TRAUMATIC DROP FOOT By: Larissa Torres Nixon, SPT Regis University July 16, 2010

T RAUMATIC D ROP F OOT By: Larissa Torres Nixon, SPT Regis University July 16, 2010.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

TRAUMATIC DROP FOOTBy: Larissa Torres Nixon, SPT
Regis University
July 16, 2010

VIDEO
http://www.youtube.com/watch?v=Q8KB2fhLDwM&feature=related

PURPOSE:
Explain the importance of doing a thorough examination on patients with traumatic drop foot and the intervention options physical therapists can offer these patients.

OBJECTIVES:
Student will be able to describe the pathology for a person with traumatic drop foot.
Student will be able to explain information obtained during the examination and evaluation for this patient.
Student will be able to discern a more thorough evaluation process for this patient based on evidentiary support.
Student will be able to develop an intervention strategy using current literature evidence.

PATIENT CONSULTATION: Pt is a 25 y.o. male
active duty Army (ADA)
Dx: Pt is status post multiple reconstruction surgery due to blast injury.
Rx: Please evaluate and treat.

WHAT IS DROP FOOT? Traumatic drop foot is
usually occupation or sport related.7
Caused by chronic compression, traction or transection of the common peroneal or deep peroneal nerve. 7
Injury to the common peroneal nerve results in weakness of all muscles innervated by the superficial and deep branches. 7

TRAUMATIC DROP FOOT: (CONT)
Tibialis anterior muscle is the primary ankle DF.2
Tibialis anterior has the highest activity at heel strike and after toe off during the swing phase. 2
Disruption leads to foot drop.
Common gait deviations include: flatfoot/forefoot contact, decreased push off, and excessive hip and knee flexion with ankle PF.

EXAMINATION: Through patient history Systems Review Special tests
Posture/Gait observation MMT ROM Sensory/proprioceptive testing Scar mobility Outcome measure: LEFS
EMG and NCV studies can be used to determine the degree of nerve damage and potential for nerve recovery. However, are not necessary to diagnose drop foot. 1

SUBJECTIVE HISTORY: Sx: c/o left drop foot, multiple trips/near falls over
the past 3 months. Pain with first few steps after getting up.
Hx: MOS: 11B, was hit by an RPG August 30, 2009 on left lower leg while deployed in Afghanistan. Was MEDDVAC’d to Germany then transferred state side.

SUBJECTIVE HISTORY: (CONT)
He had a series of 10 limb salvation surgeries from September to November 2009, including an external fixator placed at Walter Reed Army Medical Center.
SUBJECTIVE HISTORY: (CONT)
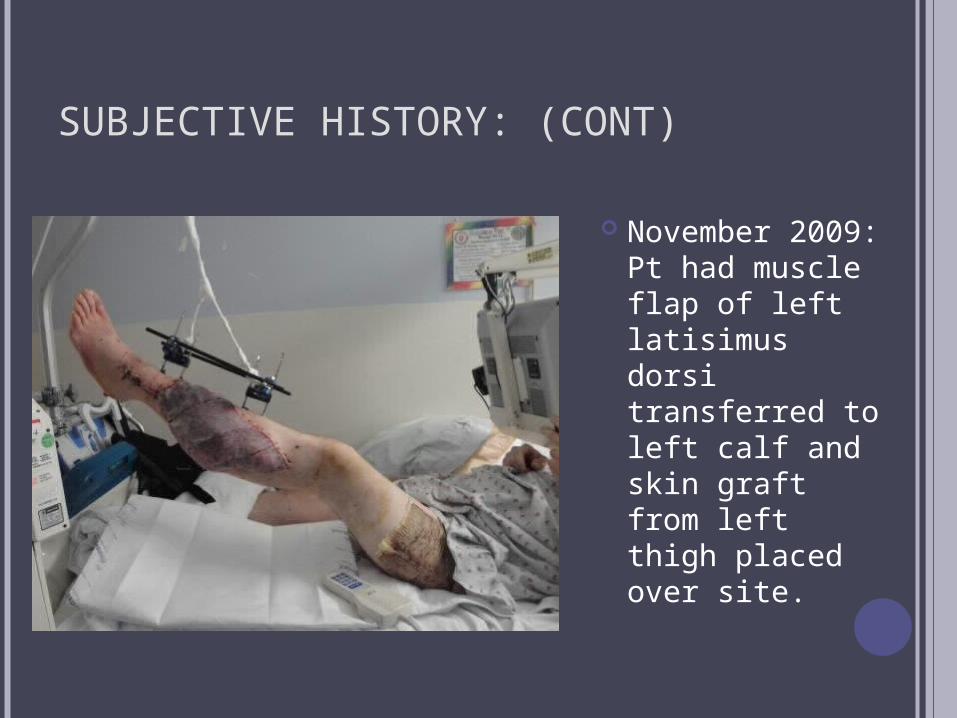
November 2009: Pt had muscle flap of left latisimus dorsi transferred to left calf and skin graft from left thigh placed over site.
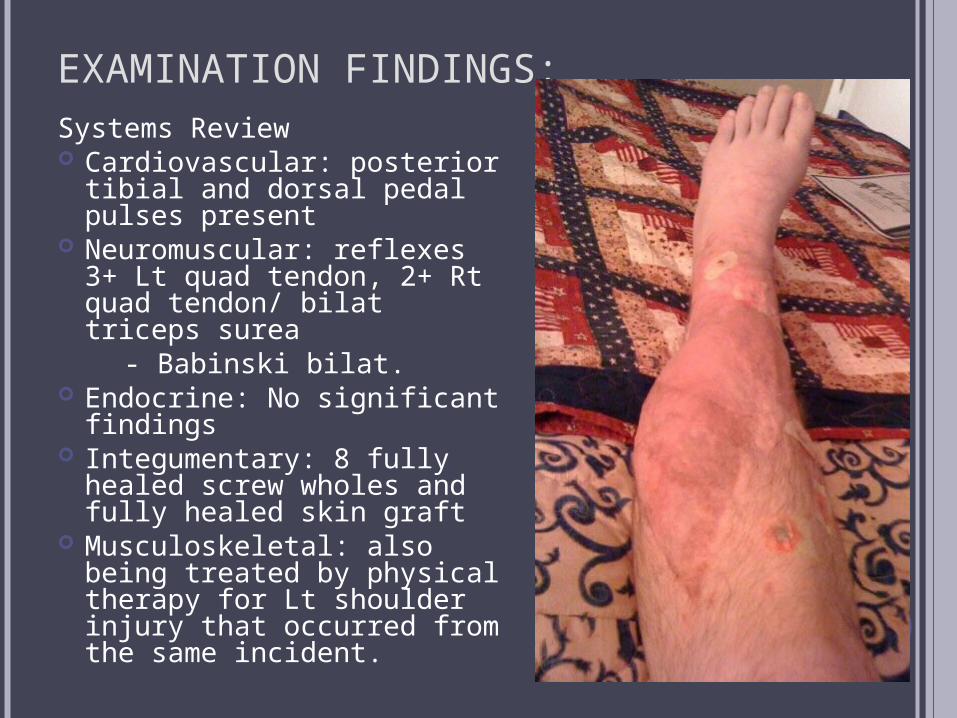
EXAMINATION FINDINGS:Systems Review Cardiovascular: posterior
tibial and dorsal pedal pulses present
Neuromuscular: reflexes 3+ Lt quad tendon, 2+ Rt quad tendon/ bilat triceps surea
- Babinski bilat. Endocrine: No significant
findings Integumentary: 8 fully
healed screw wholes and fully healed skin graft
Musculoskeletal: also being treated by physical therapy for Lt shoulder injury that occurred from the same incident.

EXAMINATION FINDINGS: (CONT) Posture observation
Assymetirical WBing to Rt LE
Excessive ER of Lt LE Gait Observation
Forefoot contact at heel strike
Excessive knee/hip flexion with swing phase
Toe drop on Lt throughout swing phase
Decreased stance time on Lt
MMT Rt LE: 5/5 throughout Lt hip flex: 5/5 Lt knee flex: 5/5 Lt knee ext: 4+/5 Lt ankle DF: 0/5 Lt ankle PF: 1/5 Lt ankle Inv: 1/5 Lt ankle Ever: 0/5 Great toe Ext: 0/5 Minimal ability to
wiggle toes noted.

EXAMINATION FINDINGS: (CONT) PROM
Rt Ankle: 0 ̊ DF to 70 ̊ PF Lt Ankle: 10 ̊ PF to 35 ̊ PF
Sensory/proprioceptive testing Light tough: diminished L4, L5, S2 on Lt 10/10 monofilament test on plantar surface of foot Balance: 30 seconds with EC on Rt, 7 seconds with
eyes open on Lt Proprioception: 4/10 correct on Lt ankle
Scar mobility Poor scar mobility of 8 pin holes and lateral ankle
incision. Outcome measure: LEFS
38/80 (where 80/80 means no disability) 4
MCID is 9 points
EXAMINATION FINDINGS:
NCV: Diminished NCV of Lt tibial nerve (35 ms),
absent on Lt peroneal nerve EMG:
Intact Lt femoral nerve, sciatic nerve Diminished activity of the Lt tibial nerve with
maximum contaction No activity of Lt common peroneal nerve and it’s
branches.
DIAGNOSIS & PROGNOSIS:
Diagnosis: Left drop foot with complete neural loss of
the common peroneal nerve and it’s branches.
Prognosis: Poor If there are no signs for nerve recovery with
EMG after 6 months then there will likely be no recovery of function.3

INTERVENTIONS & EVIDENCE:
For a patient with complete loss of muscle innervation 2,7
Maintain ankle ROMPrevent PF contractureAddress gait impairments with AFO
Long term treatments may include 2,7 Talocrural and subtalar joint fusionPosterior tibialis tendon transfer
No appropriate for this patientBKA

ORTHOSES: DOES EVIDENCE MATCH MY PATIENT?
Eberly et al. 6

ORTHOSES: DOES EVIDENCE MATCH MY PATIENT?
Patients with common peroneal nerve palsey require a more solid, rigid AFO than those with only deep peroneal nerve palsey. 8
He is still waiting to receive his AFO.

TAKE AWAY:
These returning injured soldiers will be PT patients both acutely and later in our careers.
If you have a patient with a traumatic injury always ask if the patient has pictures from the initial injury or just prior to surgery.
EMG and NCV studies done in the physical therapy clinic can provide helpful information for diagnosis and prognosis of a patients injury.
CHECK FOR UNDERSTANDING:
What are the causes of traumatic foot drop?
Which nerve(s) cause foot drop when they are damaged?
What are 2 physical therapy interventions for a patient with traumatic foot drop?

REFERENCES: Images: Photos provided by the featured patient Family practice notebook.com
http://www.fpnotebook.com/_media/AnkleAnatomyMuscleAP.gif Twin Oaks Orthotics & Prosthetics: http://www.bing.com/images/search?
q=AFO&FORM=BIFD#focal=57a9fe3e43ec50b4ffe5eef02bec67e6&furl=http%3A%2F%2Fwww.twincityop.com%2Fsitebuildercontent%2Fsitebuilderpictures%2FAFO_Family.jpg
Articles:1. Aminoff M. Electrophysiologic testing for the diagnosis of peripheral nerve injuries.
Anesthesiology [serial online]. May 2004;100(5):1298-1303.2. Baima J, Krivickas L. Evaluation and treatment of peroneal neuropathy. Current
Reviews In Musculoskeletal Medicine [serial online]. June 2008;1(2):147-153.3. Berry H, Richardson P. Common peroneal nerve palsy: a clinical and
electrophysiological review. Journal Of Neurology, Neurosurgery, And Psychiatry [serial online]. December 1976;39(12):1162-1171.
4. Binkley J, Stratford P, Lott S, Riddle D. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. Physical Therapy [serial online]. April 1999;79(4):371-383.
5. Chémali K, Tsao B. Electrodiagnostic testing of nerves and muscles: when, why, and how to order. Cleveland Clinic Journal Of Medicine [serial online]. January 2005;72(1):37-48.
6. Eberly V., Kubota K., Weiss W. To brace or not to brace: Making evidence-based decisions with our clients with neurologic impairments. Paper presented at: Combined Sections Meeting of the American Physical Therapy Association; February 1-5, 2006; San Diego, CA.
7. Elman L, McCluskey L. Occupational and sport related traumatic neuropathy. The Neurologist [serial online]. March 2004;10(2):82-96.
8. Geboers J, Drost M, Spaans F, Kuipers H, Seelen H. Immediate and long-term effects of ankle-foot orthosis on muscle activity during walking: a randomized study of patients with unilateral foot drop. Archives of Physical Medicine & Rehabilitation [serial online]. February 2002;83(2):240-245.

Related Documents











