Circulation Journal Vol.80, July 2016 Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp prognostic value of CAC in CKD, however, has not been established. Considering the prognostic importance of CAD in CKD and the insufficient diagnostic accuracy of the available tests, there is a need for better risk stratification of CKD patients in terms of CAD. 8 Editorial p 1537 To help identify the specific population at need for screen- ing tests, several biomarkers have been suggested for better risk stratification and cardiovascular outcome prediction. In oronary artery disease (CAD) is one of the leading causes of death in patients with chronic kidney dis- ease (CKD), and the cardiovascular risk in CKD patients is similar to or even higher than in those with diabetes or established CAD. 1,2 Therefore, the presence of CKD is considered as a coronary disease equivalent, and early detec- tion of CAD is a major concern in the management of CKD patients. 3 The higher risk of cardiovascular events in CKD patients has been explained by the presence of accelerated coronary artery calcification (CAC), and previous studies have shown that CKD patients have more advanced CAC. 4–7 The C Received November 19, 2015; revised manuscript received April 18, 2016; accepted May 1, 2016; released online June 2, 2016 Time for primary review: 21 days Department of Internal Medicine, Seoul National University College of Medicine, Seoul (I.-C.H., H.E.P., H.-L.K., H.M.K., J.-B.P., Y.E.Y., S.-P.L., H.-K.K., G.-Y.C., D.-W.S., Y.-J.K.); Cardiovascular Center (I.-C.H., H.M.K., J.-B.P., S.-P.L., H.-K.K., D.-W.S., Y.-J.K.), Healthcare System Gangnam Center (H.E.P.), Seoul National University Hospital, Seoul; Division of Cardiology, Department of Internal Medicine, Seoul National University Boramae Medical Center, Seoul (H.-L.K.); and Division of Cardiology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam-si, Gyeonggi-do (Y.E.Y., G.-Y.C.), Korea H.E.P. and Y.J.K. contributed equally to this work as co-corresponding authors. Mailing addresses: Hyo Eun Park, MD, Assistant Professor, Department of Internal Medicine, Seoul National University College of Medicine, Seoul National University Hospital, Healthcare System Gangnam Center, 152 Teheran-ro, Gangnam-gu, Seoul, 135-984, Korea. E-mail: [email protected] and Yong-Jin Kim, MD, PhD, Professor of Internal Medicine, Seoul National University Hospital and Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul, 110-744, Korea. E-mail: kimdamas@ snu.ac.kr ISSN-1346-9843 doi:10.1253/circj.CJ-15-1224 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected] Systemic Inflammation Is Associated With Coronary Artery Calcification and All-Cause Mortality in Chronic Kidney Disease In-Chang Hwang, MD; Hyo Eun Park, MD; Hack-Lyoung Kim, MD; Hyue Mee Kim, MD; Jun-Bean Park, MD; Yeonyee E. Yoon, MD; Seung-Pyo Lee, MD, PhD; Hyung-Kwan Kim, MD, PhD; Goo-Yeong Cho, MD, PhD; Dae-Won Sohn, MD, PhD; Yong-Jin Kim, MD, PhD Background: Presence of systemic inflammation in chronic kidney disease (CKD) is associated with advanced coronary artery calcification (CAC). The prognostic significance of this association, however, is unknown. We evaluated the associations between CAC, estimated glomerular filtration rate (eGFR) and all-cause mortality, to determine whether the associations differ according to the presence of systemic inflammation. Methods and Results: We followed 30,703 consecutive individuals who underwent CAC measurement for a median of 79 months (IQR, 65–96 months). Patients were categorized according to baseline CAC score (0, 1–99, 100–399 and ≥400), eGFR (<45, 45–59, 60–74, 75–89, 90–104, and ≥105 ml/min/1.73 m 2 ) and high-sensitivity C-reactive protein (hsCRP; <2.0, and ≥2.0 mg/L). Prevalence and extent of CAC were greater in those with lower eGFR and higher hsCRP accordingly, even after adjustment. Lower eGFR was strongly associated with higher CAC score (≥400), and the association was more significant in patients with higher hsCRP. The greater CAC burden was associated with worse outcome in the CKD patients (eGFR <60 ml/min/1.73 m 2 ) only in those with higher hsCRP. Conclusions: Patients with low eGFR and more extensive CAC had greater risk of mortality, and associations dif- fered according to the presence of systemic inflammation. Among the CKD patients, coronary evaluation may be considered for those with elevated hsCRP. (Circ J 2016; 80: 1644 – 1652) Key Words: C-reactive protein; Chronic kidney disease; Coronary calcification; Inflammation ORIGINAL ARTICLE Renal Disease

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Circulation Journal Vol.80, July 2016
1644 HWANG IC et al.Circulation JournalOfficial Journal of the Japanese Circulation Societyhttp://www.j-circ.or.jp
prognostic value of CAC in CKD, however, has not been established. Considering the prognostic importance of CAD in CKD and the insufficient diagnostic accuracy of the available tests, there is a need for better risk stratification of CKD patients in terms of CAD.8
Editorial p 1537
To help identify the specific population at need for screen-ing tests, several biomarkers have been suggested for better risk stratification and cardiovascular outcome prediction. In
oronary artery disease (CAD) is one of the leading causes of death in patients with chronic kidney dis-ease (CKD), and the cardiovascular risk in CKD
patients is similar to or even higher than in those with diabetes or established CAD.1,2 Therefore, the presence of CKD is considered as a coronary disease equivalent, and early detec-tion of CAD is a major concern in the management of CKD patients.3 The higher risk of cardiovascular events in CKD patients has been explained by the presence of accelerated coronary artery calcification (CAC), and previous studies have shown that CKD patients have more advanced CAC.4–7 The
C
Received November 19, 2015; revised manuscript received April 18, 2016; accepted May 1, 2016; released online June 2, 2016 Time for primary review: 21 days
Department of Internal Medicine, Seoul National University College of Medicine, Seoul (I.-C.H., H.E.P., H.-L.K., H.M.K., J.-B.P., Y.E.Y., S.-P.L., H.-K.K., G.-Y.C., D.-W.S., Y.-J.K.); Cardiovascular Center (I.-C.H., H.M.K., J.-B.P., S.-P.L., H.-K.K., D.-W.S., Y.-J.K.), Healthcare System Gangnam Center (H.E.P.), Seoul National University Hospital, Seoul; Division of Cardiology, Department of Internal Medicine, Seoul National University Boramae Medical Center, Seoul (H.-L.K.); and Division of Cardiology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam-si, Gyeonggi-do (Y.E.Y., G.-Y.C.), Korea
H.E.P. and Y.J.K. contributed equally to this work as co-corresponding authors.Mailing addresses: Hyo Eun Park, MD, Assistant Professor, Department of Internal Medicine, Seoul National University College of
Medicine, Seoul National University Hospital, Healthcare System Gangnam Center, 152 Teheran-ro, Gangnam-gu, Seoul, 135-984, Korea. E-mail: [email protected] and Yong-Jin Kim, MD, PhD, Professor of Internal Medicine, Seoul National University Hospital and Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul, 110-744, Korea. E-mail: [email protected]
ISSN-1346-9843 doi: 10.1253/circj.CJ-15-1224All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Systemic Inflammation Is Associated With Coronary Artery Calcification and All-Cause Mortality
in Chronic Kidney DiseaseIn-Chang Hwang, MD; Hyo Eun Park, MD; Hack-Lyoung Kim, MD; Hyue Mee Kim, MD;
Jun-Bean Park, MD; Yeonyee E. Yoon, MD; Seung-Pyo Lee, MD, PhD; Hyung-Kwan Kim, MD, PhD; Goo-Yeong Cho, MD, PhD; Dae-Won Sohn, MD, PhD; Yong-Jin Kim, MD, PhD
Background: Presence of systemic inflammation in chronic kidney disease (CKD) is associated with advanced coronary artery calcification (CAC). The prognostic significance of this association, however, is unknown. We evaluated the associations between CAC, estimated glomerular filtration rate (eGFR) and all-cause mortality, to determine whether the associations differ according to the presence of systemic inflammation.
Methods and Results: We followed 30,703 consecutive individuals who underwent CAC measurement for a median of 79 months (IQR, 65–96 months). Patients were categorized according to baseline CAC score (0, 1–99, 100–399 and ≥400), eGFR (<45, 45–59, 60–74, 75–89, 90–104, and ≥105 ml/min/1.73 m2) and high-sensitivity C-reactive protein (hsCRP; <2.0, and ≥2.0 mg/L). Prevalence and extent of CAC were greater in those with lower eGFR and higher hsCRP accordingly, even after adjustment. Lower eGFR was strongly associated with higher CAC score (≥400), and the association was more significant in patients with higher hsCRP. The greater CAC burden was associated with worse outcome in the CKD patients (eGFR <60 ml/min/1.73 m2) only in those with higher hsCRP.
Conclusions: Patients with low eGFR and more extensive CAC had greater risk of mortality, and associations dif-fered according to the presence of systemic inflammation. Among the CKD patients, coronary evaluation may be considered for those with elevated hsCRP. (Circ J 2016; 80: 1644 – 1652)
Key Words: C-reactive protein; Chronic kidney disease; Coronary calcification; Inflammation
ORIGINAL ARTICLERenal Disease
Circulation Journal Vol.80, July 2016
1645CKD, CAC, CRP and Mortality
temic inflammation has never been investigated.The aim of this study was therefore to investigate the asso-
ciations between CKD, CAC and all-cause mortality in a large cohort of >30,000 individuals. We also assessed whether the associations of CAC, CKD and mortality would differ accord-ing to the presence of systemic inflammation.
MethodsSubjectsFrom 2007 to 2011, we identified 42,195 consecutive indi-viduals who underwent coronary artery calcium score (CACS)
particular, inflammatory markers have been studied in various populations, as screening tools as well as predictors for cardio-vascular outcome, considering the mechanisms of early ath-erosclerosis.9 Regarding the development and progression of cardiovascular disease in CKD patients, the presence of low-grade systemic inflammation may be one of the main mecha-nisms.10,11 Although several small studies showed an association between CKD, CAC and systemic inflammation,12,13 it has not been investigated in a large population. Moreover, the prog-nostic significance of such associations is largely unknown, and the question of whether the associations between CKD, CAC and mortality differ according to the presence of sys-
Table 1. Baseline Characteristics
Total group (n=30,703)
eGFR (ml/min/1.73 m2)
<45 (n=348)
45–59 (n=2,482)
60–74 (n=9,720)
75–89 (n=10,216)
90–104 (n=6,143)
≥105 (n=1,794)
Age (years) 56.43±10.88 73.22±10.74 68.35±9.61 59.44±9.55 54.87±9.77 52.39±8.57 43.14±6.35
Male sex 18,311 (59.6) 172 (49.4) 1,293 (52.1) 5,968 (61.4) 6,622 (64.8) 3,445 (56.1) 811 (45.2)
HTN 8,687 (28.3) 195 (56.0) 1,228 (49.5) 3,072 (31.6) 2,645 (25.9) 1,327 (21.6) 220 (12.3)
DM 4,778 (15.6) 151 (43.4) 619 (24.9) 1,611 (16.6) 1,430 (14.0) 816 (13.3) 151 (8.4)
Dyslipidemia 3,721 (12.1) 66 (19.0) 439 (17.7) 1,204 (12.4) 1,189 (11.6) 660 (10.7) 163 (9.1)
Current smoker 7,091 (23.1) 71 (20.5) 310 (12.5) 1,808 (18.6) 2,585 (25.3) 1,745 (28.4) 572 (31.9)
Laboratory results
Hemoglobin (g/dl) 14.5 (13.4–15.6)
12.4 (11.0–14.0)
14.1 (13.1–15.2)
14.6 (13.5–15.7)
14.7 (13.5–15.7)
14.5 (13.4–15.6)
14.1 (13.0–15.6)
Fasting blood glucose (mg/dl) 94.0 (86.0–104.0)
104.5 (91.0–126.0)
98.0 (89.0–112.0)
95.0 (87.0–106.0)
93.0 (86.0–104.0)
92.0 (83.0–102.0)
88.0 (81.0–96.0)
Hemoglobin A1c (%) 5.7 (5.4–6.0)
6.1 (5.7–6.9)
5.9 (5.6–6.3)
5.7 (5.5–6.1)
5.7 (5.4–6.0)
5.7 (5.4–5.9)
5.5 (5.3–5.7)
BUN (mg/dl) 67.8 (58.3–77.9)
64.7 (53.7–75.0)
66.1 (57.2–76.5)
68.1 (58.5–78.7)
67.9 (58.4–77.8)
67.9 (58.6–77.6)
68.0 (58.6–78.1)
Creatinine (mg/dl) 1.0 (0.8–1.1)
1.6 (1.3–1.8)
1.2 (1.0–1.3)
1.1 (0.9–1.2)
1.0 (0.8–1.1)
0.8 (0.7–0.9)
0.7 (0.6–0.8)
eGFR (ml/min/1.73 m2)† 78.4 (68.6–90.5)
39.7 (32.9–42.9)
55.8 (52.4–58.2)
68.6 (65.2–72.0)
81.6 (77.9–85.5)
96.4 (93.1–100.3)
108.9 (106.7–112.3)
Total cholesterol (mg/dl) 197.0 (174.0–222.0)
176.0 (140.3–210.0)
197.0 (170.0–223.0)
201.0 (177.0–224.0)
195.0 (173.0–220.0)
196.0 (173.0–221.0)
190.0 (167.0–215.0)
Triglyceride (mg/dl) 106.0 (74.0–156.0)
127.0 (91.8–177.0)
115.0 (83.0–159.0)
109.0 (78.0–158.0)
107.0 (74.0–156.0)
101.0 (68.0–152.0)
87.0 (58.0–139.8)
HDL-C (mg/dl) 51.0 (43.0–60.0)
45.0 (38.0–56.0)
51.0 (43.0–60.0)
51.0 (43.0–60.0)
50.0 (43.0–60.0)
50.0 (43.0–60.0)
53.0 (45.0–63.0)
LDL-C (mg/dl) 113.0 (93.0–135.0)
95.0 (76.0–121.0)
112.0 (91.0–134.0)
115.6 (96.0–136.0)
113.0 (93.0–135.0)
114.0 (94.0–137.0)
110.0 (89.0–131.0)
hsCRP (mg/L) 0.10 (0.10–1.70)
1.90 (0.10–7.30)
0.70 (0.10–2.20)
0.10 (0.10–1.60)
0.20 (0.10–1.60)
0.10 (0.10–1.50)
0.10 (0.10–1.43)
Duration of follow-up (months) 78.9 (65.0–95.9)
79.9 (58.9–98.4)
88.9 (72.8–101.4)
87.7 (72.5–99.9)
81.0 (67.2–96.8)
68.1 (59.7–76.9)
63.2 (58.3–72.7)
All-cause mortality (%) 886 (2.9) 101 (29.0) 225 (9.1) 293 (3.0) 193 (1.9) 59 (1.0) 15 (0.8)
CACS=0 312 (1.5) 19 (22.1) 56 (4.9) 120 (1.9) 79 (1.1) 28 (0.6) 10 (0.6)
CACS 1–99 225 (3.7) 26 (25.7) 64 (9.3) 73 (3.3) 42 (2.1) 17 (1.6) 3 (2.3)
CACS 100–399 157 (6.6) 22 (28.2) 39 (10.2) 50 (5.8) 36 (5.0) 8 (2.5) 2 (6.7)
CACS ≥400 192 (14.4) 34 (41.0) 66 (24.7) 50 (10.8) 36 (9.7) 6 (4.4) 0 (0.0)
Annualized mortality rate (per 100 person-year)
0.44 4.75 1.30 0.43 0.28 0.17 0.15
CACS=0 0.23 3.32 0.67 0.27 0.16 0.10 0.11
CACS 1–99 0.57 4.04 1.35 0.49 0.33 0.29 0.42
CACS 100–399 1.05 4.79 1.52 0.89 0.83 0.45 1.36
CACS ≥400 2.39 7.55 3.98 1.71 1.64 0.81 0.00
Data given as mean ± SD, median (IQR; Q1–Q3), or n (%). †Calculated using the 2009 Chronic Kidney Disease Epidemiology Collaboration creatinine equation.8 BUN, blood urea nitrogen; CACS, coronary artery calcium score; CKD, chronic kidney disease; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol.
Circulation Journal Vol.80, July 2016
1646 HWANG IC et al.
Following a topogram of the chest, a calcium score scan was obtained using the retrospective method with tube voltage 120 kV, and 110 effective mAs with a 200-mm field of view. Data were reconstructed to 3-mm slice thickness with a –400-ms acquisition window. Calcium score analysis was performed on site using a dedicated workstation and Wizard VB10B (Somaris/5 VB10B-W, SynGo, Siemens, Germany). Quantita-tive CACS were calculated according to the method described by Agatston et al,18 and categorized as no CAC (CACS 0), CACS 1–99, CACS ≥100, CACS 100–399, and CACS ≥400 according to the clinical guidelines.19,20
Statistical AnalysisCategorical variables are presented as frequencies and per-centages, and continuous variables as mean ± SD or median (IQR). One-way analysis of covariance (ANCOVA) with post-hoc comparisons was used to examine the differences in CACS over the subgroups by eGFR and hsCRP, while age, sex, presence of hypertension, diabetes, dyslipidemia, smoking status, lipid profiles and Hb were used as covariates. Adjusted odds ratios (OR) for CACS >0, CACS ≥100, and CACS ≥400 were calculated using logistic regression models across the eGFR and hsCRP subgroups, using eGFR 90–104 ml/min/ 1.73 m2 with hsCRP <2.0 mg/L as the reference group. Logis-tic regression models were also used to test for interactions between eGFR and hsCRP levels for having CACS >0, CACS ≥100, and CACS ≥400.
For survival analysis, the adjusted hazards ratios (HR) for all-cause mortality were calculated across the subgroups strat-ified by eGFR (<45, 45–59, 60–74, 75–89, 90–104, and ≥105 ml/min/1.73 m2) and hsCRP (2.0 mg/L), using the sub-group of eGFR 90–104 ml/min/1.73 m2 with hsCRP <2.0 mg/L as the reference group. We used the Kaplan-Meier method and the Cox proportional hazard model for the comparison of time to event. All baseline characteristics were considered as covariates. The prognostic value of CAC burden, and its dif-ference across the subgroups divided by eGFR (60 ml/min/ 1.73 m2) and hsCRP (2.0 mg/L) were assessed, with tests for interactions between the severity of CAC and the levels of hsCRP and eGFR.
All statistical analysis was performed with SAS 9.3 (SAS Institute, Cary, NC, USA) and SPSS 20.0 (SPSS, Chicago, IL, USA), and P<0.05 was considered statistically significant.
measurement at Seoul National University Hospital, Seoul National University Bundang Hospital, and Seoul National University Hospital Healthcare System Gangnam Center. Individuals were excluded if any of the following laboratory tests were not performed: hemoglobin (Hb), fasting serum glucose, HbA1c, high-sensitivity C-reactive protein (hsCRP), creatinine, total cholesterol, triglyceride, high-density lipopro-tein cholesterol (HDL-C), and low-density lipoprotein choles-terol (LDL-C). In total, 30,703 patients were included in the analysis. Hypertension was defined as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg, or current antihypertensive therapy. Diabetes was defined as HbA1c ≥6.5% or fasting serum glucose ≥126 mg/dl. Dyslipidemia was defined as total cholesterol ≥240 mg/dl, triglycerides ≥200 mg/dl, LDL-C ≥160 mg/dl, HDL-C <40 mg/dl in men and <50 mg/dl in women, or use of lipid-lowering medications. Estimated glomerular filtration rate (eGFR) was calculated with the 2009 CKD Epidemiology Collaboration (CKD-EPI) creatinine equation, and the distribution of eGFR was categorized as <45, 45–59, 60–74, 75–89, 90–104, and ≥105 ml/min/1.73 m2 given the large epidemiologic studies showing outcomes in subgroups divided by 15 units of eGFR (ml/min/1.73 m2), which were quoted in the 2012 KDIGO clinical practice guide-line.14–16 These subgroups were further stratified according to hsCRP 2.0 mg/L, according to the recent guidelines.17
This study was carried out according to the principles of the Declaration of Helsinki and approved by the institutional review board of Seoul National University Hospital (H-1207-080-418). Given the observational nature of this study, the need for informed patient consent was waived.
Data Source and Outcome MeasureUsing the electronic medical records, we obtained the demo-graphic factors, laboratory test results, and CACS of the study population. The study outcome was all-cause mortality during follow-up. For the confirmation of death, we used the database from the Korean Ministry of Security and Public Administra-tion, and the last date of confirmation was 18 March 2016.
CAC MeasurementSubjects underwent 64-slice multidetector computed tomog-raphy (CT; SOMATOM Sensation 64 and SOMATOM Definition, Siemens Medical Solutions, Forchheim, Germany; Brilliance 64, Philips Medical Systems, Best, The Netherlands).
Table 2. Coronary Artery Calcification vs. eGFR†
n CACS CACS=0 CACS >0 CACS 1–99
CACS 100–399
CACS ≥400
Total group 30,703 66.2±283.2 (0.0, 0.0–11.8)
20,849 (67.9) 9,854 (32.1) 6,143 (20.0) 2,382 (7.8) 1,329 (4.3)
eGFR <45 ml/min/1.73 m2 348 345.0±612.7 (82.1, 0.5–374.4)
86 (24.7) 262 (75.3) 101 (29.0) 78 (22.4) 83 (23.9)
eGFR 45–59 ml/min/1.73 m2 2,482 159.7±450.6 (4.3, 0.0–112.0)
1,148 (46.3) 1,334 (53.7) 685 (27.6) 382 (15.4) 267 (10.8)
eGFR 60–74 ml/min/1.73 m2 9,720 72.6±284.6 (0.0, 0.0–22.1)
6,200 (63.8) 3,520 (36.2) 2,197 (22.6) 858 (8.8) 465 (4.8)
eGFR 75–89 ml/min/1.73 m2 10,216 57.2±282.5 (0.0, 0.0–7.0)
7,152 (70.0) 3,064 (30.0) 1,978 (19.4) 714 (7.0) 372 (3.6)
eGFR 90–104 ml/min/1.73 m2 6,143 34.4±159.9 (0.0, 0.0–0.0)
4,639 (75.5) 1,504 (24.5) 1,049 (17.1) 320 (5.2) 135 (2.2)
eGFR ≥105 ml/min/1.73 m2 1,794 8.6±61.5 (0.0, 0.0–0.0)
1,624 (90.5) 170 (9.5) 133 (7.4) 30 (1.7) 7 (0.4)
Data given as mean ± SD, median (IQR; Q1–Q3), or n (%). †Calculated using the 2009 Chronic Kidney Disease Epidemiology Collaboration creatinine equation.8 Abbreviations as in Table 1.
Circulation Journal Vol.80, July 2016
1647CKD, CAC, CRP and Mortality
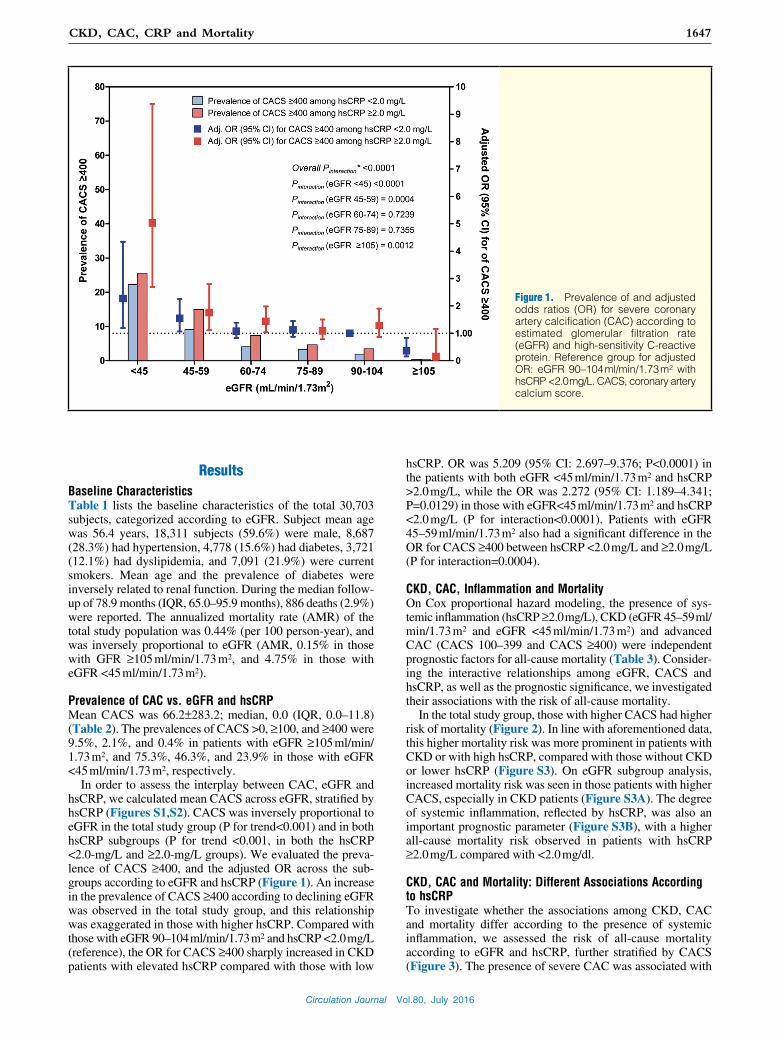
hsCRP. OR was 5.209 (95% CI: 2.697–9.376; P<0.0001) in the patients with both eGFR <45 ml/min/1.73 m2 and hsCRP >2.0 mg/L, while the OR was 2.272 (95% CI: 1.189–4.341; P=0.0129) in those with eGFR<45 ml/min/1.73 m2 and hsCRP <2.0 mg/L (P for interaction<0.0001). Patients with eGFR 45–59 ml/min/1.73 m2 also had a significant difference in the OR for CACS ≥400 between hsCRP <2.0 mg/L and ≥2.0 mg/L (P for interaction=0.0004).
CKD, CAC, Inflammation and MortalityOn Cox proportional hazard modeling, the presence of sys-temic inflammation (hsCRP ≥2.0 mg/L), CKD (eGFR 45–59 ml/ min/1.73 m2 and eGFR <45 ml/min/1.73 m2) and advanced CAC (CACS 100–399 and CACS ≥400) were independent prognostic factors for all-cause mortality (Table 3). Consider-ing the interactive relationships among eGFR, CACS and hsCRP, as well as the prognostic significance, we investigated their associations with the risk of all-cause mortality.
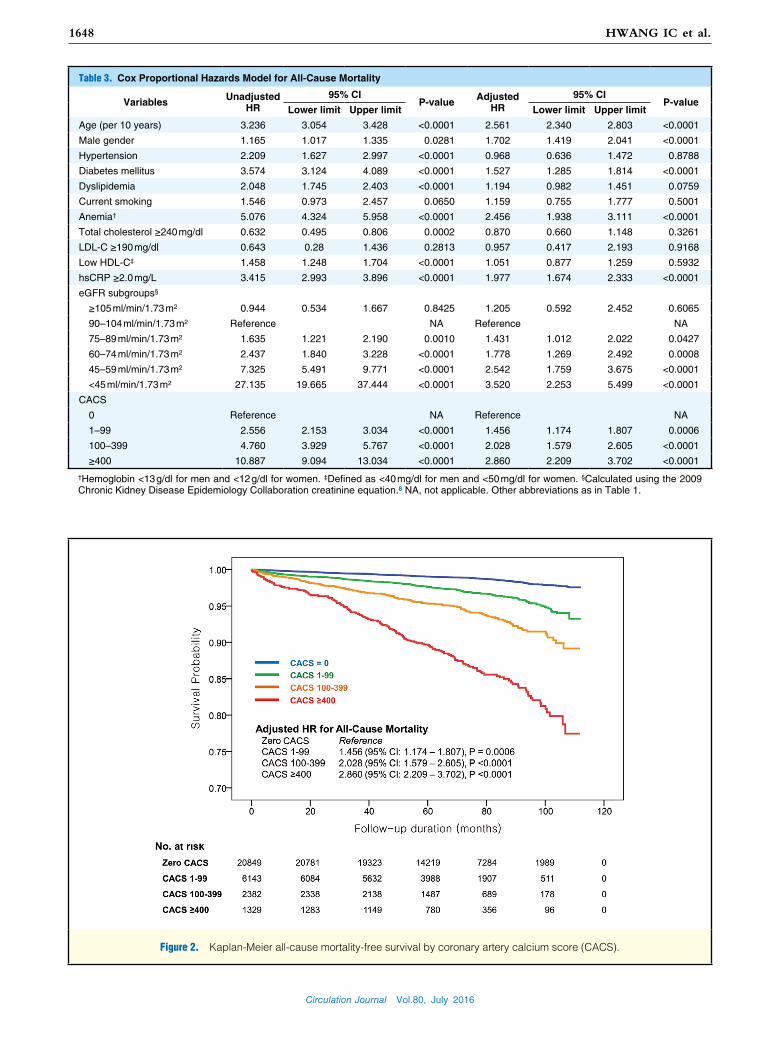
In the total study group, those with higher CACS had higher risk of mortality (Figure 2). In line with aforementioned data, this higher mortality risk was more prominent in patients with CKD or with high hsCRP, compared with those without CKD or lower hsCRP (Figure S3). On eGFR subgroup analysis, increased mortality risk was seen in those patients with higher CACS, especially in CKD patients (Figure S3A). The degree of systemic inflammation, reflected by hsCRP, was also an important prognostic parameter (Figure S3B), with a higher all-cause mortality risk observed in patients with hsCRP ≥2.0 mg/L compared with <2.0 mg/dl.
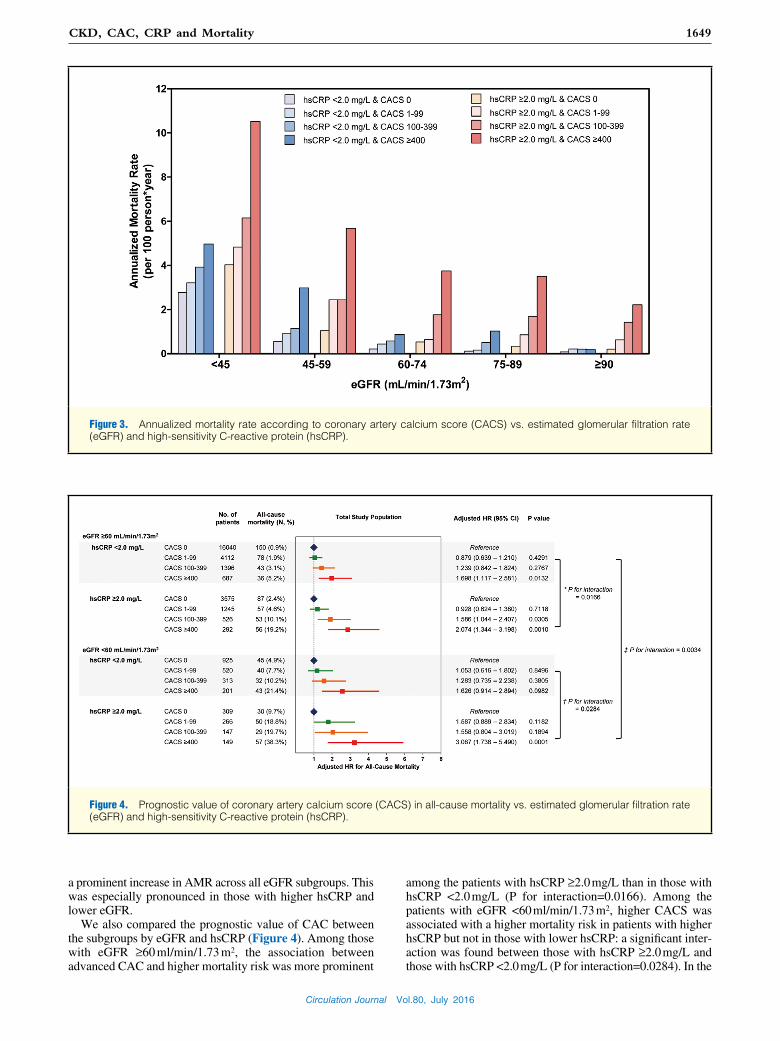
CKD, CAC and Mortality: Different Associations According to hsCRPTo investigate whether the associations among CKD, CAC and mortality differ according to the presence of systemic inflammation, we assessed the risk of all-cause mortality according to eGFR and hsCRP, further stratified by CACS (Figure 3). The presence of severe CAC was associated with
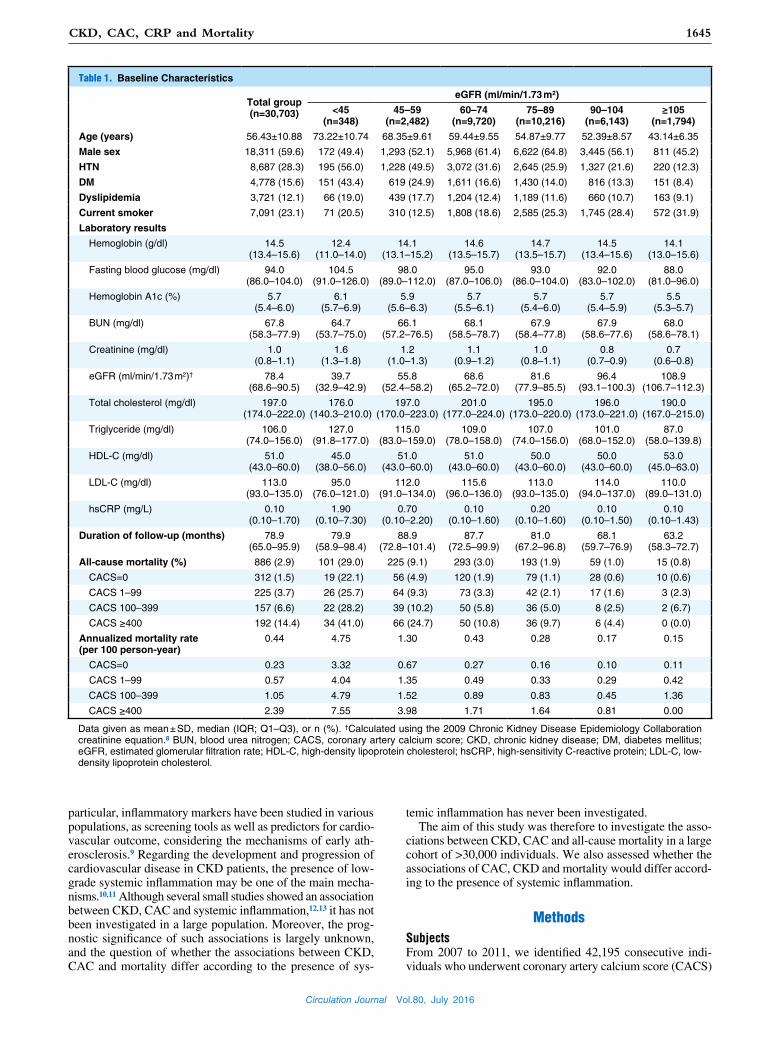
ResultsBaseline CharacteristicsTable 1 lists the baseline characteristics of the total 30,703 subjects, categorized according to eGFR. Subject mean age was 56.4 years, 18,311 subjects (59.6%) were male, 8,687 (28.3%) had hypertension, 4,778 (15.6%) had diabetes, 3,721 (12.1%) had dyslipidemia, and 7,091 (21.9%) were current smokers. Mean age and the prevalence of diabetes were inversely related to renal function. During the median follow-up of 78.9 months (IQR, 65.0–95.9 months), 886 deaths (2.9%) were reported. The annualized mortality rate (AMR) of the total study population was 0.44% (per 100 person-year), and was inversely proportional to eGFR (AMR, 0.15% in those with GFR ≥105 ml/min/1.73 m2, and 4.75% in those with eGFR <45 ml/min/1.73 m2).
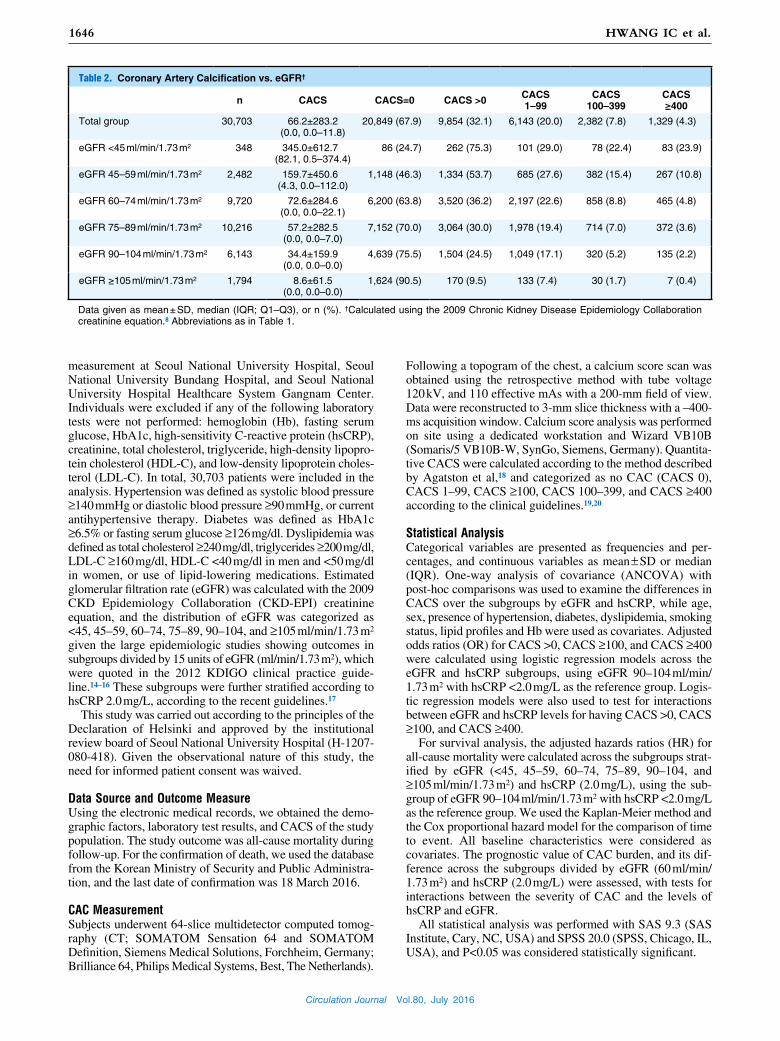
Prevalence of CAC vs. eGFR and hsCRPMean CACS was 66.2±283.2; median, 0.0 (IQR, 0.0–11.8) (Table 2). The prevalences of CACS >0, ≥100, and ≥400 were 9.5%, 2.1%, and 0.4% in patients with eGFR ≥105 ml/min/ 1.73 m2, and 75.3%, 46.3%, and 23.9% in those with eGFR <45 ml/min/1.73 m2, respectively.
In order to assess the interplay between CAC, eGFR and hsCRP, we calculated mean CACS across eGFR, stratified by hsCRP (Figures S1,S2). CACS was inversely proportional to eGFR in the total study group (P for trend<0.001) and in both hsCRP subgroups (P for trend <0.001, in both the hsCRP <2.0-mg/L and ≥2.0-mg/L groups). We evaluated the preva-lence of CACS ≥400, and the adjusted OR across the sub-groups according to eGFR and hsCRP (Figure 1). An increase in the prevalence of CACS ≥400 according to declining eGFR was observed in the total study group, and this relationship was exaggerated in those with higher hsCRP. Compared with those with eGFR 90–104 ml/min/1.73 m2 and hsCRP <2.0 mg/L (reference), the OR for CACS ≥400 sharply increased in CKD patients with elevated hsCRP compared with those with low
Figure 1. Prevalence of and adjusted odds ratios (OR) for severe coronary artery calcification (CAC) according to estimated glomerular filtration rate (eGFR) and high-sensitivity C-reactive protein. Reference group for adjusted OR: eGFR 90–104 ml/min/1.73 m2 with hsCRP <2.0 mg/L. CACS, coronary artery calcium score.
Circulation Journal Vol.80, July 2016
1648 HWANG IC et al.
Table 3. Cox Proportional Hazards Model for All-Cause Mortality
Variables Unadjusted HR
95% CIP-value Adjusted
HR95% CI
P-valueLower limit Upper limit Lower limit Upper limit
Age (per 10 years) 3.236 3.054 3.428 <0.0001 2.561 2.340 2.803 <0.0001
Male gender 1.165 1.017 1.335 0.0281 1.702 1.419 2.041 <0.0001
Hypertension 2.209 1.627 2.997 <0.0001 0.968 0.636 1.472 0.8788
Diabetes mellitus 3.574 3.124 4.089 <0.0001 1.527 1.285 1.814 <0.0001
Dyslipidemia 2.048 1.745 2.403 <0.0001 1.194 0.982 1.451 0.0759
Current smoking 1.546 0.973 2.457 0.0650 1.159 0.755 1.777 0.5001
Anemia† 5.076 4.324 5.958 <0.0001 2.456 1.938 3.111 <0.0001
Total cholesterol ≥240 mg/dl 0.632 0.495 0.806 0.0002 0.870 0.660 1.148 0.3261
LDL-C ≥190 mg/dl 0.643 0.28 1.436 0.2813 0.957 0.417 2.193 0.9168
Low HDL-C‡ 1.458 1.248 1.704 <0.0001 1.051 0.877 1.259 0.5932
hsCRP ≥2.0 mg/L 3.415 2.993 3.896 <0.0001 1.977 1.674 2.333 <0.0001
eGFR subgroups§
≥105 ml/min/1.73 m2 0.944 0.534 1.667 0.8425 1.205 0.592 2.452 0.6065
90–104 ml/min/1.73 m2 Reference NA Reference NA
75–89 ml/min/1.73 m2 1.635 1.221 2.190 0.0010 1.431 1.012 2.022 0.0427
60–74 ml/min/1.73 m2 2.437 1.840 3.228 <0.0001 1.778 1.269 2.492 0.0008
45–59 ml/min/1.73 m2 7.325 5.491 9.771 <0.0001 2.542 1.759 3.675 <0.0001
<45 ml/min/1.73 m2 27.135 19.665 37.444 <0.0001 3.520 2.253 5.499 <0.0001
CACS
0 Reference NA Reference NA
1–99 2.556 2.153 3.034 <0.0001 1.456 1.174 1.807 0.0006
100–399 4.760 3.929 5.767 <0.0001 2.028 1.579 2.605 <0.0001
≥400 10.887 9.094 13.034 <0.0001 2.860 2.209 3.702 <0.0001
†Hemoglobin <13 g/dl for men and <12 g/dl for women. ‡Defined as <40 mg/dl for men and <50 mg/dl for women. §Calculated using the 2009 Chronic Kidney Disease Epidemiology Collaboration creatinine equation.8 NA, not applicable. Other abbreviations as in Table 1.
Figure 2. Kaplan-Meier all-cause mortality-free survival by coronary artery calcium score (CACS).
Circulation Journal Vol.80, July 2016
1649CKD, CAC, CRP and Mortality
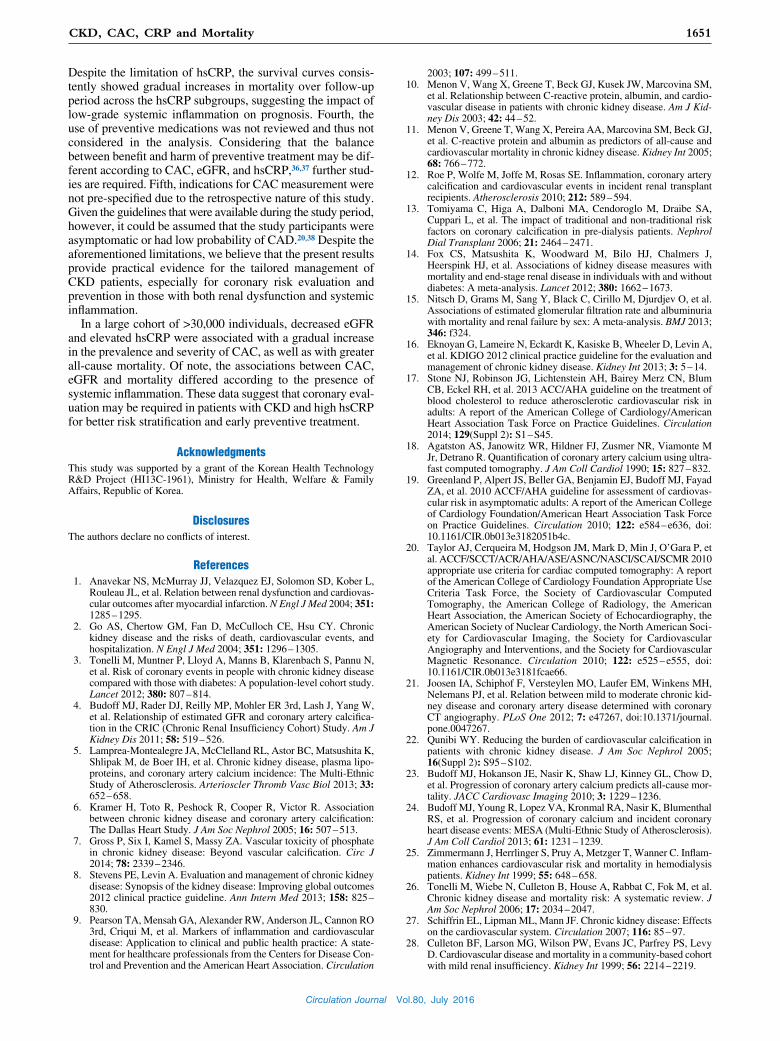
among the patients with hsCRP ≥2.0 mg/L than in those with hsCRP <2.0 mg/L (P for interaction=0.0166). Among the patients with eGFR <60 ml/min/1.73 m2, higher CACS was associated with a higher mortality risk in patients with higher hsCRP but not in those with lower hsCRP: a significant inter-action was found between those with hsCRP ≥2.0 mg/L and those with hsCRP <2.0 mg/L (P for interaction=0.0284). In the
a prominent increase in AMR across all eGFR subgroups. This was especially pronounced in those with higher hsCRP and lower eGFR.
We also compared the prognostic value of CAC between the subgroups by eGFR and hsCRP (Figure 4). Among those with eGFR ≥60 ml/min/1.73 m2, the association between advanced CAC and higher mortality risk was more prominent
Figure 3. Annualized mortality rate according to coronary artery calcium score (CACS) vs. estimated glomerular filtration rate (eGFR) and high-sensitivity C-reactive protein (hsCRP).
Figure 4. Prognostic value of coronary artery calcium score (CACS) in all-cause mortality vs. estimated glomerular filtration rate (eGFR) and high-sensitivity C-reactive protein (hsCRP).

Circulation Journal Vol.80, July 2016
1650 HWANG IC et al.
cardiovascular events,25–27 and the risk of cardiovascular death increases according to CKD stage.2,26,28 Current KDIGO guidelines state that patients with CKD need to be considered at increased risk for cardiovascular disease.8,16 The strong relationship between the presence of CKD and cardiovascular risk might be explained by several pathophysiologic mecha-nisms, including the presence of hypertension, endothelial dysfunction, chronic inflammation, oxidative stress, and the accelerated vascular calcification.27
We demonstrated that the risk of all-cause mortality increases with declining eGFR, elevated hsCRP, and increased CAC severity. Of note, the association between increased mortality risk and severity of CAC was more prominent among the patients with high hsCRP and renal dysfunction than among those without CKD or with low hsCRP. Interaction analyses also showed that the prognostic value of CAC differs accord-ing to eGFR and hsCRP levels. Together, these data support a role for systemic inflammation, as measured by hsCRP, in the acceleration of CAC and the resulting increase in mortality, especially in CKD patients.
In addition to the well-established relationship between the decreased eGFR and elevated all-cause mortality from previ-ous large studies,14,15,29 the present findings provide novel perspectives in terms of CAC screening in CKD patients. In particular, we showed the clinical usefulness of CAC mea-surement in patients with CKD, especially in those with higher hsCRP. There have been insufficient data to recommend CAC screening in CKD patients, despite the abundant evidence on the prognostic value of CAC in the general population and the fact that it does not require the use of contrast media.30,31 According to current K/DOQI guidelines, the standard meth-ods of coronary evaluation in patients under dialysis are stress echocardiography and myocardial perfusion imaging.32 The KDIGO guidelines acknowledged that the data on the appro-priate screening of CAD in CKD patients are limited, and also stated that the use of cardiac CT and magnetic resonance imaging are currently not recommended due to a lack of sup-porting evidence and the potential risk from contrast media.8,33 The present study has shown that CAC burden has additional clinical significance in CKD patients and that CAC measure-ment may be more beneficial in those with a higher degree of inflammation. These robust results support CAC screening in high-risk CKD patients, in combination with the measurement of inflammatory burden. Moreover, the synergistic effect of CAC, renal dysfunction and systemic inflammation on all-cause mortality suggests the potential benefit of cardiovascu-lar preventive measures in CKD patients with high hsCRP. Future studies are warranted to investigate the impact of CAC screening combined with early adoption of preventive treat-ment on clinical outcome.
The present study was subject to the following limitations. First, the information on established risk factors for vascular calcification in CKD patients, such as the presence of protein-uria or albuminuria, and serum calcium, phosphate, and para-thyroid hormone were not available.34,35 Although the results were adjusted for traditional risk factors such as age, sex, hypertension, diabetes, dyslipidemia, smoking status and lipid profiles, the interpretation needs caution. Second, information on the specific causes of death was not available. Given, how-ever, the well-established prognostic value of CAC for cardio-vascular events,30 the present study could have a clinical relevance. Also, it should be noted that the most frequent cause of death in CKD patients is cardiovascular events, which increases according to the stage of CKD.25,29 Third, hsCRP might be elevated by other causes such as infectious diseases.
overall study group, the prognostic value of CACS for all-cause mortality was significantly different according to the hsCRP level (P for interaction=0.0034).
DiscussionIn this large-scale real-world cohort of patients referred for CAC measurement, the prevalence and extent of CAC were inversely proportional to eGFR, especially in patients with high hsCRP. Severe CAC was independently associated with a higher risk of all-cause mortality, in a synergistic manner with decreased eGFR and elevated hsCRP. The associations between CAC burden, renal dysfunction and mortality risk differed according to the degree of inflammation, as reflected by hsCRP level.
The Dallas Heart Study was the first to show that the pres-ence of CKD (stages 3–5) was significantly associated with CAC, especially in patients with CACS ≥400.6 In the Chronic Renal Insufficiency Cohort (CRIC), Budoff et al reported a graded relationship between the severity of CKD and CAC, independent of traditional risk factors.4 In the CRIC study, the prevalence of CACS >0 increased from 61.1% in patients with eGFR 50–59 ml/min/1.73 m2 to 68.6% in patients with eGFR <30 ml/min/1.73 m2, and the prevalence of severe CAC (CACS ≥400) increased more steeply between the same eGFR patient groups, from 14.4% to 27.2%, respectively. In contrast, according to Joosen et al, mild-moderate CKD was not inde-pendently associated with coronary plaque burden after adjust-ing for traditional cardiovascular risk factors.21
We noted similar results to the Dallas Heart Study and CRIC: the presence of CAC and its severity were closely related to decreased eGFR.4,6 The association between CAC and eGFR remained significant after adjusting for traditional risk factors. This association was more evident for severe CAC, showing an exaggerated increase in adjusted OR for having CACS ≥400. Further to the previous studies, we showed that the association between CAC and eGFR is different according to the presence of systemic inflammation.
The presence of low-grade inflammation in CKD patients has been suggested to accelerate the development and progres-sion of vascular calcification.10,22 Although the exact patho-physiologic mechanisms for the presence of low-grade inflammation in CKD patients are unclear, evidence suggests that comorbidities such as diabetes, hypertension, dyslipid-emia, increased oxidative stress, and accumulation of uremic toxins accelerate inflammation in CKD patients and, thus, lead to the development and progression of atherosclerosis.12,13 These previous results suggest that the presence of trigger fac-tors promotes CAC in CKD patients, and eventually increases the risk of mortality and morbidity.
In this study, the increase in CAC burden according to declining eGFR was more prominent in patients with high hsCRP. We observed a striking difference in the OR for hav-ing severe CAC (CACS ≥400) between hsCRP <2.0- vs. ≥2.0-mg/L groups in the CKD patients. The association between CKD and severe CAC depends on the presence of low-grade inflammation, and high hsCRP may influence the progression of CAC in patients with CKD in a synergistic manner. Given that the progression of CAC is associated with cardiovascular events and mortality,23,24 the present results indicate the need for better risk stratification among CKD patients with elevated hsCRP.
The presence of CKD is a well-known risk factor for death, cardiovascular events and hospitalization. According to previ-ous reports, more than half of hemodialysis patients die of
Circulation Journal Vol.80, July 2016
1651CKD, CAC, CRP and Mortality
2003; 107: 499 – 511.10. Menon V, Wang X, Greene T, Beck GJ, Kusek JW, Marcovina SM,
et al. Relationship between C-reactive protein, albumin, and cardio-vascular disease in patients with chronic kidney disease. Am J Kid-ney Dis 2003; 42: 44 – 52.
11. Menon V, Greene T, Wang X, Pereira AA, Marcovina SM, Beck GJ, et al. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int 2005; 68: 766 – 772.
12. Roe P, Wolfe M, Joffe M, Rosas SE. Inflammation, coronary artery calcification and cardiovascular events in incident renal transplant recipients. Atherosclerosis 2010; 212: 589 – 594.
13. Tomiyama C, Higa A, Dalboni MA, Cendoroglo M, Draibe SA, Cuppari L, et al. The impact of traditional and non-traditional risk factors on coronary calcification in pre-dialysis patients. Nephrol Dial Transplant 2006; 21: 2464 – 2471.
14. Fox CS, Matsushita K, Woodward M, Bilo HJ, Chalmers J, Heerspink HJ, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet 2012; 380: 1662 – 1673.
15. Nitsch D, Grams M, Sang Y, Black C, Cirillo M, Djurdjev O, et al. Associations of estimated glomerular filtration rate and albuminuria with mortality and renal failure by sex: A meta-analysis. BMJ 2013; 346: f324.
16. Eknoyan G, Lameire N, Eckardt K, Kasiske B, Wheeler D, Levin A, et al. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int 2013; 3: 5 – 14.
17. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014; 129(Suppl 2): S1 – S45.
18. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultra-fast computed tomography. J Am Coll Cardiol 1990; 15: 827 – 832.
19. Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovas-cular risk in asymptomatic adults: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2010; 122: e584 – e636, doi: 10.1161/CIR.0b013e3182051b4c.
20. Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O’Gara P, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography: A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Soci-ety for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. Circulation 2010; 122: e525 – e555, doi: 10.1161/CIR.0b013e3181fcae66.
21. Joosen IA, Schiphof F, Versteylen MO, Laufer EM, Winkens MH, Nelemans PJ, et al. Relation between mild to moderate chronic kid-ney disease and coronary artery disease determined with coronary CT angiography. PLoS One 2012; 7: e47267, doi:10.1371/journal.pone.0047267.
22. Qunibi WY. Reducing the burden of cardiovascular calcification in patients with chronic kidney disease. J Am Soc Nephrol 2005; 16(Suppl 2): S95 – S102.
23. Budoff MJ, Hokanson JE, Nasir K, Shaw LJ, Kinney GL, Chow D, et al. Progression of coronary artery calcium predicts all-cause mor-tality. JACC Cardiovasc Imaging 2010; 3: 1229 – 1236.
24. Budoff MJ, Young R, Lopez VA, Kronmal RA, Nasir K, Blumenthal RS, et al. Progression of coronary calcium and incident coronary heart disease events: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol 2013; 61: 1231 – 1239.
25. Zimmermann J, Herrlinger S, Pruy A, Metzger T, Wanner C. Inflam-mation enhances cardiovascular risk and mortality in hemodialysis patients. Kidney Int 1999; 55: 648 – 658.
26. Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, et al. Chronic kidney disease and mortality risk: A systematic review. J Am Soc Nephrol 2006; 17: 2034 – 2047.
27. Schiffrin EL, Lipman ML, Mann JF. Chronic kidney disease: Effects on the cardiovascular system. Circulation 2007; 116: 85 – 97.
28. Culleton BF, Larson MG, Wilson PW, Evans JC, Parfrey PS, Levy D. Cardiovascular disease and mortality in a community-based cohort with mild renal insufficiency. Kidney Int 1999; 56: 2214 – 2219.
Despite the limitation of hsCRP, the survival curves consis-tently showed gradual increases in mortality over follow-up period across the hsCRP subgroups, suggesting the impact of low-grade systemic inflammation on prognosis. Fourth, the use of preventive medications was not reviewed and thus not considered in the analysis. Considering that the balance between benefit and harm of preventive treatment may be dif-ferent according to CAC, eGFR, and hsCRP,36,37 further stud-ies are required. Fifth, indications for CAC measurement were not pre-specified due to the retrospective nature of this study. Given the guidelines that were available during the study period, however, it could be assumed that the study participants were asymptomatic or had low probability of CAD.20,38 Despite the aforementioned limitations, we believe that the present results provide practical evidence for the tailored management of CKD patients, especially for coronary risk evaluation and prevention in those with both renal dysfunction and systemic inflammation.
In a large cohort of >30,000 individuals, decreased eGFR and elevated hsCRP were associated with a gradual increase in the prevalence and severity of CAC, as well as with greater all-cause mortality. Of note, the associations between CAC, eGFR and mortality differed according to the presence of systemic inflammation. These data suggest that coronary eval-uation may be required in patients with CKD and high hsCRP for better risk stratification and early preventive treatment.
AcknowledgmentsThis study was supported by a grant of the Korean Health Technology R&D Project (HI13C-1961), Ministry for Health, Welfare & Family Affairs, Republic of Korea.
DisclosuresThe authors declare no conflicts of interest.
References 1. Anavekar NS, McMurray JJ, Velazquez EJ, Solomon SD, Kober L,
Rouleau JL, et al. Relation between renal dysfunction and cardiovas-cular outcomes after myocardial infarction. N Engl J Med 2004; 351: 1285 – 1295.
2. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004; 351: 1296 – 1305.
3. Tonelli M, Muntner P, Lloyd A, Manns B, Klarenbach S, Pannu N, et al. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: A population-level cohort study. Lancet 2012; 380: 807 – 814.
4. Budoff MJ, Rader DJ, Reilly MP, Mohler ER 3rd, Lash J, Yang W, et al. Relationship of estimated GFR and coronary artery calcifica-tion in the CRIC (Chronic Renal Insufficiency Cohort) Study. Am J Kidney Dis 2011; 58: 519 – 526.
5. Lamprea-Montealegre JA, McClelland RL, Astor BC, Matsushita K, Shlipak M, de Boer IH, et al. Chronic kidney disease, plasma lipo-proteins, and coronary artery calcium incidence: The Multi-Ethnic Study of Atherosclerosis. Arterioscler Thromb Vasc Biol 2013; 33: 652 – 658.
6. Kramer H, Toto R, Peshock R, Cooper R, Victor R. Association between chronic kidney disease and coronary artery calcification: The Dallas Heart Study. J Am Soc Nephrol 2005; 16: 507 – 513.
7. Gross P, Six I, Kamel S, Massy ZA. Vascular toxicity of phosphate in chronic kidney disease: Beyond vascular calcification. Circ J 2014; 78: 2339 – 2346.
8. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann Intern Med 2013; 158: 825 – 830.
9. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A state-ment for healthcare professionals from the Centers for Disease Con-trol and Prevention and the American Heart Association. Circulation

Circulation Journal Vol.80, July 2016
1652 HWANG IC et al.
37. Blaha MJ, Budoff MJ, DeFilippis AP, Blankstein R, Rivera JJ, Agatston A, et al. Associations between C-reactive protein, coronary artery calcium, and cardiovascular events: Implications for the JUPITER population from MESA, a population-based cohort study. Lancet 2011; 378: 684 – 692.
38. Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, et al. ACCF/AHA 2007 clinical expert consensus docu-ment on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: A report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography). Circulation 2007; 115: 402 – 426.
Supplementary FilesSupplementary File 1
Figure S1. Relationship between renal function and coronary artery calcification (CAC) stratified by high-sensitivity C-reactive protein (hsCRP).
Figure S2. Mean coronary artery calcium score (CACS) vs. esti-mated glomerular filtration rate (eGFR) and high-sensitivity C-reac-tive protein (hsCRP).
Figure S3. All-cause mortality-free survival according to coronary artery calcium score (CACS) stratified by (A) estimated glomerular filtration rate (eGFR) 60 ml/min/1.73 m2, and (B) high-sensitivity C-reactive protein (hsCRP) 2.0 mg/L.
Please find supplementary file(s);http://dx.doi.org/10.1253/circj.CJ-15-1224
29. Chronic Kidney Disease Prognosis Consortium, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010; 375: 2073 – 2081.
30. Han D, Ó Hartaigh B, Gransar H, Yoon JH, Kim KJ, Kim MK, et al. Incremental benefit of coronary artery calcium score above tradi-tional risk factors for all-cause mortality in asymptomatic Korean adults. Circ J 2015; 79: 2445 – 2451.
31. Lee JH, Ó Hartaigh B, Han D, Park HE, Choi SY, Sung J, et al. Reas-sessing the usefulness of coronary artery calcium score among vary-ing racial and ethnic groups by geographic locations: Relevance of the Korea Initiatives on Coronary Artery Calcification Registry. J Cardiovasc Ultrasound 2015; 23: 195 – 203.
32. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis 2005; 45: S1 – S153.
33. Herzog CA, Asinger RW, Berger AK, Charytan DM, Diez J, Hart RG, et al. Cardiovascular disease in chronic kidney disease: A clini-cal update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2011; 80: 572 – 586.
34. He J, Reilly M, Yang W, Chen J, Go AS, Lash JP, et al. Risk factors for coronary artery calcium among patients with chronic kidney disease (from the Chronic Renal Insufficiency Cohort Study). Am J Cardiol 2012; 110: 1735 – 1741.
35. Shimbo Y, Suzuki S, Ishii H, Shibata Y, Tatami Y, Harata S, et al. Association of estimated glomerular filtration rate and proteinuria with lipid-rich plaque in coronary artery disease. Circ J 2015; 79: 2263 – 2270.
36. Hwang IC, Jeon JY, Kim Y, Kim HM, Yoon YE, Lee SP, et al. Association between aspirin therapy and clinical outcomes in patients with non-obstructive coronary artery disease: A cohort study. PLoS One 2015; 10: e0129584, doi:10.1371/journal.pone.0129584.
Related Documents