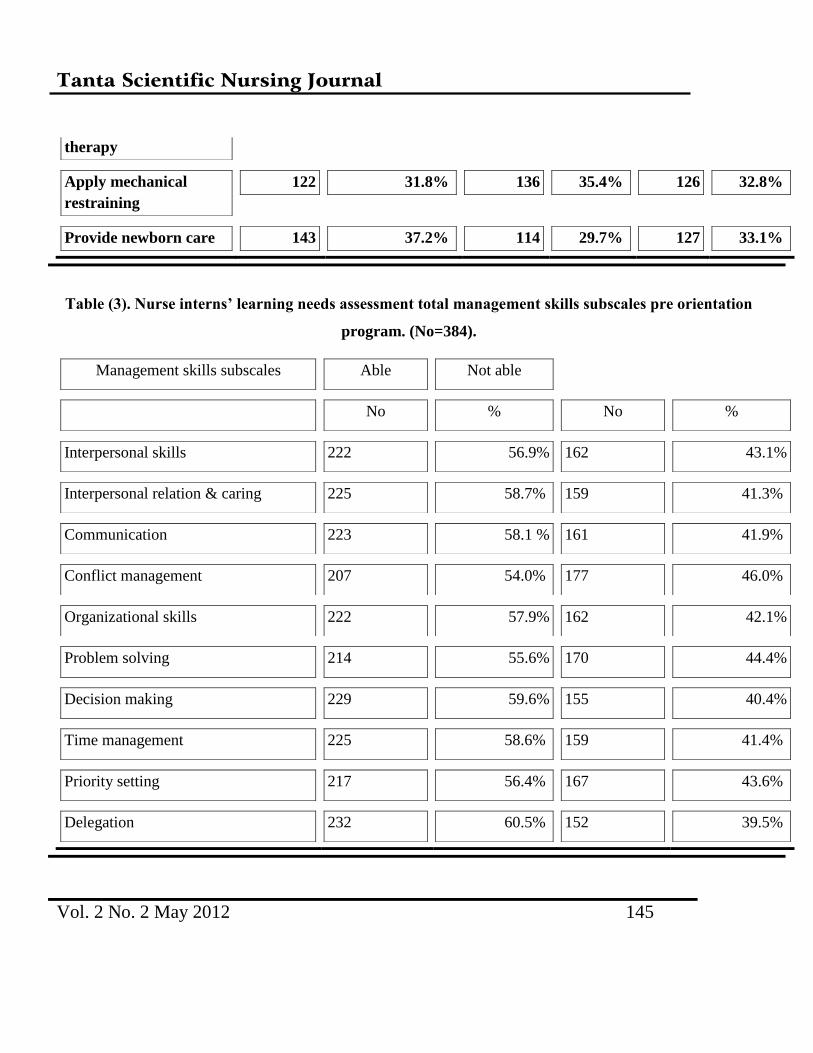
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 145
therapy
Apply mechanical
restraining
122 31.8% 136 35.4% 126 32.8%
Provide newborn care 143 37.2% 114 29.7% 127 33.1%
Table (3). Nurse interns’ learning needs assessment total management skills subscales pre orientation
program. (No=384).
Management skills subscales Able Not able
No % No %
Interpersonal skills 222 56.9% 162 43.1%
Interpersonal relation & caring 225 58.7% 159 41.3%
Communication 223 58.1 % 161 41.9%
Conflict management 207 54.0% 177 46.0%
Organizational skills 222 57.9% 162 42.1%
Problem solving 214 55.6% 170 44.4%
Decision making 229 59.6% 155 40.4%
Time management 225 58.6% 159 41.4%
Priority setting 217 56.4% 167 43.6%
Delegation 232 60.5% 152 39.5%
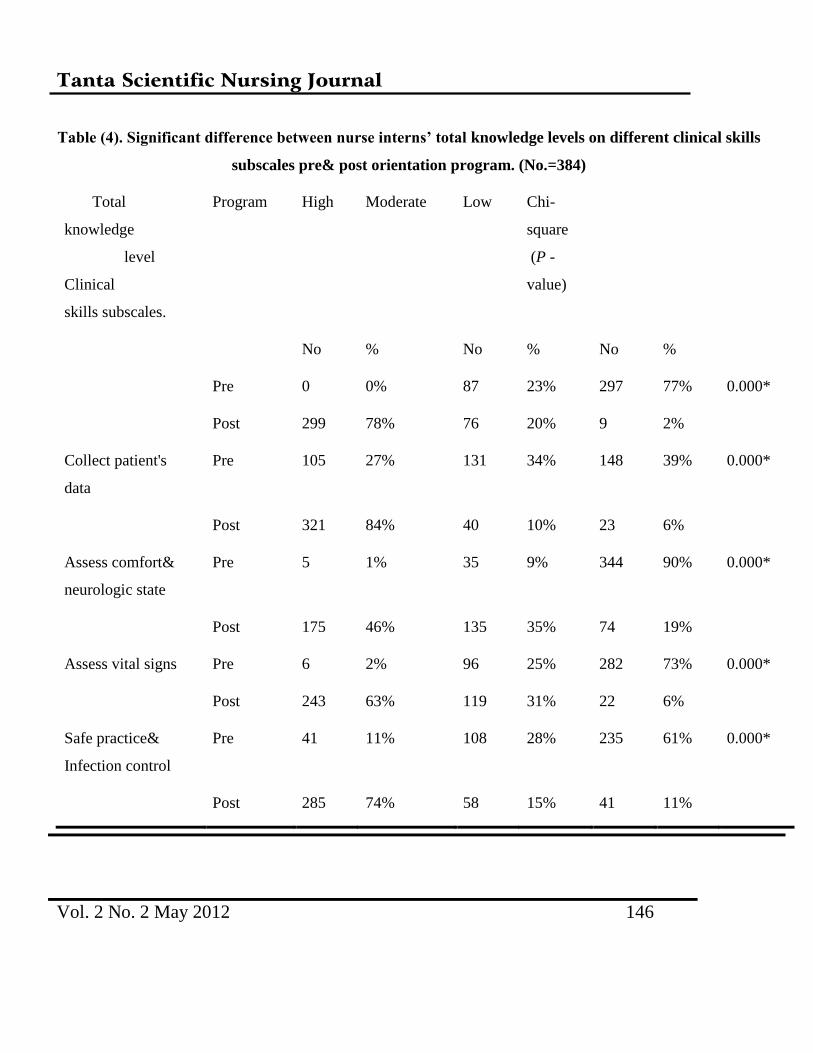
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 146
Table (4). Significant difference between nurse interns’ total knowledge levels on different clinical skills
subscales pre& post orientation program. (No.=384)
Total
knowledge
level
Clinical
skills subscales.
Program High Moderate Low Chi-
square
(P -
value)
No % No % No %
Pre 0 0% 87 23% 297 77% 0.000*
Post 299 78% 76 20% 9 2%
Collect patient's
data
Pre 105 27% 131 34% 148 39% 0.000*
Post 321 84% 40 10% 23 6%
Assess comfort&
neurologic state
Pre 5 1% 35 9% 344 90% 0.000*
Post 175 46% 135 35% 74 19%
Assess vital signs Pre 6 2% 96 25% 282 73% 0.000*
Post 243 63% 119 31% 22 6%
Safe practice&
Infection control
Pre 41 11% 108 28% 235 61% 0.000*
Post 285 74% 58 15% 41 11%
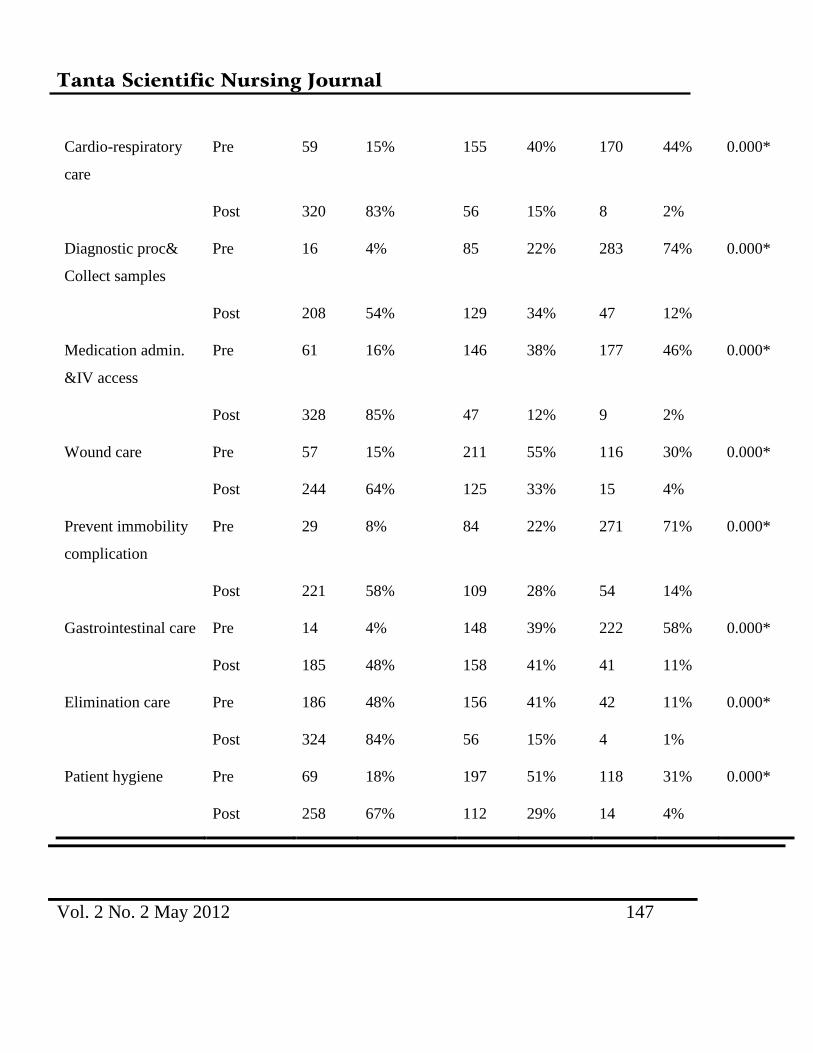
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 147
Cardio-respiratory
care
Pre 59 15% 155 40% 170 44% 0.000*
Post 320 83% 56 15% 8 2%
Diagnostic proc&
Collect samples
Pre 16 4% 85 22% 283 74% 0.000*
Post 208 54% 129 34% 47 12%
Medication admin.
&IV access
Pre 61 16% 146 38% 177 46% 0.000*
Post 328 85% 47 12% 9 2%
Wound care Pre 57 15% 211 55% 116 30% 0.000*
Post 244 64% 125 33% 15 4%
Prevent immobility
complication
Pre 29 8% 84 22% 271 71% 0.000*
Post 221 58% 109 28% 54 14%
Gastrointestinal care Pre 14 4% 148 39% 222 58% 0.000*
Post 185 48% 158 41% 41 11%
Elimination care Pre 186 48% 156 41% 42 11% 0.000*
Post 324 84% 56 15% 4 1%
Patient hygiene Pre 69 18% 197 51% 118 31% 0.000*
Post 258 67% 112 29% 14 4%
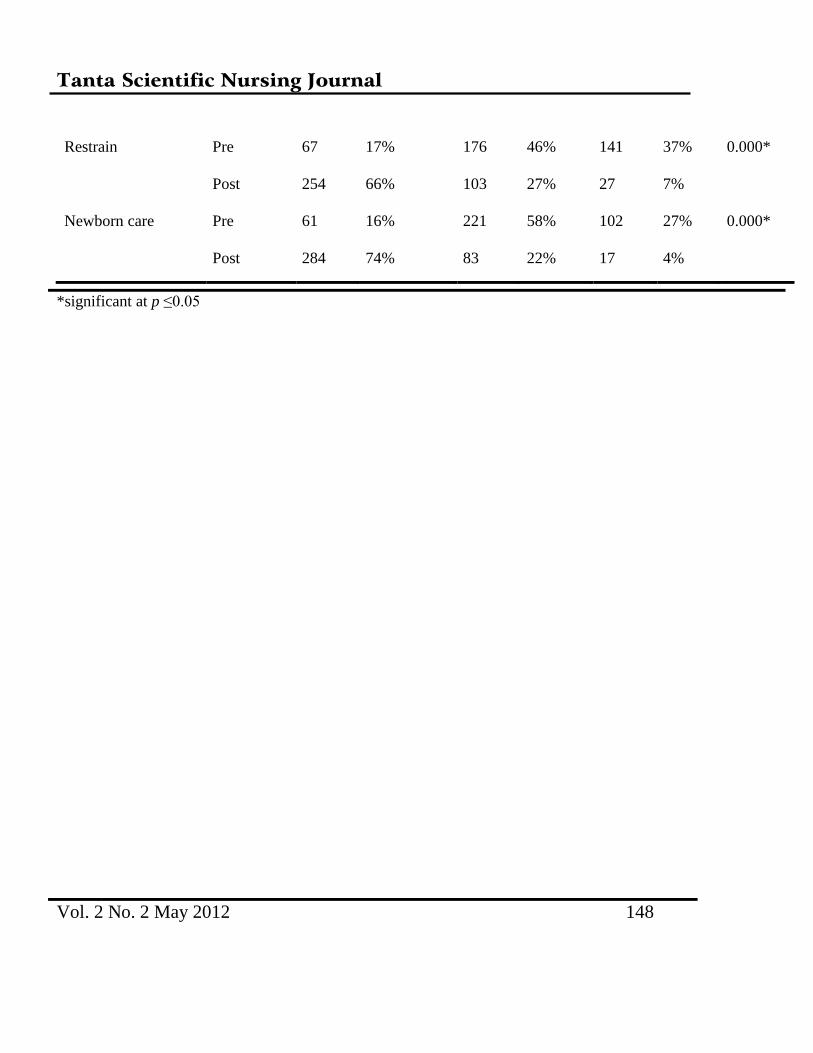
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 148
Restrain Pre 67 17% 176 46% 141 37% 0.000*
Post 254 66% 103 27% 27 7%
Newborn care Pre 61 16% 221 58% 102 27% 0.000*
Post 284 74% 83 22% 17 4%
*significant at p ≤0.05
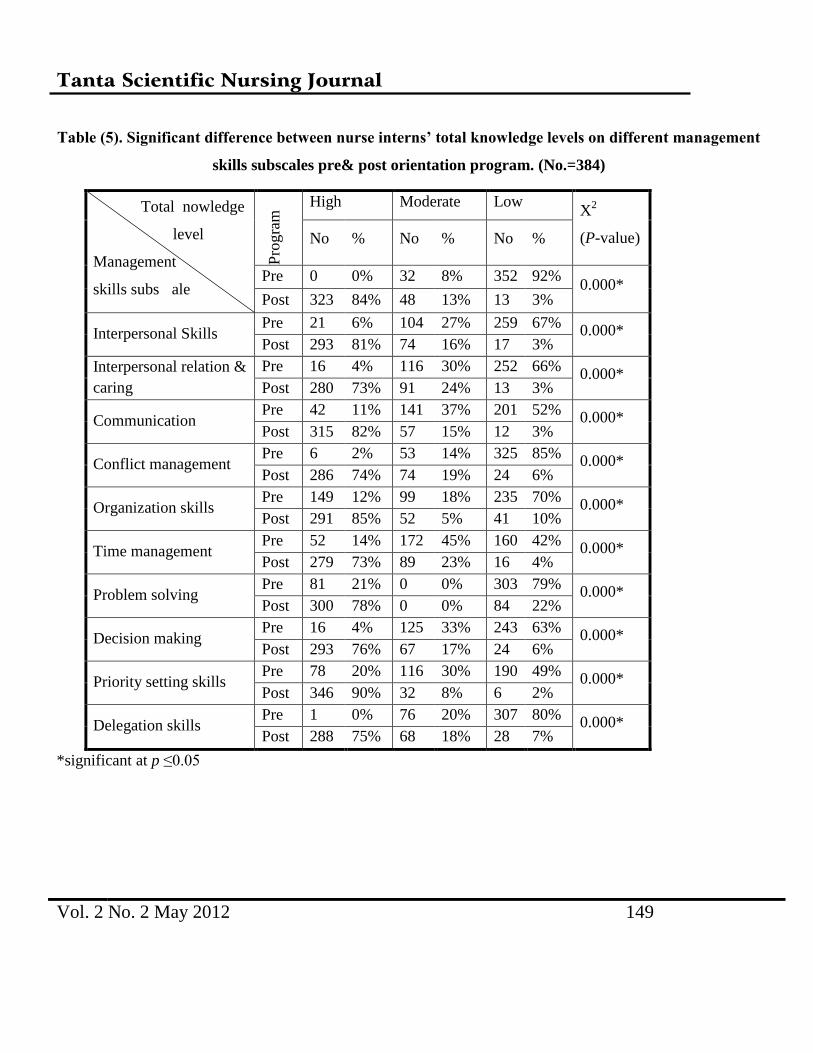
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 149
Table (5). Significant difference between nurse interns’ total knowledge levels on different management
skills subscales pre& post orientation program. (No.=384)
Total nowledge
level
Management
skills subs ale P
rogra
m High Moderate Low
X2
(P-value) No % No % No %
Pre 0 0% 32 8% 352 92% 0.000*
Post 323 84% 48 13% 13 3%
Interpersonal Skills Pre 21 6% 104 27% 259 67%
0.000* Post 293 81% 74 16% 17 3%
Interpersonal relation &
caring
Pre 16 4% 116 30% 252 66% 0.000*
Post 280 73% 91 24% 13 3%
Communication Pre 42 11% 141 37% 201 52%
0.000* Post 315 82% 57 15% 12 3%
Conflict management Pre 6 2% 53 14% 325 85%
0.000* Post 286 74% 74 19% 24 6%
Organization skills Pre 149 12% 99 18% 235 70%
0.000* Post 291 85% 52 5% 41 10%
Time management Pre 52 14% 172 45% 160 42%
0.000* Post 279 73% 89 23% 16 4%
Problem solving Pre 81 21% 0 0% 303 79%
0.000* Post 300 78% 0 0% 84 22%
Decision making Pre 16 4% 125 33% 243 63%
0.000* Post 293 76% 67 17% 24 6%
Priority setting skills Pre 78 20% 116 30% 190 49%
0.000* Post 346 90% 32 8% 6 2%
Delegation skills Pre 1 0% 76 20% 307 80%
0.000* Post 288 75% 68 18% 28 7%
*significant at p ≤0.05
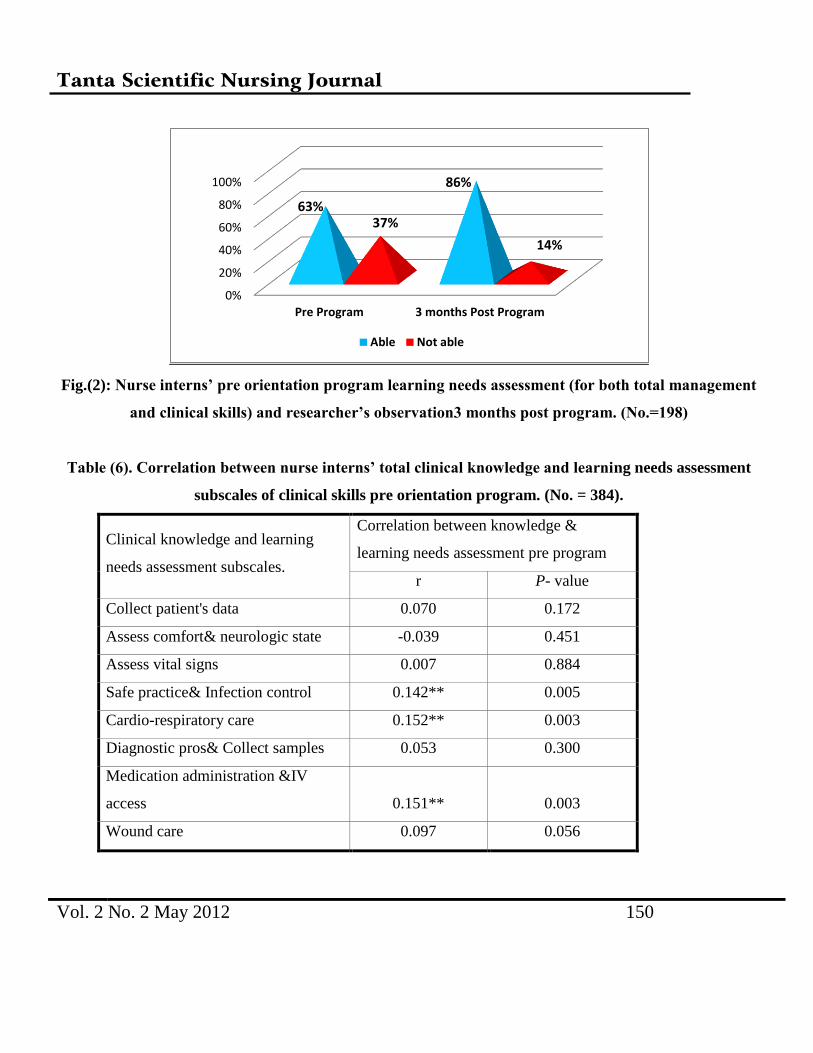
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 150
Fig.(2): Nurse interns’ pre orientation program learning needs assessment (for both total management
and clinical skills) and researcher’s observation3 months post program. (No.=198)
Table (6). Correlation between nurse interns’ total clinical knowledge and learning needs assessment
subscales of clinical skills pre orientation program. (No. = 384).
Clinical knowledge and learning
needs assessment subscales.
Correlation between knowledge &
learning needs assessment pre program
r P- value
Collect patient's data 0.070 0.172
Assess comfort& neurologic state -0.039 0.451
Assess vital signs 0.007 0.884
Safe practice& Infection control 0.142** 0.005
Cardio-respiratory care 0.152** 0.003
Diagnostic pros& Collect samples 0.053 0.300
Medication administration &IV
access 0.151** 0.003
Wound care 0.097 0.056
0%
20%
40%
60%
80%
100%
Pre Program 3 months Post Program
63%
86%
37%
14%
Able Not able
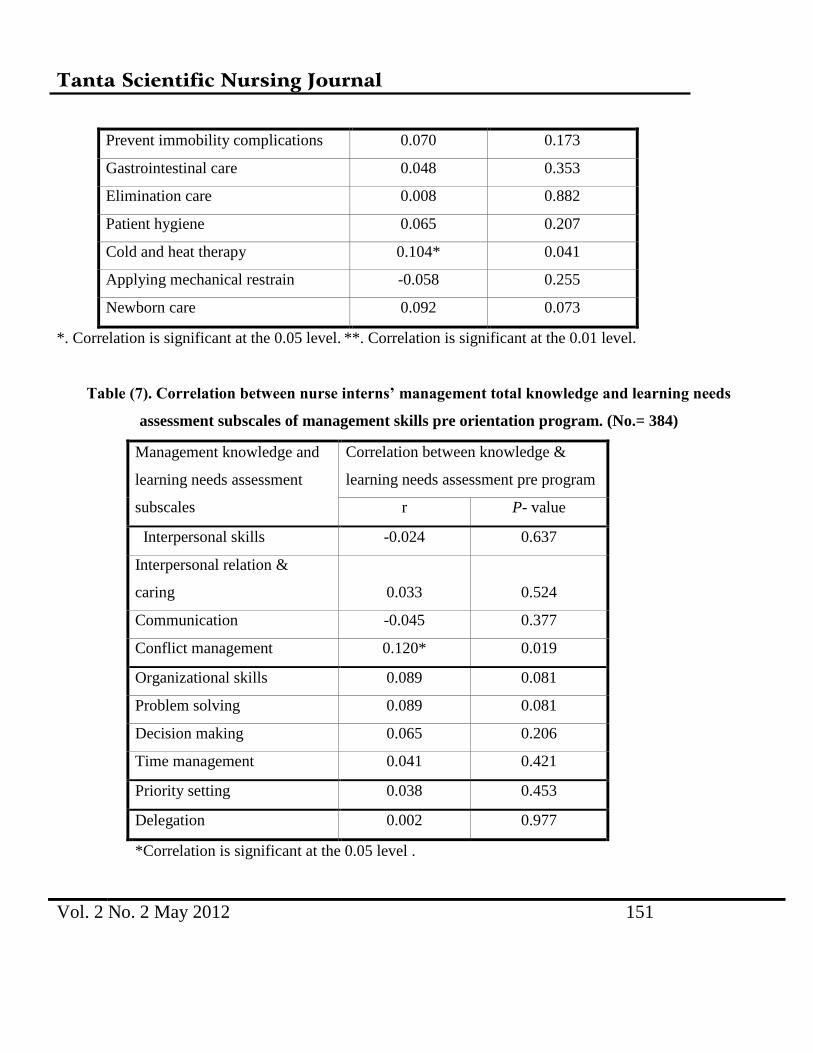
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 151
Prevent immobility complications 0.070 0.173
Gastrointestinal care 0.048 0.353
Elimination care 0.008 0.882
Patient hygiene 0.065 0.207
Cold and heat therapy 0.104* 0.041
Applying mechanical restrain -0.058 0.255
Newborn care 0.092 0.073
*. Correlation is significant at the 0.05 level. **. Correlation is significant at the 0.01 level.
Table (7). Correlation between nurse interns’ management total knowledge and learning needs
assessment subscales of management skills pre orientation program. (No.= 384)
Management knowledge and
learning needs assessment
subscales
Correlation between knowledge &
learning needs assessment pre program
r P- value
Interpersonal skills -0.024 0.637
Interpersonal relation &
caring 0.033 0.524
Communication -0.045 0.377
Conflict management 0.120* 0.019
Organizational skills 0.089 0.081
Problem solving 0.089 0.081
Decision making 0.065 0.206
Time management 0.041 0.421
Priority setting 0.038 0.453
Delegation 0.002 0.977
*Correlation is significant at the 0.05 level .
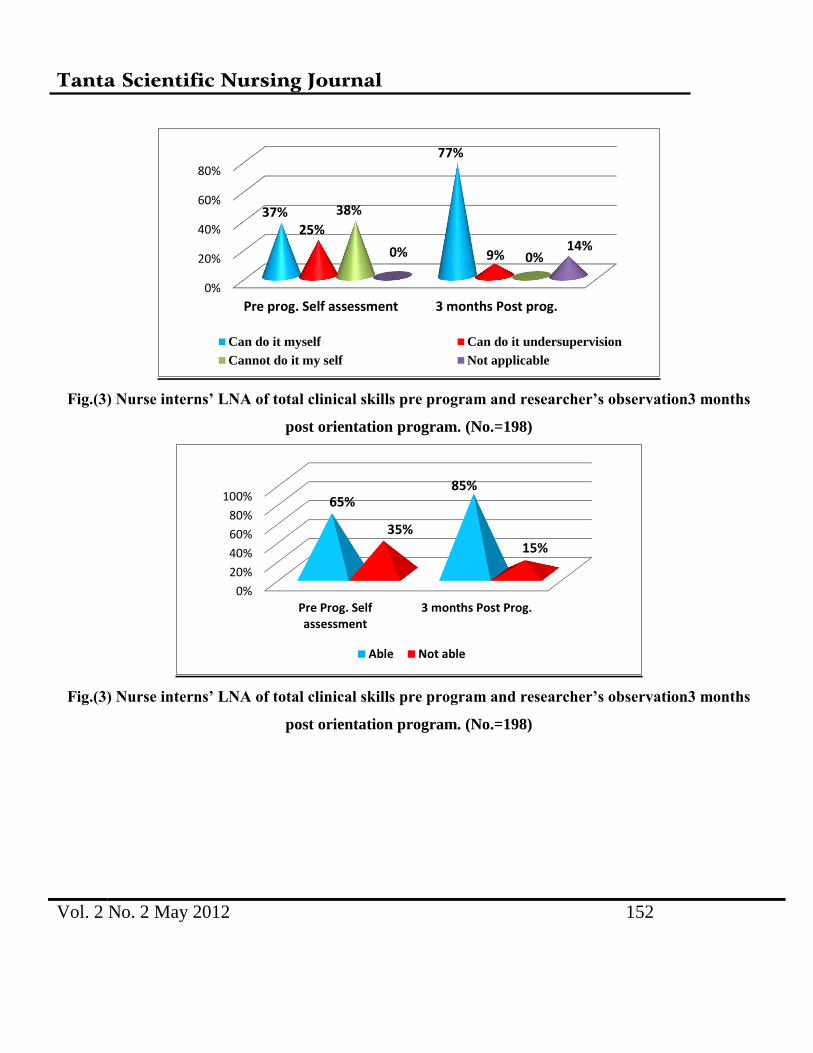
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 152
Fig.(3) Nurse interns’ LNA of total clinical skills pre program and researcher’s observation3 months
post orientation program. (No.=198)
Fig.(3) Nurse interns’ LNA of total clinical skills pre program and researcher’s observation3 months
post orientation program. (No.=198)
0%
20%
40%
60%
80%
Pre prog. Self assessment 3 months Post prog.
37%
77%
25%
9%
38%
0% 0% 14%
Can do it myself Can do it undersupervision
Cannot do it my self Not applicable
0%
20%
40%
60%
80%
100%
Pre Prog. Selfassessment
3 months Post Prog.
65% 85%
35%
15%
Able Not able
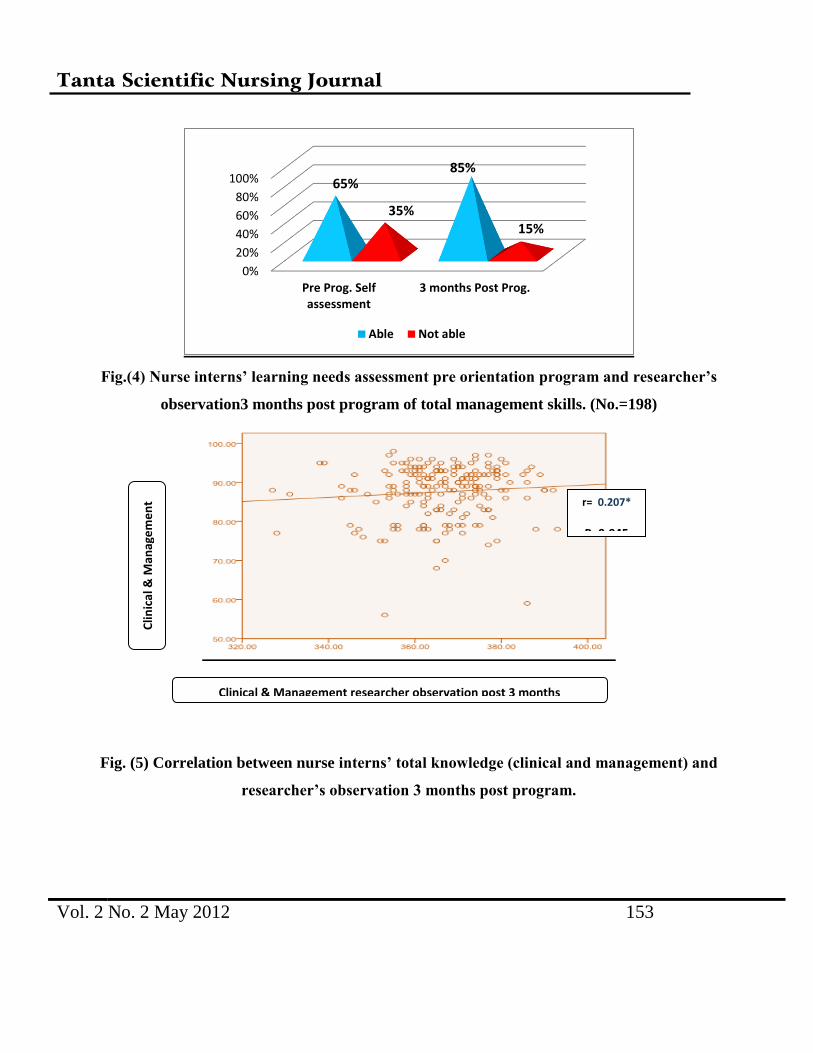
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 153
Fig.(4) Nurse interns’ learning needs assessment pre orientation program and researcher’s
observation3 months post program of total management skills. (No.=198)
Fig. (5) Correlation between nurse interns’ total knowledge (clinical and management) and
researcher’s observation 3 months post program.
0%
20%
40%
60%
80%
100%
Pre Prog. Selfassessment
3 months Post Prog.
65% 85%
35% 15%
Able Not able
Clin
ica
l & M
anag
em
en
t
kno
wle
dge
Clinical & Management researcher observation post 3 months
r= 0.207*
P=0.045

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 154
Discussion
Learning needs assessment guarantee a
relevant and accurate pre-internship
orientation program thus fosters a smooth
transition from nursing students to
professional registered nurse. Results of
using a well designed learning needs
assessment (LNA) tools can guide nursing
faculties to fill in the theory practice gap in
NIs’ performance and strengths the weak
points in the nurse interns’ knowledge.
The present study results revealed no
statistical significant correlation between
NIs’ learning needs self assessment and
their pre-orientation program knowledge on
clinical and management skills. Around
half of NIs assessed themselves as can do
clinical and management skills; in despite of
the incorrect answers for the majority of NIs
on basic knowledge test questions about
clinical and management skills. Most
probably this contradiction is due to their
overestimation of their abilities. So those
NIs require continuous and constructive
feedback on their abilities and progress to
identify gaps between their practice and
related basic knowledge. Khamis (2009)
study about the impact of management
program on competencies of NGs during
internship year supported results of the
present study and found a remarkable
disparity between nurse interns’ knowledge
and the level of their practical skills(19)
.
Feedback is an effective method of
improving performance because it allows
nurse interns to correct earlier
misunderstandings that developed during
learning process. Providing feedback can be
done fairly quickly, with little expenditure
of time to improve the learning process in
clinical setting and ensure interns’ master of
clinical tasks.
The results of present study revealed that
there is a statistical significant correlation
between nurse interns’ total knowledge
(clinical and management) with their
previous training, their graduation level and
their previous graduation school. Really NIs
got high graduation level and had previous
training in private hospitals specially those
trained in ICUs as well as those graduated
from institute or nursing schools got
opportunities to apply their learned skills in

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 155
practical situations, helped them to interact
with more experienced healthcare staff and
improved their skills performance. Beccroft
(2009) study about “internship outcomes of
one year pilot program” supported the
present study findings, and found that high
percent of nursing interns whom had an
excellent graduation level showed high
competency level, while only low percent of
nursing interns who have a good graduation
level showed moderate level of
competency(1)
.
Findings of present study showed that more
than half of NIs assessed themselves as
cannot do both clinical standard and
management skills. Those NIs’ clinical
knowledge test preprogram showed that
they had poor knowledge level regarding
both clinical and management skills.
The fact is that those NIs’ knowledge were
poor about ten out of eighteen skills
understudy including assess state of
comfort, assess neurological condition,
collect samples, assist in diagnostic
procedures, apply safe practice and infection
control measures and apply mechanical
restrain. Besides, they had poor knowledge
level regarding cardio-respiratory,
gastrointestinal, elimination, wound, and
newborn care skills.
The results of LNA revealed that around
forty percent of nurse interns assessed
themselves as being not able to carryout all
the management skills. Those NIs were not
able to carryout interpersonal skills,
organizational skills, priority setting and
delegation skills. Majority of those interns
showed low level of management
knowledge and minority were at moderate
level of knowledge.
These results may be because at the
beginning of their transition NIs suspect
their management knowledge and skills,
they still not have any refreshing courses or
orientation program. Nurse interns look for
internship years as the sparkling beginning
of their professional carrier, and they will be
treated as a trainee, they dream with
practicing under supervision of highly
experienced nursing staff, whom will
provide them with direction. Those interns
need specific job description that clarify
their role and are in need of pre-internship

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 156
orientation program to support their skills
and refresh their knowledge.
The present study findings confirmed
by Morrow (2009) whom found that novice
nurses were inadequately prepared in the
areas of critical thinking skills, decision
making and problem solving(20)
. Also
Greenwood (2000) reported that novice
nurses had poor time management skills and
prioritization, and a general inability to
convert theoretical training to real-world
situations(21)
.
Those NIs were not able to do interpersonal
relation& caring, communication and
conflict management skills. Their lack of
interpersonal management skills knowledge
is the apparent cause for their inability to
carryout these skills. Contradicting to the
present study findings Arthur (2008)
studied assessing nursing students’ basic
communication and interviewing skills
found that nurse interns rated themselves as
able to provide good therapeutic
interpersonal relations and communication
skills while providing practical care(22)
.
Present study LNA revealed that nurse
interns assessed themselves as being not
able to carryout conflict management skills.
This can be interpreted as the pre-graduate
education did not sufficiently prepare those
interns for managing conflict. They studied
lectures on conflict resolution; but they did
not have enough chance to apply theory into
practice. Even during their undergraduate
practice in healthcare setting the instructors
try to overly protect their students and
resolve any conflict with patients, nurses,
doctors, or even with their colleagues.
Obied (2008) study about management of
workplace violence against nurses
confirmed present study and found that NIs’
lack of conflict resolution strategies and
interpersonal skills constitute one of the
main reasons behind NIs’ experience of
workplace violence(23)
.
The results of the LNA of present study
showed that nurse interns assessed
themselves as being not able to carryout
organizational skill. They were not able to
do each of solve problems, make decisions,
or even mange their time. Those interns
showed low knowledge regarding
organizational skills. Those NIs lacking of
organizational knowledge and skills make

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 157
them to feel inadequate and increase their
fear of harming patients or miss any care.
They have to learn how to group
simultaneous interventions to master their
own time, skills, and be able to provide care
independently with no external guidance. So
those NIs require orientation program on
management organization knowledge to
support them to regain self confidence.
Based on the findings of LNA of present
study the nurse interns assessed themselves
as being not able to carryout interpersonal
skills.
Findings of LNA illustrated that nurse
interns assessed themselves as being not
able to carryout decision making skills.
Most probably this result reflects their lack
of decision making skills knowledge. They
answer incorrectly about questions related
to timing of decision making, steps of
decision making process and personal
barriers of decision making. So it is
suggested that a formal orientation program
that enhance critical thinking and decision
making ability should be given to NIs to
improve their knowledge and skills pre-
internship year. Consequently they will be
clinically effective in making decisions and
reduce the risk of committing errors.
Gillespie & Peterson (2009) study about
helping novice nurses make effective
clinical decisions supported the present
study findings and reported that many
novice nurses fall in different errors as they
lack critical thinking and decision making
skills. They stated that novice nurses with
limited experience in the care settings, in
which they work, tend to view decision-
making as nearly responding to patient
complaints and following protocols or
documented care plans. As they make
decisions, their focus leans toward doing,
rather than on thinking and reflecting(24)
.
LNA findings of present study revealed that
nurse interns assessed themselves as being
not able to carryout time management skills.
Those interns were not able to manage
distractions, use time saving strategies,
avoid doing others’ work, or even refuse
responsibility they cannot manage. They
cannot finish most of things they start or
being sensitive for others time. The fact is
that those NIs’ lack knowledge about each
of how to manage their time, prioritize

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 158
competing tasks in a way that best serves
patients needs, respects the team, and
maintains energy and focus throughout the
shift. So they need pre-orientation program
include educational materials on prober time
management.
Smith & Crawford (2003)
supported
present study results and found that novice
nurses is delayed in patient care, due to their
failure to administer in a timely manner,
failure to recognize and failure to intervene
in relation to patient care(25)
.
However most NGs lack the judgment,
confidence, and experience to act
decisively, until they fully develop their
clinical judgment, they must follow the
rules. If the rules don’t cover a particular
situation, they must rely on more
experienced team members for advice and
support. Further confusion may arise when
new nurses are called to help teammates
while operating within the multiple time
demands of a shift.
Saintsing et al. (2011) study about novice
nurse’s clinical decision-making and how to
avoid errors support the present study
results and found that the issues of time
management and critical thinking are two
items that are potentially dependent upon
each other. Novice nurse is likely to make
judgment errors regarding critical thinking
related to real or perceived time
constraints(26)
.
LNA results showed that NIs assessed
themselves as being not able to carry out
delegation skills. Those NIs do not trust
others to carryout their duties and do not
have the courage to take responsibility for
their delegated skills. They cannot select
and organize tasks to be delegated, cannot
select appropriate person for delegation, or
even maintain reasonable control for
delegated tasks. Those NIs got low level of
knowledge regarding delegation skills. Ruff
(2011)
study about delegation skills:
essential to the contemporary nurse
supported the present study and found that
ineffective delegation was cited by nursing
staff as one reason for missed care(27)
.
LNA revealed that NIs assessed themselves
as being not able to carry out priority setting
skills, which matches their low level of
knowledge regarding priority setting. Those
nurse interns cannot write pros and cons for

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 159
options or priorities tasks according to
goals. In addition, they cannot do each of
put clear goals and objectives, organize their
thoughts or even take time to plan their
activities. Most probably those NIs also
lack experience of early detection and
intervention for priority cases which nursing
care can prevent its deterioration.
Immediate post implementation of the
present study well design pre-internship
orientation educational program, NIs
changed significantly from being with low
to be with high level of knowledge on
clinical skills standards procedures; related
to collect patient’s data, cardio-respiratory
care, medication administration, elimination
care, prevent immobility complications,
wound care, diagnostic procedures and safe
practice and infection control; statistically
significantly improved post orientation
program. As well as, an improvement in
management knowledge level showed for
interpersonal, organizational, priority setting
and delegation skills. But still some NIs had
low knowledge level regarding clinical and
management skills, whom need to study
their learned materials.
The findings of the present study is also
supported by Roussel et al. (2006) study on
management and leadership for nurse
administrators asserted that educational
program helped nurses in keeping up to data
with new concepts, increasing knowledge
and competences, modifying their attitudes
and developing their abilities to deal with
patients and problems(28)
.
The present study researcher’s followed up
NIs during their first three months of
internship year to direct them for proper
skill acquisition and socialization. The
researcher arranged that NIs attend simple
orientation at the first three morning shifts
at the beginning of each rotation, to help
them to be familiar with the unit
environment, procedures and staff this was
carried out in cooperation with the HN of
each unit. Each NI was assigned to care for
one patient with experienced RN for first
week. The TUH HNs and number of RNs
were invited to attend with NIs their the pre-
internship orientation program implemented
by the researcher, to be sure for refreshing
their knowledge and to facilitate the future
interns’ socialization and support.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 160
The researcher intended to help NIs
socialization process by which they will
acquire the specialized knowledge, skills,
values, norms and interests needed to
perform their roles acceptably. Beside the
facilitation for professional socialization
process that integrates the cognitive and
affective domains of professional
performance governs their behavior. The
researcher believes the importance that
learning process takes place in a social
environment, so that the learning occurs
through interaction with their actual work
units. Really the attention and the clinical
supervision which NIs received at the
follow up period of internship orientation
program enhanced their sense of confidence
and improve their competence. As well as
improved their performance to role,
responsibilities and patients care quality.
Data analysis of follow up observation sheet
three months post orientation program
revealed significant improvement of NIs’
ability to carryout all clinical skills, in
comparison with their learning needs self
assessment pre-orientation program.
Researcher’s observation also revealed that
majority of nurse interns can by themselves
assess vital signs, state of comfort, collect
samples, provide cardio-respiratory care,
apply mechanical restrain and provide
newborn care. As well as NIs can by
themselves prevent immobility
complications, provide wound care, assess
neurological condition and carryout safe
practice and infection control measures.
According to the researcher’s observation
three months post orientation program nurse
interns’ ability to carryout management
skills of interpersonal, organizational,
priority setting and delegation skills were
significantly improved, in comparison with
their learning needs self assessment pre-
orientation program. So nurse interns should
attend immediate pre-internship orientation
programs to help them to refresh their
knowledge, memorize the basic clinical and
management standards needed to be applied
during their internship year. Learning needs
assessment is very important to meet nurse
interns’ individual needs and to address the
skills required for specific practice areas.
Beside their knowledge must be tested to
identify their actual educational needs.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 161
Designing, implementing the orientation
program and using different teaching
methods helped to evoke nurse interns
maximum benefits and to overcome their
individual differences. Really present
experience assured that at the beginning of
the internship year NIs need to be
supported, encouraged and mentored by the
faculty staff members until they became
confident in their clinical and management
practice.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 162
References
1. Beecroft P.C., Kunzman L., and
Krozek Ch. RN Internship: Outcomes of
a One-Year Pilot Program. Journal of
Nursing Administration. 2001;
31(12):575-82.
2. El-Sayed S.H., Zakaria A.M. and
Shazely M.M. Management Function
and Managerial Skills for Nurse Interns
at Mansoura University Hospitals. The
New Egyptian Journal of Medicine.2007;
36(5):14-22.
3. Cantrell M. and Browne A. The impact
of a nurse externship program on the
transition process from graduate to
registered nurse, Journal for Nurses in
Staff Development.2005; 21 (6) : 249–
256.
4. AboRamadan A. H. Job Analysis and
Description for Nursing Interns at Tanta
University Hospitals. Master thesis.
Faculty of nursing. Tanta University.
2006.
5. Association of Registered Nurses of
Newfoundland and Labrador.
Orientation Programs for Registered
Nurses: Best Practice Guidelines. (2003).
ARNNL .Council Policy Ends, St.
John’s, NL: Author.
6. Casey K., Fink R., Krugman M. and
Propst J. The graduate nurse experience.
Journal of Nursing Administration. 2004;
34 (6), 303–311.
7. Oermann M.H. and Garvin M.F.
Stresses and challenges for new
graduates in hospitals. Nurse Educator
Today. 2002; 22: 225–230.
8. Butler K.M. and Hardin-Pierce M.
Leadership strategies to enhance the
transition from nursing student role to
professional nurse. Nursing Leadership
Forum. 2005; 9 (3), 110–117.
9. Grant J. Learning needs assessment:
assessing the need. BMJ. 2002; 324:156–
9.
10. Lenburg C. Vermot Nurse
Internship Project, retrieved from
http//www.nursingworld.org/ojin/topic10
/tpc.htm. (2000).
11. El-Shimy H.M. Effect of
Implementing an Orientation Program
On The Nurse Interns. Egyptian Medical
Journal. 1996; 13(1):25-31.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 163
12. Stout D. "Performance Analysis for
Training". Niagara Paper Company.
1995. Niagara, WI.
13. Kelly P. Nursing Leadership&
Management. 3rd
ed. Delmar, Cengage
Learning.USA. 2012:674.
14. Adlam K. -A . , Dotchin M. &
Hayward S. Nursing first year of
practice, past, present and future:
documenting the journey in New
Zealand. Journal of Nursing
Management; 2009; 17: 570–575.
15. Hassan R.M. The performance of
Nursing Interns Related to Basic Nursing
Procedures. Unpublished thesis, Faculty
of Ain Shams University.(2001):101-2
16. Onsy N. Impact of Internship
Training Experience on Nurses’ Interns
skill Acquisition, Unpublished thesis,
Faculty of Ain Shams University.1998:
122-3
17. Ratnapalan S. and Hilliard R.I.
Needs Assessment in Postgraduate
Medical Education: A Review. Med
Educ Online [serial online] 2002;7:8.
Available from URL http://www.med-ed-
online.org
18. Donald E.M.J. and, Donald L.C.
Needs assessment. In: Continuing
Medical Education: A Primer.Westport:
CT: Praeger, 1992.
19. Khamis L. Impact of Management
Program on Competencies of
Baccalaureate Nursing Graduates During
Internship Year. Unpublished
Unpublished Doctoral Thesis. Faculty of
Nursing. Tanta University. 2009.
20. Morrow S. New graduate
transitions: leaving the nest, joining the
flight. Journal of Nursing Management.
2009; 17: 278– 287.
21. Greenwood J. Critique of the
graduate nurse: an international
perspective. Nurse Education Today.
2000; 20: 17–23.
22. Arthur D. Assessing nursing
students’ basic communication and
interviewing skills: the development and
testing of a rating scale. Journal of
Advanced Nursing. 2008; 29(3):658-659.
23. Obied H.K. Management of
workplace violence in Emergency
Hospital Tanata University.2008.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 164
Unpublished Master thesis. Faculty of
Nursing Tanta University.
24. Gillespie M. and Paterson B. L.
Helping Novice Nurses Make Effective
Clinical Decisions: The Situated Clinical
Decision-Making Framework. Nursing
Education Perspectives. 2009; 30
(3):164-170.
25. Smith J. & Crawford L.
Medication errors and difficulty in first
patient assignments of newly licensed
nurses. JONAS Healthcare Law, Ethics
and Regulation. 2003; 5: 65–67.
26. Saintsing D. , GIBSON L .M. and
Pennington A.W. The novice nurse and
clinical decision-making: how to avoid
errors. Journal of Nursing Management.
2011; 19:354–359.
27. Ruff V. A. "Delegation Skills:
Essential to the Contemporary Nurse"
(2011). Master of Arts in Nursing
Theses. St. Catherine University Paper
21.
http://sophia.stkate.edu/ma_nursing/21
28. Roussel L. and Swansburage R C.
Management and Leadership for nurse
administrators. 4th
ed., Boston, Jones and
Barlett Publ. Inc. 2006: 45,47-8,

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 165
Life Style Profile of School Age Children Suffering From Pathological Stuttering
Rahma Soliman Bahgat
Professor of Pediatric Nursing, Faculty of Nursing, Tanta University
Dr. Mohammed El-Sayed Darwish
Lecturer of Phonetics E.N.T Department, Faculty of Medicine, Head of Speech Therapy Center
Mervat Ali Abdo Said Ahmed
B. S. C. Nursing, Faculty of Nursing Tanta University
Abstract
Stuttering as a speech event that contains intraphonemic disruption, part-word repetitions,
monosyllabic whole word reputations, prolongation and silent fixations (blocks).The present
study aimed to investigate the lifestyle profile of children suffering from pathological stuttering
and to identify the factors that worsen or improve the child with pathological stuttering. This
study followed a descriptive design. The study was conducted on 60 children who were attending
the speech therapy in Tanta University. Data were collected by using two tools: questionnaire
sheet, observation checklist. The results revealed, a mean age of stuttering children, it was found
that 63.3% of children with stuttering had a mean age of 8.17+ 1.66 years. Significant difference
was found between the mean age of stuttering children and his socialization. Significant
difference was found between the mean age of stuttering children and response to treatment.
From the present study it can be concluded that the pathological stuttering as disease is easy to
diagnose, difficult to treat has many negative impact on physical, psychological, social and
spiritual aspect of children life. This study recommends that searching for the causation of
stuttering. Health education and counseling of stuttering children and their mothers includes
follow up to speech therapy, family
Introduction

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 166
School-age period characterized by
cognitive and language development
progresses rapidly. Vocabulary expands, and
Sentence structure becomes more
complex.(1)
The assessment of the progress
in language development includes
examination of three interactive components
of language itself: phonics, or speech sound;
syntax or grammar and semantics or
meaning in language forms such as word
and sentence. Usually, speech is fluent,
fluent speech is free of any interruption,
blockage but disfluency is defined as a
breakdown or blockage in the forward flow
of speech. The occurrence of disfluency is
not the same of stuttering though stuttering
is characterized by an excessive amount of
disfluency(2,3)
One of the most common
speech disorders is stuttering. This disorder
is state mixed of theses of item as; word
break, protracted telling, repeating the first
sound and lock or stopping but none of these
items are lonely defined stuttering.
It can
also be defined as speech have difficulty
speaking because of repetition, protraction,
or involuntary lock.(4,5)
Stutter is a complex,
multi-dimensional. Stuttering can range in
frequency and intensity from mild to severe.
Stress can sometimes make it worse. The
struggle to speak may be accompanied by
physical gestures or movements (6)
Prevalence of stuttering how many
people stutter at a given point in time appear
to be somewhat lower than 1 % (according
to Craig; 2002 (7)
the actual incidence is
approximately 5% with onsets. Occurring
mainly at the age Pre School (Andrews
Harris, 1964; Manson, 2002) is about 2,
5%that is, about 1in 20 children now stutter
incidence is about 5% or 1in 20 children at
same point in childhood(8).
Males stutter than
females. People who stutter make up about
1%in the West Indies, 3-4%of population
stutters. African countries seen to have the
highest prevalence of the stuttering with
about 8-9% of population stuttering (9)
Causes of stuttering in children are not
surely known, but most researchers believe
that the stuttering occurs as the result of a
variety of factors. They may include one or
more of the following First; Genetic plays
role sixty percent of all people who stutter
have close family member who also stutters
(zerbroswki, 2003). Scand; Developmental

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 167
stuttering beginning at the age of 18 months
to 2 years, as they hone their speech and
language skills. Third; neurological factors
researchers has found in some cases, there
seems to be a problem in the way language
is transmitted through the brain. Scientists
don’t know exactly why this occurs (10, 11)
Language and communication skills an
essential of school life is the use of a system
of symbols for communication and thought.
Early in school life judgments are made
intuitive on superficial appearance with
increasing experience and language at his
disposal. The child can image complex
situation think out the most appropriate
solution and anticipate the outcome. The
child has developed logical thinking from
assimilating experience into schemes (2, 3)
Life style is a way of living including
behaviors that promote or impair good
health and longevity, the young child with
stuttering must learn how to adapt their self
care and minimize any disruption of their
lifestyle (12)
so, the contents of life style
profile program of the stuttering child
should focus on the needs and capabilities of
the learners to ensure the three main
categories including survival skills, health
maintenance skills and health promoting
skills (13, 14, 15)
Stuttering education can be
divided into three main categories survival
skills, health maintenance skills and health
promotion skills
Health maintenance
preserves the present state of health and
health promotions skills maximize the
optimal level of functioning and health
hazard are reduced. The care program of
those children must invade also every aspect
of patient's life including home &school.
These skills comprise the necessity for
scheduled speech therapy, regular physical
activities, normal communication with
others.(16)
Stuttering impact in their
academic performance at school and
relationship with teacher and classmates;
according to the study of klompas and Rass(
2004) on life experience of individually with
stuttering(17)
The nurse play an important role
for the care of stuttering children which help
in improving the quality of life and
facilitating the children and family's
adaptation to this problem. She encourages
the child to adjust himself to live a
satisfactory life and to be a productive

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 168
number in the society it is very important for
nurse to study the life style of stuttering
children to be able to achieve her role
efficiency (18)
Aim of the study:
1-To investigate life style profile of school
age children suffering from pathological
stuttering.
2- Identify the factor that worsen or
improves the child with pathological
stuttering.
Materials and Method
Research design
A descriptive design was used in this study
Setting: The study was conducted at the
Speech Therapy Center of Tanta University
Hospital
Subjects:
Composed of 60 school age children
suffering from pathological stuttering and
their mothers or caregivers who attended the
previous setting were included. The
children had the following criteria: -
Both sex, Age ranged from 6-15years. Free
from any other speech problem. Started
speech therapy.
Tools of data collection:
Two Tools Were Used In Data Collection:
Tool (I): Structured Questionnaire sheet
It was developed by the researcher after
reviewing of literature to obtain the
following information:
a) Biosocial data of both pathological
stuttering children Such as:
Age, sex, birth order, educational level
Development history such as first defines of
family, sitting, walking, talking, control of
bladder, delay of language.
b) Biosocial data of mothers Such as:
Age, educational level, occupation, family
size, number of siblings, Family history of
stuttering, presence of parental
consanguinity.
c) The three main categories of health
promoting life style Profile:
Survival skills.
Health maintenance skills.
Health promotion skills.
1) Survival skills
Entailed The Following Items:
Items related to the need for speech
therapy
Relation between speech therapy and speech
production

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 169
Items related to children communication
with others.
Information about speech therapy per week
and its effect.
Schedule for speech therapy.
Psychological assessment was done to
assess psychological state of school age
children during speech session such as
(anxiety, anger, and avoidance)
(2) Health maintenance skills
They entailed The Following Items:
- Physical exercise such as different
types of sports.
-Social relations of the stuttering child
as making friendly relationship with
classmates, neighbors and participation in
activities with others, playing in groups,
school or in the club.
3) Health promoting skills
They entailed the following items: Ask
mothers about some information, if not
they should be given in counseling:
Counseling of the school age children
suffering from pathological stuttering and
their mothers
-Counseling is a kind of experience that will
help them to change their attitude, which
includes: -Help the child in every possible
way to feel that he is normal
Be ready to make reasonable change in the
environment to facilitate verbal
communication
Reduce communication stress
Be good listener
Allow time for the child to speak
-Don’t ask the child to talk when he is very
emotional stressed especially when crying
Don’t allow others to tease, ridicule,
interrupt or joke about the child's speech
Follow up visits for speech therapy and its
recording in a certain file of the outpatient
clinic
Tool (II): Observation checklist
It was developed by the researcher after
reviewing the literature to observe school
age children suffering from pathological
stuttering and their mothers during speech
therapy.
Method
1-AdministrativeProcess
An official permission was obtained
from the head of speech therapy department
for caring out this study.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 170
- Children and their mothers were
selected by using simple random
method.
- Based on reviewed literature, the tool
of study was developed.
- - Data for this study covered a period
of five months from August 2012 to
December 2012.
- Both nurses and other working in the
clinic were informed about the role
of the researcher to gain their
cooperation and secure proper
communication.
- Children and their mothers' consents
were obtained to participate in this
study.
2- Development of the Study Tools:
Two tools were designed and used in
this study: a questionnaire sheet and
observation checklist was developed after
reviewing recent literatures.
3- Ethical consideration:
Privacy and confidentiality of data
and results were considered. Also the study
samples were informed that they can with
draw from the study at any time.
4- Pilot Study:
A pilot study was carried out on a
sample of 10 children and their mothers/
caregivers to verify the applicability,
feasibility and test the clarity of the
questions and estimate the time required for
each interview. The necessary modification
was carried out. The data obtained from the
pilot study was analyzed then some
questions were restated and some items were
added.
5- The Actual Study
- Children and their mothers'/
caregivers were interviewed using a
questionnaire sheet in the outpatient
speech therapy to assess their
knowledge. Every child and his or
her mother /caregivers was
interviewed for 20-30 minutes.
- The researcher observed children
and their mothers /caregivers while
taking speech therapy regarding the
following:-
a) Speech production of school age
children such as:
- Frequency of occurrence of
stuttering.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 171
- Duration and consistency of
stuttering.
- The child uses a speech rate that is
either too fast or too slow.
- The child repeats the beginning
sound of words.
- The child repeats whole words.
- The child repeats whole phrases.
- The child uses interjections.
- The child engages in additional
behavior when speaking.
- Presence of any other speech
disorder and symptoms appear
during therapy.
- Observe mothers when
demonstrating instruction provided
by the doctors.
b) Communication Skills
To assess the following information:
Verbal and non verbal abilities
1) Vocalization such as:
-The child has difficulty to remember and
use content area terms
The child uses immature vocabulary
- The child has difficulty making word
association or comparisons
2) Social pragmatics such as:
- The child is cooperative and attentive.
- The child uses poor eye contact.
- The child is easily distracted or has short
attention.
- The child is easily frustrated or
impulsive.
- The child has difficulty using language
for the purposes.
- The child prefers structure routine and
prefers to spend more time alone rather
than in-group.
Statistical design:
The collected data were organized,
tabulated and statistically analyzed using
SPSS statistical package version 19.
Numerical variables were presented as mean
and standard deviation. for comparison of
mean values, student’s t test was used for
categorical variables , the number and
percent distribution was calculated and
difference were tested using Monte Carlo
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 172
exact test. Chi square was not used
because of small sample size and presence
of small observations in some categories
which is one of the limitations of the use of
chi square. Spearman’s correlation was used
to test association between stuttering and
total socialization score. The level of
significance was adopted at p<0.05.
Results
Table (1) shows the percentage
distribution of mothers/caregivers according
to their biosocial characteristics. It is
observed that the highest percentages of
mothers (40%) were aged 30 years, with a
mean age of (34.92+5.56) years. Illiteracy,
reading and writing prevailed in (13.4%)
and university grades in (35%) while
primary and secondary grades had more
percentage than others (51.7%). More than
half of the samples (63.3%) were
housewives but (36.7%) are employees.
Also this table shows that more than half of
the sample (55%) have 3-4 members in the
family with a mean of (3.60+1.62).
Regarding the family residence, it is clear
that about more than half 58. 3% of the
samples live in urban area and about
(41.7%) of the samples live in rural area.
Table (2) shows the percentage
distribution of children characteristics
according to family history. The positive
family history of stuttering constituted
(25%) of the sample distributed as follows:
uncles (40%) ante (33.3%) and (26.7%)
cousins. It is noticed that the start of
stuttering at three years occurred in (35%)
also gradual illness in (63.4%) This table
shows also positive parents consanguinity in
(25%) while positive sibling history of
stuttering in (16.7%).A reason for stuttering
was found in 28.3%
Table (3) shows the percentage distribution
of children according to response to
treatment. It is noticed that more than half of
the sample (61.7%) had disturbance of
normal speech. It is clear that (93.3%) had
impact of irregular speech therapy. Children
with stuttering taking therapy constituted
(53.3%), maintenance follow up at home
(11.7%) compared to those taking oral
treatment is (1.7%).

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 173
According to psychological state of
children during session, it is clear that about
half of the sample (50%) had anxiety state,
less slightly than one third of the sample
(31.7%) had anger and avoidance was found
in (18.3%).
Table (4) shows the correlation between
children response to treatment and their age
in years. A significant difference is observed
between children age in years and having
response to speech therapy (P= 0.017). No
significant differences were observed
between disturbances of a normal speech,
impact of irregular speech therapy, type of
impact, stage of treatment, function of
speech session, needs for speech per week,
content of speech session, psychological
state during speech session ( P = 0.811,
0.567, 1.000, 0.083, 1.000, 0.833, 0.317,
0.983 respectively).these findings are
illustrated in figure (4-10).
Table (5): shows the correlation between
children response to treatment and mothers'
educational level. A significant difference
was observed between mothers educational
level and having need for speech therapy
session and response to speech therapy
treatment (P= 0.05, 0.033). The table
illustrates that no significant differences
were observed between mothers educational
level and disturbance of a normal speech ,
impact of irregular speech therapy, type of
impact, stage of treatment, function of
therapy, content of speech session,
psychological state during session( P =
0.683, 0.817, 0.550, 0.500, 0.767, 0.450,
0.567 respectively ).
Table (6): illustrates the comparison of
total socialization score in relation to
language delayed. No significant difference
between socialization and delayed language
development was found (p= 0.691) and (t
test = 0.399).
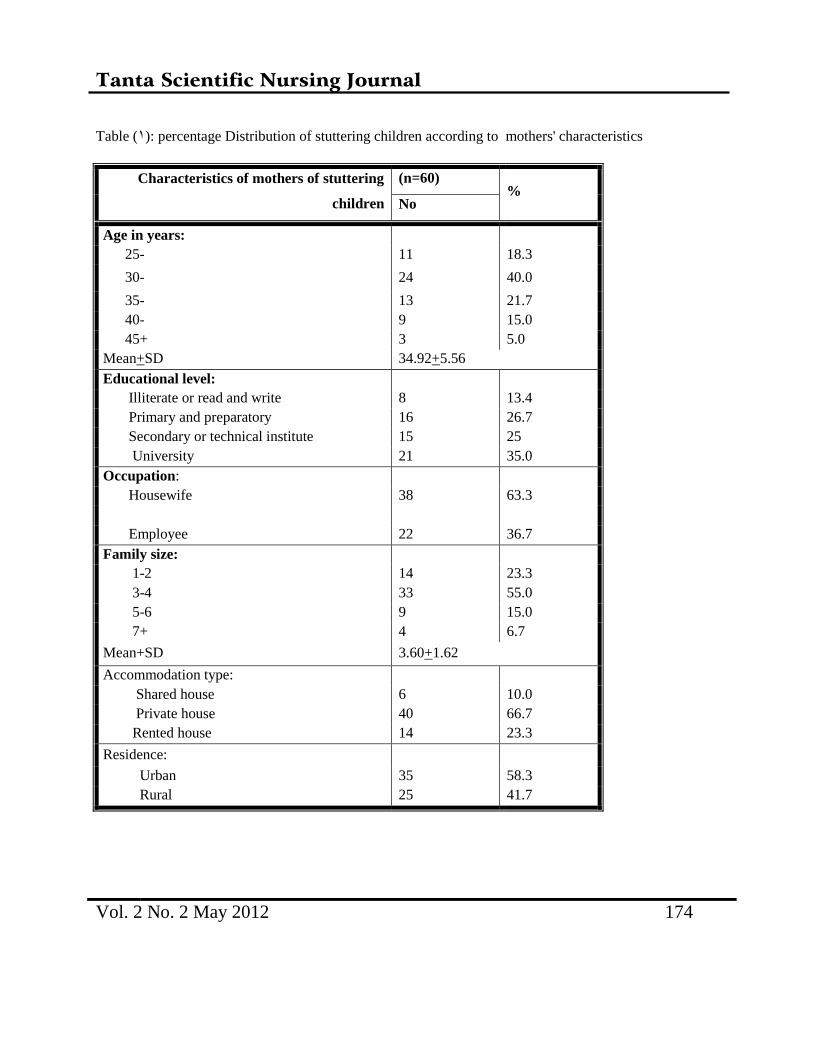
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 174
Table (1): percentage Distribution of stuttering children according to mothers' characteristics
Characteristics of mothers of stuttering
children
(n=60) %
No
Age in years:
25- 11 18.3
30- 24 40.0
35- 13 21.7
40- 9 15.0
45+ 3 5.0
Mean+SD 34.92+5.56
Educational level:
Illiterate or read and write 8 13.4
Primary and preparatory 16 26.7
Secondary or technical institute 15 25
University 21 35.0
Occupation:
Housewife 38 63.3
Employee 22 36.7
Family size:
1-2 14 23.3
3-4 33 55.0
5-6 9 15.0
7+ 4 6.7
Mean+SD 3.60+1.62
Accommodation type:
Shared house 6 10.0
Private house 40 66.7
Rented house 14 23.3
Residence:
Urban 35 58.3
Rural 25 41.7
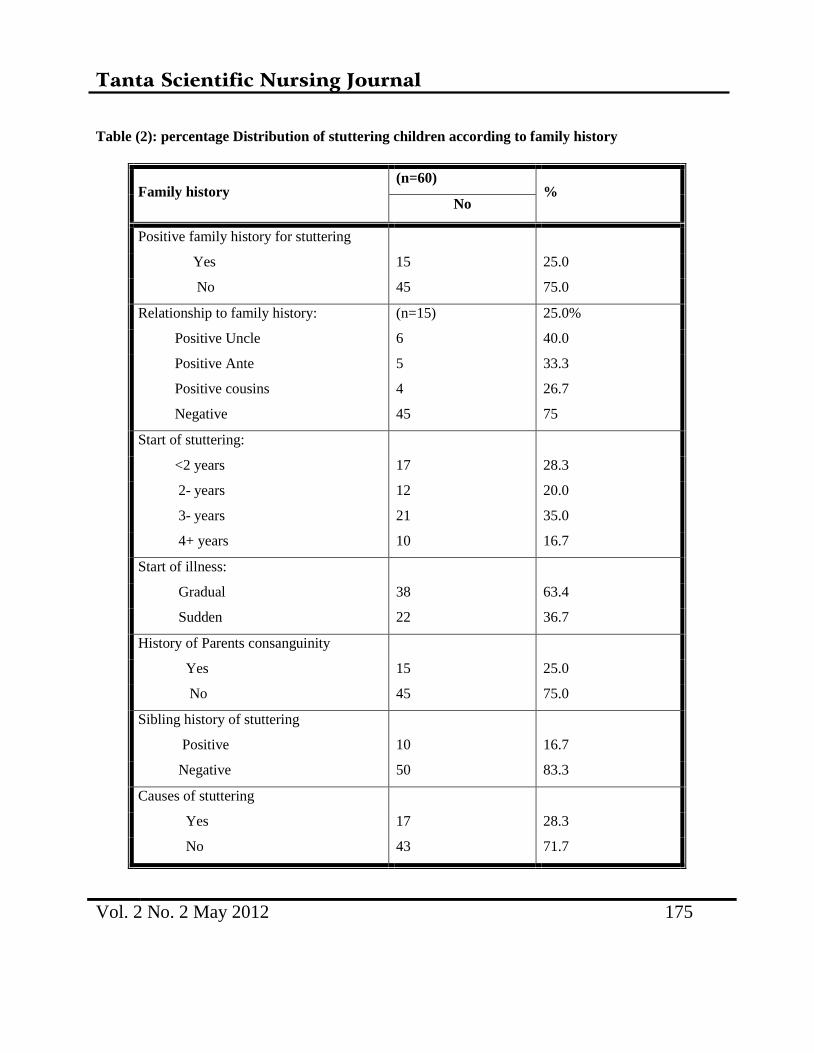
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 175
Table (2): percentage Distribution of stuttering children according to family history
Family history (n=60)
% No
Positive family history for stuttering
Yes 15 25.0
No 45 75.0
Relationship to family history: (n=15) 25.0%
Positive Uncle 6 40.0
Positive Ante 5 33.3
Positive cousins
Negative
4
45
26.7
75
Start of stuttering:
<2 years 17 28.3
2- years 12 20.0
3- years 21 35.0
4+ years 10 16.7
Start of illness:
Gradual 38 63.4
Sudden 22 36.7
History of Parents consanguinity
Yes 15 25.0
No 45 75.0
Sibling history of stuttering
Positive 10 16.7
Negative 50 83.3
Causes of stuttering
Yes 17 28.3
No 43 71.7
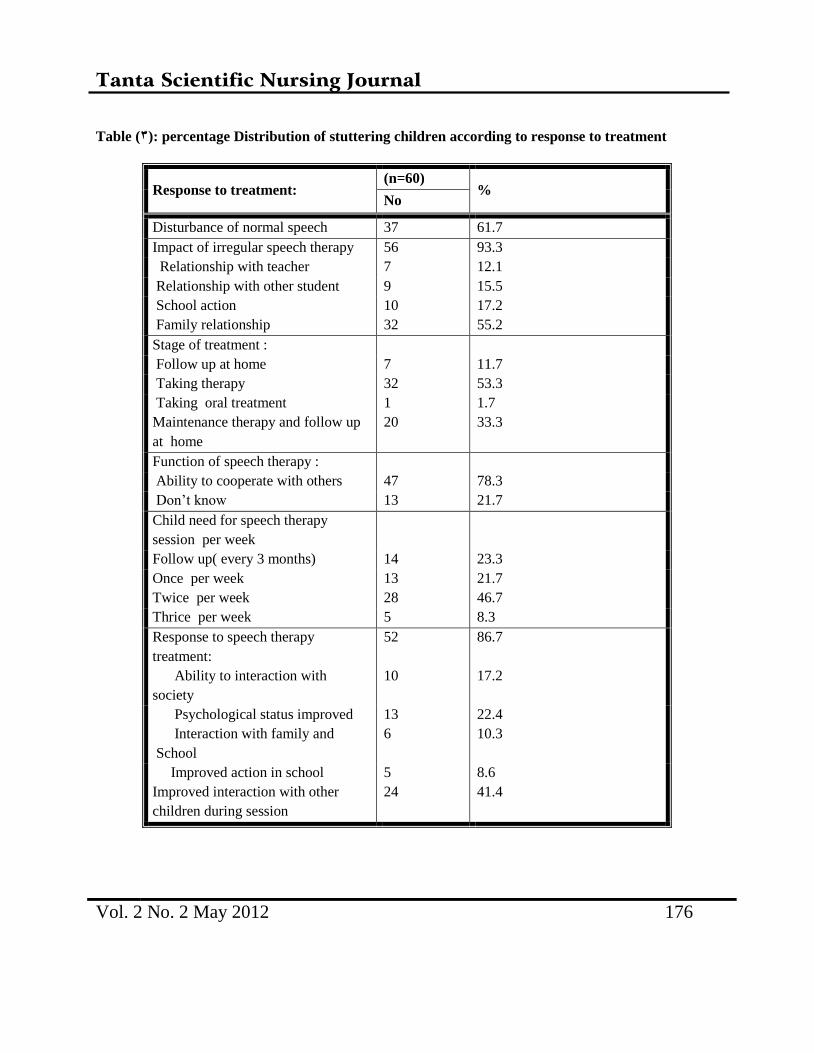
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 176
Table (3): percentage Distribution of stuttering children according to response to treatment
Response to treatment: (n=60)
% No
Disturbance of normal speech 37 61.7
Impact of irregular speech therapy 56 93.3
Relationship with teacher 7 12.1
Relationship with other student 9 15.5
School action
Family relationship
10
32
17.2
55.2
Stage of treatment :
Follow up at home 7 11.7
Taking therapy 32 53.3
Taking oral treatment
Maintenance therapy and follow up
at home
1
20
1.7
33.3
Function of speech therapy :
Ability to cooperate with others 47 78.3
Don’t know 13 21.7
Child need for speech therapy
session per week
Follow up( every 3 months) 14 23.3
Once per week 13 21.7
Twice per week 28 46.7
Thrice per week 5 8.3
Response to speech therapy
treatment:
52 86.7
Ability to interaction with
society
10 17.2
Psychological status improved 13 22.4
Interaction with family and
School
6 10.3
Improved action in school
Improved interaction with other
children during session
5
24
8.6
41.4
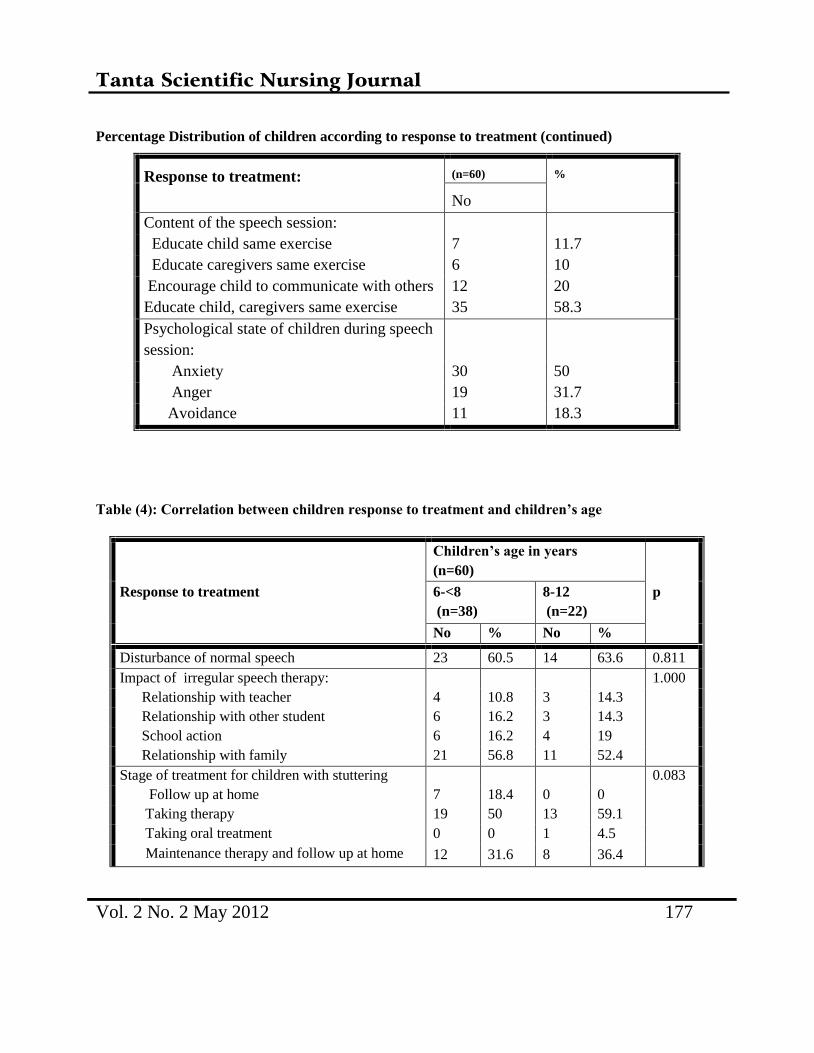
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 177
Percentage Distribution of children according to response to treatment (continued)
Response to treatment: (n=60) %
No
Content of the speech session:
Educate child same exercise 7 11.7
Educate caregivers same exercise 6 10
Encourage child to communicate with others
Educate child, caregivers same exercise
12
35
20
58.3
Psychological state of children during speech
session:
Anxiety 30 50
Anger 19 31.7
Avoidance 11 18.3
Table (4): Correlation between children response to treatment and children’s age
Response to treatment
Children’s age in years
(n=60)
p 6-<8
(n=38)
8-12
(n=22)
No % No %
Disturbance of normal speech 23 60.5 14 63.6 0.811
Impact of irregular speech therapy: 1.000
Relationship with teacher 4 10.8 3 14.3
Relationship with other student 6 16.2 3 14.3
School action 6 16.2 4 19
Relationship with family 21 56.8 11 52.4
Stage of treatment for children with stuttering 0.083
Follow up at home 7 18.4 0 0
Taking therapy 19 50 13 59.1
Taking oral treatment 0 0 1 4.5
Maintenance therapy and follow up at home 12 31.6 8 36.4
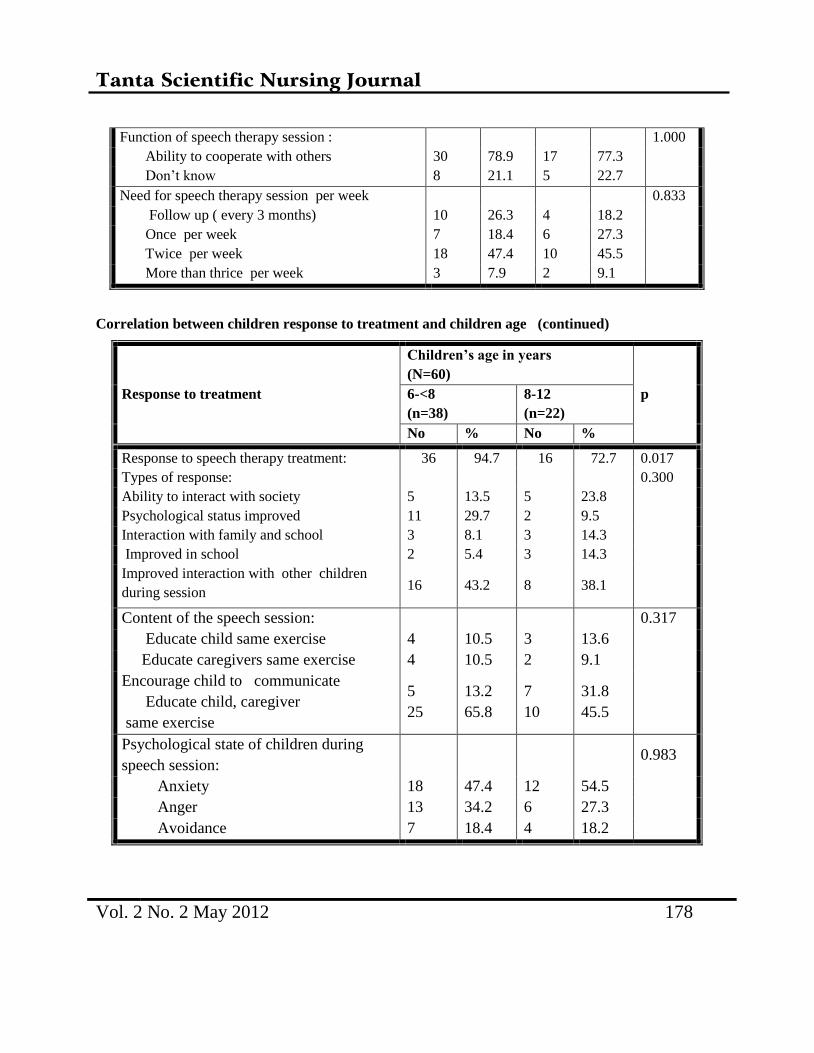
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 178
Function of speech therapy session : 1.000
Ability to cooperate with others 30 78.9 17 77.3
Don’t know 8 21.1 5 22.7
Need for speech therapy session per week 0.833
Follow up ( every 3 months) 10 26.3 4 18.2
Once per week 7 18.4 6 27.3
Twice per week 18 47.4 10 45.5
More than thrice per week 3 7.9 2 9.1
Correlation between children response to treatment and children age (continued)
Response to treatment
Children’s age in years
(N=60)
p 6-<8
(n=38)
8-12
(n=22)
No % No %
Response to speech therapy treatment: 36 94.7 16 72.7 0.017
Types of response: 0.300
Ability to interact with society 5 13.5 5 23.8
Psychological status improved 11 29.7 2 9.5
Interaction with family and school 3 8.1 3 14.3
Improved in school 2 5.4 3 14.3
Improved interaction with other children
during session 16 43.2 8 38.1
Content of the speech session: 0.317
Educate child same exercise 4 10.5 3 13.6
Educate caregivers same exercise 4 10.5 2 9.1
Encourage child to communicate
Educate child, caregiver
same exercise
5
25
13.2
65.8
7
10
31.8
45.5
Psychological state of children during
speech session: 0.983
Anxiety 18 47.4 12 54.5
Anger 13 34.2 6 27.3
Avoidance 7 18.4 4 18.2
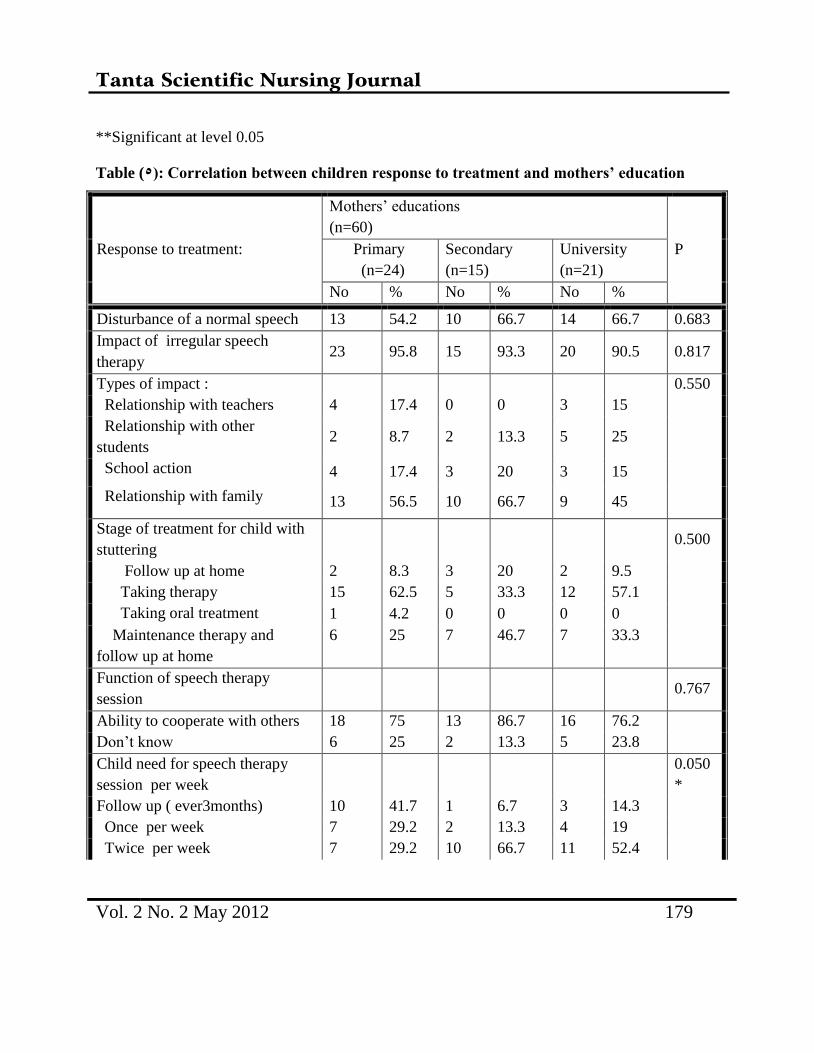
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 179
**Significant at level 0.05
Table (5): Correlation between children response to treatment and mothers’ education
Response to treatment:
Mothers’ educations
(n=60)
P Primary
(n=24)
Secondary
(n=15)
University
(n=21)
No % No % No %
Disturbance of a normal speech 13 54.2 10 66.7 14 66.7 0.683
Impact of irregular speech
therapy 23 95.8 15 93.3 20 90.5 0.817
Types of impact : 0.550
Relationship with teachers 4 17.4 0 0 3 15
Relationship with other
students 2 8.7 2 13.3 5 25
School action 4 17.4 3 20 3 15
Relationship with family 13 56.5 10 66.7 9 45
Stage of treatment for child with
stuttering 0.500
Follow up at home 2 8.3 3 20 2 9.5
Taking therapy 15 62.5 5 33.3 12 57.1
Taking oral treatment 1 4.2 0 0 0 0
Maintenance therapy and
follow up at home
6 25 7 46.7 7 33.3
Function of speech therapy
session 0.767
Ability to cooperate with others 18 75 13 86.7 16 76.2
Don’t know 6 25 2 13.3 5 23.8
Child need for speech therapy
session per week
0.050
*
Follow up ( ever3months) 10 41.7 1 6.7 3 14.3
Once per week 7 29.2 2 13.3 4 19
Twice per week 7 29.2 10 66.7 11 52.4
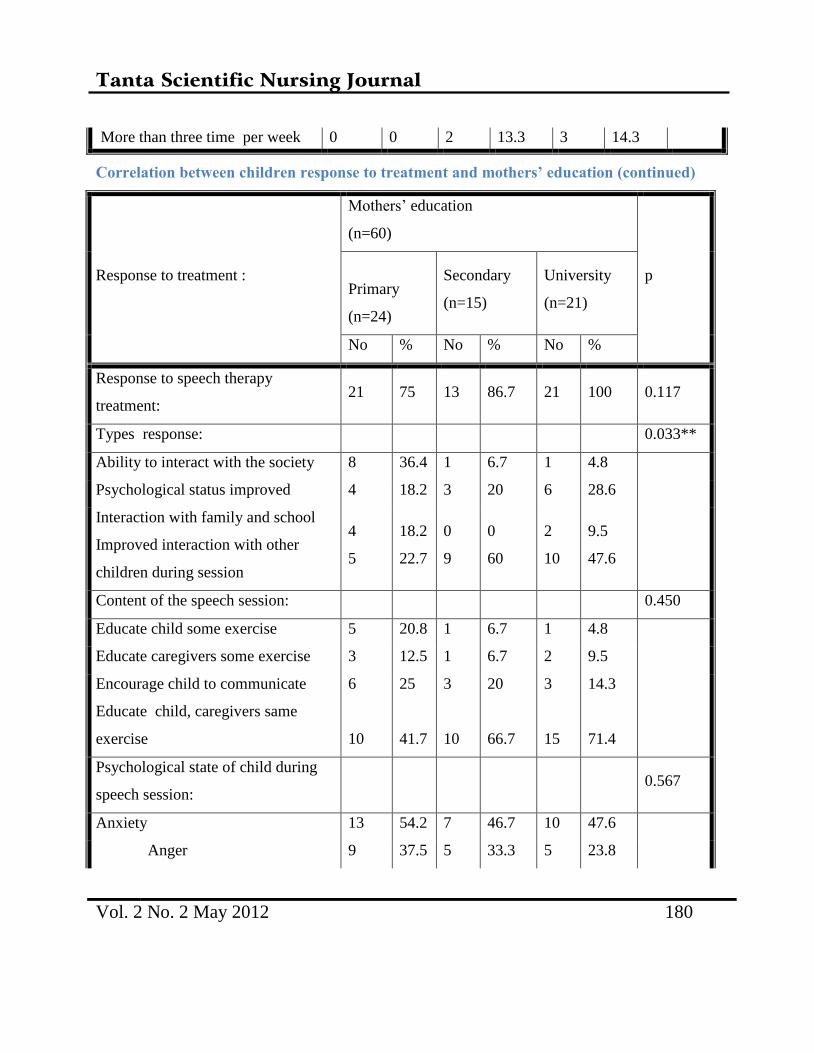
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 180
More than three time per week 0 0 2 13.3 3 14.3
Correlation between children response to treatment and mothers’ education (continued)
Response to treatment :
Mothers’ education
(n=60)
p
Primary
(n=24)
Secondary
(n=15)
University
(n=21)
No % No % No %
Response to speech therapy
treatment: 21 75 13 86.7 21 100 0.117
Types response: 0.033**
Ability to interact with the society 8 36.4 1 6.7 1 4.8
Psychological status improved 4 18.2 3 20 6 28.6
Interaction with family and school
Improved interaction with other
children during session
4
5
18.2
22.7
0
9
0
60
2
10
9.5
47.6
Content of the speech session: 0.450
Educate child some exercise 5 20.8 1 6.7 1 4.8
Educate caregivers some exercise 3 12.5 1 6.7 2 9.5
Encourage child to communicate
Educate child, caregivers same
exercise
6
10
25
41.7
3
10
20
66.7
3
15
14.3
71.4
Psychological state of child during
speech session: 0.567
Anxiety 13 54.2 7 46.7 10 47.6
Anger 9 37.5 5 33.3 5 23.8
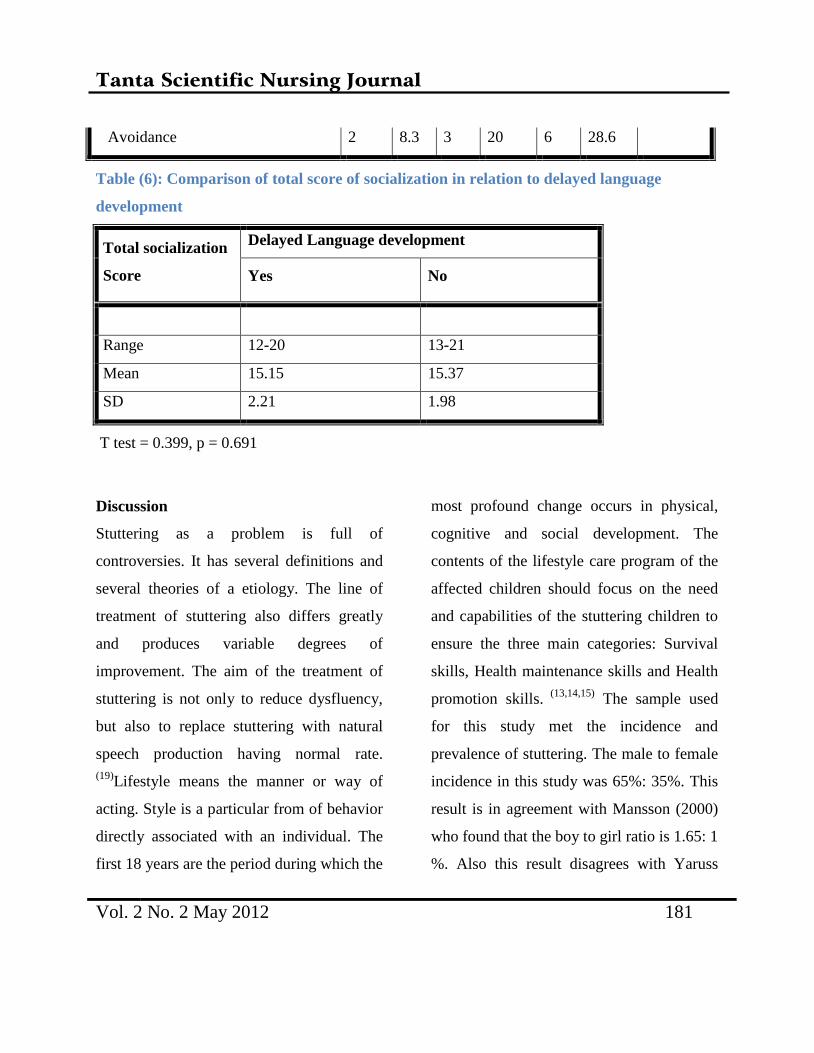
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 181
Avoidance 2 8.3 3 20 6 28.6
Table (6): Comparison of total score of socialization in relation to delayed language
development
Total socialization
Score
Delayed Language development
Yes No
Range 12-20 13-21
Mean 15.15 15.37
SD 2.21 1.98
T test = 0.399, p = 0.691
Discussion
Stuttering as a problem is full of
controversies. It has several definitions and
several theories of a etiology. The line of
treatment of stuttering also differs greatly
and produces variable degrees of
improvement. The aim of the treatment of
stuttering is not only to reduce dysfluency,
but also to replace stuttering with natural
speech production having normal rate.
(19)Lifestyle means the manner or way of
acting. Style is a particular from of behavior
directly associated with an individual. The
first 18 years are the period during which the
most profound change occurs in physical,
cognitive and social development. The
contents of the lifestyle care program of the
affected children should focus on the need
and capabilities of the stuttering children to
ensure the three main categories: Survival
skills, Health maintenance skills and Health
promotion skills. (13,14,15)
The sample used
for this study met the incidence and
prevalence of stuttering. The male to female
incidence in this study was 65%: 35%. This
result is in agreement with Mansson (2000)
who found that the boy to girl ratio is 1.65: 1
%. Also this result disagrees with Yaruss

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 182
(2006), Bloodstein (2002) and Stackhouse
(2001). They found ratio of 3 males to one
female 3:1. Boys generally have more
speech disorders because girls are speak
earlier than boy's and they are better speech
and language and specially at using speech
and language for social purposes. (21, 16,22, 23)
As regards the biosocial characteristics of
mothers according to mothers' age, the
present study revealed that the mean age
was 34.92 years. Less than half of the
sample mothers had high education, so they
are more aware to be involved in child care
and dealing with their problem, in addition
they seek earlier consultation and engage
their children in speech therapy. Regarding
family size, the present study revealed that
the mean family size was 3.60 children. In
the present study, high a percentage of
stuttering children live in urban areas (Table
1), while a low percentage (41.7%) live in
rural ones. This is in disagreement with the
study of Yaruss (2001), who revealed that
rural inhabitation was found in 55% and
urban in 29% respectively when
investigating 1818 people at two villages in
Upper Egypt. This result is due to the fact
families of children living in urban area did
not allow them to play outside the house
which prevents early communication with
peers.( 24)
As regards the family history of stuttering
children, the present study revealed parent
consanguinity was found in 25%of children
while 16.7% of them had positive sibling
history (Table 2). Consanguinity is a social
phenomenon. These results explain the
importance of counseling for the prevention
and early detection of stuttering among
children especially in positive family
history. This finding is in agreement with a
study of Andrews and Harries (2008) who
found that 25-60% of stutterers had relatives
who stuttered. (25)
Stuttering is a problem
interfering with the normal life of the
children. There are three main categories of
health promoting life style profile: Survival
skills, health promoting skills, and health
maintenance skills. Survival skills entail the
items related to the need for speech therapy
and speech production and communication
with others. Information about speech
therapy and psychological assessment
(anxiety, anger and fear) is so accurate, and

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 183
adequate knowledge is necessary to help
these children understand the nature of their
problems, therapy administration, treatment
of stuttering, child's daily activity, . These
may help them to reduce dysfluency, replace
stuttering with natural speech production
having normal rate and to improve
communication, social adjustment and self
fulfillment as much as possible Bloodstein
(2002) 20)
The results showed that the
therapy led to improvement in all
parameters. (Table 3) The improvement of
all perceptual prolongation, repetition,
blocks, went parallel with increased speech
rate, which indicates stability of the results.
Although this improvement was associated
with improvement of psychological
assessment, improvement did not reach
significant level after therapy. This was
expected because this study was conducted
for a short term evaluation and the
psychological changes need is in a long
period of therapy and follow up to show
improvement. This result is in agreement
with Cooper and Bloom (2002) who found
that speech therapy greatly improves
prognosis and extends the life span. (26)
The
present study revealed that the majority of
the sample (Table 3) suffered from the
impact of irregular speech therapy sessions;
this means that the child who maintains
regular speech therapy improves but the one
who has irregular speech therapy sessions
does not progress. Irregular speech sessions
have a major relationship with family but a
less impact on school action and relation
with others students (both of them less than
quarter of the sample). These results are in
agreement with Andrews, Craig (2002) and
Lincoln (2006) who found that the stuttering
frequency decreased to very low level post
treatment and also improvement in stuttering
frequency at least in 85% to 90% across all
assessment contexts for 9-14 year olds
stutterers. So the earlier treatment of stutter
gives the better prognosis. (27,28)
According
to psychological status, the results showed
that there was a positive linear association
between presence of anxiety and stuttering
(Table 3). Although all children therapy in
this study improved, this improvement did
not reach the significant level. This result is
in agreement with Bloodstein( 2002) who
found that the stutter scores were higher in

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 184
social anxiety than in a normal speaking.
However, negative findings were obtained
by Denial, Brutten who reported that there
was a similarity between some stuttering
characteristics as shame, avoidance, denial
and addiction. The stutterers needed as the
addicts need support and structured
recovery, from others with the same
problems. So the rule of helping group was
very important. (21)
There was a significant
difference between child age and child
response to treatment (Table 4).Young
children respond better to speech therapy
because they are still unaware about their
problem. As regards mothers' education it
had a significant positive impact on response
to speech therapy session among stuttering
children (Table 5)Those who were illiterate
and primary educated school mothers were
less competent than other groups
(secondary, university). The present study
showed that the severity of stuttering had a
significant negative effect on total
socialization. This result is in agreement
with Miller and Watson who reported that
the young stutterers had significant negative
attitudes toward speech communication and
the negative attitudes increased with age.
The present study showed that child
socialization had a positive effect on the
child with delayed language development
(Table 6). Moreover, Riley (2004) reported
that 30% of young stutterers have
simultomeonsly language difficulty.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 185
References
1- Belz L &Hunsberger M. Nursing Care
Children.2nd
ed.Landon: WB Saunders
Co, 1996; 294
2-Duffy J. Motor Speech Disorders
Substrates Differential Diagnosis and
Management. 2nd ed. St.louis: Mosby
Elsevier Co, 2005;22-27
3- Manning W& Dilollo A.
Phenomenological Understanding
Stuttering Of Successful Stuttering
Management. Fluency Disorder
Journal.2007;30(1): 1-22
4- Postma A . Detection of Errors During
Speech Production: Areviewof Speech
Monitoring Models
Cogntion.2000;77(11): 97-132
5-Golding K, Kummer A. Therapy
Techniques for Cleft Palate Speech
Disorder. 2nd. Philadelphia: Mosby
Co,2006;44-52
6- Yairi E& Ambrose N. Genetic Stuttering
Critical Review. Speech Hearing
Researcher Journal. 1996; 39(6): 771-784
7- Craig A, Peters K. Epidemiology of
Stuttering in the Communication across
the entire life Span. Speech Language
Hearing Research Journal. 2003; 45(5):
1097-11059
8 Mansson H. Childhood Stuttering
Incidence and Development disorder.
Speech Language Pathology Journal.
2000;7(3): 47-57
9- Proctor A, Duff M, Yairi E. Early
Childhood Stuttering In African and
Americans Journal. 2008;51(6) :1465-
1479
10- Kehoe T. Guide to communication most
disorders 4th ed .Bulder Co, 1997; 55-57
11-Walter H. Clinical Decision Making in
Fluency Disorder.2nded, Evised san
Diego: CA Singular Publishing, 2003;
774
12- Patricia A. Basic Nursing.4th ed .Mosby
Co, 1999; 14-19
13 – Betz C, Husbergan M . Family Center
–Nursing Care Of Children . 2nd ed .
London:WB Saunders Co,1994;1982-
2009.

Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 186
14- Wholey L, Wong D. Nursing Care Of
Infant and Children. 5th ed.
Londan:Mosby Co, 1995;999-1012
15- Steven B. Impact Of Chronic Illness. In
Family Centered Nursing Care Of
Children. Foster, Roxie: WB
SaundersCo,1989; 736-765
16- Clegg J, Hollis C, Developmental
Language Disorder –Afollow up in later
Adult Life. Child Psychology and
Psychiatry Journal.2005 ;46(2):128-149
17- Klompas M& Ross M. Social and
Behavioral Difficultes In Children With
Language Impairment. Fluency Disorder
Journal. 2004; 29(1):275-305
18-Hood G & Dincher J. Total Patient Care
Foundation and Practice. 7th ed. St laus:
Mosby Co, 1995; 313-333
19-Ambrose N, Cox N and Yairi E. Genetic
aspects of early childhood stuttering.
Speech Language and Hearing Research
Journal 2006; 36(1): 701-706.
20- Carl Dell. Treating the school age
stutter. 4thed. St. Louis: Mosby Elsevier
Co, 2000; 22-27
21- Bloodstein O. A Handbook on
Stuttering. 3rded. Chicago: Illinois Co,
2002; 261-270.
22- Yaruss J. Evaluating treatment outcomes
for adults who stutter. of Communication
Disorders Journal 2001; 34(3): 163-182.
23- Stackhouse J. Phonological awareness:
Connecting speech and literacy
problems.5thed. In B.W Hudson and M.L
Edwards Co, 2001; 157-196.
24- Yaruss J. Evaluating treatment outcomes
for adults who stutter. of Communication
Disorders Journal 2001; 34(3): 163-182.
25-Andrews G and Harris M. The syndrome
of stuttering. Speech and Hearing
Disorders Journal 2008; 21(1): 116-126.
26-Cooper C and Bloom C. Treating young
children who stutter. Paper presented at
the International Stuttering Awareness
Conference 2001; 453-654.
27- Andrews G, Craig A, Feyer A,
Hoddinott S, Howie P and Nell Son M.
Stuttering A review of research findings
and theories circa. Speech and Hearing
Research Journal 2002; 48(8): 226-246.
28- Lincoln M and Onslow M. Long term
outcome of an early intervention for
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 187
stuttering. American Speech Language
Pathology Journal 2005; 6(1):51-58.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 188
Establishing Basic Standards of Nursing care protocol at Neonatal
Intensive care unit.
*Sabah Mohamed El sayed **Prof. DR. Yomn Y. Sabry.
*** Prof. DR. Hamed M. sharkawy *Dr. Ebtisam M. elsayed and* Dr.Thanaa Ali .
Faculty of nursing,* Tanta and** Alexandria University,***Faculty of medicine, Tanta University
Abstract
The advancements in intensive care in recent decades have enabled better survival of full
spectrum of newborns. The management of neonates at NICU is based on various modalities
of support and application of fundamental principles of neonatal care. The aim of this study
was to establish basic standards of care for nurses working at Neonatal Intensive Care Unit.
The subjects of the present study consisted of 70 nurses working in Neonatal Intensive Care
Unit and responsible for providing direct care for newborn. Two tools were used to collect
data:. Knowledge assessment sheet and observation checklist to assess nurses' knowledge
and actual performance of nurses providing direct care for neonates in Neonatal Intensive Care
Unit before, immediately, and after three months from the standard application. The results.
showed that, before the standard application the total scores of knowledge for nurses were
good (3o %) and poor with percentages of 63%. It was improved immediate, and after three
months later of the standard application. There was significant difference in nurses'
performance before, immediate, and after three months of the standard application.
Conclusion: it can be concluded that all the nursing activities presented in the initial standard
as basic nursing responsibilities was enhanced. Recommendations: The developed standards
should be translated into Arabic and disseminated to the managers of health organizations.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 189
Introduction:
The neonatal period is defined as the
first four weeks subsequent to birth Some
newborns require observation and care that
is beyond the scope of a normal newborn
nursery, these are called high risk neonates
(1,2). High risk neonate can be defined as a
newborn, regardless of gestational age or
birth weight, which has a greater-than-
average chance of morbidity or mortality,
requiring early intervention that should be
delivered at neonatal intensive care unit(3).
It provides care to full spectrum of
newborns ranging from extremely
premature infants, to high-risk and
critically ill babies, to less critically ill
babies who are recovering and maturing
with increased emphasis is being placed on
the need for standards of care, as well as
mechanisms which address the barriers to
provision and use of quality care(4). The
first step in
improving quality of nursing care is an
articulation of standards of care that
provide a mean for determining quality of
care as well as accountability of the
nurses(5). A standard is defined as a
professionally agreed level of performance,
it provides the required knowledge and
skills that can be used to orient new staff
and to guide nurses in clinical practice (6).
Nurses are the key elements in critical
care. They are required to keep pace with
the rapid changes in health care, and
provide quality of patient's care in a cost-
effective manner (7)
Aim of the study: was to assess actual
performance of nurses working in Neonatal
Intensive Care Unit at Tanta University
Hospital.1
Subjects and Method:-
Research design: -
A quasi-experimental research design was
used to accomplish this study.
Setting:
This study was carried out at the Neonatal
Intensive Care Unit of Tanta University
Hospital.
Sample:
Consisted of all bedside nurses
working in NICU responsible for
providing direct care for neonates with
any health problems in the previously
mentioned setting. Their number was
70.
-Tools:
1-A Structured questionnaire sheet for
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 190
Neonatal Nursing management
competences: This tool was developed
to assess nurses' knowledge and skills
related to the basic competences needed
for neonatal care. It covered three parts;
biosocial data of the nurses, Nurses'
knowledge assessment questionnaire
2- Nurses practice observational checklist.
Method:
- All nurses were observed during
different nursing procedure at different
shifts (morning, afternoon and night
shifts).
- The questionnaire was answered on an
individual basis in the presence of the
researcher. The time needed to answer the
questionnaire ranged from thirty minutes
to one hour. Data collection of this tool
lasted approximately ten months.
- Preparation of suitable media for teaching
the nurses including; lectures, data show,
poster, video, doll for remonstration, and
book notes.
- Determining the framework of the
standards; The Donnabedian model (8)
(structure, process and outcome) was used.
Implementation of the standard care
strategies.
- Nurses were divided into ten groups,
seven nurses in each group.
-The standard of care was discussed for all
nurses included in the study; it includes 13
sessions; adequate (basic assessment,
hygienic care, sensory stimulation,
infection control, support for respiratory
effort, caloric intake and knowledge about
High Risk palliative care.)
Evaluation was done immediately and
three month later.
Part (A):-Knowledge of the
nurses regarding care of neonates
at NICU was evaluated and
classified as:
Every item was evaluated as
follow:
Correct and complete
answer was scored (2)
Correct and incomplete
answer had been scored (1)
incorrect and incomplete
answer had been scored (0)
Total score of knowledge items was
calculated in percentage and a score
of 70% or more is considered good,
60-69% fair & less than 60% was
considered poor.
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 191
Part (B):-Practice of the nurses
regarding care of neonates at NICU with
evaluated and classified as:
Every item evaluated as follow:
Competent (Correct and complete
done) had been scored (1)
incompetent (Correct and
incomplete done) had been scored
(0)
incorrect or not done had
been scored (0)
The total score of every item had been
calculated in percentage and classified as
follow:
85 and more had been considered good
70-84 % had been considered
fair.
Less than 70% had been considered
poor.
Results:
Table (1) illustrates the general
characteristics of nurses included in the
study. It was observed that, nearly two
third (60%) of the nurses were 30 to less
than 40 years old, with mean age were 31
± 6.Regarding their education, 67.1% of
nurses are secondary nursing school
graduates while 24.3 % of them have
completed their university nursing
education and only 8.6 % of them have a
technical nursing institute certification.
Unfortunately, the same table indicates that
only 12.9 % of nurses have attended
specific course/ training in neonatology,
and the majority of them (87.1%) did not
attain any course or training. It was
observed that most of them (85.7) were
married and 14.3% were single. In relation
to their years of experience in NICU, the
result reveals that the mean years of
experience in NICU were 11.6±5.8 years.
Table (2): shows the correlation between
nurses' knowledge before and immediately
after application of the standard, and
between before and three months after
application of the standards of care. It was
observed that, the nurses' levels of
knowledge regarding high risk neonates,
infection control, oxygen therapy, control
of body temperature, kangaroo care,
nutrition, re-lactation, tactile stimulation,
and support of parents (19%, 13%, 34%,
46%, 100%, 37%, 100%100%, and
99%,)respectively were incompetent
before application of the standard, while
after application of the standards either
immediately or three months later , the
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 192
nurses ' knowledge regarding the
previously mentioned topics completely
improved, With significant differences
p<0.001.Table (3): shows the correlation
between nurses' performance before,
immediately after application of the
standards, and between before and three
months later from application of the
standards. It was reveals that, the total
scores of nurses' performance regarding
control of infection were 96% incompetent
before standard compared to 61% and 69%
were incompetent immediately and after
application of the standard
respectively.Table (4) and fig. (1, 2):
represents the total score for the nurses'
knowledge and practice according to their
level of performance. It was observed that,
the total scores of nurses' knowledge were
poor with percentage 63%, where as,
immediately and after three months of the
standard application ,the total score of
knowledge improved as the majority of
them (89%) and (81%) obtained good and
fair scores respectively. As regards the
total score of practice, 80% of nurses'
performances were poor before the
standard, while after application of the
standard either immediately or after three
months, the nurses' performance improved.
statistically significant difference was
observed (p<0.001).
Table (5) and Fig (3, 4): Illustrated
the total score of nurses' performance
according to their competences. It was
observed that 63% of the nurses'
knowledge was incompetent before
standard application, compared to (8%
and10%) immediately and three months
later respectively. As regards nurses'
practices the total scores were 80%
incompetent before standard and decreased
to 30% and 36% respectively immediately
and three months later from application of
the standards. There were statistically
significant differences (p<0.001).
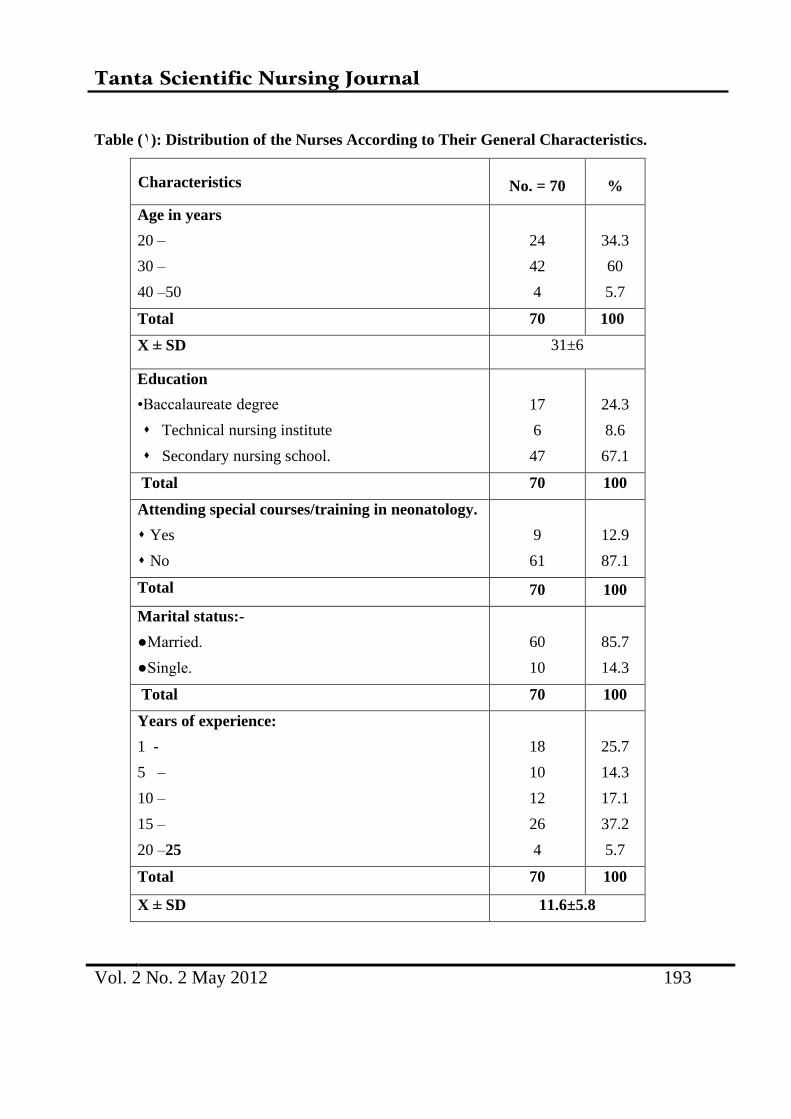
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 193
Table (1): Distribution of the Nurses According to Their General Characteristics.
Characteristics No. = 70 %
Age in years
20 –
30 –
40 –50
24
42
4
34.3
60
5.7
Total 70 100
X ± SD 31±6
Education
•Baccalaureate degree
Technical nursing institute
Secondary nursing school.
17
6
47
24.3
8.6
67.1
Total 70 100
Attending special courses/training in neonatology.
Yes
No
9
61
12.9
87.1
Total
70
100
Marital status:-
●Married.
●Single.
60
10
85.7
14.3
Total 70 100
Years of experience:
1 -
5 –
10 –
15 –
20 –25
18
10
12
26
4
25.7
14.3
17.1
37.2
5.7
Total 70 100
X ± SD 11.6±5.8
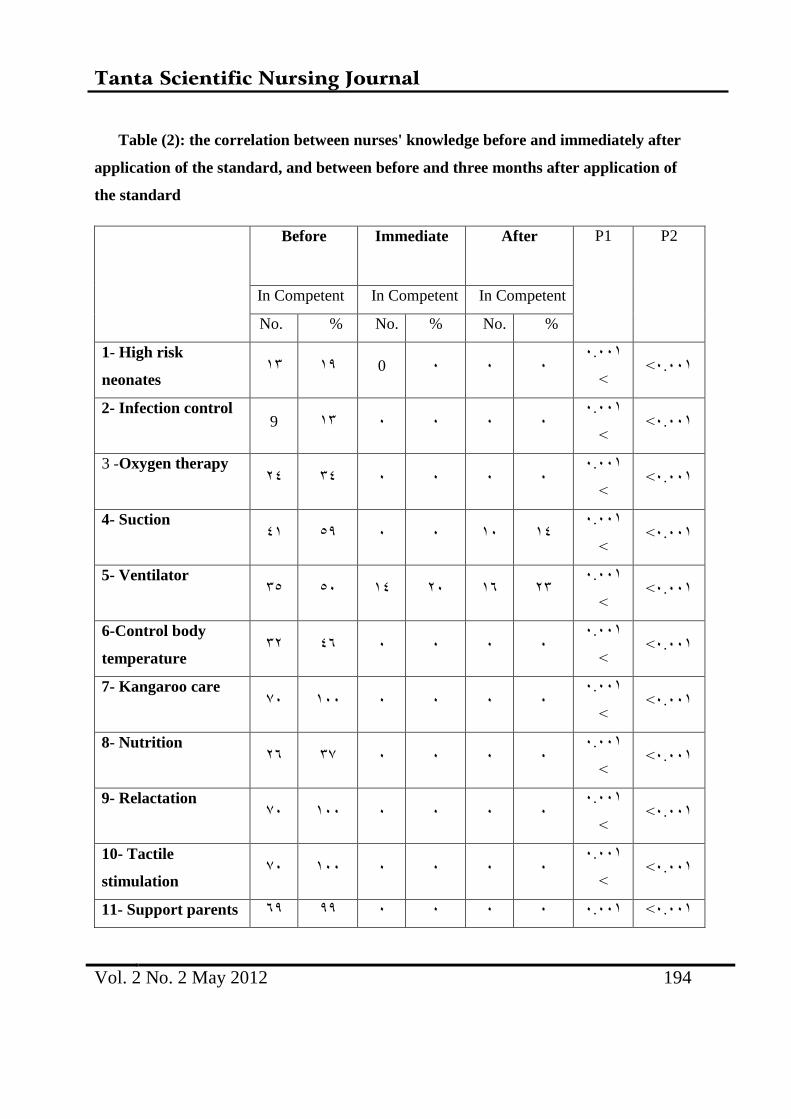
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 194
Table (2): the correlation between nurses' knowledge before and immediately after
application of the standard, and between before and three months after application of
the standard
P2 P1
After Immediate Before
In Competent In Competent In Competent
% No. % No. % No.
.0..1> .0..1
> . . . 0 11 11
1- High risk
neonates
.0..1> .0..1
> . . . . 11 9
2- Infection control
.0..1> .0..1
> . . . . 13 43
Oxygen therapy-3
.0..1> .0..1
> 13 1. . . 91 31
4- Suction
.0..1> .0..1
> 41 16 4. 13 9. 19
5- Ventilator
.0..1> .0..1
> . . . . 36 14
6-Control body
temperature
.0..1> .0..1
> . . . . 1.. 0.
7- Kangaroo care
.0..1> .0..1
> . . . . 10 46
8- Nutrition
.0..1> .0..1
> . . . . 1.. 0.
9- Relactation
.0..1> .0..1
> . . . . 1.. 0.
10- Tactile
stimulation
.0..1> .0..1. . . . 11 61 11- Support parents
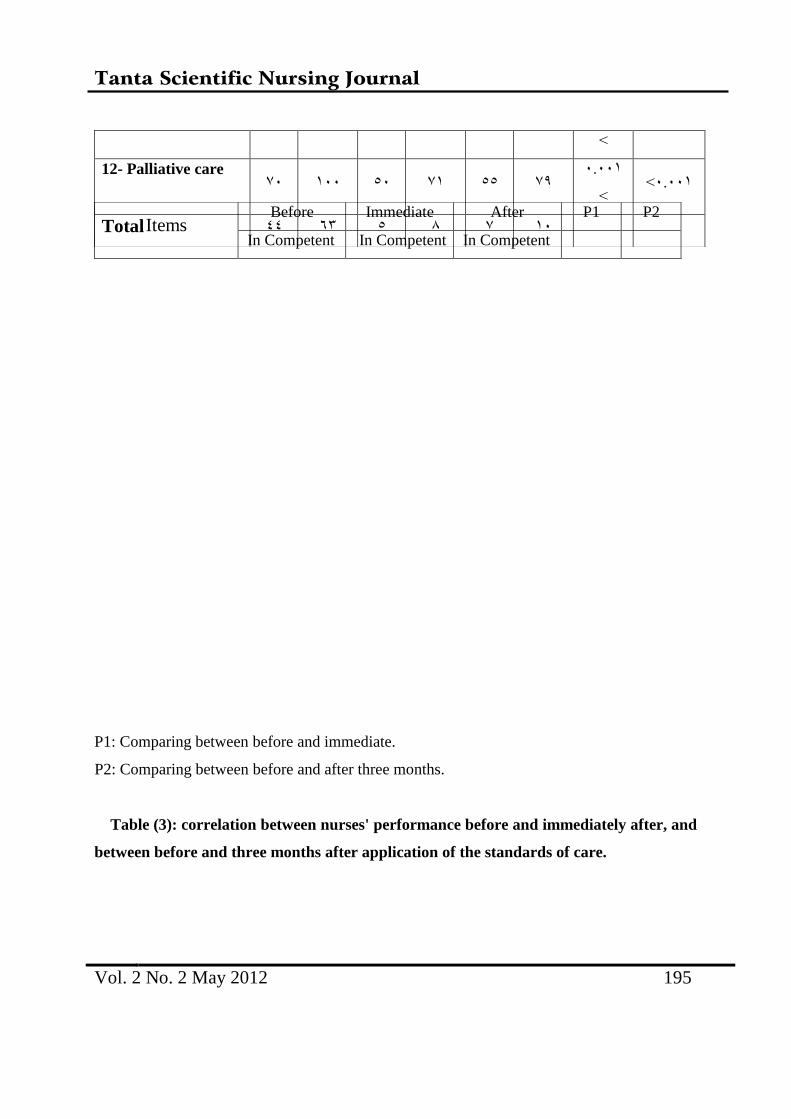
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 195
P1: Comparing between before and immediate.
P2: Comparing between before and after three months.
Table (3): correlation between nurses' performance before and immediately after, and
between before and three months after application of the standards of care.
>
.0..1> .0..1
> 01 99 01 9. 1.. 0.
12- Palliative care
1. 0 8 9 61 33 Total P2 P1 After Immediate Before
Items In Competent In Competent In Competent
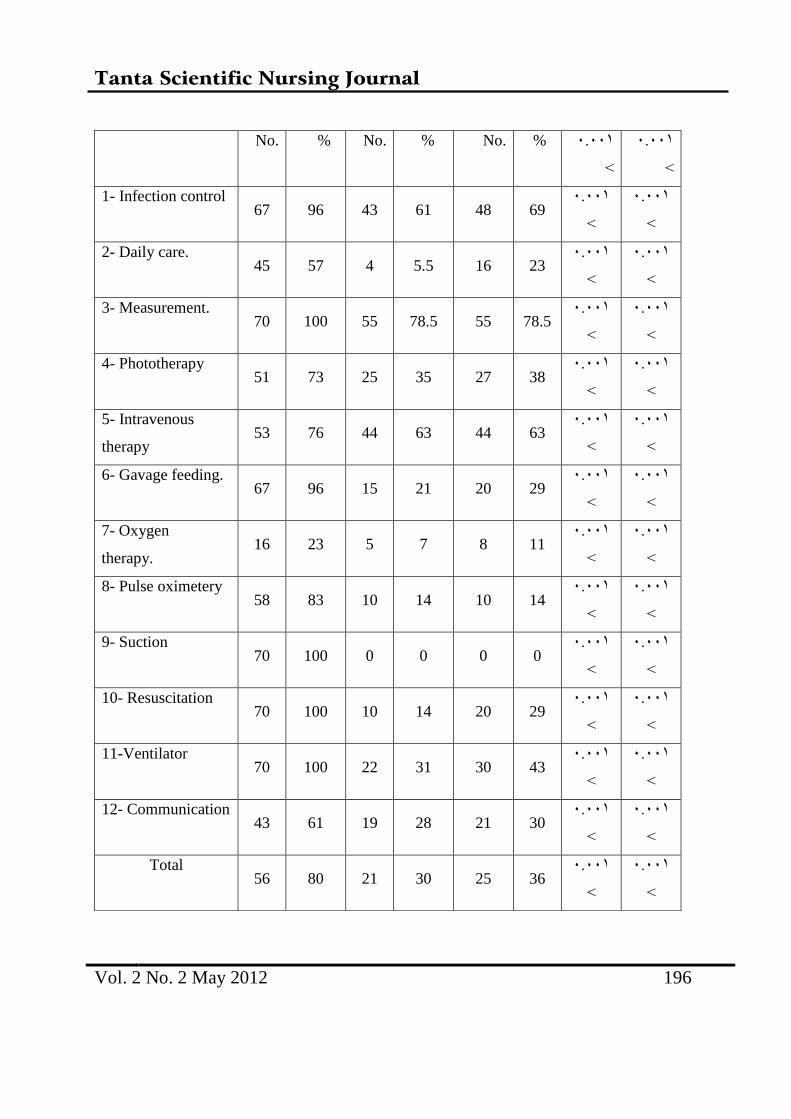
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 196
.0..1
>
.0..1
>
% No. % No. % No.
.0..1
>
.0..1
> 69 48 61 43 96 67
1- Infection control
.0..1
>
.0..1
> 23 16 5.5 4 57 45
2- Daily care.
.0..1
>
.0..1
> 78.5 55 78.5 55 100 70
3- Measurement.
.0..1
>
.0..1
> 38 27 35 25 73 51
4- Phototherapy
.0..1
>
.0..1
> 63 44 63 44 76 53
5- Intravenous
therapy
.0..1
>
.0..1
> 29 20 21 15 96 67
6- Gavage feeding.
.0..1
>
.0..1
> 11 8 7 5 23 16
7- Oxygen
therapy.
.0..1
>
.0..1
> 14 10 14 10 83 58
8- Pulse oximetery
.0..1
>
.0..1
> 0 0 0 0 100 70
9- Suction
.0..1
>
.0..1
> 29 20 14 10 100 70
10- Resuscitation
.0..1
>
.0..1
> 43 30 31 22 100 70
11-Ventilator
.0..1
>
.0..1
> 30 21 28 19 61 43
12- Communication
.0..1
>
.0..1
> 36 25 30 21 80 56
Total
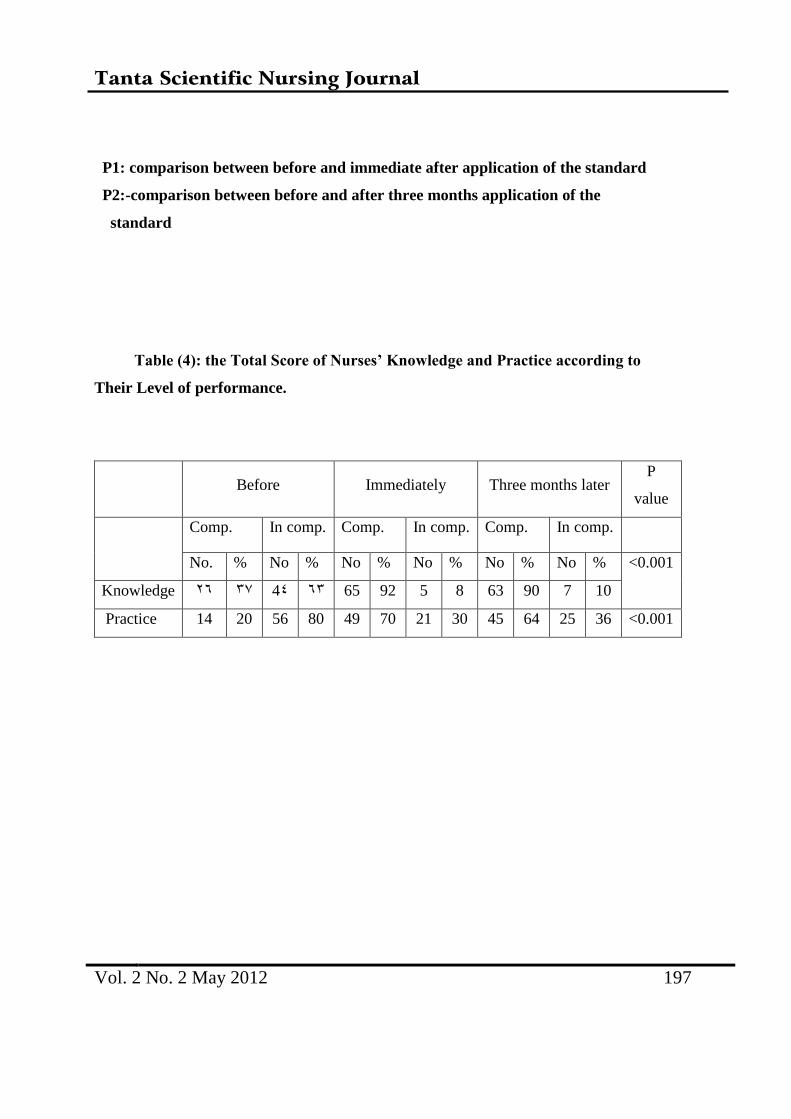
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 197
P1: comparison between before and immediate after application of the standard
P2:-comparison between before and after three months application of the
standard
Table (4): the Total Score of Nurses’ Knowledge and Practice according to
Their Level of performance.
Before Immediately Three months later
P
value
Comp. In comp. Comp. In comp. Comp. In comp.
No. % No % No % No % No % No % <0.001
Knowledge 46 10 43 61 65 92 5 8 63 90 7 10
Practice 14 20 56 80 49 70 21 30 45 64 25 36 <0.001
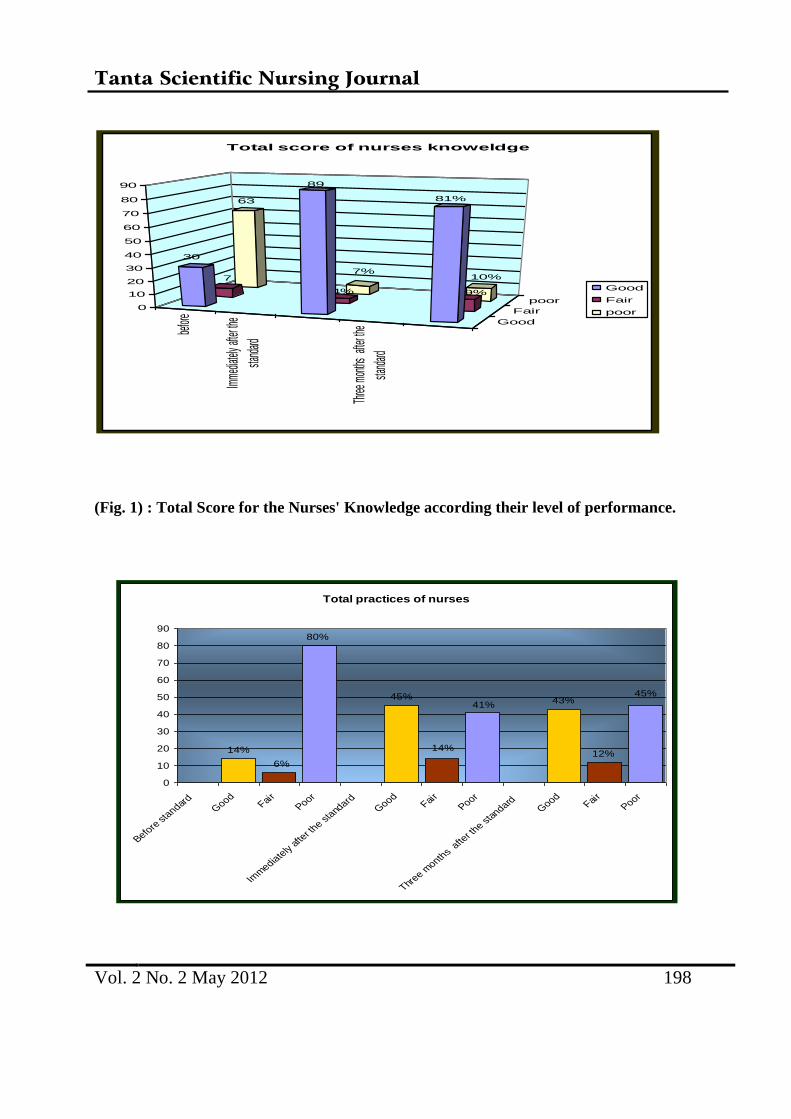
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 198
(Fig. 1) : Total Score for the Nurses' Knowledge according their level of performance.
befor
e
Imme
diatel
y afte
r the
stand
ard
Three
mon
ths a
fter th
e
stand
ard
Good
Fair
poor
63
7%10%7
4% 9%
30
89
81%
0
10
20
30
40
50
60
70
80
90
Total score of nurses knoweldge
Good
Fair
poor
Total practices of nurses
12%
45%43%
41%
14%
45%
14%
6%
80%
0
10
20
30
40
50
60
70
80
90
Before
sta
ndard
Good
Fair
Poor
Imm
ediate
ly af
ter t
he sta
ndard
Good
Fair
Poor
Three m
onths
after t
he sta
ndardG
oodFai
rPoor
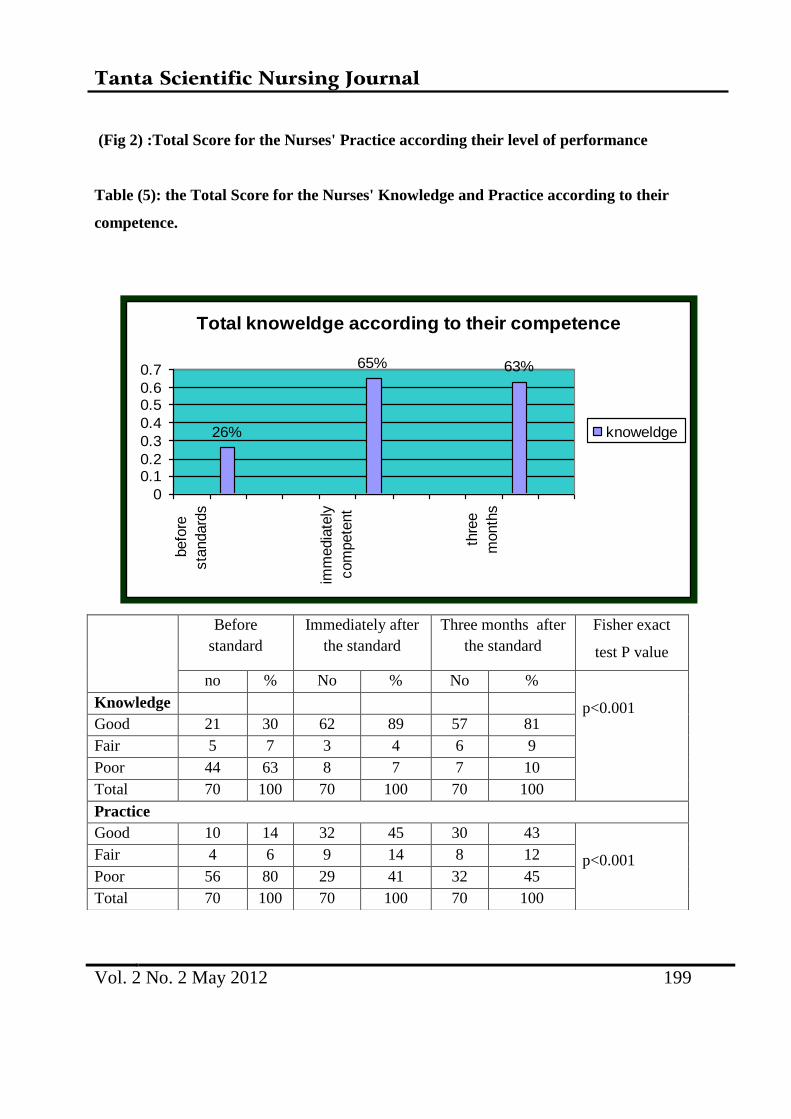
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 199
(Fig 2) :Total Score for the Nurses' Practice according their level of performance
Table (5): the Total Score for the Nurses' Knowledge and Practice according to their
competence.
Total knoweldge according to their competence
26%
65% 63%
0
0.10.2
0.3
0.4
0.50.6
0.7
befo
re
sta
ndard
s
imm
edia
tely
com
pete
nt
thre
e
month
s
knoweldge
Before
standard
Immediately after
the standard
Three months after
the standard
Fisher exact
test P value
no % No % No %
p<0.001 Knowledge
Good 21 30 62 89 57 81
Fair 5 7 3 4 6 9
Poor 44 63 8 7 7 10
Total 70 100 70 100 70 100
Practice
Good 10 14 32 45 30 43
p<0.001 Fair 4 6 9 14 8 12
Poor 56 80 29 41 32 45
Total 70 100 70 100 70 100
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 200
(Fig 3): Total Score for the Nurses' knowledge according their competences.
(Fig 4): Total Score for the Nurses' Practice according their competences
-DISCUSSION:
Maintaining and improving neonatal
care requires active involvement of
everyone in health care system, in order to
meet the needs for evaluating health care in
its totality as well as to identify whether
effective and appropriate care has been
provided. Education and training are
potential means for implementing effective
nursing care at Neonatal Intensive Care
Unit (NICU), as they alter perception,
increase knowledge, and in turn change
work practice.(9) "The current study is
figuring out that, most of nurses didn't
attend any previous in-service training
program related to neonatal care at NICU
.This finding may be owing to the shortage
of nurses' number, absence of continuing
education department in the hospital and
lack of motivation for training, as well as
increased workload in Neonatal Intensive
Care Unit. The findings of the current
study are in line with ". The British
Association of Perinatal medicine (BAPM)
(10) which stated that "a lack of trained
staff may lead to care that is unsafe.'' and
Jeffery et al (11), Vidal et al (12), stated
Total practices according to their compeences
14%
49%45%
0%
10%
20%
30%
40%
50%
60%
befo
re
sta
ndard
s
imm
edia
tely
com
pete
nt
thre
e
month
s
practices
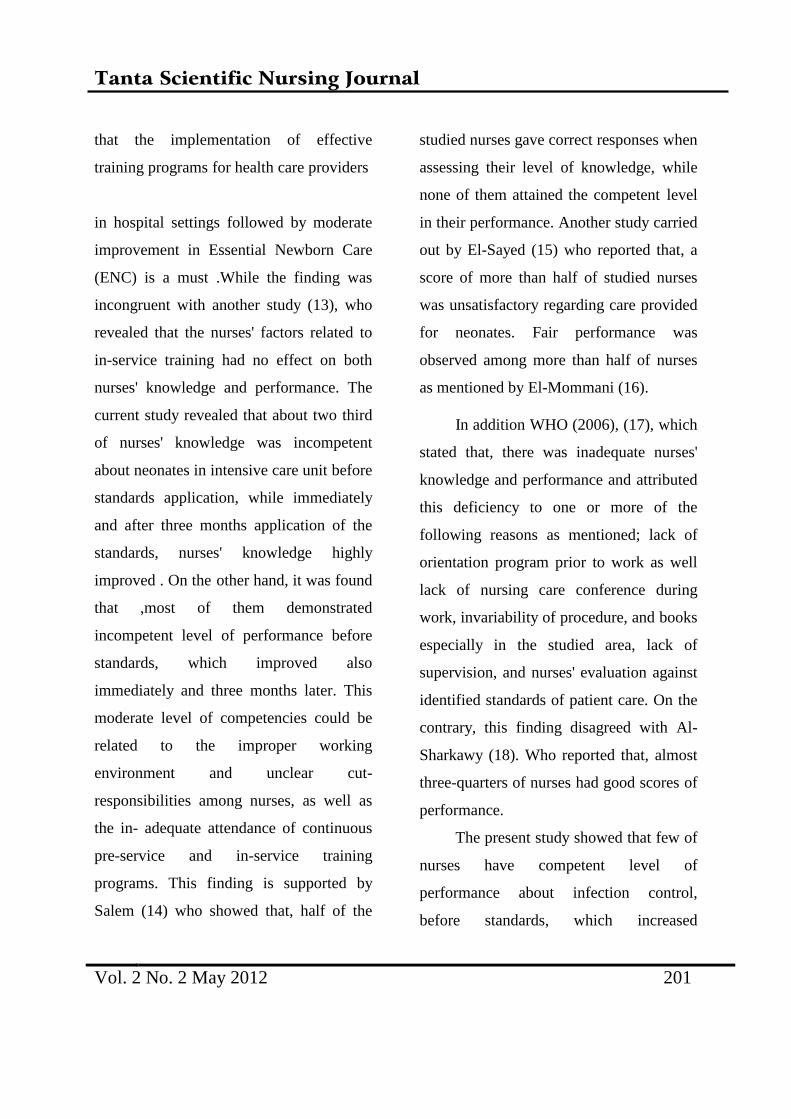
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 201
that the implementation of effective
training programs for health care providers
in hospital settings followed by moderate
improvement in Essential Newborn Care
(ENC) is a must .While the finding was
incongruent with another study (13), who
revealed that the nurses' factors related to
in-service training had no effect on both
nurses' knowledge and performance. The
current study revealed that about two third
of nurses' knowledge was incompetent
about neonates in intensive care unit before
standards application, while immediately
and after three months application of the
standards, nurses' knowledge highly
improved . On the other hand, it was found
that ,most of them demonstrated
incompetent level of performance before
standards, which improved also
immediately and three months later. This
moderate level of competencies could be
related to the improper working
environment and unclear cut-
responsibilities among nurses, as well as
the in- adequate attendance of continuous
pre-service and in-service training
programs. This finding is supported by
Salem (14) who showed that, half of the
studied nurses gave correct responses when
assessing their level of knowledge, while
none of them attained the competent level
in their performance. Another study carried
out by El-Sayed (15) who reported that, a
score of more than half of studied nurses
was unsatisfactory regarding care provided
for neonates. Fair performance was
observed among more than half of nurses
as mentioned by El-Mommani (16).
In addition WHO (2006), (17), which
stated that, there was inadequate nurses'
knowledge and performance and attributed
this deficiency to one or more of the
following reasons as mentioned; lack of
orientation program prior to work as well
lack of nursing care conference during
work, invariability of procedure, and books
especially in the studied area, lack of
supervision, and nurses' evaluation against
identified standards of patient care. On the
contrary, this finding disagreed with Al-
Sharkawy (18). Who reported that, almost
three-quarters of nurses had good scores of
performance.
The present study showed that few of
nurses have competent level of
performance about infection control,
before standards, which increased
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 202
immediately and after three months
application of the standards. This low level
of performance may be due to shortage of
staff, absence of continuous observation
from health professionals and lack of work
motivation either verbal or financial .This
result is congruent with Abd-alla (19). who
found inadequate nurses knowledge and
practice related to nosocomial infection,
principle of disinfectant, sterilization, and
standard infection control precautions and
he interpreted that by the lack of nurses'
awareness with importance of infection
control and safe health practice. Attia (20)
and El-Shenawy (21) revealed that control
of infection in ICU was considered a total
responsibility of the nurse as stated by the
entire expert group included in their
studies.
A large number of premature infants
require prolonged ventilatory support. In
order to provide this support an artificial
airway must be inserted. This airway can
be established in one of two ways, either
with an end tracheal tube or by the means
of a tracheotomy tube. Regardless of which
method is used, the neonate’s upper airway
is by passed, thus reducing the neonate’s
ability to clear secretions spontaneously.
Additionally, the presence of the tube may
lead to an increase in sputum production.
For these reasons neonates with an
artificial airway in place will require
airway suctioning (22). Endotracheal
intubation may be necessary for the
ventilation process. The nurse must
constantly ensure tube placement, stability
and patency. End tracheal intubation and
subsequent oxygen therapy decrease ciliary
activity and accelerate mucus production.
Appropriate suctioning of the end tracheal
tube is required to aid in the outflow of
pulmonary secretions and assure patent
airway. (23,24-5)
The present study revealed that half
of nurses were competent in performing
suctioning before standard application and
it increased to include all of them
immediately and after three months
application of standards. . Increased
awareness that suctioning is one of nurses'
own responsibilities could be the reason
behind this competent level of
performance, in addition to the
understanding of the danger of
accumulation of these secretions in the
neonates' airway. The Finding of the
present study was in-accordance with El-
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 203
Mommani (16) who reported that ,more
than half of nurses demonstrated poor level
of performance in suction procedure, and
another(13) who reported that ,suction was
satisfactory in only few numbers of nurses.
The result of the current study is in the line
with Salman (7) who revealed that, three
quarter of nurses gave competent answers
about assisting pediatricians during end
tracheal tube insertion. Moreover, most of
nurses scored competent in performing
suctioning.
Anthropometric measurements help
in assessing neonates' growth and
development. When combined with other
measurements, they are used to form an
index that becomes useful (WHO 2009)
(26). Anthropometric indices such as
height for age, weight for age and weight
for height can be compared to recognized
standards of growth to decide if the
individual or populations under
investigation are within the normal for
size, proportion or composition. (27) As
regards this aspect, the present study
revealed that, the majority of the studied
nurses demonstrated incompetent level of
performance in taking the neonates'
general measurements. This could be
attributed to the fact that pediatricians
usually do the measurements on admission
as a part of their physical examination.
Weight is an important measurement
which should be performed by the nurses
and couldn't be measured, in spite of the
fact that weighing the neonate is
considered as a part of their routine nursing
care which should be performed every
night shift, this could be attributed to
unawareness of the nurses that weighing
should be done regularly to protect rapid
decrease in body weight which may result
from dehydration or insufficient caloric
intake.
The findings of the current study are
in harmony with a study carried out by El-
Sayed (15) who reported that none of the
studied nurses had taken the general
measurements for the neonates.
Furthermore, El-Mommani (16) stated that
the lowest scores were assigned to taking
general measurements, and Mahmoud (28)
reported that approximately two-thirds of
nurses were unsatisfactory in this aspect. In
addition Al-Sharkawy (18) found that only
few numbers of the studied nurses were
good in taking general measurements for
neonates. Mohamed (13) found that the
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 204
majority of nurses did not take the length,
the head and chest circumferences, while
weighing the neonates was done by more
than one-quarter of nurses.
Conclusion: Recommendations:-
Conclusion: it can be concluded that there
was an enhancement in nurses' knowledge
and moderate improvement in performance
after application of the standard.
Recommendations: The developed
standards should be translated into Arabic
and disseminated to the managers of health
organizations
References
1- Australian Resuscitation Council.
Guideline 13.1 introduction to
Resuscitation of the newborn infants.
New Zealand Resuscitation
Council.2010.
2- Brookside A. Obstetric and Newborn
Care II:-Medical Education Diversion.
2007 ;20
3- Hill K. Choi Y. Neonatal mortality in
the developing world. Journal
Demographic Research: 2006; 18
(14):429
4- Duderstadt k. Health of U.S. Children
from the global view. Journal of
pediatric health care.2007; 21(6), 403-
406
5- Royal collage of Nursing. Setting
standards of care. Nursing standard,
1994; 3-8
6- Vetter N. The hospital from center to
community support London: chapman
and flall Co., 1995; 183-87
7- Salman M. Establishing basic standards
for nursing management of neonates
with respiratory distress syndrome at el
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 205
shatby children's hospital .Doctorial
thesis in Critical Care department,
Faculty
of Nursing, Alexandria University
, 2008
8- World Health Organization .Bulletin of
the World Health Organization, 2000;
1475
9- Needleman J., Ellen T. Kenneth W,
Brandes K. Performance Measurement
of Nursing Care: State of the Science
and the Current Consensus. Braneis
University 4..8 .
http://mcr.sagepub.com
10- The British Association of Perinatal
Medicine. Standards for Hospitals
providing neonatal intensive and high
dependency care.2nd ed. 2001
11- Jeffery H, Kocova M., .The impact of
Evidence Based Education on Perinatal
Capacity- Building Initiative in
Macedonia, Medical education 2004;
38,435-447
12- Vidal S, Ronfani l, Mello M,
Comparison of Two Training
Strategies for Essential Newborn Care
in Brazil. Bulletin of the World Health
Organization 2001; 79(2): 1024- 1031
13- Mohamed E. Assessment of Nurses'
Knowledge and Performance
Regarding Nursing Care given to
Chronic Renal Failure Patient Under-
goining Maintenance Hemodialysis.
Thesis Submitted for the Partial
Fulfillment of Master Degree in
Medical Surgical Department Faculty
of Nursing .Tanta University. 2008; 55-
62
14- Salem A. Development of Nursing
Practice Standards for Emergency
Trauma Patients. Unpublished
Doctoral Thesis in Critical Care
Nursing. Faculty of Nursing,
Alexandria University 2006; 120
15- El-Sayed E. Designing and evaluation
an educational program to nurses at
premature unit, Tanta University.
Unpublished Doctrol thesis in
Pediatric Nursing. Faculty of Nursing.
Alexandria University 1996; 61-71
16- El-Mommani M Quality of nursing
care provided in the neonatal
intensive care unit of Princes Badia
Teaching Hospital. Jordan.
Unpublished Doctoral Thesis
submitted to the High Institute of
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 206
Public Health, University of
Alexandria 2002.
17- WHO. Improving health worker
performance. Evidence and
Information for Policy, Department
of Human Resources for Health
Geneva, September 2006
18- Al-Sharkawy S. Improving an in-
service training program for the
pediatric nurses about care of
preterm and low birth weight infants.
Unpublished Doctoral Thesis in
Pediatric Nursing. Faculty of Nursing,
Ain Shams University 1991; 68-70
19- Abd-alla. A. Impact of Health
Education on Infection Control
Measures in Operating Theater.
Thesis Submitted for the Partial
Fulfillment of Doctorial Degree in
the Medical- Surgical Nursing
Science. Tanta University 2008; 90
20- Attia A. Development of An
Instrument to Measure Basic Standards
for Critical Care Nursing.
Unpublished Doctoral Thesis in
Medical- Surgical Nursing.
Faculty of Nursing, Alexandria
University 1992; 87- 90
21- El- Shenawy S. Establishing Standards
for Prevention and Control of
Nosocomial Infection in the Intensive
Care Unit at the Alexandria main
University hospital. Unpublished
Doctoral Thesis in Critical Care
Nursing. Faculty of Nursing,
Alexandria University 2002; 235
22- Buglass, E. Tracheotomy care:
Tracheal Suctioning and
Humidification. British Journal of
Nursing. 1999. 8(8): 500-504
23- Pillitteri A. Maternal and child health
nursing: Care of the childbearing and
childbearing family. 4th ed.
Philadelphia: Lippincott Williams and
Wilkins Co., 2003; 739 – 43, 1081– 85,
1371- 3.
24- Niel-Weise B, Snoeren R, Van De
Broek P. Policies for Endotracheal
Suctioning of Patients Receiving
Mechanical Ventilation: a Systematic
Review of Randomized Control Trials.
Infection Control and Hospital
Epidemiology Journal 2007; 28(5):
531- 6
25- Andrews D, Deboer S, and Adams K.
Securing Pediatric Endotracheal Tubes:
Tape it like you mean it. Australian
Tanta Scientific Nursing Journal
Vol. 2 No. 2 May 2012 207
Emergency Nursing Journal 2007;
10(2): 30- 3.
26- World Heath Organization. Newborns:
reducing mortality; 2009; 333.
27- Morton P, Fontaine D, Hudak C, Gallo
B. Critical Care Nursing: A holistic
Approach. 8th ed. Philadelphia:
Lippincott Williams and Wilkins Co.,
2005; 36- 84
28- Mahmoud-M, Assessment of Nursing
Care Provided for Neonates with
Hyperbilirubinemia Exposed to
Phototherapy. Unpublished M.Sc.
Thesis in Pediatric Nursing. Faculty of
Nursing, Alexandria University 2004
d
Related Documents











