Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: an update to the obesity guidance produced by the National Institute for Health and Clinical Excellence T. Brown 1 and C. Summerbell 2 1 School of Health and Social Care, University of Teesside, Middlesbrough; 2 School for Medicine and Health, Wolfson Research Institute, Durham University, Stockton on Tees, UK Received 18 December 2007; revised 8 May 2008; accepted 27 June 2008 Address for correspondence: C Summerbell, School for Medicine and Health, Wolfson Research Institute, Durham University, Stockton on Tees, UK TS17 6BH, UK. E-mail: [email protected] Summary To determine the effectiveness of school-based interventions that focus on chang- ing dietary intake and physical activity levels to prevent childhood obesity. MEDLINE and EMBASE were searched (January 2006 to September 2007) for controlled trials of school-based lifestyle interventions, minimum duration of 12 weeks, reporting weight outcome. Thirty-eight studies were included; 15 new studies and 23 studies included within the National Institute for Health and Clinical Excellence obesity guidance. One of three diet studies, five of 15 physical activity studies and nine of 20 combined diet and physical activity studies dem- onstrated significant and positive differences between intervention and control for body mass index. There is insufficient evidence to assess the effectiveness of dietary interventions or diet vs. physical activity interventions. School-based physical activity interventions may help children maintain a healthy weight but the results are inconsistent and short-term. Physical activity interventions may be more successful in younger children and in girls. Studies were heterogeneous, making it difficult to generalize about what interventions are effective. The find- ings are inconsistent, but overall suggest that combined diet and physical activity school-based interventions may help prevent children becoming overweight in the long term. Physical activity interventions, particularly in girls in primary schools, may help to prevent these children from becoming overweight in the short term. Keywords: Children, obesity, prevention, systematic review. obesity reviews (2009) 10, 110–141 Introduction In developed countries, the prevalence of obesity among children is increasing (1). In addition, obesity in childhood is known to be an independent risk factor for adult obesity (2). Therefore, there is a need to develop interventions to reduce the prevalence of obesity in children. Because there is good evidence that obesity is related to the energy content of the diet and an increasingly sedentary lifestyle, these interventions should focus on changing these behav- iours. Schools have been a popular setting for implemen- tation of interventions, as they offer continuous, intensive contact with children. School infrastructure and physical environment, policies, curricula and staff have potential to positively influence child health. However, despite the apparent advantages of addressing childhood obesity in a school setting, a relative lack of effectiveness of a number of major interventions to reduce childhood obesity has brought into question the wisdom of allocating scarce resources to school-based interventions. obesity reviews doi: 10.1111/j.1467-789X.2008.00515.x 110 © 2008 The Authors Journal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Systematic review of school-based interventions thatfocus on changing dietary intake and physical activitylevels to prevent childhood obesity: an update to theobesity guidance produced by the National Institutefor Health and Clinical Excellence
T. Brown1 and C. Summerbell2
1School of Health and Social Care, University
of Teesside, Middlesbrough; 2School for
Medicine and Health, Wolfson Research
Institute, Durham University, Stockton on Tees,
UK
Received 18 December 2007; revised 8 May
2008; accepted 27 June 2008
Address for correspondence: C Summerbell,
School for Medicine and Health, Wolfson
Research Institute, Durham University,
Stockton on Tees, UK TS17 6BH, UK. E-mail:
SummaryTo determine the effectiveness of school-based interventions that focus on chang-ing dietary intake and physical activity levels to prevent childhood obesity.MEDLINE and EMBASE were searched (January 2006 to September 2007) forcontrolled trials of school-based lifestyle interventions, minimum duration of12 weeks, reporting weight outcome. Thirty-eight studies were included; 15 newstudies and 23 studies included within the National Institute for Health andClinical Excellence obesity guidance. One of three diet studies, five of 15 physicalactivity studies and nine of 20 combined diet and physical activity studies dem-onstrated significant and positive differences between intervention and controlfor body mass index. There is insufficient evidence to assess the effectiveness ofdietary interventions or diet vs. physical activity interventions. School-basedphysical activity interventions may help children maintain a healthy weight butthe results are inconsistent and short-term. Physical activity interventions may bemore successful in younger children and in girls. Studies were heterogeneous,making it difficult to generalize about what interventions are effective. The find-ings are inconsistent, but overall suggest that combined diet and physical activityschool-based interventions may help prevent children becoming overweight in thelong term. Physical activity interventions, particularly in girls in primary schools,may help to prevent these children from becoming overweight in the short term.
Keywords: Children, obesity, prevention, systematic review.
obesity reviews (2009) 10, 110–141
Introduction
In developed countries, the prevalence of obesity amongchildren is increasing (1). In addition, obesity in childhoodis known to be an independent risk factor for adult obesity(2). Therefore, there is a need to develop interventions toreduce the prevalence of obesity in children. Because thereis good evidence that obesity is related to the energycontent of the diet and an increasingly sedentary lifestyle,these interventions should focus on changing these behav-
iours. Schools have been a popular setting for implemen-tation of interventions, as they offer continuous, intensivecontact with children. School infrastructure and physicalenvironment, policies, curricula and staff have potential topositively influence child health. However, despite theapparent advantages of addressing childhood obesity in aschool setting, a relative lack of effectiveness of a numberof major interventions to reduce childhood obesity hasbrought into question the wisdom of allocating scarceresources to school-based interventions.
obesity reviews doi: 10.1111/j.1467-789X.2008.00515.x
110 © 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

In 2004, the National Institute for Health and ClinicalExcellence (NICE) commissioned the Institute for HealthSciences and Social Care at the University of Teesside tocarry out a series of rapid reviews on the prevention ofoverweight and obesity. These reviews formed part of thesupporting evidence for the NICE obesity guidance (3).This systematic review aimed to examine new researchevidence and update the review of interventions for theprevention of overweight and obesity in school children,contained within the NICE obesity guidance (3).
The main objective of this review was to determine theeffectiveness of interventions that focus on improving dietand physical activity (PA) behaviours in school children. Asecondary aim was to identify study characteristics thatmay affect outcome such as gender, age, socioeconomicstatus, setting, process indicators and contextual factors.
Methods
Study inclusion criteria were identical to the criteria usedwithin the NICE obesity guidance (3), with one exception:this review only includes studies that reported a weightoutcome. Weight could be presented as change or absolutevalues (at baseline and follow-up) and could include anymeasure of weight, including but not restricted to, bodymass index (BMI), BMI z-score, percentage of body fat,skin-fold thickness and percentage of overweight. A studywas included if the design was a randomized controlledtrial or controlled clinical trial, of a lifestyle intervention,set in schools and at least 12 weeks of duration. School-aged children, 5–18 years old, were included. Study designsthat compared lifestyle interventions with usual care orwith other active interventions were included.
A lifestyle intervention was defined as including healthyeating, increase in PA, reduction in sedentary behaviours,behaviour therapy, social support and education for dietand activity behaviours. Studies were only included if thestudy did not recruit children on the basis of weight (or anyother measure of weight). Studies were not included orexcluded based on the aim of the study. Studies were notexcluded on the basis of language. Studies in children withcritical illness or eating disorders were excluded.
The interventions, lumped within each comparison (diet,PA, diet plus PA), could vary by mode of delivery andcontent. This would facilitate comparison of whether lessexpensive and more easily feasible interventions were aseffective as more expensive interventions that involvedgreat expense and effort.
The search strategy was identical to that used for theNICE obesity guidance (3). The electronic databases,MEDLINE and EMBASE, were searched on 25 September2007 – from January 2006 to September 2006, week 2(MEDLINE) and week 38 (EMBASE). Copies of the fullsearch strategies are available on request. All references
identified in the searches were electronically imported intothe reference managing software. All titles and abstractswere initially screened for inclusion by one researcher(TJB). The full text of references identified as potentiallyrelevant or references that could not be rejected with cer-tainty were obtained and assessed independently by tworeviewers (TJB, CS) using the predefined inclusion criteria.Differences between reviewers regarding assessment of fulltexts were resolved by discussion. The reference lists ofthese studies were checked for other relevant studies.
Data extraction was performed by one reviewer (TJB).Details were extracted regarding study design, setting, par-ticipants, aim, intervention, duration, sample size, dropout,change in BMI (or other weight outcome howeverreported), potential confounders and process indicators.
Data from the studies identified in the update searchwere integrated with data from the trials that fit the inclu-sion criteria and were included in the review of interven-tions for the prevention of overweight and obesity in schoolchildren, contained within the NICE obesity guidance (3).
When absolute values for weight or BMI were reported,the change was calculated by subtracting values at baselinefrom values at follow-up.
Results
Literature search
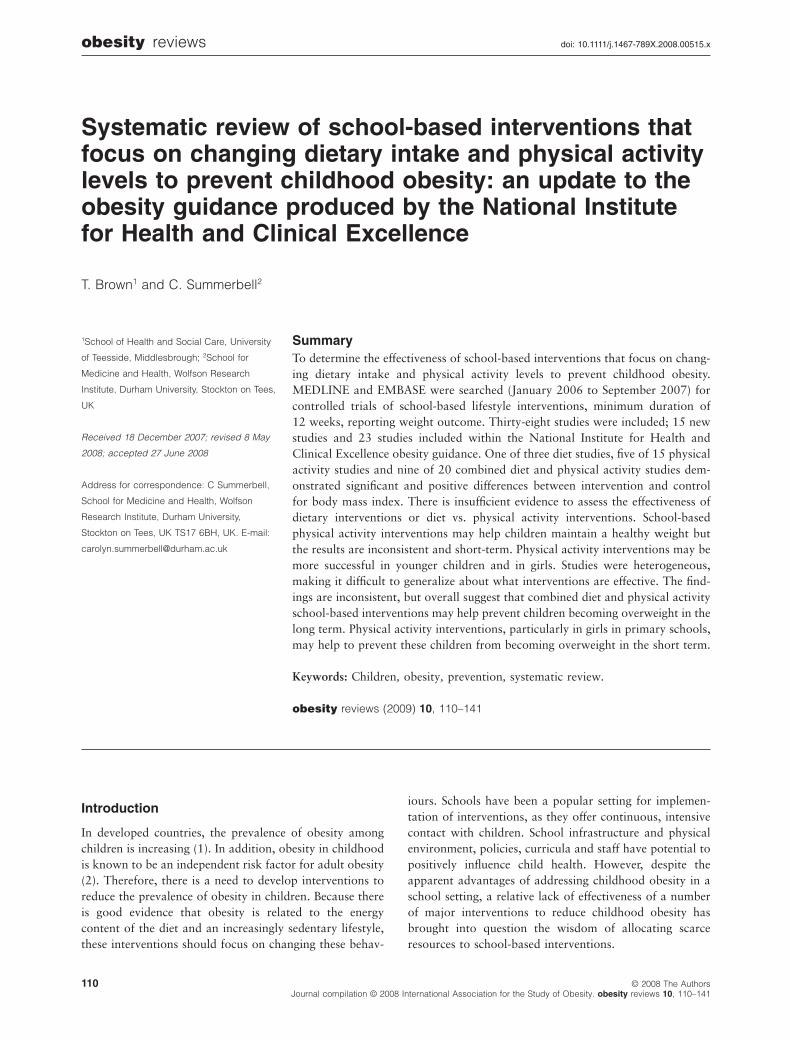
Seven hundred and thirteen references were identified inMEDLINE and 840 in EMBASE. Initial screening of thereferences produced 70 potentially relevant referenceswhich were obtained as full papers. Fifteen new studies(4–20) were included and two additional papers (21,22)provided longer term follow-up data for two studies (23–26) included within the NICE obesity guidance (3).Twenty-three studies (23–50) were included from the NICEobesity guidance (3) (Fig. 1).
Five studies that fit the inclusion criteria for this reviewbut do not currently have a weight outcome published wereidentified. These are the ‘Intervention centered on adoles-cents’ PA and sedentary behaviour’ study (51), the Kinder-Sportstudie (52), the ‘5-2-1 Go!’ study (53), the ‘JUMP-in’study (54) and the Trial of Activity for Adolescent Girls(55).
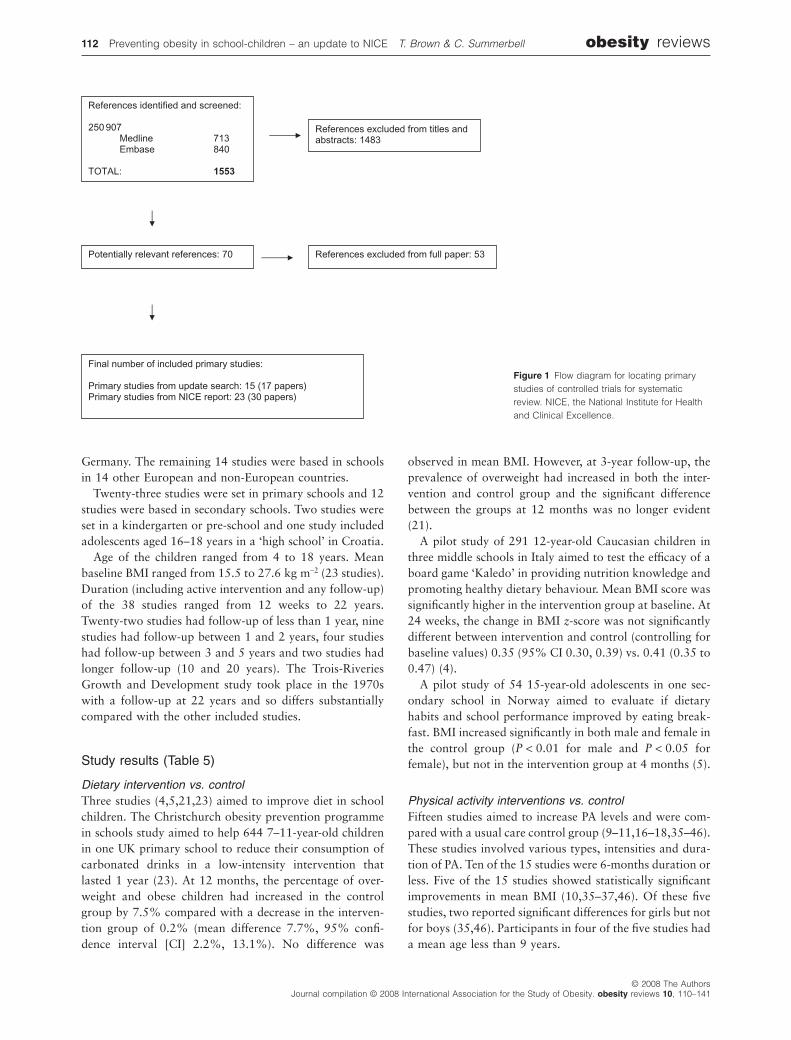
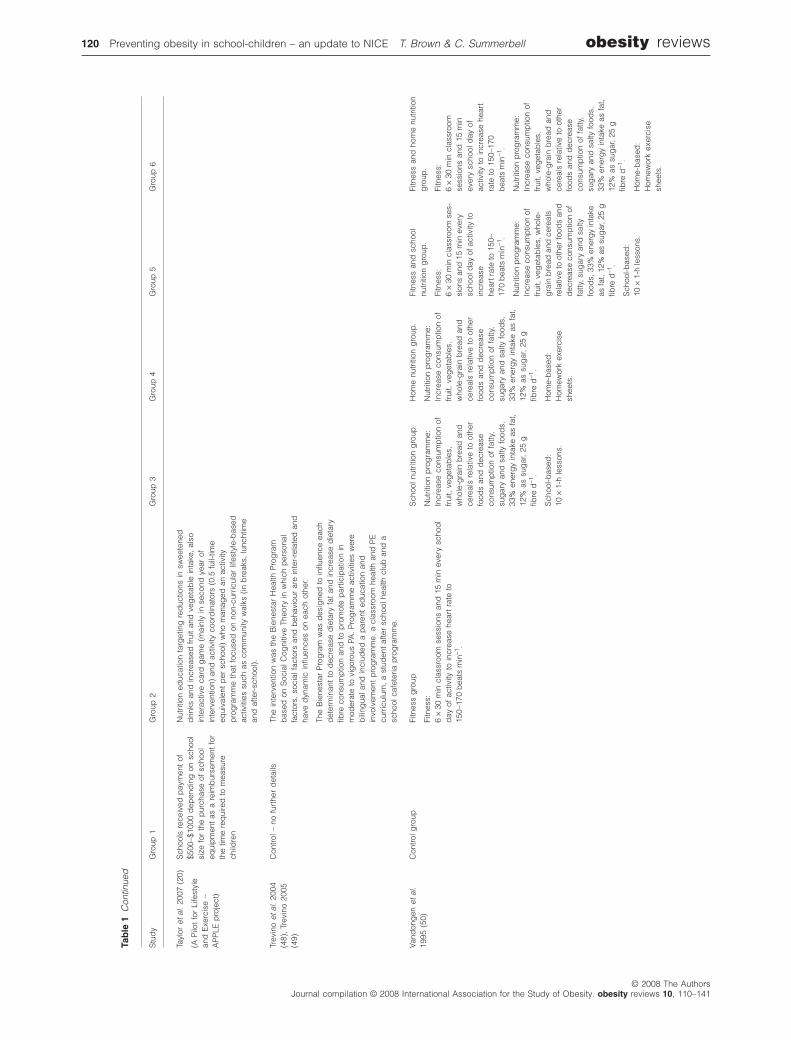
Three studies (4,5,21,23) were dietary interventions(Tables 1 and 2), 15 studies were PA interventions(9–11,16–18,35–46) (Tables 1 and 3) and 20 studies(6–8,12–15,19,20,22,24–34,47–50) were combined dietand PA interventions (Tables 1 and 4), of which five aimedto improve cardiovascular health or reduce the risk ofdiabetes.
Seventeen of the 38 studies were conducted in Americanschools, three were based in UK primary schools, and twowere set in Australian schools and two in schools in
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 111
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141
Germany. The remaining 14 studies were based in schoolsin 14 other European and non-European countries.
Twenty-three studies were set in primary schools and 12studies were based in secondary schools. Two studies wereset in a kindergarten or pre-school and one study includedadolescents aged 16–18 years in a ‘high school’ in Croatia.
Age of the children ranged from 4 to 18 years. Meanbaseline BMI ranged from 15.5 to 27.6 kg m-2 (23 studies).Duration (including active intervention and any follow-up)of the 38 studies ranged from 12 weeks to 22 years.Twenty-two studies had follow-up of less than 1 year, ninestudies had follow-up between 1 and 2 years, four studieshad follow-up between 3 and 5 years and two studies hadlonger follow-up (10 and 20 years). The Trois-RiveriesGrowth and Development study took place in the 1970swith a follow-up at 22 years and so differs substantiallycompared with the other included studies.
Study results (Table 5)
Dietary intervention vs. controlThree studies (4,5,21,23) aimed to improve diet in schoolchildren. The Christchurch obesity prevention programmein schools study aimed to help 644 7–11-year-old childrenin one UK primary school to reduce their consumption ofcarbonated drinks in a low-intensity intervention thatlasted 1 year (23). At 12 months, the percentage of over-weight and obese children had increased in the controlgroup by 7.5% compared with a decrease in the interven-tion group of 0.2% (mean difference 7.7%, 95% confi-dence interval [CI] 2.2%, 13.1%). No difference was
observed in mean BMI. However, at 3-year follow-up, theprevalence of overweight had increased in both the inter-vention and control group and the significant differencebetween the groups at 12 months was no longer evident(21).
A pilot study of 291 12-year-old Caucasian children inthree middle schools in Italy aimed to test the efficacy of aboard game ‘Kaledo’ in providing nutrition knowledge andpromoting healthy dietary behaviour. Mean BMI score wassignificantly higher in the intervention group at baseline. At24 weeks, the change in BMI z-score was not significantlydifferent between intervention and control (controlling forbaseline values) 0.35 (95% CI 0.30, 0.39) vs. 0.41 (0.35 to0.47) (4).
A pilot study of 54 15-year-old adolescents in one sec-ondary school in Norway aimed to evaluate if dietaryhabits and school performance improved by eating break-fast. BMI increased significantly in both male and female inthe control group (P < 0.01 for male and P < 0.05 forfemale), but not in the intervention group at 4 months (5).
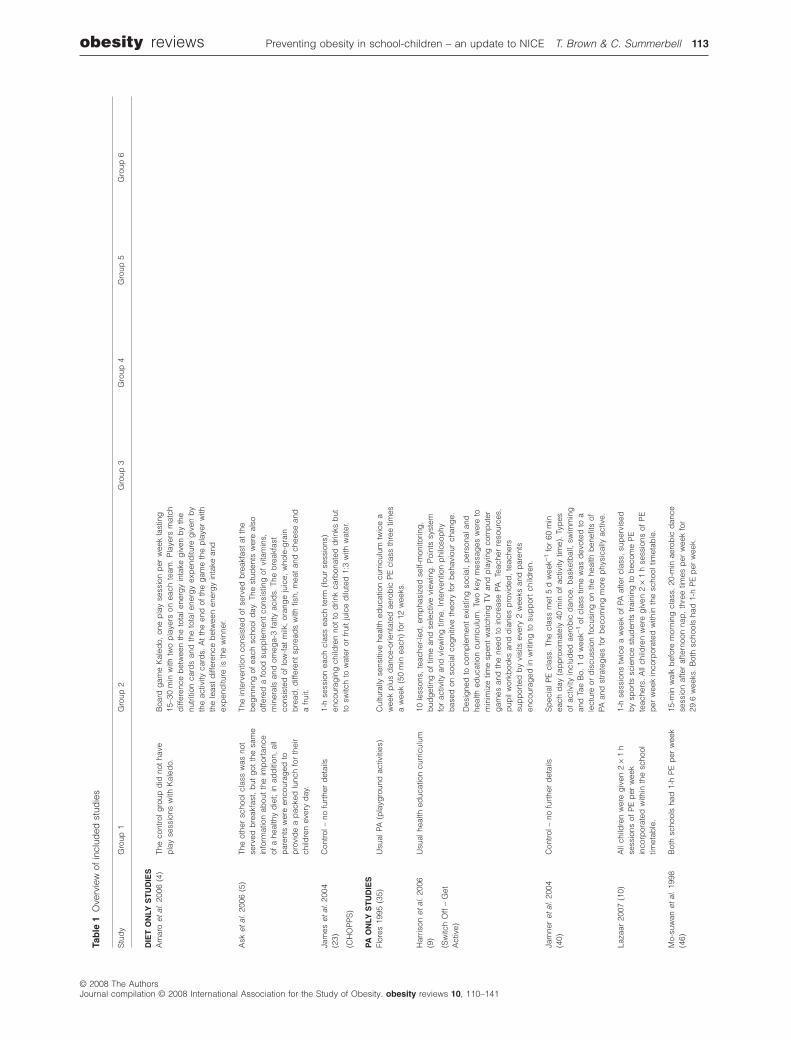
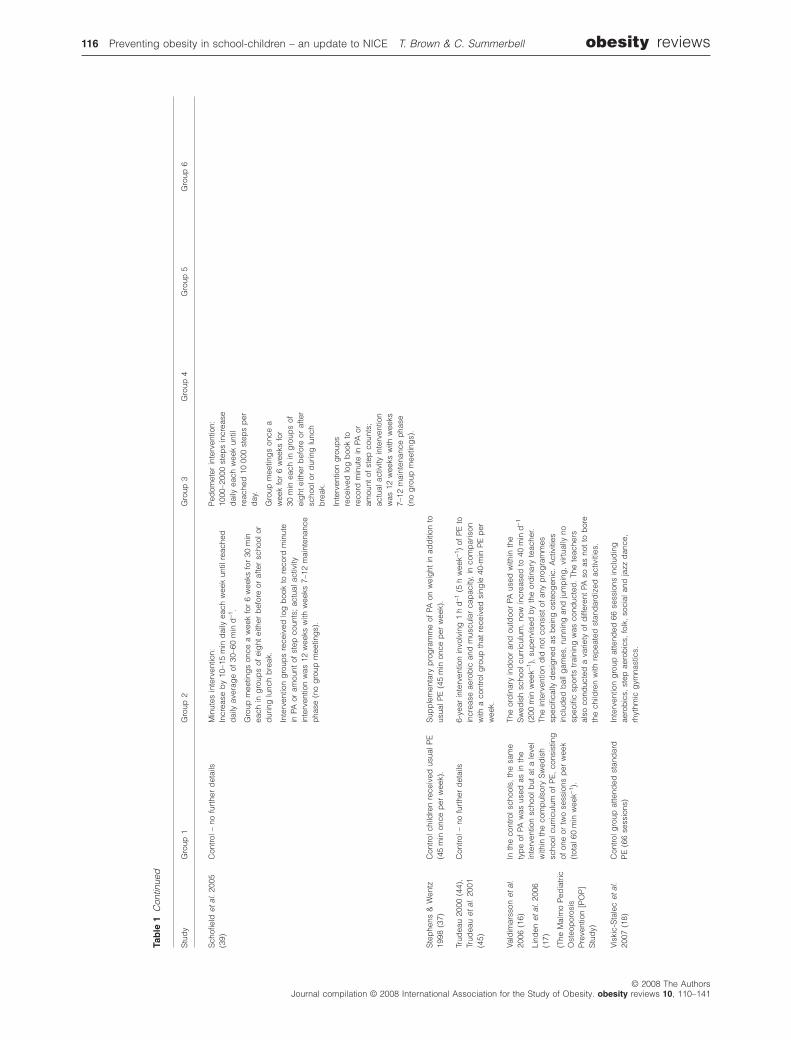
Physical activity interventions vs. controlFifteen studies aimed to increase PA levels and were com-pared with a usual care control group (9–11,16–18,35–46).These studies involved various types, intensities and dura-tion of PA. Ten of the 15 studies were 6-months duration orless. Five of the 15 studies showed statistically significantimprovements in mean BMI (10,35–37,46). Of these fivestudies, two reported significant differences for girls but notfor boys (35,46). Participants in four of the five studies hada mean age less than 9 years.
References identified and screened:
250 907Medline 713
Embase 840
TOTAL: 1553
References excluded from titles and abstracts: 1483
Potentially relevant references: 70 References excluded from full paper: 53
Final number of included primary studies:
Primary studies from update search: 15 (17 papers) Primary studies from NICE report: 23 (30 papers)
Figure 1 Flow diagram for locating primarystudies of controlled trials for systematicreview. NICE, the National Institute for Healthand Clinical Excellence.
112 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141
Tab
le1
Ove
rvie
wof
incl
uded
stud
ies
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
DIE
TO
NLY
ST
UD
IES
Am
aro
etal
.20
06(4
)Th
eco
ntro
lgro
upd
idno
tha
vep
lay
sess
ions
with
Kal
edo.
Boa
rdg
ame
Kal
edo,
one
pla
yse
ssio
np
erw
eek
last
ing
15–3
0m
inw
ithtw
op
laye
rson
each
team
.P
laye
rsm
atch
diff
eren
ceb
etw
een
the
tota
lene
rgy
inta
keg
iven
by
the
nutr
ition
card
san
dth
eto
tale
nerg
yex
pen
ditu
reg
iven
by
the
activ
ityca
rds.
At
the
end
ofth
eg
ame
the
pla
yer
with
the
leas
td
iffer
ence
bet
wee
nen
erg
yin
take
and
exp
end
iture
isth
ew
inne
r.
Ask
etal
.20
06(5
)Th
eot
her
scho
olcl
ass
was
not
serv
edb
reak
fast
,b
utg
otth
esa
me
info
rmat
ion
abou
tth
eim
por
tanc
eof
ahe
alth
yd
iet;
inad
diti
on,
all
par
ents
wer
een
cour
aged
top
rovi
de
ap
acke
dlu
nch
for
thei
rch
ildre
nev
ery
day
.
The
inte
rven
tion
cons
iste
dof
serv
edb
reak
fast
atth
eb
egin
ning
ofea
chsc
hool
day
.Th
est
uden
tsw
ere
also
offe
red
afo
odsu
pp
lem
ent
cons
istin
gof
vita
min
s,m
iner
als
and
omeg
a-3
fatty
acid
s.Th
eb
reak
fast
cons
iste
dof
low
-fat
milk
,or
ang
eju
ice,
who
le-g
rain
bre
ad,
diff
eren
tsp
read
sw
ithfis
h,m
eat
and
chee
sean
da
frui
t.
Jam
eset
al.
2004
(23)
(CH
OP
PS
)
Con
trol–
nofu
rthe
rd
etai
ls1-
hse
ssio
nea
chcl
ass
each
term
(fou
rse
ssio
ns)
enco
urag
ing
child
ren
not
tod
rink
carb
onat
edd
rinks
but
tosw
itch
tow
ater
orfr
uit
juic
ed
ilute
d1:
3w
ithw
ater
.
PAO
NLY
ST
UD
IES
Flor
es19
95(3
5)U
sual
PA(p
layg
roun
dac
tiviti
es)
Cul
tura
llyse
nsiti
vehe
alth
educ
atio
ncu
rric
ulum
twic
ea
wee
kp
lus
dan
ce-o
rient
ated
aero
bic
PE
clas
sth
ree
times
aw
eek
(50
min
each
)fo
r12
wee
ks.
Har
rison
etal
.20
06(9
)
(Sw
itch
Off
–G
etA
ctiv
e)
Usu
alhe
alth
educ
atio
ncu
rric
ulum
10le
sson
s,te
ache
r-le
d,
emp
hasi
zed
self-
mon
itorin
g,
bud
get
ing
oftim
ean
dse
lect
ive
view
ing
.P
oint
ssy
stem
for
activ
ityan
dvi
ewin
gtim
e.In
terv
entio
np
hilo
sop
hyb
ased
onso
cial
cog
nitiv
eth
eory
for
beh
avio
urch
ang
e.
Des
igne
dto
com
ple
men
tex
istin
gso
cial
,p
erso
nala
ndhe
alth
educ
atio
ncu
rric
ulum
.Tw
oke
ym
essa
ges
wer
eto
min
imiz
etim
esp
ent
wat
chin
gTV
and
pla
ying
com
put
erg
ames
and
the
need
toin
crea
sePA
.Te
ache
rre
sour
ces,
pup
ilw
orkb
ooks
and
dia
ries
pro
vid
ed,
teac
hers
sup
por
ted
by
visi
tsev
ery
2w
eeks
and
par
ents
enco
urag
edin
writ
ing
tosu
pp
ort
child
ren.
Jam
ner
etal
.20
04(4
0)C
ontro
l–no
furt
her
det
ails
Sp
ecia
lPE
clas
s.Th
ecl
ass
met
5d
wee
k-1fo
r60
min
each
day
(ap
pro
xim
atel
y40
min
ofac
tivity
time)
.Ty
pes
ofac
tivity
incl
uded
aero
bic
dan
ce,
bas
ketb
all,
swim
min
gan
dTa
eB
o.1
dw
eek-1
ofcl
ass
time
was
dev
oted
toa
lect
ure
ord
iscu
ssio
nfo
cusi
ngon
the
heal
thb
enefi
tsof
PAan
dst
rate
gie
sfo
rb
ecom
ing
mor
ep
hysi
cally
activ
e.
Laza
ar20
07(1
0)A
llch
ildre
nw
ere
giv
en2
¥1
hse
ssio
nsof
PE
per
wee
kin
corp
orat
edw
ithin
the
scho
oltim
etab
le.
1-h
sess
ions
twic
ea
wee
kof
PAaf
ter
clas
s,su
per
vise
db
ysp
orts
scie
nce
stud
ents
trai
ning
tob
ecom
eP
Ete
ache
rs.
All
child
ren
wer
eg
iven
2¥
1h
sess
ions
ofP
Ep
erw
eek
inco
rpor
ated
with
inth
esc
hool
timet
able
.
Mo-
suw
anet
al.
1998
(46)
Bot
hsc
hool
sha
d1-
hP
Ep
erw
eek
15-m
inw
alk
bef
ore
mor
ning
clas
s,20
-min
aero
bic
dan
cese
ssio
naf
ter
afte
rnoo
nna
p,
thre
etim
esp
erw
eek
for
29.6
wee
ks.
Bot
hsc
hool
sha
d1-
hP
Ep
erw
eek.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 113
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
Pan
gra
ziet
al.
2003
(43)
No
treat
men
tco
ntro
lP
LAY
Pro
mot
es30
–60
min
mod
erat
eto
vig
orou
sPA
dai
ly,
15-m
inac
tivity
bre
akea
chd
ayto
teac
hva
riety
ofPA
,p
rom
otes
attit
udes
and
beh
avio
urs
tosu
stai
nac
tive
hab
itsfo
rlif
e;in
clud
esse
lf-m
onito
ring
and
self-
awar
enes
s.
PLA
Yis
not
inte
nded
tore
pla
ceco
mp
rehe
nsiv
eP
Ep
rog
ram
me
but
act
asim
por
tant
sup
ple
men
t.
The
inte
rven
tion
com
pris
edth
ree
stag
es:
Ste
p1:
pro
mot
ep
lay
beh
avio
ur(fi
rst
wee
k)te
ache
rsan
dst
uden
tsp
artic
ipat
ed,
mor
ew
alki
ng,
less
stan
din
g,
sitti
ng,
child
ren
wer
ein
form
edab
out
the
imp
orta
nce
ofPA
and
iden
tified
app
rop
riate
adul
tro
lem
odel
s.
Ste
p2:
teac
her-
dire
cted
activ
ities
(3w
eeks
)g
ames
and
activ
ities
that
wer
een
joya
ble
and
coul
db
ep
laye
dou
tsid
esc
hool
.
Ste
p3:
enco
urag
ese
lf-d
irect
edac
tivity
(8w
eeks
)w
ithst
uden
tsai
min
gto
achi
eve
30m
inof
activ
ityp
erd
ayin
dep
end
ently
ofte
ache
rou
tsid
esc
hool
.Tr
eatm
ent
and
PE
scho
ols;
child
ren
rece
ived
log
shee
tssi
mila
rto
the
PLA
Yon
esb
utw
ere
aske
dto
reco
rdth
eir
afte
rsc
hool
activ
ities
(act
ive
and
sed
enta
ry).
PE
Pro
mot
es30
–60
min
mod
erat
eto
vig
orou
sPA
dai
ly,
15-m
inac
tivity
bre
akea
chd
ayto
teac
hva
riety
ofPA
,p
rom
otes
attit
udes
and
beh
avio
urs
tosu
stai
nac
tive
hab
itsfo
rlif
e;in
clud
esse
lf-m
onito
ring
and
self-
awar
enes
s.
PLA
Yis
not
inte
nded
tore
pla
ceco
mp
rehe
nsiv
eP
Ep
rog
ram
me
but
act
asim
por
tant
sup
ple
men
t.
The
inte
rven
tion
com
pris
edth
ree
stag
es:
Ste
p1:
pro
mot
ep
lay
beh
avio
ur(fi
rst
wee
k)te
ache
rsan
dst
uden
tsp
artic
ipat
ed,
mor
ew
alki
ng,
less
stan
din
g,
sitti
ng,
child
ren
wer
ein
form
edab
out
the
imp
orta
nce
ofPA
and
iden
tified
app
rop
riate
adul
tro
lem
odel
s.
Ste
p2:
teac
her-
dire
cted
activ
ities
(3w
eeks
)g
ames
and
activ
ities
that
wer
een
joya
ble
and
coul
db
ep
laye
dou
tsid
esc
hool
.
Ste
p3:
enco
urag
ese
lf-d
irect
edac
tivity
(8w
eeks
)w
ithst
uden
tsai
min
gto
achi
eve
30m
inof
activ
ityp
erd
ayin
dep
end
ently
ofte
ache
rou
tsid
esc
hool
.Tr
eatm
ent
and
PE
scho
ols,
child
ren
rece
ived
log
shee
tssi
mila
rto
the
PLA
Yon
esb
utw
ere
aske
dto
reco
rdth
eir
afte
rsc
hool
activ
ities
(act
ive
and
sed
enta
ry).
PLA
Y+
PE
Pro
mot
es30
–60
min
mod
erat
eto
vig
orou
sPA
dai
ly,
15-m
inac
tivity
bre
akea
chd
ayto
teac
hva
riety
ofPA
,p
rom
otes
attit
udes
and
beh
avio
urs
tosu
stai
nac
tive
hab
itsfo
rlif
e;in
clud
esse
lf-m
onito
ring
and
self-
awar
enes
s.
PLA
Yis
not
inte
nded
tore
pla
ceco
mp
rehe
nsiv
eP
Ep
rog
ram
me
but
act
asim
por
tant
sup
ple
men
t.
The
inte
rven
tion
com
pris
edth
ree
stag
es:
Ste
p1:
pro
mot
ep
lay
beh
avio
ur(fi
rst
wee
k)te
ache
rsan
dst
uden
tsp
artic
ipat
ed,
mor
ew
alki
ng,
less
stan
din
g,
sitti
ng,
child
ren
wer
ein
form
edab
out
the
imp
orta
nce
ofPA
and
iden
tified
app
rop
riate
adul
tro
lem
odel
s.
Ste
p2:
teac
her-
dire
cted
activ
ities
(3w
eeks
)g
ames
and
activ
ities
that
wer
een
joya
ble
and
coul
db
ep
laye
dou
tsid
esc
hool
.
Ste
p3:
enco
urag
ese
lf-d
irect
edac
tivity
(8w
eeks
)w
ithst
uden
tsai
min
gto
achi
eve
30m
inof
activ
ityp
erd
ayin
dep
end
ently
ofte
ache
rou
tsid
esc
hool
.Tr
eatm
ent
and
PE
scho
ols,
child
ren
rece
ived
log
shee
tssi
mila
rto
the
PLA
Yon
esb
utw
ere
aske
dto
reco
rdth
eir
afte
rsc
hool
activ
ities
(act
ive
and
sed
enta
ry).
114 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
Pat
eet
al.
2005
(38)
Con
trol–
nofu
rthe
rd
etai
lsLE
AP,
bas
edon
soci
alec
olog
ical
mod
eld
raw
nm
ainl
yfro
mso
cial
cog
nitiv
eth
eory
;LE
AP
pro
ject
staf
fsu
pp
orte
dth
eLE
AP
team
sw
ithin
the
scho
ols
whi
chin
clud
eda
LEA
Pch
amp
ion;
girl
-frie
ndly
PAof
mod
erat
eto
vig
orou
sPA
for
50%
orm
ore
ofP
Ecl
ass
time
(aer
obic
s,d
ance
,w
alki
ng,
self-
def
ence
,m
artia
lart
s,w
eig
httr
aini
ngp
lus
com
pet
itive
spor
tan
dtr
aditi
onal
PE
).
Env
ironm
enta
lcha
nge
incl
uded
role
mod
ellin
gb
ysc
hool
staf
f,fa
mily
and
com
mun
ity-b
ased
activ
ities
.
Rob
bin
set
al.
2006
(11)
(Girl
son
the
mov
e)
Afte
rco
mp
letin
gco
mp
uter
ized
que
stio
nnai
res,
each
girl
inth
eco
ntro
lgro
upre
ceiv
eda
hand
out
listin
gth
ePA
reco
mm
end
atio
ns.
Toen
cour
age
PA,
each
girl
inth
ein
terv
entio
ng
roup
rece
ived
com
put
eriz
ed,
ind
ivid
ually
tailo
red
feed
bac
km
essa
ges
bas
edon
her
resp
onse
sto
the
que
stio
nnai
res,
ind
ivid
ualc
ouns
ellin
gfro
mth
esc
hool
’sP
NP
and
tele
pho
neca
llsan
dm
ailin
gs
from
atr
aine
dre
sear
chas
sist
ant.
Eac
hw
elln
ess
cent
rest
affe
db
yP
NP,
soci
alw
orke
ran
dm
edic
alas
sist
ant.
Rob
inso
n19
99(3
6)C
ontro
l–no
furt
her
det
ails
Bas
edon
Ban
dur
a’s
soci
alco
gni
tive
theo
ry;
18¥
less
ons
of30
–50
min
,in
clud
edse
lf-m
onito
ring
ofTV
,vi
deo
tap
ean
dvi
deo
gam
eus
e,th
en10
-dtu
rn-o
ff,th
en7-
hb
udg
et,
child
ren
taug
htto
bec
ome
sele
ctiv
evi
ewer
san
dad
voca
tors
ofre
duc
ing
med
iaus
e.P
aren
tali
nvol
vem
ent.
Sal
liset
al.
1993
,19
97(4
1,42
)C
ontro
l–no
furt
her
det
ails
Two
inte
rven
tion
gro
ups
rece
ivin
gth
esa
me
pro
gra
mm
e–
pro
vid
edb
yte
ache
rstr
aine
dfo
rto
tal3
8h
in-h
ouse
over
2ye
ars.
3¥
30-m
incl
asse
sp
erw
eek
incl
udin
gw
arm
-up
,fit
ness
activ
ities
such
asw
alk/
run/
jog
/aer
obic
dan
cean
dsp
orts
skill
ssu
chas
socc
er/b
aske
tbal
l/sof
tbal
l;p
lus
wee
kly
30-m
inse
lf-m
anag
emen
ttr
aini
ng,
also
ince
ntiv
esan
dp
aren
tali
nvol
vem
ent
thro
ugh
new
slet
ters
and
sig
natu
reon
wee
kly
goa
lshe
ets.
Two
inte
rven
tion
gro
ups
rece
ivin
gth
esa
me
pro
gra
mm
e–
pro
vid
edb
yce
rtifi
edP
Esp
ecia
list.
3¥
30-m
incl
asse
sp
erw
eek
incl
udin
gw
arm
-up
,fit
ness
activ
ities
such
asw
alk/
run/
jog
/aer
obic
dan
cean
dsp
orts
skill
ssu
chas
socc
er/b
aske
tbal
l/sof
tbal
l;p
lus
wee
kly
30-m
inse
lf-m
anag
emen
ttr
aini
ng,
also
ince
ntiv
esan
dp
aren
tal
invo
lvem
ent
thro
ugh
new
slet
ters
and
sig
natu
reon
wee
kly
goa
lshe
ets.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 115
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141
Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
Sch
ofiel
det
al.
2005
(39)
Con
trol–
nofu
rthe
rd
etai
lsM
inut
esin
terv
entio
n:In
crea
seb
y10
–15
min
dai
lyea
chw
eek
until
reac
hed
dai
lyav
erag
eof
30–6
0m
ind
-1.
Gro
upm
eetin
gs
once
aw
eek
for
6w
eeks
for
30m
inea
chin
gro
ups
ofei
ght
eith
erb
efor
eor
afte
rsc
hool
ord
urin
glu
nch
bre
ak.
Inte
rven
tion
gro
ups
rece
ived
log
boo
kto
reco
rdm
inut
ein
PAor
amou
ntof
step
coun
ts;
actu
alac
tivity
inte
rven
tion
was
12w
eeks
with
wee
ks7–
12m
aint
enan
cep
hase
(no
gro
upm
eetin
gs)
.
Ped
omet
erin
terv
entio
n:10
00–2
000
step
sin
crea
sed
aily
each
wee
kun
tilre
ache
d10
000
step
sp
erd
ay.
Gro
upm
eetin
gs
once
aw
eek
for
6w
eeks
for
30m
inea
chin
gro
ups
ofei
ght
eith
erb
efor
eor
afte
rsc
hool
ord
urin
glu
nch
bre
ak.
Inte
rven
tion
gro
ups
rece
ived
log
boo
kto
reco
rdm
inut
ein
PAor
amou
ntof
step
coun
ts;
actu
alac
tivity
inte
rven
tion
was
12w
eeks
with
wee
ks7–
12m
aint
enan
cep
hase
(no
gro
upm
eetin
gs)
.
Ste
phe
ns&
Wen
tz19
98(3
7)C
ontro
lchi
ldre
nre
ceiv
edus
ualP
E(4
5m
inon
cep
erw
eek)
.S
upp
lem
enta
ryp
rog
ram
me
ofPA
onw
eig
htin
add
ition
tous
ualP
E(4
5m
inon
cep
erw
eek)
.
Trud
eau
2000
(44)
,Tr
udea
uet
al.
2001
(45)
Con
trol–
nofu
rthe
rd
etai
ls6-
year
inte
rven
tion
invo
lvin
g1
hd
-1(5
hw
eek-1
)of
PE
toin
crea
seae
rob
ican
dm
uscu
lar
cap
acity
,in
com
par
ison
with
aco
ntro
lgro
upth
atre
ceiv
edsi
ngle
40-m
inP
Ep
erw
eek.
Vald
imar
sson
etal
.20
06(1
6)
Lind
enet
al.
2006
(17)
(The
Mal
mo
Ped
iatr
icO
steo
por
osis
Pre
vent
ion
[PO
P]
Stu
dy)
Inth
eco
ntro
lsch
ools
,th
esa
me
typ
eof
PAw
asus
edas
inth
ein
terv
entio
nsc
hool
but
ata
leve
lw
ithin
the
com
pul
sory
Sw
edis
hsc
hool
curr
icul
umof
PE
,co
nsis
ting
ofon
eor
two
sess
ions
per
wee
k(t
otal
60m
inw
eek-1
).
The
ord
inar
yin
doo
ran
dou
tdoo
rPA
used
with
inth
eS
wed
ish
scho
olcu
rric
ulum
,no
win
crea
sed
to40
min
d-1
(200
min
wee
k-1),
sup
ervi
sed
by
the
ord
inar
yte
ache
r.Th
ein
terv
entio
nd
idno
tco
nsis
tof
any
pro
gra
mm
essp
ecifi
cally
des
igne
das
bei
ngos
teog
enic
.A
ctiv
ities
incl
uded
bal
lgam
es,
runn
ing
and
jum
pin
g,
virt
ually
nosp
ecifi
csp
orts
trai
ning
was
cond
ucte
d.
The
teac
hers
also
cond
ucte
da
varie
tyof
diff
eren
tPA
soas
not
tob
ore
the
child
ren
with
rep
eate
dst
and
ard
ized
activ
ities
.
Visk
ic-S
tale
cet
al.
2007
(18)
Con
trolg
roup
atte
nded
stan
dar
dP
E(6
6se
ssio
ns)
Inte
rven
tion
gro
upat
tend
ed66
sess
ions
incl
udin
gae
rob
ics,
step
aero
bic
s,fo
lk,
soci
alan
dja
zzd
ance
,rh
ythm
icg
ymna
stic
s.
116 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
CO
MB
INE
DD
IET
AN
DPA
ST
UD
IES
Cab
alle
roet
al.
2003
(33)
(Pat
hway
s)
Con
trol–
nofu
rthe
rd
etai
lsFo
urco
mp
onen
ts:
(1)
Cha
nge
ind
ieta
ryin
take
(Pat
hway
sg
uid
elin
esfo
rfo
od-s
ervi
cep
erso
nnel
and
reg
ular
visi
tb
yP
athw
ays
nutr
ition
ist
tosu
pp
ort
and
mon
itor
scho
ollu
nche
s).
(2)
Incr
ease
inPA
(3¥
30-m
inm
oder
ate
tovi
gor
ous
PAb
ased
onS
PAR
Kp
rog
ram
me
[see
Sal
lis19
93{4
1}]
per
wee
kd
urin
gte
rm-t
ime,
exer
cise
bre
akd
urin
gcl
assr
oom
time
and
gui
ded
pla
yd
urin
gre
cess
).(3
)A
clas
sroo
mcu
rric
ulum
focu
sed
onhe
alth
yea
ting
and
lifes
tyle
(12
wee
ksye
ar-1
,8
wee
ksin
fifth
gra
de,
twic
ew
eekl
y45
-min
clas
sroo
mle
sson
sin
teg
ratin
gso
cial
lear
ning
theo
ryw
ithA
mer
ican
–Ind
ian
trad
ition
san
din
dig
enou
sle
arni
ngm
odes
such
asst
ory
telli
ng).
(4)
Afa
mily
-invo
lvem
ent
pro
gra
mm
e(f
amily
fun
nig
hts,
wor
ksho
ps,
even
tsat
scho
olan
dfu
np
acks
linke
dto
clas
sroo
mcu
rric
ulum
).
Dan
ielz
iket
al.
2007
(6)
(KO
PS
)
Con
trol–
nofu
rthe
rd
etai
ls6-
hco
urse
ofnu
triti
oned
ucat
ion
follo
wed
by
20m
inof
‘act
ive
bre
ak’(
eat
frui
tan
dve
get
able
sev
ery
day
,re
duc
ein
take
ofhi
gh-
fat
food
s,ke
epac
tive
for
atle
ast
1h
d-1
,d
ecre
ase
TVco
nsum
ptio
nto
1h
d-1
).
Mes
sag
eal
sog
iven
top
aren
ts.
Thre
esc
hool
sre
ceiv
edin
terv
entio
np
erye
ar.
Don
nelly
etal
.19
96(3
4)C
ontro
l–no
furt
her
det
ails
Com
pon
ents
incl
uded
anu
triti
onin
terv
entio
n(c
hang
esto
scho
ollu
nche
sus
ing
Lunc
hpow
er!
whi
chis
are
duc
eden
erg
y,fa
tan
dso
diu
mlu
nch
and
nutr
ition
educ
atio
nin
curr
icul
um)
and
PAin
terv
entio
nof
30–4
0m
ind
-13
dw
eek-1
ofae
rob
icac
tiviti
es.
Elia
kim
etal
.20
07(7
)C
ontro
l–no
furt
her
det
ails
Nut
ritio
nale
duc
atio
nin
teg
rate
din
tocu
rric
ulum
,45
min
d-1
6d
wee
k-1of
exer
cise
trai
ning
mai
nly
circ
uit
trai
ning
,al
soen
cour
aged
tore
duc
ese
den
tary
beh
avio
ur.
Gor
tmak
eret
al.
1999
(28)
(Pla
net
Hea
lth)
Con
trol–
nofu
rthe
rd
etai
lsP
rom
otio
nof
PA,
mod
ifica
tion
ofd
ieta
ryin
take
(dec
reas
ing
cons
ump
tion
ofhi
gh-
fat
food
s,in
crea
sing
frui
tan
dve
get
able
cons
ump
tion)
and
red
uctio
nof
sed
enta
ryb
ehav
iour
s(w
itha
stro
ngem
pha
sis
onre
duc
ing
TVvi
ewin
g).
Und
erp
inne
db
yb
ehav
iour
alch
ang
ean
dso
cial
cog
nitiv
eth
eory
.32
clas
sroo
mle
sson
sof
45m
inea
chov
ertw
osc
hool
year
s.
Gra
fet
al.
2005
(29)
Con
trol–
nofu
rthe
rd
etai
lsTh
eS
TEP
TWO
pro
gra
mm
e,w
hich
isd
esig
ned
for
over
wei
ght
and
obes
ech
ildre
n,co
nsis
ted
ofhe
alth
educ
atio
nan
dPA
del
iver
edb
ya
team
ofnu
triti
onis
ts,
gym
nast
s,p
sych
olog
ists
and
med
ical
doc
tors
.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 117
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
Hae
rens
etal
.20
06(8
)C
ontro
l–no
furt
her
det
ails
The
PAen
viro
nmen
tali
nter
vent
ion
focu
sed
onin
crea
sing
leve
lsof
mod
erat
eto
vig
orou
sPA
toat
leas
t60
min
d-1
.S
choo
lsw
ere
enco
urag
edto
crea
tem
ore
opp
ortu
nitie
sto
be
phy
sica
llyac
tive
dur
ing
bre
aks,
atno
onor
afte
rsc
hool
hour
s.Th
isre
sulte
din
aw
eekl
yor
gan
izat
ion
ofan
aver
age
4.7
hof
extr
aPA
.Sch
ools
enco
urag
edva
ryin
gco
nten
tofP
A,n
on-c
omp
etiti
veac
tiviti
esen
cour
aged
and
extr
asp
orts
mat
eria
lsp
rovi
ded
.
Ove
rtw
osc
hool
year
sa
tota
loff
our
clas
sho
urs
spen
ton
pro
mot
ing
PAat
the
per
sona
llev
el–
com
put
erta
ilore
dPA
incl
udin
gfe
edb
ack
bas
edon
per
sona
lphy
sica
lfitn
ess
and
bas
edon
stag
esof
chan
ge
theo
ry.
Food
inte
rven
tion
focu
sed
onin
crea
sing
frui
tcon
sum
ptio
nto
atle
astt
wo
pie
ces
per
day
,red
ucin
gso
ftd
rink
and
incr
easi
ngw
ater
cons
ump
tion
and
red
uce
fati
ntak
e(f
ree
orlo
w-p
rice
wat
eran
dfr
uitm
ade
avai
lab
le).
Ove
rtw
osc
hool
year
sa
tota
loft
wo
clas
sho
urs
spen
tin
pro
mot
ing
heal
thy
eatin
gat
per
sona
llev
el–
com
put
erta
ilore
din
ter-
vent
ion.
Par
enta
linv
olve
men
tinc
lud
edad
ultc
omp
uter
tailo
red
inte
rven
tion
for
fati
ntak
ean
dPA
.
Kai
net
al.
2004
(30)
Con
trol–
nofu
rthe
rd
etai
lsIn
terv
entio
nch
ildre
nre
ceiv
ed8–
11h
die
tary
educ
atio
nin
sixt
hg
rad
ean
d5–
6h
for
seve
nth
and
eig
hth
gra
de
over
6m
onth
s;90
min
wee
k-1of
PA(s
por
t)b
ysc
hool
PE
/cla
ssro
omte
ache
ror
rese
arch
PE
for
6m
onth
s;ac
tive
rece
sson
cea
day
for
the
last
3m
onth
s;he
alth
yki
osks
;p
aren
tali
nvol
vem
ent
(tw
om
eetin
gs)
and
spec
ial
activ
ities
incl
udin
gp
rize
for
eatin
gth
em
ost
heal
thy
snac
ks.
Luep
ker
etal
.19
96(4
7)
(CAT
CH
)
Con
trols
choo
lsre
ceiv
edus
ual
care
Mod
ifica
tions
tosc
hool
food
serv
ice
(30%
fat)
,en
hanc
edP
E(m
oder
ate
tovi
gor
ous
activ
ityfo
r40
%cl
ass
time)
and
clas
sroo
mhe
alth
curr
icul
a.
Inte
nsity
but
not
dur
atio
nof
PE
less
ons
chan
ged
inin
terv
entio
ng
roup
com
par
edw
ithco
ntro
l.
Mod
ifica
tions
tosc
hool
food
serv
ice
(30%
fat)
,en
hanc
edP
E(m
oder
ate
tovi
gor
ous
activ
ityfo
r40
%cl
ass
time)
and
clas
sroo
mhe
alth
cur-
ricul
a,an
d28
ofth
e56
inte
rven
tion
scho
ols
also
had
fam
ilyed
ucat
ion
(act
ivity
pac
ksan
dfa
mily
fun
nig
hts)
.
Inte
nsity
but
notd
urat
ion
ofP
Ele
sson
sch
ang
edin
inte
rven
tion
gro
upco
m-
par
edw
ithco
ntro
l.
Man
ios
etal
.19
98,
1999
,20
02(2
4–26
)
Kaf
atos
etal
.20
07(2
2)
(Cre
tan
Hea
lthan
dN
utrit
ion
Ed
ucat
ion
Pro
gra
m)
Con
trol–
nofu
rthe
rd
etai
lsN
utrit
ion
com
pon
ent
com
pris
ed13
–17
hcl
assr
oom
mat
eria
lsco
nduc
ted
by
clas
ste
ache
rea
chye
ar;
4–6
hcl
assr
oom
mat
eria
lon
theo
ryof
PE
and
2¥
45m
inP
Ep
erw
eek
by
PE
teac
hers
.Th
eore
tical
fram
ewor
kb
ased
onso
cial
cog
nitiv
eth
eory
,ta
rget
ing
child
ren
and
par
ents
,so
cial
and
phy
sica
lenv
ironm
ent.
Ad
apte
d‘K
now
Your
Bod
y’sc
hool
heal
thp
rom
otio
np
rog
ram
me.
118 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
Ros
enb
aum
etal
.20
07(1
2)C
ontro
l–no
furt
her
det
ails
45-m
incl
assr
oom
sess
ion
once
per
wee
kin
teg
rate
din
tore
gul
arsc
ienc
ep
rog
ram
me
and
taug
htb
yth
est
udy
inve
stig
ator
s.
Nut
ritio
ned
ucat
ion
and
die
tary
mod
ifica
tion
tolo
wer
die
tary
fat,
swee
tene
dd
rinks
and
fast
orsu
per
size
dfo
odco
nsum
ptio
n.E
xerc
ise
sess
ions
cons
iste
dof
dan
ce/n
o-co
ntac
tki
ckb
oxin
gth
ree
times
per
wee
kor
atte
ndre
gul
arg
ymcl
asse
s–
exer
cise
sess
ions
sup
ervi
sed
by
one
stud
yin
vest
igat
or.
Sah
ota
etal
.20
01(3
2)
(AP
PLE
S)
Con
trol–
nofu
rthe
rd
etai
lsIn
clud
edte
ache
rtr
aini
ng,
mod
ifica
tion
ofsc
hool
mea
ls,
the
dev
elop
men
tof
scho
olac
tion
pla
nsta
rget
ing
the
curr
icul
um,
PE
,tu
cksh
ops
and
pla
ygro
und
activ
ities
.
Sah
ota
used
ap
opul
atio
nap
pro
ach
und
erp
inne
db
yth
eH
ealth
-Pro
mot
ing
Sch
ools
phi
loso
phy
and
the
inte
rven
tion
invo
lved
the
who
lesc
hool
com
mun
ityin
clud
ing
par
ents
,te
ache
rsan
dca
terin
gst
aff.
Sal
liset
al.
2003
(27)
Con
trol–
nofu
rthe
rd
etai
lsTh
ep
rimar
yai
ms
ofth
ein
terv
entio
nw
ere:
(1)
Incr
ease
the
tota
lene
rgy
exp
end
iture
from
PAb
yth
est
uden
tp
opul
atio
nat
scho
ol.
(2)
Dec
reas
eth
eg
ram
sof
tota
lsat
urat
edd
ieta
ryfa
tp
urch
ased
orb
roug
htto
scho
olb
yst
uden
ts.
One
inte
rven
tion
com
pon
ent
was
des
igne
dto
incr
ease
PAin
PE
clas
ses
thro
ugh
chan
gin
gle
sson
cont
ext,
less
onst
ruct
ure
and
teac
her
beh
avio
ur.
Ano
ther
inte
rven
tion
com
pon
ent
was
inte
nded
toin
crea
sePA
onca
mp
usd
urin
gle
isur
ep
erio
ds
thro
ugho
utth
esc
hool
day
.
Inte
rven
tions
with
scho
olfo
odse
rvic
est
aff
and
man
ager
sw
ere
und
erta
ken
top
rovi
de
mor
elo
w-f
atch
oice
sat
thes
eso
urce
s.
Sin
gh
etal
.20
07(1
4)
(Dut
chO
bes
ityIn
terv
entio
nin
Teen
ager
s[D
OiT
stud
y])
Con
trols
choo
lsm
aint
aine
dre
gul
arcu
rric
ulum
Inte
rven
tion
dev
elop
edus
ing
map
pin
gp
roto
col,
whi
chis
bas
edon
theo
ryan
dem
piri
cale
vid
ence
.11
less
ons
inB
iolo
gy
and
PE
that
aim
edto
incr
ease
awar
enes
san
db
ehav
iour
alch
ang
esco
ncer
ning
ener
gy
inta
kean
dou
tput
.R
educ
ehi
gh-
sug
ar,
hig
h-fa
tsn
acks
,su
gar
-sw
eete
ned
bev
erag
es,
red
uce
sed
enta
ryan
din
crea
seac
tive
beh
avio
urs,
ind
ivid
ually
tailo
red
advi
cevi
ain
tern
etor
CD
-RO
M,
add
ition
alP
Ecl
asse
sen
cour
aged
,ch
ang
esto
scho
olca
ntee
n.
Sp
ieg
elet
al.
2006
(15)
Con
trol–
nofu
rthe
rd
etai
lsIn
terv
entio
nb
ased
onth
eTh
eory
ofR
easo
ned
Act
ion.
Pro
gra
mm
edin
teg
rate
din
tova
rious
par
tsof
the
core
curr
icul
um,
incl
ude
wel
lnes
s,nu
triti
on,
PAan
dfit
ness
.In
terv
entio
ncl
asse
sfo
llow
eda
10-m
inae
rob
icex
erci
sero
utin
eea
chd
ayd
urin
gcl
ass
time.
Web
site
pro
vid
edre
sour
ces
for
teac
hers
,st
uden
tsan
dp
aren
ts.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 119
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141
Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
Tayl
oret
al.
2007
(20)
(AP
ilot
for
Life
styl
ean
dE
xerc
ise
–A
PP
LEp
roje
ct)
Sch
ools
rece
ived
pay
men
tof
$500
–$10
00d
epen
din
gon
scho
olsi
zefo
rth
ep
urch
ase
ofsc
hool
equi
pm
ent
asa
reim
bur
sem
ent
for
the
time
req
uire
dto
mea
sure
child
ren
Nut
ritio
ned
ucat
ion
targ
etin
gre
duc
tions
insw
eete
ned
drin
ksan
din
crea
sed
frui
tan
dve
get
able
inta
ke,
also
inte
ract
ive
card
gam
e(m
ainl
yin
seco
ndye
arof
inte
rven
tion)
and
activ
ityco
ord
inat
ors
(0.5
full-
time
equi
vale
ntp
ersc
hool
)w
hom
anag
edan
activ
ityp
rog
ram
me
that
focu
sed
onno
n-cu
rric
ular
lifes
tyle
-bas
edac
tiviti
essu
chas
com
mun
ityw
alks
(inb
reak
s,lu
ncht
ime
and
afte
r-sc
hool
).
Trev
ino
etal
.20
04(4
8),
Trev
ino
2005
(49)
Con
trol–
nofu
rthe
rd
etai
lsTh
ein
terv
entio
nw
asth
eB
iene
star
Hea
lthP
rog
ram
bas
edon
Soc
ialC
ogni
tive
Theo
ryin
whi
chp
erso
nal
fact
ors,
soci
alfa
ctor
san
db
ehav
iour
are
inte
r-re
late
dan
dha
ved
ynam
icin
fluen
ces
onea
chot
her.
The
Bie
nest
arP
rog
ram
was
des
igne
dto
influ
ence
each
det
erm
inan
tto
dec
reas
ed
ieta
ryfa
tan
din
crea
sed
ieta
ryfib
reco
nsum
ptio
nan
dto
pro
mot
ep
artic
ipat
ion
inm
oder
ate
tovi
gor
ous
PA.
Pro
gra
mm
eac
tiviti
esw
ere
bili
ngua
land
incl
uded
ap
aren
ted
ucat
ion
and
invo
lvem
ent
pro
gra
mm
e,a
clas
sroo
mhe
alth
and
PE
curr
icul
um,
ast
uden
taf
ter
scho
olhe
alth
club
and
asc
hool
cafe
teria
pro
gra
mm
e.
Vand
ong
enet
al.
1995
(50)
Con
trolg
roup
Fitn
ess
gro
up
Fitn
ess:
6¥
30m
incl
assr
oom
sess
ions
and
15m
inev
ery
scho
old
ayof
activ
ityto
incr
ease
hear
tra
teto
150–
170
bea
tsm
in-1
.
Sch
ooln
utrit
ion
gro
up.
Nut
ritio
np
rog
ram
me:
Incr
ease
cons
ump
tion
offr
uit,
veg
etab
les,
who
le-g
rain
bre
adan
dce
real
sre
lativ
eto
othe
rfo
ods
and
dec
reas
eco
nsum
ptio
nof
fatty
,su
gar
yan
dsa
ltyfo
ods,
33%
ener
gy
inta
keas
fat,
12%
assu
gar
,25
gfib
red
-1.
Sch
ool-b
ased
:10
¥1-
hle
sson
s.
Hom
enu
triti
ong
roup
.
Nut
ritio
np
rog
ram
me:
Incr
ease
cons
ump
tion
offr
uit,
veg
etab
les,
who
le-g
rain
bre
adan
dce
real
sre
lativ
eto
othe
rfo
ods
and
dec
reas
eco
nsum
ptio
nof
fatty
,su
gar
yan
dsa
ltyfo
ods,
33%
ener
gy
inta
keas
fat,
12%
assu
gar
,25
gfib
red
-1.
Hom
e-b
ased
:H
omew
ork
exer
cise
shee
ts.
Fitn
ess
and
scho
olnu
triti
ong
roup
.
Fitn
ess:
6¥
30m
incl
assr
oom
ses-
sion
san
d15
min
ever
ysc
hool
day
ofac
tivity
toin
crea
sehe
artr
ate
to15
0–17
0b
eats
min
-1.
Nut
ritio
np
rog
ram
me:
Incr
ease
cons
ump
tion
offr
uit,
veg
etab
les,
who
le-
gra
inb
read
and
cere
als
rela
tive
toot
her
food
san
dd
ecre
ase
cons
ump
tion
offa
tty,s
ugar
yan
dsa
ltyfo
ods,
33%
ener
gy
inta
keas
fat,
12%
assu
gar
,25
gfib
red
-1.
Sch
ool-b
ased
:10
¥1-
hle
sson
s.
Fitn
ess
and
hom
enu
triti
ong
roup
.
Fitn
ess:
6¥
30m
incl
assr
oom
sess
ions
and
15m
inev
ery
scho
old
ayof
activ
ityto
incr
ease
hear
tra
teto
150–
170
bea
tsm
in-1
.
Nut
ritio
np
rog
ram
me:
Incr
ease
cons
ump
tion
offr
uit,
veg
etab
les,
who
le-g
rain
bre
adan
dce
real
sre
lativ
eto
othe
rfo
ods
and
dec
reas
eco
nsum
ptio
nof
fatty
,su
gar
yan
dsa
ltyfo
ods,
33%
ener
gy
inta
keas
fat,
12%
assu
gar
,25
gfib
red
-1.
Hom
e-b
ased
:H
omew
ork
exer
cise
shee
ts.
120 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le1
Con
tinue
d
Stu
dy
Gro
up1
Gro
up2
Gro
up3
Gro
up4
Gro
up5
Gro
up6
War
ren
etal
.20
03(3
1)C
ontro
lN
utrit
ion
gro
up
Und
erp
inne
db
yS
ocia
lCog
nitiv
eTh
eory
and
took
pla
cein
lunc
htim
ecl
ubs
whe
rean
inte
ract
ive
and
age-
app
rop
riate
nutr
ition
and
/or
PAcu
rric
ulum
was
del
iver
edb
yth
ere
sear
chte
am,
with
bot
hin
volv
ing
par
ents
.Th
ein
terv
entio
nra
nfo
r20
wee
ksov
erfo
ursc
hool
term
s(a
pp
roxi
mat
ely
14m
onth
s).
PAg
roup
Und
erp
inne
db
yS
ocia
lC
ogni
tive
Theo
ryan
dto
okp
lace
inlu
ncht
ime
club
sw
here
anin
tera
ctiv
ean
dag
e-ap
pro
pria
tenu
triti
onan
d/o
rPA
curr
icul
umw
asd
eliv
ered
by
the
rese
arch
team
,w
ithb
oth
invo
lvin
gp
aren
ts.
The
inte
rven
tion
ran
for
20w
eeks
over
four
scho
olte
rms
(ap
pro
xim
atel
y14
mon
ths)
.
Nut
ritio
nan
dPA
gro
up
Und
erp
inne
db
yS
ocia
lC
ogni
tive
Theo
ryan
dto
okp
lace
inlu
ncht
ime
club
sw
here
anin
tera
ctiv
ean
dag
e-ap
pro
pria
tenu
triti
onan
d/o
rPA
curr
icul
umw
asd
eliv
ered
by
the
rese
arch
team
,w
ithb
oth
invo
lvin
gp
aren
ts.
The
inte
rven
tion
ran
for
20w
eeks
over
four
scho
olte
rms
(ap
pro
xim
atel
y14
mon
ths)
.
Will
iam
son
etal
.20
07(1
9)
(Wis
eM
ind
Pro
ject
)
Act
ive
cont
rolp
rog
ram
me
was
tom
odify
child
ren’
sb
elie
fson
the
use
and
abus
eof
tob
acco
,al
coho
lan
dill
icit
dru
gs
Wis
eM
ind
isb
ased
onno
tion
that
with
the
know
led
ge
and
envi
ronm
enta
lcha
nges
stud
ents
can
mak
ew
ise
dec
isio
nsab
out
nutr
ition
,PA
and
sub
stan
ceus
e/ab
use.
Inte
rven
tion
req
uire
dla
rge-
scal
een
viro
nmen
tal
mod
ifica
tions
with
inth
esc
hool
s(v
end
ing
mac
hine
sin
all
scho
ols
elim
inat
edb
efor
est
udy)
.
Toim
pro
vehe
alth
yea
ting
,in
crea
sePA
,d
ecre
ase
sed
enta
ryb
ehav
iour
and
enco
urag
eth
esa
me
beh
avio
ural
chan
ges
outs
ide
scho
ol.
Die
tary
goa
lsw
ere
five
frui
tan
dve
get
able
sp
erd
ay,
less
than
30%
tota
len
erg
yfro
mfa
t,le
ssth
an10
%to
tale
nerg
yfro
msa
tura
ted
fat,
20–3
0g
fibre
d-1
.
Wis
eM
ind
staf
fw
orke
dcl
osel
yw
ithte
ache
rsan
dca
fete
riap
erso
nnel
toen
cour
age
app
rop
riate
por
tion
size
s,ca
lorie
san
dnu
trie
ntco
nten
tof
lunc
hes.
Vario
usm
edia
used
.In
doo
ran
dou
tdoo
rp
lysu
pp
lies
pro
vid
ed.
Mon
thly
new
slet
ter
emai
led
top
aren
tsp
lus
wei
ght
gai
np
reve
ntio
nw
ebsi
teav
aila
ble
tofa
mili
es.
CH
OP
PS
,th
eC
hris
tchu
rch
obes
ityp
reve
ntio
np
rog
ram
me
insc
hool
s;PA
,p
hysi
cala
ctiv
ity;
PE
,p
hysi
cale
duc
atio
n;P
NP,
pae
dia
tric
nurs
ep
ract
ition
er;
SPA
RK
,S
por
ts,
Pla
yan
dA
ctiv
eR
ecre
atio
nfo
rK
ids.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 121
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le2
Die
tin
terv
entio
nsto
pre
vent
obes
ityin
scho
olch
ildre
n
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
nB
MI
(SD
)kg
m-2
Aim
Follo
w-u
p/n
otas
sess
ed%
Am
aro
etal
.20
06(4
)R
CT
Clu
ster
by
clas
s
Pilo
tst
udy.
Det
ecta
ble
diff
eren
cein
BM
Iz-
scor
ech
ang
ew
ithty
pe
one
erro
rra
teof
0.05
and
80%
pow
erw
as0.
366.
Set
ting
:16
clas
ses
inth
ree
mid
dle
scho
ols
inN
aple
s,Ita
ly
Par
ticip
ants
:29
1ch
ildre
n,A
ge
12(1
1–14
)C
auca
sian
I:18
8C
:10
3
BM
Iz-
scor
e:I:
0.47
(0.9
3)n
=15
3C
:0.
15(0
.88)
n=
88
Tote
stef
ficac
yof
ab
oard
gam
eK
aled
oin
pro
vid
ing
nutr
ition
know
led
ge
and
pro
mot
ing
heal
thy
die
tary
beh
avio
ur.
24w
eeks
I:19
%C
:15
%
Ask
etal
.(5
)R
CT
Clu
ster
by
clas
s
Sm
allp
ilot
stud
y,p
ower
not
rep
orte
d
Set
ting
:Tw
ote
nth
gra
de
clas
ses
inon
elo
wer
seco
ndar
ysc
hool
inru
rald
istr
ict
ofS
outh
ern
Nor
way
Par
ticip
ants
:54
adol
esce
nts
Ag
e15
I:26
C:
28
Med
ian
BM
I(r
ang
e):
I:m
ale;
22.6
(17.
8–33
.6);
fem
ale
21.8
(16.
9–27
.3)
C:
mal
e;21
.7(1
7.0–
29.4
);fe
mal
e21
.6(1
6.7–
28.4
)
Toev
alua
teif
die
tary
hab
itsan
dsc
hool
per
form
ance
imp
rove
din
alo
wer
seco
ndar
ysc
hool
clas
sas
are
sult
ofin
trod
ucin
gb
reak
fast
.
4m
onth
s
I:0%
C:
0%
Jam
eset
al.
2004
(23)
(CH
OP
PS
)R
CT
Clu
ster
by
clas
s
90%
pow
erto
det
ect
diff
eren
ces
of0.
14b
etw
een
cont
rola
ndin
terv
entio
ng
roup
s.
Set
ting
:19
clas
ses
insi
xP
rimar
ysc
hool
sin
Dor
set,
UK
Par
ticip
ants
:M
ale/
fem
ale:
324/
320
Ag
e:8.
7(7
–10.
9)
I:32
5C
:31
9
I:17
.4(0
.6)
C:
17.6
(0.7
)
Tore
duc
eco
nsum
ptio
nof
carb
onat
edd
rinks
.12
-mon
thin
terv
entio
nw
ithfo
llow
-up
at3
year
s
12m
onth
s:I:
9%C
:13
%
3ye
ars:
I:33
%C
:33
%
CH
OP
PS
,th
eC
hris
tchu
rch
obes
ityp
reve
ntio
np
rog
ram
me
insc
hool
s;B
MI,
bod
ym
ass
ind
ex;
SD
,st
and
ard
dev
iatio
n;R
CT,
rand
omiz
edco
ntro
lled
tria
l;I,
inte
rven
tion;
C,
cont
rol.
122 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141
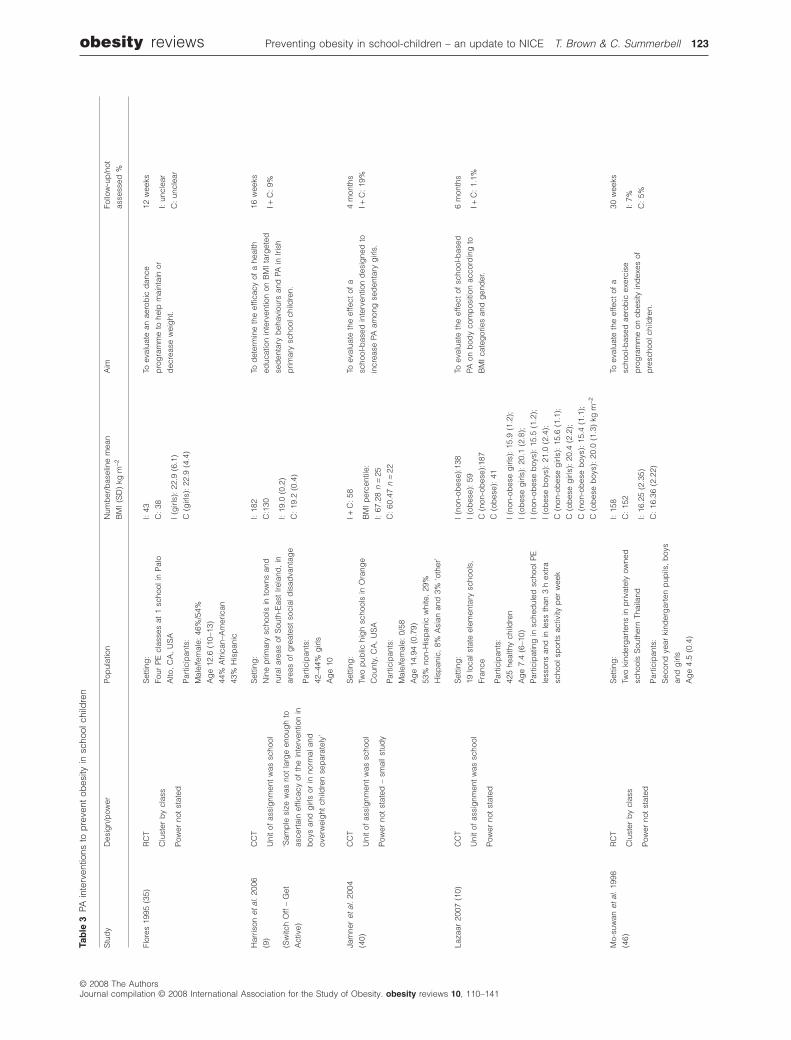
Tab
le3
PAin
terv
entio
nsto
pre
vent
obes
ityin
scho
olch
ildre
n
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
n
BM
I(S
D)
kgm
-2A
imFo
llow
-up
/not
asse
ssed
%
Flor
es19
95(3
5)R
CT
Clu
ster
by
clas
s
Pow
erno
tst
ated
Set
ting
:
Four
PE
clas
ses
at1
scho
olin
Pal
o
Alto
,C
A,
US
A
Par
ticip
ants
:
Mal
e/fe
mal
e:46
%/5
4%
Ag
e12
.6(1
0–13
)
44%
Afr
ican
–Am
eric
an
43%
His
pan
ic
I:43
C:
38
I(g
irls)
:22
.9(6
.1)
C(g
irls)
:22
.9(4
.4)
Toev
alua
tean
aero
bic
dan
ce
pro
gra
mm
eto
help
mai
ntai
nor
dec
reas
ew
eig
ht.
12w
eeks
I:un
clea
r
C:
uncl
ear
Har
rison
etal
.20
06
(9)
(Sw
itch
Off
–G
et
Act
ive)
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
‘Sam
ple
size
was
not
larg
een
oug
hto
asce
rtai
nef
ficac
yof
the
inte
rven
tion
in
boy
san
dg
irls
orin
norm
alan
d
over
wei
ght
child
ren
sep
arat
ely’
Set
ting
:
Nin
ep
rimar
ysc
hool
sin
tow
nsan
d
rura
lare
asof
Sou
th-E
ast
Irela
nd,
in
area
sof
gre
ates
tso
cial
dis
adva
ntag
e
Par
ticip
ants
:
42–4
4%g
irls
Ag
e10
I:18
2
C:1
30
I:19
.0(0
.2)
C:
19.2
(0.4
)
Tod
eter
min
eth
eef
ficac
yof
ahe
alth
educ
atio
nin
terv
entio
non
BM
Ita
rget
ed
sed
enta
ryb
ehav
iour
san
dPA
inIr
ish
prim
ary
scho
olch
ildre
n.
16w
eeks
I+C
:9%
Jam
ner
etal
.20
04
(40)
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
Pow
erno
tst
ated
–sm
alls
tud
y
Set
ting
:
Two
pub
lichi
gh
scho
ols
inO
rang
e
Cou
nty,
CA
,U
SA
Par
ticip
ants
:
Mal
e/fe
mal
e:0/
58
Ag
e14
.94
(0.7
9)
53%
non-
His
pan
icw
hite
,29
%
His
pan
ic,
8%A
sian
and
3%‘o
ther
’
I+C
:58
BM
Ip
erce
ntile
:
I:67
.28
n=
25
C:
60.4
7n
=22
Toev
alua
teth
eef
fect
ofa
scho
ol-b
ased
inte
rven
tion
des
igne
dto
incr
ease
PAam
ong
sed
enta
ryg
irls.
4m
onth
s
I+C
:19
%
Laza
ar20
07(1
0)C
CT
Uni
tof
assi
gnm
ent
was
scho
ol
Pow
erno
tst
ated
Set
ting
:
19lo
cals
tate
elem
enta
rysc
hool
s,
Fran
ce
Par
ticip
ants
:
425
heal
thy
child
ren
Ag
e7.
4(6
–10)
Par
ticip
atin
gin
sche
dul
edsc
hool
PE
less
ons
and
inle
ssth
an3
hex
tra
scho
olsp
orts
activ
ityp
erw
eek
I(n
on-o
bes
e):1
38
I(o
bes
e):
59
C(n
on-o
bes
e):1
87
C(o
bes
e):
41
I(n
on-o
bes
eg
irls)
:15
.9(1
.2);
I(o
bes
eg
irls)
:20
.1(2
.8);
I(n
on-o
bes
eb
oys)
:15
.5(1
.2);
I(o
bes
eb
oys)
:21
.0(2
.4);
C(n
on-o
bes
eg
irls)
:15
.6(1
.1);
C(o
bes
eg
irls)
:20
.4(2
.2);
C(n
on-o
bes
eb
oys)
:15
.4(1
.1);
C(o
bes
eb
oys)
:20
.0(1
.3)
kgm
-2
Toev
alua
teth
eef
fect
ofsc
hool
-bas
ed
PAon
bod
yco
mp
ositi
onac
cord
ing
to
BM
Ica
teg
orie
san
dg
end
er.
6m
onth
s
I+C
:1.
1%
Mo-
suw
anet
al.
1998
(46)
RC
T
Clu
ster
by
clas
s
Pow
erno
tst
ated
Set
ting
:
Two
kind
erg
arte
nsin
priv
atel
yow
ned
scho
ols
Sou
ther
nTh
aila
nd
Par
ticip
ants
:
Sec
ond
year
kind
erg
arte
np
upils
,b
oys
and
girl
s
Ag
e4.
5(0
.4)
I:15
8
C:
152
I:16
.25
(2.3
5)
C:
16.3
6(2
.22)
Toev
alua
teth
eef
fect
ofa
scho
ol-b
ased
aero
bic
exer
cise
pro
gra
mm
eon
obes
ityin
dex
esof
pre
scho
olch
ildre
n.
30w
eeks
I:7%
C:
5%
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 123
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le3
Con
tinue
d
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
n
BM
I(S
D)
kgm
-2A
imFo
llow
-up
/not
asse
ssed
%
Pan
gra
ziet
al.
2003
(43)
CC
T
Con
trols
choo
lsw
ere
not
rand
omly
sele
cted
Pow
erno
tst
ated
Set
ting
:
35sc
hool
sin
Ariz
ona,
US
A
Par
ticip
ants
:
boy
san
dg
irls
Ag
e9.
8(0
.6)
PLA
Y+
PE
:18
3
PE
only
:17
5
PLA
Yon
ly:
150
No
treat
men
tco
ntro
l:91
BM
Ino
tre
por
ted
Toev
alua
teth
eef
fect
sof
the
PLA
Y
inte
rven
tion.
12w
eeks
I:un
clea
r
C:
uncl
ear
Pat
eet
al.
2005
(38)
RC
T
Clu
ster
by
scho
ol
Pow
erno
tst
ated
Set
ting
:
24hi
gh
scho
ols
in14
Sou
thC
arol
ina
coun
ties,
US
A
Par
ticip
ants
:
Mal
e/fe
mal
e:0/
2744
Ag
e13
.6
48.7
%A
fric
an–A
mer
ican
,46
.7%
whi
te
I:15
23
C:
1221
I:22
.9(5
.4),
863
C:
23.0
(5.5
),74
1
Toev
alua
tesc
hool
-bas
edPA
inte
rven
tion
amon
ghi
gh
scho
olg
irls.
6m
onth
s
I+C
:42
%
Rob
bin
set
al.
2006
(11)
(Girl
son
the
mov
e)
RC
T
Clu
ster
by
gra
de
(6,7
,8)
‘The
smal
lsam
ple
size
may
have
pre
clud
edth
eab
ility
tod
etec
t
sig
nific
ant
diff
eren
ceb
etw
een
the
gro
ups’
Set
ting
:
Wel
lnes
sce
ntre
sin
two
mid
dle
scho
ols
inM
ichi
gan
,U
SA
(low
-soc
ioec
onom
ic
geo
gra
phi
car
eas
inth
eM
idw
est)
Par
ticip
ants
:
Mal
e/fe
mal
e:0/
77
Ag
e:11
–14
raci
ally
div
erse
sed
enta
ryg
irls,
self-
iden
tified
asb
eing
inth
e
‘con
tem
pla
tion’
and
‘pre
par
atio
n’
stag
esof
chan
ge
I:45
C:
32
I: Sch
ool1
,se
vent
hg
rad
e:n
=19
;24
.55
(9.8
9)
Sch
ool2
:si
xth
gra
de
n=
22;
23.2
9
(5.3
7)
Sch
ool2
:ei
ght
hg
rad
en
=4;
22.2
6
(4.1
1)
C:
Sch
ool1
:si
xth
gra
de:
n=
8;24
.15
(8.2
2)
Sch
ool2
:se
vent
hg
rad
en
=15
;21
.88
(5.1
2)
Sch
ool1
:ei
ght
hg
rad
en
=9;
24.5
9
(5.3
0)
Tod
eter
min
eth
efe
asib
ility
ofan
ind
ivid
ually
tailo
red
PAp
rog
ram
me
plu
s
nurs
eco
unse
lling
inte
rven
tion
in
incr
easi
ngPA
.
12w
eeks
I:0%
C:
0%
Rob
inso
net
al.
1999
(36)
RC
T
Clu
ster
by
scho
ol
Des
igne
dto
have
80%
pow
erto
det
ect
anef
fect
size
of0.
20or
gre
ater
.
Set
ting
:
Two
pub
licel
emen
tary
scho
ols
inS
an
Jose
,C
A,
US
A
Par
ticip
ants
:
Boy
san
dg
irls
Ag
e8.
9
I:95
C:
103
I:18
.38
(3.6
7)
C:
18.1
0(3
.77)
Toev
alua
tea
scho
ol-b
ased
inte
rven
tion
tore
duc
eTV
,vi
deo
tap
ean
dvi
deo
gam
eus
eon
adip
osity
.
6m
onth
s
I:3%
C:
3%
Sal
liset
al.
1993
,
1997
(41,
42)
(SPA
RK
)
RC
T
Clu
ster
by
scho
ol
Pow
erno
tst
ated
Set
ting
:
Sev
ensu
bur
ban
elem
enta
rysc
hool
sin
Sou
ther
nC
alifo
rnia
,U
SA
Par
ticip
ants
:
Boy
san
dg
irls
Ag
e9.
25
85%
non-
His
pan
icw
hite
I+C
:74
5
BM
Ino
tre
por
ted
Toev
alua
tea
scho
ol-b
ased
inte
rven
tion
invo
lvin
gP
Ean
dse
lf-m
anag
emen
t
(del
iver
edei
ther
by
spec
ialis
tsor
teac
hers
)on
wei
ght
and
adip
osity
.
2ye
ars
I+C
:26
%
124 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le3
Con
tinue
d
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
n
BM
I(S
D)
kgm
-2A
imFo
llow
-up
/not
asse
ssed
%
Sch
ofiel
det
al.
2005
(39)
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
Pow
erno
tst
ated
Set
ting
:
Thre
ehi
gh
scho
ols
ince
ntra
l
Que
ensl
and
,A
ustr
alia
Par
ticip
ants
:
Mal
e/fe
mal
e:0/
85
Ag
e15
.8
Low
activ
eg
irls
I(P
edom
eter
):27
I(M
inut
es):
28
C:
30
I(P
edom
eter
):22
.3(4
.1);
I(M
inut
es):
23.7
(6.6
);
C:
24.5
(5.5
)
Top
ilot
effic
acy
ofus
ing
ped
omet
eras
bas
isof
time
effic
ient
yet
effe
ctiv
e
non-
curr
icul
umsc
hool
-bas
ed
pro
gra
mm
e.
12w
eeks
I(P
edom
eter
):15
%
I(M
inut
es):
25%
C:
20%
Ste
phe
ns&
Wen
tz
1998
(37)
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
Pow
erno
tst
ated
Set
ting
:
Two
urb
anel
emen
tary
pub
licsc
hool
sin
Cle
vela
nd,
OH
,U
SA
Par
ticip
ants
:
I:m
ale/
fem
ale:
44%
/56%
Ag
e8.
4
98%
Afr
ican
–Am
eric
an;
C:
mal
e/fe
mal
e:57
%/4
3%
Ag
e8.
4
78%
Afr
ican
–Am
eric
an;
‘Pre
dom
inan
tlyfro
mlo
w-in
com
e
fam
ilies
’
I:un
clea
r(4
5at
follo
w-u
p)
C:
uncl
ear
(44
atfo
llow
-up
)
Wei
ght
(kg
)
I:25
.4
C:
26.1
Toev
alua
tea
scho
ol-b
ased
sup
ple
men
tary
pro
gra
mm
eof
PAon
wei
ght
inad
diti
onto
usua
lPE
.
15w
eeks
I+C
:un
clea
r
Trud
eau
2000
(44)
,
Trud
eau
etal
.20
01
(45)
(The
Troi
s-R
iver
ies
Gro
wth
and
Dev
elop
men
tst
udy)
CC
T
Pow
erno
tst
ated
–su
bg
roup
anal
ysis
unlik
ely
tob
ep
ower
ed
Set
ting
:
Prim
ary
scho
ols
inTr
ois-
Riv
iere
s,
Que
bec
,C
anad
a
Par
ticip
ants
:
boy
san
dg
irls
Ag
e6
Fren
chd
esce
nt
I:27
2
C:
275
BM
Ino
tre
por
ted
Toev
alua
tew
heth
era
pro
gra
mm
eof
PAan
dfit
ness
insc
hool
child
ren
over
6
year
sw
ould
resu
ltin
enha
nced
card
iova
scul
arfit
ness
inad
ulth
ood
.
6ye
arin
terv
entio
nan
d22
year
follo
w-u
p.
I:75
%
C:
76%
Ran
dom
sele
cted
sam
ple
asse
ssed
at22
-yea
rfo
llow
-up
Vald
imar
sson
etal
.
2006
(16)
Lind
enet
al.
2006
(17)
(The
Mal
mo
Ped
iatr
ic
Ost
eop
oros
is
Pre
vent
ion
[PO
P]
Stu
dy)
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
The
smal
lsam
ple
size
may
have
pre
clud
edth
eab
ility
tod
etec
t
sig
nific
ant
diff
eren
ceb
etw
een
the
gro
ups
Set
ting
:
Four
scho
ols
inm
idd
lecl
ass
area
of
Mal
mo,
Sw
eden
Par
ticip
ants
:
Mal
e/fe
mal
e:0/
53
Ag
e:I:
7.6;
C:
7.9;
Hea
lthy,
Cau
casi
an,
Tann
erst
age
1
I:55
C:
64
I:16
.9(2
.9)
n=
49
C:
16.3
(1.9
)n
=49
Tod
eter
min
ew
heth
era
gen
eral
,
mod
erat
ely
inte
nse
exer
cise
inte
rven
tion
pro
gra
mm
eco
uld
incr
ease
the
accr
ualo
fb
one
min
eral
cont
ent
and
area
lbon
em
iner
ald
ensi
tyan
d
incr
ease
bon
ew
idth
.
2ye
ars
I:11
%
C:
22%
Visk
ic-S
tale
cet
al.
2007
(18)
CC
T
Pow
erno
tst
ated
Set
ting
:
Hig
hsc
hool
,Z
agre
b,
Cro
atia
Par
ticip
ants
:
Mal
e/fe
mal
e:0/
220
Ag
e16
–18
Clin
ical
lyhe
alth
y
I:11
5
C:
105
I:21
.05
(2.1
2)n
=11
5
C:
20.1
(1.8
3)n
=10
2
Gre
ater
bod
yw
eig
htin
Inte
rven
tion
gro
upco
mp
ared
with
cont
rol
Toan
alys
eth
eim
pac
tof
spec
ial
pro
gra
mm
edP
Ein
clud
ing
dan
ce,
aero
bic
san
drh
ythm
icg
ymna
stic
son
the
dev
elop
men
tof
mot
oran
d
func
tiona
lab
ilitie
san
dm
orp
holo
gic
al
char
acte
ristic
sof
fem
ale
four
th-g
rad
e
hig
hsc
hool
ers
inZ
agre
b.
One
acad
emic
year
I:0%
C:
3%
PA,
phy
sica
lact
ivity
;P
E,
phy
sica
led
ucat
ion;
SPA
RK
,S
por
ts,
Pla
yan
dA
ctiv
eR
ecre
atio
nfo
rK
ids;
BM
I,b
ody
mas
sin
dex
;S
D,
stan
dar
dd
evia
tion;
RC
T,ra
ndom
ized
cont
rolle
dtr
ial;
CC
T,co
ntro
lled
clin
ical
tria
l;I,
inte
rven
tion;
C,
cont
rol.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 125
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le4
Com
bin
edd
iet
and
PAin
terv
entio
nsto
pre
vent
obes
ityin
scho
olch
ildre
n
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
nB
MI
(SD
)kg
m-2
Aim
Follo
w-u
p/n
otas
sess
ed%
Cab
alle
roet
al.
2003
(33)
(Pat
hway
s)
RC
T
Clu
ster
by
scho
ol
Pow
erno
tst
ated
Set
ting
:41
elem
enta
rysc
hool
sin
7A
mer
ican
–Ind
ian
com
mun
ities
inA
rizon
a,N
ewM
exic
o,S
outh
Dak
ota,
US
A
Par
ticip
ants
:A
mer
ican
–Ind
ian
scho
olch
ildre
n.A
ge
7.6
(0.6
)
I:87
9C
:82
5
I:19.
0C
:19.
1
Toev
alua
tea
scho
ol-b
ased
mul
ti-co
mp
onen
tin
terv
entio
nto
red
uce
%b
ody
fat
inA
mer
ican
–Ind
ian
child
ren.
3ye
ars
I:17
%C
:17
%
Dan
ielz
iket
al.
2007
(6)
(Kie
lOb
esity
Pre
vent
ion
Stu
dy)
CC
T
Long
itud
inal
dat
a
Pow
erno
tst
ated
Set
ting
:32
prim
ary
scho
ols
inK
iel,
Ger
man
y
Par
ticip
ants
:49
–50%
boy
sA
ge
6
I:78
0C
:14
20
Med
ian
BM
I(in
ter-
qua
rtile
rang
e)I:
15.6
(14.
8–15
.7)
n=
344
C:
15.4
(14.
6–16
.4)
n=
1420
Toev
alua
tefe
asib
ility
and
4-ye
arou
tcom
eof
scho
ol-b
ased
heal
thp
rom
otio
non
over
wei
ght
3.8
(0.4
)ye
ars
I:56
%C
:0%
Don
nelly
etal
.19
96(3
4)C
CT
Uni
tof
assi
gnm
ent
was
scho
ol
Pow
erno
tst
ated
Set
ting
:E
lem
enta
rysc
hool
sin
rura
lN
ebra
ska,
US
A
Par
ticip
ants
:B
oys
and
girl
sA
ge
9.2
94%
Whi
te,
42–4
4%re
ceiv
edfre
ean
dre
duc
edsc
hool
lunc
hes.
I:10
2C
:23
6
I:18
.3(3
.9)
C:
18.5
(3.4
)
Toev
alua
tea
scho
ol-b
ased
PAan
dnu
triti
onp
rog
ram
me
toat
tenu
ate
obes
ityan
dp
rom
ote
fitne
ss.
2ye
ars
I:57
%C
:73
%
Elia
kim
etal
.20
07(7
)R
CT
Clu
ster
by
clas
s
Pow
erno
tst
ated
Set
ting
:Fo
urp
re-s
choo
lcla
sses
inup
per
-mid
dle
clas
sS
ES
com
mun
ity,
Ora
nit,
Isra
el
Par
ticip
ants
:M
ale/
fem
ale:
58/4
3A
ge
5–6
I:54
C:
47
I:15
.7(0
.2)
C:
15.9
(0.2
)
Tost
udy
effe
cts
ofa
brie
fsc
hool
-bas
edhe
alth
pro
mot
ion
inte
rven
tion
14w
eeks
I:0%
C:
0%
Gor
tmak
eret
al.
1999
(28)
(Pla
net
Hea
lth)
RC
T
Clu
ster
by
scho
ol
Onl
y33
inci
den
tca
ses
ofob
esity
‘lim
ited
the
stat
istic
alp
ower
ofth
est
udy
tod
etec
td
iffer
ence
s’
Set
ting
:10
seco
ndar
ysc
hool
sin
Bos
ton,
US
A
Par
ticip
ants
:M
ale/
fem
ale:
52%
/48%
Ag
e11
.7(
0.7)
Hig
her
%A
fric
an–A
mer
ican
girl
sin
cont
rols
choo
ls(1
7vs
.10
%)
and
His
pan
icb
oys
inco
ntro
lsch
ools
(18
vs.
12%
).
I+C
:15
60
I:20
.6(4
.5)
n=
641
C:
20.7
(4.0
)n
=65
4
Toev
alua
teim
pac
tof
scho
ol-b
ased
heal
thb
ehav
iour
inte
rven
tion
know
nas
Pla
net
Hea
lthon
obes
ityam
ong
boy
san
dg
irls
ing
rad
es6
to8.
Two
scho
olye
ars
I+C
:17
%
Gra
fet
al.
2005
(29)
STE
PTW
O
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
Pow
erno
tst
ated
Set
ting
:S
even
prim
ary
scho
ols
inC
olog
ne,
Ger
man
y
Par
ticip
ants
:M
ale/
fem
ale:
830/
848
girl
sA
ge
8.2
(1.3
)
I+C
:16
78
I+C
:17
.1(2
.9)
Top
rese
ntth
eb
asel
ine
and
final
dat
afro
mth
eS
TEP
TWO
pro
gra
mm
e.8–
9m
onth
s
I+C
:89
%O
nly
sub
sam
ple
invi
ted
tota
kep
art
inst
udy
126 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le4
Con
tinue
d
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
nB
MI
(SD
)kg
m-2
Aim
Follo
w-u
p/n
otas
sess
ed%
Hae
rens
etal
.20
06(8
)R
CT
Clu
ster
by
scho
ol
The
anal
yses
show
edth
atan
n=
300
inea
chg
roup
was
suffi
cien
tto
pow
erth
est
udy
at0.
8an
dto
det
ect
ad
iffer
ence
of0.
3in
BM
I,g
iven
the
0.05
leve
lof
sig
nific
ance
.
Set
ting
:15
mid
dle
scho
ols
with
tech
nica
land
voca
tiona
ltra
inin
gin
Wes
t-Fl
and
ers,
Bel
giu
m
Par
ticip
ants
:In
terv
entio
nw
ithp
aren
tals
upp
ort:
Mal
e/fe
mal
e:60
%/4
0%A
ge
1368
%lo
wer
SE
S;
Inte
rven
tion
with
out
par
enta
lsup
por
t:M
ale/
fem
ale:
84%
/16%
Ag
e13
year
s79
%lo
wer
SE
SC
:m
ale/
fem
ale:
41%
/59%
Ag
e13
52%
low
erS
ES
I(p
aren
tsu
pp
ort)
:12
26I
(with
out
par
ent
sup
por
t):
1006
C:
759
I(p
aren
tsu
pp
ort)
:19
.68
(3.8
3);
I(w
ithou
tp
aren
tsu
pp
ort:
19.5
2(3
.50)
;C
:18
.96
(3.2
8)
Toev
alua
teth
eef
fect
sof
a2-
year
mid
dle
scho
olPA
and
heal
thy
food
inte
rven
tion,
incl
udin
gan
envi
ronm
enta
land
com
put
er-t
ailo
red
com
pon
ent
onB
MI
and
BM
Iz-
scor
ein
boy
san
dg
irls.
21m
onth
s(t
wo
scho
olye
ars)
I(p
aren
tsu
pp
ort)
:21
%I
(with
out
par
ent
sup
por
t):
28%
C:
22%
Kai
net
al.
2004
(30)
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
Pos
tho
cp
ower
0.8,
alp
ha0.
05
Set
ting
:Fi
vep
rimar
ysc
hool
sin
San
tiag
o,C
uric
o,C
asab
lanc
a,C
hile
Par
ticip
ants
:M
ale/
fem
ale:
I:53
.5%
/46.
5%;
C:
52%
/48%
Ag
e10
.6(2
.6)
(Ap
pro
xim
atel
y35
%re
ceiv
edsc
hool
lunc
hp
rog
ram
me)
.
I:23
75C
:12
02
I:19
.6(3
.8)
n=
2141
C:
19.2
(3.6
)n
=94
5
Toev
alua
tea
scho
ol-b
ased
nutr
ition
educ
atio
nan
dPA
inte
rven
tion
onad
ipos
ityan
dp
hysi
calfi
tnes
s.
6m
onth
s
I:10
%C
:21
%
Luep
ker
etal
.19
96(4
7)(C
ATC
H)
RC
T
Clu
ster
by
scho
ol
Sam
ple
size
det
erm
ined
–ad
equa
tely
pow
ered
Set
ting
:96
pub
licst
ate
scho
ols
in12
scho
old
istr
icts
inC
alifo
rnia
,Lo
uisi
ana,
Min
neso
taan
dTe
xas
Par
ticip
ants
:M
ale/
fem
ale:
2645
/246
1A
ge
8.76
Eth
nica
llyd
iver
se(w
hite
,A
fric
an–A
mer
ican
and
His
pan
ic).
I+C
:51
06
I:17
.68
(3.2
3),
1627
C:
17.5
8(2
.90)
,23
32
Toev
alua
tea
scho
ol-b
ased
inte
rven
tion
incl
udin
ga
hom
ep
rog
ram
me
for
the
prim
ary
pre
vent
ion
ofca
rdio
vasc
ular
dis
ease
.
3ye
ars
I+C
:20
%
Man
ios
etal
.19
98,
1999
,20
02(2
4–26
)K
afat
oset
al.
2007
(22)
(Cre
tan
Hea
lthan
dN
utrit
ion
Ed
ucat
ion
Pro
gra
m)
CC
T
Uni
tof
assi
gnm
ent
was
scho
ol
Pow
erno
tst
ated
Set
ting
:P
rimar
ysc
hool
sin
Irak
lioan
dR
ethi
mno
(inte
rven
tion)
and
Cha
nia
(con
trol)
Cre
te,
Gre
ece
Par
ticip
ants
:M
ale/
fem
ale:
509/
453
Ag
e5.
5–6.
5
I:60
2C
:44
4
I:16
.2(2
.2),
231
C:
16.3
(2.3
),16
2
Toev
alua
tea
scho
ol-b
ased
inte
rven
tion
invo
lvin
ga
heal
than
dnu
triti
onel
emen
tan
da
phy
sica
lfitn
ess
and
activ
ityel
emen
t,on
chro
nic
dis
ease
risk
fact
ors
I:un
clea
rC
:un
clea
rse
par
ate
rand
omsa
mp
les
anal
ysed
at3
year
s,6
year
san
d10
year
s
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 127
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le4
Con
tinue
d
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
nB
MI
(SD
)kg
m-2
Aim
Follo
w-u
p/n
otas
sess
ed%
Ros
enb
aum
etal
.20
07(1
2)R
CT
Clu
ster
by
clas
s
Pow
erno
tst
ated
Set
ting
:N
ewYo
rkC
ityp
ublic
scho
ol
Par
ticip
ants
:M
ale/
fem
ale:
31/4
2A
ge
14ye
ars
Firs
tor
seco
ndg
ener
atio
nin
the
US
maj
ority
with
orig
ins
inth
eD
omin
ican
Rep
ublic
(His
pan
ic).
53%
with
know
naf
fect
edfir
stor
seco
ndd
egre
ere
lativ
ew
ithty
pe
IId
iab
etes
I+C
:79
I:24
.7(1
.4)
n=
49C
:24
.3(1
.8)
n=
24
Toev
alua
teth
eef
fect
ofsc
hool
-bas
edin
terv
entio
nco
nsis
ting
ofhe
alth
,nu
triti
onan
dex
erci
secl
asse
sp
lus
anae
rob
icex
erci
sep
rog
ram
me
ond
iab
etes
risk.
12w
eeks
I+C
:8%
Sah
ota
etal
.20
01(3
2)
AP
PLE
S
RC
T
Clu
ster
by
scho
ol
80%
pow
erto
det
ect
diff
eren
cein
mea
nsof
ano
rmal
lyd
istr
ibut
edou
tcom
em
easu
reof
atle
ast
1.8
SD
at5%
sig
nific
ance
leve
l
Set
ting
:10
prim
ary
scho
ols
inLe
eds,
UK
Par
ticip
ants
:B
oys
and
girl
sA
ge
8(7
–11)
I:31
4C
:32
2
BM
IS
Dsc
ore:
I:0.
12(1
.01)
C:
0.04
(1.1
7)
Ass
esse
dth
eim
pac
tof
ap
rimar
ysc
hool
-bas
edin
terv
entio
n,w
hich
incl
uded
teac
her
trai
ning
,m
odifi
catio
nof
scho
olm
eals
,th
ed
evel
opm
ent
ofsc
hool
actio
np
lans
targ
etin
gth
ecu
rric
ulum
,P
E,
tuck
shop
san
dp
layg
roun
dac
tiviti
es.
1ye
ar
I:7%
C:
6%
Sal
liset
al.
2003
(27)
RC
T
Clu
ster
,sc
hool
sra
ndom
ized
by
dis
tric
t
Pow
erno
tst
ated
Set
ting
:24
pub
licm
idd
lesc
hool
sin
San
Die
go
Cou
nty,
Cal
iforn
ia,
US
A
Par
ticip
ants
:49
%fe
mal
e,44
.5%
non-
whi
te,
39.5
%re
ceiv
edfre
eor
red
uced
scho
olm
eals
,36
.4%
wer
eb
usse
dto
scho
ol.
Mea
nag
eno
tre
por
ted
.
Mea
nen
rolm
ent
acro
ss24
scho
ols
was
1109
(SD
356)
stud
ents
per
scho
ol
BM
Ino
tre
por
ted
Toev
alua
teth
eef
fect
sof
envi
ronm
enta
l,p
olic
yan
dso
cial
mar
ketin
gin
terv
entio
nson
PAan
dfa
tin
take
ofm
idd
lesc
hool
stud
ents
.
Two
scho
olye
ars
Num
ber
asse
ssed
inea
chg
roup
atfo
llow
-up
not
rep
orte
d
Sin
gh
etal
.20
07(1
4)
(Dut
chO
bes
ityIn
terv
entio
nin
Teen
ager
s[D
OiT
stud
y])
RC
T
Clu
ster
,b
ysc
hool
orlo
catio
nan
dst
ratifi
edb
yur
ban
vs.
rura
l
Sam
ple
size
of50
0–60
0fro
m16
scho
ols
was
req
uire
d–
stud
yad
equa
tely
pow
ered
Set
ting
:18
pre
voca
tiona
lsec
ond
ary
scho
ols
(of
the
low
est
educ
atio
nall
evel
),th
eN
ethe
rland
s
Par
ticip
ants
:M
ale/
fem
ale:
492/
561
Ag
e12
.7
I:60
0C
:45
3
Ig
irls:
19.0
(3.0
)C
girl
s:19
.48
(3.3
8)I
boy
s:18
.16
(2.6
4)C
boy
s:19
.05
(2.8
6)
Toev
alua
tew
heth
era
scho
ol-b
ased
mul
ti-co
mp
onen
the
alth
pro
mot
ion
for
Dut
chad
oles
cent
sw
ould
be
succ
essf
ulin
pos
itive
lyin
fluen
cing
bod
yco
mp
ositi
ons
and
aero
bic
fitne
ss.
8m
onth
s
I+C
:7%
128 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le4
Con
tinue
d
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
nB
MI
(SD
)kg
m-2
Aim
Follo
w-u
p/n
otas
sess
ed%
Sp
ieg
elet
al.
2006
(15)
(Wel
lnes
sA
cad
emic
san
dYo
u[W
AYst
udy]
)
RC
T
Pow
er:
sam
ple
size
not
men
tione
db
utre
lativ
ely
larg
esa
mp
le
Set
ting
:69
clas
ses,
16el
emen
tary
scho
ols
acro
ssfo
urst
ates
,U
SA
Par
ticip
ants
:S
tud
ents
info
urth
and
fifth
gra
de
I:un
clea
r(5
34co
mp
lete
d)
C:
uncl
ear
(479
com
ple
ted
)
Mea
nb
asel
ine
BM
I:no
tst
ated
.39
.4%
cont
rola
nd36
.4%
inte
rven
tion
wer
eov
erw
eig
htor
atris
kfo
rov
erw
eig
ht.
Toev
alua
teth
eef
fect
iven
ess
ofa
mul
tidis
cip
linar
yel
emen
tary
scho
ol-b
ased
inte
rven
tion.
6m
onth
s
I:13
.7%
C:
16.2
%
Tayl
oret
al.
2007
(20)
(AP
ilot
for
Life
styl
ean
dE
xerc
ise
–A
PP
LEp
roje
ct)
CC
T
Pilo
tst
udy
Stu
dy
had
pot
entia
lto
det
ect
anef
fect
size
of0.
3in
any
ofth
em
easu
res
with
80%
pow
erw
ithth
eus
eof
5%le
velo
fsi
gni
fican
ce
Set
ting
:se
ven
prim
ary
scho
ols
in2
com
mun
ities
,O
tag
o,N
ewZ
eala
nd
Par
ticip
ants
:M
ale/
fem
ale:
246/
223
Ag
e7.
7(5
–12)
82.6
%w
hite
Inte
rven
tion
child
ren
wer
ele
aner
(P=
0.00
4)w
ithsm
alle
rw
aist
circ
umfe
renc
e(P
=0.
001)
I:27
9C
:23
4
I:17
.4(2
.4)
n=
250
C:
18.2
(3.3
)n
=21
9
Tod
eter
min
eef
fect
iven
ess
ofa
2-ye
arco
ntro
lled
com
mun
ity-b
ased
inte
rven
tion
top
reve
ntex
cess
ive
wei
ght
gai
nin
5–12
-yea
r-ol
dch
ildre
nb
yen
hanc
ing
opp
ortu
nitie
sfo
rhe
alth
yea
ting
and
non-
curr
icul
arPA
.
2ye
ars
I:un
clea
rC
:un
clea
rC
hild
ren
enro
lled
atd
iffer
ent
time
poi
nts
Trev
ino
etal
.20
04(4
8),
Trev
ino
2005
(49)
RC
T
Clu
ster
Pow
erno
tst
ated
Set
ting
:N
ine
Ele
men
tary
scho
ols
loca
ted
inlo
w-in
com
ein
ner
city
neig
hbou
rhoo
ds
ofth
eS
anA
nton
ioIn
dep
end
ent
Sch
ool
Dis
tric
t,TX
,U
SA
Par
ticip
ants
:M
ale/
fem
ale:
47%
/53%
Ag
eI:
9.8;
C:
9.7
97%
ofst
uden
tsw
ere
Mex
ican
–Am
eric
an,
mor
eth
an95
%w
ere
inth
eU
SD
epar
tmen
tof
Ag
ricul
ture
food
assi
stan
cep
rog
ram
s,av
erag
eof
3.5
peo
ple
occu
pie
dea
chho
useh
old
,m
ean
hous
ehol
din
com
esU
S$1
033
7in
the
inte
rven
tion
gro
upan
dU
S$1
169
1in
the
cont
rols
choo
ls.
I:20
0C
:18
9
Ib
oys:
19.2
3(4
.78)
Ig
irls:
18.9
2(4
.87)
Cb
oys:
19.1
8(4
.14)
Cg
irls:
19.9
0(5
.42)
Toev
alua
teth
eef
fect
ofth
eB
iene
star
Hea
lthP
rog
ram
(pro
gra
mm
ed
esig
ned
tore
duc
eris
kfa
ctor
sas
soci
ated
with
the
onse
tof
typ
e2
dia
bet
es)
onp
hysi
calfi
tnes
sin
low
-inco
me
Mex
ican
–Am
eric
anch
ildre
n.
8m
onth
s
I:0%
C:
1%
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 129
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Tab
le4
Con
tinue
d
Stu
dy
Des
ign/
pow
erP
opul
atio
nN
umb
er/b
asel
ine
mea
nB
MI
(SD
)kg
m-2
Aim
Follo
w-u
p/n
otas
sess
ed%
Vand
ong
enet
al.
1995
(50)
RC
T
Clu
ster
by
scho
ol
Pow
erca
lcul
atio
nsb
ased
onal
pha
leve
l0.0
5an
db
eta
leve
lof
0.8
tod
etec
td
iffer
ence
offiv
ela
ps
ofLe
ger
run
with
aS
Dof
14
Set
ting
:30
scho
ols
inW
este
rnA
ustr
alia
Par
ticip
ants
:A
ge
10–1
2
Fitn
ess
gro
up:
n=
81b
oys
and
77g
irls
Fitn
ess
and
scho
olnu
triti
ong
roup
:n
=81
boy
san
d81
girl
s
Sch
ooln
utrit
ion
gro
up:
n=
91b
oys
and
108
girl
s
Sch
oola
ndho
me
nutr
ition
gro
up:
n=
58b
oys
and
68g
irls
Hom
enu
triti
ong
roup
:n
=97
boy
san
d84
girl
s
Con
trolg
roup
:n
=78
boy
san
d67
girl
s.
BM
I(k
gm
-2)
atb
asel
ine:
Fitn
ess
gro
up:
18.2
(17.
7–18
.7)
boy
s,18
.2(1
7.7–
18.7
)g
irls.
Fitn
ess
and
scho
olnu
triti
ong
roup
:18
.1(1
7.5–
18.8
)b
oys,
17.9
(17.
4–18
.5)
girl
s
Sch
ooln
utrit
ion
gro
up:
18.0
(17.
5–18
.5)
boy
s,17
.5(1
7.0–
17.9
)g
irls
Sch
oola
ndho
me
nutr
ition
gro
up:
18.2
(17.
4–19
.0)
boy
s,17
.5(1
6.8–
18.2
)g
irls
Hom
enu
triti
ong
roup
:17
.7(1
7.2–
18.1
)b
oys,
18.2
(16.
9,18
.9)
girl
s
Con
trolg
roup
:18
.1(1
7.5–
18.6
)b
oys,
17.6
(16.
9–18
.3)
girl
s
Toev
alua
tep
rog
ram
me
offit
ness
and
nutr
ition
alon
ean
dco
mb
ined
and
scho
olan
dho
me-
bas
ednu
triti
onp
rog
ram
mes
toim
pro
veca
rdio
vasc
ular
heal
th.
9m
onth
s
All
gro
ups:
15%
War
ren
etal
.20
03(3
1)(B
eS
mar
t)R
CT
Ind
ivid
uals
rand
omiz
ed
Not
pow
ered
Set
ting
:Th
ree
prim
ary
scho
ols
inO
xfor
d,
UK
Par
ticip
ants
:C
hild
ren
Ag
e5–
7
Nut
ritio
nin
terv
entio
n:56
;PA
inte
rven
tion:
54;
Com
bin
ednu
triti
onan
dPA
inte
rven
tion:
54;
C:
54
Nut
ritio
nin
terv
entio
n:16
.1(2
.7)
PAin
terv
entio
n:16
.0(2
.0)
Com
bin
ednu
triti
onan
dPA
inte
rven
tion:
15.8
(2.0
)C
:15
.5(1
.6)
Be
Sm
art
was
asc
hool
and
fam
ily-b
ased
inte
rven
tion
top
reve
ntob
esity
inch
ildre
nag
ed5–
7ye
ars.
20-w
eek
inte
rven
tion
over
14m
onth
s.
Nut
ritio
nin
terv
entio
n:25
%PA
inte
rven
tion:
22%
Com
bin
ednu
triti
onan
dPA
inte
rven
tion:
22%
C:
15%
Will
iam
son
etal
.20
07(1
9)
(Wis
eM
ind
Pro
ject
)
RC
T
Clu
ster
by
scho
ol
Pilo
tst
udy,
not
pow
ered
tod
etec
tsi
gni
fican
td
iffer
ence
s
Set
ting
:Fo
urp
rivat
eC
atho
licsc
hool
s,U
SA
Par
ticip
ants
:M
ale/
fem
ale:
333/
328
Ag
e9.
294
.9%
whi
te
I:31
3C
(act
ive
cont
rol):
348
Mea
nb
asel
ine
BM
I:no
tst
ated
.B
MI
per
cent
ileof
allc
hild
ren
atb
asel
ine:
59.8
(30.
34)
Wei
ght
for
allc
hild
ren
atb
asel
ine:
35.7
kg(1
2.21
)
Tote
stw
heth
eran
envi
ronm
enta
lap
pro
ach
for
wei
ght
gai
np
reve
ntio
nd
eliv
ered
insc
hool
sw
asm
ore
effe
ctiv
efo
rw
eig
htg
ain
pre
vent
ion
inco
mp
aris
onw
ithan
activ
eco
ntro
lp
rog
ram
me
that
used
anen
viro
nmen
tala
pp
roac
hto
pre
vent
sub
stan
ceab
use.
18m
onth
s(2
acad
emic
year
s)
I:10
%A
ctiv
eC
:13
%
PA,
phy
sica
lact
ivity
;P
E,
phy
sica
led
ucat
ion;
SPA
RK
,S
por
ts,
Pla
yan
dA
ctiv
eR
ecre
atio
nfo
rK
ids;
BM
I,b
ody
mas
sin
dex
;S
D,
stan
dar
dd
evia
tion;
RC
T,ra
ndom
ized
cont
rolle
dtr
ial;
CC
T,co
ntro
lled
clin
ical
tria
l;I,
inte
rven
tion;
C,
cont
rol;
SE
S,
soci
oeco
nom
icst
atus
.
130 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Table 5 Results of included studies
Study Results Comments
DIET ONLY STUDIESAmaro et al. 2006 (4) Change in BMI z-score at 24 weeks was not significantly different between
intervention and control (controlling for baseline values) 0.345 (95% CI 0.299 to0.390) vs. 0.405 (0.345 to 0.465).
Significant baseline difference betweengroups on BMI z-score.
Ask et al. 2006 (5) BMI increased – statistically significant in both male and female in the controlgroup (P < 0.01 for male and P < 0.05 for female), but not in the interventiongroup.
James et al. 2004(23)
(CHOPPS)
Change in BMI over 12 months not significantly different between interventionand control 0.7 (0.2) vs. 0.8 (0.3) kg m-2.
Percentage of overweight and obese children increased in the control groupby 7.5% at 12-months compared with a decrease in the intervention group of0.2% (mean difference 7.7%, 95% CI 2.2, 13.1).
Assessed at 3 years: age and sex-specific BMI z-scores (SD scores) hadincreased in the control group by 0.10 (SD 0.53) but decreased in theintervention group by -0.01 (SD 0.58), with a mean difference of 0.10 (95% CI-0.00 to 0.21, P = 0.06).
The prevalence of overweight increased in both the intervention and controlgroup at 3 years and the significant difference between the groups seen at 12months was no longer evident.
Mean change in BMI:Intervention: 1.88 (SD 1.71)Control: 2.14 (SD 1.64)Mean difference of 0.26 (-0.07 to 0.58, P = 0.12)
The waist circumference increased in both groups after 3 years with a meandifference of 0.09 (-0.06 to 0.26, P = 0.25).
PA ONLY STUDIESFlores 1995 (35) Statistically significant reductions in BMI between intervention and control girls
at 12 weeks:Intervention girls: 22.1 (SD 6.0); Control girls 22.5 (SD 4.4)
This represents a change of -0.8 kg m-2 in the intervention group and+0.3 kg m-2 in the control group (P < 0.05).
No statistically significant change between intervention and control boys forBMI (BMI -0.2 kg m-2 intervention boys vs. -0.6 kg m-2 control boys).
Harrison et al. 2006(9)
(Switch Off – GetActive)
No statistically significant change between intervention and control for BMI,-0.08 (95% CI -0.38 to 0.22, P = 0.63)
Jamner et al. 2004(40)
The intervention had no significant effect on BMI percentile, 67.28 at baselineand 66.74 at 4 months; % body fat 32.64 at baseline and 31.85 at 4 months.
Lazaar 2007 (10) Average BMI remained unchanged overtime; however, there was significantdifference between groups for BMI (for both genders and obese andnon-obese).
The pattern of response to PA intervention was similar in girls and boysalthough the magnitude of change in anthropometric variables was greater ingirls. There was a greater response in obese children than non-obese children.
Mo-suwan et al. 1998(46)
Both intervention and control groups experienced reduction in BMI and notsignificantly different between groups at 30 weeks:
One school had swim class for 1 h perweek (adjustments made for thesechildren).Intervention: 15.76 (2.46)
Control: 15.94 (2.26)
Not significant.
No significant difference between groups in skin-fold thickness at 30 weeks.
Intervention girls had significantly lower mean BMI at 30 weeks thanintervention boys (P < 0.01).
Intervention girls had lower likelihood of having an increased BMI slope thanthe control girls (OR 0.32; 95% CI 0.18, 0.56).
Pangrazi et al. 2003(43)
No significant differences between groups were found for BMI.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 131
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Table 5 Continued
Study Results Comments
Pate et al. 2005 (38) % Girls classified as overweight or at risk for overweight (at least 85thpercentile BMI 34% both groups) or overweight (at least 95th percentile BMI17% both groups) did not differ between intervention and control.
Slightly higher % African–Americangirls lost to follow-up.
Robbins et al. 2006(11)
‘Girls on the Move’
No significant differences between intervention vs. control and pre vs. postBMI.
Robinson 1999 (36) Compared with controls, children in the intervention group had statisticallysignificant relative decreases in BMI -0.45 kg m-2 with 95% CI -0.73, -0.17,P = 0.002; TSF -1.47 mm with 95% CI -2.41, -0.54, P = 0.002; and waist-to-hipratio -0.02 with 95% CI -0.03, -0.01, P < 0.001.
Assessors blinded
Sallis et al. 1993,1997 (41,42)
Specialist PA promotion programme did not produce significant reductions inchildren’s BMI or adiposity. No differences observed between teacher-led andspecialist-led programme.
Interim results only (2-year data from3-year study).
All boys in all three groups increased their BMI over 2 years.
Control girls had significantly lower BMI than girls in either teacher-led orspecialist-led intervention group (P < 0.01).
Actual data for BMI and skin-foldthickness is only presented in graphicalform.
Changes in skin-fold thickness not significant between groups in girls or boys.
Schofield et al. 2005(39)
No significant difference between groups for BMI or from baseline to follow-up.
Stephens & Wentz1998 (37)
Control group gained significantly more weight (P < 0.001). Weight (kg)intervention vs. control at 15 weeks = 25.8 vs. 27.0.
Significantly more black children inintervention compared with controlgroup (P < 0.01).Significant decrease in skin-fold thickness intervention vs. control, P < 0.01.
Baseline: 25 vs. 26 mm
15 weeks: 23.5 vs. 28.5 mm
Trudeau 2000 (44),Trudeau et al. 2001(45)
(The Trois-RiveriesGrowth andDevelopment study)
No significant difference between intervention and control with respect to BMI,body fat, skin-fold thickness, waist-to-hip ratio (Trudeau 2000). Baseline valuesnot reported.
Random selected sample (22% oforiginal group) contacted by telephonefor follow-up.
Comparisons of tracking suggested intervention and control developed similargains in BMI and skin-fold thickness over 22-year interval (Trudeau et al. 2001).
Change in BMI (kg m-2) over 22-year intervention vs. control: 5.7 (0.4) female(n = 57), 8.6 (0.4) male (n = 56) vs. 5.8 (0.3) female (n = 38), 8.0 (0.2) male(n = 40).
BMI was not significantly different between intervention and control groups atage 10, 11, 12 and 34 years.
Skin-fold thickness change also available (not significant between groups).
Valdimarsson et al.2006 (16),Linden et al. 2006(17)
(POP Study)
Mean annual change in weight:Intervention: 3.9 kg (1.6) n = 49Control: 3.2 kg (1.3) n = 50
Control group exercised more duringleisure time at baseline compared withintervention groups.
Viskic-Stalec et al.2007 (18)
Initially greater baseline body weight in intervention group decreased andbody weight in control group remained almost unchanged. Dance activitieshad the most favourable effect on body weight.
Initially greater baseline body weight inintervention group
Change in BMI: I: -0.74 n = 115; C: +0.47 n 102
COMBINED DIET AND PA STUDIESCaballero et al. 2003(33)
(Pathways)
No significant difference in weight, BMI, % body fat or skin-fold thicknessbetween intervention and control groups. BMI in the intervention group atbaseline was 19.0, at follow-up 22.0. In the control group BMI was 19.1 kg m-2
at baseline and 22.2 kg m-2 at follow-up. Mean difference in BMI = -0.2 (95%CI -0.50, 0.15) kg m-2.
% body fat increased by approximately 7% in both groups at 3 years.
132 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Table 5 Continued
Study Results Comments
Danielzik et al. 2007(6)
(KOPS)
Median change in BMI (inter-quartile range): Significant difference in median BMI atbaseline between groups – lower incontrol.
I: 1.7 (0.7, 3.1);C: 1.8 (0.9, 3.3)
Non-significant difference between groups re BMI. Intervention increasedremission of overweight with no significant effect on incidence – effect morepronounced in girls.
Donnelly et al. 1996(34)
Significant increase in BMI in both groups from baseline to follow-up but nosignificant difference between groups.
Eliakim et al. 2007 (7) Significant between group difference in BMI (intervention BMI remained sameas baseline and control BMI increased).
Gortmaker et al. 1999(28);
(Planet Health)
At 2 years: prevalence of obesity among girls in the intervention schools wasreduced compared with controls, controlling for baseline obesity (OR 0.47;95% CI 0.24, 0.93; P = 0.03).
Outcome assessors blinded.
Among boys obesity declined among both control and intervention students;however, after controlling for covariates, there was no significant difference inoutcome (OR 0.85; 95% CI 0.52, 1.39, P = 0.48).
There was greater remission of obesity among intervention girls vs. control girls(OR 2.16; 95% CI 1.07, 4.35, P = 0.04).
Graf et al. 2005 (29) The increase in BMI tended to be lower in those undergoing intervention meandifference in BMI for the intervention and control groups were 0.27 kg m-2 and0.66 kg m-2 respectively (P = 0.069).
Intervention group had higher BMI,waist circumference and bloodpressure at baseline than control.
After intervention, the increase in waist circumference with time was lower thanthe controls (3.11 cm and 4.56 cm respectively).
Body weight showed high correlationswith the result of bioelectric analyses(r = 0.770, P � 0.001) and waistcircumference (r = 0.857, P � 0.001),and low correlation with the waist-to-hipratio (r = 0.180, P = 0.001) adjusted forgender and age.
Haerens et al. 2006(8)
A significant gender by condition interaction was found. Therefore, results arepresented separately for boys and girls.
In girls, BMI and BMI z-score increased significantly less in the interventionwith parental support group compared with the control group (P < 0.05) or theintervention – alone group (P = 0.05). In boys, no significant positiveintervention effects were found.
Kain et al. 2004 (30) BMI significantly higher in control boys only at 6 months compared withintervention boys (intervention boys BMI maintained while control boys BMIincreased).
Significantly more obese in interventionschools.
Luepker et al. 1996(47)
(CATCH)
BMI did not differ significantly between groups at 3 years.
Manios et al. 1998,1999, 2002 (24–26)
At 3 years:Change in BMI (kg m-2) +0.7 (1.5) vs. +1.7 (1.4) intervention vs. control,P < 0.0005.
At 6 years:BMI change intervention vs. control: +3.68 (SE 0.16) n = 356 vs. +4.28 (SE0.16) n = 285, P < 0.05
At 6 years:Bicep skin-fold thickness (mm) change intervention vs. control: +2.97 (SE 0.24)n = 356 vs. +4.47 (SE 0.24) n = 285, P < 0.001.
At 6 years:Tricep skin-fold thickness (mm) change intervention vs. control: +6.46 (SE 0.38)n = 356 vs. +7.90 (SE 0.39) n = 285, P < 0.0
At 10 years:BMI z-scoreIntervention: -0.09 (0.09) n = 85;Control: 0.17 (0.09), n = 91, P = 0.042
Kafatos et al. 2007(22)
(Cretan Health andNutrition EducationProgram)
Rosenbaum et al.2007 (12)
BMI (and % body fat) significantly lower in intervention group compared withcontrol and compared with baseline.
Classroom element was mandatorywhereas exercise element wasvoluntary.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 133
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Table 5 Continued
Study Results Comments
Sahota et al. 2001(32)
(APPLES)
At 1 year, there was no difference in change in BMI between the children inthe two groups (BMI SD score, weighted mean difference 0 (95% CI -0.1, 0.1).
Sallis et al. 2003 (27) There was a significant reduction in BMI among intervention boys, comparedwith control boys, but there was no effect for girls.
Boys BMI (kg m-2) at baseline for the intervention and control groups, 20.12(0.98) and 19.68 (0.63) respectively. BMI for the controls and the boys in theintervention group after 2 years 20.04 (0.85) and 19.84 (0.61).
Girls BMI (kg m-2) at baseline for the intervention and control groups, 19.76(0.77) and 19.52 (0.89) respectively. BMI for the girls in the intervention groupand the controls after 2 years 19.88 (1.16) and 19.73 (1.16) respectively.
Gender-specific analyses revealed the time by condition interaction wassignificant for boys (F = 12.16, P = 0.00) with a large effect size of d = 1.10.The intervention was not significant for girls (F = 0.73, P = 0.396), and theeffect size was small.
Singh et al. 2007 (14)
(Dutch ObesityIntervention inTeenagers [DOiTstudy])
BMI
Intervention vs. control girls: -0.05 (95% CI -0.18 to 0.08)
Intervention vs. control boys: -0.02 (95% CI -0.11 to 0.16)
No significant intervention effects were found for BMI (or BMI class) althoughtended to favour intervention group.
Spiegel et al. 2006(15)
Change in BMI: Intervention: 0.1606; Control: 0.5210, P = 0.01
Significant shifts in BMI were noted in the intervention group, with a 2%reduction in overweight (BMI > 85% for age and sex) youth in the interventiongroup There was no significant shift in the comparison group, but there was anotable reduction in the intervention group in overweight and at risk foroverweight classification, which was most significant at the at risk foroverweight (BMI-for-age between 85% to 95%) level.
Taylor et al. 2007 (20)
(A Pilot for Lifestyleand Exercise –APPLE project)
Mean BMI z-score was significantly lower in intervention children than incontrol children by 0.09 (95% CI: 0.01, 0.18) after 1 year and 0.26 (95% CI:0.21, 0.32) at 2 years. Changes in BMI did not result from variation in heightz-scores but rather from differences in relative weight between intervention andcontrol children over time. Waist circumference was also significantly lower at 2years in intervention children (-1.0 cm). The prevalence of overweight did notdiffer between the intervention and control groups.
Participants recruited in 2003 werefollowed up at 2004 and 2005;participants recruited at 2004 werefollowed up at 2005.
An interaction existed between intervention group and overweight status(P = 0.029), such that mean BMI z-score was reduced in normal-weight (-0.29;95% CI: -0.38, -0.21) but not overweight (-0.02; 95% CI: -0.16, 0.12)intervention children relative to controls.
Trevino et al. 2004(48), Trevino 2005(49)
% body fat: did not differ between groups; adjusted difference intervention(n = 619) vs. control (n = 602) +0.18 (95% CI, -1.75–2.11), P = 0.56
Vandongen et al.1995 (50)
No significant difference between groups for sub scapular skin-fold thickness(mm), % body fat or BMI (kg m-2) respectively at 1 year:
Triceps skin-fold thickness decreased significantly in fitness + school nutritiongroup compared with controls.
Warren et al. 2003(31)
No significant changes in the rates of overweight and obesity were seen as aresult of the three different approaches
Subject numbers too small forstatistical analyses;This study may have been subject toceiling effects as the study populationwas relatively well educated as 39% ofparents had obtained either a degreeor a post-graduate qualification.
Williamson et al. 2007(19)
(Wise Mind Project)
Both programmes associated with significant weight gain prevention inchildren with higher BMI z-scores at baseline.
All students within the schools wereexposed to the environmentalintervention.
CHOPPS, the Christchurch obesity prevention programme in schools; PA, physical activity; CI, confidence interval; BMI, body mass index; SD, standard deviation; OR, oddsratio; SE, standard error; TSF, tricep skinfold; I, intervention; C, control.
134 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Two hours extra physical education (PE) per week sig-nificantly improved BMI compared with control at 6months but did not significantly change BMI overtime (10).There was a greater magnitude of change in girls comparedwith boys and in obese compared with non-obese children.The study was set in 19 primary schools in France among425 7-year-old children.
A 6 month intervention to encourage reduction in TV,videotape and video game usage (18 lessons of 30–50 min,self-monitoring and a 7 h TV use budget per week) in9-year-olds resulted in significant reduction in BMI, skin-fold thickness, waist circumference and waist-to-hip ratioin intervention children compared with controls (36). Themean difference in BMI (adjusted for baseline age and sex)was -0.45 kg m-2 (95% CI -0.73, -0.17; P = 0.002).
A 15-week PA intervention in low-income, minorityschool children (mean age 8 years) demonstrated signifi-cantly more weight gain among controls and significantdecreases in skin-fold thickness among interventionchildren (37).
A 12-week aerobic dance intervention (150 min of danceper week over three sessions) in African–American andHispanic children (mean age 13 years) significantly reducedBMI but only among intervention girls compared withcontrol girls (-0.8 kg m-2 and 0.3 kg m-2 respectively) (35).
A 30-week aerobic exercise programme – encouraging apre-class walk and three 20-min aerobic sessions per week– in kindergarten children (aged 4–5 years) in Thailandproduced results that varied by gender (46). A reduction inBMI occurred in both intervention and control groups andwas not significantly different between groups. However,the intervention girls had significantly lower mean BMI at30 weeks than intervention boys (P < 0.01) and lower like-lihood of having an increased BMI slope than the controlgirls (odds ratio: 0.32; 95% CI: 0.18, 0.56).
Ten of the studies did not report significant improve-ments in mean BMI or percentage of overweight. Five ofthese studies were among female adolescents in secondaryschools. These included a 6-month intervention promotinga supportive school environment and programme cham-pion (38), a 12-week intervention targeting moderateactivity (walking) in low-active girls (39), a 4-month inter-vention promoting additional PE classes (40), a 12-weekintervention including individual counselling from a schoolnurse (11) and an aerobic, dance and gymnastic pro-gramme (66 sessions) over one academic year in 16–18-year-olds in Croatia (18).
Five studies among children (aged 8–10 years) found nodifference in mean BMI or weight between control andintervention groups. These included a 12-week PA pro-gramme supplementary to usual PE (43), a 2-year specialistPA programme (41,42), a 16-week intervention to reduceTV and computer game usage in 312 children from nineprimary schools in Ireland (9), a 2-year intervention to
improve bone mineral content in 53 girls from four primaryschools in Sweden (16,17) and a 22-year follow-up in a22% subsample of a 6-year PA intervention in primaryschool children in Quebec (44,45).
Three of the five studies among children included head-to-head comparisons. The 2-year specialist PA programme(41,42), Sports, Play and Active Recreation for Kids, wascompared with trained teacher-led PA and a usual PEcontrol group. Both the specialist and teacher-led interven-tions provided three 30-min sessions of PA per week.Results for boys showed that the control group had signifi-cantly lower BMI at 6 and 12-months (P = 0.05), but not at18-months. All boys in all three groups increased their BMIover 2 years. Girls’ results showed the control group tohave lower BMI at each time point and this reached sig-nificance at 18-months (P < 0.01).
The 12-week PA programme supplementary to usual PE(43) had four conditions: PLAY and PE, PLAY only, PEonly and control (no PE or PLAY). No significant differ-ences were found at 12 weeks between the intervention orcontrol groups for BMI.
The 12-week intervention among low-active high schoolgirls in Australia (39) compared the use of a pedometer toencourage increase in steps walked and a group encouragedto increase time in activity compared with control. Nosignificant differences were found between the three groupsfor BMI at 12 weeks or from baseline to follow-up for anygroup.
Diet and physical activity interventionsTwenty studies (6–8,12–15,19,20,22,24–34,47–50) aimedto increase PA and improve diet among school children.Three of these studies aimed to prevent cardiovasculardisease and two aimed to reduce the risk of developingdiabetes.
Diet and physical activity studies demonstratingsignificant and positive effect between interventionand control groupsNine (7,8,12,15,20,22,24–28,30) of the 20 studies showedsignificant improvements in mean BMI in the interventioncompared with the control groups; one study (Kiel ObesityPrevention study [KOPS]) (6) showed both significant andnon-significant results and one study nearly reached signifi-cance (29). There were two studies in boys only (27,30)(non-significant in girls), two studies in girls only (8,28)(non-significant in boys) and five studies in both girls andboys.
A 6-month dietary education and sport intervention(including active recess, healthy kiosks, special activitiesand parental involvement) in over 3500 11-year-old chil-dren in five primary schools in Chile maintained baselineBMI in intervention boys while BMI in control boysincreased (30). This resulted in a significant difference
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 135
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

between groups at 6 months for boys only (non-significantdifference in BMI at 6 months for girls).
An environmental, policy and social marketing interven-tion in over 1100 11–13-year-old children in 24 middleschools in the USA showed significant reduction in BMI inthe intervention boys (but not girls) compared with controlover two school years (27).
‘Planet Health’ (28) promoted PA, modification ofdietary intake and reduction of sedentary behaviours (witha strong emphasis on reducing TV viewing) in over 1500children aged 12 years in 10 secondary schools in the USA.The intervention significantly reduced the prevalence ofobesity (odds ratio 0.47, 95% CI 0.24, 0.93, P = 0.03) andincreased remission of obesity in intervention girls com-pared with control girls over two school years. There wasno significant difference in prevalence of obesity betweenintervention boys and control boys.
One intervention combined environmental changes withpersonal computer-tailored feedback on BMI, with andwithout parental support, compared with control in nearly3000 13-year-olds in 15 middle schools in Belgium. Theintervention included 4.7 h extra PE per week. In girls, BMIand BMI z-score increased significantly less in the inter-vention with parental support group compared with thecontrol group (P < 0.05) or the intervention-alone group(P = 0.05). In boys, no significant positive interventioneffects were found after two school years (8).
A diet and activity intervention that aimed to preventcardiovascular disease in school children in Crete by adapt-ing the ‘Know Your Body’ programme showed significantimprovements compared with control at 3 and 6 years forBMI and skin-folds. At 3 years the change in BMI was0.7 kg m-2 (standard deviation [SD] 1.5) in the interventiongroup compared with 1.7 kg m-2 (SD 1.4) in the controlgroup (P < 0.0005) (24,25). At 6 years, the change inBMI (mean and standard error [SE]) was 3.68 kg m-2 (SE0.16, n = 356) in the intervention group compared with4.28 kg m-2 (SE 0.16, n = 285) in the control group(P < 0.05) (26). At 10 years, the mean change in BMIz-score was -0.09 (SD 0.09, n = 85) in the interventiongroup and 0.17 (SD 0.09, n = 91) in the control group(P = 0.042) (22).
A 12-week diet and activity intervention to reduce riskof diabetes showed a significant improvement in percent-age of body fat and BMI compared with control in 7314-year-old adolescents in one New York public school.These adolescents were first or second generationmigrants to the USA, mainly from the Dominican Repub-lic, and 53% had a first or second degree relative withtype II diabetes (12).
The APPLE study of 460 8-year-old children from sevenprimary schools in the USA significantly reduced the rate ofexcessive weight gain in children at 2 years, although thismay be limited to those not initially overweight. BMI
z-score was significantly lower in intervention than incontrol children by a mean of 0.09 (95% CI: 0.01, 0.18) at1 year and 0.26 (95% CI: 0.21, 0.32) at 2 years, but theprevalence of overweight did not differ. An interactionexisted between intervention group and overweight status(P = 0.029), such that mean BMI z-score was reduced innormal weight (-0.29; 95% CI: -0.38, -0.21) but notoverweight (-0.02; 95% CI: -0.16, 0.12) intervention chil-dren relative to controls (20).
The WAY programme was a PA and wellness programmethat was incorporated into the curriculum. It included somefamily involvement in approximately 1000 9–11-year-olds(US grade 4–5) in 16 primary schools in the USA. At6-months, there was a significant reduction in risk of devel-oping overweight and a 2% reduction in overweight(BMI > 85% for age and sex) in the intervention group butnot the control group. BMI in the intervention vs. controlchildren was 0.16 kg m-2 vs. 0.52 kg m-2 (P = 0.01) at 6months (15).
A 14-week nutrition education and circuit training plusencouragement to reduce sedentary behaviours resulted ina significant difference in BMI in approximately 100 5–6-year-old children in four pre-schools in Israel. The BMIremained stable in the intervention children and increasedby 0.3 kg m-2 in the control children (7).
A 3.8-year follow-up of the KOPS longitudinal data in2200 6-year-olds in 32 primary schools in Germanyincreased remission of overweight with no significant effecton incidence; this effect was more pronounced in girls.However, there was significant difference in median BMI atbaseline between the groups (lower BMI in control group)(6).
The STEP TWO programme in over 1600 8-year-oldchildren in seven primary schools in Germany demon-strated that the increase in BMI and waist circumferencetended to be lower in those undergoing intervention com-pared with controls (BMI 0.27 kg m-2 vs. 0.66 kg m-2,P = 0.069 respectively) (29).
Diet and physical activity studies demonstratingnon-significant effect between intervention andcontrol groupsTwo studies that found no significant difference in meanBMI between intervention and control children wereUK-based. One study (Be Smart) (31) of approximately 1005–7-year-old children was insufficiently powered to detectdifferences in BMI at 14 months’ follow-up. AnotherUK-based study (Active Programme Promoting Lifestyle inSchools [APPLES]) (32) that was sufficiently poweredincluded teacher training, modification of school meals,school action plans targeting the curriculum, PE, tuckshops and playground activities. The intervention wasunderpinned by the Health-Promoting Schools philosophyand the intervention involved the whole school community
136 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

including parents, teachers and catering staff. At 1 year,there was no significant difference in change in BMIbetween the children in the two groups.
An additional seven studies reported that interventionhad no effect on BMI. Six of these studies were in primaryschool children. These included a 3-year PA and dietaryintervention included modifying school lunches in over1700 8-year-old American–Indian children (33), a 2-yearUS-based intervention included modifying school lunches(34) in over 300 9-year-old children, a large 3-year cardio-vascular risk reduction programme (47), a 1-year pro-gramme to improve cardiovascular health (50), a study(48,49) that aimed to prevent diabetes in over 1200 low-income Mexican–American 9-year-olds and a pilot study(The Wise Mind Project) (19) in 661 9-year-old childrenfrom four private Catholic schools in the USA comparingan environmental approach for weight gain preventionwith an environmental approach to prevent substanceabuse. Both active interventions were associated with sig-nificant weight gain prevention in children with higher BMIz-scores at baseline.
One study that did not show a significant difference inBMI between intervention and control groups was in ado-lescents. The 8-month Dutch Obesity Intervention in Teen-agers study (13,14) included environmental changes to theschool canteen in nearly 1000 13-year-olds in 18 secondaryschools in the Netherlands.
Process evaluations
Information on process and process evaluations wereeither not reported as part of the studies included in thisreview or included but with little detail (except [32]). Themajority of the interventions were at least in part pro-vided by existing staff that were trained by research staff.There was a tendency for the combined diet and PA inter-ventions to involve more school personnel and for theintervention to be integrated into the curriculum. Theredid not appear to be a pattern that these interventions(that were more likely to be sustainable) were more likelyto be successful.
There was no consistent pattern to the results in terms offamily involvement.
Process evaluations indicate that these lifestyle interven-tions may be better implemented if built into the curricu-lum. Overall, authors reported that parents respondedpositively to diet and PA changes but this did not necessar-ily lead to behaviour change or change in BMI. However, itis of course the level of engagement with the interventionthat has an impact on involvement, and this was notreported in any meaningful way in any of the papersincluded in this review.
Male adolescents who ate breakfast at school for 4months reported a significant increase in school content-
ment (P < 0.05) (5). The students missed the free breakfastprovision when it was stopped; however, teachers were notsatisfied with the serving of breakfasts in classrooms.
The 12-week PA intervention by Robbins et al. (11)reported that the school nurses experienced difficulty coun-selling some girls who lacked places, resources and socialsupport for engaging in PA. Some girls expressed that theirparents discouraged PA at home because of the noise andthe low importance placed on being physically active ascompared with doing homework or chores.
Planet Health (28) reported that schools experiencedwith interdisciplinary curricula found it easier to imple-ment Planet Health material. Another study reported thatPE was implemented because it was incorporated into thecurriculum (30).
The UK-based APPLES (32) intervention was successfulin changing the ethos of the schools and the attitudes of thechildren, but had little effect on children’s behaviour otherthan a modest increase in the consumption of vegetables.Eighty-nine per cent of the actions points were imple-mented in the 10 schools and changes were made to foodprovision. Both parents and teachers were supportive of thedietary education and promotion of PA. Parental question-naires (64% returned) suggested improvements such aspromotion of healthier break-time snacks with enforce-ment by school, material on healthy eating for children andfun PA ideas. Of the 20 teachers invited, 19 attended andwere satisfied with the training, resources and materialsoffered. Children had higher scores for knowledge andattitudes, and were positive about the intervention in focusgroups.
One UK-based feasibility study (31) considered the sus-tainability of their intervention and concluded that it wouldbe too expensive and unsustainable as it was delivered bynon-school personnel. Children enjoyed the practical tasks,quizzes and tasting. Eighty-three per cent of parentsthought their child had benefited from the programme andall teachers thought that components should be integratedinto the personal, social and health education curriculum.
Pathways (33) was a culturally sensitive diet and PAintervention. The classroom curriculum was delivered suc-cessfully (94%) and the food service guidelines were imple-mented (78%), with most schools achieving the minimumPE sessions per week. Parents who attended the familyevents responded positively. The intervention was designedto be delivered by existing staff and was integrated into theschool curriculum. Despite all these elements, this relativelylarge 3-year study did not significantly improve children’sweight or BMI.
Discussion
This review expands and updates the evidence base oflifestyle interventions to prevent obesity in school children.
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 137
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

The rate of publications of interventions to preventobesity in school children is increasing dramatically.Twenty-three studies were identified between 1990 and2005. An additional 15 studies were identified between2006 and September 2007. The percentage of studies set insecondary schools is increasing. Seven of the 15 studiesidentified in the update search are based in secondaryschools, whereas only six of the original 23 studies werebased in secondary schools.
One of three (33%) diet studies, five of 15 (33%) PAstudies and nine of 20 (45%) combined diet and PA studiesdemonstrated significant differences between interventionand control for BMI.
There is insufficient evidence to assess the effectiveness ofdietary interventions to prevent obesity in school childrenor the relative effectiveness of diet vs. PA interventions.
School-based interventions to increase PA and reducesedentary behaviour may help children to maintain ahealthy weight but the results are inconsistent and short-term. PA interventions may be more successful in youngerchildren and in girls.
Two PA interventions that aimed to reduce sedentarybehaviour by reducing TV viewing and video/computergames in 9–10-year-olds produced conflicting results.
Six PA interventions included dance (two studies were ingirls only and four studies in boys and girls). Of these sixstudies, two were successful in reducing BMI in interven-tion girls but not boys (35,46) and four studies were unsuc-cessful (18,38,40) with one study (41,42) demonstrating asignificantly lower BMI in control girls compared withintervention girls (regardless of whether the PA interven-tion was led by a specialist or a teacher).
The effectiveness of combined diet and PA school-basedinterventions to prevent obesity is equivocal.
The majority of the longer-term studies (at least 1 year)were combined diet and PA interventions. The diet and PAinterventions also tended to be larger studies comparedwith the diet studies and the PA studies. However, overallthere did not appear to be a consistent pattern betweensignificant effect and the size and duration of the study. Itwas not the case that all large long-term studies, under-pinned by theory, involving existing school staff, the wholeschool community and significant environmental modifica-tions, were successful. It is not clear whether it is moreeffective to target single or multiple behaviour change out-comes (energy restriction and increased PA). There is someevidence of effectiveness for both simultaneous and sequen-tial behaviour change interventions (56). The developmentof health behaviour theory of multiple behaviour changehas the potential to create better understanding of whysome ‘simple’ interventions appear more effective thanmore complex interventions and vice versa (57). This willenable more effective behaviour change interventions toprevent obesity in children.
Some interventions showed different and inconsistenteffects for girls and boys (aged 10–14 years) and thereasons for this are unclear. Two of the combined diet andPA interventions significantly improved BMI in boys butnot girls and two combined diet and PA interventions sig-nificantly improved BMI in girls but not boys. All fourstudies were in children aged between 10 and 14 years andit may be that in this age group genders respond differentlyto different elements of the interventions.
It is interesting that some interventions appear to vary ineffectiveness according to gender, age or weight status of thechildren. Although some studies only recruited childrenfrom ethnic minorities, none of the other studies assessedweight according to ethnic minority status. None of theincluded studies assessed weight by socioeconomic status. Apaper on KOPS (published after the search for this review)showed that the intervention was associated with a reducedcumulative 4-year incidence of overweight only in childrenfrom families with high socioeconomic status (SES) (58).
Some studies were not adequately powered to detectdifferences between the intervention and control groups.Some studies were pilot studies to test the feasibility of theintervention. It is unclear whether some of the interventionswere of sufficient length or intensity to produce a changeweight or BMI.
Assessment of effectiveness can be exacerbated by weak-nesses in assessment measures. For example, there is highintraindividual variance in movement measured by pedom-eters or accelerometers reaching >20% (59). Although age-specific BMI is the most commonly used definition ofoverweight and reported outcome for these studies, otherproxy measures for assessing body fatness are useful andwould provide a more comprehensive picture of childhoodoverweight both at specific time points and across time.Indeed skin-fold thickness of adolescents has been shownto be a better predictor of high body fatness in adultscompared with BMI (60).
The majority of the studies did not provide adequatedata for meta-analysis and in some cases it was necessaryto rely on authors’ reporting of significant or non-significant effects of the interventions. The studies wereheterogeneous in terms of design, participants, interven-tion and outcomes, making it difficult to generalize aboutwhat interventions are effective in preventing obesity.Existing studies and initiatives need to be better evaluatedusing quantitative and qualitative outcomes and focusingon study and study population characteristics that mayimpact on effectiveness. There is a need for research toview behaviour change within the context of an obe-sogenic environment (61) and the co-dependency of thesuccess of prevention interventions upon a ‘paradigm shiftin thinking’ (62).
In conclusion, the findings are inconsistent, but overallsuggest that combined diet and PA interventions may help
138 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

to prevent children becoming overweight in the long term.Dietary interventions such as providing breakfast foradolescents and PA interventions particularly in girls inprimary schools may help to prevent these children frombecoming overweight in the short term.
Conflict of Interest Statement
No conflict of interest was declared.
Acknowledgements
Brown and Summerbell thank the following: Janis Eklund,Leonard Epstein, Stef Kremers, Chantal Simon, SamSpiegel, Jean Wiecha and Lukas Zahner for providing clari-fication, and Magnus Karlsson, Leen Haerens, AmikaSingh and Natasa Viskic-Stalec for additional data.
References
1. World Health Organisation. The challenge of obesity inEurope. World wide web 2007. [WWW document]. URL http://www.euoro.who.int/document/E90711.pff (accessed July 2008).2. Parsons TJ, Power C, Logan S, Summerbell CD. Childhoodpredictors of adult obesity; a systematic review. Int J Obes 1999;23(Suppl. 12): S1–S10.3. National Institute for Health and Clinical Excellence (NICE).Obesity: The Prevention, Identification, Assessment and Manage-ment of Overweight and Obesity in Adults and Children. Clinicalguideline. CG43. National Institute for Health and Clinical Excel-lence (NICE): London, 2006. Ref Type: Report.4. Amaro S, Viggiano A, Di Costanzo A, Madeo I, Viggiano A,Baccari ME, Marchitelli E, Raia M, Viggiano E, Deepak S, MondaM, De Luca B. Kaledo, a new educational board-game, givesnutritional rudiments and encourages healthy eating in children: apilot cluster randomized trial. Eur J Pediatr 2006; 165: 630–635.5. Ask AS, Hernes S, Aarek I, Johannessen G, Haugen M. Changesin dietary pattern in 15-year-old adolescents following a 4 monthdietary intervention with school breakfast – a pilot study. Nutr J2006; 5: 33.6. Danielzik S, Pust S, Muller MJ. School-based interventions toprevent overweight and obesity in prepubertal children: processand 4 years outcome evaluation of the Kiel Obesity PreventionStudy (KOPS). Acta Paediatr Suppl 2007; 96: 19–25.7. Eliakim A, Nemet D, Balakirski Y, Epstein Y. The effects ofnutritional-physical activity school-based intervention on fatnessand fitness in preschool children. J Pediatr Endocrinol 2007; 20:711–718.8. Haerens L, Deforche B, Maes L, Stevens V, Cardon G, DeBourdeaudhuij I. Body mass effects of a physical activity andhealthy food intervention in middle schools. Obesity (SilverSpring) 2006; 14: 847–854.9. Harrison M, Burns CF, McGuinness M, Heslin J, Murphy NM.Influence of a health education intervention on physical activityand screen time in primary school children: ‘Switch Off – GetActive’. J Sci Med Sport 2006; 9: 388–394.10. Lazaar N, Aucouturier J, Ratel S, Rance M, Meyer M, DucheP. Effect of physical activity intervention on body composition inyoung children: Influence of body mass index status and gender.Acta Paediatrica Int J Paediatr 2007; 96: 1315–1320.
11. Robbins LB, Gretebeck KA, Kazanis AS, Pender NJ. Girls onthe move program to increase physical activity participation. NursRes 2006; 55: 206–216.12. Rosenbaum M, Nonas C, Weil R, Horlick M, Fennoy I,Vargas I, Kringas P, El Camino Diabetes Prevention Group.School-based intervention acutely improves insulin sensitivity anddecreases inflammatory markers and body fatness in junior highschool students [see comment]. J Clin Endocrinol Metab 2007; 92:504–508.13. Singh ASC. Design of the Dutch Obesity Intervention in Teen-agers (NRG-DOiT): systematic development, implementation andevaluation of a school-based intervention aimed at the preventionof excessive weight gain in adolescents. BMC Public Health 2006;304: 6. Article Number: 304.14. Singh AS, Chinapaw MJ, Brug J, van Mechelen W. Short-termeffects of school-based weight gain prevention among adolescents[see comment]. Arch Pediatr Adolesc Med 2007; 161: 565–571.15. Spiegel SA, Foulk D. Reducing overweight through a multi-disciplinary school-based intervention. Obesity (Silver Spring)2006; 14: 88–96.16. Valdimarsson O, Linden C, Johnell O, Gardsell P, KarlssonMK. Daily physical education in the school curriculum in prepu-bertal girls during 1 year is followed by an increase in bone mineralaccrual and bone width – data from the prospective controlledMalmo pediatric osteoporosis prevention study. Calcif Tissue Int2006; 78: 65–71.17. Linden C, Ahlborg HG, Besjakov J, Gardsell P, Karlsson MK.A school curriculum-based exercise program increases bonemineral accrual and bone size in prepubertal girls: 2-year datafrom the pediatric osteoporosis prevention (POP) study. J BoneMiner Res 2006; 21: 829–835.18. Viskic-Stalec N, Stalec J, Kati R, Podvorac D, Katovi D. Theimpact of dance-aerobics training on the morpho-motor status infemale high-schoolers. Coll Antropol 2007; 31: 259–266.19. Williamson DA, Copeland AL, Anton SD, Champagne C, HanH, Lewis L, Martin C, Newton RL Jr. Sothern M, Stewart T, RyanD. Wise Mind Project: a school-based environmental approach forpreventing weight gain in children. Obesity (Silver Spring) 2007;15: 906–917.20. Taylor RW, McAuley KA, Barbezat W, Strong A, WilliamsSM, Mann J. APPLE Project: 2-y findings of a community-basedobesity prevention program in primary school-age children. Am JClin Nutr 2007; 86: 735–742. Ref Type: Journal (Full).21. James J, Thomas P, Kerr D. Preventing childhood obesity:2-year follow-up results from the Christchurch obesity preventionprogramme in schools (CHOPPS). BMJ 2007; 335: 762. Ref Type:Journal (Full).22. Kafatos I, Manios Y, Moschandreas J, Kafatos A, PreventiveMedicine and Nutrition Clinic University of Crete Research Team.Health and nutrition education program in primary schools ofCrete: changes in blood pressure over 10 years. Eur J Clin Nutr2007; 61: 837–845.23. James J, Thomas P, Cavan D, Kerr D. Preventing childhoodobesity by reducing consumption of carbonated drinks: clusterrandomised controlled trial. BMJ 2004; 328: 1237–1239.24. Manios Y, Kafatos A, Mamalakis G. The effects of a healtheducation intervention initiated at first grade over a 3-year period:physical activity and fitness indices. Health Educ Res 1998; 13:593–606.25. Manios Y, Moschandreas J, Hatzis C, Kafatos A. Evaluation ofa health and nutrition education program in primary school chil-dren of Crete over a 3-year period. Prev Med 1999; 28: 149–159.26. Manios Y, Moschandreas J, Hatzis C, Kafatos A. Health andnutrition education in primary schools of Crete: changes in chronic
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 139
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

disease risk factors following a 6-year intervention programme.Br J Nutr 2002; 88: 315–324.27. Sallis JF, McKenzie TL, Conway TL, Elder JP, Prochaska JJ,Brown M, Zive MM, Marshall SJ, Alcaraz JE. Environmentalinterventions for eating and physical activity: a randomized con-trolled trial in middle schools. Am J Prev Med 2003; 24: 209–217.28. Gortmaker SL, Peterson K, Wiecha J, Sobol AM, Dixit S, FoxMK, Laird N. Reducing obesity via a school-based interdiscipli-nary intervention among youth: Planet Health. Arch PediatrAdolesc Med 1999; 153: 409–418.29. Graf C, Rost SV, Koch B, Heinen S, Falkowski G, Dordel S,Bjarnason-Wehrens B, Sreeram N, Brockmeier K, Christ H, PredelHG. Data from the STEP TWO programme showing the effect onblood pressure and different parameters for obesity in overweightand obese primary school children. Cardiol Young 2005; 15: 291–298.30. Kain J, Uauy R, Albala C, Vio F, Cerda R, Leyton B. School-based obesity prevention in Chilean primary school children:methodology and evaluation of a controlled study. Int J Obes2004; 28: 483–493.31. Warren JM, Henry CJ, Lightowler HJ, Bradshaw SM,Perwaiz S. Evaluation of a pilot school programme aimed at theprevention of obesity in children. Health Promot Int 2003; 18:287–296.32. Sahota P, Rudolf MC, Dixey R, Hill AJ, Barth JH, Cade J.Randomised controlled trial of primary school based interventionto reduce risk factors for obesity. BMJ 2001; 323: 1029–1032.33. Caballero B, Clay T, Davis SM, Ethelbah B, Rock BH,Lohman T, Norman J, Story M, Stone EJ, Stephenson L, Stevens J,Pathways Study Research Group. Pathways: a school-based, ran-domized controlled trial for the prevention of obesity in American–Indian schoolchildren. Am J Clin Nutr 2003; 78: 1030–1038.34. Donnelly JE, Jacobsen DJ, Whatley JE, Hill JO, Swift LL,Cherrington A, Polk B, Tran ZV, Reed G. Nutrition and physicalactivity program to attenuate obesity and promote physical andmetabolic fitness in elementary school children. Obes Res 1996; 4:229–243.35. Flores R. Dance for health: improving fitness in African–American and Hispanic adolescents. Public Health Rep 1995; 110:189–193.36. Robinson TN. Reducing children’s television viewing toprevent obesity: a randomized controlled trial. JAMA 1999; 282:1561–1567.37. Stephens MB, Wentz SW. Supplemental fitness activities andfitness in urban elementary school classrooms. Fam Med 1998; 30:220–223.38. Pate RR, Ward DS, Saunders RP, Felton G, Dishman RK,Dowda M. Promotion of physical activity among high-school girls:a randomized controlled trial. Am J Public Health 2005; 95:1582–1587.39. Schofield L, Mummery WK, Schofield G. Effects of a con-trolled pedometer-intervention trial for low-active adolescent girls.Med Sci Sports Exerc 2005; 37: 1414–1420.40. Jamner MS, Spruijt-Metz D, Bassin S, Cooper DM. A con-trolled evaluation of a school-based intervention to promote physi-cal activity among sedentary adolescent females: project FAB.J Adolesc Health 2004; 34: 279–289.41. Sallis JF, McKenzie TL, Alcaraz JE, Kolody B, Hovell MF,Nader PR. Project SPARK. Effects of physical education onadiposity in children. Ann N Y Acad Sci 1993; 699: 127–136.42. Sallis JF, McKenzie TL, Alcaraz JE, Kolody B, Faucette N,Hovell MF. The effects of a 2-year physical education program(SPARK) on physical activity and fitness in elementary school
students. Sports, Play and Active Recreation for Kids. Am J PublicHealth 1997; 87: 1328–1334.43. Pangrazi RP, Beighle A, Vehige T, Vack C. Impact of Promot-ing Lifestyle Activity for Youth (PLAY) on children’s physicalactivity. J Sch Health 2003; 73: 317–321.44. Trudeau F. Follow-up of participants in the TROIS-Riveresgrowth and development study: examining their health-relatedfitness and fisk factors as adults. Am J Hum Biol 2000; 12: 207–213.45. Trudeau F, Shephard RJ, Arsenault F, Laurencelle L. Changesin adiposity and body mass index from late childhood to adultlife in the Trois-Rivieres study. Am J Hum Biol 2001; 13: 349–355.46. Mo-suwan L, Pongprapai S, Junjana C, Puetpaiboon A.Effects of a controlled trial of a school-based exercise program onthe obesity indexes of preschool children. Am J Clin Nutr 1998;68: 1006–1011.47. Luepker RV, Perry CL, McKinlay SM, Nader PR, Parcel GS,Stone EJ, Stone EJ, Webber LS, Elder JP, Feldman HA, JohnsonCC et al. Outcomes of a field trial to improve children’s dietarypatterns and physical activity. The Child and Adolescent Trial forCardiovascular Health. CATCH collaborative group. JAMA 1996;275: 768–776.48. Trevino RP, Yin Z, Hernandez A, Hale DE, Garcia OA,Mobley C. Impact of the Bienestar school-based diabetes mellitusprevention program on fasting capillary glucose levels: a random-ized controlled trial 44. Arch Pediatr Adolesc Med 2004; 158:911–917.49. Trevino RP. Effect of the Bienestar health program on physicalfitness in low-income Mexican–American Children. Hispanic JBehav Sci 2005; 27: 120–132.50. Vandongen R, Jenner DA, Thompson C, Taggart AC, SpickettEE, Burke V, Beilin LJ, Milligan RA, Dunbar DL. A controlledevaluation of a fitness and nutrition intervention program on car-diovascular health in 10- to 12-year-old children. Prev Med 1995;24: 9–22.51. Simon C, Wagner A, Platat C, Arveiler D, Schweitzer B,Schlienger JL, Triby E. ICAPS: a multilevel program to improvephysical activity in adolescents. Diabetes Metab 2006; 32: 41–49.52. Zahner L, Puder JJ, Roth R, Schmid M, Guldimann R, PuhseU, Knopfli M, Braun-Fahrlander C, Marti B, Kriemler S. A school-based physical activity program to improve health and fitness inchildren aged 6–13 years (Kinder-Sportstudie KISS): study designof a randomized controlled trial [ISRCTN15360785]. BMC PublicHealth 2006; 6: 147.53. Austin SB, Kim J, Wiecha J, Troped PJ, Feldman HA, PetersonKE. School-based overweight preventive intervention lowers inci-dence of disordered weight-control behaviors in early adolescentgirls. Arch Pediatr Adolesc Med 2007; 161: 865–869.54. Jurg ME, Kremers SP, Candel MJ, Van der Wal MF, De MeijJS. A controlled trial of a school-based environmental interventionto improve physical activity in Dutch children: JUMP-in, kids inmotion. Health Promot Int 2006; 21: 320–330.55. Evenson KR, Scott MM, Cohen DA, Voorhees CC. Girls’perception of neighborhood factors on physical activity, sedentarybehavior, and body mass index: the trial of activity for adolescentgirls. Obesity 2007; 15: 430–445. Ref Type: Journal (Full).56. Prochaska JO. Multiple Health Behavior Research representsthe future of preventive medicine. Prev Med 2008; 46: 281–285.57. Noar SM, Chabot M, Zimmerman RS. Applying healthbehavior theory to multiple behavior change: considerations andapproaches. Prev Med 2008; 46: 275–280.58. Plachta-Danielzik S, Pust S, Asbeck I, Czerwinski-Mast M,Langnäse K, Fischer C, Bosy-Westphal A, Kriwy P, Müller M.
140 Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell obesity reviews
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Four-year follow-up of school-based intervention on overweightchildren: the KOPS study. Obesity 2007; 15: 3159–3169.59. Bader N, Bosy-Westphal A, Dilba B, Müller MJ. Intra- andinter-individual variability of resting energy expenditure in healthymale subjects – biological and methodological variability of restingenergy expenditure. Br J Nutr 2005; 94: 843–849.60. Nooyens ACJ, Koppe LLJ, Visscher TLS, Twisk JWR, KemperHCG, Schuit AJ, van Mechelen W, Seidell JC. Adolescent skinfoldthickness is a better predictor of high body fatness in adults than isbody mass index: the Amsterdam Growth and Health Longitudi-nal Study. Am J Clin Nutr 2007; 85: 1533–1539.
61. Swinburn B, Egger G, Raza F. Dissecting obesogenic environ-ments: the development and application of a framework for iden-tifying and prioritizing environmental interventions for obesity.Prev Med 1999; 29: 563–570.62. Government Office for Science. ‘Tackling Obesity: FutureChoices – Project Report’. Department for Innovation, Universitiesand Skills: London, 2007. [WWW document]. URL http://www.foresight.gov.uk/Obesity/obesity_final/17.pdf (accessed July2008).
obesity reviews Preventing obesity in school-children – an update to NICE T. Brown & C. Summerbell 141
© 2008 The AuthorsJournal compilation © 2008 International Association for the Study of Obesity. obesity reviews 10, 110–141

Related Documents











