Systematic Review: Pharmacological and Behavioral Treatment for Trichotillomania Michael H. Bloch, Angeli Landeros-Weisenberger, Philip Dombrowski, Ben Kelmendi, Ryan Wegner, Jake Nudel, Christopher Pittenger, James F. Leckman, and Vladimir Coric Trichotillomania is a psychiatric condition characterized by compulsive hair pulling. Three interventions have been studied in the treatment of trichotillomania: habit-reversal therapy (HRT) and pharmacotherapy with either selective-serotonin reuptake inhibitors (SSRI) or clomi- pramine. This systematic review compared the efficacy of these interventions in blinded, randomized clinical trials. The electronic databases of Medline, Premedline, PsychINFO, Embase, and the Cochrane Central Register of Controlled Trials were searched for relevant trials using the search terms “trichotillomania” or “hair pulling.” Trials were eligible for inclusion if they compared habit-reversal therapy, SSRI pharmacotherapy, or clomipramine pharmacotherapy to each other or placebo and employed randomization and blinded assessment of outcome. Our primary outcome measure was mean change in trichotillomania severity. The summary statistic was standardized mean difference. Seven studies were eligible for inclusion in this review. Overall, meta-analysis demonstrated that habit-reversal therapy (effect size [ES] 1.14, 95% confidence interval [CI] 1.89, .38) was superior to pharmacotherapy with clomipramine (ES .68, 95% CI 1.28, .07) or SSRI (ES .02, 95% CI .32, .35). Clomipramine was more efficacious than placebo, while there was no evidence to demonstrate that SSRI are more efficacious than placebo in the treatment of trichotillomania. Future studies on trichotillomania should seek to determine if HRT can demonstrate efficacy against more rigorous control conditions that account for non-specific effects of therapy and determine if HRT can be an effective intervention for trichotillomania beyond the few sites where it is currently practiced in research studies. Future therapy and pharmacotherapy studies in trichotillomania should employ larger sample sizes and intention-to-treat analysis and seek to validate clinical rating scales of trichotillomania severity. Key Words: Clomipramine, habit-reversal therapy, meta-analysis, selec- tive serotonin reuptake inhibitors, systematic review, trichotillomania T richotillomania (TTM) is a psychiatric condition character- ized by compulsive hair pulling. Despite often being quite impairing and affecting approximately .6% to 1% of the population (1,2), trichotillomania has been rather sparsely studied. The three main therapeutic modalities for trichotillomania that have been studied are: 1) pharmacotherapy with a selective serotonin reuptake inhibitor (SSRI); 2) pharmacotherapy with clomipramine, a tricyclic antidepressant; and 3) habit-reversal therapy (HRT). Recent data from the Trichotillomania Impact Project suggest that pharma- cotherapy with SSRI is the most frequently employed intervention to treat TTM (3). A recent review on this topic also recommended that the use of SSRI “such as citalopram ... may be preferable (in relation to clomipramine) given the superior safety and tolerability of this drug class for related conditions, such as obsessive-compulsive disorder (OCD), and the positive results reported for an open-label study with trichotillomania patients” (4). The purpose of this sys- tematic review is to evaluate the evidence supporting the efficacy of these three interventions compared with placebo and to compare the efficacy of these treatment modalities with each other. Criteria for Considering Studies for This Review Types of Studies This review included randomized, controlled, clinical trials published in scientific literature with blinded assessment of clinical outcome. Types of Participants Participants were required to be older than age 16 and have a primary psychiatric diagnosis of trichotillomania or chronic hair pulling by DSM-IV criteria (5). Types of Interventions The three interventions included in this study were use of a selective serotonin reuptake inhibitor, clomipramine, or habit- reversal therapy. Habit-reversal therapy is a cognitive behavioral therapy tech- nique for trichotillomania and Tourette’s syndrome (6). The habit-reversal therapy program for trichotillomania consists of four main components. Self-monitoring. The self-monitoring component has the patient keep records of hair-pulling behavior. Awareness Training. Awareness training increases patient awareness of both hair-pulling behavior and high-risk situations that frequently trigger hair-pulling behaviors. Stimulus Control. Stimulus control includes techniques ei- ther to decrease opportunities to pull hair or to interfere with or prevent pulling (i.e., wearing gloves in high-risk situations). Stimulus-Response Intervention or Competing Response Intervention. Stimulus-response intervention is defined as de- veloping activities to substitute when the desire for hair pulling occurs, such as deep muscle relaxation or taking a walk. Competing response intervention is defined as teaching the subject to engage in a physically incompatible behavior (to the pulling) for a fixed period of time (i.e., 1 minute) or until the urge goes away. In HRT, patients are permitted to pull hair only after these activities are completed. For inclusion in this review, HRT arms of studies were required to include all four of these components. Additional components and techniques could be added to the therapeutic intervention and still qualify for consideration as an HRT inter- vention for this review. Acceptable control interventions for pharmacological inter- ventions in this review were either placebo or an active control condition. Active control was defined as any treatment modality From the Yale Child Study Center (MHB, AL-W, PD, JN, CP, JFL) and Depart- ment of Psychiatry (MHB, BK, RW, VC), Yale University School of Medi- cine, New Haven, Connecticut. Address reprint requests to Michael Bloch, M.D., Yale Child Study Center, 230 South Frontage Road, New Haven, CT 06520; E-mail: Michael.bloch@ yale.edu. Received March 20, 2007; revised May 13, 2007; accepted May 25, 2007. BIOL PSYCHIATRY 2007;xx:xxx 0006-3223/07/$32.00 doi:10.1016/j.biopsych.2007.05.019 © 2007 Society of Biological Psychiatry ARTICLE IN PRESS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

STMJ
TopotpodsCdtdFt
Kt
TpTbrtdctttddsttt
C
T
pc
F
A
R
0d
ARTICLE IN PRESS
ystematic Review: Pharmacological and Behavioralreatment for Trichotillomaniaichael H. Bloch, Angeli Landeros-Weisenberger, Philip Dombrowski, Ben Kelmendi, Ryan Wegner,
ake Nudel, Christopher Pittenger, James F. Leckman, and Vladimir Coric
richotillomania is a psychiatric condition characterized by compulsive hair pulling. Three interventions have been studied in the treatmentf trichotillomania: habit-reversal therapy (HRT) and pharmacotherapy with either selective-serotonin reuptake inhibitors (SSRI) or clomi-ramine. This systematic review compared the efficacy of these interventions in blinded, randomized clinical trials. The electronic databasesf Medline, Premedline, PsychINFO, Embase, and the Cochrane Central Register of Controlled Trials were searched for relevant trials using
he search terms “trichotillomania” or “hair pulling.” Trials were eligible for inclusion if they compared habit-reversal therapy, SSRIharmacotherapy, or clomipramine pharmacotherapy to each other or placebo and employed randomization and blinded assessment ofutcome. Our primary outcome measure was mean change in trichotillomania severity. The summary statistic was standardized meanifference. Seven studies were eligible for inclusion in this review. Overall, meta-analysis demonstrated that habit-reversal therapy (effectize [ES] � �1.14, 95% confidence interval [CI] � �1.89, �.38) was superior to pharmacotherapy with clomipramine (ES � �.68, 95%I � �1.28, �.07) or SSRI (ES � .02, 95% CI � �.32, .35). Clomipramine was more efficacious than placebo, while there was no evidence toemonstrate that SSRI are more efficacious than placebo in the treatment of trichotillomania. Future studies on trichotillomania should seek
o determine if HRT can demonstrate efficacy against more rigorous control conditions that account for non-specific effects of therapy andetermine if HRT can be an effective intervention for trichotillomania beyond the few sites where it is currently practiced in research studies.uture therapy and pharmacotherapy studies in trichotillomania should employ larger sample sizes and intention-to-treat analysis and seek
o validate clinical rating scales of trichotillomania severity.ey Words: Clomipramine, habit-reversal therapy, meta-analysis, selec-ive serotonin reuptake inhibitors, systematic review, trichotillomania
richotillomania (TTM) is a psychiatric condition character-ized by compulsive hair pulling. Despite often being quiteimpairing and affecting approximately .6% to 1% of the
opulation (1,2), trichotillomania has been rather sparsely studied.he three main therapeutic modalities for trichotillomania that haveeen studied are: 1) pharmacotherapy with a selective serotonineuptake inhibitor (SSRI); 2) pharmacotherapy with clomipramine, aricyclic antidepressant; and 3) habit-reversal therapy (HRT). Recentata from the Trichotillomania Impact Project suggest that pharma-otherapy with SSRI is the most frequently employed intervention toreat TTM (3). A recent review on this topic also recommended thathe use of SSRI “such as citalopram ... may be preferable (in relationo clomipramine) given the superior safety and tolerability of thisrug class for related conditions, such as obsessive-compulsiveisorder (OCD), and the positive results reported for an open-labeltudy with trichotillomania patients” (4). The purpose of this sys-ematic review is to evaluate the evidence supporting the efficacy ofhese three interventions compared with placebo and to comparehe efficacy of these treatment modalities with each other.
riteria for Considering Studies for This Review
ypes of StudiesThis review included randomized, controlled, clinical trials
ublished in scientific literature with blinded assessment oflinical outcome.
rom the Yale Child Study Center (MHB, AL-W, PD, JN, CP, JFL) and Depart-ment of Psychiatry (MHB, BK, RW, VC), Yale University School of Medi-cine, New Haven, Connecticut.
ddress reprint requests to Michael Bloch, M.D., Yale Child Study Center, 230South Frontage Road, New Haven, CT 06520; E-mail: [email protected].
eceived March 20, 2007; revised May 13, 2007; accepted May 25, 2007.
006-3223/07/$32.00oi:10.1016/j.biopsych.2007.05.019
Types of ParticipantsParticipants were required to be older than age 16 and have a
primary psychiatric diagnosis of trichotillomania or chronic hairpulling by DSM-IV criteria (5).
Types of InterventionsThe three interventions included in this study were use of a
selective serotonin reuptake inhibitor, clomipramine, or habit-reversal therapy.
Habit-reversal therapy is a cognitive behavioral therapy tech-nique for trichotillomania and Tourette’s syndrome (6). Thehabit-reversal therapy program for trichotillomania consists offour main components.
Self-monitoring. The self-monitoring component has thepatient keep records of hair-pulling behavior.
Awareness Training. Awareness training increases patientawareness of both hair-pulling behavior and high-risk situationsthat frequently trigger hair-pulling behaviors.
Stimulus Control. Stimulus control includes techniques ei-ther to decrease opportunities to pull hair or to interfere with orprevent pulling (i.e., wearing gloves in high-risk situations).
Stimulus-Response Intervention or Competing ResponseIntervention. Stimulus-response intervention is defined as de-veloping activities to substitute when the desire for hair pullingoccurs, such as deep muscle relaxation or taking a walk.Competing response intervention is defined as teaching thesubject to engage in a physically incompatible behavior (to thepulling) for a fixed period of time (i.e., 1 minute) or until the urgegoes away. In HRT, patients are permitted to pull hair only afterthese activities are completed.
For inclusion in this review, HRT arms of studies wererequired to include all four of these components. Additionalcomponents and techniques could be added to the therapeuticintervention and still qualify for consideration as an HRT inter-vention for this review.
Acceptable control interventions for pharmacological inter-ventions in this review were either placebo or an active control
condition. Active control was defined as any treatment modalityBIOL PSYCHIATRY 2007;xx:xxx© 2007 Society of Biological Psychiatry

btaAltm
T
P
cosiSohGs(sbstt
S
2osmPwarc
M
S
s(e
orsca4t
D
rdowf
2 BIOL PSYCHIATRY 2007;xx:xxx M.H. Bloch et al.
w
ARTICLE IN PRESS
elieved to be ineffective for trichotillomania at the initiation ofhe study and placed in the design of the experimental protocols a control condition for the active treatment intervention.cceptable control conditions for a therapy trial could be wait-
ist, psychosupportive or psychoanalytic sessions, and any otherherapeutic techniques previously studied and deemed mini-ally or ineffective in the treatment of trichotillomania.
ypes of Outcome Measures
rimary OutcomesOur primary outcome was defined as mean improvement in a
linical scale measuring trichotillomania severity (continuousutcome) conducted by a blinded rater. Acceptable clinicalcales for rating of trichotillomania (in their order of preference)ncluded the National Institute of Mental Health Trichotillomaniaeverity Scale or Trichotillomania Impairment Scale (7), anyther measurement of the severity of hair pulling (i.e., counts ofairs pulled out or videotaped ratings of hair loss), or the Clinicallobal Impressions Improvement Scale (8). Self-report measures
uch as the Massachusetts General Hospital Hairpulling ScaleMGH-HS) were only eligible to be the primary outcome mea-ure in double-blind studies—studies in which subjects werelinded to their own treatment assignment (9). In double-blindtudies, MGH-HS was the most preferred scale to measurerichotillomania outcome based on its common use and valida-ion in trichotillomania (10).
earch Strategy for Identification of Studies
The electronic databases of PubMed, PsychINFO (1967–005), Embase (1974–2000), and the Cochrane Central Registerf Controlled Trials (CENTRAL, as of 2006, Issue 1) wereearched for relevant trials. PubMed was searched using theedical subject headings “trichotillomania” or “hair pulling.”sychINFO, Embase, and CENTRAL were searched with the keyords “trichotillomania” or “hair pulling.” The references ofppropriate papers for this study, as well as any appropriateeview articles in this area, were additionally searched foritations of further relevant published and unpublished research.
ethods of the Review
election of StudiesThe titles and abstracts of studies obtained by the search
trategy outlined above were scrutinized by two reviewersM.H.B. and A.L.-W.) to determine if they were potentiallyligible for inclusion in this review.
Eligibility for selection into the study was based on scrutinyf the full articles for the following inclusion criteria: 1)andomized clinical trials with a control group or a compari-on between active treatments; 2) blinded assessment oflinical outcome; 3) patient population with a primary psychi-tric diagnosis of trichotillomania or chronic hair pulling; and) comparison of SSRI, clomipramine, and habit-reversalherapy to each other or a control condition.
ata CollectionSpecifically designed forms/coding sheets were used by two
eviewers (M.H.B. and A.L.-W.) independently working to collectata on methods, participants, dropouts, interventions, andutcome measurements. Any disagreement between reviewersas resolved through discussion and obtaining more information
rom the study investigators.
ww.sobp.org/journal
Choice of Summary StatisticsFor our primary outcome, mean improvement in trichotillo-
mania severity was measured as standardized mean differenceand was pooled for overall meta-analysis. Standardized meandifference was favored over weighted mean difference as theprimary outcome because rating scales differed between in-cluded studies.
For the inclusion of crossover trials along with traditionalparallel-group trials in our cumulative meta-analysis, three dif-ferent methods were used. These methods were derived from thestandard, accepted methodology for incorporating crossover intometa-analysis in the scientific literature (11,12). If there weresignificant carryover effects observed in the statistical analysis ofa crossover study, then data were analyzed only up until thepoint of the first crossover; thus, only data from the initial, firstrandomized treatment would be used. If no significant carryovereffects were observed and individual subject data were availablefor baseline and outcome data after each crossover period, thenall the data were available to compute the actual measurementsof treatment effect needed for this study–mean difference andstandard deviation. If individual subject data were not availablefrom the original manuscript, then the reported subject number,mean difference in treatments, and p value or t-statistic was usedto retrieve the standard deviation of paired observations. Themean difference and standard deviation of this measure can beestimated from available data based on two equations:
d � Xa � Xp
where d equals the difference in means between the activetreatment (Xa) and control (Xp); and
SD(d) � (d * �n)/T
where SD(d) is the standard deviation in mean differencesbetween treatments, n is the sample size, and T is the t-statisticfrom the paired t test of the outcome (11).
The standardized mean difference (effect size [ES] � d/SD[d])and standard error of standardized mean difference {[t (95%confidence interval for n-1 degrees of freedom)/1.96]/�n} werecomputed from the two values above for inclusion in meta-analysis. Crossover and parallel group studies were then incor-porated into a single meta-analysis using the generic inversevariation method of RevMan 4.2.8 (The Nordic Cochrane Centre,The Cochrane Collaboration, Copenhagen, Denmark). A randomeffects model was chosen for meta-analysis, as there was con-siderable heterogeneity between studies.
Assessment of Publication BiasRelevant data from all the included trials was entered into a
funnel plot (trial effect size plotted against sample size) to detectany publication bias (13).
Assessment of HeterogeneityHeterogeneity of treatment response was assessed from the
forest plot of weighted mean differences and relative risk ofindividual studies. Statistical estimates of heterogeneity wereperformed using the I-square heterogeneity statistic in RevMan.
Sensitivity AnalysisSensitivity analyses were conducted to determine the robust-
ness of reviewers’ conclusions to methodological assumptionsmade in conducting this systematic review. In particular, sensi-tivity analyses were conducted to determine the effects of subject
dropout. Our primary outcome measure reported treatment
eiccfWco
D
I
wcmSppto(stsst
E
frbteo
R
OC
iiw1wlts1dwpaisa(todtp
M.H. Bloch et al. BIOL PSYCHIATRY 2007;xx:xxx 3
ARTICLE IN PRESS
ffects based on the original authors’ analysis of the completersn each study; in sensitivity analysis, we used the last observationarried forward assumption for missing data. In last observationarried forward analysis, we assumed all dropouts had a changerom baseline score of 0 in the severity of their symptoms (14).e then re-analyzed our outcomes using the last observation
arried forward assumption to determine the robustness ofriginal conclusions on completers.
escription of Studies
ncluded StudiesSeven studies involving analysis of 157 completers in these trials
ere included in this systematic review. Table 1 depicts the mainharacteristics of studies included in this review. These trials were ofoderate-to-good quality, scoring 20 to 34 on the Quality Rating
cale (possible range 0–46). Trial size ranged from 13 to 16articipants (in crossover trials) and 16 to 40 completers (inarallel-group trials). All studies relied on recruitment of volun-eers, rather than epidemiologically representative samples, tobtain their subject pool. None of the four parallel-group trials15–18) used intention-to-treat analysis and three of the fourtudies had significant dropout rates (16% to 30%). Additionally,wo of the three crossover studies (19,20) had dropouts in theirtudy that cannot be accounted for in the analysis of crossovertudies. The Swedo et al. (7) study had no dropouts during thereatment phase of their study.
xcluded StudiesThree open-label SSRI studies examining fluoxetine (21),
luvoxamine (22), and citalopram (23) were excluded from thiseview because they lacked a placebo comparison group andlinded clinical ratings of outcome. One behavioral therapy trialhat compared HRT with negative practice training (6) wasxcluded because it did not include blinded clinical ratings ofutcome.
esults
utcome 1: Selective Serotonin Reuptake Inhibitors Versusontrol Condition
Four studies involving 72 completers contributed to analysisn this outcome. Christenson et al. (20) was a crossover studynvolving 16 completers (of 17) that compared efficacy of 6eeks of fluoxetine (maximum dose 80 mg, mean dose 77.5 �0 mg, maximal length of treatment with maximal tolerated doseas 2 weeks) to 6 weeks of placebo after a 2-week placebo
ead-in phase and a 5-week washout period after the firstreatment assignment. Streichwein and Thornby (19) was aimilarly designed crossover study involving 16 completers (of9) that compared efficacy of 12 weeks of fluoxetine (maximumose 80 mg, mean dose 78.8 � mg, maximal length of treatmentith maximal tolerated dose was 6 weeks) to 12 weeks oflacebo with a 5-week washout period between treatmentssignments. There were no significant carryover effects revealedn either crossover study, and thus, data from all periods of thetudy were included in the analysis. Van Minnen et al. (16) wasparallel-group study that compared 12 weeks of fluoxetine
maximum dose 60 mg, maximal length of treatment at maximalolerated dose was 10 weeks) (9 completers of 13) to 12 weeksf wait-list (10 completers of 15). Dougherty et al. (17) was aouble-blind, parallel-group study that compared 12-week ser-raline (maximum dose 200 mg/day) with placebo after a 2-week
lacebo lead-in phase. Fifteen of 19 subjects who were treatedwith sertraline and 16 of 18 subjects who received placebocompleted the 12-week pharmacological treatment phase of thisstudy.
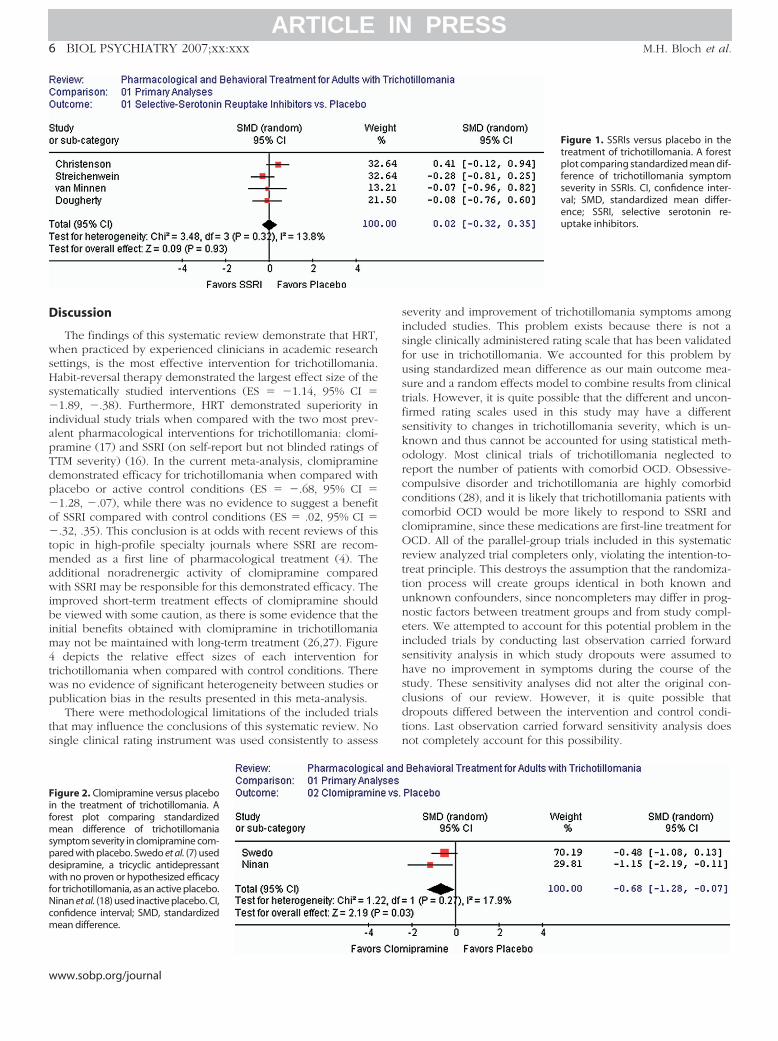
In the overall meta-analysis, there was no significant differ-ence between control conditions and SSRI pharmacotherapy(z � .09, p � �.93). The overall estimated ES was .02 (95%confidence interval [CI] � �.32, .35) favoring placebo (Figure 1).None of the four included studies individually reported a signif-icant difference between SSRI and control conditions. The com-parison for efficacy between SSRI and control conditions was notsignificantly different under the last observation carried forwardsensitivity analysis (ES � �.01, 95% CI � �.28, .26).
Outcome 2: Clomipramine Versus Control ConditionTwo studies involving 24 completers contributed to this
analysis. Swedo et al. (7) was a crossover study involving 13women that compared 5 weeks of clomipramine treatment(maximum dose 250 mg, mean dose 180.8 � 56.0 mg) with5-week desipramine treatment (maximum dose 250 mg, meandose 173.1 � 33.0 mg), which was considered an active controlcondition for this trial. There was a 2-week placebo lead-in phasefor this trial and no washout period between treatment phases.This study demonstrated no significant carryover effects, so datafrom all phases of the study were included in analysis. Ninanet al. (18) was a parallel-group study with 11 completers (of 16)that compared 9 weeks of clomipramine (maximum dose 250mg, mean dose 116.7 mg) with 9 weeks of placebo (maximumdose 250 mg, mean dose 250 mg). There were four dropoutsduring clomipramine treatment and one dropout during placebotreatment in this study.
The overall meta-analysis among completers in these studiesdemonstrated a significant treatment effect favoring clomipra-mine compared with the control condition (ES � �.68, 95%CI � �1.28, �.07). Figure 2 depicts the forest plot of thismeta-analysis comparing efficacy of clomipramine with thecontrol condition. Under the last observation carried forwardsensitivity analysis, this result remained significant (ES � �.60,95% CI � �1.18, �.11).
Outcome 3: Habit-Reversal Therapy Versus Control ConditionThree trials involving 59 completers contributed to the anal-
ysis of this outcome. Woods et al. (15) compared the benefit of12 completers of habit-reversal therapy plus acceptance andcommitment therapy (ACT) versus 13 wait-list control compl-eters. Acceptance and commitment therapy seeks to targetavoidance behaviors using exercises and metaphors that pro-mote acceptance of private events such as feelings, thoughts, andurges, while also seeking to focus the client on moving towardher goals (24). Participants received 10 HRT/ACT sessions overthe course of 12 weeks. There were two dropouts in the HRT/ACTgroup and one dropout in the wait-list group not included in theanalysis. Van Minnen et al. (16) compared 14 completers of HRT to10 of the 15 completers of the wait-list control subjects (blindedratings of hair loss were unavailable in 5 of the wait-list controlsubjects). Habit-reversal therapy was composed of six 45-minutebiweekly sessions. There was one dropout in the HRT but nodropouts in the wait-list control subjects in this study. Ninan et al.(18) compared five completers of HRT who received nine weeklysessions with five completers who received double-blind placebotreatment. There were two dropouts in the HRT and one dropout inthe placebo group of this study.
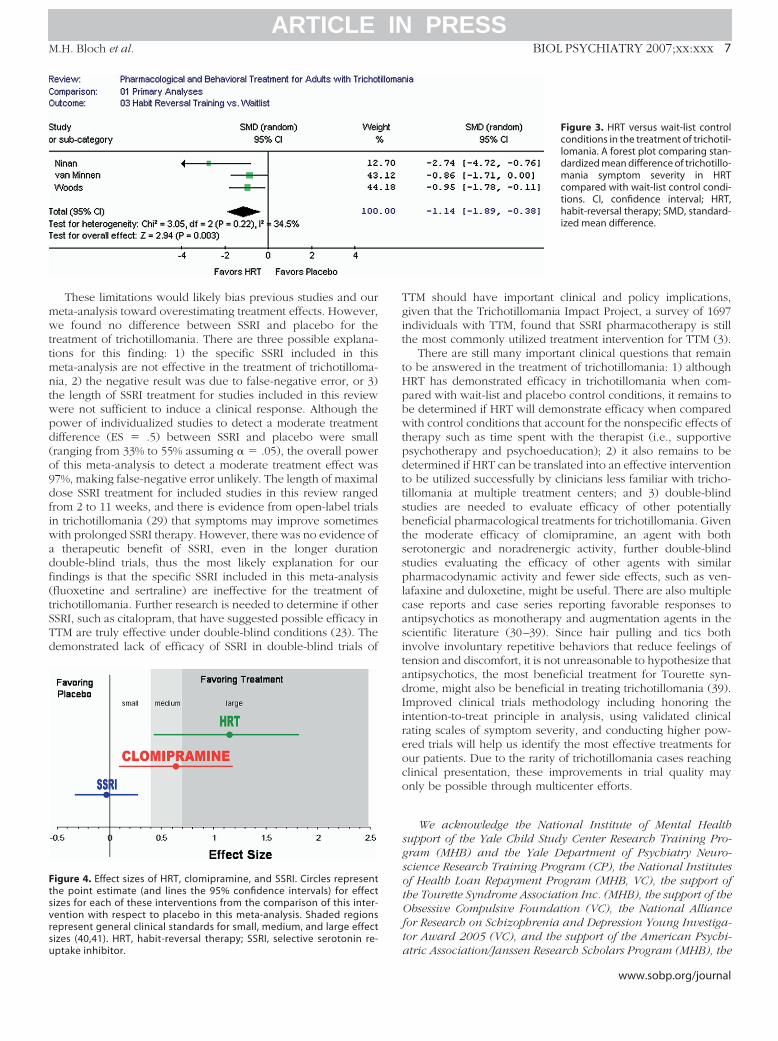
The overall meta-analysis demonstrated a significant benefit
of HRT compared with wait-list/placebo control conditionswww.sobp.org/journal
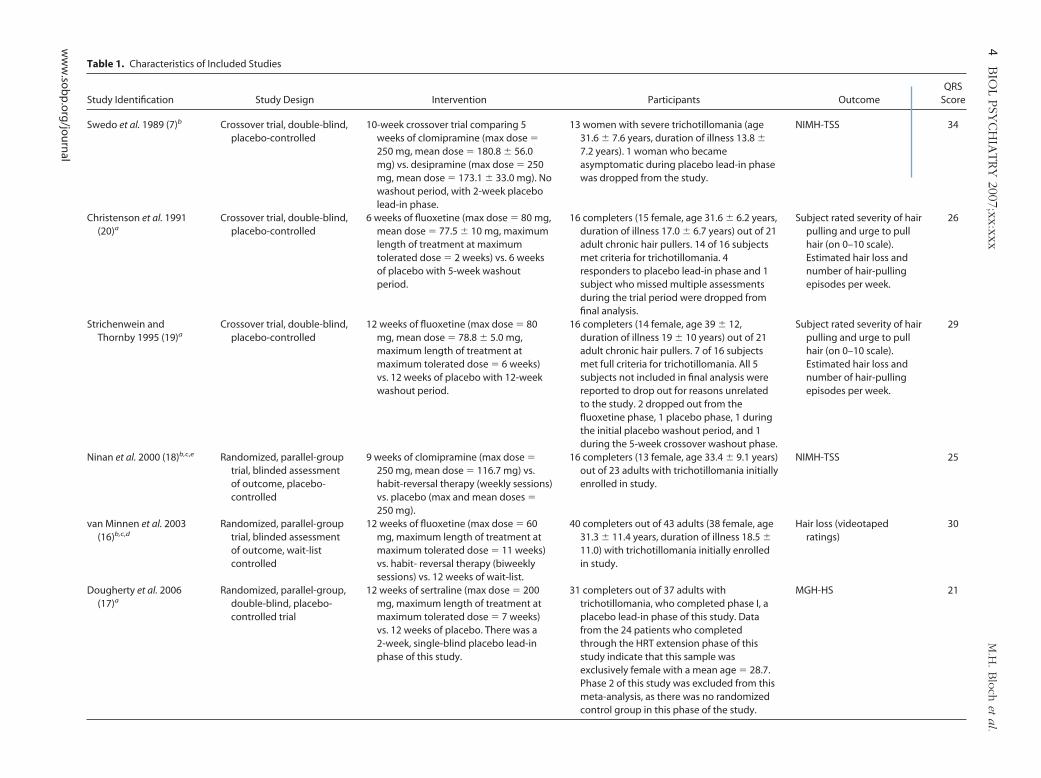
Table 1. Characteristics of Included Studies
Study Identification Study Design Intervention Participants OutcomeQRS
Score
Swedo et al. 1989 (7)b Crossover trial, double-blind,placebo-controlled
10-week crossover trial comparing 5weeks of clomipramine (max dose �250 mg, mean dose � 180.8 � 56.0mg) vs. desipramine (max dose � 250mg, mean dose � 173.1 � 33.0 mg). Nowashout period, with 2-week placebolead-in phase.
13 women with severe trichotillomania (age31.6 � 7.6 years, duration of illness 13.8 �7.2 years). 1 woman who becameasymptomatic during placebo lead-in phasewas dropped from the study.
NIMH-TSS 34
Christenson et al. 1991(20)a
Crossover trial, double-blind,placebo-controlled
6 weeks of fluoxetine (max dose � 80 mg,mean dose � 77.5 � 10 mg, maximumlength of treatment at maximumtolerated dose � 2 weeks) vs. 6 weeksof placebo with 5-week washoutperiod.
16 completers (15 female, age 31.6 � 6.2 years,duration of illness 17.0 � 6.7 years) out of 21adult chronic hair pullers. 14 of 16 subjectsmet criteria for trichotillomania. 4responders to placebo lead-in phase and 1subject who missed multiple assessmentsduring the trial period were dropped fromfinal analysis.
Subject rated severity of hairpulling and urge to pullhair (on 0–10 scale).Estimated hair loss andnumber of hair-pullingepisodes per week.
26
Strichenwein andThornby 1995 (19)a
Crossover trial, double-blind,placebo-controlled
12 weeks of fluoxetine (max dose � 80mg, mean dose � 78.8 � 5.0 mg,maximum length of treatment atmaximum tolerated dose � 6 weeks)vs. 12 weeks of placebo with 12-weekwashout period.
16 completers (14 female, age 39 � 12,duration of illness 19 � 10 years) out of 21adult chronic hair pullers. 7 of 16 subjectsmet full criteria for trichotillomania. All 5subjects not included in final analysis werereported to drop out for reasons unrelatedto the study. 2 dropped out from thefluoxetine phase, 1 placebo phase, 1 duringthe initial placebo washout period, and 1during the 5-week crossover washout phase.
Subject rated severity of hairpulling and urge to pullhair (on 0–10 scale).Estimated hair loss andnumber of hair-pullingepisodes per week.
29
Ninan et al. 2000 (18)b,c,e Randomized, parallel-grouptrial, blinded assessmentof outcome, placebo-controlled
9 weeks of clomipramine (max dose �250 mg, mean dose � 116.7 mg) vs.habit-reversal therapy (weekly sessions)vs. placebo (max and mean doses �250 mg).
16 completers (13 female, age 33.4 � 9.1 years)out of 23 adults with trichotillomania initiallyenrolled in study.
NIMH-TSS 25
van Minnen et al. 2003(16)b,c,d
Randomized, parallel-grouptrial, blinded assessmentof outcome, wait-listcontrolled
12 weeks of fluoxetine (max dose � 60mg, maximum length of treatment atmaximum tolerated dose � 11 weeks)vs. habit- reversal therapy (biweeklysessions) vs. 12 weeks of wait-list.
40 completers out of 43 adults (38 female, age31.3 � 11.4 years, duration of illness 18.5 �11.0) with trichotillomania initially enrolledin study.
Hair loss (videotapedratings)
30
Dougherty et al. 2006(17)a
Randomized, parallel-group,double-blind, placebo-controlled trial
12 weeks of sertraline (max dose � 200mg, maximum length of treatment atmaximum tolerated dose � 7 weeks)vs. 12 weeks of placebo. There was a2-week, single-blind placebo lead-inphase of this study.
31 completers out of 37 adults withtrichotillomania, who completed phase I, aplacebo lead-in phase of this study. Datafrom the 24 patients who completedthrough the HRT extension phase of thisstudy indicate that this sample wasexclusively female with a mean age � 28.7.Phase 2 of this study was excluded from thismeta-analysis, as there was no randomizedcontrol group in this phase of the study.
MGH-HS 21
4B
IOL
PSY
CH
IATRY
2007;xx:xxxM
.H.B
loch
eta
l.
ww
w.so
bp
.org
/jou
rnal
ARTICLE IN PRESS

le1
.(C
on
tin
ued
)
dy
IDSt
ud
yD
esig
nIn
terv
enti
on
Part
icip
ants
Ou
tco
me
QRS
Sco
re
od
set
al.2
006
(15)
cRa
nd
om
ized
,par
alle
l-g
rou
ptr
ial,
blin
ded
asse
ssm
ent
ofo
utc
om
e,w
ait-
list
con
tro
lled
12w
eeks
ofh
abit
-rev
ersa
ltra
inin
gp
lus
acce
pta
nce
and
com
mit
men
ttr
ain
ing
(10
sess
ion
s)vs
.12
wee
kso
fwai
t-lis
t
25co
mp
lete
rs(2
3w
om
en,a
ge
33.4
�9.
1ye
ars,
du
rati
on
ofi
llnes
s22
.7ye
ars)
ou
to
f28
adu
lts
wit
htr
ich
oti
llom
ania
.21
sub
ject
sd
rop
ped
ou
to
fth
eH
RTan
d1
sub
ject
ou
to
fth
ew
ait-
list
gro
up
NIM
H-T
IS29
Foo
tno
tes
inco
lum
n1
rep
rese
nt
the
ou
tco
mes
each
ind
ivid
ual
stu
dy
con
trib
ute
dto
the
ove
rall
met
a-an
alys
is.
HRT
,hab
it-r
ever
salt
her
apy;
MG
H-H
S,M
assa
chu
sett
sG
ener
alH
osp
ital
Hai
rpu
llin
gSc
ale;
NIM
H-T
IS,N
atio
nal
Inst
itu
teo
fMen
talH
ealt
hTr
ich
oti
llom
ania
Imp
airm
entS
cale
;NIM
H-T
SS,N
atio
nal
Inst
itu
teen
talH
ealt
hTr
ich
oti
llom
ania
Seve
rity
Scal
e;Q
RS,Q
ual
ity
Rati
ng
Scal
e;SS
RI,s
elec
tive
sero
ton
inre
up
take
inh
ibit
or.
aSS
RIvs
.pla
ceb
o.
bC
lom
ipra
min
evs
.pla
ceb
o.
c HRT
vs.w
ait-
list
con
tro
l.dH
RTvs
.SSR
I.f C
lom
ipra
min
evs
.SSR
I.eH
RTvs
.clo
mip
ram
ine.
M.H. Bloch et al. BIOL PSYCHIATRY 2007;xx:xxx 5
ARTICLE IN PRESS
(ES � �1.14, 95 CI � �1.89, �.38). Two of these threeindividual studies demonstrated a significant effect comparedwith wait-list or placebo on the primary outcome measure usedin this review. Van Minnen et al. (16) demonstrated a significantreduction in TTM severity according to the MGH-HS but not onblinded ratings of hair loss. Blinded rating of hair loss was usedas the primary outcome in this systematic review becauseMGH-HS ratings were not blinded to treatment assignment. Theforest plot demonstrating the results of this overall meta-analysisis depicted in Figure 3. This result remained significant in lastobservation carried forward sensitivity analysis (ES � �.97, 95CI � �1.48, �.47). No randomized controlled studies wereexcluded from this meta-analysis because the therapy studiedfailed to meet criteria of HRT.
Outcome 4: Habit-Reversal Therapy Versus SelectiveSerotonin Reuptake Inhibitors
Only one study, van Minnen et al. (16), compared HRT withSSRI in the treatment of trichotillomania. This study compared 11completers of 12 weeks of fluoxetine treatment with 14 compl-eters of six 45-minute, biweekly HRT sessions. Videotapedratings of hair loss by blinded clinicians were available for 9 of 11subjects in the fluoxetine group and for all 14 HRT completers.There was a trend toward a benefit of HRT compared with SSRIreported in this study (ES � �.73, 95% CI � �1.60, .14) on theonly blinded clinical rating of hair loss, which failed to reachstatistical significance. In this study, there were two dropouts inthe fluoxetine group and one dropout from HRT. Under lastobservation carried forward sensitivity analysis, this result alsofailed to reach statistical significance (ES � �.76, 95% CI ��1.53, .01). The main outcome measure of this study, theMGH-HS, a subject self-report measure rather than a rating byblinded clinician, was available on all 25 completers and dem-onstrated a larger and significant treatment effect (ES � �1.96,95% CI � �2.94, �.97) compared with the videotaped ratings ofhair loss conducted by blinded assessors.
Outcome 5: Habit-Reversal Therapy Versus ClomipramineNinan et al. (18) was the only study that compared HRT with
clomipramine. This study compared 6 (out of 10) completers of9 weeks of clomipramine treatment to 5 (out of 7) completers of9, 45-minute, weekly HRT sessions. This study found a statisti-cally significant benefit of HRT compared with clomipramine(ES � �1.74, 95% CI � �3.23, �.25). This result remainedsignificant even assuming last observation carried forward sen-sitivity analysis (ES � �1.20, 95% CI � �2.27, �.13).
Outcome 6: Clomipramine Versus Selective SerotoninReuptake Inhibitors
No blinded studies were found in the published scientificliterature that directly compared efficacy of these pharmacolog-ical agents. There was one scientific abstract presented on thissubject in 1993 (25). This abstract reported the results of a24-week, double-blind, randomized crossover study in 12 tricho-tillomania patients comparing 10 weeks of clomipramine treat-ment (mean dosage 200 � 15 mg) with 10 weeks of fluoxetine(mean dosage 75 � 5 mg) with a 4-week placebo washout phase.Both interventions demonstrated a reduction in trichotillomaniaseverity over time and there was no significant difference be-tween the efficacies of these two treatments. The exact data from
this study were not available or ever published.Tab
Stu
Wo
ofM
www.sobp.org/journal
D
wsHs�iapTdp�o�tmawibim4twp
ts
FifmspdwfNcm
6 BIOL PSYCHIATRY 2007;xx:xxx M.H. Bloch et al.
w
ARTICLE IN PRESS
iscussion
The findings of this systematic review demonstrate that HRT,hen practiced by experienced clinicians in academic research
ettings, is the most effective intervention for trichotillomania.abit-reversal therapy demonstrated the largest effect size of the
ystematically studied interventions (ES � �1.14, 95% CI �1.89, �.38). Furthermore, HRT demonstrated superiority in
ndividual study trials when compared with the two most prev-lent pharmacological interventions for trichotillomania: clomi-ramine (17) and SSRI (on self-report but not blinded ratings ofTM severity) (16). In the current meta-analysis, clomipramineemonstrated efficacy for trichotillomania when compared withlacebo or active control conditions (ES � �.68, 95% CI �1.28, �.07), while there was no evidence to suggest a benefitf SSRI compared with control conditions (ES � .02, 95% CI �.32, .35). This conclusion is at odds with recent reviews of this
opic in high-profile specialty journals where SSRI are recom-ended as a first line of pharmacological treatment (4). The
dditional noradrenergic activity of clomipramine comparedith SSRI may be responsible for this demonstrated efficacy. The
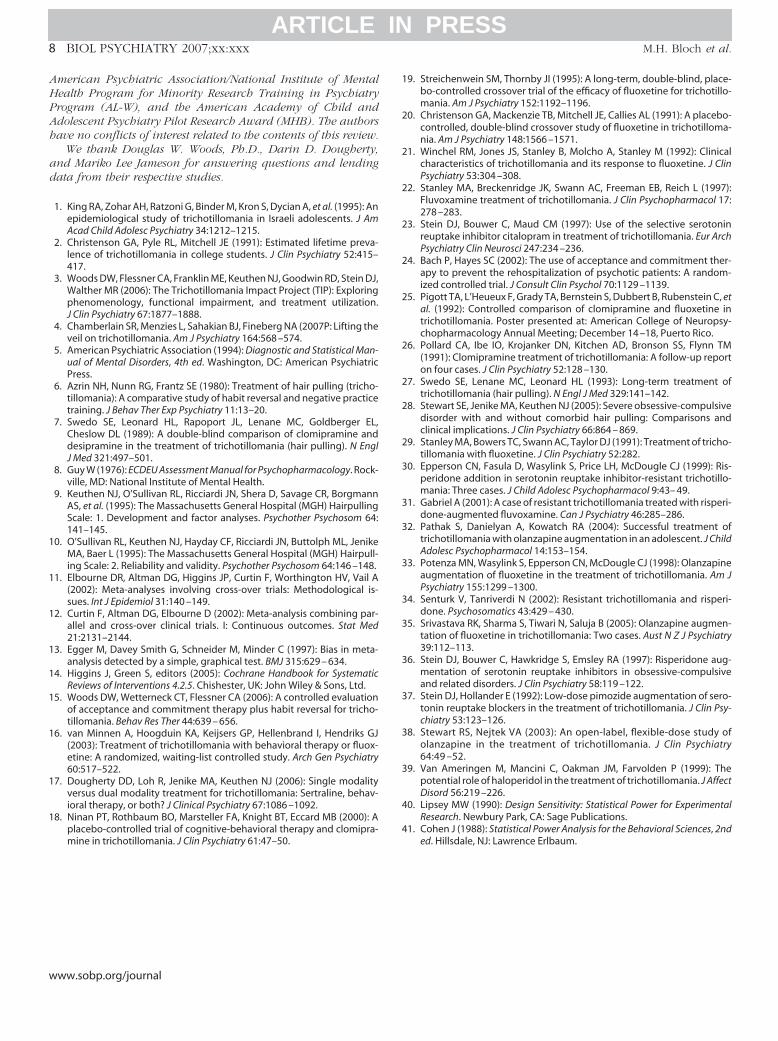
mproved short-term treatment effects of clomipramine shoulde viewed with some caution, as there is some evidence that thenitial benefits obtained with clomipramine in trichotillomaniaay not be maintained with long-term treatment (26,27). Figuredepicts the relative effect sizes of each intervention for
richotillomania when compared with control conditions. Thereas no evidence of significant heterogeneity between studies orublication bias in the results presented in this meta-analysis.
There were methodological limitations of the included trialshat may influence the conclusions of this systematic review. Noingle clinical rating instrument was used consistently to assess
igure 2. Clomipramine versus placebon the treatment of trichotillomania. Aorest plot comparing standardized
ean difference of trichotillomaniaymptom severity in clomipramine com-ared with placebo. Swedo et al. (7) usedesipramine, a tricyclic antidepressantith no proven or hypothesized efficacy
or trichotillomania, as an active placebo.inan et al. (18) used inactive placebo. CI,onfidence interval; SMD, standardizedean difference.
ww.sobp.org/journal
severity and improvement of trichotillomania symptoms amongincluded studies. This problem exists because there is not asingle clinically administered rating scale that has been validatedfor use in trichotillomania. We accounted for this problem byusing standardized mean difference as our main outcome mea-sure and a random effects model to combine results from clinicaltrials. However, it is quite possible that the different and uncon-firmed rating scales used in this study may have a differentsensitivity to changes in trichotillomania severity, which is un-known and thus cannot be accounted for using statistical meth-odology. Most clinical trials of trichotillomania neglected toreport the number of patients with comorbid OCD. Obsessive-compulsive disorder and trichotillomania are highly comorbidconditions (28), and it is likely that trichotillomania patients withcomorbid OCD would be more likely to respond to SSRI andclomipramine, since these medications are first-line treatment forOCD. All of the parallel-group trials included in this systematicreview analyzed trial completers only, violating the intention-to-treat principle. This destroys the assumption that the randomiza-tion process will create groups identical in both known andunknown confounders, since noncompleters may differ in prog-nostic factors between treatment groups and from study compl-eters. We attempted to account for this potential problem in theincluded trials by conducting last observation carried forwardsensitivity analysis in which study dropouts were assumed tohave no improvement in symptoms during the course of thestudy. These sensitivity analyses did not alter the original con-clusions of our review. However, it is quite possible thatdropouts differed between the intervention and control condi-tions. Last observation carried forward sensitivity analysis doesnot completely account for this possibility.
Figure 1. SSRIs versus placebo in thetreatment of trichotillomania. A forestplot comparing standardized mean dif-ference of trichotillomania symptomseverity in SSRIs. CI, confidence inter-val; SMD, standardized mean differ-ence; SSRI, selective serotonin re-uptake inhibitors.
mwttmntwpd(o9dfiwadf(tSTd
Ftsvrsu
M.H. Bloch et al. BIOL PSYCHIATRY 2007;xx:xxx 7
ARTICLE IN PRESS
These limitations would likely bias previous studies and oureta-analysis toward overestimating treatment effects. However,e found no difference between SSRI and placebo for the
reatment of trichotillomania. There are three possible explana-ions for this finding: 1) the specific SSRI included in thiseta-analysis are not effective in the treatment of trichotilloma-ia, 2) the negative result was due to false-negative error, or 3)he length of SSRI treatment for studies included in this reviewere not sufficient to induce a clinical response. Although theower of individualized studies to detect a moderate treatmentifference (ES � .5) between SSRI and placebo were smallranging from 33% to 55% assuming � � .05), the overall powerf this meta-analysis to detect a moderate treatment effect was7%, making false-negative error unlikely. The length of maximalose SSRI treatment for included studies in this review rangedrom 2 to 11 weeks, and there is evidence from open-label trialsn trichotillomania (29) that symptoms may improve sometimesith prolonged SSRI therapy. However, there was no evidence oftherapeutic benefit of SSRI, even in the longer duration
ouble-blind trials, thus the most likely explanation for ourindings is that the specific SSRI included in this meta-analysisfluoxetine and sertraline) are ineffective for the treatment ofrichotillomania. Further research is needed to determine if otherSRI, such as citalopram, that have suggested possible efficacy inTM are truly effective under double-blind conditions (23). Theemonstrated lack of efficacy of SSRI in double-blind trials of
igure 4. Effect sizes of HRT, clomipramine, and SSRI. Circles representhe point estimate (and lines the 95% confidence intervals) for effectizes for each of these interventions from the comparison of this inter-ention with respect to placebo in this meta-analysis. Shaded regionsepresent general clinical standards for small, medium, and large effectizes (40,41). HRT, habit-reversal therapy; SSRI, selective serotonin re-
ptake inhibitor.TTM should have important clinical and policy implications,given that the Trichotillomania Impact Project, a survey of 1697individuals with TTM, found that SSRI pharmacotherapy is stillthe most commonly utilized treatment intervention for TTM (3).
There are still many important clinical questions that remainto be answered in the treatment of trichotillomania: 1) althoughHRT has demonstrated efficacy in trichotillomania when com-pared with wait-list and placebo control conditions, it remains tobe determined if HRT will demonstrate efficacy when comparedwith control conditions that account for the nonspecific effects oftherapy such as time spent with the therapist (i.e., supportivepsychotherapy and psychoeducation); 2) it also remains to bedetermined if HRT can be translated into an effective interventionto be utilized successfully by clinicians less familiar with tricho-tillomania at multiple treatment centers; and 3) double-blindstudies are needed to evaluate efficacy of other potentiallybeneficial pharmacological treatments for trichotillomania. Giventhe moderate efficacy of clomipramine, an agent with bothserotonergic and noradrenergic activity, further double-blindstudies evaluating the efficacy of other agents with similarpharmacodynamic activity and fewer side effects, such as ven-lafaxine and duloxetine, might be useful. There are also multiplecase reports and case series reporting favorable responses toantipsychotics as monotherapy and augmentation agents in thescientific literature (30–39). Since hair pulling and tics bothinvolve involuntary repetitive behaviors that reduce feelings oftension and discomfort, it is not unreasonable to hypothesize thatantipsychotics, the most beneficial treatment for Tourette syn-drome, might also be beneficial in treating trichotillomania (39).Improved clinical trials methodology including honoring theintention-to-treat principle in analysis, using validated clinicalrating scales of symptom severity, and conducting higher pow-ered trials will help us identify the most effective treatments forour patients. Due to the rarity of trichotillomania cases reachingclinical presentation, these improvements in trial quality mayonly be possible through multicenter efforts.
We acknowledge the National Institute of Mental Healthsupport of the Yale Child Study Center Research Training Pro-gram (MHB) and the Yale Department of Psychiatry Neuro-science Research Training Program (CP), the National Institutesof Health Loan Repayment Program (MHB, VC), the support ofthe Tourette Syndrome Association Inc. (MHB), the support of theObsessive Compulsive Foundation (VC), the National Alliancefor Research on Schizophrenia and Depression Young Investiga-tor Award 2005 (VC), and the support of the American Psychi-
Figure 3. HRT versus wait-list controlconditions in the treatment of trichotil-lomania. A forest plot comparing stan-dardized mean difference of trichotillo-mania symptom severity in HRTcompared with wait-list control condi-tions. CI, confidence interval; HRT,habit-reversal therapy; SMD, standard-ized mean difference.
atric Association/Janssen Research Scholars Program (MHB), the
www.sobp.org/journal
AHPAh
ad
1
1
1
1
1
1
1
1
1
8 BIOL PSYCHIATRY 2007;xx:xxx M.H. Bloch et al.
w
ARTICLE IN PRESS
merican Psychiatric Association/National Institute of Mentalealth Program for Minority Research Training in Psychiatryrogram (AL-W), and the American Academy of Child anddolescent Psychiatry Pilot Research Award (MHB). The authorsave no conflicts of interest related to the contents of this review.
We thank Douglas W. Woods, Ph.D., Darin D. Dougherty,nd Mariko Lee Jameson for answering questions and lendingata from their respective studies.
1. King RA, Zohar AH, Ratzoni G, Binder M, Kron S, Dycian A, et al. (1995): Anepidemiological study of trichotillomania in Israeli adolescents. J AmAcad Child Adolesc Psychiatry 34:1212–1215.
2. Christenson GA, Pyle RL, Mitchell JE (1991): Estimated lifetime preva-lence of trichotillomania in college students. J Clin Psychiatry 52:415–417.
3. Woods DW, Flessner CA, Franklin ME, Keuthen NJ, Goodwin RD, Stein DJ,Walther MR (2006): The Trichotillomania Impact Project (TIP): Exploringphenomenology, functional impairment, and treatment utilization.J Clin Psychiatry 67:1877–1888.
4. Chamberlain SR, Menzies L, Sahakian BJ, Fineberg NA (2007P: Lifting theveil on trichotillomania. Am J Psychiatry 164:568 –574.
5. American Psychiatric Association (1994): Diagnostic and Statistical Man-ual of Mental Disorders, 4th ed. Washington, DC: American PsychiatricPress.
6. Azrin NH, Nunn RG, Frantz SE (1980): Treatment of hair pulling (tricho-tillomania): A comparative study of habit reversal and negative practicetraining. J Behav Ther Exp Psychiatry 11:13–20.
7. Swedo SE, Leonard HL, Rapoport JL, Lenane MC, Goldberger EL,Cheslow DL (1989): A double-blind comparison of clomipramine anddesipramine in the treatment of trichotillomania (hair pulling). N EnglJ Med 321:497–501.
8. Guy W (1976): ECDEU Assessment Manual for Psychopharmacology. Rock-ville, MD: National Institute of Mental Health.
9. Keuthen NJ, O’Sullivan RL, Ricciardi JN, Shera D, Savage CR, BorgmannAS, et al. (1995): The Massachusetts General Hospital (MGH) HairpullingScale: 1. Development and factor analyses. Psychother Psychosom 64:141–145.
0. O’Sullivan RL, Keuthen NJ, Hayday CF, Ricciardi JN, Buttolph ML, JenikeMA, Baer L (1995): The Massachusetts General Hospital (MGH) Hairpull-ing Scale: 2. Reliability and validity. Psychother Psychosom 64:146 –148.
1. Elbourne DR, Altman DG, Higgins JP, Curtin F, Worthington HV, Vail A(2002): Meta-analyses involving cross-over trials: Methodological is-sues. Int J Epidemiol 31:140 –149.
2. Curtin F, Altman DG, Elbourne D (2002): Meta-analysis combining par-allel and cross-over clinical trials. I: Continuous outcomes. Stat Med21:2131–2144.
3. Egger M, Davey Smith G, Schneider M, Minder C (1997): Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629 – 634.
4. Higgins J, Green S, editors (2005): Cochrane Handbook for SystematicReviews of Interventions 4.2.5. Chishester, UK: John Wiley & Sons, Ltd.
5. Woods DW, Wetterneck CT, Flessner CA (2006): A controlled evaluationof acceptance and commitment therapy plus habit reversal for tricho-tillomania. Behav Res Ther 44:639 – 656.
6. van Minnen A, Hoogduin KA, Keijsers GP, Hellenbrand I, Hendriks GJ(2003): Treatment of trichotillomania with behavioral therapy or fluox-etine: A randomized, waiting-list controlled study. Arch Gen Psychiatry60:517–522.
7. Dougherty DD, Loh R, Jenike MA, Keuthen NJ (2006): Single modalityversus dual modality treatment for trichotillomania: Sertraline, behav-ioral therapy, or both? J Clinical Psychiatry 67:1086 –1092.
8. Ninan PT, Rothbaum BO, Marsteller FA, Knight BT, Eccard MB (2000): A
placebo-controlled trial of cognitive-behavioral therapy and clomipra-mine in trichotillomania. J Clin Psychiatry 61:47–50.ww.sobp.org/journal
19. Streichenwein SM, Thornby JI (1995): A long-term, double-blind, place-bo-controlled crossover trial of the efficacy of fluoxetine for trichotillo-mania. Am J Psychiatry 152:1192–1196.
20. Christenson GA, Mackenzie TB, Mitchell JE, Callies AL (1991): A placebo-controlled, double-blind crossover study of fluoxetine in trichotilloma-nia. Am J Psychiatry 148:1566 –1571.
21. Winchel RM, Jones JS, Stanley B, Molcho A, Stanley M (1992): Clinicalcharacteristics of trichotillomania and its response to fluoxetine. J ClinPsychiatry 53:304 –308.
22. Stanley MA, Breckenridge JK, Swann AC, Freeman EB, Reich L (1997):Fluvoxamine treatment of trichotillomania. J Clin Psychopharmacol 17:278 –283.
23. Stein DJ, Bouwer C, Maud CM (1997): Use of the selective serotoninreuptake inhibitor citalopram in treatment of trichotillomania. Eur ArchPsychiatry Clin Neurosci 247:234 –236.
24. Bach P, Hayes SC (2002): The use of acceptance and commitment ther-apy to prevent the rehospitalization of psychotic patients: A random-ized controlled trial. J Consult Clin Psychol 70:1129 –1139.
25. Pigott TA, L’Heueux F, Grady TA, Bernstein S, Dubbert B, Rubenstein C, etal. (1992): Controlled comparison of clomipramine and fluoxetine intrichotillomania. Poster presented at: American College of Neuropsy-chopharmacology Annual Meeting; December 14 –18, Puerto Rico.
26. Pollard CA, Ibe IO, Krojanker DN, Kitchen AD, Bronson SS, Flynn TM(1991): Clomipramine treatment of trichotillomania: A follow-up reporton four cases. J Clin Psychiatry 52:128 –130.
27. Swedo SE, Lenane MC, Leonard HL (1993): Long-term treatment oftrichotillomania (hair pulling). N Engl J Med 329:141–142.
28. Stewart SE, Jenike MA, Keuthen NJ (2005): Severe obsessive-compulsivedisorder with and without comorbid hair pulling: Comparisons andclinical implications. J Clin Psychiatry 66:864 – 869.
29. Stanley MA, Bowers TC, Swann AC, Taylor DJ (1991): Treatment of tricho-tillomania with fluoxetine. J Clin Psychiatry 52:282.
30. Epperson CN, Fasula D, Wasylink S, Price LH, McDougle CJ (1999): Ris-peridone addition in serotonin reuptake inhibitor-resistant trichotillo-mania: Three cases. J Child Adolesc Psychopharmacol 9:43– 49.
31. Gabriel A (2001): A case of resistant trichotillomania treated with risperi-done-augmented fluvoxamine. Can J Psychiatry 46:285–286.
32. Pathak S, Danielyan A, Kowatch RA (2004): Successful treatment oftrichotillomania with olanzapine augmentation in an adolescent. J ChildAdolesc Psychopharmacol 14:153–154.
33. Potenza MN, Wasylink S, Epperson CN, McDougle CJ (1998): Olanzapineaugmentation of fluoxetine in the treatment of trichotillomania. Am JPsychiatry 155:1299 –1300.
34. Senturk V, Tanriverdi N (2002): Resistant trichotillomania and risperi-done. Psychosomatics 43:429 – 430.
35. Srivastava RK, Sharma S, Tiwari N, Saluja B (2005): Olanzapine augmen-tation of fluoxetine in trichotillomania: Two cases. Aust N Z J Psychiatry39:112–113.
36. Stein DJ, Bouwer C, Hawkridge S, Emsley RA (1997): Risperidone aug-mentation of serotonin reuptake inhibitors in obsessive-compulsiveand related disorders. J Clin Psychiatry 58:119 –122.
37. Stein DJ, Hollander E (1992): Low-dose pimozide augmentation of sero-tonin reuptake blockers in the treatment of trichotillomania. J Clin Psy-chiatry 53:123–126.
38. Stewart RS, Nejtek VA (2003): An open-label, flexible-dose study ofolanzapine in the treatment of trichotillomania. J Clin Psychiatry64:49 –52.
39. Van Ameringen M, Mancini C, Oakman JM, Farvolden P (1999): Thepotential role of haloperidol in the treatment of trichotillomania. J AffectDisord 56:219 –226.
40. Lipsey MW (1990): Design Sensitivity: Statistical Power for ExperimentalResearch. Newbury Park, CA: Sage Publications.
41. Cohen J (1988): Statistical Power Analysis for the Behavioral Sciences, 2nded. Hillsdale, NJ: Lawrence Erlbaum.
Related Documents











