REVIEW Systematic review and meta-analysis of prophylactic mesh placement for prevention of incisional hernia following midline laparotomy A. Bhangu • J. E. Fitzgerald • P. Singh • N. Battersby • P. Marriott • T. Pinkney Received: 10 February 2013 / Accepted: 18 May 2013 / Published online: 28 May 2013 Ó Springer-Verlag France 2013 Abstract Purpose Incisional hernia is a common long-term com- plication after laparotomy. This study investigated whether prophylactic mesh reinforcement of laparotomy reduced the rate of incisional hernia, with emphasis on trial design and quality. Methods A systematic review of published literature was performed for studies comparing incisional hernia presence following conventional closure or prophylactic mesh rein- forcement. Studies were assessed using the Cochrane Risk of Bias Tool, the Jadad score and the Newcastle Ottawa Scale (NOS). The primary endpoint was incisional hernia, assessed by meta-analysis. Results Seven studies [four randomised controlled trials (RCTs) and three prospective trials] included 588 patients; 262 received mesh reinforcement. All studies included elective patients at high risk of incisional hernia. Six incorporated a polypropylene mesh and one a biologic mesh. Four studies were judged high quality by NOS and two of four RCTs were at low risk of bias, although overall outcome assessment from all studies was either poor or mediocre. Mesh significantly reduced the rate of incisional hernia [odds ratio (OR) 0.15, p \ 0.001]; the same effect was seen in RCTs only (OR 0.17, p \ 0.001). A borderline increase of seroma seen with a fixed effect model (OR 1.82, p = 0.050) was not seen with a random effect model (OR 1.86, p = 0.210, I 2 = 45 %). Conclusion Mesh reinforcement of laparotomy signifi- cantly reduced the rate of incisional hernia in high-risk patients. However, poor assessment of secondary outcomes limits applicability; routine placement in all patients cannot yet be recommended. More evidence regarding the rates of adverse events, cost-benefits and quality of life are needed. Keywords Hernia Á Prophylaxis Á Mesh Á Incisional hernia Introduction Incisional hernia following laparotomy is one of the most frequent long-term complications, affecting 20 % of unselected patients and up to 50 % of high-risk (e.g. obese) patients [1, 2]. This can lead to significant morbidity including pain, deformity, emergency re-admission and re- operation, with a resultant financial burden [1]. Incisional hernia repair is strongly associated with recurrence, leading to further morbidity and patient dissatisfaction, together with the associated healthcare and economic costs [3]. Comorbidities that increase the likelihood of incisional hernia following laparotomy include diabetes, pulmonary disease and connective tissue disorders, such as aneurysmal disease [4]. Amongst these higher risk individuals, incidence of post-operative hernia can reach 50 % [5]. The INLINE study meta-analysed the optimal method for sutured closure On behalf of the West Midlands Research Collaborative. Committee of the West Midlands Research Collaborative—David Bartlett, Kaori Futaba, Pritesh Mistry, Caroline Richardson, Elizabeth Hepburn, Abhilasha Patel, Paul Marriott, Andrew Torrance, Dion Morton. Electronic supplementary material The online version of this article (doi:10.1007/s10029-013-1119-2) contains supplementary material, which is available to authorized users. A. Bhangu (&) Á J. E. Fitzgerald Á P. Singh Á N. Battersby Á P. Marriott Á T. Pinkney Academic Department of Surgery, Room 29, 4th Floor, Queen Elizabeth Hospital, Edgbaston, Birmingham B15 2TH, UK e-mail: [email protected] 123 Hernia (2013) 17:445–455 DOI 10.1007/s10029-013-1119-2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
REVIEW
Systematic review and meta-analysis of prophylactic meshplacement for prevention of incisional hernia following midlinelaparotomy
A. Bhangu • J. E. Fitzgerald • P. Singh •
N. Battersby • P. Marriott • T. Pinkney
Received: 10 February 2013 / Accepted: 18 May 2013 / Published online: 28 May 2013
� Springer-Verlag France 2013
Abstract
Purpose Incisional hernia is a common long-term com-
plication after laparotomy. This study investigated whether
prophylactic mesh reinforcement of laparotomy reduced
the rate of incisional hernia, with emphasis on trial design
and quality.
Methods A systematic review of published literature was
performed for studies comparing incisional hernia presence
following conventional closure or prophylactic mesh rein-
forcement. Studies were assessed using the Cochrane Risk
of Bias Tool, the Jadad score and the Newcastle Ottawa
Scale (NOS). The primary endpoint was incisional hernia,
assessed by meta-analysis.
Results Seven studies [four randomised controlled trials
(RCTs) and three prospective trials] included 588 patients;
262 received mesh reinforcement. All studies included
elective patients at high risk of incisional hernia. Six
incorporated a polypropylene mesh and one a biologic
mesh. Four studies were judged high quality by NOS and
two of four RCTs were at low risk of bias, although overall
outcome assessment from all studies was either poor or
mediocre. Mesh significantly reduced the rate of incisional
hernia [odds ratio (OR) 0.15, p \ 0.001]; the same effect
was seen in RCTs only (OR 0.17, p \ 0.001). A borderline
increase of seroma seen with a fixed effect model (OR
1.82, p = 0.050) was not seen with a random effect model
(OR 1.86, p = 0.210, I2 = 45 %).
Conclusion Mesh reinforcement of laparotomy signifi-
cantly reduced the rate of incisional hernia in high-risk
patients. However, poor assessment of secondary outcomes
limits applicability; routine placement in all patients cannot
yet be recommended. More evidence regarding the rates of
adverse events, cost-benefits and quality of life are needed.
Keywords Hernia � Prophylaxis � Mesh � Incisional
hernia
Introduction
Incisional hernia following laparotomy is one of the most
frequent long-term complications, affecting 20 % of
unselected patients and up to 50 % of high-risk (e.g. obese)
patients [1, 2]. This can lead to significant morbidity
including pain, deformity, emergency re-admission and re-
operation, with a resultant financial burden [1]. Incisional
hernia repair is strongly associated with recurrence, leading
to further morbidity and patient dissatisfaction, together
with the associated healthcare and economic costs [3].
Comorbidities that increase the likelihood of incisional
hernia following laparotomy include diabetes, pulmonary
disease and connective tissue disorders, such as aneurysmal
disease [4]. Amongst these higher risk individuals, incidence
of post-operative hernia can reach 50 % [5]. The INLINE
study meta-analysed the optimal method for sutured closure
On behalf of the West Midlands Research Collaborative.
Committee of the West Midlands Research Collaborative—David
Bartlett, Kaori Futaba, Pritesh Mistry, Caroline Richardson, Elizabeth
Hepburn, Abhilasha Patel, Paul Marriott, Andrew Torrance, Dion
Morton.
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10029-013-1119-2) contains supplementarymaterial, which is available to authorized users.
A. Bhangu (&) � J. E. Fitzgerald � P. Singh � N. Battersby �P. Marriott � T. Pinkney
Academic Department of Surgery, Room 29, 4th Floor, Queen
Elizabeth Hospital, Edgbaston, Birmingham B15 2TH, UK
e-mail: [email protected]
123
Hernia (2013) 17:445–455
DOI 10.1007/s10029-013-1119-2

of elective midline laparotomy, and found convincing evi-
dence that a continuous, slowly absorbable suture provided
the optimum risk reduction of incisional hernia [2]. Addi-
tional measures to further reduce this risk, even following
optimum sutured closure, require investigation.
Prophylactic mesh reinforcement of midline wounds has
the potential to be an effective intervention in reducing the
risk of incisional hernia formation. Due to the possibility of
adverse effects and increased costs, several questions
remain. Firstly, specific patient groups who will benefit are
yet to be established. Secondly, the adverse event profile
requires definition, particularly regarding the risk of ser-
oma, haematoma and surgical site infection following mesh
implantation. Finally, the cost-effectiveness requires anal-
ysis, including changes in the duration of the index surgical
procedure. This systematic review aimed to determine
whether prophylactic mesh reinforcement of laparotomy
wounds reduced the rate of incisional hernia, with partic-
ular emphasis on the methodological quality of included
studies.
Methods
Data sources and search strategy
A pre-specified study protocol for this systematic review
was designed and registered with the PROSPERO database
(International Prospective Register of Systematic Reviews,
www.crd.york.ac.uk/prospero, record number: CRD4201
2003179). A systematic search of the OVID SP version of
Medline, Pubmed version of Medline, Embase, the Coch-
rane Library, ClinicalTrials.gov and Google Scholar was
performed for published studies comparing mesh closure
versus conventional closure following laparotomy for any
reason. To assess contemporary evidence, only studies
published after 1980 were included and no language
restrictions were applied. The search was performed
independently by two researchers. The search strategies
used are presented in supplemental table 1. MeSH terms
were used to search Medline and Embase. A manual search
of reference lists in relevant systematic reviews was
undertaken to further identify trials of potential interest.
Abstracts and conference proceedings were excluded
because of the high probability of incomplete data. Cita-
tions were collated with EndNote Reference Manager
(Version X4, Thomson Reuters) and duplicates removed.
The last search was performed in October 2012.
Inclusion and exclusion criteria
To be included, studies had to satisfy the following pre-
determined criteria: (1) include midline laparotomy only;
(2) report post-operative incisional hernia rate (as either
primary or secondary endpoint); (3) design was a ran-
domised controlled trial, prospective observational or ret-
rospective cohort study; (4) published after 1980; (5)
reporting ten or more patients.
Studies were excluded if they: (1) were designed as case
reports, letters, or with \10 patients; (2) considered par-
astomal hernia prevention; (3) included management of the
open abdomen (i.e. in relation to a planned fascial defect).
Data extraction
Two authors extracted data independently. Discrepancies
in outcome extraction were resolved by re-examination and
discussion of the relevant study to achieve consensus. Data
extracted on study design included: randomisation tech-
nique, intervention arms, method of linea alba closure, type
of mesh, definition of incisional hernia. Details relating to
patients included: number, age, gender, operation indica-
tion, presence of diabetes, cardiovascular disease, con-
nective tissue disease, obesity, smoking, mean length of
incision and previous abdominal surgery/laparotomy. The
primary outcome assessed for meta-analysis was the rate of
incisional hernia. Secondary outcomes recorded were rates
of adverse events.
Assessment of bias and study quality
Risk of bias and study quality was assessed in several
ways, in order to allow a multi-domain comparison and to
allow comparison between randomised and non-random-
ised studies. Two reviewers independently allocated study
quality and disagreement was resolved by re-examining the
relevant paper until consensus was achieved.
Firstly, all studies were evaluated using the Newcastle–
Ottawa Scale (NOS) [6]. This assessment examined three
factors: method of patient selection, comparability of the
study groups and number of outcomes reported. Although
initially intended to quality assess non-randomised studies,
the fields were adapted to suit the study population and
outcome measures in the present meta-analysis, and was
applied to all included studies irrespective of design. A score
of seven and above was used to indicate high quality [7].
Secondly, the Cochrane Risk of Bias Tool was used for
randomised trials [8]. The risk of bias tool covers six
domains of bias: selection bias, performance bias, detection
bias, attrition bias, reporting bias, and other bias. Each
domain was scored as a high or low risk of bias and an
overall high and low risk status was assigned. Studies with
inadequate randomisation, unblinded outcome assessment,
and high ([10 %) or unexplained losses to follow-up were
considered to be factors for high risk of bias. Thirdly, the
Jadad scale was used to score RCTs in the domains of
446 Hernia (2013) 17:445–455
123

randomisation, blinding and losses to follow-up using the
five available points (supplemental table 2) [9]. Fourthly,
details on measures used to determine and record outcomes
were collated. Finally, a pre-specified assessment of pub-
lication bias was performed by means of a funnel plot.
Statistical analysis
Meta-analysis was conducted according to guidelines from
the Preferred Reporting Items for Systematic reviews and
Meta-Analysis group (PRISMA) [10]. The odds ratio (OR)
was used as the statistical measure for dichotomous out-
comes and the weighted mean difference (WMD) for
continuous variables. ORs were calculated from the origi-
nal data and meta-analysed using the Mantel–Haenszel
method. An OR of [1.0 indicated greater risk of an
adverse event occurring in the experimental group. A
p value of \0.05 was considered significant for all analy-
ses. Statistical algorithms were used to calculate the stan-
dard deviation if unavailable.
Between-study heterogeneity was assessed using the I2
and v2 statistic, and funnel plots. Higher values of I2 and
the v2 statistic signified increasing levels of heterogeneity,
with a p value \0.05 or an I2 [ 50 % indicating significant
heterogeneity [11]. To take into account the effects of this
heterogeneity, both fixed and random effect models are
presented [12]. Statistical analysis was performed using
Review Manager 5.0 (Copenhagen: The Nordic Cochrane
Centre, The Cochrane Collaboration, 2008).
Sensitivity analysis
Pre-planned sensitivity analysis was planned for the fol-
lowing groups, if two or more studies were available: RCTs
only; RCTs at low risk of bias; studies with NOS score of
seven and above; abdominal aortic aneurysm (AAA) repair
patients only; obesity-related surgery only.
Results
The final analysis included seven studies (Fig. 1), of which
four were RCTs [13–16] and three were prospective trials
[4, 17, 18]. These studies included 588 randomised
References identified after initial search and from reference lists
n=1526
Excluded by abstract/ title n=900
Duplicates records excluded n=581
Excluded n=38: No mesh prophylaxis: 14 Letter/review: 9 Emergent/ planned delayed
closure: 8 Non-comparative mesh
prophylaxis: 4 Non-human: 2 Overlap: 1
Full text reviewed n=45
Included in final review n=7
Abstracts reviewed n=945
Fig. 1 PRISMA flowchart of
included studies
Hernia (2013) 17:445–455 447
123

patients, of whom 262 (44.6 %) received mesh reinforce-
ment of the incision. All studies included adults, with
48.1 % being male (age and BMI distributions are shown
in supplemental table 3).
Inclusion criteria
All studies included patients who were considered to be at
high risk of incisional hernia, including those with
abdominal aortic aneurysms [13], those undergoing open
bariatric procedures for obesity [4, 16–18] and cohorts of
patients with mixed-risk factors [14, 15]. Specific inclusion
criteria are shown in Table 1 and co-morbidities affecting
included patients are shown in supplemental table 4.
Surgical details/mesh details
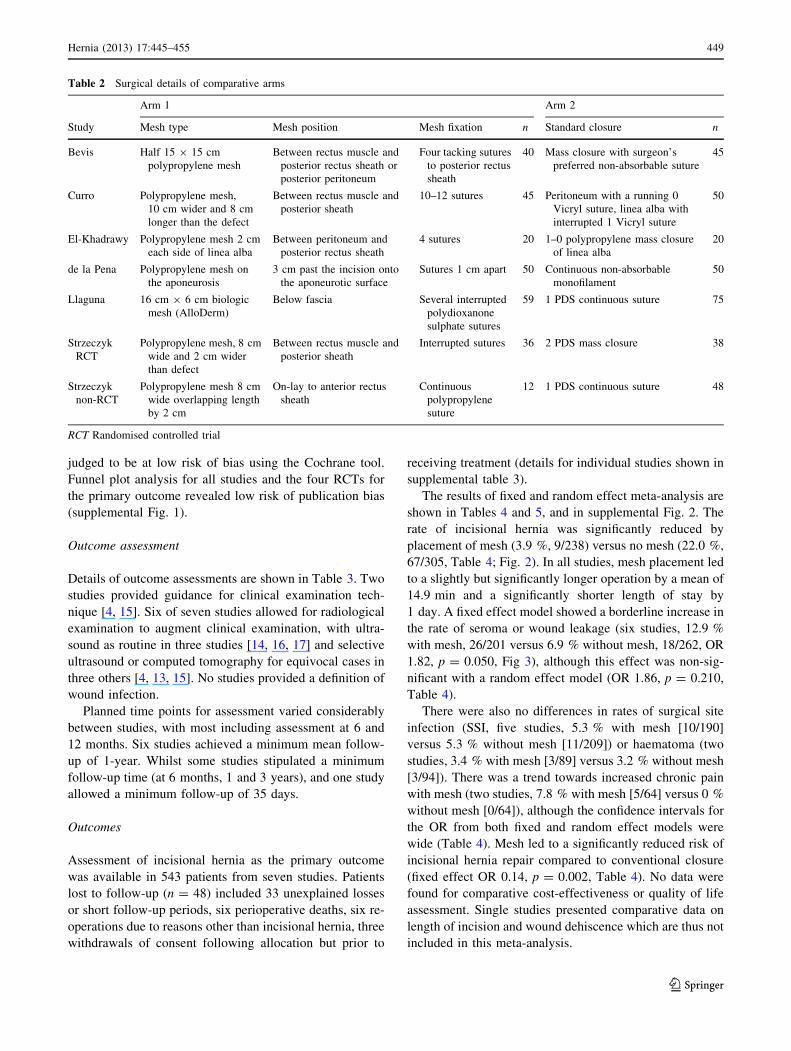
Six of seven studies considered a polypropylene mesh, with
only one prospective study considering a biologic mesh
(Table 2). Three studies stipulated placement between the
rectus muscle and posterior rectus sheath, two above the
anterior rectus sheath (on-lay method) and two deep to the
posterior rectus sheath (sub-lay method). All meshes were
fixed into position with sutures. For the conventional arm,
six studies stipulated a continuous mass closure and one
interrupted sutures of linea alba. Incision types are shown
in supplemental table 5.
Risk of bias
Two of four RCTs provided adequate detail of randomi-
sation, including specifying pre-operative randomisation
[14, 16]. Only one study stipulated a blinded assessor for
post-operative visits [16]. In four studies, the nature of the
person performing clinical assessment was unstated. One
randomised study [15] and one prospective [4] study were
at high risk of bias due to high or unexplained losses to
follow-up.
When scored using the Newcastle–Ottawa Scale, four of
the seven studies achieved seven or more stars and one
achieved nine stars (Table 1 and supplemental table 6).
When assessing the four RCTs with the Cochrane Risk of
Bias Tool, two were considered to be at high risk and two
at low risk of bias (supplemental table 7). RCTs scored
one, two, three and five points on the Jadad scale (sup-
plemental table 8); those scoring three and five were also
Table 1 Cohort demographics
Study Years Setting Design Operation High-risk inclusion
criteria?
If non-RCT,
selection for mesh
NOS
score
Risk
of
biasAAA Bariatric Unclear
Bevis 2010 3 Southwest
hospitals,
UK
RCT 85 0 0 Patients undergoing
abdominal aneurysm
repair
7 Low
Curro 2011 Messina,
Italy
PNR 0 95 0 Morbidly obese undergoing
biliopancreatic diversion
Two consecutive
time periods
7 NA
El-Khadrawy 2009 Tanta, Egypt RCT 0 0 40 C1 risk factors that may
affect the healing process
7 High
de la Pena 2003 Jerez, Spain RCT 0 0 100 High risk of incisional
hernia or one of:
neoplastic pathology,
age [70, respiratory
failure, malnutrition,
BMI [30, smokes [20
cigarettes daily
6 High
Llaguna 2011 New York,
USA
PNR 0 134 0 Patients undergoing Roux-
en-Y gastric bypass
One surgeon
operating at 2
hospital with
different policies
5 NA
Strzeczyk
RCT
2006 Lodz,
Poland
RCT 0 74 0 Morbid obesity undergoing
Roux-en-Y gastric bypass
9 Low
Strzeczyk
non-RCT
2002 Lodz,
Poland
PNR 0 60 0 Patients undergoing Roux-
en-Y gastric bypass
Patients considered
to be at high risk
of hernia
(morbidly obese
with clinically
significant
morbidity)
6 NA
AAA Abdominal aortic aneurysm, RCT randomised controlled trial, PNR prospective non-randomised, NA non-applicable
448 Hernia (2013) 17:445–455
123
judged to be at low risk of bias using the Cochrane tool.
Funnel plot analysis for all studies and the four RCTs for
the primary outcome revealed low risk of publication bias
(supplemental Fig. 1).
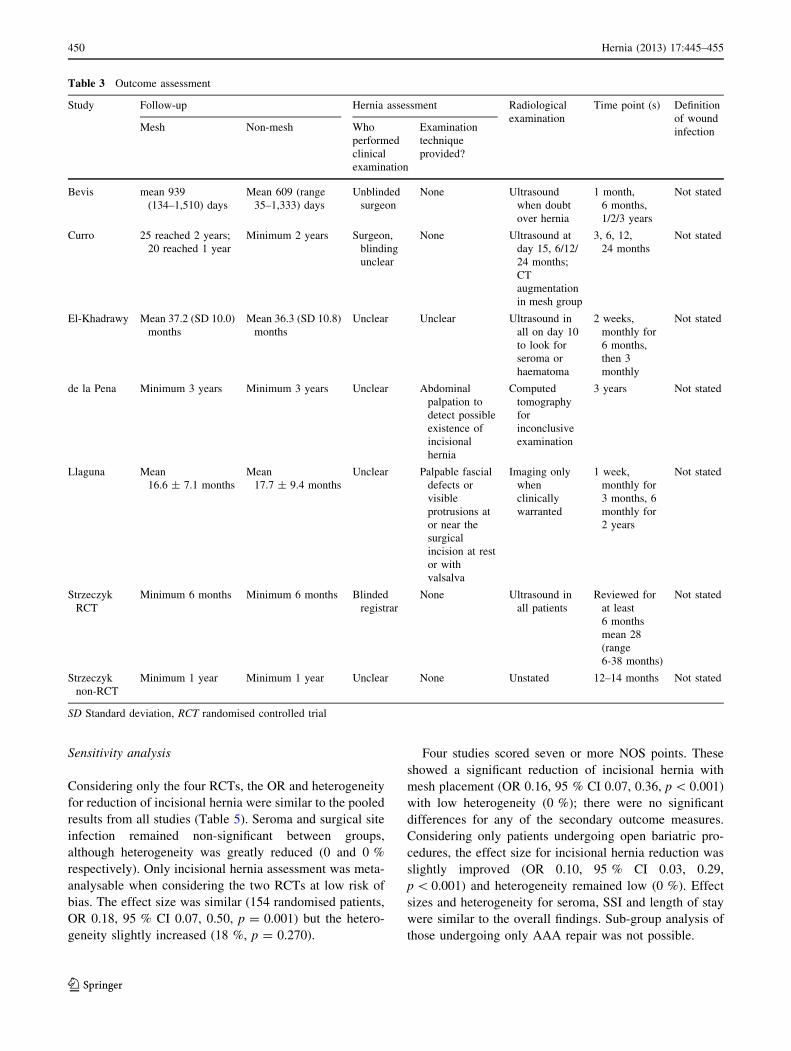
Outcome assessment
Details of outcome assessments are shown in Table 3. Two
studies provided guidance for clinical examination tech-
nique [4, 15]. Six of seven studies allowed for radiological
examination to augment clinical examination, with ultra-
sound as routine in three studies [14, 16, 17] and selective
ultrasound or computed tomography for equivocal cases in
three others [4, 13, 15]. No studies provided a definition of
wound infection.
Planned time points for assessment varied considerably
between studies, with most including assessment at 6 and
12 months. Six studies achieved a minimum mean follow-
up of 1-year. Whilst some studies stipulated a minimum
follow-up time (at 6 months, 1 and 3 years), and one study
allowed a minimum follow-up of 35 days.
Outcomes
Assessment of incisional hernia as the primary outcome
was available in 543 patients from seven studies. Patients
lost to follow-up (n = 48) included 33 unexplained losses
or short follow-up periods, six perioperative deaths, six re-
operations due to reasons other than incisional hernia, three
withdrawals of consent following allocation but prior to
receiving treatment (details for individual studies shown in
supplemental table 3).
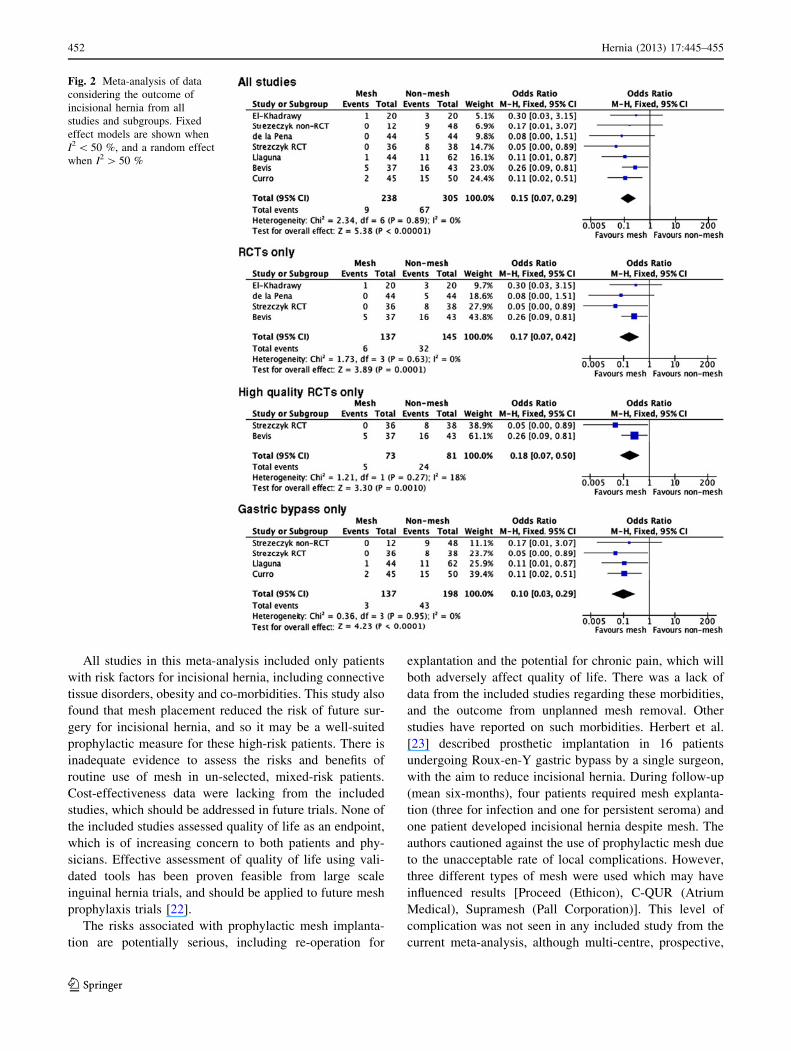
The results of fixed and random effect meta-analysis are
shown in Tables 4 and 5, and in supplemental Fig. 2. The
rate of incisional hernia was significantly reduced by
placement of mesh (3.9 %, 9/238) versus no mesh (22.0 %,
67/305, Table 4; Fig. 2). In all studies, mesh placement led
to a slightly but significantly longer operation by a mean of
14.9 min and a significantly shorter length of stay by
1 day. A fixed effect model showed a borderline increase in
the rate of seroma or wound leakage (six studies, 12.9 %
with mesh, 26/201 versus 6.9 % without mesh, 18/262, OR
1.82, p = 0.050, Fig 3), although this effect was non-sig-
nificant with a random effect model (OR 1.86, p = 0.210,
Table 4).
There were also no differences in rates of surgical site
infection (SSI, five studies, 5.3 % with mesh [10/190]
versus 5.3 % without mesh [11/209]) or haematoma (two
studies, 3.4 % with mesh [3/89] versus 3.2 % without mesh
[3/94]). There was a trend towards increased chronic pain
with mesh (two studies, 7.8 % with mesh [5/64] versus 0 %
without mesh [0/64]), although the confidence intervals for
the OR from both fixed and random effect models were
wide (Table 4). Mesh led to a significantly reduced risk of
incisional hernia repair compared to conventional closure
(fixed effect OR 0.14, p = 0.002, Table 4). No data were
found for comparative cost-effectiveness or quality of life
assessment. Single studies presented comparative data on
length of incision and wound dehiscence which are thus not
included in this meta-analysis.
Table 2 Surgical details of comparative arms
Arm 1 Arm 2
Study Mesh type Mesh position Mesh fixation n Standard closure n
Bevis Half 15 9 15 cm
polypropylene mesh
Between rectus muscle and
posterior rectus sheath or
posterior peritoneum
Four tacking sutures
to posterior rectus
sheath
40 Mass closure with surgeon’s
preferred non-absorbable suture
45
Curro Polypropylene mesh,
10 cm wider and 8 cm
longer than the defect
Between rectus muscle and
posterior sheath
10–12 sutures 45 Peritoneum with a running 0
Vicryl suture, linea alba with
interrupted 1 Vicryl suture
50
El-Khadrawy Polypropylene mesh 2 cm
each side of linea alba
Between peritoneum and
posterior rectus sheath
4 sutures 20 1–0 polypropylene mass closure
of linea alba
20
de la Pena Polypropylene mesh on
the aponeurosis
3 cm past the incision onto
the aponeurotic surface
Sutures 1 cm apart 50 Continuous non-absorbable
monofilament
50
Llaguna 16 cm 9 6 cm biologic
mesh (AlloDerm)
Below fascia Several interrupted
polydioxanone
sulphate sutures
59 1 PDS continuous suture 75
Strzeczyk
RCT
Polypropylene mesh, 8 cm
wide and 2 cm wider
than defect
Between rectus muscle and
posterior sheath
Interrupted sutures 36 2 PDS mass closure 38
Strzeczyk
non-RCT
Polypropylene mesh 8 cm
wide overlapping length
by 2 cm
On-lay to anterior rectus
sheath
Continuous
polypropylene
suture
12 1 PDS continuous suture 48
RCT Randomised controlled trial
Hernia (2013) 17:445–455 449
123
Sensitivity analysis
Considering only the four RCTs, the OR and heterogeneity
for reduction of incisional hernia were similar to the pooled
results from all studies (Table 5). Seroma and surgical site
infection remained non-significant between groups,
although heterogeneity was greatly reduced (0 and 0 %
respectively). Only incisional hernia assessment was meta-
analysable when considering the two RCTs at low risk of
bias. The effect size was similar (154 randomised patients,
OR 0.18, 95 % CI 0.07, 0.50, p = 0.001) but the hetero-
geneity slightly increased (18 %, p = 0.270).
Four studies scored seven or more NOS points. These
showed a significant reduction of incisional hernia with
mesh placement (OR 0.16, 95 % CI 0.07, 0.36, p \ 0.001)
with low heterogeneity (0 %); there were no significant
differences for any of the secondary outcome measures.
Considering only patients undergoing open bariatric pro-
cedures, the effect size for incisional hernia reduction was
slightly improved (OR 0.10, 95 % CI 0.03, 0.29,
p \ 0.001) and heterogeneity remained low (0 %). Effect
sizes and heterogeneity for seroma, SSI and length of stay
were similar to the overall findings. Sub-group analysis of
those undergoing only AAA repair was not possible.
Table 3 Outcome assessment
Study Follow-up Hernia assessment Radiological
examination
Time point (s) Definition
of wound
infectionMesh Non-mesh Who
performed
clinical
examination
Examination
technique
provided?
Bevis mean 939
(134–1,510) days
Mean 609 (range
35–1,333) days
Unblinded
surgeon
None Ultrasound
when doubt
over hernia
1 month,
6 months,
1/2/3 years
Not stated
Curro 25 reached 2 years;
20 reached 1 year
Minimum 2 years Surgeon,
blinding
unclear
None Ultrasound at
day 15, 6/12/
24 months;
CT
augmentation
in mesh group
3, 6, 12,
24 months
Not stated
El-Khadrawy Mean 37.2 (SD 10.0)
months
Mean 36.3 (SD 10.8)
months
Unclear Unclear Ultrasound in
all on day 10
to look for
seroma or
haematoma
2 weeks,
monthly for
6 months,
then 3
monthly
Not stated
de la Pena Minimum 3 years Minimum 3 years Unclear Abdominal
palpation to
detect possible
existence of
incisional
hernia
Computed
tomography
for
inconclusive
examination
3 years Not stated
Llaguna Mean
16.6 ± 7.1 months
Mean
17.7 ± 9.4 months
Unclear Palpable fascial
defects or
visible
protrusions at
or near the
surgical
incision at rest
or with
valsalva
Imaging only
when
clinically
warranted
1 week,
monthly for
3 months, 6
monthly for
2 years
Not stated
Strzeczyk
RCT
Minimum 6 months Minimum 6 months Blinded
registrar
None Ultrasound in
all patients
Reviewed for
at least
6 months
mean 28
(range
6-38 months)
Not stated
Strzeczyk
non-RCT
Minimum 1 year Minimum 1 year Unclear None Unstated 12–14 months Not stated
SD Standard deviation, RCT randomised controlled trial
450 Hernia (2013) 17:445–455
123

Discussion
The main finding of this systematic review is the evidence
for reduced occurrence of incisional hernia in high-risk
patients following prophylactic mesh implantation. How-
ever, when making recommendations for widespread use,
this has to be balanced against the mediocre study design,
inconsistent outcome assessment and uncertainty of true
secondary outcome rates.
Assessing trial quality, risk of bias and outcome
reporting is controversial, can be difficult and is often
inadequately performed [19, 20]. This meta-analysis used
three methods of assessing studies. Four studies scored
seven or above NOS points and two of the included RCTs
were deemed to be at low risk of bias. The assessment
systems did not have perfect agreement, although only one
RCT was deemed to be at low risk of bias and scored
highly on the NOS and Jadad scales. Whilst general het-
erogeneity was low and performing sub-group analyses
compensated for the quality differences, the overall
assessment detected the mixed nature of quality and thus
overall high risk of bias; this was an advantage of assessing
quality using several metrics rather than single tools. The
RCTs were not without limitations, particularly relating to
randomisation reporting and blinding of assessors. Their
generalisability is further limited by their application to
specific populations (e.g. AAA repair patients) in specific
geographical locations. More evidence to support the pri-
mary outcome in a wider range of clinical settings is still
required.
Assessment of secondary outcomes related to adverse
events showed no significant differences between arms, but
studies were inadequate to completely assess these. How-
ever, a trend towards increased seroma formation with
mesh carried borderline significance with a fixed effect
model, but non-significance with a random effect model,
which reflects clinical heterogeneity. Since pooled assess-
ment of seroma formation from the high-quality RCTs was
not possible due to a lack of data, more high-quality evi-
dence to definitively identify these rates is thus required.
Two RCTs which assessed chronic pain found a possible
trend towards an increase with mesh (OR 6.63, 95 % CI
0.77, 56.86, p = 0.080); however, no definition of chronic
pain was given and the assessment methods were unclear
with neither study using validated measurement tools [14,
15]. A definition of surgical site infection was not provided
by any of the included studies. When assessed prospec-
tively, with an accepted definition and the intention of
identifying all events, the risk of SSI has recently been
proven to be higher than expected in elective colorectal
surgery and can approach 25–45 % [21]. Without active,
independent and standardised assessment for adverse
events, it may be that the rates seen within the included
studies of the present meta-analysis are under-estimated.
Table 4 Meta-analysis of outcome measures from all studies
Outcome Studies
(patients)
Fixed effect p Random effect p Heterogeneity p
OR or WMD OR or WMD I2 (%) v2
Incisional hernia 7 (543) 0.15 (0.07, 0.29) \0.001 0.16 (0.08, 0.33) \0.001 0 2.3 0.89
Seroma or wound leakage 6 (463) 1.82 (0.99, 3.37) 0.050 1.86 (0.70, 4.97) 0.210 45 9.1 0.11
Surgical site infection 5 (409) 1.04 (0.43, 2.49) 0.940 0.97 (0.36, 2.59) 0.950 2 4.1 0.39
Haematoma 2 (183) 1.03 (0.23, 4.72) 0.970 1.08 (0.22, 5.33) 0.930 0 0.6 0.44
Duration of surgery 2 (180) 14.9 (12.1, 17.7) \0.001 14.9 (12.1, 17.7) \0.001 0 0.3 0.6
Length of stay 2 (169) -1.02 (-1.37, -0.67) \0.001 -1.02 (-1.37, -0.67) \0.001 0 0.7 0.42
Chronic wound pain 2 (128) 6.63 (0.77, 56.86) 0.080 6.57 (0.76, 56.69) 0.090 0 0.04 0.84
Surgical repair of hernia (all patients) 2 (175) 0.14 (0.04, 0.50) 0.002 0.15 (0.04, 0.52) 0.003 0 0.44 0.51
OR odds ratio, WMD weighted Mean Difference
Table 5 Meta-analysis of outcome measures from randomised controlled trials
Outcome Studies (patients) Fixed Effect p Random Effect p Heterogeneity p
OR or WMD OR or WMD I2 v2
Incisional hernia 4 (282) 0.17 (0.07, 0.42) \0.001 0.20 (0.08, 0.50) \0.001 0 1.7 0.63
Seroma or wound leakage 3 (202) 1.03 (0.40, 2.62) 0.950 1.07 (0.41, 2.82) 0.890 0 1.3 0.52
Surgical site infection 3 (208) 0.73 (0.22, 2.42) 0.610 0.74 (0.22, 2.50) 0.630 0 0.54 0.76
Chronic wound pain 2 (128) 6.63 (0.77, 56.86) 0.080 6.57 (0.76, 56.69) 0.090 0 0.04 0.84
OR Odds ratio, WMD weighted mean difference
Hernia (2013) 17:445–455 451
123
All studies in this meta-analysis included only patients
with risk factors for incisional hernia, including connective
tissue disorders, obesity and co-morbidities. This study also
found that mesh placement reduced the risk of future sur-
gery for incisional hernia, and so it may be a well-suited
prophylactic measure for these high-risk patients. There is
inadequate evidence to assess the risks and benefits of
routine use of mesh in un-selected, mixed-risk patients.
Cost-effectiveness data were lacking from the included
studies, which should be addressed in future trials. None of
the included studies assessed quality of life as an endpoint,
which is of increasing concern to both patients and phy-
sicians. Effective assessment of quality of life using vali-
dated tools has been proven feasible from large scale
inguinal hernia trials, and should be applied to future mesh
prophylaxis trials [22].
The risks associated with prophylactic mesh implanta-
tion are potentially serious, including re-operation for
explantation and the potential for chronic pain, which will
both adversely affect quality of life. There was a lack of
data from the included studies regarding these morbidities,
and the outcome from unplanned mesh removal. Other
studies have reported on such morbidities. Herbert et al.
[23] described prosthetic implantation in 16 patients
undergoing Roux-en-Y gastric bypass by a single surgeon,
with the aim to reduce incisional hernia. During follow-up
(mean six-months), four patients required mesh explanta-
tion (three for infection and one for persistent seroma) and
one patient developed incisional hernia despite mesh. The
authors cautioned against the use of prophylactic mesh due
to the unacceptable rate of local complications. However,
three different types of mesh were used which may have
influenced results [Proceed (Ethicon), C-QUR (Atrium
Medical), Supramesh (Pall Corporation)]. This level of
complication was not seen in any included study from the
current meta-analysis, although multi-centre, prospective,
Fig. 2 Meta-analysis of data
considering the outcome of
incisional hernia from all
studies and subgroups. Fixed
effect models are shown when
I2 \ 50 %, and a random effect
when I2 [ 50 %
452 Hernia (2013) 17:445–455
123

independent assessment would be needed to more defini-
tively answer this question.
By analysing study design and risk of bias, this meta-
analysis has implications for future trial design and out-
come reporting. Based on the findings of this study, it is
feasible that future RCTs will find a significant risk
reduction of incisional hernia when mesh is placed. Thus,
careful attention should be paid to the adverse event and
quality of life profile. A future RCT should ideally be
multi-centred, adequately powered, contain a range of
patients at high risk of incisional hernia, and allow for
blinded patient and clinician outcome assessment. Such
outcome assessment should be optimised, to include dis-
crete definitions of outcome measures, a defined clinical
examination technique and supplementation with appro-
priate radiological imaging.
From the present meta-analysis, there was variation in
the assessment times in the included studies, which was
often short. Since only 50 % of incisional hernias become
clinically apparent after 5 months, 75 % after 2 years and
98 % after 5 years [24], correct timing of assessments is
important in hernia detection. As a result, it is feasible that
some of the included studies have not revealed true hernia
rates. However, delaying the findings of trials denies
patients and clinicians early evidence on which to base
treatment decisions. Imaging assessment of hernias carries
two benefits: (1) it allows for standardisation of hernia
detection (especially for computed tomography), and (2) it
may allow for early identification of late clinically relevant
hernias, and thus early delivery of trial results [25]. Finally,
thorough provision for assessment of quality of life
(including pain) and cost-effectiveness should be assessed
and ensured. Recommendations for design and outcome
assessment relevant to future trial design are shown in
Table 6.
A remaining question is whether the findings of this
study can influence the daily practice of the operating
surgeon. Our meta-analysis has limitations, which primar-
ily surround the quality of studies included. It is reasonable
that individually selected patients at high-risk warrant
prophylaxis with mesh. These patients should ideally be
included within prospective, randomised multicentre trials,
which will accurately assess the primary endpoint and
adverse event profile in a standardised way.
Currently, clinical trials registered concerning prophy-
lactic mesh placement include the PRIMAAT trial (pre-
vention of incisional hernia by mesh augmentation after
midline laparotomy for aortic aneurysm treatment, http://
clinicaltrials.gov/ct2/show/NCT00757133), which aims to
randomise 120 patients and complete by December 2013.
The ProphMesh trial (Prophylactic Mesh Implantation
for the Prevision of Incisional Hernia, http://clinicaltrials.
gov/ct2/show/NCT01203553) aims to randomise 150
patients and complete by July 2015. The Austrian Hernia
Fig. 3 Meta-analysis of data
considering the outcome of
seroma or wound leakage from
all studies and subgroups. Fixed
effect models are shown when
I2 \ 50 %, and a random effect
when I2 [ 50 %
Hernia (2013) 17:445–455 453
123

Study Group will randomise 300 patients with BMI [27
to the same effect, to complete by January 2016 (http://
clinicaltrials.gov/ct2/show/NCT01507870). In the meantime,
the present meta-analysis provides the most up-to-date
evidence, and perhaps more importantly can inform future
trial design.
Future studies may also provide information to allow for
optimisation of mesh type and position to reduce adverse
events. From studies included in the present meta-analysis,
only one assessed the use of biologic mesh and none
considered emergency patients. Emergency patients, who
often have complex and/or contaminated wounds, are at
high risk of incisional hernia and warrant inclusion in an
RCT. Conventional mesh is typically avoided due to the
perceived risk of infection. It may be that biologic mesh
reduces the risk of SSI in this group and may reduce
chronic pain in a wider group of patients, although
increased risk of seroma formation is a concern; further
evaluation is required [26]. A prospective, single arm study
of biologic mesh closure of 80 patients with contaminated
ventral incisional hernias has revealed infection related
events in 24 patients and seroma in 22, although no com-
parative arm was assessed [27]. The Reinforcement of
Closure of Stoma Site trial will randomise patients
undergoing stoma closure to either suture repair or suture
repair with biologic mesh reinforcement (http://www.rocss.
bham.ac.uk) These wounds act as a frequent and controlled
model for complex and contaminated wounds, where in-
cisional hernia may occur in up to 30 % of patients [25,
28]. Patients undergoing re-laparotomy (e.g. excision of
recurrent cancer or following earlier un-related abdominal
incision) may also be considered high risk and may benefit
from mesh prophylaxis. Temporary bridging of the open
abdomen is a different research question, with the question
of prophylaxis relating to those undergoing primary fascial
closure or at the time of delayed primary closure.
Conclusion
Mesh prophylaxis of midline laparotomy wounds reduced
the rate of incisional hernias in high-risk patients. How-
ever, the secondary outcome measures, including adverse
events, cost-effectiveness and quality of life, have not yet
been adequately assessed to recommend routine mesh
placement in all patients. Well-designed, multicentre RCTs
are required to assess the safety profile more completely.
The findings of this systematic review and meta-analysis
should inform their design, including the need for
Table 6 Recommended core
elements for future trial design
CT Computed tomography,
CDC Centre for Disease
Control, VAS Visual Analogue
Scale
Domain Recommendation Notes
Inclusion criteria Elective (high risk) Obese, AAA, re-laparotomy, other co-
morbidities
Emergency (high risk) Contaminated or dirty, other high risk
Elective (mixed risk) Benefits in low versus high risk
Methodology Mesh position defined Sub-lay, in-lay, on-lay etc.
Mesh type analysis Synthetic versus biologic
Optimum synthetic types
Primary outcome Incisional hernia Blinded outcome assessors
Definition of clinical hernia requires consensus
Standardised clinical examination technique
CT detection for early trial results
Secondary
outcomes
Surgical site infection Defined by CDC criteria
Seroma Definition and classification of size require
consensus
Haematoma Definition and classification of size require
consensus
Intra-operative details/length of
stay
Quality of life Consensus of optimal validated tool required
Cost-effectiveness
Pain Assessed using VAS and hernia specific tools
Blinded outcome assessors
Timing of
assessments
Pre-operative
Early post-operative 30 days
Mid-term 3 months
Long-term 1, 2, 3, 5 years
454 Hernia (2013) 17:445–455
123
improved definition of outcomes, blinded outcome assess-
ment, and assessment of quality of life and cost-effec-
tiveness. The effectiveness in unselected/mixed-risk and
emergency patients is unknown and further evidence is
required from these cohorts.
Conflicts of interest All authors declares no conflicts of interest.
References
1. van’t Riet M, Steyerberg EW, Nellensteyn J, Bonjer HJ, Jeekel J
(2002) Meta-analysis of techniques for closure of midline
abdominal incisions. Br J Surg 89:1350–1356
2. Diener MK, Voss S, Jensen K, Buchler MW, Seiler CM (2010)
Elective midline laparotomy closure: the INLINE systematic
review and meta-analysis. Ann Surg 251:843–856
3. Gecim IE, Kocak S, Ersoz S, Bumin C, Aribal D (1996) Recur-
rence after incisional hernia repair: results and risk factors. Surg
Today 26:607–609
4. Llaguna OH, Avgerinos DV, Nagda P, Elfant D, Leitman IM,
Goodman E (2011) Does prophylactic biologic mesh placement
protect against the development of incisional hernia in high-risk
patients? World J Surg 35:1651–1655
5. Capella RF, Iannace VA, Capella JF (2007) Reducing the inci-
dence of incisional hernias following open gastric bypass surgery.
Obes Surg 17:438–444
6. Wells G SB, O’Connell D et al (2000) The Newcastle–Ottawa
Scale (NOS) for assessing the quality of non-randomised studies
in meta-analyses. In: 3rd Symposium on systematic reviews:
beyond the basics. Improving quality and impact, Oxford, UK
7. Bhangu A, Nepogodiev D, Gupta A, Torrance A, Singh P (2012)
Systematic review and meta-analysis of outcomes following
emergency surgery for Clostridium difficile colitis. Br J Surg
99:1501–1513
8. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman
AD, Savovic J, Schulz KF, Weeks L, Sterne JA (2011) The
Cochrane Collaboration’s tool for assessing risk of bias in ran-
domised trials. BMJ 343:d5928
9. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ,
Gavaghan DJ, McQuay HJ (1996) Assessing the quality of
reports of randomized clinical trials: is blinding necessary?
Control Clin Trials 17:1–12
10. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC,
Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D
(2009) The PRISMA statement for reporting systematic reviews
and meta-analyses of studies that evaluate healthcare interven-
tions: explanation and elaboration. Brit Med J 339:b2700
11. Lau J, Ioannidis JP, Schmid CH (1997) Quantitative synthesis in
systematic reviews. Ann Intern Med 127:820–826
12. DerSimonian R, Laird N (1986) Meta-analysis in clinical trials.
Control Clin Trials 7:177–188
13. Bevis PM, Windhaber RA, Lear PA, Poskitt KR, Earnshaw JJ,
Mitchell DC (2010) Randomized clinical trial of mesh versus
sutured wound closure after open abdominal aortic aneurysm
surgery. Br J Surg 97:1497–1502
14. El-Khadrawy OH, Moussa G, Mansour O, Hashish MS (2009)
Prophylactic prosthetic reinforcement of midline abdominal
incisions in high-risk patients. Hernia 13:267–274
15. Gutierrez de la Pena C, Medina Achirica C, Dominguez-Adame
E, Medina Diez J (2003) Primary closure of laparotomies with
high risk of incisional hernia using prosthetic material: analysis
of usefulness. Hernia 7:134–136
16. Strzelczyk JM, Szymanski D, Nowicki ME, Wilczynski W,
Gaszynski T, Czupryniak L (2006) Randomized clinical trial of
postoperative hernia prophylaxis in open bariatric surgery. Br J
Surg 93:1347–1350
17. Curro G, Centorrino T, Low V, Sarra G, Navarra G (2012) Long-
term outcome with the prophylactic use of polypropylene mesh in
morbidly obese patients undergoing biliopancreatic diversion.
Obes Surg 22:279–282
18. Strzelczyk J, Czupryniak L, Loba J, Wasiak J (2002) The use of
polypropylene mesh in midline incision closure following gastric
by-pass surgery reduces the risk of postoperative hernia.
Langenbecks Arch Surg 387:294–297
19. Hartling L, Ospina M, Liang Y, Dryden DM, Hooton N, Krebs
Seida J, Klassen TP (2009) Risk of bias versus quality assessment
of randomised controlled trials: cross sectional study. Brit Med J
339:b4012
20. Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song
F, Petticrew M, Altman DG (2003) Evaluating non-randomised
intervention studies. Health Technol Assess 7:iii-x, 1–173
21. Anthony T, Murray BW, Sum-Ping JT, Lenkovsky F, Vornik VD,
Parker BJ, McFarlin JE, Hartless K, Huerta S (2011) Evaluating
an evidence-based bundle for preventing surgical site infection: a
randomized trial. Arch Surg 146:263–269
22. Eklund A, Montgomery A, Bergkvist L, Rudberg C (2010)
Chronic pain 5 years after randomized comparison of laparo-
scopic and Lichtenstein inguinal hernia repair. Br J Surg
97:600–608
23. Herbert GS, Tausch TJ, Carter PL (2009) Prophylactic mesh to
prevent incisional hernia: a note of caution. Am J Surg
197:595–598 (discussion 598)
24. Pollock AV, Evans M (1989) Early prediction of late incisional
hernias. Brit J Surg 76:953–954
25. Bhangu A, Fletcher L, Kingdon S, Smith E, Nepogodiev D,
Janjua U (2012) A clinical and radiological assessment of inci-
sional hernias following closure of temporary stomas. Surgeon
10:321–325
26. Lopez-Cano M, Armengol M, Quiles MT, Biel A, Velasco J,
Huguet P, Mestre A, Delgado LM, Gil FX, Arbos MA (2012)
Preventive midline laparotomy closure with a new bioabsorbable
mesh: an experimental study. J Surg Res 181:160–169
27. Itani KM, Rosen M, Vargo D, Awad SS, Denoto G 3rd, Butler CE
(2012) Prospective study of single-stage repair of contaminated
hernias using a biologic porcine tissue matrix: the RICH Study.
Surgery 152:498–505
28. Bhangu A, Nepogodiev D, Futaba K (2012) Systematic review
and meta-analysis of the incidence of incisional hernia at the site
of stoma closure. World J Surg 36:973–983
Hernia (2013) 17:445–455 455
123
Related Documents











