JHT READ FOR CREDIT ARTICLE #322. Scientific/Clinical Article Swing traction versus no-traction for complex intra-articular proximal inter-phalangeal fractures Lisa J. O’Brien PhD, MClSc (Hand & Upper Limb Rehabilitation), BAppSc (Occupational Therapy) a, b, * , Andrew T. Simm MBBS c , Ian W.H. Loh MBBS d , Kim M. Griffiths BOccThy e a Department of Occupational Therapy, The Alfred, Melbourne, Victoria, Australia b Department of Occupational Therapy, Monash University, Melbourne, Victoria, Australia c Plastic and Reconstructive Unit, Melbourne Health, Melbourne, Victoria, Australia d Department of Plastic Surgery, The Alfred, Melbourne, Victoria, Australia e Department of Occupational Therapy, Monash Health, Melbourne, Victoria, Australia article info Article history: Received 24 March 2014 Received in revised form 15 July 2014 Accepted 15 July 2014 Available online 23 July 2014 Keywords: Dislocation Finger Fracture Orthosis Traction Introduction: Traction orthoses are thought to optimize recovery from intra-articular finger fractures by restoring joint space and allowing early motion. Evidence to date has, however, consisted only of case series. Purpose of the study: To compare swing traction versus no-traction management of complex fractures of proximal inter-phalangeal (PIP) finger joints. We hypothesized that there is no long-term (i.e. >12 month) difference between swing traction and no-traction (with or without surgical fixation) in terms of motion, pain, function, patient satisfaction, or treatment cost. Methods: Adults with a history of complex PIP fractures affecting 30% of articular surface injury were identified from database searches at three public hospitals and a private clinic and invited to participate. X-rays taken at the time of injury were graded by two blinded assessors, and participants attended a clinic for measurement of range of motion (ROM) and self-reported function, pain, and satisfaction at least one year post injury. Participant data were then were grouped by treatment provided. One group (N ¼ 17) was treated with swing traction and the other group (N ¼ 14) had no-traction. The primary outcome was combined motion of the PIP and distal inter-phalangeal (DIP) joints, expressed as both total active motion and Strickland score. Secondary outcomes were physical function and symptoms as measured by the Disabilities of Arm, Shoulder and Hand (DASH), patient satisfaction, pain, complication rates, and cost of treatment, based on mean resource consumption per group. Results: Patients treated with swing traction had greater finger motion than those in the no-traction group, which was statistically and clinically significant. There were no differences in patient ratings of function, pain or satisfaction. Complications, such as swan-neck deformity, cold sensitivity, malunion, infection, or adhesions occurred in over half of both groups of participants. During the treatment phase, the swing traction group attended hand therapy an average of 13.3 times, and the no-traction group attended 11.7 times. Average costs for swing tractionwere less than for surgical fixation with no-traction. Discussion: The significantly different range of motion found in our study did not translate to better DASH scores. The DASH is designed to measure global upper limb physical functioning and symptoms, but lacks sensitivity in populations with finger injuries. Conclusions: Patients treated with the swing traction protocol had greater range of motion in the finger, however this did not translate to improved patient ratings of function, pain or satisfaction. A basic cost comparison indicated that swing traction may be less expensive than other forms of surgical repair. Level of evidence: 3. Crown Copyright Ó 2014 Published by Elsevier Inc. on behalf of Hanley & Belfus, an imprint of Elsevier Inc. All rights reserved. Grant & financial support: 2009 Victorian Occupational Therapy Trust Research Grant ($4,000AUD). We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated. The manuscript submitted does not contain information about medical device(s). * Corresponding author. Monash University, P.O. Box 527, Frankston, Victoria 3199 Australia. Tel.: þ61 3 9904 4100; fax: þ61 3 99044613. E-mail address: [email protected] (L.J. O’Brien). Contents lists available at ScienceDirect Journal of Hand Therapy journal homepage: www.jhandtherapy.org 0894-1130/$ e see front matter Crown Copyright Ó 2014 Published by Elsevier Inc. on behalf of Hanley & Belfus, an imprint of Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jht.2014.07.003 Journal of Hand Therapy 27 (2014) 309e316

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

lable at ScienceDirect
Journal of Hand Therapy 27 (2014) 309e316
Contents lists avai
Journal of Hand Therapy
journal homepage: www.jhandtherapy.org
JHT READ FOR CREDIT ARTICLE #322.Scientific/Clinical Article
Swing traction versus no-traction for complex intra-articularproximal inter-phalangeal fractures
Lisa J. O’Brien PhD, MClSc (Hand & Upper Limb Rehabilitation), BAppSc (Occupational Therapy) a,b,*,Andrew T. Simm MBBS c, Ian W.H. Loh MBBS d, Kim M. Griffiths BOccThy e
aDepartment of Occupational Therapy, The Alfred, Melbourne, Victoria, AustraliabDepartment of Occupational Therapy, Monash University, Melbourne, Victoria, Australiac Plastic and Reconstructive Unit, Melbourne Health, Melbourne, Victoria, AustraliadDepartment of Plastic Surgery, The Alfred, Melbourne, Victoria, AustraliaeDepartment of Occupational Therapy, Monash Health, Melbourne, Victoria, Australia
a r t i c l e i n f o
Article history:Received 24 March 2014Received in revised form15 July 2014Accepted 15 July 2014Available online 23 July 2014
Keywords:DislocationFingerFractureOrthosisTraction
Grant & financial support: 2009 Victorian OccupatGrant ($4,000AUD). We certify that no party having athe research supporting this article has or will conforganization with which we are associated. The macontain information about medical device(s).
0894-1130/$ e see front matter Crown Copyright � 2http://dx.doi.org/10.1016/j.jht.2014.07.003
Introduction: Traction orthoses are thought to optimize recovery from intra-articular finger fractures byrestoring joint space and allowing early motion. Evidence to date has, however, consisted only of caseseries.Purpose of the study: To compare swing traction versus no-traction management of complex fractures ofproximal inter-phalangeal (PIP) finger joints. We hypothesized that there is no long-term (i.e. >12month) difference between swing traction and no-traction (with or without surgical fixation) in terms ofmotion, pain, function, patient satisfaction, or treatment cost.Methods: Adults with a history of complex PIP fractures affecting �30% of articular surface injury wereidentified from database searches at three public hospitals and a private clinic and invited to participate.X-rays taken at the time of injury were graded by two blinded assessors, and participants attended aclinic for measurement of range of motion (ROM) and self-reported function, pain, and satisfaction atleast one year post injury. Participant data were then were grouped by treatment provided. One group(N ¼ 17) was treated with swing traction and the other group (N ¼ 14) had no-traction. The primaryoutcome was combined motion of the PIP and distal inter-phalangeal (DIP) joints, expressed as both totalactive motion and Strickland score. Secondary outcomes were physical function and symptoms asmeasured by the Disabilities of Arm, Shoulder and Hand (DASH), patient satisfaction, pain, complicationrates, and cost of treatment, based on mean resource consumption per group.Results: Patients treated with swing traction had greater finger motion than those in the no-tractiongroup, which was statistically and clinically significant. There were no differences in patient ratings offunction, pain or satisfaction. Complications, such as swan-neck deformity, cold sensitivity, malunion,infection, or adhesions occurred in over half of both groups of participants. During the treatment phase,the swing traction group attended hand therapy an average of 13.3 times, and the no-traction groupattended 11.7 times. Average costs for swing traction were less than for surgical fixation with no-traction.Discussion: The significantly different range of motion found in our study did not translate to better DASHscores. The DASH is designed to measure global upper limb physical functioning and symptoms, but lackssensitivity in populations with finger injuries.Conclusions: Patients treated with the swing traction protocol had greater range of motion in the finger,however this did not translate to improved patient ratings of function, pain or satisfaction. A basic costcomparison indicated that swing traction may be less expensive than other forms of surgical repair.Level of evidence: 3.Crown Copyright � 2014 Published by Elsevier Inc. on behalf of Hanley & Belfus, an imprint of Elsevier
Inc. All rights reserved.
ional Therapy Trust Researchdirect interest in the results ofer a benefit on us or on anynuscript submitted does not
* Corresponding author. Monash University, P.O. Box 527, Frankston, Victoria 3199Australia. Tel.: þ61 3 9904 4100; fax: þ61 3 99044613.
E-mail address: [email protected] (L.J. O’Brien).
014 Published by Elsevier Inc. on behalf of Hanley & Belfus, an imprint of Elsevier Inc. All rights reserved.

L.J. O’Brien et al. / Journal of Hand Therapy 27 (2014) 309e316310
Introduction statistical purity of randomized controlled trials, results can be bothscientifically rigorous and more relevant to clinicians than a stan-
Intra-articular fracture dislocations of the finger commonlyinvolve the base of the middle phalanx usually in impaction,dislocation, and pilon types of injuries.1 The typical injury mecha-nism is a direct force applied to the fingertip with hyperextensionand axial loading of the proximal inter-phalangeal (PIP) jointcausing impaction of the articular surface of the middle phalanxonto the condyles of the proximal phalanx. The incidence of theseinjuries is estimated at 19% of phalangeal fractures, with commi-nuted or large-fragment PIP joint injuries comprising 2.2% of thetotal.2
Unstable PIP joint dislocations, and those with significantcomminution or fragment displacement, are usually treated sur-gically.3 Surgical options include internal fixation (usually screwsinto fracture fragments, with or without bone grafts4) percuta-neous pinning,5 or external fixation and traction.4 Internal fixationis technically difficult, time consuming, and can result in significantcomplications.6,7 Traction is less technically demanding as it canrequire as little as one percutaneous k-wire. As it does not require asurgical incision, the potential for complication and development ofscar tissue is also reduced. Traction is thought to work by reducingthe fracture by capsulo-ligamentotaxis, defined as the realigning offracture fragments as a result of tension applied across the fractureby the surrounding soft tissue8 and preventing shortening ofcollateral ligaments. Early motion aims to minimize adhesions inand around the joint, and promote cartilage healing.4
Several different types of traction devices that allow movementat the affected joint have been described. For ease of discussionthese can be classified as either finger-based frames (such as theSuzuki frame,9e14 or the S-quattro,6,15) or dynamic orthoses with aforearm or hand component. Of the latter group, the original“banjo” orthosis was first described in 1946,16 with severalimprovements since described, including the Schenck design17
which allowed passive mobilization between two points on acircular frame. More recently, “swing” orthoses which hinge at thelevel of the injured joint have been recommended, with designersclaiming that their smaller size minimally impacts on daily routine,improves compliance and allows pain-free rehabilitation.18,19 Theseassertions have, however, been challenged in a qualitative study ofpatients undergoing this treatment.20 A review of all publicationson swing traction undertaken for this study found that, apart fromtwo case series of 14 and 5 patients respectively,19,21 all are practiceforums which describe the orthosis’ design and fabrication, but donot present any patient data. Apart from a small 1991 study7
(comparing open reduction (N ¼ 9), banjo traction (N ¼ 6),Schenck orthosis (N ¼ 1), and no-traction (N ¼ 4) at an average of25months post injury) and a conference abstract for a single-centerretrospective analysis of 41 patients treated with either a Suzukiframe or amodified Banjo orthosis,22 there are no published clinicaltrials comparing any of the skeletal traction treatments with analternative treatment. Neither study described how participantswere allocated to treatment, nor did they provide statistical ana-lyzes between groups. Also, with the exception of one case seriesthat reviewed patients at an average of 56 months post injury,9 nostudies have included the long-term follow up of patients necessaryto identify the impact of post-traumatic arthrosis on finger pain,stiffness, and function.
Given the injury’s low incidence, and resulting difficultyrecruiting adequate sample sizes, it is not surprising that there areno prospective clinical trials into the efficacy of traction treatment.In similarly rare health conditions, there is a growing trend to useobservational studies, often referred to as comparative effective-ness research (CER) to directly compare the results of differenttreatment regimens.23 Whilst observational studies lack the
dard clinical trial providing key variables in comparison groups areeither matched at baseline or controlled for in analysis.
Our study aimed to compare outcomes by treatment type inpatients who had sustained complex PIP fractures at least one yearpreviously. One group of patients (from one hospital) were treatedwith swing traction; the other (including patients from the firsthospital and three other centers) had no-traction. We hypothesizedthat there would be no difference between groups in terms ofmotion, pain, function, patient satisfaction, and incidence ofcomplications.
Materials and methods
This cohort study involved patients from three public hospitalsand one private clinic located in Melbourne, Australia. Data wascollected between 2009 and 2014 and the study was approved bythe Ethics Committees of Monash University, the Alfred Hospital,andMonash Health. Potentially eligible participants were identifiedby searches of all involved centers’ hand surgery databases usingICD codes specific to finger fractures and dislocations. The first orthird author then checked patients’ x-rays and medical files toensure inclusion criteria were met. Those eligible were contactedby mail and telephone (where possible) and invited to participate.Informed consent was obtained in writing prior to data collection.
Inclusion criteria
Patients eligible for this trial were adults aged >18 years with adiagnosis of complex, comminuted, or unstable intra-articularfracture of the PIP joint sustained at least one year previously.They also needed to be able to give informed written consent inEnglish.
Exclusion criteria
Those with co-existing rheumatologic illness were excluded.
Interventions at the time of injurySwing traction group. All participants in this group came from onlyone of the study hospitals (the others did not offer traction at thetime of the patient’s injury). Prior to surgery, the hand therapistfabricated a thermoplastic forearm/hand componentwith amovablehinged outrigger attached at the level of the injured joint. Theoutrigger was covered at the distal end with thermoplastic materialin which two dressmaker’s hooks were embedded. After surgicalplacement of a K-wire through the bone distal to the injured joint,the orthosis was applied to the patient, with rubber bands attachingthe K-wire to the hooks in the outrigger, thus providing a distractionforce. Early designs were dorsally applied, however in later cases, avolar design was used as it provided greater stability (Figs. 1 and 2).The treating surgeon checked reduction radiographically to ensuretraction was sufficient to restore normal joint space. Distractionforces were not routinely measured, as this would be consideredunreliable due to the tendency for rubber bands to attenuate afterprolonged stretch. X-rays were repeated weekly, and tractionadjusted by changing the size and number of rubber bands requiredto maintain joint space. The hand therapist instructed the patient tocomplete 10 passive flexion/extension exercises of the injured jointeach hour, and this was commenced immediately post-surgery. Atthe end of the first week the aimwas to produce 45� of motion, withincremental increases of 5� per week for the next five weeks. Thepatient was instructed to wear the orthosis continuously until thesurgeon removed the k-wire. K-wires were removed between 30
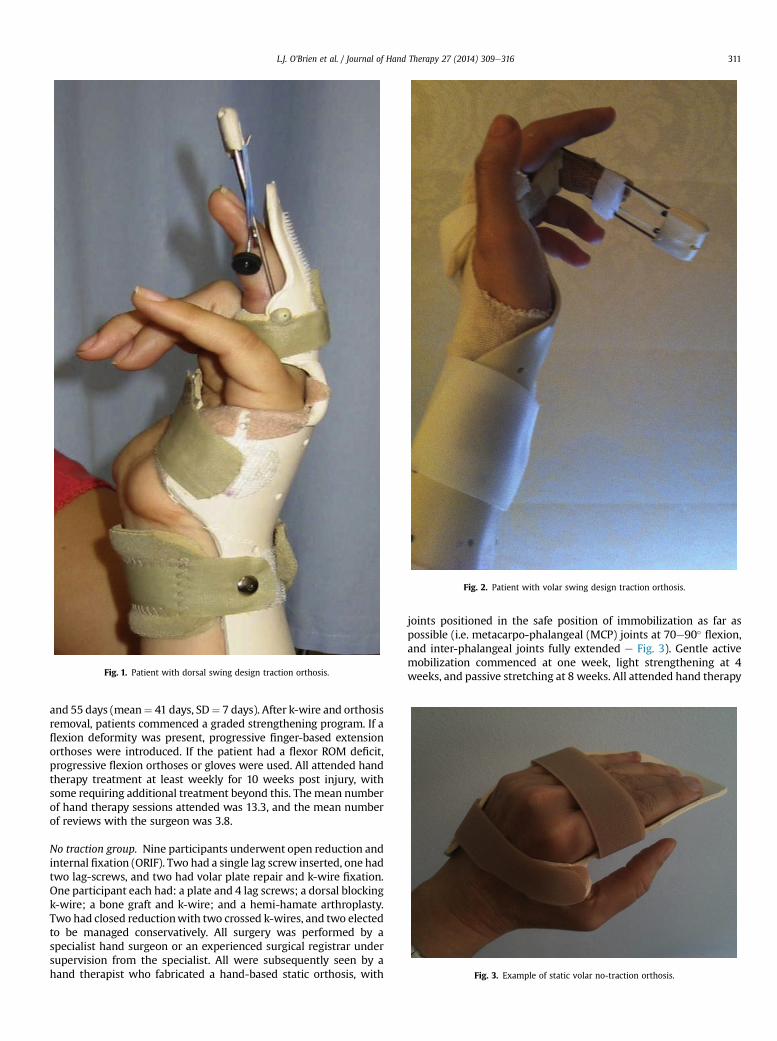
Fig. 2. Patient with volar swing design traction orthosis.
Fig. 1. Patient with dorsal swing design traction orthosis.
Fig. 3. Example of static volar no-traction orthosis.
L.J. O’Brien et al. / Journal of Hand Therapy 27 (2014) 309e316 311
and 55 days (mean¼ 41 days, SD¼ 7 days). After k-wire and orthosisremoval, patients commenced a graded strengthening program. If aflexion deformity was present, progressive finger-based extensionorthoses were introduced. If the patient had a flexor ROM deficit,progressive flexion orthoses or gloves were used. All attended handtherapy treatment at least weekly for 10 weeks post injury, withsome requiring additional treatment beyond this. The mean numberof hand therapy sessions attended was 13.3, and the mean numberof reviews with the surgeon was 3.8.
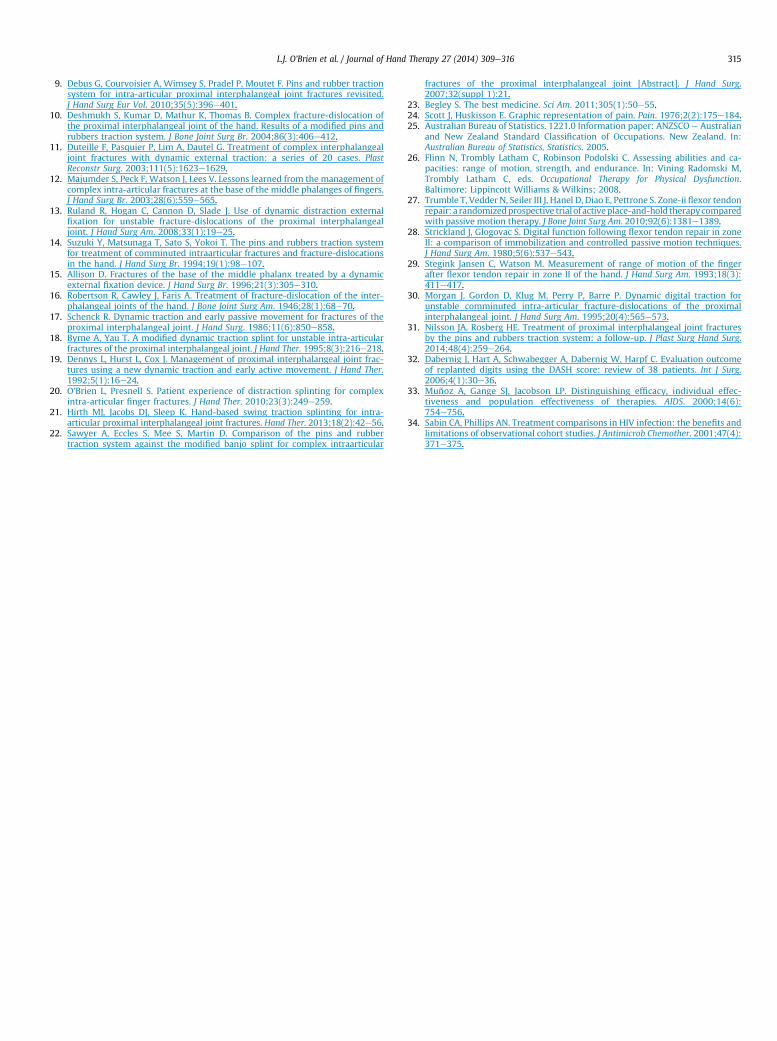
No traction group. Nine participants underwent open reduction andinternal fixation (ORIF). Two had a single lag screw inserted, one hadtwo lag-screws, and two had volar plate repair and k-wire fixation.One participant each had: a plate and 4 lag screws; a dorsal blockingk-wire; a bone graft and k-wire; and a hemi-hamate arthroplasty.Two had closed reductionwith two crossed k-wires, and two electedto be managed conservatively. All surgery was performed by aspecialist hand surgeon or an experienced surgical registrar undersupervision from the specialist. All were subsequently seen by ahand therapist who fabricated a hand-based static orthosis, with
joints positioned in the safe position of immobilization as far aspossible (i.e. metacarpo-phalangeal (MCP) joints at 70e90� flexion,and inter-phalangeal joints fully extended e Fig. 3). Gentle activemobilization commenced at one week, light strengthening at 4weeks, and passive stretching at 8 weeks. All attended hand therapy

Table 1Demographic injury and treatment data
Swing traction group(N ¼ 17)
No traction group(N ¼ 14)
Age (years) 36.7 � 9.5 (25e60) 45.9 � 12.1 (22e68)Sex, male, n 11 10Follow up duration, months 32.6 � 20.1 (12e93) 39.7 � 22.6 (12e76)Days post injury to
treatment6 � 4 (0e12) 10 � 11.3 (0e30)
Dominant hand injured, n 6 3Ratio or CIF:FD 11:6 7:7% of articular surface
damaged39.6 � 10.7 (30e60) 41.6 � 10.1 (30e50)
Sports injury, n 12 10Injured finger Index, n 1 3
Middle, n 5 1Ring, n 6 1Little, n 5 9
Number of hand therapysessions received
13.3 � 3.83 11.73 � 7.52
Number of reviews withsurgeon
3.83 � 1.33 3.36 � 1.02
Data are expressed as mean � standard deviation with range in parentheses unlessotherwise indicated. There were no statistically significant differences betweengroups at baseline on any injury, demographic, or treatment variable.CIF: Complex Intra-articular Fracture; FD: Fracture Dislocation.
L.J. O’Brien et al. / Journal of Hand Therapy 27 (2014) 309e316312
treatment at least weekly for 10 weeks post injury, with somerequiring additional treatment beyond this. Management ofextensor or flexor deficits was the same as for the swing tractiongroup. Those with k-wire fixation had the wires removed at a meanof 28 days post operatively. The mean number of hand therapysessions attended was 11.9 (11.3 for those treated conservatively),and the mean number of reviews with the surgeon was 3.4 (3.3 forthose treated conservatively).
Data collectionThe second and third authors, both hand surgery registrars (US
equivalent: senior/chief residents in surgery) blinded to treatmentgroup, independently graded participants’ pre-treatment x-rays.They estimated the percentage of articular surface affected, thencoded injuries as either Complex intra Articular Fracture (CIF) orfracture dislocation (FD). Inter-rater reliability was 85% on firstassessment and, where opinions differed, results were discussedand a consensus reached.
The first and fourth authors (experienced hand therapists)collected data from the participants regarding previous injuries tothe hand or finger, hand dominance, finger injured, pain (usingthe 10 cm Visual Analogue Scale24), satisfaction with result ofinjury (measured on a 5 point likert scale, with 1 ¼ very dissat-isfied and 5 ¼ very satisfied), and current employment status.25
Participants then completed the DASH, a 30 item self-reportfunctional outcome and symptom scale with a maximum scoreof 100 indicating an extreme impairment. The hand therapistmeasured active range of motion of PIP, and distal inter-phalangeal (DIP) joints using a 15 cm steel finger goniometerfollowing a standardized protocol with a dorsal approach.26
Therapists met prior to data collection to ensure consistency ofassessment technique and instrumentation. The first authorassessed participants from The Alfred, Eastern Health, and theprivate clinic, and the fourth author assessed those fromDandenong hospital. Raw scores for total arc of motion werecalculated by summing total flexion at PIP and DIP joints, withextension deficits at both joints subtracted from this figure. Themean clinically important difference (CID) of combined range ofmotion of the PIP and DIP joints was deemed to be 20�, as thisallows stronger grasp and easier release of items.27 Strickland’soriginal system for classifying finger movement was then used tocategorize range of movement outcome.28 This simplification ofthe Total Active Motion (TAM) system was originally designed toevaluate outcomes post flexor tendon injuries, but has been usedfor intra-articular PIP fractures.9 It does not include motion of themetacarpo-phalangeal joints, as this is usually not affected in PIPfractures and could therefore bias the measurement of the func-tional result. In this system, the total flexion minus the extensiondeficit (calculated as above) is then compared with a theoreticalfinger in which this value would be 175�. Results are classified (asa percentage score compared with 175�) into four categories:excellent (85e100%) good (70e84%) fair (50e69%) and poor(�49%).27 Strickland’s system is useful as it provides comparisonwith a norm, and the availability of a normal contralateral finger isnot a prerequisite for the measurement.29 Information regardingcomplications and further surgery was extracted from the pa-tient’s medical record, and verified with the patient in casetreatment was sought outside the original hospital.
In addition, a post-hoc analysis of average resource cost pertreatment was undertaken, encompassing the number of therapysessions and reviews with the surgeon, direct surgical and hospitalcosts, and orthosis fabrication cost. Calculations are based on in-formation supplied by the primary hospital’s Clinical CostingManager, and standard hourly pay rates for senior clinician thera-pists employed in public hospitals in Victoria, Australia.
Statistical methodsAn a-priori power analysis estimated that with 16 per group,
this study would have 80% power to detect a difference in range ofmotion equivalent to one standard deviationwith a 2-sided p-valueof 0.05. As we were unable to recruit 16 participants to the no-traction group, a post-hoc power calculation was conducted,finding that this study had 76.9% power to detect a difference be-tween groups on the primary outcome. All data were analyzedusing SPSS version 20 (SPSS Inc., Chicago, IL, USA). Group com-parisons were made using student t-tests for normally distributedvariables, and skewed data (e.g. DASH scores) were log transformedwhere necessary. For complications, the number of participants ineach group experiencing problems was expressed as a proportion.Data were then analyzed as the difference in proportions betweenthe two groups, and are presented as odds ratios with 95% confi-dence intervals. A two-sided p-value of 0.05 was considered to bestatistically significant.
Results
Forty-nine potentially eligible patients were identified fromdatabase searches of all study sites. We were unable to establishcontact with ten potentially eligible individuals, three were unableto consent (due to cognitive or language barriers) and five declinedto be involved. Thirty-one participants underwent evaluations bythe researchers, with all swing-traction participants recruited fromone hospital. The no-traction group included two individuals (onefrom the primary hospital, and one from a private clinic) whodeclined traction, but all others were from the second and thirdhospitals. Participant demographics and injury characteristics aresummarized in Table 1. All participants had returned to full timework, study, or home duties at the time of review. A summary ofresults is presented in Table 2.
Primary outcome: range of motion
The mean combined range of motion of the PIP and DIP in theswing traction group was 141.9�; in the no-traction group it was100.8�. This was statistically significant (p ¼ 0.008) and clinicallyimportant as it was double the mean CID of 20�. Strickland score
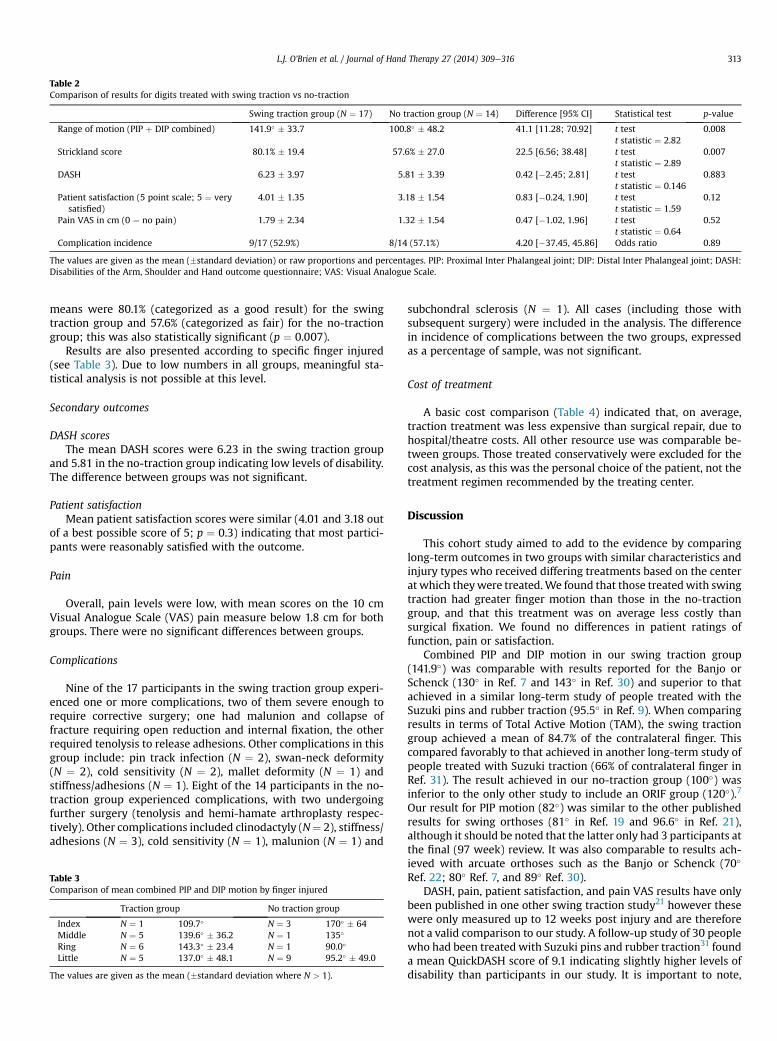
Table 2Comparison of results for digits treated with swing traction vs no-traction
Swing traction group (N ¼ 17) No traction group (N ¼ 14) Difference [95% CI] Statistical test p-value
Range of motion (PIP þ DIP combined) 141.9� � 33.7 100.8� � 48.2 41.1 [11.28; 70.92] t testt statistic ¼ 2.82
0.008
Strickland score 80.1% � 19.4 57.6% � 27.0 22.5 [6.56; 38.48] t testt statistic ¼ 2.89
0.007
DASH 6.23 � 3.97 5.81 � 3.39 0.42 [�2.45; 2.81] t testt statistic ¼ 0.146
0.883
Patient satisfaction (5 point scale; 5 ¼ verysatisfied)
4.01 � 1.35 3.18 � 1.54 0.83 [�0.24, 1.90] t testt statistic ¼ 1.59
0.12
Pain VAS in cm (0 ¼ no pain) 1.79 � 2.34 1.32 � 1.54 0.47 [�1.02, 1.96] t testt statistic ¼ 0.64
0.52
Complication incidence 9/17 (52.9%) 8/14 (57.1%) 4.20 [�37.45, 45.86] Odds ratio 0.89
The values are given as the mean (�standard deviation) or raw proportions and percentages. PIP: Proximal Inter Phalangeal joint; DIP: Distal Inter Phalangeal joint; DASH:Disabilities of the Arm, Shoulder and Hand outcome questionnaire; VAS: Visual Analogue Scale.
L.J. O’Brien et al. / Journal of Hand Therapy 27 (2014) 309e316 313
means were 80.1% (categorized as a good result) for the swingtraction group and 57.6% (categorized as fair) for the no-tractiongroup; this was also statistically significant (p ¼ 0.007).
Results are also presented according to specific finger injured(see Table 3). Due to low numbers in all groups, meaningful sta-tistical analysis is not possible at this level.
Secondary outcomes
DASH scoresThe mean DASH scores were 6.23 in the swing traction group
and 5.81 in the no-traction group indicating low levels of disability.The difference between groups was not significant.
Patient satisfactionMean patient satisfaction scores were similar (4.01 and 3.18 out
of a best possible score of 5; p ¼ 0.3) indicating that most partici-pants were reasonably satisfied with the outcome.
Pain
Overall, pain levels were low, with mean scores on the 10 cmVisual Analogue Scale (VAS) pain measure below 1.8 cm for bothgroups. There were no significant differences between groups.
Complications
Nine of the 17 participants in the swing traction group experi-enced one or more complications, two of them severe enough torequire corrective surgery; one had malunion and collapse offracture requiring open reduction and internal fixation, the otherrequired tenolysis to release adhesions. Other complications in thisgroup include: pin track infection (N ¼ 2), swan-neck deformity(N ¼ 2), cold sensitivity (N ¼ 2), mallet deformity (N ¼ 1) andstiffness/adhesions (N ¼ 1). Eight of the 14 participants in the no-traction group experienced complications, with two undergoingfurther surgery (tenolysis and hemi-hamate arthroplasty respec-tively). Other complications included clinodactyly (N¼ 2), stiffness/adhesions (N ¼ 3), cold sensitivity (N ¼ 1), malunion (N ¼ 1) and
Table 3Comparison of mean combined PIP and DIP motion by finger injured
Traction group No traction group
Index N ¼ 1 109.7� N ¼ 3 170� � 64Middle N ¼ 5 139.6� � 36.2 N ¼ 1 135�
Ring N ¼ 6 143.3� � 23.4 N ¼ 1 90.0�
Little N ¼ 5 137.0� � 48.1 N ¼ 9 95.2� � 49.0
The values are given as the mean (�standard deviation where N > 1).
subchondral sclerosis (N ¼ 1). All cases (including those withsubsequent surgery) were included in the analysis. The differencein incidence of complications between the two groups, expressedas a percentage of sample, was not significant.
Cost of treatment
A basic cost comparison (Table 4) indicated that, on average,traction treatment was less expensive than surgical repair, due tohospital/theatre costs. All other resource use was comparable be-tween groups. Those treated conservatively were excluded for thecost analysis, as this was the personal choice of the patient, not thetreatment regimen recommended by the treating center.
Discussion
This cohort study aimed to add to the evidence by comparinglong-term outcomes in two groups with similar characteristics andinjury types who received differing treatments based on the centerat which theywere treated.We found that those treatedwith swingtraction had greater finger motion than those in the no-tractiongroup, and that this treatment was on average less costly thansurgical fixation. We found no differences in patient ratings offunction, pain or satisfaction.
Combined PIP and DIP motion in our swing traction group(141.9�) was comparable with results reported for the Banjo orSchenck (130� in Ref. 7 and 143� in Ref. 30) and superior to thatachieved in a similar long-term study of people treated with theSuzuki pins and rubber traction (95.5� in Ref. 9). When comparingresults in terms of Total Active Motion (TAM), the swing tractiongroup achieved a mean of 84.7% of the contralateral finger. Thiscompared favorably to that achieved in another long-term study ofpeople treated with Suzuki traction (66% of contralateral finger inRef. 31). The result achieved in our no-traction group (100�) wasinferior to the only other study to include an ORIF group (120�).7
Our result for PIP motion (82�) was similar to the other publishedresults for swing orthoses (81� in Ref. 19 and 96.6� in Ref. 21),although it should be noted that the latter only had 3 participants atthe final (97 week) review. It was also comparable to results ach-ieved with arcuate orthoses such as the Banjo or Schenck (70�
Ref. 22; 80� Ref. 7, and 89� Ref. 30).DASH, pain, patient satisfaction, and pain VAS results have only
been published in one other swing traction study21 however thesewere only measured up to 12 weeks post injury and are thereforenot a valid comparison to our study. A follow-up study of 30 peoplewho had been treated with Suzuki pins and rubber traction31 founda mean QuickDASH score of 9.1 indicating slightly higher levels ofdisability than participants in our study. It is important to note,

Table 4Resource cost comparison
Swing traction No traction
Orthosis fabrication (based on current hospital fees for insured patients) $220 $90Therapy sessions (@$45/hr based on senior clinician hourly rate) 13.3 � $45 ¼ $598.50 11.7 � $45 ¼ $526.50Reviews with surgeons (@$105.55a) 3.8 � $105.55 ¼ $401.09 3.3 � $105.55 ¼ $348.32Mean surgery cost $2600.00 $3900.00Totals $3819.59 $4864.82
All costs are in Australian Dollars.a Medicare scheduled fee for consultation in consulting rooms.
L.J. O’Brien et al. / Journal of Hand Therapy 27 (2014) 309e316314
however, that that study’s mean time since surgery was 6.1 years,compared to our 2.8 years. All other studies used different methodsto classify pain so it is not possible to compare results for thesemeasures.
It is interesting that the significant difference in range of motionfound in our study did not translate to better DASH scores. TheDASH is designed to measure global upper limb physical func-tioning and symptoms, but its lack of sensitivity in populationswith finger injuries has led to calls for an additional digital mod-ule.32 It also does not consider hand dominance, and it is possiblethat participants, given the time since injury, adapted their dailyactivities to use their non-injured hand more. A search of theliterature revealed no finger-specific functional outcome scales thatcould be used for similar studies.
In terms of complications, our finding of complications in 52.9%of the swing traction group is higher than that reported in the otherstudy using this style of orthosis (42% in19), with pin track infection,swan-neck deformity, stiffness, and cold sensitivity being the keyissues reported. The other swing traction case series (N ¼ 5) notedcomplications in 2 cases (pin site infection and web spaceirritation).
Study limitations
Ideally, a study comparing two interventions would be con-ducted as a randomized controlled trial. This methodology wasconsidered unfeasible given the rarity of the injury and strongsurgeon and therapist preferences for particular treatment pro-tocols at the respective centers. We chose an observational cohortstudy where treatment was provided at the individual’s own cen-ter, however we ensured that assessors not involved in the treat-ment measured the outcomes. This allowed us to conduct ameasure of individual effectiveness in amethod similar to that usedin studies of treatments for other rare diseases.33 This comparisonis “unbiased if the groups have the same prognosis at baseline andare treated similarly during follow-up (except for differences thatare a direct consequence of whether the patient started regimen Aor B)”34(p372) As with all non-randomized studies, however, themajor disadvantage of our design was the inability to ensure thatgroups were equal at baseline on variables not measured, and thatall treatment variables (other than the presence of swing traction)were strictly controlled. In the no-traction group especially, therewas a variety of surgical treatment provided compared to thetraction group.
Unfortunately, numbers enrolled in our study were lower thanexpected, which may have limited our power to detect a differencebetween groups on some variables. Due to logistical issues associ-ated with the length of time in the recruitment phase, we wereunable to use a blinded assessor for range of motion however bothassessors met prior to the study to ensure they applied consistenttechnique and instruments. Finally, treatment was provided bydifferent hand surgery and therapy teams in the respective hospi-tals, introducing potentially confounding variables such as surgical
technique, and timing of mobilization commencement. Whilst thenumber of therapy sessions was comparable between groups, theintensity of therapy treatment is unknown.
In summary, there are many different methods for treatingcomplex intra-articular finger fractures, and in the absence ofstrong evidence from comparative studies, treatment is still basedon the experience, skill, and preference of individual surgeons andhand therapists.4,19 Research into this area has been difficult for thisreason, as well as the challenges involved in long-term follow-up ofpotential participants. Future research will need to be multi-centerto enable an adequate sample size, and should aim for consistenttreatment protocols within and across comparison groups.
Conclusion
This study showed statistically and clinically significant betterrange of motion in the swing traction group at a mean of 33monthspost injury, and basic cost analysis showed that this treatment maybe less expensive than surgical repair. The increased motion,however, did not translate to improved patient ratings of pain,satisfaction, or physical function. The lack of impact on functioningis most likely explained by the DASH’s lack of sensitivity in pop-ulations with single finger injuries. Complications, such as swan-neck deformity, cold sensitivity, malunion, infection, or adhesionsoccurred in over half of both groups of participants, reflecting thechallenging nature of these complex injuries. Long-term outcomes,in terms of low pain and high function, were encouraging in bothgroups.
Acknowledgments
The authors wish to acknowledge Ben Cunningham who pio-neered distraction treatment at The Alfred. We are also indebted toMarco Luthe (Alfred Health) and Philippa Harrison (MonashHealth) for additional costing and treatment data.
References
1. Combs J. It’s not “Just a Finger”. J Athl Train. 2000;35(2):168e178.2. O’Rourke S, Gaura S, Bartona N. Long-term outcome of articular fractures of the
phalanges: an eleven year follow up. J Hand Surg Br. 1989;14(2):183e193.3. Scougall P, Prosser R. Metacarpal and phalangeal fractures. In: Prosser R,
Conolly W, eds. Rehabilitation of the Hand and Upper Limb. Eastbourne:Butterworth-Heinemann; 2003.
4. Ng C, Oliver C. Fractures of the proximal interphalangeal joints of the fingers.J Bone Joint Surg Br. 2009;91(6):705e712.
5. Vitale MA, White NJ, Strauch RJ. A percutaneous technique to treat unstabledorsal fractureedislocations of the proximal interphalangeal joint. J Hand Surg.2011;36(9):1453e1459.
6. Khan W, Fahmy N. The S-Quattro in the management of acute intraarticularphalangeal fractures of the hand. J Hand Surg Br. 2006;31(1):79e92.
7. Stern P, Roman R, Kiefhaber T, McDonough J. Pilon fractures of the proximalinterphalangeal joint. J Hand Surg. 1991;16(5):844e850.
8. Kissel CG, Husain ZS, Cottom JM, Scott RT, Vest J. Early clinical and radio-graphic outcomes after treatment of displaced intra-articular calcaneal frac-tures using delta-frame external fixator construct. J Foot Ankle Surg. 2011;50(2):135e140.
L.J. O’Brien et al. / Journal of Hand Therapy 27 (2014) 309e316 315
9. Debus G, Courvoisier A, Wimsey S, Pradel P, Moutet F. Pins and rubber tractionsystem for intra-articular proximal interphalangeal joint fractures revisited.J Hand Surg Eur Vol. 2010;35(5):396e401.
10. Deshmukh S, Kumar D, Mathur K, Thomas B. Complex fracture-dislocation ofthe proximal interphalangeal joint of the hand. Results of a modified pins andrubbers traction system. J Bone Joint Surg Br. 2004;86(3):406e412.
11. Duteille F, Pasquier P, Lim A, Dautel G. Treatment of complex interphalangealjoint fractures with dynamic external traction: a series of 20 cases. PlastReconstr Surg. 2003;111(5):1623e1629.
12. Majumder S, Peck F, Watson J, Lees V. Lessons learned from the management ofcomplex intra-articular fractures at the base of the middle phalanges of fingers.J Hand Surg Br. 2003;28(6):559e565.
13. Ruland R, Hogan C, Cannon D, Slade J. Use of dynamic distraction externalfixation for unstable fracture-dislocations of the proximal interphalangealjoint. J Hand Surg Am. 2008;33(1):19e25.
14. Suzuki Y, Matsunaga T, Sato S, Yokoi T. The pins and rubbers traction systemfor treatment of comminuted intraarticular fractures and fracture-dislocationsin the hand. J Hand Surg Br. 1994;19(1):98e107.
15. Allison D. Fractures of the base of the middle phalanx treated by a dynamicexternal fixation device. J Hand Surg Br. 1996;21(3):305e310.
16. Robertson R, Cawley J, Faris A. Treatment of fracture-dislocation of the inter-phalangeal joints of the hand. J Bone Joint Surg Am. 1946;28(1):68e70.
17. Schenck R. Dynamic traction and early passive movement for fractures of theproximal interphalangeal joint. J Hand Surg. 1986;11(6):850e858.
18. Byrne A, Yau T. A modified dynamic traction splint for unstable intra-articularfractures of the proximal interphalangeal joint. J Hand Ther. 1995;8(3):216e218.
19. Dennys L, Hurst L, Cox J. Management of proximal interphalangeal joint frac-tures using a new dynamic traction and early active movement. J Hand Ther.1992;5(1):16e24.
20. O’Brien L, Presnell S. Patient experience of distraction splinting for complexintra-articular finger fractures. J Hand Ther. 2010;23(3):249e259.
21. Hirth MJ, Jacobs DJ, Sleep K. Hand-based swing traction splinting for intra-articular proximal interphalangeal joint fractures. Hand Ther. 2013;18(2):42e56.
22. Sawyer A, Eccles S, Mee S, Martin D. Comparison of the pins and rubbertraction system against the modified banjo splint for complex intraarticular
fractures of the proximal interphalangeal joint [Abstract]. J Hand Surg.2007;32(suppl 1):21.
23. Begley S. The best medicine. Sci Am. 2011;305(1):50e55.24. Scott J, Huskisson E. Graphic representation of pain. Pain. 1976;2(2):175e184.25. Australian Bureau of Statistics. 1221.0 Information paper: ANZSCO e Australian
and New Zealand Standard Classification of Occupations. New Zealand. In:Australian Bureau of Statistics, Statistics. 2005.
26. Flinn N, Trombly Latham C, Robinson Podolski C. Assessing abilities and ca-pacities: range of motion, strength, and endurance. In: Vining Radomski M,Trombly Latham C, eds. Occupational Therapy for Physical Dysfunction.Baltimore: Lippincott Williams & Wilkins; 2008.
27. Trumble T, Vedder N, Seiler III J, Hanel D, Diao E, Pettrone S. Zone-ii flexor tendonrepair: a randomizedprospective trialof activeplace-and-hold therapycomparedwith passive motion therapy. J Bone Joint Surg Am. 2010;92(6):1381e1389.
28. Strickland J, Glogovac S. Digital function following flexor tendon repair in zoneII: a comparison of immobilization and controlled passive motion techniques.J Hand Surg Am. 1980;5(6):537e543.
29. Stegink Jansen C, Watson M. Measurement of range of motion of the fingerafter flexor tendon repair in zone II of the hand. J Hand Surg Am. 1993;18(3):411e417.
30. Morgan J, Gordon D, Klug M, Perry P, Barre P. Dynamic digital traction forunstable comminuted intra-articular fracture-dislocations of the proximalinterphalangeal joint. J Hand Surg Am. 1995;20(4):565e573.
31. Nilsson JA, Rosberg HE. Treatment of proximal interphalangeal joint fracturesby the pins and rubbers traction system: a follow-up. J Plast Surg Hand Surg.2014;48(4):259e264.
32. Dabernig J, Hart A, Schwabegger A, Dabernig W, Harpf C. Evaluation outcomeof replanted digits using the DASH score: review of 38 patients. Int J Surg.2006;4(1):30e36.
33. Muñoz A, Gange SJ, Jacobson LP. Distinguishing efficacy, individual effec-tiveness and population effectiveness of therapies. AIDS. 2000;14(6):754e756.
34. Sabin CA, Phillips AN. Treatment comparisons in HIV infection: the benefits andlimitations of observational cohort studies. J Antimicrob Chemother. 2001;47(4):371e375.
L.J. O’Brien et al. / Journal of Hand Therapy 27 (2014) 309e316316
JHT Read for CreditQuiz: #322
Record your answers on the Return Answer Form found on thetear-out coupon at the back of this issue or to complete onlineand use a credit card, go to JHTReadforCredit.com. There isonly one best answer for each question.
#1. The design of the study is
a. RCTsb. a case seriesc. a retrospective cohortd. a prospective cohort#2. In designing the study the authors hypothesized that therewould be ____________ between PIP fractures treated withswing traction and those with no traction
a. no long term difference in outcomesb. significantly better outcomesc. slightly better outcomesd. random differences#3. The authors found
a. less pain in the no-traction groupb. equal ROM in both groupsc. better function, but no better ROM, in the swing tractiongroupd. better ROM, but no better function, in the swing traction
group
#4. The swing traction apparatusa. was fabricated and applied entirely by a CHTb. was fabricated and applied by a certified orthotistc. required pin placement by a surgeond. was pre fabricated and then fitted by a CHT
#5. The complication rate was essentially the same in both groups
a. falseb. trueWhen submitting to the HTCC for re-certification, please batch yourJHT RFC certificates in groups of 3 or more to get full credit.
Related Documents











