SYMPOSIUM DEEL II : TRANSFUSIECOMITÉS IN ACTIE Moderatoren: Prof. Dr. V. Deneys, Stuurgroep BeQuinT, werkgroep opleiding & vorming, CHU Namur Apr.-biol. L. De Keersmaecker, Stuurgroep BeQuinT, Jan Yperman Ziekenhuis 1. Implementation and monitoring of bedside scan system 2. Uitwerking van kwaliteitsindicatoren 3. Use of a dynamical dashboard to improve and assure the use of a new bedside scanning system of blood components 4. Onafhankelijke bloednames: continue en gerichte communicatie noodzakelijk 5. Implementatie bloedbankautomaat voor decentrale uitgifte + International, prospective haemovigilance study on methylene blue-treated plasma [UZ Gent]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SYMPOSIUM DEEL II :
TRANSFUSIECOMITÉS IN ACTIE
Moderatoren:
Prof. Dr. V. Deneys,
Stuurgroep BeQuinT, werkgroep opleiding & vorming, CHU Namur
Apr.-biol. L. De Keersmaecker,
Stuurgroep BeQuinT, Jan Yperman Ziekenhuis
1. Implementation and monitoring of bedside scan system
2. Uitwerking van kwaliteitsindicatoren
3. Use of a dynamical dashboard to improve and assure the
use of a new bedside scanning system of blood components
4. Onafhankelijke bloednames: continue en gerichte
communicatie noodzakelijk
5. Implementatie bloedbankautomaat voor decentrale uitgifte
+ International, prospective haemovigilance study on
methylene blue-treated plasma [UZ Gent]
SYMPOSIUM PARTIE II :
COMITÉS DE TRANSFUSION EN ACTION
Modérateurs:
Prof. Dr. V. Deneys,
Comité de pilotage BeQuinT, GT éducation & formation, CHU Namur
Pharm.-biol. L. De Keersmaecker,
Comité de pilotage BeQuinT, Jan Yperman Ziekenhuis
1. Implémentation et suivi d’un système de scannage au lit du patient
2. Elaboration d’indicateurs qualité
3. Utilisation d’un tableau de bord dynamique pour améliorer et assurer
l’application d’un nouveau système de scannage de composants
sanguins au lit du patient
4. Importance d’un feedback continu et ciblé pour la validation du groupe
sanguin
5. Implémentation d’un automate banque de sang pour la distribution
décentralisée + International, prospective haemovigilance study on
methylene blue-treated plasma [UZ Gent]
Implementation and monitoring of bedside scan system AZ St Jan Brugge-Oostende, campus Brugge
Symposium
1er juin 2017 – 1 juni 2017
Dr. Barbara Cauwelier
Implementatie en benchmarking bedside scansysteem
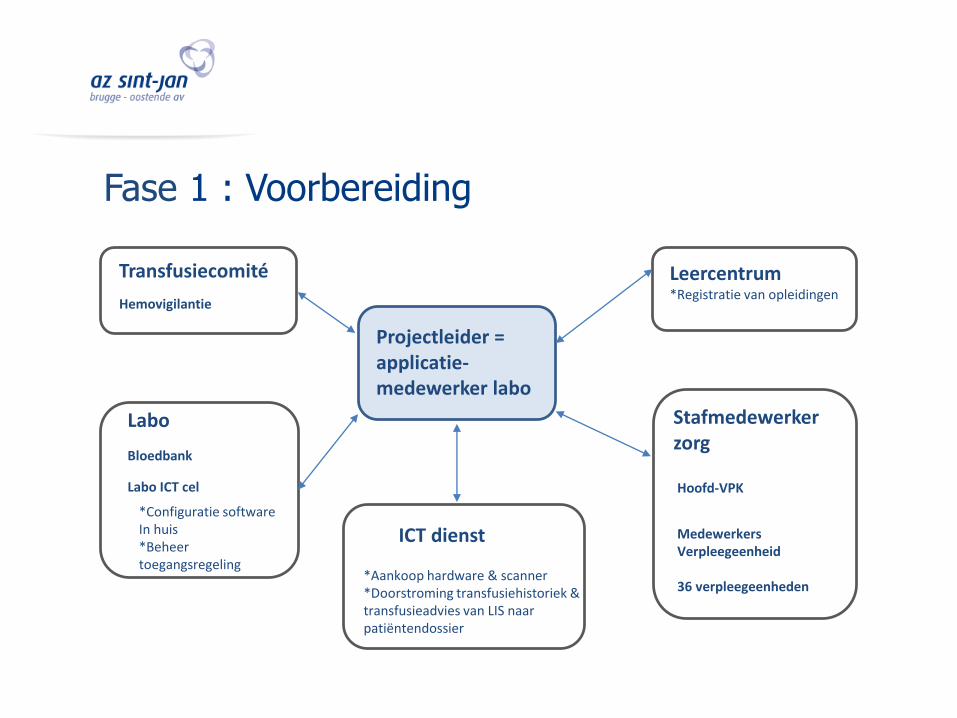
Transfusiecomité
Labo
Labo ICT cel
*Configuratie software In huis*Beheer toegangsregeling
Bloedbank
Hemovigilantie
Projectleider = applicatie-medewerker labo
Medewerkers Verpleegeenheid
36 verpleegeenheden
Hoofd-VPK
Stafmedewerker zorg
Leercentrum*Registratie van opleidingen
ICT dienst
*Aankoop hardware & scanner*Doorstroming transfusiehistoriek & transfusieadvies van LIS naar patiëntendossier
Fase 1 : Voorbereiding
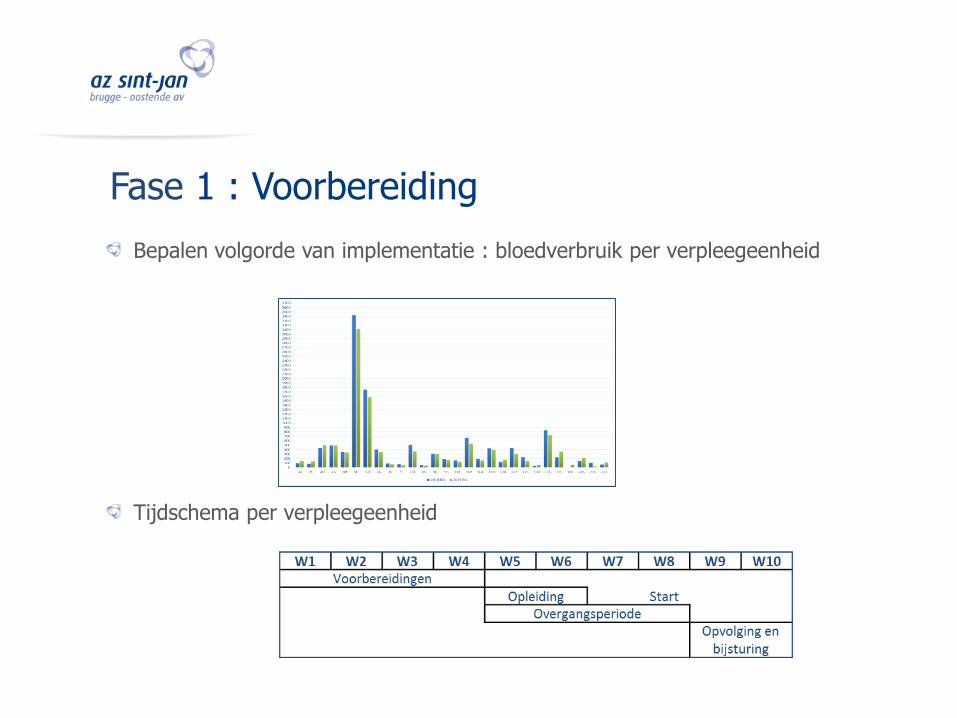
Bepalen volgorde van implementatie : bloedverbruik per verpleegeenheid
Tijdschema per verpleegeenheid
Fase 1 : Voorbereiding
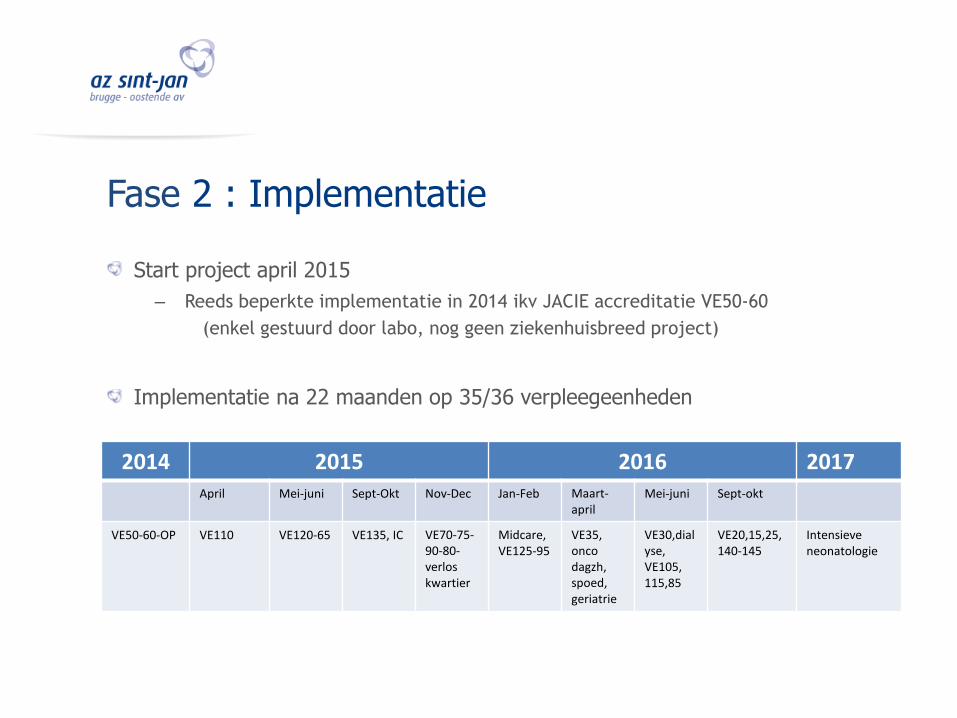
Fase 2 : Implementatie
Start project april 2015
– Reeds beperkte implementatie in 2014 ikv JACIE accreditatie VE50-60
(enkel gestuurd door labo, nog geen ziekenhuisbreed project)
Implementatie na 22 maanden op 35/36 verpleegeenheden
2014 2015 2016 2017April Mei-juni Sept-Okt Nov-Dec Jan-Feb Maart-
aprilMei-juni Sept-okt
VE50-60-OP VE110 VE120-65 VE135, IC VE70-75-90-80-verloskwartier
Midcare, VE125-95
VE35, oncodagzh, spoed,geriatrie
VE30,dialyse, VE105, 115,85
VE20,15,25,140-145
Intensieveneonatologie
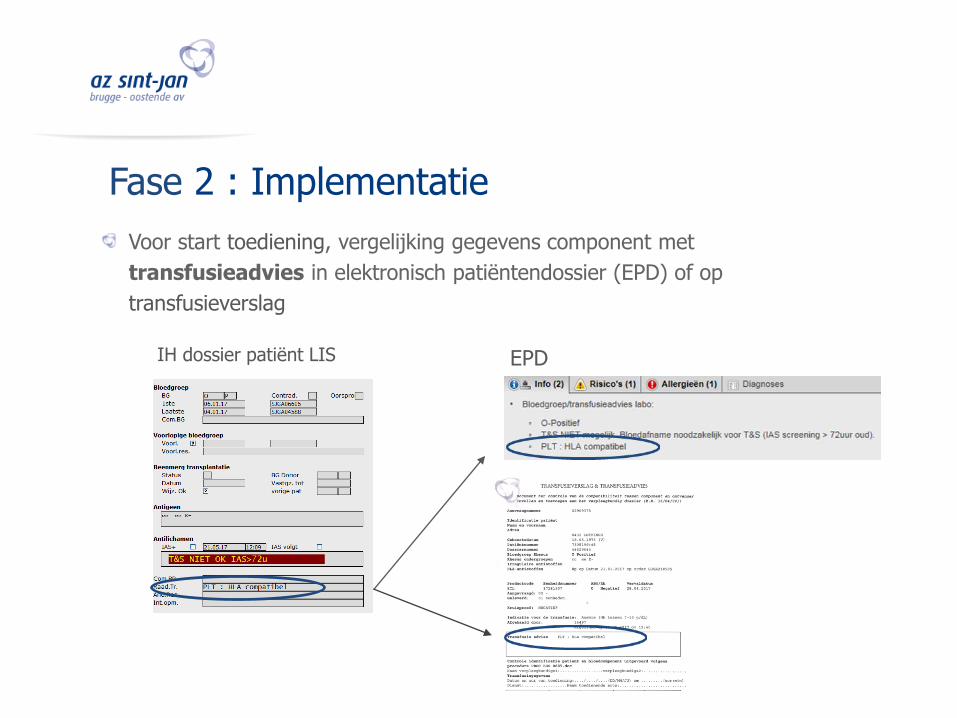
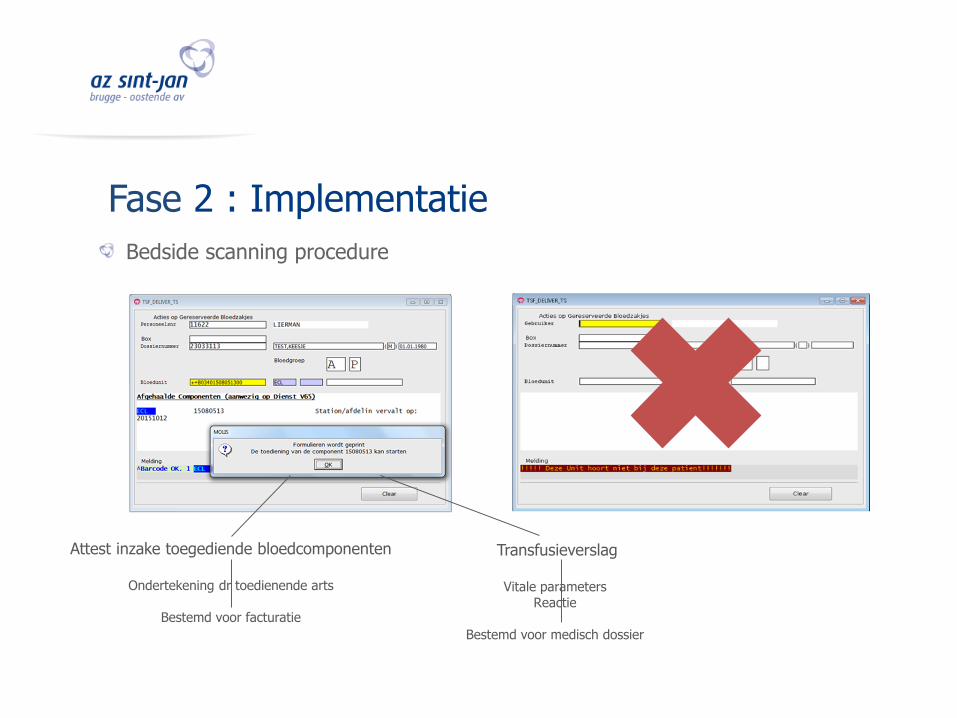
Voor start toediening, vergelijking gegevens component met
transfusieadvies in elektronisch patiëntendossier (EPD) of op
transfusieverslag
Fase 2 : Implementatie
IH dossier patiënt LIS EPD
Fase 2 : Implementatie
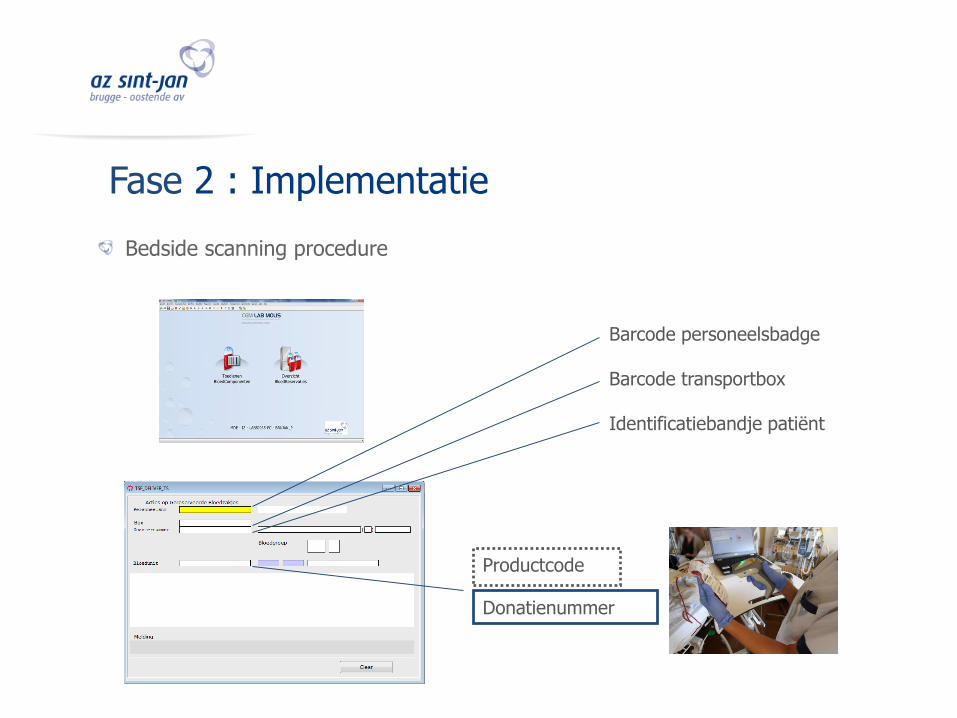
Productcode
Donatienummer
Barcode personeelsbadge
Barcode transportbox
Identificatiebandje patiënt
Bedside scanning procedure
Fase 2 : Implementatie
Attest inzake toegediende bloedcomponenten
Ondertekening dr toedienende arts
Bestemd voor facturatie
Transfusieverslag
Vitale parameters Reactie
Bestemd voor medisch dossier
Bedside scanning procedure
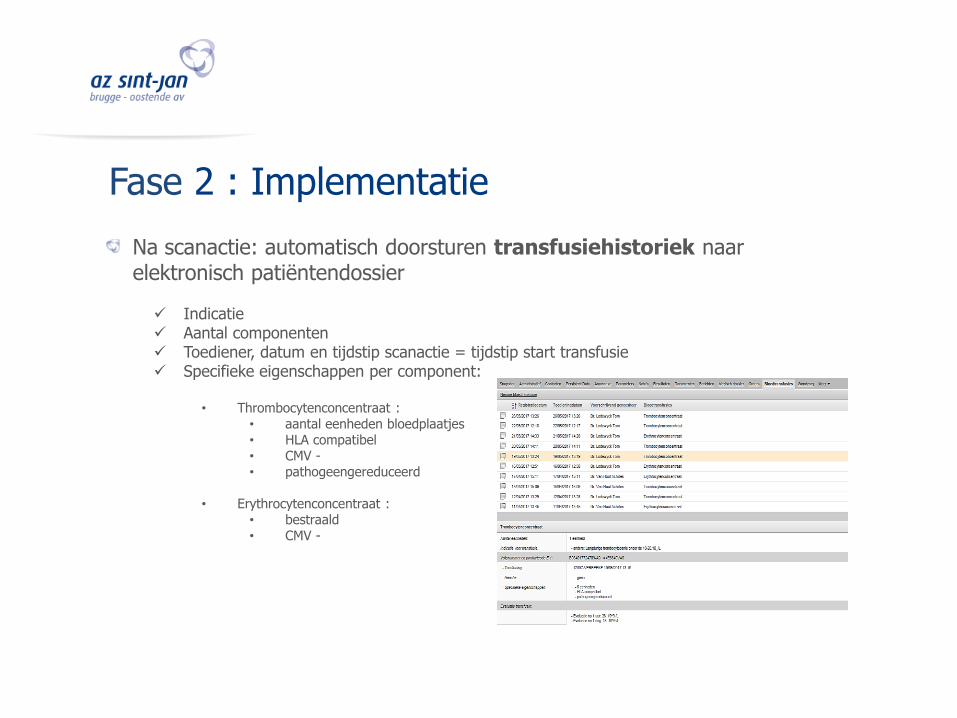
Na scanactie: automatisch doorsturen transfusiehistoriek naar elektronisch patiëntendossier
Indicatie Aantal componenten Toediener, datum en tijdstip scanactie = tijdstip start transfusie Specifieke eigenschappen per component:
• Thrombocytenconcentraat :• aantal eenheden bloedplaatjes • HLA compatibel• CMV -• pathogeengereduceerd
• Erythrocytenconcentraat :• bestraald • CMV -
Fase 2 : Implementatie
Fase 3 : Benchmarking
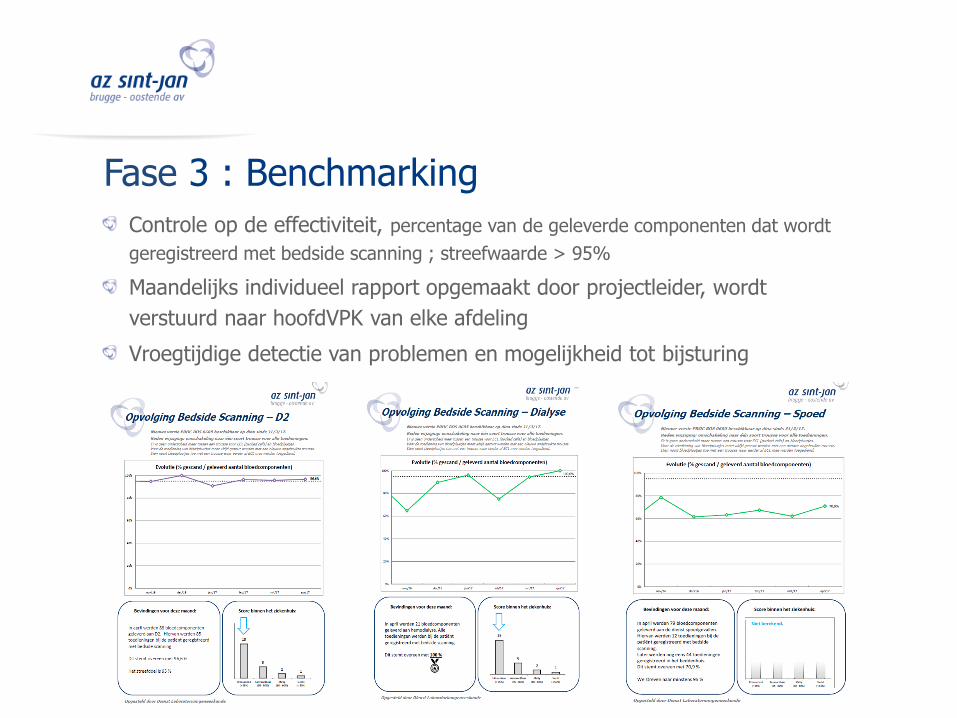
Controle op de effectiviteit, percentage van de geleverde componenten dat wordt
geregistreerd met bedside scanning ; streefwaarde > 95%
Maandelijks individueel rapport opgemaakt door projectleider, wordt
verstuurd naar hoofdVPK van elke afdeling
Vroegtijdige detectie van problemen en mogelijkheid tot bijsturing
Problemen ?
Foutief gebruik software of hardware / menselijke fouten
• Scanner werkt niet :– Niet opgeladen
– Op verkeerde docking station opgeladen
• Software niet beschikbaar op laptop– Vervanging defect toestel door ICT ZH , applicatie niet opnieuw
geïnstalleerd
Fase 3 : Benchmarking
Dank aan
Matthias Decoster (projectleider )
Ria Matton (kwaliteitsmedewerker hemovigilantie)
Tom Lierman (IT cel labo)
Shirley Wallaert (leercentrum)
ICT ziekenhuis

Elaboration d’indicateurs qualitéCliniques de l'Europe
Symposium
1er juin 2017 – 1 juni 2017
Transfusion : Indicateurs de qualité pour le nursing
1 JUIN 2017
DR. ALBERT VEYS
M. OLIVIER LANG
MME COLINE VANDER BORGHT
M. CARMELO GIUNTA
• 709 lits
• Deux sites :
• Sainte Elisabeth à Uccle
• Saint Michel à Etterbeek
• Un laboratoire et une banque de sang sur chaque site
• Au niveau du laboratoire : GLIMS + module transfusion intégré
• Au niveau nursing : Cybertrack
MISE EN PERSPECTIVE
Les Cliniques de l’Europe
• CED : 4794 poches
• PVI : 227 poches
• Plaquettes : 3833 unités
MISE EN PERSPECTIVE
Activité transfusionnelle 2016
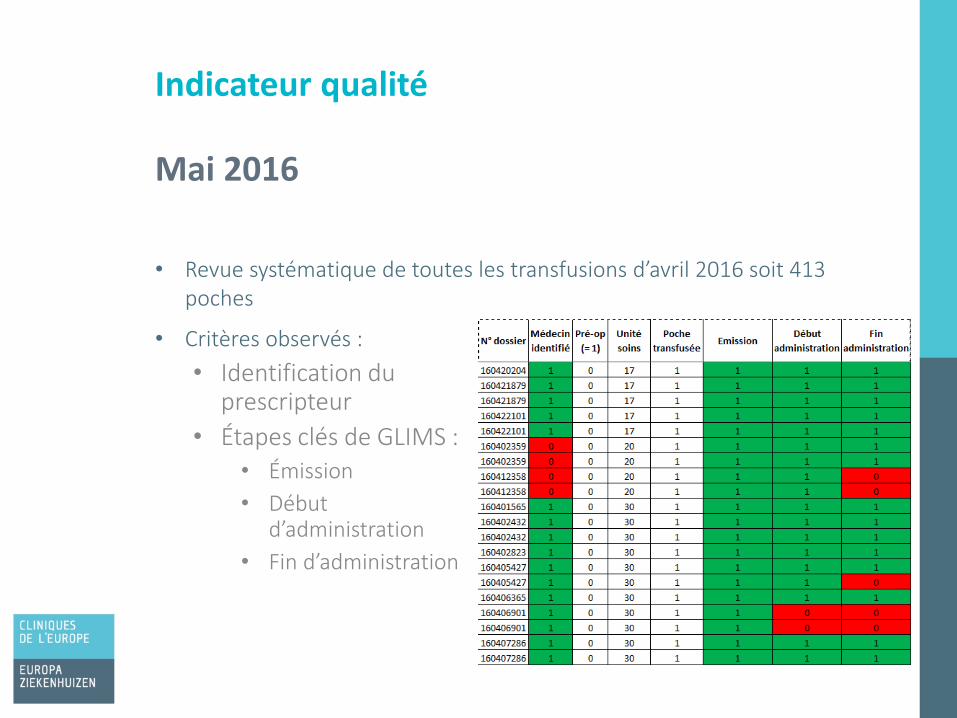
• Revue systématique de toutes les transfusions d’avril 2016 soit 413 poches
Indicateur qualité
Mai 2016
• Critères observés :
• Identification du prescripteur
• Étapes clés de GLIMS :• Émission
• Début d’administration
• Fin d’administration
• Choix d’un indicateur de qualité :
• % de début d’administration via Cybertrack par unité de soin
• C’est un indicateur fondamental car le début d’administration via Cybertrack sécurise trois éléments :
• Le cross-matching électronique poche-patient
• La date de péremption de la poche
• La péremption des test pré-transfusionnels (72h)
• Objectif à 1 an : se maintenir au dessus de 90 %
INDICATEUR QUALITÉ
Juin 2016 : Comité de transfusion
• L’absence de cross-matching via Cybertrack au chevet du patient sera considéré comme un Nearmiss
• Dès lors, suivi quotidien des transfusions et repérage des Nearmisses
• Report des données dans un fichier Excel
• Enquête de terrain dans les unités de soins• Causes du Nearmiss : erreur d’émission de la poche,
bug, …
INDICATEUR QUALITÉ
Juin 2016 : Comité de transfusion
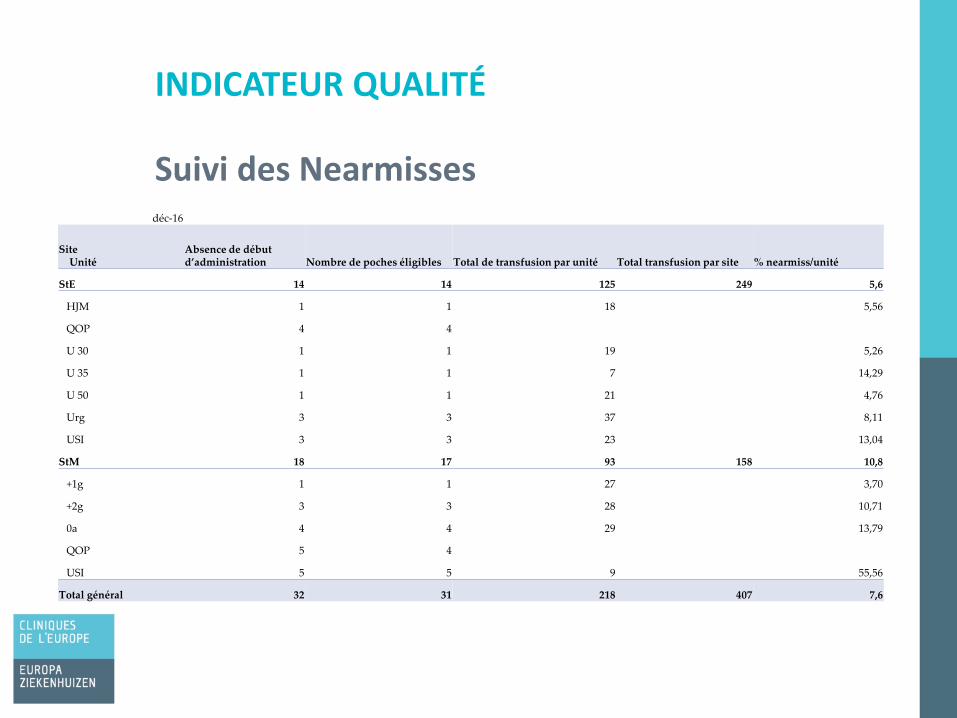
INDICATEUR QUALITÉ
Suivi des Nearmissesdéc-16
SiteUnité
Absence de début d’administration Nombre de poches éligibles Total de transfusion par unité Total transfusion par site % nearmiss/unité
StE 14 14 125 249 5,6
HJM 1 1 18 5,56
QOP 4 4
U 30 1 1 19 5,26
U 35 1 1 7 14,29
U 50 1 1 21 4,76
Urg 3 3 37 8,11
USI 3 3 23 13,04
StM 18 17 93 158 10,8
+1g 1 1 27 3,70
+2g 3 3 28 10,71
0a 4 4 29 13,79
QOP 5 4
USI 5 5 9 55,56
Total général 32 31 218 407 7,6
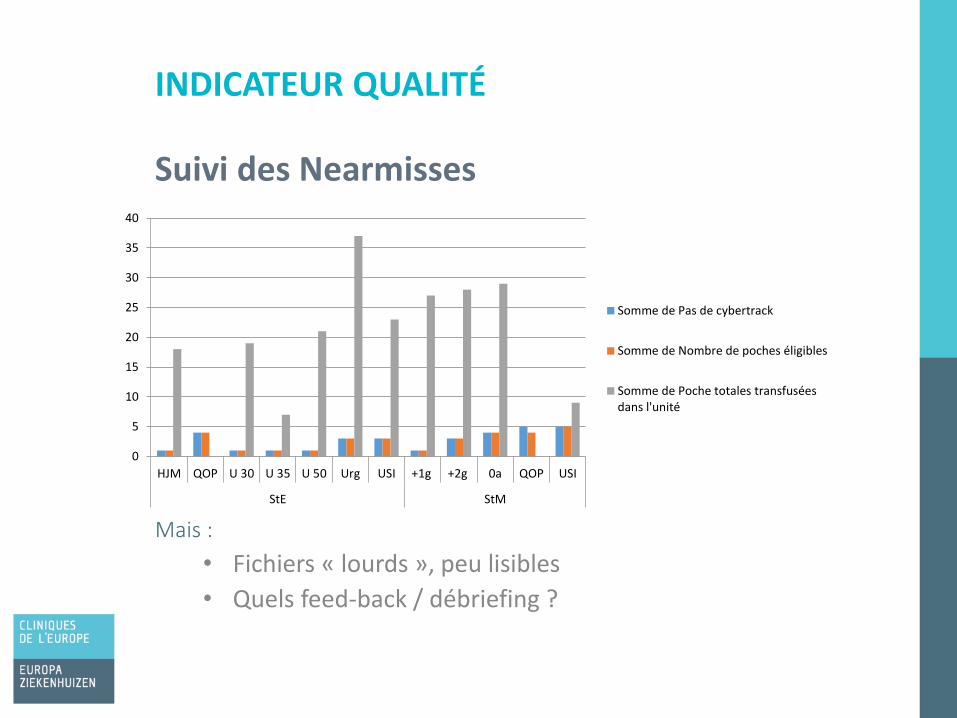
Mais :
• Fichiers « lourds », peu lisibles
• Quels feed-back / débriefing ?
INDICATEUR QUALITÉ
Suivi des Nearmisses
0
5
10
15
20
25
30
35
40
HJM QOP U 30 U 35 U 50 Urg USI +1g +2g 0a QOP USI
StE StM
Somme de Pas de cybertrack
Somme de Nombre de poches éligibles
Somme de Poche totales transfuséesdans l'unité
5 fois par an, l’équipe qualité et sécurité patient (QIPS) initie une campagne de formation et de communication portant sur un sujet particulier (hygiène des mains, double identification des patients, etc) visant différents publics cible via des affiches, newsletters, mails, audits, diffusion de nouvelles procédures et implication de la ligne hiérarchique…
Prise de 3 décisions :
• Choisir des indicateurs de qualité supplémentaires
• Créer et renvoyer un tableau de bord explicite et visuel vers les unités de soins par unité de soins
• Réaliser un tutoriel vidéo
INDICATEURS QUALITÉ
Avril – mai 2017 : 4e thématique transversale!
• Clôture effective électronique via Cybertrack
• Notification de l’absence de réaction transfusionnelle
• Intervalle de temps entre la délivrance de la poche et le début d’administration inférieur à 20 minutes
• Chaîne du froid
• Stocks secondaire « pirates » ? Hormis QOP
• Réalisation de la transfusion lorsqu’il y a assez de personnel dans l’unité c’est-à-dire en semaine (Lu-Ve) de 7 h à 17 h hors urgences, soins intensifs et QOP
INDICATEURS QUALITÉ
Indicateurs supplémentaires
INDICATEURS QUALITÉ
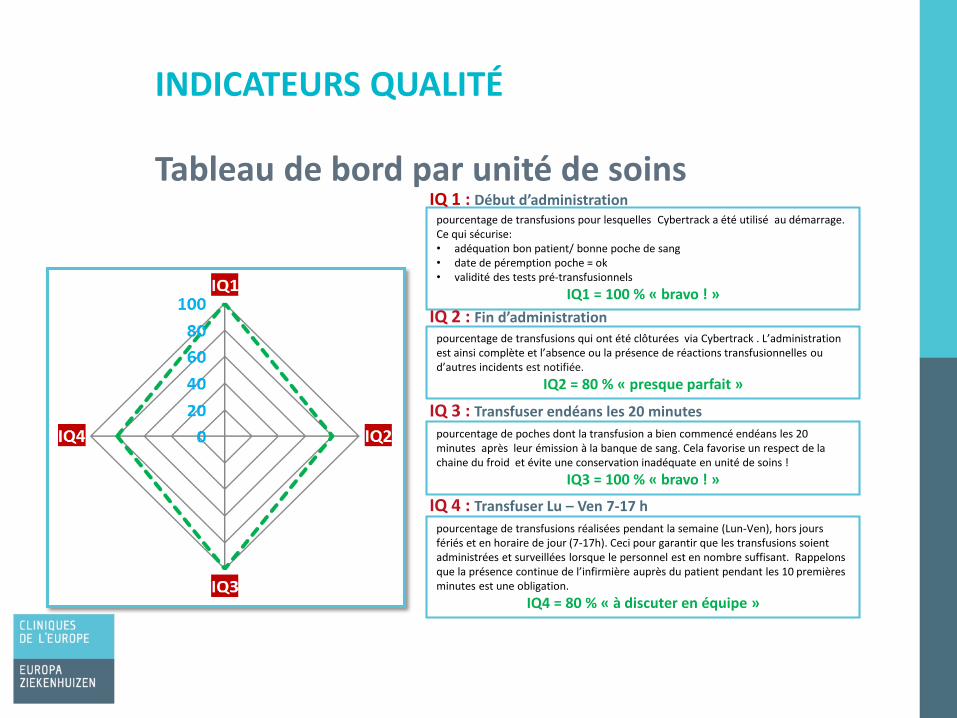
Tableau de bord par unité de soinspourcentage de transfusions pour lesquelles Cybertrack a été utilisé au démarrage. Ce qui sécurise: • adéquation bon patient/ bonne poche de sang• date de péremption poche = ok• validité des tests pré-transfusionnels
IQ1 = 100 % « bravo ! »
IQ 1 : Début d’administration
IQ 2 : Fin d’administration
IQ 3 : Transfuser endéans les 20 minutes
IQ 4 : Transfuser Lu – Ven 7-17 h
pourcentage de transfusions qui ont été clôturées via Cybertrack . L’administration est ainsi complète et l’absence ou la présence de réactions transfusionnelles ou d’autres incidents est notifiée.
IQ2 = 80 % « presque parfait »
pourcentage de poches dont la transfusion a bien commencé endéans les 20 minutes après leur émission à la banque de sang. Cela favorise un respect de la chaine du froid et évite une conservation inadéquate en unité de soins !
IQ3 = 100 % « bravo ! »
pourcentage de transfusions réalisées pendant la semaine (Lun-Ven), hors jours fériés et en horaire de jour (7-17h). Ceci pour garantir que les transfusions soient administrées et surveillées lorsque le personnel est en nombre suffisant. Rappelons que la présence continue de l’infirmière auprès du patient pendant les 10 premières minutes est une obligation.
IQ4 = 80 % « à discuter en équipe »
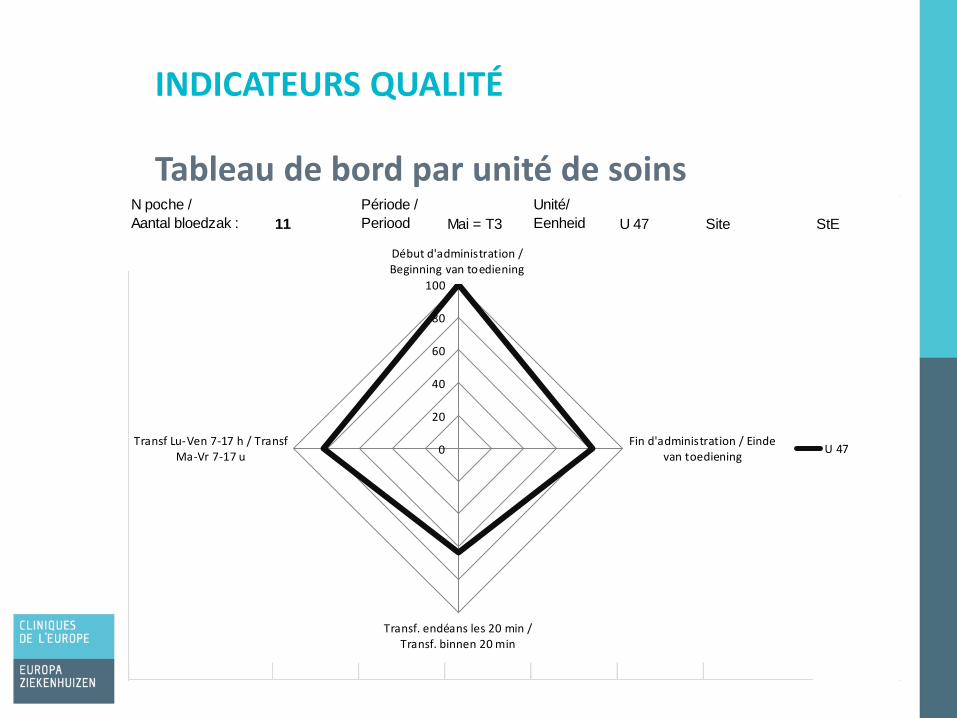
INDICATEURS QUALITÉ
Tableau de bord par unité de soinsN poche /
Aantal bloedzak : 11
Période /
Periood Mai = T3
Unité/
Eenheid U 47 Site StE
0
20
40
60
80
100
Début d'administration /Beginning van toediening
Fin d'administration / Eindevan toediening
Transf. endéans les 20 min /Transf. binnen 20 min
Transf Lu-Ven 7-17 h / TransfMa-Vr 7-17 u
U 47
Home made : smart phone, logiciel de montage
Durée 7 minutes
Choix direct des chapitres si nécessaire
Fr – Ndl
Disponible sur tous les PC de la clinique
TUTORIEL
Processus Cybertrack « happy flow »
• Institutionnalisation du feed-back / débriefing via les tableaux de bord
• A quel rythme ? Mensuel, trimestriel ?
• Qui ? • Directeur qualité et soins + cadres de soins
• Infirmiers chef
• Unités de soin
• Nearmiss = Déclaration d’évènement indésirable
ET DEMAIN ?
Prochains challenges
• Récupération plus automatisée des datas
• Data warehouse
• Biologistes : « mispl », query au niveau de GLIMS
• E-Learning certifiant : autorisation à pratiquer les transfusions
• Prescription électronique
• Implique le corps médical
• Parallèle entre la prescription électronique et la biologie médicale
• Projet institutionnel 2018 dans le cadre de l’accréditation de l’hôpital
ET DEMAIN ?
Prochains challenges
Merci pour votre attention
BEDANKT VOOR UW AANDACHT
Use of a dynamical dashboard to improve and assure the use
of a new bedside scanning system of blood components
UZ Brussel
1er juin 2017 – 1 juni 2017
Gebruik van een dynamisch dashboard om de
toepassing van een nieuw bedside scanning
systeem van bloedcomponenten te verzekeren
Jana Vanden Broeck,
referentiepersoon transfusie
34 22-6-2017
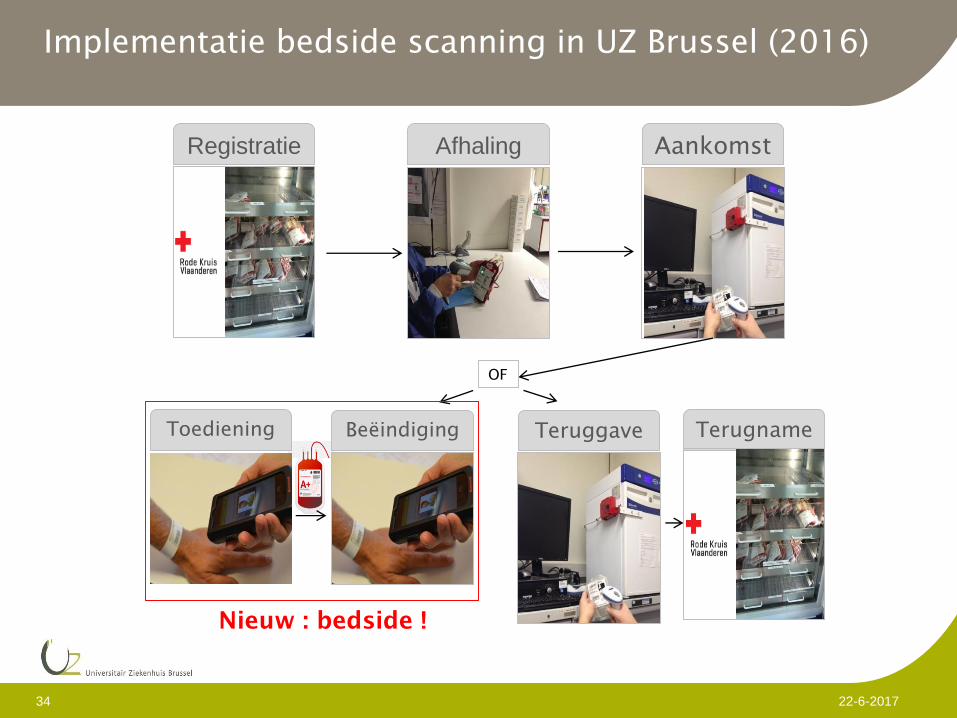
Implementatie bedside scanning in UZ Brussel (2016)
Registratie
Terugname
Afhaling Aankomst
TeruggaveBeëindigingToediening
OF
Nieuw : bedside !
Team
35 22-6-2017
Jana Vanden Broeck, vpk.-specialist transfusie
Jamie Verelst en Daan Van Heghe, software engineers, IT
Luk Wouters, directie verpleegkunde
Kim Goedmakers, Cel Beleidsinformatie
Rik Schots, voorzitter transfusiecomité
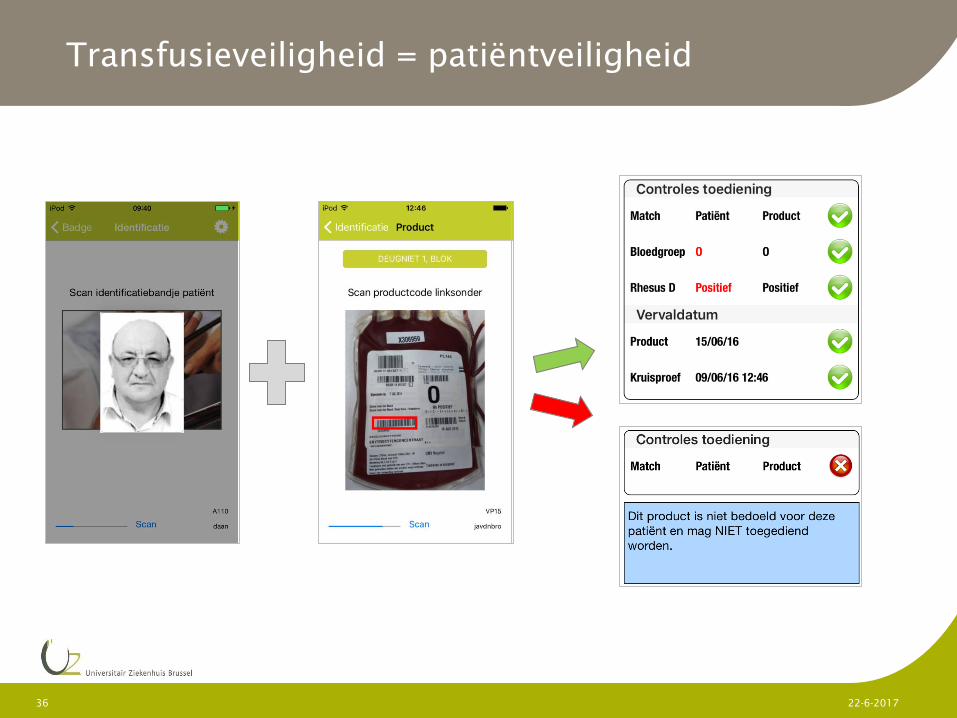
Transfusieveiligheid = patiëntveiligheid
36 22-6-2017

Gebruiksvriendelijkheid
37 22-6-2017
Barcodes scannen
+instructie via
foto’s
Inclusief
registratie
parameters
Overzicht
voorgeschreven
bloedcomponente
n
Mobiel
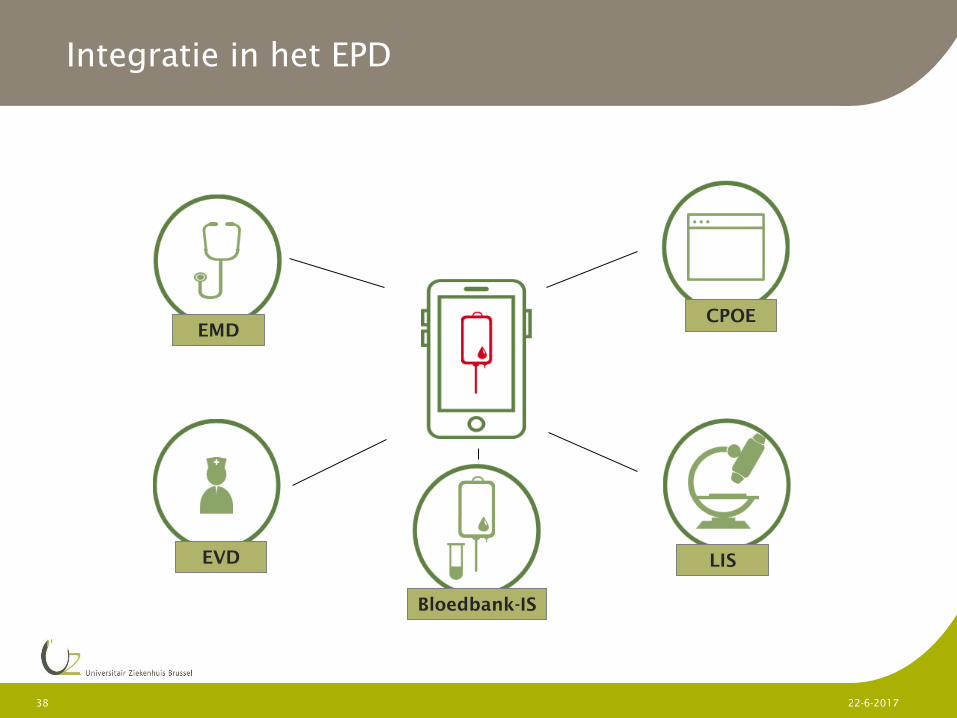
Integratie in het EPD
38 22-6-2017
EMD
EVD
CPOE
LIS
Bloedbank-IS
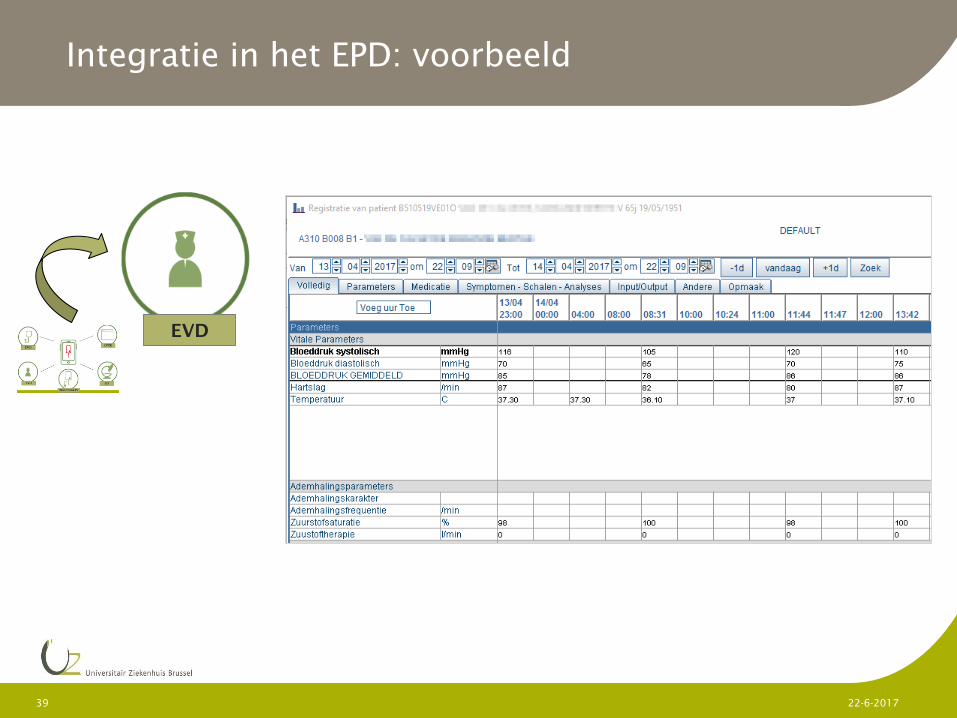
Integratie in het EPD: voorbeeld
39 22-6-2017
EVD
E-learning
+ demo’s
Stapsgewijze implementatie
Opleiding
40 22-6-2017
Correcte toepassing van bedside
scanning bij start en einde van
transfusies (=bloedtracing)
veilige transfusie verzekeren
streefdoel: > 95%
Doelstellingen
41 22-6-2017
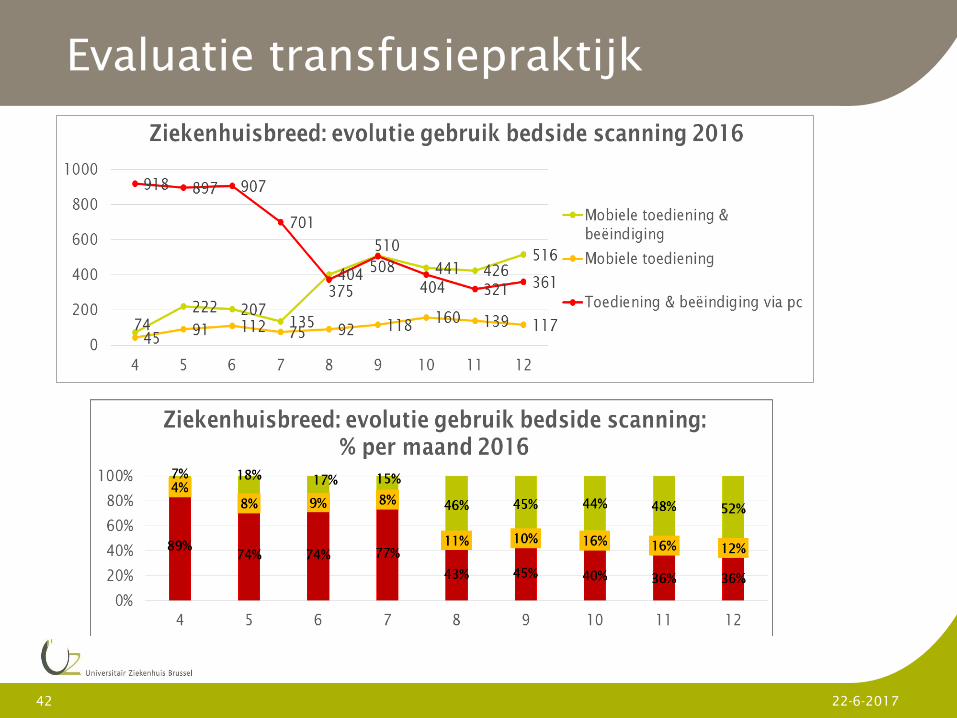
Evaluatie transfusiepraktijk
42 22-6-2017
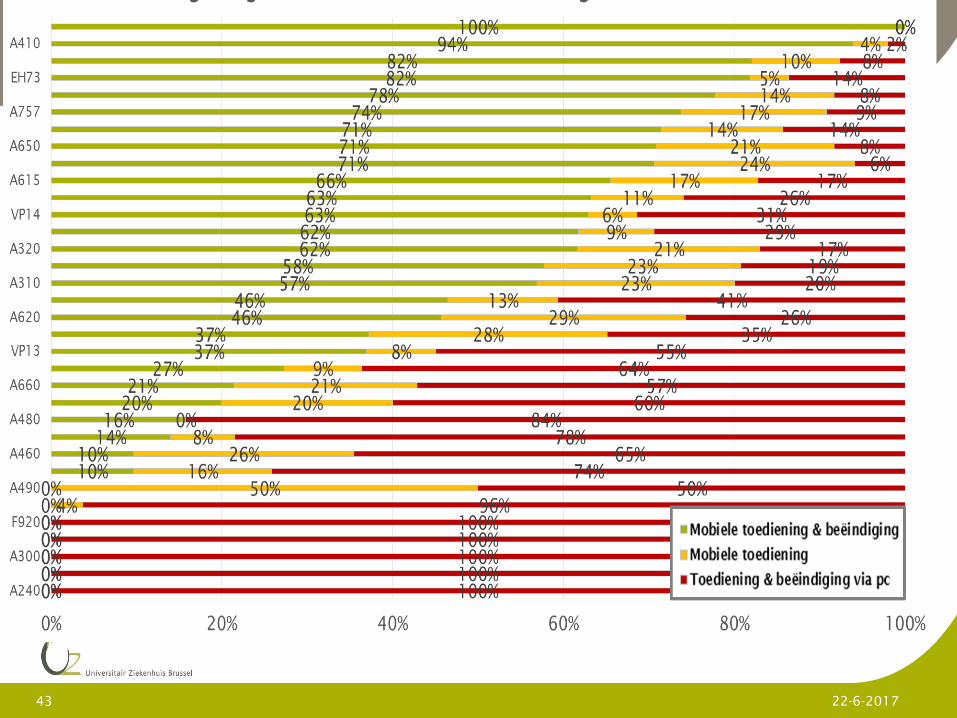
Evaluatie transfusiepraktijk
43 22-6-2017
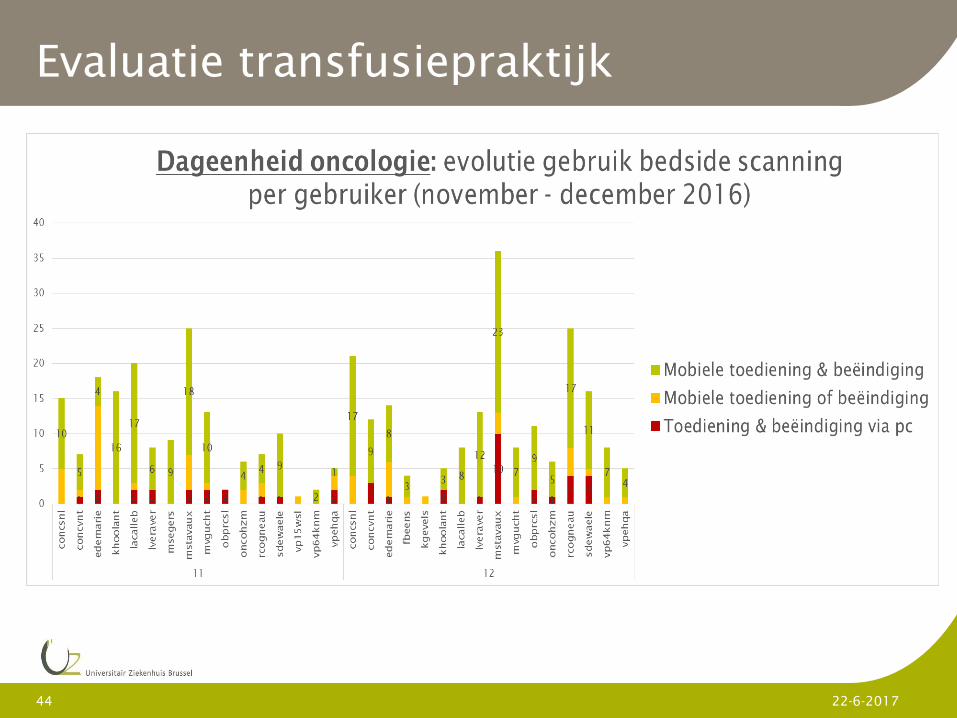
44 22-6-2017
Evaluatie transfusiepraktijk
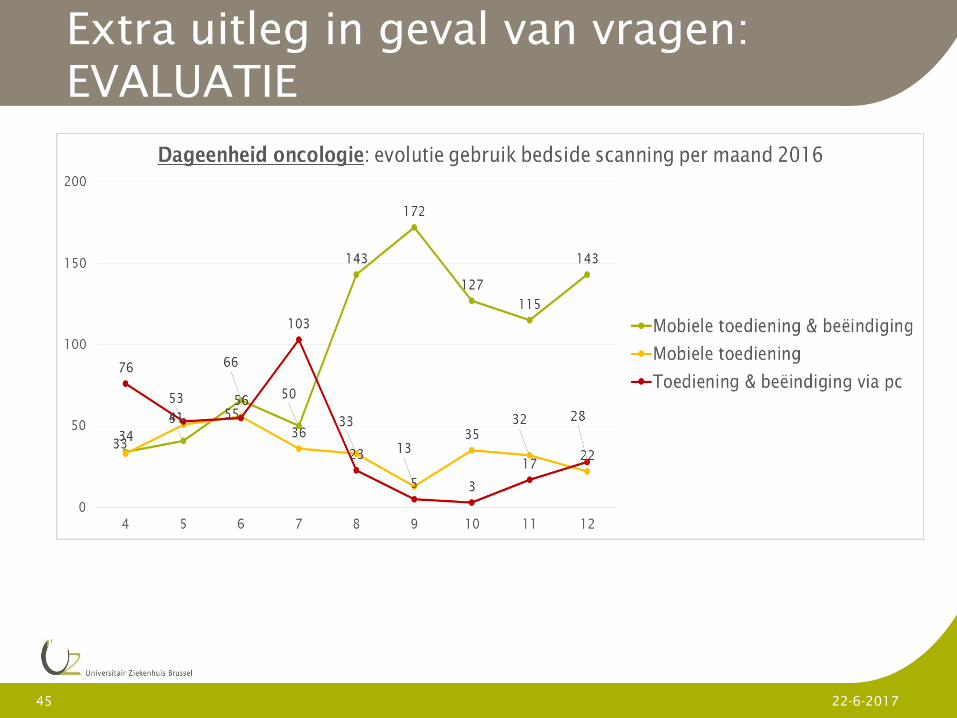
Extra uitleg in geval van vragen:
EVALUATIE
45 22-6-2017
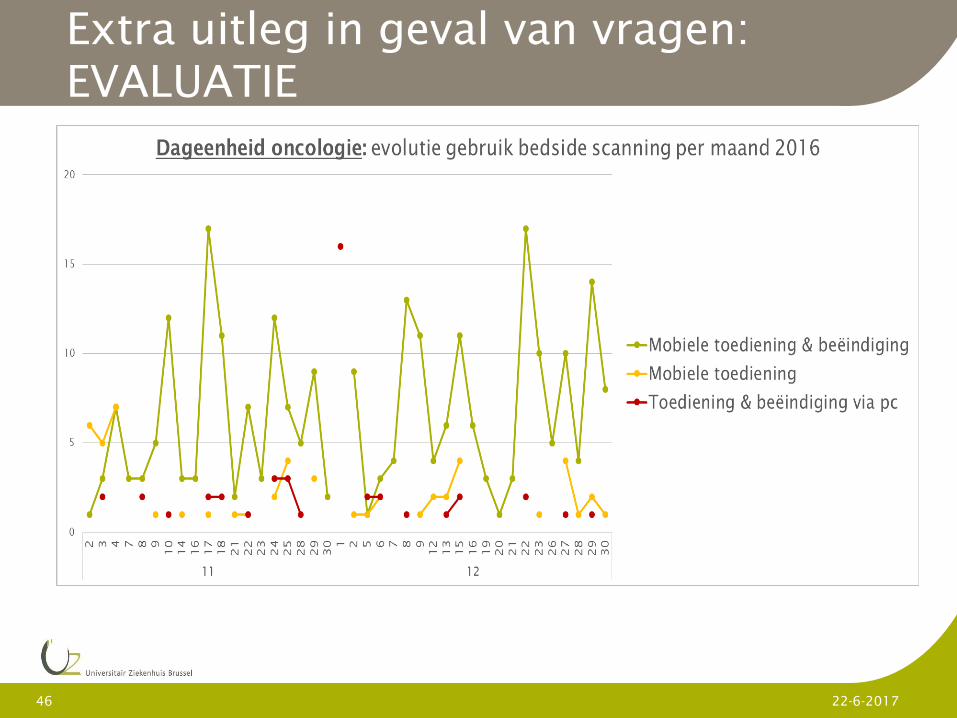
Extra uitleg in geval van vragen:
EVALUATIE
46 22-6-2017
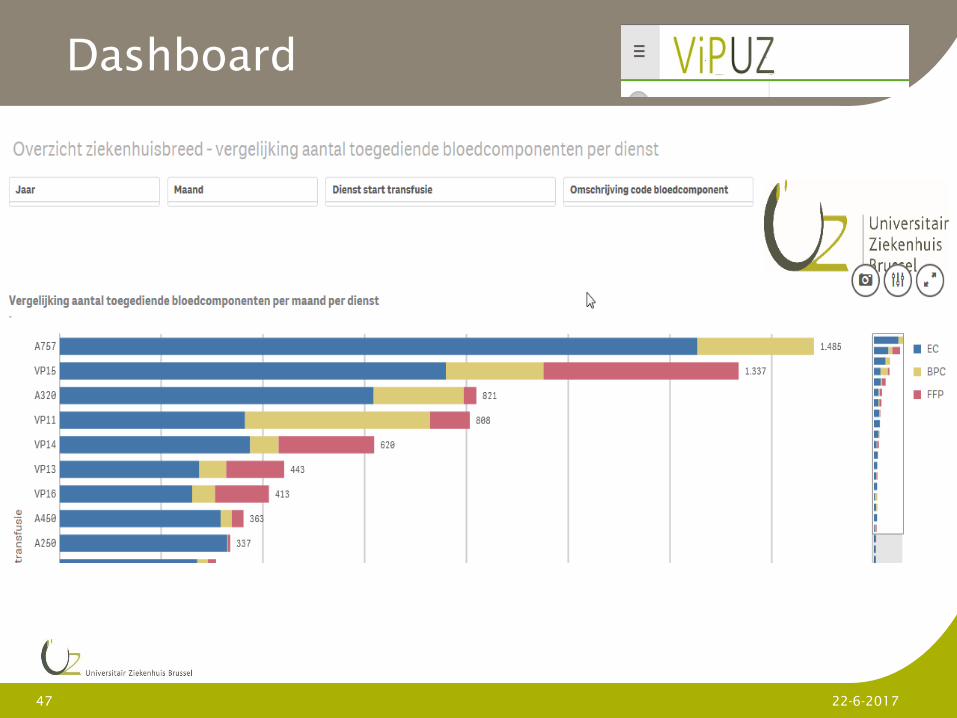
Dashboard
47 22-6-2017
Besluit
48 22-6-2017
Lessons learnt:
• Nog ruimte voor verbetering = nood voor verdere opvolging
• Positief effect van gepersonaliseerde feedback
naar hoofdvpk. a.d.h.v. dashboard
• WIFI-probleem
Next steps:
Gebruik dashboard voor analyse en feedback over bloedverbruik

Onafhankelijke bloednames: continue en gerichte
communicatie noodzakelijk UZA
Symposium
1er juin 2017 – 1 juni 2017

Independent blood samples
requires continuous and
dedicated communication
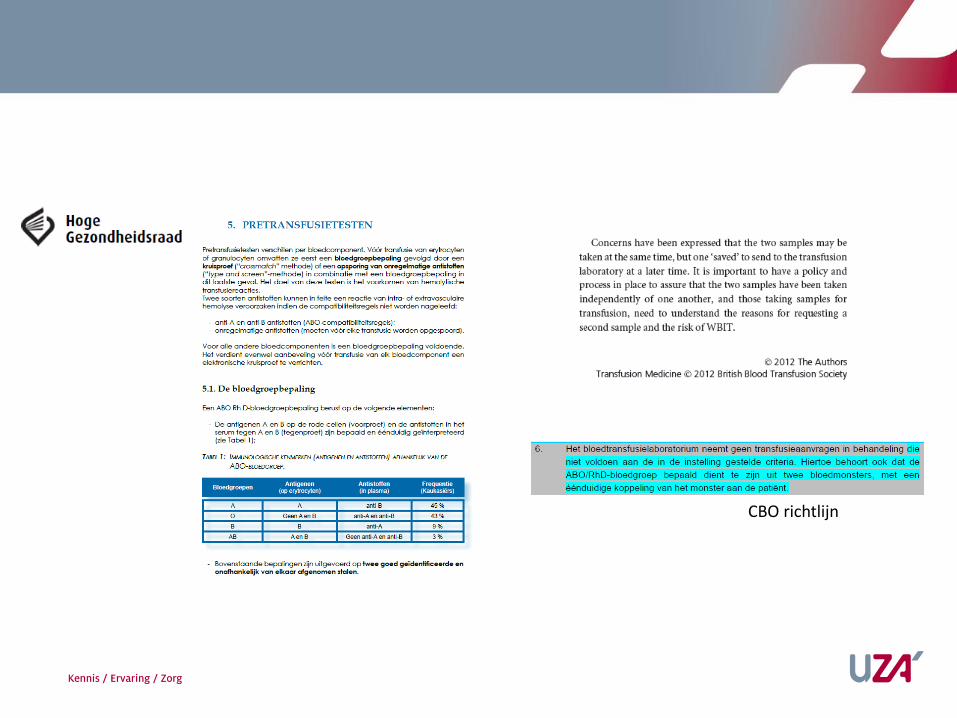
Problem
CBO richtlijn
Problem
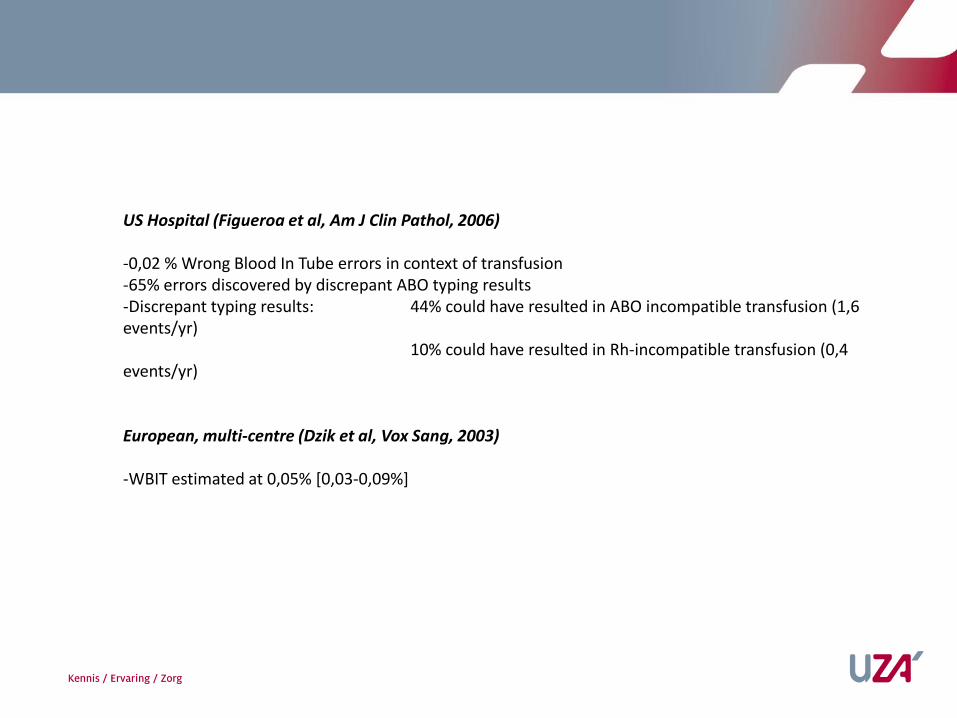
US Hospital (Figueroa et al, Am J Clin Pathol, 2006)
-0,02 % Wrong Blood In Tube errors in context of transfusion-65% errors discovered by discrepant ABO typing results-Discrepant typing results: 44% could have resulted in ABO incompatible transfusion (1,6 events/yr)
10% could have resulted in Rh-incompatible transfusion (0,4 events/yr)
European, multi-centre (Dzik et al, Vox Sang, 2003)
-WBIT estimated at 0,05% [0,03-0,09%]
UZA situation
-UZA immune hematology: 1 january 2015
-Blood group requires at least 2 independent samples: at least differing in time of prelevation
-Order of immune hematology tests/blood components on paper
-Availablity of less than 2 samples is blocking for delivery of ABO-identical ECL, absence of time stamp on bloodorder is not
-Frequently observed during pre-/post-/analytical phase at time of ECL order: no 2 independent samples available (or not identifiable as independent)
• Additional workload for laboratory personnel (phone calls, search for archived sample,…)• Delay in release of ECL or at least excessive use of type O blood• Risk of ABO incompatible transfusion if only observed during post-analytical phase
UZA situation
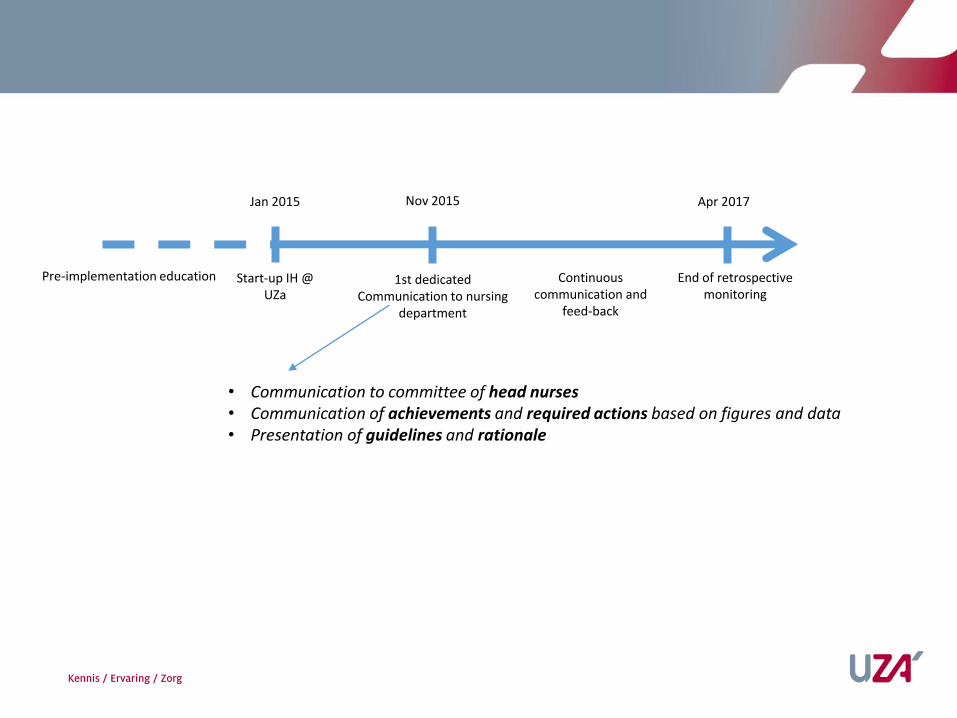
Jan 2015
Pre-implementation education Start-up IH @ UZa
Nov 2015
1st dedicatedCommunication to nursing
department
Continuouscommunication and
feed-back
Apr 2017
End of retrospectivemonitoring
• Communication to committee of head nurses • Communication of achievements and required actions based on figures and data• Presentation of guidelines and rationale
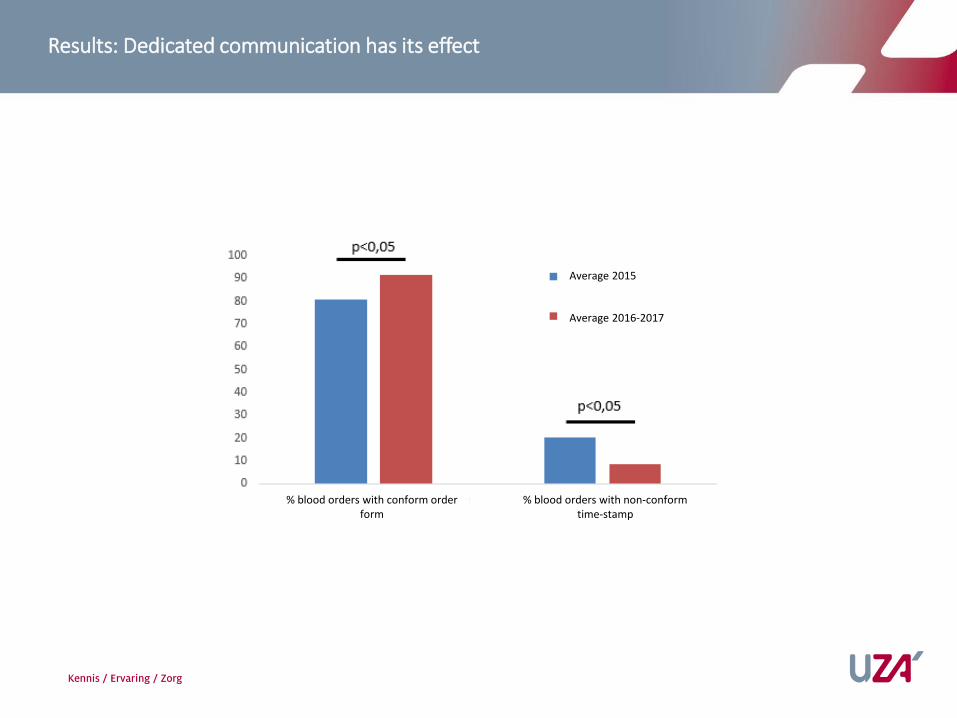
Results: Dedicated communication has its effect
% blood orders with conform order form
% blood orders with non-conform time-stamp
Average 2015
Average 2016-2017
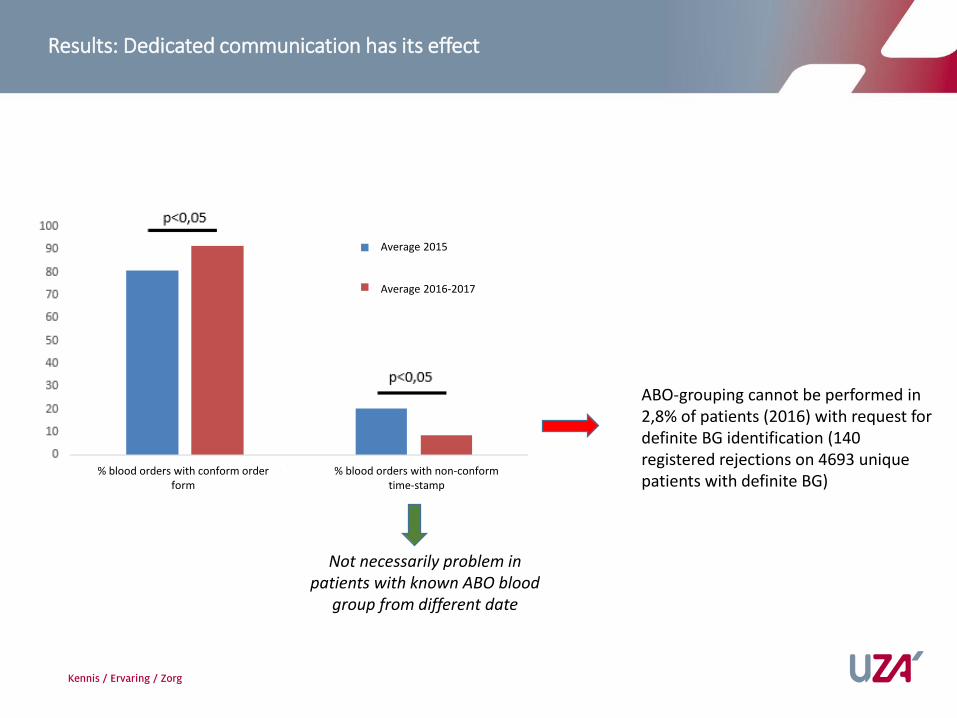
Results: Dedicated communication has its effect
% blood orders with conform order form
% blood orders with non-conform time-stamp
Average 2015
Average 2016-2017
Not necessarily problem in patients with known ABO blood
group from different date
ABO-grouping cannot be performed in 2,8% of patients (2016) with request fordefinite BG identification (140 registered rejections on 4693 uniquepatients with definite BG)
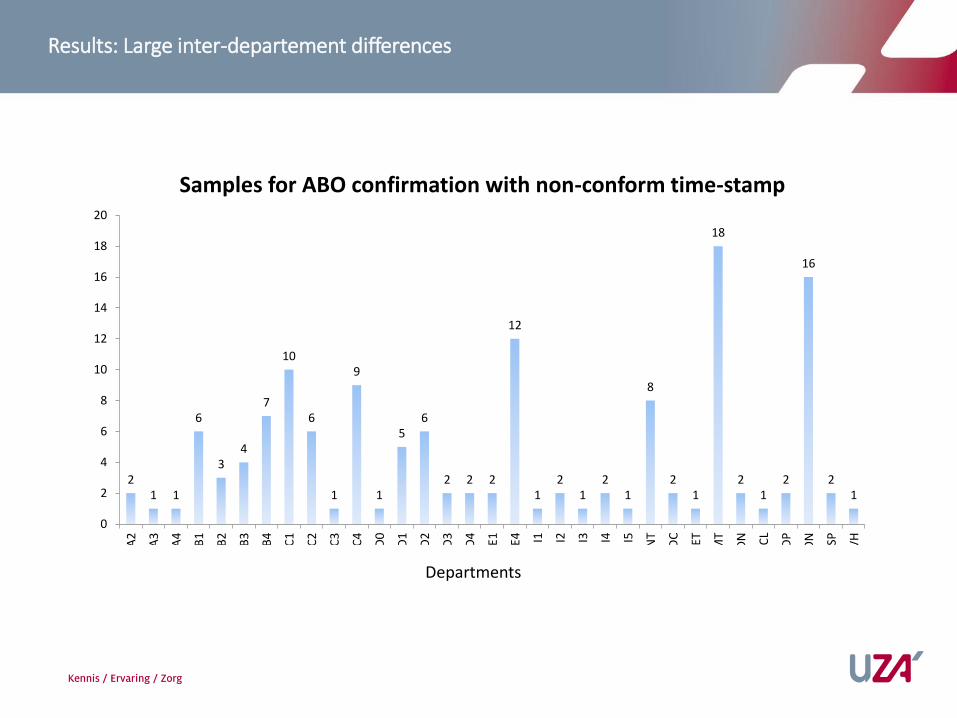
Results: Large inter-departement differences
Departments
21 1
6
34
7
10
6
1
9
1
56
2 2 2
12
12
12
1
8
21
18
21
2
16
21
0
2
4
6
8
10
12
14
16
18
20
A2
A3
A4
B1
B2
B3
B4
C1
C2
C3
C4
D0
D1
D2
D3
D4 E1 E4 I1 I2 I3 I4 I5
AN
T
CD
C
GET
HM
T
ND
N
OC
L
PD
P
SON SP
TVH
Samples for ABO confirmation with non-conform time-stamp
Conclusions and Future outlook
-Independent ABO blood group confirmation requires continuous and dedicated communication in a non-paperless setting
-Further communication at individual department and nurse level to further reduce non-conform ABO identification orders and/or blood-orders
-Additional electronic support? Integration in EHR?
Team
• Stijn Lambrecht en Jan Van den Bossche, Klinische Biologie, ziekenhuisbloedbank, UZA
• Dirk Maes, hemovigilantie-medewerker, UZA
• Paul van Aken, directeur patientenzorg, UZA
• Rudi de Paep, voorzitter transfusie-comité, UZA
• Guy Hans, medisch directeur, UZA

Implementatie bloedbankautomaat voor decentrale uitgifteAZ Delta
Symposium
1er juin 2017 – 1 juni 2017

Implementatie Haemobank voor (de)centrale uitgifte ECL
APR. BIOL. Eline Verhoye
KORTE INHOUD
• Uitdagingen bloedbank fusieziekenhuis AZ Delta
• Visie toekomstige organisatie bloedbank AZ Delta
• Pilootproject Haemobank AZ Delta Roeselare – stadscampus
o Verloop pilootproject
o Validatie en opleiding medewerkers
o SWOT analyse
1/6/2017 Apr. Biol. Eline Verhoye 62
Uitdagingen bloedbank fusieziekenhuis AZ Delta
1/6/2017 Apr. Biol. Eline Verhoye 63

Uitdagingen bloedbank fusieziekenhuis AZ Delta
Huidige situatie:
1/6/2017 Apr. Biol. Eline Verhoye 64
Campus Wilgenstraat
Campus Brugsesteenweg
Campus Westlaan
Campus Menen
Ardolab
ECL 172/149PLC 8Octaplas 10
ECL 5975PLC 1215Octaplas 2157
ECL 857PLC 29Octaplas 101

Campus Torhout
Uitdagingen bloedbank fusieziekenhuis AZ Delta
Toekomstige situatie:
1/6/2017 Apr. Biol. Eline Verhoye 65
Campus Wilgenstraat
Campus Brugsesteenweg
Campus Westlaan
Campus Menen
Ardolab
ECL 172/149PLC 8Octaplas 10
ECL 5975PLC 1215Octaplas 2157
ECL 857PLC 29Octaplas 101
ECL 1396PLC 35Octaplas 91

Campus Torhout
Uitdagingen bloedbank fusieziekenhuis AZ Delta
Toekomstige situatie:
1/6/2017 Apr. Biol. Eline Verhoye 66
Campus Brugsesteenweg
Campus Menen
Campus Oekene
Uitdagingen bloedbank fusieziekenhuis AZ Delta
1. Bemanning bloedbank in campus met oriëntatie planbare zorg
1/6/2017 Apr. Biol. Eline Verhoye 67

Uitdagingen bloedbank fusieziekenhuis AZ Delta
1. Bemanning bloedbank in campus met oriëntatie planbare zorg
2. Overbruggen grote afstand tussen medische diensten en labo/bloedbank
1/6/2017 Apr. Biol. Eline Verhoye 68
Laboratoriumgeneeskunde
Spoed/OK
1/6/2017 Apr. Biol. Eline Verhoye 69
Visie toekomstige organisatie bloedbank AZ Delta

Visie toekomstige organisatie bloedbank AZ Delta
Bloedbankautomatisatie met bewaring/afhaling nabij patiënt
1/6/2017 Apr. Biol. Eline Verhoye 70
Campus BrugsesteenwegCampus Oekene
LIS + BTM
1/6/2017 Apr. Biol. Eline Verhoye 71
Pilootproject Haemobank AZ Delta Roeselare stadscampus
Pilootproject Haemobank stadscampus
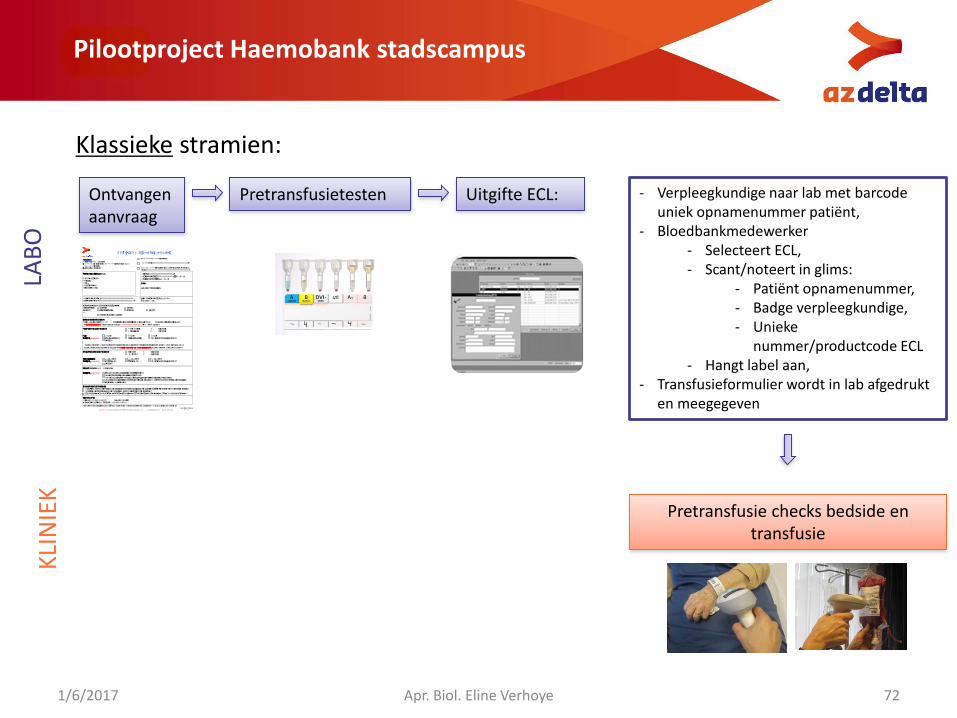
Klassieke stramien:
1/6/2017 Apr. Biol. Eline Verhoye 72
Ontvangen aanvraag
Pretransfusietesten Uitgifte ECL:
LAB
OK
LIN
IEK
- Verpleegkundige naar lab met barcode uniek opnamenummer patiënt,
- Bloedbankmedewerker - Selecteert ECL,- Scant/noteert in glims:
- Patiënt opnamenummer,- Badge verpleegkundige,- Unieke
nummer/productcode ECL- Hangt label aan,
- Transfusieformulier wordt in lab afgedrukt en meegegeven
Pretransfusie checks bedside en transfusie
Bloedbank Wilgenstraat 2, 8800 Roeselare t 051 23 39 69 (Wilgenstraat) / 051 23 60 20 (Brugsesteenweg) / 056 52 23 31 (Menen) e [email protected]
AANVRAAG BLOEDPRODUCTEN
URGENT reden: ……………………………………………………………………………...
STANDAARD PROCEDURE (oa. preop)
Paën den ficae (klever): Naam en voornaam: Geslacht: Adres: Geboortedatum: Opnamenummer:
ARTS
Stempel + handtekening
BLOEDNAME: Datum: …………/…………/………… Tijds p: … : … uur Monsterafnemer (naam + paraaf): ……….………….…………
THROMBOCYTENCONCENTRAAT standaard … eenheden HLA-comp. … eenheden Trombocyten: < 10x10
9
/l PLT < 50x109
/l PLT > 50x109
/l PLT Indicae (verplicht!): therapeusch profylacsch hematologische ziekte na chemo andere: …
PLASMA (Octaplas LG) … eenheden Indicae (verplicht!): trombosche trombocytopenische purpura (TTP) geïsoleerde tekorten aan stollingsfoctor V of XI massale hemorragieën met gecombineerd tekort aan stollingsfactoren of trombolyse hemorragische accidenten door overdosering an vitamine K waarvoor medische correce noodzakelijk neonatale wisseltransfusie
!!Een definieve bloedgroep (zie labogids) dient steeds gekend te zijn! De indicae voor transfusie moet conform BC25.06.2002 opgenomen worden in het
INFORMATIE AAN PATIENT: De paënt is door de aanvragende arts ingelicht over de noodzakelijkheid en bijhorende poten ële risico’s van de bloedtransfusie(s). De vertrouwenspersoon/voogd van de paënt is door de aanvragende arts ingelicht. Noch de paënt, noch de vertrouwenspersoon/voogd konden door de aanvragende arts ingelicht worden owv. medische redenen.
NOODPROCEDURE (ongekruist bloed met risico op transfusiereace)
reden:………………………………………………………………………………………………..
AZ Delta vzw Rode-Kruisstraat 20, 8800 Roeselare t 051 23 71 11 e [email protected] w www.azdelta.be
Dienst:…………………………………………….. Geplande ingreep: ………………………….. op … / … / … Geplande toediening: … / … / …
ERYTHROCYENCONCENTRAAT EC volwassenen … eenheden EC zuigelingen … eenheden Hb: < 7 g/dl 7-9 g/dl > 9 g/dl Indicae (verplicht!): pre-/postoperaef acuut bloedverlies hematologische ziekte na chemo andere: … Het bloedmonster (EDTA-tube) gebruikt voor het uitvoeren van de kruisproef of screenen op irreguliere an stoffen is max. 72 uur geldig. Dit wil
zeggen dat bloed voor de paënt beschikbaar is tot max. 72 uur na het jds p van bloedafname. Nadien is een nieuwe bloedafname vereist.
LABORATORIUMANALYSES (15+17) bloedgroep ABO-Rh controle bloedgroep (nieuwe bloedafname!) compabiliteitstest (T&S, KP)
Een bloedgroepbepaling is slechts geldig als deze op 2 ona ankelijke bloedafnames, in AZ Delta, is bepaald.
Gekende an stoffen*: ………………………………………………………………… Gekend met transfusiereace*? JA/NEE Laatste transfusie*:…………………………………………………………………….. * Indien buiten AZ Delta
Specifieke indicae voor bijzondere producten Type product: bestraald ander: … Indicae: transplantpaënt neonaat ander: … OF Zie transfusiebeleid Cyberlab
B.H.55 versie 1 pag 1/2 0520 1623
Bloedbank Wilgenstraat 2, 8800 Roeselare t 051 23 39 69 (Wilgenstraat) / 051 23 60 20 (Brugsesteenweg) / 056 52 23 31 (Menen) e [email protected]
AANVRAAG BLOEDPRODUCTEN
URGENT reden: ……………………………………………………………………………...
STANDAARD PROCEDURE (oa. preop)
Paën den ficae (klever): Naam en voornaam: Geslacht: Adres: Geboortedatum: Opnamenummer:
ARTS
Stempel + handtekening
BLOEDNAME: Datum: …………/…………/………… Tijds p: … : … uur Monsterafnemer (naam + paraaf): ……….………….…………
THROMBOCYTENCONCENTRAAT standaard … eenheden HLA-comp. … eenheden Trombocyten: < 10x10
9
/l PLT < 50x109
/l PLT > 50x109
/l PLT Indicae (verplicht!): therapeusch profylacsch hematologische ziekte na chemo andere: …
PLASMA (Octaplas LG) … eenheden Indicae (verplicht!): trombosche trombocytopenische purpura (TTP) geïsoleerde tekorten aan stollingsfoctor V of XI massale hemorragieën met gecombineerd tekort aan stollingsfactoren of trombolyse hemorragische accidenten door overdosering an vitamine K waarvoor medische correce noodzakelijk neonatale wisseltransfusie
!!Een definieve bloedgroep (zie labogids) dient steeds gekend te zijn! De indicae voor transfusie moet conform BC25.06.2002 opgenomen worden in het
INFORMATIE AAN PATIENT: De paënt is door de aanvragende arts ingelicht over de noodzakelijkheid en bijhorende poten ële risico’s van de bloedtransfusie(s). De vertrouwenspersoon/voogd van de paënt is door de aanvragende arts ingelicht. Noch de paënt, noch de vertrouwenspersoon/voogd konden door de aanvragende arts ingelicht worden owv. medische redenen.
NOODPROCEDURE (ongekruist bloed met risico op transfusiereace)
reden:………………………………………………………………………………………………..
AZ Delta vzw Rode-Kruisstraat 20, 8800 Roeselare t 051 23 71 11 e [email protected] w www.azdelta.be
Dienst:…………………………………………….. Geplande ingreep: ………………………….. op … / … / … Geplande toediening: … / … / …
ERYTHROCYENCONCENTRAAT EC volwassenen … eenheden EC zuigelingen … eenheden Hb: < 7 g/dl 7-9 g/dl > 9 g/dl Indicae (verplicht!): pre-/postoperaef acuut bloedverlies hematologische ziekte na chemo andere: … Het bloedmonster (EDTA-tube) gebruikt voor het uitvoeren van de kruisproef of screenen op irreguliere an stoffen is max. 72 uur geldig. Dit wil
zeggen dat bloed voor de paënt beschikbaar is tot max. 72 uur na het jds p van bloedafname. Nadien is een nieuwe bloedafname vereist.
LABORATORIUMANALYSES (15+17) bloedgroep ABO-Rh controle bloedgroep (nieuwe bloedafname!) compabiliteitstest (T&S, KP)
Een bloedgroepbepaling is slechts geldig als deze op 2 ona ankelijke bloedafnames, in AZ Delta, is bepaald.
Gekende an stoffen*: ………………………………………………………………… Gekend met transfusiereace*? JA/NEE Laatste transfusie*:…………………………………………………………………….. * Indien buiten AZ Delta
Specifieke indicae voor bijzondere producten Type product: bestraald ander: … Indicae: transplantpaënt neonaat ander: … OF Zie transfusiebeleid Cyberlab
B.H.55 versie 1 pag 1/2 0520 1623
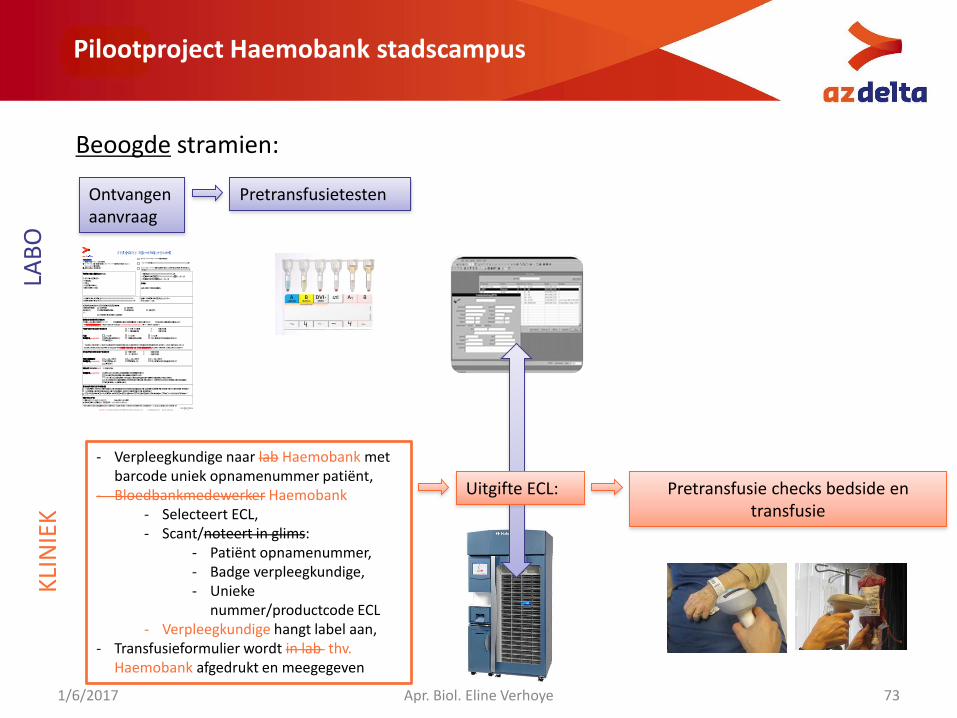
Pilootproject Haemobank stadscampus
Beoogde stramien:
1/6/2017 Apr. Biol. Eline Verhoye 73
Ontvangen aanvraag
Pretransfusietesten
Uitgifte ECL: Pretransfusie checks bedside en transfusie
LAB
O
- Verpleegkundige naar lab Haemobank met barcode uniek opnamenummer patiënt,
- Bloedbankmedewerker Haemobank- Selecteert ECL,- Scant/noteert in glims:
- Patiënt opnamenummer,- Badge verpleegkundige,- Unieke
nummer/productcode ECL- Verpleegkundige hangt label aan,
- Transfusieformulier wordt in lab thv. Haemobank afgedrukt en meegegeven
KLI
NIE
K
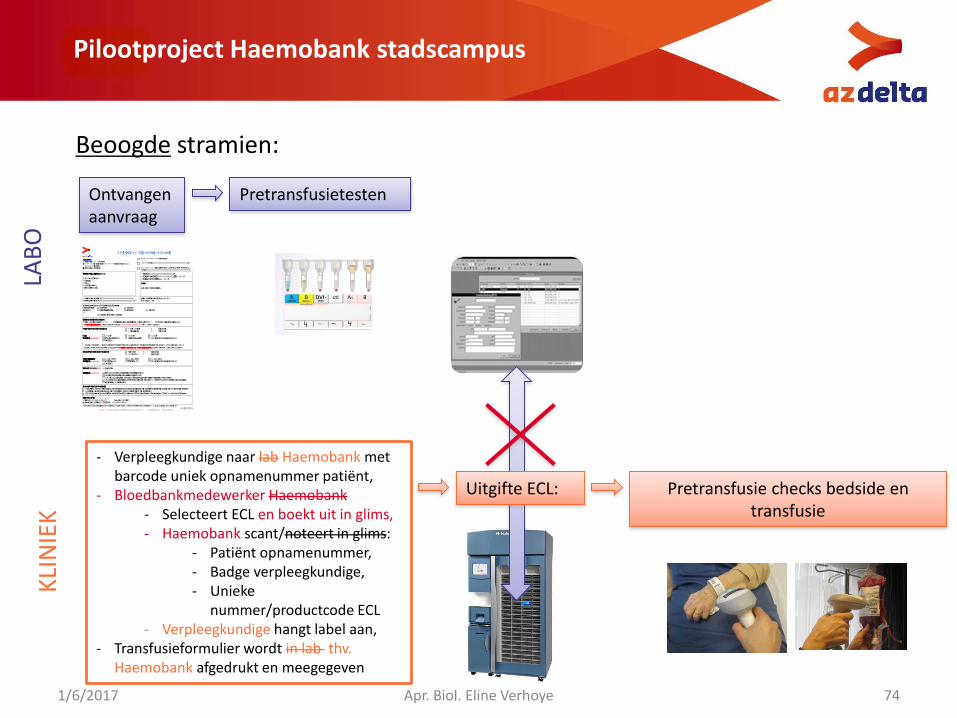
Pilootproject Haemobank stadscampus
Beoogde stramien:
1/6/2017 Apr. Biol. Eline Verhoye 74
Ontvangen aanvraag
Pretransfusietesten
Uitgifte ECL: Pretransfusie checks bedside en transfusie
LAB
OK
LIN
IEK
- Verpleegkundige naar lab Haemobank met barcode uniek opnamenummer patiënt,
- Bloedbankmedewerker Haemobank- Selecteert ECL en boekt uit in glims,- Haemobank scant/noteert in glims:
- Patiënt opnamenummer,- Badge verpleegkundige,- Unieke
nummer/productcode ECL- Verpleegkundige hangt label aan,
- Transfusieformulier wordt in lab thv. Haemobank afgedrukt en meegegeven
Bloedbank Wilgenstraat 2, 8800 Roeselare t 051 23 39 69 (Wilgenstraat) / 051 23 60 20 (Brugsesteenweg) / 056 52 23 31 (Menen) e [email protected]
AANVRAAG BLOEDPRODUCTEN
URGENT reden: ……………………………………………………………………………...
STANDAARD PROCEDURE (oa. preop)
Paën den ficae (klever): Naam en voornaam: Geslacht: Adres: Geboortedatum: Opnamenummer:
ARTS
Stempel + handtekening
BLOEDNAME: Datum: …………/…………/………… Tijds p: … : … uur Monsterafnemer (naam + paraaf): ……….………….…………
THROMBOCYTENCONCENTRAAT standaard … eenheden HLA-comp. … eenheden Trombocyten: < 10x10
9
/l PLT < 50x109
/l PLT > 50x109
/l PLT Indicae (verplicht!): therapeusch profylacsch hematologische ziekte na chemo andere: …
PLASMA (Octaplas LG) … eenheden Indicae (verplicht!): trombosche trombocytopenische purpura (TTP) geïsoleerde tekorten aan stollingsfoctor V of XI massale hemorragieën met gecombineerd tekort aan stollingsfactoren of trombolyse hemorragische accidenten door overdosering an vitamine K waarvoor medische correce noodzakelijk neonatale wisseltransfusie
!!Een definieve bloedgroep (zie labogids) dient steeds gekend te zijn! De indicae voor transfusie moet conform BC25.06.2002 opgenomen worden in het
INFORMATIE AAN PATIENT: De paënt is door de aanvragende arts ingelicht over de noodzakelijkheid en bijhorende poten ële risico’s van de bloedtransfusie(s). De vertrouwenspersoon/voogd van de paënt is door de aanvragende arts ingelicht. Noch de paënt, noch de vertrouwenspersoon/voogd konden door de aanvragende arts ingelicht worden owv. medische redenen.
NOODPROCEDURE (ongekruist bloed met risico op transfusiereace)
reden:………………………………………………………………………………………………..
AZ Delta vzw Rode-Kruisstraat 20, 8800 Roeselare t 051 23 71 11 e [email protected] w www.azdelta.be
Dienst:…………………………………………….. Geplande ingreep: ………………………….. op … / … / … Geplande toediening: … / … / …
ERYTHROCYENCONCENTRAAT EC volwassenen … eenheden EC zuigelingen … eenheden Hb: < 7 g/dl 7-9 g/dl > 9 g/dl Indicae (verplicht!): pre-/postoperaef acuut bloedverlies hematologische ziekte na chemo andere: … Het bloedmonster (EDTA-tube) gebruikt voor het uitvoeren van de kruisproef of screenen op irreguliere an stoffen is max. 72 uur geldig. Dit wil
zeggen dat bloed voor de paënt beschikbaar is tot max. 72 uur na het jds p van bloedafname. Nadien is een nieuwe bloedafname vereist.
LABORATORIUMANALYSES (15+17) bloedgroep ABO-Rh controle bloedgroep (nieuwe bloedafname!) compabiliteitstest (T&S, KP)
Een bloedgroepbepaling is slechts geldig als deze op 2 ona ankelijke bloedafnames, in AZ Delta, is bepaald.
Gekende an stoffen*: ………………………………………………………………… Gekend met transfusiereace*? JA/NEE Laatste transfusie*:…………………………………………………………………….. * Indien buiten AZ Delta
Specifieke indicae voor bijzondere producten Type product: bestraald ander: … Indicae: transplantpaënt neonaat ander: … OF Zie transfusiebeleid Cyberlab
B.H.55 versie 1 pag 1/2 0520 1623
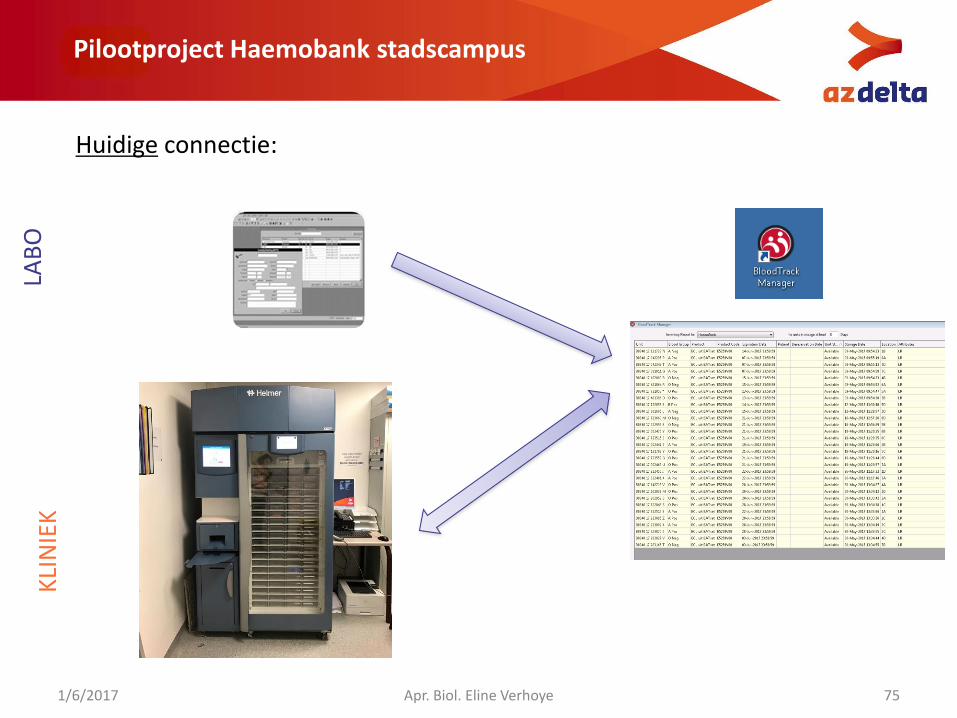
Pilootproject Haemobank stadscampus
Huidige connectie:
1/6/2017 Apr. Biol. Eline Verhoye 75
LAB
OK
LIN
IEK
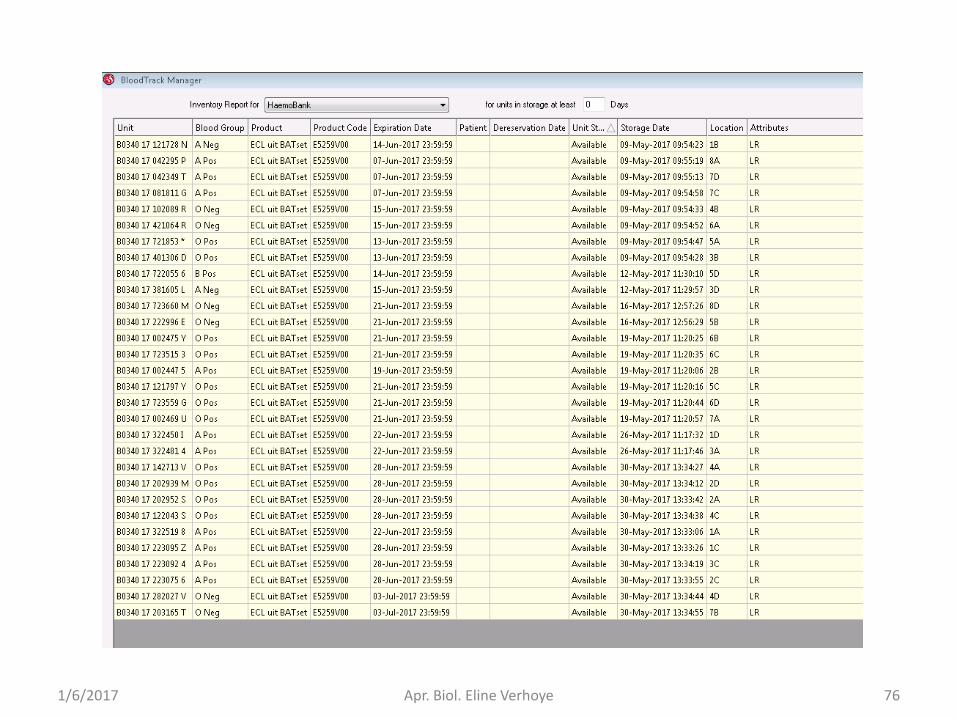
1/6/2017 Apr. Biol. Eline Verhoye 76
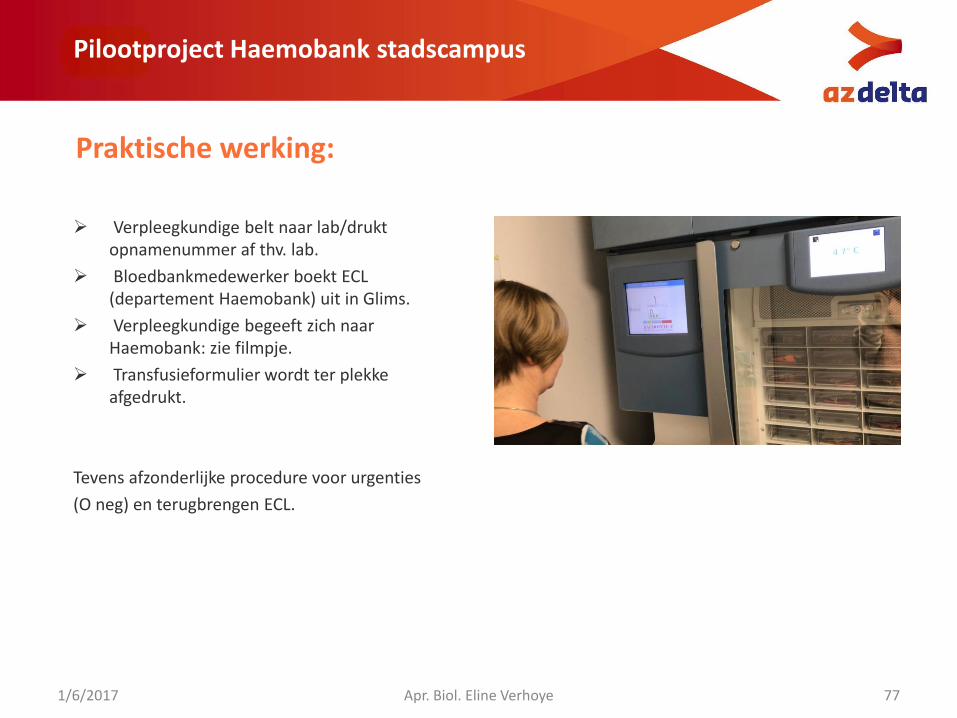
Pilootproject Haemobank stadscampus
Verpleegkundige belt naar lab/drukt opnamenummer af thv. lab.
Bloedbankmedewerker boekt ECL (departement Haemobank) uit in Glims.
Verpleegkundige begeeft zich naar Haemobank: zie filmpje.
Transfusieformulier wordt ter plekke afgedrukt.
Tevens afzonderlijke procedure voor urgenties
(O neg) en terugbrengen ECL.
Praktische werking:
1/6/2017 Apr. Biol. Eline Verhoye 77
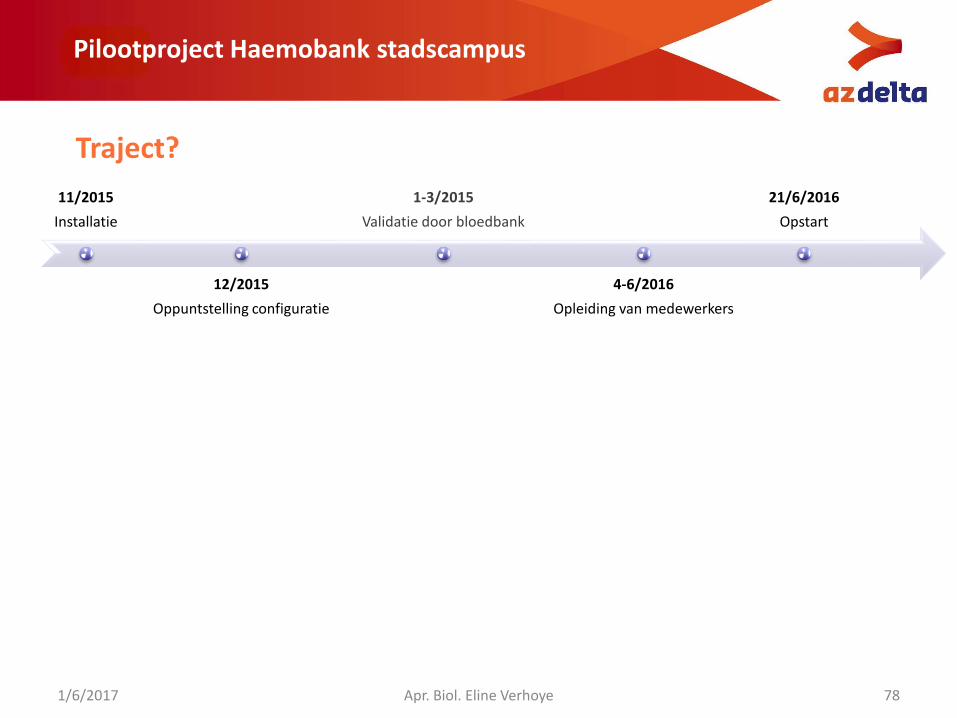
Pilootproject Haemobank stadscampus
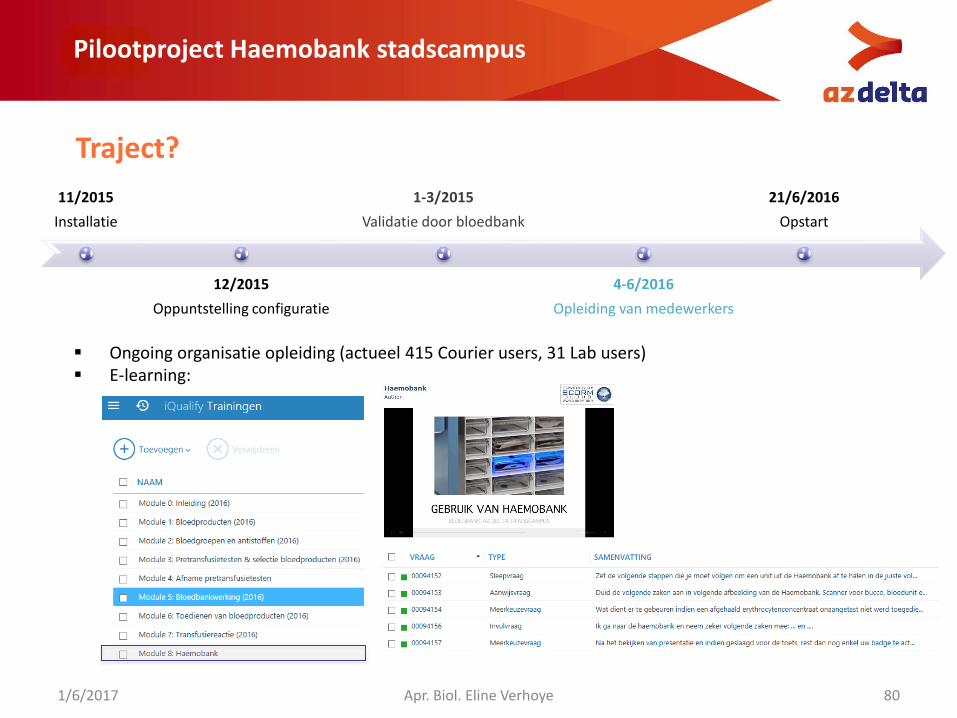
11/2015
Installatie
12/2015
Oppuntstelling configuratie
1-3/2015
Validatie door bloedbank
4-6/2016
Opleiding van medewerkers
21/6/2016
Opstart
Traject?
1/6/2017 Apr. Biol. Eline Verhoye 78
11/2015
Installatie
12/2015
Oppuntstelling configuratie
1-3/2015
Validatie door bloedbank
4-6/2016
Opleiding van medewerkers
21/6/2016
Opstart
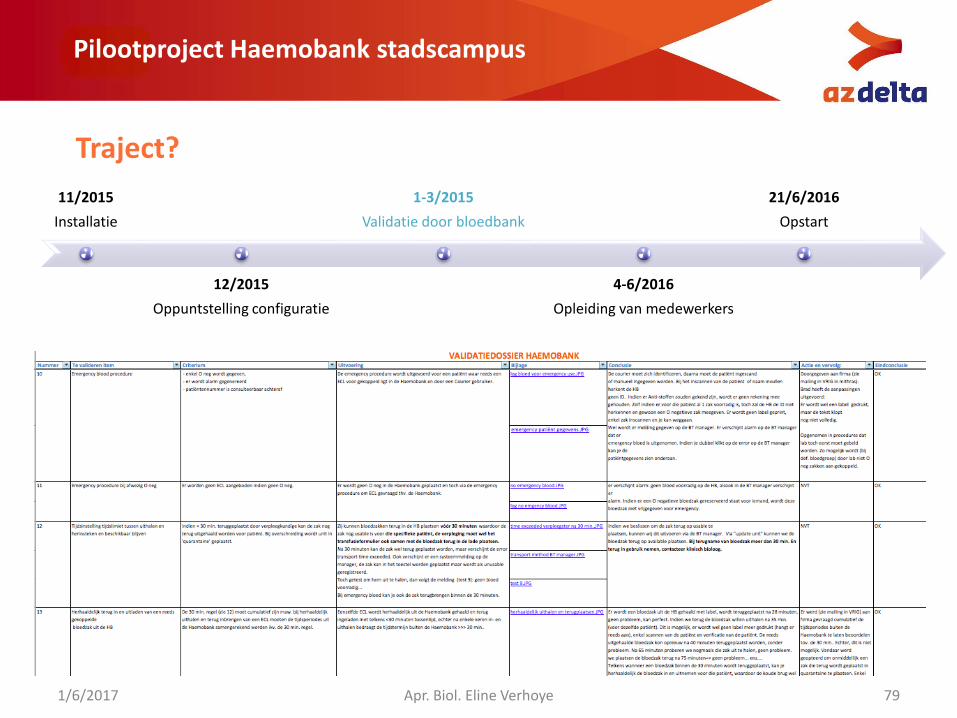
Pilootproject Haemobank stadscampus
Traject?
1/6/2017 Apr. Biol. Eline Verhoye 79
11/2015
Installatie
12/2015
Oppuntstelling configuratie
1-3/2015
Validatie door bloedbank
4-6/2016
Opleiding van medewerkers
21/6/2016
Opstart
Pilootproject Haemobank stadscampus
Traject?
1/6/2017 Apr. Biol. Eline Verhoye 80
Ongoing organisatie opleiding (actueel 415 Courier users, 31 Lab users) E-learning:
Pilootproject Haemobank stadscampus
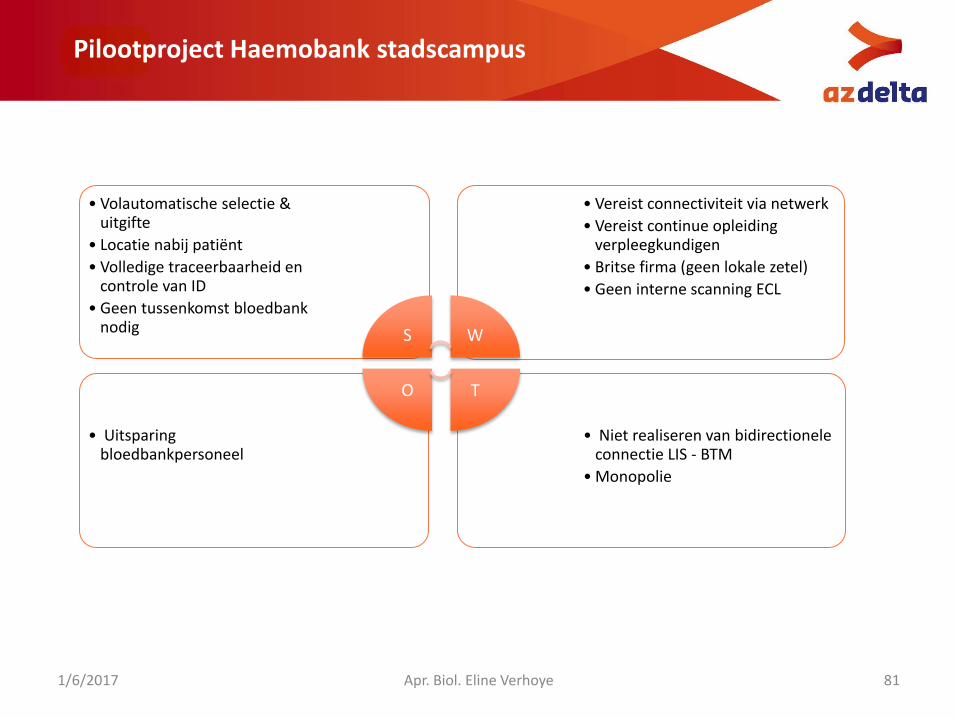
1/6/2017 Apr. Biol. Eline Verhoye 81
• Niet realiseren van bidirectioneleconnectie LIS - BTM
• Monopolie
• Uitsparing bloedbankpersoneel
• Vereist connectiviteit via netwerk
• Vereist continue opleiding verpleegkundigen
• Britse firma (geen lokale zetel)
• Geen interne scanning ECL
• Volautomatische selectie & uitgifte
• Locatie nabij patiënt
• Volledige traceerbaarheid en controle van ID
• Geen tussenkomst bloedbank nodig S W
TO
International, prospective haemovigilance study on
methylene blue-treated plasmaUZ Gent
Symposium
1er juin 2017 – 1 juni 2017

Vox Sanguinis (2017)
ORIGINAL PAPER© 2017 International Society of Blood Transfusion
DOI: 10.1111/vox.12510
International, prospective haemovigilance study on
methylene blue-treated plasma
L. Noens,1 Ma. D. Vilarin~o,2 A. Megalou3 & H. Qureshi4
1Universitair Ziekenhuis, Gent, Belgium2Complejo Universitario de Santiago de Compostela, Santiago de Compostela, Spain3Evaggelismos General Hospital of Athens, Athens, Greece4University Hospitals of Leicester NHS Trust, Leicester, UK
Received: 13 July 2016,
revised 27 December 2016,
accepted 11 February 2017
Background and objectives Methylene blue is a phenothiazine dye, which incombination with visible light has virucidal and bactericidal properties, disrupt-ing the replication of a broad range of enveloped viruses and some non-envel-
oped viruses. The study objective was to collect data on adverse reactionsoccurring with methylene blue plasma administered in a routine clinical practice
environment and document their characteristics and severity.
Materials and methods This was an open label, multicentre, non-controlled, non-randomized, non-interventional study. Patients who receive a methylene blue
plasma transfusion were observed for any signs and symptoms (adverse reactions)within 24 h safter the start of the transfusion, in different hospitals for a studyduration of at least 1 year.
Results A total of 19 315 methylene blue plasma units were transfused. There wereeight patients with adverse reactions recorded during the study, one of themserious. Two had more than one reaction (two and four, respectively). Three
patients had previous transfusions with methylene blue plasma only.
Conclusion Methylene blue plasma has a very acceptable safety profile with a rate of serious adverse reactions of 0·5/10 000 units.
Key words: blood safety, haemovigilance, methylene blue, pathogen reduction.
MacoPharma improved the original Springe method by
developing the THERAFLEX MB-Plasma system [3], mar-
keted in several countries worldwide as a PR system for
plasma to reduce the risk of transmission of pathogens.
The system comprises a disposable kit incorporating MB
and partially an MB removal filter (BLUEFLEX) as well as
an illumination device for the application of the visible
light.
In 2011, the French national drug regulatory agency
ANSM (previously known as AFSSAPS) decided to pro-
gressively stop the clinical use of MB-treated plasma. One
reason for this decision was a reported higher risk of sev-
ere allergic reactions for patients transfused with MB-
treated plasma as compared to patients transfused with
plasma treated with other PR methods [4]. In contrast, this
higher risk has not been observed in other countries even
in those not using the BLUEFLEX plasma filter after
illumination; however, the available data come from their
Introduction
The implementation of pathogen reduction (PR) for labile
blood components aims at reducing a potential infection
risks mainly by emerging pathogens.
The technology to use methylene blue (MB) for the PR
of plasma for therapeutic use was first developed by the
Blood Centre of the German Red Cross, Springe, Germany,
and has been used in clinical practice for 20 years [1]. MB
is a phenothiazine dye, which, in combination with
visible light, has virucidal properties by interacting with
nucleic acids and disrupting the replication of a broad
range of enveloped viruses and some non-enveloped
viruses [2] as well as other micro-organisms.
Correspondence: Lucien Noens, Blood Bank, Universitair Ziekenhuis, De
Pintelaan 185, Ghent 9000,Belgium
E-mail: [email protected]
1
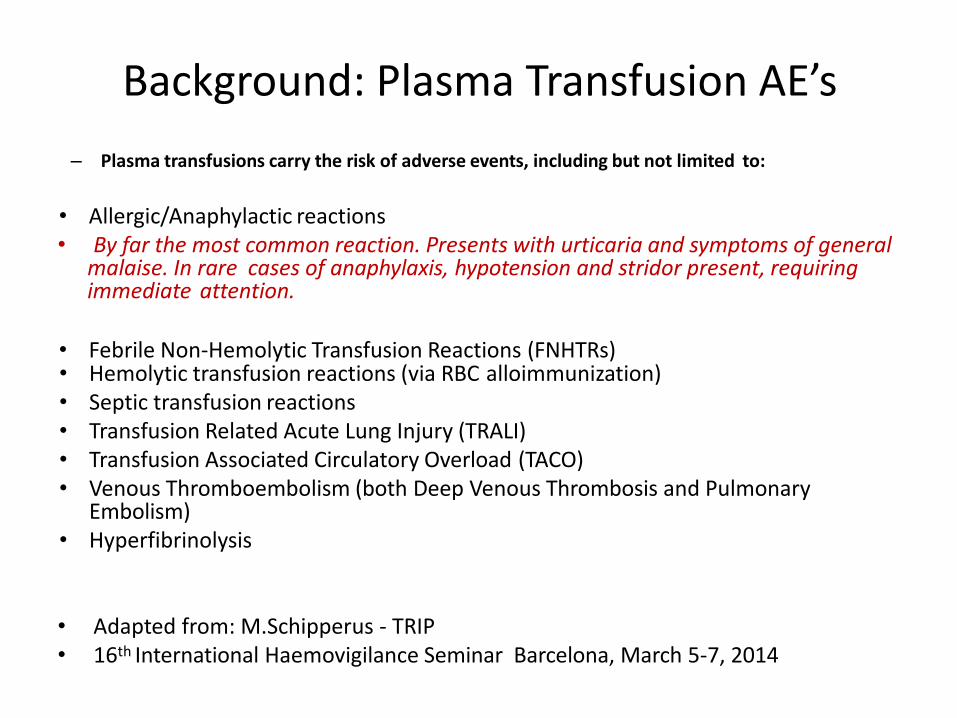
Background: Plasma Transfusion AE’s
– Plasma transfusions carry the risk of adverse events, including but not limited to:
• Allergic/Anaphylactic reactions• By far the most common reaction. Presents with urticaria and symptoms of general
malaise. In rare cases of anaphylaxis, hypotension and stridor present, requiringimmediate attention.
• Febrile Non-Hemolytic Transfusion Reactions (FNHTRs)• Hemolytic transfusion reactions (via RBC alloimmunization)• Septic transfusion reactions• Transfusion Related Acute Lung Injury (TRALI)• Transfusion Associated Circulatory Overload (TACO)• Venous Thromboembolism (both Deep Venous Thrombosis and Pulmonary
Embolism)• Hyperfibrinolysis
• Adapted from: M.Schipperus - TRIP • 16th International Haemovigilance Seminar Barcelona, March 5-7, 2014
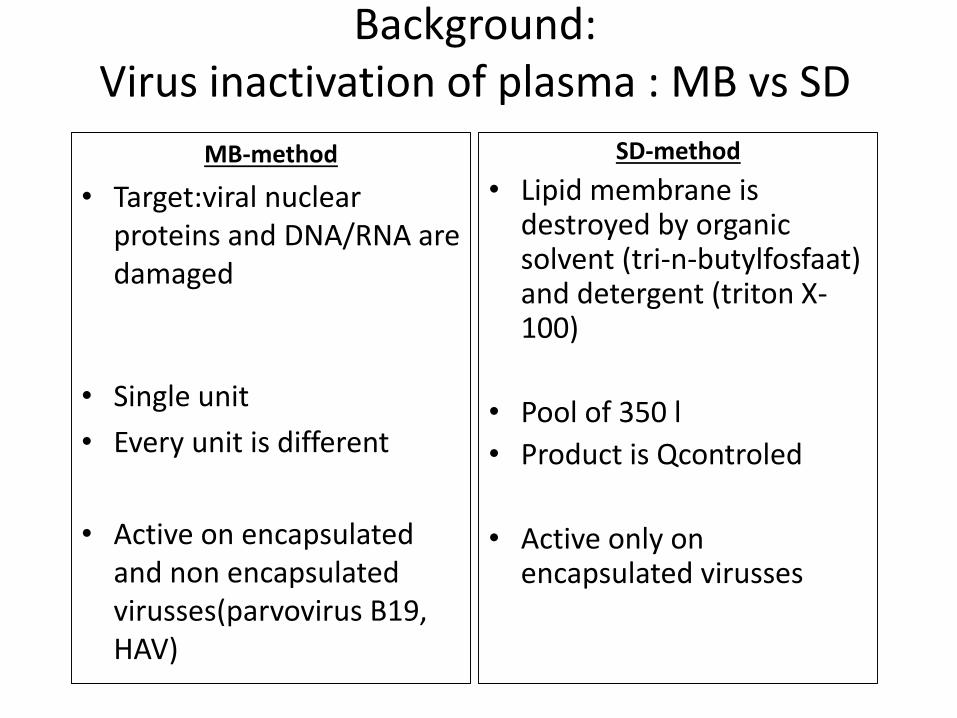
Background: Virus inactivation of plasma : MB vs SD
MB-method
• Target:viral nuclearproteins and DNA/RNA are damaged
• Single unit
• Every unit is different
• Active on encapsulatedand non encapsulatedvirusses(parvovirus B19, HAV)
SD-method
• Lipid membrane is destroyed by organicsolvent (tri-n-butylfosfaat)and detergent (triton X-100)
• Pool of 350 l
• Product is Qcontroled
• Active only onencapsulated virusses
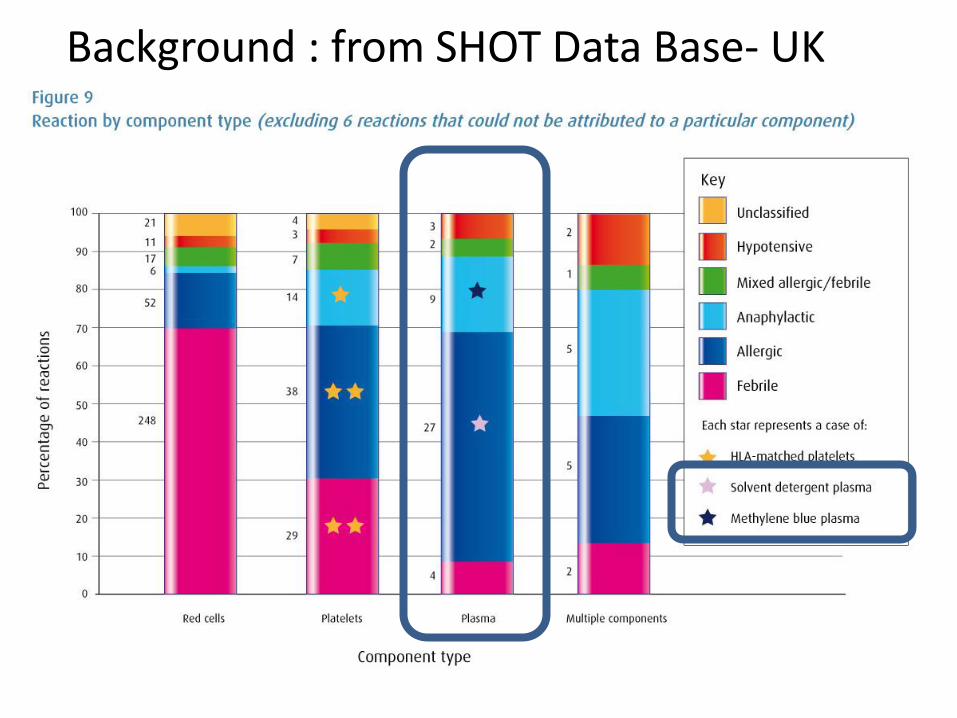
Background : from SHOT Data Base- UK
Background: France – ANSM*
• ‘In 2011, the French national drug regulatory agency ANSM (previously known as AFSSAPS) decided to progressively stop the clinical use of MB-treated plasma. One reason for this decision was a reported higher risk of severe allergic reactions for patients transfused with MB- treated plasma as compared to patients transfused with plasma treated with other PR methods [4]. ‘
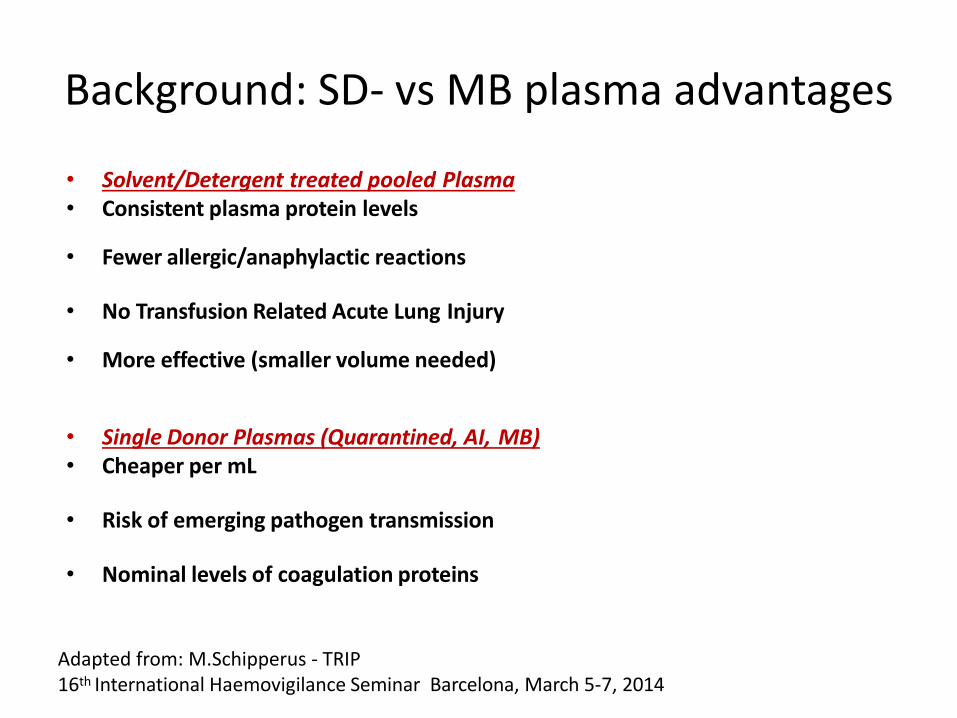
Background: SD- vs MB plasma advantages
• Solvent/Detergent treated pooled Plasma• Consistent plasma protein levels
• Fewer allergic/anaphylactic reactions
• No Transfusion Related Acute Lung Injury
• More effective (smaller volume needed)
• Single Donor Plasmas (Quarantined, AI, MB)• Cheaper per mL
• Risk of emerging pathogen transmission
• Nominal levels of coagulation proteins
Adapted from: M.Schipperus - TRIP 16th International Haemovigilance Seminar Barcelona, March 5-7, 2014
16th International Haemovigilance Seminar Barcelona, March 5-7, 2014
Indications and side effects of plasma and plasma products
The rate of allergic/anaphylactic reactions when transfusing
SDP is between 76% and 94% lower than that ofFFP*
*Krusius, Tom. "Pooled SD-pathogen inactivated FFP as an alternative to regular FFP", ESTM Course on
Appropriate use of plasma products, Zagreg, Croatia. 14-18 November 2012. Conference Presentation.
SDP vs. Q-FFP – advantages:
Solvent/Detergent treated pooled PlasmaConsistent plasma protein levels
Fewer allergic/anaphylactic reactions
No Transfusion Related Acute Lung Injury
More effective (smaller volume needed)
Single Donor Plasmas (Quarantined, AI, MB)Cheaper per mL
M. Schipperus, MD/PhD
Nominal levels of coagulation proteins
International, prospective haemovigilance
study on methylene blue-treated plasmaBackground and objectives Methylene blue is a phenothiazine dye, which in
combination with visible light has virucidal and bactericidal properties, disrupting the
replication of a broad range of enveloped viruses and some non-enveloped viruses.
The study objective was to collect data on adverse reactions occurring with
methylene blue plasma administered in a routine clinical practice environment and
document their characteristics and severity.
Materials and methods This was an open label, multicentre, non-controlled,
non- randomized, non-interventional study. Patients who receive a methylene blue
plasma transfusion were observed for any signs and symptoms (adverse reactions)
within 24 hs after the start of the transfusion, in different hospitals for a study
duration of at least 1 year.
Results A total of 19 315 methylene blue plasma units were transfused. There were
eight patients with adverse reactions recorded during the study, one of them serious.
Two had more than one reaction (two and four, respectively). Three patients had
previous transfusions with methylene blue plasma only.
Conclusion
Methylene blue plasma has a very acceptable safety profile with a rate of serious
adverse reactions of 0·5/10 000 units.
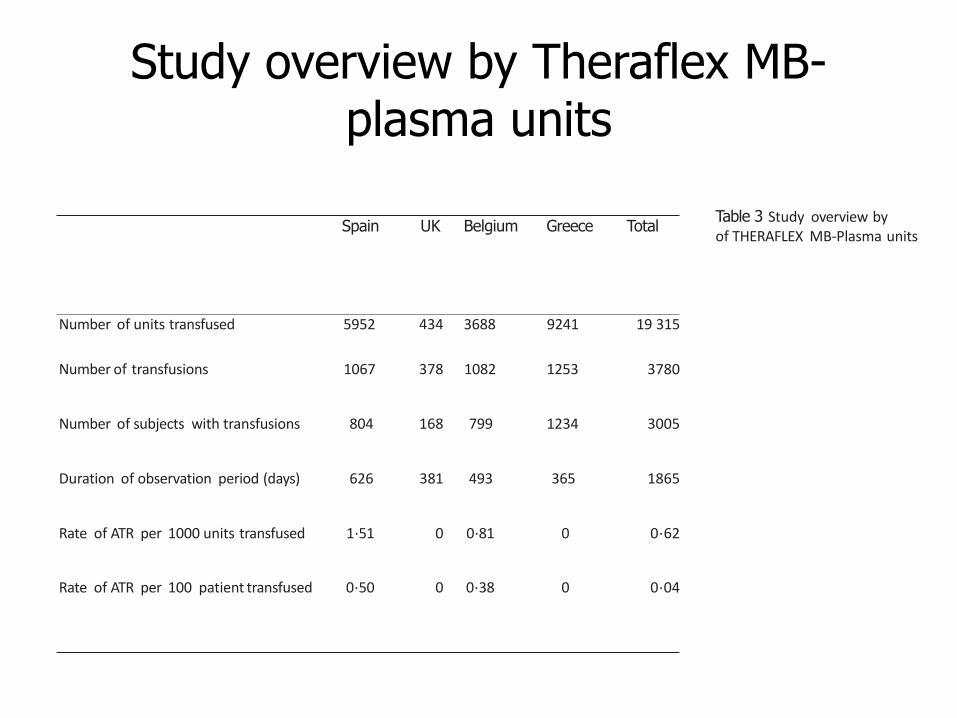
Study overview by Theraflex MB-plasma units
Spain UK Belgium Greece TotalTable 3 Study overview byof THERAFLEX MB-Plasma units
Number of units transfused 5952 434 3688 9241 19 315
Number of transfusions 1067 378 1082 1253 3780
Number of subjects with transfusions 804 168 799 1234 3005
Duration of observation period (days) 626 381 493 365 1865
Rate of ATR per 1000 units transfused 1·51 0 0·81 0 0·62
Rate of ATR per 100 patient transfused 0·50 0 0·38 0 0·04
Annualized transfusion reaction rate:
No. of transfused units/transfusion episodes with at least one transfusion reaction
over the whole observation period×365·24
Duration of observational period [days]
Country Year Total units SATR/10 000
Austria, Belgium,
France, Greece, Spain,
UK [12]
2007–2011 1 547 105 0·2
France (ANSM) [13] 2008–2012 750 564 0·3–1·0France [14] 2000–2011 10 283 1·0
Greece [15] 2001–2011 132 325 0
Austria [16] 2009–2014 23 920 0
United Kingdom [17, 20] 2012–2013 29 441 0·6–0·7
Belgium [18, 19] 2012–2013 150 322 0·2–1·0
Belgium, Greece, Spain
and UK (this study)
2013–2015 19 315 0·5
Country Year System Total Units SATR/10 000
France (ANSM) [13] 2008–2012 Quarantine 265 460 0·1–0·3
Amotosalen 298 856 0·3–0·8
Solvent-Detergent 535 490 0·3–0·5
France [14] 2000–2011 Quarantine 40 631 0·2
Amotosalen 36 035 0·6
Solvent-Detergent 19 015 0·0
Greece [15] 2001–2011 Quarantine 314 895 0·7Austria [16] 2009–2014 Quarantine 32 217 0·2
United Kingdom [17, 20] 2012–2013 Quarantine 549 053 1·0–1·1
United Kingdom [17, 20] 2012–2013 Solvent-Detergent 157 142 0·1–0·3
.
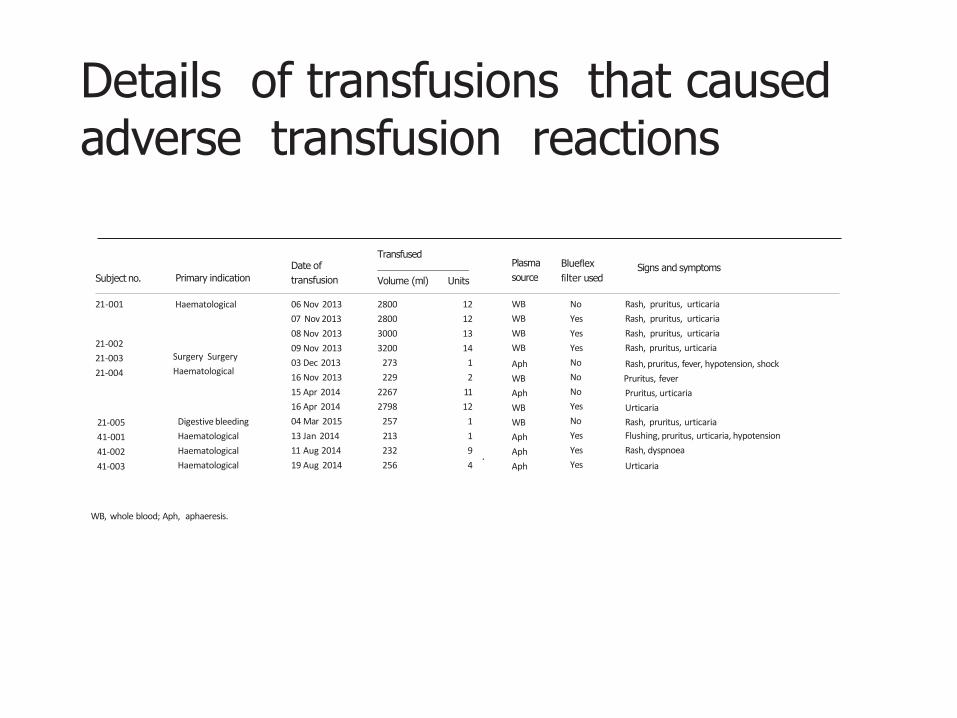
Details of transfusions that caused adverse transfusion reactions
Subject no. Primary indication
Date of
transfusion
Plasma
source
Blueflex
filter usedSigns and symptoms
Transfused
Volume (ml) Units
21-001 Haematological
21-002
21-003
21-004
Surgery Surgery
Haematological
21-005
41-001
41-002
41-003
Digestive bleeding
Haematological
Haematological
Haematological
06 Nov 2013
07 Nov 2013
08 Nov 2013
09 Nov 2013
03 Dec 2013
16 Nov 2013
15 Apr 2014
16 Apr 2014
04 Mar 2015
13 Jan 2014
11 Aug 2014
19 Aug 2014
2800
2800
3000
3200
273
229
2267
2798
257
213
232
256
12
12
13
14
1
2
11
12
1
1
9
4
WB
WB
WB
WB
Aph
WB
Aph
WB
WB
Aph
Aph
Aph
No
Yes
Yes
Yes
No
No
No
Yes
No
Yes
Yes
Yes
Rash, pruritus, urticaria
Rash, pruritus, urticaria
Rash, pruritus, urticaria
Rash, pruritus, urticaria
Rash, pruritus, fever, hypotension, shock
Pruritus, fever
Pruritus, urticaria
Urticaria
Rash, pruritus, urticaria
Flushing, pruritus, urticaria, hypotension
Rash, dyspnoea
Urticaria
WB, whole blood; Aph, aphaeresis.
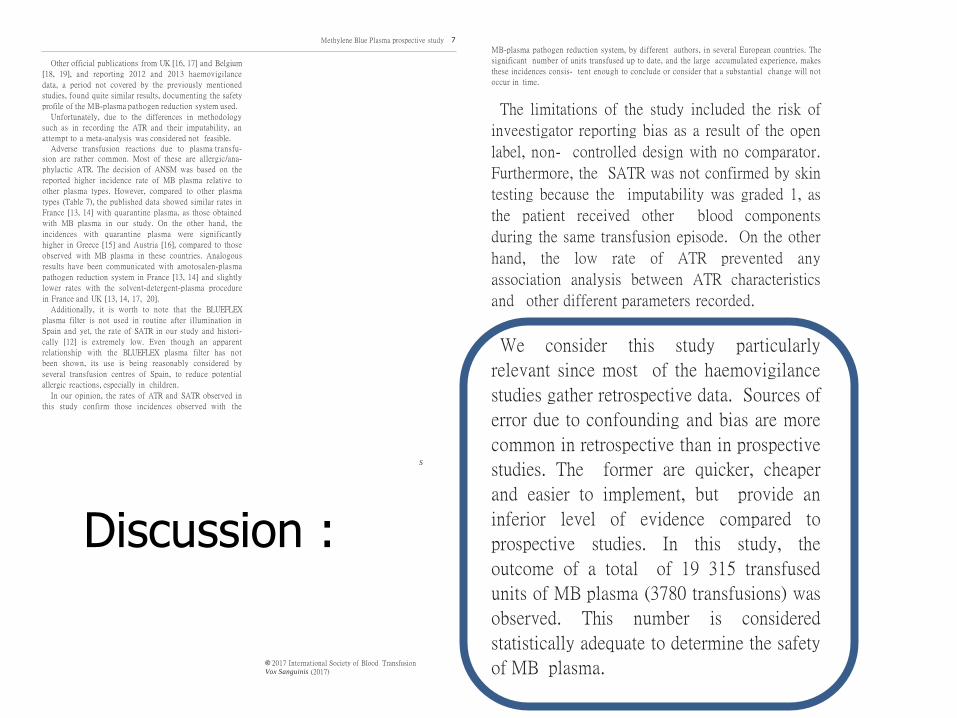
Other official publications from UK [16, 17] and Belgium
[18, 19], and reporting 2012 and 2013 haemovigilance
data, a period not covered by the previously mentioned
studies, found quite similar results, documenting the safety
profile of the MB-plasma pathogen reduction system used.
Unfortunately, due to the differences in methodology
such as in recording the ATR and their imputability, an
attempt to a meta-analysis was considered not feasible.
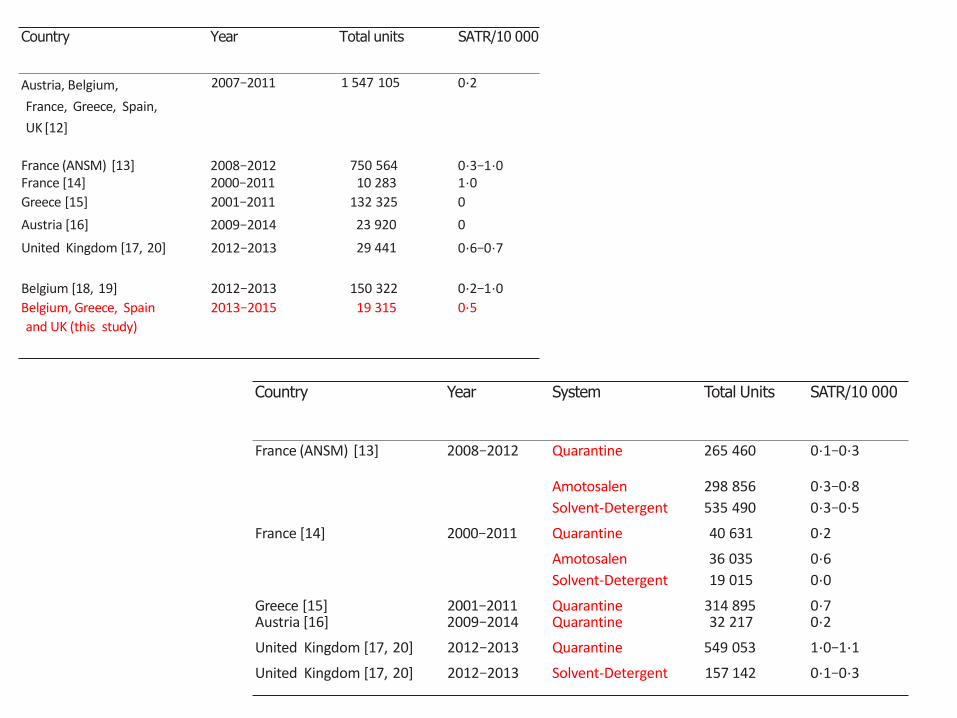
Adverse transfusion reactions due to plasma transfu-sion are rather common. Most of these are allergic/ana-
phylactic ATR. The decision of ANSM was based on the
reported higher incidence rate of MB plasma relative to
other plasma types. However, compared to other plasma
types (Table 7), the published data showed similar rates in
France [13, 14] with quarantine plasma, as those obtained
with MB plasma in our study. On the other hand, the
incidences with quarantine plasma were significantly
higher in Greece [15] and Austria [16], compared to those
observed with MB plasma in these countries. Analogous
results have been communicated with amotosalen-plasma
pathogen reduction system in France [13, 14] and slightly
lower rates with the solvent-detergent-plasma procedure
in France and UK [13, 14, 17, 20].
Additionally, it is worth to note that the BLUEFLEX
plasma filter is not used in routine after illumination in
Spain and yet, the rate of SATR in our study and histori-
cally [12] is extremely low. Even though an apparent
relationship with the BLUEFLEX plasma filter has not
been shown, its use is being reasonably considered by
several transfusion centres of Spain, to reduce potential
allergic reactions, especially in children.
In our opinion, the rates of ATR and SATR observed in
this study confirm those incidences observed with the
MB-plasma pathogen reduction system, by different authors, in several European countries. The
significant number of units transfused up to date, and the large accumulated experience, makes
these incidences consis- tent enough to conclude or consider that a substantial change will not
occur in time.
The limitations of the study included the risk of
inveestigator reporting bias as a result of the open
label, non- controlled design with no comparator.
Furthermore, the SATR was not confirmed by skin
testing because the imputability was graded 1, as
the patient received other blood components
during the same transfusion episode. On the other
hand, the low rate of ATR prevented any
association analysis between ATR characteristics
and other different parameters recorded.
We consider this study particularly
relevant since most of the haemovigilance
studies gather retrospective data. Sources of
error due to confounding and bias are more
common in retrospective than in prospective
studies. The former are quicker, cheaper
and easier to implement, but provide an
inferior level of evidence compared to
prospective studies. In this study, the
outcome of a total of 19 315 transfused
units of MB plasma (3780 transfusions) was
observed. This number is considered
statistically adequate to determine the safety
of MB plasma.
S
© 2017 International Society of Blood TransfusionVox Sanguinis (2017)
Methylene Blue Plasma prospective study 7
Discussion :
Related Documents



![Welkom, HIV Monitoring Part 7 - Health[e]Foundation...Stichting Rode Kruis Bloedbank Dag 1, deel 1: “Update, HIV behandeling” 19.00-19.05 Opening NASKHO 19.05-19.15 Opening ASNA](https://static.cupdf.com/doc/110x72/60426fc15d838a12ef7ced14/welkom-hiv-monitoring-part-7-healthefoundation-stichting-rode-kruis-bloedbank.jpg)







