
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


1
Table of Contents
H O W T O U S E T H I S M O N O G R A P H
This CME activity contains both audio and print components. To receive credit, the participant should listen to the CDs or tapes, review the monograph and complete the post-test and evaluation form located in the back of this monograph or on our website. This monograph contains edited comments, clinical trial schemas, graphics and references that supplement the audio program. ColorectalCancerUpdate.com includes an easy-to-use interac-tive version of this monograph with links to relevant full-text articles, abstracts, trial information and other web resources indicated here in red underlined text.
2 CME Information
4 Editor’s Note: Content King
6 Daniel G Haller, MD Professor of Medicine
Associate Chief for Clinical Affairs University of Pennsylvania Cancer Center Editor-in-Chief Journal of Clinical Oncology Philadelphia, Pennsylvania
10 Charles S Fuchs, MD, MPH Associate Professor of Medicine
Dana-Farber Cancer Institute Boston, Massachusetts
14 Peter C Enzinger, MD Instructor in Medicine, Harvard Medical School
Clinical Director, Gastrointestinal Cancer Center Dana-Farber Cancer Institute Boston, Massachusetts
18 Post-test
19 Evaluation

Colorectal Cancer Update A CME Audio Series and Activity
2
S T A T E M E N T O F N E E D / T A R G E T A U D I E N C E
Colorectal cancer is among the most common cancers in the United States, and the arena of colorectal cancer treatment continues to evolve. Published results from ongoing clinical trials lead to the emergence of new thera-peutic agents and regimens and changes in indications, doses and schedules for existing treatments. In order to offer optimal patient care — including the option of clinical trial participation — the practicing medical oncologist must be well informed of these advances.
To bridge the gap between research and patient care, Colorectal Cancer Update utilizes one-on-one discus-sions with leading oncology investigators. By providing access to the latest research developments and expert perspectives, this CME activity assists medical oncologists in the formulation of up-to-date clinical management strategies.
G L O B A L L E A R N I N G O B J E C T I V E S
Upon completion of this activity, participants should be able to:
• Critically evaluate the clinical implications of emerging clinical trial data in colorectal cancer treatment.
• Counsel patients about the risks and benefits of adjuvant and neoadjuvant chemotherapy.
• Develop and explain a management strategy for patients with metastatic colorectal cancer.
• Describe ongoing clinical trials in colorectal cancer and counsel patients about the availability of ongoing clinical trials.
P U R P O S E O F T H I S I S S U E O F C O LO R E C TA L C A N C E R U P D AT E
The purpose of Issue 6 of Colorectal Cancer Update is to support these global objectives by offering the perspec-tives of Drs Haller, Fuchs and Enzinger on the integration of emerging clinical research data into the management of colorectal cancer.
A C C R E D I T A T I O N S T A T E M E N T
Research To Practice is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
C R E D I T D E S I G N A T I O N S T A T E M E N T
Research To Practice designates this educational activity for a maximum of 3 category 1 credits toward the AMA Physician’s Recognition Award. Each physician should claim only those credits that he/she actually spent in the activity.
3
F A C U L T Y D I S C L O S U R E S
As a provider accredited by the Accreditation Council for Continuing Medical Education, it is the policy of Research To Practice to require the disclosure of any significant financial interest or any other relationship the sponsor or faculty members have with the manufacturer(s) of any commercial product(s) discussed in an educational presen-tation. The presenting faculty reported the following:
This educational activity contains discussion of published and/or investigational uses of agents that are not indicated by the Food and Drug Administration. Research To Practice does not recommend the use of any agent outside of the labeled indications. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications and warnings. The opinions expressed are those of the presenters and are not to be construed as those of the publisher or grantor.
G E N E R I C T R A D E M A N U FA C T U R E R
bevacizumab Avastin™ Genentech BioOncology
capecitabine Xeloda® Roche Laboratories Inc
cetuximab Erbitux™ ImClone Systems
fluorouracil (5-FU) Various Various
irinotecan Camptosar® Pfizer Inc
leucovorin calcium Various Various
oxaliplatin Eloxatin® Sanofi-Synthelabo Inc
trastuzumab Herceptin® Genentech BioOncology
UFT (tegafur+uracil) Not FDA-Approved —
Pharmaceutical agents discussed in this program
Daniel G Haller, MDGrants/Research Support, Consultant, and Honorarium: Bristol-Myers Squibb Company, Pfizer Inc, Roche Laboratories Inc, Sanofi-Synthelabo Inc Speakers Bureau: Sanofi-Synthelabo Inc
Charles S Fuchs, MD, MPHGrants/Research Support: AstraZeneca Pharmaceuticals LP, Genentech BioOncology, Pfizer Inc, Sanofi-Synthelabo Inc Speakers Bureau: Genentech BioOncology, Pfizer Inc, Sanofi-Synthelabo Inc
Peter C Enzinger, MDGrants/Research Support and Honorarium: Aventis Pharmaceuticals Inc, Bristol-Myers Squibb Company, Genentech BioOncology, ImClone Systems, Pfizer Inc, Roche Laboratories Inc, Sanofi-Synthelabo Inc

Editor’s Note
4
Dan Haller is an oncologic gadfly and editor of the premiere source of clinical research information for medical oncologists — a royal blue rag called the Journal of Clinical Oncology. For a long time, I have wanted to sit down and talk with this important figure in all of our lives, but my initial attempts to interview him were gently rebuffed. Fortunately, we finally hooked up in the very unpresi-dential “Presidential Suite” at the Westin O’Hare (complimentary fruit basket included).
Dan is a busy guy and he graciously gave up a dinner invitation to chat with me about colorectal cancer research and the “Think Tank” that he was attending and I was moderating the following day (see our next issue, a special edition on this event). However, before we got to that, I had to ask him about his life as the editor of JCO.
Listening to Dan speak, I quickly got the feeling that his role is a lot like that of the O’Hare chief air traffic controller directing the effort at one of the world’s busiest hubs just a few blocks away. Dan has a team of associate editors who electronically sift through article submissions and pick the very best to publish in the world’s most trusted oncology periodical.
The extraordinary efficiency of this team is good news for docs and particularly for their patients, in that the most valued “seal of approval” is publication in a peer-reviewed journal, and the JCO is clearly where the best stuff usually lands. I sensed a wee bit of competitiveness when Dan referred to a white “throwaway journal” that scoops some of the more prominent research papers.
For example, it must have rankled him a bit that the June 3 issue of the aforemen-tioned “other” (New England) journal included the first report from the MOSAIC trial defining FOLFOX as the new standard of care for adjuvant therapy of colorectal cancer and the paper by Herb Hurwitz on his landmark study of IFL plus bevacizumab in patients with metastatic disease.
I like Dan a lot. He is smart, funny, amazingly well-read and seems to have a good heart. It’s a pleasure to be able to bring leading figures like Dan, and the other two researchers interviewed for this issue — Charles Fuchs and Peter Enzinger — to a national audience of physicians.
Content King

5
Cancer patients and health care professionals are all a lot better off because Dan and his coeditors are efficiently and effectively directing traffic in oncologic skies that seem more crowded but also more interesting every year.
— Neil Love, MD [email protected]
Select recent publications in the “blue journal”Benson AB 3rd et al. American Society of Clinical Oncology recommendations on adjuvant chemo-therapy for stage II colon cancer. J Clin Oncol 2004;22(16):3408-19. Abstract
Cassidy J et al. XELOX (capecitabine plus oxaliplatin): Active first-line therapy for patients with metastatic colorectal cancer. J Clin Oncol 2004;22(11):2084-91. Abstract
Gerard JP et al. Improved sphincter preservation in low rectal cancer with high-dose preoperative radiotherapy: The lyon R96-02 randomized trial. J Clin Oncol 2004;22(12):2404-9. Abstract
Gill S et al. Pooled analysis of fluorouracil-based adjuvant therapy for stage II and III colon cancer: Who benefits and by how much? J Clin Oncol 2004;22(10):1797-806. Abstract
Grothey A et al. Survival of patients with advanced colorectal cancer improves with the availability of fluorouracil-leucovorin, irinotecan, and oxaliplatin in the course of treatment. J Clin Oncol 2004;22(7):1209-14. Abstract
Gunderson LL et al. Impact of T and N stage and treatment on survival and relapse in adjuvant rectal cancer: A pooled analysis. J Clin Oncol 2004;22(10):1785-96. Abstract
Hoff PM et al. Phase II study of capecitabine in patients with fluorouracil-resistant metastatic colorectal carcinoma. J Clin Oncol 2004;22(11):2078-83. Abstract
Lal R et al. A randomized trial comparing defined-duration with continuous irinotecan until disease progression in fluoropyrimidine and thymidylate synthase inhibitor-resistant advanced colorectal cancer. J Clin Oncol 2004;22(15):3023-31. Abstract
Martenson JA Jr et al. Phase III study of adjuvant chemotherapy and radiation therapy compared with chemotherapy alone in the surgical adjuvant treatment of colon cancer: Results of Intergroup protocol 0130. J Clin Oncol 2004;22(16):3277-83. Abstract
Saltz LB et al. Phase II trial of cetuximab in patients with refractory colorectal cancer that expresses the epidermal growth factor receptor. J Clin Oncol 2004;22(7):1201-8. Abstract
Temple LK et al. Use of surgery among elderly patients with stage IV colorectal cancer. J Clin Oncol 2004;22(17):3475-84. Abstract
Thirion P et al; Meta-Analysis Group in Cancer. Modulation of fluorouracil by leucovorin in patients with advanced colorectal cancer: An updated meta-analysis. J Clin Oncol 2004;22(18):3766-75. Abstract
6
E D I T E D C O M M E N T S
Daniel G Haller, MD
MOSAIC adjuvant trialIn this study, the addition of oxaliplatin resulted in a 23 percent overall reduction in the risk of relapse — 24 percent for patients with Stage III and 20 percent for patients with Stage II disease. We’ll learn about survival in approximately one year. Dan Sargent’s model demonstrating that three-year disease-free survival predicts five-year outcomes is much more stable for patients with Stage III than Stage II disease (André 2004, Sargent 2004).
Nonprotocol adjuvant therapy options for patients with colon cancer In my clinic, I use modified FOLFOX6 or modified FOLFOX7 as adjuvant therapy in patients with colon cancer. I wouldn’t consider FOLFOX4 unacceptable, but it is a 1996 regimen. Data from the OPTIMOX trial demonstrated that FOLFOX4 has more neutropenia compared to FOLFOX7 because of the bolus 5-FU, but the two regimens offer comparable efficacy (André 2003). Either modified FOLFOX6 or modified FOLFOX7 are acceptable adjuvant therapy options. I educate clinicians to stay away from FOLFOX4 because they may have more negative experiences with that regimen.
I don’t consider CAPOX an adjuvant option, but I do consider it a default. In patients who cannot deal with a pump or a port — and those are relatively few in my practice — and for whom I believe combination therapy is a better option, I’d rather use CAPOX than 5-FU or capecitabine alone.
X-ACT adjuvant trialIn patients with advanced disease, the Mayo Clinic regimen of 5-FU/leucovorin has been compared to capecitabine; the response rate for capecitabine was higher, while median survival was the same (Twelves 2001). If the advanced disease model roughly predicts for benefit in the adjuvant setting, the results from the X-ACT adjuvant trial should come as no surprise. As expected, adjuvant capecitabine showed equivalency to the Mayo Clinic regimen in patients with Stage III disease. This well-conducted study also demonstrated that patients
Dr Haller is a Professor of Medicine and Associate Chief for Clinical Affairs at the University of Pennsylvania Cancer Center in Philadelphia, Pennsylvania and Editor-in-Chief of the Journal of Clinical Oncology.
7
treated with adjuvant capecitabine had a trend toward improved overall survival (Cassidy 2004).
Adjuvant therapy trial comparing CAPOX to the Roswell Park or the Mayo Clinic regimenIn a Phase II trial of 96 patients with metastatic colorectal cancer, a 55 percent response rate was reported for capecitabine plus oxaliplatin (CAPOX) as first-line therapy (Cassidy 2004), which is similar to the response rate for FOLFOX. Hence, a trial complementary to the MOSAIC adjuvant trial will compare CAPOX to either the Roswell Park or the Mayo Clinic regimen.
The trial accrued ahead of schedule and has enrolled 1,800 patients with Stage III disease. Within 12 months, we should have toxicity data for the largest popula-tion of patients treated with capecitabine and oxaliplatin. The efficacy data will probably be available in 2006. I believe the results will be similar to the results from the MOSAIC adjuvant trial.
Treatment options for patients with colorectal cancer recurrence after adjuvant therapy My approach to patients with a colorectal cancer recurrence after adjuvant therapy depends on when the relapse occurs. Obviously, this is now an issue because of the results from the MOSAIC adjuvant trial. In a patient who relapses less than six months after adjuvant FOLFOX and still has neuropathy, I would use FOLFIRI plus bevacizumab as first-line therapy. That type of patient would need all the help available, not sequential therapy.
A patient who relapses four years after adjuvant FOLFOX and doesn’t have neuropathy could be treated as a “virgin patient,” and whichever chemotherapy regimen is the best for that patient should be selected, independent of their adjuvant therapy. In those situations, I base my chemotherapy decision on the Tournigand data (Tournigand 2004). Then, I select the most tolerable and effica-cious biologic agent and marry it to the chemotherapeutic regimen that is best for the patient.
The best regimen is dependent upon both its efficacy and toxicity. For example, the first violinist in the Philadelphia Orchestra might be treated with FOLFIRI plus bevacizumab. In my clinic, patients will not be treated with IFL plus bevaci-zumab; they also won’t be treated with capecitabine plus bevacizumab outside of a trial. For the non-violinist, most often FOLFOX plus bevacizumab would be selected.
In certain patients, bolus 5-FU/leucovorin — the Roswell Park regimen — plus bevacizumab, as used in the trial by Kabbinavar (Kabbinavar 2004) and one of the arms of the trial by Hurwitz, would be a reasonable option. Based on the data from the trial by Hurwitz, the efficacy of the Roswell Park regimen plus bevacizumab is somewhere in between the efficacy for IFL alone and IFL plus bevacizumab. I believe the Roswell Park regimen plus bevacizumab is probably less efficacious than FOLFOX plus bevacizumab.

8
Treatment options for patients with rectal cancer I believe preoperative chemoradiation therapy is now the gold standard for patients with rectal cancer. Since the 1991 consensus conference, the American model for the management of rectal cancer had generally consisted of surgery followed by postoperative chemoradiation therapy for patients with Stage II or Stage III disease.
Currently, either adjuvant or neoadjuvant chemoradiation therapy are accept-able options. Based on the German Rectal Cancer trial comparing preoperative and postoperative chemoradiation therapy, more people will be switching to the preoperative model (Sauer 2003). In the United States, preoperative or postopera-tive radiation therapy alone would be unacceptable options.
Neoadjuvant chemotherapy options for patients with rectal cancer We’re mostly using neoadjuvant chemoradiation therapy, so I believe a standard regimen would consist of infusional 5-FU and radiation therapy. According to Joel Tepper’s presentation of the Intergroup-0114 trial results, the bolus regimen has more toxicity and equal efficacy (Tepper 2002); however, patients who are confounded by infusional therapy might choose one of the bolus regimens.
In patients who absolutely do not want infusional therapy, the cumulative data for capecitabine suggest that it could be substituted. I’m not willing to simply say capecitabine can be substituted in every patient, but I believe it’s an option. I’d like to see the equivalency data in the curative model from the NSABP-R-04 trial.
The NSABP-R-04 trial will utilize capecitabine throughout the radiation therapy. We are conducting a trial using capecitabine on a Monday-to-Friday schedule because we want the drug administered at the same time as the radiation therapy. With our schedule, diarrhea, hand-foot syndrome and, hence, a break in therapy may be less likely to occur.
ECOG-E3200This study enrolled approximately 880 patients who had been treated with 5-FU and irinotecan (1.1). The trial was designed before FOLFOX was approved as second-line therapy, and it compared bevacizumab alone to FOLFOX4 with or without bevacizumab (Giantonio 2004).
The bevacizumab dose tested in E3200 was 10 mg/kg because the correct dose was unknown at the time the study was designed. I believe the approved dose of 5 mg/kg is the right dose.
So far, the combination of FOLFOX4 plus bevacizumab has demonstrated safety. The bevacizumab-alone arm was terminated early, because the survival data were not quite good enough for the antibody alone; therefore, in patients with disease progression on first-line therapy, bevacizumab alone was not as good as the best available chemotherapy. We don’t, however, know whether an antibody might be an effective maintenance therapy in patients who are responding to therapy.

9
Select publicationsAndré T et al. FOLFOX7 compared to FOLFOX4. Preliminary results of the randomized optimox study. Proc ASCO 2003;22:253;Abstract 1016.
André T et al; Multicenter International Study of Oxaliplatin/5-Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC) Investigators. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 2004;350(23):2343-51. Abstract
Cassidy J et al; Capecitabine Colorectal Cancer Study Group. First-line oral capecitabine therapy in metastatic colorectal cancer: A favorable safety profile compared with intravenous 5-fluorouracil/leucovorin. Ann Oncol 2002;13(4):566-75. Abstract
Cassidy J et al. XELOX (capecitabine plus oxaliplatin): Active first-line therapy for patients with metastatic colorectal cancer. J Clin Oncol 2004;22(11):2084-91. Abstract
Giantonio BJ et al. The addition of bevacizumab (anti-VEGF) to FOLFOX4 in previously treated advanced colorectal cancer (advCRC): An updated interim toxicity analysis of the Eastern Cooperative Oncology Group (ECOG) study E3200. Proc ASCO GI Symposium 2004;Abstract 241.
Kabbinavar FF et al. Bevacizumab (a monoclonal antibody to vascular endothelial growth factor) to prolong progression-free survival in first-line colorectal cancer (CRC) in subjects who are not suitable candidates for first-line CPT-11. J Clin Oncol 2004;22(14 Suppl);Abstract 3516.
Sargent DJ et al. Disease-free survival (DFS) vs. overall survival (OS) as a primary endpoint for adjuvant colon cancer studies: Individual patient data from 12,915 patients on 15 randomized trials. J Clin Oncol 2004;22(14 Suppl);Abstract 3502.
Sauer R et al; German Rectal Cancer Group. Adjuvant vs. neoadjuvant radiochemotherapy for locally advanced rectal cancer: The German trial CAO/ARO/AIO-94. Colorectal Dis 2003;5(5):406-15. Abstract
Tepper JE et al. Adjuvant therapy in rectal cancer: Analysis of stage, sex, and local control — final report of Intergroup 0114. J Clin Oncol 2002;20(7):1744-50. Abstract
Tournigand C et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: A randomized GERCOR study. J Clin Oncol 2004;22(2):229-37. Abstract
Twelves C et al; Xeloda Colorectal Cancer Study Group. Capecitabine (Xeloda) improves medical resource use compared with 5-fluorouracil plus leucovorin in a phase III trial conducted in patients with advanced colorectal carcinoma. Cancer 2001;37(5):597-604. Abstract
Eligibility: Patients with advanced or metastatic colorectal cancer that has been treated with a fluoropyrimidine-based regimen and an irinotecan-based regimen, either alone or in combination
R
[Oxaliplatin + infusional 5-FU + leuco-vorin + bevacizumab] every 2 weeks
SOURCE: NCI Physician Data Query, October 2003.
Protocol IDs: E-3200, CTSU Accrual: 880 patients (Closed)
1.1 Phase III Randomized Study of Oxaliplatin, Fluorouracil and Leucovorin Calcium with or without Bevacizumab versus Bevacizumab Only in Patients with Previously Treated Advanced or Metastatic Colorectal Adenocarcinoma
[Oxaliplatin + infusional 5-FU + leuco-vorin] every 2 weeks
Bevacizumab every 2 weeks

1 0
E D I T E D C O M M E N T S
1 0
E D I T E D C O M M E N T S
Charles S Fuchs, MD, MPH
Recently reported rectal cancer trials EORTC-22921 randomly assigned patients with T3 and T4 lesions to preoperative radiation therapy or preoperative radiation therapy plus chemotherapy, the latter being a more standard approach in the United States. The preliminary results demonstrated advantages for the addition of chemotherapy to preop-erative radiation therapy — better tumor downstaging; smaller tumors; less lymphatic, venous and perineural (LVN) invasion; and fewer positive nodes.
We must wait for longer follow-up, but the preliminary results support the addition of chemotherapy to preoperative radiation therapy (Bosset 2004). This may not be an interesting question to United States investigators because we’re already comfortable adding chemo-therapy. NSABP-R-03 compared preoperative to postoperative chemoradiation therapy. Three trials had actually attempted to perform this randomization, but had problems with accrual. In fact, NSABP-R-03 didn’t accrue well, with only 267 of the 900 projected patients enrolled. The analysis of those 267 patients suggests that preoperative chemoradiation therapy is reasonably tolerated and provides a trend toward improved sphincter preservation and disease-free and overall survival (Roh 2004).
Because the German Rectal Cancer (CAO/ARO/AIO-94) trial was able to complete accrual, it is the definitive study. The trial asked the same question: Is preoperative or postoperative chemoradiation therapy better? Among over 800 patients enrolled, preoperative chemoradiation therapy resulted in a much higher rate of sphincter preservation and a trend toward better disease-free and overall survival. We may see significant benefits in terms of overall survival when the study matures (Sauer 2003).
Bevacizumab as a potential radiation sensitizerIn Nature Medicine earlier this year, Chris Willett reported preliminary data from the first six patients with rectal cancer who were enrolled in a Phase I trial of bevacizumab in combination with chemoradiation therapy. The trial demon-strated tolerability and interesting biologic data suggesting that bevacizumab
Dr Fuchs is an Associate Professor of Medicine at the Dana-Farber Cancer Institute in Boston, Massachusetts.

1 1
might improve the efficacy of radiation therapy to treat rectal tumors. Patients received bevacizumab on day one, and two weeks later they were treated with 5-FU plus bevacizumab and radiation therapy. Endoscopies and CT scans were performed before and 12 days after bevacizumab was administered. Better tumor blood flow and lower interstitial pressure was noted 12 days after bevaci-zumab administration (Willett 2004).
In terms of the preclinical data from animal models and mice xenografts, synergy has been demonstrated for bevacizumab and radiation therapy. The reason for the synergy may be related to bevacizumab’s ability to normalize the tumor vasculature, which allows for better oxygen perfusion to the tumors and makes them more sensitive to radiation therapy. Also, bevacizumab reduces interstitial pressure in tumors, which also potentially enhances the ability of oxygen delivery and radiation sensitization (Lee 2000).
Potential synergy between bevacizumab and chemotherapyConcern that bevacizumab might reduce blood flow and not allow chemo-therapy to enter the tumors led to preclinical trials being conducted. However, by reducing interstitial pressure, bevacizumab actually improved the perfusion of chemotherapy into the tumor. In an animal model, irinotecan concentrations within tumors were measured before and after bevacizumab or placebo. With bevacizumab, much higher concentrations of irinotecan were delivered within the tumor, suggesting the hypothesis of improved tumor vasculature.
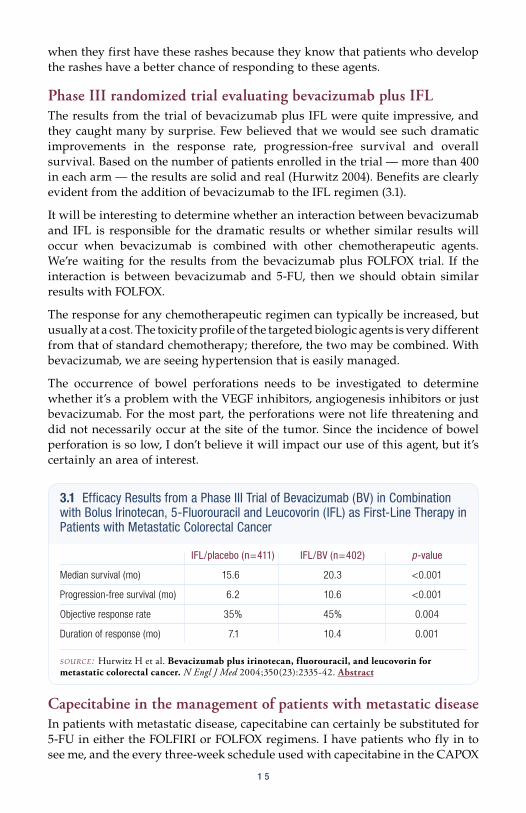
X-ACT adjuvant trialX-ACT was a well designed trial comparing bolus 5-FU/leucovorin to capecitabine as adjuvant therapy for patients with colon cancer. The results from this trial (2.1) suggest equivalence for capecitabine and bolus 5-FU/leucovorin. Although the difference was a few percent, a slight trend towards improved overall survival with capecitabine approached statistical significance (Cassidy 2004). NSABP-C-06 evaluating UFT — an alternative oral fluoropyrimidine — confirmed the X-ACT adjuvant trial results. Adjuvant UFT was as good as bolus 5-FU/leucovorin in patients with Stage II and Stage III colon cancer (Wolmark 2004). I believe adjuvant capecitabine is a reasonable alternative to 5-FU/leucovorin. Personally, I’d like to see a rigorous trial in the adjuvant setting to determine whether capecitabine is equivalent to infusional 5-FU.
CALGB-89803: Adjuvant IFL trial CALGB-89803 randomly assigned patients with Stage III disease to adjuvant therapy with the Roswell Park regimen of 5-FU/leucovorin or the Saltz regimen of IFL. We were confident that study would be positive, but, in fact, it was not. Surprisingly, no differences between 5-FU/leucovorin and IFL were found, no matter how the data was evaluated. Patients treated with IFL had more toxicity and a slightly higher rate of toxic deaths. Therefore, IFL should not be used in the adjuvant setting (Saltz 2004). It is disappointing that a survival benefit was not found with adjuvant IFL, but the door is not closed on adjuvant irinotecan. The Pan-European Trials in Adjuvant Colorectal Cancer (PETACC-3) trial evaluated

1 2
adjuvant FOLFIRI, an infusional schedule of 5-FU and irinotecan. Data from that trial are not yet available. Like the MOSAIC adjuvant trial that used oxaliplatin and infusional 5-FU, irinotecan and infusional 5-FU may also be beneficial.
Trial evaluating bevacizumab plus 5-FU/leucovorin as first-line therapy in patients with metastatic diseaseAn interesting alternative to the Hurwitz trial evaluating IFL plus bevaci-zumab was a trial that enrolled patients who were not candidates for a three-drug regimen because of age or impaired performance status. Admittedly, the inclusion criteria can be debated because older individuals do not necessarily perform worse on a three-drug regimen. The trial randomly assigned approxi-mately 200 patients treated with the Roswell Park regimen of 5-FU/leucovorin to placebo or bevacizumab.
A proportionate and similar, although not statistically significant, benefit was seen with the addition of bevacizumab, as evidenced in the Hurwitz trial. The results weren’t statistically significant because the study wasn’t powered to evaluate survival. Apparently, bevacizumab can be added to any 5-FU-containing regimen and offer a benefit (Kabbinavar 2004).
Role of capecitabine in the management of patients with metastatic diseaseThree randomized trials have shown that capecitabine is equivalent to bolus 5-FU/leucovorin (Van Cutsem 2004; Hoff 2001). In patients with metastatic disease, an important question is whether capecitabine is equivalent to infusional 5-FU, because the Europeans have demonstrated that infusional 5-FU is better than bolus 5-FU (de Gramont 1997). Data are supportive of FOLFOX and FOLFIRI, which also utilize infusional 5-FU. Whether infusional 5-FU/leucovorin can be replaced by capecitabine in FOLFOX and FOLFIRI may seem like a mundane question; however, if bolus 5-FU is inferior to infusional 5-FU, we need to know whether capecitabine is equivalent to infusional 5-FU.
2.1 X-ACT Study: Randomized Phase III Adjuvant Trial Comparing Capecitabine to Bolus 5-FU/Leucovorin in Patients with Dukes’ C Colon Cancer
Capecitabine 5-FU/LV (n=1,004) (n=983) HR (95% CI) p-value
Primary endpoint 3-y DFS 64.2% 60.6% 0.87 (0.75-1.00) 0.0528
Secondary endpoint 3-y RFS 65.5% 61.9% 0.86 (0.74-0.99) 0.0407 3-y OS 81.3% 77.6% 0.84 (0.69-1.01) 0.0706
LV=leucovorin, HR=hazard ratio, CI=confidence interval, DFS=disease-free survival, RFS=relapse-free survival, OS=overall survival
SOURCE: Cassidy J et al. Presentation. ASCO 2004;Abstract 3509.

1 3
Based on response rates approaching 45 to 50 percent with CAPOX and CAPIRI, (Cassidy 2004; Bajetta 2004) I believe they are reasonable options. The TREE study compares CAPOX to FOLFOX and a bolus schedule of 5-FU/leucovorin/oxali-platin. Although the study isn’t powered to evaluate efficacy, we can determine the relative tolerability of CAPOX. Similarly, the BIG-C study, in its first iteration, compared CAPIRI to FOLFIRI and a modified version of IFL.
I prefer infusional 5-FU because it’s more tried and true. I discuss capecitabine, particularly with patients who are really uncomfortable with a port or for whom confounding factors prevent the use of a port. Then, we talk about CAPOX or CAPIRI as options that aren’t as well studied as the more standard infusional 5-FU approaches. I’ve certainly used CAPOX and CAPIRI as palliative treatment. Another issue is the lack of data for the addition of bevacizumab to these capecitabine-containing regimens.
Select publicationsBosset JF et al. Does the addition of chemotherapy (CT) to preoperative radiotherapy (preopRT) increase the pathological response in patients with resected rectal cancer: Report of the 22921 EORTC phase III trial. J Clin Oncol 2004;22 (14 Suppl);Abstract 3504.
Cassidy J et al. Capecitabine (X) vs bolus 5-FU/leucovorin (LV) as adjuvant therapy for colon cancer (the X-ACT study): Efficacy results of a phase III trial. J Clin Oncol 2004;22(14 Suppl);Abstract 3509.
Cassidy J et al. XELOX (capecitabine plus oxaliplatin): Active first-line therapy for patients with metastatic colorectal cancer. J Clin Oncol 2004;22(11):2084-91. Abstract
de Gramont A et al. Randomized trial comparing monthly low-dose leucovorin and fluorouracil bolus with bimonthly high-dose leucovorin and fluorouracil bolus plus continuous infusion for advanced colorectal cancer: A French Intergroup study. J Clin Oncol 1997;15(2):808-15. Abstract
Hoff PM et al. Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: Results of a randomized phase III study. J Clin Oncol 2001;19(8):2282-92. Abstract
Kabbinavar FF et al. Bevacizumab (a monoclonal antibody to vascular endothelial growth factor) to prolong progression-free survival in first-line colorectal cancer (CRC) in subjects who are not suitable candidates for first-line CPT-11. J Clin Oncol 2004;22(14 Suppl);Abstract 3516.
Lee CG et al. Anti-vascular endothelial growth factor treatment augments tumor radiation response under normoxic or hypoxic conditions. Cancer Res 2000;60(19):5565-70. Abstract
Roh MS et al. Response to preoperative multimodality therapy predicts survival in patients with carcinoma of the rectum. J Clin Oncol 2004;22(14 Suppl);Abstract 3505.
Saltz L et al. Irinotecan plus fluorouracil/leucovorin (IFL) versus fluorouracil/leucovorin alone (FL) in stage III colon cancer (intergroup trial CALGB C89803). J Clin Oncol 2004;22(14 Suppl);Abstract 3500.
Sauer R. Adjuvant Versus Neoadjuvant Combined Modality Treatment for Locally Advanced Rectal Cancer: First Results of the German Rectal Cancer Study (CAO/ARO/AIO-94). Int J Radiat Oncol Biol Phys 2003;57(2 Suppl):124;Abstract 2.
Van Cutsem E et al. Oral capecitabine vs intravenous 5-fluorouracil and leucovorin: Integrated efficacy data and novel analyses from two large, randomised, phase III trials. Br J Cancer 2004;90(6):1190-7. Abstract
Willett CG et al. Direct evidence that the VEGF-specific antibody bevacizumab has antivascular effects in human rectal cancer. Nat Med 2004;10(2):145-7. Abstract
Wolmark N et al. A phase III trial comparing oral UFT to FULV in stage II and III carcinoma of the colon: Results of NSABP Protocol C-06. J Clin Oncol 2004;22(14 Suppl);Abstract 3508.
1 3

1 4
E D I T E D C O M M E N T S
1 4
Peter C Enzinger, MD
Monotherapy with targeted biologic agents Initially, cetuximab alone was not expected to achieve major responses. Additionally, preclinical data demonstrated that cetuximab was synergistic with irinotecan, which led to the initial trial by Len Saltz that was presented at ASCO 2001.
In that trial, cetuximab in combination with irinotecan demonstrated a 22.5 percent response rate in patients with irinotecan-refractory disease. We participated in a subse-quent trial, also led by Len Saltz, demon-strating that cetuximab alone had quite promising activity (Saltz 2001, 2002).
I believe monotherapy with cetuximab and other targeted biologic agents has significant activity in about 10 percent of patients. In the trial by Kabbinavar et al, published in the Journal of Clinical Oncology in 2003, bevacizumab alone had a nine percent response rate in patients with 5-FU-refractory disease (Kabbinavar 2003). It’s noteworthy that a small percentage of patients have dramatic responses to monotherapy with targeted biologic agents.
Skin rashes associated with targeted biologic agentsThe severe acne flares associated with cetuximab may, in part, be due to the loading dose that was initially proposed. In the early trials, patients were treated with a 400 mg/m2 loading dose followed by 250 mg/m2 weekly. The idea was to saturate the receptors but, in retrospect, I’m not sure that was wise.
When these patients stopped cetuximab and restarted at the standard weekly dose, the rashes didn’t occur to the same extent. I believe we’re now moving toward a standard starting dose of 250 mg/m2 and not using loading doses, which may be reducing the incidence of the severe acneform rashes.
The rash associated with cetuximab is phenotypically the same as the rash associated with the tyrosine kinase inhibitors; however, it’s not clear whether these agents cause the rash in the same way. Both types of rashes involve the chest, neck, face, scalp and upper back. These rashes are important indicators of response in patients with colorectal cancer. Many of our patients are pleased
Dr Enzinger is an Instructor in Medicine at Harvard Medical School and Clinical Director of the Gastrointestinal Cancer Center at the Dana-Farber Cancer Institute in Boston, Massachusetts.
when they first have these rashes because they know that patients who develop the rashes have a better chance of responding to these agents.
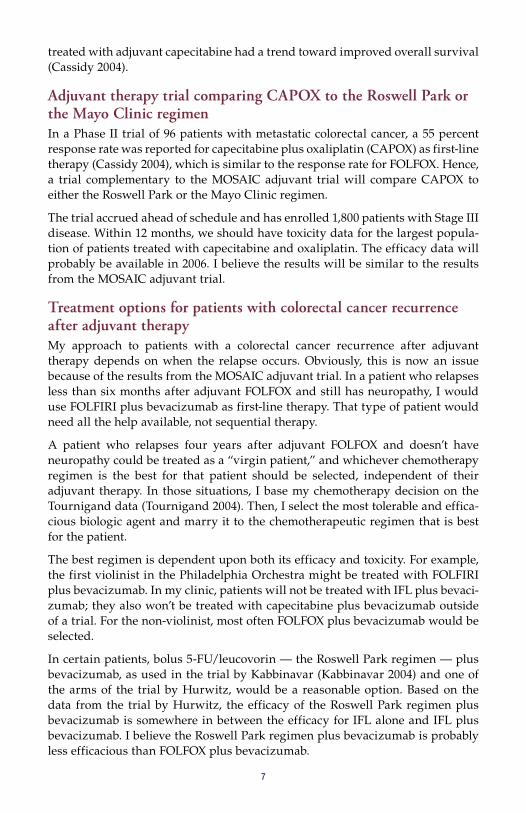
Phase III randomized trial evaluating bevacizumab plus IFL The results from the trial of bevacizumab plus IFL were quite impressive, and they caught many by surprise. Few believed that we would see such dramatic improvements in the response rate, progression-free survival and overall survival. Based on the number of patients enrolled in the trial — more than 400 in each arm — the results are solid and real (Hurwitz 2004). Benefits are clearly evident from the addition of bevacizumab to the IFL regimen (3.1).
It will be interesting to determine whether an interaction between bevacizumab and IFL is responsible for the dramatic results or whether similar results will occur when bevacizumab is combined with other chemotherapeutic agents. We’re waiting for the results from the bevacizumab plus FOLFOX trial. If the interaction is between bevacizumab and 5-FU, then we should obtain similar results with FOLFOX.
The response for any chemotherapeutic regimen can typically be increased, but usually at a cost. The toxicity profile of the targeted biologic agents is very different from that of standard chemotherapy; therefore, the two may be combined. With bevacizumab, we are seeing hypertension that is easily managed.
The occurrence of bowel perforations needs to be investigated to determine whether it’s a problem with the VEGF inhibitors, angiogenesis inhibitors or just bevacizumab. For the most part, the perforations were not life threatening and did not necessarily occur at the site of the tumor. Since the incidence of bowel perforation is so low, I don’t believe it will impact our use of this agent, but it’s certainly an area of interest.
Capecitabine in the management of patients with metastatic diseaseIn patients with metastatic disease, capecitabine can certainly be substituted for 5-FU in either the FOLFIRI or FOLFOX regimens. I have patients who fly in to see me, and the every three-week schedule used with capecitabine in the CAPOX
1 5
3.1 Efficacy Results from a Phase III Trial of Bevacizumab (BV) in Combination with Bolus Irinotecan, 5-Fluorouracil and Leucovorin (IFL) as First-Line Therapy in Patients with Metastatic Colorectal Cancer
IFL/placebo (n=411) IFL/BV (n=402) p-value
Median survival (mo) 15.6 20.3 <0.001
Progression-free survival (mo) 6.2 10.6 <0.001
Objective response rate 35% 45% 0.004
Duration of response (mo) 7.1 10.4 0.001
SOURCE: Hurwitz H et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350(23):2335-42. Abstract
1 6
and CAPIRI regimens is certainly more convenient, whereas both the FOLFIRI and FOLFOX regimens are administered on an every two-week schedule.
I’m impressed with the publication by Scheithauer in the Journal of Clinical Oncology in which a higher dose of capecitabine was administered for seven days with oxaliplatin. In that trial, the shorter every two-week schedule appeared to have better efficacy and similar toxicity compared to the every three-week schedule (Scheithauer 2003).
In my experience, oxaliplatin 130 mg/m2 every three weeks may not be as well tolerated as 85 mg/m2 every two weeks. I have noted more fatigue and diarrhea with higher doses of oxaliplatin administered less frequently. I also like to create more frequent synergy between oxaliplatin and either infusional 5-FU or capecitabine.
Because this is palliative therapy, capecitabine may be beneficial for patients who are uncomfortable with a portacath or those who would like a longer every three-week schedule. In my practice, I use 5-FU and capecitabine interchangeably. When a patient wants to know which is the most proven therapy, I explain that FOLFOX and FOLFIRI have more confirmed data because of the Phase III trials; however, for savvy patients who are willing to take a bit of a risk and would like the added convenience of capecitabine, I believe either CAPIRI or CAPOX are very viable alternatives.
Choosing between irinotecan- or oxaliplatin-containing regimensWhen deciding between irinotecan- or oxaliplatin-containing regimens, the primary question in my mind is the patient’s liver function. In patients with compromised liver function, particularly an elevated bilirubin, I steer away from irinotecan.
Oxaliplatin should be used as first-line therapy in any patient with a bilirubin greater than 2 mg/dL. Oxaliplatin up front can downsize the tumor. Then, when the patient’s disease progresses or the patient must discontinue oxaliplatin because of toxicity, their liver function is typically improved and irinotecan may be used as second-line therapy.
A gray area exists for patients who do not have an elevated bilirubin but have significant elevations in ALT or AST, or for patients with a small increase in their prothrombin time (PT), or in whom a large part of the liver has been replaced by tumor. Again, an agent that is not metabolized in the liver may be better initially for those types of patients.
A year ago, I was concerned about the use of oxaliplatin in patients with compro-mised renal function. Fortunately, in the interim, data have been presented and published suggesting that patients with compromised renal function seem to do well with oxaliplatin.
However, data for patients with the worst renal function is scanty (Takimoto 2003). Another factor I consider when choosing between irinotecan and oxaliplatin is the patient’s need to use their hands (ie, typists, virtuosos and craftsmen).

1 7
In those patients, I would shy away from oxaliplatin up front, especially since many patients may now have the ability to work part-time. On the other hand, oxaliplatin may be better for the patient with an ostomy who already has diarrhea. Although oxaliplatin plus infusional 5-FU can cause diarrhea, the incidence is less than with irinotecan and infusional 5-FU.
Role of fluoropyrimidine monotherapyIn a compromised patient — one with a borderline performance status — I would certainly use capecitabine or 5-FU as monotherapy. In patients presenting very late with the disease who have barely squeaked through a palliative surgery and are having difficulty in coming back to a performance status of two, I would consider initiating therapy with capecitabine or weekly bolus 5-FU.
Until recently, I would have used capecitabine or 5-FU alone in a patient with an elevated bilirubin. Fortunately, we can now use oxaliplatin in these patients. Even with dramatically attenuated doses, the combination of oxaliplatin and 5-FU would be preferable to full doses of 5-FU alone. I believe synergy occurs with the combination.
Select publicationsCunningham D et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 2004;351(4):337-45. Abstract
Hurwitz H et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350(23):2335-42. Abstract
Kabbinavar F et al. Phase II, randomized trial comparing bevacizumab plus fluorouracil(FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003;21(1):60-5. Abstract
Saltz L et al. Cetuximab (IMC-C225) plus irinotecan (CPT-11) is active in CPT-11-refractory colorectal cancer (CRC) that expresses epidermal growth factor receptor (EGFR). Proc ASCO 2001;Abstract 7.
Saltz L et al. Single agent IMC-C225 (Erbitux™) has activity in CPT-11-refractory colorectal cancer (CRC) that expresses the epidermal growth factor receptor (EGFR). Proc ASCO 2002;Abstract 504.
Saltz LB et al. Irinotecan plus fluorouracil/leucovorin (IFL) versus fluorouracil/leucovorin alone (FL) in stage III colon cancer (Intergroup trial CALGB C89803). J Clin Oncol 2004;22(14 Suppl);Abstract 3500.
Scheithauer W et al. Randomized multicenter phase II trial of two different schedules of capecitabine plus oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol 2003;21(7):1307-12. Abstract
Takimoto CH et al; National Cancer Institute Organ Dysfunction Working Group Study. Dose-escalating and pharmacological study of oxaliplatin in adult cancer patients with impaired renal function: A National Cancer Institute Organ Dysfunction Working Group Study. J Clin Oncol 2003;21(14):2664-72. Abstract

1 8
Post-test:
Q U E S T I O N S ( P L E A S E C I R C L E A N S W E R ) :
Colorectal Cancer Update — Issue 6, 2004
1. In the MOSAIC adjuvant trial, the addition of oxaliplatin resulted in:
a. A 23 percent overall reduction in the risk of relapse
b. A significant increase in overall survivalc. Both a and bd. None of the above
2. The X-ACT adjuvant trial demonstrated equivalency between the Mayo Clinic regimen and:
a. FOLFOX4b. Capecitabinec. FOLFIRId. All of the abovee. None of the above
3. According to ECOG-E3200, bevacizumab is being studied in combination with irinotecan.
a. Trueb. False
4. Which of the following trials provide evidence to support preoperative chemoradiation therapy in patients with rectal cancer?
a. EORTC-2291b. NSABP-R-03c. The German Rectal Cancer (CAO/ARO/
AIO-94) triald. All of the abovee. None of the above
5. NSABP-C-06 confirmed the results from the X-ACT trial, demonstrating that adjuvant therapy with capecitabine was comparable to infusional 5-FU/leucovorin.
a. Trueb. False
6. Which of the following trials evaluated adjuvant IFL in patients with Stage III colorectal cancer?
a. PETACC-3b. BIG-Cc. CALGB-89803d. Both a and ce. None of the above
7. Bevacizumab has been shown to offer a benefit when added to:
a. IFLb. 5-FU/leucovorinc. FOLFOXd. Both a and be. Both a and c
8. In patients with irinotecan-refractory disease, ___________ has demonstrated a 22.5 percent response rate.
a. Cetuximab monotherapy b. Cetuximab in combination with irinotecanc. Both of the aboved. None of the above
9. In patients with metastatic disease, bevacizumab plus IFL has been found to improve ____________________ compared to IFL alone.
a. The response rateb. The progression-free survivalc. The overall survivald. Both a and be. All of the above
10. In a trial by Scheithauer, capecitabine plus oxaliplatin administered in a shorter every two-week schedule appeared to have better efficacy and similar toxicity compared to an every three-week schedule.
a. Trueb. False
11. Recently published data indicate that oxali-platin can be safely administered to patients with impaired renal function.
a. Trueb. False
12. In the Phase II randomized trial by Kabbinavar, comparing bevacizumab plus FU/LV with FU/LV alone in patients with metastatic colorectal cancer, the response rate with bevacizumab alone in patients with 5FU-refractory disease was 9%.
a. Trueb. False
Post-test Answer Key: 1a, 2b, 3b, 4d, 5b, 6d, 7d, 8b, 9e, 10a, 11a, 12a

1 9
Evaluation Form:
5 = 4 = 3 = 2 = 1 = N/A = Outstanding Good Satisfactory Fair Poor not applicable to this issue of CCU
Research To Practice respects and appreciates your opinions. To assist us in evaluating the effectiveness of this activity and to make recommendations for future educational offerings, please complete this evaluation form. A certificate of completion is issued upon receipt of your completed evaluation form.
Please answer the following questions by circling the appropriate rating:
To what extent does this issue of CCU address the following global learning objectives?
• Critically evaluate the clinical implications of emerging clinical trial data in colorectal cancer treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
• Counsel patients about the risks and benefits of adjuvant and neoadjuvant chemotherapy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
• Develop and explain a management strategy for patients with metastatic colorectal cancer. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
• Describe ongoing clinical trials in colorectal cancer and counsel patients about the availability of ongoing clinical trials.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
G L O B A L L E A R N I N G O B J E C T I V E S
Daniel G Haller, MD 5 4 3 2 1 5 4 3 2 1
Charles S Fuchs, MD, MPH 5 4 3 2 1 5 4 3 2 1
Peter C Enzinger, MD 5 4 3 2 1 5 4 3 2 1
E F F E C T I V E N E S S O F T H E I N D I V I D U A L F A C U L T Y M E M B E R S
Faculty Knowledge of Subject Matter Effectiveness as an Educator
Colorectal Cancer Update — Issue 6, 2004
1 9
5 = 4 = 3 = 2 = 1 = N/A = Outstanding Good Satisfactory Fair Poor not applicable to this issue of CCU
O V E R A L L E F F E C T I V E N E S S O F T H E A C T I V I T Y
Objectives were related to overall purpose/goal(s) of activity . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Related to my practice needs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Will influence how I practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Will help me improve patient care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Stimulated my intellectual curiosity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Overall quality of material . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Overall, the activity met my expectations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Avoided commercial bias or influence. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 4 3 2 1 N/A
Please answer the following questions by circling the appropriate rating:
2 0
Evaluation Form:
R E Q U E S T F O R C R E D I T — please print clearly
Name: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Specialty: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ME No.:. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Last 4 Digits of SSN (required): . . . . . . . . . . . . . . . . . . . . . . . . . . .
Street Address: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Box/Suite: . . . . . . . . . . . . . . . . . . . . . . . .
City, State, Zip: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Telephone: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Fax: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Email: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
I certify my actual time spent to complete this educational activity to be ____________ hour(s).
Signature: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Date: . . . . . . . . . . . . . . . . . . . . . . . . . .
Will the information presented cause you to make any changes in your practice?
5 Yes 5 No
If yes, please describe any change(s) you plan to make in your practice as a result of this activity:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
What other topics would you like to see addressed in future educational programs?
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
What other faculty would you like to hear interviewed in future educational programs?
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Degree:
5 MD 5 PharmD 5 NP 5 BS 5 DO 5 RN 5 PA 5 Other . . . . . . . . . . . . .
F O L L O W - U P
As part of our ongoing, continuous, quality-improvement effort, we conduct post-activity follow-up surveys to assess the impact of our educational interventions on professional practice. Please indicate your willingness to participate in such a survey:
5 Yes, I would be willing to participate 5 No, I’m not willing to participate in a follow-up survey. in a follow-up survey.
Additional comments about this activity:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Research To Practice designates this educational activity for a maximum of 3 category 1 credits toward the AMA Physician’s Recognition Award. Each physician should claim only those credits that he/she actually spent in the activity.
Colorectal Cancer Update — Issue 6, 2004
To obtain a certificate of completion and receive credit for this activity, please complete the Post-test, fill out the Evaluation Form and mail or fax both to: Research To Practice, One Biscayne Tower, 2 South Biscayne Boulevard, Suite 3600, Miami, FL 33131, FAX 305-377-9998. You may also complete the Post-test and Evaluation online at www.ColorectalCancerUpdate.com/CME.


Related Documents











