1/16/2018 This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 1 Taking the Gloves Off - Evidence Informed Manual Therapy For Upper Extremity Conditions: Part I Derek Vraa, PT, DPT Wil Kolb, PT, DPT Matthew Vraa, PT, DPT, MBA Michael Gans, PT, DPT Mary Beth Geiser, PT, DPT Dustin McGann, PT, DPT Jeevan Pandya, PT, DPT Eric Wilson, PT, DPT, DSc Combined Sections Meeting – New Orleans, LA. February 22, 2018 This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers Objectives • Apply an impairment based evaluation of the Upper Extremity. • Identify selected OMPT techniques used in the management of subacromial pain syndrome, adhesive capsulitis and SICK scapula. • Develop a differential diagnosis for conditions in the cervical, thoracic, shoulder, elbow, wrist, and hand to identify conditions where manual therapy intervention will be most effective. • Understand recent literature surrounding OMPT for upper extremity conditions. This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers Disclosures • Derek Vraa, PT, DPT - The views expressed herein are those of the individual & do not reflect those of the United States Air Force or the Department of Defense • Wil Kolb, PT, DPT - None • Matthew Vraa, PT, DPT, MBA – I am unfortunately related to one of the other speakers on this panel. • Michael Gans, PT, DPT - None • Mary Beth Geiser, PT, DPT - None • Dustin McGann, PT, DPT - None • Jeevan Pandya, PT, DPT - None • Eric Wilson, PT, DPT, DSc - The views expressed herein are those of the individual & do not reflect those of the United States Air Force or the Department of Defense This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers Regional Interdependence & Upper Extremity Manual Therapy Derek Vraa, PT, DPT Board Certified Orthopaedic Specialist Certified Strength & Conditioning Specialist Certified Manual Trigger Point Therapist Fellow, American Academy of Orthopaedic Manual Physical Therapists Senior Faculty, USAF Tactical Sports & OMPT Fellowship Program [email protected] This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers What is Regional Interdependence (RI)? • “Dysfunction in any unit of the system will cause delivery of abnormal stresses to other segments of the system with the development of a subsequent dysfunction here as well” – Erhard & Bowling 1977 • “…seemingly unrelated impairments in a remote anatomical region may contribute to, or be associated with, the patient’s primary complaint.”-Wainner et al. 2007 This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers Why Regional Interdependence? • Pain referral patterns vary • Literature support • Clinical support • Pathoanatomical & biomedical models don’t explain all pain • Lack of improvement with current localized treatment This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 1
Taking the Gloves Off - Evidence Informed Manual Therapy For Upper
Extremity Conditions: Part I
Derek Vraa, PT, DPT
Wil Kolb, PT, DPT
Matthew Vraa, PT, DPT, MBA
Michael Gans, PT, DPT
Mary Beth Geiser, PT, DPT
Dustin McGann, PT, DPT
Jeevan Pandya, PT, DPT
Eric Wilson, PT, DPT, DSc
Combined Sections Meeting – New Orleans, LA. February 22, 2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers
Objectives
• Apply an impairment based evaluation of the Upper Extremity.
• Identify selected OMPT techniques used in the management of subacromial pain syndrome, adhesive capsulitis and SICK scapula.
• Develop a differential diagnosis for conditions in the cervical, thoracic, shoulder, elbow, wrist, and hand to identify conditions where manual therapy intervention will be most effective.
• Understand recent literature surrounding OMPT for upper extremity conditions.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Disclosures• Derek Vraa, PT, DPT - The views expressed herein are those of the
individual & do not reflect those of the United States Air Force or the Department of Defense
• Wil Kolb, PT, DPT - None
• Matthew Vraa, PT, DPT, MBA – I am unfortunately related to one of the other speakers on this panel.
• Michael Gans, PT, DPT - None
• Mary Beth Geiser, PT, DPT - None
• Dustin McGann, PT, DPT - None
• Jeevan Pandya, PT, DPT - None
• Eric Wilson, PT, DPT, DSc - The views expressed herein are those of the individual & do not reflect those of the United States Air Force or the Department of DefenseThis information is the property of the speakers and should not
be distributed or otherwise used without the express written permission of the speakers
Regional Interdependence & Upper Extremity Manual Therapy
Derek Vraa, PT, DPTBoard Certified Orthopaedic Specialist
Certified Strength & Conditioning Specialist
Certified Manual Trigger Point Therapist
Fellow, American Academy of Orthopaedic Manual Physical Therapists
Senior Faculty, USAF Tactical Sports & OMPT Fellowship Program
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers
What is Regional Interdependence (RI)?
• “Dysfunction in any unit of the system will cause delivery of abnormal stresses to other segments of the system with the development of a subsequent dysfunction here as well” – Erhard & Bowling 1977
• “…seemingly unrelated impairments in a remote anatomical region may contribute to, or be associated with, the patient’s primary complaint.”-Wainner et al. 2007
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Why Regional Interdependence?
• Pain referral patterns vary
• Literature support
• Clinical support
• Pathoanatomical & biomedical models don’t explain all pain
• Lack of improvement with current localized treatment
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 2
How Does Manual Therapy Work?
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Bialosky. Man Ther. 2009Bialosky. J Orthop Sports Phys Ther. 2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
The Case for Regional Interdependence
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Regional Interdependence Lateral Elbow Pain (LEP)
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Regional Impairments Associated with LEP
• Waugh. Arch Phys Med Rehabil. 2004• Prospective Cohort of 83 LE patients
• Multimodal care at 11 different sites
• 57% had cervical impairments
• Berglund. Manual Therapy. 2008• 31 patients with lateral elbow pain (LEP) & 31 asymptomatic controls (C)
• 70% of LEP reported pain in the cervical /thoracic regions vs 16% in asymptomatic group
• 58% of LEP reported lateral elbow pain during radial nerve testing vs 13% in asymptomatic group
• Significantly less ROM was noted in cervical FLX/EXT in LEP (P<.01)
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Elbow Pain/PPT
• Vicenzino. Pain. 1996
• Struijs. Phys Ther. 2003
• Cleland. J Man Manip Ther. 2005
• Fernández-Carnero. J Man Physiol Ther. 2008
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 3
Elbow Disability
• Cleland. J Man Manip Ther. 2005
• Abbott JH. Man Ther. 2001
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Pain Free Grip Strength
• Vicenzino. Pain. 1996
• Cleland. J Man Manip Ther. 2005
• Fernández-Carnero. J Man Physiol Ther. 2008
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Health Care Resources
• Cleland. J Orthop Sports Phys Ther. 2004
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Regional Interdependence & Hand Pain
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
•De-La-Llave-Rincon. J Ortho Sports Phys Ther. 2011• Case control blinded study
• 71 females, age 35-59• Diagnosed with Carpal Tunnel Syndrome (CTS) via EMG
examined for ROM restrictions
• Regardless of severity, females with CTS exhibited loss of cervical ROM
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Regional Interdependence & Shoulder Pain
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 4
Decreased Pain
• Bang & Deyle. J Orthop Sports Phys Ther. 2000
• Dunning. J Manipulative Physiol Ther. 2015
• Bergman. Ann Intern Med. 2004
• Strunce. J Man Manip Ther. 2009
• Boyles. Man Ther. 2009
• Bergman. J Man Physiol Ther. 2010
• Kardouni. Man Ther. 2015
• Wassinger. Man Ther. 2016
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Improving Function/Recovery
• Bang & Deyle. J Orthop Sports Phys Ther. 2000
• Dunning. J Manipulative Physiol Ther. 2015
• Strunce. J Man Manip Ther. 2009
• Boyles. Man Ther. 2009
• Bergman. Ann Intern Med, 2004
• Bergman. J Man Physiol Ther. 2010
• Kardouni. Man Ther. 2015
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Improving Muscular Activity/Strength
• Bang & Deyle, JOSPT, 2000
• Cleland, JMMT, 2004
• Liebler, JMMT, 2001
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Improving Shoulder Mechanics/Range of Motion• Strunce. J Man Manip Ther. 2009
• Bergman. J Man Physiol Ther. 2010
• Haxby-Abbott. Man Ther. 2001
• Kardouni. J Othop Sports Phys Ther. 2015
• Muth. J Othop Sports Phys Ther. 2012
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Health Care Resources
• Rhon. Ann Intern Med. 2014
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Systematic Reviews
• Walser. J Man Manip Ther. 2009• There is limited evidence to support the use of TSM for shoulder conditions,
but there is enough evidence to encourage the pursuit of additional research to determine if TSM is effective for such treatment
• Aoyagi. Man Ther. 2015• There is very low quality evidence that Spinal Manipulation is not better nor
inferior than other interventions in the management of upper limb pain
• Peek. J Man Manip Ther. 2015• Thoracic manual therapy accelerated recovery and reduced pain and disability
immediately and for up to 52 weeks compared with usual care for Non-Specific Shoulder Pain
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 5
Regional Interdependence & the Thoracic Spine
Mintken. Phys Ther. 20010Mintken. J Orthop Sports Phys Ther. 2017
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Case Examples
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
References• Abbott JH. Mobilization with movement applied to the elbow affects shoulder range of movement in subjects with lateral epicondylalgia. Man Ther. 2001 Aug 31;6(3):170-7.
• Aoyagi M, Mani R, Jayamoorthy J, Tumilty S. Determining the level of evidence for the effectiveness of spinal manipulation in upper l imb pain: A systematic review and meta-analysis. Man Ther. 2015 Aug 31;20(4):515-23.
• Bialosky JE, Beneciuk JM, Bishop MD, et al. Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. J Orthop Sports Phys Ther. 2018 Jan;48(1):8-18.
• Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009 Oct;14(5):531-8.
• Bergman GJ, Winters JC, Groenier KH, Meyboom-de Jong B, Postema K, van der Heijden GJ. Manipulative therapy in addition to usual care for patients with shoulder complaints: results of physical examination outcomes in a randomized controlled trial. J Man Physiol Ther. 2010 Feb 28;33(2):96-101..
• Bergman GJ, Winters JC, Groenier KH, Pool JJ, Meyboom-de Jong B, Postema K, van der Heijden GJ. Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain: a randomized, controlled trial. Ann Intern Med. 2004 Sep 21;141(6):432-9
• Boyles RE, Ritland BM, Miracle BM, Barclay DM, Faul MS, Moore JH, Koppenhaver SL, Wainner RS. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. 2009 Aug 31;14(4):375-80.
• Cleland J, Selleck B, Stowell T, Browne L, Alberini S, St. Cyr H, Caron T. Short-term effects of thoracic manipulation on lower trapezius muscle strength. J Man Manip Ther. 2004 Apr 1;12(2):82-90.
• Dunning J, Mourad F, Giovannico G, Masell i F, Perreault T, Fernández-de-las-Peñas C. Changes in shoulder pain and disability after thrust manipulation in subjects presenting with second and third rib syndrome. J Man Physiol Ther. 2015 Aug 31;38(6):382-94.
• Fernández-Carnero J, Fernández-de-las-Peñas C, Cleland JA. Immediate hypoalgesic and motor effects after a single cervical spine manipulation in subjects with lateral epicondylalgia. J Man Phys iol Ther. 2008 Dec 31;31(9):675-81
• Kardouni JR, Pidcoe PE, Shaffer SW, Finucane SD, Cheatham SA, Sousa CO, Michener LA. Thoracic spine manipulation in individuals with subacromial impingement syndrome does Not immediately alter thoracic spine kinematics, thoracic excursion, or scapular kinematics: a randomized controlled trial. J Othop Sports Phys Ther. 2015 Jul;45(7):527-38.
• Kardouni JR, Shaffer SW, Pidcoe PE, Finucane SD, Cheatham SA, Michener LA. Immediate changes in pressure pain sensitivity after thoracic spinal manipulative therapy in patients with subacromial impingement syndrome: a randomized controlled study. Man Ther. 2015 Aug 31;20(4):540-6.
• Liebler EJ, Tufano-Coors L, Douris P, Makofsky HW, McKenna R, Michels C, Rattray S. The effect of thoracic spine mobil ization on lower trapezius strength testing. J Man Manip Ther. 2001 Oct 1;9(4):207-12.
• Muth S, Barbe MF, Lauer R, McClure P. The effects of thoracic spine manipulation in subjects with signs of rotator cuff tendinopathy. J Orthop Sports Phys Ther. 2012 Dec;42(12):1005-16.
• Peek AL, Miller C, Heneghan NR. Thoracic manual therapy in the management of non-specific shoulder pain: a systematic review. J Man Manip Ther. 2015 Sep 1;23(4):176-87.
• Rhon DI, Boyles RB, Cleland JA. One-Year Outcome of Subacromial Corticosteroid Injection Compared With Manual Physical Therapy for the Management of the Unilateral Shoulder Impingement Syndrome. A Pragmatic Randomized TrialOne-Year Outcome of CSI and MPT for Management of SIS. Annals Intern Med. 2014 Aug 5;161(3):161-9.
• Struijs PAA, Damen PJ, Bakker EWP, et al. Manipulation of the wrist for management of lateral epicondylitis: a randomized pilot study. Phys Ther. 2003;83:608–616.
• Strunce JB, Walker MJ, Boyles RE, Young BA. The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain. J Man Manip Ther. 2009 Dec 1;17(4):230-6.
• Walser RF, Meserve BB, Boucher TR. The effectiveness of thoracic spine manipulation for the management of musculoskeletal conditions: a systematic review and meta-analysis of randomized clinical trials. J Man Manip Ther. 2009 Dec 1;17(4):237-46.
• Wassinger CA, Rich D, Cameron N, Clark S, Davenport S, Lingelbach M, Smith A, Baxter GD, Davidson J. Cervical & thoracic manipulations: acute effects upon pain pressure threshold and self -reported pain in experimentally induced shoulder pain. Man Ther. 2016 Feb 29;21:227-32.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Is Manual Physical Therapy Effective for the Shoulder?
Wil Kolb, PT, DPT
Board Certified Specialist in Orthopaedics
Fellow of the American Academy of Orthopaedic Manual Physical Therapists
Assistant Professor Department of Physical Therapy
Waldron College of Health Sciences, Radford University
Orthopedic Manual Therapy OF THE SHOULDER COMPLEX
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
OMPT for the Shoulder (SIS)SR&MA Results (Steuri 2017 Br J Sports Med)
• “Very low quality evidence… exercise should be considered for pts with SIS symptoms and tape, ECSWT, laser or MT might be added.”
• “MT was superior to doing nothing or sham”
• “MT plus exercise was superior to exercise alone (but only at the shorter follow-ups)”
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Overview: OMPT for the Shoulder (SIS)
• “The available evidence supports the use of MT for non-specific shoulder pain and ankle sprains, but NOT for SIS impingement syndrome in adults.”
Southerst, D., Yu, H., Randhawa, K., Côté, P., D’Angelo, K., Shearer, H. M., ... & Dion, S. (2015). The effectiveness of
manual therapy for the management of musculoskeletal disorders of the upper and lower extremities: a systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Chiropractic & manual
therapies, 23(1), 30. This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 6
Overview: OMPT for the Shoulder (SIS)
• “Low to Moderate Evidence MT for pain that may not be clinically meaningful”
• “…unclear whether MT used alone or added to an exercise program improves function”
Desjardins-Charbonneau, A., Roy, J. S., Dionne, C. E., Frémont, P., MacDermid, J. C., & Desmeules, F.
(2015). The efficacy of manual therapy for rotator cuff tendinopathy: a systematic review and meta-analysis. journal of orthopaedic & sports physical therapy, 45(5), 330-350.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Shoulder Evidence Conundrum
Poor DX
agreement
High
Treatment
Variability
Lower
Quality
Evidence
(SR’s & MA’s)
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Difficulties with Shoulder Diagnosis
Cyriax Selective Tissue Tension• DeWinter. Ann Rheum Dis. 1999 (Kappa 0.44)
• Pellecchia. JOSPT. 1996 (Kappa 0.88)
Patho-anatomical Examination• Hegedus. Physical Therapy In Sport. 2014
• Biderwolf. IJSPT. 2013
Treatment Based Classification• Carter. Physiotherapy.2012 (Kappa 0.66)
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Flaw in the Review Process for OMPT
Case Study
N=1
• Single Case in front of you with a concordantsign
• Test
• Treat
• Re-Test
RCT
N = Multiple
• Inclusion Criteria SIS = Poor Agreement of DX sign(s)
• Generalized Treatment
• Lower Effectiveness
SR+MA
N = Pooled
• Inclusion Criteria SIS = Less Agreement
• More Generalized
• Exponentially Lower Effectiveness
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
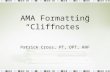
Frost et. al. J Shd Elbow Sx. 1999 MRI study industrial workers:
• Twenty-two (55%) subjects in the impingement group and 16 (52%) subjects in the control group had a pathologic supraspinatus tendon
• As age Increases findings increase
Hey SIS - Get a NEW Paradigm
Picture above: (a) Ant Acromial enthesophyte; (b) bursal-side partial thickness SS tear. Image from Mulyadi et al. MRI of impingement syndromes of the shoulder. Clinical Radiology (2009) 64, 307e318.This information is the property of the speakers and should not
be distributed or otherwise used without the express written permission of the speakers
Hey SIS - Get a NEW Paradigm Lewis J. “Rotator Cuff Tendinopathy: Navigating the Diagnosis- Management Conundrum”. JOSPT 2015.
SIS is a misnomer
• Neer states “95% of SIS is from acromion but this evidence is equivocal”
Reasons?
• Imaging (or even surgery) does not correlate to symptoms
• Testing is based on gold standard of imaging
Result = many undergo surgery on shoulder tissues that may not be the cause of their symptoms
Image from Mulyadi et al. MRI of impingement syndromes of the shoulder. Clinical Radiology (2009) 64, 307e318
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 7
Hey SIS - Get a NEW Paradigm Lewis J. “Rotator Cuff Tendinopathy: Navigating the Diagnosis- Management Conundrum”. JOSPT 2015.
New Paradigm? TBC for Shoulder?
1. Change the T-Spine posture
2. Change Scapular position
3. Change GHJ position
4. Symptom neuromodulation – manual therapy
Reference https://www.londonshoulderclinic.com/wp-content/uploads/2016/08/SSMPv6-2016.pdf
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
OMPT for Shoulder Conditions SUMMAY
• Support of Patho-anatomical classification with the current literature into:• Impingement / Tendinopathy• Adhesive Capsulitis
•How Effective is Manual Therapy for these conditions?
Study Design Considerations:A)OMPT AloneB) OMPT with
ExerciseC) Time Frame:
1. LAB Based (Immediate Effects) vs.
2. Pragmatic (Long Term Effects)This information is the property of the speakers and should not
be distributed or otherwise used without the express written permission of the speakers
Rhon. Ann Intern Med. 2014 Impingement / Tendinopathy
• N=104. Steroid Injection vs. Manual PT group
• 6 visits of impairment based manual PT for CT and shoulder regions
Results:
• Both groups improved with SPADI > 50% maintained through one year
• Steroid vs Manual PT group had more SIS related visits 60% vs 37% including additional steroid injections 38% vs 20%
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Rhon et al: Impairment based PT
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Manual Therapy Specific for Shoulder Impingement / Tendinopathy
1) GHJ Mobilization with movement (MWM)
2) AC mobilization
3) Scapular mobilization
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
MWM Shoulder
With belt end range
contract-relax
Stabilize scapula and
apply posterolateral GH
joint glideThis information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 8
MWM Shoulder
Kachingwe JMMT 2008
• Randomized into 4 Groups:• Supervised Exercise
• Exercise and GHJ mobilization
• Exercise and GHJ MWM
• Wait and see
• No statistical significance but MWM better Pain and ROM
• 6 Visits
Teys Manual Therapy 2008
• MWM vs Sham vs Control
• 1 Visit Only
• Stat Sig Difference ROM and Pain Pressure Threshold
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Delgado-Gil 2015 Shoulder MWM vs ShamJournal of manipulative and physiological therapeutics
• MWM or Sham (No Ex)
• ONLY 4 visits
• RESULTS: Stat Sig improvements in • Pain with Flexion,
• Pain-Free Shoulder Flexion,
• Max Shoulder Flexion
MWM Sham
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
MWM w Belt
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Scapular Specific Mobilization Evidence (SIS)Scapular Retraction Test(Kibler 2006 Am J Sports Med )
Scapular Assistance Test (Rabin 2006 JOSPT)
Scapular Reposition Test (Tate 2008 JOSPT)
Scapula Post Tilt and External Rotation avoiding Full RetractionThis information is the property of the speakers and should not
be distributed or otherwise used without the express written permission of the speakers
Scapula Focused Approach
SR of Bury 2016 Manual Therapy
• 4 Studies met criteria
• Benefits in short term 6 weeks are gone by 3 months
• Early changes in pain are not clinically significant
• Scapula position/movement evidence is conflicting
• Struyf 2013• Scap Mob+Ex vs GHJ Mob+Ex
• Sig Diff Function and Pain
• Surenkok 2009 • Scapular Mobilization Single
treatment effective for Tendinopathy, Tenosynovitis and Adhesive Capsulitis
• Sig Diff with Shd Function, ROM, but NOT Pain
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
2 Hands on Scapula: Protraction & Retraction with Upward tilt
1 Hand on scapula, 1 hand Humeral long axis glide: Lateral scapula mobilizationThis information is the property of the speakers and should not
be distributed or otherwise used without the express written permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 9
Summary for Shoulder Tendinopathy
More Research clearly needed!
Difficulty with experimental designs:
• Pragmatic studies too different for SR’s….BUT this is how we should treat
• How to define and classify tendinopathy?
Reminders:
• Treat the entire patient (RI)
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Adhesive Capsulitis – OMPT vs Injection
2014 Conclusions:•MT & EX not as
effective as Steroid Injection
•Unclear Benefit
• Similar To Sham Ultrasound
Page, M. J., Green, S., Kramer, S., Johnston, R. V., McBain, B., Chau, M., & Buchbinder, R. (2014). Manual therapy and exercise for adhesive capsulitis (frozen shoulder). The Cochrane Library.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Interventions Joint Mobilization“C” weak evidence
• Vermeulen. Phys Ther. 2006
• Bulgen. Ann Rhem Dis. 1984
• Nicholson. JOSPT. 1985
• Vermeulen. Phys Ther. 2000
• Chen. Aust J Physio (N). 2009
• Yang. Phys Ther. 2007
• Tanaka. Clin Rheumatol. 2010
• Johnson. JOSPT. 2007
Kelley JOSPT. 2013Adhesive Capsulitis
CLINICAL PRACTICE GUIDELINE
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Adhesive Capsulitis Phases
Painful Freezing Thawing
Pain > Stiff Stiff > Pain
PainSevere
Night PainStiff Pain at End Range
Stiff Minimal
Pain
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
AC Outcomes OMPT - PAINAuthor Journal Result Brief
Guler-Uysal 2004 Swiss Med Wkly + Cyriax approach
Vermeulen 2006 PTJ = Maitland - Hi Grade (III-IV) better VS Lo Grade (I-II) *1 year
Johnson 2007 JOSPT = Translational - POST Glide > ANT Glide for ER
Buchbinder 2007 Arthritis Rheum = Maitland + Spinal Mobs
Kumar 2012 Rehabil + Maitland & Ex vs EX only
Doner 2013 J Rehabil Med + MWM+Ex+TENS VS Ex+TENS alone
Park 2014 J Phys Ther Sci + Maitland+Kaltenborn+MWM & Distension vs Gen PT
Paul 2014 Clin Ortho Relat Res = Maitland mobs 10 min distraction Inferior Capsule
Espinoza 2015 Medwave + Posterior Mob vs Usual PT; Exclude Hi Irritability
Ali 2015 Pak J Med Sci = Maitland & Ex vs EX only: AP/PA/Inferior-Caudal
Agarwal 2016 J Phys Ther Sci + Reverse Mob vs Kaltenborn’s caudal & post
Celik 2016 Clin Rehab = Mobs Inf/Ant/Post + ROM Ex VS ROM Ex only (*1yr)
Adapted & Updated from Noten 2016 Arch Phys Med RehabThis information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Comparisons & Therapeutic Validity?
What is PT?• Hot Pak
• Ultrasound
• TENS• Diathermy
• Shoulder Pulley
Hoogeboom 2012 PloS one• Patient Eligibility
• Patient Selection• Irritability?
• Competences and setting• Who provided the intervention?• Intervention matched ?
• Rationale
• Content• Intensity monitored• Adjusted & Personalized
• Adherence• What is acceptable
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 10
AC Outcomes OMPT - ROMAuthor Journal Result Brief
Nicholson 1985 JOSPT = Mobilization all directions+ Ex VS Ex only
Guler-Uysal 2004 Swiss Med Wkly + Cyriax approach
Vermeulen 2006 PTJ + Maitland - Hi Grade (III-IV) better VS Lo Grade (I-II) *1 year
Buchbinder 2007 Arthritis Rheum + Maitland + Spinal Mobs
Johnson 2007 JOSPT + Translational - POST Glide > ANT Glide for ER
Tanaka 2010 Clin Rheum + Mobilization - HEP adherence did best
Kumar 2012 Rehabil + Maitland & Ex vs EX only
Yang 2012 Man Ther + Maitland End Range & Scap Mobs VS Mid Range Mob + EX
Doner 2013 J Rehabil Med + MWM added to usual PT of Modalities + Ex
Park 2014 J Phys Ther Sci + Maitland+Kaltenborn+MWM & Distension vs Gen PT
Paul 2014 Clin Ortho Relat Res = Maitland mobs 10 min distraction Inferior Capsule
Ali 2015 Pak J Med Sci = Maitland & Ex vs EX only: AP/PA/Inferior-Caudal
Espinoza 2015 Medwave + Posterior Mob vs Usual PT; Exclude Hi Irritability
Agarwal 2016 J Phys Ther Sci + Reverse Mob vs Kaltenborn’s caudal & post
Celik 2016 Clin Rehab + Mobs Inf/Ant/Post + ROM Ex VS ROM Ex only (*1yr)Adapted & Updated from Noten 2016 Arch Phys Med Rehab
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Vermeulen. Phys Ther. 2006High-Grade Mobilization Better
Significant Findings:
• High Grade 3-4 better, slightly
• Grade 1&2 also effective
0
10
20
30
40
50
60
70
80
Passive ABD 3Months
Passive ABD 12Months
Active ER 12Months
Passive ER 12Months
HIGH GRADE
LOW GRADE
Techniques: Inferior, Ant, Post & Distraction glides Also Reverse Distraction
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Park 2014 J PT Sci
1. Intensive mobilization + steroid injection with capsular distension (IMSID);
2. Intensive mobilization (IM); = Maitland Mobs, End Range, Kaltenborn and MWM
3. Steroid injection with capsular distension (SID);
4. General physical therapy only (GPT) = Hot Pak, TENS, Diathermy (No ex listed) ALL Groups ? Stretching HEP?
Image from: http://cambridgeshoulder.co.uk/shoulder/frozen-shoulder/
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Adhesive Capsulitis – OMPT Summary
• More Research Clearly needed with “Wait & See” Controls• Benefits of OMPT not readily apparent
• Subject Selection: Staging and Irritability
• Combo approach of Steroid, Distention and OMPT appears best
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Taking The Gloves OffReferences Shoulder Tendinopathy
1. Biederwolf, N. E. (2013). A proposed evidence-based shoulder special testing examination algorithm: clinical utility based
on a systematic review of the literature. International journal of sports physical therapy, 8(4), 427.
2. Bury, J., West, M., Chamorro-Moriana, G., & Littlewood, C. (2016). Effectiveness of scapula-focused approaches in patients
with rotator cuff related shoulder pain: a systematic review and meta-analysis. Manual therapy, 25, 35-42.
3. Carter, T., Hall, H., McIntosh, G., Murphy, J., MacDougall, J., & Boyle, C. (2012). Intertester reliability of a classification
system for shoulder pain. Physiotherapy, 98(1), 40-46.
4. Delgado-Gil, J. A., Prado-Robles, E., Rodrigues-de-Souza, D. P., Cleland, J. A., Fernández-de-las-Peñas, C., & Alburquerque-
Sendín, F. (2015). Effects of mobilization with movement on pain and range of motion in patients with unilateral shoulder
impingement syndrome: a randomized controlled trial. Journal of manipulative and physiological therapeutics, 38(4), 245-
252.
5. Desjardins-Charbonneau, A., Roy, J. S., Dionne, C. E., Frémont, P., MacDermid, J. C., & Desmeules, F. (2015). The efficacy of
manual therapy for rotator cuff tendinopathy: a systematic review and meta-analysis. journal of orthopaedic & sports
physical therapy, 45(5), 330-350.
6. de Winter, A. F., Jans, M. P., Scholten, R. J., Devillé, W., van Schaardenburg, D., & Bouter, L. M. (1999). Diagnostic
classification of shoulder disorders: interobserver agreement and determinants of disagreement. Annals of the Rheumatic
Diseases, 58(5), 272-277.
7. Frost, P., Andersen, J. H., & Lundorf, E. (1999). Is supraspinatus pathology as defined by magnetic resonance imaging
associated with clinical sign of shoulder impingement?. Journal of Shoulder and Elbow Surgery, 8(6), 565-568.
8. Hegedus, E. J., Cook, C., Lewis, J., Wright, A., & Park, J. Y. (2015). Combining orthopedic special tests to improve diagnosi s
of shoulder pathology. Physical Therapy in Sport, 16(2), 87-92.
9. Kachingwe, A. F., Phillips, B., Sletten, E., & Plunkett, S. W. (2008). Comparison of manual therapy techniques with
therapeutic exercise in the treatment of shoulder impingement: a randomized controlled pilot clinical trial. Journal of
manual & manipulative therapy, 16(4), 238-247.
10. Kibler, W. B., Sciascia, A., & Dome, D. (2006). Evaluation of apparent and absolute supraspinatus strength in patients with
shoulder injury using the scapular retraction test. The American journal of sports medicine, 34(10), 1643-1647.
11. Pellecchia, G. L., Paolino, J., & Connell, J. (1996). Intertester reliability of the Cyriax evaluation in assessing patients with
shoulder pain. Journal of Orthopaedic & Sports Physical Therapy, 23(1), 34-38.
12. Lewis, J., McCreesh, K., Roy, J. S., & Ginn, K. (2015). Rotator cuff tendinopathy: navigating the diagnosis-management
conundrum. journal of orthopaedic & sports physical therapy, 45(11), 923-937.
13. Mulyadi, E., Harish, S., O'Neill, J., & Rebello, R. (2009). MRI of impingement syndromes of the shoulder. Clinical
radiology, 64(3), 307-318.
14. Steuri, R., Sattelmayer, M., Elsig, S., Kolly, C., Tal, A., Taeymans, J., & Hilfiker, R. (2017). Effectiveness of conservative
interventions including exercise, manual therapy and medical management in adults with shoulder impingement: a
systematic review and meta-analysis of RCTs. Br J Sports Med, 51(18), 1340-1347.
15. Southerst, D., Yu, H., Randhawa, K., Côté, P., D’Angelo, K., Shearer, H. M., ... & Dion, S. (2015). The effectiveness of manual
therapy for the management of musculoskeletal disorders of the upper and lower extremities: a systematic review by the
Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Chiropractic & manual therapies, 23(1), 30.
16. Rabin, A., Irrgang, J. J., Fitzgerald, G. K., & Eubanks, A. (2006). The intertester reliability of the scapular assistance
test. Journal of Orthopaedic & Sports Physical Therapy, 36(9), 653-660.
17. Rhon, D. I., Boyles, R. B., & Cleland, J. A. (2014). One-Year Outcome of Subacromial Corticosteroid Injection Compared With
Manual Physical Therapy for the Management of the Unilateral Shoulder Impingement SyndromeA Pragmatic Randomized
TrialOne-Year Outcome of CSI and MPT for Management of SIS. Annals of internal medicine, 161(3), 161-169.
18. Struyf, F., Nijs, J., Mollekens, S., Jeurissen, I., Truijen, S., Mottram, S., & Meeusen, R. (2013). Scapular-focused treatment in
patients with shoulder impingement syndrome: a randomized clinical trial. Clinical rheumatology, 32(1), 73-85.
19. Surenkok, O., Aytar, A., & Baltaci, G. (2009). Acute effects of scapular mobilization in shoulder dysfunction: a double -blind
randomized placebo-controlled trial. Journal of Sport Rehabilitation, 18(4), 493-501.
20. Tate, A. R., Mcclure, P., Kareha, S., & Irwin, D. (2008). Effect of the scapula reposition test on shoulder impingement
symptoms and elevation strength in overhead athletes. journal of orthopaedic & sports physical therapy, 38(1), 4-11.
21. Teys, P., Bisset, L., & Vicenzino, B. (2008). The initial effects of a Mulligan's mobilization with movement technique on
range of movement and pressure pain threshold in pain-limited shoulders. Manual therapy, 13(1), 37-42.
Kolb WH (@KolbWil)This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Taking The Gloves Off: Kolb WH (@KolbWil)References Frozen shoulder contracture syndrome
1. Agarwal, S., Raza, S., Moiz, J. A., Anwer, S., & Alghadir, A. H. (2016). Effects of two different mobilization techniques on pain, range of motion and functional disability in patients with adhesive capsulitis: a comparative study. Journal of physical therapy science, 28(12), 3342-3349.
2. Ali, S. A., & Khan, M. (2015). Comparison for efficacy of general exercises with and without mobilization therapy for the management of adhesive capsulitis of shoulder-An interventional study. Pakistan journal of medical sciences, 31(6), 1372.
3. Buchbinder, R., Youd, J. M., Green, S., Stein, A., Forbes, A., Harris, A., ... & Wright, W. J. (2007). Efficacy and cost‐effectiveness of physiotherapy following glenohumeral joint distension for adhesive capsulitis: A randomized trial. Arthritis Care & Research, 57(6), 1027-1037.
4. Doner, G., Guven, Z., Atalay, A., & Celiker, R. (2013). Evaluation of Mulligan's technique for adhesive capsulitis of the shoulder. Journal of rehabilitation medicine, 45(1), 87-91.
5. Espinoza, H. J. G., Pavez, F., Guajardo, C., & Acosta, M. (2015). Glenohumeralposterior mobilization versus conventional physiotherapy for primary adhesive capsulitis: a randomized clinical trial. Medwave, 15, e6267.
6. Hoogeboom, T. J., Oosting, E., Vriezekolk, J. E., Veenhof, C., Siemonsma, P. C., De Bie, R. A., ... & Van Meeteren, N. L. (2012). Therapeutic validity and effectiveness of preoperative exercise on functional recovery after joint replacement: a systematic review and meta-analysis. PloS one, 7(5), e38031.
7. Kelley, M. J., Shaffer, M. A., Kuhn, J. E., Michener, L. A., Seitz, A. L., Uhl, T. L., ... & Davies, G. J. (2013). Shoulder pain and mobility deficits: adhesive capsulitis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the Orthopaedic Section of the American Physical Therapy Association. Journal of Orthopaedic & Sports Physical Therapy, 43(5), A1-A31.
8. Kumar, A., Kumar, S., Aggarwal, A., Kumar, R., & Das, P. G. (2012). Effectiveness of Maitland Techniques in idiopathic shoulder adhesive capsulitis. ISRN Rehabilitation, 2012.
9. Neviaser, R. J., & Neviaser, T. J. (1987). The Frozen Shoulder Diagnosis and Management. Clinical orthopaedics and related research, 223, 59-64.
10. Noten, S., Meeus, M., Stassijns, G., Van Glabbeek, F., Verborgt, O., & Struyf, F. (2016). Efficacy of different types of mobilization techniques in patients with primary adhesive capsulitis of the shoulder: a systematic review. Archives of physical medicine and rehabilitation, 97(5), 815-825.
11. Page, M. J., Green, S., Kramer, S., Johnston, R. V., McBain, B., Chau, M., & Buchbinder, R. (2014). Manual therapy and exercise for adhesive capsulitis (frozen shoulder). The Cochrane Library.
12. Park, S. W., Lee, H. S., & Kim, J. H. (2014). The effectiveness of intensive mobilization techniques combined with capsular distension for adhesive capsulitis of the shoulder. Journal of physical therapy science, 26(11), 1767-1770.
13. Paul, A., Rajkumar, J. S., Peter, S., & Lambert, L. (2014). Effectiveness of sustained stretching of the inferior capsule in the management of a frozen shoulder. Clinical Orthopaedics and Related Research®, 472(7), 2262-2268.
14. Vermeulen, H. M., Rozing, P. M., Obermann, W. R., Le Cessie, S., & VlietVlieland, T. P. (2006). Comparison of high-grade and low-grade mobilization techniques in the management of adhesive capsulitis of the shoulder: randomized controlled trial. Physical Therapy, 86(3), 355-368.
15. Yang, J. L., Chang, C. W., Chen, S. Y., Wang, S. F., & Lin, J. J. (2007). Mobilization techniques in subjects with frozen shoulder syndrome: randomized multiple-treatment trial. Physical therapy, 87(10), 1307-1315.
16. Yang, J. L., Jan, M. H., Chang, C. W., & Lin, J. J. (2012). Effectiveness of the end-range mobilization and scapular mobilization approach in a subgroup of subjects with frozen shoulder syndrome: a randomized control trial. Manual therapy, 17(1), 47-52.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 11
Clinical Decision MakingMatthew Vraa, PT, DPT, MBA,
Board Certified Orthopaedic Specialist
Certified Manual Trigger Point Therapist
Fellow, American Academy of Orthopaedic Manual Physical Therapists
Program Director, Rasmussen College - Physical Therapist Assistant Program
“Good decisions come from experience. Experience comes from making bad decisions.”
- Mark TwainThis information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Your next patient
• Referring Diagnosis: Shoulder pain.
• Orders: Evaluation and treat.
• Your hypothesis?• Possible
• Probabilistic
• Problematic
• Planed Tests/Measures
• Planned Intervention
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Your Last Examination
• How many minutes did it take?
• How many hypotheses did you generate?
• What clinical reasoning processes did you employ?
• Was your knowledge sufficient to interpret what you saw?
• Did you effectively plan the physical examination?
• Did you reflect on your examination after the fact to identify gaps?
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Clinical Decision MakingDoody & McAteer. Physiotherapy. 2002Criterion Novices Experts
Mean number of hypotheses generated* 9.2 12.7
Mean time to generate first hypothesis (seconds) 108 (SD 63.60) 112 (SD 62.17)
When majority of hypotheses were generated Physical Exam Subjective Exam
Mean time to complete subjective exam* 8.60 (SD 2.83) 14.22 (SD 6.47)
Mean time to complete physical exam* 20.00 (SD 7.92) 13.93 (SD 5.37)
Mean treatment time 22.10 (SD 15.12) 17.88 (SD 12.85)
Total Time with evaluation 44.92 (SD 17.87) 46.00 (SD 10.60)
Ratio of time on subjective exam versus physical exam 1 : 2.32 1 : 1
Errors in clinical reasoning Errors No errors
Completion of clinical reasoning processes Incomplete Complete
* Statistically significant p < 0.05This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Clinical Decision Making Differences
Novice
• Closed interviews
• Data evaluation
• Process driven
• Judgment after data
• Current knowledge about tests
• Skills are not automatic
• Routine Evaluation/Treatment
• Reflection on Action
Expert
• Open interviews
• Intuitive data gathering
• Prioritization driven
• Diagnostic/Pattern recognition
• Testing for intervention success
• Ability to multi-task
• Improvisational Performances
• Refection in/for Action
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Clinical Decision Making Differences
• Doody & McAteer. Physiotherapy. 2002
• May et al. Aust J Physiother. 2008
• Frew et al. Hong Kong J Occ Ther. 2008.
• Wainwright et al. Phys Ther. 2010.
• Elvén et al. Physiother Theory Pract. 2015.
• Roots et al. Int J Osteopath Med. 2016
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 12
Other ProfessionalsAllen, et al. Int J Med Inform. 1998
Med Students Residents Physicians
Novice Expert
-Less ability to gather evidence for competing diagnosis-Often use negative evidence or questions when hypothesis is unclear-Segmented information from competing diagnosis
-Less accurate initial hypothesis-Inefficient evidence (data) gathering strategies-Higher proportion of negative question (r/o)
-More accurate initial hypothesis-Use more predictive or positive questions to refine diagnosis
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Clinical Reasoning: A Developmental Process
Deductive Reasoning
• Hypothesis-Theoretical-Deductive
Deductive Reasoning
& Inductive Reasoning
Inductive Reasoning
• Pattern Recognition
Time and Meaningful Reflection on Experiences
ReflectionOn Action
Reflection In Action
Reflection For Action
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Good Clinical Decision Making
• Where do you start?
Knowledge / Understanding
Experience
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
How to build your clinical decision making
• 1) Build your Hypotheses Generation Ability• HOAC II Tool
• SCRIPT Tool
• Forward Thinking
• Pattern Recognition
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Hypothesis-Algorithm for CliniciansRothstein, et al. Phys Ther. 2003.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Hypothesis-Algorithm for CliniciansRothstein, et al. Phys Ther. 2003.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 13
Systematic Clinical Reasoning in Physical Therapy (SCRIPT)Baker et al. Phys Ther. 2017
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Forward Thinking
• Taking your hypothesis to the next level. • If this…..then….
• Not just thinking down the line, but also the reasoning why it would occur or could occur.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Pattern recognition
• Reasoning that takes specific information and makes a broader generalization that it considered probable
• More precise problem representation
• Problem representation- the disease
• Recognition that all elements are present
• Skills- ability to process and develop problem representation; knowledge of disease scripts Patient Signs & Symptoms
Appraisal of data
Remaining Hypothesis
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Things that affect your pattern recognition
• Knowledge and Experience about/with• Condition and mimicking conditions
• Condition frequency in population and clinic
• Condition Mechanism of Injury
• Cases where you were• Correct
• Incorrect
• Reflection on it.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Forward thinking and pattern recognition require better problem representation• Incorporate all significant symptoms and signs
• Describe them as accurately as possible
• Emphasize the most specific features
• Avoid distracting by minor signs, symptoms or non specific findings
• Match the patients presentation to classic disease description
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Future Thinking and Pattern Recognition Problems• Confirmation Bias: Only running test that rule in your hypothesis
• Just because you think it is a certain condition, you need to be diligent to check other hypothesis.
• Asking Open Ended Questions that provide you answers vs Closed Ended ones that bias your thinking
• Need to use Sensitive Tests to rule out.• Need to use Specific Tests to rule in.
• Attempting to link all findings to one condition.• Occam's razor
• Multiple diseases/conditions can have similar presentations• Understand different features/presentations• Understand similar features/presentations
Condition A
Condition B
Condition C
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 14
How to build your clinical decision making
• 1) Build your Hypotheses Generation Ability• HOAC II Tool
• SCRIPT Tool
• Forward Thinking
• Pattern Recognition
• 2) Evidence Based Practice• Clinician Experience
• Best Research
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Evidence Based Practice
EBP
Clinical Experience
Best Research Evidence
Patient Values &
Preference
“The conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients.” - Sacket, et al. BMJ. 1996.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
What happens when we don’t have high level evidence to support what we are doing or our clinical decision making?
Transitive Relationships
• A is to B. B is to C. Therefore A is to C
Intersection Relationship
• A intersects with B.
• B Intersects with C.
• C intersects with A.
• Therefore A, B, and C intersect.
Study A
Study B
Study C
Study A
Study B
Study C
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
How to build your clinical decision making
• 1) Build your Hypotheses Generation Ability• HOAC II Tool
• SCRIPT Tool
• Forward Thinking
• Pattern Recognition
• 2) Evidence Based Practice• Clinician Experience
• Best Research
• Patient Preference
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
The customer is always right. Right?
• May not always be right, but patient values/ expectations can affect outcomes and need to be considered in patient selection for interventions.
• Bialosky, et al. Phys Ther. 2010.
• Puentedura, et al. J OrthopSports Phys Ther. 2012.
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
How to build your clinical decision making
• 1) Build your Hypotheses Generation Ability• HOAC II Tool
• SCRIPT Tool
• Forward Thinking
• Pattern Recognition
• 2) Evidence Based Practice• Clinician Experience
• Best Research
• Patient Preference
• 3) Test – Treat - Retest
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers

1/16/2018
This information is the property of the speakers and should not be distributed or otherwise used without the express written permission of the speakers 15
Clinical Reasoning?????
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Take Home
• Reflect on action, in action and for action.
• Use best evidence when possible.• Use lower when you don’t have “top of the mountain” evidence.
• When your patient doesn’t match study criteria, look for the strongest predictors.
• Lack of Evidence is different than Evidence of Lack
• Pattern recognition and clinician experience is a part of EBM.
• Reflect upon the individual patient in front on you (n=1)• Test, Treat, Re-test
• If you try something and it works, it is therapy. If it doesn’t work, then it is evaluation.
• You can find out, what it is, by what it isn’t.This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
References• Allen VG, Arocha JF, Patel VL. Evaluating evidence against diagnostic hypotheses in clinical decision making by students, residents and physicians. Int
J Med Inform. 1998 Aug-Sep;51(2-3):91-105.• Baker SE, Painter EE, Morgan BC, Kaus AL, Petersen EJ, Allen CS, Deyle GD, Jensen GM. Systematic Clinical Reasoning in Physical Therapy (SCRIPT):
Tool for the Purposeful Practice of Clinical Reasoning in Orthopedic Manual Physical Therapy. Phys Ther. 2017 Jan 1;97(1):61-70.• Bialosky JE, Bishop MD, Cleland JA. Individual expectation: an overlooked, but pertinent, factor in the treatment of individuals experiencing
musculoskeletal pain. Phys Ther. 2010 Sep;90(9):1345-55. • Doody, C and McAteer, M. Clinical reasoning of expert and novice physiotherapists in an outpatient orthopaedic setting. Physiotherapy. 2002 May;
88(5): 258-268.• Elvén M, Hochwälder J, Dean E, Söderlund A. A clinical reasoning model focused on clients' behavior change with reference to physiotherapists: its
multiphase development and validation. Physiother Theory Pract. 2015 May;31(4):231-43.• Frew K, Joyce E, Tanner B, Gray M. Clinical Reasoning and the International Classification of Functioning: A Linking Framework. Hong Kong J Occ Ther.
2008;18(2): 68-72.• May S, Greasley A, Reeve S, Withers S. Expert therapists use specific clinical reasoning processes in the assessment and management of patients
with shoulder pain: a qualitative study. Aust J Physiother. 2008;54(4):261-6.• Puentedura EJ, Cleland JA, Landers MR, Mintken PE, Louw A, Fernández-de-Las-Peñas C. Development of a clinical prediction rule to identify patients
with neck pain likely to benefit from thrust joint manipulation to the cervical spine. J Orthop Sports Phys Ther. 2012 Jul;42(7):577-92. • Roots S, Niven E. Moran R. Osteopaths' clinical reasoning during consultation with patients experiencing acute low back pain: A qualitative case
study approach. Int J Osteopath Med. 2016; 19(3): 20-34.• Rothstein JM, Echternach JL. Hypothesis-oriented algorithm for clinicians. A method for evaluation and treatment planning. Phys Ther. 1986
Sep;66(9):1388-94. • Rothstein JM, Echternach JL, Riddle DL. The Hypothesis-Oriented Algorithm for Clinicians II (HOAC II): a guide for patient management. Phys Ther.
2003 May;83(5):455-70.• Wainwright SF, Shepard KF, Harman LB, Stephens J. Novice and experienced physical therapist clinicians: a comparison of how reflection is used to
inform the clinical decision-making process. Phys Ther. 2010 Jan;90(1):75-88.This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Shoulder Case
This information is the property of the speakers and should not be distributed or otherwise used without the express written
permission of the speakers
Related Documents