T Staging: Rectal cancer T1 invades submucosa T2 invades muscularis propria T3 invades subserosa or perirectal tissues T4 invades peritoneum, organs or structure (15% of cases)

T Staging: Rectal cancer
Jan 14, 2016
T1 invades submucosa. T2 invades muscularis propria. T3 invades subserosa or perirectal tissues. T4 invades peritoneum, organs or structures (15% of cases). T Staging: Rectal cancer. T4: Female. T4: Rectal cancer. Prostatic Involvement. T4: Male. Anterior T4 Rectal cancer. APR - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

T Staging: Rectal cancer
T1 invades submucosa
T2 invades muscularis propria
T3 invades subserosa or perirectal tissues
T4 invades peritoneum, organs or structures(15% of cases)

T4: Female

T4: Rectal cancer




Prostatic Involvement

T4: Male


Anterior T4 Rectal cancer
APR +
Radical prostatectomy

APR + Radical Prostate

T4: Posterior Rectal cancer

T4 Strategy: Staging
EUA, cystoscopy
MR pelvis
CT abdo, thorax
? PET scan

T4 Strategy: Adjuvant therapy
RTH
Chemo/RTH
Intra op RTH
HIPEC: Hyperthermic Intra Peritoneal CT

Pre-operative RTH plays a major role
Only a minority will be cured with RTH alone
Pre-operative CRTH has increased risks
Phase II studies oxaliplatin, irinotecan and
capecitabine
What do we do with complete regression?
Adjuvant Rx for fixed tumours

Current optimum CRT schedule
Radiotherapy with 3 or 4 field plan
45 Gy in 25 # over 5 weeks
Capecitabine 825mg/m2 bd for 5 weeks

Stomas
Stenting
Nephrostomies
T4 Strategy: Pre-emptive surgery

T4 Strategy: Definitive surgery
Engage the team
Stent the ureters
En bloc resection
? IP Chemotherapy (peritoneal reflection)

Total Pelvic Clearance
Christie NHST 2001 -2005
MDT Assessment Consecutive patients 100
Total Pelvic Clearance 45
Unsuitable for surgery 55

TPC: Surgical candidates
Nutrition
Renal function
Liver function
? Disease confined to pelvis

Outcome of radical surgery
Primary v recurrent disease
Munro v mountain
30 - 80% 5y survival
Lenhert et al 2002, Sanfilippo et al 2001, Law et al 2000

Total Pelvic Clearance
n mortality morbidity% %
Adachi et al 1999 9 0% 44%
Kakuda et al 2003 22 5% 68%
Jimenez et al 2003 55 5.5% 40+%
Nakafusa et al 2004 53 0% 49%
Sharma et al 2005 48 4.2% 75%
Sagar et al 2005 18 1.6% na
Christie 2006 45 0% 11% op
38% non op

Christie: Total Pelvic Clearance
Operative
Stoma Revision 2Perineal wound 2SBO 1
Complications
Non operative
Infections 12PE/DVT 1/1Bleeding 1MI 1CVA 1

Christie: Total Pelvic Clearance
0
2
4
6
8
10
12
14
16
<40 40-50 50-60 60-70 >70
Age
Number

T4 Tumours: HIPEC
Peritoneal involvement
Complete excision
Intraperitoneal mitomycin C
3 bolus over 90min @ 41-
43°C

Peritoneal metastasis

T4 : Palliative therapies
CRT
Pain relief
Tumour ablation
Tumour resection
Drainage of sepsis
Stenting and stomas

Survival: Cyto + HIPEC
0
20
40
60
2y 3y 5y
CRC
PSM



T Staging: Rectal cancer
T4 Male
Invading adjacent organs

T4: Rectal cancer


Anterior T4 rectal tumour
APR + Radical Prostate


Survival: Cytoreduction + HIPEC
CRC Peritoneal v liver resections
CRC complete
CRC incomplete

T4 : Palliative therapies
CRT
Pain relief
Tumour ablation
Tumour resection
Drainage of sepsis
Stenting and stomas

What of it! She would have died anyway without the operation.
There you are gentleman,you’ve seen the operation that everyone said was impossible, performed with complete success.
But Doctor, the patient’s dead!
T4: Palliative surgery

Survival: Cyto + HIPEC
0
20
40
60
2y 3y 5y
CRC
PSM
Liverresection

Total Pelvic Clearance

Peritoneal carcinomatosis
Sugarbaker

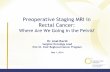
Survival with Colorectal Liver MetastasesSurvival with Colorectal Liver Metastases
0
20
40
60
80
100
120
0 1 2 3 4 5 6 7 8 9 10
Resected
Not resected
Unresectable%
years Scheele 1993Scheele 1993




Surgical candidates
Nutrition
Renal function
Liver function
Proximal small bowel loops
Disease confined to pelvis, R/LIF +/- omentum

T4 adjuvant IORT
Fixed / inoperable tumours
RTH + resection N = 248
Local recurrence free survival 11%
RTH + resection + IORT N = 78
Local recurrence free survival 2.6%
Sadahiro et al Dis Colon Rectum 2001

RTH for fixed rectal tumours
• 45 - 65% have potentially curable resections after radiotherapy
• 50% develop local recurrence
• Only a minority will be cured with RTH alone
(Martenson et al, in Cancer of the colon, rectum and anus 1995)

Pre-operative CRT
(Videtic et al, 1998)
Small studies n = 7-64
5FU, FA, cisplatin, mmc
RTh 40Gy/20#, 50Gy/30#
Resectability 70 -100%
Pathology T0 4 -72%
DFS 60 -80%

Preoperative RTH + Raltitrexed(tomudex)
ASCO 2003
Fixed / inoperable tumoursChristie and Walsgrave
N = 36 MR T3: 17 T4: 19
Response: 81%Curative resection: 64%Path T0: 14%

T4 Strategy: Pre-emptive surgery
Stenting
Stomas
Nephrostomies

HIPEC

HIPEC

Vaginal vault recurrence

Abdo/pelvis 20-35%
Liver 40-50%
Lung 16%
Brain 8 %
Bone 4-6%
Metastatic disease

Advanced disease
Related Documents